
Submitted:
24 September 2024
Posted:
25 September 2024
You are already at the latest version
Abstract
Chylothorax is a rare complication occurring after cardio-thoracic surgical procedures. This condition presents challenges about diagnosis and treatment. Operative ductal ligation is the method of choice for relapsing or refractory cases, and it can be performed through the aid of IGC injection for the identification of chylous leakage. Our report presents the use of ICG fluorescence during VATS to successfully identify and treat a left-sided post-surgical chylothorax. The patient underwent a pulmonary wedge resection for a suspect malignant lesion and developed chylous leakage in the early postoperative period. On postoperative day 7 the patient underwent a revision thoracoscopy for hemostasis and thoracic duct ligation. ICG injections have been performed through bilateral inguinal lymph nodes and approximately 15 minutes after we performed the re-thoracoscopy with effective identification and ligation of the chyle leakage. ICG fluorescence-guided VATS is a valuable and effective method for managing postoperative chylothorax, especially for left-sided leaks.
The video of the procedure can be found at: https://zenodo.org/records/13786288
Keywords:
chylothorax
; thoracic surgery
; indocyanine green fluorescence
; lymph nodes
1. Introduction
Chylothorax is a rare but insidious complication that can occur after thoracic surgery procedures with a range of incidence from 0,5% to 2% [1]. This condition is more frequently associated with esophageal surgery or mediastinal lymphadenectomies. Standard treatment includes conservative measures as first approach, such as somatostatin administration and lipid-free diet; however, persistent high-output chylothorax often necessitates more invasive approaches. Lymphangiography can be used both as a diagnostic and a therapeutic tool, as it allows to identify the leakage site and to embolize the injured lymphatic vessel. Surgical intervention is reserved for refractory or relapsing cases and its aim is to ligate the thoracic duct from the right hemithorax [2]. However, the presence of accessory lymphatic vessels and the impossibility to properly identify the leakage site may result in the failure of the procedure. Our report presents the use of ICG fluorescence during VATS to successfully identify and treat a left-sided chylothorax, emphasizing the efficacy of this technique in targeted, site-specific interventions.
2. Case Presentation and Methods
We present the case of a 54-year-old female with a pulmonary PET-positive lesion in the left upper lobe. The patient underwent triportal thoracoscopic wide wedge resection of the left upper lobe with adequate macroscopic surgical margins and hilar-mediastinal lymphadenectomy. Intraoperative frozen section analysis was negative for malignancy and did not show any atypia. The surgical procedure took off swiftly without any criticalities. On postoperative day 1, the patient developed chylous drainage from the pleural drain, with outputs up to 1000 ml daily for the next 4 days. A fat-free diet was immediately initiated and chylous output progressively diminished but did not disappear completely. On postoperative day 7, the patient suffered from an episode of tachycardia and hypotension, associated with cold diaphoresis. We noticed active bleeding from the drainage with a mean of 100 ml/h of hematic output and we decided to take the patient back to the operating room for evacuation of hemothorax and hemostasis. Concurrently, we decided to address the persistent left-sided chylous effusion.
A total of 3 mg of ICG diluted in 5 ml of saline solution was injected bilaterally into the inguinal lymph nodes by our interventional radiologist while the patient was supine and intubated. Approximately 15 minutes elapsed from the ICG injection to the reopening of the previous surgical incisions. At the exploration in the pleural cavity, we individuated two blood clots adherent to the parenchymal suture, but no active bleeding sources. Eventually, with the dedicated ICG filter in the thoracoscopic optics camera, lymphatic vessels on the left side were clearly visualized, and the leakage point was precisely identified at the level of the previous carinal lymphadenectomy. The leak was successfully sealed with metal clips (Figure 1) and with application of nebulized cyanoacrylate for further tissues sealing. The patient had no further chylous drainage and resumed oral lipid-free intake on postoperative day 1 following the second surgery. She needed oral and endovenous ionic compensation because of hyponatremia, hypokalemia, hypocalcemia, hypophosphatemia and hypomagnesemia. Thoracic drains were removed on postoperative day 5 due to the absence of air or chylous leakage and the patient was dismissed on postoperative day 6 in good overall clinical conditions.
4. Discussion
ICG fluorescence is widely used in various surgical fields for the intraoperative localization of lesions and real-time visualization of segmental anatomy, or for tumor and sentinel node identification [3]. In thoracic surgery, in particular, ICG fluorescence is used for the individuation of the anatomical intersegmental planes for sublobar resections, in order to allow the most precise separation of the pulmonary parenchyma [4]. ICG use in the management of iatrogenic chylothorax is not yet standardized in the literature. This case report highlights the effectiveness of using ICG fluorescence-guided VATS lymphatic duct ligation to manage left-sided chylothorax. The technique allowed us the precise identification and ligation of the leaking lymphatic vessels on the left side, which is crucial in preventing complications associated with prolonged chylous drainage. This case deviates from the standard of right-sided thoracic duct ligations, showcasing the advantages of targeted intervention when precise localization is feasible.
5. Conclusions
ICG fluorescence-guided VATS is a valuable and effective method for managing postoperative chylothorax, especially for left-sided leaks. This case report highlights its use as a reliable technique for visualizing and addressing lymphatic leaks during thoracic surgery.
Author Contributions
Conceptualization, L.L., M.B. and A.Bu.; methodology, A.Bo.; software, V.V. and L.L.; validation, G.C., E.F. and S.N.; formal analysis, G.C.; investigation, A.Bu.; resources, L.L. and A.Bu; data curation, A.R.; writing—original draft preparation, L.L and A.Bu.; writing—review and editing, S.N., A.R. and G.C.; visualization, E.F.; supervision, F.R.; project administration, F.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical Committee in our center does not require approval for case reports. Written informed consent was obtained from the patient for the enrollment in this study.
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to privacy.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Martucci, N.; Tracey, M.; Rocco, G. Postoperative Chylothorax. Thorac Surg Clin. 2015, 25, 523–528. [Google Scholar] [CrossRef] [PubMed]
- McGrath, E.E.; Blades, Z.; Anderson, P.B. Chylothorax: aetiology, diagnosis and therapeutic options. Respir Med. 2010, 104, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Morales-Conde, S.; Licardie, E.; Alarcón, I.; Balla, A. Indocyanine green (ICG) fluorescence guide for the use and indications in general surgery: recommendations based on the descriptive review of the literature and the analysis of experience. Cir Esp (Engl Ed). 2022, 100, 534–554. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.S.; Ong, B.H.; Chao, Y.K.; Wright, G.M.; Sekine, Y.; Wong, I.; Hao, Z.; Zhang, G.; Chaturvedi, H.; Thammineedi, S.R.; Law, S.; Kim, H.K. Use of Indocyanine Green Fluorescence Imaging in Thoracic and Esophageal Surgery. Ann Thorac Surg. 2023, 115, 1068–1076. [Google Scholar] [CrossRef] [PubMed]
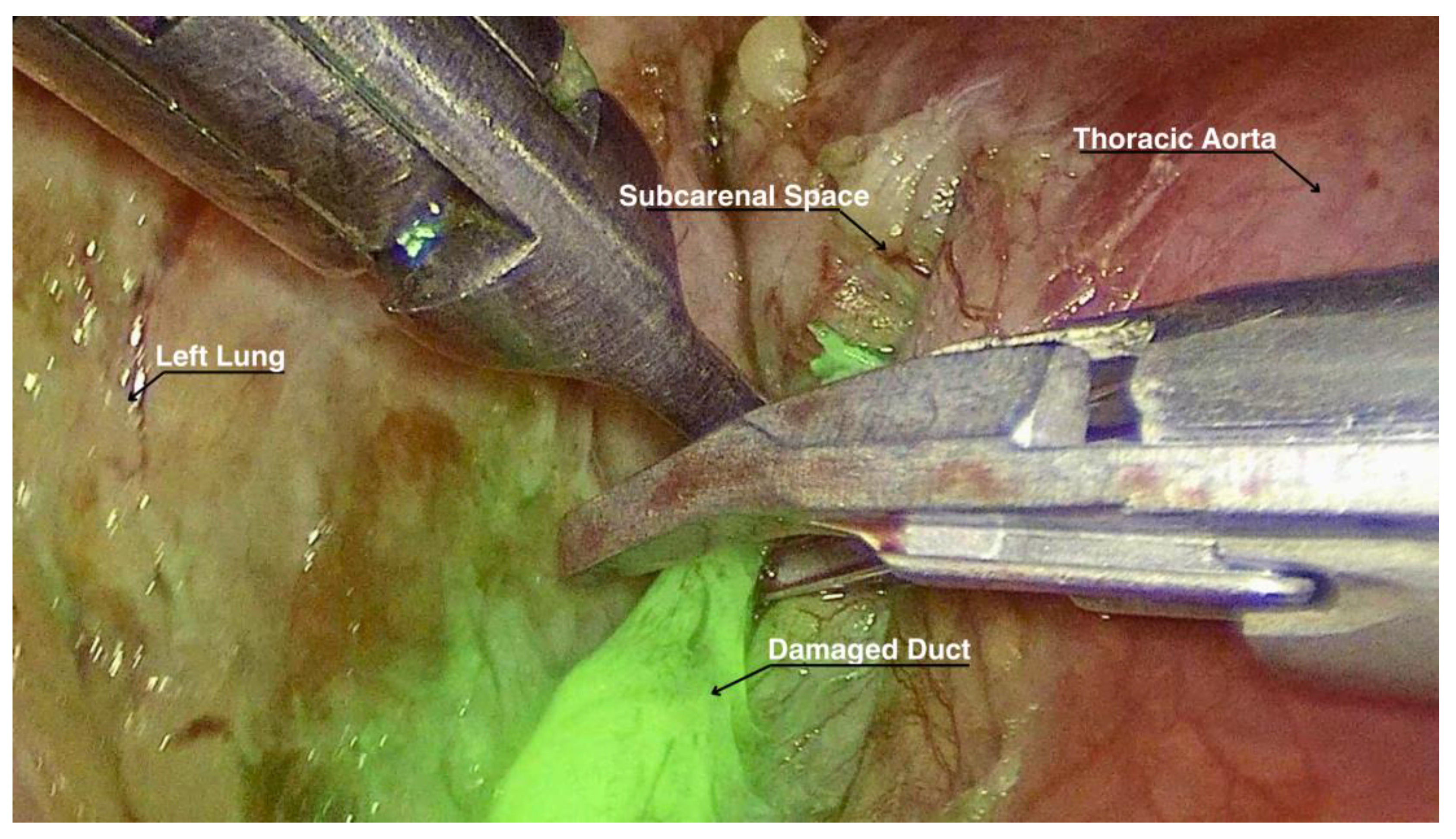
Figure 1.
Lymphatic duct highlightened by ICG while being ligated.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



