Submitted:
14 October 2024
Posted:
15 October 2024
You are already at the latest version
Abstract
Despite the significant advancements in hearing aid technology, adoption rates remain low, with stigma continuing to be a major barrier. This review aims to systematically assess the origins and current state of hearing aid stigma, as well as explore potential strategies for allevi-ating it. The review examines societal perceptions, psychological impacts, and recent technolog-ical advancements that can influence hearing aid adoption and reduce stigma. Methods: A systematic review of literature from peer-reviewed journals and reputable sources was conducted, analyzing papers on hearing aid stigma, adoption rates, and technological solu-tions. The articles were categorized by their focus on either stigma causes, societal factors, or technological advancements aimed at improving adoption. Results: The review identifies stigma as a complex, multifaceted issue driven primarily by ageism, disability perception, and the association of hearing aids with aging and incapability. Despite technological improvements, the studies surveyed listed stigma as a major factor in non-adoption. Technological advancements such as artificial intelligence in sound processing, multifunctional features, and innovative design have shown potential in reducing stigma and improving user experience. Conclusions: Alleviating the stigma of hearing aids requires a multi-pronged approach, com-bining improvements in technology with changes in societal perceptions. Multifunctional devices, advanced signal processing, and aesthetic improvements can drive adoption, but broader public health campaigns and education are also essential to changing societal attitudes and fostering greater acceptance of hearing aids.
Keywords:
Hearing Aid
; Hearing Loss
; Adoption Rate
; Stigma
; Design
; Functionality
1. Introduction
The human sense of hearing is an extraordinary capability, allowing us to perceive and interpret a vast array of sounds from the environment, from the subtle rustling of leaves to the nuanced tones of speech and music. Our ears are sophisticated biological sensor systems that transduce sound waves into neural impulses (Figure 1). The ears and brain work in tandem to process these sounds effortlessly, enabling us to locate their sources, understand complex auditory signals, and even filter out background noise—all without conscious effort [1]. This remarkable sense operates continuously, often unnoticed, as we navigate through our daily lives, taking it for granted as long as it functions normally. It’s only when our hearing is impaired that we begin to appreciate its vital role in our connection to the world around us.
Hearing loss may be the world’s largest pandemic that many fail to notice, care about or mention. According to the World Health Organization, a staggering 1.5 billion people globally suffer from some type of hearing loss (≥20 dB elevated hearing thresholds at audible frequencies) [3]. Of these hearing-impaired population, nearly half a billion live with “disabling” hearing loss, meaning that to live a normal life, they require hearing assistance.
The prevalence of hearing loss, generally progressing with age, is a global phenomenon. A study on the prevalence of hearing impairment in the United States in 2019, according to age and severity, shows that approximately 30% of people in the age group of 50 to 59 years suffer from hearing loss, which increases to over 70% for the age group of 70 to 79 years, and exceeds 85% for people over 80 years [4]. As another example, Figure 2 shows the summary of a retrospective study of over 10,000 Japanese men and women, between 10 to 99 years of age, for their hearing loss evaluated by pure-tone audiometric tests spanning sound frequencies of 125 to 8,000 Hz [5]. This study, published in the Lancet Regional Health – Western Pacific, shows the steady progression of hearing loss with age, with worse hearing thresholds at higher sound frequencies in older ages.
Hearing loss, if left untreated, also has significant knock-on effects, or comorbidities. According to Hughes, et al., who conducted a comprehensive survey regarding the mental health impacts of hearing loss, untreated hearing loss forces those afflicted into social withdrawal, as they are therefore unable to participate in normal and routine conversations [6]. That social withdrawal coupled with the other cerebral detriments of hearing loss, such as dementia, could be one of the most significant causes for cognitive decline in elderly people [3,6]. Outside of mental health, hearing loss also has a proven comorbidity with obesity and cardiovascular diseases, as hearing-impaired persons are more likely to not participate in social events, and therefore become highly sedentary [7]. Patients with hearing impairment have been shown to suffer from increased risks of falls [8]. Not only does hearing loss drastically undermine the health of the hearing-impaired individuals, but because of its detriments to cognition and intelligence, 1 trillion “international dollars,” are lost because of it yearly, according to the World Health Organization [3]. Hearing loss, clearly, from a public health and economic perspective, could be one of the world’s most perilous conditions.
Sensorineural hearing loss (SNHL) is the most common form of hearing impairment, by some estimates accounting for nearly 90% of all hearing loss cases [9]. The other 10% is conductive hearing loss (CHL) of which earwax buildup is the most common subset, in addition to pathologies of the tympanic membrane and the middle ear structures [10]. Sensorineural hearing loss largely relates to either damages or de-innervation of the cilia hair cells that transform sounds to become understandable electrical signals that are relayed to the auditory cortex of the brain in the form of nerve impulses. Simply put, SNHL is derived from issues with the inner ear. Treatments for SNHL include both hearing aids and cochlear implants, but some estimates account for 80% of SNHL cases being treatable with hearing aids [9]. These patients have hearing loss that ranges from mild up to severe, accounting for more than 1 billion people [11]. The other 20% of SNHL patients could be cochlear implant candidates, that serve as an artificially innerved cochlea, implanted into the inner ear. Cochlear implants are a great solution for those who are severely or profoundly deaf, yet because of their narrow patient focus and significantly higher costs due to surgical procedures, they are not as ubiquitous as hearing aids [9].
As depicted in Figure 3, at their inception, hearing aids were rudimentary and mechanical systems, relying on passive amplification techniques. The ear trumpet of Madame de Meuron, for example, was a simple, funnel-shaped device that captured sound and directed it into the ear, while Frederick Rein's acoustic chair for King John VI of Portugal incorporated hidden sound-collecting tubes into a piece of furniture, allowing the user to hear conversations more clearly without the need for a conspicuous device. The mid-20th century marked a major milestone with the advent of body-worn hearing aids utilizing vacuum tube technology, a significant leap in portable amplification devices around 1940s. This was further refined by the 1970s with the introduction of transistor-based body-worn hearing aids, which offered greater miniaturization and efficiency.
Though the initial effects of these hearing aids seemed positive, an inability to distinguish signals (voices and other important sounds) from noise (everything else), made these hearing aids, and indeed many low-end digital hearing aids largely inadequate. Today’s state of the art hearing aids, however, are far more advanced than a rudimentary sum of its parts. Currently, hearing aids make use of digital signal processing techniques within the amplifier, making the sound passed on to the wearer far better and clearer. Also at their earlier iterations, hearing aids were large, obtrusive and were required to be worn on the body with wires connecting to the earpieces. Now, as all of the components that make up hearing aids have become far smaller, hearing aids can be made to be completely invisible inside the wearer’s ear canal in invisible-in-canal (IIC) designs, or nearly invisible form-factors such as completely-in-canal (CIC) and receiver-in-canal (RIC) styles, or more conspicuous designs such as in-the-canal (ITC), in-the-ear (ITE), or the traditional behind-the-ear (BTE) forms [12].
In their most basic form, a hearing aid consists of a microphone, picking up sounds from the wearer’s environment and transforming them into electric signals; an amplifier, increasing the power of those signals and processing them; and a receiver, more commonly known as a speaker, playing those signals into the ear canal; and a battery powering the device [12]. Modern hearing aid designs have refined these basic components into highly sophisticated, miniaturized devices that offer a range of customizable features and styles to meet individual needs. Advances in digital signal processing allow for precise amplification and noise reduction, while modern receivers deliver clearer, more natural sound. Additionally, contemporary hearing aids often incorporate wireless connectivity, enabling seamless integration with smartphones and other devices [13].
Unfortunately, many people delay seeking help until their hearing impairment severely impacts their daily life, despite the availability of hearing aids that can enhance communication, social interaction, and overall well-being. This gap underscores the need for increased education, accessibility, and support to encourage more individuals to take advantage of the hearing solutions available to them. According to the National Institute on Deafness and Other Communication Disorders, a surprisingly small percentage of Americans who could benefit from hearing aids actually use them, with estimates ranging from just 16% to 30% [14]. This disparity highlights a significant public health issue, as millions of individuals are missing out on the improved quality of life that hearing aids can provide. The reasons for this low adoption rate are multifaceted, including social stigma, cost barriers, lack of awareness, and a general reluctance to acknowledge hearing loss as a problem. In this paper, we review the historical stigma associated with hearing aids and examine the ways to alleviate it with improvements in designs and increased functionalities.
2. Survey of Prior Research
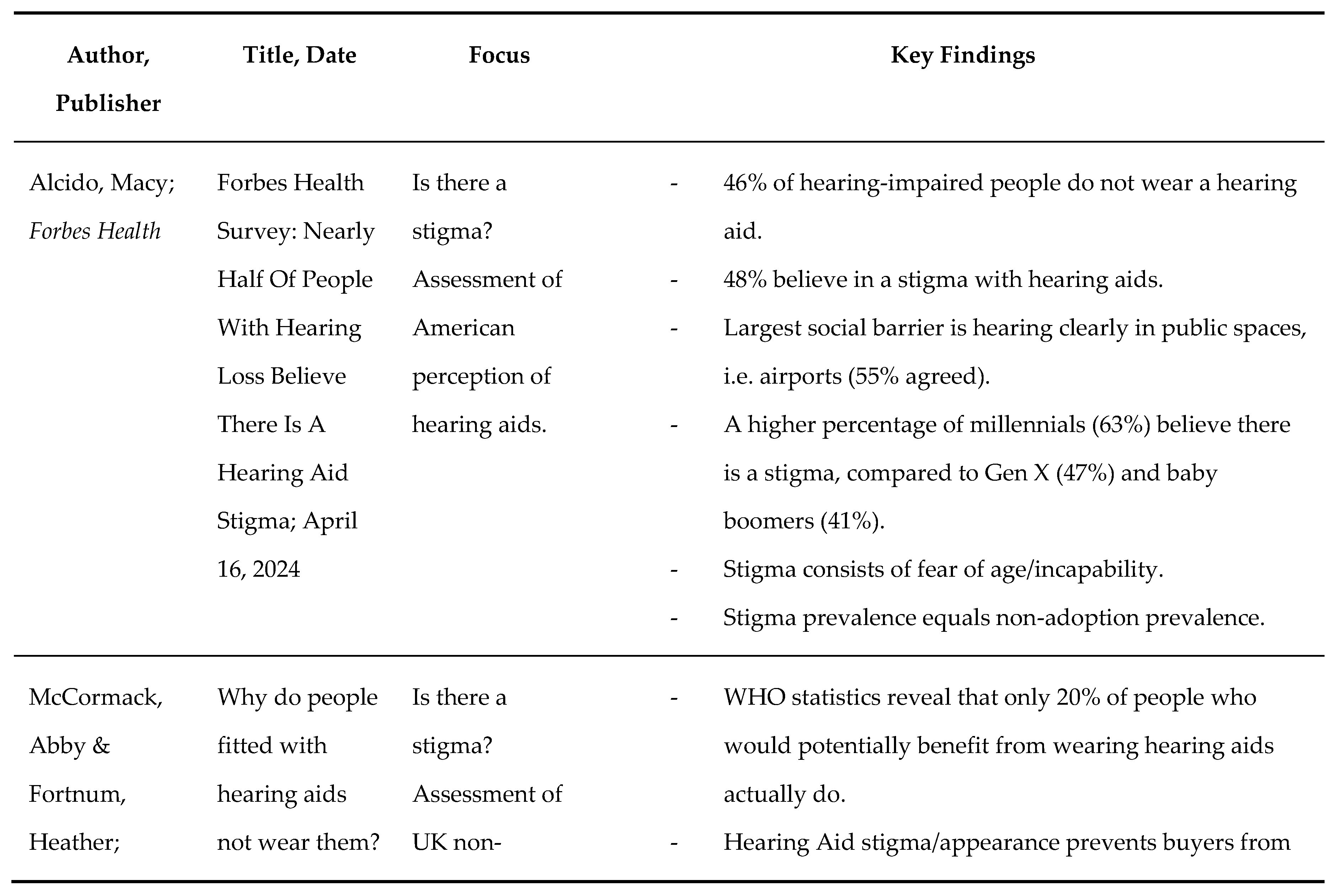
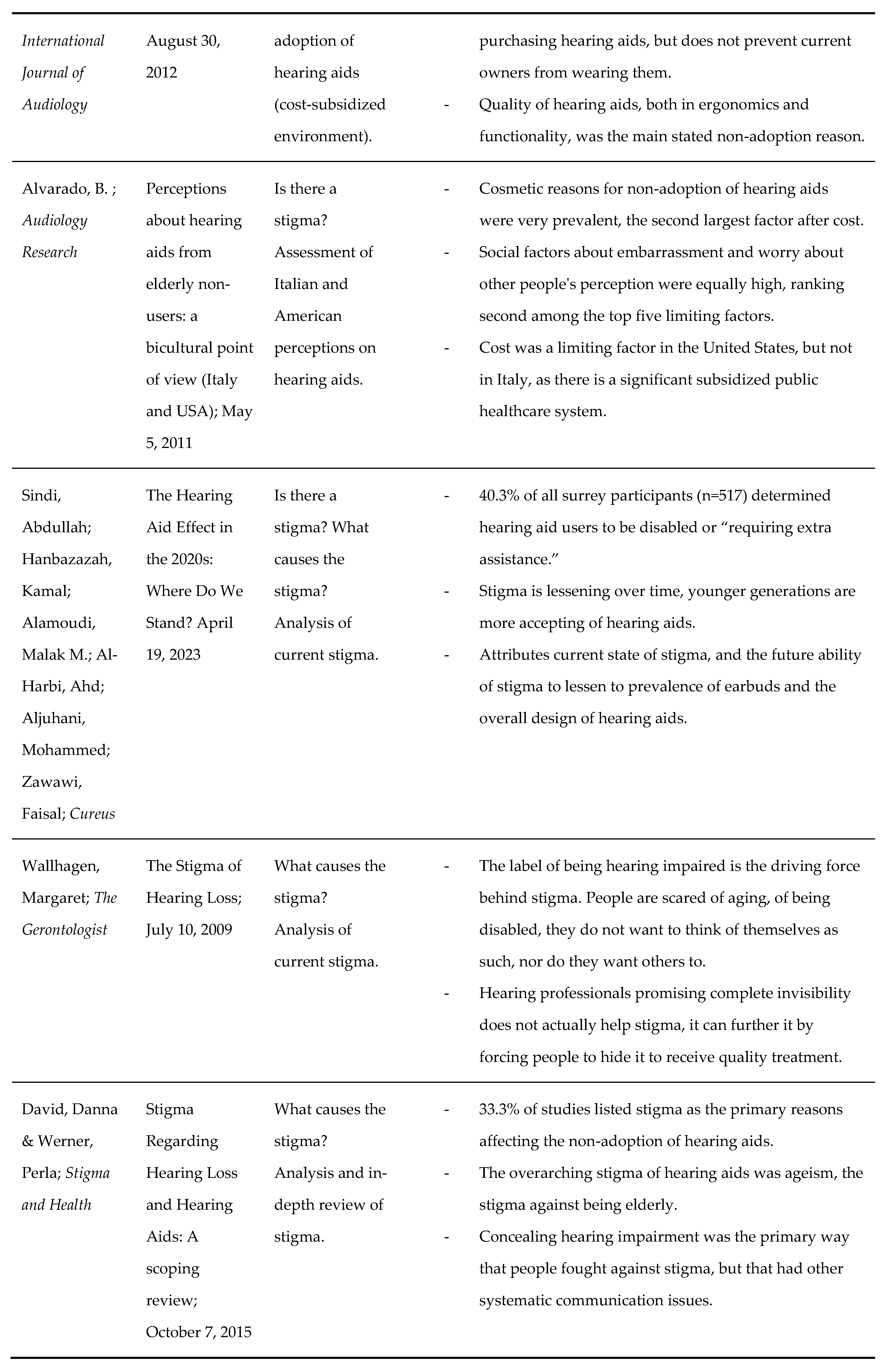
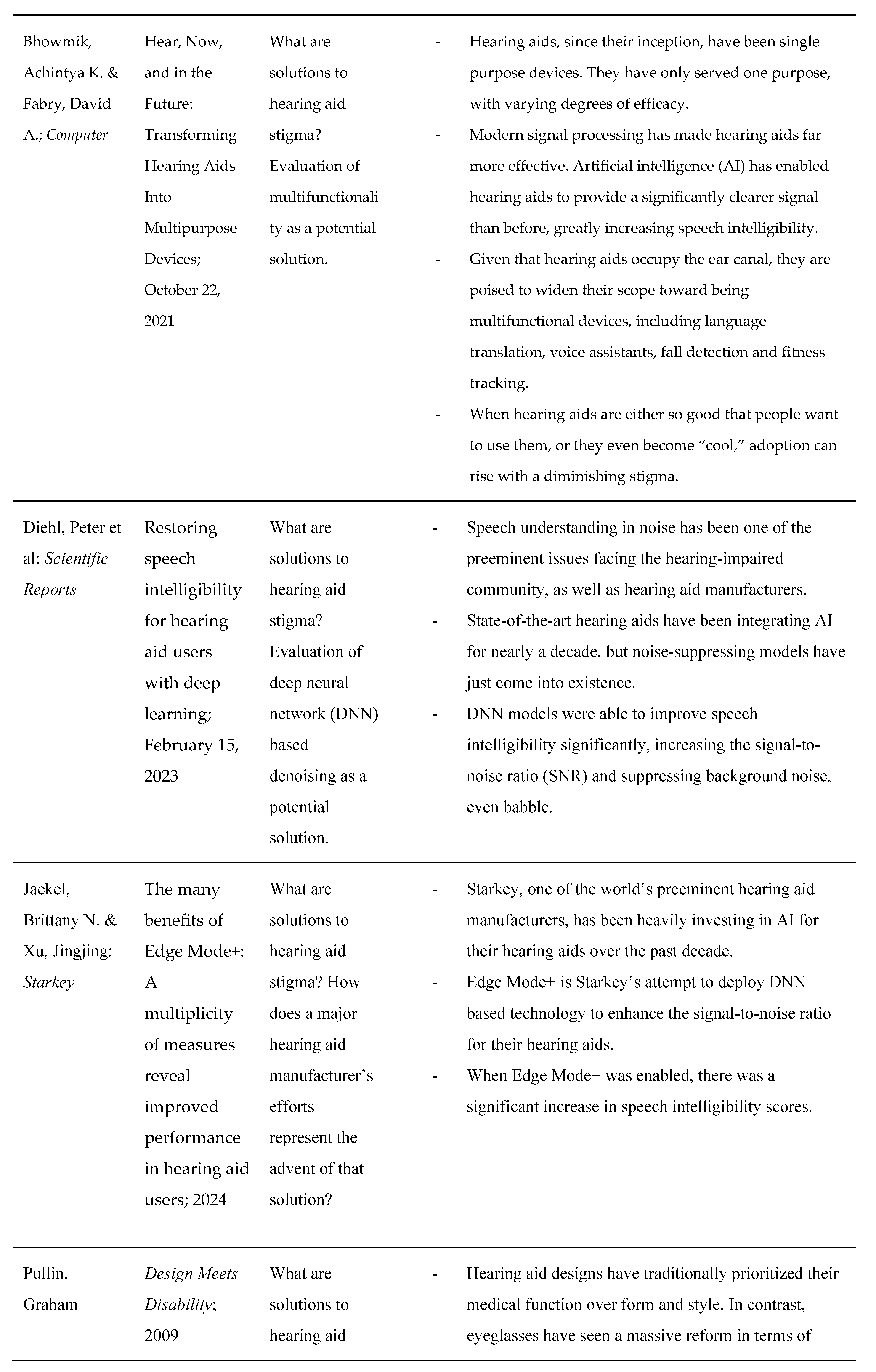
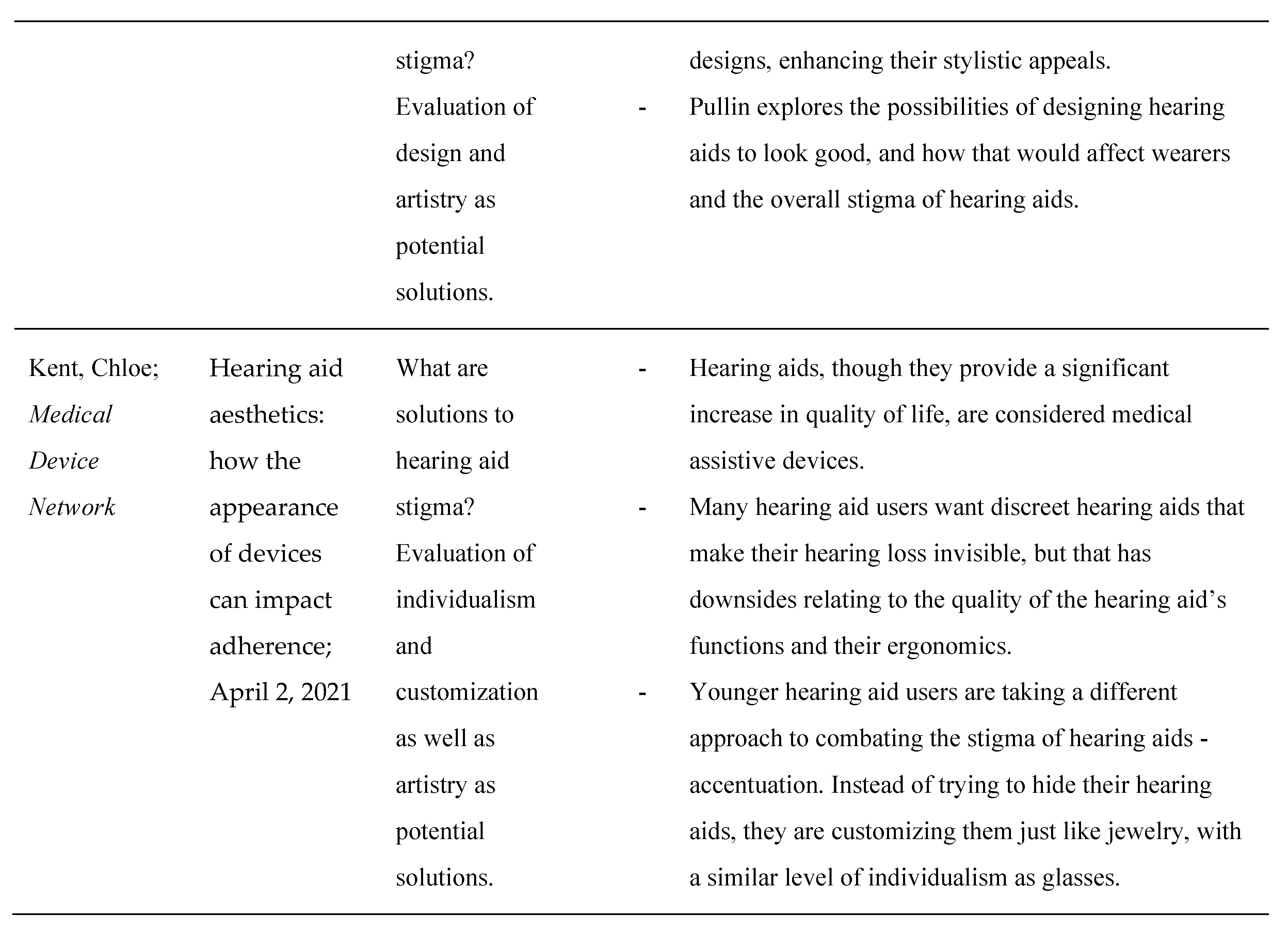
The body of research on hearing aid stigma offers a comprehensive understanding of the various factors contributing to the non-adoption or underuse of hearing aids, despite their potential to significantly enhance quality of life. In this section, we will review key studies that have systematically analyzed the social, psychological, and technological dimensions of hearing aid stigma. Table 1 provides a summary of notable research works, organized by authors, publication details, and their focus areas. These studies provide insights into both the causes of stigma—such as ageism, perceptions of disability, and concerns about aesthetics—and explore potential solutions, including advancements in technology and design. This survey aims to contextualize the current state of hearing aid adoption and identify pathways to reducing the associated stigma.
2.1. Is There a Stigma?
In short, yes, the surveys reveal that there continues to be a stigma associated with hearing loss as a whole, but especially regarding hearing aids as the main solution to hearing loss. A multitude of papers, spanning two decades, and multiple continents, state stigma as either the primary cause of hearing aid non-adoption or one of the leading causes.
Most recently, Mary Alcido, writing for Forbes Health, conducted a survey on the limited adoption of hearing aids [15]. She concluded that 46% of hearing-impaired people do not wear a hearing aid. More pertinently, however, out of the entire survey pool, 48% of people believed that hearing aids are stigmatized. The stigma, Alcido noted, was rooted in a fear of aging and incapability (i.e. people do not want to be perceived, nor do they want to perceive themselves as old or disabled). Importantly, and optimistically, however, the Forbes survey also demonstrated that hearing aid stigma was less prevalent in younger generations, indicating that the stigma could naturally decrease over time.
As somewhat of a foil to Alcido’s survey, Abby McCormack and Heather Fortnum’s 2012 study for the International Journal of Audiology as well as Beatriz Alvarado’s 2011 article for Audiology Research were also reviewed [16,17]. Those papers offered an international and historical insight into hearing aid stigma to examine its evolution and global expanse. These two research works were conducted through rote mathematical anthropological analysis. McCormack and Fortnum observed current hearing aid users in the United Kingdom. Though they found quality to be the greatest inhibitor to regular use for users who already owned hearing aids, they found that stigma was the largest barrier to purchasing hearing aids in the first place. Alvarado compared hearing aid users in the United States and Italy. Though they found cost to be the largest barrier, cosmetic and social reasons for hearing aid non-adoption (all of the individual factors that make up stigma), occupied more of the highest-ranked positions overall. Additionally, cost was only a factor in the United States, as Italy has a large public healthcare system subsidizing hearing aids.
In a larger and more quantitative approach to hearing aid analysis, Sergei Kochkin’s examination of the MarkeTrak VII survey on hearing loss also saw stigma to be a significant inhibitor [18]. Kochkin concluded that “nearly half (48%) indicated that stigma contributed to their desire not to wear hearing aids.” Apart from cost and perceived lack of need, which could also be attributed to stigma, stigma alone was the largest factor relating to hearing aid non-adoption. Additionally, though her paper is more poignant when examining what causes the stigma of hearing aids, one quotation from Margaret Wallhagen’s 2009 paper discussing the stigma of hearing loss as a whole is highly important to evaluating the presence of stigma [19]. She found that “even if hearing aids were given away by the government at no cost to the user, 65% of the hearing-impaired population would decline the offer.”
2.2. What Causes the Stigma?
As a distinctly psychological and sociological issue, there are many factors and facets of hearing aid stigma, yet all of these factors can be roughly categorized as systemic and societal ageism and ableism.
Though Abdullah Sindi (et al)’s paper for Cureus Journal does provide a wide overview of hearing aid stigma, it also provides analysis on the stigma, differentiating it from the articles above [20]. Sindi et al presented their participants (n=517) with various pictures of hearing people, and hearing-impaired people, who were hearing aid users, and asked them if they believed that the hearing-impaired people seemed disabled or “required additional assistance.” They found that 40.3% of people (n= ~208) believed that hearing aid users fit the aforementioned description. Their survey thus points toward ageism as a root cause of the stigma. Just like the Forbes Health survey, Sindi et al also optimistically claim diminishing stigma amongst younger generations. They attribute that transition to the prevalence of earbuds and the future designs of hearing aids.
Margaret Wallhagen’s 2009 paper entitled “The Stigma of Hearing Loss,” is one of the seminal articles relating to its namesake subject, though it is somewhat dated [19]. Wallhagen attributes the stigma, simply to the label of being hearing-impaired, as well as the convention of hiding a hearing impairment, in pursuit of a solution. She claims that hearing aid professionals who constantly push hearing aid discretion and invisibility could actually be empowering the stigma of hearing aids instead of their patients.
In a 2015 review article not dissimilar to this paper, Danna David and Perla Werner examine all of the surveys surrounding hearing aid adoption [21]. They found that 33.3% of all surveys listed hearing aid stigma as the primary reason for non-adoption. Just like Wallhagen, they found that ageism and the pursuit of concealment were the main causes behind stigma.
2.3. How Can the Stigma Be Alleviated?
Though this point will be further elaborated in the analysis and discussion portions of this paper, hearing aid stigma can be categorized as observed or perceived. Observed stigma is impacted by design, and perceived stigma, which could be categorized as the “crowded room effect,” is affected by functionality.
Graham Pullin’s book, Design Meets Disability, is an important resource to consider when assessing design and its impact on observed stigma of hearing aids [22]. In the book, Pullin explores the impact of industrial designs and color palettes from popular consumer electronic devices, and how that might affect the stigma of hearing aids. Pullin also provides an anecdote of a teenager wearing a bright white, ostensibly visible hearing device, and how confident he seemed comparatively.
Chloe Kent, in a 2021 Medical Device Network article, also explores the potential for the intersection of design and hearing loss, however differently from Pullin [23]. Kent advocates for individualism and customization of hearing aids, similar to glasses. She claims that it is far more important, for the sake of eliminating hearing aid stigma, to make hearing aids look good than to make them invisible, especially if invisibility trumps functionality. She also says that younger generations are especially attuned to this kind of design independence from the medical world.
Bhowmik and Fabry, in an IEEE Computer article, outlined the path forward for hearing aids to become multifunctional devices, transcending their primary purpose of amplifying sound [13]. The computational processing power in modern hearing aids has become so advanced, and the connectivity to the cloud so pervasive, that they are able to integrate fall detection and fitness tracking sensors, language translation capabilities, and virtual assistants into the hearing aids. The scope of multifunctionality is that hearing aids can become devices that people want to wear instead of have to wear.
Artificial intelligence has significant capabilities within the audio world. In two papers, one scientific and the other clinical, Peter Diehl et al writing for Scientific Reports and Brittany Jaekel and Jingjing Xu in a Starkey Hearing whitepaper, assess the potential of deep neural network (DNN) based denoising algorithms as a major improvement in hearing aid performance and functionality [24,25]. They found that that incorporating DNN algorithms was able to reliably improve speech intelligibility scores, by increasing signal-to-noise ratios (SNRs). In short, DNNs are a significant potential solution to hearing loss affecting the ability to understand speech in noisy environments. Just like in the Scientific Reports trial, Starkey's work found success in speech intelligibility improvement when the DNN algorithms were enabled.
3. Analysis and Discussion
For as long as hearing aids have existed, users have struggled with the stigma of wearing them and a belief that wearing hearing aids indicates old age, frailty and or disability [17,20]. This stigma can be observed (i.e. how a user thinks about themselves and the way their hearing aids might look), or perceived (i.e. how a non-user in views the user or how a user thinks a non-user views them) [15,19,20]. Importantly, observed stigma often feeds perceived stigma. For example, in a Cureus Journal survey completed in 2023, 40% of participants observed hearing aid wearers to either be “handicapped,” or “requiring extra assistance” to complete tasks. In order to avoid being viewed in such a way, many patients simply refuse to wear hearing aids. This perceived stigma can be referred to as the “crowded room effect” – the desire by users when they walk into a crowded room to “fit in,” to not be the “odd person out,” or to not be “different.” Heffernan, Coulson and Ferguson did a study trying to understand the underlying factors that support hearing aid stigma, that can manifest themselves as observed stigma or the crowded room effect [26]. They found that a fear of aging and a desire to maintain a normal appearance were the two most significant reasons for stigma. Potent Design and functionality of hearing aids can significantly abase both the observed stigma and the perceived stigma, by fighting against the stereotypical correlation between aging and hearing aids [20,26].
3.1. Observed Stigma and the Impact of Design
For reasons of simple necessity, the design of hearing aids has often reflected their functional use. The most ubiquitous design form currently is the RIC, where the speaker, referred to as the receiver, is placed in the ear canal and the device, consisting of the battery pack, microphones, and processors, sits behind the ear connected by a thin translucent conducting wire over the top of the ear. This form has been effective in aggregating the component parts of hearing aids but their visual appearance has typically still been perceived as medical in nature [12]. Contrast this to the emergence of consumer electronic earphones or earbuds, such as Apple AirPods launched in December 2016. These devices, while not as medically advanced or effective as prescription hearing aids, are now worn by over 100 million people worldwide [27] and “carry none of the social stigma sometimes associated with hearing aids.” However, it must also be considered that these earphones are fully occluding devices with limited battery life, and as such can’t replace the hearing aids for their comfortable all-day use. In addition, the consumer electronic earbuds come with their own form of stigma. Will it be socially acceptable to wear them at a family dinner or in a business meeting? The potential however exists for an improvement in the design form of hearing aids to improve the observed stigma. This opportunity also extends to the style of hearing aids. For years the eyeglass industry fought against a similar visual stigma, observed and perceived [28]. That stigma was popularized by the fact that Clark Kent takes off his glasses to become Superman [29]. Then, starting in the ‘70s, eyeglass manufacturers turned to thermoset plastics and exotic materials to revolutionize the design style of glasses [22]. As of 2024, more than 4 billion people wear glasses [30]. Vision impaired people have, in many cases, become proud of their glasses. As the glasses industry revolutionized, their lives improved. The same opportunity exists for hearing device designers. If the hearing-impaired population can like wearing hearing aids, and not feel denigrated while wearing them, then they will wear their hearing aids more frequently, improving their quality of life and diminishing the risks of hearing loss’s comorbidities.
3.2. Perceived Stigma and the Impact of Functionality
Improving the observed stigma of hearing aids will increase the likelihood of adoption as self-acceptance promotes usage. But, how about the perceived stigma, the reluctance to walk into a crowded room wearing hearing aids for fear of being viewed differently. One answer lies in increasing the number of people in the room wearing them. That desire, or necessity, of wearing hearing aids is driven in a large part by their functionality [15]. Hearing aid functionality has two core parts: sound quality and feature richness. Hearing aids with excellent sound quality should be able to capture, amplify and deliver sound to the user nearly as though they had normal hearing. Sound quality also means limiting feedback within the ear canal, and isolating speech in noisy scenarios. That quality is now based on advanced digital sound processing, some of which is powered by neural networks [13,24,25]. Hearing aids that are feature-rich are multifunctional. Capitalizing off of the unique biology of the ear canal, as well as the fact that a hearing aid sits in the ear, hearing aids now can have body tracking sensors, fall detection, and the ability to provide language translation and personal voice assistant functions improving the wearing experience of the user [13]. In turn, more people should want to wear hearing aids, driving up their adoption rate. Thus, more people in a “crowded room” will be wearing hearing aids, lessening the stigma of standing out in a crowd of otherwise non hearing aid wearers.
Design and functionality of hearing aids are not completely independent, either. Ergonomics of hearing aids are one of the elements that cross over between those two categories. Many older and hearing-impaired patients also struggle with dexterity issues or neuropathy. Though those patients might desire discreet, small, even invisible hearing aids, those hearing aids are impossible for them to use. Therefore, the larger, easy to manipulate, simply designed full shell ITE hearing aids, that, consequently, might show more, are also crucial [16].
3.3. Toward Alleviating the Stigma
De-stigmatizing hearing aids, like many things, starts with the device designers and ends with the consumer. Having spent decades improving the quality of hearing, designers now have the opportunity to combine form with function and deliver products that users are excited to wear. Depending on the form factor used, hearing aids can be customized with the user's favorite color or pattern, branded with their favorite luxury marque, or reflect their alma mater, or favorite artist. All of this holds the potential to lower the stigma of hearing aids by allowing the user, for perhaps the first time in their life, to “show off” and “be proud” of wearing them. In this way the observed stigma of hearing aids can begin to abate the same way the observed stigma of eyeglasses has greatly diminished over time. In his presentation to the Microsoft Research organization, Graham Pullin, while describing work by Charles and Ray Eames, says that “designers from art school backgrounds can enrich” design for disabilities, as that culture can make more interesting and possibly, more functional designs that are as beautiful as they are useful [31]. He even says that “a teenager wearing a white hearing aid, which was more visible than a flesh-pink one, looked self-confident wearing it.” That encounter mirrors how hearing aid stigma can potentially be averted through accentuation and great design [22]. When that happens, the stigma for the use of those disability aiding products may be reduced. In turn, the effects of those disabilities are diminished, and the quality of life increases for those afflicted. Clinical problem solving need not be absent from hearing aid design, as that problem solving ensures that form does not overtake function, but there should be some element of beauty and fashionable sophistication that is also present. Significant strides are being made in this direction. For example, the state-of-the-art modern hearing aids are starting to offer more visually attractive designs than the traditional devices of the past [13].
Functionality is equally important as it eliminates the perceived stigma of hearing aids by making them devices that hearing-impaired people want to wear instead of have to wear. Advancements in features such as language translation, fall detection, geo-location and fitness tracking have revolutionized the value of hearing aids to users and their families [13]. Today, there is no reason a user of advanced hearing aids should not feel as empowered, or more, in their life as an AirPods user does when they don their devices. Figure 4 shows the digital demonstrations of this functionality – either through their fitness tracking software or their voice-enhancement algorithms. As hearing aids become more valuable to the user, their adoption rate should rise. That rise, in turn, should increase the number of people in a crowded room wearing hearing aids and the perceived stigma (if even still present) should fall.
Dementia and cognitive decline due to a lack of interpersonal communication are two of hearing loss’s most significant comorbidities. Even for current hearing aid users, a difficulty to distinguish speech from noise is one of their most common complaints, and that issue is perhaps the decisive factor influencing the aforementioned comorbidities. As such, many choose to go without their hearing aids, as they feel that they are not helping, furthering those problems. A program or device, therefore, that could effectively suppress noise, especially in loud environments such as restaurants, is critical. With modern advancements in artificial intelligence, especially through development of algorithms based on deep neural networks integrated in the hearing aid, rapid progress is being made in this direction [25,32,33].
Voice isolation techniques are analogous to similar technologies used in the music industry. In that sector, producers have begun to use DNNs to isolate certain stems or instruments in a given track of music. By using a time to frequency domain transform (TFDT), then allowing a DNN to recognize patterns in the frequency signatures of sounds, producers can isolate and tune a specific instrument. Likewise, though it is more difficult to isolate speech than music, this same process can be used to isolate voices from noise [34]. As an example, IRIS Audio applied voice isolation software to call centers and other noisy mission-critical environments where clear communication is critical [35]. An example of the effectiveness of DNN-based voice isolation is a University of Washington experiment, where they tuned regular, noise-canceling headphones to isolate voices and suppress all noise except for the sole person to whom the subject wanted to listen [36]. The advent of voice isolation technologies alone is not groundbreaking to solving the sigma of hearing aids, rather it is simply a new function that could drastically improve the experiences of hearing aid wearers, allowing them to see the full benefits of hearing aids, solving their hearing loss.
Manchaiah and Stephens conducted a survey that assessed how likely people were to disregard the hearing aid stigma. They found that those who had more profound hearing loss were more likely to be hearing aid adopters, despite stigma [37]. Their study could indicate that, as people perceive hearing aids to be more useful to them, they are more likely to use hearing aids, regardless of stigma. As of now, only the profoundly hearing-impaired feel that hearing aids are effective enough to warrant that, yet if hearing aids were to become far better, functionally, then no doubt more people would use them, across the hearing loss spectrum.
Design and functionality, alone, can greatly reduce the stigma of hearing aids for both current hearing aid wearers or immediate candidates who are soon to make a decision on whether or not to begin using hearing aids. For the rest of the population, however, awareness needs to be raised about hearing aids, both in their current forms, and in their possible future, more advanced forms. A study completed by David et. al. demonstrated that when non-hearing-impaired people watched videos about hearing aids, and the benefits that can be derived from them, they were both intrigued about hearing aids, either for themselves or for others, and had a greater sense of sympathy for the hearing impaired and their use of hearing aids [21].
The results of that study clearly show the effectiveness of education against hearing aid stigma. As hearing aids become more advanced, therefore, public health organizations, as well as the hearing aid ecosystem could launch broad campaigns about the benefits of hearing aids. Those campaigns could mirror other public health campaigns in their effectiveness and sympathy derived for those affected, similar to the Mothers Against Drunk Driving campaign of the 1980s [38]. Though those two campaigns are different in their focus, elements of outreach and the design of the campaigns could be mirrored to ensure the success of a campaign for hearing aid adoption. The hearing aid awareness campaigns, if done well, could be a major catalyst for the reduction of hearing aid stigma through design and functionality.
4. Conclusions
Hearing aids have undergone remarkable advancements in recent years, transforming from rudimentary sound amplification tools into sophisticated, multi-functional devices that utilize artificial intelligence to enhance sound quality and offer additional features like fall detection, physical activity and social engagement tracking, and even language translation. Despite these innovations, the adoption rate of hearing aids remains strikingly low, with a very small fraction of people who need them actually using them.
In this paper, we have examined the pervasive stigma associated with hearing aids, which continues to be a significant barrier to their widespread adoption. We have explored how the stigma—both observed and perceived—can be alleviated by improving the design and functionality of hearing aids. By drawing parallels with the evolution of eyeglasses, which successfully transitioned from a stigmatized necessity to a fashion statement, this paper argues that hearing aids can similarly overcome their negative perception. By integrating multiple functions besides design improvements, hearing aids can transform into must-have health and communication devices that many would want to wear. The discussion also emphasizes the importance of public awareness and education in reducing stigma and increasing acceptance of hearing aids, ultimately aiming to improve the quality of life for millions of individuals with hearing loss.
As hearing aid designers continue to create products that both look better and perform better, both the perceived stigma of wearing them and the observed stigma of being “disabled” will be reduced, paving the way to a world where hearing-impaired people are not discriminated against for wanting a better quality of life. As that happens, one of the world's largest pandemics, comprising one-fifth of the world’s total population, can be improved and those afflicted can receive the hearing care that they require and deserve.
Author Contributions
Conceptualization, E.M. and A.B.; methodology, E.M. and A.B. investigation, E.M. and A.B.; data curation, E.M. and A.B.; writing – original draft preparation, E.M.; writing, review and editing, E.M. and A.B. All Authors have read and agreed to the published version of the manuscript.
References
- Schnupp, J., Nelken, I., & King, A. (2011). Auditory neuroscience: Making sense of sound. MIT Press. [CrossRef]
- Chittka, L., & Brockmann, A. (2009, February 15). Anatomy of the human ear [Illustration]. Wikimedia Commons. https://upload.wikimedia.org/wikipedia/commons/d/d2/Anatomy_of_the_Human_Ear.svg.
- World Health Organization. (2021). World report on hearing [Brochure]. World Health Organization. https://iris.who.int/bitstream/handle/10665/339956/9789240021570-eng.pdf?sequence=1.
- Lin, F. R. (2024). Age-related hearing loss. New England Journal of Medicine, 390(16), 1505–1512. [CrossRef]
- Wasano, K., Kaga, K., & Ogawa, K. (2021). Patterns of hearing changes in women and men from denarians to nonagenarians. The Lancet Regional Health - Western Pacific, 9, 100131. [CrossRef]
- Hughes, S. E., Hutchings, H. A., Rapport, F. L., McMahon, C. M., & Boisvert, I. (2021). Social connectedness and perceived stigma in adults with hearing loss: A systematic narrative review. American Journal of Audiology, 30(3), 668-683.
- Fabry, D. (2015, December 14). "America must confront hearing loss: Column." USA Today. https://www.usatoday.com/story/opinion/2015/12/14/hearing-loss-deaf-mental-health-column/77288420/.
- Lin, F. R. and Ferrucci, L. (2012). Hearing loss and falls among older adults in the United States. Arch Intern Med. 172(4):369-71. [CrossRef] [PubMed] [PubMed Central]
- Tanna, R. J., Lin, J. W., & De Jesus, O. (Updated 2023, August 23). "Sensorineural hearing loss." National Library of Medicine. Retrieved July 12, 2024, from https://www.ncbi.nlm.nih.gov/books/NBK565860/.
- Sooriyamoorthy, T., & De Jesus, O. (2023, August 3). "Conductive hearing loss." StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK563267/.
- "Hearing loss & tinnitus statistics." (n.d.). Hearing Health Foundation. https://hearinghealthfoundation.org/hearing-loss-tinnitus-statistics#:~:text=About%2080%20percent%20of%20hearing,and%20improved%20quality%20of%20life.
- "Hearing aids." (2022, October 11). National Institute on Deafness and Other Communication Disorders. Retrieved September 27, 2024, from https://www.nidcd.nih.gov/health/hearing-aids.
- Bhowmik, A. K. and Fabry, D. A. (2021). Hear, Now and in the Future: Transforming Hearing Aids into Multipurpose Devices. Computer 54, 108-120.
- "Quick statistics about hearing, balance, & dizziness." (2024, September 20). National Institute on Deafness and Other Communication Disorders. Retrieved September 27, 2024, from https://www.nidcd.nih.gov/health/statistics/quick-statistics-hearing#:~:text=About%2028.8%20million%20U.S.%20adults%20could%20benefit%20from%20using%20hearing%20aids.&text=Among%20adults%20ages%2070%20and,aids%20have%20ever%20used%20them.
- Alcido, M. (2024, April 16). "Forbes health survey: Nearly half of people with hearing loss believe there is A hearing aid stigma." Forbes. https://www.forbes.com/health/hearing-aids/hearing-aids-stigma-survey/#:~:text=Nearly%20half%20(48%25)%20of,communications%20with%20friends%20and%20family.
- McCormack, A., & Fortnum, H. (2013). Why do people fitted with hearing aids not wear them? International Journal of Audiology, 52(5), 360-368. [CrossRef]
- Alvarado, B. (2011). "Perceptions about hearing aids from elderly non-users: A bicultural point of view (Italy and USA)." Audiology Research, 1(26). [CrossRef]
- Kochkin, S. (2007). MarkeTrak VII: Obstacles to adult non-user adoption of hearing aids. Hearing Journal, 60(4), 24-50.
- Wallhagen, M. I. (2009). "The stigma of hearing loss." The Gerontologist, 50(1), 66-75. [CrossRef]
- Sindi, A., Hanbazazah, K., Alamoudi, M. M., Al-Harbi, A., Aljuhani, M., & Zawawi, F. (2023). "The hearing aid effect in the 2020s: Where do we stand?." Cureus. [CrossRef]
- David, D., Werner, P., & Stutter, E. (2018). Reducing stigma toward hearing aids: Can informative videos help? American Journal of Audiology, 27(1), 55-62.
- Pullin, G. (2009). Design meets disability. MIT Press.
- Kent, C. (2021, April 2). "Hearing aid aesthetics: How the appearance of devices can impact adherence." Medical Device Network. Retrieved August 6, 2024, from https://www.medicaldevice-network.com/features/hearing-aid-aesthetics/.
- Diehl, P. U., Singer, Y., Zilly, H., Schönfeld, U., Meyer-Rachner, P., Berry, M., Sprekeler, H., Sprengel, E., Pudszuhn, A., & Hofmann, V. M. (2023). Restoring speech intelligibility for hearing aid users with deep learning. Scientific Reports, 13(1). [CrossRef]
- Jaekel, B. N., & Xu, J. (2024). "The many benefits of Edge Mode+: A multiplicity of measures reveal improved performance in hearing aid users." Starkey. https://cdn.mediavalet.com/usil/starkeyhearingtech/L-xSXyLLKkOLKM_v6LUPnA/HdC0F04O402ZtognLDvn6w/Original/Starkey%20Benefits%20of%20Edge%20ModePlus%20White%20Paper.pdf.
- Heffernan, E., Coulson, N. S., & Ferguson, M. A. (2022). Understanding the complex factors influencing hearing aid use in older adults: A qualitative study. International Journal of Audiology, 61(1), 33-41.
- "Airpods are becoming a platform." (2019, November 19). Above Avalon. Retrieved August 14, 2024, from https://www.aboveavalon.com/notes/tag/How+many+people+wear+AirPods.
- "The history of eyeglasses." (2020, March 4). Charlotte Eye, Ear, Nose & Throat Associates, P.A. Retrieved August 14, 2024, from https://www.ceenta.com/news-blog/the-history-of-eyeglasses.
- Andie. (2015, January 19). “Superman changes to Clark and then back and forth [Video].” Youtube. https://youtu.be/tNUu6Lf9mVU.
- Sadovsky, G. (2024, April 1). "Eyewear industry statistics and facts 2024." Overnight Glasses. Retrieved August 6, 2024, from https://www.overnightglasses.com/eyewear-industry-statistics/#:~:text=Over%204%20billion%20people%20across,eyewear%20market%20across%20the%20globe.
- Microsoft Research. (2016, September 7). Design meets disability [Video]. Youtube. https://www.youtube.com/watch?v=uMmgJP8pP0c.
- Fabry, D. A. and Bhowmik, A. K. (2021). Improving Speech Understanding in Noise and Monitoring Health with Hearing Aids using Artificial Intelligence and Embedded Sensors. Seminars in Hearing 42, 3, 295-308.
- Zhang, T. and Bhowmik, A. (2018). Enhancing Speech in Noisy and Reverberant Environments Using Deep Learning Techniques. SID Symp. Digest of Tech. Papers 49, 467.
- Kar, A. (2023). "Improved vocal isolation from varying repeating structures for musical signals." Applied Acoustics, 214, 109688. [CrossRef]
- IRIS Audio Technologies. (2023). "Research identifies three key impacts of noise on call centers and hybrid work environments.".
- Milne, S., & Taguchi, K. (2024, May 23). "AI headphones let wearer listen to a single person in a crowd, by looking at them just once." UW News. Retrieved August 23, 2024, from https://www.washington.edu/news/2024/05/23/ai-headphones-noise-cancelling-target-speech-hearing/.
- Manchaiah, V., & Stephens, D. (2013). The role of self-reported hearing disability and hearing handicap in predicting hearing aid use. Trends in Amplification, 17(1), 48-57.
- Fell, J. C., & Voas, R. B. (2006). "Mothers against drunk driving (MADD): The first 25 years." Traffic Injury Prevention, 7(3), 195-212. [CrossRef]
Figure 1.
Anatomy of the human ear, highlighting key structures involved in hearing [2]. The outer ear captures sound waves, which travel through the ear canal to the eardrum. The middle ear, containing the ossicles, amplifies these vibrations, transmitting them to the inner ear where the cochlea converts them into neural signals for the brain to process.
Figure 1.
Anatomy of the human ear, highlighting key structures involved in hearing [2]. The outer ear captures sound waves, which travel through the ear canal to the eardrum. The middle ear, containing the ossicles, amplifies these vibrations, transmitting them to the inner ear where the cochlea converts them into neural signals for the brain to process.
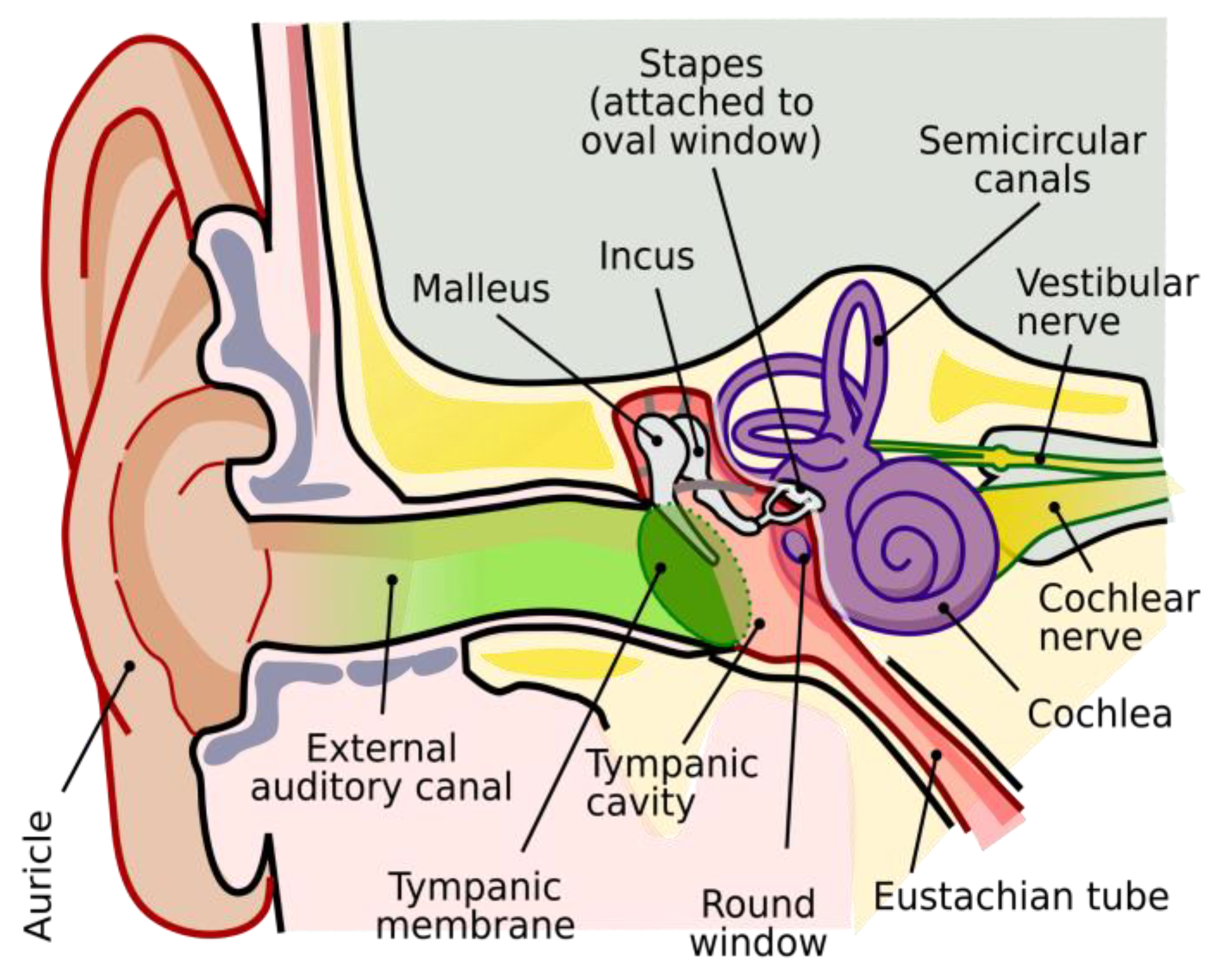
Figure 2.
The age-related progression of hearing loss across different frequencies (125 to 8000 Hz) for Japanese men (A) and women (B). The data, collected from over 10,000 individuals aged 10 to 99 years, show that hearing thresholds progressively increase (indicating worse hearing) with age, particularly at higher frequencies [5].
Figure 2.
The age-related progression of hearing loss across different frequencies (125 to 8000 Hz) for Japanese men (A) and women (B). The data, collected from over 10,000 individuals aged 10 to 99 years, show that hearing thresholds progressively increase (indicating worse hearing) with age, particularly at higher frequencies [5].
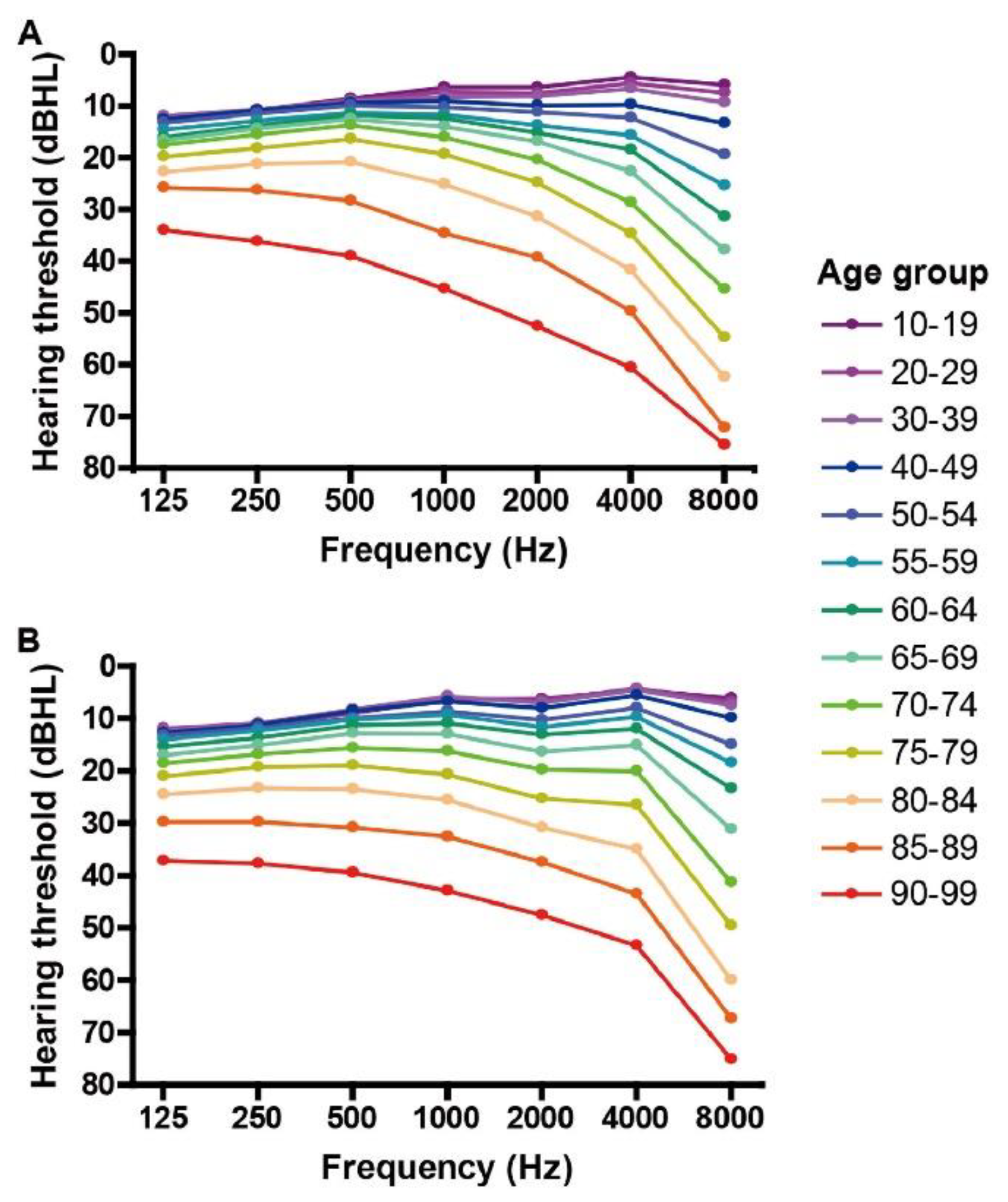
Figure 3.
Top-left: Madame de Meuron with ear trumpet, an early form of hearing aids dating back to the 17th century. Top-right: Frederick Rein's acoustic chair, designed for King John VI of Portugal in the early 19th-century. Middle-left: Body-worn hearing aids based on vacuum tube, circa 1944. Middle-right: Transistor body-worn hearing aids, circa 1979. Bottom: Modern hearing aids in 2024. From the left to right: invisible in-canal (IIC), completely in-canal (CIC), in-the-canal (ITC), in-the-ear (ITE), micro receiver-in-canal (Micro RIC), and receiver-in-canal (RIC) designs, all from Starkey Hearing.
Figure 3.
Top-left: Madame de Meuron with ear trumpet, an early form of hearing aids dating back to the 17th century. Top-right: Frederick Rein's acoustic chair, designed for King John VI of Portugal in the early 19th-century. Middle-left: Body-worn hearing aids based on vacuum tube, circa 1944. Middle-right: Transistor body-worn hearing aids, circa 1979. Bottom: Modern hearing aids in 2024. From the left to right: invisible in-canal (IIC), completely in-canal (CIC), in-the-canal (ITC), in-the-ear (ITE), micro receiver-in-canal (Micro RIC), and receiver-in-canal (RIC) designs, all from Starkey Hearing.
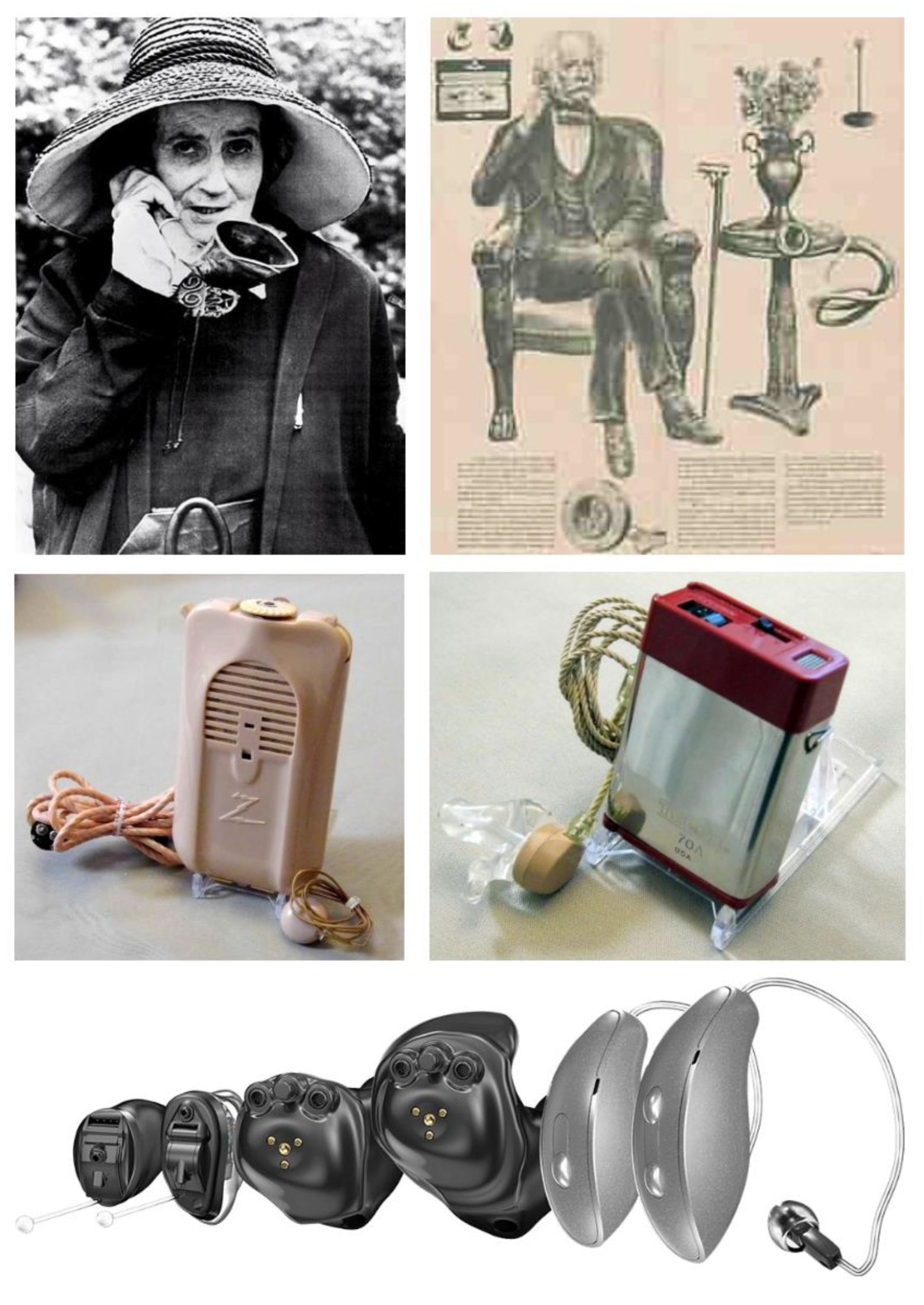
Figure 4.
Two demonstrations of new features to expand the hearing aid functionality. The first image is how the fitness tracking data from Starkey’s hearing aids is shown to the wearer. The second image is a demonstration of how their first DNN-based denoising software worked [13]. The current generation of advanced hearing aids from Starkey incorporates a DNN accelerator embedded within the processor of the devices.
Figure 4.
Two demonstrations of new features to expand the hearing aid functionality. The first image is how the fitness tracking data from Starkey’s hearing aids is shown to the wearer. The second image is a demonstration of how their first DNN-based denoising software worked [13]. The current generation of advanced hearing aids from Starkey incorporates a DNN accelerator embedded within the processor of the devices.
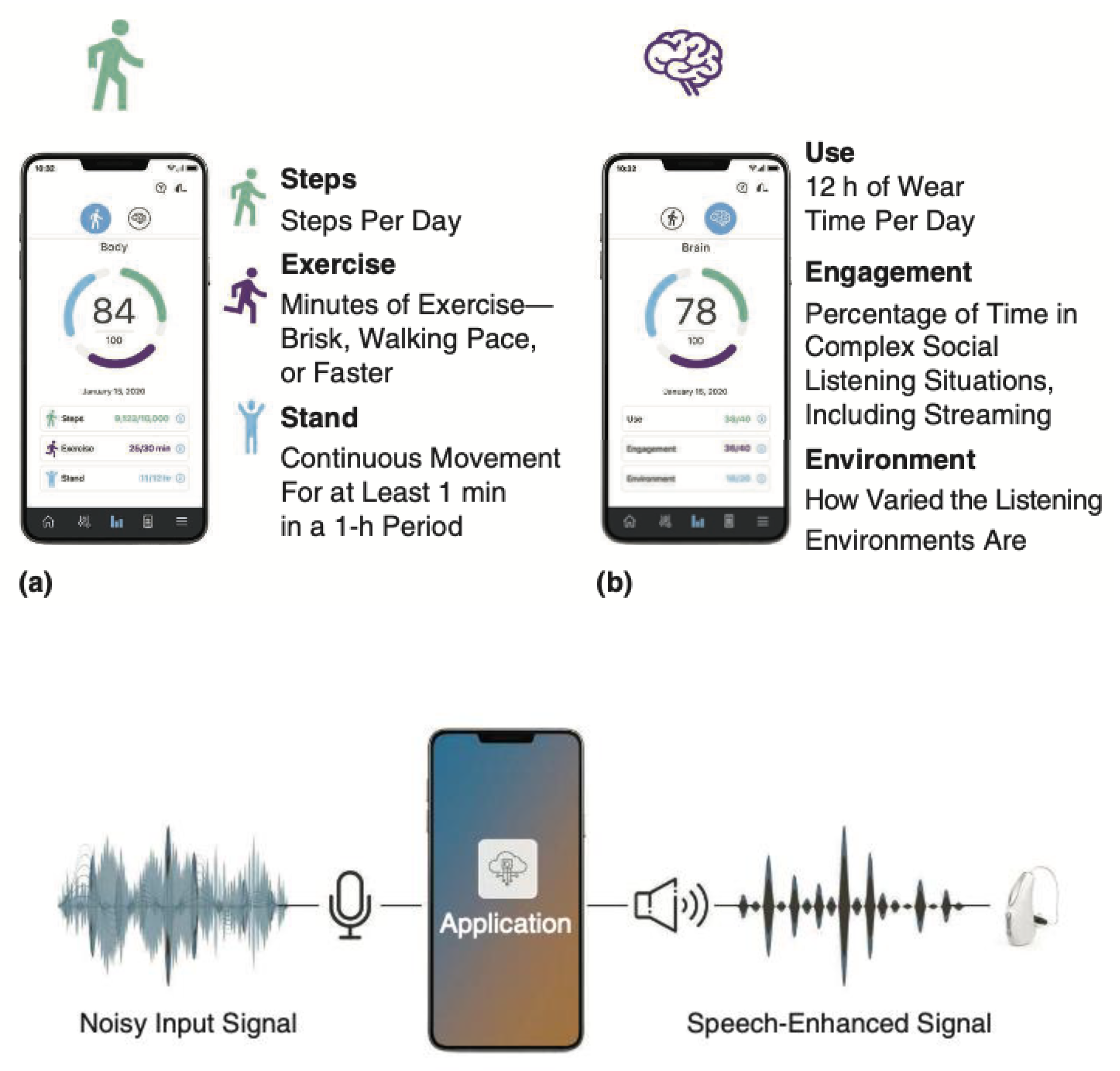

Table 1.
Presentation of systematically reviewed papers, identifying their authors, publishers, titles, dates, broadly categorized and specific foci, and key findings that support the review.
Table 1.
Presentation of systematically reviewed papers, identifying their authors, publishers, titles, dates, broadly categorized and specific foci, and key findings that support the review.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



