Submitted:
05 October 2024
Posted:
07 October 2024
You are already at the latest version
Abstract
Atopic dermatitis (AD) impacts various aspects of patients' lives. The most reported factors affecting clinical burden are itching and psychological disturbances (e.g., depression, anxiety or even suicidal thoughts). Also, AD affects school and work-related activities, even career advancement. Thus, AD patient management and decisions regarding advanced/systemic therapy are complex, requiring consideration of multiple disease-related factors: age; disease severity; patient medical history and comorbidities; previous topical therapy use and any adverse reactions; treatment efficacy concerns; patient preferences, expectations and fears; pregnancy planning; ability and willingness to adhere to the treatment regimen; impact on intimate and social relationships and work/school performance; and treatment-related risks and any associated psychological or psychiatric issues. Current guidelines and systematic reviews support the safety and efficacy of systemic therapy (conventional, biologics, JAK inhibitors) for treating AD. When topical therapy and phototherapy are insufficient, conventional systemic therapies (cyclosporine, methotrexate, azathioprine) are used, or advanced treatments can be introduced, like biologics and JAK inhibitors (baricitinib, upadacitinib, and abrocitinib), which have been approved for moderate to severe AD. Additional biologics being evaluated in clinical trials include lebrikizumab, nemolizumab, eblasakimab, and OX40/OX40L. Ultimately, there is great value in a personalized and multidisciplinary approach to AD management, as has been supported by numerous studies and clinical practice over time.
Keywords:
atopic dermatitis
; treatment
; quality of life
; disease burden
; therapy
; economic costs
; psychological aspects
; daily activities
; JAK inhibitors
; biologics
; dupilumab
; atopic eczema
1. Introduction
Atopic dermatitis (AD) is a chronic skin disease that often impacts emotional well-being, work productivity, daily activities, and more. The most common manifestations of AD include eczematous skin lesions, dryness, and itching, along with impaired sleeping. Clinically, AD is a dermatosis characterized by episodes of acute flare-ups and remissions, with symptoms that can vary [1,2]. In the acute stage of AD, lesions are erythematous, sometimes accompanied by exudation, erosions, crusts and scales. Gradually, chronic skin changes develop, often resulting in persistent lichenified lesions (Figure 1). Among the clinical features of AD, itching is most frequently reported, although its prevalence varies (ranging from 21% to 100%)[3,4,5,6]. The disease is more common in children but can occur at any age, presenting with various clinical pictures.
Not all aspects of the etiopathogenic processes underlying AD have been definitively established. Nevertheless, AD is recognized as a multifactorial disease with numerous etiological and contributing factors, including an impaired skin barrier, genetic predisposition, susceptibility to allergies, Th2-mediated immune responses, and decreased antimicrobial peptides among others [1,2,7,8,9].
The quality of life for patients with AD is significantly affected by the disease, with the extent of the impact largely dependent on its severity. Additionally, AD imposes a significant burden on society, primarily due to its high prevalence, which has increased since the late 20th century. This prevalence, in the general population, is notably higher in children (up to 10-20%) compared to adults (3–5%) [10,11,12]. Also, since psychological changes such as depression and anxiety are also common in AD patients, it is important to consider various factors when approaching the disease, rather than focusing solely on skin lesions [13].
Since AD is non-fatal by nature, it is often neglected compared to more severe and life-threatening diseases. However, several studies indicate it carries with it an enormous burden due to its significant impact on wellbeing and consequent psychosocial effects [14,15,16]. Thus, it is necessary to consider not only the clinical aspects of AD but the economic and human cost of the disease as well, remembering that both adults and adolescents are affected [13]. Understanding the burden of AD on individuals and society is key for designing effective public health policies, including intervention priorities and resource allocation [17]. Therefore, it is essential to evaluate the burden of AD through scientific evidence in order to inform both doctors and patients about the disease and its characteristics (Figure 2). It can help decision-makers in developing treatment strategies.
2. The Impact of Atopic Dermatitis on Emotional and Psychological States
Research indicates that the most reported factors affecting clinical burden are itching (pruritus) and psychological disturbances such as depression and anxiety (51% and 49%, respectively) [13]. Among the most significant impacts are its negative effect on sleep, primarily due to itching. This is supported by evidence of impaired sleeping indicators and decreased melatonin production [18,19]. While short-term sleep deprivation, such as a single night of poor sleep, is typically manageable, the impact of lack of sleep is significantly intensified in chronic diseases like AD. In such cases, sleep disorders occur in most patients. These disturbances can lead to additional issues, including reliance on sleeping pills, decreased concentration and lethargy [20].
In the past, AD was commonly known as "neurodermitis" due to the psychological features and changes observed in these patients, who were often perceived as neurotic [21]. This is because of the associated occurrence of anxiety and depression that significantly burdens AD patients compared to the general population. Numerous studies have reported a high prevalence of depression among patients with AD [3,22,23,24]. Research indicates that the prevalence of depression among these patients averages 18%, with a range from 3% to 57%. These findings align with self-reported data on depression, which average 26% (ranging from 10% to 37%) [25,26]. Moreover, the results of numerous studies show that the average prevalence of anxiety in AD patients is 24.12% (ranging from 1.2% to 64%). According to a study conducted in Iran, 50% of dermatological patients suffered from psychiatric comorbidities [27].
A particularly important topic to consider here is stress, which can both contribute to and result from AD. Studies indicate that psychological stress is prevalent among patients with AD, with 46% experiencing high stress and 21% experiencing moderate stress [21,28,29]. Many AD patients report an association between recent stressful events and disease exacerbation, a finding supported by research/literature data [30]. Physically, the visibility and functional impact of AD skin lesions often lead to low levels of happiness and higher levels of anxiety, depression and feelings of stress [31]. Negative social and psychological changes can also result in depression, anxiety, and even suicidal ideation (44%) and suicide attempts (36%) [29,32]. Physiologically, altered cortisol levels (as a marker of stress) have also been confirmed in AD patients. In the early phase of the disease, increased cortisol values were recorded (overactivated HPA axis). This stimulates skin neural structures, deteriorates the skin's Th2 response, and reinforces habitual scratching. In the later stages of AD, there is a weaker HPA axis function and a shift to a Th1-dominant response [21,33]. When taking the above into account, addressing the impact of stress on patients, especially young individuals with AD, could be vital for improving their mental health [7].
According to research comparing patients with AD during exacerbation to those who are asymptomatic (in AD remission), the severity of AD (as measured by SCORAD values) positively correlates with impaired quality of life (DLQI) and the overall impact of the disease on daily life and symptom management [34]. Impaired quality of life (DLQI) also associated with certain personality features (anxiety, obsession, depression, somatization). Thus, when managing patients, it is important to consider not only the severity of AD but also how personality characteristics such as anxiety disorders, somatization, obsession, and depression affect quality of life.
There have also been observations that certain habits and behaviours, such as smoking and alcohol use, may be linked to increased stress and depression in AD patients [7]. In turn, these habits negatively impact AD, leading to a vicious circle. According to literature, smoking stimulates the surface of immune cells, increases the total number of white blood cells, and increases Th2 cells responsible for allergic immune responses and IL-4 (key in the treatment of chronic inflammation). This process promotes the development of allergic diseases such as AD by enhancing hypersensitivity to environmental antigens [35]. Exposure to smoking, either through personal use or from household members and friends, increases the risk of developing AD [36]. Excessive alcohol consumption is also negatively associated with AD, as alcohol increases IgE production, which stimulates Th2 cells and exacerbates AD (similar to the effects of smoking). It also causes skin dryness and an acute inflammatory response due to histamine release from acetaldehyde [7,37,38,39].
Specific issues are also noted in sensitive populations such as adolescents who suffer from AD, who often struggle with body image due to chronic/recurrent inflammatory lesions. Thus, aesthetic and functional skin lesions lead to low happiness, high stress, and depression [3]. Additionally, smoking and alcohol consumption in adolescents with AD reduce immune function, which exacerbates the condition and increases stress and depressive symptoms. Overall, adolescents with AD may struggle with establishing a healthy body image and may experience significant social and psychological issues [29].
However, engaging in physical activities can help patients with AD reduce psychological stress. According to research results, those who engage in regular physical activity have a 30% lower risk of stress than those who do not. This is likely because physical activity helps reduce cortisol levels (secreted in significant amounts in response to stress) and helps produce and activate endorphins that directly affect the brain [40,41]. According to several studies, physical activity positively impacts the mental health of allergy sufferers (AD, asthma, and allergic rhinitis). However, in AD patients, physical activity may delay recovery of damaged skin, and sweating associated with it can cause itching and worsening; therefore, further research on this topic is needed [42,43].
In addition to the emotional, psychological and mental health issues associated with AD, social functioning problems ultimately arise [44]. Consequently, recent management guidelines for AD now emphasize the importance of addressing the psychological aspects of the disease, which may require psychosomatic counselling or sometimes even psychiatric drugs.
3. The Impact of Atopic Dermatitis on Daily Activities, Work Productivity, and Quality of Life
Patients with AD, particularly those with moderate to severe forms, often experience a noticeable impact on their effectiveness and productivity at work or school due to frequent exacerbations [45]. Aside from typical AD lesions, itching, and sleep disturbances, individuals with AD also have an atopic constitution that predisposes them to contact dermatitis, often on the hands. This additional skin condition can further disrupt their productivity and affect their work performance [46,47]. According to an international study, 32% of AD patients reported that the disease affects their school or work activities, while 14% noticed difficulties in career advancement [45]. AD significantly impacts productivity, with research showing 68.8 days lost annually due to absenteeism and productivity loss. Notably, productivity loss accounts for the majority of this impact, with 54 lost days, which is three times higher than absenteeism, which accounts for 14.8 lost days [48,49,50,51,52,53,54,55]. Productivity loss significantly depends on the severity of AD. According to literature data, patients with severe AD lost an average of 26.5 days due to absenteeism and 92.5 days due to productivity loss, while patients with mild AD lost an average of 2.5 days due to absenteeism and 13.6 days due to productivity loss [51,56].
Frequent doctor visits also have a significant impact on patients. According to studies, AD patients make between 2.8 to 16.3 visits to a dermatologist annually, with an average of 8.6 visits [50,57,58,59]. Additionally, visits to primary care or general practitioners average 16.5 annually and significantly depend on AD severity. For example, patients with moderate to severe AD had 20.44 annual visits to the doctor [58,60]. Furthermore, research shows that AD patients sometimes visit non-dermatological specialists, such as allergy and internal medicine specialists (with a rate of 0.2-0.4 visits annually) [50,58]. As the severity of AD increases, visits to the emergency department become more frequent, although admissions to the emergency room remain rare [59,60,61,62,63]. According to previous study results, the average annual number of emergency department visits varies: 0.5 per patient for milder cases (grade 2 severity), 0.92 visits for patients with grade 3 severity, and 1.41 visits for those with grade 4 severity [59,60,62]. The average annual number of hospitalizations ranged from 0.03 to 1.2 admissions—more frequent for patients with grade 4 severity (0.75 per year) than those with grade 2 severity (0.45 per year) [59,62,63].
4. Economic Costs of Atopic Dermatitis
The treatment of AD imposes a significant financial burden due to the disease’s prevalence and chronic nature. Indirect costs, such as loss of productivity, often exceed direct treatment costs. There is notable variability in cost estimates across studies from countries with different income levels. Based on multiple studies, the total cost of AD per patient, expressed as an average annual cost, is estimated at $5,246 (2020), with a range from $769 to $23,638 [50,51,60,64]. This average total cost is lower than the combined average of direct and indirect costs due to differences in data sources and calculation methods. Numerous studies have reported that the average annual direct costs reach $4,411 [50,65,66], while the average annual indirect costs have been reported in three studies and equal $9,068 [50].
Several studies on AD confirm significant reductions in patient quality of life and increased school or work absenteeism due to AD [13,67]. Findings on this topic vary across the literature. Drucker et al. estimated the total annual cost per patient in the U.S. to range from $3,302 to $4,463, while Fasseeh et al. estimated it at $4,411 (which is not limited to the U.S.) [13,63]. The burden of AD might be underestimated in low- and middle-income countries as, despite the abundance of literature on this subject, most research comes from high-income countries (low- and middle-income countries were not equally represented in the literature). A study on the global burden of disease found a positive correlation between the burden of AD and gross domestic product - however, this may be due to insufficient data and underreporting of AD in low- and middle-income countries [12].
5. Standard Therapy and Advanced Treatment Possibilities
The treatment of AD has significantly advanced, with regulatory institutions worldwide approving new drugs for AD patients, while other medications remain in various stages of clinical trials. Current AD therapy includes routine skincare, avoidance of triggers, topical and systemic treatment, and other measures. According to current global recommendations and guidelines, the treatment of AD primarily depends on the severity of the disease [24,68,69,71]. The 2018 guidelines classify AD severity into mild, moderate, and severe based on the SCORAD index/questionnaire (SCORAD >50 or persistent eczema is severe; SCORAD 25-50 or recurrent eczema is moderate; SCORAD <25 or transient eczema is mild).
However, regardless of severity, the primary treatment for all forms involves patient and family education, regular use of emollients and oil baths, and the identification and avoidance of environmental factors (non-specific irritants and specific allergens) that exacerbate the disease [68]. Typical topical AD therapy primarily involves topical corticosteroids, which are generally the most effective at controlling skin lesions [2]. However, these should be used for relatively short periods due to potential adverse effects such as skin atrophy, rebound phenomenon, telangiectasias, striae, folliculitis, purpura, contact dermatitis, adrenal suppression, etc. [2,69]. It is known that "corticophobia" is frequent among AD patients, therefore, when lesions persist, topical immunomodulators are recommended (tacrolimus and pimecrolimus) [2]. Another topical option is topical crisaborole, a boron-based phosphodiesterase 4 inhibitor (PDE-4), which inhibits overactive PDE-4 enzymes contributing to AD manifestations [2,69].
In addition, phototherapy, including UVB 311 nm, and occasionally UVA1 and PUVA, can be used for severe forms of AD in adults. Phototherapy is mainly administered two to three times per week.
When topical therapy and phototherapy are insufficient for the management of AD, there is a need for conventional systemic therapies (cyclosporine, methotrexate, azathioprine) or alternative systemic treatments, such as biologics and Janus kinase (JAK) inhibitors [2,68]. Conventional systemic drugs for AD include certain immunosuppressants that calm skin inflammation [2]. Among systemic medications for AD, only cyclosporine has been approved for AD, while azathioprine, methotrexate, and mycophenolate mofetil are prescribed off-label. Cyclosporine is an immunosuppressant that inhibits various immune cells (like T cells, NK cells, antigen presentation by APCs, and production of IL-2 and GM-CSF). However, while adverse reactions are multiple, they are relatively uncommon and include nephrotoxic effects, hypertension, changed blood counts, gingival hyperplasia, hypertrichosis, headaches, etc.). Methotrexate is an immunosuppressant that inhibits the synthesis of cell structures (DNA, RNA, purines), thereby inhibiting T cells. Its side effects include hepatotoxicity, leukopenia, thrombocytopenia, etc.. It is available in oral and subcutaneous forms and is typically taken with folic acid to mitigate adverse effects. Azathioprine, a purine analogue, blocks DNA synthesis in T and B cells. Its potential side effects include hepatotoxicity, gastrointestinal symptoms, leukopenia, etc. Mycophenolate mofetil is an immunosuppressant drug used to treat various autoimmune and inflammatory conditions. Its adverse effects include nausea, diarrhoea, infections, and other complications.
Recently, several drugs have been approved for moderate to severe AD, including biological drugs that predominantly inhibit interleukins (IL-4, IL-13, IL-33)[2,68].Dupilumab is a biologic that blocks IL-4 and IL-13 receptors and is indicated for patients with moderate to severe AD resistant to standard therapy. Though side effects are infrequent, they can include ocular complications, conjunctivitis, injection site reactions, etc. [21,72]. Tralokinumab is another biological agent, a monoclonal anti-IL-13 antibody, also indicated for moderate to severe AD unresponsive to topical preparations [73]. Additional biologics being evaluated in clinical trials include lebrikizumab, nemolizumab, eblasakimab, OX40/OX40L and others.
In addition to systemic therapies previously mentioned, three JAK inhibitors – baricitinib, upadacitinib, and abrocitinib – have been approved for moderate to severe AD. There is limited data available on the effectiveness of other JAK inhibitors (ruxolitinib, tofacitinib, and deucravacitinib) [2]. JAK inhibitors affect intracellular transducing signals, which in turn influence blood cell formation and the functioning of the immune system. JAKs phosphorylate and activate cell transcription, which modulates intracellular processes, including genetic expression. Nowadays, JAK inhibitors are among the best treatment options for severe AD due to their effectiveness and safety [2,74]. Based on real-life data results, they provide rapid improvement in AD symptoms (especially itching), leading to an improved patient quality of life. Although the safety profile is favourable, long-term safety data are still limited. Potential side effects include upper respiratory tract infections, increased blood lipids, nausea and abdominal pain, herpes virus infections, acne, creatine kinase elevation, thrombocytosis, headache, etc. [2]. One study (meta-analysis) by Silverberg et al. compared the effectiveness of targeted systemic therapies for the treatment of moderate to severe AD [24,69]. According to their results, upadacitinib 30 mg daily, upadacitinib 15 mg daily and abrocitinib 200 mg daily were the most effective targeted systemic therapies during their follow-up (12 to 16 weeks of AD treatment)[24].
However, when approaching patient care, it is important to note that therapy depends on the specific form of AD and the severity of the disease. For mild forms of AD, in addition to skin care, topical anti-inflammatory therapy (class II topical glucocorticoids) is recommended during periods of exacerbation [68]. If necessary, as in the case of secondary infection, treatment with antiseptic compresses or silver-infused wraps may be advised. For persistent AD lesions and specific areas (e.g., lesions on the face, neck, folds, and anogenital region), topical calcineurin inhibitors (tacrolimus ointment and pimecrolimus cream, approved for use in patients aged two years and older) are recommended as the therapy of choice. Systemic antibiotic therapy is recommended only in cases of extensive superinfections.
For moderate forms of AD, in addition to primary treatment, proactive therapy with topical tacrolimus or class II or III topical glucocorticoids is advised (e.g., for glucocorticoids twice weekly for up to 16 weeks, and calcineurin inhibitors for up to 52 weeks). For chronic lichenified lesions in AD that recur despite topical therapy, phototherapy (such as UVB) is advised. However, prior evaluation for potential contraindications and photosensitivity is needed [68].
For severe forms of AD where disease control is not achieved through primary treatment measures, topical therapies, phototherapy, or systemic immunosuppressive therapy are recommended for adults. Options include cyclosporine A (for 3 to 6 months), short-term oral glucocorticoids (up to 7 days), mycophenolate mofetil, and methotrexate. Phototherapy such as PUVA (psoralen and UVA), or alitretinoin (for isolated hand eczema) may also be considered. For moderate to severe forms of AD that do not respond to topical treatments and/or phototherapy and where systemic conventional therapy is not recommended, biological therapy is indicated. The first line of biological therapy is dupilumab, a monoclonal antibody that blocks IL-4 and IL-13 receptors. Additionally, psychological support and alternative treatment methods can also be considered [68].
Most AD patients have mild to moderate disease, which is usually well managed with emollients, standard topical anti-inflammatory preparations, and by avoiding triggers. However, a significant number of patients still do not achieve adequate control with this therapy [70]. For patients with moderate to severe AD who do not respond to topical therapy and where phototherapy is not suitable, systemic treatment is necessary to control the disease, reduce symptoms, prevent relapses, and improve quality of life (Figure 3). Nevertheless, when considering the introduction of systemic therapy for AD, it is crucial to carefully evaluate the known risks of conventional immunosuppressive treatments, such as the side effects of cyclosporine. Until recently, corticosteroid therapy was the most common systemic treatment for AD, with 10% of AD patients receiving this treatment, although it is less commonly employed in children with AD [71].
Guidelines and systematic reviews from national associations provide evidence of the safety and efficacy of systemic therapy (conventional, biologics, JAK inhibitors) for treating AD [68,71]. Thus, according to one study which examined AD patients' needs related to therapeutic goals (through a comprehensive survey of 1,678 AD patients), their most crucial therapeutic goal was to reduce itching, even more important than healing all skin lesions [4] However, many other AD-related needs are also essential, including perceived quality of life, as results show that AD patients experience significantly impaired quality of life (as confirmed by their DLQI scores). Although no significant differences in quality of life were found between men and women, significant differences were observed across different ages, e.g., older adults reported significantly lower quality of life compared to younger adults. General health levels were also lower in older adults than in younger adults, likely due to factors associated with ageing, such as reduced mobility and increased difficulties in daily activities.
Considering the impact of AD duration on patients, those with a shorter duration of AD (up to one year) experience greater impairment in quality of life compared to those with a longer duration (over one year). The difference is likely because newer patients have not yet adapted to the disease or developed effective coping strategies [4].
6. Decision to Initiate Systemic Therapy
Studies on the needs of AD patients and their therapy decisions indicate various disease-related requirements that significantly differ by age, gender, and disease duration, making it more critical for older patients to achieve therapeutic goals compared to younger individuals. This is particularly evident in their needs for fewer side effects, greater enjoyment of life, confidence in therapy, and reduced depression (based on surveys)[4]. However, the ability to lead a normal sexual life is more important for younger adults than for older ones, as anticipated. In terms of gender, women placed greater emphasis on achieving faster improvement in skin appearance, feeling more comfortable in public, healing all skin lesions, maintaining a normal daily life, and not fearing disease progression [4].
Different findings have been observed regarding the impact of disease duration on AD patients. According to a study by Augustin et al., patients with a shorter AD duration (up to one year) expressed a greater need for reassurance that the disease will not worsen, for healing all skin lesions, for a clear diagnosis and effective therapy, and for confidence in their treatment (i.e., those with shorter disease duration experienced a more significant burden)[4]. However, study results differ, as previous research had found that patients with longer disease duration may experience a more significant overall burden. It is also necessary to consider the patient's individual characteristics, such as age, gender, disease duration, and many other factors. Occasionally, there is a poor correlation between the patient's needs and their quality of life (DLQI). This discrepancy may suggest that patients' needs can differ significantly from their perceived burden of the disease and quality of life, highlighting the need for additional evaluation.
When approaching an AD patient who may be a candidate for systemic therapy, it is necessary to determine the severity of the disease using scoring scales that quantify AD severity (there are over 20 such scales available)[2,68,71]. The two most used scoring scales are the Scoring of Atopic Dermatitis (SCORAD) and the Eczema Area and Severity Index (EASI). The SCORAD scale assesses the intensity of disease manifestations, the extent of affected areas, sleep loss, and itching. The EASI score, on the other hand, provides a more comprehensive evaluation by incorporating additional clinical data. However, quantifying the severity of AD is often challenging because the lesions are sometimes diffuse and poorly defined. Many European dermatologists, for instance, prefer using a SCORAD >25 to categorize the disease as moderate to severe. However, relying on a single scoring scale has several drawbacks given the characteristic flares and remissions of AD. Multiple assessments are often needed to accurately reflect the baseline state of the disease, flares, and therapeutic responses. It is also important to evaluate the severity and frequency of AD flares using various methods, taking into account their impact on quality of life and the effectiveness of current therapy. Self-assessment scales, such as the Patient-Oriented Eczema Measure (POEM) and the Patient-Oriented SCORAD, can also be useful. These scales reflect the patient's perspective on the disease course between consultations. Repeated documentation of the presence of severe, extensive disease and/or significant impairment in quality of life (despite adequate topical therapy) can justify the transition to systemic therapy [71].
In addition to assessing the severity of the disease, it is also essential to consider the impact of the disease on their quality of life. Even localized AD affecting small areas (e.g., only the face, hands, or genital area) can significantly impact the patient's emotional state, social interactions, and daily activities. However, scoring scales are time-consuming for routine clinical practices and assess only certain aspects of the disease, making them primarily useful in clinical trials [71]. Moreover, an assessment based solely on a scoring system cannot determine the need for systemic therapy; a comprehensive and holistic assessment is still required.
From a therapeutic perspective, the availability of targeted immunomodulation, such as JAK inhibitors and biologics, with lower risks to patient safety, facilitates the introduction of systemic therapies by lowering the threshold for its use [2,68]. Experience with several advanced therapies, when compared to conventional treatments, indicates that these newer options may offer superior efficacy and short-term safety. Registries are valuable for evaluating long-term safety and efficacy profiles, allowing comparisons between conventional immunosuppressive therapies and emerging new therapies. The threshold for introducing advanced therapies is often lower in moderate AD, aiming to improve disease response and quality of life, as well as to potentially prevent disease progression and future comorbidities [71].
Overall, greater needs for AD treatment are observed with older age, more severe disease, and greater impairment in quality of life, with the extent of impairment correlating with an increased need for treatment. The most recent approach to treating patients with AD is focused on therapy that targets and achieves minimal disease activity (MDA), where the decision on therapy is based on both patient and clinician decisions [69]. In clinical practice, it is recommended that both physicians and patients collaborate in advance to identify specific needs and potential therapeutic goals, leading to an individualized and personalized therapeutic decision through a shared decision-making process and a multidisciplinary approach [4]. Thus, clinicians and patients (or caregivers) should consider multiple factors when deciding whether and when to introduce systemic therapy (Figure 3). However, universally accepted defined criteria are not yet defined [71].
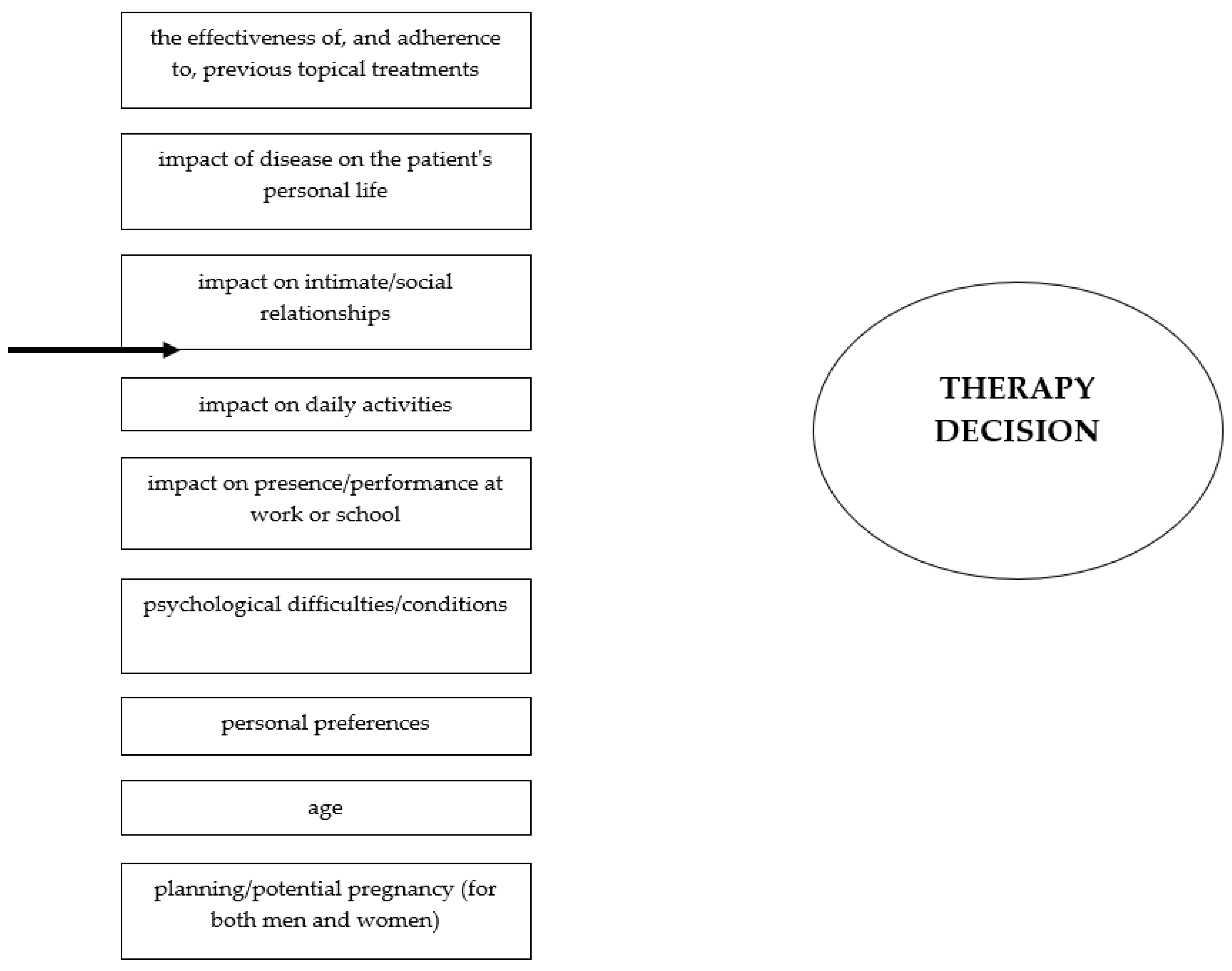
So, before initiating systemic therapy for AD, it is necessary to consider several key factors that determine whether a patient is a suitable candidate for this treatment. Systemic therapy is usually introduced for patients who fail to respond to adequate topical therapy or who experience frequent relapses, often requiring the prolonged use of high-potency topical corticosteroids. In patients with moderate to severe forms of AD, several factors should be considered, including frequent recurrences of the disease, previous adverse effects of therapy, such as skin atrophy, and the effectiveness and adherence to previous topical treatments. It is also important to assess the impact of the disease on the patient's personal life, including intimate aspects and pregnancy planning, social relationships, and engagement in activities. Additionally, the disease's impact on work or school performance and the presence of concurrent AD-related psychological difficulties or relevant prior psychological disorders should be evaluated. During discussions with the patient, it is necessary to determine their willingness and ability to adhere to the treatment regimen, understand their expectations for the treatment, and their concerns about side effects. When choosing systemic therapy, it is important to integrate the patient's medical history, treatment preferences, and risk factors associated with the therapy [68]. In addition, it is also important to consider associated factors such as atopic comorbidities, autoimmune diseases, cardiometabolic disorders, along with behavioural disorders, associated neuropsychiatric comorbidities, and others [75]. Potential allergens and comorbidities (primarily allergic diseases, like allergic asthma, allergic rhinoconjunctivitis, oral allergy syndrome, food allergy, etc.) should also be considered and treated [76,77]. For example, AD patients are often allergic to inhaled allergens (type I reactions) or, occasionally, to contact allergens (delayed type IV allergic reactions) [2,76]. These conditions also should be taken into account when deciding on therapy for AD.
It is important that patients are informed in advance by their dermatologists or other medical doctors about the effectiveness of the treatment and potential side effects. This information should be discussed with both the patient and their family. Therefore, a shared decision-making process that considers all these factors, along with the risks and benefits of each therapy, is recommended [71]. The best approach involves a personalized and multidisciplinary strategy that involves comprehensive care, potentially involving other professionals, such as psychologists, pulmonologists, allergists, ear–nose–throat specialists, immunologists, paediatricians, nutritionists, gastroenterologists, and psychiatrists. This approach helps optimize treatment by considering not only the patient's age and disease severity but also a range of disease-related and concomitant factors.
7. Conclusion
Overall, the management of patients with AD and decisions regarding systemic therapy are complex, requiring consideration of multiple factors. Overall, factors to consider before introducing systemic therapy for AD include: the severity of AD, treatment efficacy concerns, previous topical therapy and its adverse reactions, patient preferences, age, pregnancy planning, ability and willingness to adhere to the treatment regimen, patient expectations and fears, impact on personal life, intimate aspects, social relationships, work or school performance, patient history and comorbidities, therapeutic preferences, treatment-related risks, and any associated psychological or psychiatric issues. Therefore, coordinated activities involving physicians, patients, their families, and society are highly beneficial. When considering different aspects of AD management, a multidisciplinary approach has shown improvements in both clinical conditions and disease-related problems. This approach helps patients develop more effective coping mechanisms, gain more control over their AD, adhere to therapy, and ultimately improve their quality of life, as well as that of their families. This interdisciplinary and personalized approach has shown great value in clinical practice and is supported by studies that have demonstrated improvements in both AD symptoms and related complications.
Author Contributions
Conceptualization, L.L.-M.; methodology, validation, and investigation, L.L.-M., E.P., and L.Z.; resources and data curation, T.C., E.B., I.L., and L.S.; writing—original draft preparation, writing—review and editing, R.T., E.B. L.D., E.P., and M.Š.; supervision, L.L.-M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of this study are openly available in PubMed or available in other sources.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Russo, F.; Santi, F.; Cioppa, V.; Orsini, C.; Lazzeri, L.; Cartocci, A.; Rubegni, P. Meeting the needs of patients with atopic dermatitis: a multidisciplinary approach. Dermatitis. 2022, 33, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Lugović-Mihić, L.; Meštrović-Štefekov, J.; Potočnjak, I.; Cindrić, T.; Ilić, I.; Lovrić, I.; Skalicki, L.; Bešlić, I.; Pondeljak, N. Atopic dermatitis: disease features, therapeutic options, and a multidisciplinary approach. Life (Basel) 2023, 13, 1419. [Google Scholar] [CrossRef] [PubMed]
- Ameen, M.; Rabe, A.; Blanthorn-Hazell, S.; Millward, R. Prevalence and clinical profile of atopic dermatitis (AD) in England—a population-based cohort study using the Clinical Practice Research Datalink (CPRD) and Hospital Episode Statistics (HES). Value Health. 2020, 23, 745. [Google Scholar] [CrossRef]
- Augustin, M.; Langenbruch, A.; Blome, C.; Gutknecht, M.; Werfel, T.; Ständer, S.; Steinke, S.; Kirsten, N.; Silva, N.; Sommer, R. Characterizing treatment-related patient needs in atopic eczema: insights for personalized goal-oriented care. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 142–152. [Google Scholar] [CrossRef]
- Chee, A.; Branca, L.; Jeker, F.; Vogt, D.R.; Schwegler, S.; Navarini, A.; Itin, P.; Mueller, S.M. When life is itchy: What harms, helps, and heals from a patient’s perspective? Differences and similarities in skin diseases. Dermatol. Ther. 2020, 33, e13606. [Google Scholar] [CrossRef]
- Falissard, B.; Simpson, E.L.; Guttman-Yassky, E.; Papp, K.A.; Barbarot, S.; Gadkari, A.; Saba, G.; Gautier, L.; Abbe, A.; Eckert, L. Qualitative assessment of adult patients' perceptions of atopic dermatitis using natural language processing analysis in a cross-sectional study. Dermatol. Ther.(Heidelb.). 2020, 10, 297–305. [Google Scholar] [CrossRef]
- Park, J.H.; Prochnow, T.; Chang, J.; Kim, S.J. Health-related behaviors and psychological status of adolescent patients with atopic dermatitis: a web-based survey of Korean youth risk behavior in 2019. Patient Prefer. Adherence. 2023, 17, 739–747. [Google Scholar] [CrossRef]
- El Hachem, M.; Di Mauro, G.; Rotunno, R.; Giancristoforo, S.; De Ranieri, C.; Carlevaris, C.M.; Verga, M.C.; Dello Iacono, I. Pruritus in pediatric patients with atopic dermatitis: a multidisciplinary approach-summary document of the Italian expert group. Ital. J. Pediatr. 2020, 46, 1–9. [Google Scholar] [CrossRef]
- Bieber, T. Atopic dermatitis: an expanded therapeutic framework for a complex disease. Nat. Rev. Drug Discov. 2022, 21, 21–40. [Google Scholar] [CrossRef]
- Williams, H.; Stewart, A.; von Mutius, E.; Cookson, W.; Anderson, H.R. Is eczema really on the increase worldwide? J. Allergy Clin. Immunol. 2008, 121, 947–954.e15. [Google Scholar] [CrossRef]
- Ring, J.; Zink, A.; Arents, B.W.M.; Seitz, I.A.; Mensing, U.; Schielein, M.C.; Wettemann, N.; de Carlo, G.; Fink-Wagner, A. Atopic eczema: disease burden and individual suffering—results from a large EU study in adults. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1331–1340. [Google Scholar] [CrossRef] [PubMed]
- Laughter, M.R.; Maymone, M.B.C.; Mashayekhi, S.; Arents, B.W.M.; Karimkhani, C.; Langan, S.M.; Dellavalle, R.P.; Flohr, C. The global burden of atopic dermatitis: lessons from the Global Burden of Disease Study 1990–2017. Br. J. Dermatol. 2021, 184, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Fasseeh, A.N.; Elezbawy, B.; Korra, N.; Tannira, M.; Dalle, H.; Aderian, S.; Abaza, S.; Kaló, Z. The burden of atopic dermatitis in adults and adolescents: a systematic review of the literature. Dermatol. Ther. (Heidelb). 2022, 12, 2653–2668. [Google Scholar] [CrossRef] [PubMed]
- Mann, C.; Dreher, M.; Weess, H.G.; Staubach, P. Sleep disorders in patients with urticaria and atopic dermatitis: an underestimated burden. Acta Derm. Venereol. 2020, 100, 1–6. [Google Scholar] [CrossRef]
- Pedersen, C.J.; Uddin, M.J.; Saha, S.K.; Darmstadt, G.L. Prevalence and psychosocial impact of atopic dermatitis in Bangladeshi children and families. PLoS One. 2021, 16, e0249824. [Google Scholar] [CrossRef]
- Marron, S.E.; Cebrian-Rodriguez, J.; Alcalde-Herrero, V.M.; Garcia-Latasa de Aranibar, F.J.; Tomas-Aragones, L. Psychosocial impact of atopic dermatitis in adults: a qualitative study. Actas Dermosfiliogr. (Engl Ed). 2020, 111, 513–517. [Google Scholar] [CrossRef]
- Devleesschauwer, B.; Maertens de Noordhout, C.; Smit, G.S.; Duchateau, L.; Dorny, P.; Stein, C.; Van Oyen, H.; Speybroeck, N. Quantifying the burden of disease to support public health policy in Belgium: opportunities and limitations. BMC Public Health. 2014, 14, 1196. [Google Scholar] [CrossRef]
- Jaworek, A.K.; Jaworek, M.; Szafraniec, K.; Wojas-Pelc, A.; Szepietowski, J.C. Melatonin and sleep disorders in patients with severe atopic dermatitis. Postepy Dermatol. Alergol. 2021, 38, 746–751. [Google Scholar] [CrossRef]
- Bešlić, I.; Lugović-Mihić, L.; Vrtarić, A.; Bešlić, A.; Škrinjar, I.; Hanžek, M.; Crnković, D.; Artuković, M. Melatonin in dermatologic allergic diseases and other skin conditions: current trends and reports. Int. J. Mol. Sci. 2023, 24, 4039. [Google Scholar] [CrossRef]
- Yu, S.H.; Attarian, H.; Zee, P.; Silverberg, J.I. Burden of sleep and fatigue in US adults with atopic dermatitis. Dermatitis. 2016, 27, 50–58. [Google Scholar] [CrossRef]
- Meštrović-Štefekov, J.; Novak-Bilić, G.; Kuna, M.; Pap, N.; Lugović-Mihić, L. Psychological stress in patients with atopic dermatitis. Acta Dermatovenerol. Croat. 2018, 26, 297–303. [Google Scholar] [PubMed]
- Lee, S.H.; Lee, S.H.; Lee, S.Y.; Lee, B.; Lee, S.H.; Park, Y.L. Psychological health status and health-related quality of life in adults with atopic dermatitis: a national cross-sectional study in South Korea. Acta Derm. Venereol. 2018, 98, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, A.; Fujita, H.; Arima, K.; Inoue, T.; Dorey, J.; Fukushima, A.; Taguchi, Y. Health-care resource use and current treatment of adult atopic dermatitis patients in Japan: A retrospective claims database analysis. J. Dermatol. 2019, 46, 652–661. [Google Scholar] [CrossRef]
- Silverberg, J.I.; Lei, D.; Yousaf, M.; Janmohamed, S.R.; Vakharia, P.P.; Chopra, R.; Chavda, R.; Gabriel, S.; Patel, K.R.; Singam, V.; et al. Association of atopic dermatitis severity with cognitive function in adults. J. Am. Acad. Dermatol. 2020, 83, 1349–1359. [Google Scholar] [CrossRef]
- Arima, K.; Gupta, S.; Gadkari, A.; Hiragun, T.; Kono, T.; Katayama, I.; Demiya, S.; Eckert, L. The burden of atopic dermatitis among Japanese adults: an analysis of data from the 2013 National Health and Wellness Survey. J. Dermatol. 2018, 45, 390–396. [Google Scholar] [CrossRef]
- Eckert, L.; Gupta, S.; Gadkari, A.; Mahajan, P.; Gelfand, J.M. Disease burden in adults with atopic dermatitis: analysis of survey data from France, Germany, Italy, Spain, and the United Kingdom. J. Am. Acad. Dermatol. 2019, 81, 187–195. [Google Scholar] [CrossRef]
- Arbabi, M.; Zhand, N.; Samadi, Z.; Ghaninejad, H.; Golestan, B. Psychiatric comorbidity and quality of life in patients with dermatological diseases. Iran J. Psychiatry. 2009, 4, 102–106. [Google Scholar]
- Kwon, J.A.; Park, E-C. ; Lee, M.; Yoo, K-B.; Park, S. Does stress increase the risk of atopic dermatitis in adolescents? Results of the Korean Youth Risk Behavior Web-Based Survey (KYRBWS-VI). PLoS One. 2013, 8, e67890. [Google Scholar]
- Schut, C.; Weik, U.; Tews, N.; Gieler, U.; Deinzer, R.; Kupfer, J. Psychophysiological effects of stress management in patients with atopic dermatitis: a randomized controlled trial. Acta Derm. Venereol. 2013, 93, 57–61. [Google Scholar] [CrossRef]
- Lugović-Mihić, L.; Meštrović-Štefekov, J.; Cvitanović, H.; Bulat, V.; Duvančić, T.; Pondeljak, N.; Tolušić-Levak, M.; Lazić-Mosler, E.; Novak-Bilić, G. The COVID-19 pandemic and recent earthquake in Zagreb together significantly increased the disease severity of patients with atopic dermatitis. Dermatology (Basel, Switzerland) 2023, 239(1), 91–98. [Google Scholar] [CrossRef]
- Choi, C. Factors affecting life satisfaction among adolescents with atopic dermatitis. Stud. Korean Youth. 2015, 26, 111–144. [Google Scholar]
- Sandhu, J.K.; Wu, K.K.; Bui, T.-L.; Armstrong, A.W. Association between atopic dermatitis and suicidality: a systematic review and meta-analysis. JAMA Dermatol. 2019, 155, 178–187. [Google Scholar] [CrossRef]
- Pondeljak, N.; Lugović-Mihić, L. Stress-induced interaction of skin immune cells, hormones, and neurotransmitters. Clin. Ther. 2020, 42, 757–770. [Google Scholar] [CrossRef]
- Lugović-Mihić, L.; Meštrović-Štefekov, J.; Ferček, I.; Pondeljak, N.; Lazić-Mosler, E.; Gašić, A. Atopic dermatitis severity, patient perception of the disease, and personality characteristics: how are they related to quality of life? Life (Basel). 2021, 11, 1434. [Google Scholar] [CrossRef]
- Yanbaeva, D.G.; Dentener, M.A.; Creutzberg, E.C.; Wesseling, G.; Wouters, E.F. Systemic effects of smoking. Chest. 2007, 131, 1557–1566. [Google Scholar] [CrossRef]
- Krämer, U.; Lemmen, C.; Behrendt, H.; Link, E.; Schäfer, T.; Gostomzyk, J.; Scherer, G.; Ring, J. The impact of environmental tobacco smoke on eczema and allergic sensitization in children. Br. J. Dermatol. 2004, 150, 111–118. [Google Scholar] [CrossRef]
- McFadden, J.; Thyssen, J.; Basketter, D.; Puangpet, P.; Kimber, I. T-helper 2 immune skewing in pregnancy/early life: chemical exposures and development of atopic disease and allergy. Br. J. Dermatol. 2015, 172, 584–591. [Google Scholar] [CrossRef]
- Nakashima, C.; Ishida, Y.; Kitoh, A.; Otsuka, A.; Kabashima, K. Interaction of peripheral nerves and mast cells, eosinophils, and basophils in the development of pruritus. Exp. Dermatol. 2019, 28, 1405–1411. [Google Scholar] [CrossRef]
- Zhu, Y.-B.; Xu, L.; Wang, Y.; Zhang R, Wang, Y.C.; Li, J.B.; Mu, D. The posterior thalamic nucleus mediates histaminergic itch of the face. Neuroscience. 2020, 444, 54–63. [Google Scholar] [CrossRef]
- Kong, S.; Koo, J.; Lim, S.K. Association between stress and physical activity in Korean adolescents with atopic dermatitis based on the Korea Youth Risk Behavior Survey 2018-2019. Int. J. Environ. Res. Public Health. 2020, 17, 8175. [Google Scholar] [CrossRef]
- Mücke, M.; Ludyga, S.; Colledge, F.; Gerber, M. The impact of regular physical activity and fitness on stress reactivity measured using the Trier Social Stress Test protocol: a systematic review. Sports Med. 2018, 48, 2607–2622. [Google Scholar] [CrossRef] [PubMed]
- O’Dougherty, M.; Hearst, M.O.; Syed, M.; Kurzer, M. S:; Schmitz, K.H. Life events, perceived stress, and depressive symptoms in a physical activity intervention for young adult women. Ment. Health Phys. Act. 2012, 5, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Murota, H.; Yamaga, K.; Ono, E.; Murayama, N.; Yokozeki, H.; Katayama, I. Why does sweat lead to itching in atopic dermatitis? Exp. Dermatol. 2019, 28, 1416–1421. [Google Scholar] [CrossRef] [PubMed]
- Koszorú, K.; Borza, J.; Gulácsi, L.; Sárdy, M. Quality of life of patients with atopic dermatitis. Cutis. 2019, 104, 174–177. [Google Scholar] [PubMed]
- Zuberbier, T.; Orlow, S.J.; Paller, A.S.; Taïeb, A.; Allen, R.; Hernanz-Hermosa, J.M.; Ocampo-Candiani, J.; Cox, M.; Langeraar, J.; Simon, J.C. Patient perspectives on the management of atopic dermatitis. J. Allergy Clin. Immunol. 2006, 118, 226–232. [Google Scholar] [CrossRef]
- Japundžić, I.; Bembić, M.; Špiljak, B.; Parać, E.; Macan, J.; Lugović-Mihić, L. Work-Related Hand Eczema in Healthcare Workers: Etiopathogenic Factors, Clinical Features, and Skin Care. Cosmetics 2023, 10, 134. [Google Scholar] [CrossRef]
- Lugović-Mihić, L.; Ferček, I.; Duvančić, T.; Bulat, V.; Ježovita, J.; Novak-Bilić, G.; Šitum, M. Occupational contact dermatitis amongst dentists and dental technicians. Acta Clin. Croat. 2016, 55, 293–300. [Google Scholar] [CrossRef]
- Wei, W.; Ghorayeb, E.; Andria, M.; Walker, V.; Schnitzer, J.; Kennedy, M.; Chen, Z.; Belland, A.; White, J.; Silverberg, J.I. Real-world study evaluating the adequacy of existing systemic treatments for patients with moderate-to-severe atopic dermatitis (QUEST-AD): baseline treatment patterns and unmet needs assessment. Ann. Allergy Asthma Immunol. 2019, 123, 381–388.e2. [Google Scholar] [CrossRef]
- Eckert, L.; Gupta, S.; Amand, C.; Gadkari, A.; Mahajan, P.; Gelfand, J.M. The burden of atopic dermatitis in adults in the United States: data on healthcare resource utilization from the 2013 National Health and Wellness Survey. J. Am. Acad. Dermatol. 2018, 78, 54–61. [Google Scholar] [CrossRef]
- Ariëns, L.F.M.; Van Nimwegen, K.J.M.; Shams, M.; De Bruin, D.T.; Van der Schaft, J.; Van Os-Medendorp, H.; De Bruin-Weller, M. Economic burden of adult patients with moderate-to-severe atopic dermatitis indicated for systemic treatment. Acta Derm. Venereol. 2019, 99, 762–768. [Google Scholar] [CrossRef]
- Murota, H.; Inoue, S.; Yoshida, K.; Ishimoto, A. Cost-of-illness study for adult atopic dermatitis in Japan: a cross-sectional web-based survey. J. Dermatol. 2020, 47, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Le, P.H.; Vo, T.Q. Economic burden and productivity loss associated with eczema: a prevalence-based follow-up study in Vietnam. J. Pak. Med. Assoc. 2019, 69, S57–S63. [Google Scholar]
- Lin, Y.; Chu, C.; Cho, Y.; Lee, C.; Tsai, C.; Tang, C. PSY11 Work productivity and activity impairment among patients with atopic dermatitis in Taiwan. Value Health. 2019, 22, S376. [Google Scholar] [CrossRef]
- Langenbruch, A.; Radtke, M.; Franzke, N.; Ring, J.; Foelster-Holst, R.; Augustin, M. Quality of healthcare for atopic eczema in Germany: results of the national health study AtopicHealth. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Ezzedine, K.; Shourick, J.; Merhand, S.; Sampogna, F.; Taïeb, C. Impact of atopic dermatitis in adolescents and their parents: a French study. Acta Derm. Venereol. 2020, 100, 00294. [Google Scholar] [CrossRef]
- Andersen, L.; Nyeland, M.E.; Nyberg, F. Increasing severity of atopic dermatitis is associated with a negative impact on work productivity among adults with atopic dermatitis in France, Germany, the UK, and the USA. Br. J. Dermatol. 2020, 182, 1007–1016. [Google Scholar] [CrossRef]
- Katoh, N.; Saeki, H.; Kataoka, Y.; Etoh, T.; Teramukai, S.; Takagi, H.; Tajima, Y.; Ardeleanu, M.; Rizova, E.; Arima, K. Adult Atopic Dermatitis Disease Registry in Japanese patients with moderate to severe atopic dermatitis (ADDRESS-J): baseline characteristics, treatment history, and disease burden. J. Dermatol. 2019, 46, 290–300. [Google Scholar] [CrossRef]
- Shalom, G.; Babaev, M.; Kridin, K.; Schonmann, Y.; Horev, A.; Dreiher, J.; Cohen, A.D. Health service utilization by 116,816 patients with atopic dermatitis in Israel. Acta Derm. Venereol. 2019, 99, 370–374. [Google Scholar] [CrossRef]
- Eckert, L.; Gupta, S.; Amand, C.; Gadkari, A.; Mahajan, P.; Gelfand, J.M. Impact of atopic dermatitis on health-related quality of life and productivity in adults in the United States: analysis using the National Health and Wellness Survey. J. Am. Acad. Dermatol. 2017, 77, 274–279e3. [Google Scholar] [CrossRef]
- Sicras-Mainar, A.; Navarro-Artieda, R.; Carrillo, J.C. Economic impact of atopic dermatitis in adults: a population-based study (IDEA study). Actas Dermosifiliogr. (Engl. Ed.) 2018, 109, 35–46. [Google Scholar] [CrossRef]
- Dieris-Hirche, J.; Gieler, U.; Petrak, F.; Milch, W.; Te Wildt, B.; Dieris, B.; Herpertz, S. Suicidal ideation in adult patients with atopic dermatitis: a German cross-sectional study. Acta Derm. Venereol. 2017, 97, 1189–1195. [Google Scholar] [CrossRef] [PubMed]
- Girolomoni, G.; Luger, T.; Nosbaum, A.; Gruben, D.; Romero, W.; Llamado, LJ.; DiBonaventura, M. Economic and psychosocial burden of comorbidities in adults with moderate to severe atopic dermatitis in Europe: a cross-sectional survey analysis. Dermatol Ther.(Heildeb.). 2020, 11, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Drucker, A.M.; Qureshi, A.A.; Amand, C.; Villeneuve, S.; Gadkari, A.; Chao, J.; Kuznik, A.; Bégo-Le-Bagousse, G.; Eckert, L. Healthcare resource utilization and costs among adults with atopic dermatitis in the United States: a claims-based analysis. J. Allergy Clin. Immunol. Pract. 2018, 6, 1342–1348. [Google Scholar] [CrossRef] [PubMed]
- Launois, R.; Ezzedine, K.; Cabout, E.; Reguai, Z.; Merrhand, S.; Heas, S.; Seneschal, J.; Misery, L.; Taieb, C. The importance of out-of-pocket costs for adult patients with atopic dermatitis in France. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1921–1927. [Google Scholar] [CrossRef]
- Väkevä, L.; Niemelä, S.; Lauha, M.; Pasternack, R.; Hannuksela-Svahn, A.; Hjerppe, A.; Joensuu, A.; Soronen, M.; Ylianttila, L.; Pastila, R.; et al. Narrowband ultraviolet B phototherapy improves quality of life in patients with psoriasis and atopic dermatitis up to 3 months: results of an observational multicenter study. Photodermatol. Photoimmunol. Photomed. 2019, 35, 332–338. [Google Scholar] [CrossRef]
- Schild, M.; Weber, V.; Galetzka, W.; Enders, D.; Zügel, F.S.; Gothe, H. Health resource utilization and associated costs among patients with atopic dermatitis—a retrospective cohort study based on German health claims data. Value Health. 2020, 23, S745. [Google Scholar] [CrossRef]
- Reed, B.; Blaiss, M.S. The burden of atopic dermatitis. Allergy Asthma Proc. 2018, 39, 406–410. [Google Scholar] [CrossRef]
- Wollenberg, A.; Barbarot, S.; Bieber, T.; Christen-Zaech, S.; Deleuran, M.; Fink-Wagner, A.; Gieler, U.; Girolomoni, G.; Lau, S.; Muraro, A.; et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: Part I. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 657–682. [Google Scholar] [CrossRef]
- Silverberg, J.I.; Howe, W. Atopic dermatitis (eczema): pathogenesis, clinical manifestations, and diagnosis. Available online: https://www.uptodate.com/contents/atopic-dermatitis-eczema-pathogenesis-clinical-manifestations-and-diagnosis (accessed on 18 September 2024).
- Silverberg, J.I.; Gooderham, M.; Katoh, N.; Aoki, V.; Pink, A.E.; Binamer, Y.; Rademaker, M.; Fomina, D.; Gutermuth, J.; Ahn, J.; et al. Combining treat-to-target principles and shared decision-making: International expert consensus-based recommendations with a novel concept for minimal disease activity criteria in atopic dermatitis. J. Eur. Acad. Dermatol. Venereol. 2024. [Google Scholar] [CrossRef]
- Simpson, E.L.; Bruin-Weller, M.; Flohr, C.; Ardern-Jones, M.R.; Barbarot, S.; Deleuran, M.; Bieber, T.; Vestergaard, C.; Brown, S.J.; Cork, M.J.; et al. When does atopic dermatitis warrant systemic therapy? Recommendations from an expert panel of the International Eczema Council. J. Am. Acad. Dermatol. 2017, 77, 623–633. [Google Scholar] [CrossRef]
- Kojanova, M.; Tanczosova, M.; Strosova, D.; Cetkovska, P.; Fialova, J.; Dolezal, T.; Machovcova, A.; Gkalpakiotis, S. BIOREP Study Group. Dupilumab for the treatment of atopic dermatitis: Real-world data from the Czech Republic BIOREP registry. J. Dermatol. Treat. 2022, 33, 2578–2586. [Google Scholar] [CrossRef] [PubMed]
- Berger, T.G. Evaluation and management of severe refractory atopic dermatitis (eczema) in adults. Available online: https://www.uptodate.com/contents/evaluation-and-management-of-severe-refractory-atopic-dermatitis-eczema-in-adults#H1361784051 (accessed on 18 September 2024).
- Lauffer, F.; Biedermann, T. Einschätzungen zur Therapie der moderaten bis schweren atopischen dermatitis mit januskinaseinhibitoren [Janus kinase inhibitors for the treatment of atopic dermatitis-evaluation of current data and practical experience]. Dermatologie (Heidelb.). 2022, 73, 520–528. [Google Scholar] [PubMed]
- Thyssen, J.P.; Werfel, T.; Barbarot, S.; Hunter, H.J.A.; Pierce, E.; Sun, L.; Cirri, L.; Buchanan, A.S.; Lu, N.; Wollenberg, A. Maintained improvement in physician- and patient-reported outcomes with baricitinib in adults with moderate-to-severe atopic dermatitis who were treated for up to 104 weeks in a randomized trial. J. Dermatolog Treat. 2023, 34, 2190430. [Google Scholar] [CrossRef] [PubMed]
- Pols, D. H.; Wartna, J. B.; Moed, H.; van Alphen, E. I.; Bohnen, A. M.; Bindels, P. J. Atopic dermatitis, asthma and allergic rhinitis in general practice and the open population: a systematic review. Scan J Prim Health Care 2016, 34(2), 143–150. [Google Scholar] [CrossRef]
- Kelava, N.; Lugović-Mihić, L.; Duvančić, T.; Romić, R.; Šitum, M. Oral allergy syndrome--the need of a multidisciplinary approach. Acta Clin. Croat. 2014, 53, 210–219. [Google Scholar]
- Yu, J.; Milam, E.C. Comorbid scenarios in contact dermatitis: atopic dermatitis, irritant dermatitis, and extremes of age. J Allergy Clin Immunol Pract. 2024, 12(9), 2243–2250. [Google Scholar] [CrossRef]
Figure 1.
Common skin manifestation of atopic dermatitis in adults (image from the archive of the main author, Prof. L. Lugović-Mihić).
Figure 1.
Common skin manifestation of atopic dermatitis in adults (image from the archive of the main author, Prof. L. Lugović-Mihić).

Figure 2.
Areas of patient life affected by atopic dermatitis.
Figure 3.
Goals of therapy for atopic dermatitis.
Figure 3.
Factors influencing the decision over systemic therapy for atopic dermatitis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



