
Submitted:
04 October 2024
Posted:
05 October 2024
You are already at the latest version
Abstract
Background/Objectives: The introduction of robotic surgery has revolutionized surgical procedures bringing significant improvements in procedures such as radical prostatectomy. In Poland, robotic technology was first used in public healthcare in 2010 for colorectal surgery in Wrocław. Public funding for robotic urologic surgery began in 2022. The aim of this study is to evaluate the impact of integrating a stable source of funding on the development and utilization of robotic surgery. Methods: Using data from the National Health Fund, a retrospective analysis of these procedures was conducted, focusing on radical prostatectomies from the beginning of the funding period to November 2023. Results: The study showed that in the first year of public funding (2022), 2,149 radical prostatectomies were performed using robotic systems, and this number almost doubled to 4,331 by October 2023. Patients aged 60 years and older accounted for more than 80% of those undergoing robotic surgery. The rise in the popularity of robotic surgery is attributed to its advantages, including high precision, reduced invasiveness in the surgical field, minimized bleeding and pain, and reduced postoperative wound size. The use of robotic surgery also brings environmental benefits. Conclusions: The growing number of robot-assisted surgeries in Poland reflects the increasing role of robotics in medicine. These advances meet the growing demand for healthcare services and demonstrate the precision and effectiveness of robotic technology, potentially improving healthcare access and outcomes. Further implementation and refinement of robotic solutions are necessary to meet the changing needs of medical specialties.
Keywords:
Robotic-Assisted Surgery
; Robotic-Assisted Prostatectomy
; Healthcare financing
; medical robotics
1. Introduction
The growing number of robotic system services indicates the progressive development of robotics in medicine and surgery [1,2,3,4,5]. Robotic surgery has revolutionized urology, particularly in the treatment of prostate cancer, since the early 2000s [4,6,7,8,9,10,11]. Robotic systems offer improved visualization, high-resolution imaging, reduced tremor, improved dexterity, and improved clinical outcomes, including decreased postoperative pain, faster recovery, and lower complication rates, than traditional surgery [12,13]. However, despite these benefits, adoption has been slow in regions such as Poland, mainly because of high costs and limited public funding. Robotic surgery was first introduced in Poland in 2010 and public financing began in 2022 for radical prostatectomy, an essential treatment for prostate cancer [14]. Public funding has improved access to this advanced technology, which may lead to improved outcomes in a larger patient population. Although new tools can enhance patient safety, they pose challenges that require further research and analysis.
1.1. Robotic Technology in Surgery
The use of robotics in urological procedures has significantly improved surgical precision, patient outcome, and operative efficiency. Robotic systems facilitate the performance of tasks independently or under human guidance by using advanced effectors and receptors [3,4,12,13,15]. Robot-assisted surgery in urology has significantly improved the treatment of prostate cancer, offering three-dimensional visualization, increased precision, and reduced tremors [12,13]. In Poland, robotic technology was first used in 2010 at the Specialist Hospital in Wrocław to perform colorectal surgery in a 71-year-old man, and the procedures were financed by the hospital or external sources [14]. In April 2022, the Polish public health care system began financing robot-assisted radical prostatectomy under the reimbursement code "L31R - radical prostatectomy with the use of a robotic system.” This funding has expanded access to robotic surgery, particularly in urology, and offers clinical benefits, such as increased precision, reduced blood loss, faster recovery, and improved patient outcomes [16]. For example, the da Vinci platform provides high-resolution 3D visualization and tremor-filtered control, enabling precise dissection and suturing, which is particularly critical in restricted pelvic anatomy during prostate surgery [12,13]. The decision to fund robotic surgery aligns with global trends in which robotics is becoming increasingly the standard of care. This change is expected to significantly improve the quality of surgical care in Poland, particularly for patients with prostate cancer, and may pave the way for broader application in other surgical specialties. This study aimed to analyze the impact of public funding on the adoption of robot-assisted radical prostatectomy in Poland by examining trends in procedure volume, patient demographics, and healthcare expenditure since the implementation of public financing.
2. Materials and Methods
This retrospective analysis was conducted using data from the National Health Fund (NFZ) database, focusing on robotic radical prostatectomy procedures in Poland. This study covers the period from April 2022, when public funding for these procedures began, to November 2023, the last month for which complete data were reported.
2.1. Data Collection and Sources
Data were collected from the National Health Fund (NFZ), which manages and maintains detailed records of publicly funded healthcare services in Poland. The National Health Fund collects information from healthcare providers that are reimbursed for services in the public healthcare system. Data included patient demographics, types of procedures performed, healthcare facilities, and related costs [17]. The analysis focused on medical services coded as L31R, which means "radical prostatectomy using a robotic system." These codes, as part of the "Homogeneous Patient Group" (HPG) or Homogeneous Patient Groups, provide precise categorization and tracking of medical services, allowing the study to focus specifically on procedures related to robot-assisted radical prostatectomy [18]. Healthcare providers reported the number of procedures performed for the NHF and detailed patient information, including age, diagnosis, and clinical information. Data were aggregated, anonymized, and made available to researchers who could access them for epidemiological research and healthcare analysis. This dataset enables researchers to analyze trends in healthcare services, such as the number of radical prostatectomies performed, patient outcomes, and the financial costs of such procedures over time. Data collected by the National Health Fund are helpful in retrospective analyses of medical procedures such as the increase in the number of robot-assisted radical prostatectomies in Poland after the introduction of public financing in 2022. By comparing annual procedure volumes, patient demographics, and outcomes, researchers can assess the impact of new financing models on the availability and efficiency of healthcare services [19]. The structured and detailed data collection process of the National Health Fund provides a solid basis for healthcare analysis, supporting clinical research, and policy decisions to improve patient care in Poland.
2.2. Inclusion and Exclusion Criteria
The analysis included all patients who underwent robot-assisted radical prostatectomy financed by the public health care system (NFZ) between April 2022 and November 2023. Exclusion criteria included procedures not funded by the public payer or surgeries unrelated to prostate cancer treatment.
2.3. Data Standardization and Financial Adjustments
Financial data were adjusted using the 2018 purchasing power parity (PPP) exchange rate to allow for international comparisons, which was calculated as 1 USD = 1787 PLN. This adjustment allows for comparisons between countries by eliminating differences in price levels [16]. Final cost data were presented in Polish zloty (PLN) and U.S. dollars (USDPPP) to standardize the financial analysis and facilitate the international context.
2.4. Analysis Methodology
The analysis assessed vital factors, such as procedure volume, patient demographics, and healthcare costs.
The total number of robot-assisted radical prostatectomies performed during the study period was calculated. The age distribution of patients undergoing the procedure was determined and aggregated into appropriate age groups. The financial burden of robotic prostatectomies in the Polish healthcare system during the study period was analyzed. The number of procedures and trends in financial expenditure were tracked and compared across age groups.
2.5. Statistical Analysis
All data were analyzed using descriptive statistics. Continuous variables, such as the number of procedures and associated costs, are expressed as means with standard deviations. Categorical variables such as patient age were reported as percentages. The association between the number of procedures and healthcare expenditures was also assessed to determine whether the increased use of robotic surgery had a proportional effect on healthcare costs. The correlation between the number of procedures and total healthcare expenditure was analyzed to identify significant trends.
2.6. Ethical Considerations
All data used in this study were obtained from publicly available NHF datasets, which ensured compliance with ethical standards regarding patient confidentiality and data protection. The NHF anonymized all patient data before making them available for analysis, thus ensuring that no personal or confidential information was available to the researchers.
3. Results
In Poland, despite the use of robotic systems since 2010 (over 13 years), it was only in mid-2022 that these procedures began to be financed by the public payer [7]. In the early period of financing radical prostatectomy procedures (the year when public funding began, 2022), the public payer financed these procedures for 2,149 patients the following year (partial data until October 2023), almost doubling the number of patients treated using this technology to 4,331 [Figure 1].
Eligibility for patient qualifications involves a specific medical specialty and a confirmed malignant tumor diagnosis. Concurrently, the NFZ President's regulation [7] specified substantive conditions, particularly the surgeons' experience in performing the procedures. In the initial period of financing (2022), more than 2,100 radical prostatectomies using a robotic system were performed, and in the subsequent year, an increase of more than 120% was noted [Figure 1]. The increase in patient numbers correlates with public payer expenses [Figure 2], which amounted to 60,086 thousand PLN (33,207 thousand USD PPP) in 2022 and 121,262 thousand PLN (67,857 thousand USD PPP) in 2023.
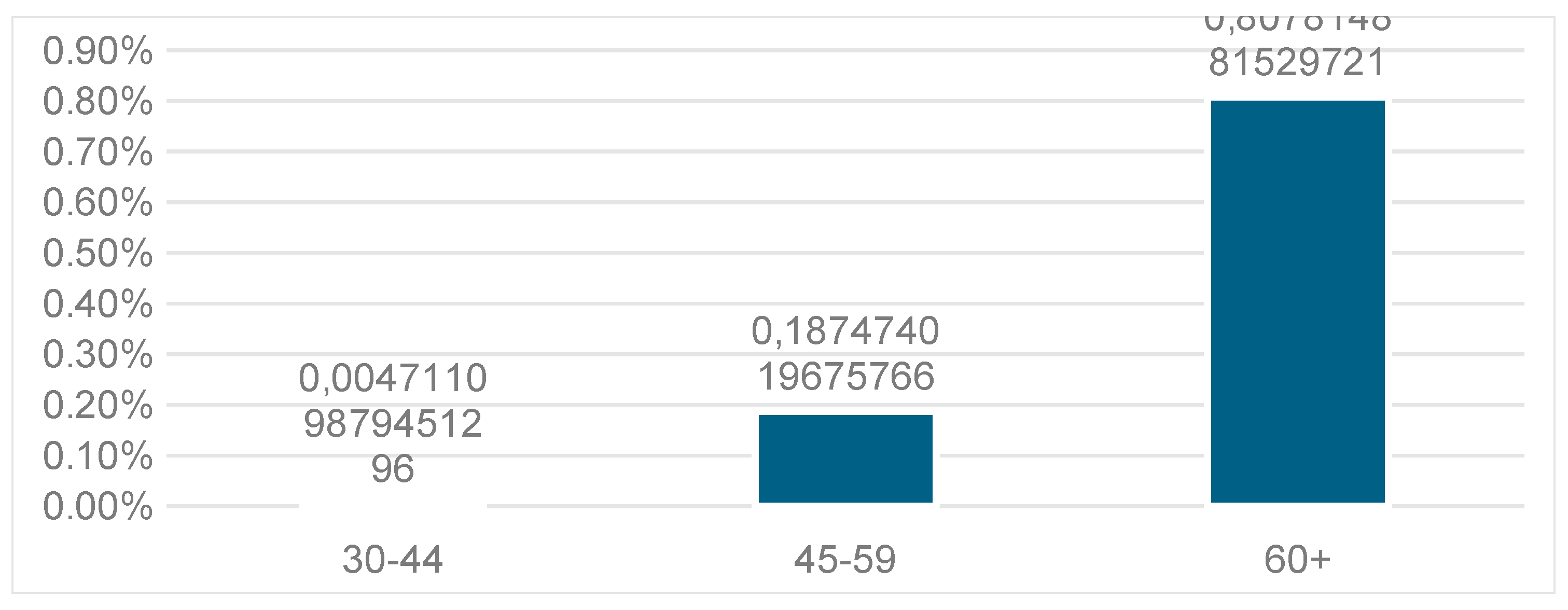
Patients aged ≥ 60 years accounted for over 80% of those who received robotic technology services [Figure 3].
Robotic technologies were the least used by younger patients (age group 30-44 years - 0.47%). The cost and funding distributions across age groups were similar, averaging approximately 25,000 PLN per patient (14,450 USDPPP).
4. Discussion
Robot-assisted radical prostatectomy (RARP) has become the leading surgical approach for the treatment of prostate cancer owing to its precision and minimally invasive nature. Prostate cancer remains the second leading cause of cancer-related death in men, underscoring the importance of advances in surgical treatment to improve patient outcomes [20]. Although robotic systems were introduced in Poland in 2010, their widespread use remained limited until the introduction of public funding for the RARP in 2022. Prostatectomy is one of the most frequently performed procedures assisted by robotic systems [19] worldwide, including Poland. The use of robotic technology in the surgical treatment of malignant tumors highlights the need for its implementation by patients and healthcare professionals [19].
Our analysis showed a significant increase in procedures after public funding was obtained, doubling the number of patients in one year. This highlights the critical role of healthcare funding in expanding access to advanced medical technologies.
The application of robotics in medicine is global and increasingly common; this surgery technology allows for high precision, reduced operative field size, and minimized bleeding, pain, or infection risk post-surgery. The development of robotic surgery is most noticeable in the United States, where many companies focus on surgical procedures [21]. Prostatectomy is a recognized procedure in the U.S. urology field that uses surgical robots [22].
Since the U.S. Food and Drug Administration (FDA) approved the innovative da Vinci robotic platform, a fourth-generation platform has been introduced [23]. A literature analysis indicates that laparoscopic radical prostatectomy using a robotic system is the preferred form of this procedure for many patients [13,24,25].
Data analysis conducted in the U.K. from to 2017-2019 shows that 88% of all radical prostatectomy services were performed using a robotic system [13]. As indicated, the number of radical prostatectomy procedures using surgical robots in Poland doubled after these procedures were included in the public funding catalog [Figure 1]. The Minister of Health's decision results from societal demand for technological solutions in clinical practice [19]. Moreover, the increase in services the year after public funding introduction may be due to growing public awareness [19].
Over 80% of the patients in Poland who underwent radical prostatectomy using a robotic system were aged over 60 years. Factors influencing this result include the average age of cancer onset and the increasing incidence rate (at diagnosis) with age [26]. Although technological advancements are less "acceptable" to older individuals (there is still a need for an essential personal patient-doctor relationship in this group) [27], they are the primary beneficiaries of services using medical robots [Figure 3]. It is important to note that the application of robotic surgical systems worldwide is not limited to radical prostatectomy procedures [2,3,4,13,15,28]. Owing to its minimally invasive nature, the da Vinci robotic surgical system is also used in pediatric urology for urinary tract reconstruction procedures [29].
Studies have consistently demonstrated the ability of RARP to minimize complications, such as urinary incontinence and erectile dysfunction, which are common challenges in prostate cancer surgery. Nerve-sparing RARP has been shown to provide equivalent oncologic outcomes, such as biochemical recurrence and tumor-specific survival, compared to non-nerve-sparing techniques, even in high-risk patients. This highlights the role of RARP in preserving critical structures, while maintaining effective cancer control. International comparisons and cost-effectiveness: International data further support the superiority of RARP over the traditional laparoscopic methods. Robot-assisted prostatectomy has resulted in better long-term cancer control, justifying the high initial costs of robotic systems [8,9,10,11]. Although RARP requires a significant initial investment, its ability to reduce biochemical recurrence rates and improve patient outcomes over time makes it a cost-effective treatment option for prostate cancer. These global trends are consistent with our findings in Poland, where public funding significantly increased access to robotic surgery. In addition to improving cancer control, RARP improves patient recovery and postoperative outcomes. Studies have indicated that RARP leads to shorter hospital stays, less blood loss, and faster recovery than open surgery [4,6,7,8,9,10,11]. The minimally invasive nature of robotic surgery lowers complication rates and benefits patients and healthcare systems by reducing the costs associated with extended hospital stays and postoperative complications. Demographically, more than 80% of patients undergoing RARP in Poland are aged 60 years or older, reflecting the typical demographics of patients with prostate cancer. Older patients may be less familiar with technological advances and less likely to ask about robotic procedures if they have already undergone surgery. However, the precision and reduced invasiveness of RARP makes it particularly beneficial for this age group, which is more susceptible to postoperative complications. There is also an increasing demand for RARP among older patients in Poland, which suggests an increase in public awareness of the benefits of robotic surgery. Despite the advantages of the RARP, expanding its use in Poland is associated with financial challenges. The high cost of robotic systems, maintenance, and associated consumables still limits their widespread adoption. Although public funding has significantly improved access, financial constraints may limit the availability of these procedures in some regions or patient groups.
Nevertheless, cost-effectiveness analyses in the U.K. indicate that RARP is a worthwhile long-term investment, further underlining the need for strategic resource allocation to sustain this growth [11]. In addition to its clinical and financial benefits, robotic surgery can reduce the environmental impact on healthcare. Studies indicate that RARP produces less carbon dioxide owing to shorter operating times, reduced resource consumption, and reusable materials, making it a more environmentally sustainable option [11]. Minimal invasiveness is beneficial for the postoperative recovery process. Initially, radical prostatectomy was associated with extensive blood loss [30]. With the introduction of laparoscopic and robotic surgery procedures, morbidity has been reduced [31,32,33,34]. Increased precision in preserving neural and vascular structures and improved visualization during robot-assisted surgery have reduced the rates of urinary incontinence or erectile dysfunction following robot-assisted surgery [35].
The future increase in robotic surgical system procedures may also be influenced by the growing environmental awareness [36,37]. A multicenter study conducted in 2023 [38] comparing laparoscopic and robotic surgery indicated that robotic surgical systems have a positive impact on the global climate. The study showed that the radical prostatectomy procedure using a surgical system generates less carbon dioxide emissions due to shorter operation times, hospital stays, and reusable materials[37].
As healthcare systems increasingly prioritize environmental sustainability, this may further accelerate the adoption of robotic surgery. Following global trends, the use of robotic systems in Poland is likely to expand to other surgical specialties. Further investment in robotic technology and research on cost-effectiveness and sustainability will be crucial for integrating robotic surgery into the Polish healthcare system.
5. Conclusions
The growing number of services that use robotic systems indicates the progressive development of robotics in medicine. The implemented solutions can respond to the ever-increasing demands for medical services. The precision and effectiveness of robotic technology procedures, shortening recovery and hospitalization time, can increase the availability of medical services. The development of robotics in medicine and the implementation of robotic systems in clinical practice in Poland are still at an early stage compared with other countries. Meeting the challenges and needs resulting from technological progress and the direction of its development is possible owing to further implementation and improvement of solutions in the field of robotic applications in medicine in various medical specialties. Public funding for robot-assisted radical prostatectomy (RARP) in Poland has significantly increased access to this advanced surgical technology, doubling the number of procedures during the first year of implementation. RARP offers numerous benefits, including increased precision, reduced postoperative complications, and faster recovery, which contribute to improved patient outcomes, particularly in the treatment of prostate cancer. The results of this study are consistent with global trends, showing that RARP significantly reduces complications, such as urinary incontinence and erectile dysfunction, compared with traditional techniques. The increased availability of prostatectomy procedures combined with reduced postoperative complications demonstrates that RARP is an effective treatment option for prostate cancer, especially in older patients, who are the primary beneficiaries of these minimally invasive procedures. However, high robotic systems and maintenance costs remain significant barriers to their wider adoption. Despite the long-term cost-effectiveness of RARP, further research on resource allocation and cost management is necessary to ensure its sustainable expansion.
Furthermore, the potential of robotic systems to reduce the environmental impact of surgical procedures further supports their adoption as healthcare systems worldwide, thereby increasing sustainability. In conclusion, the implementation of robotic surgery in Poland represents a significant step forward in prostate cancer treatment driven by public demand and government funding. Further investment in robotic technology and research into cost management and environmental sustainability are critical to expanding access to services and improving patient outcomes across the healthcare spectrum.
Author Contributions
Conceptualization, A.Ś., and T.K.; methodology, A.Ś., and W.G.; software, K.F., and T.K.; validation, M.B.; formal analysis, M.S.; investigation, A.Ś.; resources, M.S. and K.F.; data curation, A.Ś., and T.K.; writing—original draft preparation, M.S. and K.F.; writing—review and editing, W.W. and W.G.; visualization, W.W., and M.B.; supervision, W.G.; project administration, M.B., and W.G.; funding acquisition, A.Ś. All the authors have read and agreed to the published version of the manuscript.
Funding
This study received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Torrent-Sellens, J.; Jiménez-Zarco, A.I.; Saigí-Rubió, F. Do People Trust in Robot-Assisted Surgery? Evidence from Europe. Int J Environ Res Public Health 2021, 18. [Google Scholar] [CrossRef]
- Yagur, Y.; Martino, M.A.; Sarofim, M.; Almoqren, M.; Anderson, H.; Robertson, J.; Choi, S.; Rosen, D.; Chou, D. Implementation and outcomes in benign gynecological surgery with HUGO™ RAS system 12 months initial experience. J Robot Surg 2024, 18, 350. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Chen, J.; Wang, B.; Liu, X.; Jiang, S.; Li, Z.; Li, W.; Li, Z.; Wei, F. Evaluating the Status and Promising Potential of Robotic Spinal Surgery Systems. Orthop Surg 2024. [Google Scholar] [CrossRef] [PubMed]
- Falola, A.F.; Dada, O.S.; Adeyeye, A.; Ezebialu, C.O.; Fadairo, R.T.; Okere, M.O.; Ndong, A. Analyzing the emergence of surgical robotics in Africa: a scoping review of pioneering procedures, platforms utilized, and outcome meta-analysis. J Minim Invasive Surg 2024, 27, 142–155. [Google Scholar] [CrossRef] [PubMed]
- Iftikhar, M.; Saqib, M.; Zareen, M.; Mumtaz, H. Artificial intelligence: revolutionizing robotic surgery: review. Ann Med Surg (Lond) 2024, 86, 5401–5409. [Google Scholar] [CrossRef]
- Wu, Z.; Wang, Z.; Moschovas, M.C.; Bertolo, R.; Campi, R.; Rivas, J.G.; Wei, Y.; Xia, D.; Xu, B.; Zhu, Q.; et al. Robot-assisted Single-port Radical Prostatectomy with the SHURUI SP and da Vinci SP Platforms: Comparison of the Technology, Intraoperative Performance, and Outcomes. Eur Urol Open Sci 2024, 67, 26–37. [Google Scholar] [CrossRef]
- Olivero, A.; Tappero, S.; Chierigo, F.; Maltzman, O.; Secco, S.; Palagonia, E.; Piccione, A.; Bocciardi, A.M.; Galfano, A.; Dell'Oglio, P. A Comprehensive Overview of Intraoperative Complications during Retzius-Sparing Robot-Assisted Radical Prostatectomy: Single Series from High-Volume Center. Cancers (Basel) 2024, 16. [Google Scholar] [CrossRef]
- Nguyen, T.T.; Moukhtar Hammad, M.A.; Dobbs, R.W.; Vuong, H.G.; Basilius, J.; Quy, K.; Ngo, H.T.T.; Nguyen, A.; Tran, T.T.M.; Khanmammadova, N.; et al. A comparison of surgical outcomes between outpatient and inpatient robot-assisted radical prostatectomy: A systematic review and meta-analysis. Prostate International 2024. [Google Scholar] [CrossRef]
- Chislett, B.; Omran, G.; Harvey, M.; Bolton, D.; Lawrentschuk, N. Progressing Towards Same-Day Discharges After Robotic-Assisted Radical Prostatectomy; Safe and Cost Effective to Discharge Without Routine Blood Tests. Res Rep Urol 2023, 15, 471–477. [Google Scholar] [CrossRef]
- Chandrasekar, T.; Tilki, D. Robotic-assisted vs. open radical prostatectomy: an update to the never-ending debate. Translational Andrology and Urology 2018, S120–S123. [Google Scholar] [CrossRef]
- Wang, L.; Wang, B.; Ai, Q.; Zhang, Y.; Lv, X.; Li, H.; Ma, X.; Zhang, X. Long-term cancer control outcomes of robot-assisted radical prostatectomy for prostate cancer treatment: a meta-analysis. Int Urol Nephrol 2017, 49, 995–1005. [Google Scholar] [CrossRef] [PubMed]
- Koukourikis, P.; Rha, K.H. Robotic surgical systems in urology: What is currently available? Investig Clin Urol 2021, 62, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Handa, A.; Gaidhane, A.; Choudhari, S.G. Role of Robotic-Assisted Surgery in Public Health: Its Advantages and Challenges. Cureus 2024, 16, e62958. [Google Scholar] [CrossRef] [PubMed]
- J., G. Robot da Vinci w Polsce – zastosowanie, dostępność, NFZ. Available online: https://www.zwrotnikraka.pl/robot-da-vinci-w-polsce-zastosowanie/ (accessed on accessed on 16 April 2024).
- Rudnicka, Z.; Pręgowska, A.; Glądys, K.; Perkins, M.; Proniewska, K. Advancements in artificial intelligence-driven techniques for interventional cardiology. Cardiol J 2024, 31, 321–341. [Google Scholar] [CrossRef] [PubMed]
- Development, O.f.E.C.-o.a. OECD. Purchasing Power Parities (PPP). Available online: https://data.oecd.org/conversion/purchasing-power-parities-ppp.htm (accessed on 16 April 2024).
- National Health Fund, Annual Report 2021]. https://www.nfz.gov.pl/raport2021. National Health Fund, 2022, Annual Report 2021], https://www.nfz.gov.pl/raport2021. Available online: https://www.nfz.gov.pl/raport2021 (accessed on 16 october 2024).
- [National Health Fund, JGP Information [JGP Information Brochure]. https://www.nfz.gov.pl/jgp]. [National Health Fund, 2023, JGP Information [JGP Information Brochure]. Available online: https://www.nfz.gov.pl/jgp (accessed on 16 october 2024).
- Sosnowski, R.; Jakubiak, K.; Kamecki, H.; Kade, G.; Drewa, T.; Szydełko, T.; Chłosta, P.; Kania, P.; Jarzemski, P. Robot-Assisted Surgery in Poland: The Past, the Present, and the Perspectives for the Future. Société Internationale d’Urologie Journal 2024, 5, 142–147. [Google Scholar] [CrossRef]
- OECD iLibrary. Krajowe profile dotyczące nowotworów: Polska 2023; OECD Publishing: Paris, F., 2023. Krajowe profile dotyczące nowotworów: Polska 2023. [CrossRef]
- States., i.R.T.R.S.C.i.t.U. iData Research. Top 8 Robotic Surgery Companies in the United States. Available online: https://idataresearch.com/top-robotic-surgery-companies-in-the-united-states/ (accessed on 6 may 2024).
- Chung, G.; Hinoul, P.; Coplan, P.; Yoo, A. Trends in the diffusion of robotic surgery in prostate, uterus, and colorectal procedures: a retrospective population-based study. J Robot Surg 2021, 15, 275–291. [Google Scholar] [CrossRef]
- Dobbs, R.W.; Halgrimson, W.R.; Talamini, S.; Vigneswaran, H.T.; Wilson, J.O.; Crivellaro, S. Single-port robotic surgery: the next generation of minimally invasive urology. World J Urol 2020, 38, 897–905. [Google Scholar] [CrossRef]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur Urol 2021, 79, 243–262. [Google Scholar] [CrossRef]
- De Marchi, D.; Mantica, G.; Tafuri, A.; Giusti, G.; Gaboardi, F. Robotic surgery in urology: a review from the beginning to the single-site. AME Medical Journal 2021, 7. [Google Scholar] [CrossRef]
- Risk., N.C.I.A.a.C. Age and Cancer Risk. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/age (accessed on 6 may 2024).
- Roine, R.; Ohinmaa, A.; Hailey, D. Assessing telemedicine: a systematic review of the literature. Cmaj 2001, 165, 765–771. [Google Scholar]
- Doulgeris, J.J.; Gonzalez-Blohm, S.A.; Filis, A.K.; Shea, T.M.; Aghayev, K.; Vrionis, F.D. Robotics in Neurosurgery: Evolution, Current Challenges, and Compromises. Cancer Control 2015, 22, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Mittal, S.; Srinivasan, A. Robotics in Pediatric Urology: Evolution and the Future. Urol Clin North Am 2021, 48, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, V.; Reimold, P.; Goertz, M.; Hofer, L.; Dieffenbacher, S.; Nyarangi-Dix, J.; Duensing, S.; Hohenfellner, M.; Hatiboglu, G. Evolution of Salvage Radical Prostatectomy from Open to Robotic and Further to Retzius Sparing Surgery. J Clin Med 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Walz, J.; Burnett, A.L.; Costello, A.J.; Eastham, J.A.; Graefen, M.; Guillonneau, B.; Menon, M.; Montorsi, F.; Myers, R.P.; Rocco, B.; et al. A critical analysis of the current knowledge of surgical anatomy related to optimization of cancer control and preservation of continence and erection in candidates for radical prostatectomy. Eur Urol 2010, 57, 179–192. [Google Scholar] [CrossRef]
- Iwahashi, Y.; Deguchi, R.; Muraoka, S.; Wakamiya, T.; Yamashita, S.; Kikkawa, K.; Kohjimoto, Y.; Hara, I. Impact of postoperative sexual function on health-related quality of life after robot-assisted radical prostatectomy. Curr Urol 2024, 18, 148–154. [Google Scholar] [CrossRef]
- Shin, Y.S.; Pak, S.W.; Hwang, W.; Jo, S.B.; Kim, J.W.; Oh, M.M.; Park, H.S.; Moon, D.G.; Ahn, S.T. Urethral Sparing versus Trans-Vesical Robot-Assisted Simple Prostatectomy: A Comparative Analysis of Perioperative, Postoperative Outcomes, and Ejaculation Preservation. World J Mens Health 2024. [Google Scholar] [CrossRef]
- Schlegel, P.N.; Walsh, P.C. Neuroanatomical approach to radical cystoprostatectomy with preservation of sexual function. J Urol 1987, 138, 1402–1406. [Google Scholar] [CrossRef]
- Ma, J.; Xu, W.; Chen, R.; Zhu, Y.; Wang, Y.; Cao, W.; Ju, G.; Ren, J.; Ye, X.; He, Q.; et al. Robotic-assisted versus laparoscopic radical prostatectomy for prostate cancer: the first separate systematic review and meta-analysis of randomised controlled trials and non-randomised studies. Int J Surg 2023, 109, 1350–1359. [Google Scholar] [CrossRef]
- Robinson, P.N.; Surendran, K.; Lim, S.J.; Robinson, M. The carbon footprint of surgical operations: a systematic review update. Ann R Coll Surg Engl 2023, 105, 692–708. [Google Scholar] [CrossRef]
- Fuschi, A.; Pastore, A.L.; Al Salhi, Y.; Martoccia, A.; De Nunzio, C.; Tema, G.; Rera, O.A.; Carbone, F.; Asimakopoulos, A.D.; Sequi, M.B.; et al. The impact of radical prostatectomy on global climate: a prospective multicentre study comparing laparoscopic versus robotic surgery. Prostate Cancer Prostatic Dis 2024, 27, 272–278. [Google Scholar] [CrossRef]
- Rizan, C.; Bhutta, M.F. Environmental impact and life cycle financial cost of hybrid (reusable/single-use) instruments versus single-use equivalents in laparoscopic cholecystectomy. Surg Endosc 2022, 36, 4067–4078. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Number of patients receiving services using robotic technologies (own elaboration based on the National Health Fund (NFZ) databases).
Figure 1.
Number of patients receiving services using robotic technologies (own elaboration based on the National Health Fund (NFZ) databases).
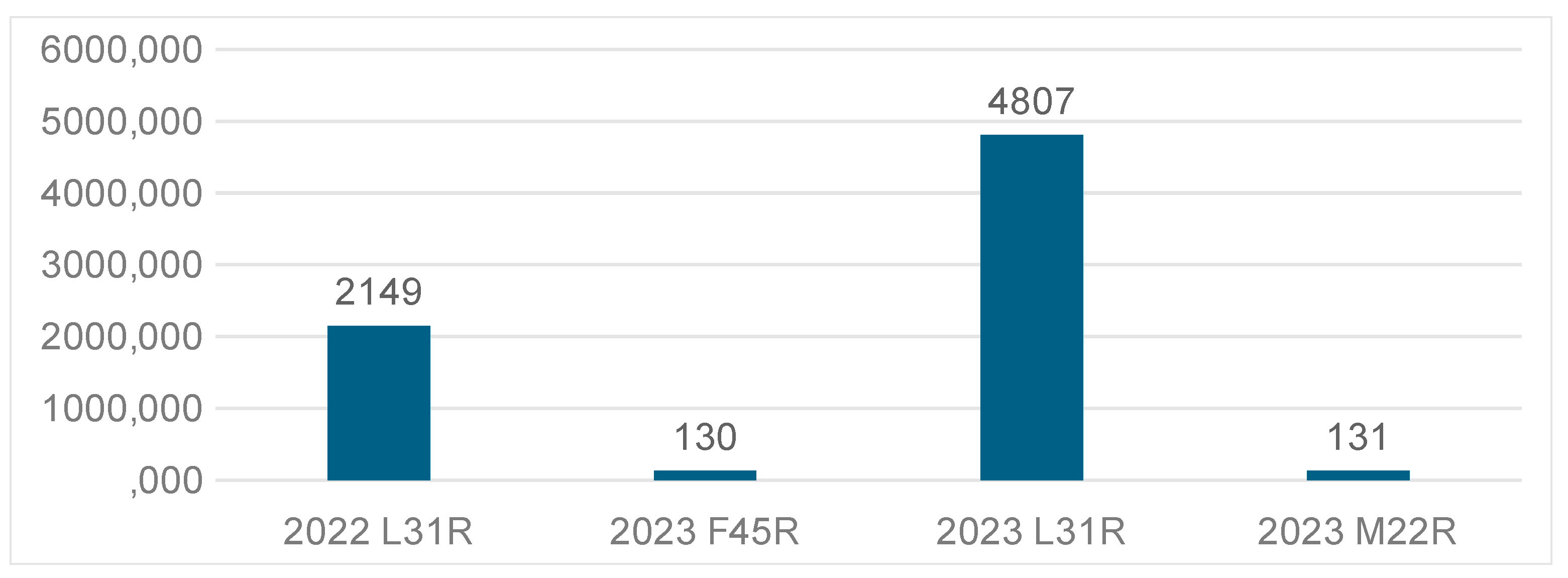
Figure 2.
Public payer (NFZ) expenses related to financing healthcare services provided using robotic systems (own elaboration based on the National Health Fund (NFZ) databases).
Figure 2.
Public payer (NFZ) expenses related to financing healthcare services provided using robotic systems (own elaboration based on the National Health Fund (NFZ) databases).
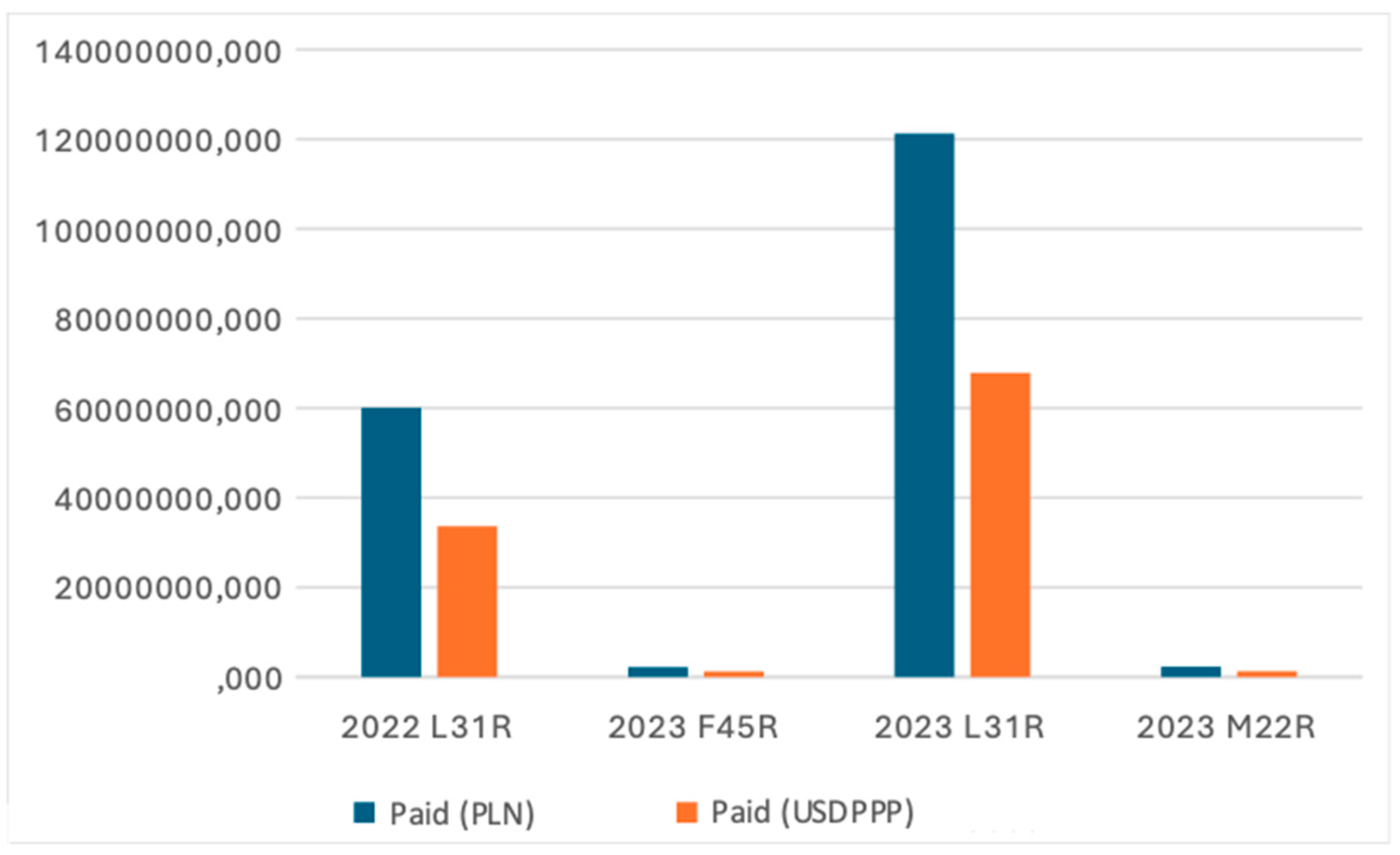
Figure 3.
Patient population age group distribution (own elaboration based on the National Health Fund (NFZ) databases).
Figure 3.
Patient population age group distribution (own elaboration based on the National Health Fund (NFZ) databases).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



