Submitted:
02 October 2024
Posted:
04 October 2024
You are already at the latest version
Abstract
Medical ozone is a redox regulator with beneficial effects in oxidative etiology diseases such as rheumatoid arthritis (RA). The aim of this study was to conduct a holistic review from different pharmacological trials involving ozone in model diseases as well as the clinical response of RA patients. The ROS involved in RA and its relationship to the main pathological pathways of this autoimmune disease were here considered. The integrator analysis of experimental results from animals with clinical findings have revealed that both methotrexate (MTX) and medical ozone share common mechanisms via adenosinergic regulation. This finding has enabled us to propose a new pharmacological mechanism in the treatment of RA. We concluded that MTX + medical ozone combined therapy reduces ROS overproduction and the generation of proinflammatory cytokines, and decreases anti-cyclic citrullinate peptide levels by a mutual mechanism involving adenosine A1 receptors.
Keywords:
Ozone
; Reactive Oxygen Species
; Rheumatoid Arthritis
; Methotrexate
; A1 Adenosine Receptors
1. Introduction
The loss of cellular redox balance leads to oxidative stress (OS) as a result of an excessive production of Reactive Oxygen Species (ROS) that exceed antioxidant defenses [1] and cause cellular damage with loss of vital functions.
It is important to note that OS does not always promote damage. Some ROS participate in signaling mechanisms and regulate processes essential for life. A good example is nitric oxide, a free radical and vasodilator, released by endothelial cells; its deficit is associated with cardiovascular and other diseases. OS is involved in a variety of autoimmune diseases of oxidative etiology [2,3], particularly rheumatoid arthritis (RA). RA is a chronic systemic autoimmune disease causing progressive disability and premature death [4]. It is a symmetric peripheral disease involving bone erosion, proximal involvement and destructive bone lesions. In addition to this, RA patients display synovitis, morning stiffness and/or immobility of their proximal interphalangeal joints [5]. Finally, such patients suffer joint failure due to cartilage damage and severely weakened tendons and ligaments [6].
In the development of RA, a proinflammatory and hypoxic scenario is generated in the synovial tissue, which leads to an overproduction of Reactive Oxygen Species (ROS) with DNA damage and mitochondrial dysfunction. The synovium is the principal target as it is associated with the degree of RA activity. This compartment is severely infiltrated by immune system cells leading to neovascularization [7]. The joints of patients affected by RA show inflammation, edematous synovial tissue with hyperemia and other alterations [8].
One important source of ROS in RA is the mitochondria. In particular, the superoxide anion radical is generated in the mitochondrial electron transport chain with the participation of complexes I, II and III [9]. This ROS is a precursor of other ROS, such as hydrogen peroxide, which triggers a cascade of reactions giving rise to different molecules involved in RA. The accumulation of ROS in the mitochondria leads to the modification of functions such as the activation of the mitochondrial permeability transition pore. An extension of the opening time of these pores can induce an explosive increase of ROS that damage the mitochondria itself which is linked to different pathological conditions expressed in the form of comorbidities of RA [10,11]. On the other hand, the joints of patients with RA are in a state of hypoxia, which is linked, as an additional factor, to the production of ROS [12]. ROS levels have been correlated with the degree of RA activity, C-reactive protein and antibodies against cyclic citrullinated peptides in the blood of patients with RA, with ROS being reported as an indirect indicator of the degree of synovial inflammation in these patients [13,14].
Neutrophils represent 60% of total leukocytes. These cells are part of the innate immunity, constituting the first lines of defense against infections and orchestrating adaptive immune responses. It has been suggested that neutrophil extracellular traps (NETs), activation of peptidyl arginine deiminase (PAD), and generation of citrullinated peptides are at the core of RA pathogenesis. Activated neutrophils accumulate in synovial fluid and tissue. Moreover, fibroblasts such as synoviocytes internalize NET-associated citrullinated peptides, recruit antigen-presenting cells that present this peptide-NET complex to CD4+ T cells to produce an autoimmune response [16].
Neutrophil levels in RA patients are significantly higher than in subjects with other arthritic diseases. Their concentrations were positively correlated with inflammation and disease severity. ROS are released by neutrophil degranulation, including superoxide anion radical, increased mitochondrial and extracellular oxidative stress with a decrease in antioxidant defense mechanisms in RA [17,18].
Macrophages, together with neutrophils, belong to the set of cells that constitute innate immunity. Macrophages release high levels of ROS produced by different sources and sites of formation. The first identified source of superoxide anion radical generation by macrophages was NADPH Oxidase located in the plasma membrane, which produces the superoxide radical by transfer of an electron from NADPH to oxygen. It is worth noting that, in the macrophage, we find other sites of ROS production – of mitochondrial origin – such as the formation of hydrogen peroxide by monoamine oxidase (MAO) in the outer membrane of the mitochondria; a superoxide anion radical, hydrogen peroxide and hydroxyl radical in the mitochondrial matrix, through the electron transport chain. In addition to this we also find hydrogen peroxide with a participation of cytochrome C in the inner membrane of the mitochondria, plus superoxide anion radical and hydrogen peroxide in the cytosol due to the metabolism of xanthine via xanthine oxidase [19]. From the above, it is evident that the superoxide anion radical is released by macrophages from different sites and by different enzymes and can play a central role in the triggering of RA.
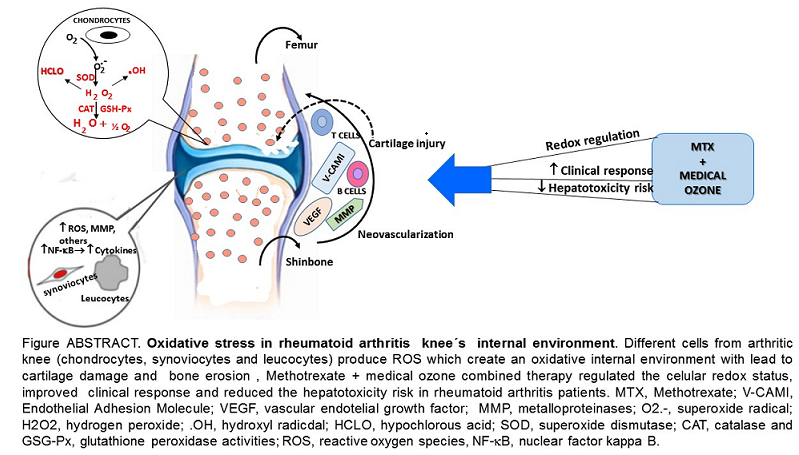
Figure 1 shows the main ROS involved in different events associated with the development and progression of RA (superoxide radicals, hydrogen peroxide, hydroxyl radical and hypochlorous acid) [7].
The aim of this review has been to perform a holistic analysis of a selection of redox results from different studies on medical ozone in disease and clinical models. In this review, the interrelation between animal studies and clinical response in patients with RA is discussed. An integrative analysis has led to the proposal of a new mechanism of action. We conclude that the improvement observed in the clinical response of patients with RA treated with the combined therapy methotrexate + medical ozone, compared to monotherapy, is the result of a common mechanism of action, shared by methotrexate and medical ozone, with the participation of adenosinergic transmission.
2. Medical Ozone, a Regulator of Redox Targets with an Impact on RA
2.1. Studies in Animal Models
Medical ozone is made up of an ozone/oxygen mixture (O3/O2) obtained by electrosynthesis by passing a current of pure O2 through a silent electrical discharge generated by specific equipment designed for such purposes, obtaining an ozone concentration between 0.05 and 5 volume percent [20].
Studies carried out in different disease models using experimental animals, have shown that medical ozone “per se” is capable of regulating the cellular redox state by acting on different processes involved in RA: this is referred to in Figure 1.
In acute (carrageenan-induced synovitis) and chronic models through administration of a fraction of the streptococcal wall, glycan/polysaccharide peptide (PG/PS), the beneficial effects of medical ozone were demonstrated by the reduction of inflammation and pain in the acute model (Figure 2). Likewise, in the chronic model, the levels of mRNA transcripts for TNF-α and Il-1β were reduced in the group treated with ozone when compared to those in the control group, which had been treated with the inducer PG/PS and the PG/PG + oxygen group (ozone vehicle) [21].
It is evident how medical ozone, administered by rectal insufflation, prevented carrageenan-mediated inflammation (0.73 ± 0.04 vs. 3 ± 0.5 mm, respectively) without differing significantly from the control (saline) (0.2 ± 0.08). The participation of adenosine A1 receptors in the anti-inflammatory actions of ozone was demonstrated when DPCPX (8-cyclopentyl-1,3-dipropylxanthine), a specific antagonist of these receptors, blocked the protective effects of medical ozone by reestablishing the inflammatory process (3 ± 0.5 vs 2.8 ± 0.9 mm).
The participation of adenosine has an important significance in the therapeutic actions of methotrexate (MTX) in the treatment of patients with RA. Adenosine is considered to be one of the probable mechanisms of action of MTX, due to its capacity to inhibit the release of proinflammatory cytokines [23]. The beneficial effects of ozone, mediated by A1 adenosine receptors, have been demonstrated in different disease models: one example is the ischemia/reperfusion injury of the liver [24]. In this model, medical ozone was shown to promote adenosine accumulation by regulating the activity of adenosine deaminase, the enzyme responsible for its degradation to inosine [25],
In another experiment ozone reduced the time up to the first seizure in a pentylenetetrazol-induced seizures [26], as well as in carrageenan-induced synovitis [22].
The expression of A1 receptors is redox-dependent. In one report, ROS induced an increase in the expression of adenosine A1 receptors; this was supported by the finding that incubation of cells with H2O2 and catalase, a hydrogen peroxide scavenger, attenuated the expression of adenosine A1 receptors [27].
Figure 3 shows the mRNA levels for the proinflammatory cytokines TNF-α and IL-1β, which, together with IL-6, are characteristic of the cytokine storm in RA [21].
Preconditioning with medical ozone significantly reduced the concentrations of both cytokines that are generated as a result of an activation of the nuclear transcription factor NF-kB.
Figure 4 shows the results of immunohistochemistry of the p65 subunit of NF-κB in ischemia/reperfusion (I/R) of the liver.
The p65 subunit of NF-κB is the one that recognizes response elements in DNA and promotes the transcription of proinflammatory cytokines (Figure 1). In Figure 4 intense p65 immunoreactivity was observed in the I/R group, while the ozone-treated animals showed only scattered zones of reaction. The results suggest that ozone regulates the expression of this factor – among other mechanisms, by its actions on the control of hydrogen peroxide generation (Figure 1), one of the activators of this factor.
It can be seen how, in the acute synovitis model, ozone restored the concentrations of hydroperoxides to control levels as well as MDA, the terminal product of lipid peroxidation, which is generated by the formation of hydroxyl radicals through the peroxidation of membrane lipids (Figure 1). MDA has been recognized as a biogenic aldehyde forming adducts with proteins and contributing to the loss of immune tolerance, among other effects [28,29].
In the chronic model, an increase in SOD was observed, capturing superoxide radicals and generating hydrogen peroxide. This is reduced to water and oxygen by an increase in catalase activity, which increased in all treatment groups.
Legend: TH, total hydroperoxides; MDA (malondialdehyde); O3 (ozone); O2 (oxygen) (*) (relative content/mg protein x 10; SOD (superoxide dismutase) activity; CAT (catalase) activity; PG/PS (peptidoglyan/polysaccharide). The mean ± SD is here given. Different letters indicate significant differences (p <0.05) [21, 22].
Hypochlorous acid (HCLO) is another ROS involved in RA (Figure 1). It originates from hydrogen peroxide in the presence of a halogen (mainly chlorine). The enzyme Mieloperoxidase (MPO), abundant in neutrophils and macrophages, catalyzes the reaction. Figure 5 shows the effects of medical ozone on MPO activity in an ischemia/reperfusion model.
The results show that ozone regulated the activity of the enzyme that catalyzes the formation of HCLO, which was significantly lower in the group treated with ozone compared to the group subjected to I/R and O2 + I/R damage. Of note are the results in the group that received oxygen (ozone vehicle) where the damage was greater than that of I/R. The results obtained, at an experimental level, demonstrate that medical ozone is able to act on the different ROS involved in RA and that medical ozone per se exerts beneficial effects in the experimental models of arthritis studied.
2.2. Studies in Patients with Rheumatoid Arthritis
The treatment options available for RA, where methotrexate (MTX) remains the gold standard for this disease plus the so-called biologicals that can reduce pain and stiffness, exhibit a limited effectiveness accompanied by multiple adverse effects such as nausea, hepatotoxicity, hemato/metabolic disorders and interstitial lung diseases. Biological agents (e.g. anti-TNF-α antibodies) are effective, but have adverse effects such as infections in the infusion process and at the injection site, as well as differences in efficacy. With the advent of these new therapies, the treatment of patients with RA has improved. However, due to the heterogeneity and complexity of the pathological mechanisms in RA, some patients still have a poor clinical response, which means that the development of new therapies is still a priority [30].
Through an oxidative pre/postconditioning mechanism validated in different disease models and in clinical studies [31], medical ozone has demonstrated its efficacy in diseases of oxidative etiology. Since RA is an autoimmune disease associated with severe and chronic oxidative stress, it is expected that medical ozone will have beneficial effects in the treatment of RA.
The results in patients with RA treated using the combined therapy MTX + medical ozone were in line with experimental studies. A decrease in swollen and painful joints was observed, as well as an improvement in the performance of daily activities; this included a reduction in the levels of antibodies against cyclic citrullinated peptides and an increase in antioxidant defenses accompanied by a decrease in redox markers which indicate damage.
Table 2 shows the results obtained after 21 days of treatment for patients treated with MTX and for those who received MTX + medical ozone [32].
No significant differences (p >0.05) between either group were observed for the variables DAS28 and HAQ-DI at the beginning of the study. The DAS28 decreased significantly (p <0.05) in the MTX + Ozone group, whereas there were no changes in the MTX group. At the end of the clinical study, differences (p <0.05) were observed between both groups. HAQ-DI showed results similar to DAS28. and MTX + medical ozone improved the patients' disabilities, whereas the MTX group ended without changes. Again, significant differences (p<0.05) were found between both groups at the end of the study showing beneficial results for the group of patients receiving the combined therapy. Both acute phase reactants (CRP and ESR) decreased (p <0.05) in the MTX + medical ozone group, whereas the MTX group showed no significant changes (p >0.05) at the end of the study.
The MTX + medical ozone group reduced (p<0.05) autoantibodies against cyclic citrullinated peptides, which were not modified (p > 0.05) in the group not treated with ozone. Similarly, autoantibody levels in the MTX + ozone group were lower than in the MTX group at the end of the study. These results indicate that medical ozone can achieve a reduction in the autoimmune response and are in line with clinical markers (DAS28, HAQ-DI and acute phase reactants).
2.2.1. Levels of Redox Biomarkers in the Groups at the End of the Study
Plasma biomarkers of protection (Antioxidant Defenses) and damage (Injury Biomarkers) were studied in both groups of patients (Figure 6). MTX + ozone increased the capacity of the endogenous antioxidant system to counteract oxidative damage, resulting in a significant decrease (p<0.05) in damage to biomolecules (lipids, MDA and proteins, AOPP), as well as in TH levels and nitric oxide concentrations. By contrast, patients who did not receive ozone showed a reduction in their antioxidant defenses and a higher level of damage (Figure 6A and Figure 6B). To find out whether there was any relationship between redox markers and clinical variables, the correlations between these variables were evaluated where only correlations could be found after treatment with MTX + medical ozone; this suggests a stabilization of the antioxidant/prooxidant balance in the patients. GSH was the only protective redox marker that correlated (p<0.05) with all clinical variables (GSH vs CRP = 0.68, VCG = 0.63, DAS28 = 0.57 and HAQ-DI = 0.72) whereas SOD correlated with acute phase reactants and the Disability Index suggesting its participation in the inflammatory process (SOD vs CRP = 0.5, VCG = 0.51 and HAQ-DI = 0.61).
In addition to the clinical efficacy observed for the combined therapy MTX + medical ozone, the hepatoprotective effects of ozone are added in a model for hepatotoxicity induced by carbon tetrachloride, increasing antioxidant defenses (SOD, CAT, GSH), reducing injury markers (lipid peroxidation), thus preserving the concentrations of calcium-dependent ATPase, glucose-6-phosphate dehydrogenase, hepatic glycogen and phospholipase A.
Likewise, the levels of transaminases and cholinesterase were reestablished with less general liver damage and a decrease in the area damaged by lipidosis [33,34].
The clinical study in patients with RA showed that treatment with the combined therapy MTX + ozone reduced the risk of hepatotoxicity 4 times compared to monotherapy [35].
3. Discussion
The results of the experimental models developed showed that medical ozone “per se” exhibited beneficial effects in diseases involving cartilage and bone remodeling.
Synovitis is a critical pathological event preceding the clinical onset of RA [36]. The anti-inflammatory effects of ozone were mediated by the activity of adenosine A1 receptors, a reduction in oxidative damage to proteins (AOPP and Fructosylamine) and lipid peroxidation (MDA). A decrease in the inflammatory process is probably the most important goal in the therapy of synovitis. mRNA and proteins for A1, A2a, A2b and A3 adenosine receptors are expressed in human synoviocytes. The results show that the adenosine A1 receptor is involved in the anti-inflammatory effects of medical ozone in carrageenan-induced synovitis in Wistar rats (Figure 2). These results agree with the disappearance of the anti-inflammatory effects and the protection provided by ozone against oxidative damage when the specific antagonist of adenosine A1 receptors (DPCPX) was tested – as demonstrated by ankle inflammation, damage to proteins and lipids, as well as a notable reduction in plasma antioxidant capacity (FRAP) [22].
Previous results had shown that adenosine receptor A1 was associated with the protective effects of ozone. In damage by ischemia / reperfusion of the liver, activation of A1 receptors with CCPA (2-chloro-N6-cyclopentyladenosin), a specific agonist of the A1 receptors, corresponded to the reduction of transaminases, whereas blocking these receptors by DPCPX increased liver damage [24]. In another study, ozone increased the latency of the first convulsive crisis and restored cell redox balance in pentylenetetrazol seizures (PTZ) in mice. DPCPX completely abolished the protection provided by ozone, evidenced the role of adenosine receptors A1 against brain damage [26]. The anti-inflammatory effects of ozone, mediated by adenosine A1 receptors, can be the consequence of a transferable oxidative stress induced by ozone. This stress, when it was induced by certain specific antineoplastic agents and H2O2, regulated the expression of A1 adenosine receptors in the smooth muscle cells of hamsters. [37]. By promoting a generation of ROS, light and transient, ozone regulates cell redox balance and can represent a stimulus for the expression of A1 adenosine receptors. Advance Oxidation Protein Products are markers of oxidative damage to proteins and the increase in their levels in patients with AR have been observed. In addition, synoviocytes such as fibroblasts (FLSS) are related to oxidative stress. An exposure of FLSS to AOPP regulated the mRNAs and the expression of proinflammatory cytokines, metalloproteinases of the matrix and the growth factor of the vascular endothelium in a manner dependent on the concentration. The degradation of IκB and the nuclear translocation of NF-κB-P65, induced by AOPP were blocked significantly by antioxidant activity, such as superoxide dismutase, N-acetyl-L-cysteine and NADPH oxidase inhibitors. [38]. Medical ozone was able to maintain the concentrations of AOPP at the control group.
Lipid peroxidation leading to the formation of protein adducts promotes proinflammatory responses characterizing a variety of chronic conditions [39]. Malondialdehyde (MDA) is one of those ubiquitous products involved in disease pathogenesis, and its levels are increased in synovial fluid. MDA was significantly reduced by ozone treatment, with respect to all experimental groups studied, suggesting the decrease of hydroxyl radicals available to initiate and trigger peroxidative damage of cell membranes, and also suggesting a decrease in RA-associated events mediated by this aldehyde (Figure 1).
Medical ozone exerted beneficial effects on local inflammation, induced by carrageenan, and these results were corroborated in the systemic and chronic model of arthritis.
TNF-α is a proinflammatory cytokine, activating the NF-κB pathway, leading to a cascade of other proinflammatory cytokines [40]. Furthermore, it is known to increase the production of mitochondrial reactive oxygen species. Current biological therapies, including anti-TNF-α inhibitors, result in disease improvement and prevent joint erosion, in spite of the fact that clinical studies on the efficacy of TNF-α blocking agents clearly show that about 40% of patients receiving this therapy are non-responders [41]. When TNF-α and IL-1β mRNA levels were determined in spleen homogenates, it was observed that ozone treatment decreased (p<0.05) the concentration of these transcripts compared to the PG/PS and PG/PS + oxygen groups (Figure 3). Both cytokines are generated when NF-κB is activated, but at the same time, TNF-α is an activator of NF-κB which gives rise to a vicious circle perpetuating the chronic inflammatory process. For this reason, such results indicate that medical ozone treatment contributes to a decrease in the pathological cascade of NF-κB. The protective effects of ozone may be a consequence of its ability to regulate the activity of the p65 subunit of NF-κB, which was demonstrated by ischemic/reperfusion damage to the liver (Figure 4). The efficacy of ozone in RA can not only be explained by its acting on the generation of proinflammatory cytokines alone, since the disruption of the cellular redox balance is closely related to cartilage damage, bone remodeling and the autoimmune response itself. Ozone therapy was able to regulate cellular redox balance (Figure 5). It is known that ROS can function as a second messenger to activate NF-κB, which orchestrates the expression of a spectrum of genes involved in the inflammatory response. Overproduction of NO contributes to the pathogenesis of chronic arthritis. In humans, circulating levels of nitrate/nitrite are present in arthritic patients and synovial tissues of RA patients express and produce abnormally high amounts of NO [42].
Simultaneously with NO, other redox markers were also studied (Table 1). PG/PS and PG/PS + oxygen exhibited a low SOD activity whereas PG/PS + Ozone and control (-) showed no significant differences. An increase in NO and a decrease in SOD represent, pathologically, an "explosive mixture." The accumulation of superoxide radicals in the presence of overproduced NO leads to the formation of peroxynitrite, a known cytotoxin. Modest increases in superoxide and NO (10-fold in each case) will increase peroxynitrite formation 100-fold. Under proinflammatory conditions, such as in RA, a simultaneous production of superoxide and NO (1000-fold) will increase peroxynitrite formation 1,000,000-fold [43]. Increased SOD promotes the formation of hydrogen peroxide which may produce additional damage to biomolecules. However, hydrogen peroxide is reduced if catalase activity is increased. PG/PS + Ozone showed an increase compared to all other experimental groups (Control, PG/PS and PG/PS + Oxygen) (Table 1). Although the control (-) value needed no increased in CAT, the PG/PS and PG/PS + oxygen values did indicate a severe oxidative stress and a low catalase activity: these, by consequence, are by themselves a sure sign of damage.
Medical ozone increased the therapeutic efficacy of MTX in patients with RA. An improvement in the clinical status (reduction in pain, DAS28, HAQ-DI and acute phase reactants) was observed, as well as a reduction in autoantibodies (anti-CCP) and oxidative stress [32].
It should be noted that MTX halted the progression of the disease: this represents an important therapeutic response. However, there were no significant differences in the group of patients receiving MTX only, when comparing the beginning and the end of the study. By contrast, patients treated with the MTX + ozone combined therapy significantly improved (p<0.05) in the context of both clinical variables and cellular redox status, suggesting that – in the context of monotherapy (MTX) – the combination MTX + ozone enhances clinical response and exerts an additive or synergistic effect on the response of patients with RA as included in this study. These effects suggest that they are the result of the contribution made by each of the components of the combined therapy (MTX and ozone) in the control of the disease, given that both agents share common therapeutic targets, such as redox balance and actions associated with adenosine. The integration of the results obtained in the different studies carried out with medical ozone in RA (experimental and clinical) allow us to propose a new mechanism of action explaining both the results obtained in disease models and the clinical response of patients (Figure 7).
The proposed mechanism is based on adenosinergic participation, common to MTX and medical ozone, as essential mechanisms in the treatment of RA capable of regulating the redox state, the production of proinflammatory cytokines and arthritogenic lymphocytes.
4. Conclusion
In an integrative analysis of the results of the present study, the mechanism of action proposed by the authors is found to be the principal aspect found on administration of the combined therapy as described by the authors. Both (MTX and ozone) share common molecular events, which explains the significant improvement in the clinical response where patients were treated with MTX + ozone. These results are expressed by the different studies carried out at a preclinical level, such as (a) the participation of the A1 adenosine receptors in the anti-inflammatory and analgesic effects of medical ozone, (b) the reduction in the expression of proinflammatory cytokines, and (c) a regulation of the cellular redox state. These benefits of combined therapy are expanded when a reduction in the risk of hepatotoxicity of MTX + ozone is additionally demonstrated in patients with RA in comparison with monotherapy.
5. Future Directions
Medical ozone is capable not only of stopping the progression of RA but also improving clinical and redox indicators in these patients. The pleiotropy of medical ozone increases its therapeutic efficacy in diseases of oxidative etiology, which means that its efficacy/effectiveness can be hypothesized in patients with RA detected at an early stage (< 1 year). Hence, even if they are carriers of this autoimmune disease, they remain asymptomatic, with a good quality of life and without the adverse reactions of the drugs otherwise used to control this immune dysfunction. Further research in this field is currently being developed by our own research group.
Author Contributions
Conceptualization, O.S.L.F., G.T.O., R.V.-H., G.L.C. and I.S.E.; Methodology, O.S.L.F. and G.T.O.; Software, G.T.O.; Validation, M.E.C.V.; Investigation, O.S.L.F., G.T.O., G.L.C., I.S.E. and M.E.C.V.; Resources, R.V.-H., G.L.C. and I.S.E.; Data curation, G.T.O. and R.V.-H.; Writing—original draft, O.S.L.F.; Writing—review & editing, O.S.L.F., G.T.O., R.V.-H., G.L.C., I.S.E. and M.E.C.V.; Supervision, G.L.C. and M.E.C.V.; Project administration, I.S.E. and M.E.C.V.; Funding acquisition, O.S.L.F. and R.V.-H. All authors have read and agreed to the published version of the manuscript.
Funding
Research here conducted has received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data used are cited in this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- López-Armada, M.J.; Fernández-Rodríguez, J.A.; Blanco, F.J. . Mitochondrial Dysfunction and Oxidative Stress in Rheumatoid Arthritis. Antioxidants 2022, 11, 1151. [Google Scholar] [CrossRef] [PubMed]
- Souliotis, V.L.; Vlachogiannis, N.I.; Argyriou, A.; Ntouros, P.A.; Sfikakis, P.P. . DNA Damage Response and Oxidative Stress in Systemic Autoimmunity. Int. J. Mol. Sci. 2020, 21, 55. [Google Scholar] [CrossRef] [PubMed]
- Wójcik, P.; Gęgotek, A.; Žarković, N.; Skrzydlewska, E. Oxidative Stress and Lipid Mediators Modulate Immune Cell Functions in Autoimmune Diseases. Int. J. Mol. Sci. 2021, 22, 723. [Google Scholar] [CrossRef] [PubMed]
- Guo, Q.; Wang, Y.; Xu, D.; Nossent, J.; Pavlos, N.J.; Xu, J. Rheumatoid arthritis: Pathological mechanisms and modern pharmacologic therapies. Bone Res. 2018, 6, 15. [Google Scholar] [CrossRef]
- Saalfeld, W.; Mixon, A.M.; Zelie, J.; Lydon, E.J. Differentiating Psoriatic Arthritis from Osteoarthritis and Rheumatoid Arthritis: A Narrative Review and Guide for Advanced Practice Providers. Rheumatol. Ther. 2021, 8, 1493–1517. [Google Scholar] [CrossRef] [PubMed]
- Bullock, J.; Rizvi, S.A.; Saleh, A.M.; Ahmed, S.S.; Do, D.P.; Ansari, R.A.; Ahmed, J. Rheumatoid arthritis: A brief overview of the treatment. Med. Princ. Pract. 2018, 27, 501–507. [Google Scholar] [CrossRef]
- Wang, X.; Fan, D.; Cao, X.; Ye, Q.; Wang, Q.; Zhang, M.; Xiao, C. The Role of Reactive Oxygen Species in the Rheumatoid Arthritis-Associated Synovial Microenvironment. Antioxidants 2022, 11, 1153. [Google Scholar] [CrossRef] [PubMed]
- Buckley, C.D.; Ospelt, C.; Gay, S.; Midwood, K.S. Location, location, location: How the tissue microenvironment affects inflammation in RA. Nat. Rev. Rheumatol 2021, 17, 195–212. [Google Scholar] [CrossRef]
- Jing, W.; Liu, C.; Su, C.; Liu, L.; Chen, P.; Li, X.; Zhang, X.; Yuan, B.; Wang, H.; Du, X. Role of reactive oxygen species and mitochondrial damage in rheumatoid arthritis and targeted drugs. Front. Immunol. 2023, 14, 1107670. [Google Scholar] [CrossRef]
- Kan, S.; Duan, M.; Liu, Y.; Wang, C.; Xie, J. Role of mitochondria in physiology of chondrocytes and diseases of osteoarthritis and rheumatoid arthritis. Cartilage 2021, 13, 1102S–1121S. [Google Scholar] [CrossRef]
- Bolduc, J.A.; Collins, J.A.; Loeser, R.F. Reactive oxygen species, aging and articularcartilage homeostasis. Free Radic Biol. Med. 2019, 132, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Zorov, D.B.; Juhaszova, M.; Sollott, S.J. Mitochondrial reactive oxygen species (ROS) and ROS-induced ROS release. Physiol. Rev. 2014, 94, 909–950. [Google Scholar] [CrossRef] [PubMed]
- Oğul, Y.; Gür, F.; Cengiz, M.; Gür, B.; Sarı, R.A.; Kızıltunç, A. Evaluation of oxidant and intracellular anti-oxidant activity in rheumatoid arthritis patients: In vivo and in silico studies. Int. Immunopharmacol. 2021, 97, 107654. [Google Scholar] [CrossRef]
- Kardeş, S.; Karagülle, M.; Durak, I.; Karagülle, M.Z. Association of oxidative stress with clinical characteristics in patients with rheumatoid arthritis. Eur. J. Clin. Investig. 2018, 48, e12858–e12858. [Google Scholar] [CrossRef] [PubMed]
- Wright, H.L.; Moots, R.J.; Edwards, S.W. The multifactorial role of neutrophils in rheumatoid arthritis. Nat. Rev. Rheumatol. 2014, 10, 593–601. [Google Scholar] [CrossRef]
- O’Neil, L.J.; Kaplan, M.J. Neutrophils in rheumatoid arthritis: Breaking immune tolerance and fueling disease. Trends Mol. Med. 2019, 25, 215–227. [Google Scholar] [CrossRef]
- Bedouhène, S.; Dang, P.M.-C.; Hurtado-Nedelec, M.; El-Benna, J. Neutrophil degranulation of azurophil and specific granules. Methods Mol. Biol. 2020, 2087, 215–222. [Google Scholar] [CrossRef]
- Kaushal, J.; Kamboj, A.; Anupam, K.; Tandon, A.; Sharma, A.; Bhatnagar, A. Interplay of redox imbalance with matrix gelatinases in neutrophils and their association with disease severity in rheumatoid arthritis patients. Clin. Immunol. 2022, 237, 108965. [Google Scholar] [CrossRef]
- Canton, M.; Sanchez-Rodrıguez, R.; Spera, I.; Venegas, F.C.; Favia, M.; Viola, A.; Castegna, A. Reactive Oxygen Species in Macrophages: Sources and Targets. Front. Immunol. 2021, 12, 734229. [Google Scholar] [CrossRef]
- Rilling, S.H. 30 years of ozone/oxygen therapy: a historical perspective. Proceedings Eleventh Ozone World Congress. Ozone in Medicine. San Francisco M-1-3,M-1-6 [1993].
- Vaillant, J.D.; Fraga, A.; Díaz, M.T.; Mallok, A.; Viebahn-Hänsler, R.; Fahmy, Z.; Barberá, A.; Delgado, L.; Menéndez, S.; Fernández, O.S.L. Ozone oxidative postconditioning ameliorates joint damageand decreases pro-inflammatory cytokine levels and oxidative stress in PG/PS-induced arthritis in rats. Eur. J. Pharmacol. 2013, 714, 318–324. [Google Scholar] [CrossRef]
- Oru, G.T.; Viebhan-Haensler, R.; Matos, Y.H.; DíazRodríguez, D.; Orta, M.C.; Fernández, O.S.L. Medical ozone prevents inflammatory effects from carrageenan-induced knee joint synovitis in rats through A1 adenosine receptor, as well as lipid and protein oxidative damages. J. Sci. Res. Stud. 2018, 5, 65–72. [Google Scholar]
- Friedman, B.; Cronstein, B. Methotrexate mechanism in treatment of rheumatoid arthritis. Jt. Bone Spine. 2019, 86, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Fernández, L.; Ajamieh, H.H.; Berlanga, J.; Menéndez, S.; Viebahn-Hansler, R.; Re, L.; Carmona, A.M. Ozone oxidative preconditioning is mediated by A1adenosine receptors in a rat model of liver ischemia/reperfusion. Transplantation 2008, 21, 39–48. [Google Scholar] [CrossRef]
- Peralta, C.; Vals, C.; Bartrons, R.; León, O.S.; Gelpí, E.; Roselló-Catafau, J. Effect of ozone treatment on Reactive Oxygen Species and Adenosine production during hepatic ischemia-reperfusion. Free. Radic. Res. 2000, 33, 595–605. [Google Scholar] [CrossRef]
- Mallok, A.; Vaillant, J.D.; Soto, M.T.D.; Viebahn-Hansler, R.; de los Angeles Béquer Viart, M.; Pérez, A.F.; Cedeño, R.I.D.; Fernández, O.S.L. Ozone protective effects against PTZ-induced generalized seizures are mediated by re-establishment of cellular redox balance and A1 adenosine receptors. Neurol. Res. 2015, 37, 204–210. [Google Scholar] [CrossRef]
- Ramkumar, V.; Hallam, D.M.; Nie, Z. Adenosine, oxidative stress and cytoprotection. Jpn. J. Pharmacol. 2001, 86, 65–74. [Google Scholar] [CrossRef]
- Thiele, G.M.; Duryee, M.J.; Hunter, C.D.; England, B.R.; Fletcher, B.S.; Daubach, E.C.; Pospisil, T.P.; Klassen, L.W.; Mikuls, T.R. Immunogenic and Inflammatory Responses to Citrullinated Proteins Are Enhanced Following Modification with Malondialdehyde-Acetaldehyde Adducts. Int. Immunopharmacol. 2020, 83, 106433. [Google Scholar] [CrossRef] [PubMed]
- Willis, M.S.; Thiele, G.M.; Tuma, D.J.; Klassen, L.W. T cell proliferative responses to malondialdehyde/acetaldehyde haptenated protein are scavenger receptor mediated. Int. Immunopharmacol. 2003, 3, 1381–1399. [Google Scholar] [CrossRef]
- Ishibash, T. Molecular Hydrogen: New Antioxidant and Antiinflammatory Therapy for Rheumatoid Arthritis and Related Diseases. Curr. Pharm. Des. 2013, 19, 6375–6381. [Google Scholar] [CrossRef]
- Fernandez, O.S.L. Ozonoterapia. El condicionamiento oxidativo fundamento de su eficacia clinica. Ed. ODREI Publisher. Alemania [2014].
- Fernandez, O.S.L.; Viebahn-Hansler, R.; Cabreja, G.L.; Espinosa, I.S.; Matos, Y.H.; Roche, L.D.; Santos, B.T.; Oru, G.T.; Vega, J.C.P. Medical ozone increases methotrexate clinical response and improves cellular redox balance in patients with rheumatoid arthritis. Eur. J. Pharmacol. 2016, 789, 313–318. [Google Scholar] [CrossRef]
- León, O.S.; Menéndez, S.; Merino, N.; Castillo, R.; Sam, S.; Pérez, L.; Cruz, E.; Bocci, V. Ozone oxidative preconditioning: a protection against cellular damage by free radicals. Mediat. Inflamm. 1998, 7, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Candelario-Jalil, E.; Mohammed-Al-Dalain, S.; Fernández, O.S.L.; Menéndez, S.; Pérez-Davison, G.; Merino, N.; Sam, S.; Ajamieh, H.H. Oxidative Preconditioning Affords Protection Against Carbon Tetrachloride-induced Glycogen Depletion and Oxidative Stress in Rats. J. Appl. Toxicol. 2001, 21, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Oru, G.T.; Viebhan-Haensler, R.; Cabreja, G.L.; Espinosa, I.S.; Santos, B.T.; Vega, J.C.P.; Cintas, S.S.; Fernández, O.S.L. . Medical Ozone Reduces the Risk of γ-Glutamyl Transferase and Alkaline Phosphatase Abnormalities and Oxidative Stress in Rheumatoid Arthritis Patients Treated with Methotrexate. SM J Arthritis Res. 2017, 1, 1004. [Google Scholar]
- Wang, X.; Fan, D.; Cao, X.; Ye, Q.; Wang, Q.; Zhang, M.; Xia, C. The role of reactive oxygen speciesism the rheumatoid arthritis-associated synovial microenvironment. Antioxidants 2022, 11, 1153. [Google Scholar] [CrossRef]
- Huang, L.; Tang, Y.; Sperlagh, B. Glial Purinergic Signaling-Mediated Oxidative Stress (GPOS) in Neuropsychiatric Disorders. Oxidative Med. Cell. Longev. 2022, 2022, 1075440. [Google Scholar] [CrossRef]
- Zheng, S.; Zhong, Z.M.; Qin, S.; Chen, G.X.; Wu, Q.; Zeng, J.H.; Ye, W.B.; Li, W.; Yuan, K.; Yao, L.; et al. Advanced oxidation protein products induce inflammatory response in fibroblast-like synoviocytes through NADPH oxidase-dependent activation of NF-κB. Cell Physiol. Biochem. 2013, 32, 972–985. [Google Scholar]
- Surapneni, K.M.; Chandrasada Gopan, V.S. Lipid peroxidation and antioxidant status in patients with rheumatoid arthritis. Indian J. Clin. Biochem. 2008, 23, 41–44. [Google Scholar] [CrossRef]
- Li, R.-L.; Duan, H.-X.; Liang, Q.; Huang, Y.-L.; Wang, L.-Y.; Zhang, Q.; Wu, C.-J.; Liu, S.-Q.; Peng, W. Targeting matrix metalloproteases: A promising strategy for herbal medicines to treat rheumatoid arthritis. Front. Immunol. 2022, 13, 1046810. [Google Scholar] [CrossRef]
- Ferreira, H.B.; Melo, T.; Paiva, A.; Domingues, M.D.R. Insights in the Role of Lipids, Oxidative Stress and Inflammation in Rheumatoid Arthritis. New Trends in Lipidomic Investigations. New Trends in Lipidomic Investigations. Antioxidants 2021, 10. [Google Scholar] [CrossRef]
- Mirdad, T.M.; Al-Ani, B.; Aseeri, F.F.; Kamar, S.S.; Mirdad, R.; AlGilban, H.M.; Haidara, M.A.; Abbas, A.M.; Dawood, A.F. Suppression of Nitrosative Stress and Inflammation of the Knee Joint Synovium in Collagen Type II-Induced Rheumatoid Arthritis by the Inhibition of Glycogen Synthase Kinase-3ß. Int. J. Morphol. 2022, 40, 84–90. [Google Scholar] [CrossRef]
- Pacher, P.; Beckman, J.S.; Tobin, Y.M.; Liandet, L. Nitric oxide and peroxinitrite in health and disease. Physiol. Rev. 2007, 87, 315–424. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Role of oxidative stress in Rheumatoid Arthritis. The main Reactive Oxygen Species (ROS) involved in inflammatory injury to tissues are (O2.-), superoxide radicals; (H2O2), hydrogen peroxide: (.OH) hydroxyl radicals and (HCLO), hypochlorous acid. There is a close cross-talk among cells and these ROS: mitochondria along with macrophages and neutrophils releasing superoxide radicals; these are metabolized to hydrogen peroxide that triggers new ROS such as HCLO which impact directly on immunogenic and arthritogenic properties, hydroxyl radicals which peroxide membranes lipids with the formation of toxic aldehydes (MDA, 4-HNE); these in turn increase ROS, a dysfunctional mitochondria, angiogenesis and other effects. Linked to the above, hydrogen peroxide activates NF-B which produce the “cytokine storm” associated to inflammation, pannus, angiogenesis with cartilage damage and bone erosion. To be noticed is that NF-B is able to activate itself through the cytokines TNF-α and IL-1β perpetuating a proinflammatory vicious circle. LPO, lipid peroxidation; MDA, malondialdehyde, 4-HNE, 4-hydroxy-2-nonenal; TNF-α, Tumor Necrosis Factor alpha; IL, interleukin; MMP, Metalloproteinase; VEGF, Vascular Endothelial Growth Factor; NF-B, Nuclear Factor kappa B.
Figure 1.
Role of oxidative stress in Rheumatoid Arthritis. The main Reactive Oxygen Species (ROS) involved in inflammatory injury to tissues are (O2.-), superoxide radicals; (H2O2), hydrogen peroxide: (.OH) hydroxyl radicals and (HCLO), hypochlorous acid. There is a close cross-talk among cells and these ROS: mitochondria along with macrophages and neutrophils releasing superoxide radicals; these are metabolized to hydrogen peroxide that triggers new ROS such as HCLO which impact directly on immunogenic and arthritogenic properties, hydroxyl radicals which peroxide membranes lipids with the formation of toxic aldehydes (MDA, 4-HNE); these in turn increase ROS, a dysfunctional mitochondria, angiogenesis and other effects. Linked to the above, hydrogen peroxide activates NF-B which produce the “cytokine storm” associated to inflammation, pannus, angiogenesis with cartilage damage and bone erosion. To be noticed is that NF-B is able to activate itself through the cytokines TNF-α and IL-1β perpetuating a proinflammatory vicious circle. LPO, lipid peroxidation; MDA, malondialdehyde, 4-HNE, 4-hydroxy-2-nonenal; TNF-α, Tumor Necrosis Factor alpha; IL, interleukin; MMP, Metalloproteinase; VEGF, Vascular Endothelial Growth Factor; NF-B, Nuclear Factor kappa B.
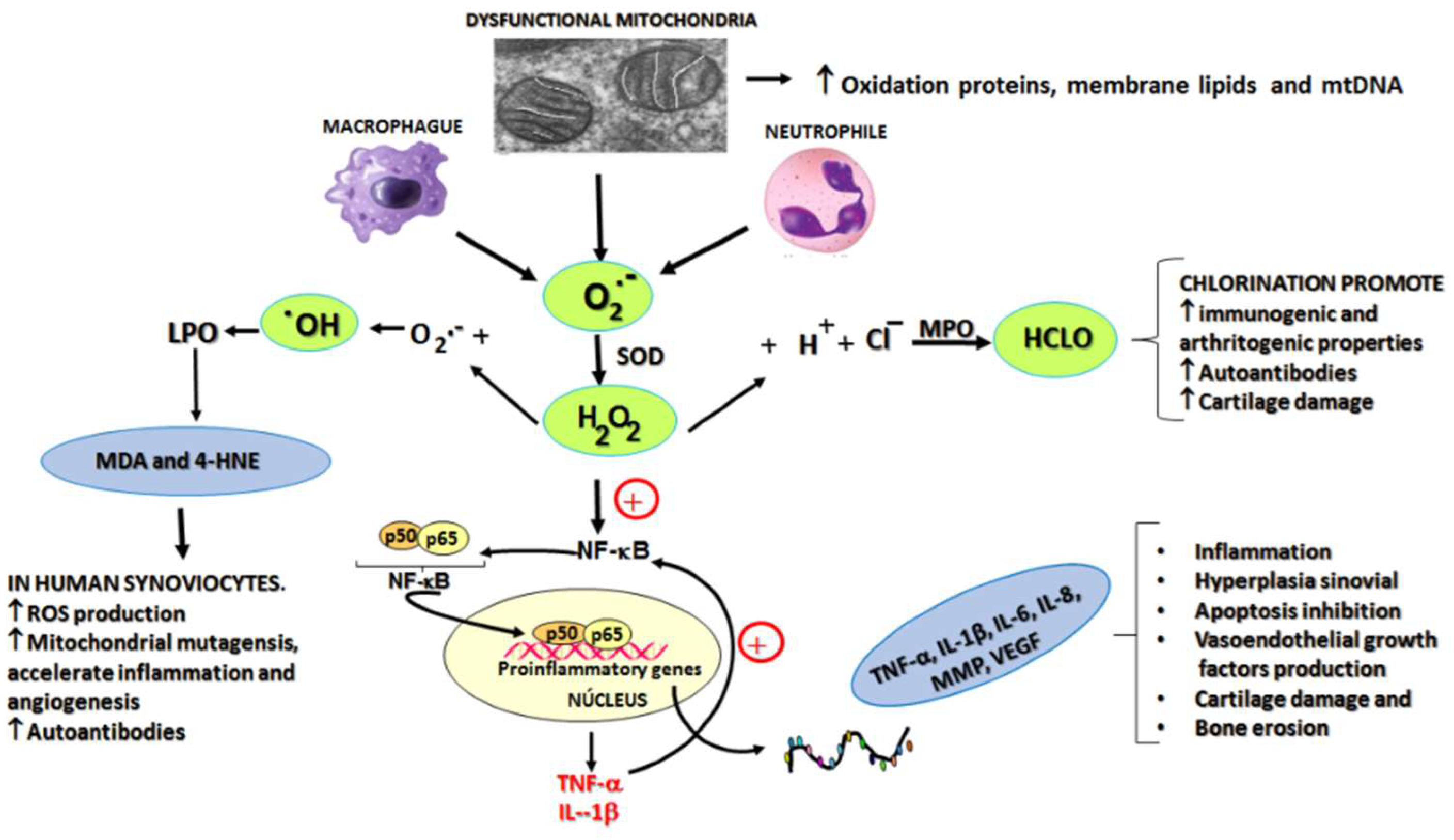
Figure 2.
The effects of medical ozone on carrageenan-induced knee inflammation in the acute model in BALB/c mice, 4 hours after carrageenan administration. Data represent the mean ± SD of each group (n=5). Different letters indicate significant differences (p 0,05) between groups [22].
Figure 2.
The effects of medical ozone on carrageenan-induced knee inflammation in the acute model in BALB/c mice, 4 hours after carrageenan administration. Data represent the mean ± SD of each group (n=5). Different letters indicate significant differences (p 0,05) between groups [22].
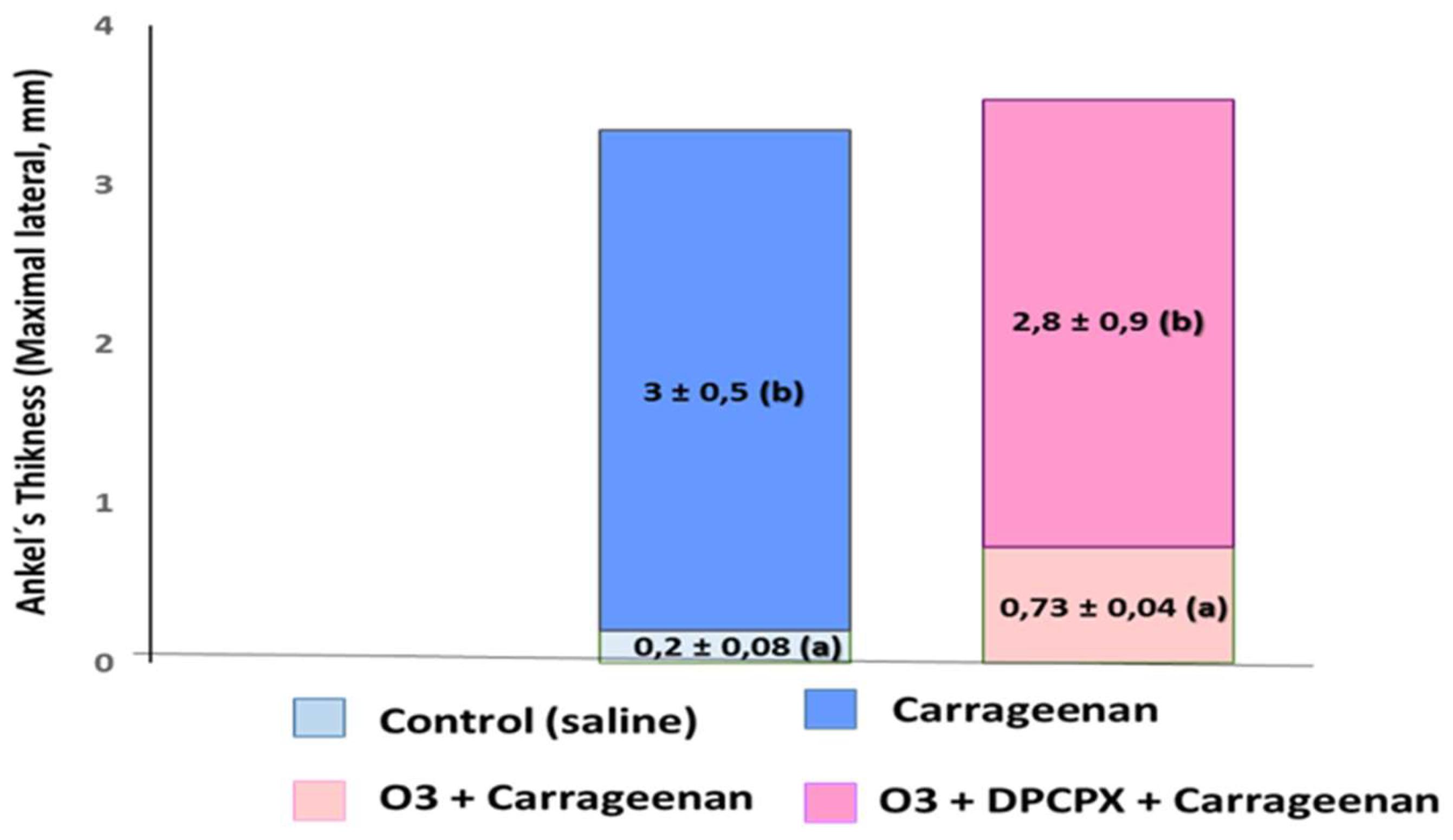
Figure 3.
TNF-α and IL-1β mRNA levels in spleen homogenates of Lewis rats in a PG/PS-induced arthritis model showing the influence of ozone/oxygen treatments. Different letters indicate significant differences (p <0.05) [21].
Figure 3.
TNF-α and IL-1β mRNA levels in spleen homogenates of Lewis rats in a PG/PS-induced arthritis model showing the influence of ozone/oxygen treatments. Different letters indicate significant differences (p <0.05) [21].
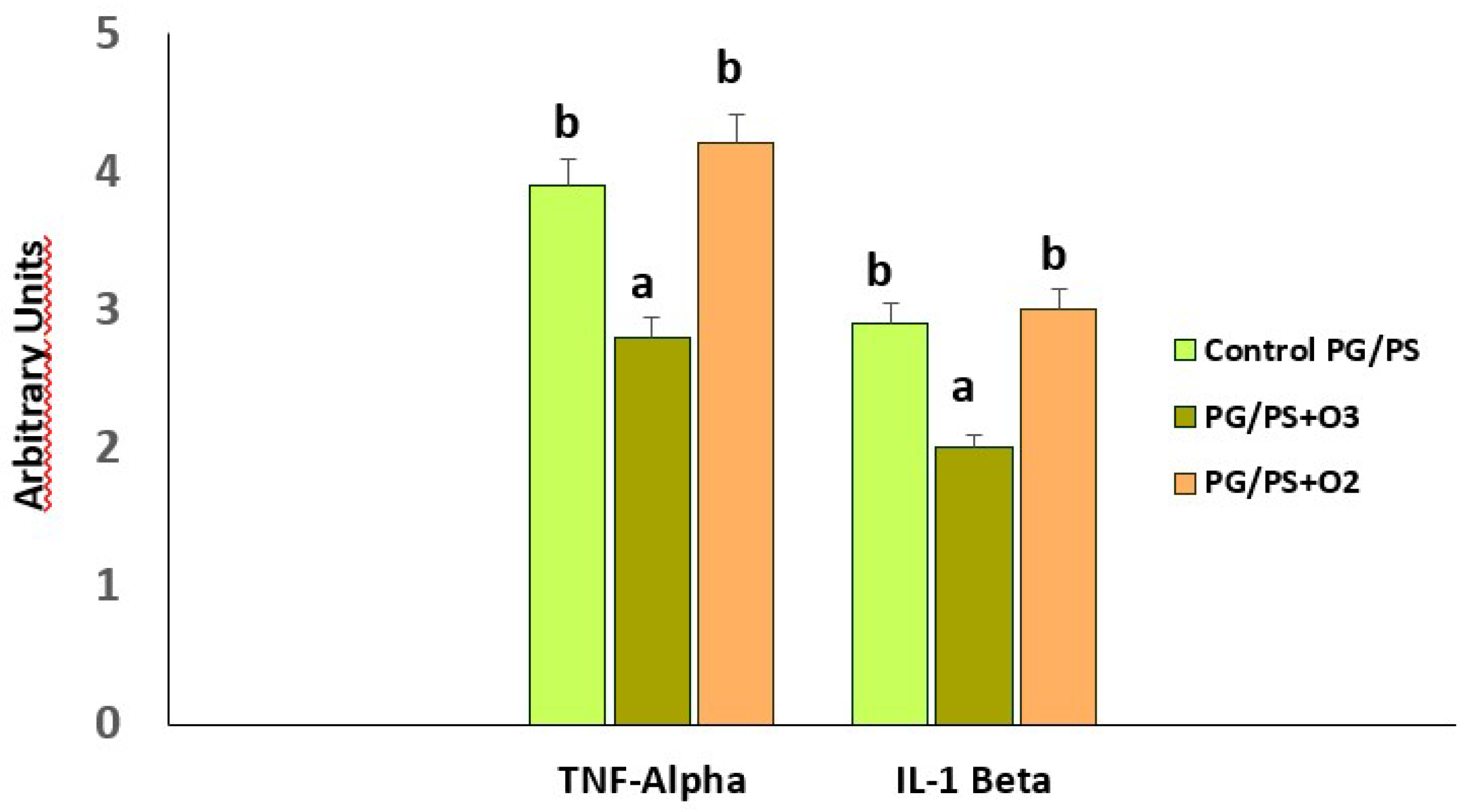
Figure 4.
Immunohistochemistry of liver slides. Data shown are representative of at least seven rats. Sham operated animals submitted to anesthesia and laparotomy; I/R 90 min of ischemia followed by 90 min of reperfusion; O3+I/R, animals preconditioned with ozone and subjected to I/R. Arrows indicate the reaction intensity between p65 subunit with its antibody [24].
Figure 4.
Immunohistochemistry of liver slides. Data shown are representative of at least seven rats. Sham operated animals submitted to anesthesia and laparotomy; I/R 90 min of ischemia followed by 90 min of reperfusion; O3+I/R, animals preconditioned with ozone and subjected to I/R. Arrows indicate the reaction intensity between p65 subunit with its antibody [24].
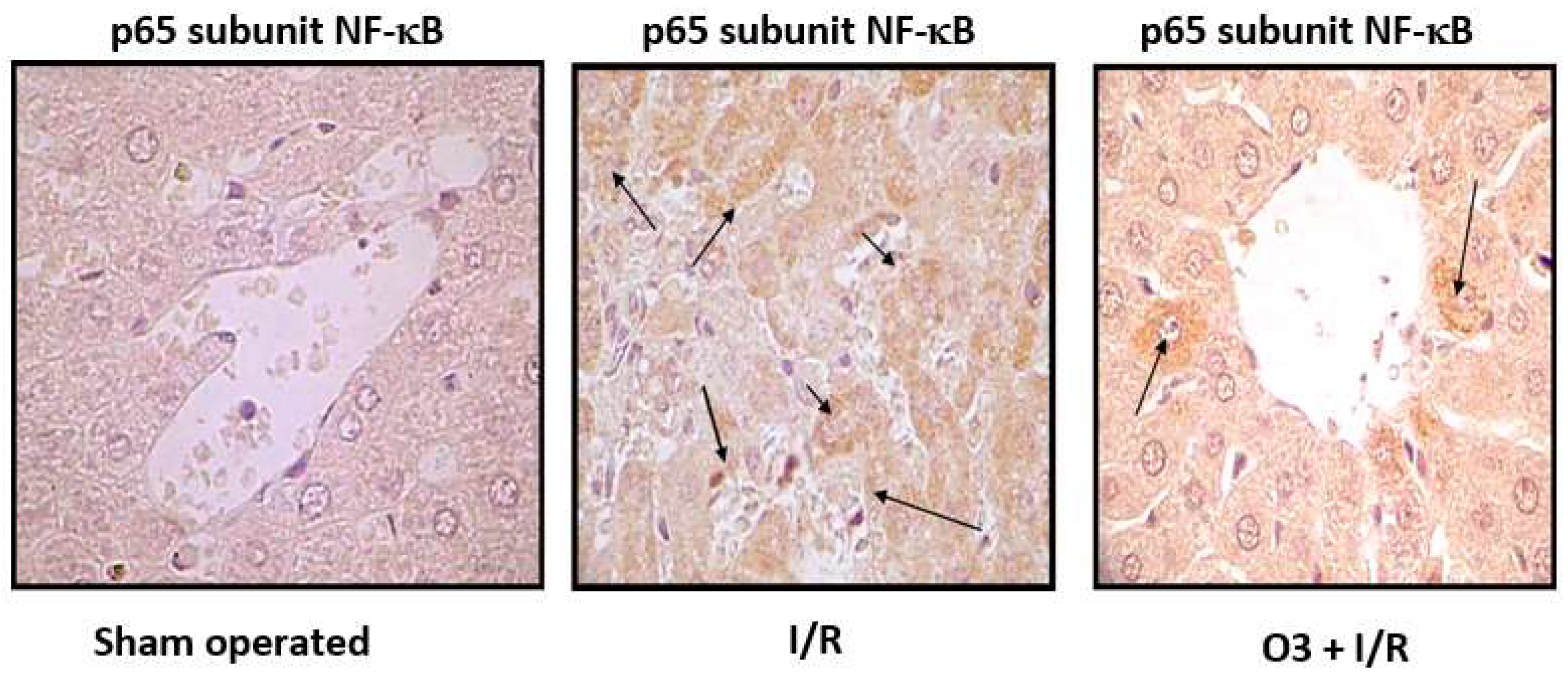
Figure 5.
Effects of medical ozone on myeloperoxidase enzyme activity in liver homogenates subjected to I/R. Mean ± SD of 5 rats in each group is represented. Different letters indicate significant differences (p< 0.05). I/R, ischemia/reperfusion; MPO, myeloperoxidase; O3, medical ozone; O2, oxygen.
Figure 5.
Effects of medical ozone on myeloperoxidase enzyme activity in liver homogenates subjected to I/R. Mean ± SD of 5 rats in each group is represented. Different letters indicate significant differences (p< 0.05). I/R, ischemia/reperfusion; MPO, myeloperoxidase; O3, medical ozone; O2, oxygen.
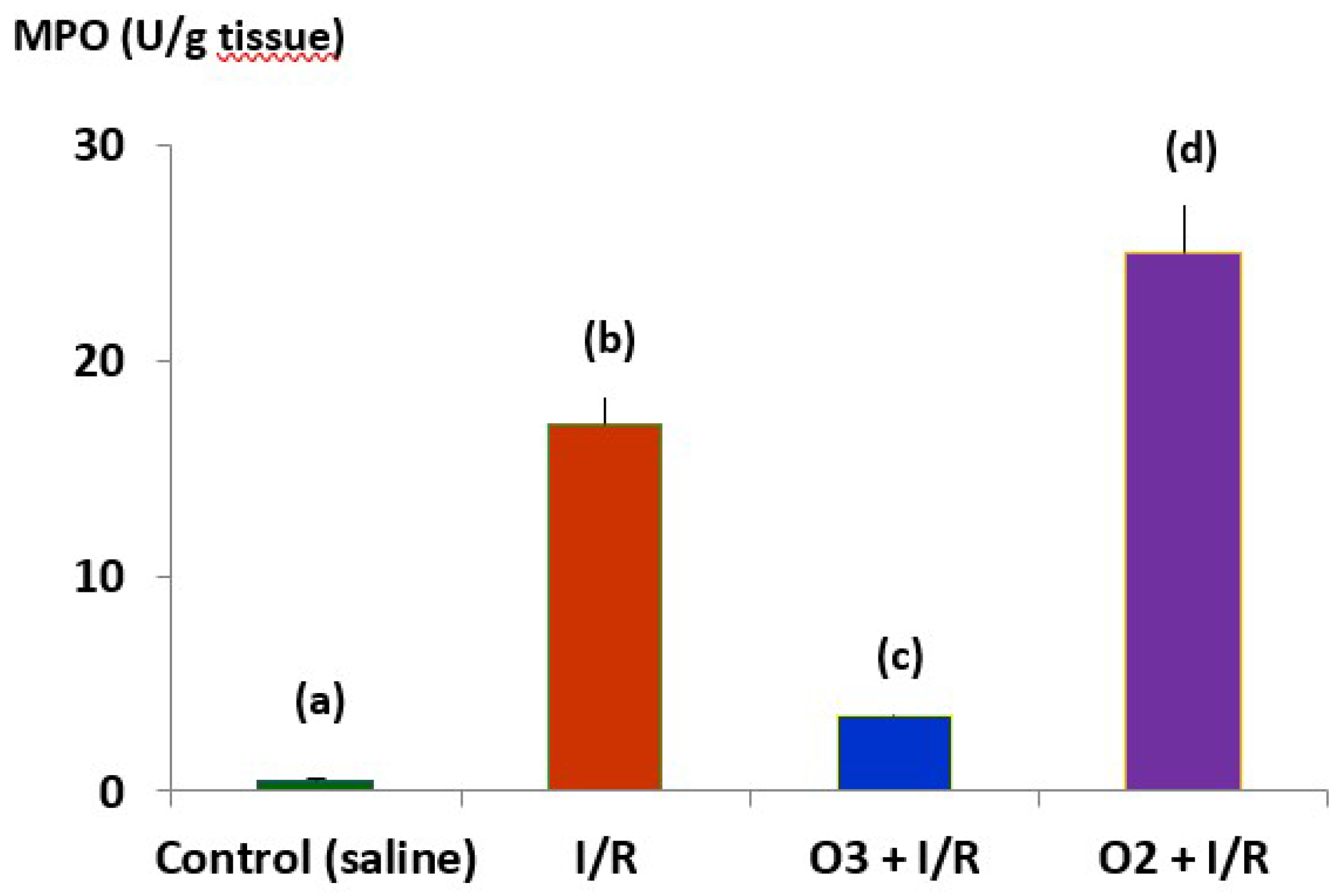
Figure 6.
Redox status of RA patients treated with MTX and MTX+ozone combination therapy at the end of the study (24 hours after the last medical ozone treatment). (A) Antioxidant defense markers, (B) Injury markers. The units of each marker are: SOD (superoxide dismutase activity, U/ml/min), CAT (catalase activity, U/L/min), GSH (reduced glutathione), NO (nitric oxide), AOPP (Advanced Oxidation Protein Products), TH (Total Hydroperoxides) and MDA (Malondialdehyde, µM). Linear (MTX + Ozone) signifies the linear tendency of experimental data. The data represent the mean ± SD of each group. [31].
Figure 6.
Redox status of RA patients treated with MTX and MTX+ozone combination therapy at the end of the study (24 hours after the last medical ozone treatment). (A) Antioxidant defense markers, (B) Injury markers. The units of each marker are: SOD (superoxide dismutase activity, U/ml/min), CAT (catalase activity, U/L/min), GSH (reduced glutathione), NO (nitric oxide), AOPP (Advanced Oxidation Protein Products), TH (Total Hydroperoxides) and MDA (Malondialdehyde, µM). Linear (MTX + Ozone) signifies the linear tendency of experimental data. The data represent the mean ± SD of each group. [31].
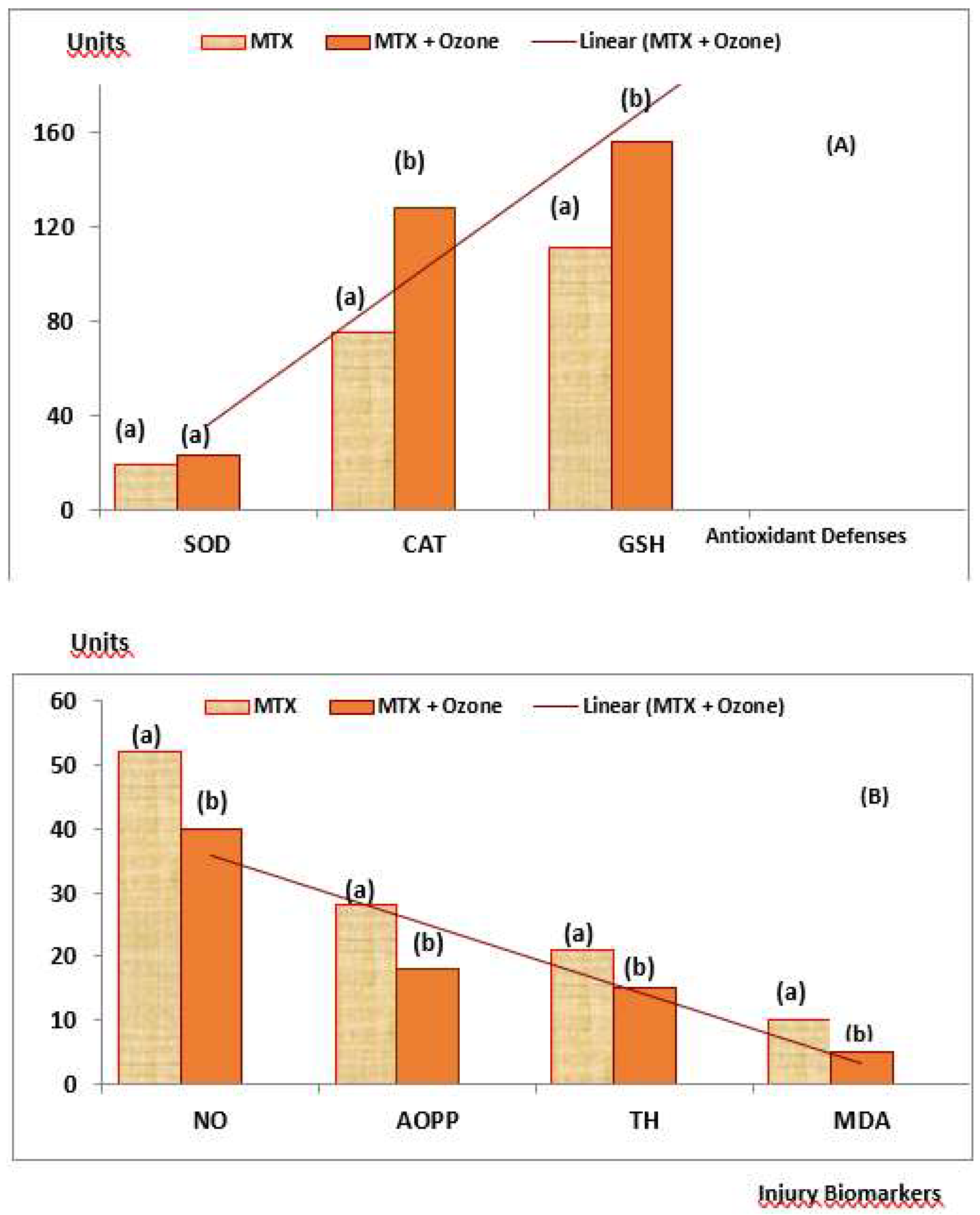
Figure 7.
Probable mechanism of action for the combined MTX+ozone therapy that integrates both the experimental results and the clinical response of patients suffering from RA, here explaining the beneficial effects of the introduction of medical ozone in pharmacotherapeutic treatment.
Figure 7.
Probable mechanism of action for the combined MTX+ozone therapy that integrates both the experimental results and the clinical response of patients suffering from RA, here explaining the beneficial effects of the introduction of medical ozone in pharmacotherapeutic treatment.
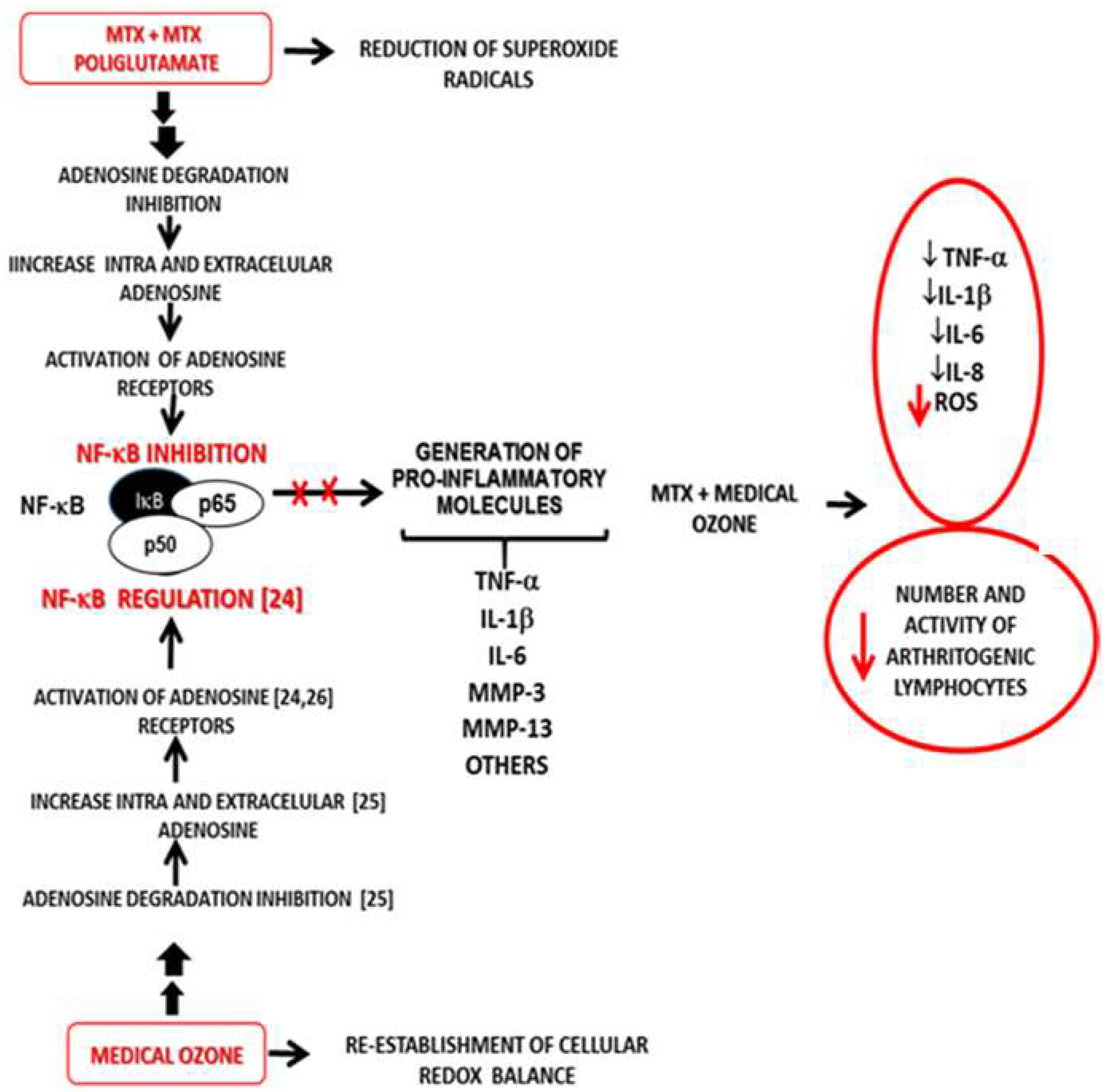

Table 1.
A number of redox marker levels in rat spleen homogenates in (A) carrageenan-induced synovitis and (B) PG/PS chronic arthritis models treated with ozone/oxygen.
Table 1.
A number of redox marker levels in rat spleen homogenates in (A) carrageenan-induced synovitis and (B) PG/PS chronic arthritis models treated with ozone/oxygen.
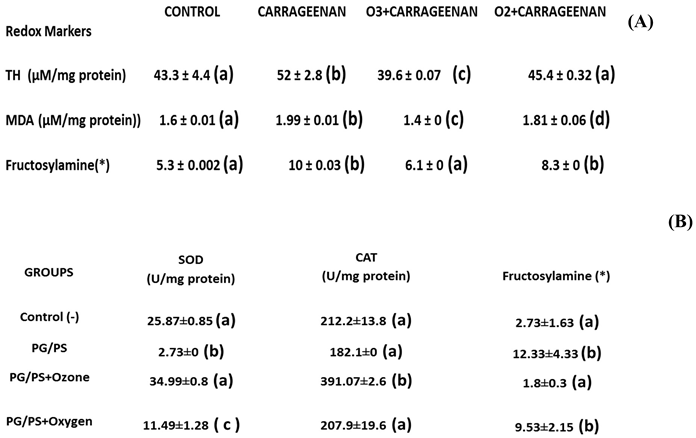 |
Table 2.
A number of redox marker levels in rat spleen homogenates in (A) carrageenan-induced synovitis and (B) PG/PS chronic arthritis models treated with ozone/oxygen.Table 2. Clinical variables of patients with RA at the beginning and at the end of the study.
Table 2.
A number of redox marker levels in rat spleen homogenates in (A) carrageenan-induced synovitis and (B) PG/PS chronic arthritis models treated with ozone/oxygen.Table 2. Clinical variables of patients with RA at the beginning and at the end of the study.
| MTX (n = 30) MTX | ||||
| Clinical Variables | Start | End | Start | End |
|
Pain DAS28 HAQ-DI CRP (mg/L) ESR Anti-CCP (U/ml) |
8.2 ± 0.47(a) 5.64 ± 0.36(a) 1.53 ± 0.16(a) 21.08 ± 7.12(a) 40.9 ± 6.62(a) 102.8 ± 34(a) |
7 ± 0.65(a) 5.21 ± 0.37(a) 1.14 ± 0.17(a) 13.14 ± 4.26(a) 40.3 ± 6.08(a) 119.2 ± 39(a) |
9.2 ± 0.37(a) 6.4 ± 0.22(a) 1.80 ± 0.10(a) 16.2 ± 4.75(a) 36.7 ± 6.38(a) 107 ± 62(a) |
4.7 ± 0.33(b,c) 3.2 ± 0.37(b,c) 0.75 ± 0.07(b,c) 5.53 ± 1.48(b,c) 20 ± 4.64(b,c) 89.7 ± 33(b,c) |
Legend:MTX group: Methotrexate + Ibuprofen + Folic acid. MTX+ozone group; same as MTX group + medical ozone: DAS28. Disease activity (low 3.2; moderate 3.2 and 5.1; high 5.1. HAQ-DI, Disability Index Questionnaire (+ 1.25); CRP, “C” Reactive Protein (+ 6 mg/L in serum); ESR, Erythrocyte Sedimentation Rate (male 7-8 mm, female 11-16 mm); Anti-CCP, antibodies against Cyclic Citrullinated Peptides (10 U/mL in serum). "Start" stands for the begin of the study and "End" for termination of the final ozone treatment 21 days after "Start". All data shown represent mean ± SD. Mean values with different letters indicate significant differences (p<0.05) (c) (p<0.05) on day 21 (at the end of the study) “MTX + ozone group” vs “MTX group” [32].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



