
Submitted:
15 August 2024
Posted:
27 August 2024
You are already at the latest version
Abstract
Purpose: This study was designed to investigate the ability of telemonitoring involving a secure elec-tronic database called “Alsayed System for Applied Medical-Care Improvement” (ASAMI) to detect at least 95% of acute exacerbations of chronic obstructive pulmonary disease (AECOPD). Methods: This prospective observational study, which took place over 16 months in 2022-2023, was based at a medi-cal center in Jordan. The study group participants were patients with COPD (from seven countries) with mixed levels of airflow limitation severity, and every participant was followed for six months. A customized, password-protected version of ASAMI was used to collect data during the study. The implemented diary included questions on daily symptoms such as cough, dyspnea, sputum, and daily physical activities. The detection of AECOPD events was initially based on daily questionnaires com-pleted by patients, followed by the assessment of a healthcare practitioner. Results: 87 participants were monitored for AECOPD. During the study, 78/87 (89.7%) patients presented with one or more exacerbation episodes. The mean (range) age was 59.7 (45-81) years, predominantly male (66%), with moderate airflow limitation (n=42, 48%). Compliance with the provision of daily symptom data was very high, 98% over the entire study period. A total of 189 confirmed AECOPD episodes were reported. Almost all patients and practitioners showed favorable satisfaction with the role of the ASAMI-related service (96% reported a score of 10 satisfaction). The telemonitoring tool was able to detect 99% of AECOPD episodes. Conclusion: The novel ASAMI software was effective as a telemonitoring tool to detect the episodes of AECOPD. The tool was suggested for daily, continuous reporting of respiratory symptoms, with the key benefits being ease of use, patient acceptance, and collation of supplementary data when exacerbations occur. The effects of its widespread use on decision-making can be clarified by evaluating its impact on routine clinical decision-making.
Keywords:
ASAMI
; COPD
; Exacerbations
; Middle East
; Telehealth
; Telemedicine
1. Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive airway inflammatory disease leading to fixed airflow obstruction. [1, 2] COPD is a significant cause of hospitalization and reduced quality of life and ranks the fourth most common cause of death globally. [2] Deteriorations of the respiratory symptoms beyond typical daily symptoms termed acute exacerbations of COPD (AECOPD) lead to accelerated lung function decline, increased morbidity, and mortality. [2] Different contributing factors, like infection, play a crucial role in the complex landscape of AECOPD [3-7]. Understanding this relationship is paramount for managing and rapidly detecting AECOPD.
It is well established in asthma and COPD that encouraging self-management can lead to better disease control and fewer unscheduled doctor visits. [8-12] With the ubiquitous nature of technology today, it stands to reason that digital technologies may be utilized to facilitate the self-management of chronic diseases such as COPD.
Due to individuals' reluctance to see their physician for consultations, telehealth services have increased dramatically over the COVID-19 era. [13, 14] However, telehealth services allowed for regular healthcare involvement for these individuals with chronic diseases. Regarding COPD, reduced AECOPD or hospitalizations could have a positive cost impact if patients were encouraged to employ self-management plans as an alternative treatment option.
Recent comprehensive studies have determined that remote patient monitoring can improve health status and possibly prevent exacerbations. Commonly, these evaluations struggle to draw conclusions and propose further study. [15, 16]
We postulated that providing patients with COPD and other suspected respiratory causes of dyspnea with telemonitoring support during an integrated respiratory clinic delivery would reduce unscheduled care events.
This prospective study was designed to investigate the ability of telemonitoring involving a secure electronic database called “Alsayed System for Applied Medical-Care Improvement” (ASAMI) to detect at least 95% of AECOPD in the study cohort of COPD patients.
2. Materials and Methods
2.1. Study Design and Participants Selection Criteria
This prospective observational study that took place over 16 months in 2022 and 2023 was based in Al-Rayhan Medical Center, Amman, Jordan. The study group participants were patients with COPD with mixed levels of airflow limitation severity (GOLD grades I-IV).
The approval of the study was sought and gained from the Research Ethics Board of Al-Rayhan Medical Center (ARMC-2022-IRB-1-3), following the Research Ethics and Governance Policies and Procedures and the Declaration of Helsinki. All subjects gave written informed consent. No interventions were performed on patients. During the study, participants’ medical care continued with their own physicians.
Every participant was followed for six months. The study participants were gathered from respiratory consultant clinics or were recommended by primary care workers. This study utilized a medical case note review in ASAMI. The attendance records of all consecutive patients presenting to the medical center were screened for eligibility by the primary research assistant (RA). The complete medical notes of patients who fit the study criteria were selected for further review. The principal investigator reviewed such notes at regular intervals and decided on study eligibility.
Patients with FEV1/FVC (forced expiratory volume in one second / forced vital capacity) < 70 % had the spirometry classification of grades I-IV severity depending on post-bronchodilator FEV1 % predicted to be eligible for the study. Mild airflow limitation (Grade I): has FEV1 80% predicted; moderate airflow limitation (Grade II): 50%-79%; severe airflow limitation (Grade III): 30%-49%; and very severe airflow limitation (Grade IV): <30%. The aforementioned criteria agree with the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2023 guideline [2].
The following represents the selection criteria for the study participants:
The inclusion criteria
- Aged 40 years and over.
- A history of breathing problems categorized as COPD GOLD grade I to IV at the time of informed consent.
- All participants reported, at the baseline visit, being current smokers or ex-smokers (previously having consumed ten or more packs per year).
- Having less than 20% reversibility in FEV1 (forced expiratory volume in one second) and less than 200 ml increase in FEV1 following the administration of salbutamol (200 µg).
- Willingness to provide informed consent and a willingness to use the website or the telephone platform, respond to clinical team notifications, and follow professional advice. This allowed for up to six months of symptom monitoring from a distance, with follow-up assistance available by phone.
The exclusion criteria
- A history of asthma.
- A history of seasonal allergic rhinitis.
- Patients with a significant co-morbidity which might prevent them from being able to withstand the study procedure.
Patients with GOLD grade IV disease, by the very nature of the severity of their disease, often have other co-morbidities and are often too severe to participate in a study where there is frequent clinical assessment. Therefore, patients with GOLD grade IV were not actively recruited into the study. However, if they volunteered and met eligibility criteria, they were invited to participate in the study.
2.2. Practitioners and Tutorial
A convenience sample consisting of General Practitioners (n=4), residents (n=3), consultant physician (n=1), final-year medical (n=3), and pharmacy students (n=7) was enrolled in the study. After explaining the study procedure, all practitioners who consented to the study were included in the sample.
The training was intended to familiarize the practitioners with the trial website. During training, all practitioners were assigned unique log-ins, passwords, and one sample case as practice material. Practice sessions were supervised by the primary investigator in group sessions of 2-3 practitioners each. Context-specific help was provided at each step on the website for assistance during the practice session. All practitioners completed their assigned practice cases and were recruited for the study.
The practitioners were allowed to complete their assessments of the cases from any computer connected to the Internet at any time. After logging into the website, practitioners assessed the patient. All clinical decisions, and the time taken to complete each step, were recorded.
2.3. Data Collection and Assessment of AECOPD
From eligible patient notes, the primary RA extracted data regarding patient details, date and time of patient assessment; details of clinical presentation such as symptoms, past medical and family history; examination findings, tests performed, and differential diagnosis and management plan; referral for specialist or senior opinion; and outcome of the assessment. These data were entered directly into the ASAMI database. This study utilized a medical case note review in ASAMI as introduced in our previous studies [17, 18].
ASAMI is a novel system developed for several reasons such as electronic medical file, decision-making for diagnosis and treatmnent, and consultation request. The tool was suggested for daily, regular reporting of respiratory symptoms, with the key benefits being ease of use, patient acceptance, and collation of supplementary data when exacerbations occur.
A list of variables assessed during the study is included in Table 1. Figure 1 shows the criteria for a suspected onset of an AECOPD and confirmation of an exacerbation.
Initiating at study enrolment, participants were requested to complete the diary every day of the study duration (Table 2). This diary included questions on daily symptoms such as cough, dyspnea, sputum, and daily physical activities. Full validation (translation and back translation) was performed. Face and content validly were ensured and assessed by three experts in questionable verification to ensure the clarity and accuracy. The research team reviewed the electronic data daily. Every subject in the study had at least one home visit scheduled for each AECOPD event during the study period. Follow-up visits for the end of the AECOPD took place until one month after the end of the study period. Any AECOPD not resolved by that extended period was described as continuing events.
Participants were notified of their daily diary (Table 2). After answering all daily questions, the diaries were encrypted and wirelessly transferred to a data server. The staff was notified when one or more symptoms increased in severity by two levels on a given day; any symptom reached its worst level on a given day; or a participant reported a health-system encounter for a respiratory problem; reported symptoms of a respiratory infection; had not transmitted two consecutive daily diaries; or requested staff contact. Participants whose diaries fit one of the criteria listed above were contacted and followed according to Figure 1. During hospitalizations (if needed), staff visited the participants as soon as it was medically safe to do so. Participants continued their diary contributions while in the hospital with the agreement of attending physicians.
We evaluated the severity of AECOPD using the Anthonisen criterion [19]. The length of an AECOPD was defined as the time between the date an exacerbation was confirmed and the date the participant reported normal breathing.
Follow-up visits for the end of exacerbation took place until one month after the end of the study period. Any exacerbations that were not resolved by that extended period were described as continuing events. Exacerbation severity was graded retrospectively during data analysis according to Anthonisen criteria [20]. AECOPD: acute exacerbation of the chronic obstructive pulmonary disease.
2.4. Follow-Up Satisfaction
Patients’ and practiotioners’ satisfaction with the services they received and provided was assessed at the end of the study accorng to a rect sudy with some modifications [21]. Satisfaction was evaluated through four questions (choice of satisfaction ranged from 1 to 10, with a higher score indicating better satisfaction):
- How did you like the service you received? (for patients only);
- Do you think this service is needed for every patient that enters the clinic? (for patients and practitioners);
- Was the service provided effectively? (for patients and practitioners);
- Was the time spent on the tutorial sufficient and useful? (for practitioners only).
2.5. Statistical Analysis
Assessment of compliance with the completion of daily diary questionnaires and the detection of AECOPD were descriptive. Data are given as frequency (%) of participants, unless otherwise specified. The mean (standard deviation) or median (interquartile range) were used when appropriate. SPSS version 26 was used.
3. Results
3.1. Baseline Characteristics
Out of the 92 COPD patients sampled for baseline screening, three were ineligible, one refused to participate, one withdrew, and 87 were monitored for the AECOPD for six months. During the study, 78/87 (89.7%) patients presented with one or more exacerbation episodes. The majority of the participants (n = 45, 52%) were based in Jordan, while 12 (14%) the United Arab Emirates, 9 (10%) Palestine, 8 (9%) Saudi Arabia, 6 (7%) Iraq, 5 (6%) Syria, and 2 (2%) Qatar. The demographic and clinical characteristics of the 87 participants who completed the study extension and were monitored for AECOPD are included in Table 3.
The baseline characteristics for the participants showed that the mean (range) age was 59.7 (45-81) years, predominantly male (66%), with moderate airflow limitation (n=42, 48%), followed by GOLD III (n=24, 28%), GOLD I (n=18, 21%), and GOLD IV (n=3, 3%). The mean (SD) FEV1 was 58.7 (7.5)% of predicted. The most commonly used reliever treatment was a short-acting beta-2 agonist (SABA) (n=57, 66%), and the most frequently used controller medications were the combination of a long-acting beta-2 agonist (LABA) and long-acting muscarinic antagonist (LAMA( (n=45, 52%) (Table 3).
3.2. Characteristics of AECOPD
Compliance with the provision of daily symptom data was very high, 98% over the entire study period. Of the 191 potential AECOPD reports, 189 cases met the Anthonisen criteria from 87 patients. Using daily questionnaires, 81 (43%) single event-days were identified by Anthonisen Class 1 criteria, and 60 (32%) single event-days were identified by Anthonisen Class 2 criteria. Only 18 AECOPD episodes from 18 participants were hospitalized. Seventy-eight exacerbation episodes (41%) required oral prednisone, and 120 (63%) required an antibiotic (Table 4).
Non-return to normal breathing was reported in 2 cases (3%). The median (range) was 9 (2-36) days for the 187 AECOPD, where the participants reported a return to normal breathing before the study conclusion (Table 4). Only one AECOPD episode was missed using the telemonitoring tool, which required hospital admission; accordingly, this study tool was able to detect 99% of AECOPD episodes.
3.3. Patients’ and Practitioner’ Satisfaction with the Service
Almost all patients and practitioners who participated in the study showed favorable satisfaction with the role of the ASAMI-related service. Most patients and practitioners chose 10 for any of the questions, delivering high satisfaction with the provided care service (96% reported an absolute score of 10 satisfaction).
4. Discussion
This study was designed purely to examine the clinical performance of the ASAMI system and identify its potential utility in medical centers or clinics in the detection of AECOPD as earlier as possible. This study demonstrated the applicability of telemonitoring using the novel ASAMI database.
Because early management improves outcomes and quality of life, diagnosing AECOPD as soon as possible is necessary. [22] Cessation of smoking, vaccination, inhaled maintenance treatments, and oxygen therapy may minimize the onset and severity of illness [23, 24]. Early detection and treatment of AECOPD could improve outcomes and health status.
Exacerbations reduce FVC, FEV1, and PEF, making them suitable for remote monitoring. [25] From photoplethysmography waveforms, commercial pulse oximeters may measure oxygen saturation (SpO2), heart rate, and breathing frequency. [26] Recently, machine learning has been related to functional imaging [27] airway volume and hospital admission history to AECOPD. [28] Despite advancements in remote patient monitoring, healthcare utilization is unlikely to be affected. This can inaccurately report exacerbations, resulting in unnecessary actions. [29] Recent comprehensive studies have determined that remote patient monitoring can improve health status and possibly prevent exacerbations. Commonly, these evaluations struggle to draw conclusions and propose further study. [15, 16]
Breathing frequency, oxygen saturation, heart rate at the end of an endeavor, and walking distance have been associated with exacerbations. [26, 30] In other studies, machine learning has related image-based airway volume and resistance [27] or hospitalization history (Cavailles, Melloni et al. 2020) to exacerbation risk. According to some systematic reviews, telemonitoring interventions for COPD may not enhance mortality, quality of life, exercise ability, or outcomes of AECOPD. [16, 29]
Self-reported healthcare utilization [31], including antibiotic and systemic corticosteroid prescriptions, was lower than AECOPD defined by the usual three-out-of-three or two-out-of-three Anthonisen criteria. [32] The modified Anthonisen criteria [33] produced a higher exacerbation rate than the original criteria. [32] Thus, integrating more symptoms and physiological signs provides a complete picture of COPD and its daily variations.
According to a recent study, the strongest predictors of AECOPD identified by classic or modified Anthonisen criteria were the use of inhaled short-acting bronchodilators and a drop in SpO2 below 90%. [31] As exacerbations become more symptom-based, inhaled short-acting bronchodilators and SpO2 below 90% become stronger predictors. These markers could be evaluated daily to reveal disease control variability. COPD patients' peak expiratory flow is unreliable because of high variability. [34]
Individuals who are prescribed antibiotics or systemic corticosteroids may not know when to utilize them if they are not provided with strict guidelines. Telemonitoring of COPD patients may aid in formulating more effective treatment recommendations.
Recent technological developments, such as telehealth services and/or remote monitoring devices, are increasingly being used to aid patients in managing chronic diseases. The electronic medical record has been attempted in the past. [35, 36] However, the limited uptake of electronic medical records capable of recording sufficient narrative clinical detail currently in clinical practice indicates that a stand-alone system may prove much more practical in the medium term. [37] Part of the underlying structure has been described briefly in this study, and more details of the content will be detailed in future studies. The main hypotheses underlying the development of ASAMI were to improve the quality of decision-making in different medical settings.
Different clinical sites are high-risk clinical areas for adverse medical events [13, 14, 17, 38, 39]. ASAMI is a novel system thatwas developed for several reasons, including decreasing medical errors, mainly due to lack of medical documentation. The Institute of Medicine report has brought the problem of medical error under intense scrutiny. [40] While the use of computerized prescription software has been shown to reduce the incidence of medication-related errors substantially. [41, 42] Given the practitioner's satisfaction with the ASAMI tool in this study, the ability to rapidly enter patient features may allow frequent use by clinicians during most patient encounters. An assessment of the impact of the system in a real-life setting should be performed as a future plan to examine the effects of the ASAMI database on clinicians in actual patients in their natural environment.
Our research has some limitations. The number of patients was limited. We could not compare COPD patients into phenotypes or examine if different phenotypes or airflow limitations had distinct outcomes due to the small number of subjects.
5. Conclusions
The novel ASAMI software that recorded the patients' daily symptoms, medication use, and other medical information was effective as a telemonitoring tool to detect the episodes of AECOPD as soon as possible. The tool may be used in any location, and patients accepted the device and only required low-level support.
The ASAMI aid can be of potential use in medical centers. The effects of its widespread use on decision-making can be clarified by evaluating its impact on routine clinical decision-making.
The tool was suggested for daily, regular reporting of respiratory symptoms, with the key benefits being ease of use, patient acceptance, and collation of supplementary data when exacerbations occur.
Supplementary Materials
Screenshot of some of the data collection part in the ASAMI database for one case.
Funding
This research received no external funding”.
Acknowledgments
I would like to acknowledge the participants and the healthcare team supported this study, including but not limited to Dr Yazan Alsayed Alotabi from Al-Rayhan Medical Center.
Conflicts of Interest
“The authors declare no conflict of interest.”.
References
- NICE Chronic Obstructive Pulmonary disease: quick reference guide, National Institute for Health and Care Excellence; National Institute for Health and Care Excellence, 2010.
- GOLD The Global Initiative for Chronic Obstructive Lung Disease (GOLD). https://goldcopd.org/2023-gold-report-2/ (1 January).
- Alsayed, A.R.; Abed, A.; Khader, H.A.; Al-Shdifat, L.M.H.; Hasoun, L.; Al-Rshaidat, M.M.D.; Alkhatib, M.; Zihlif, M. Molecular Accounting and Profiling of Human Respiratory Microbial Communities: Toward Precision Medicine by Targeting the Respiratory Microbiome for Disease Diagnosis and Treatment. Int. J. Mol. Sci. 2023, 24, 4086. [Google Scholar] [CrossRef] [PubMed]
- Alsayed, A. R.; Al-Dulaimi, A.; Alkhatib, M.; Al Maqbali, M.; Al-Najjar, M. A. A.; Al-Rshaidat, M. M. , A comprehensive clinical guide for Pneumocystis jirovecii pneumonia: A missing therapeutic target in HIV-uninfected patients. Expert Review of Respiratory Medicine 2022, 16, (11–12), 1167. [Google Scholar] [CrossRef] [PubMed]
- Alsayed, A.R.; Abed, A.; Khader, H.A.; Hasoun, L.; Al Maqbali, M.; Al Shawabkeh, M.J. The role of human rhinovirus in COPD exacerbations in Abu Dhabi: molecular epidemiology and clinical significance. Libyan J. Med. 2024, 19, 2307679. [Google Scholar] [CrossRef] [PubMed]
- Alsayed, A.R.; Abed, A.; Jarrar, Y.B.; Alshammari, F.; Alshammari, B.; Basheti, I.A.; Zihlif, M. Alteration of the Respiratory Microbiome in Hospitalized Patients with Asthma–COPD Overlap during and after an Exacerbation. J. Clin. Med. 2023, 12, 2118. [Google Scholar] [CrossRef] [PubMed]
- Alsayed, A. R.; Abed, A.; Al Shawabkeh, M. J.; Aldarawish, R. R.; Al-Shajlawi, M.; Alabbas, N. , Human Rhinovirus: Molecular and Clinical Overview. Pharmacy Practice (Granada) 2024, 22, (1), 1. [Google Scholar]
- Halpin, D.M.; Decramer, M.; Celli, B.; Kesten, S.; Liu, D.; Tashkin, D.P.; Celli, B.; Liu, D. Exacerbation frequency and course of COPD. Int. J. Chronic Obstr. Pulm. Dis. 2012, 7, 653–661. [Google Scholar] [CrossRef]
- Anzueto, A.; Leimer, I.; Kesten, S. , Impact of frequency of COPD exacerbations on pulmonary function, health status and clinical outcomes. International journal of chronic obstructive pulmonary disease 2009, 4, 245–251. [Google Scholar]
- Alsayed, A.R. Illustrating How to Use the Validated Alsayed_v1 Tools to Improve Medical Care: A Particular Reference to the Global Initiative for Asthma 2022 Recommendations. Patient Preference Adherence 2023, ume 17, 1161–1179. [Google Scholar] [CrossRef]
- Al-kilkawi, Z. M.; Basheti, I. A.; Obeidat, N. M.; Saleh, M. R.; Hamadi, S.; Abutayeh, R.; Nassar, R.; Alsayed, A. R. , Evaluation of the Association between Inhaler technique and Adherence in Asthma Control: Cross-Sectional Comparative Analysis Study between Amman and Baghdad. Pharmacy Practice 2024, 22, (1), 1–12. [Google Scholar]
- Al-Hamaden, R.A.; Abed, A.; Khader, H.; Hasoun, L.; Al-Dulaimi, A.H.; Alsayed, A. Knowledge and Practice of Healthcare Professionals in the Medical Care of Asthma Adult Patients in Jordan with a Particular Reference to Adherence to GINA Recommendations. J. Multidiscip. Heal. 2024, ume 17, 391–404. [Google Scholar] [CrossRef]
- Alsayed, A.R.; Halloush, S.; Hasoun, L.; Alnatour, D.; Al-Dulaimi, A.; Alnajjar, M.S.; Blaibleh, A.; Al-Imam, A.; Alshammari, F.; A Khader, H. Perspectives of the community in the developing countries toward telemedicine and pharmaceutical care during the COVID-19 pandemic. Pharm. Pr. (Internet) 2022, 20, 2618–2618. [Google Scholar] [CrossRef]
- Khader, H.; Alsayed, A.; Hasoun, L. Z.; Alnatour, D.; Awajan, D.; Alhosanie, T. N.; Samara, A. , Pharmaceutical care and telemedicine during COVID-19: A cross-sectional study based on pharmacy students, pharmacists, and physicians in Jordan. Pharmacia 2022, 69, (3), 891–901. [Google Scholar] [CrossRef]
- Cruz, J.; Brooks, D.; Marques, A. Home telemonitoring effectiveness in COPD: a systematic review. Int. J. Clin. Pr. 2014, 68, 369–378. [Google Scholar] [CrossRef] [PubMed]
- McCabe, C.; McCann, M.; Brady, A.M. Computer and mobile technology interventions for self-management in chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2017, 2020, CD011425. [Google Scholar] [CrossRef]
- Alsayed, A. R.; Al-Dulaimi, A.; Alnatour, D.; Awajan, D.; Alshammari, B. , Validation of an assessment, medical problem-oriented plan, and care plan tools for demonstrating the clinical pharmacist's activities. Saudi Pharm J 2022, 30, (10), 1464–1472. [Google Scholar] [CrossRef]
- Alsayed, A.R.; Hasoun, L.; A Khader, H.; Al-Dulaimi, A.; AbuAwad, A.; Basheti, I.; Al Maqbali, M. Evaluation of the effectiveness of educational medical informatics tutorial on improving pharmacy students’ knowledge and skills about the clinical problem-solving process. Pharm. Pr. (Internet) 2022, 20, 01–08. [Google Scholar] [CrossRef] [PubMed]
- Anthonisen, N.R.; Manfreda, J.; Warren, C.P.W.; Hershfield, E.S.; Harding, G.K.M. Antibiotic Therapy in Exacerbations of Chronic Obstructive Pulmonary Disease. Ann. Intern. Med. 1987, 106, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Anthonisen, N.R.; Manfreda, J.; Warren, C.P.W.; Hershfield, E.S.; Harding, G.K.M. Antibiotic Therapy in Exacerbations of Chronic Obstructive Pulmonary Disease. Ann. Intern. Med. 1987, 106, 196–204. [Google Scholar] [CrossRef]
- Al-Awaisheh, R. I.; Alsayed, A. R.; Basheti, I. A. , Assessing the Pharmacist's Role in Counseling Asthmatic Adults Using the Correct Inhaler Technique and Its Effect on Asthma Control, Adherence, and Quality of Life. Patient Prefer Adherence 2023, 17, 961–972. [Google Scholar] [CrossRef]
- Wilkinson, T.M.A.; Donaldson, G.C.; Hurst, J.R.; Seemungal, T.A.R.; Wedzicha, J.A. Early Therapy Improves Outcomes of Exacerbations of Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2004, 169, 1298–1303. [Google Scholar] [CrossRef] [PubMed]
- GOLD, Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (GOLD). 2023.
- Alsayed, A.R.; Abu-Samak, M.S.; Alkhatib, M. Asthma-COPD Overlap in Clinical Practice (ACO_CP 2023): Toward Precision Medicine. J. Pers. Med. 2023, 13, 677. [Google Scholar] [CrossRef] [PubMed]
- Sund, Z.; Powell, T.; Greenwood, R.; Jarad, N. Remote daily real-time monitoring in patients with COPD – A feasibility study using a novel device. Respir. Med. 2009, 103, 1320–1328. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.A.; Velardo, C.; Farmer, A.; Tarassenko, L. Exacerbations in Chronic Obstructive Pulmonary Disease: Identification and Prediction Using a Digital Health System. J. Med Internet Res. 2017, 19, e69. [Google Scholar] [CrossRef] [PubMed]
- Lanclus, M.; Clukers, J.; Van Holsbeke, C.; Vos, W.; Leemans, G.; Holbrechts, B.; Barboza, K.; De Backer, W.; De Backer, J. Machine Learning Algorithms Utilizing Functional Respiratory Imaging May Predict COPD Exacerbations. Acad. Radiol. 2018, 26, 1191–1199. [Google Scholar] [CrossRef]
- Cavailles, A.; Melloni, B.; Motola, S.; Dayde, F.; Laurent, M.; Le Lay, K.; Caumette, D.; Luciani, L.; Lleu, P.L.; Berthon, G.; et al. Identification of Patient Profiles with High Risk of Hospital Re-Admissions for Acute COPD Exacerbations (AECOPD) in France Using a Machine Learning Model. Int. J. Chronic Obstr. Pulm. Dis. 2020, ume 15, 949–962. [Google Scholar] [CrossRef]
- Li, X.; Xie, Y.; Zhao, H.; Zhang, H.; Yu, X.; Li, J. Telemonitoring Interventions in COPD Patients: Overview of Systematic Reviews. BioMed Res. Int. 2020, 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Rubio, N.; A Parker, R.; Drost, E.M.; Pinnock, H.; Weir, C.J.; Hanley, J.; Mantoani, L.C.; MacNee, W.; McKinstry, B.; A Rabinovich, R. Home monitoring of breathing rate in people with chronic obstructive pulmonary disease: observational study of feasibility, acceptability, and change after exacerbation. Int. J. Chronic Obstr. Pulm. Dis. 2017, ume 12, 1221–1231. [Google Scholar] [CrossRef]
- Cooper, C.B.; Sirichana, W.; Arnold, M.T.; Neufeld, E.V.; Taylor, M.; Wang, X.; A Dolezal, B. Remote Patient Monitoring for the Detection of COPD Exacerbations. Int. J. Chronic Obstr. Pulm. Dis. 2020, 15, 2005–2013. [Google Scholar] [CrossRef] [PubMed]
- Anthonisen, N. R.; Manfreda, J.; Warren, C. P. W. , Antiobiotic therapy in exacerbations of chronic obstructive pulmonary disease. Annals of Internal Medicine 1987, 106, (2), 196–204. [Google Scholar] [CrossRef]
- Burge, S.; Wedzicha, J. COPD exacerbations: definitions and classifications. Eur. Respir. J. 2003, 21, 46S–53s. [Google Scholar] [CrossRef]
- So, J.Y.; Lastra, A.C.; Zhao, H.; Marchetti, N.; Criner, G.J. Daily Peak Expiratory Flow Rate and Disease Instability in Chronic Obstructive Pulmonary Disease. Chronic Obstr. Pulm. Dis. J. COPD Found. 2016, 3, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Welford, C. R. In A comprehensive computerized patient record with automated linkage to QMR, Proceedings of the Annual Symposium on Computer Application in Medical Care, 1994; American Medical Informatics Association: p 814.
- Elhanan, G.; A Socratous, S.; Cimino, J.J. In Integrating DXplain into a clinical information system using the World Wide Web, Proceedings of the AMIA Annual Fall Symposium, 1996; American Medical Informatics Association: p 348.
- Berner, E.S.; Detmer, D.E.; Simborg, D. Will the Wave Finally Break? A Brief View of the Adoption of Electronic Medical Records in the United States. J. Am. Med Informatics Assoc. 2004, 12, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Weingart, N. S.; Wilson, R. M.; Gibberd, R. W.; Harrison, B. , Epidemiology of medical error. Bmj 2000, 320, (7237), 774–777. [Google Scholar] [CrossRef]
- Burroughs, T.E.; Waterman, A.D.; Gallagher, T.H.; Waterman, B.; Adams, D.; Jeffe, D.B.; Dunagan, W.C.; Garbutt, J.; Cohen, M.M.; Cira, J.; et al. Patient Concerns about Medical Errors in Emergency Departments. Acad. Emerg. Med. 2005, 12, 57–64. [Google Scholar] [CrossRef]
- Institute of Medicine Committee on Quality of Health Care in, A., In To Err is Human: Building a Safer Health System, Kohn, L. T.; Corrigan, J. M.; Donaldson, M. S., Eds.
- Copyright 2000 by the National Academy of Sciences. All rights reserved.: Washington (DC), 2000.
- Fortescue, E.B.; Kaushal, R.; Landrigan, C.P.; McKenna, K.J.; Clapp, M.D.; Federico, F.; Goldmann, D.A.; Bates, D.W. Prioritizing Strategies for Preventing Medication Errors and Adverse Drug Events in Pediatric Inpatients. Pediatrics 2003, 111, 722–729. [Google Scholar] [CrossRef]
- Kaushal, R.; Bates, D. , Information technology and medication safety: what is the benefit? BMJ Quality & Safety 2002, 11, (3), 261–265. [Google Scholar]
Figure 1.
Flow chart of the criteria of a suspected onset of an exacerbation and confirmation of an AECOPD.
Figure 1.
Flow chart of the criteria of a suspected onset of an exacerbation and confirmation of an AECOPD.
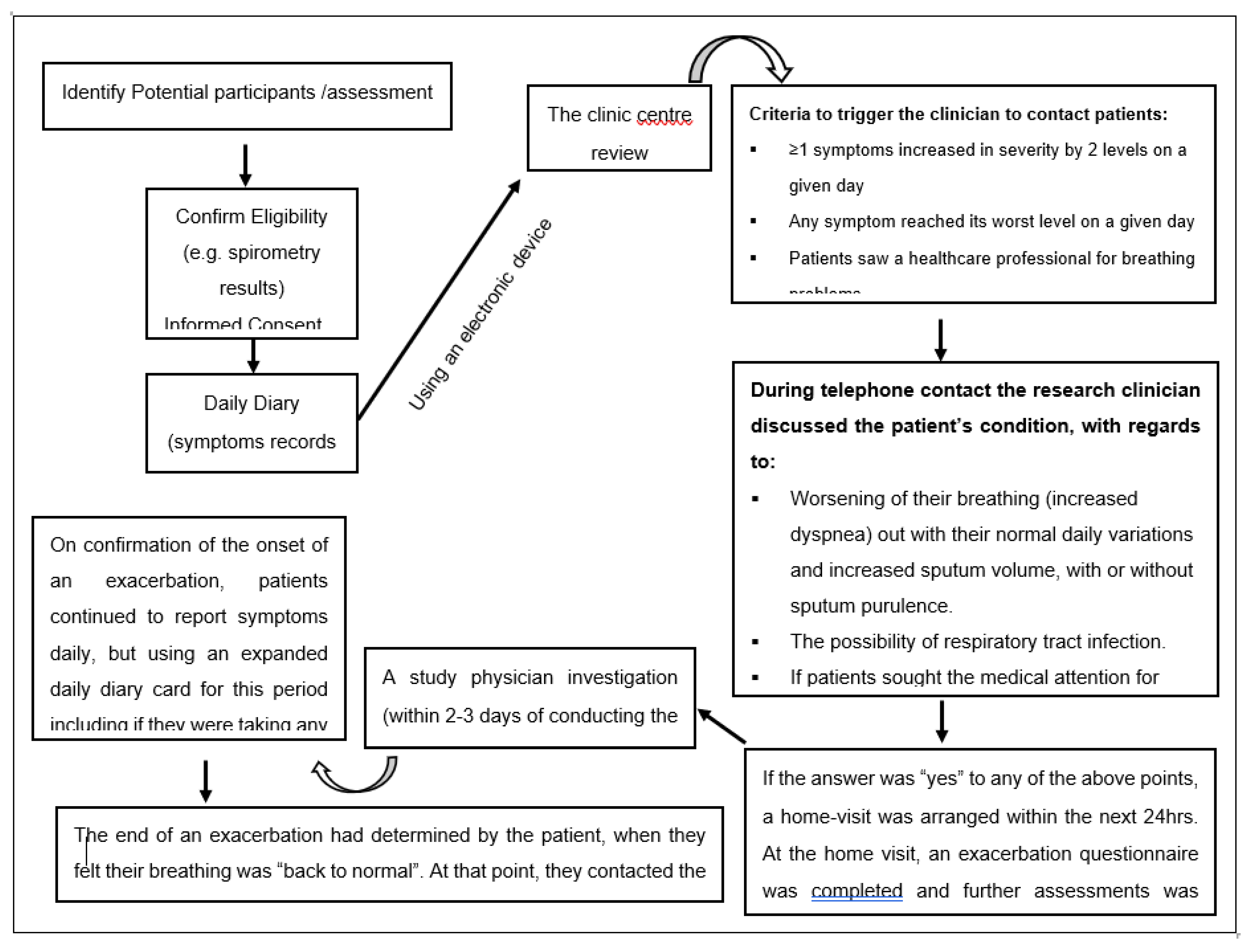

Table 1.
List of variables assessed during the study.
| Visit | Baseline | Daily | Exacerbation | Final |
|---|---|---|---|---|
| Eligibility (inclusion/exclusion criteria) | * | |||
| Consent | * | |||
| Data collection using ASAMI database | * | * | * | |
| Symptoms (daily diary) | * | * | * | * |
| Peak Expiratory Flow Rate | * | * | * | * |
| Pulmonary Function Test (Spirometry using Spirolab®) | * | * | * | |
| Spontaneous sputum collection (optional) | * | * | ||
| Nursing assessment | * | * | * | |
| Adverse events (to study procedures) | * | * | * | |
| Concomitant medications | * | * | * |
Table 2.
List of daily diary assessed during the study.
| Daily Diary Questions | أسئلة يوميات يومية | |
|---|---|---|
| 1 | Did you cough Today? | هل سعلت اليوم؟ |
| □ No □ Mild □ Moderate □ Severe □ Very severe |
□ لا □ خفيف □ معتدل □ شديد □ شديد جدا |
|
| 2 | Did you cough up phlegm Today? | هل تسعل البلغم اليوم؟ |
| □ No □ Yes |
□ لا □ نعم |
|
| 3 | Did you have breathing problems Today? | هل عانيت من مشاكل في التنفس اليوم؟ |
| □ No □ Mild □ Moderate □ Severe □ Very severe |
□ لا □ خفيف □ معتدل □ شديد □ شديد جدا |
|
| 4 | Did breathing problems interfere with any of your regular activities (Such as working, walking, hobbies, meeting friends, shopping, or family visits) Today? | هل تعارضت مشاكل التنفس مع أي من أنشطتك المعتادة (مثل العمل ، أو المشي ، أو الهوايات ، أو مقابلة الأصدقاء ، أو التسوق ، أو الزيارات العائلية) اليوم؟ |
| □ No □ Mild □ Moderate □ Severe □ Very severe |
□ لا □ خفيف □ معتدل □ شديد □ شديد جدا |
|
| 5 | Have you had any of the symptoms of a cold or flu shown below (such as Runny/stuffy nose, change in phlegm color or stickiness, sore throat, fever, shivers, chest congestion? today? | هل عانيت من أي من أعراض البرد أو الأنفلونزا (مثل سيلان الأنف ، أو تغير في لون البلغم أو اللزوجة ، أو التهاب الحلق ، أو الحمى ، أو الرعشة ، أو احتقان الصدر؟ |
| □ No □ Yes |
□ لا □ نعم |
|
| 6 | Did you increase the frequency of using the respiratory symptoms reliever medication Today? | هل قمت بزيادة تكرار استخدام الدواء المسكن لأعراض الجهاز التنفسي اليوم؟ |
| □ No □ Yes |
□ لا □ نعم |
|
| 7 | Did your oxygen saturation become below 90% Today? | هل أصبحت قراءة التشبع بالأكسجين أقل من 90٪ اليوم؟ |
| □ No □ Yes |
□ لا □ نعم |
|
| 8 | Did you see a healthcare professional Today for breathing problems or a cold? | هل رأيت أخصائي رعاية صحية اليوم لمشاكل في التنفس أو نزلة برد؟ |
| □ No □ Yes |
□ لا □ نعم |
|
| 9 | Is there anything you want the team to contact you about? | هل هناك أي شيء تريد أن يتصل بك الفريق بشأنه؟ |
| □ No □ Yes |
□ لا □ نعم |
|
| When exacerbation was Confirmed | عندما تم تأكيد تفاقم الحالة | |
| 1 | Did you take prednisone Today? | هل تناولت بريدنيزون اليوم؟ |
| □ No □ Yes |
□ لا □ نعم |
|
| 2 | Did you take an antibiotic Today? | هل تناولت المضاد الحيوي اليوم؟ |
| □ No □ Yes |
□ لا □ نعم |
|
| 3 | Do you think your breathing is back to normal Today? | هل تعتقد أن تنفسك وأعراضك عادت إلى طبيعته اليوم؟ |
| □ No □ Yes □ Don’t know |
□ لا □ نعم □ لا أعرف |
Table 3.
The demographic and clinical characteristics of the participants monitored for AECOPD (N = 87).
Table 3.
The demographic and clinical characteristics of the participants monitored for AECOPD (N = 87).
| Participant Descriptions | GOLD I (n = 18), II (n = 42), III (n = 24), IV (n = 3) | |
|---|---|---|
| Age, M (range), y | 59.7 (45-81) | |
| Male / Female | 57 (66) / 30 (34) | |
| Current smokers | 18 (21) | |
| Smoking, median (IQR), pack-y | 44 (40) | |
| BMI, M (SD), kg/m2 | 27.7 (5.4) | |
| Postbronchodilator FEV1% predicted at the baseline, M (SD) | 58.7 (7.5) | |
| ED visit due to breathing difficulties in the previous year | 18 (21) | |
| ≥ 1 hospitalization for breathing difficulties in the previous year | 12 (14) | |
| Participant medications at baseline | ||
| SABA | 57 (66) | |
| SAMA | 3 (3) | |
| SABA + SAMA | 18 (21) | |
| LABA | 3 (3) | |
| LAMA | 18 (21) | |
| LAMA + LABA | 45 (52) | |
| ICS + LABA | 15 (17) | |
| LAMA + ICS + LABA | 6 (7) | |
Data are given as No. (%) of participants unless otherwise specified. “ICS: Inhaled corticosteroids; LABA: Long-acting beta-2 agonist; SABA: short-acting beta-2 agonist; LAMA: Long-acting muscarinic antagonists; OCS: Oral corticosteroids; BMI: body mass index; ED: emergency department; GOLD: Global Initiative for Chronic Obstructive Lung Disease; IQR: interquartile range; M: Mean”.
Table 4.
Descriptions of the participants’ AECOPD.
| Descriptions of AECOPD | GOLD I (n = 9), II (n = 42), III (n = 24), IV (n = 3) | |
|---|---|---|
| AECOPD no. by Anthonisen type | ||
| 1a | 81 (43) | |
| 2 | 60 (32) | |
| 3 | 48 (25) | |
| Total | 189 | |
| AECOPD per participant, No. | ||
| 0 | 3 | |
| 1 | 26 | |
| 2 | 18 | |
| 3 | 11 | |
| ≥ 4 | 8 | |
| AECOPD need any healthcare professional help | 120 (63) | |
| AECOPD required to visit a respiratory specialist | 21 (12) | |
| AECOPD required ED treatment | 18 (10) | |
| AECOPD required hospitalization | 18 (10) | |
| AECOPD lengthb, median (range), days | 9 (2-36) | |
| AECOPD with prednisone prescription, without hospitalization | 78 (41) | |
| AECOPD with an antibiotic prescription, without hospitalization | 120 (63) | |
| The absolute decrease in % predicted FEV1 postbronchodilator at AECOPD from baseline, M (SD) | 5.2 (7.3) | |
| Unresolved AECOPD (no return to normal breathing)b | 6 (3) | |
Data are given as No. (%) unless otherwise specified. a Most severe.b Data included for 187/189 (99%) AECOPD episodes; no return to normal breathing by the end of the study was reported for two patients.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



