
Submitted:
27 August 2024
Posted:
28 August 2024
You are already at the latest version
Abstract
The aim of the study was to investigate the effects of Botox injection therapy, with or without wearing thermoformed occlusal splints, in patients with sleep apnea and nocturnal bruxism and to determine their degree of satisfaction after completing the therapy. The selected patients (n = 36, 24 female and 12 male) with sleep apnea and nocturnal bruxism were divided into two groups. The first group of 18 patients (G1) was treated by injecting Botox (Allergan) into the masseter muscle. The 18 patients in the second group (G2) benefited from associated therapy represented by Botox injections in masseter muscle and the wear of thermoformed occlusal splints. Four monitoring sessions were realized: at baseline, at three weeks, at three months, and at six months after the effectuation of treatments. The associated therapy (Botox and thermoformed occlusal splints) presented much better results over time in decreasing the sleep apnea and nocturnal bruxism symptoms than the one represented only by injections with Botox, but Botox injections presented a rapid relief of both disease signs. Patient satisfaction after the applied treatments was very good, but in patients with associated therapy, it was better after six months than in first-group patients.
Keywords:
sleep apnea
; nocturnal bruxism
; Botox-Allergan
; thermoformed occlusal splints
; patient's satisfaction
1. Introduction
Sleep apnea and bruxism are sleep disorders with multifactorial etiologies, but stress is involved in their etiologies, alongside the presence of acute and chronic diseases.
Sleep apnea, characterized by the breathing stopping when asleep, is associated with a decrease in oxygen saturation in sleep and disturbs the quality and duration of sleep, inducing the apparition of symptoms such as loud and disruptive snoring, gasping for air during sleep, and daytime fatigue [1,2].
The prevalence of sleep disorders has increased in recent decades. According to research realized by Lechner et al. [3], 38% of men and 30.4% of women reported snoring at night; also, 8.7% of men and 5.6% of women declared that they stopped breathing at night [4,5,6].
The specific feature of sleep apnea is represented by recurrent pauses in respiration, which induce intermittent hypoxia, hypercapnia, and oxygen desaturation in the blood, which can suddenly increase the risk of various diseases [9].
Bruxism (teeth grinding) is a parafunctional oral activity. Teeth grinding or clenching during sleep is known as nocturnal bruxism [10,11].
Bruxism is an illness with complex pathology due to various primary or secondary factors (vicious habits such as smoking and/or alcohol/drug abuse, chronic fatigue, insomnia, occlusal imbalances, facial muscle or nerve dysfunctions, anxious states, stress, administration of antidepressants, epilepsy, etc.) [12]. The prevalence of sleep bruxism is between 21 and 30% of the population, and it was noticed that a significant factor in the apparition of sleep bruxism is represented by age and gender (it is more frequent in women) [13,14].
Bruxism can be classified into nocturnal and diurnal/awake bruxism. After severity, bruxism can be mild, moderate, or severe [15,16].
The characteristic symptomatology of moderate nocturnal bruxism manifests itself in the morning and is represented by facial pain, stiffness of the masticatory muscles and temporomandibular joint (TMJ), discomfort when mobilizing the temporomandibular joint, headache, and alteration of the structure of the dental hard tissues [17,18]. This condition can remain undiagnosed until the apparition of local dental lesions (repeated friction of the occlusal surface of the teeth that can induce enamel abrasion, enamel cracks, and carious lesions) and, ulteriorly, the apparition of affections in the orofacial area [19,20].
In establishing the correct diagnosis of moderate sleep apnea and moderate nocturnal bruxism, the important role belongs to the partners of the affected persons, who can signal the characteristic manifestations observed during sleep [21,22].
Sleep apnea and nocturnal bruxism negatively affect sleep quality and patient quality of life [23,24,25].
Botulinum toxin type A (BoNT-A), the purified form of the most strong poison known, is obtained from Clostridium botulinum type A. It is used for stopping the delivery of acetylcholine, and it is used for treating many diseases, like chronic sialorrhea, muscular dystonia, and spasm, but also in cosmetic applications [25,26,27,28,29].
Intraoral dental devices such as occlusal splints or thermoformed mouthpieces are recommended to decrease inappropriate occlusal forces due to nocturnal bruxism. At the same time, by increasing the space between the dental arches in occlusion, occlusal splints can be used to improve the symptoms characteristic of nocturnal apnea [30,31].
The aim of this study was to investigate the effects of Botox injection therapy, with or without wearing thermoformed occlusal splints, on patients with moderate sleep apnea and nocturnal bruxism and to determine the patients’ satisfaction degree after completing the applied treatments.
2. Materials and Methods
The study was realized in conformity with the ethical principles and the good clinical practice of the Helsinki Declaration [32].
The procedures of the study were authorized by the Ethics Committee of the Faculty of Dental Medicine, Titu Maiorescu University in Bucharest (Decision No. 6 of January 14, 2019). The selected patients were properly and individually informed regarding the demands of the study, and they signed the informed consent.
The study was performed between March 2019 and April 2024, but the COVID-19 pandemic conditions caused a 14-month break in research.
2.1. Selection of Patients
All authors attended calibration courses to ensure the accuracy of each patient’s anamnesis, clinical examination, diagnosis, and then similar application of clinical procedures for the reliability of the results.
The presence of sleep apnea and nocturnal bruxism symptoms was assessed by anamnesis, oral examination, and the utilization of questionnaires for the objective and subjective symptoms, and regarding the satisfaction and quality of life related to sleep bruxism and nocturnal bruxism (used at baseline and at the last monitoring session). The complaints that were taken into consideration at anamnesis of sleep apnea and nocturnal bruxism were the morning headache, the facial pain or fatigue, the jaw-muscle fatigue, the teeth grinding or jaw clenching sounds during sleep (related by the family or the sleep partner), and the self-perception of the teeth grinding and/or clenching and of jaw clenching.
The objective symptomatology of bruxism that was observed at intraoral examination was related to unphysiological tooth wear, hypertrophy or hypertonicity of the masticatory muscle bundles, trismus, tongue indentation, and buccal mucosa ridges.
The questionnaire for subjective symptoms to ascertain the patients with sleep apnea and nocturnal bruxism contained seven questions: awakening in the morning with a dry mouth or sore throat; morning pain in masseter muscles; morning fatigue; morning headaches and jaw pain; diurnal difficulty in focusing; excessive daytime sleepiness. This questionnaire was completed by both the patients and their partners.
The selected patients (n = 36, 24 female and 12 male), with moderate sleep apnea and moderate nocturnal bruxism, were divided into two groups. The first group of 18 patients (G1) was treated by injecting Botox (Allergan, AbbVie Ltd., UK) into the masseter muscle. The 18 patients in the second group (G2) benefited from associated therapy represented by injections with Botox and the wear of thermoformed occlusal splints applied to the mandibular dental arch. The sample of patients participating in the study is presented in Table 1.
Inclusion criteria were: male and female patients between 31 and 50 years of age, with good health status; moderate sleep apnea and nocturnal bruxism symptomatology; moderate tooth wear; non-smoker patients; absence of parafunctional habits; confirmed non-allergic patients to used dental materials; the patient’s acceptance to participate in the study with signed informed consent; the possibility of patients to come for the effectuation of treatments and of follow-up sessions.
Exclusion criteria were: Botox allergy; allergy to the materials used for thermoformed occlusal splints; more than two missing teeth in the posterior area of the dental arches; extended prosthetic restorations; adult orthodontic patients; upper respiratory and pulmonary disorders; heart disease; simulators; infections; systemic disorders/diseases; pregnancy; lactation; antipsychotic or/and psychotropic treatments; patients with mental disabilities; uncooperative patients.
The flow diagram of the study is presented in Figure 1.
2.2. Performing Botox-Allergan Injections
Prior to beginning the therapies, a Botox allergy test was performed on each patient.
Botox (Allergan) powder (vacuum-dried Clostridium botulinum type A toxin) was solubilized and diluted under sterile conditions (in conformity with the manufacturer’s instructions) with 2.5 mL of bacteriostatic 0.9% Sodium chlorine per 100 units of Botox powder. Aespio fine micro-syringes and BD Microlance 3 needles were used for administration of the treatment with Botox (Figure 2). The points of injection were noted after careful palpation of the temporomandibular area. In addition, measurements were made to ensure the accurate localization of each muscle bundle. A skin marker was used to map the injection points to ensure precision and reduce the risk of asymmetry. All patients were asked to clench their jaws so the masseter muscle could be identified more easily. The angle and the edge of the mandible were drawn. After measuring the drawing lines of the sides of the masseter muscle, the final draw was at least 1 cm lower than the edge of the masseter. In general, the focus was on the lower part of the masseter muscle. 5 units of Botox solution were injected at 5 points on the masseters, at a distance of 1 cm between them and 1 cm from the previously drawn edges, in order to limit the possibility of affecting other muscles. The masseter muscle is a very strong muscle and needs much larger amounts of Botox than other muscles of the face. An entire ampoule of 50 units was used for the first treatment. After 3 weeks from the first treatment, the patients were recalled to verify their progress. During monitoring, after obtaining the results, if it was necessary, another 50 units of Botox were injected, but these cases were exceptions. The next assessments were after three and six months. The Botox injection sites used in the study are presented in Figure 3.
Always, bilateral Botox injections were performed, even if one side of the masseter muscle was stronger or more developed than the other. At baseline, the same amount of Botox was injected on both sides. At the first follow-up (performed after three weeks), a different quantity of Botox was injected on one side compared to the other, as needed. After these three weeks, there was a pause in the injection of Botox in order to observe how the treatment of sleep apnea and nocturnal bruxism evolves. After the last monitoring session, Botox injections were administered as needed, between one and two injections per six months, according to the faster or slower metabolism of the patients.
In order to relieve the errors and realize good investigations, objective appreciations, measurements, and treatment, all the patient’s images were captured with the “ImageJ” and “OBSERV 520” systems and preserved on “Consentz” software for the encrypted storage of patients’ data.
2.3. Manufacturing the Thermoformed Occlusal Splints
The thermoformed occlusal splints used in this study covered the mandibular dental arch in totality and were manufactured by the thermo- and vacuum processes. The hard layer of Erkoloc-Pro sheet is made of polyethylene terephthalate glycol, and the soft layer is made of a thermoplastic polyurethane. The manufacturing was done by vacuuming the softened Erkoloc-Pro sheet at approximately 130°C on the model of hard plaster located in the Erkoform-3d+ thermoforming device (Erkodent-Erich Kopp GmbH, Pfalzgrafenweiler, Germany) [33]. After obtaining by vacuum and pression the specific shape of the thermoformed occlusal splints, they were processed, finished, and polished.
Thermoformed occlusal splints were distributed to the patients of the second group (G2) at baseline. These patients continued to wear the thermoformed occlusal splints even after the last assessment (six months).
2.4. Questionnaires Regarding the Symptomatology and the Satisfaction of Patients
Four assessments were performed (at baseline and then at three weeks, three months, and six months) to determine the presence of objective and subjective symptoms.
The objective symptoms were represented by the presence of signs of contraction in the temporal and masseter muscle bundles (hypertrophy or hypertonicity), trismus, tongue indentation, and buccal mucosa ridges.
To find out the existence of sleep apnea and nocturnal bruxism in the patients, a seven-question questionnaire was designed. These questions regarding subjective symptoms were necessary for the correct selection of patients in this study. Responses were presented in five grades: never (=strongly disagree), rarely (=disagree), sometimes (=not sure), usually (=agree), and always (=strongly agree), and were completed by the patients and by their bed partners (roommates). These questions were related to: awakening in the morning with a dry mouth or sore throat; morning pain in the masseter muscle; morning fatigue; morning headaches; jaw pains; diurnal (daytime) difficulty in focusing; excessive daytime sleepiness.
To reveal the satisfaction and quality of patients’ lives relating to the outcomes of applied treatments, a ten-question questionnaire was designed. Responses were presented in five grades: very dissatisfied, quite dissatisfied, neither satisfied nor dissatisfied, quite satisfied, and very satisfied. The used questions were: How satisfied are you now with your sleep?; How satisfied are you now with your absence of contractions at bundle level in masseter muscle? How satisfied are you now with your ability to perform your daily living activities? How satisfied are you now with your capacity for work?; How satisfied are you with your actual condition of concentration?; How satisfied are you with the applied therapy?; How satisfied are you now with your oral health?; How satisfied are you now with yourself? How do you evaluate your quality of life now?.
Figure 4 presents the visit schedule.
3. Results
At all four assessment sessions, both groups of patients (G1 and G2) exhibited relief of discomfort in sleep apnea and nocturnal bruxism in comparison with baseline.
The therapy with Botox injections produced adequate results, especially in the second group of patients (G2) (Figure 5).
During the monitoring period, in all assessment sessions, it was noticed that all the investigated symptomatology’s decreased in intensity.
Table 2 presents the results regarding the studied objective symptoms, noted at baseline and at the last follow-up session.
It can be observed that, if initially the investigated objective symptomatology was present in all patients from both research groups (G1 and G2), at the last evaluation session (performed at six months), no patient presented any of those objective symptoms.
The answers received from the patients and their bed partners to the questionnaire used for the subjective symptomatology of sleep apnea and nocturnal bruxism and filled out at baseline are presented in Table 3 (where never=strongly disagree; rarely=disagree; sometimes=not sure; usually=agree; always=strongly agree).
Table 4 presents the answers received at the last assessment from the patients and their bed partners to the questionnaire about the subjective symptoms of sleep apnea and nocturnal bruxism.
It can be observed that the subjective symptomatology investigated at baseline was present in all patients from both research groups and in all patients’ bed partners. It is visible that the higher frequency was in answers with “sometimes” (not sure), “usually” (agree), and “always” (strongly agree) grades. At the last assessment (at six months), all the patients of the two investigated groups and all their bed partners had the highest frequency of subjective symptomatology noted with “never”, and the qualifiers “usually” (agree) and “always” (strongly agree) had the value 0 (=0%).
It should be mentioned that, at the second and third evaluation sessions (performed at three weeks and three months), all the noted values were situated between those of Table 2 and Table 4. These values were decreasing from “always” (=strongly agree) to “rarely” (disagree) and “never” (=strongly disagree) at the second and third evaluation sessions.
Table 5 presents the satisfaction degree in patients’ life quality after the applied treatments, noted in both groups of patients (G1: n=18, and G2: n=18) at baseline (B) and at the fourth (last) follow-up session (LFu).
It should be underlined that the first group of patients did not wear thermoformed occlusal splints.
The associated treatment with Botox injection and occlusal splints presented immediate results with good effects, and the patients declared that they were very satisfied with the obtained results. After the finalization of applied treatments, the filled-out questionnaires regarding the satisfaction of patients revealed that their life quality had greatly improved. Also, by studying Table 2, Table 3, Table 4 and Table 5, it can be observed that the quality and well-being level of life of patients were greatly increased in both groups.
The results of this study regarding the therapy with Botox and occlusal splints for moderate sleep apnea and nocturnal bruxism show that these types of treatments are non-invasive, reliable, facile to accomplish, reversible, comfortable, and effortlessly accepted by patients.
4. Discussion
Sleep apnea and nocturnal bruxism belong to sleep disorders. These conditions can represent risk factors associated with specific clinical manifestations that affect the quality of life; therefore, it is very important that these disorders are treated [34]. Among the causes that can induce sleep disorders are depression, anxiety, constant stress, changing the time zone, various diseases (heart, stomach, kidney, or lung diseases), taking drugs that cause insomnia or drowsiness, environmental changes, aging, etc. [35].
Bruxism is an illness with complex pathology due to various primary or secondary factors (vicious habits such as smoking and/or alcohol/drug abuse, chronic fatigue, insomnia, occlusal imbalances, facial muscle or nerve dysfunctions, anxious states, stress, administration of antidepressants, epilepsy, etc.) [36,37].
Lobbezoo et al. [38] reported that sleep (nocturnal) bruxism is a masticatory muscle activity that occurs in sleep, and it can be distinguished as rhythmic or non-rhythmic. In healthy people, bruxism should not be considered a disorder but a behavior that may present a risk or protective factor in some particular clinical cases.
Shivamurthy et al. [39] consider that one of the predisposing factors for the development of temporomandibular disorders (which include bruxism) could be represented by stress, so screening performed at a young age could aid in the prevention and progression of the disease.
In accordance with many studies, botulinum toxin type A has proven its effectiveness in various therapies, but only when applied accurately [40,41,42,43,44].
In conformity with the review conducted by Li et al. [45], the therapy with Botox represents a reliable and efficient therapy in decreasing the pain intensity and ameliorating the functional movements of the masticatory muscles and temporomandibular joints in patients with temporomandibular dysfunctions. They consider that the dose of 60–100 U injected bilaterally can represent a beneficial solution for treating the pain that appeared due to temporomandibular dysfunctions. The rigidity of the masticatory muscles is decreased by injections with Botox, and the stiffness of the temporalis muscles is improved. Due to the modification of masseter muscle function, changes appear in the other masticatory muscles too, which are favorable in offering functional and cosmetic outcomes. All this is achieved by the simultaneous evaluation and treatment of all the masticatory muscles, including the temporalis muscle [46].
According to Yağci et al. [47], the risk of bruxism is higher in depressed patients, those with poor quality of sleep, and those with shockingly childish experiences.
Masseter muscle, although it is the strongest muscle in the human body, does not need to be weakened too much by injecting Botox, because it can lead to difficulties in the patient’s mastication, which negatively affects their functionality and quality of life [48,49]. Fortunately, any Botox treatment is completely reversible, and the muscles return to normal after a period of several months [50,51].
The benefits mechanisms offered by the occlusal splints are not yet obvious [52], but the study conducted by Bergmann et al. [53] confirms the efficiency and safety of the use of occlusal splints in the treatment of sleep bruxism.
In their study, Albagieh et al. [54] concluded that occlusal splints can be used for the treatment of extensive variants of temporomandibular disorders (TMDs), as well as bruxism, headaches, reduced vertical dimension of occlusion, and so on, but there are no evident proofs that the treatment with occlusal splints is better than physiotherapy in the treatment of TMDs.
After the review realized by Duarte et al. [55], at the moment there is not adequate scientific evidence to advocate or infirm the existence of a link between sleep, bruxism, and quality of life in the general population.
In their study, Mercan Başpınar et al. [25] observed that decreased oral health in relation to the quality of life and low sleep quality would be expected in the presence of nocturnal bruxism. They underlined the fact that the patients may not be aware of their situation until it is clearly presented by a dentist.
The ideal treatment options for sleep apnea and nocturnal bruxism are represented by the multidisciplinary approaches [47]. Because the etiology of bruxism is multifactorial, interdisciplinary collaboration is necessary to increase the success rate of treatment [56].
The systematic review effectuated by Ferrillo [57] indicates that a multidisciplinary approach involving rehabilitation dentistry, physical medicine, as well as psychology is compulsory for the suitable diagnosis and treatment of patients with sleep disorders.
The clinical relevance of this preliminary study is given by the favorable results obtained in the therapy with Botox and thermoformed occlusal splints for moderate sleep apnea and nocturnal bruxism.
The limitations of this preliminary study are due to the limited number of patients in the study groups, the short time interval of the monitoring, and the lack of statistical analyses.
5. Conclusions
Associated therapy of sleep apnea and bruxism with Botox and thermoformed occlusal splints represented a reliable and efficacious treatment for decreasing the specific symptomatology. Also, the results of the study demonstrated that the applied therapies improved patient satisfaction and quality of life.
Associated therapy of sleep apnea and bruxism with Botox and thermoformed occlusal splints represented a reliable and efficacious treatment for decreasing the specific symptomatology. Also, the results of the study demonstrated that the applied therapies improved patient satisfaction and quality of life.
Sleep apnea and nocturnal bruxism have significant implications for the health status, financial condition, and life satisfaction of those affected, so these conditions require a personalized approach to both diagnosis and management Future studies with larger cohorts of patients with moderate sleep apnea and nocturnal bruxism are needed.
In addition, the study of the cumulative action of factors such as gender, ages, smoking, alcohol and caffeine consumption, and consumption of drugs and addictive substances can complete the interpretation of previous studies and working hypotheses.
Author Contributions
Conceptualization, Anamaria Bechir and Edwin Sever Bechir; Data curation, Andrada Camelia Nicolau and Edwin Sever Bechir; Formal analysis, Anamaria Bechir and Edwin Sever Bechir; Investigation, Talaat Gabriel Rezk Gavrilă, Anamaria Bechir, Andrada Camelia Nicolau and Edwin Sever Bechir; Methodology, Talaat Gabriel Rezk Gavrilă and Andrada Camelia Nicolau; Project administration, Edwin Sever Bechir; Resources, Anamaria Bechir and Edwin Sever Bechir; Software, Talaat Gabriel Rezk Gavrilă and Edwin Sever Bechir; Supervision, Talaat Gabriel Rezk Gavrilă and Anamaria Bechir; Validation, Talaat Gabriel Rezk Gavrilă, Anamaria Bechir and Andrada Camelia Nicolau; Visualization, Anamaria Bechir and Andrada Camelia Nicolau; Writing—original draft, Talaat Gabriel Rezk Gavrilă and Anamaria Bechir; Writing—review & editing, Talaat Gabriel Rezk Gavrilă, Andrada Camelia Nicolau and Edwin Sever Bechir. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was realized in conformity with the ethical principles and the good clinical practice of the Helsinki Declaration [32]. The procedures of the study were authorized by the Ethics Committee of the Faculty of Dental Medicine, Titu Maiorescu University in Bucharest (Decision No. 6 of January 14, 2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study, and written informed consent has been obtained from the patients to publish this paper.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Cumpston, E., Chen, P. Sleep Apnea Syndrome. [Updated 2023 Sep 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available online: https://www.ncbi.nlm.nih.gov/books/NBK564431/ (accessed on February 2024).
- Slowik, J.M., Sankari, A., Collen, J.F. Obstructive Sleep Apnea. [Updated 2024 Mar 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459252/ (accessed on February 2024).
- Lechner, M., Breeze, C.E., Ohayon, M.M., Kotecha, B. Snoring and breathing pauses during sleep: interview survey of a United Kingdom population sample reveals a significant increase in the rates of sleep apnoea and obesity over the last 20 years—data from the UK sleep survey. Sleep Med. 2019, 54, 250-256. [CrossRef]
- Borsini, E., Noguiera, F., Nigro, C. Apnea-hypopnea index in sleep studies and the risk of over-simplification. Sleep Science, 2018, 11, 1, 45–48. [CrossRef]
- Abbasi, A., Gupta, S.S., Sabharwal, N., Meghrajani, V., Sharma, S., Kamholz, S., Kupfer, Y. A comprehensive review of obstructive sleep apnea. Sleep Sci. 2021, 14, 2, 142-154. [CrossRef]
- Leigh, C., Faigenblum, M., Fine, P., Blizard, R., Leung, A. General dental practitioners’ knowledge and opinions of snoring and sleep-related breathing disorders. Br Dent J. 2021, 1, 9, 569-574. [CrossRef]
- Ayalew, M.P., Nemomssa, H.D., Simegn, G.L. Sleep apnea syndrome detection and classification of severity level from ECG and SpO2 signals. Health Technol 2021, 5, 13. [CrossRef]
- Kazubowska-Machnowska, K., Jodkowskam, A., Michalek-Zrabkowska, M., Wieckiewicz, M., Poreba, R., Dominiak, M., Gac, P., Mazur, G., Kanclerska, J., Martynowicz, H. The Effect of Severity of Obstructive Sleep Apnea on Sleep Bruxism in Respiratory Polygraphy Study. Brain Sci. 2022,12, 7, 828. [CrossRef]
- Lv, R., Liu, X., Zhang, Y. et al. Pathophysiological mechanisms and therapeutic approaches in obstructive sleep apnea syndrome. Sig Transduct Target Ther 2023, 8, 218. [CrossRef]
- Available online: https://www.sleepfoundation.org/bruxism.
- Craciun, A.E., Cerghizan, D., Popsor, S., Bica, C. Bruxism in Children and Adolescents and its Association with Some Possible Aetiological Factors. Curr Health Sci J. 2023, 49, 2, 257-262. [CrossRef]
- Golanska, P.; Saczuk, K.; Domarecka, M.; Kuć, J.; Lukomska-Szymanska, M. Temporomandibular Myofascial Pain Syndrome—Aetiology and Biopsychosocial Modulation. A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 15, 7807. [CrossRef]
- Osses-Anguita, Á.E.; Sánchez-Sánchez, T.; Soto-Goñi, X.A.; García-González, M.; Alén Fariñas, F.; Cid-Verdejo, R.; Sánchez Romero, E.A.; Jiménez-Ortega, L. Awake and Sleep Bruxism Prevalence and Their Associated Psychological Factors in First-Year University Students: A Pre-Mid-Post COVID-19 Pandemic Comparison. Int. J. Environ. Res. Public Health 2023, 20, 3, 2452. [CrossRef]
- Zieliński, G.; Pająk, A.; Wójcicki, M. Global Prevalence of Sleep Bruxism and Awake Bruxism in Pediatric and Adult Populations: A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 14, 4259. [CrossRef]
- Balasubramaniam, R., Paesani, D., Koyano, K., Tsukiyama, Y., Carra, M.C., Lavigne, G.J. Sleep Bruxism. In: Farah, C., Balasubramaniam, R., McCullough, M. Contemporary Oral Medicine. 2019, Springer, Cham. [CrossRef]
- Available online: https://www.bruxism.org.uk/what-is-bruxism.php.
- Ohlmann, B., Waldecker, M., Leckelm M., Bömicke, W., Behnisch, R., Rammelsberg, P., Schmitter, M., Correlations between Sleep Bruxism and Temporomandibular Disorders. J Clin Med. 2020, 9, 2, 611. [CrossRef]
- Iacob, S.M., Chisnoiu, A.M., Objelean, A., Fluerașu, M.I., Moga, R.R., Buduru, S.D. Correlation between bruxism, occlusal dysfunction and musculo-articular status, Romanian Journal of Oral Rehabilitation 2022, 14, 3, 48-55.
- Wetselaar, P., Vermaire, E.J.H., Lobbezoo, F., Schuller, A.A. The prevalence of awake bruxism and sleep bruxism in the Dutch adult population. J Oral Rehabil. 2019, 46, 7, 617-623. [CrossRef]
- Thayer, M.L.T., Ali, R. The dental demolition derby: bruxism and its impact—part 1: background. Br Dent J. 2022; 232, 8, 515-521. [CrossRef]
- Thomas, D.C., Patel, J., Kumar, S.S., Dakshinamoorthy, J., Greenstein, Y.,Kamalam Ravindran, H., Kodaganallur Pitchumani, P. Sleep related bruxism—comprehensive review of the literature based on a rare case presentation, Frontiers of Oral and Maxillofacial Medicine, 2024, 6, 3, 1-14. Available online: https://fomm.amegroups.org/article/view/67995.
- Available online: https://www.sleepfoundation.org/sleep-apnea/link-between-sleep-apnea-and-teeth-grinding.
- Özsoy, H.E., Gaş, S., Aydın, K.C. The Relationship between Stress Levels, Sleep Quality, and Oral Health-related Quality of Life in Turkish University Students with Self-reported Bruxism. J Turk Sleep Med. 2022, 9, 1, 64-72. [CrossRef]
- Colonna, A., Manfredini, D. Bruxism: An orthodontist’s perspective, Seminars in Orthodontics, 2024, 30, 3, 318-324. [CrossRef]
- Mercan Başpınar, M., Mercan, Ç., Mercan, M., Arslan Aras, M. Comparison of the Oral Health-Related Quality of Life, Sleep Quality, and Oral Health Literacy in Sleep and Awake Bruxism: Results from Family Medicine Practice. Int J Clin Pract. 2023, 30, 2023, 1186278. [CrossRef]
- Available online: https://go.drugbank.com/drugs/DB00083.
- Rasetti-Escargueil, C.; Palea, S. Embracing the Versatility of Botulinum Neurotoxins in Conventional and New Therapeutic Applications. Toxins 2024, 16, 261. [CrossRef]
- Park, M.Y., Ahn, K.Y. Scientific review of the aesthetic uses of botulinum toxin type A. Arch Craniofac Surg. 2021, 22, 1, 1-10. [CrossRef]
- Brin, M.F., Burstein, R. Botox (onabotulinumtoxinA) mechanism of action. Medicine (Baltimore). 2023, 102, S1, e32372. [CrossRef]
- Bechir, E.S., Bechir, A., Arghir, O.A., Ciavoi, G., Gioga, C., Curt Mola, F., Dascalu, I.T. Results in the Use of Two Types of Polymeric Appliances in the Therapy of Some Mild Sleep Apnea Simptoms, Rev. Mat. Plastice Bucuresti, 2017, 54, 2, 304-308. Available online: http://www.revmaterialeplastice.ro/archive.asp.
- Costăchel, B.C.; Bechir, A.; Burcea, A.; Mihai, L.L.; Ionescu, T.; Marcu, O.A.; Bechir, E.S. Evaluation of Abfraction Lesions Restored with Three Dental Materials: A Comparative Study. Clin. Pract. 2023, 13, 1043–1058. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.verywellhealth.com/declaration-of-helsinki-4846525.
- Available online: https://ndsonline.co.uk/products/proform-3mm-dual-laminate-blanks-erkodent.
- González, A., Montero, J., Gómez Polo, C. Sleep Apnea-Hypopnea Syndrome and Sleep Bruxism: A Systematic Review. J Clin Med. 2023, 23, 12, 3, 910. [CrossRef]
- Merrill, R.M., Ashton, M.K., Angell, E. Sleep disorders related to index and comorbid mental disorders and psychotropic drugs. Ann Gen Psychiatry. 2023, 22, 1, 23. [CrossRef]
- Cervantes-Chavarría, A.R., Utsman-Abarca, R., Herrero-Babiloni, A.. Bruxism an issue between the myths and fact. Odovtos International Journal of Dental Sciences, 2022, 24, 3, 15-21. [CrossRef]
- Vlăduțu, D.E.; Ionescu, M.; Mercuț, R.; Noveri, L.; Lăzărescu, G.; Popescu, S.M.; Scrieciu, M.; Manolea, H.O.; Iacov Crăițoiu, M.M.; Ionescu, A.G.; Mercuț, V. Ecological Momentary Assessment of Masseter Muscle Activity in Patients with Bruxism. Int. J. Environ. Res. Public Health 2023, 20, 1, 581. [CrossRef]
- Lobbezoo F, Ahlberg J, Raphael KG, Wetselaar P, Glaros AG, Kato T, Santiago V, Winocur E, De Laat A, De Leeuw R, Koyano K, Lavigne GJ, Svensson P, Manfredini D. International consensus on the assessment of bruxism: Report of a work in progress. J Oral Rehabil. 2018, 45, 11, 837-844. [CrossRef]
- Shivamurthy, P.G., Kumari, N., Sadaf, A., Meghana, M.B., Azhar, H., Sabrish, S. Use of Fonseca’s Questionnaire to assess the prevalence and severity of Temporomandibular disorders among university students—a cross sectional study. Dentistry 3000. 2022, 10, 1, a001. [CrossRef]
- Witmanowski, H., Błochowiak, K. The whole truth about botulinum toxin—a review. Postepy Dermatol Alergol. 2020, 37, 6, 853-861. [CrossRef]
- Dickison, C., Leggit, J.C. Botulinum toxin for chronic pain: What’s on the horizon? J Fam Pract. 2021, 70, 9, 442-449. [CrossRef]
- Abbas, R.H., Koshy, R.R., Fathima, Y., Weerasekara, R.A., Sherin, Z., Selvakumar, N., Korrapati, N.H. The clinical approach to botulinum toxin in dermatology: A literature review. CosmoDerma 2023, 3, 58, 1-8. [CrossRef]
- Malcangi, G.; Patano, A.; Pezzolla, C.; Riccaldo, L.; Mancini, A.; Di Pede, C.; Inchingolo, A.D.; Inchingolo, F.; Bordea, I.R.; Dipalma, G.; Inchingolo, A.M.. Bruxism and Botulinum Injection: Challenges and Insights. J. Clin. Med. 2023, 12, 4586. [CrossRef]
- Ângelo, D.F.; Sanz, D.; Maffia, F.; Cardoso, H.J. Outcomes of IncobotulinumtoxinA Injection on Myalgia and Arthralgia in Patients Undergoing Temporomandibular Joint Arthroscopy: A Randomized Controlled Trial. Toxins 2023, 15, 376. [Google Scholar] [CrossRef] [PubMed]
- Li, K., Tan, K., Yacovelli, A., Bi, W.G. Effect of botulinum toxin type A on muscular temporomandibular disorder: A systematic review and meta-analysis of randomized controlled trials. J Oral Rehabil.2024, 51, 886-897. [CrossRef]
- Mierzwa, D., Olchowy, C., Olchowy, A., Nawrot-Hadzik, I., Dąbrowski, P., Chobotow, S., Grzech-Leśniak, K., Kubasiewicz-Ross, P., Dominiak, M. Botox Therapy for Hypertrophy of the Masseter Muscle Causes a Compensatory Increase of Stiffness of Other Muscles of Masticatory Apparatus. Life (Basel). 2022 12, 6, 840. [CrossRef]
- Yağci, İ., Taşdelen, Y., Kivrak, Y. Childhood Trauma, Quality of Life, Sleep Quality, Anxiety and Depression Levels in People with Bruxism. Noro Psikiyatr Ars. 2020, 57, 2, 131-135. [CrossRef]
- Chirico, F.; Bove, P.; Fragola, R.; Cosenza, A.; De Falco, N.; Lo Giudice, G.; Audino, G.; Rauso, G.M. Biphasic Injection for Masseter Muscle Reduction with Botulinum Toxin. Appl. Sci. 2021, 11, 6478. [CrossRef]
- Corcoran, N.M., Goldman, E.M. Anatomy, Head and Neck, Masseter Muscle. [Updated 2023 Jun 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available online: https://www.ncbi.nlm.nih.gov/books/NBK539869/.
- Rathod, N.N., John, R.S. Botulinum Toxin Injection for Masseteric Hypertrophy Using 6 Point Injection Technique—A Case Report. Proposal of a Clinical Technique to Quantify Prognosis. Clin Cosmet Investig Dent. 2023, 15, 45-49. [CrossRef]
- Blanco-Rueda, J.A., López-Valverde, A., Márquez-Vera, A., Méndez-Sánchez, R., López-García, E., López-Valverde, N. Preliminary Findings of the Efficacy of Botulinum Toxin in Temporomandibular Disorders: Uncontrolled Pilot Study. Life (Basel). 2023, 13, 2, 345. [CrossRef]
- Jagger, R., King, E. Occlusal Splints for Bruxing and TMD—A Balanced Approach?, Restorative Dentistry, Dent Update 2018, 45, 912–918. [CrossRef]
- Bergmann, A., Edelhoff, D., Schubert, O., Erdelt, K.J., Pho Duc, J.M. Effect of treatment with a full-occlusion biofeedback splint on sleep bruxism and TMD pain: a randomized controlled clinical trial. Clin Oral Investig. 2020, 24, 11, 4005-4018. [CrossRef]
- Albagieh, H., Alomran, I., Binakresh, A., Alhatarisha, N., Almeteb, M., Khalaf, Y., Alqublan, A., Alqahatany, M. Occlusal splints-types and effectiveness in temporomandibular disorder management. Saudi Dent J. 2023, 35, 1, 70-79. [CrossRef]
- Duarte, J., Pauletto, P., Massignan, C., Bolan, M., Domingos, F.L., Curi Hallal, A.L., De Luca Canto, G. Association between Sleep Bruxism and Quality of Life: A Systematic Review. Journal of Oral & Facial Pain and Headache. 2020. 34, 4, 341-352. [CrossRef]
- Mercan Başpınar, M., Mercan, Ç., Mercan, M., Arslan Aras, M. Comparison of the Oral Health-Related Quality of Life, Sleep Quality, and Oral Health Literacy in Sleep and Awake Bruxism: Results from Family Medicine Practice. Int J Clin Pract. 2023, 30, 2023, 1186278. [CrossRef]
- Lal, S.J., Sankari, A., Weber, K.K. Bruxism Management. [Updated 2024 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available online: https://www.ncbi.nlm.nih.gov/books/NBK482466/.
- Ferrillo, M.; Ammendolia, A.; Paduano, S.; Calafiore, D.; Marotta, N.; Migliario, M.; Fortunato, L.; Giudice, A.; Michelotti, A.; de Sire, A. Efficacy of rehabilitation on reducing pain in muscle-related temporomandibular disorders: A systematic review and meta-analysis of randomized controlled trials. J. Back Musculoskelet. Rehabil. 2022, 35, 921–936. [CrossRef]
Figure 1.
The flow chart of the study.
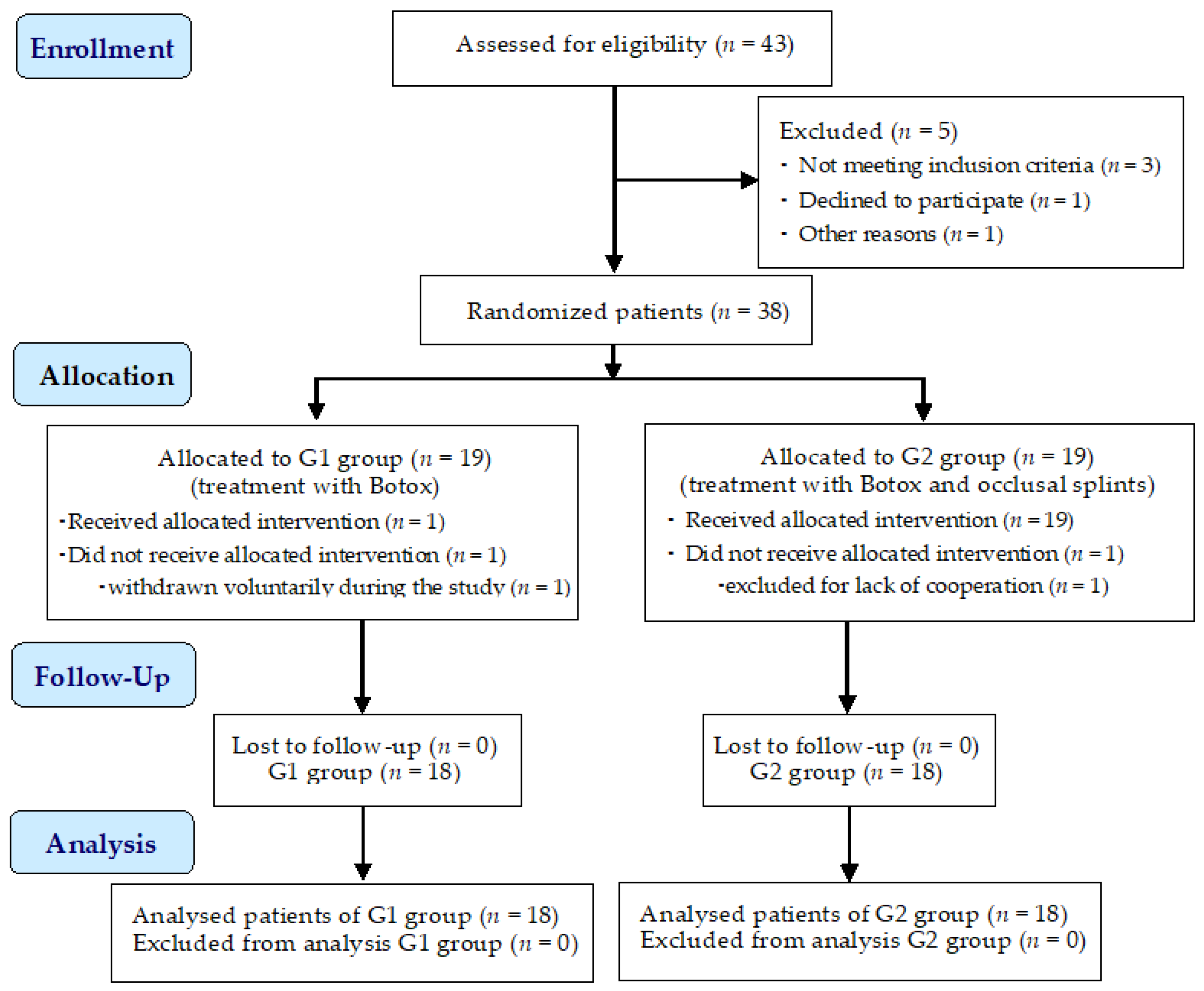
Figure 2.
Presentation of: a. Botox powder; b. Sodium chlorine solution; c. Aespio fine micro syringe; d. BD Microlance needles.
Figure 2.
Presentation of: a. Botox powder; b. Sodium chlorine solution; c. Aespio fine micro syringe; d. BD Microlance needles.
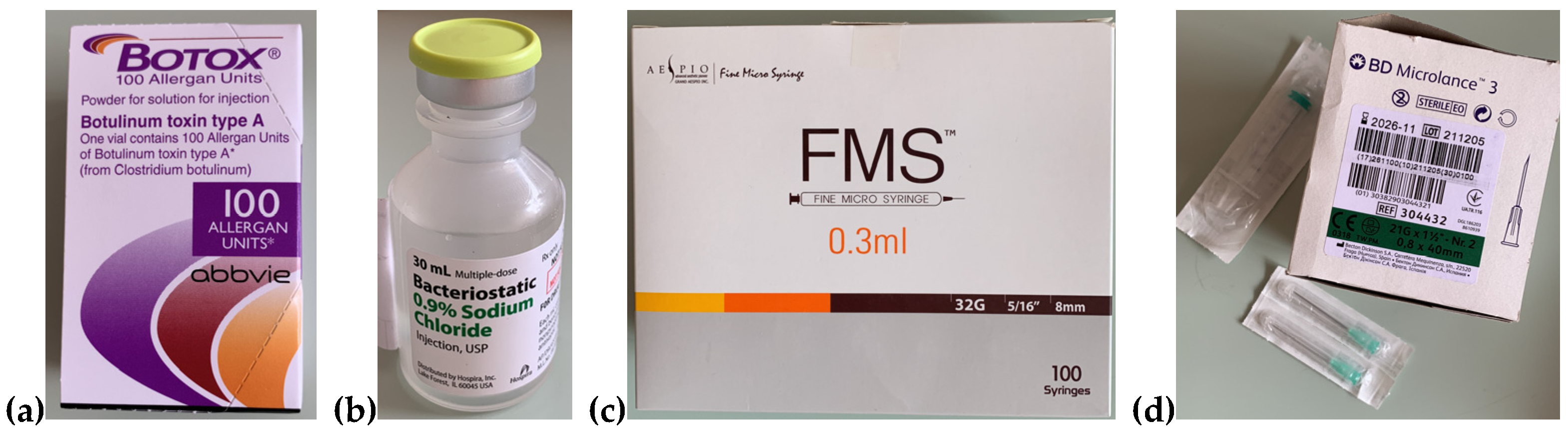
Figure 3.
The Botox injection sites used in the study.

Figure 4.
Visit schedule.

Figure 5.
Aspect of a female patient belonging to the G2 group, at baseline (left) and at the fourth assessment (right), after the injection with Botox and wearing of thermoformed occlusal splint.
Figure 5.
Aspect of a female patient belonging to the G2 group, at baseline (left) and at the fourth assessment (right), after the injection with Botox and wearing of thermoformed occlusal splint.


Table 1.
Sample of the patients participating in the study.
| All patients | Group 1 (G1) | Group 2 (G2) | |
|---|---|---|---|
| No of patients | 36 | 18 | 18 |
| Age (mean ± years) | 31-50 year | Male Female |
33-50 (mean 41,5 ± 8.5) 31-48 (mean 39.5 ± 8.5) |
| Gender M/F | Male 12 (34%) | 6 (33.33%) | 6 (33.33%) |
| Female 24 (66%) | 12 (66.66%) | 12 (66.66%) |
Table 2.
The results regarding the studied objective symptoms, noted at baseline and at the last follow-up session.
Table 2.
The results regarding the studied objective symptoms, noted at baseline and at the last follow-up session.
| Objective symptom | Patients group | Baseline | Lastfollow-up session | |||
| Present | Absent | Present | Absent | |||
| 1. | Contraction of the temporal muscle bundles | G1 | 18 (100%) | 0 (0%) | 0 (0%) | 18 (100%) |
| G2 | 18 (100%) | 0 (0%) | 0 (0%) | 18 (100%) | ||
| 2. | Contraction of the masseter muscle bundles | G1 | 18 (100%) | 0 (0%) | 0 (0%) | 18 (100%) |
| G2 | 18 (100%) | 0 (0%) | 0 (0%) | 18 (100%) | ||
| 3. | Trismus | G1 | 18 (100%) | 0 (0%) | 0 (0%) | 18 (100%) |
| G2 | 18 (100%) | 0 (0%) | 0 (0%) | 18 (100%) | ||
| 4. | Tongue indentation | G1 | 18 (100%) | 0 (0%) | 0 (0%) | 18 (100%) |
| G2 | 18 (100%) | 0 (0%) | 0 (0%) | 18 (100%) | ||
| 5. | Buccal mucosa ridges | G1 | 18 (100%) | 0 (0%) | 0 (0%) | 18 (100%) |
| G2 | 18 (100%) | 0 (0%) | 0 (0%) | 18 (100%) | ||
Table 3.
Questionnaire for the patients and their bed partners about subjective symptoms: responses at baseline.
Table 3.
Questionnaire for the patients and their bed partners about subjective symptoms: responses at baseline.
| Questions addressed to patients (n = 36) | Responses | Questions addressed to patients’ bed partner’s (n = 36) | Responses | ||
|---|---|---|---|---|---|
|
Sleep disruption (episodes of stopping breathing) |
never | 3 (=8.33%) |
Sleep disruption (episodes of stopping breathing) |
never | 0 (=0%) |
| rarely | 11 (=30.55%) | rarely | 1 (=2.77%) | ||
| sometimes | 5 (=13.88%) | sometimes | 2 (=5.55%) | ||
| usually | 11 (=30.55%) | usually | 4 (=11.11%) | ||
| always | 6 (=16.66%) | always | 29 (=80.55%) | ||
| Nocturnal bruxism (teeth grinding or clenching) | never | 0 (=0%) | Nocturnal bruxism (teeth grinding or clenching) |
never | 1 (=2.77%) |
| rarely | 1 (=2.77%) | rarely | 3 (=8.33%) | ||
| sometimes | 6 (=16.66%) | sometimes | 6 (=16.66%) | ||
| usually | 9 (=25.0%) | usually | 12 (=33.33%) | ||
| always | 20 (=55.55%) | always | 14 (=38.88%) | ||
| Awakening in the morning with a dry mouth or sore throat | never | 0 (=0%) | Snoring | never | 0 (=0%) |
| rarely | 4 (=11.11%) | rarely | 2 (=5.55%) | ||
| sometimes | 7 (=19.44%) | sometimes | 13 (=36.11%) | ||
| usually | 12 (=33.33%) | usually | 12 (=33.33%) | ||
| always | 13 (=36.11%) | always | 9 (=25.0%) | ||
| Morning pain in the masseter muscle | never | 0 (=0%) | Waking during the night and gasping or choking | never | 0 (=0%) |
| rarely | 3 (=8.33%) | rarely | 4 (=11.11%) | ||
| sometimes | 4 (=11.11%) | sometimes | 5 (=13.88%) | ||
| usually | 9 (=25.0%) | usually | 19 (=52.77%) | ||
| always | 20 (=55.55%) | always | 8 (=22.22%) | ||
| Morning fatigue, headaches, and jaw pain |
never | 0 (=0%) | Mood changes (e.g., depressive or irritable) |
never | 3 (=8.33%) |
| rarely | 5 (=13.88%) | rarely | 9 (=25.0%) | ||
| sometimes | 8 (=22.22%) | sometimes | 8 (=22.22%) | ||
| usually | 12 (=33.33%) | usually | 9 (=25.0%) | ||
| always | 11 (=30.55%) | always | 7 (=19.44%) | ||
| Diurnal (daytime) difficulty in focusing |
never | 0 (=0%) | Diurnal (daytime) difficulty in focusing |
never | 1 (=2.77%) |
| rarely | 1 (=2.77%) | rarely | 3 (=8.33%) | ||
| sometimes | 12 (=33.33%) | sometimes | 5 (=13.88%) | ||
| usually | 12 (=33.33%) | usually | 16 (=44.44%) | ||
| always | 11 (=30.55%) | always | 12 (=33.33%) | ||
| Excessive daytime sleepiness | never | 1 (=2.77%) | Excessive daytime sleepiness | never | 6 (=16.66%) |
| rarely | 8 (=22.22%) | rarely | 6 (=16.66%) | ||
| sometimes | 9 (=25.0%) | sometimes | 7 (=19.44%) | ||
| usually | 7 (=19.44%) | usually | 8 (=22.22%) | ||
| always | 11 (=30.55%) | always | 9 (=25.0%) | ||
Table 4.
Questionnaire for the patients and their bed partners about subjective symptoms: responses at the last follow-up session.
Table 4.
Questionnaire for the patients and their bed partners about subjective symptoms: responses at the last follow-up session.
| Questions addressed to patients (n = 36) | Responses | Questions addressed to patients’ bed partner’s (n = 36) | Responses | ||
|---|---|---|---|---|---|
|
Sleep disruption (episodes of stopping breathing) |
never | 30 (=83.33%) |
Sleep disruption (episodes of stopping breathing) |
never | 26 (=72.22%) |
| rarely | 2 (=5.55%) | rarely | 6 (=16.66%) | ||
| sometimes | 3 (=8.33%) | sometimes | 4 (=11.11%) | ||
| usually | 1 (=2.77%) | usually | 0 (=0%) | ||
| always | 0 (=0%) | always | 0 (=0%) | ||
| Nocturnal bruxism (teeth grinding or clenching) | never | 31 (=86.11%) | Nocturnal bruxism (teeth grinding or clenching) |
never | 27 (=75%) |
| rarely | 3 (=8.33%) | rarely | 6 (=16.66%) | ||
| sometimes | 1 (=2.77%) | sometimes | 3 (=8.33%) | ||
| usually | 1 (=2.77%) | usually | 0 (=0%) | ||
| always | 0 (=0%) | always | 0 (=0%) | ||
| Awakening in the morning with a dry mouth or sore throat | never | 31 (=86.11%) | Snoring | never | 30 (=83.33%) |
| rarely | 4 (=11.11%) | rarely | 3 (=8.33%) | ||
| sometimes | 1 (=2.77%) | sometimes | 2 (=5.55%) | ||
| usually | 0 (=0%) | usually | 1 (=2.77%) | ||
| always | 0 (=0%) | always | 0 (=0%) | ||
| Morning pain in the masseter muscle | never | 32 (=88.88%) | Waking during the night and gasping or choking | never | 28 (=77.77%) |
| rarely | 2 (=5.55%) | rarely | 5 (=13.88%) | ||
| sometimes | 2 (=5.55%) | sometimes | 3 (=8.33%) | ||
| usually | 0 (=0%) | usually | 0 (=0%) | ||
| always | 0 (=0%) | always | 0 (=0%) | ||
| Morning fatigue, headaches, and jaw pain |
never | 29 (=80.55%) | Mood changes (e.g., depressive or irritable) |
never | 30 (=83.33%) |
| rarely | 4 (=11.11%) | rarely | 3 (=8.33%) | ||
| sometimes | 3 (=8.33%) | sometimes | 3 (=8.33%) | ||
| usually | 0 (=0%) | usually | 0 (=0%) | ||
| always | 0 (=0%) | always | 0 (=0%) | ||
| Diurnal (daytime) difficulty in focusing |
never | 26 (=72.22%) | Diurnal (daytime) difficulty in focusing |
never | 27 (=75%) |
| rarely | 7 (=19.44%) | rarely | 7 (=19.44%) | ||
| sometimes | 3 (=8.33%) | sometimes | 2 (=5.55%) | ||
| usually | 0 (=0%) | usually | 0 (=0%) | ||
| always | 0 (=0%) | always | 0 (=0%) | ||
| Excessive daytime sleepiness | never | 28 (=77.77%) | Excessive daytime sleepiness | never | 29 (=80.55%) |
| rarely | 4 (=11.11%) | rarely | 4 (=11.11%) | ||
| sometimes | 4 (=11.11%) | sometimes | 3 (=8.33%) | ||
| usually | 0 (=0%) | usually | 0 (=0%) | ||
| always | 0 (=0%) | always | 0 (=0%) | ||
* never=strongly disagree, rarely=disagree, sometimes=not sure, usually=agree, always= strongly agree.
Table 5.
Results regarding the degree of changes in patients’ life quality after the applied treatments (baseline and last follow-up).
Table 5.
Results regarding the degree of changes in patients’ life quality after the applied treatments (baseline and last follow-up).
| Group | Very dissatisfied |
Quite dis- satisfied |
Neither satisfied nor dissatisfied | Quite satisfied |
Very satisfied |
||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| B | LFu | B | LFu | B | LFu | B | LFu | B | LFu | ||
| How satisfied are you with your sleep? | G1 | 12 66.66% |
0 0% |
2 11,11% |
0 0% |
2 11.11% |
0 0% |
1 5.55% |
2 11.11% |
1 5.55% |
16 88.88% |
| G2 | 11 61.11% | 0 0% |
3 16.66% |
0 0% |
2 11.11% |
0 0% |
1 5.55% |
1 5.55% |
1 5.55% |
17 94.44% |
|
| How satisfied are you about the contractions in masseter muscle? | G1 | 10 55.55% |
0 0% |
4 22.22% |
0 0% |
2 11.11% |
1 5.55% |
1 5.55% |
2 11.11% |
1 5.55% |
15 83.33% |
| G2 | 12 66.66% |
0 0% |
3 16.66% |
0 0% |
2 11.11% |
0 0% |
1 5.55% |
1 5.55% |
0 0% |
17 94.44% |
|
| How satisfied are you now about your ability to perform daily living activities? | G1 | 11 61.11% |
0 0% |
5 27.77% |
0 0% |
1 5.55% |
0 0% |
1 5.55% |
2 11.11% |
0 0% |
16 88.88% |
| G2 | 12 66.66% | 0 0% |
4 22.22% |
0 0% |
1 5.55% | 0 0% |
1 5.55% |
1 5.55% |
0 0% |
17 94.44% |
|
| How satisfied are you now with your capacity for work? | G1 | 10 55.55% |
0 0% |
5 27.77% |
0 0% |
2 11.11% |
0 0% |
1 5.55% |
2 11.11% |
0 0% |
16 88.88% |
| G2 | 10 55.55% |
0 0% |
4 22.22% |
0 0% |
2 11.11% |
0 0% |
2 11.11% |
1 5.55% |
0 0% |
17 94.44% |
|
| How satisfied are you now with your condition of concentration? |
G1 | 12 66.66% |
0 0% |
3 16.66% |
0 0% |
1 5.55% |
1 5.55% |
1 5.55% |
2 11.11% |
1 5.55% |
15 83.33% |
| G2 | 13 72.22% |
0 0% |
2 11.11% |
0 0% |
1 5.55% |
0 0% |
1 5.55% |
1 5.55% |
1 5.55% |
17 94.44% |
|
| How satisfied are you now with the applied therapy? | G1 | 0 0% |
0 0% |
0 0% |
0 0% |
0 0% |
0 0% |
0 0% |
1 5.55% |
0 0% |
17 94.44% |
| G2 | 0 0% |
0 0% |
0 0% |
0 0% |
0 0% |
0 0% |
0 0% |
0 0% |
0 0% |
18 100% |
|
| How was the nocturnal comfort with your occlusal splint? | - | - | - | - | - | - | - | - | - | - | - |
| G2 | 3 16.66% |
0 0% |
3 16.66% |
0 0% |
3 16.66% |
1 5.55% |
4 22.22% |
2 11.11% |
5 27.77% |
15 83.33% |
|
| How satisfied are you now with the health of your orofacial system? | G1 | 6 33.33% |
0 0% |
6 33.33% |
0 0% |
4 22.22% |
0 0% |
3 16.66% |
2 11.11% |
1 5.55% |
16 88.88% |
| G2 | 6 33.33% |
0 0% |
6 33.33% |
0 0% |
3 16.66% |
0 0% |
3 16.66% |
1 5.55% |
0 0% |
17 94.44% |
|
| How satisfied are you now with yourself? | G1 | 6 33.33% |
0 0% |
5 27.77% |
0 0% |
3 16.66% |
1 5.55% |
3 16.66% |
3 16.66% |
1 5.55% |
14 77.77% |
| G2 | 6 33.33% |
0 0% |
4 22.22% |
0 0% |
4 22.22% |
0 0% |
3 16.66% |
2 11.11% |
1 5.55% |
16 88.88% |
|
| How do you evaluate now your overall quality of life? | G1 | 3 16.66% |
0 0% |
5 27.77% |
0 0% |
4 22.22% |
0 0% |
3 16.66% |
2 11.11% |
3 16.66% |
16 88.88% |
| G2 | 4 22.22% |
0 0% |
3 16.66% |
0 0% |
4 22.22% |
0 0% |
4 22.22% |
1 5.55% |
3 16.66% |
17 94.44% |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



