Submitted:
24 August 2024
Posted:
26 August 2024
You are already at the latest version
Abstract
Introduction: This review explores the literature and presents institutional cases of concurrent robotic multisite surgery—in particular, robot-assisted radical prostatectomy (RARP) and robot-assisted partial nephrectomy (RAPN) for synchronous prostate and kidney cancers. We highlight dual-console synchronous robotic procedures, emphasizing the unique docking tech-nique developed.
Aim: The aims of the study were to evaluate the feasibility, safety, and clinical outcomes of concurrent RARP and RAPN for synchronous prostate cancer and small renal tumors, as well as other concurrent robotic multisite surgeries, and to compare institutional findings with the existing literature.
Materials and Methods: We describe the unique docking technique used in our procedures, which facilitates atraumatic transitions between surgeries using the same port sites. Additionally, eligible studies on concurrent robotic multisite surgery that were published in English were retrieved from the MEDLINE, Embase, and Cochrane Library databases. Data on operative time, blood loss, complications, and postoperative outcomes were extracted.
Results: Eight cases from our institution demonstrated the feasibility and safety of the proposed approach, which is consistent with previous reports. The unique docking technique and dual-console setup enhance surgical precision, offering significant benefits in patient outcomes. As part of the litera-ture review, nine retrospective studies involving 40 cases of concurrent RARP and RAPN were reviewed. Additionally, eleven retrospective studies involving 392 cases of concomitant RARP and robotic transabdominal preperitoneal inguinal hernia repair (RTAPPIHR) were analyzed.
Conclusions: Concurrent RARP and RAPN for synchronous prostate and kidney tumors is a viable and effective approach. Our early experience suggests that this and other combined procedures can optimize patient care and reduce costs. Prospective trials are needed to validate these findings and further refine the techniques.
Keywords:
robotic surgery
; robot-assisted partial nephrectomy
; robot-assisted radical prostatectomy
; concurrent multisite surgery
; synchronous prostate and kidney cancers
1. Introduction
Robotic surgery has revolutionized the field of urology, offering enhanced precision and minimally invasive options for complex surgical procedures. The concurrent execution of robot-assisted radical prostatectomy (RARP) and robot-assisted partial nephrectomy (RAPN) is an innovative approach to managing synchronous primary cancers of the prostate and kidney. This combined procedure allows benefitting from the advantages of robotic systems to perform two major surgeries in a single setting, reducing the patient morbidity and healthcare costs associated with separate operations.
Reports in the literature indicate that single-setting robotic surgeries for both conditions are feasible and safe, providing benefits such as reduced abdominal trauma, shorter recovery times, and lower overall hospitalization costs [1,2,3,4]. This is important, as the increasing use of prostate cancer screening and cross-sectional imaging has led to increases in the incidental detection of synchronous renal tumors in patients with diagnosed and staged prostate cancer [1,2]. However, combining these surgical procedures require meticulous surgical planning and advanced expertise in robotic surgery.
This article presents an institutional case series of concurrent robotic multisite surgery from the Urology Department, Institute of Medical Sciences, Faculty of Medicine, Collegium Medicum, Cardinal Stefan Wyszyński University in Warsaw alongside a comprehensive literature review, with particular attention to concurrent RARP and RAPN surgeries performed using the da Vinci X robotic system with dual-console capabilities.
2. Aim
The aim of this study is to evaluate the feasibility, safety, and clinical outcomes of concurrent robotic-assisted radical prostatectomy (RARP) and robotic-assisted partial nephrectomy (RAPN) for the treatment of synchronous prostate cancer and small renal tumors. By presenting an institutional case series and reviewing the literature, this study seeks to demonstrate the efficacy of simultaneous robotic multisite surgery, specifically focusing on the unique docking techniques and surgical approaches utilized. Additionally, by comparing the institutional findings with the existing literature, we can highlight the advantages and potential challenges of this combined surgical procedure. Through detailed analysis of operative times, blood loss, complications, and postoperative outcomes, the study aspires to provide valuable insights that could enhance surgical practices and patient care in the field of urological oncology.
3. Material and Methods
3.1. Patient Selection for the Institutional Case Series
This study includes a retrospective analysis of patients treated at the Urology Department, Institute of Medical Sciences, Faculty of Medicine, Collegium Medicum, Cardinal Stefan Wyszyński University in Warsaw, who were subjected to concurrent robotic multisite surgery.
Between 2021 and 2024, four patients were diagnosed with synchronous prostate cancer and small renal tumors; two of them underwent concurrent robot-assisted radical prostatectomy (RARP) and robot-assisted partial nephrectomy (RAPN). The inclusion criteria were the following:
- Confirmed diagnosis of localized prostate cancer suitable for radical prostatectomy in patients not suitable for or unwilling to undergo active surveillance;
- Incidental detection of a small renal tumor (≤4 cm) suitable for partial nephrectomy;
- Eligibility for minimally invasive robotic surgery based on overall health status and absence of contraindications;
- The absence of extensive adhesions in the peritoneal cavity after multiple abdominal surgeries and the absence of perirenal “toxic fat” significantly complicating surgical dissection.
The two other patients did not meet these criteria. As a result, they were subjected to non-simultaneous robot-assisted surgical treatment and were therefore not part of our eight-patient case series.
In the same time frame, three patients were diagnosed with synchronous prostate cancer and inguinal hernia, and all of them underwent concurrent robot-assisted radical prostatectomy and robotic transabdominal preperitoneal inguinal hernia repair (RTAPPIHR).
Additionally, three other patients underwent various combinations of robot-assisted surgeries, including partial nephrectomy, adrenalectomy, total trans-obturator tape (TOT) removal, cystolithotomy, and radical prostatectomy, demonstrating the capability and versatility of robotic systems in managing complex multiorgan surgical interventions within a single operative session.
3.2. Surgical Techniques
- RARP + RAPN
All surgeries were performed using the da Vinci X robotic system with dual-console capabilities (Figure 1). The surgical team consisted of two experienced robotic surgeons. The procedures were carried out under general anesthesia, with the patient in different positions for each procedure.
-
Robot-Assisted Partial Nephrectomy (RAPN):
- ◦
- The patient was initially placed in the lateral decubitus position (Figure 2).
- ◦
- One 12 mm laparoscopic trocar (assistant trocar) and four 8 mm robotic trocars were used (a total number of five).
- ◦
- The renal artery was isolated (Figure 3), clamped during the tumor resection, and unclamped after renorrhaphy.
- ◦
- The renal tumor was excised with a margin of healthy tissue.
- ◦
-
Renal reconstruction (renorrhaphy) was performed using a two-layer closure technique:
- ▪
- The inner layer was closed using a 3-0 monofilament suture on a 26 mm needle (Figure 4).
- ▪
- The outer layer (fibrous capsule and tumor bed) was closed using a barbed 3-0 V-lock™ suture on a 26 mm needle, with Hem-o-lock™ clips and TachoSil™ hemostatic material placed under the outer sutures.
- ◦
- After decompression of the renal artery, hemostasis was verified at the pressure of a 6 mm column of mercury inside the peritoneal cavity.
- ◦
- The kidney tumor was pulled out in the Endo Bag™ with the assistant’s trocar.
- 2.
-
Repositioning:
- ◦
- After the completion of RAPN, the robotic system was undocked.
- ◦
- Arm 4 switched position to the opposite side in the da Vinci X robotic system.
- ◦
- The patient was repositioned to the supine Trendelenburg position at a 30-degree angle, and the robotic system was re-docked for RARP.
- 3.
-
Robot-Assisted Radical Prostatectomy (RARP):
- ◦
- Trocar placement for RARP was modified by using the previous incisions from the RAPN procedure. Four 8 mm robotic trocars and two 11 mm laparoscopic trocars were used (a total number of six) (Figure 5).
- ◦
- The fourth robotic arm port was closed, and two new incisions were made: one for a laparoscopic trocar and one for a robotic trocar.
- ◦
- The key steps included the dissection of the prostate with bladder neck sparing when possible (Figure 6), control of the dorsal venous complex, nerve-sparing techniques when applicable, and vesicourethral anastomosis with a continuous double-needle suture.
- ◦
- A bladder–urethral anastomosis leak test of 300 mL in the bladder was performed.
- ◦
- The prostatectomy specimen was pulled out with the assistant’s trocar in the Endo Bag™.
- ◦
- Only one 18 Ch Redon drain was inserted into the peritoneal cavity after the combined procedure.
- 4.
-
Robotic Instruments
- ◦
-
The same robotic instruments were used for both procedures:
- ▪
- Large needle driver;
- ▪
- ProGrasp forceps;
- ▪
- Monopolar curved scissors;
- ▪
- Fenestrated bipolar forceps.
- II.
- RARP + RTAPPIHR
This discussion will primarily focus on the transabdominal preperitoneal (TAPP) approach, which is frequently chosen during RARP due to its compatibility with the transperitoneal surgical route of the prostatectomy. The same robotic instruments were used for both procedures:
- ▪
- Large needle driver;
- ▪
- ProGrasp forceps;
- ▪
- Monopolar curved scissors;
- ▪
- Maryland bipolar forceps.
- 1.
-
Patient Preparation and Port Placement:
- ◦
- The patient is positioned in a steep Trendelenburg position to enhance access to the abdominal cavity and pelvic anatomical structures.
- ◦
- A six-port configuration is typically employed to facilitate optimal access to both the prostate and the inguinal regions.
- 1.
-
Dissection and Identification of the Hernia:
- ◦
- Following mobilization of the prostate and incision of the endopelvic fascia, the surgeon inspects the inguinal regions for the presence of hernias.
- ◦
- Indirect hernias are identified by a dilated internal ring (Figure 7), while direct hernias are recognized due to defects medial to the epigastric vessels.
- 1.
-
Reduction of the Hernia Sac:
- ◦
- The hernia sac is carefully dissected and reduced back into the abdominal cavity, ensuring that no contents remain within it.
- 1.
-
Mesh Placement:
- ◦
- A polypropylene mesh is selected for its strength and compatibility with biological tissues. The size of the mesh is determined by the dimensions of the defect.
- ◦
- The mesh is introduced into the abdominal cavity and positioned over the hernia defect (Figure 8) through the assistant laparoscopic port, ensuring adequate coverage to prevent recurrence.
- 1.
-
Fixation of the Mesh:
- ◦
- The mesh is secured using non-absorbable sutures, with fixation points typically including Cooper’s ligament and the transversalis fascia. Care is taken to avoid major blood vessels and nerves to prevent complications such as bleeding or chronic pain.
- 1.
-
Completion of Prostatectomy:
- ◦
- After the hernia repair, the prostatectomy is completed, including lymph node dissection (if indicated), specimen extraction, and vesicourethral anastomosis.
- 1.
-
Reperitonealization:
- ◦
- The peritoneal flap is closed over the mesh using a continuous suturing technique at the end of surgery. This step is vital to prevent bowel adhesions and mesh migration, which are potential complications of intra-abdominal mesh placement.
- ◦
- A final inspection ensures hemostasis and the integrity of the repair before the abdominal incisions are closed.
3.3. Data Collection and Analysis for the Review of the Literature
Data, if available, were collected retrospectively from patient medical records pertaining to cases treated at our institution, as well as from relevant studies published in English and retrieved in full-text versions from the MEDLINE, Embase, and Cochrane Library databases. The literature search was conducted using keywords such as "robot-assisted surgery," "radical prostatectomy," "partial nephrectomy," "simultaneous surgery," "synchronous cancers," "robotic inguinal hernia repair," "combined surgical procedures," and "simultaneous robotic-assisted interventions." All identified articles were thoroughly reviewed, and only those studies that provided detailed and relevant clinical or perioperative data pertinent to the outcomes of interest were included in the analysis. The collected data included the following:
- Operative time (total surgery time and console time for each separate procedure, if available);
- Estimated blood loss;
- Perioperative complications;
- Pathological outcomes, including biopsy results and post-prostatectomy histopathology in Gleason scores, as well as post-partial nephrectomy histopathology;
- Hemoglobin levels pre- and post-operation;
- Estimated glomerular filtration rate (eGFR) levels pre- and post-operation (24 h after surgery if available);
- Hospitalization period;
- Indications for surgery (if needed to be explained).
Descriptive statistics were used to summarize the data. For continuous quantitative variables, such as operative time, estimated blood loss, hemoglobin levels, and eGFR levels, arithmetic means were calculated to provide central tendency of the data. For categorical qualitative variables, such as perioperative complications and pathological outcomes, frequencies and percentages were used to describe the distribution of these events. These descriptive statistics provided a comprehensive summary of the collected data, which was essential for comparing the institutional outcomes with those reported in the existing literature. This approach facilitated a robust assessment of the feasibility, clinical effectiveness, and safety of the concurrent procedures by contextualizing our findings within the broader scope of published research.
3.4. Ethical Considerations
The study was conducted in accordance with the ethical standards of the institutional and national research committee and with the 1964 Declaration of Helsinki and its later amendments. Informed consent was obtained from all individual participants included in the study.
4. Results
4.1. Overview
The outcomes documented in this study offer a thorough analysis of robotic multisite surgical procedures conducted at our institution, with detailed data provided in Table 1, Table 2, Table 3 and Table 4.
Table 1 focuses on simultaneous procedures involving robot-assisted radical prostatectomy (RARP) and robot-assisted partial nephrectomy (RAPN), highlighting key clinical outcomes including operative time, estimated blood loss, and postoperative complications. Table 2 examines cases where RARP and RAPN were performed at different intervals, offering insights into the surgical approach and patient recovery associated with staged operations. Table 3 delves into the integration of RARP with robotic transabdominal preperitoneal inguinal hernia repair (RTAPPIHR) focusing on perioperative outcomes and complication rates, while Table 4 encapsulates the results from other complex, concurrent robotic interventions carried out at our facility.
To contextualize our institutional findings, we compared them with data from existing literature on robotic multisite surgery, as synthesized in Table 5, Table 6 and Table 7.
Table 5 contrasts our concurrent RARP and RAPN outcomes with those reported globally, evaluating parameters such as operative time, blood loss, and renal function preservation. Table 6 aggregates results from studies on the combination of RARP with robot-assisted inguinal hernia repair, juxtaposing them against our institutional experience. Finally, Table 7 reviews additional concurrent robotic procedures analogous to those performed in our institution, offering a comparative perspective on the safety and feasibility of these complex surgeries.
4.2. Cumulative Analysis
- I.
- Concurrent RARP + RAPN
- 1.
-
Operative Time:
- ◦
- The mean operative time across studies ranged from 390 to 430 min. In comparison, our institutional study reported the shortest operative time of 315 min, demonstrating higher efficiency (Figure 9).
- 2.
-
Console Time:
- ◦
- Console times varied between 250 and 335 min across the studies. Our institutional data showed a console time of 270 min, which falls within this range and indicates a consistent performance.
- 3.
-
Estimated Blood Loss:
- ◦
- Blood loss was generally low across studies, averaging between 200 and 330 mL. Our study reported an estimated blood loss of 300 mL, which is consistent with the range observed in other studies (Figure 9).
- 4.
-
Complications:
- ◦
- None of the reviewed studies, including ours, reported significant perioperative complications (Clavien–Dindo), confirming the overall safety of the procedure.
- 5.
-
Positive Surgical Margins:
- ◦
- While positive surgical margins were observed in a small percentage of cases across various studies, none were reported in our study, highlighting the precision of our surgical technique.
- 6.
-
Renal Function:
- ◦
- The postoperative estimated glomerular filtration rate (eGFR) generally showed a slight decline immediately but had stabilized by the one-month follow-up in most studies, with values ranging between −4 and −5 mL/min/1.73 m². Notably, our study showed an increase in eGFR of +24.85 mL/min/1.73 m², indicating an exceptional renal function outcome compared with the other studies. Comprehensive postoperative care, including meticulous management of hydration and renal perfusion, can aid in the recovery of renal function.
- 7.
-
Hospitalization:
- ◦
- The length of hospital stay varied between 2 and 8 days in the reviewed studies. Our institutional study reported a hospitalization time of 5.5 days, which is within this range and suggests comparable postoperative recovery times.
Summary
Our study shows a significantly shorter operative time and a notable increase in postoperative eGFR compared with those in other studies while maintaining consistent console times, blood loss, complication rates, and hospitalization durations. These results highlight the safety, efficiency, and effectiveness of our surgical approach, particularly in renal function outcomes.
- II.
- Concurrent RARP + Robotic Inguinal Hernia Repair (IHR)
- 1.
-
Operative Time:
- ◦
- The operative time reported in the literature ranged from 140 to 192.5 min, with additional values being indicated as “+10 over RARP” and “+24 over RARP”. In our study, the average operative time was 221.6 min, exceeding the upper end of this range. This extended duration may be attributed to the complexity and precision required in our surgical procedures (one patient with concomitant locally advanced prostate cancer and three hernia sites), which could involve more intricate steps and careful handling of anatomical structures.
- 2.
-
Estimated Blood Loss:
- ◦
- The blood loss reported in the studies varied from 50 to 175 mL. Our study documented an average estimated blood loss of 358.3 mL, which was significantly higher than the values reported in the literature. This notable difference might be due to various aforementioned factors, patient comorbidities, and the meticulous recording of intraoperative blood loss in our institution. Further investigation into intraoperative blood management strategies could be beneficial.
- 3.
-
Complications:
- ◦
- Complications were generally minimal across all studies, with descriptions ranging from “None” to “Minor”. In our study, complications were classified as “Minor (Grade I–II)”, aligning with the literature and confirming the procedural safety. The low rate of significant complications underscores the efficacy of our surgical technique and postoperative care protocols.
- 4.
-
Recurrence Rate:
- ◦
- The recurrence rate in the literature ranged from 0% to 11%. Our study noted an absence of recurrences, which is consistent with the best outcomes in the literature. This suggests that our surgical methods are highly effective in achieving durable repairs and preventing recurrence (Figure 10).
- 5.
-
Hernia Side:
- ◦
- The reviewed studies predominantly reported unilateral hernias, with bilateral cases being less common. In our study, we observed two cases of a right-sided hernia and one bilateral case with an additional epigastric (linea alba) hernia. This distribution is in line with the literature, indicating that our patient cohort is representative of the general population undergoing similar procedures.
- 6.
-
Patient BMI:
- ◦
- The average BMI reported in the studies ranged from 26.47 to 28.0 kg/m². Our study did not provide data on BMI, which limits direct comparison. However, future studies should include BMI as a variable to better understand its impact on surgical outcomes and to allow for a more comprehensive analysis.
- 7.
-
Hospital Stay:
- ◦
- The length of hospital stay varied from 1 to 6 days in the reviewed studies. Our study reported an average hospital stay of 7 days, slightly exceeding the upper range reported in the literature. This prolonged hospitalization might reflect our institution’s cautious approach to pre-, intra-, and postoperative care, ensuring complete recovery before discharge in complex cases. Reviewing and optimizing postoperative protocols could potentially reduce the length of stay without compromising patient safety.
- 8.
-
Follow-Up Period:
- ◦
- The follow-up period in the literature ranged from 9 to 36.6 months. Our study had a follow-up period ranging from 15 to 35 months, which is consistent with the literature. Adequate follow-up is crucial for monitoring long-term outcomes and ensuring the durability of surgical repairs.
Summary
Our institutional study demonstrates outcomes that are largely consistent with those reported in the literature concerning the safety and efficacy of surgical procedures. Despite a longer operative time and higher blood loss in our cohort, these factors did not adversely affect the low recurrence and complication rates. The slightly prolonged hospital stay suggests a need to review and optimize postoperative care protocols to reduce recovery times. These findings underscore the effectiveness of our surgical approach while highlighting areas for potential improvement, such as minimizing blood loss and hospital stay duration.
- III.
- Other Concurrent Robotic Multisite Surgery Procedures
- 1.
-
Limited Case Volume:
- ◦
- The surgical interventions discussed, including robot-assisted adrenalectomy (RAA) in conjunction with robot-assisted partial nephrectomy (RAPN) and robot-assisted cystolithotomy (RACLT) performed concurrently with robot-assisted radical prostatectomy (RARP), are rarely performed surgical procedures. Both our institutional data and existing literature emphasize that these procedures reserved for selected cases, reflecting their niche status in urological robotic surgery.
- 2.
-
Non-Standardized, Individualized Approaches:
- ◦
- These procedures often represent customized surgical solutions tailored to the unique clinical situations of patients with complex or concurrent pathologies. The inherent variability in these surgical combinations presents a challenge in establishing a standardized protocol or reliably predicting outcomes across different patient populations.
- 3.
-
Limitations in Deriving Conclusive Evidence:
- ◦
- The small number of cases analyzed makes it difficult to derive definitive conclusions regarding the overall safety and efficacy of these interventions. Although the outcomes from both our institution and the broader literature suggest that these surgeries can be performed with a favorable safety profile and minimal complications, the limited scope of available data necessitates cautious interpretation when considering broader applications.
- 4.
-
Contextual Understanding and Observational Insights:
- ◦
- Despite the constraints imposed by the small sample size, certain trends emerge from the data. The operative times, intraoperative blood loss, and complication rates observed in our cases are consistent with those documented in the literature, implying that these complex procedures can yield satisfactory outcomes with meticulous patient selection and surgical precision. However, the slightly prolonged hospital stays in our cohort, in comparaison to those reported in the literature, might indicate a more conservative approach to postoperative care, which should be reevaluated in order to streamline recovery protocols.
Summary
Although the limited case volume and non-standardized nature of these concurrent robotic multisite surgeries restrict the ability to generalize findings, the similarity in outcomes across various reports and out institutional data provides valuable context. These observations suggest that, with appropriate surgical planning and expertise, even complex and uncommon multisite robotic procedures can be performed successfully, with outcomes that align with established safety and efficacy standards.
5. Discussion
- I.
- RARP + RAPN
Feasibility and Safety
The concurrent performance of RARP and RAPN offers a unique approach to managing patients with synchronous primary cancers of the prostate and kidney. The concurrent execution of RARP and RAPN has been demonstrated to be feasible and safe across multiple studies. For instance, Boncher et al. reported a mean operative time of 410 min with no perioperative complications in a series of four patients [1]. Similarly, Guttilla et al. observed no significant complications in their study of three patients, with a mean operative time of 390 min [5]. In our institutional experience, both procedures were completed without significant intraoperative complications or conversions to open surgery, with a mean operative time of 315 min and minimal blood loss. This aligns with the findings from Akpinar et al., who reported an average operative time of 400 min and low blood loss [8]. Additionally, Piccoli et al. demonstrated that simultaneous robotic surgeries are feasible, highlighting their efficiency and safety in a larger cohort of seven patients [9].
Oncological Outcomes
Pathological examination of our patients revealed no cases of positive surgical margins following RARP or RAPN, although they have been reported in the literature. For example, Jung et al. reported two cases of positive margins in a study of five patients [6]. The importance of achieving negative margins cannot be overstated, as positive margins are associated with a higher risk of cancer recurrence [5,9,26].
Renal Function
Postoperative renal function was closely monitored in our patients, with eGFR measurements being taken several hours and several dozen hours postoperatively. None of our patients experienced a temporary decline in eGFR immediately following surgery. This finding is inconsistent with the transient renal impairment that is often observed after partial nephrectomy due to ischemia-reperfusion injury [7]. Similar findings were also reported by Raheem et al., who observed temporary declines in eGFR that stabilized within a month [2]. Long-term preservation of renal function remains a critical consideration in partial nephrectomy, and our results suggest that concurrent surgery does not significantly compromise renal outcomes [3,4].
Technical Considerations
The use of the da Vinci X robotic system with dual-console capabilities allowed for the efficient execution of both procedures. The need for repositioning and re-docking adds complexity but is manageable with a well-coordinated team. Modifications to trocar placement, as described by Valero et al., facilitate the transition between procedures, optimizing efficiency and minimizing additional incisions [7]. Additionally, Cochetti et al. emphasized the importance of dual-console systems in improving surgical outcomes by allowing the simultaneous participation of two surgeons, thereby enhancing the learning curve and surgical efficiency [3]. Notably, our docking method has not been previously described in the literature, and it additionally uses the dual-console technique.
Limitations and Future Directions
Our study’s limitations include its small sample size and retrospective design. Further research with larger cohorts and prospective data is necessary to validate these findings and refine the surgical approach. Similar recommendations were made by multiple studies, emphasizing the need for larger studies to confirm their findings [2,7,8]. Additionally, long-term follow-up is essential to assess the durability of oncological control and renal function, as highlighted by multiple authors [4,6,9].
- II.
- RARP + RTAPPIHR
Feasibility and Safety
The concurrent performance of RARP and RTAPPIHR has proven to be both feasible and safe. Multiple studies have confirmed that the addition of IHR during RARP does not significantly increase operative time or complication rates. For example, Mourmouris et al. reported that the addition of RTAPP IHR only minimally increased the mean console time by 24 min and did not result in significant postoperative complications or hernia recurrences during an average follow-up of 32.1 months [14]. Joshi et al. also demonstrated no postoperative complications or hernia recurrences at a mean follow-up of 34 months [11]. Moreover, Rogers et al. found that combining RARP with IHR did not significantly alter perioperative outcomes. Their study highlighted that simultaneous hernia repair reduced the need for subsequent surgical interventions for hernia repair, demonstrating the safety and efficiency of this combined approach. The median follow-up in their study was 36.6 months, with no mesh-related complications reported, further supporting the safety of this procedure [16].
Outcomes
The outcomes from concurrent RARP and IHR have generally been favorable, with low recurrence rates and minimal postoperative complications. Finley et al. reported no hernia recurrences or mesh-related complications in their series of 49 herniorrhaphies performed during RARP [10]. In a similar way, Atmaca et al. found no significant difference in operative time or estimated blood loss between patients undergoing RARP alone and those undergoing concurrent RARP and IHR, with no mesh-related complications during a median follow-up of 13 months [17]. Bajpai et al. demonstrated that the addition of IHR to RARP did not adversely affect perioperative outcomes, including estimated blood loss and hospital stay [19]. Furthermore, a study by Jaber et al. indicated that the combined procedure resulted in low rates of mesh-related complications, reaffirming the positive outcomes associated with this surgical approach [27].
Technical Considerations
Several technical considerations are crucial for optimizing outcomes in concurrent RARP and IHR. Key factors include the type of mesh used and its placement and fixation techniques. Mourmouris et al. used a non-prosthetic, tissue-based technique for direct inguinal hernias involving suturing the lateral edge of the rectus abdominis muscle sheath to the ileopectineal ligament [14]. Atmaca et al. employed various mesh types, such as Ventralight ST and 3DMax, fixed with laparoscopic tackers and absorbable sutures, to prevent mesh migration and postoperative complications such as seroma formation and adhesions [17]. Joshi et al. utilized both polypropylene and polyester meshes, secured with titanium tacks and closed with a running absorbable suture, to ensure effective fixation and minimize the risk of postoperative complications [11]. Bajpai et al. highlighted the importance of using adhesion-resistant meshes to reduce the risk of postoperative complications, particularly given the proximity of the mesh to the vesicourethral anastomosis during the transperitoneal procedure [19].
Limitations and Future Directions
Despite the encouraging results, several limitations must be acknowledged. Most studies on concurrent RARP and IHR are retrospective and involve relatively small sample sizes, limiting the generalizability of their findings. Additionally, longer follow-up periods are needed to fully assess the long-term outcomes and potential complications associated with this combined approach. Soto-Palou et al. emphasized the need for standardized surgical techniques and mesh types to ensure consistent outcomes across different institutions [28].
Future research should focus on prospective multicenter studies with larger patient cohorts to validate the current findings and refine surgical techniques. Investigating the cost-effectiveness of concurrent RARP and IHR compared with separate procedures could also provide valuable insights for clinical practice. Additionally, exploring the impact of various mesh types and fixation methods on long-term outcomes and patient quality of life would help optimize the procedure.
In conclusion, concurrent RARP and RTAPPIHR is a feasible and safe approach with favorable outcomes. Further research is needed to confirm these findings and refine the surgical techniques and materials used in this combined approach to optimize patient care.
- III.
- Other Concurrent Urological Robotic Multisite Surgery Procedures
Feasibility and Safety
The feasibility of concurrent urological robotic surgery multisite procedures has been demonstrated across various studies. Pisipati et al. reported on the safety and technical feasibility of combined upper and lower urinary tract robotic surgery, highlighting acceptable complication rates and good oncological outcomes [29]. Similarly, Ferrari et al. successfully performed the concurrent excision of a retroperitoneal paraganglioma and radical prostatectomy using a robotic approach, with no complications reported, reinforcing the feasibility of these complex procedures [30]. Furthermore, Gul et al. conducted a study on RAPN and robot-assisted adrenalectomy, showing that these concurrent procedures not only were feasible but also did not result in any significant postoperative complications [24].
The safety outcomes for concurrent robotic urological multisite surgeries are promising. Tan et al. reported no significant complications in patients undergoing RARP and robot-assisted cystolithotomy, highlighting the procedure’s safety [21]. Moreover, Tonooka et al. highlighted that in complex cases, such as concurrent RAPN and robot-assisted laparoscopic ileocecal resection for synchronous cancers, the minimally invasive approach reduced surgical risks and facilitated quicker recovery, emphasizing the advantages of concurrent procedures in managing multiorgan medical conditions [31]
Outcomes
The outcomes of concurrent robotic multisite urological surgery procedures are generally favorable, with multiple studies documenting successful results. Tan et al. documented no significant complications in patients undergoing combined RARP and robot-assisted cystolithotomy procedures, with early discharge and improved urinary symptoms [21]. Ferrari et al. emphasized no postoperative complications in concurrent excision of retroperitoneal paraganglioma and radical prostatectomy [30]. Flavin et al. noted the benefits of robotic surgery, such as lower morbidity, improved convalescence, reduced postoperative pain, a shorter hospital stay, and better cosmetic outcomes compared with open procedures [32].
Technical considerations
The technical considerations for performing concurrent robotic urological multisite surgeries encompass several critical aspects. Preoperative planning necessitates meticulous imaging and strategic preparation. Manfredi et al. underscored the importance of utilizing 3D augmented-reality models to enhance perioperative outcomes and inform surgical approaches in robot-assisted urologic procedures [33]. Intraoperatively, advanced robotic instruments are essential for achieving precision. Hashira et al. demonstrated the feasibility and safety of a humanoid hand system for robotic urological surgery, providing stable assistance through a small incision port [34]. Zhang et al. highlighted the use of 3D image reconstruction in robotic urological surgery, reporting no conversions to open surgery and minimal blood loss, thus emphasizing the significance of advanced imaging techniques in postoperative management [35].
Limitations and Future Directions
Smaller healthcare facilities may struggle with the financial and logistical demands associated with the implementation of concurrent urological robotic surgeries. To address these challenges, effective training programs and strategic resource allocation are imperative. Furthermore, continuous technological advancements and robust policy support are crucial for the broader adoption of these surgical techniques. The coordination of multisite surgeries necessitates the intricate integration of various systems and teams, which requires robust real-time communication to mitigate potential errors [36]. Additionally, the training of surgeons presents a significant challenge, as mastering robotic systems necessitates substantial investment in simulation-based programs and ongoing assessment [37]. In summary, the future of concurrent urological robotic surgery hinges on overcoming these multifaceted barriers.
The da Vinci™ system, developed by Intuitive Surgical in Sunnyvale, USA, has been the cornerstone of robotic-assisted laparoscopic surgeries, including radical prostatectomies, nephrectomies, and cystectomies. The success of this technology has catalyzed the development of several new platforms, such as Versius™ (by CMR Surgical in Cambridge, UK), Hugo™ RAS (by Medtronic in Minneapolis, USA), Senhance™ (by Asensus Surgical in Durham, USA), Avatera™ (by Avateramedical GmbH in Jena, Germany), Revo-I™ (by Meere Company Inc. in Yongin, South Korea), and Hinotori™ (by Medicaroid Inc. in Kobe, Japan) which promise to enhance the versatility, cost effectiveness, and accessibility of robotic surgical systems [38,39]. The recently developed single-port robotic surgery systems aim to reduce surgical trauma by operating through a single incision, potentially improving cosmetic outcomes and reducing recovery times and tissue trauma. These systems offer the benefits of minimally invasive surgery while overcoming the limitations associated with traditional multi-port systems, such as increased complexity and longer operative times [38]. The integration of artificial intelligence, machine learning, and augmented reality into robotic systems could enhance precision, reduce errors, and provide real-time assistance to surgeons [39]. Increased competition and technological advancements are expected to drive down costs, making these systems more accessible to a broader range of healthcare providers and patients [38]. Proctoring, whether in person or remotely, positively impacts surgical performance, particularly in intermediate tasks. This approach can significantly enhance training and proficiency, making robotic surgery more accessible globally [40].
6. Conclusions
Concurrent RARP and RAPN for patients with synchronous prostate cancer and small renal tumors is a feasible and safe approach. Our institutional experience and review of the literature suggest that this combined procedure offers advantages in terms of reduced morbidity and healthcare costs, with acceptable oncological and renal outcomes. Careful patient selection, meticulous surgical techniques, and thorough postoperative monitoring are essential to optimize the outcomes of the procedure.
The future of concurrent urological robotic multisite surgery procedures is promising, with significant advancements in single-port systems, training programs, and the integration of new technologies. These developments are expected to enhance the precision, cost effectiveness, and accessibility of robot-assisted surgery, ultimately improving patient outcomes and expanding the reach of minimally invasive surgical options in urology.
Author Contributions
Conceptualization, D.R.B., L.M. and A.A.A.; methodology, D.R.B.; software, D.R.B. and L.D.; validation, D.R.B. and A.A.A.; formal analysis, D.R.B.; investigation, D.R.B., A.A.A.; resources, D.R.B., L.M. ; data curation, D.R.B.; writing—original draft preparation, D.R.B.; writing—review and editing, D.R.B., L.M., Z.W.A., L.D. and A.A.A.; visualization, D.R.B. , Z.W.A and A.A.A.; supervision, A.A.A.; project administration, D.R.B.; funding acquisition, D.R.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the retrospective design and data collection.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
These are exclusively data in the system of the Multidisciplinary Hospital in Warsaw-Miedzylesie. Public access to data is not possible and is not permitted for data protection reasons. Anonymous patient records are presented in tables.
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper. The authors have no financial relationships with any entities, do not employ or receive funding from any organizations that could be perceived as a conflict of interest, and have no personal or financial interests that could have influenced the research reported in this paper.
References
- Boncher, N.; Vricella, G.; Greene, G.; Madi, R. Concurrent Robotic Renal and Prostatic Surgery: Initial Case Series and Safety Data of a New Surgical Technique. J. Endourol. 2010, 24, 1625–1629. [Google Scholar] [CrossRef]
- Raheem, A.A.; Santok, G.D.; Kim, D.K.; Troya, I.S.; Alabdulaali, I.; Choi, Y.D.; Rha, K.H. Simultaneous Retzius-Sparing Robot-Assisted Radical Prostatectomy and Partial Nephrectomy. Int. Neurourol. J. 2016, 57, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Cochetti, G.; Cocca, D.; Maddonni, S.; Paladini, A.; Sarti, E.; Stivalini, D.; Mearini, E. Combined Robotic Surgery for Double Renal Masses and Prostate Cancer: Myth or Reality? Medicina 2020, 56, 318. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.N.; Eun, D.; Menon, M.; Rogers, C.G. Combined Robotic-Assisted Laparoscopic Partial Nephrectomy and Radical Prostatectomy. J. Soc. Laparoendosc. Surg. 2009, 13, 229–232. [Google Scholar]
- Guttilla, A.; Crestani, A.; Zattoni, F.; Secco, S.; Dal Moro, F.; Valotto, C.; Zattoni, F. Combined Robotic-Assisted Retroperitoneoscopic Partial Nephrectomy and Extraperitoneal Prostatectomy. Urologia 2012, 79, 62–64. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.H.; Arkoncel, F.R.P.; Lee, J.W.; Oh, C.K.; Yusoff, N.A.M.; Kim, K.J.; Rha, K.H. Initial Clinical Experience of Simultaneous Robot-Assisted Bilateral Partial Nephrectomy and Radical Prostatectomy. Yonsei Med. J. 2012, 53, 236–239. [Google Scholar] [CrossRef]
- Valero, R.; Sawczyn, G.; Garisto, J.; Yau, R.; Kaouk, J. Multiquadrant Combined Robotic Radical Prostatectomy and Left Partial Nephrectomy: A Combined Procedure by a Single Approach. Actas Urol. Esp. 2020, 44, 119–124. [Google Scholar] [CrossRef]
- Akpinar, C.; Suer, E.; Turkolmez, K.; Beduk, Y. Combined Robotic-Assisted Laparoscopic Radical Prostatectomy and Partial Nephrectomy: Rare Coincidence. Urology 2019, 128, 1–4. [Google Scholar] [CrossRef]
- Piccoli, M.; Esposito, S.; Pecchini, F.; Francescato, A.; Colli, F.; Gozzo, D.; Trapani, V.; Alboni, C.; Rocco, B. Full Robotic Multivisceral Resections: The Modena Experience and Literature Review. Updates Surg. 2021, 73, 229–241. [Google Scholar] [CrossRef]
- Finley, D.S.; Rodriguez, E., Jr.; Ahlering, T.E. Combined Inguinal Hernia Repair with Prosthetic Mesh During Transperitoneal Robot-Assisted Laparoscopic Radical Prostatectomy: A 4-Year Experience. J. Urol. 2007, 178, 1296–1300. [Google Scholar] [CrossRef]
- Joshi, A.R.T.; Spivak, J.; Rubach, E.; Goldberg, G.; DeNoto, G. Concurrent Robotic Trans-Abdominal Pre-Peritoneal (TAP) Herniorrhaphy During Robotic-Assisted Radical Prostatectomy. Int. J. Med. Robot. Comput. Assist. Surg. 2010, 6, 311–314. [Google Scholar] [CrossRef] [PubMed]
- Kyle, C.C.; Hong, M.K.H.; Challacombe, B.J.; Costello, A.J. Outcomes after Concurrent Inguinal Hernia Repair and Robotic-Assisted Radical Prostatectomy. J. Robot. Surg. 2010, 4, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.K.; Montgomery, D.P.; Porter, J.R. Concurrent Transperitoneal Repair for Incidentally Detected Inguinal Hernias During Robotically Assisted Radical Prostatectomy. Urology 2013, 82, 1320–1322. [Google Scholar] [CrossRef] [PubMed]
- Mourmouris, P.; Argun, O.B.; Tufek, I.; Obek, C.; Skolarikos, A.; Tuna, M.B.; Keskin, S.; Kural, A.R. Nonprosthetic Direct Inguinal Hernia Repair During Robotic Radical Prostatectomy. J. Endourol. 2016, 30, 218–222. [Google Scholar] [CrossRef]
- Ludwig, W.W.; Sopko, N.A.; Azoury, S.C.; Dhanasopon, A.; Mettee, L.; Dwarakanath, A.; Steele, K.E.; Nguyen, H.T.; Pavlovich, C.P. Inguinal hernia repair during extraperitoneal robot-assisted laparoscopic radical prostatectomy. J. Endourol. 2016, 30, 208–211. [Google Scholar] [CrossRef]
- Rogers, T.; Parra-Davila, E.; Malcher, F.; Hartmann, C.; Mastella, B.; de Araújo, G.; Ogaya-Pinies, G.; Ortiz-Ortiz, C.; Hernandez-Cardona, E.; Patel, V.; et al. Robotic Radical Prostatectomy with Concomitant Repair of Inguinal Hernia: Is It Safe? Robot. Surg. 2017. [CrossRef]
- Atmaca, A.F.; Hamidi, N.; Canda, A.E.; Keske, M.; Ardicoglu, A. Concurrent Repair of Inguinal Hernias with Mesh Application During Transperitoneal Robotic-Assisted Radical Prostatectomy: Is It Safe? Urol. J. 2018, 15, 2955–2960. [Google Scholar] [CrossRef]
- Xia, L.; Taylor, B.L.; Patel, N.A.; Chelluri, R.R.; Raman, J.D.; Scherr, D.S.; Guzzo, T.J. Concurrent Inguinal Hernia Repair in Patients Undergoing Minimally-Invasive Radical Prostatectomy: A National Surgical Quality Improvement Program Study. J. Endourol. 2018, 32, 1181–1186. [Google Scholar] [CrossRef]
- Bajpai, R.R.; Razdan, S.; Sanchez-Gonzalez, M.A.; Razdan, S. Simultaneous Robotic Assisted Laparoscopic Prostatectomy (RALP) and Inguinal Herniorrhaphy (IHR): Proof-of-Concept Analysis from a High-Volume Center. Hernia 2019, 23, 679–686. [Google Scholar] [CrossRef]
- Bedir, F.; Altay, M.S.; Kocatürk, H.; Bedir, B.; Hamidi, N.; Canda, A.E. Concurrent Inguinal Hernia Repair During Robot-Assisted Transperitoneal Radical Prostatectomy: Single Center Experience. Robot. Surg. Res. Rev. 2021, 8, 39–44. [Google Scholar] [CrossRef]
- Tan, G.Y.; Sooriakumaran, P.; Peters, D.L.; Srivastava, A.; Tewari, A. Cystolithotomy during robotic radical prostatectomy: Single-stage procedure for concomitant bladder stones. Indian J. Urol. 2012, 28, 99–101. [Google Scholar] [CrossRef] [PubMed]
- Macedo, F.I.; O'Connor, J.; Mittal, V.K.; Hurley, P. Robotic removal of eroded vaginal mesh into the bladder. Int. J. Urol. 2013, 20, 1144–1146. [Google Scholar] [CrossRef] [PubMed]
- Sappal, S.; Sulek, J.; Smith, S.C.; Hampton, L.J. Intrarenal adrenocortical adenoma treated by robotic partial nephrectomy with adrenalectomy. J. Endourol. Case Rep. 2016, 2, 41–43. [Google Scholar] [CrossRef]
- Gul, Z.G.; Liaw, C.W.; Reddy, A.; Mehrazin, R. Robotic-assisted partial nephrectomy and adrenalectomy: Case of a pheochromocytoma invading into renal parenchyma. Case Rep. Urol. 2020, 2020, 7321015. [Google Scholar] [CrossRef]
- Olive, E.J.; Linder, B.J. Robotic-assisted intravesical mesh excision following retropubic midurethral sling. Int. Urogynecol. J. 2024, 35, 921–923. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.H.; Kim, H.W.; Oh, C.K.; Song, J.M.; Chung, B.H.; Hong, S.J.; Rha, K.H. Simultaneous Robot-Assisted Laparoendoscopic Single-Site Partial Nephrectomy and Standard Radical Prostatectomy. Yonsei Med. J. 2014, 55, 535–538. [Google Scholar] [CrossRef]
- Jaber, A.R.; Moschovas, M.C.; Rogers, T.; Saikali, S.; Perera, R.; Loy, D.G.; Sandri, M.; Roof, S.; Diaz, K.; Ortiz, C.; et al. Simultaneous hernia repair following robotic-assisted radical prostatectomy is safe with low rates of mesh-related complications. J. Robot Surg. 2023, 17, 1653–1658. [Google Scholar] [CrossRef]
- Soto-Palou, F.G.; Sánchez-Ortiz, R.F. Outcomes of minimally invasive inguinal hernia repair at the time of robotic radical prostatectomy. Curr. Urol. Rep. 2017, 18, 43. [Google Scholar] [CrossRef]
- Pisipati, S.; Bach, C.; Daneshwar, D.; Rowe, E.W.; Koupparis, A.J. Concurrent upper and lower urinary tract robotic surgery: A case series. Can. Urol. Assoc. J. 2014, 8, e853–e858. [Google Scholar] [CrossRef]
- Ferrari, M.; Sangalli, M.; Zanoni, M.; Ghezzi, M.; Fabbri, F.; Sozzi, F.; Rigatti, P.; Cestari, A. Incidental retroperitoneal paraganglioma in patient candidate to radical prostatectomy: Concurrent surgical treatments by robotic approach. Can. Urol. Assoc. J. 2015, 9, E539–E541. [Google Scholar] [CrossRef]
- Tonooka, T.; Takiguchi, N.; Ikeda, A.; Soda, H.; Hoshino, I.; Sato, N.; Iwatate, Y.; Nabeya, Y. A case of concurrent robotic-assisted partial nephrectomy and laparoscopic ileocecal resection for synchronous cancer of the kidney and ascending colon. Gan To Kagaku Ryoho 2019, 46, 166–168. (In Japanese) [Google Scholar] [PubMed]
- Flavin, K.; Prasad, V.; Gowrie-Mohan, S.; Vasdev, N. Renal physiology and robotic urological surgery. Eur. Med. J. Urol. 2017, 2, 90–96. [Google Scholar] [CrossRef]
- Manfredi, M.; Piramide, F.; Amparore, D.; Burgio, M.; Busacca, G.; Colombo, M.; Piana, A.; De Cillis, S.; Checcucci, E.; Fiori, C.; et al. Augmented reality: The smart way to guide robotic urologic surgery. Mini-Invasive Surg. 2022, 6, 40. [Google Scholar] [CrossRef]
- Hashira, I.; Kato, R.; Ishizaka, K. Development of a humanoid hand system to support robotic urological surgery. In Proceedings of the 2022 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Glasgow, Scotland, UK; 2022; pp. 4849–4852. [Google Scholar] [CrossRef]
- Zhang, K.; Zhu, G.; Li, H.; Francisco, P.J.M. Application of 3D Image Reconstruction in Robotic Urological Surgery. Chin. J. Urol. 2018, 39, 690–693. [Google Scholar] [CrossRef]
- El Sherbiny, A.; Eissa, A.; Ghaith, A.; Morini, E.; Marzotta, L.; Sighinolfi, M.C.; Micali, S.; Bianchi, G.; Rocco, B. Training in Urological Robotic Surgery: Future Perspectives. Arch. Esp. Urol. 2018, 71, 97–107. [Google Scholar]
- Hung, A.J.; Patil, M.B.; Zehnder, P.; Cai, J.; Ng, C.K.; Aron, M.; Gill, I.S.; Desai, M.M. Concurrent and predictive validation of a novel robotic surgery simulator: A prospective, randomized study. J. Urol. 2012, 187, 630–637. [Google Scholar] [CrossRef]
- Hughes, T.; Rai, B.; Madaan, S.; Chedgy, E.; Somani, B. The availability, cost, limitations, learning curve and future of robotic systems in urology and prostate cancer surgery. J. Clin. Med. 2023, 12, 2268. [Google Scholar] [CrossRef]
- Brassetti, A.; Ragusa, A.; Tedesco, F.; Prata, F.; Cacciatore, L.; Iannuzzi, A.; Bove, A.M.; Anceschi, U.; Proietti, F.; D’annunzio, S.; et al. Robotic surgery in urology: History from PROBOT® to HUGOTM. Sensors 2023, 23, 7104. [Google Scholar] [CrossRef]
- Carneiro, A.; Claros, O.R.; Cha, J.D.; Kayano, P.P.; Apezzato, M.; Wagner, A.A.; Lemos, G.C. Can remote assistance for robotic surgery improve surgical performance in simulation training? A prospective clinical trial of urology residents using a simulator in South America. Int. Braz. J. Urol. 2022, 48, 952–960. [Google Scholar] [CrossRef]
Figure 1.
Dual-console robotic surgery.

Figure 2.
Patient in the lateral decubitus position during robot-assisted partial nephrectomy (RAPN).
Figure 2.
Patient in the lateral decubitus position during robot-assisted partial nephrectomy (RAPN).

Figure 3.
Left renal artery isolation.
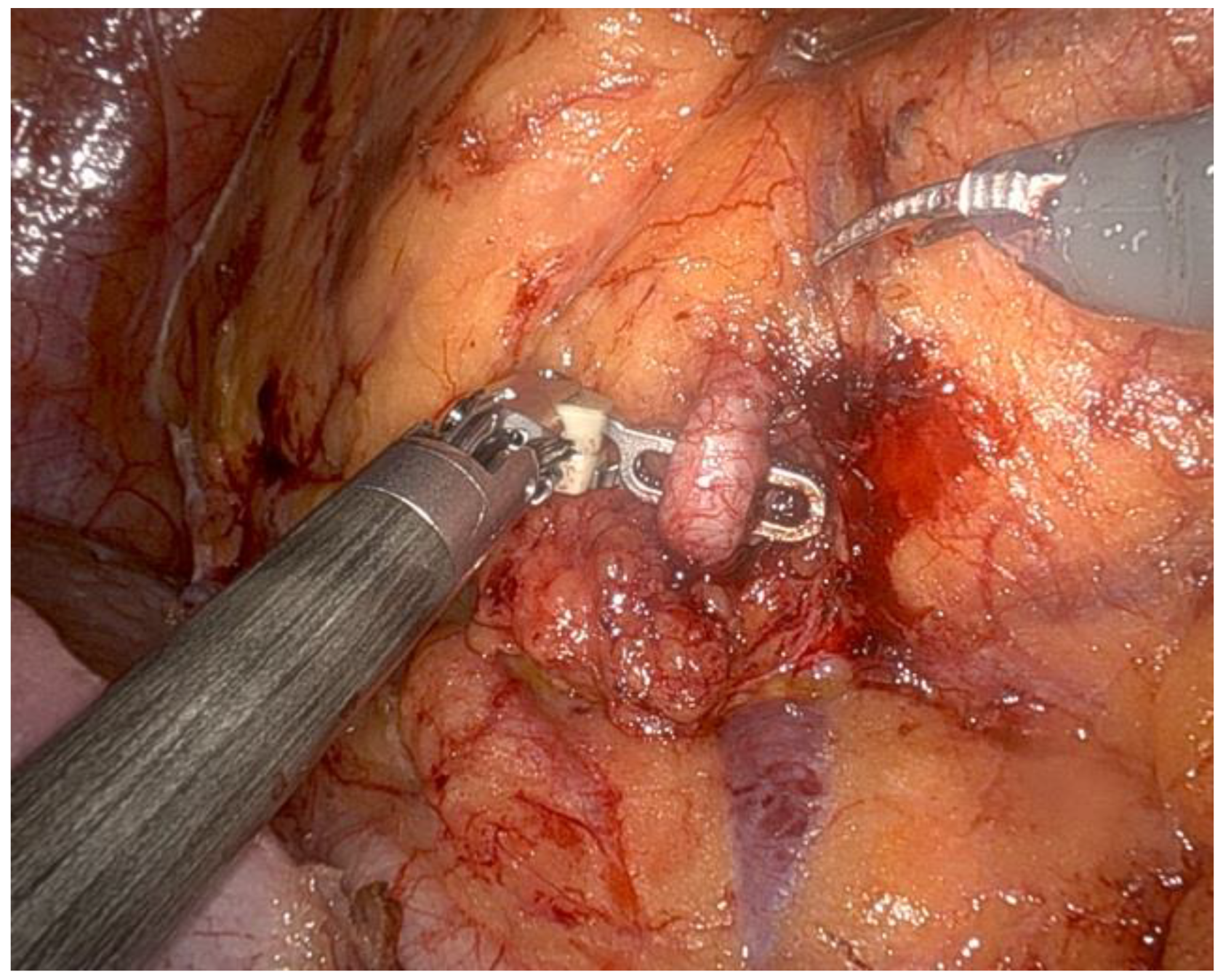
Figure 4.
Renorrhaphy of the tumor bed (inner layer).
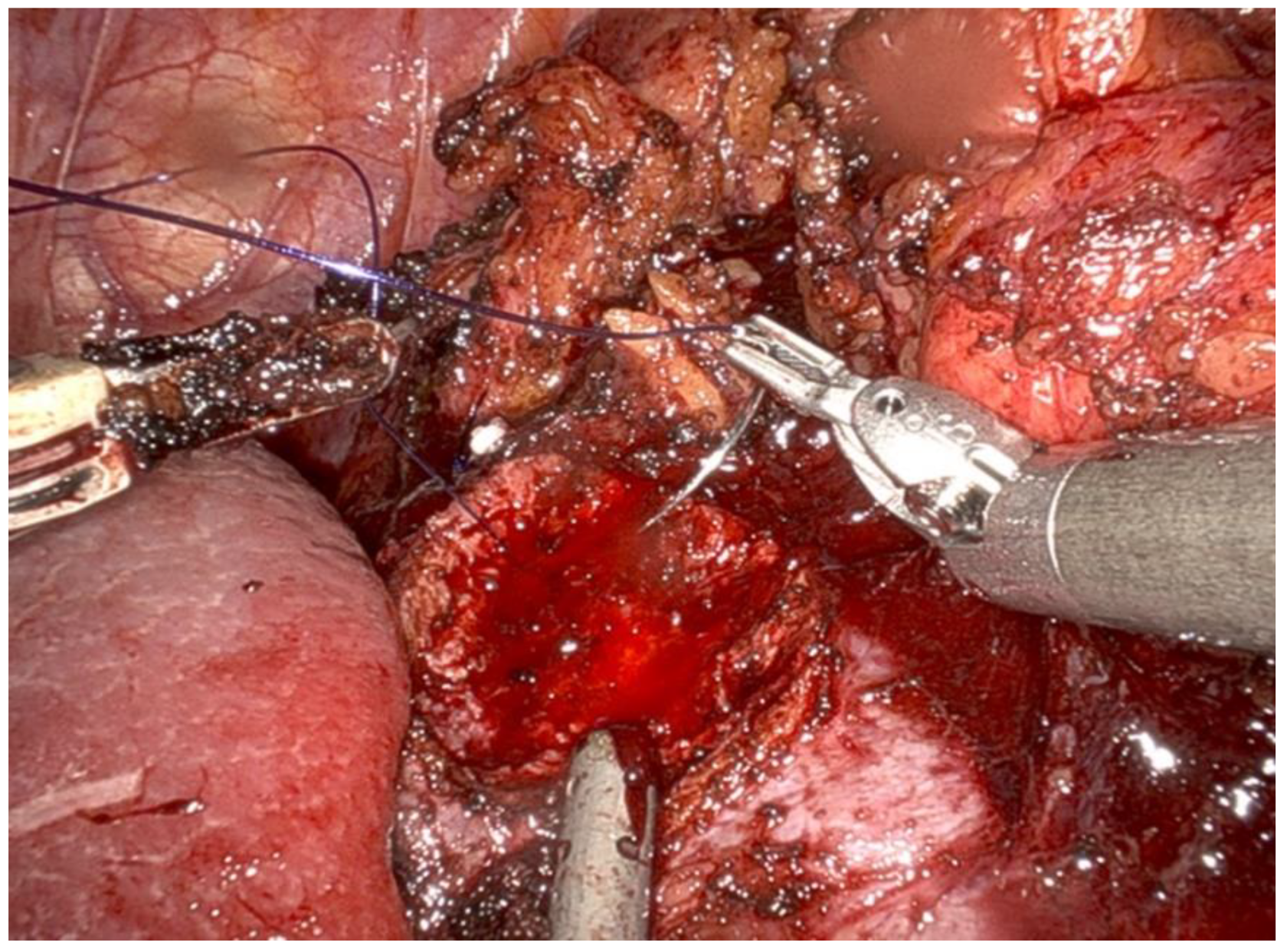
Figure 5.
Trocar port placement for the combined robot-assisted radical prostatectomy (RARP) + robot-assisted partial nephrectomy (RAPN) procedure (a–d): red dots—trocar sites used only during RARP, green dots—trocar sites used only during RAPN, red dots with green rim—trocar sites common to both RARP and RAPN, P1–P4—trocar sites for robotic arms during RARP, K1–K4—trocar sites for robotic arms during RAPN, Pa—trocar sites for the assistant during RARP, Ka—trocar sites for the assistant during RAPN.
Figure 5.
Trocar port placement for the combined robot-assisted radical prostatectomy (RARP) + robot-assisted partial nephrectomy (RAPN) procedure (a–d): red dots—trocar sites used only during RARP, green dots—trocar sites used only during RAPN, red dots with green rim—trocar sites common to both RARP and RAPN, P1–P4—trocar sites for robotic arms during RARP, K1–K4—trocar sites for robotic arms during RAPN, Pa—trocar sites for the assistant during RARP, Ka—trocar sites for the assistant during RAPN.
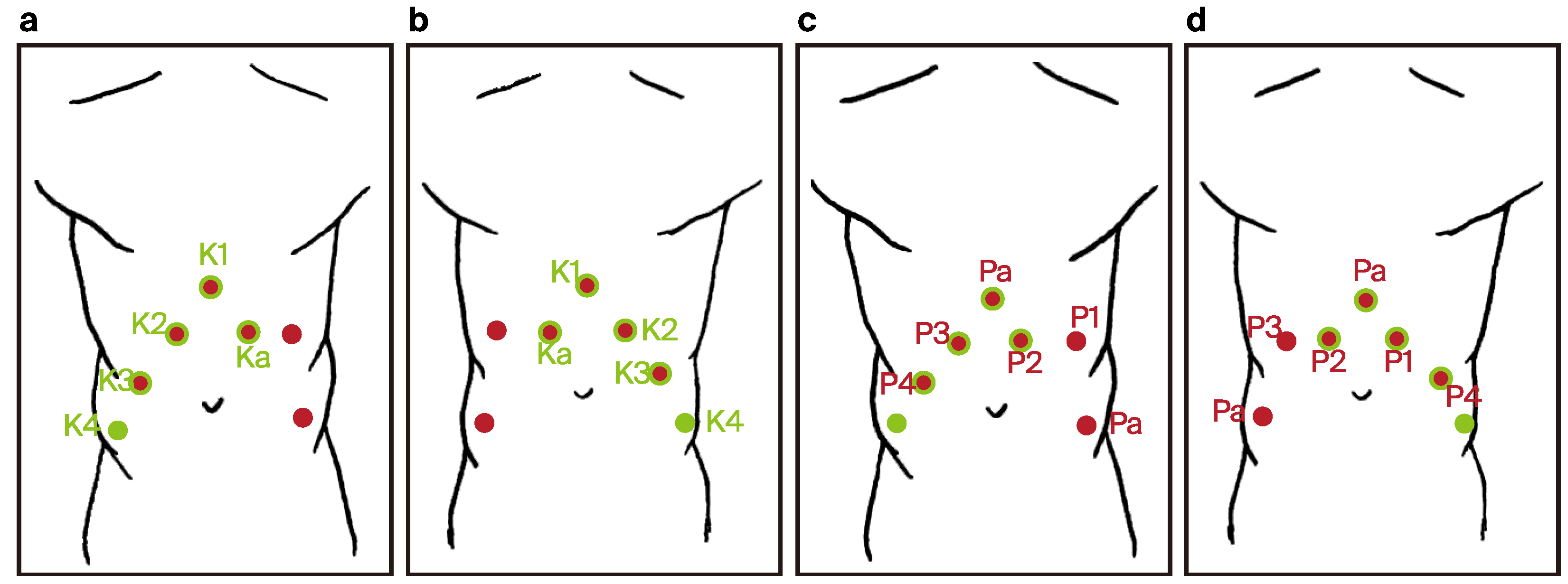
Figure 6.
Bladder neck sparing technique.
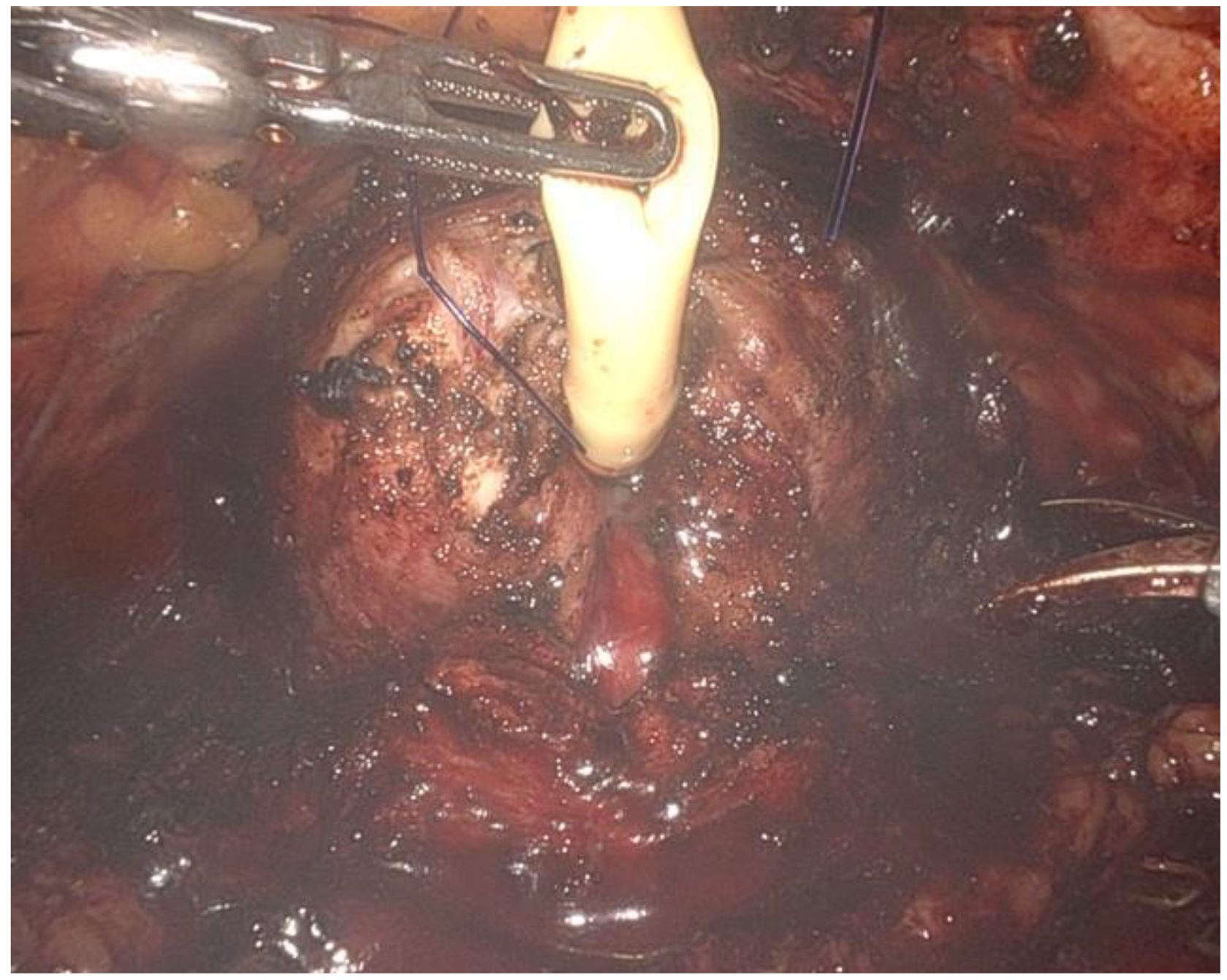
Figure 7.
Indirect hernia sac with dilated inguinal ring (arrow).
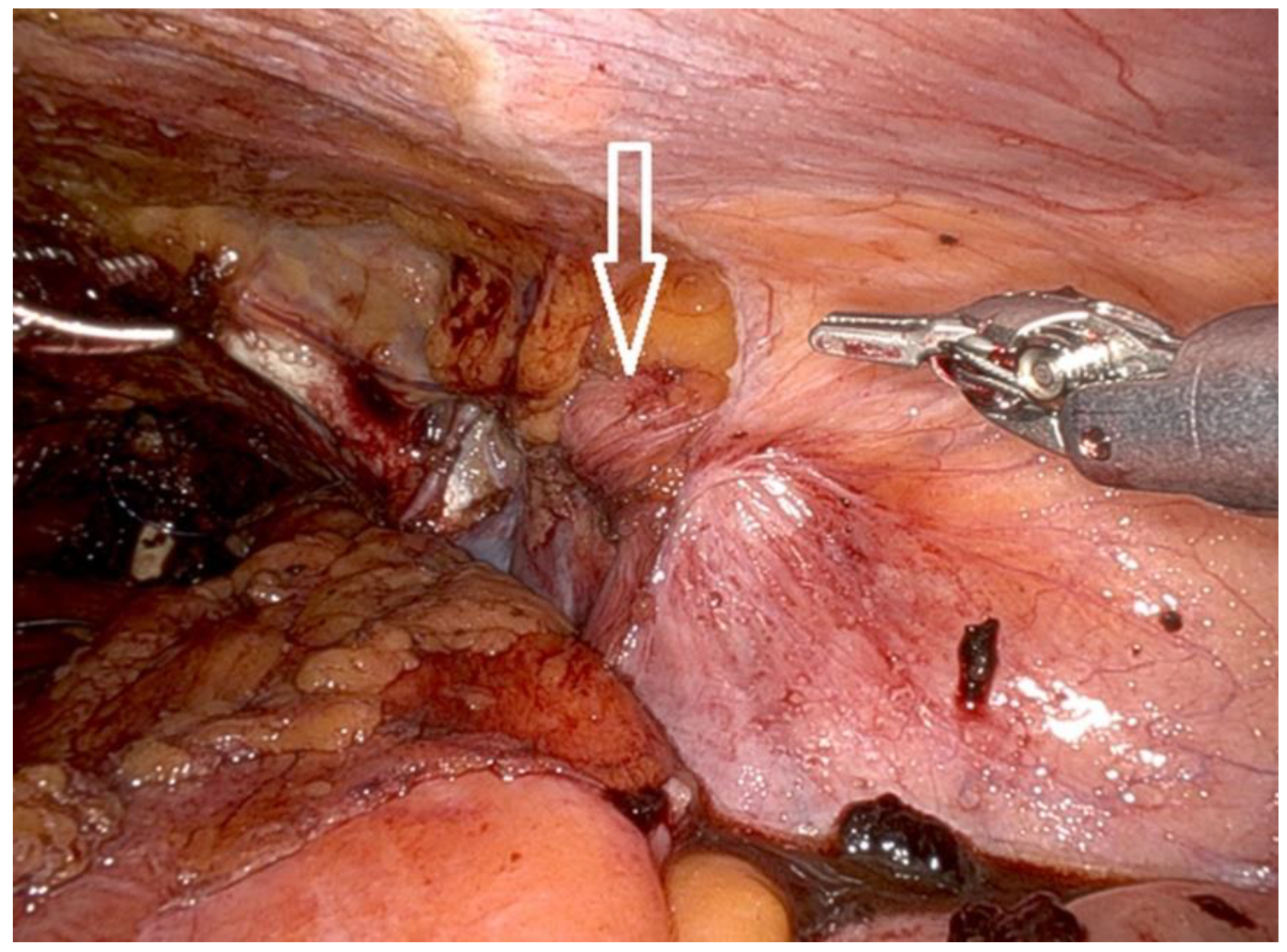
Figure 8.
Mesh positioning over the hernia defect.
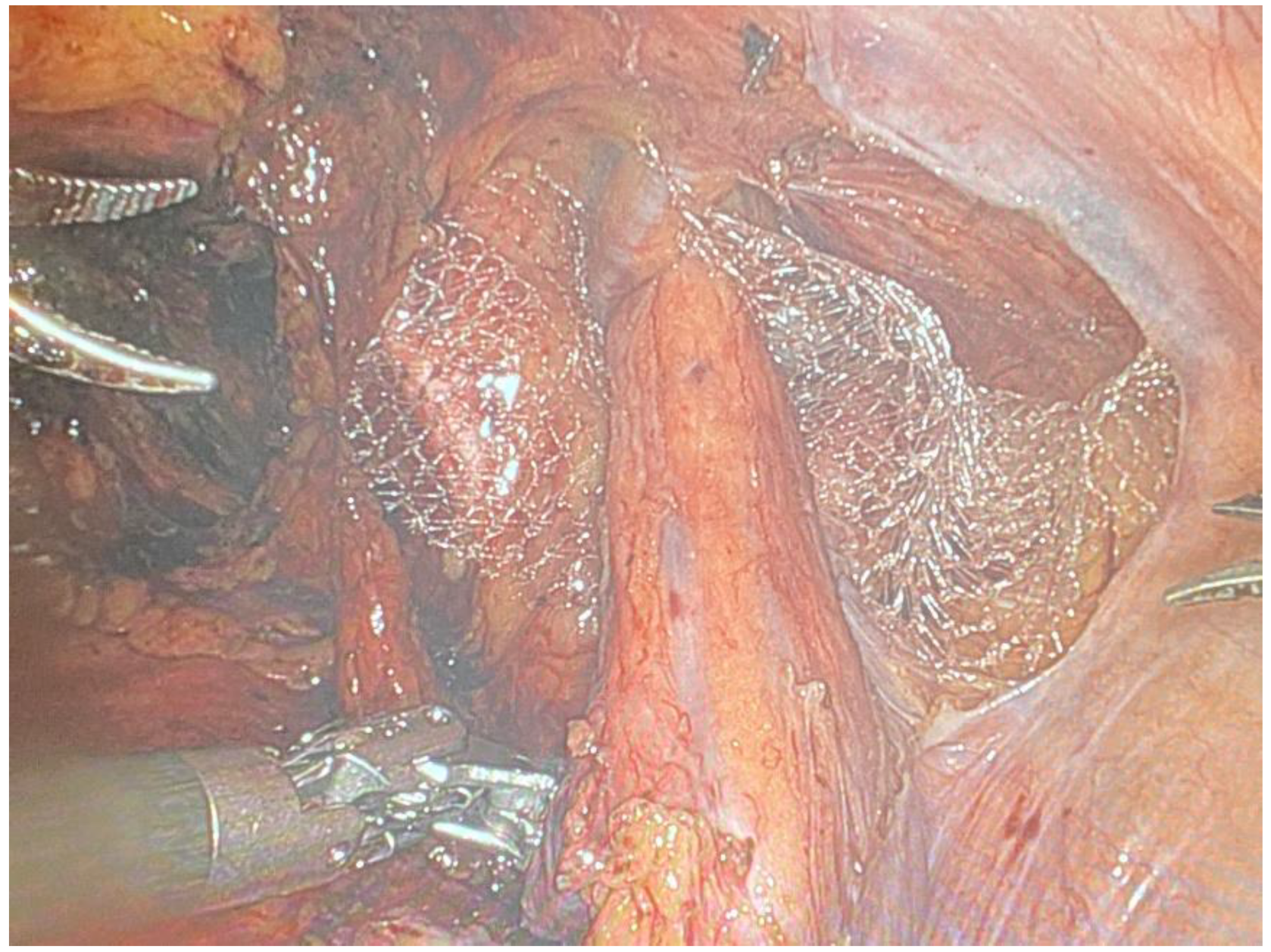
Figure 9.
a) Mean operative time (min) and b) mean estimated blood loss (mL) with confidence intervals among scientific reports [1,2,3,4,5,6,7,8,9] on concurrent RALP + RAPN.
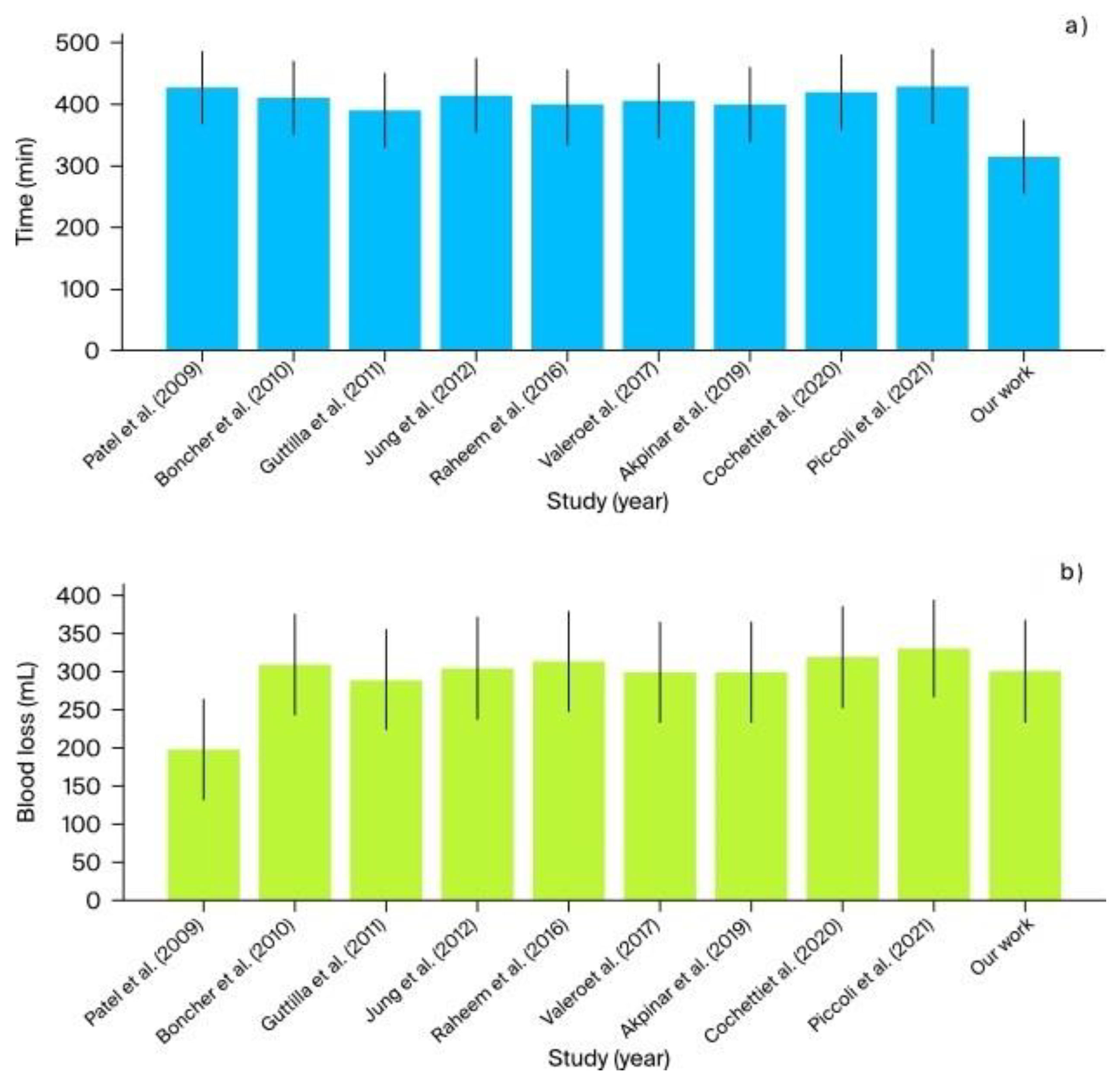
Figure 10.
Hernia recurrence rate with confidence intervals among scientific reports [1,2,3,4,5,6,7,8,9] on concurrent robot-assisted radical prostatectomy (RARP) and robotic inguinal hernia reiair (IHR).
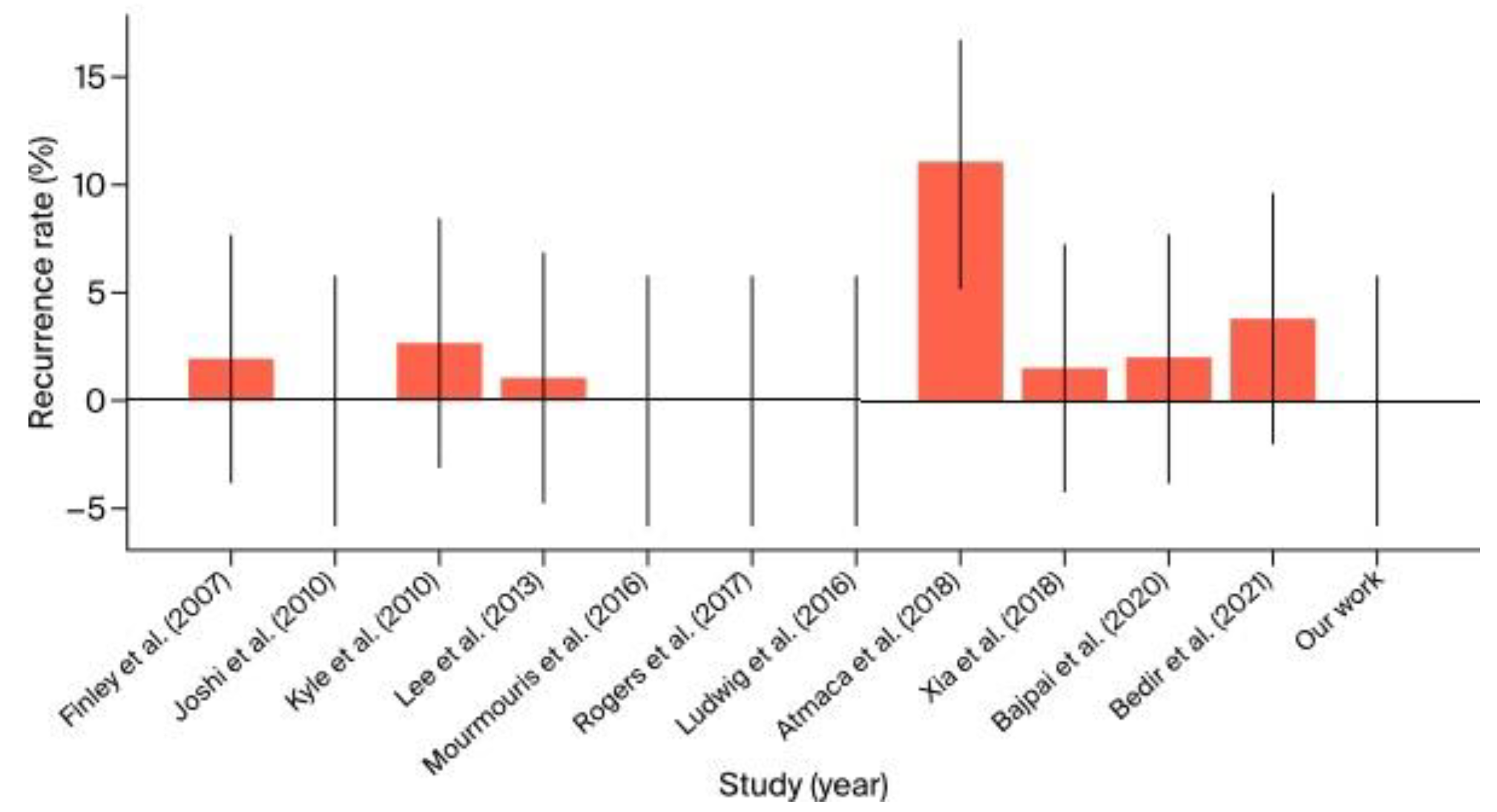

Table 1.
Detailed outcomes for institutional cases of concurrent robot-assisted radical prostatectomy (RARP) + robot-assisted partial nephrectomy (RAPN). *estimated glomerular filtration rate.
Table 1.
Detailed outcomes for institutional cases of concurrent robot-assisted radical prostatectomy (RARP) + robot-assisted partial nephrectomy (RAPN). *estimated glomerular filtration rate.
| Patient Number | Operation Date | Hospitalization Period | Preoperative Hemoglobin (mmol/L) | Postoperative Hemoglobin (mmol/L) |
Preoperative eGFR* (mL/min/1.73 m²) |
Postoperative eGFR* (mL/min/1.73 m²) |
Preoperative Prostate Cancer Clinical Stage and Biopsy Result | Post-Prostatectomy Stage and Histopathology Result | Preoperative Kidney Tumor Clinical Stage and Side | Postoperative Kidney Tumor Histopathology Result | Total Operative Time (min.) | Console Time (min.) |
Estimated Blood Loss (mL) |
Complications (Clavien–Dindo) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 (of 4) | 30.06.2023 | 27.06.2023–04.07.2023 7 days in total 4 days postoperatively |
8.9 | 8.3 | 66.1 | 99.5 | Adenocarcinoma Gleason 8 (4 + 4) ISUP Grade 4 cT2bN0M0 |
Adenocarcinoma Gleason 8 (4 + 4) ISUP Grade 4 pT2cN0M0R0 5 lymph nodes dissected during extended pelvic lymph node dissection |
cT1a solid tumor right side, upper pole |
Oncocytoma without involvement of surrounding fatty tissue R0 | 345 | RAPN 105 REPOSITIONING 50 RARP + extended pelvic lymph node dissection 190 |
350 | None |
| 2 (of 4) | 13.12.2023 | 12.12.2023–16.12.2023 4 days in total 3 days postoperatively |
9.4 | 9.1 | 73.6 | 89.9 | Adenocarcinoma Gleason 7 (3 + 4) ISUP Grade 2 cT2bN0M0 |
Adenocarcinoma Gleason 7 (3 + 4) ISUP Grade 2 pT2cN0M0R0 without end |
cT2a cystic tumor Bosniak III right side, posterior aspect |
pT0 Necrotic connective tissue fragments in the form of a cyst; neoplastic tissue was not found. |
285 | RAPN 65 REPOSITIONING 30 RARP 180 |
250 | None |
Table 2.
Detailed outcomes for institutional cases of multitemporal robot-assisted radical prostatectomy (RARP) + robot-assisted partial nephrectomy (RAPN). *estimated glomerular filtration rate.
Table 2.
Detailed outcomes for institutional cases of multitemporal robot-assisted radical prostatectomy (RARP) + robot-assisted partial nephrectomy (RAPN). *estimated glomerular filtration rate.
| Patient Number | Operation Date | Hospitalization Period | Preoperative Hemoglobin (mmol/L) | Postoperative Hemoglobin (mmol/L) | Preoperative eGFR* (mL/min/1.73m²) | Postoperative eGFR* (mL/min/1.73m²) | Preoperative Prostate Cancer Clinical Stage and Biopsy Result | Post-Prostatectomy Stage and Histopathology Result | Preoperative Kidney Tumor Clinical Stage and Side | Preoperative Kidney Tumor Histopathology Result | Total Operative Time (min.) | Console Time (min.) | Estimated Blood Loss (mL) | Complications (Clavien–Dindo) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 3 (of 4) | RARP (2nd) 11.09.2023 RAPN (1st) 05.07.2023 extensive adhesions in the peritoneal cavity, perirenal “toxic fat” | RARP (2nd) 06.09.2023—15.09.2023 9 days in total 4 days postoperatively RAPN (1st) 28.06.2023–09.07.2023 11 days in total 4 days postoperatively | RARP 8.5 RAPN 8.5 | RARP 6.9 RAPN 7.7 | RARP 96.5 RAPN 93.6 | RARP 95.6 RAPN 87.4 | Adenocarcinoma Gleason 7 (3 + 4) ISUP Grade 2 cT2bN0M0 | Adenocarcinoma Gleason 7 (3 + 4) ISUP Grade 2 pT2cN0M0R0 without extended pelvic lymph node dissection | cT1a solid tumor left side, upper pole | pT0 Histo-oncological changes in the examined material were absent | RAPN 210 RARP 225 | RAPN 170 RARP 205 | RAPN 350 RARP 550 | Grade II Fever, treated with antibiotic therapy |
| 4 (of 4) | RARP + extended pelvic lymph node dissection 13.02.2024 RAPN 27.05.2024 | RARP + extended pelvic lymph node dissection (1st) 12.02.2024–17.02.2024 5 days in total 4 days postoperatively RAPN (2nd) 26.05.2024–31.05.2024 5 days in total 4 days postoperatively | RARP + extended pelvic lymph node dissection 8.4 RAPN 8.8 | RARP + extended pelvic lymph node dissection 7.6 RAPN 7.9 | RARP + extended pelvic lymph node dissection 88.9 RAPN 79.1 | RARP + extended pelvic lymph node dissection 63.6 RAPN 72.3 | Adenocarcinoma Gleason 7 (4 + 3) ISUP Grade 3 cT3N1M0 locally advanced tumor, preoperative PSA 64 ng/ml | Adenocarcinoma Gleason 8 (4 + 4) ISUP Grade 4 pT2cN0M0 7 lymph nodes dissected during extended pelvic lymph node dissection | cT1b cystic tumor Bosniak III left side, posterior aspect | Papillary renal cell carcinoma, type 1, G2). The tumor mass showed foci of necrosis and congestion. pT1bR0 | RAPN 230 RARP + extended pelvic lymph node dissection 230 | RAPN 200 RARP + extended pelvic lymph node dissection 195 | RAPN 300 RARP 250 | None |
Table 3.
Detailed outcomes for institutional cases of concurrent robot-assisted radical prostatectomy (RARP) + robotic transabdominal preperitoneal inguinal hernia repair (RTAPPIHR). *estimated glomerular filtration rate.
Table 3.
Detailed outcomes for institutional cases of concurrent robot-assisted radical prostatectomy (RARP) + robotic transabdominal preperitoneal inguinal hernia repair (RTAPPIHR). *estimated glomerular filtration rate.
| Patient Number | Operation Date | Hospitalization Period | Preoperative Hemoglobin (mmol/l) | Postoperative Hemoglobin (mmol/l) | Preoperative eGFR* (ml/ min/ 1,73 m²) | Postoperative eGFR* (ml/ min/ 1,73 m²) | Preoperative Prostate Cancer Clinical Stage and Biopsy Result | Post-Prostatectomy Stage and Histopathology Result | Hernia side | Total Operative Time (min.) | RARP Console Time (min.) | Inguinal Hernia repair Console Time (min.) | Estimated Blood Loss (ml) | Complications (Clavien–Dindo) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 (of 3) | 17.08.2021 | 11.08.2021–20.08.2021 9 days in total 3 days postoperatively | 9,8 | N/A | 92,2 | N/A | Adenocarcinoma Gleason 6 (3 + 3) ISUP Grade 1 cT2aN0M0 | Adenocarcinoma Gleason 6 (3 + 3) ISUP Grade 1 pT2aN0MxR0 | RIGHT SIDE | 195 | 135 | 25 | 150 | Grade I SARS-CoV-2 infection requiring antipyretics | |
| 2 (of 3) | 20.10.2021 + extended pelvic lymph node dissection | 18.10.2021–25.10.2021 7 days in total 5 days postoperatively | 9,7 | 9,2 | 81 | N/A | Adenocarcinoma Gleason 7 (3 + 4) ISUP Grade 2 cT3N0M0 | Adenocarcinoma Gleason 7 (4 + 3) ISUP Grade 3 pT3aN0MxR0 | RIGHT SIDE | 200 | 165 | 40 | 225 | NONE | |
| 3 (of 3) | 09.02.2023 + extended pelvic lymph node dissection | 08.02.2023–13.02.2023 5 days in total 4 days postoperatively | 8,6 | 5,9 | 66,3 | 82,5 | Adenocarcinoma Gleason 7 (3 + 4) ISUP Grade 2 cT2bN0M0 | Adenocarcinoma Gleason 8 (4 + 4) ISUP Grade 4 pT3bN0MxR1 single-point positive surgical margin | BOTH SIDES + EPIGASTRIC HERNIA (LINEA ALBA) | 270 | 155 | 65 | 700 | Grade II Red Cell Concentrate Transfusion |
Table 4.
Detailed outcomes for institutional cases of other concurrent robotic multisite surgery procedures. *estimated glomerular filtration rate.
Table 4.
Detailed outcomes for institutional cases of other concurrent robotic multisite surgery procedures. *estimated glomerular filtration rate.
| Patient Number | Operation Date and Type of Robotic Procedure | Indication | Hospitalization Period | Pre-operative Hemoglobin (mmol/L) | Postoperative Hemoglobin (mmol/L) |
Preoperative eGFR* (mL/min/1.73 m²) |
Postoperative eGFR* (mL/min/1.73 m²) |
Preoperative Prostate Cancer Clinical Stage and Biopsy Result | Post-Prostatectomy Stage and Histopathology Result | Postoperative Kidney Tumor Histopathology Result | Total Operative Time (min) | Console Time (min) | Estimated Blood Loss (mL) | Complications (Clavien–Dindo) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 (of 3) | 08.05.2023 RAPN + IPSILATERAL ROBOT-ASSISTED ADRENALECTOMY (RAA) |
cT4N0M0 PERIPHERAL UPPER POLE KIDNEY TUMOR WITH ADRENAL INVOLVEMENT |
07.05.2023–15.05.2023 8 days in total 7 days postoperatively |
8.6 | 8.0 | 107.7 | 123.2 | N/A | N/A | Clear cell renal cell carcinoma (RCC Fuhrman 2 WHO G2 R0 |
265 | 230 | 800 | Grade II Red Cell Concentrate Transfusion |
| 2 (of 3) | 27.06.2023 ROBOT-ASSISTED TOTAL TRANS-OBTURATOR TAPE (TOT) REMOVAL + ROBOT-ASSISTED CYSTOLITHOTOMY (RACLT) |
INTRAVESICAL TRANS-OBTURATOR TAPE (TOT) EROSION WITH CONCOMITANT BLADDER STONE | 27.06.2023–04.07.2023 7 days in total 7 days postoperatively |
7.5 | 6.5 | 96.1 | 82.9 | N/A | N/A | N/A | 125 | 100 | 250 | None |
| 3 (of 3) | 29.12.2023 RALP + ROBOT-ASSISTED CYSTOLITHOTOMY (RACLT) |
ORGAN-CONFINED PROSTATE CANCER WITH CONCOMITANT BLADDER STONE | 28.12.2023–03.01.2024 6 days in total 5 days postoperatively |
8.7 | 8.2 | 98.1 | 103.6 | Adenocarcinoma Gleason 6 (3 + 3) ISUP Grade 1 cT2aN0M0 |
Adenocarcinoma Gleason 9 (4 + 5) ISUP Grade 5 pT2cN0M0R0 |
N/A | 165 | 130 | 200 | None |
Table 5.
Summary of cases of concurrent robot-assisted radical prostatectomy (RARP) + robot-assisted partial nephrectomy (RAPN) from the literature in comparison with the authors’ own (institutional) surgical results (chronological order).
Table 5.
Summary of cases of concurrent robot-assisted radical prostatectomy (RARP) + robot-assisted partial nephrectomy (RAPN) from the literature in comparison with the authors’ own (institutional) surgical results (chronological order).
| Study (Year of Surgery) | Country | Number of Patients | Robotic System | Institution | Mean Operative Time (min.) | Mean Console Time (min.) | Mean Estimated Blood Loss (mL) | Complications (Clavien-Dindo) |
Positive Surgical Margins | Mean Preoperative eGFR* (mL/min/1.73 m²) |
Mean Preoperative eGFR* (mL/min/1.73 m²) |
Calculated Mean Difference in eGFR* before and after Surgery (mL/min/1.73 m²) | Follow-Up | Mean Hospitalization Time (Days) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patel et al. (2009) [4] | USA | 1 | da Vinci S | Henry Ford Hospital | 427 | 335 | 200 | None | None | N/A 1.1 mg/dL creatinine level |
N/A | N/A | 4 months | 2 |
| Boncher et al. (2010) [1] | USA | 4 | da Vinci S | Michigan State University | 410 | 270 | 310 | None | 1 | 82 | 78 | −4 | 1 month | 7 |
| Guttilla et al. (2011) [5] | Italy | 3 | da Vinci S | University of Padua | 390 | 250 | 290 | None | 0 | 83 | 78 | −5 | 1 month | 6 |
| Jung et al. (2012) [6] | South Korea | 5 | da Vinci Si | Seoul National University Hospital | 415 | 275 | 305 | None | 2 | 84 | 79 | −5 | 1 month | 7 |
| Raheem et al. (2016) [2] | South Korea | 6 | da Vinci Xi | Yonsei University College of Medicine | 395 | 255 | 315 | None | 2 | 80 | 75 | −5 | 1 month | 5 |
| Valero et al. (2017) [7] | USA | 3 | da Vinci Xi | Cleveland Clinic | 405 | 265 | 300 | None | 1 | 85 | 80 | −5 | 1 month | 6 |
| Akpinar et al. (2019) [8] | Turkey | 5 | da Vinci Xi | Istanbul University | 400 | 260 | 300 | None | 1 | 85 | 80 | −5 | 1 month | 7 |
| Cochetti et al. (2020) [3] | Italy | 6 | da Vinci Xi | University of Perugia | 420 | 280 | 320 | None | 1 | 80 | 75 | −5 | 1 month | 8 |
| Piccoli et al. (2021) [9] | Brazil | 7 | da Vinci Xi | Hospital de Clínicas de Porto Alegre | 430 | 290 | 330 | None | 1 | 86 | 82 | −4 | 1 month | 7 |
| Drobot et al. (2023) | Poland | 2 | da Vinci X | Multidisciplinary Hospital in Warsaw-Miedzylesie | 315 | 270 | 300 | None | 0 | 69.85 | 94.7 | +24.85 | 12 months | 5.5 |
Table 6.
Summary of concurrent robot-assisted radical prostatectomy (RARP) + robot-assisted inguinal hernia repair (IHR) cases from the literature in comparison with the authors’ own surgical results (chronological order). *estimated glomerular filtration rate.
Table 6.
Summary of concurrent robot-assisted radical prostatectomy (RARP) + robot-assisted inguinal hernia repair (IHR) cases from the literature in comparison with the authors’ own surgical results (chronological order). *estimated glomerular filtration rate.
| Author (Year of Study) | Center (Country) | Number of Surgeries | Number of Hernia Repairs | Repair Method | Mean Operative Time (min.) | Blood Loss (mL) | Complications (Clavien-Dindo) |
Follow-Up (Months) |
Recurrence Rate | Hernia Side(Left–L/Right–R/Bilateral–B) | Average BMI (kg/m2) | Hospital Stay (Days) | Years of Surgeries—Time Frame |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Finley et al. (2007) [10] |
University of California-Irvine (USA) |
533 | 49 | Mesh | +10 over RARP |
N/A | None | 15.3 | 2% | 31 L 9 R |
N/A | N/A | 2002–2006 |
| Joshi et al. (2010) [11] |
North Shore University Hospital, NY (USA) |
4 | 6 | Mesh | +24 over RARP |
N/A | None | 34 | 0% | 2 L 2 R 2 B |
N/A | N/A | 2008–2009 |
| Kyle et al. (2010) [12] |
Royal Melbourne Hospital (Australia) |
700 | 37 | Mesh | +5–10 over RARP |
N/A | None | 29 | 2.7% | 18 L 14 R 5 B |
27.1 | 2 | 2005–2009 |
| Lee et al. (2013) [13] |
University of Iowa, Iowa (USA) |
1118 | 91 | Mesh | 185 | 170 | 1 recurrence, others not significant | 9–12 | 1.1% | 41 L 29 R 22 B |
27.5 | 1 | 2010–2012 |
| Mourmouris et al. (2016) [14] |
Acibadem Maslak Hospital, Istanbul (Turkey) |
1005 | 29 | Nonprosthetic | 147 | 175 | None | 32.1 | 0% | 7 L 14 R 8 B |
26.47 | 4,3 | 2013–2015 |
| Ludwig et al. (2016) [15] |
University of Pittsburgh Medical Center (USA) |
71 | 11 | Mesh | 160 | 100 | Minor | 36 | 0% | 5 L 3 R 3 B |
27.0 | 2 | 2010–2014 |
| Rogers et al. (2017) [16] |
Florida Hospital, Celebration, FL (USA) |
1139 | 39 | Mesh transabdominal preperitoneal (TAPP) |
188 | 110.87 | 10.26% Minor | N/A | 0% | N/A | 26.8 | N/A | 2008–2015 |
| Atmaca et al. (2018) [17] |
Health Sciences University (Turkey) |
100 | 38 | Mesh | 160 | 50 | 7% (Minor) | 36.6 | 11% | 19 L 12 R 7 B |
N/A | N/A | 2014–2017 |
| Xia et al. (2018) [18] |
Johns Hopkins University School of Medicine (USA) |
198 | 25 | Mesh | 155 | 110 | None | 20 | 1.5% | 10 L 8 R 7 B |
27.3 | 2 | 2015–2017 |
| Bajpai et al. (2020) [19] |
Miami Cancer Institute (USA) |
104 | 35 | Mesh | 140 | 120 | None | 18 | 2% | 15 L 12 R 8 B |
27.5 | 2 | 2017–2019 |
| Bedir et al. (2021) [20] |
Erzurum Regional Training Hospital (Turkey) |
26 | 32 | Mesh | 192.5 | 100 | None | 18 | 3.8% | 10 L 11 R 5 B |
28.0 | 6 | 2018–2020 |
| Drobot et al. (2024) |
Multidisciplinary Hospital in Warsaw-Miedzylesie (Poland) |
241 | 3 | Mesh transabdominal preperitoneal (TAPP) | 221.6 151.6 mean RARP console time 43.3 mean IHR console time |
358,3 | Minor (Grade I–II) | 15–35 | 0% | 2 B 1 B |
N/A | 7 (4 postoperative days) |
2021–2024 |
Table 7.
Summary of cases of other corresponding concurrent robotic multisite surgery procedures from the literature (chronological order).
Table 7.
Summary of cases of other corresponding concurrent robotic multisite surgery procedures from the literature (chronological order).
| Author | Year | Institution | Country | Procedure | Condition | Discharge Day | Surgery Time | Console Time | Complications |
|---|---|---|---|---|---|---|---|---|---|
| Tan, G.Y. et al. [21] | 2012 | Weill Cornell Medical College | USA | Robotic-assisted radical prostatectomy and cystolithotomy | Prostate cancer with bladder stones | Postoperative day 1 discharge | N/A | N/A | None |
| Macedo, F.I.B. et al. [22] | 2013 | James Buchanan Brady Foundation | USA | Robotic removal of eroded vaginal mesh into the bladder | Vaginal mesh erosion with bladder involvement | N/A | N/A | N/A | None |
| Sappal, S. et al. [23] | 2016 | Virginia Commonwealth University | USA | Robotic-assisted partial nephrectomy and adrenalectomy | Intrarenal adrenocortical adenoma | Postoperative day 1 discharge | 2 h 10 min | 14 min | None |
| Gul, Z.G. et al. [24] | 2020 | Icahn School of Medicine at Mount Sinai | USA | Robotic-assisted partial nephrectomy and adrenalectomy | Pheochromocytoma | Postoperative day 1 discharge | N/A | N/A | None |
| Olive, E.J. et al. [25] | 2024 | Mayo Clinic | USA | Robotic-assisted intravesical mesh excision | Intravesical mesh erosion with stone | Postoperative day 1 discharge | N/A | N/A | None |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



