Submitted:
18 September 2024
Posted:
18 September 2024
You are already at the latest version
Abstract
Cirrhosis is a critical global health issue, responsible for 2.4% of deaths worldwide in 2019. The Global Burden of Disease Study reported a near doubling of decompensated cirrhosis cases from 1990 to 2017. In the U.S., cirrhosis is the 12th leading cause of death and often requires hospitali-zation and procedural interventions for severe complications such as hepatocellular carcinoma, ascites, hepatic encephalopathy, and variceal bleeding. This study aims to identify racial, ethnic, and socioeconomic disparities in receiving critical interventions among U.S. patients with de-compensated cirrhosis during 2020-2021. We conducted a retrospective cross-sectional analysis using 2020-2021 National Inpatient Sample data of adult patients (≥18 years) with cirrhosis-related and cirrhosis complication-related ICD-10 codes and who underwent procedures for cirrhosis-related indications such as esophagogastroduodenoscopy (EGD) for variceal hemor-rhage, transjugular intrahepatic portosystemic shunt (TIPS) for variceal hemorrhage or refractory ascites, hemodialysis for acute kidney failure or hepatorenal syndrome, and liver transplantation We collected data on patient baseline clinicodemographic and procedural outcomes. Statistical analyses included multivariable logistic regression to assess for associations with outcomes. There were significant disparities in procedure utilization: White and Hispanic patients more likely than Black patients to receive EGD and TIPS, while Black and Hispanic patients had higher odds of receiving hemodialysis. Insurance type also influenced access, with Private/HMO insurance holders having higher odds of undergoing procedures. These findings underscore the need for targeted interventions to address healthcare inequities.
Keywords:
Decompensated Cirrhosis
; Portal Hypertension
; Health Disparities
; Hepatology
; TIPS
; EGD
; Liver transplantation
1. Introduction
As a leading cause of death worldwide, cirrhosis was associated with 2.4% of global deaths in 2019. It can lead to severe complications such as hepatocellular carcinoma (HCC), ascites, hepatic encephalopathy, and variceal bleeding. The Global Burden of Disease (GBD) Study 2017 shows that the global number of decompensated cirrhosis cases nearly doubled from 1990 to 2017, reaching 10.6 million cases. These complications contribute to cirrhosis being the 12th leading cause of death in the United States. [1,2,3]
Hospitalization for critical interventions is often required for complications associated with cirrhosis. Previous research by Nephew et al. (2023) highlighted racial and ethnic disparities in receipt of complex lifesaving procedures from 2009 to 2018. [3] However, in general, there is a paucity of data on socioeconomic disparities in such interventions for patients with decompensated cirrhosis. It is essential to comprehend these disparities to effectively target public health and equity interventions.
To address these highlighted deficiencies in the field, we aimed to identify the latest trends in racial and ethnic disparities and establish the association of socioeconomic status in the receipt of targeted critical interventions among patients with decompensated cirrhosis in the U.S.
2. Materials and Methods
A retrospective cross-sectional analysis was conducted using 2020 and 2021 National Inpatient Sample (NIS) data. The inclusion criteria included adult patients (aged 18 years or older) and who had at least one ICD-10 code associated with cirrhosis and one code associated with complication (Table A1). Data were collected for several demographic variables, including age, gender, race, ethnicity, insurance status, and comorbid conditions. Variables showing significant relationships were included as covariates in the logistic regression models. Outcomes of interest included receiving hemodialysis for hepatorenal syndrome (HRS) or acute kidney injury (AKI), transjugular intrahepatic portosystemic shunt (TIPS) for ascites or variceal hemorrhage (VH), esophagogastroduodenoscopy (EGD) for VH, and liver transplantation (LT) for overall decompensated cirrhosis.
Chi-square tests were performed on summary statistics for categorical variables to assess distributional differences between racial groups; two-sided P values were considered significant at <0.05. Univariate logistic regression was employed in the study to determine correlations between categorical variables and results. To provide a consistent metric for comparing procedure rates across demographic groups, annual standardized procedure rates (ASPR) per 1000 admissions were calculated.
The strength of the relationships between categorical variables was determined using measures of association such as Cramer's V, and the overall statistical significance of these relationships was evaluated using chi-square tests. Each analysis focused on a specific group of cirrhosis patients based on their complications, while excluding other cases that could interfere with the results. In the analysis of TIPS for patients with VH, cases involving ascites were left out. Similarly, in the analysis of ascites, cases with VH were excluded. Additionally, patients with heart failure were removed from the TIPS analysis because heart failure is a unique contraindication for the TIPS procedure (Figure A1). In addition, Chi-square tests showed that payment method and race had a significant relationship (P < 0.05), but Cramer's V indicated that this relationship was weak (value of 0.09). Given this, in all logistic regression models, payment method and race were included as covariates. This means we adjusted the models to account for the effects of these factors. By doing so, we aimed to better understand the connection between health outcomes, payment methods, and race, without the results being skewed by differences in the distribution of these factors.
3. Results
3.1. Patient Characteristics
Out of the 320,984 hospitalized patients with cirrhosis, 206,394 (64.43%) had decompensated cirrhosis. The median age of decompensated cirrhosis patients was 61 years (IQR: 52-69), with a range of 19 to 90 years. The median number of diagnoses was 20 (IQR: 16-25), with a range of 1 to 40. The median number of procedures was 2 (IQR: 1-3), with a range of 0 to 25. The median length of stay was 5 days (IQR: 3-9), with a range of 0 to 354 days. The total charges had a mean of $95,748.59, with a range of $113 to $9,615,387 and a median of $53,837 (IQR: $30,029-$103,153.75).
In terms of demographics, 66.4% of patients identified as White, 16.8% as Hispanic, 10.0% as Black, and 6.8% as belonging to Pacific Islander, Asian, and Native American, collectively labeled as other ethnic groups in this study. The age distribution is as follows: 47.8% of the participants were between the ages of 60 and 79; 38.0% were between the ages of 40 and 59; 7.1% were between the ages of 19 and 40; and 7.1% were over the age of 80. In terms of gender, 50.5% of the population was identified as male, while 39.5% was identified as female. Medicare was utilized by 45.7% of patients, Medicaid by 25.6%, private or HMO insurance by 19.8%, and other payment methods by 9.0%. Non-elective hospitalizations accounted for 95.6% of decompensated cases (Figure A1).
For White individuals, Medicare utilization is almost twice as high as Medicaid utilization. In contrast, Hispanic and Black individuals show a balanced reliance on both Medicare and Medicaid. Other ethnic groups also show a balanced reliance on both Medicare and Medicaid. Regarding Private or HMO insurance, White individuals show lower utilization compared to Medicare. However, all other ethnic groups rely on Medicare at least twice as much as they do on Private or HMO insurance (Figure A2).
Figure 1 illustrates the proportion and organization of cirrhosis complications based on race. In our sample, we found the distribution of complications seems consistent across ethnicities. However, numerically, the Other ethnic groups show the highest rate of HCC at 6.7%. Black individuals have a lower rate of variceal hemorrhage (VH) at 3.7% compared to White individuals at 5.5%. They also have a higher rate of hepatic encephalopathy (HE) at 13.9% compared to Hispanics at 11.9%, but slightly lower than the Other ethnic group at 12.4%. These findings are consistent with prior research that has shown racial disparities in the complications of cirrhosis. Hispanic patients have a higher incidence of HCC, while Black patients are more susceptible to HE [4]. VH is less common among White patients [5].
3.2. Racial and Ethnic
3.2.1. Racial and Ethnic: EGD for VH
White, Hispanic, and other ethnic groups have significantly higher odds of undergoing EGD for variceal hemorrhage (VH) compared to Black individuals. The odds ratios (OR) are 1.279 for Hispanic (95% CI, 1.179-1.387), 1.275 for White (95% CI, 1.183-1.374), and 1.403 for other ethnic groups belonging to Pacific Islander, Asian, and Native America (95% CI, 1.272-1.549), all with p-values less than 0.001. Additionally, other ethnic groups have higher odds compared to Hispanic individuals (OR 1.097; 95% CI, 1.013-1.189; p=.023) (Figure 2). There was no significant difference between Hispanic and White individuals for receiving EGD for VH (Table A2).
3.2.3. Racial and Ethnic: TIPS for VH and Ascites
For VH, White individuals had the highest odds of receiving TIPS compared to Hispanic (OR, 1.236; 95% CI, 1.138-1.342, P<.001) or Black individuals (OR, 1.199, 95% CI, 1.042-1.379, P=.011). Individuals from other ethnic groups had higher odds of receiving TIPS for VH compared to Hispanic (OR, 1.237; 95% CI, 1.086-1.409, P=.001) and Black individuals (OR, 1.403; 95% CI, 1.271-1.549, P<.001) (Figure 3A). There was no significant difference between Black and Hispanic individuals (Table A3).
For ascites, White individuals had the highest odds of receiving TIPS compared to Black (OR, 1.776; 95% CI, 1.579-1.997, P<.001), Hispanic (OR, 1.160; 95% CI, 1.085-1.239, P<.001), and individuals from other ethnic groups (OR, 1.148; 95% CI, 1.040-1.266, P=.006). Hispanic individuals had significantly higher odds of receiving TIPS for ascites compared to Black individuals (OR, 1.531; 95% CI, 1.347-1.741, P<.001). (Figure 3B). There was no significant difference between individuals from other ethnic groups and Hispanic individuals in receiving TIPS for ascites (Table A3).
3.2.4. Racial and Ethnic: Hemodialysis/Continuous Renal Replacement Therapy (CRRT) for HRS or AKI
Individuals from other racial or ethnic groups had higher odds of receiving HD/CRRT for HRS or AKI compared to White individuals (OR, 1.304; 95% CI, 1.256-1.354, P<.001), Black (OR, 1.051; 95% CI, 1.007-1.096, P=.022) and Hispanic individuals (OR, 1.096; 95% CI, 1.046-1.146, P<.001) (Figure 4). Hispanic individuals had higher odds compared to White individuals (OR, 1.241; 95% CI, 1.208-1.275), followed by Black individuals compared to White individuals (OR, 1.191; 95% CI, 1.154-1.229), both with p-values less than 0.001. White individuals generally had lower odds of receiving Hemodialysis for HRS or AKI than Hispanic, Black, and Individuals from other ethnic or racial groups. (Table A4).
3.2.5. Racial and Ethnic: LT
Differences in the likelihood of receiving liver transplants for decompensated cirrhosis and HCC were observed among various racial groups, all with p-values less than 0.001. Individuals from other ethnic groups had the highest odds of receiving a liver transplantation compared to Black (OR: 1.981, 95% CI: 1.795-2.187), Hispanic (OR, 1.208; 95% CI, 1.117-1.307), and White individuals (OR, 1.183; 95% CI, 1.105-1.267) (Figure 5). White individuals had higher odds of receiving a liver transplantation compared to Black individuals (OR, 1.674; 95% CI, 1.548-1.811), while there was no significant difference between White and Hispanic individuals. Hispanic individuals had higher odds compared to Black individuals (OR, 1.640; 95% CI, 1.502-1.790). White and Hispanic individuals generally had higher odds compared to Black individuals, with individuals from other ethnic groups having the highest odds overall (Table A5).
3.3. Socieconomic
3.3.1. Socieconomic: EGD for VH
Patients with Private or HMO insurance had higher odds of receiving EGD for VH compared to Medicare recipients (OR, 1.196; 95% CI, 1.135-1.260; P<.001), Medicaid recipients (OR, 1.072; 95% CI, 1.016-1.131, P= .011), and other payment methods (OR, 1.087; 95% CI, 1.017-1.161, P=.015). Medicaid recipients had higher odds of receiving EGD compared to Medicare recipients (OR, 1.116; 95% CI, 1.063-1.171, P<.001) (Figure 6). Overall, patients with Private or HMO insurance had the highest odds of receiving EGD, followed by Medicaid recipients, and those with other payment methods (Table A6).
3.3.3. Socieconomic: TIPS for VH and Ascites
For VH, Private or HMO insurance holders had higher odds of receiving TIPS compared to those with Medicare and other payment methods. Private or HMO had an OR of 1.388 compared to Medicare recipients (95% CI, 1.273-1.514) and an OR of 1.557 compared to other payment methods (95% CI, 1.385-1.750). Medicaid recipients had higher odds compared to Medicare recipients (OR, 1.316, 95% CI: 1.212-1.429) and compared to other payment methods (OR, 1.476, 95% CI: 1.317-1.654), all with p-values less than 0.001 (Figure 7A). There was no significant difference between Private or HMO and Medicaid recipients and between individuals with other payment methods and Medicare recipients (Table A7).
For ascites, individuals with Private or HMO insurance had higher odds of receiving TIPS compared to Medicare (OR, 1.214; 95% CI, 1.142-1.292), Medicaid (OR: 1.220; 95% CI, 1.145-1.300), and other payment methods (OR, 1.649; 95% CI, 1.493-1.820), all with p-values less than 0.001. Both Medicare and Medicaid recipients had higher odds compared to other payment methods (Figure 7B). There was no significant difference between Medicare and Medicaid recipients (Table A7).
3.3.4. Socieconomic: Hemodialysis/CRRT for HRS or AKI
Individuals with Private or HMO insurance had significantly higher odds compared to both Medicare (OR, 1.544; 95% CI, 1.505-1.584) and Medicaid recipients (OR, 1.052; 95% CI, 1.022-1.082). They also had higher odds compared to other payment methods (OR, 1.505; 95% CI, 1.439-1.572). Medicaid recipients had higher odds of receiving hemodialysis compared to Medicare (OR, 1.468; 95% CI: 1.432-1.505) and other payment methods (OR, 1.430; 95% CI, 1.369-1.494). All with p-values less than 0.001 (Figure 8). There was no significant difference between other payments and Medicare recipients (Table A8).
3.3.5. Socieconomic: LT for overall decompensated cirrhosis
Patients with Private or HMO insurance had higher odds of receiving a liver transplantation compared to Medicare, all with p-values less than 0.001, (OR, 4.021; 95% CI, 3.848-4.201), Medicaid recipients (OR, 3.859; 95% CI, 3.660-4.068), and other payment methods (OR, 4.305; 95% CI, 3.954-4.688) (Figure 9). There was no significant difference between Medicare and Medicaid and between Medicare and other payment methods. Private or HMO insurance holders generally had the highest odds, followed by Medicaid recipients, with Medicare recipients and other payment methods having the lowest odds (Table A9).
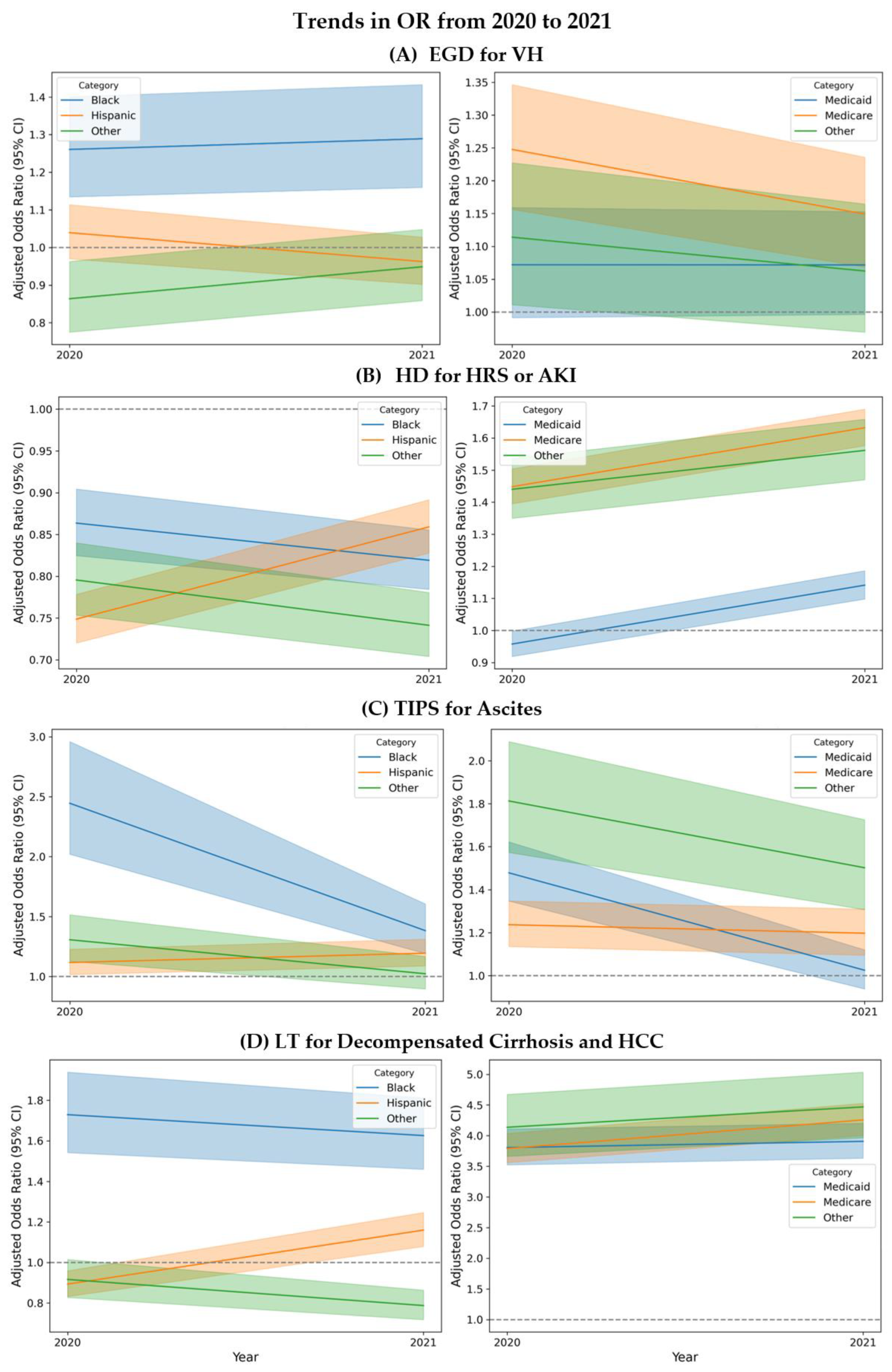
3.4. Trends in Disparities
To analyze trends in disparities between 2020 and 2021, complication procedures were divided by year and ranked by the ASPR, as shown in Figure 10. The trends indicate that, for most procedures, White individuals had an increasing OR compared to Hispanic individuals, suggesting a widening disparity. Conversely, the OR for White individuals decreased when compared to Black individuals, except for the case of EGD for variceal bleeding, where no decrease was observed.
Regarding payment methods, the analysis revealed that in 8 out of 12 comparisons, individuals with Private or HMO insurance saw an increase in OR, meaning these payment methods were associated with higher odds of undergoing these procedures.
A notable finding is that disparities tend to widen as procedures become less common or more complex. This suggests a negative correlation between OR and ASPR: as the ASPR decreases, indicating rarer or more intricate procedures, the odds ratios tend to increase, highlighting growing disparities.
4. Discussion
The use of critical medical procedures varied significantly in 2020-2021 among various demographic and socioeconomic groups, according to this thorough and nationwide study of hospitalized patients with decompensated cirrhosis. These results highlight the ongoing disparities that disproportionately impact healthcare outcomes and access of specific racial, ethnic, and socioeconomic groups.
The complexity of managing cirrhosis in different racial groups is highlighted by the interplay of complications. Minority populations frequently face challenges in obtaining timely and high-quality healthcare, resulting in deteriorated health outcomes and an elevated risk of severe complications [3]. Socioeconomic factors and healthcare accessibility have a substantial impact on the management and outcomes of cirrhosis. According to research, there is a greater occurrence of complications like ascites and HE among Black and Hispanic patients. Additionally, these patients are less likely to receive liver transplants promptly. [4,5].
Guidelines advise timely upper endoscopic evaluation to identify the source of bleeding and provide therapy (within 12 hours of acute VH presentation). [6] According to our findings, other ethnic minorities (Asian or Pacific Islanders and Native Americans), Hispanic, and White patients were more likely than Black individuals to undergo EGD for variceal hemorrhage. This contrasts with earlier research that found no statistically significant differences in the likelihood of obtaining an upper endoscopy for VH across all racial and ethnic groupings [3]. This implies that Black patients may face new barriers that prevent them from receiving this necessary treatment, which is important in managing variceal bleeding.
TIPS should be taken into consideration for patients who have uncontrolled acute VH (salvage TIPS) or who rebleed despite endoscopic variceal ligation (EVL) and vasoactive therapy ("rescue" TIPS). [6] According to our study findings, White patients were more likely than Black and Hispanic patients to receive TIPS for VH, which suggests that the White community has better access to or referral pathways for this procedure. Additionally, White patients were more likely than Black or Hispanic patients to receive TIPS for ascites. Even after controlling for comorbidities and ruling out heart failure and nonesophageal variceal bleeding as potential confounding factors, Hispanic patients continued to have higher odds of receiving a TIPS than did Black patients. These findings highlight a consistent pattern of lower access for Black individuals.
Patients with active bleeding during endoscopy who have a Child-Turcotte-Pugh (CTP) score of class B score >7 and a CTP class C score of 10–13 should have TIPS within 24–72 hours of their first endoscopy, according to AASLD practice guidelines [6]. Ascites and hepatic encephalopathy are examples of CTP parameters that we were able to control for; however, laboratory parameters that affect disease severity and TIPS indication were not included, such as albumin, bilirubin, and prothrombin time. Consequently, it should be taken into consideration for future research to fully account for CTP scores.
Black patients had greater odds than White patients when it came to hemodialysis/CRRT for HRS and AKI. Due to a higher prevalence of underlying chronic kidney disease and other comorbidities in this population, there appears to be a greater burden of severe renal complications among Black patients with cirrhosis [7]. The increased use of hemodialysis and CRRT, however, may also be the result of a lack of access to other cutting-edge treatments, which makes the patient dependent on this readily obtained therapy.
Black patients had a lower likelihood of receiving liver transplantation (LT), a life-saving procedure, than White and Hispanic patients. These disparities could be caused by various elements including referral trends, socioeconomic status, cultural beliefs, and/or biases in the transplant assessment procedure.
Access to these key interventions was further impacted by the type of insurance. Compared to people on Medicare or Medicaid, those with private or HMO insurance were more likely to have procedures done. For instance, the odds of receiving TIPS for VH and liver transplantation were substantially higher for individuals with private/HMO insurance than for those with Medicaid and Medicare. This highlights the critical role of insurance coverage in determining access to advanced medical procedures, as seen in procedures with lower ASPR presenting with higher OR values. This might be due to the higher cost of such procedures. For example, with procedures less common like LT, the magnitude of the disparities becomes broader.
When considering both race and payment method, the Medicare enrollment distribution for Black and White individuals is comparable (46.1% for Black individuals and 48.4% for White individuals). Medicare is less likely than Medicaid and Private/HMO to be associated with procedures in 4 out of 5 procedure-complication analyses. However, Black individuals have a lower ASPR than White individuals in every analysis, except for HD/CRRT for AKI.
Further studies should investigate these aspects to better understand and address the barriers faced by underrepresented groups. By standardizing best practices and guaranteeing that all patients, regardless of their background, receive timely and appropriate interventions, programs like the Cirrhosis Quality Collaborative (CQC) may also be a major factor in improving equity in cirrhosis care. Benchmarking and exchanging best practices can be facilitated by putting quality improvement programs like the CQC into action. In addition, legislative changes can contribute to developing inclusive plans, promoting policy changes and improving insurance coverage to guarantee that every patient has fair access to life-saving treatments.
Education and research play a fundamental role in creating strategies that work and guarantee fair access to healthcare for all patients with decompensated cirrhosis. It is essential to improve referral and treatment pathways by educating providers and implementing standardized protocols. Encouraging patient education via support groups and health literacy initiatives can give patients more agency. To sum up, securing funding and encouraging teamwork for interdisciplinary research on healthcare disparities.
The study period from 2020 to 2021 coincided with the COVID-19 pandemic, which likely impacted healthcare delivery and access. This context is important, as the pandemic may have either exacerbated existing disparities or created new ones due to changes in healthcare availability, prioritization of limited resources, and patient willingness to undergo procedures However, one would expect that many of the typical barriers to healthcare access (such as transportation and communication) should be smaller when studying an inpatient population.
Our study has several limitations that must be acknowledged. Firstly, as a retrospective analysis using the National Inpatient Sample (NIS) data, it is subject to the inherent limitations of administrative data, including potential coding errors and misclassification. Additionally, the NIS lacks detailed clinical information, such as the severity of liver disease or specific indications for procedures, which may influence treatment decisions and outcomes. The absence of outpatient data also restricts our understanding of the continuum of care for cirrhosis patients. Furthermore, while we adjusted for various demographic and clinical factors, residual confounding by unmeasured variables such as socioeconomic status, patient preferences, and provider biases may still exist. Finally, the generalizability of our results may be limited by variations in healthcare practices and policies across different regions and institutions. These limitations highlight the need for further research using comprehensive and longitudinal data to better understand and address healthcare disparities in patients with decompensated cirrhosis.
5. Conclusions
In conclusion, this study highlights significant disparities in the utilization of critical medical procedures among patients with decompensated cirrhosis. The findings call for urgent public health and policy interventions to address these inequities and ensure that all patients have equitable access to lifesaving procedures. By addressing these disparities, we can move towards a more equitable healthcare system that provides high-quality care for all individuals with cirrhosis.
Author Contributions
M.M.S. drafted the manuscript, collected the data, and is the article guarantor. K.A.S. and A.A. were responsible for the review of the literature. C.A.S.; software, performed the statistical analysis and drafted the methodology. T.G.C. and M.J.M. were responsible for the study conception, editing, critical review, and supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
Ethical review and approval were waived for this study due to publicly available database study.
Data Availability Statement
Data are contained within the article.
Acknowledgments
None.
Conflicts of Interest
Dr. Cotter is supported by the Clinical, Translational and Outcomes Research Awards in Liver Diseases (CTORA) award from the American Association for the Study of Liver Diseases (AASLD) and by the National Institute On Alcohol Abuse And Alcoholism of the National Institutes of Health (NIAAA) under Award Number K23AA031310. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Appendix A
Figure A1.
Study participation flow diagram.
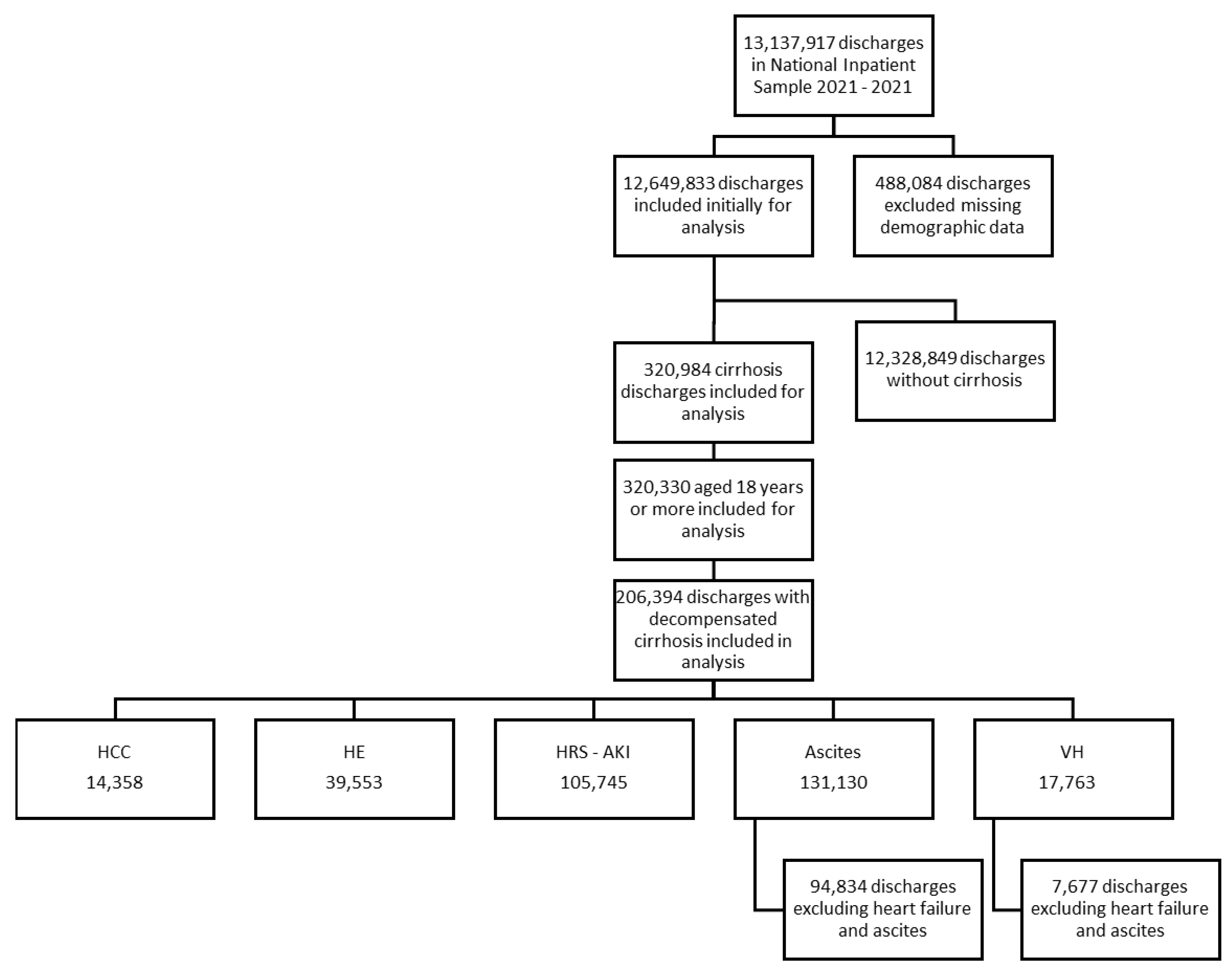
Figure A2.
Baseline characteristics.
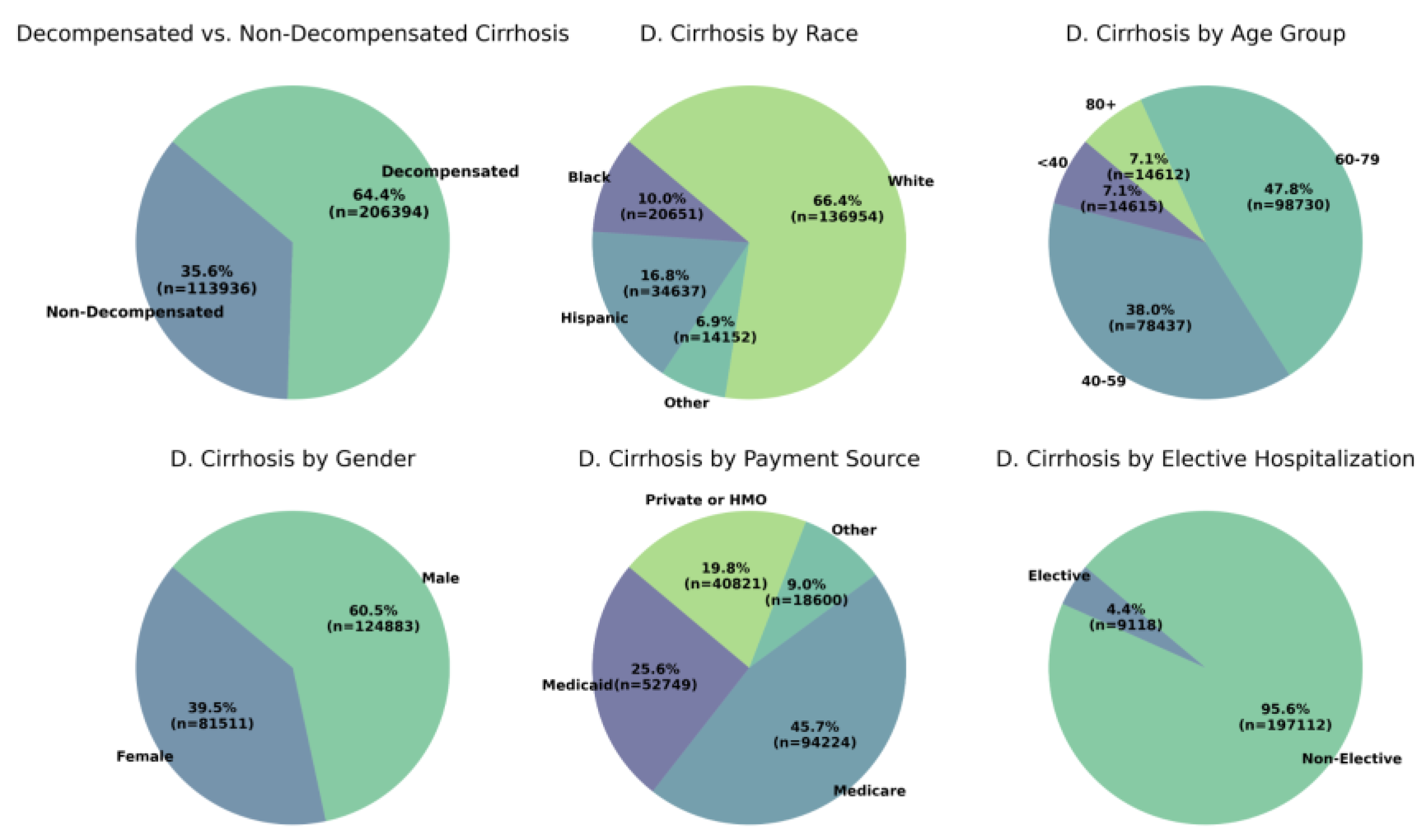
Figure A3.
Distribution of payment method among racial and ethnic groups.
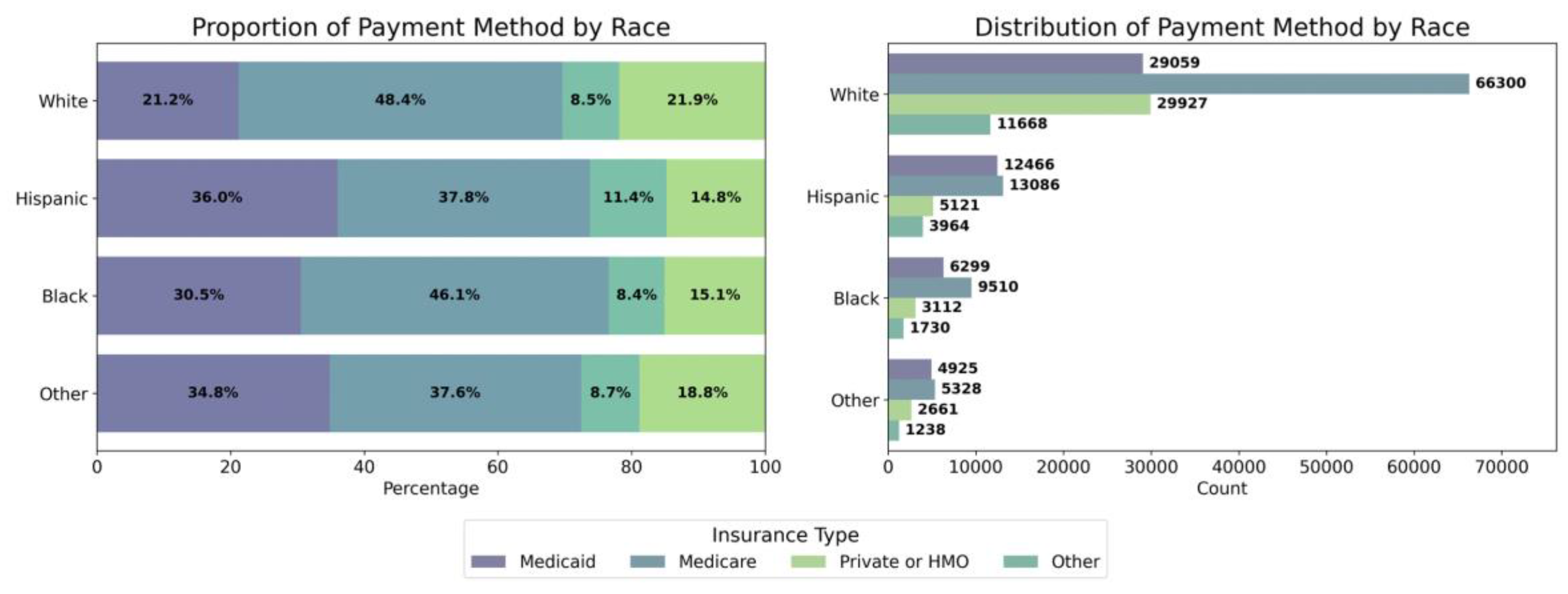

Table A1.
ICD-10 Codes used for inclusion, exclusion and procedure identification.
| Category | Subcategory | ICD-10 Codes |
| Cirrhosis Codes | Hepatic Fibrosis and Sclerosis | K740, K7400, K7401, K7402, K741, K742 |
| Biliary Cirrhosis | K743, K744, K745 | |
| Unspecified Cirrhosis of Liver | K7460 | |
| Other Cirrhosis of Liver | K7469 | |
| Alcoholic Cirrhosis of Liver | K7030, K7031 | |
| Alcoholic Fibrosis and Sclerosis | K702 | |
| Complication Codes | Ascites | R188, K7031, K7011, K7151 |
| VH (Variceal Hemorrhage) | I8501, I8511 | |
| HE (Hepatic Encephalopathy) | G9340, G9341, G9349, R40*, K7041, K7111, K7201, K7211, K7291, B190, B1911, B1921 | |
| SCC (Somnolence, stupor, and coma) | R40 | |
| HRS or AKI (Hepatorenal Syndrome or Acute) | K767, N170, N171, N172, N178, N179 | |
| HCC (Hepatocellular Carcinoma) | C220, C228, C229 | |
| Procedure Codes | EGD (Upper Gastrointestinal Endoscopy) | 0DJ08ZZ, 0D983ZX, 0D958ZX, 0DJ08ZZ, 0D953ZX, 0DJ68ZZ, 0D963ZX, 0DJ07ZZ, 0D568ZZ, 0D578ZZ, 0D588ZZ, 0D598ZZ, 0D5A8ZZ, 0D718ZZ, 0D728ZZ, 0D738ZZ, 0D748ZZ, 0D758ZZ, 0D768ZZ, 0D778ZZ, 0D788ZZ, 0D798ZZ, 0D7A8ZZ, 0D718DZ, 0D728DZ, 0D738DZ, 0D748DZ, 0D758DZ, 0D768DZ, 0D778DZ, 0D788DZ, 0D798DZ, 0D7A8DZ, 0D9180Z, 0D918ZX, 0D918ZZ, 0D9280Z, 0D928ZX, 0D928ZZ, 0D9380Z, 0D938ZX, 0D938ZZ, 0D9480Z, 0D948ZX, 0D948ZZ, 0D9580Z, 0D958ZX, 0D958ZZ, 0D9680Z, 0D968ZX, 0D968ZZ, 0D9780Z, 0D978ZX, 0D978ZZ, 0D9880Z, 0D988ZX, 0D988ZZ, 0D9980Z, 0D998ZX, 0D998ZZ, 0D9A80Z, 0D9A8ZX, 0D9A8ZZ, 0DB18ZX, 0DB18ZZ, 0DB28ZX, 0DB28ZZ, 0DB38ZX, 0DB38ZZ, 0DB48ZX, 0DB48ZZ, 0DB58ZX, 0DB58ZZ, 0DB68ZX, 0DB68ZZ, 0DB78ZX, 0DB78ZZ, 0DB88ZX, 0DB88ZZ, 0DB98ZX, 0DB98ZZ, 0DBA8ZX, 0DBA8ZZ, 0DC18ZZ, 0DC28ZZ, 0DC38ZZ, 0DC48ZZ, 0DC58ZZ, 0DC68ZZ, 0DC78ZZ, 0DC88ZZ, 0DC98ZZ, 0DCA8ZZ, 0DJ08ZZ, 06L30ZZ, 0D554ZZ, 0D518ZZ, 0D528ZZ, 0D538ZZ, 0D548ZZ, 0D558ZZ, 0D568ZZ, 0W3P8ZZ, 3E0G8TZ, 0DQ78ZZ, 0DQ68ZZ, 0DQ28ZZ, 0DQ38ZZ, 0DQ58ZZ, 0DQ48ZZ, 06L38CZ, 06L34CZ, 06L38ZZ, 3E0G8GC, 06L28CZ, 06L28ZZ, 0DL57DZ, 0DL58DZ |
| TIPS (Transjugular Intrahepatic Portosystemic Shunt) * | 06183J4, 06184J4, 06183JY, 061847Y, 061849Y, 06184AY, 06184JY, 06184KY, 06184ZY, 06183DY, 06184DY | |
| Hemodialysis and CRRT | Z992, Z4901, Z4931, 5A1D00Z, 5A1D60Z, 5A1D70Z, 5A1D80Z, 5A1D90Z | |
| Liver Tx (Liver transplantation) | 0FY00Z0, 0FY00Z1, 0FY00Z2 | |
| RBC Tx (Red Blood Cell Transfusion) | 30233N1, 30243N1, 30233N0, 30233P0, 30233P1 | |
| Platelets Tx (Platelets Transfusion) | 30233R1, 30243R1, 30230R0 | |
| FFP Tx (Fresh Frozen Plasma Transfusion) | 30233K1, 30243K1, 30233K0, 30233L0, 30233L1 | |
| Exclusion Codes | Heart Failure ** | 39891, 40211, 40291, 40401, 40411, 40403, 40413, 40491, 40493, 428x, I0981, I110, I130, I132, I50 |
* VH and ascites were mutually excluded when analyzing for TIPS.** Patients with exclusion codes for HF were excluded when analyzing TIPS.
Table A2.
EGD for VH by Racial and Ethnic Groups.
| Complication | Procedure | Chi2 | P_Chi2 | OR | CI_Lower | CI_Upper | P_OR | Category1 | Category2 | ASPR_C1 | ASPR_C2 |
| VH | EGD | 57.976 | 1.59E-12 | 1.101 | 1.023 | 1.184 | 1.027E-02 | Other | White | 863.208 | 851.616 |
| VH | EGD | 57.976 | 1.59E-12 | 1.003 | 0.957 | 1.052 | 8.967E-01 | Hispanic | White | 851.639 | 851.616 |
| VH | EGD | 57.976 | 1.59E-12 | 1.275 | 1.183 | 1.374 | 0.000E+00 | White | Black | 851.616 | 817.863 |
| VH | EGD | 57.976 | 1.59E-12 | 1.097 | 1.013 | 1.189 | 2.310E-02 | Other | Hispanic | 863.208 | 851.639 |
| VH | EGD | 57.976 | 1.59E-12 | 1.403 | 1.272 | 1.549 | 0.000E+00 | Other | Black | 863.208 | 817.863 |
| VH | EGD | 57.976 | 1.59E-12 | 1.279 | 1.179 | 1.387 | 0.000E+00 | Hispanic | Black | 851.639 | 817.863 |
Table A3.
TIPS for VH and Ascites by Racial and Ethnic Groups.
| Complication | Procedure | Chi2 | P_Chi2 | OR | CI_Lower | CI_Upper | P_OR | Category1 | Category2 | ASPR_C1 | ASPR_C2 |
| VH | TIPS | 36.676 | 5.39E-08 | 1.236 | 1.138 | 1.342 | 4.500E-07 | White | Hispanic | 51.346 | 41.531 |
| VH | TIPS | 36.676 | 5.39E-08 | 0.999 | 0.891 | 1.121 | 9.926E-01 | White | Other | 51.346 | 50.539 |
| VH | TIPS | 36.676 | 5.39E-08 | 1.199 | 1.042 | 1.379 | 1.124E-02 | White | Black | 51.346 | 42.032 |
| VH | TIPS | 36.676 | 5.39E-08 | 1.237 | 1.086 | 1.409 | 1.355E-03 | Other | Hispanic | 50.539 | 41.531 |
| VH | TIPS | 36.676 | 5.39E-08 | 1.031 | 0.885 | 1.201 | 6.928E-01 | Black | Hispanic | 42.032 | 41.531 |
| VH | TIPS | 36.676 | 5.39E-08 | 1.199 | 1.009 | 1.425 | 3.886E-02 | Other | Black | 50.539 | 42.032 |
| Ascites | TIPS | 121.43 | 3.79E-26 | 1.160 | 1.085 | 1.239 | 1.159E-05 | White | Hispanic | 15.060 | 12.974 |
| Ascites | TIPS | 121.43 | 3.79E-26 | 1.148 | 1.040 | 1.266 | 6.037E-03 | White | Other | 15.060 | 13.151 |
| Ascites | TIPS | 121.43 | 3.79E-26 | 1.776 | 1.579 | 1.997 | 0.000E+00 | White | Black | 15.060 | 8.506 |
| Ascites | TIPS | 121.43 | 3.79E-26 | 1.010 | 0.904 | 1.130 | 8.559E-01 | Other | Hispanic | 13.151 | 12.974 |
| Ascites | TIPS | 121.43 | 3.79E-26 | 1.531 | 1.347 | 1.741 | 0.000E+00 | Hispanic | Black | 12.974 | 8.506 |
| Ascites | TIPS | 121.43 | 3.79E-26 | 1.547 | 1.335 | 1.794 | 1.000E-08 | Other | Black | 13.151 | 8.506 |
Table A4.
Hemodialysis for HRS or AKI by Racial and Ethnic Groups.
| Complication | Procedure | Chi2 | P_Chi2 | OR | CI_Lower | CI_Upper | P_OR | Category1 | Category2 | ASPR_C1 | ASPR_C2 |
| HRS or AKI | HD | 476.46 | 6.02E-103 | 1.304 | 1.256 | 1.354 | 0.000E+00 | Other | White | 103.026 | 80.990 |
| HRS or AKI | HD | 476.46 | 6.02E-103 | 1.241 | 1.208 | 1.275 | 0.000E+00 | Hispanic | White | 98.836 | 80.990 |
| HRS or AKI | HD | 476.46 | 6.02E-103 | 1.191 | 1.154 | 1.229 | 0.000E+00 | Black | White | 95.413 | 80.990 |
| HRS or AKI | HD | 476.46 | 6.02E-103 | 1.051 | 1.007 | 1.096 | 2.191E-02 | Other | Hispanic | 103.026 | 98.836 |
| HRS or AKI | HD | 476.46 | 6.02E-103 | 1.095 | 1.046 | 1.146 | 9.100E-05 | Other | Black | 103.026 | 95.413 |
| HRS or AKI | HD | 476.46 | 6.02E-103 | 1.042 | 1.004 | 1.082 | 2.973E-02 | Hispanic | Black | 98.836 | 95.413 |
| HRS or AKI | HD | 45.27 | 1.71E-11 | 1.068 | 1.047 | 1.090 | 0.000E+00 | Male | Female | 89.040 | 83.711 |
Table A5.
LT for Decompensated Cirrhosis by Racial and Ethnic Groups.
| Complication | Procedure | Chi2 | P_Chi2 | OR | CI_Lower | CI_Upper | P_OR | Category1 | Category2 | ASPR_C1 | ASPR_C2 |
| D. Cirrhosis | Liver Tx | 234.39 | 1.55E-50 | 1.021 | 0.971 | 1.074 | 0.414 | White | Hispanic | 12.35 | 12.18 |
| D. Cirrhosis | Liver Tx | 234.39 | 1.55E-50 | 1.183 | 1.105 | 1.267 | 0.000 | Other | White | 14.56 | 12.35 |
| D. Cirrhosis | Liver Tx | 234.39 | 1.55E-50 | 1.674 | 1.548 | 1.811 | 0.000 | White | Black | 12.35 | 7.36 |
| D. Cirrhosis | Liver Tx | 234.39 | 1.55E-50 | 1.208 | 1.117 | 1.307 | 0.000 | Other | Hispanic | 14.56 | 12.18 |
| D. Cirrhosis | Liver Tx | 234.39 | 1.55E-50 | 1.640 | 1.502 | 1.790 | 0.000 | Hispanic | Black | 12.18 | 7.36 |
| D. Cirrhosis | Liver Tx | 234.39 | 1.55E-50 | 1.981 | 1.795 | 2.187 | 0.000 | Other | Black | 14.56 | 7.36 |
| D. Cirrhosis | Liver Tx | 51.84 | 6.04E-13 | 1.147 | 1.104 | 1.193 | 0.000 | Male | Female | 12.60 | 11.02 |
Table A6.
EGD for VH by Payment Method.
| Complication | Procedure | Chi2 | P_Chi2 | OR | CI_Lower | CI_Upper | P_OR | Category1 | Category2 | ASPR_C1 | ASPR_C2 |
| VH | EGD | 48.83 | 1.42E-10 | 1.116 | 1.063 | 1.171 | 9.000E-06 | Medicaid | Medicare | 852.45 | 839.22 |
| VH | EGD | 48.83 | 1.42E-10 | 1.196 | 1.135 | 1.260 | 0.000E+00 | Private/HMO | Medicare | 861.39 | 839.22 |
| VH | EGD | 48.83 | 1.42E-10 | 1.101 | 1.034 | 1.172 | 2.690E-03 | Other | Medicare | 851.95 | 839.22 |
| VH | EGD | 48.83 | 1.42E-10 | 1.072 | 1.016 | 1.131 | 1.071E-02 | Private/HMO | Medicaid | 861.39 | 852.45 |
| VH | EGD | 48.83 | 1.42E-10 | 1.014 | 0.952 | 1.080 | 6.739E-01 | Medicaid | Other | 852.45 | 851.95 |
| VH | EGD | 48.83 | 1.42E-10 | 1.087 | 1.017 | 1.161 | 1.459E-02 | Private/HMO | Other | 861.39 | 851.95 |
Table A7.
TIPS for VH and Ascites by Payment Method.
| Complication | Procedure | Chi2 | P_Chi2 | OR | CI_Lower | CI_Upper | P_OR | Category1 | Category2 | ASPR_C1 | ASPR_C2 |
| VH | TIPS | 96.19 | 1.02E-20 | 1.055 | 0.972 | 1.145 | 1.988E-01 | Private/HMO | Medicaid | 56.19 | 53.39 |
| VH | TIPS | 96.19 | 1.02E-20 | 1.388 | 1.273 | 1.514 | 0.000E+00 | Private/HMO | Medicare | 56.19 | 42.18 |
| VH | TIPS | 96.19 | 1.02E-20 | 1.557 | 1.385 | 1.750 | 0.000E+00 | Private/HMO | Other | 56.19 | 37.65 |
| VH | TIPS | 96.19 | 1.02E-20 | 1.316 | 1.212 | 1.429 | 0.000E+00 | Medicaid | Medicare | 53.39 | 42.18 |
| VH | TIPS | 96.19 | 1.02E-20 | 1.476 | 1.317 | 1.654 | 0.000E+00 | Medicaid | Other | 53.39 | 37.65 |
| VH | TIPS | 96.19 | 1.02E-20 | 1.121 | 0.997 | 1.261 | 5.616E-02 | Medicare | Other | 42.18 | 37.65 |
| Ascites | TIPS | 119.42 | 1.03E-25 | 1.005 | 0.945 | 1.067 | 8.838E-01 | Medicare | Medicaid | 13.84 | 13.61 |
| Ascites | TIPS | 119.42 | 1.03E-25 | 1.214 | 1.142 | 1.292 | 0.000E+00 | Private/HMO | Medicare | 16.68 | 13.84 |
| Ascites | TIPS | 119.42 | 1.03E-25 | 1.358 | 1.232 | 1.496 | 0.000E+00 | Medicare | Other | 13.84 | 10.28 |
| Ascites | TIPS | 119.42 | 1.03E-25 | 1.220 | 1.145 | 1.300 | 0.000E+00 | Private/HMO | Medicaid | 16.68 | 13.61 |
| Ascites | TIPS | 119.42 | 1.03E-25 | 1.351 | 1.225 | 1.491 | 0.000E+00 | Medicaid | Other | 13.61 | 10.28 |
| Ascites | TIPS | 119.42 | 1.03E-25 | 1.649 | 1.493 | 1.820 | 0.000E+00 | Private/HMO | Other | 16.68 | 10.28 |
Table A8.
Hemodialysis for HRS or AKI by Payment Method.
| Complication | Procedure | Chi2 | P_Chi2 | OR | CI_Lower | CI_Upper | P_OR | Category1 | Category2 | ASPR_C1 | ASPR_C2 |
| HRS or AKI | HD | 1706.49 | 0.00E+00 | 1.544 | 1.505 | 1.584 | 0.000E+00 | Private or HMO | Medicare | 107.895 | 72.939 |
| HRS or AKI | HD | 1706.49 | 0.00E+00 | 1.468 | 1.432 | 1.505 | 0.000E+00 | Medicaid | Medicare | 103.289 | 72.939 |
| HRS or AKI | HD | 1706.49 | 0.00E+00 | 1.026 | 0.984 | 1.070 | 2.287E-01 | Other | Medicare | 75.104 | 72.939 |
| HRS or AKI | HD | 1706.49 | 0.00E+00 | 1.052 | 1.022 | 1.082 | 4.470E-04 | Private or HMO | Medicaid | 107.895 | 103.289 |
| HRS or AKI | HD | 1706.49 | 0.00E+00 | 1.504 | 1.439 | 1.572 | 0.000E+00 | Private or HMO | Other | 107.895 | 75.104 |
| HRS or AKI | HD | 1706.49 | 0.00E+00 | 1.430 | 1.369 | 1.494 | 0.000E+00 | Medicaid | Other | 103.289 | 75.104 |
Table A9.
Liver transplantation for Decompensated Cirrhosis by Payment Method.
| Complication | Procedure | Chi2 | P_Chi2 | OR | CI_Lower | CI_Upper | P_OR | Category1 | Category2 | ASPR_C1 | ASPR_C2 |
| D. Cirrhosis | Liver Tx | 6850.82 | 0.00E+00 | 3.859 | 3.660 | 4.068 | 0.000 | Private or HMO | Medicaid | 29.81 | 7.83 |
| D. Cirrhosis | Liver Tx | 6850.82 | 0.00E+00 | 1.042 | 0.984 | 1.103 | 0.158 | Medicaid | Medicare | 7.83 | 7.56 |
| D. Cirrhosis | Liver Tx | 6850.82 | 0.00E+00 | 1.116 | 1.017 | 1.224 | 0.021 | Medicaid | Other | 7.83 | 6.94 |
| D. Cirrhosis | Liver Tx | 6850.82 | 0.00E+00 | 4.021 | 3.848 | 4.201 | 0.000 | Private or HMO | Medicare | 29.81 | 7.56 |
| D. Cirrhosis | Liver Tx | 6850.82 | 0.00E+00 | 4.305 | 3.954 | 4.688 | 0.000 | Private or HMO | Other | 29.81 | 6.94 |
| D. Cirrhosis | Liver Tx | 6850.82 | 0.00E+00 | 1.071 | 0.981 | 1.169 | 0.128 | Medicare | Other | 7.56 | 6.94 |
References
- Huang, D.Q.; Terrault, N.A.; Tacke, F.; Gluud, L.L.; Arrese, M.; Bugianesi, E.; Loomba, R. Global epidemiology of cirrhosis - aetiology, trends and predictions. Nat. Rev. Gastroenterol. Hepatol. 2023, 20, 388–398. [Google Scholar] [CrossRef] [PubMed]
- Moon, A.M.; Singal, A.G.; Tapper, E.B. Contemporary Epidemiology of Chronic Liver Disease and Cirrhosis. Division of Gastroenterology and Hepatology, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA; Division of Digestive and Liver Diseases, University of Texas Southwestern Medical Center, Dallas, TX, USA; Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, MI, USA; Gastroenterology Section, Veterans Affairs Ann Arbor Healthcare System, Ann Arbor, MI, USA.
- Nephew, L.D.; Knapp, S.M.; Mohamed, K.A.; et al. Trends in Racial and Ethnic Disparities in the Receipt of Lifesaving Procedures for Hospitalized Patients With Decompensated Cirrhosis in the US, 2009-2018. JAMA Netw. Open 2023, 6, e2324539. [Google Scholar] [CrossRef]
- Nguyen, G. C., Thuluvath, P. J., & Thuluvath, A. J. (2020). Racial disparities in liver disease: Implications for hepatitis C virus screening, diagnosis, and treatment. Gastroenterology. [CrossRef]
- Tapper, E. B., & Saini, S. D. (2021). Racial and Ethnic Disparities in Chronic Liver Disease and Hepatitis C. Journal of Clinical Gastroenterology. [CrossRef]
- Kaplan, D.E.; Ripoll, C.; Thiele, M.; Fortune, B.E.; Simonetto, D.A.; Garcia-Tsao, G.; Bosch, J. AASLD Practice Guidance on risk stratification and management of portal hypertension and varices in cirrhosis. Hepatology 2024, 79, 1180–1211. [Google Scholar] [CrossRef] [PubMed]
- United States Renal Data System. 2022 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, US Department of Health and Human Services; 2022. Accessed May 22, 2023. https://usrds-adr.niddk.nih.gov/2022.
Figure 1.
Distribution of cirrhosis complications among racial and ethnic groups.
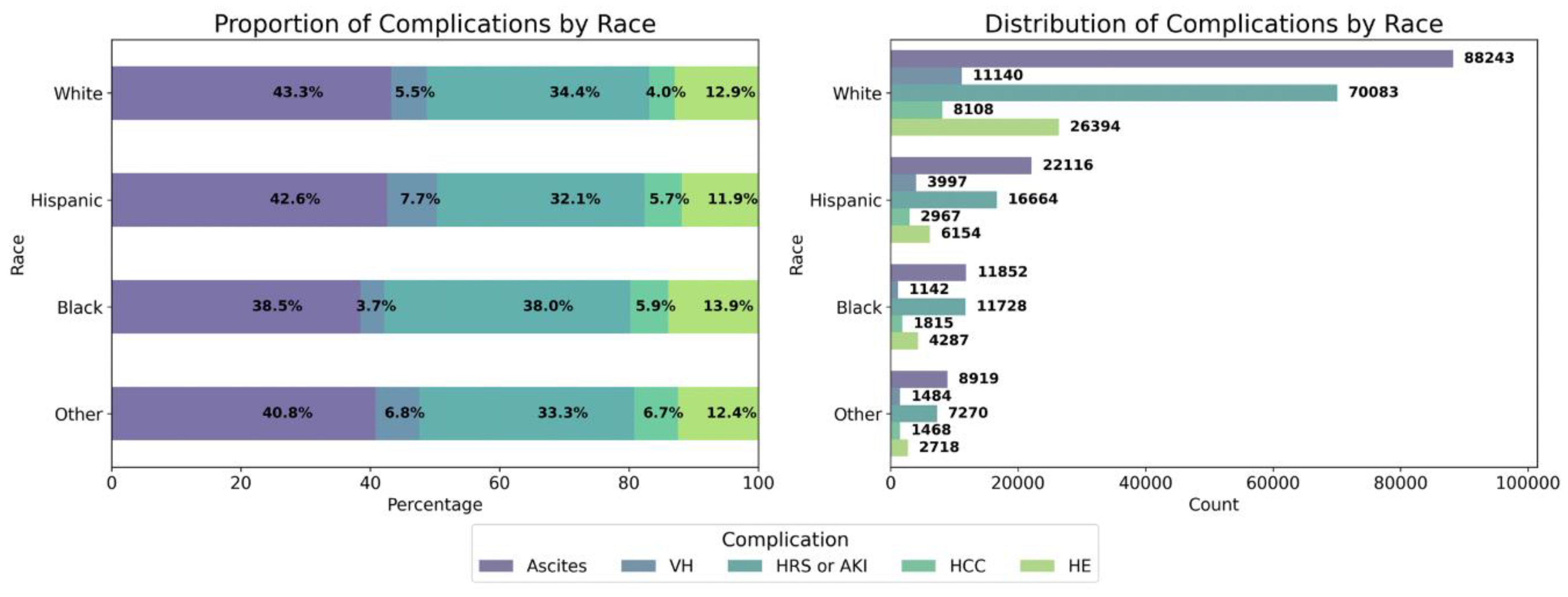
Figure 2.
Black individuals generally had lower odds of undergoing EGD when compared to White, Hispanic, and individuals from other ethnic groups. The ASPR of EGD for VH was highest among individuals from other ethnic groups at 863.208 per 1000 admissions, followed by Hispanic patients at 851.639, White patients at 851.616, and Black patients at 817.863 per 1000 admissions.
Figure 2.
Black individuals generally had lower odds of undergoing EGD when compared to White, Hispanic, and individuals from other ethnic groups. The ASPR of EGD for VH was highest among individuals from other ethnic groups at 863.208 per 1000 admissions, followed by Hispanic patients at 851.639, White patients at 851.616, and Black patients at 817.863 per 1000 admissions.
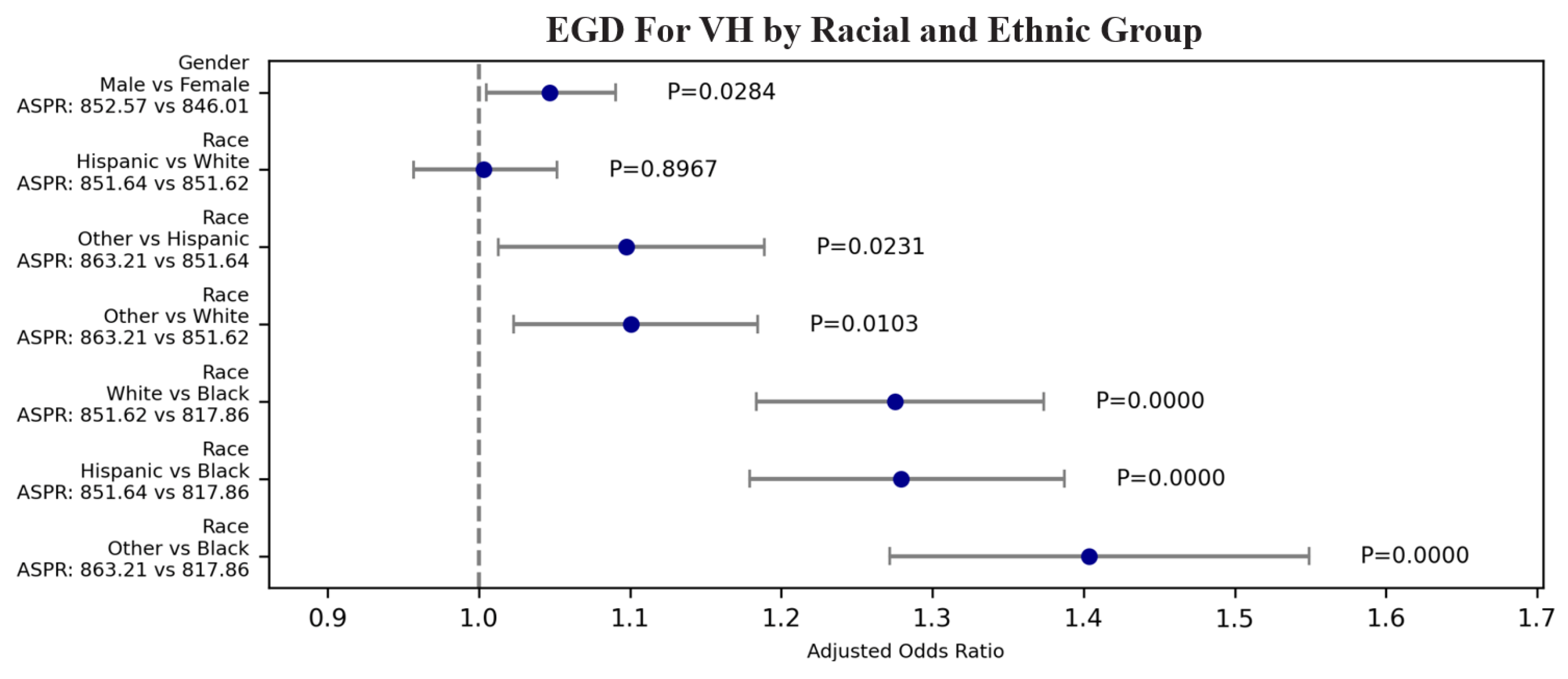
Figure 3.
(A) The ASPR of TIPS for VH was highest among White patients at 51.35 per 1000 admissions, followed by patients of other ethnic groups at 50.54, Black patients at 42.03, and Hispanic patients at 41.53 per 1000 admissions. (B) The ASPR of TIPS for ascites was highest among White patients at 15.06 per 1000 admissions, followed by patients of other ethnic groups at 13.15, Hispanic patients at 12.97, and Black patients at 8.51 per 1000 admissions.
Figure 3.
(A) The ASPR of TIPS for VH was highest among White patients at 51.35 per 1000 admissions, followed by patients of other ethnic groups at 50.54, Black patients at 42.03, and Hispanic patients at 41.53 per 1000 admissions. (B) The ASPR of TIPS for ascites was highest among White patients at 15.06 per 1000 admissions, followed by patients of other ethnic groups at 13.15, Hispanic patients at 12.97, and Black patients at 8.51 per 1000 admissions.
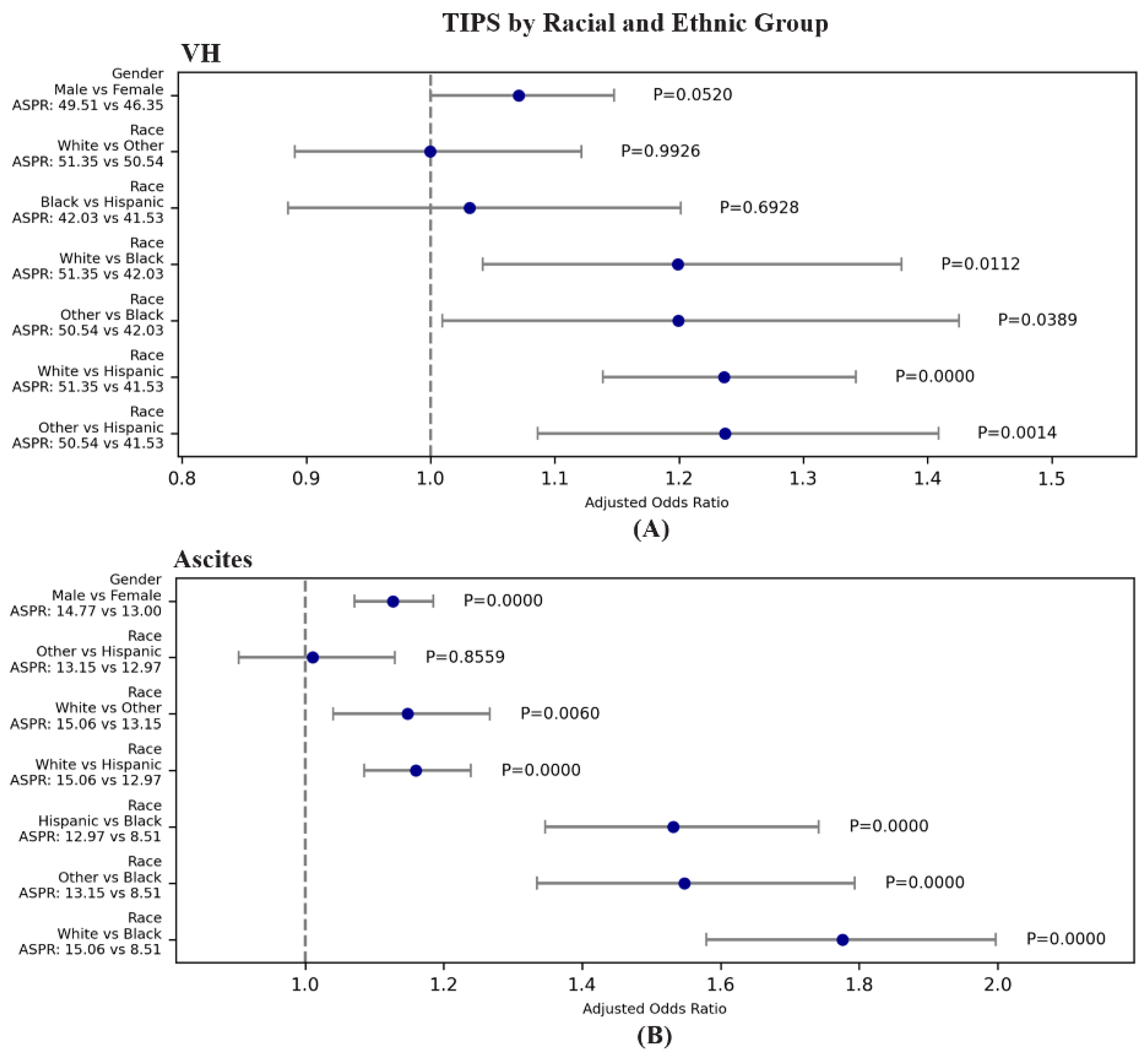
Figure 4.
The ASPR of hemodialysis for HRS or AKI was highest among individuals from other ethnic groups at 103.03 per 1000 admissions, followed by Hispanic patients at 98.84, Black patients at 95.41, and White patients at 80.99 per 1000 admissions.
Figure 4.
The ASPR of hemodialysis for HRS or AKI was highest among individuals from other ethnic groups at 103.03 per 1000 admissions, followed by Hispanic patients at 98.84, Black patients at 95.41, and White patients at 80.99 per 1000 admissions.
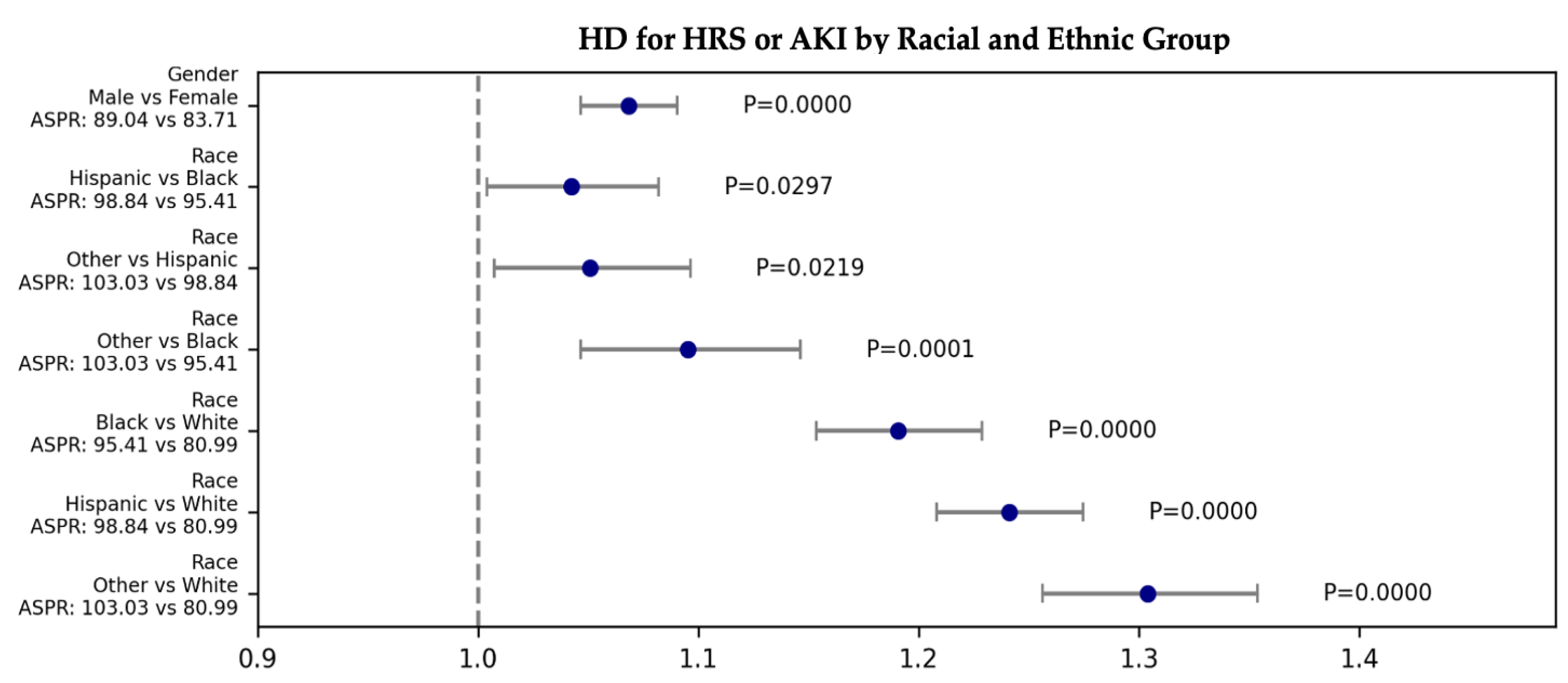
Figure 5.
The ASPR of liver transplants for decompensated cirrhosis was highest among individuals from other ethnic groups at 14.56 per 1000 admissions, followed by White patients at 12.35 Hispanic patients at 12.18, and Black patients at 7.36 per 1000 admissions.
Figure 5.
The ASPR of liver transplants for decompensated cirrhosis was highest among individuals from other ethnic groups at 14.56 per 1000 admissions, followed by White patients at 12.35 Hispanic patients at 12.18, and Black patients at 7.36 per 1000 admissions.
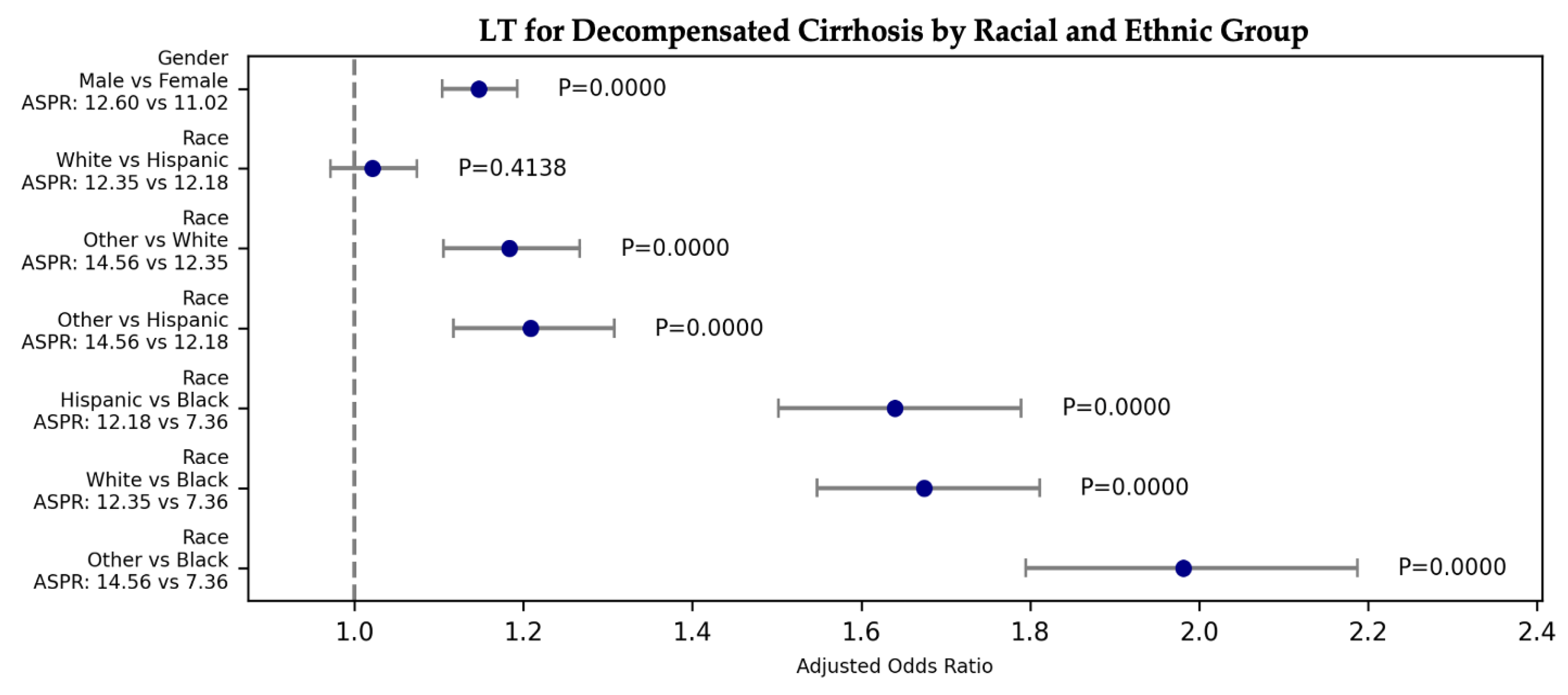
Figure 6.
The ASPR of EGD for VH was highest among patients with Private or HMO insurance at 861.39 per 1000 admissions, followed by Medicaid recipients at 852.45, patients with other payment methods at 851.95, and Medicare recipients at 839.22 per 1000 admissions.
Figure 6.
The ASPR of EGD for VH was highest among patients with Private or HMO insurance at 861.39 per 1000 admissions, followed by Medicaid recipients at 852.45, patients with other payment methods at 851.95, and Medicare recipients at 839.22 per 1000 admissions.
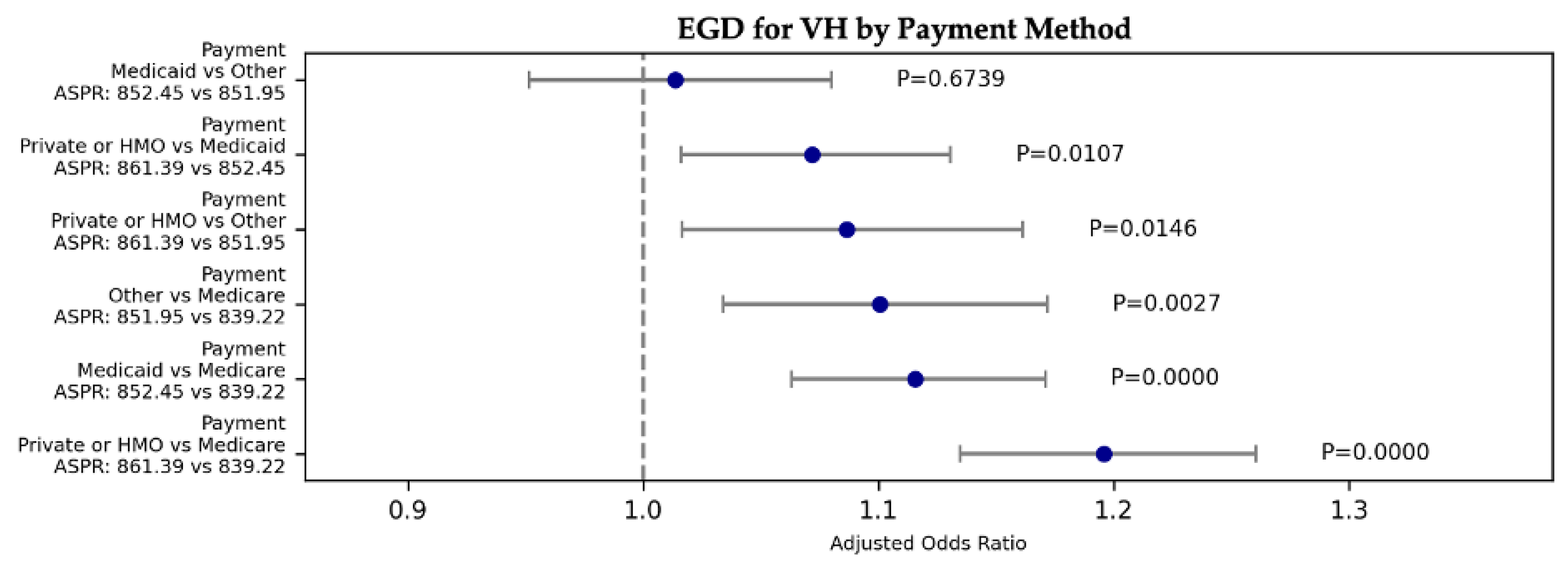
Figure 7.
(A) Patients with Private or HMO insurance had the highest ASPR for TIPS for VH at 56.19 per 1000 admissions, followed by Medicaid recipients at 53.39, Medicare recipients at 42.18, and those with other payment methods at 37.65 per 1000 admissions. (B) Patients with Private or HMO insurance had the highest ASPR for TIPS for ascites at 16.68 per 1000 admissions, followed by Medicare recipients at 13.84, Medicaid recipients at 13.61, and those with other payment methods at 10.28 per 1000 admissions.
Figure 7.
(A) Patients with Private or HMO insurance had the highest ASPR for TIPS for VH at 56.19 per 1000 admissions, followed by Medicaid recipients at 53.39, Medicare recipients at 42.18, and those with other payment methods at 37.65 per 1000 admissions. (B) Patients with Private or HMO insurance had the highest ASPR for TIPS for ascites at 16.68 per 1000 admissions, followed by Medicare recipients at 13.84, Medicaid recipients at 13.61, and those with other payment methods at 10.28 per 1000 admissions.
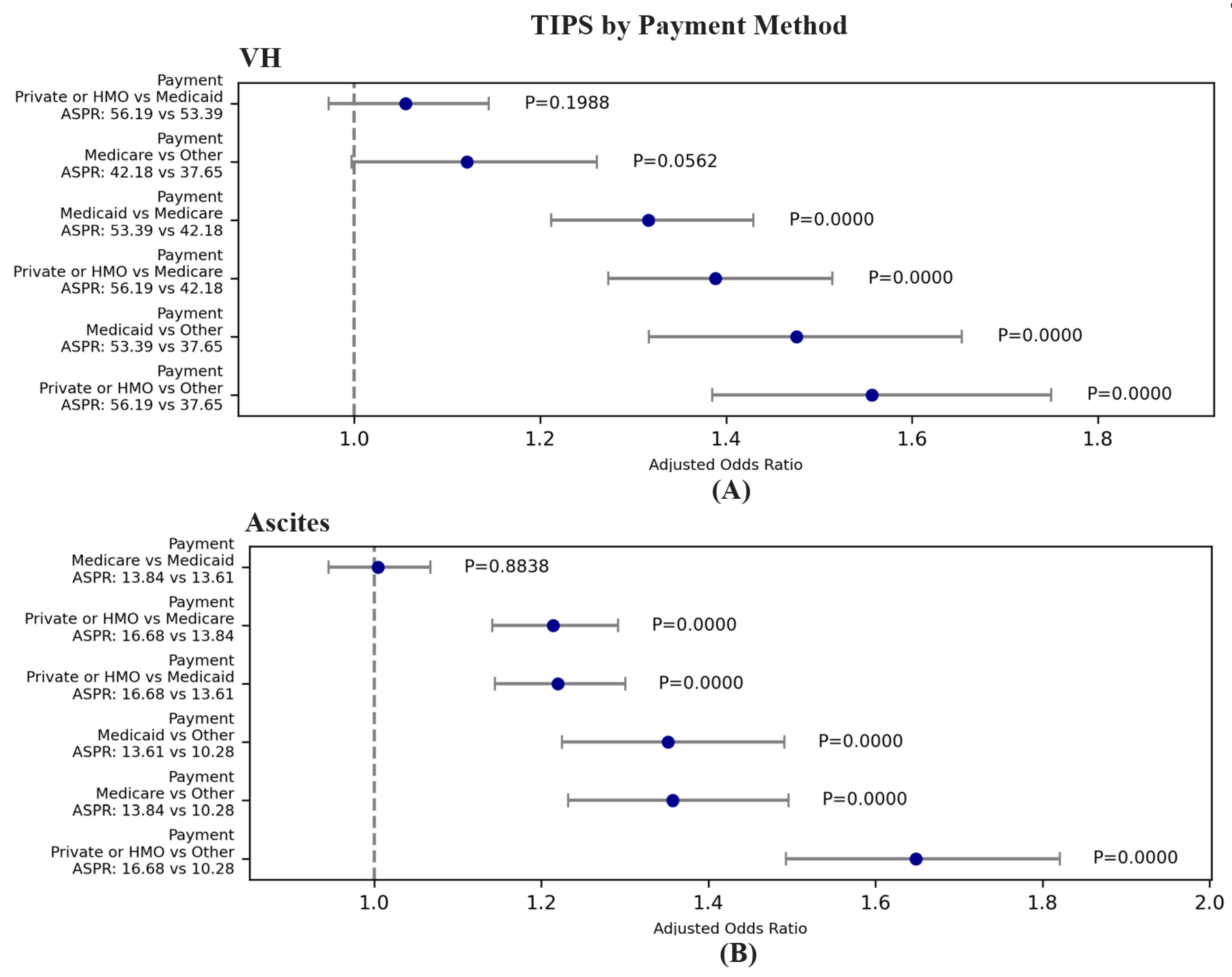
Figure 8.
Private or HMO insurance holders had the highest odds of receiving hemodialysis/CRRT for HRS or AKI, followed by Medicaid recipients. Medicare and other payment methods had the lowest odds. The ASPR of hemodialysis/CRRT for HRS or AKI was highest among individuals with Private or HMO insurance at 107.90 per 1000 admissions, followed by Medicaid recipients at 103.29, individuals with other payment methods at 75.10, and Medicare recipients at 72.94 per 1000 admissions.
Figure 8.
Private or HMO insurance holders had the highest odds of receiving hemodialysis/CRRT for HRS or AKI, followed by Medicaid recipients. Medicare and other payment methods had the lowest odds. The ASPR of hemodialysis/CRRT for HRS or AKI was highest among individuals with Private or HMO insurance at 107.90 per 1000 admissions, followed by Medicaid recipients at 103.29, individuals with other payment methods at 75.10, and Medicare recipients at 72.94 per 1000 admissions.
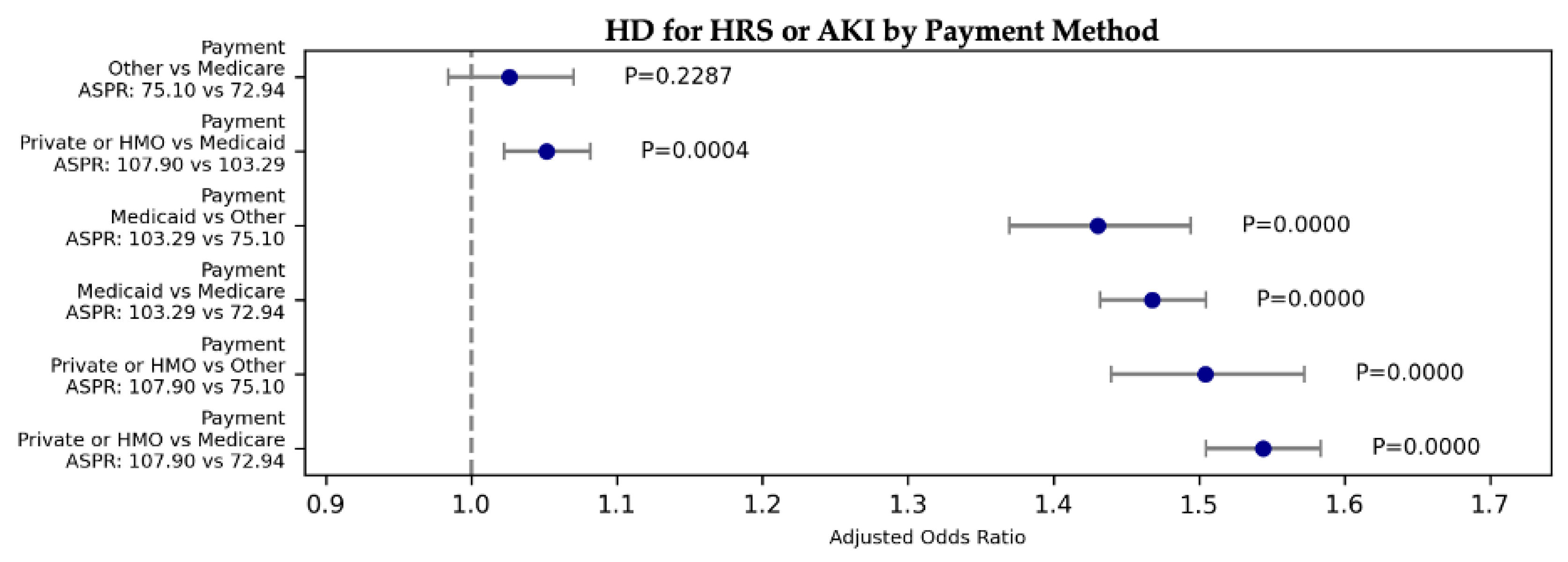
Figure 9.
The ASPR of liver transplants for decompensated cirrhosis was highest among individuals with Private or HMO insurance at 29.81 per 1000 admissions, followed by Medicaid recipients at 7.83, Medicare recipients at 7.56, and other payment methods at 6.94 per 1000 admissions.
Figure 9.
The ASPR of liver transplants for decompensated cirrhosis was highest among individuals with Private or HMO insurance at 29.81 per 1000 admissions, followed by Medicaid recipients at 7.83, Medicare recipients at 7.56, and other payment methods at 6.94 per 1000 admissions.
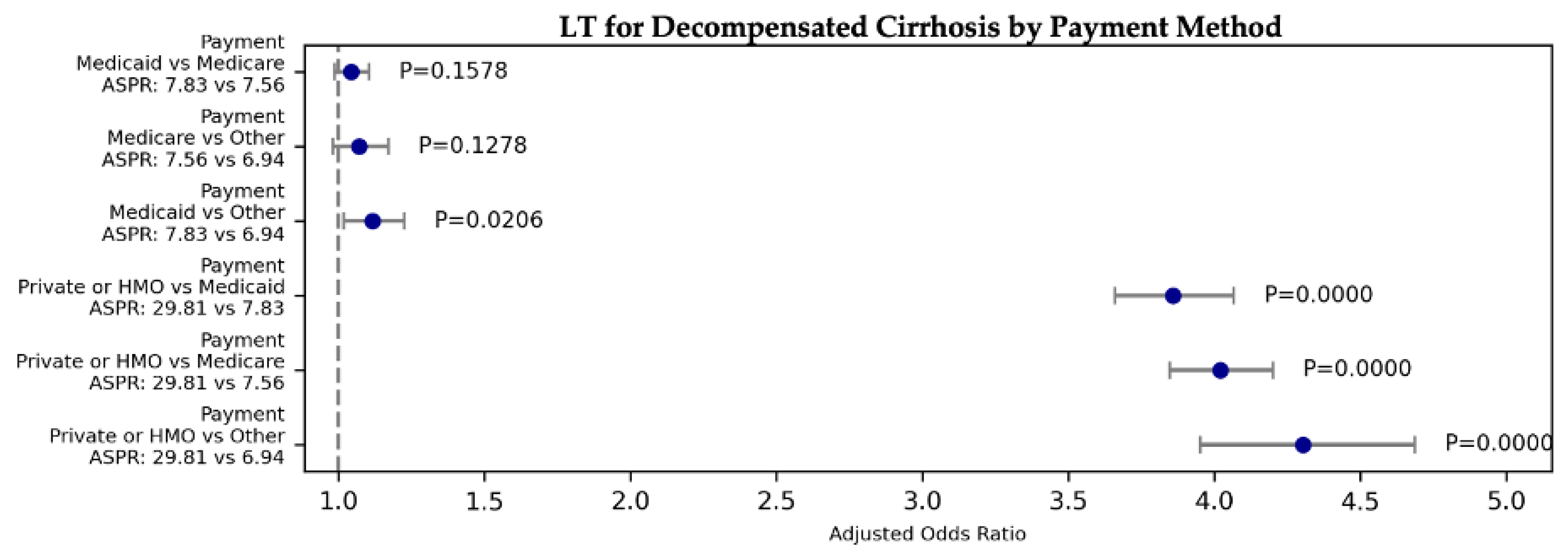
Figure 10.
For all odds ratios (ORs), the reference group is White patients for race and private insurance for payment method. Lines indicate estimates; shading, 95% CIs.
Figure 10.
For all odds ratios (ORs), the reference group is White patients for race and private insurance for payment method. Lines indicate estimates; shading, 95% CIs.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



