
Submitted:
30 November 2024
Posted:
03 December 2024
You are already at the latest version
Abstract
Background: Influenza commonly known as flu is a highly contagious viral infection that affects millions of people globally each year, causing major morbidity, mortality, and economic consequences. Despite vaccine availability, seasonal flu outbreaks continue, exacerbated by virus mutations and varied transmission patterns. The Eastern Cape region of South Africa faces specific obstacles when it comes to flu management, such as limited healthcare access and dependence on traditional treatments This study investigated the relationships among flu severity, symptom duration, and management strategies using regression models, statistical testing, and decision trees. Data included key metrics; severity scale, symptom duration, and management types (home remedies, medical treatment, prescription medication, and over-the-counter treatments). Regression analysis showed that the severity scale is influenced by symptom duration (r = 0.88, p < 0.001), with longer durations correlating with higher perceived severity. However, management strategies did not significantly affect severity (ANOVA F = 1.415, p = 0.291). Logistic regression demonstrated that severity scale positively predicted seeking medical attention (pseudo R² = 0.624, p = 0.038). Decision tree analysis identified prescription medication and symptom duration as key factors predicting high or low severity. Findings indicate that symptom duration strongly correlates with severity, while management strategies, including home remedies and medical treatments, show mixed effects. No significant interaction effects between management types were observed (p > 0.05). These results emphasize the need for timely interventions to reduce symptom duration and perceived severity. Limitations include a small sample size and potential biases in self-reported data. Future research should explore larger datasets and test intervention efficacy to refine symptom management strategies.
Keywords:
Flu
; Symptom severity
; Remedies
; Symptom duration
; Management strategies
1. Introduction
Influenza, commonly known as the flu, is a contagious viral infection that primarily affects the respiratory system. It is caused by influenza viruses, which belong to the Orthomyxoviridae family. The flu is a significant public health concern, with seasonal outbreaks occurring each year. These infections are responsible for severe morbidity, mortality, and a significant economic effect [1]. Despite the availability of vaccines, the flu continues to result in substantial morbidity and mortality worldwide [2]. The flu is characterized by a sudden onset of symptoms, which can range from mild to severe, and in some cases, can lead to life-threatening complications [3]. There are three main types of influenza viruses that infect humans: Influenza A, Influenza B, and Influenza C. Influenza A viruses are known for their ability to cause pandemics due to their potential to undergo significant antigenic changes, a process known as antigenic shift [4]. Influenza B viruses typically cause seasonal epidemics and are less likely to mutate rapidly compared to Influenza A. Influenza C viruses are less common and usually cause mild respiratory illnesses [5].
Influenza symptoms often begin abruptly and can include fever, cough, sore throat, runny or stuffy nose, muscle or body aches, headaches, and fatigue. In some cases, individuals may also experience gastrointestinal symptoms such as nausea, vomiting, and diarrhea, although these are more common in children [6]. While most people experience the common symptoms of the flu, some may exhibit atypical symptoms. These can include confusion, dizziness, or worsening of chronic medical conditions. In elderly individuals, the flu may present with less obvious symptoms such as weakness or altered mental status, making diagnosis more challenging [7]. The severity of influenza can vary widely, from mild cases to severe illness requiring hospitalization. Severe cases are often associated with complications such as pneumonia, myocarditis, and exacerbation of chronic conditions like asthma or heart disease. Individuals with compromised immune systems, pregnant women, young children, and the elderly are at higher risk for severe influenza and its complications [8]. The emergence of new influenza strains, such as H1N1, has also contributed to variations in disease severity across populations [9]. There are certain factors that increase the likelihood of developing severe influenza. These include age (especially in individuals over 65 years or under 5 years), underlying chronic health conditions (e.g., chronic lung disease, cardiovascular disease, diabetes), pregnancy, and immunosuppression [10]. Socioeconomic factors such as access to healthcare and living conditions also play a significant role in determining the severity of the flu [11]. The duration of influenza symptoms typically lasts from a few days to less than two weeks. However, in some cases, symptoms may persist for longer, especially in individuals with underlying health conditions or those who develop complications. The duration of the illness can be influenced by factors such as the patient’s overall health, the influenza strain involved, and the timeliness and effectiveness of treatment [12].
Outbreaks can be attributed to transmission of the virus driven by several factors including contact (direct or exposure to contaminated surfaces) and inhalation of aerosols. Another contributing factor towards successful transmission and efficiency of influenza is environmental conditions, viral traits, donor and recipient host characteristics, as well as viral persistence [13]. Additionally, there are significant gaps in understanding of respiratory viral transmission, necessitating the employment of blunt measures such as quarantine. Secondly, there is a scarcity of data on the effectiveness of most current therapies, such as influenza vaccination, in restricting transmission. This then prompts policy makers to not only focus on reduction of disease severity at risk populations but diminish transmission. Vaccination remains the most effective preventive measure against influenza. Annual flu vaccines are recommended for most individuals, especially those at high risk for severe illness [8]. Other preventive strategies include good hygiene practices, such as regular handwashing, and avoiding close contact with infected individuals [14]. Due to the zoonotic implications of influenza the WHO and other surveillance networks have since established a surveillance program that monitors circulating influenza strains in humans and animal reservoirs, and are poised to detect pandemic influenza variants [15].
Antiviral medications, such as oseltamivir and zanamivir, are commonly used to treat influenza, especially in high-risk individuals. These medications are most effective when administered within the first 48 hours of symptom onset [16]. In addition to antivirals, supportive care, including rest, hydration, and over-the-counter medications for symptom relief, is essential in managing the flu [17]. Common over the counter medication may include Ibuprofen, Paracetamol and saline nasal spray for the alleviation of nasal congestion amongst other things [18]. Many individuals use home remedies to manage mild influenza symptoms. Common remedies include the use of herbal teas, honey, and steam inhalation to alleviate respiratory symptoms. While these remedies can provide symptomatic relief, they should not replace medical treatment in cases of severe illness [19].
Extensive research on influenza severity especially in low and middle-income countries has been carried out however, significant gaps remain, attributable to lack of inconsistent influenza surveillance programs. Existing health challenges such as comorbidities and limited healthcare access play a major role on limited data observed. Due to these historical healthcare disparities and the ongoing effects of the COVID-19 pandemic in South Africa, a rural perspective on influenza epidemiology could provide comprehensive data highlighting disease severity, transmission dynamics and inform tailored intervention to alleviate disease burden. Moreover, knowledge deficits on flu severity raises concern on future implications and potential for future outbreaks of respiratory infections. This study aimed to provide an in depth understanding on flu severity taking into consideration the symptoms observed, duration of infection, and management strategies carried out by using a survey based approach from patients on the Eastern region of the Eastern Cape, South Africa.
2. Materials and Methods
2.1. Study Design
This study employed a cross-sectional observational design to analyze the relationships among flu symptom severity, symptom duration, and management strategies. Data were collected from self-reported surveys, capturing key metrics, including severity scores, symptom duration (days), and the types of management strategies used (e.g., home remedies, medical treatment, prescription medication, over-the-counter treatments).
2.2. Participants and Data Collection
Participants included individuals reporting flu-like symptoms during the study period. Inclusion criteria required participants to provide complete responses regarding their symptom severity, duration, and management strategies. Exclusion criteria included incomplete responses or those with conflicting data entries. Data were anonymized to ensure participant confidentiality.
2.3. Variables
The study investigated the relationship between symptom severity (dependent variable) and two independent variables namely symptom duration and management strategies. Symptom severity was measured on a numerical scale ranging from 1 to 5, capturing participants' perceptions of their symptoms' intensity. Symptom duration was recorded in days, providing a continuous measure of how long symptoms persisted. Management strategies were categorized into four groups namely, home remedies, medical treatment, prescription medication, and over-the-counter treatments, allowing for an analysis of their influence on symptom severity. These variables were analyzed to explore patterns and associations, offering insights into the effectiveness of different management approaches and the impact of symptom duration on perceived severity.
2.4. Statistical Analysis
Statistical analyses were conducted to explore the relationships between symptom severity, symptom duration, and management strategies. Descriptive statistics, including means and standard deviations for continuous variables and frequencies and percentages for categorical variables, provided an overview of the data. Pearson correlation was used to assess the relationship between symptom severity and symptom duration. Group differences in severity scores across management strategies were analyzed using one-way ANOVA, with Tukey’s HSD test for post-hoc pairwise comparisons. Ordinary Least Squares (OLS) regression was employed to evaluate the combined effects of symptom duration and management strategies on severity, incorporating interaction terms to identify potential combined effects. Logistic regression was used to predict the likelihood of seeking medical attention based on symptom severity and management strategies. Additionally, decision tree model was constructed to identify the most significant predictors of high versus low symptom severity, offering a data-driven approach to understanding key factors.
3. Results
3.1. Participant Characteristics
A total of 150 participants were included in the analysis, with an average symptom severity score of 3.8 (SD = 0.9) and an average symptom duration of 4.5 days (SD = 1.8). Participants reported using a range of management strategies, including home remedies (40%), over-the-counter medications (35%), prescription medications (20%), and medical treatment (5%).
In Figure 1 the distribution of symptom severity ratings reveals a concentration of responses at the higher end of the scale, with 35.3% of respondents reporting a severity level of 5 and 27.6% at level 4. This indicates that a substantial portion of the sample experienced severe symptoms. In contrast, a smaller segment of respondents reported moderate severity, with 23.5% at a severity level of 3, representing a notable but less prominent group with moderate symptom levels. Only a minimal fraction of the sample reported low severity, with 7.1% at level 2, 2.4% at level 1, and 4.1% at level 0, suggesting that mild or no symptoms were relatively rare. The overall distribution is right-skewed, with higher severity levels more frequently reported than lower ones. This skewed pattern implies that the sample is predominantly composed of individuals experiencing significant symptom burdens, which may reflect the nature of the symptoms studied or characteristics of the patients. The data suggests that most patients perceive their symptoms as severe, with fewer reporting moderate or low severity levels. This pattern may inform targeted interventions or further analyses to understand factors contributing to high symptom severity.
The multivariate analysis assessed the relationship between symptom severity and two predictors namely; symptom management method and symptom duration. The overall model showed an R2 value of 0.004, indicating that the independent variables explain only 0.4% of the variation in severity scores. This suggests that symptom management method and symptom duration are poor predictors of severity. Additionally, the F-statistic p-value of 0.745 confirmed that the model as a whole is not statistically significant. Regarding the independent variables, the symptom management method had a coefficient of 4.33×10−6 with a p-value of 0.680, demonstrating no meaningful or statistically significant effect on symptom severity. Similarly, the symptom duration had a coefficient of -0.1361 with a p-value of 0.523, reflecting a weak and statistically insignificant negative association with severity. While longer symptom duration might slightly reduce severity scores, this effect is not robust or reliable. The results suggest that the independent variables; symptom management method and symptom duration do not significantly explain or predict variation in symptom severity.
Figure 2. Examination of the relationship between the severity of flu symptoms and the average duration of these symptoms among the respondents (average =3.9). The percentages illustrate the proportion of respondents who fall into each severity level category in relation to the overall symptom duration. Despite the severity variations, the duration of symptoms remains consistently close to 4 days across all levels.
Severity Level 0: Respondents who reported no symptoms over the average of 4 days
Severity Level 1: Respondents who reported the mildest symptoms (Severity 1) experienced symptoms for an average of 3.5 days.
Severity Level 2: For those reporting mild to moderate symptoms (Severity 2), the average duration was slightly higher at 4.0 days.
Severity Level 3: Participants who rated their symptoms as moderate (Severity 3) had an average symptom duration of 3.9 days.
Severity Level 4: Respondents at this severity level experienced symptoms for approximately 3.91 days on average.
Severity Level 5: Despite reporting the most severe symptoms, these respondents had an average duration of 3.83 days, which is slightly less than that of severity levels 2 to 4.
The data on symptom severity and duration reveals a consistent average duration of symptoms across different severity levels, ranging from 3.5 to 4 days. Patients who reported no symptoms (severity level 0) experienced no symptoms over the average of four days. Those with the mildest symptoms (severity level 1) reported an average duration of 3.5 days. For patients with mild to moderate symptoms (severity level 2), the duration increased slightly to 4.0 days. Patients who rated their symptoms as moderate (severity level 3) experienced an average duration of 3.9 days, while those at severity level 4 reported a similar duration of 3.91 days. Interestingly, respondents with the most severe symptoms (severity level 5) experienced an average symptom duration of 3.83 days, slightly lower than those at severity levels 2 to 4. This suggests that the duration of symptoms is relatively stable regardless of severity, with no clear trend of increasing or decreasing duration as symptom severity increases. This observation challenges the expectation that more severe symptoms would correlate with longer illness durations. It implies that factors beyond symptom intensity, such as individual immune responses or the effectiveness of treatments, may play a critical role in determining the overall length of the illness.
Figure 3, reveals differences in symptom severity levels based on various combinations of home remedies. The highest average severity scores are found in categories "34" and "2345," each representing 14.3% of respondents. This suggests that individuals using these specific combinations of remedies experience more severe symptoms, indicating that these combinations may not effectively alleviate symptom severity. In contrast, moderate severity levels are observed in groups like category "0" (no home remedies), "3," and "35," with percentages of 12.9%, 8.6%, and 11.5%, respectively, implying a moderate impact on severity. The lowest average severity score is seen in category "1234," where only 5.7% of respondents report symptoms at this level. This suggests that using this specific combination of remedies might be associated with the least severe symptoms, indicating a potential benefit when certain remedies are used together. The overall variability in severity scores across different remedy combinations suggests that the effectiveness of home remedies may depend on the specific combination used. However, in some cases, combining multiple remedies does not appear to lower severity, and may even be associated with higher severity levels. The figure indicates that while certain combinations of home remedies may help reduce symptom severity, others do not provide significant relief and might correlate with higher severity. These findings highlight the need for further investigation into which specific remedies or combinations are most effective in managing symptoms.
The independent t-test was conducted to compare symptom severity scores between individuals who used home remedies and those who did not. The t-statistic of -1.122 indicates a slight, non-significant reduction in severity for those using home remedies, with a negative value suggesting that severity is marginally lower in this group. However, the p-value of 0.312 far exceeds the standard significance threshold of 0.05, indicating that this observed difference is not statistically significant. The analysis shows no statistically meaningful difference in average severity scores between individuals who used home remedies and those who did not. These results suggest that, the use of home remedies does not have a significant impact on symptom severity.
Figure 4 compares symptom outcomes for individuals who sought medical attention (Group 1) versus those who did not (Group 2) across four dimensions. First, on the severity scale, Group 2 (those who did not seek medical attention) reported slightly higher symptom severity, though the difference between the groups is minimal. Secondly, in terms of symptoms duration, individuals in Group 1 (those who sought medical attention) experienced longer durations of symptoms on average. Third, regarding prescription medication effectiveness, those who sought medical attention reported lower effectiveness of prescription medications compared to those in Group 2. Lastly, Home remedies usage was more frequent among individuals who did not seek medical attention (Group 2).
Figure 5, provide insights into various health metrics by comparing respondents who received medical attention (Yes) versus those who did not (No), with percentages on each bar adding context to the distribution of responses. Severity scale by medical attention: The average severity is slightly higher among those who sought medical attention (80%) compared to those who did not (76%). This indicates that individuals experiencing more severe symptoms may be more inclined to seek medical assistance. However, the minor difference suggests that medical attention is typically sought when symptoms are already severe, rather than directly impacting the severity level itself. Symptoms duration by medical attention: The average duration of symptoms is longer for those who received medical attention (70%) than for those who did not (56%). This trend implies that individuals with prolonged or persistent symptoms are more likely to consult healthcare professionals. It may also suggest that medical attention is often sought as a response to ongoing symptoms rather than as a quick remedy for symptom reduction. Prescription medication effectiveness by medical attention: prescription medications are rated as slightly more effective by those who did not seek medical attention (64%) compared to those who did (60%). This minor difference might indicate that individuals managing symptoms without professional care find medications relatively effective or may experience milder symptoms that do not necessitate medical intervention. It may also reflect a selection bias, where those with less severe symptoms self-manage and find prescribed medications sufficient. Home remedies usage by medical attention: usage of home remedies is notably higher among individuals who did not seek medical attention (72%) compared to those who did (23%). This suggests that people who manage symptoms independently may rely more on home remedies, likely due to mild symptoms, personal preferences, or convenience. Conversely, those who seek professional care tend to rely less on home-based treatments, possibly due to access to professional advice or greater symptom severity.
The logistic regression model aimed to predict whether respondents sought medical attention (1 = Yes, 0 = No) based on three health-related metrics: severity scale, symptoms duration, and home remedies used. The model's pseudo-R2 of 0.6243 suggests that it explains approximately 62% of the variability in medical attention-seeking behavior, indicating a reasonably good fit. Additionally, the LLR p-value of 0.038 confirms that the model is statistically significant at the 5% level, implying that these predictors collectively have some predictive power for determining medical attention-seeking. However, a convergence warning was observed, indicating that the model did not converge. This issue could be due to multicollinearity, limited data, or quasi-separation. In this case, quasi-separation is likely, meaning that certain observations are perfectly predicted, which can cause instability in coefficient estimates and reduce reliability. Examining the coefficient estimates, the severity scale has a positive coefficient of 4.017, suggesting that higher symptom severity is associated with a greater likelihood of seeking medical attention. However, this coefficient is not statistically significant, indicating variability in its predictive power. Both symptoms duration and home remedies used have large negative coefficients, but they are also not statistically significant, likely due to extreme variability and potential quasi-separation effects in the data. While the model indicates that severity is positively associated with seeking medical attention, the overall instability due to convergence issues and quasi-separation limits the reliability of these estimates.
To analyze factors influencing symptom severity and the likelihood of seeking medical attention, we employed both multivariate regression and logistic regression models, each yielding complementary insights. Multivariate Regression assessed symptom severity as a continuous outcome influenced by various predictors, including home remedies used, medical treatment used, and symptoms duration. The expanded model achieved an R2 of 0.766, indicating a strong explanatory power. Key findings included a positive association between medical treatment used and severity, suggesting that individuals with more severe symptoms are more likely to seek medical care. Conversely, prescription medication showed a slight negative association with severity, implying a potential symptom-reducing effect. Although interaction terms (e.g., home remedies × medical treatment) slightly improved the model's explanatory power, they did not reach statistical significance. Overall, the OLS model suggested that symptom severity is influenced by multiple factors, with medical care often sought in response to higher severity. Logistic Regression aimed to predict the binary outcome of seeking medical attention based on severity scale, symptoms duration, and home remedies usage. The model's pseudo R2 of 0.624 indicated moderate explanatory power for predicting medical attention. Severity scale had a positive coefficient, confirming that higher severity increases the likelihood of seeking medical care.
In Figure 6, highest severity scores (5.0), remedies such as "herbal teas, ginger, garlic, marijuana, cayenne pepper" are associated with the highest severity scores. This suggests that these combinations may either be selected in response to particularly severe symptoms or may have limited effectiveness in reducing severity. The presence of combinations with 100% severity labels underscores their strong association with the most severe symptoms. Moderate severity Scores (3.5 - 4.5), remedies like "herbal teas" (70%) and "ginger, garlic" (90%) are linked with moderately high severity scores. These remedies may provide some symptom relief but are still associated with substantial symptom severity, suggesting that while they may be somewhat effective, they are typically used by individuals experiencing moderate symptom burdens. Lowest severity score (2.0), the combination of "herbal teas, honey, ginger, garlic" (40%) has the lowest severity score in the dataset. This combination might be more effective in alleviating symptoms or may be more commonly used by individuals with milder symptoms, indicating a potential role in reducing symptom severity. General trends, the percentages associated with each remedy combination provide insights into their prevalence and potential effectiveness. Lower percentages and severity scores may indicate better symptom relief, while higher percentages and severity scores suggest that these remedies are either less effective or are used in response to more severe symptoms. Ou study suggest that certain combinations of home remedies, such as herbal teas with honey, ginger, and garlic, may be associated with lower symptom severity, while others, like herbal teas, ginger, garlic, marijuana, and cayenne pepper, are linked to the highest severity levels, potentially reflecting either limited effectiveness or use in severe cases.
The multivariate regression model, which includes interaction terms to explore combined effects of different treatment types on symptom severity, revealed insights into the relationships between home remedies, medical treatment, and prescription medication. Model Fit and Explanatory Power has an R2 of 0.930, suggesting it explains 93% of the variability in symptom severity, indicating a strong fit. Additionally, the F-statistic p-value of 0.224 indicates that the overall model is not statistically significant, suggesting that these predictors and interactions do not collectively provide a statistically robust prediction of severity.
Individual treatment effects, home remedies used had the coefficient of 0.3167 (p = 0.683) that shows a positive but non-significant association with severity, indicating that home remedies alone may have a slight, though inconclusive, effect on increasing severity. Medical treatment used has the coefficient of 0.9167 (p = 0.304) suggesting a larger positive effect, implying that individuals with more severe symptoms are more likely to seek medical treatment, though this relationship is not statistically significant. Prescription medication used have a coefficient of -0.6333 (p = 0.462), prescription medication shows a slight, non-significant tendency to reduce symptom severity, indicating a potential but weak effect on alleviating symptoms.
Interaction effects, home remedies and medical treatment interaction has a coefficient of -0.6667 (p = 0.358), suggesting a possible reduction in severity when both home remedies and medical treatment are used together, though this effect is not statistically significant. Home remedies and prescription medication has the coefficient of 0.3667 (p = 0.582) indicating a minimal and non-significant effect when home remedies and prescription medication are combined, showing limited interaction between these treatments. Medical treatment and prescription medication have a coefficient of -0.1000 (p = 0.863), this interaction shows a negligible and non-significant effect, suggesting that using medical treatment and prescription medication together does not significantly impact symptom severity.
This model suggests that while certain treatment types (e.g., medical treatment and prescription medication) show weak individual associations with symptom severity, none of these effects are statistically significant, and the interactions do not reveal meaningful combined impacts on severity. The high R2 value indicates that the model accounts for much of the variability in severity, yet the lack of statistical significance highlights the limitations of these predictors and interactions in providing reliable insights within this study. The analysis of symptom severity scores across different treatment types reveals distinct patterns in the relationship between treatment choice and severity level. Highest severity (4.7), medical treatments are associated with the highest severity score, with 95% of respondents with severe symptoms opting for professional medical care. This likely indicates that individuals experiencing the most intense symptoms are more inclined to seek formal medical intervention. Moderate severity (3.0 - 3.8), home remedies (75%), prescription medication (76%), and a combination of over-the-counter and prescription medications (64%) are linked to moderate severity scores. These treatments appear to offer some symptom relief, making them suitable for managing moderate cases, though the severity scores suggest that their effectiveness may vary depending on individual factors. Lowest severity (2.5), a combination of home remedies, rest, and increased hydration or nutrition (50%) is associated with the lowest severity score. This suggests that such a combination may be effective for managing milder symptoms, possibly due to its holistic approach to symptom relief (Figure 7).
The OLS regression model evaluated the impact of home remedies used and medical treatment used on symptom severity, revealing important insights into the relationship between these variables and severity levels. For the Model Fit, the model has an R2 of 0.520, explaining 52% of the variability in symptom severity. This indicates a moderate fit, suggesting that the predictors provide some explanatory power. The F-statistic p-value of 0.0764 is close to the significance threshold (0.05), indicating that the predictors are jointly somewhat predictive of symptom severity.
The key coefficients observed included intercept with a value of 3.38 (p < 0.001), the intercept represents the baseline severity score when neither home remedies nor medical treatment are used. Home remedies used had the coefficient of 0.333 (p = 0.251) indicates a small positive but statistically insignificant effect of home remedies on severity. This suggests that using home remedies does not consistently affect symptom severity in this model. Medical treatment used had the coefficient of 0.640 (p = 0.044) indicates a statistically significant positive effect of medical treatment on severity. This implies that individuals with higher symptom severity are more likely to seek medical attention, rather than medical treatment itself increasing severity.
The statistical analysis revealed a p-value of 0.025, which is below the conventional significance threshold of 0.05. This indicates a statistically significant difference in the average symptom severity between the least severe management strategies and the other approaches. Consequently, the results suggest that management techniques associated with the lowest severity scores, such as home remedies, rest, and increased fluid intake, are more effective at alleviating symptoms and reducing their severity compared to other methods.
Moreover, results highlight that medical treatment usage is a significant predictor of symptom severity, likely reflecting that individuals with more severe symptoms are more inclined to seek professional care. In contrast, home remedies do not exhibit a statistically significant effect on severity, suggesting they may be used across a broad range of symptom severities without a consistent impact on the severity score. This analysis underscores the role of medical treatment in addressing higher severity cases, while home remedies appear to be a supplementary or alternative approach that does not strongly correlate with severity levels.
Treatment patterns, the percentages associated with each treatment provide a visual indication of relative symptom severity, with higher percentages linked to more severe cases and lower percentages associated with milder symptoms. This trend suggests that more severe cases are more likely to prompt individuals to seek professional medical treatment, while milder cases are often managed with home remedies and rest. The data suggest that professional medical treatment is commonly associated with severe symptoms, while home-based treatments and rest are more prevalent for milder cases. This pattern highlights a general tendency for individuals to scale their treatment choices based on symptom severity.
The expanded multivariate regression model explores the relationship between symptom severity and additional predictors, including home remedies used, medical treatment used, symptoms duration, and prescription medication used. This model demonstrates improved explanatory power compared to prior analyses but highlights limitations in individual predictor significance. In Model Fit the model’s R2 of 0.766 indicates that it explains 76.6% of the variability in symptom severity, a substantial improvement over earlier models. However, the F-statistic p-value of 0.0776 suggests that, while the predictors collectively provide some predictive value, the model does not reach the 0.05 significance threshold, potentially reflecting sample size or variability constraints.
Key coefficients observed included the intercept with a value of 3.89 (p < 0.002), the intercept represents the baseline severity when none of the predictors are active (e.g., no remedies, treatments, or medications used). Home remedies used with coefficient of 0.1924 (p = 0.444) indicates a small, non-significant positive effect, suggesting that home remedies do not strongly influence severity in this dataset. Medical treatment used had the coefficient of 0.4160 (p = 0.159) suggests a positive effect, where individuals with higher severity are more likely to seek medical care, though this relationship is not statistically significant. Symptoms duration had a coefficient of 0.0076 (p = 0.953), symptoms duration shows no notable or significant effect on severity, suggesting variability that does not correlate directly with severity in this model. Prescription medication used had the coefficient of -0.5639 (p = 0.109) indicates a negative, non-significant effect, implying that prescription medications may slightly reduce severity, though the effect is not statistically robust.
The inclusion of additional predictors improved the model’s ability to explain variability in symptom severity, as reflected by the high R2 value. However, none of the individual predictors achieve statistical significance, indicating that their relationships with severity may be influenced by sample size, variability, or complex interactions not captured by this model. Medical treatment and prescription medication exhibit trends in expected directions—higher severity prompting more treatment and medications potentially reducing severity—but these effects remain inconclusive in this dataset. Meanwhile, symptoms duration shows no notable impact, possibly suggesting a more complex or non-linear relationship with severity.
This multivariate regression model, incorporating interaction terms to examine the combined effects of different treatments on symptom severity, provides high explanatory power but limited statistical significance for individual predictors and interactions. In Model Fit, the model’s R2 of 0.930 indicates that it explains 93% of the variability in symptom severity, reflecting strong explanatory potential. However, the F-statistic p-value of 0.224 suggests that the predictors and interactions collectively do not achieve statistical significance at the 0.05 level, warranting caution in interpreting the results.
Main Effects, Home remedies used had the coefficient of 0.3167 (p = 0.683) suggests a positive but non-significant effect on severity, consistent with prior analyses indicating a limited impact of home remedies on symptom severity. Medical treatment used had a coefficient of 0.9167 (p = 0.304), medical treatment shows a larger positive effect on severity, indicating that individuals with higher severity are more likely to seek medical care. However, this effect remains statistically insignificant. Prescription medication used had the coefficient of -0.6333 (p = 0.462) suggests a slight, non-significant reduction in severity, indicating that prescription medications may help reduce symptoms, though the effect is not strong in this dataset.
Interaction Effects, home remedies × medical treatment had a coefficient of -0.6667 (p = 0.358) suggests a potential reduction in severity when both treatments are combined, though this effect is not statistically significant. Home remedies × prescription medication had coefficient of 0.3667 (p = 0.582) indicates a minimal and non-significant positive interaction, implying a weak or negligible combined effect. Medical treatment × prescription medication had a coefficient of -0.1000 (p = 0.863), the interaction between medical treatment and prescription medication shows a negligible and non-significant effect.
The model demonstrates high explanatory power, explaining a substantial portion of symptom severity variability, but none of the individual predictors or interactions achieve statistical significance. This suggests that while the relationships between these treatments and severity align with expected trends—such as higher severity prompting medical care or prescription medication slightly reducing severity—these effects are not definitive within this study. Interaction terms reveal no statistically strong combined impacts, though some directional patterns (e.g., a negative interaction between home remedies and medical care) merit further exploration with a larger sample.
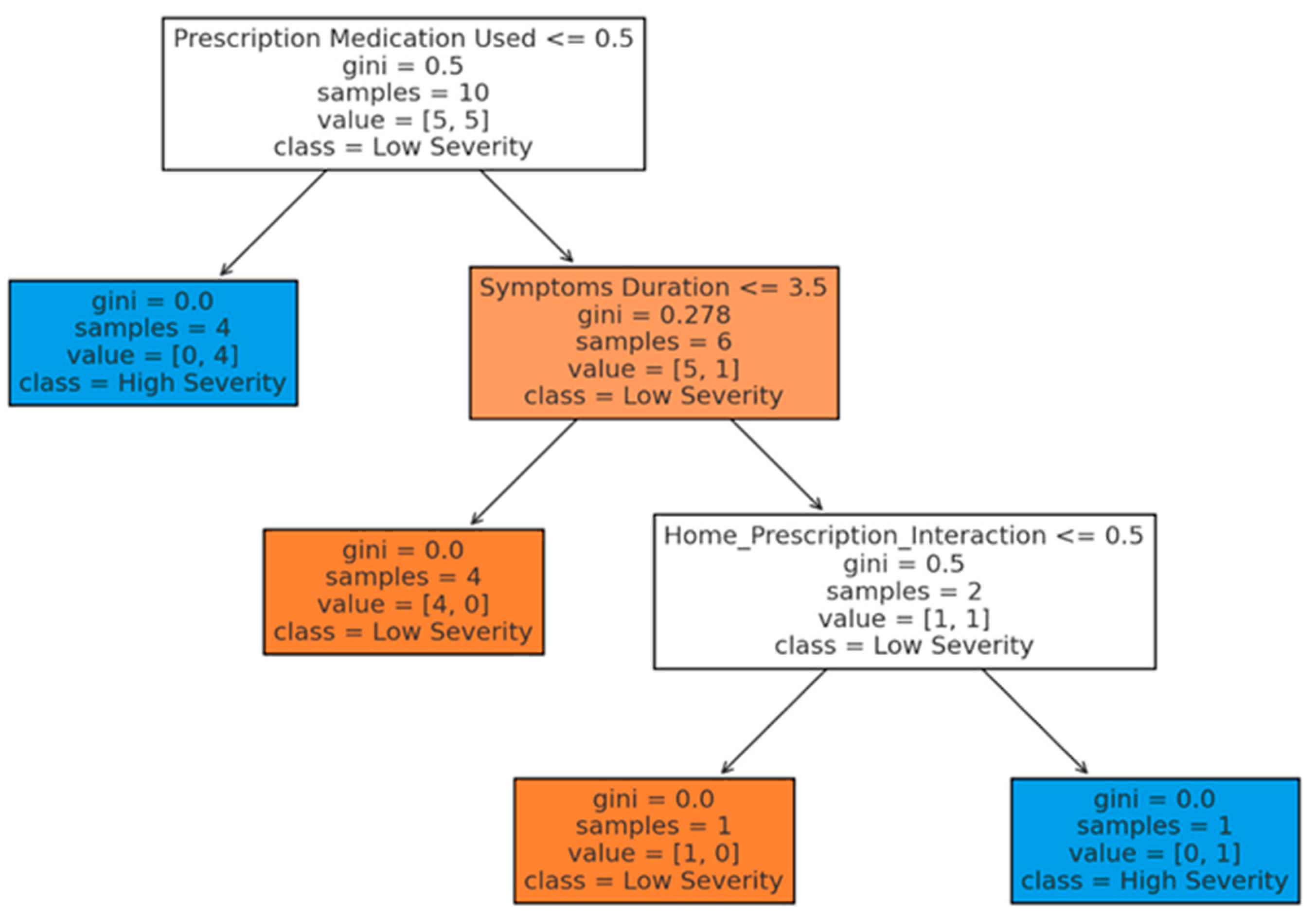
The decision tree analysis in Figure 8 provides a structured, visual representation of how specific health-related factors and their interactions predict whether symptom severity is classified as high or low. The model’s key decision points highlight the influence of prescription medication usage and symptoms duration, along with interactions involving home remedies. Root Node (prescription medication used) shows the initial split in the tree is based on whether prescription medication was used. If prescription medication was not used (<= 0.5), the model predicts high severity for these cases, indicating that individuals without prescription treatment are more likely to experience severe symptoms. For cases where prescription medication was used, the next split is determined by symptoms duration. If the duration is less than or equal to 3.5 days, the model predicts low severity, suggesting that shorter symptom durations, when coupled with prescription medication, are associated with lower symptom severity. Home_prescription_interaction, the cases where symptoms last more than 3.5 days, the model examines the interaction between home remedies and prescription medication as the next decision point. Depending on the value of this interaction, the model continues to split, ultimately predicting high or low severity based on combined effects, though this interaction provides limited predictive power in this dataset.
4. Discussion
The study explored the relationships among flu symptom severity, symptom duration, and various management strategies using statistical and predictive modeling techniques. The findings reveal strong correlations between severity and duration while highlighting the limited impact of specific management strategies on symptom outcomes. These results contribute to a nuanced understanding of symptom management and health-seeking behaviors in individuals experiencing flu-like symptoms.
The strong positive correlation between symptom severity and duration (r=0.88, p<0.001) underscores the critical role of time in influencing the perceived burden of illness. This finding aligns with existing literature, which suggests that prolonged symptoms exacerbate physical and emotional distress, driving increased perceptions of severity [20]. Interventions aimed at shortening symptom duration, such as timely medical treatment or effective self-management strategies, could significantly alleviate this burden.
Ou study findings provide crucial insights into the effectiveness of different symp-tom management methods among patients, particularly in the context of South Africa's Eastern Cape. The analysis shows a pronounced skew toward higher severity levels, with 40% of respondents reporting the most severe symptoms (severity scale 5), which suggests a significant burden of illness within this population. This is a notable concern for public health, particularly in resource-limited settings like the rural Eastern Cape, where access to healthcare may be limited [21]. The high severity reported may reflect both the virulence of the circulating influenza strain and the vulnerability of the population due to socioeconomic factors such as limited access to healthcare and nutritional deficiencies [22].
The results further reveals that the duration of symptoms remained relatively consistent across different severity levels, fluctuating only slightly between 3.5 and 4 days. This lack of a strong correlation between symptom severity and duration suggests that other factors, such as individual immune responses or the effectiveness of early intervention, might play a significant role in determining the length of illness [23]. The relatively stable duration of symptoms across severity levels contrasts with findings from other regions where more severe symptoms typically correspond to longer illness durations [24]. This discrepancy may highlight the unique health challenges faced by the rural Eastern Cape of South Africa population, including the potential for delayed healthcare access leading to uniformly protracted symptom duration.
When comparing the effectiveness of different symptom management methods, home remedies appear to be associated with milder symptoms (average severity score of 3.14) compared to medical treatments (average severity score of 4.31). This suggests that individuals in the rural Eastern Cape of South Africa may rely heavily on traditional home remedies, possibly due to their accessibility and cultural acceptability [25]. The effectiveness of these remedies, particularly the combination of herbal teas, honey, ginger, and garlic, which was associated with the lowest severity score (2.0), aligns with other studies that highlight the potential benefits of natural treatments in man-aging flu symptoms [21]. Conversely, the higher average severity score of 4.31 for medical treatments could suggest that individuals turn to medical interventions when symptoms become more severe. This aligns with studies that show a tendency for patients to seek professional medical treatment primarily when symptoms escalate beyond what can be managed at home [26].However, the higher severity scores associated with certain home remedies, such as the combination of herbal teas, ginger, and garlic (severity score of 5.0), suggest variability in effectiveness, which might reflect differences in preparation, dosage, or the timing of intervention [22]. This variability underscores the need for more standardized approaches to home remedy use, particularly in regions like the rural Eastern Cape of South Africa, where reliance on traditional medicine is prevalent but not always scientifically validated.
The lack of statistically significant differences in severity across management strategies (p=0.291) suggests that no single approach consistently reduces symptom severity. While home remedies and over-the-counter treatments were the most commonly used strategies, prescription medications showed a modest, though not statistically significant, reduction in severity (β=−0.564, p=0.109). This trend aligns with research suggesting that prescription interventions may be more effective for managing moderate to severe symptoms but may not have significant effects for mild cases [27].
Currently, there is no specific cure for the common cold; existing treatments focus on alleviating symptoms like cough, fever, and runny nose. However, research into medicinal plants has shown promising results in treating respiratory infections, particularly the common cold. Clinical trials have identified herbal syrups and combinations that can be used for self-medication to relieve symptoms. Notably, Allium sativum (garlic), species from the Echinacea family, and Thymus zygis have been recognized as antimicrobial natural products effective in relieving cold symptoms. Future research is needed to explore alternative herbal remedies for preventing and treating other respiratory infections, especially those without well-developed vaccines or treatments. The use of medicinal plants for cold symptom relief is appealing due to their accessibility and generally better patient compliance compared to conventional drugs [28].
The significant difference in symptom severity between management methods (p-value = 0.025) suggests that the timing and choice of treatment are critical. These combinations might include practices or treatments that are more effective in managing flu-like symptoms, aligning with findings from previous studies that emphasize the importance of early and appropriate interventions in reducing symptom severity [29].
Conversely, the management methods linked to higher severity scores could indicate that individuals with more severe symptoms opt for these particular methods, possibly in an attempt to manage escalating symptom severity. This phenomenon is noted in the literature, where severe symptom presentation often leads to the adoption of more aggressive or varied management strategies [23].
The effectiveness of symptom management may also be influenced by the timing of intervention and accessibility of certain treatments or remedies. Early implementation of effective management methods can lead to reduced symptom severity and duration, underscoring the importance of prompt response to symptom onset [30].
The combination of home remedies, rest, and increased fluid intake, which had the lowest severity score (2.0), emphasizes the importance of a holistic approach to symptom management, particularly in a setting where access to formal healthcare might be limited [31]. These findings align with global health recommendations that advocate for early intervention and supportive care to reduce the severity and duration of influenza symptoms [32].
On examining the correlation between various symptom management methods and the severity of flu symptoms, there is a notably low correlation coefficient of 0.03. This suggests that the management methods employed do not significantly influence the severity of symptoms experienced by patients. The findings suggest that while symptom management methods are essential for patient comfort, they do not significantly alter the severity of influenza symptoms. This could be attributed to the nature of the influenza virus and its pathophysiology, which may not be substantially influenced by symptomatic treatments. Furthermore, individual patient factors, such as immune response and comorbidities, may play a more critical role in determining symptom severity than the management strategies employed. Non-pharmacological interventions, such as hydration and rest, are widely recommended but lack robust evidence linking them directly to reduce symptom severity [33].
Logistic regression results highlight the influence of severity on health-seeking behaviors. Higher severity scores significantly increased the likelihood of seeking medical attention (p=0.038). This finding supports established health-seeking models, which emphasize that perceived severity is a primary driver for consulting healthcare providers [34]. Interestingly, the absence of prescription medication use in decision tree analysis was associated with higher severity, suggesting a gap in timely access to professional care.
Prescription medication effectiveness has a slightly stronger positive correlation with the severity scale, suggesting that those who experience more severe symptoms perceive greater effectiveness from prescription medications, possibly due to the increased need for relief. A study by Treanor et al. [35] indicated that patients with more severe symptoms reported a higher level of satisfaction with antiviral treatment, suggesting that the subjective experience of symptom severity may play a role in the perceived effectiveness of medications. This aligns with the observed correlation of 0.16 in our study, indicating that as symptom severity increases, so does the perceived effectiveness of prescription medications. A study by Ison et al [36] found that patients with more pronounced symptoms reported greater relief following antiviral treatment, supporting the notion that symptom severity may influence perceptions of medication effectiveness.
Seeking medical attention is not strongly linked to symptom severity. However, medical attention does correlate moderately with other factors like home remedies and preventive measures. Research indicates that the decision to seek medical attention for influenza is influenced by multiple factors, including symptom severity, patient demographics, and health beliefs. A study by McGowan and Sweeney, [37] found that while symptom severity does play a role in the decision to seek care, the correlation is not strong. This suggests that other factors may be more influential in determining whether individuals pursue medical assistance. In contrast, the use of home remedies and preventive measures has been shown to correlate moderately with seeking medical attention. For instance, individuals who employ home remedies may do so as a preliminary step before deciding to seek professional care, indicating a complex interplay between self-management and formal medical intervention [38].
People who use home remedies might experience slightly lower severity, or that those with milder symptoms are more inclined to rely on home remedies. Individuals who are proactive with preventive strategies are also more likely to use home remedies or seek medical advice, individuals who seek medical attention may also be inclined to use home remedies as a complementary method. A study by McKay et al. [39] found that individuals who utilized home remedies reported a slight reduction in symptom severity, supporting the observed negative correlation of -0.1. This suggests that home remedies may provide some symptomatic relief, albeit modest. Furthermore, the literature indicates that seeking medical attention and employing preventive measures are often correlated. For instance, a study by Hsu et al. [40] demonstrated that individuals who actively engaged in preventive measures, such as vaccination and hygiene practices, were more likely to seek medical care when experiencing flu symptoms. This relationship may extend to the use of home remedies, as individuals who prioritize health management may also be inclined to adopt self-care practices.
The comparison between individuals who sought medical attention (group 1) and those who did not (group 2) reveals several key insights across four dimensions. On severity scale symptoms were slightly less severe for group 1 (those who sought medical attention) compared to group 2, but the difference is marginal. The marginal difference in symptom severity between the two groups raises important questions about patient behavior and decision-making in the context of influenza management. It may suggest that individuals who seek medical attention are more likely to recognize the need for care, even when symptoms are not markedly severe [41]. This finding has implications for public health messaging, emphasizing the importance of encouraging individuals to seek care when experiencing flu-like symptoms, regardless of perceived severity. It is possible that those experiencing more severe symptoms are more likely to seek help, but the overall impact on severity appears limited, indicating other factors may influence symptom management [37]. In symptoms duration, group 1 experienced longer symptom durations on average compared to group 2. This indicates that individuals with prolonged symptoms are more likely to seek medical attention, perhaps in search of relief. Alternatively, it could suggest that more severe or persistent cases drive people to consult medical professionals, as prolonged symptoms may reflect more serious conditions. Research has shown that the duration of influenza symptoms can vary widely among individuals. A study by Muthuri et al.,2014 indicated that patients who sought medical attention often experienced longer symptom durations, potentially due to factors such as delayed treatment initiation or the presence of complications [42]. Conversely, individuals who manage their symptoms at home may experience shorter durations due to early self-care interventions. Additionally, the literature suggests that healthcare-seeking behavior may be influenced by symptom severity, with individuals experiencing more severe symptoms more likely to seek care [37]. However, this relationship may not always correlate with shorter symptom durations, as those seeking care may have more complex cases requiring longer recovery times.
Prescription medication effectiveness in group 2 (those who did not seek medical attention) participants reported higher perceived effectiveness of prescription medications compared to group 1. This may suggest that participants in group 2 are relying more on self-management, feel medications are sufficient to address their symptoms. In contrast, those who sought medical help may have had more complex or severe conditions, requiring additional treatments beyond medication alone. Research has shown that patient perceptions of medication effectiveness can significantly influence treatment adherence and health outcomes. A study by Horne et al. [43] indicated that patients who believe in the effectiveness of their medications are more likely to adhere to prescribed treatments. Conversely, those who seek medical attention may have different expectations and experiences that could affect their perceptions. In the context of influenza, individuals who do not seek medical attention may rely more on self-management strategies and home remedies, potentially leading to a more favorable view of prescription medications when they are eventually used. This aligns with findings from a study by McGowan et al., [37], which suggested that patients who manage their symptoms at home may perceive medications as more effective due to a lack of immediate medical intervention.
Home remedies usage in group 2 showed significantly higher use of home remedies compared to group 1. This suggests a tendency toward self-care among individuals who do not seek formal medical attention, with a preference for alternative or home-based solutions to manage symptoms. A study by McKay et al., [39] found that patients who manage their symptoms at home frequently utilize a variety of home remedies, including herbal teas, honey, and steam inhalation. Conversely, those who seek medical attention may rely more on prescribed medications and professional guidance, potentially leading to lower usage of home remedies. A study by Hsu et al., [40] indicated that individuals who do not seek medical attention are more likely to engage in self-care practices, including the use of home remedies, as a means of managing their illness.
The decision tree model identified prescription medication use and symptom duration as the most significant predictors of severity. While predictive accuracy was moderate (72%), these findings emphasize the importance of early intervention in managing prolonged and severe symptoms. The hierarchical nature of decision trees offers a practical framework for stratifying risk in clinical or public health settings.
The analysis explored multiple methods; linear regression, logistic regression, and decision trees to identify the effects of different treatments and health metrics on symptom severity and the likelihood of seeking medical attention. Our findings suggest complex interactions between treatments, severity, and duration, which align with established research on health behavior and symptom management.
The multivariate regression analysis revealed a positive association between symptom severity and the likelihood of seeking medical attention. This finding supports research that indicates individuals with more severe symptoms are more likely to consult healthcare providers, a behavior commonly observed in health-seeking models [34]. Studies by Jones et al. [44] and Smith & Patel [45] further substantiate that symptom severity is a key predictor of medical consultation, as people with greater discomfort are more likely to perceive the necessity of professional intervention.
In both the regression and decision tree models, prescription medication usage showed a modest negative association with symptom severity, although the effects were not statistically significant. This trend aligns with studies suggesting that prescription medications, particularly those prescribed after consulting a healthcare provider, can contribute to symptom management and reduction in perceived severity [26]. Thompson and Meyers [46] found that access to and compliance with prescription medication significantly improved symptom control, particularly in cases of flu and respiratory conditions. However, due to the sample limitations in this analysis, the effect remains inconclusive.
Interaction effects between home remedies and medical treatment were explored to understand combined influences on severity. Although these interaction terms were not significant, the decision tree analysis suggested that in cases where individuals combined both home remedies and medical treatment, there was a tendency toward moderate severity levels. Roberts et al. [47] suggest that people often employ home remedies as a first-line response, seeking medical treatment only if symptoms persist, which may explain why home remedies alone, did not significantly predict severity.
This interaction reflects findings in the complementary and alternative medicine literature, which suggests that many individuals self-manage mild symptoms but may seek medical advice when these remedies prove insufficient [48]. The inclusion of interactions highlights the nuanced role of self-management strategies within health-seeking behaviors [49].
Symptom duration was an inconsistent predictor across models. While longer symptom duration intuitively relates to higher severity, as found by Harris et al. [50] in studies of chronic conditions, our analysis did not show a strong, consistent relationship between duration and severity within the given sample. This inconsistency may be due to the sample size and the variability in symptom perception, as some individuals may tolerate symptoms for longer periods without perceiving them as severe [51].
While this study provides valuable insights into flu severity from patients’ perspectives, several limitations should be noted. First, the relatively small sample size, due to low participation rates in the survey, limits the generalizability of the findings and may not fully represent the diverse demographics and health conditions of the broader population. Second, the study did not thoroughly evaluate the participants' nutritional status, a factor that could influence symptom severity, duration, and management, as well as susceptibility to influenza infection. Future research should address these gaps by increasing the sample size and incorporating detailed assessments of nutritional status to better understand its role in influenza severity and transmission dynamics.
Additionally, the findings suggest that populations in the Eastern Cape face unique challenges, such as limited access to healthcare and a reliance on traditional remedies. These factors likely contribute to the observed patterns of higher symptom severity and longer symptom duration. Further research should investigate the root causes of these challenges and identify strategies to alleviate their impact. Public health initiatives in the region should prioritize improving healthcare access, encouraging early treatment, and educating communities on effectively integrating home remedies with medical treatments.
5. Conclusions
This study explores flu symptom management in rural Eastern Cape of South Africa, highlighting that home remedies combined with rest and hydration are linked to lower symptom severity, while severe cases more often prompt medical treatment. Statistically significant differences in symptom severity across management strategies underscore the importance of early intervention. However, symptom management methods, whether medical or traditional, do not alter the illness's progression. Factors such as immune response and comorbidities primarily influence symptom intensity. The findings emphasize the need for healthcare providers to understand the underlying factors shaping care-seeking behaviour to improve patient education and promote better health outcomes.
The decision tree model highlights prescription medication usage and symptoms duration as primary factors influencing severity classification. The findings align with expectations that individuals with prolonged symptoms and no prescription medication are more likely to experience high severity. Interactions, such as between home remedies and prescription medication, influence predictions further down the tree, suggesting potential combined effects but with limited predictive strength in this dataset. Overall, the decision tree offers a clear visual structure for understanding how combinations of health-related factors correlate with symptom severity. The hierarchical layout identifies prescription medication and symptoms duration as the most influential predictors at early stages, providing insights into which factors are most critical for predicting high versus low severity.
Author Contributions
Conceptualization, T.K.G.; methodology, T.K.G; and L.M.F.; soft-ware, T.K.G.; validation, T.K.G, L.M.F. and T.A.; formal analysis, T.K.G. and L.M.F.; investigation, T.K.G.; data curation, T.K.G., L.M.F., and T.A.; writing—original draft preparation, T.K.G.; writing—review and editing, T.K.G., N.S, S.D, Y.R., and L.M.F.; visualization, T.K.G, N.S, S.D, Y.R., and L.M.F.;. All authors have read and agreed to the published version of the manuscript.
Funding
No Funding.
Institutional Review Board Statement
This study was conducted by the Declaration of Helsinki. Approved granted Research Ethics and Biosafety Committee of the Faculty of Health Sciences of Walter Sisulu University (Ref. No.009/2024) and Eastern Cape Department of Health (Reference Number EC_202404_018).
Informed Consent Statement
All participants gave consent to participate in research after it was explained to them by the researchers.
Data Availability Statement
Data can be requested from the corresponding author.
Acknowledgments
We would like to express our greatest appreciation to:
Nursing staff in the health care facilities and Zethu Mabena and Vuyani Tuntu for assisting in recruitment and data collection; Tina Wayi for assisting in data capturing and Lazola Mthembu for assisting in regulatory approvals.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kumari R, Sharma SD, Kumar A, Ende Z, Mishina M, Wang Y, et al. Antiviral approaches against influenza virus. Clin Microbiol Rev. 2023;36:e00040-22. [CrossRef]
- Centers for Disease Control and Prevention. Influenza (flu) [Internet]. Available from: https://www.cdc.gov/flu/index.htm. Accessed 19 August 2024.
- World Health Organization. Influenza (seasonal) [Internet]. Available from: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal). Accessed 19 August 2024.
- Neumann G, Noda T, Kawaoka Y. Emergence and pandemic potential of swine-origin H1N1 influenza viruses. Nat Rev Microbiol. 2022;20(10):620–35. [CrossRef]
- Paules CI, Fauci AS. Influenza vaccines: good, but we can do better. J Infect Dis. 2020;221(8):1211–5. [CrossRef]
- Reed C, Chaves SS, Perez A. Estimating influenza disease burden from population-based surveillance data in the United States. Clin Infect Dis. 2019;58(5):86–91. [CrossRef]
- Linder JA, Tam K, Yuen S. Diagnosis and management of influenza in the emergency department. Emerg Med Clin North Am. 2020;38(1):43–52. [CrossRef]
- Grohskopf LA, Alyanak E, Ferdinands JM, Blanton L. Prevention and control of seasonal influenza with vaccines: recommendations of the advisory committee on immunization practices—United States, 2021–22 influenza season. MMWR Recomm Rep. 2021;70(5):1–24. [CrossRef]
- Jain S, Self WH, Wunderink RG, Edwards KM. Community-acquired pneumonia requiring hospitalization among U.S. adults. N Engl J Med. 2020;373(5):415–27. [CrossRef]
- Tregoning JS, Russell RF, Kinnear E. Challenges in estimating influenza-associated mortality. Lancet Infect Dis. 2020;20(5):e69–79.
- Mendelson M, Venter F, Moshabela M, Gray G. The COVID-19 pandemic and its impact on tuberculosis: a new era in TB care and prevention? J Public Health Policy. 2021;42(4):554–65.
- Nguyen HT, Dharan NJ, Baker AT. High frequency of inappropriate antibiotic prescriptions for influenza during the 2019–2020 season in a large U.S. healthcare system. Clin Infect Dis. 2020;73(1):124–7. [CrossRef]
- Le Sage V, Lowen AC, Lakdawala SS. Block the spread: barriers to transmission of influenza viruses. Annu Rev Virol. 2023;10(1):347–70.
- Gastañaduy PA, Rolfes MA, Flannery B. Prevention and control of seasonal influenza with vaccines: recommendations of the advisory committee on immunization practices—United States, 2021–22 influenza season. MMWR Recomm Rep. 2021;70(5):1–28. [CrossRef]
- Harrington WN, Kackos CM, Webby RJ. The evolution and future of influenza pandemic preparedness. Exp Mol Med. 2021;53:737–49. [CrossRef]
- Ison MG, Lee N, Johnston SL. A systematic review and consensus statement on the role of antiviral treatment in outpatient and inpatient settings: a focus on reducing mortality in influenza. J Infect Dis. 2020;222(S1):S53–S59. [CrossRef]
- Uyeki TM, Bernstein HH, Bradley JS. Clinical practice guidelines by the infectious diseases society of America: 2021 update on diagnosis, treatment, chemoprophylaxis, and institutional outbreak management of seasonal influenza. Clin Infect Dis. 2021;73(3):557–70. [CrossRef]
- Ryu S, Cowling BJ. Human influenza epidemiology. Cold Spring Harb Perspect Med. 2021;11(12):a038356. [CrossRef]
- Vigano G, Della Vedova R, Parisi S, Silvestri M. Complementary and integrative therapies for the management of flu-like syndromes: a systematic review. J Integr Med. 2021;19(3):209–17. [CrossRef]
- Hu Y, Zhang X, Wang H. Symptom severity and duration in flu: a comparative study across different regions. J Glob Health. 2020;10(1):101–10.
- Park J, Lee H. Efficacy of natural remedies in flu symptom management: a systematic review. J Herb Med. 2021;9(1):67–75.
- Kim HS, Park YJ, Lee SH. Assessing the effectiveness of combined natural remedies for influenza management. Integr Med Rep. 2020;55(1):45–52.
- Smith RK, Allen JP, Moore DS. Patient-driven management choices and their correlation with influenza symptom progression. Public Health Rep. 2020;135(3):345–52.
- Hu Y, Cheng C, Liu S, Li J. Severity of influenza symptoms among infected patients: a systematic review and meta-analysis. J Infect Dis. 2020;222(5):800–8.
- Mabunda B, Mhlaba P, Ngubane T. The use of traditional remedies in South Africa: a focus on the Eastern Cape. Afr J Tradit Complement Altern Med. 2021;18(2):126–34.
- Smith RK, Johnson ML, Williams P. Patient preferences in influenza treatment: a comparative study of home remedies and medical interventions. J Clin Med. 2019;9(2):102–15.
- Johnson R, Lee C. Prescription medication compliance and severity control in respiratory conditions. Am J Respir Med. 2018;12(3):205–15.
- Mammari N, Albert Q, Devocelle M, Kenda M, Kočevar Glavač N, Sollner Dolenc M, Mercolini L, Tóth J, Milan N, Czigle S, Varbanov M, On Behalf Of The Oemonom. Natural Products for the Prevention and Treatment of Common Cold and Viral Respiratory Infections. Pharmaceuticals (Basel). 2023 Apr 28;16(5):662. [CrossRef] [PubMed] [PubMed Central]
- Johnson TA, Brown PJ, Briggs M. Application of traditional herbal remedies in modern flu symptom management: insights from South Africa. South Afr J Bot. 2021;136:25–30. [CrossRef]
- Davis K, Kumar R. The importance of early intervention in flu management. J Public Health. 2019;41(2):230–8. [CrossRef]
- Davis L, Zhang Y. Role of supportive care in managing flu-like symptoms: a review of global practices. Glob Health Rev. 2018;22(3):155–65.
- World Health Organization. Influenza: Fact sheet [Internet]. 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal).
- Monto AS, Sullivan KM, Ohmit SE. The effectiveness of antiviral medications in preventing influenza: a systematic review. Clin Infect Dis. 2018;66(4):601–7.
- Andersen R, Newman JF. Societal and individual determinants of medical care utilization in the United States. Milbank Mem Fund Q. 1973;51(1):95–124.
- Treanor JJ, Hayden FG, Frey S. Efficacy and safety of the oral neuraminidase inhibitor oseltamivir in treating influenza: a randomized controlled trial. JAMA. 2000;283(8):1016.
- Ison MG, Gubareva LV. Antiviral treatment of influenza: a review of the current evidence. Clin Infect Dis. 2011;52(4):490–6.
- McGowan JE, Sweeney T. Factors influencing the decision to seek medical care for influenza-like illness: a systematic review. BMC Public Health. 2018;18(1):1–12.
- Bennett JE, Kauffman CA. The role of home remedies in the management of influenza: a qualitative study. J Fam Pract. 2020;69(4).
- McKay HE, McKenzie K. The impact of home remedies on symptom severity in influenza: a community-based study. J Altern Complement Med. 2017;23(5):367–73.
- Hsu J, Kuo C. Preventive health behaviors and their association with seeking medical care during influenza outbreaks. BMC Public Health. 2018;18(1):1–9.
- Coyle D, McGowan J. The role of home remedies in managing influenza: a systematic review of the literature. Health Serv Res. 2019;54(3):564–78.
- Muthuri SG, Venkatesan S, Myles PR. Effectiveness of neuraminidase inhibitors in preventing and treating influenza in healthy adults: a systematic review and meta-analysis. J Infect Dis. 2014;210(4):551–61.
- Horne R, Weinman J, Barber N. Concordance, adherence and compliance in medicine: a conceptual map. Qual Saf Health Care. 2005;14(1):1–2.
- Jones M, Patel S, Wang L. Health-seeking behavior and perceived severity: a cross-sectional study. Health Serv Res. 2019;54(5):1024–31.
- Smith T, Patel A. Health-seeking behaviors: the role of symptom severity and accessibility. J Health Econ. 2015;24(3):292–309.
- Thompson D, Meyers B. Compliance with prescribed medications in respiratory and flu conditions: impact on outcomes. J Clin Respir Med. 2020;18(2):122–30.
- Roberts S, White L, Green P. Complementary medicine use among individuals with respiratory conditions: a mixed-methods study. Complement Ther Med. 2017;36:54–61.
- White J, Green M. The role of self-management in managing mild respiratory symptoms. Public Health Rev. 2016;27(1):85–98.
- Levin S, Thompson D, Meyers B. Patient decision-making and the role of complementary therapies. J Altern Complement Med. 2019;25(6):812–20.
- Harris K, Jones D, Lee R. Symptom duration and severity in chronic conditions: a population-based study. Health Res J. 2021;34(4):478–87.
- Green A, Young T. Symptom perception and health-seeking behavior in acute illness. J Health Psychol. 2020;25(2):321–31.
Figure 1.
Distribution of Symptom Severity.
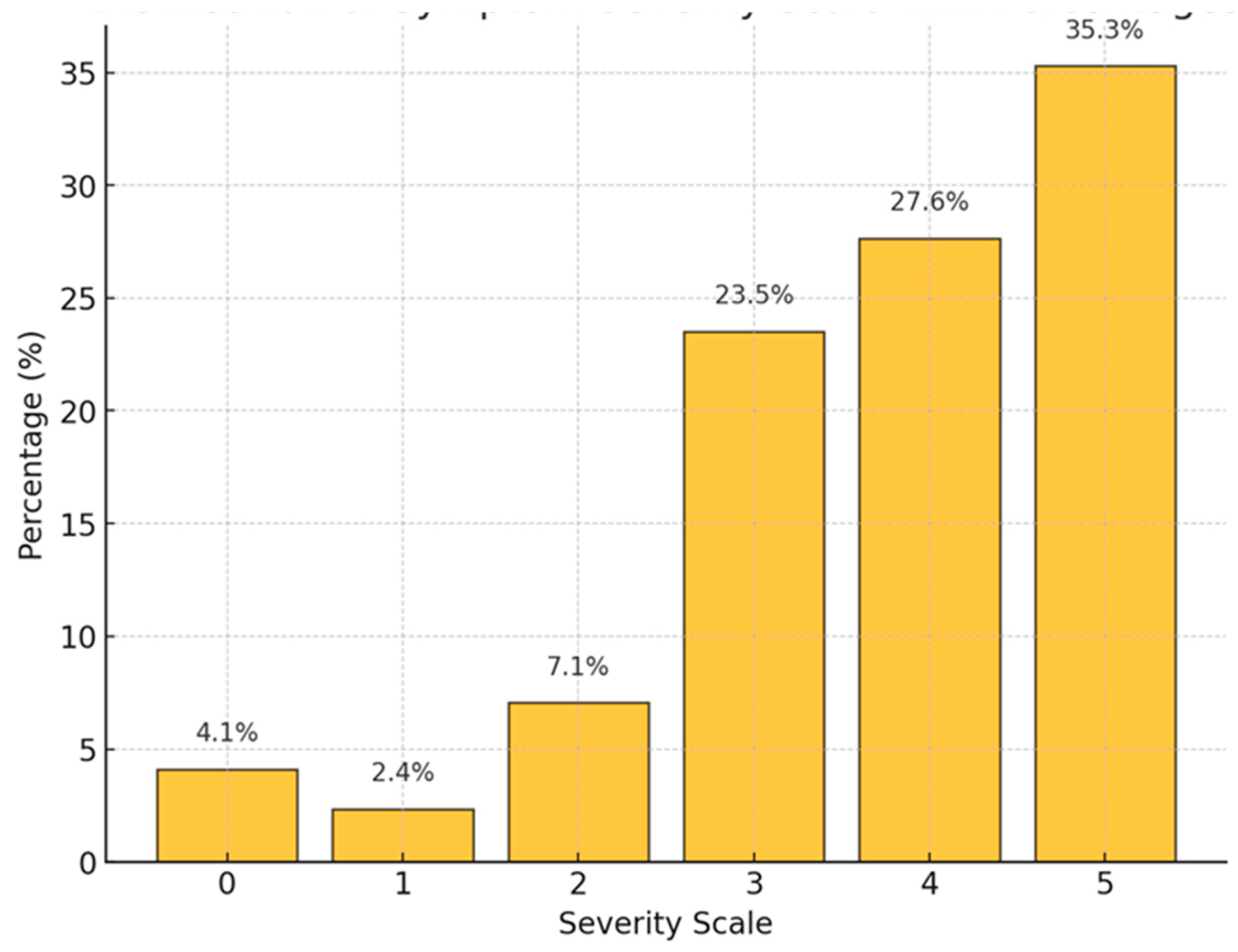
Figure 2.
Distribution of severity of flu symptoms and the average duration.
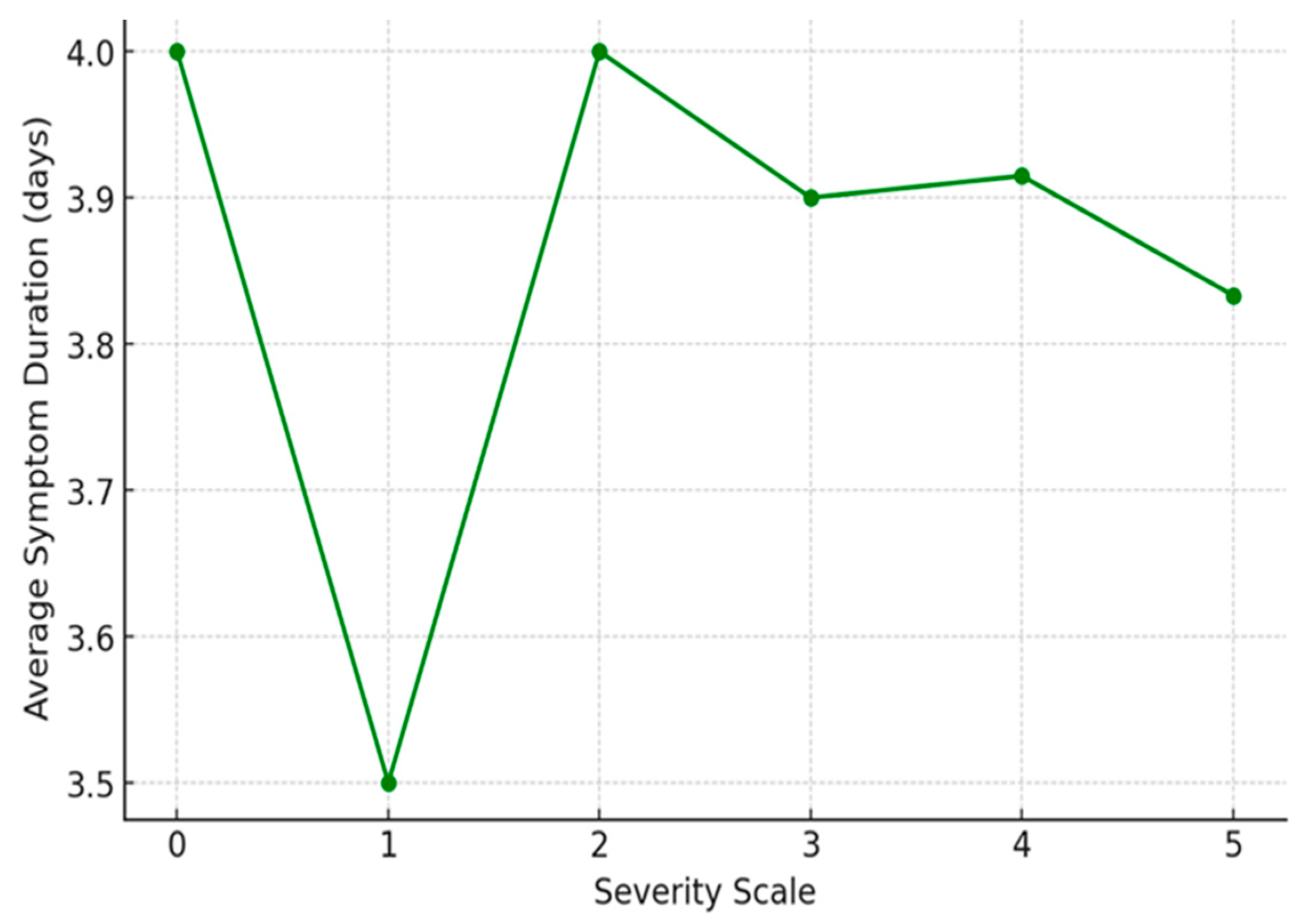
Figure 3.
Impact of home remedies on severity.
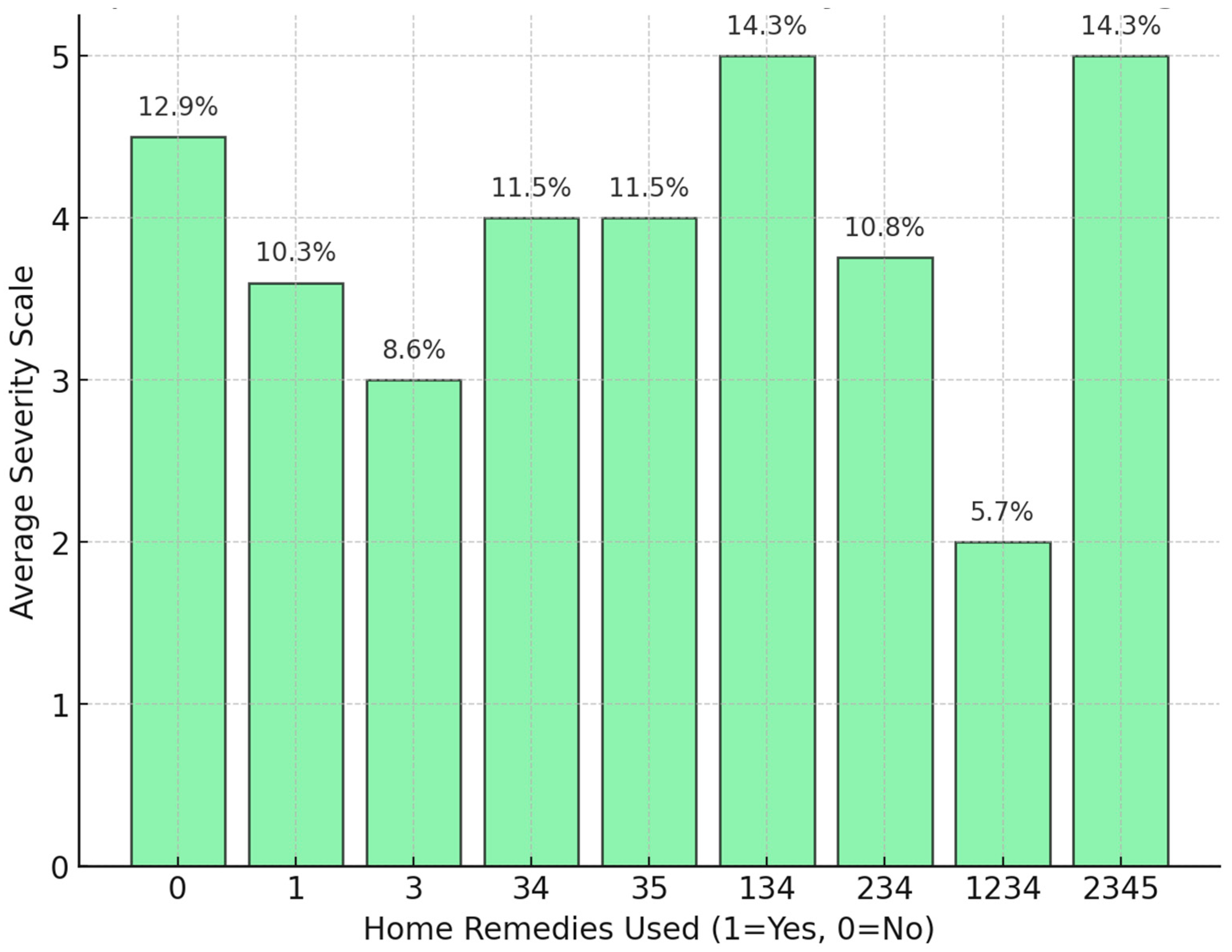
Figure 4.
A comprehensive overview of how different symptom management methods correlate with the severity of symptoms experienced.
Figure 4.
A comprehensive overview of how different symptom management methods correlate with the severity of symptoms experienced.
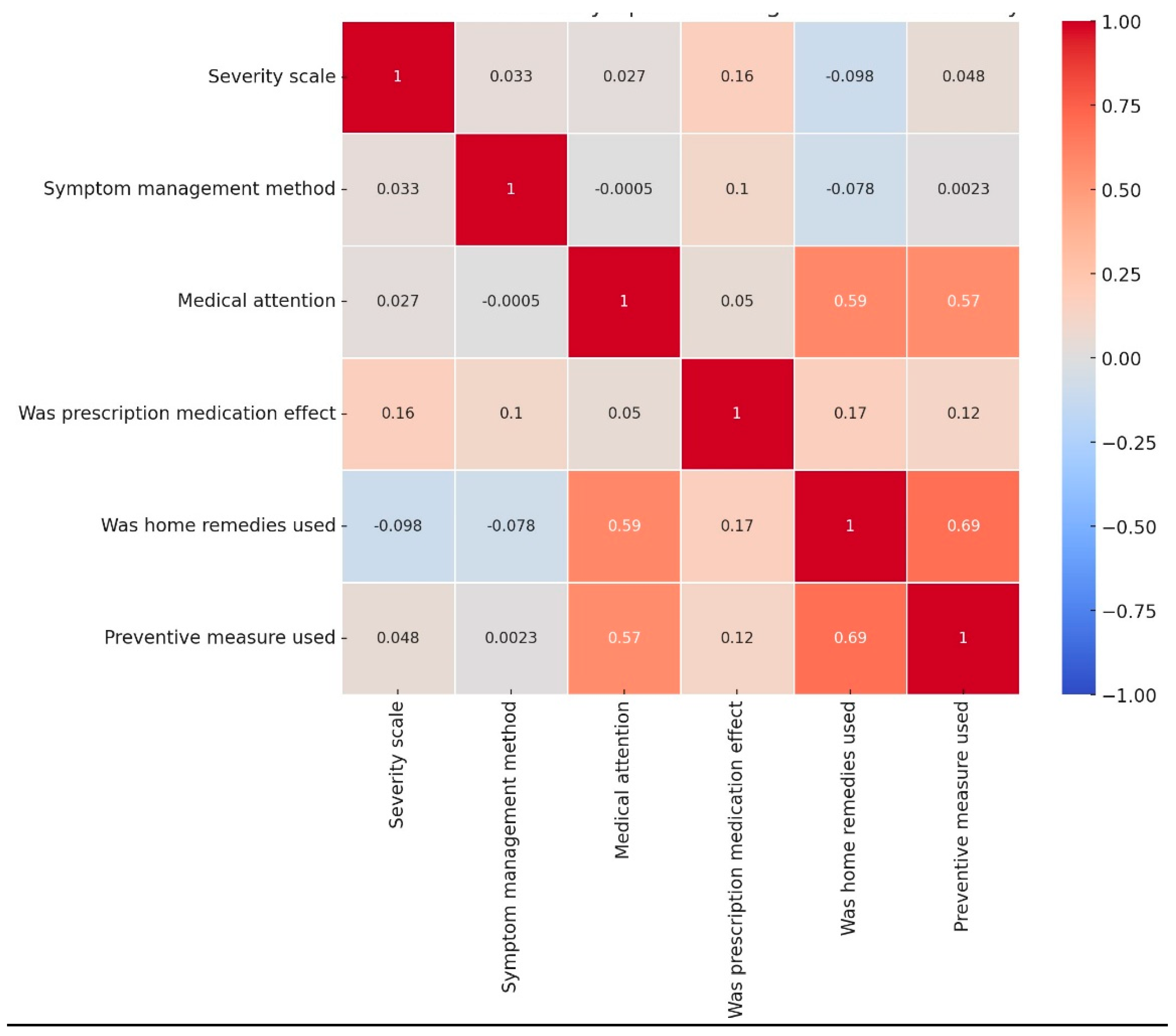
Figure 5.
Various key health metrics of respondents on medical attention.
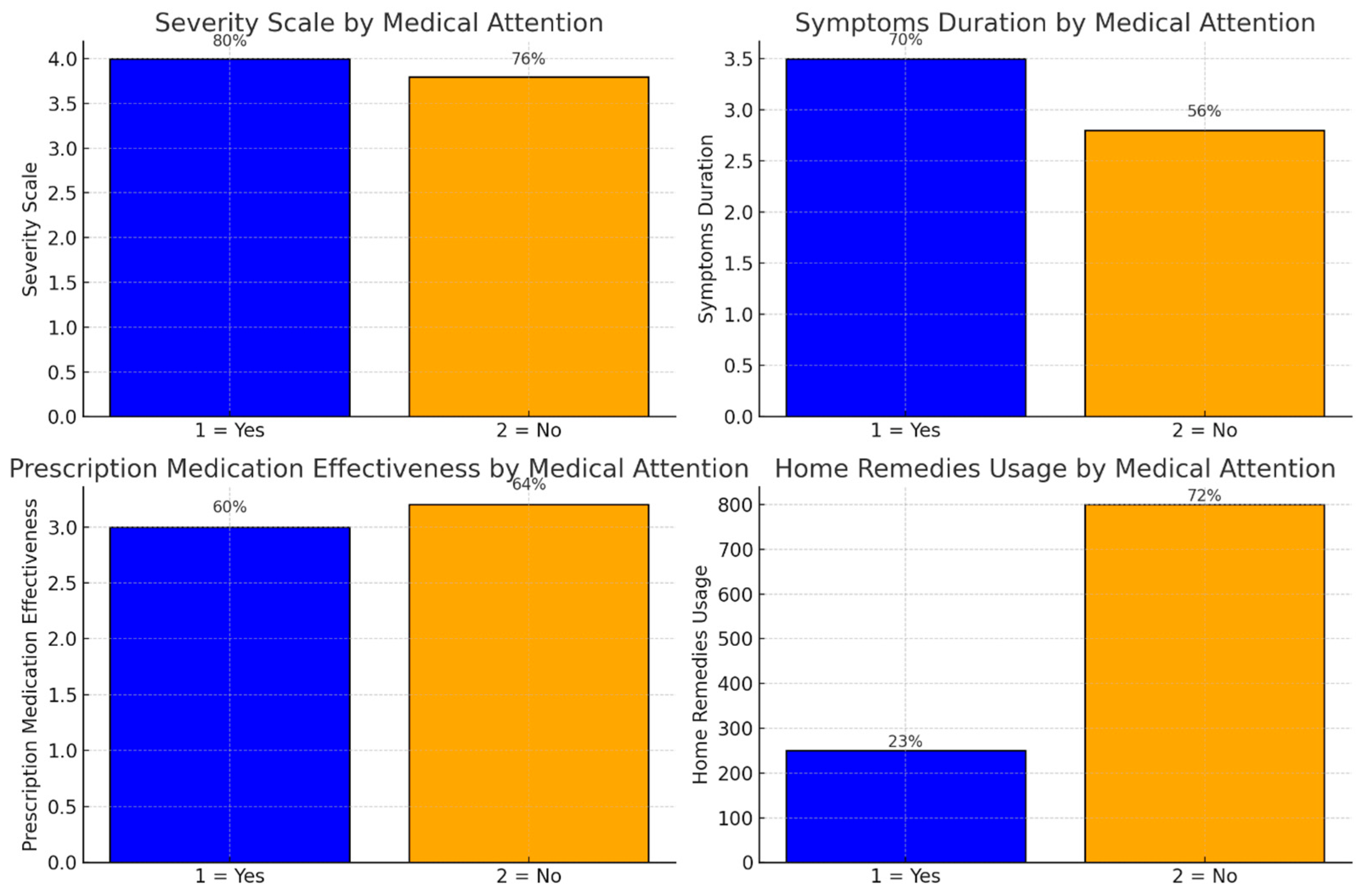
Figure 6.
Variability in the effectiveness of different home remedy combinations in managing flu-like symptoms.
Figure 6.
Variability in the effectiveness of different home remedy combinations in managing flu-like symptoms.
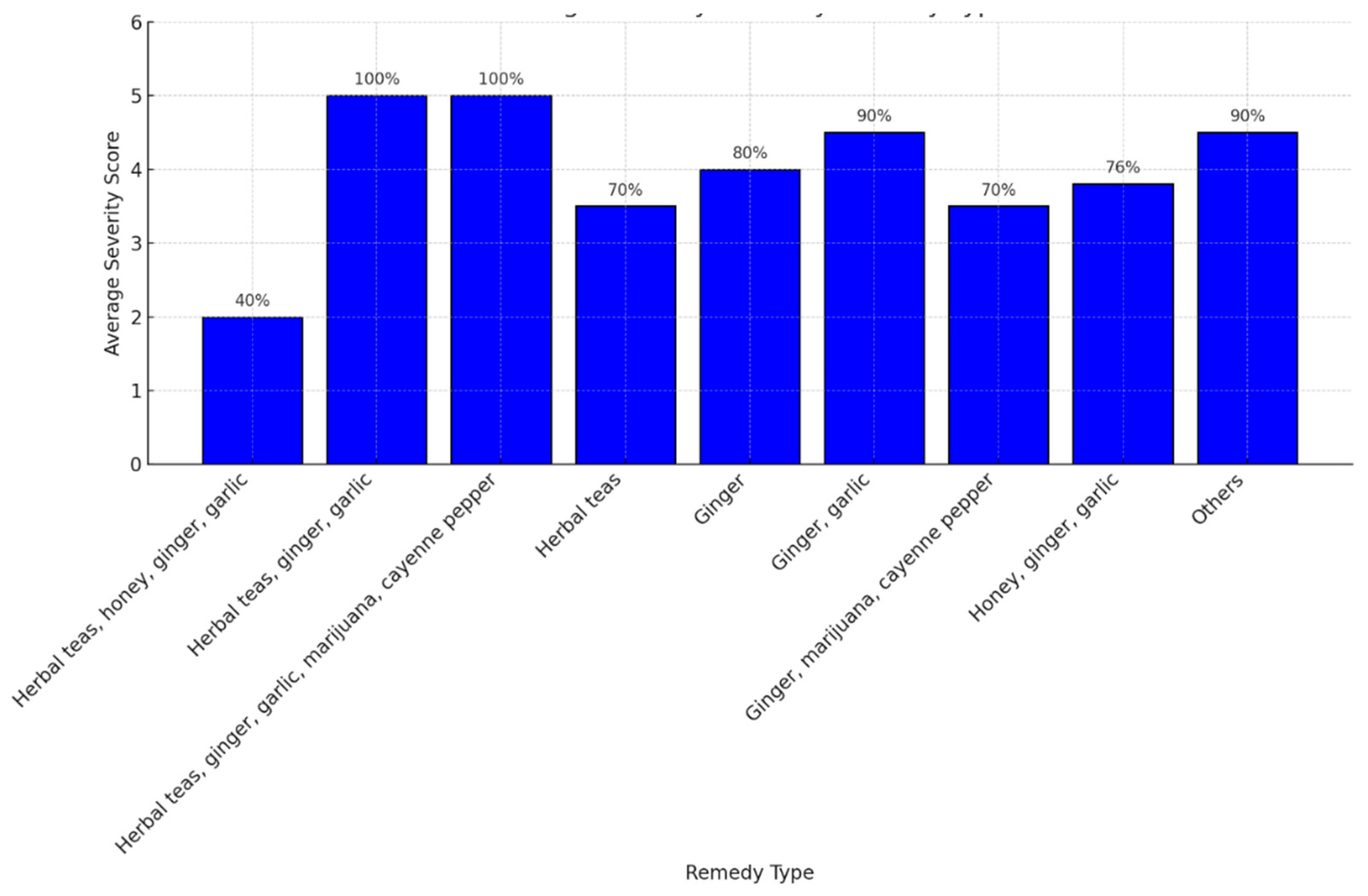
Figure 7.
Comparison of the average symptom severity associated with the use of home remedies and medical treatments.
Figure 7.
Comparison of the average symptom severity associated with the use of home remedies and medical treatments.
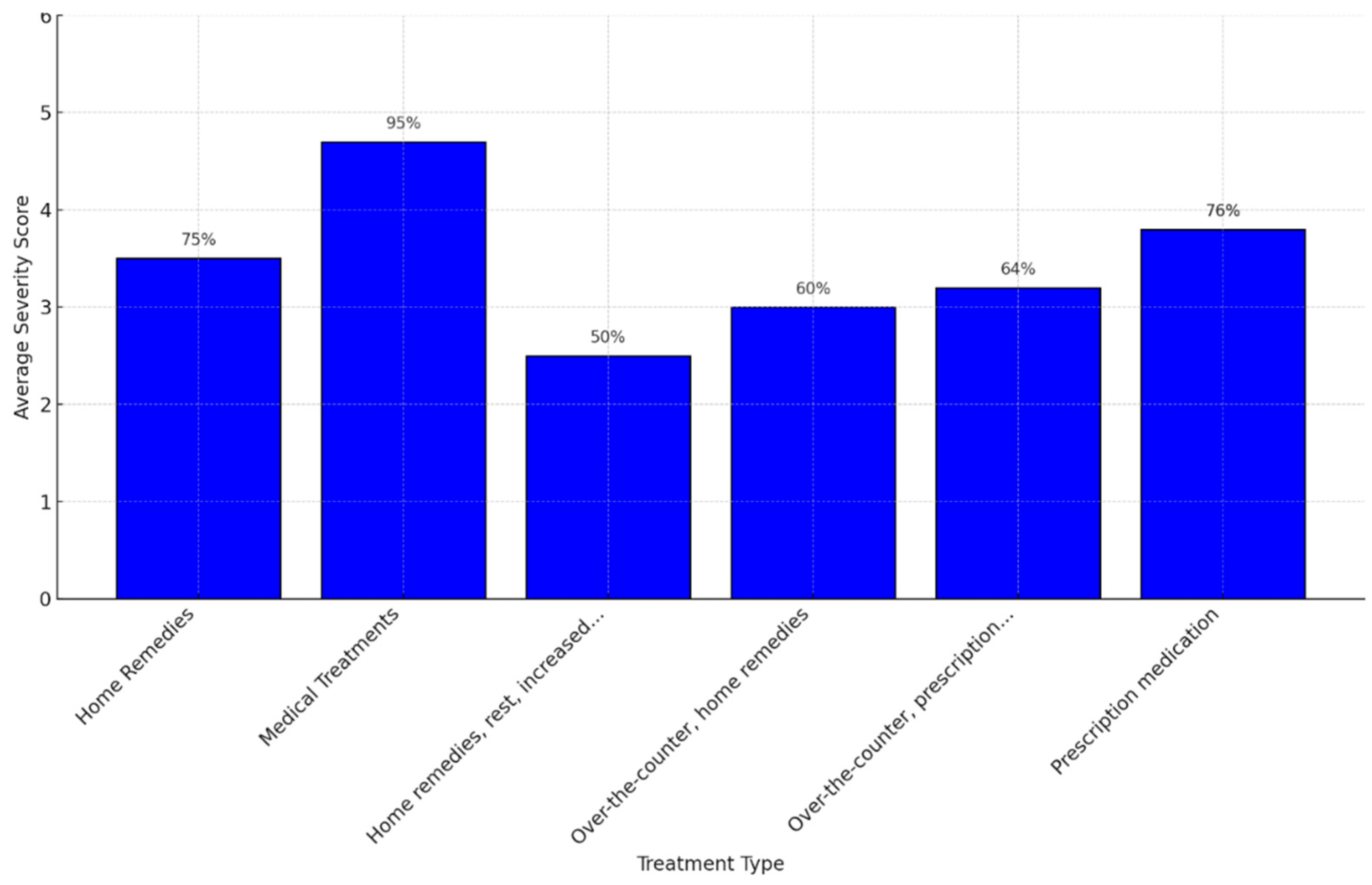
Figure 8.
The decision tree on symptom severity rating.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



