Submitted:
13 March 2025
Posted:
17 March 2025
You are already at the latest version
Abstract
Alzheimer's disease (AD) is a progressive neurodegenerative disorder primarily marked by cognitive decline and memory loss. Oxidative stress (OS) has emerged as a critical factor in AD pathogenesis, contributing to hallmark features such as amyloid-β (Aβ) plaque formation, tau hyperphosphorylation, and synaptic dysfunction. This review delves into the complex mechanisms driving reactive oxygen species (ROS) production, including mitochondrial dysfunction, metal ion dysregulation, and impaired antioxidant defenses, and examines their damaging effects on neuronal integrity. Elevated ROS levels in the aging brain cause oxidative modifications to lipids, proteins, and DNA, leading to neuronal atrophy, synapse loss, and cognitive impairment. Mitochondrial dysfunction amplifies OS by disrupting cellular energy metabolism and further promoting neurodegeneration through excessive ROS generation and reduced ATP production. Despite strong evidence linking OS to AD, clinical trials with antioxidant therapies have yielded inconsistent results. However, emerging therapeutic strategies, including targeted mitochondrial antioxidants and combination therapies, offer promising avenues for mitigating OS-related damage. This review emphasizes the need for a multifaceted therapeutic approach to address the complexity of OS in AD, with the goal of developing more effective treatments and improving patient outcomes.
Keywords:
alzheimer's disease
; oxidative stress
; mitochondrial dysfunction
; antioxidant
; reactive oxygen species
1. Introduction
Alzheimer's disease (AD) is a progressive neurodegenerative disorder that significantly impacts the elderly population and primarily manifests as cognitive impairment, memory loss, and compromised daily activities [1]. Globally, AD stands as the foremost cause of dementia accounting for 60-80% of all cases, and is the sixth leading cause of death among Americans aged 65 and older [2,3]. Approximately 6.7 million Americans currently live with AD while worldwide cases are exceeding 55 million with a highly projection to almost the triple of this number by 2050 [3,4]. This escalating prevalence, along with an aging global demographic, underscores the formidable challenge AD presents to healthcare systems worldwide [3].
AD is marked by two primary neuropathological hallmarks: the extracellular deposition of Aβ peptides forming diffuse and neuritic plaques and the intracellular accumulation of neurofibrillary tangles (NFTs) composed of hyperphosphorylated tau proteins [5,6]. These core features are widespread across the brain, inducing neuronal atrophy and synaptic loss, ultimately leading to neurodegeneration [6,7]. While these hallmarks are fundamental to understanding AD, they are part of a more complex pathogenesis. The development of AD also involves a broader spectrum of pathophysiological changes, including neuroinflammation, blood-brain barrier (BBB) dysfunction, mitochondrial dysfunction, and OS [8,9,10]. These core features are integrated through interconnected hypotheses, such as the amyloidogenic cascade, tauopathy, neurovascular dysfunction, and the impacts of OS and neuroinflammation [9,11]. Each of these hypotheses is integrated through various mechanistic relationships, suggesting a multifaceted and interconnected approach which are crucial for fully understanding and addressing the progression of AD, as shown in Figure 1 [12]. According to these core hypotheses, OS emerges as a central element in the pathophysiology of AD, particularly as it bridges several core hypotheses including amyloid cascade, tau protein, inflammation, and metal ions [13,14]. Extensive research, including studies by Butterfield’s group, has documented extensive oxidative damage in AD brains, linking it to the marked accumulation of Aβ and NFTs [15,16,17]. This oxidative damage is particularly detrimental due to the brain’s unique vulnerability to OS. The brain's high oxygen demand, accounts for 20% of the total body consumption is coupled with its abundance of peroxidation-sensitive lipids and cerebrospinal fluid that poorly binds iron, heightens the brain's vulnerability to oxidative damage [18]. Moreover, the brain's antioxidant defense mechanisms play a role in its higher susceptibility to OS and neurodegeneration [19]. This environment can lead to neuronal damage through several mechanisms such as increased intracellular calcium, excitotoxicity, and the breakdown of cellular components including lipids, proteins, and DNA [20,21].
Mitochondrial dysfunction is a crucial factor in AD's progression, evidenced by the reduced number and impaired functionality of mitochondria, highly due to defects in the electron transport chain (ETC) enzymes [17,22]. This mitochondrial impairment fosters ROS accumulation and further OS, disrupting calcium homeostasis and signal transduction, ultimately contributing to synaptic loss and neurodegeneration [23,24]. The complex interplay between reactive species and cellular antioxidant defenses underscores the importance of understanding their sources, regulation, and effects. This knowledge is crucial for developing therapeutic strategies to mitigate OS-related damage in various diseases, including AD [25]. Despite the central role of OS in AD pathology, current therapies predominantly target other aspects of the disease.
Recent therapeutic advances have been particularly noteworthy lightening this growing health concern. In particular, the U.S. Food and Drug Administration (FDA) has granted accelerated approval of monoclonal antibodies Aducanumab and Lecanemab, reflecting the general urgency for therapeutic strategies for AD [26]. These monoclonal antibodies target amyloid-beta peptides implicated in AD pathology and are designed to modify disease progression, contrasting with traditional symptomatic treatments such as acetylcholinesterase inhibitors and N-methyl-D-aspartate antagonists like memantine [27]. The emergence of these therapies highlights a shift towards more targeted approaches that address the underlying mechanisms of AD, reflecting the ongoing need for a comprehensive and multidimensional strategy in combating this pervasive disease.
Despite growing evidence showing OS as an essential factor in the development and progression of AD, the exact mechanisms and interactions between OS and AD pathology remain unclear. Additionally, clinical trials applying antioxidant therapies have yielded inconsistent and often disappointing results. This review aims to provide a comprehensive exploration of the intricate roles played by OS and mitochondrial dysfunction in AD pathophysiology. We will delve into the multifaceted interactions between oxidative damage and the key pathological features of AD, such as Aβ plaques, tau hyperphosphorylation, and synaptic dysfunction. Furthermore, we will assess how mitochondrial dysfunction exacerbates disease progression and contributes to neurodegeneration. By synthesizing current research findings, this review seeks to improve our understanding of the mechanisms underlying AD and the dual role that ROS plays in both neuronal health and disease. In addition, we will highlight recent advancements in antioxidant therapies and innovative strategies targeting OS, offering promising avenues for the development of effective treatments for AD.
2. Materials and Methods
In preparing this comprehensive review, we conducted an extensive search of the PubMed and Google Scholar databases for articles published between 1994 and 2024 as shown in Figure 2. Our search incorporated key terms such as oxidative stress, mitochondrial dysfunction, and Alzheimer’s disease, aiming to capture a wide range of studies that explored these factors in AD. Unlike systematic reviews that adhere to strict inclusion and exclusion criteria, our approach included diverse research perspectives covering in vitro, in vivo, and clinical studies, to provide a more holistic understanding of how oxidative stress and mitochondrial dysfunction contribute to pathology. We prioritized research articles that offered meaningful insights into these mechanisms, while still allowing for a broad representation of the current research landscape on AD.
3. Oxidative Stress
OS arises from an imbalance between the production of ROS and reactive nitrogen species (RNS), and the cell’s capacity to neutralize these reactive intermediates or repair the damage they cause [28,29]. This imbalance, often associated with mitochondrial dysfunction, can result in significant harm to cellular components such as lipids, proteins, polysaccharides, DNA and RNA [30]. High ROS levels lead to free radical damage, specifically to cell membranes and DNA, compromising cellular function and survival. Consequently, the resulting DNA oxidation can affect gene transcription and replication, while the RNA oxidation primarily results in strand breaks and ribosomal dysfunction [31,32]. Lipid peroxidation, particularly that of unsaturated fatty acids, produces compounds like isoprostanes, MDA, and 4-hydroxynonenal (HNE), which impair cellular membrane integration and protein functions [33,34]. The resulting oxidative damage to mitochondrial components can exacerbate ROS production, damage mitochondrial DNA, and trigger apoptosis through mechanisms involving the redox-sensitive protein Thioredoxin-1 (Trx-1) and Apoptosis Signal-regulating Kinase 1 (ASK-1), as well as other redox proteins and the p53 pathway, which activates proapoptotic genes [35,36]. This can create a vicious cycle where OS damages biomolecules, which in turn, further amplifies ROS production [37].
At the molecular level, OS involves various molecules and free radicals derived from molecular oxygen [38]. Free radicals are chemical species with an unpaired electron in their outer shell, making them highly reactive [39]. Molecular oxygen in its ground state is a bi-radical with two unpaired electrons sharing the same spin, making it relatively unreactive [28]. However, when one of these electrons is excited, it changes its spin, allowing the oxygen molecule to react readily with other electron pairs, particularly those involving double bonds. This reaction produces singlet oxygen, a highly potent oxidant [25]. The reduction of oxygen by one electron generates relatively stable intermediates, leading to the formation of an O2•− [28,40]. This anion is a precursor to most ROS and a key player in OS chain reactions. O₂•⁻ is a precursor to many reactive oxygen species (ROS) and plays a crucial role in OS chain reactions. However, antioxidants primarily function to neutralize O₂•⁻ by donating electrons, preventing its participation in reactions that generate highly reactive species such as OH•. In contrast, hydroxyl radicals are typically formed through the Fenton reaction, where O₂•⁻ facilitates the reduction of transition metals (e.g., Fe³⁺ to Fe²⁺), which then catalyze the conversion of hydrogen peroxide (H₂O₂) into OH• [38,40]. This process is catalyzed by reduced transition metals, which can be re-reduced by O2•− hence further perpetuating the cycle [29,40]. O2•− can also react with other radicals, such as nitric oxide (NO•), and form peroxynitrite (ONOO−), an extremely potent oxidant driving reactive RNS [25,41].
O2•− is primarily produced by mitochondria and regulated by both enzymatic and non-enzymatic processes [42,43]. The ETC leaks electrons to oxygen making it a significant source of O2•− in many tissues [44]. Key enzymatic sources of O2•− include Nicotinamide Adenine Dinucleotide Phosphate (NADPH) oxidases in various cell membranes, cytochrome P450 enzymes, and H2O2-dependent oxygenases [38,45]. Another source is the conversion of xanthine dehydrogenase to xanthine oxidase [46]. Non-enzymatic production occurs via direct oxygen transfer by reduced coenzymes or prosthetic groups like flavin or iron-sulfur clusters or by xenobiotics after enzymatic reduction [47,48].
Mitochondria also employ several mechanisms to mitigate ROS and regulate the steady-state concentration of O2•− [49]. Superoxide dismutase (SOD) enzymes dismutate O2•− to H2O2, which is further reduced to water [48,49]. Mitochondrial SOD (MnSOD or SOD2) eliminates O2•− in the matrix or inner membrane, while copper-zinc SOD (SOD1) functions in the cytoplasm [50]. Cytochrome c in the intermembrane space reduces superoxide anion, regenerating oxygen [51]. Moreover, ubiquinol (QH2) acts as a reducing agent, detoxifying various peroxides [52]. Mitochondria also has DNA repair enzymes to correct oxidative damage, maintaining genetic integrity [25].
The complex interplay between ROS and RNS with cellular antioxidant defenses is important for understanding the sources, regulation, and mechanisms of action of these reactive species [30]. The accompanying Figure 3 illustrates how mitochondrial dysfunction leads to ROS production, highlighting the ETC role and its implications in OS and AD.
4. Oxidative Stress in Alzheimer's Disease
Brain membrane phospholipids rich in polyunsaturated fatty acids are particularly susceptible to free radical attacks, leading to lipid peroxidation - a prominent feature in AD [53,54]. The brain is highly susceptible to ROS-induced OS due to its significant energy demand, high oxygen requirement, and mitochondrial activity [14]. Neuronal cells contain high levels of lipids and iron, with the latter being found in Aβ and NFT deposits, catalyzing H2O2 into OH• by the Fenton reaction. The Fenton reaction is an oxidation process in which iron salts, particularly ferrous ions (Fe2+), catalyze the oxidation of organic substrates with H2O2. This reaction produces highly reactive hydroxyl radicals (OH•), which are potent inducers of OS. Fenton reaction forms a self-propagating loop, as the free radicals generated exacerbate oxidative damage to cellular components, promoting Aβ plaque formation and accelerating ROS production [53,55,56].
Biometals such as iron, zinc, and copper play critical roles in Aβ aggregation and neurodegeneration, with copper exacerbating OS as a potent mediator of OH• found in elevated levels in amyloid plaques [53]. Elevated levels of oxidative damage markers are found in individuals with symptoms of preclinical Alzheimer's disease (PCAD), amnestic mild cognitive impairment (aMCI), and AD [38].
Markers of protein oxidation, such as protein carbonyls (PCs), are elevated in AD-affected brain regions rich in Aβ-peptide senile plaques [38]. Furthermore, lipid peroxidation markers, including protein-conjugated HNE, F2-isoprostanes, and F4-isoprostanes, are increased in patients diagnosed with AD, aMCI, and particularly in the hippocampus of patients with PCAD. [57]. Elevated 3-nitrotyrosine (3-NT) levels indicate damage by ONOO− and the biomarker 8-hydroxy-deoxyguanosine (8-OHdG) reflects oxidative damage to both nuclear and mitochondrial DNA [58,59].
The consequences of oxidative and nitrosative damage include disrupted glucose metabolism, loss of ion gradients, impaired action potentials, and calcium imbalance [57]. OS also affects protein function and can impair critical enzymes like glutamine synthetase (GS) and creatine kinase, which are reduced in AD pathology. This reduction is linked to altered glutamate concentrations, increased excitotoxicity, and decreased energy metabolism [60].
5. Mitochondrial Dysfunction in Alzheimer's Disease
Mitochondria, the powerhouse of the cell, are pivotal in oxidative phosphorylation-driven energy production and generating adenosine triphosphate (ATP) [61]. This process makes them a significant source of reactive ROS due to ETC activity in the inner membrane [44]. A considerable amount of cellular H2O2 originates from mitochondria, which can quickly convert to superoxide (O2-) due to electron leakage during energy production [44,62].
OS severely impacts proteins involved in mitochondrial ATP production and glycolysis [63]. Impaired cellular metabolism leads to increased ROS production, creating a vicious cycle of OS and increased cellular damage [64]. Reduced ATP levels cause heightened mitochondrial activity, further escalating ROS production and electron leakage from the ETC [65].
Mitochondrial dysfunction is evident early in AD and affects various aspects of mitochondrial function, including energy metabolism, calcium homeostasis, and the expression of mitochondrial DNA (mtDNA) [66]. Glucose metabolism, closely linked to cognitive function, is essential for monitoring AD progression [67]. In AD, energy metabolism genes, such as those of the mitochondrial ETC, are decreased in the posterior cingulate cortex, a region affected early in the disease progression [68]. The reduced glucose metabolism in the AD brain is associated with decreased activity of mitochondrial ETC enzymes like pyruvate dehydrogenase, alpha-ketoglutarate dehydrogenase complex, and cytochrome oxidase [67,69]. This reduction correlates with clinical symptoms and is consistent with the presence of Aβ plaques. Furthermore, AD brains show higher levels of mtDNA oxidation and mutations compared to age-matched controls due to the proximity of mtDNA to ROS generation sites and the lack of protective histone proteins [70,71,72]. These mtDNA mutations impact mitochondrial function and the number of mitochondria, which are lower in AD brains than controls [73]. Interestingly, mitochondrial size in AD brains is increased, which is attributed to impaired fusion and fission dynamics resulting from abnormal protein expression. Dihydrosphingosine phosphate lyase (DPL1) is a protein mainly expressed in the cytoplasm and is recruited to mitochondria during fission. DPL1 is increased in AD and may also interact with Aβ and phosphorylated tau, contributing to AD pathophysiology [74]. Therefore, excessive mitochondrial fission may enhance oxidative and nitrosative stress in AD pathology.
Calcium, an essential cellular signaling messenger, is dysregulated in AD, which consequently leads to neurons becoming more susceptible to neurodegeneration. [75]. ROS produced from mitochondrial damage can disrupt calcium homeostasis and impair the endoplasmic reticulum's ability to buffer calcium, which is detrimental to cell signaling and survival [76]. Increased levels of calcium-related enzymes in AD patients further highlight this proposed mechanism of cellular dysregulation. [75].
Finally, mitochondria are crucial in apoptosis, with ROS activating caspases that induce pro-apoptotic proteins like Bcl-2-associated X protein (Bax) to translocate to the mitochondrial membrane. [77]. This translocation results in the formation of the mitochondrial membrane permeability transition pore, releasing cytochrome c and triggering cell death. [78].
Although there is some controversy regarding these processes, the role of mitochondrial dysfunction in AD is evident. [79]. The intricate interplay between mitochondrial dysfunction and OS underscores the importance of early detection and potential therapeutic strategies aimed at restoring mitochondrial function and mitigating oxidative damage in AD. [65].
6. Oxidative Stress Impact on Cellular Functions
The impact of OS on cellular function is profound and multifaceted. Lipid peroxidation, for instance, damages cell membranes, affecting their fluidity and permeability. [80]. This damage compromises the integrity and function of the cell membrane, leading to cellular instability. Similarly, protein oxidation can alter enzyme activities and disrupt protein-protein interactions, thereby interfering with critical cellular processes. [81].
6.1. Protein Oxidation
In AD, ROS mediates protein oxidation such as lysine, arginine, proline, and threonine, which results in introducing hydroxyl groups or generating reactive protein-based carbonyls and aldehydes in AD; these products are produced after the oxidation for further cells’ components (lipids, DNA, and sugars,) work in a loop cycle of protein oxidation. [82]. This process also involves the cleavage of peptide bonds via the α-amidation pathway or the oxidation of glutamyl residues. [38]. ROS can also interact with lipids, DNA, and sugars, producing reactive carbonyl derivatives and aldehydes that further react with proteins to form protein-bound carbonyls [38,82]. Measurement of protein carbonylation is a reliable indicator of oxidative damage linked to several OS conditions, aging, physiological disorders, and AD. [83].
6.2. Lipid Oxidation
Lipid peroxidation, a crucial process in OS, results in the formation of several aldehyde by-products, including MDA, HNE, and acrolein. [84]. Among these, HNE and MDA are the most abundant, while acrolein is highly reactive. [85]. Elevated levels of HNE-histidine and glutathione-HNE adducts have been observed in AD brains. [86]. Proteomic analysis has shown a significant increase in protein-bound HNE in these brains. [85]. F2-isoprostanes (F2-IsoPs) and neuroprostheses are also significantly elevated in patients with MCI and late-stage AD. [87]. Increased acrolein levels are found in the hippocampus and temporal cortex of AD patients, regions where OS is exceptionally high. [88]. Due to its high reactivity, acrolein is both a marker of lipid peroxidation and an initiator of OS, forming adducts with proteins, lipids, and nucleic acids. [85].
Lipid peroxidation occurs not only in the brains of MCI patients but also in those with preclinical AD, suggesting that oxidative damage may play an early role in the disease pathogenesis. [85]. Aβ induces lipid peroxidation of membranes, correlating strongly with the presence of antioxidant enzymes, amyloid plaques, and NFTs in AD brains. [38]. OS breakdown products such as HNE, acrolein, MDA, and F2-isoprostanes are more prevalent in AD brains compared to age-matched controls. Particularly, HNE can modify proteins, inhibiting neuronal glucose and glutamate transporters, Na-K ATPases, and disrupting intracellular calcium signaling, ultimately triggering apoptotic mechanisms. [38,89,90,91,92].
The first evidence of Aβ-induced lipid peroxidation was demonstrated using electron paramagnetic resonance (EPR) methods. [93]. Aβ addition to synaptosomes led to a rapid loss of the EPR signal, indicating lipid-centered free radical formation. [14,93]. Subsequent studies using a murine model of mutant presenilin-1 (PS-1) supported these findings, showing oxidative damage in the brain. [94]. A proposed mechanism involves the Aβ42 peptide, which in its oligomeric form can integrate into the lipid bilayer of neuronal membranes, adopting an α-helical structure. [90,95,96]. This conformation contributes to oxidative damage and neurotoxicity. [90]. The interaction between specific amino acid residues within the peptide, such as the sulfur atom of methionine and the oxygen atom of isoleucine, facilitates one-electron oxidation, generating free radicals that propagate lipid peroxidation. [97]. This process leads to the formation of lipid peroxyl radicals and lipid hydroperoxides which together contribute to the OS observed in AD. [84,98].
6.3. DNA Oxidation
OS significantly impacts DNA integrity in AD, contributing to its pathogenesis and disease progression. [38,99]. ROS, particularly OH•, can cause various forms of DNA damage, including strand breaks, DNA-DNA and DNA-protein cross-linking, and the formation of oxidized base adducts [100,101]. These modifications can lead to mutations, and altered protein synthesis affects protein synthesis such as hydroxylation, protein carbonylation, and nitration. [38,101,102]. One of the most prominent markers of oxidative DNA damage is 8-OH-guanosine, which forms when ROS reacts with guanine. [103]. Due to its low oxidation potential, guanine is readily oxidized and forms several by-products, including 2,6-diamino-4-hydroxy-5-formamidopyrimidine (FapyGua) and 7,8-dihydro-8-oxoguanine (8-OHG) [104,105]. ROS attack on DNA leads to more than 20 oxidized base adducts [106]. The most common oxidative DNA damage includes single-strand breaks (SSBs) and double-strand breaks (DSBs), with DSBs being more toxic and capable of altering gene transcription [107]. SSBs occur due to the breakdown of the DNA sugar-phosphate backbone following ROS oxidation, while DSBs can result in changes in the transcription of gene promoters near break sites. [106,107].
The capacity to repair DNA damage is compromised in AD. [108]. Studies indicate a decline in the efficiency of the base excision repair (BER) pathway and other DNA repair mechanisms. [108,109]. This impairment is evidenced by reduced recruitment of repair proteins such as p53-binding protein 1 (53BP1) to sites of damage and lower levels of critical proteins involved in double-strain break (DSB) repair, including DNA PKcs and the MRN complex. [110,111]. Elevated levels of γH2AX, a marker of DSBs, have been found in the neurons and astrocytes of AD patients, indicating persistent DNA damage. [112].
7. Neurobiological Implications
7.1. Oxidative Stress and Aβ Plaques
The formation of Aβ plaques is intricately linked to OS, with Aβ peptides, particularly Aβ42, prone to aggregation and forming insoluble fibrils that deposit as plaques in the brain [113]. OS enhances the production and aggregation of Aβ [114]. ROS can induce the expression of amyloid precursor protein (APP) and influence the activity of secretases that process APP, favoring the production of amyloidogenic Aβ fragments [41]. Moreover, Aβ itself can generate ROS, creating a vicious cycle where OS promotes Aβ production, and Aβ, in turn, generates more ROS [114]. This self-propagating loop exacerbates oxidative damage and plaque formation, with biometals like iron, copper, and zinc in amyloid plaques further accelerating ROS production through Fenton reactions [114].
Further compounding this issue, Aβ has been shown to enhance ROS production and cause mitochondrial dysfunction, exacerbating OS. [96,115]. Research indicates that brain regions with higher Aβ expression exhibit more significant levels of protein oxidation and lipid peroxidation than the cerebellum, which has relatively low levels of Aβ. [116]. Amyloid plaques predominantly contain Aβ with a methionine sulfoxide modification, suggesting that lipid peroxidation is an early event in neurodegeneration. [117]. When incorporated into lipid bilayer membranes, Aβ induces OS, leading to lipid peroxidation and subsequent damage to nucleic acids and proteins. [96,118]. Proteins are mainly subjected to oxidative damage, which can result in irreversible structural modifications such as unfolding, aggregation, and the disassociation of subunits, ultimately leading to functional loss. [119] .
In both AD patients and transgenic mice models, Aβ has been shown to interact with the mitochondrial enzyme Aβ-binding alcohol dehydrogenase (ABAD), causing mitochondrial dysfunction, increased ROS production, and eventual apoptosis. [119,120]. Apoptosis, a primary mode of cell death in AD progression, is closely associated with elevated oxidative and nitrosative stress (OS&NS), as observed in AD models. [121]. Treatment of fibroblasts derived from AD patients with the Aβ peptide leads to the oxidation of anti-apoptotic proteins such as vimentin and heat shock protein 60 (HSP60). Likewise, neuroblastoma cells treated with Aβ (1-42) show increased oxidation of anti-apoptotic proteins glutaredoxin-1 (GRX-1) and TRX-1. [122] . Furthermore, increased levels of the pro-apoptotic protein p53 and its oxidized form have been detected in the AD brain, further contributing to increased apoptosis. [123,124]. Overall, the induction of Aβ significantly contributes to the heightened oxidative status observed in AD.
7.2. Oxidative Stress and Tau Hyperphosphorylation
Tau protein is critical in stabilizing microtubules and ensuring smooth neuronal signal transmission. [125]. Numerous studies have demonstrated that OS contributes to the hyperphosphorylation of tau proteins. [126]. The peroxidation end product Carbonyl-4-HNE has been identified as a key factor in the accumulation of hyperphosphorylated tau. [127]. However, the exact relationship between tau hyperphosphorylation and OS remains unclear. In animal studies, exposure to OS -inducing compounds has been shown to increase the activity of glycogen synthase kinase 3β (GSK3β), a Ser/Thr kinase that hyperphosphorylates tau proteins, thereby exacerbating disease pathology. [127,128]. Besides GSK3β, OS also influences other kinases, promoting tau hyperphosphorylation. [127]. Additional research has indicated that OS reduces peptidyl-prolyl cis-trans isomerase 1 (Pin1) in AD brains. [128]. Pin1 is crucial for the dephosphorylation of tau proteins. [126]. The decrease in antioxidant molecules like GSH and the use of buthionine sulfoximine further contribute to increased tau hyperphosphorylation under OS conditions. [127]. Moreover, OS can directly induce tau hyperphosphorylation by affecting protein phosphatase 2A (PP2A) [127]. Under OS, GSK3β activity is heightened while PP2A activity is diminished, activating the extracellular signal-regulated kinase 1/2 (ERK1/2) pathway, leading to apoptosis. [127,128].
Studies show that low doses of GSK-3β inhibitors protect neuron cells from OS-induced apoptosis, while higher doses can have the opposite effect [129]. Increased GSK-3β and the p25 activator of cyclin-dependent kinase five halts mitochondrial movement in neurons, but GSK-3β inhibition reverses axonal transport disruption caused by Tau overexpression [130,131]. ROS-mimicking mitochondrial OS promotes Tau phosphorylation by increasing GSK-3β activity [132].
Overall, OS, mitochondrial dysfunction, and Aβ involvement are interconnected with Tau pathology, and Tau pathology also induces OS and mitochondrial damage, partly by modulating Aβ toxicity [52].
7.3. Oxidative Stress and Glutamatergic Signaling and Synaptic Dysfunction
Neuronal pathology and neurotransmitter system dysfunction are critical factors in various neurodegenerative diseases, including AD. [133,134]. While astrocytes play essential roles in regulating synaptic transmission, supplying nutrients to neurons, controlling vasodilation, maintaining BBB permeability, and responding to injury and immune challenges [135], glutamate, the primary excitatory neurotransmitter produced in neurons, plays a central role in synaptic function and brain plasticity. However, excessive glutamate contributes to neurodegenerative diseases, brain trauma, seizures, and cerebral ischemic injury. [136,137,138].
Glutamate activates ionotropic receptors (NMDAR, AMPA, and kainate) and metabotropic receptors. [139]. Although astrocytes are crucial for glutamate recycling, primarily through glutamate uptake mediated by glutamate aspartate transporter (GLAST or EAAT1) and glutamate transporter 1 (GLT-1 or EAAT2), neurons are the primary producers of glutamate. The enzyme GS, primarily found in astrocytes, converts glutamate to glutamine, which is recycled back to neurons. [140,141]. Proper regulation of glutamate is essential for neuronal survival; low levels compromise neuron viability, while excess glutamate leads to excitotoxicity, characterized by increased intracellular calcium through heightened NMDAR activity, impairing synaptic function and causing neuronal cell death. [141,142]. In AD, impaired glutamate homeostasis and NMDAR dysfunction contribute to OS exacerbation. [143].
Synaptic dysfunction is a hallmark of AD, and glutamatergic neurons are particularly affected. Synapses, specialized neuronal regions for signaling, rely on precise mechanisms such as neurotransmitter biosynthesis, delivery, synaptic vesicle formation, receptor binding, and neurotransmitter removal. [144]. Calcium is critical in mediating synaptic transmission by triggering synaptic vesicle release through voltage-gated calcium channels. [145]. Disruption in any step can severely impact synaptic function and cognitive abilities. In AD, progressive memory impairment is closely associated with synaptic dysfunction, mainly through the inhibition of long-term potentiation (LTP) and enhancement of long-term depression (LTD) in the hippocampus. [146,147]. Glutamate plays a key role in synaptic plasticity, including LTP, which is crucial for learning and memory formation. [148]. LTP strengthens synapses by increasing the efficiency of glutamatergic signaling, whereas LTD weakens synapses [149]. In AD, impaired glutamatergic signaling reduces the capacity for LTP and enhances LTD, contributing to memory deficits and cognitive decline. [150].
Extensive research indicates a direct relationship between OS and synaptic dysfunction in AD. [143,151]. ROS, Aβ, and phosphorylated tau independently and synergistically affect NMDAR activity, which is crucial for excitatory synaptic transmission and plasticity [152,153]. Aβ reduces surface NMDA receptors, triggers NMDA-mediated calcium influx, and induces excitotoxicity, exacerbating OS and impairing neuronal function. [154,155]. Memantine targets non-synaptic NMDA receptors involved in excitotoxicity due to glutamate spillover. [156,157]. Additionally, soluble Aβ species promote AMPA receptor internalization, affecting synaptic plasticity and causing synaptic dysfunction and dendritic spine loss. [158].
OS significantly impacts synaptic integrity and function, especially in synaptic membranes rich in polyunsaturated fatty acids, which are highly susceptible to lipid peroxidation, which changes the physical properties of cellular membranes and impairs the function of membrane-bound proteins. [159,160]. Furthermore, Aβ oligomers are particularly toxic to synapses, inducing OS by interacting with synaptic receptors and disrupting calcium homeostasis. [161,162]. Excessive glutamate resulting from impaired astrocytic glutamate transporters overstimulates NMDA receptors, leading to a large influx of calcium into neurons. [163]. Elevated intracellular calcium levels activate detrimental cellular events, including calcium-dependent enzymes like calpains, phospholipases, and nitric oxide synthase (NOS), which increase ROS production. [163]. Together with the overwhelming damage to the antioxidant defenses that disrupt cellular processes in neurons, mitochondrial dysfunction also contributes to synaptic loss. [164]. Mitochondrial dysfunction leads to decreased ATP production, which alters the function of ATP-dependent vesicular transporters responsible for packaging and releasing neurotransmitters into the synaptic cleft. This reduction in energy supply results in inefficient neurotransmitter release and decreased receptor binding affinity, causing diminished synaptic transmission over time [163].
8. Recent Advances in Alzheimer's Disease Therapeutics Targeting Oxidative Stress
Currently, the FDA-approved drugs for treating AD include galantamine, donepezil, memantine, rivastigmine, and the combination drug Namzaric (donepezil and memantine). Tacrine was the first drug approved for AD treatment, but it was later withdrawn due to hepatotoxicity. [128,165]. Acetylcholinesterase inhibitors are beneficial in almost all stages of dementia, yet their efficacy in MCI and prodromal AD remains unproven. [165]. Memantine is effective for moderate to severe AD, possibly by mitigating the glutamate-induced excitotoxicity, as it is an NMDA receptor antagonist, but does not significantly mitigate cognitive decline. [165]. Recently, anti-amyloid-β antibodies, such as aducanumab, lecanemab, and gantenerumab, have also been included in the FDA-approved drugs and have garnered attention for AD treatment. [26]. These monoclonal IgG1 antibodies target aggregated forms of Aβ, and growing clinical evidence supports the beneficial role of Aβ immunotherapy in improving AD conditions. [166]. These medications, however, provide only symptomatic relief without halting disease progression or altering its outcomes. [167].
Emerging therapeutic developments include naturally occurring polyphenolic compounds that act as antioxidants and confer neuroprotection in AD. [168]. In general, polyphenols have exhibited various biological activities against several human diseases. [169,170]. They also potentially modulate gut dysbiosis. [171]. When it comes to AD, polyphenols either reduce the production of ROS or enhance antioxidant release. [169]. For instance, α-lipoic acid, a dithiol antioxidant compound, acts as a free radical scavenger and mitigates H2O2 or iron-induced pathologies by inhibiting ferroptosis. It reduces the iron required for converting H2O2 into OH• via the Fenton reaction by forming chelates with iron. Additionally, it decreases brain calcium content and calpain activity, thereby preventing neuronal cell death. [172].
Green tea polyphenols, rich in (-)-epigallocatechin-3-gallate (EGCG), scavenge free radicals, chelate metal ions, and inhibit the nuclear translocation of NF-кB, alleviating OS and protecting against various AD-promoting factors [173]. Polyphenolic compounds can cross the BBB and promote neuroprotection [174]. In contrast, ROS have been found to disrupt the BBB by activating several signaling pathways, leading to tight junction activation, adherent junction modification, mitochondrial membrane pore activation, and cytoskeletal disorganization. This disruption results in BBB dysfunction and further exacerbates other pathological conditions, including neuroinflammation, progressing to AD. Naturally occurring polyphenols such as stilbenes, flavanones, isoflavones, and phenolic acids act as antioxidants, mitigating BBB dysfunction associated with increased OS [175].
Since mitochondrial dysfunction is one primary source of free radicals, identifying antioxidants that act in mitochondria’s proximity is crucial in ameliorating OS-induced AD. Antioxidants like coenzyme Q10, MitoQ, and dimebon are potent in alleviating mitochondrial dysfunction and associated oxidative damage, thereby reducing cognitive decline in AD patients. [176]. Thus, polyphenols are considered potential therapeutic molecules for treating OS-induced AD.
Aside from mitochondrial dysfunction, the contents of the inflammatory system can also impact AD’s progression. ROS activates protein kinase C and the Mitogen-Activated Protein Kinase (MAPK) pathway, triggering the release of inflammatory cytokines and chemokines. These inflammatory cells synthesize free radicals, further stimulating other inflammatory mediators. Consequently, anti-inflammatory drugs can be employed to reduce OS-induced damage and prevent neurodegeneration. Tumor Necrosis Factor-alpha (TNF-α) is a significant stimulator of cytokines and other inflammatory mediators, leading to the abnormal cleavage of APP. TNF-α also stimulates the Nuclear Factor kappa B (NFκB) pathway, producing Aβ. Inhibiting TNF-α in AD patients has been found to mitigate cognitive defects. [177]. TNF-α inhibitors, such as etanercept, can reduce TNF-α-induced neuronal damage.
Carvedilol, a nonselective β-blocker and α-1 blocker used for cardiovascular diseases, may also be effective in AD due to its ability to block harmful β-adrenergic signaling that exacerbates neuroinflammation, OS and Aβ toxicity. By reducing neuroinflammation and ROS levels and protecting against Aβ-induced synaptic dysfunction, Carvedilol holds promise in slowing AD progression and promoting neuronal survival through its neuroprotective effects on oxidative and inflammatory pathways. [178,179]. Carvedilol is currently in phase IV clinical trials with 29 participants enrolled. This study, designed as a randomized, triple-blind, and parallel assignment, has shown that Carvedilol inhibits apoptosis, reduces ROS levels, and mitigates Aβ toxicity. Carvedilol promotes neuronal growth and survival by regulating Interleukin-1 beta (IL-1β) expression. Furthermore, it activates the Nrf2/ARE pathway Figure 4, increasing the levels of heme oxygenase-1 (HO-1) and NAD(P)H quinone oxidoreductase-1 (NQO-1) in HT22 cells, thereby alleviating OS [180,181].
In a related effort, melatonin is undergoing phase III trials to treat AD by decreasing OS and amyloidogenesis. Melatonin scavenges ROS and activates the Nrf2/HO-1 pathway, elevating antioxidant levels such as catalase, superoxide dismutase, and GPx. [182,183,184]. As a pineal hormone, melatonin inhibits β and γ secretase enzymes while increasing α secretase activity, thus reducing amyloidogenesis. It is highly efficient in neuroprotection during early-stage AD. Similarly, Pramipexole is in phase II trials with an open-label, single-group assignment design involving 20 participants. Preclinical studies in APPswe/PS1dE9 mice models have shown that Pramipexole, a dopamine agonist, exhibits neuroprotective effects by scavenging free radicals and mitigating OS in mitochondria. It activates the Nrf2/HO-1 pathway, increases IL-10 generation, and improves cognitive functions. Additionally, Pramipexole activates the CREB pathway, reducing over-expressed RCAN1 levels. [185,186,187,188].
Moreover, Resveratrol is in phase II trials to evaluate its effectiveness in preventing AD progression. This randomized, single-centered study with quadruple masking and parallel group assignment includes 119 participants. Preclinical studies in Tg19959 and APP/PS1 transgenic mice models have shown that Resveratrol reduces tau pathology by activating AMPK and reducing OS. It also inhibits the Phosphoinositide 3-Kinase / Protein Kinase B (PI3K/AKT) pathway and stimulates PP2A activation, promoting tau dephosphorylation and neuronal survival [189,190,191]. Adding to the list, Etanercept is in phase I clinical trials with an open-label, crossover assignment model involving 12 participants. Studies in AD mouse models have demonstrated that Etanercept decreases TNF-α levels in the brain, reducing ROS production via NADPH oxidase and improving cognitive function. As an anti-TNF-α drug, Etanercept reduces OS, evidenced by decreased MDA levels and increased antioxidant levels such as SOD and GPx [192,193,194,195,196].
Epigallocatechin-gallate (EGCG) is being evaluated in phase III trials for its benefits in early-stage AD. With 200 participants, this randomized, double-blind, crossover assignment study has shown that EGCG, which contains hydroxyl groups, neutralizes free radicals, modulates pro-apoptotic proteins Bax and Bad, and regulates mitochondrial permeability. It also activates the Nrf2/ARE pathway, alleviating OS and providing neuroprotection. [197,198].
Genistein, in a phase II trial with a randomized, parallel assignment, and quadruple masking study design, involves 27 participants. Experiments on streptozotocin-induced rat models have shown that Genistein induces autophagy and promotes Aβ clearance. It hinders kinases such as cyclic Adenosine Monophosphate (cAMP)-dependent protein kinase, protein kinase C, and phosphorylase kinase. Genistein also promotes neuronal survival by attenuating OS via the Phosphoinositide 3-Kinase / Protein Kinase B (Akt) / Nuclear Factor Erythroid 2-Related Factor 2 / Kelch-like ECH-Associated Protein 1 (PI3K/Akt/Nrf2/Keap1) pathway and activates the cAMP/CREB-BDNF-TrkB signaling pathway, enhancing cAMP levels and CREB and TrkB phosphorylation. [199,200,201].
Figure 4 illustrates how exogenous and endogenous antioxidant defenses work together to eliminate ROS/RNS, highlighting the Nrf2 pathway's activation and its role in OS regulation.
9. Conclusions and Future Directions
OS plays an essential role in the pathophysiology and progression of AD. ROS and RNS contribute to neuronal toxicity through lipid peroxidation, protein oxidation, and DNA damage. Mitochondrial dysfunction aggravates ROS production, disrupting cellular metabolism and accelerating neurodegeneration. Moreover, OS interacts with key pathological hallmarks of AD, including Aβ aggregation, tau hyperphosphorylation, and synaptic dysfunction, creating a self-perpetuating cycle of neuronal injury. Despite growing evidence showing the linking of OS to AD, antioxidant-based therapeutic strategies have resulted in inconsistent clinical outcomes, showing the complexity of the disease. While significant progress has been made in understanding OS-driven neurodegeneration, numerous challenges hinder the clinical translation of OS-targeting therapies. One of the significant limitations is the inconsistent efficacy of antioxidants in clinical trials, which can be attributed to poor bioavailability, inadequate BBB permeability, and interindividual variability in OS profiles. Moreover, conventional antioxidant administration often results in systemic distribution rather than targeted neuroprotection. Advances in nanotechnology, particularly nanoparticle-based and liposomal delivery systems, may enhance brain-specific antioxidant delivery and improve therapeutic outcomes. The heterogeneity of AD pathogenesis further complicates OS-targeted interventions, as genetic, environmental, and lifestyle factors contribute to disease variability. A shift toward personalized medicine, rather than a one-size-fits-all antioxidant approach, is critical for improving treatment efficacy.
A promising research area for future investigation is the development of precision antioxidant therapies that selectively target ROS sources while preserving essential redox signaling. Mitochondria-targeted antioxidants offer a potential strategy to mitigate oxidative damage while maintaining metabolic integrity. Additionally, multi-target therapeutic approaches combining antioxidants with neuroprotective agents, anti-inflammatory compounds, and amyloid-targeting strategies may enhance overall treatment efficacy. Early detection remains crucial for successful intervention, necessitating the identification of reliable redox-based biomarkers for AD diagnosis. Peripheral markers such as oxidized glutathione (GSSG), HNE, and F2-isoprostanes may facilitate early disease progression detection and monitoring. Another emerging area of interest is the gut-brain axis in OS regulation. Alterations in gut microbiota composition have been implicated in neuroinflammation and oxidative imbalance, suggesting that probiotic-based and microbiota-targeted interventions may offer novel avenues for modulating OS and mitigating AD pathology.
Longitudinal cohort studies will be essential to establish causal relationships between OS and AD progression. Given that oxidative damage accumulates over decades before clinical symptoms emerge, long-term follow-up studies are necessary to validate therapeutic interventions and optimize the timing of interventions. Addressing these challenges will be critical to advancing OS-targeted therapies and developing more effective AD prevention and treatment strategies.
Author Contributions
All authors contributed to this manuscript’s conceptualization, writing, editing, and reviewing. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) declare financial support was received for this article's research, authorship, and/or publication.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Knopman, D.S.; Amieva, H.; Petersen, R.C.; Chételat, G.; Holtzman, D.M.; Hyman, B.T.; Nixon, R.A.; Jones, D.T. Alzheimer disease. Nat Rev Dis Primers 2021, 7, 33. [CrossRef] [PubMed]
- Association, A.s. 2019 Alzheimer's disease facts and figures. Alzheimer's & dementia 2019, 15, 321-387.
- Association, A.s. What is Alzheimer’s Disease? Available online: https://www.alz.org/alzheimers-dementia/what-is-alzheimers#:~:text=Alzheimer's%20disease%20accounts%20for%2060%2D80%25%20of%20dementia%20cases.&text=Alzheimer's%20is%20not%20a%20normal,affects%20a%20person%20under%2065. (accessed on 4.14.2024).
- Organization, W.H. Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on.
- DeTure, M.A.; Dickson, D.W. The neuropathological diagnosis of Alzheimer’s disease. Molecular Neurodegeneration 2019, 14, 32. [CrossRef] [PubMed]
- Hampel, H.; Hardy, J.; Blennow, K.; Chen, C.; Perry, G.; Kim, S.H.; Villemagne, V.L.; Aisen, P.; Vendruscolo, M.; Iwatsubo, T.; et al. The Amyloid-β Pathway in Alzheimer’s Disease. Molecular Psychiatry 2021, 26, 5481-5503. [CrossRef]
- Serrano-Pozo, A.; Frosch, M.P.; Masliah, E.; Hyman, B.T. Neuropathological alterations in Alzheimer's disease. Cold Spring Harbor perspectives in medicine 2011, 1, a006189.
- Al-Ghraiybah, N.F.; Wang, J.; Alkhalifa, A.E.; Roberts, A.B.; Raj, R.; Yang, E.; Kaddoumi, A. Glial cell-mediated neuroinflammation in Alzheimer’s disease. International journal of molecular sciences 2022, 23, 10572.
- Alkhalifa, A.E.; Al-Ghraiybah, N.F.; Odum, J.; Shunnarah, J.G.; Austin, N.; Kaddoumi, A. Blood–Brain Barrier Breakdown in Alzheimer’s Disease: Mechanisms and Targeted Strategies. International journal of molecular sciences 2023, 24, 16288.
- Nunomura, A.; Perry, G.; Aliev, G.; Hirai, K.; Takeda, A.; Balraj, E.K.; Jones, P.K.; Ghanbari, H.; Wataya, T.; Shimohama, S. Oxidative damage is the earliest event in Alzheimer disease. Journal of Neuropathology & Experimental Neurology 2001, 60, 759-767.
- Mehta, R.I.; Mehta, R.I. The Vascular-Immune Hypothesis of Alzheimer's Disease. Biomedicines 2023, 11. [CrossRef]
- Du, X.; Wang, X.; Geng, M. Alzheimer’s disease hypothesis and related therapies. Translational Neurodegeneration 2018, 7, 2. [CrossRef]
- Bai, R.; Guo, J.; Ye, X.-Y.; Xie, Y.; Xie, T. Oxidative stress: The core pathogenesis and mechanism of Alzheimer’s disease. Ageing research reviews 2022, 77, 101619. [PubMed]
- Perluigi, M.; Di Domenico, F.; Butterfield, D.A. Oxidative damage in neurodegeneration: Roles in the pathogenesis and progression of Alzheimer disease. Physiological Reviews 2024, 104, 103-197.
- Butterfield, D.A.; Swomley, A.M.; Sultana, R. Amyloid β-peptide (1–42)-induced oxidative stress in Alzheimer disease: importance in disease pathogenesis and progression. Antioxidants & redox signaling 2013, 19, 823-835.
- Bell, S.M.; Barnes, K.; De Marco, M.; Shaw, P.J.; Ferraiuolo, L.; Blackburn, D.J.; Venneri, A.; Mortiboys, H. Mitochondrial dysfunction in Alzheimer’s disease: a biomarker of the future? Biomedicines 2021, 9, 63. [CrossRef]
- Misrani, A.; Tabassum, S.; Yang, L. Mitochondrial dysfunction and oxidative stress in Alzheimer’s disease. Frontiers in aging neuroscience 2021, 13, 57.
- Halliwell, B. Oxidative stress and neurodegeneration: where are we now? Journal of neurochemistry 2006, 97, 1634-1658.
- Kim, G.H.; Kim, J.E.; Rhie, S.J.; Yoon, S. The Role of Oxidative Stress in Neurodegenerative Diseases. Exp Neurobiol 2015, 24, 325-340. [CrossRef] [PubMed]
- Wang, H.; Patterson, C. Atherosclerosis: risks, mechanisms, and therapies; John Wiley & Sons: 2015.
- Dong, X.X.; Wang, Y.; Qin, Z.H. Molecular mechanisms of excitotoxicity and their relevance to pathogenesis of neurodegenerative diseases. Acta Pharmacol Sin 2009, 30, 379-387. [CrossRef]
- Alqahtani, T.; Deore, S.L.; Kide, A.A.; Shende, B.A.; Sharma, R.; Chakole, R.D.; Nemade, L.S.; Kale, N.K.; Borah, S.; Deokar, S.S. Mitochondrial dysfunction and oxidative stress in Alzheimer’s disease, and Parkinson’s disease, Huntington’s disease and amyotrophic lateral sclerosis-an updated review. Mitochondrion 2023.
- Perez Ortiz, J.M.; Swerdlow, R.H. Mitochondrial dysfunction in Alzheimer's disease: Role in pathogenesis and novel therapeutic opportunities. British journal of pharmacology 2019, 176, 3489-3507.
- Wang, X.; Wang, W.; Li, L.; Perry, G.; Lee, H.-g.; Zhu, X. Oxidative stress and mitochondrial dysfunction in Alzheimer's disease. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease 2014, 1842, 1240-1247. [CrossRef] [PubMed]
- Huang, W.J.; Zhang, X.; Chen, W.W. Role of oxidative stress in Alzheimer's disease. Biomedical reports 2016, 4, 519-522. [PubMed]
- Food, U.; Administration, D. FDA grants accelerated approval for Alzheimer’s drug. FDA News Release 2021.
- Wang, Y. An insider's perspective on FDA approval of aducanumab. Alzheimers Dement (N Y) 2023, 9, e12382. [CrossRef]
- Persson, T.; Popescu, B.O.; Cedazo-Minguez, A. Oxidative stress in Alzheimer’s disease: why did antioxidant therapy fail? Oxidative medicine and cellular longevity 2014, 2014.
- Valko, M.; Rhodes, C.; Moncol, J.; Izakovic, M.; Mazur, M. Free radicals, metals and antioxidants in oxidative stress-induced cancer. Chemico-biological interactions 2006, 160, 1-40.
- Koopman, W.J.; Nijtmans, L.G.; Dieteren, C.E.; Roestenberg, P.; Valsecchi, F.; Smeitink, J.A.; Willems, P.H. Mammalian mitochondrial complex I: biogenesis, regulation, and reactive oxygen species generation. Antioxidants & redox signaling 2010, 12, 1431-1470.
- Forster, M.J.; Dubey, A.; Dawson, K.M.; Stutts, W.A.; Lal, H.; Sohal, R.S. Age-related losses of cognitive function and motor skills in mice are associated with oxidative protein damage in the brain. Proceedings of the National Academy of Sciences 1996, 93, 4765-4769.
- Levine, R.L.; Williams, J.A.; Stadtman, E.P.; Shacter, E. [37] Carbonyl assays for determination of oxidatively modified proteins. In Methods in enzymology; Elsevier: 1994; Volume 233, pp. 346-357.
- Mustafa, S.A.; Karieb, S.S.; Davies, S.J.; Jha, A.N. Assessment of oxidative DNA damage, transcriptional expression of key genes, lipid peroxidation and histopathological changes in carp Cyprinus carpio L. following exposure to chronic hypoxic and subsequent recovery in normoxic conditions. Mutagenesis 2015, 30, 107-116. [CrossRef]
- Headlam, H.A.; Davies, M.J. Markers of protein oxidation: different oxidants give rise to variable yields of bound and released carbonyl products. Free Radical Biology and Medicine 2004, 36, 1175-1184. [CrossRef]
- Nadeau, P.J.; Charette, S.J.; Toledano, M.B.; Landry, J. Disulfide bond-mediated multimerization of Ask1 and its reduction by thioredoxin-1 regulate H2O2-induced c-Jun NH2-terminal kinase activation and apoptosis. Molecular biology of the cell 2007, 18, 3903-3913. [CrossRef]
- Yamamoto, H.; Ozaki, T.; Nakanishi, M.; Kikuchi, H.; Yoshida, K.; Horie, H.; Kuwano, H.; Nakagawara, A. Oxidative stress induces p53-dependent apoptosis in hepatoblastoma cell through its nuclear translocation. Genes to Cells 2007, 12, 461-471. [PubMed]
- Cheignon, C.m.; Tomas, M.; Bonnefont-Rousselot, D.; Faller, P.; Hureau, C.; Collin, F. Oxidative stress and the amyloid beta peptide in Alzheimer’s disease. Redox biology 2018, 14, 450-464. [PubMed]
- Gella, A.; Durany, N. Oxidative stress in Alzheimer disease. Cell Adh Migr 2009, 3, 88-93. [CrossRef] [PubMed]
- Andreyev, A.Y.; Kushnareva, Y.E.; Starkov, A. Mitochondrial metabolism of reactive oxygen species. Biochemistry (Moscow) 2005, 70, 200-214. [CrossRef]
- Sheldon, R. Metal-catalyzed oxidations of organic compounds: mechanistic principles and synthetic methodology including biochemical processes; Elsevier: 2012.
- Doorn, J.A.; Petersen, D.R. Covalent adduction of nucleophilic amino acids by 4-hydroxynonenal and 4-oxononenal. Chemico-biological interactions 2003, 143, 93-100. [CrossRef]
- Therade-Matharan, S.; Laemmel, E.; Duranteau, J.; Vicaut, E. Reoxygenation after hypoxia and glucose depletion causes reactive oxygen species production by mitochondria in HUVEC. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology 2004, 287, R1037-R1043. [CrossRef]
- Turrens, J.F. Mitochondrial formation of reactive oxygen species. The Journal of physiology 2003, 552, 335-344. [CrossRef]
- Turrens, J.F. Mitochondrial formation of reactive oxygen species. J Physiol 2003, 552, 335-344. [CrossRef]
- Yan, S.D.; Chen, X.; Fu, J.; Chen, M.; Zhu, H.; Roher, A.; Slattery, T.; Zhao, L.; Nagashima, M.; Morser, J. RAGE and amyloid-β peptide neurotoxicity in Alzheimer's disease. Nature 1996, 382, 685-691.
- Kusano, T.; Nishino, T.; Okamoto, K.; Hille, R.; Nishino, T. The mechanism and significance of the conversion of xanthine dehydrogenase to xanthine oxidase in mammalian secretory gland cells. Redox Biol 2023, 59, 102573. [CrossRef]
- Corvo, M.L.; Marinho, H.S.; Marcelino, P.; Lopes, R.M.; Vale, C.A.; Marques, C.R.; Martins, L.C.; Laverman, P.; Storm, G.; Martins, M.B.A. Superoxide dismutase enzymosomes: Carrier capacity optimization, in vivo behaviour and therapeutic activity. Pharmaceutical research 2015, 32, 91-102.
- Fridovich, I. Superoxide radical and superoxide dismutases. Oxygen and Living Processes: An Interdisciplinary Approach 1981, 250-272.
- Zorov, D.B.; Juhaszova, M.; Sollott, S.J. Mitochondrial reactive oxygen species (ROS) and ROS-induced ROS release. Physiol Rev 2014, 94, 909-950. [CrossRef]
- Okado-Matsumoto, A.; Fridovich, I. Subcellular distribution of superoxide dismutases (SOD) in rat liver: Cu, Zn-SOD in mitochondria. Journal of Biological Chemistry 2001, 276, 38388-38393. [PubMed]
- Butler, J.; Koppenol, W.H.; Margoliash, E. Kinetics and mechanism of the reduction of ferricytochrome c by the superoxide anion. Journal of Biological Chemistry 1982, 257, 10747-10750.
- Andrés, C.M.C.; Pérez de la Lastra, J.M.; Andrés Juan, C.; Plou, F.J.; Pérez-Lebeña, E. Superoxide Anion Chemistry-Its Role at the Core of the Innate Immunity. International journal of molecular sciences 2023, 24. [CrossRef]
- Huang, W.J.; Zhang, X.; Chen, W.W. Role of oxidative stress in Alzheimer's disease. Biomed Rep 2016, 4, 519-522. [CrossRef]
- Chew, H.; Solomon, V.A.; Fonteh, A.N. Involvement of Lipids in Alzheimer's Disease Pathology and Potential Therapies. Front Physiol 2020, 11, 598. [CrossRef]
- Cheignon, C.; Tomas, M.; Bonnefont-Rousselot, D.; Faller, P.; Hureau, C.; Collin, F. Oxidative stress and the amyloid beta peptide in Alzheimer's disease. Redox Biol 2018, 14, 450-464. [CrossRef]
- Ahmad, W.; Ijaz, B.; Shabbiri, K.; Ahmed, F.; Rehman, S. Oxidative toxicity in diabetes and Alzheimer’s disease: mechanisms behind ROS/RNS generation. Journal of biomedical science 2017, 24, 1-10.
- Butterfield, D.A.; Halliwell, B. Oxidative stress, dysfunctional glucose metabolism and Alzheimer disease. Nat Rev Neurosci 2019, 20, 148-160. [CrossRef]
- Bradley-Whitman, M.A.; Lovell, M.A. Biomarkers of lipid peroxidation in Alzheimer disease (AD): an update. Arch Toxicol 2015, 89, 1035-1044. [CrossRef]
- Schaur, R.J.; Siems, W.; Bresgen, N.; Eckl, P.M. 4-Hydroxy-nonenal—A bioactive lipid peroxidation product. Biomolecules 2015, 5, 2247-2337. [CrossRef]
- Zeevalk, G.D.; Bernard, L.P.; Sinha, C.; Ehrhart, J.; Nicklas, W.J. Excitotoxicity and oxidative stress during inhibition of energy metabolism. Dev Neurosci 1998, 20, 444-453. [CrossRef] [PubMed]
- Rolfe, D.F.; Brown, G.C. Cellular energy utilization and molecular origin of standard metabolic rate in mammals. Physiol Rev 1997, 77, 731-758. [CrossRef] [PubMed]
- Wong, H.S.; Dighe, P.A.; Mezera, V.; Monternier, P.A.; Brand, M.D. Production of superoxide and hydrogen peroxide from specific mitochondrial sites under different bioenergetic conditions. J Biol Chem 2017, 292, 16804-16809. [CrossRef] [PubMed]
- Kowalczyk, P.; Sulejczak, D.; Kleczkowska, P.; Bukowska-Ośko, I.; Kucia, M.; Popiel, M.; Wietrak, E.; Kramkowski, K.; Wrzosek, K.; Kaczyńska, K. Mitochondrial Oxidative Stress-A Causative Factor and Therapeutic Target in Many Diseases. International journal of molecular sciences 2021, 22. [CrossRef]
- Afzal, S.; Abdul Manap, A.S.; Attiq, A.; Albokhadaim, I.; Kandeel, M.; Alhojaily, S.M. From imbalance to impairment: the central role of reactive oxygen species in oxidative stress-induced disorders and therapeutic exploration. Front Pharmacol 2023, 14, 1269581. [CrossRef]
- Clemente-Suárez, V.J.; Redondo-Flórez, L.; Beltrán-Velasco, A.I.; Ramos-Campo, D.J.; Belinchón-deMiguel, P.; Martinez-Guardado, I.; Dalamitros, A.A.; Yáñez-Sepúlveda, R.; Martín-Rodríguez, A.; Tornero-Aguilera, J.F. Mitochondria and Brain Disease: A Comprehensive Review of Pathological Mechanisms and Therapeutic Opportunities. Biomedicines 2023, 11. [CrossRef]
- Bell, S.M.; Barnes, K.; De Marco, M.; Shaw, P.J.; Ferraiuolo, L.; Blackburn, D.J.; Venneri, A.; Mortiboys, H. Mitochondrial Dysfunction in Alzheimer's Disease: A Biomarker of the Future? Biomedicines 2021, 9. [CrossRef]
- Yan, X.; Hu, Y.; Wang, B.; Wang, S.; Zhang, X. Metabolic Dysregulation Contributes to the Progression of Alzheimer's Disease. Front Neurosci 2020, 14, 530219. [CrossRef] [PubMed]
- Liang, W.S.; Reiman, E.M.; Valla, J.; Dunckley, T.; Beach, T.G.; Grover, A.; Niedzielko, T.L.; Schneider, L.E.; Mastroeni, D.; Caselli, R.; et al. Alzheimer's disease is associated with reduced expression of energy metabolism genes in posterior cingulate neurons. Proc Natl Acad Sci U S A 2008, 105, 4441-4446. [CrossRef]
- Eckert, A.; Schmitt, K.; Götz, J. Mitochondrial dysfunction - the beginning of the end in Alzheimer's disease? Separate and synergistic modes of tau and amyloid-β toxicity. Alzheimers Res Ther 2011, 3, 15. [CrossRef]
- Wang, X.; Wang, W.; Li, L.; Perry, G.; Lee, H.G.; Zhu, X. Oxidative stress and mitochondrial dysfunction in Alzheimer's disease. Biochim Biophys Acta 2014, 1842, 1240-1247. [CrossRef]
- Khan, S.M.; Cassarino, D.S.; Abramova, N.N.; Keeney, P.M.; Borland, M.K.; Trimmer, P.A.; Krebs, C.T.; Bennett, J.C.; Parks, J.K.; Swerdlow, R.H.; et al. Alzheimer's disease cybrids replicate beta-amyloid abnormalities through cell death pathways. Ann Neurol 2000, 48, 148-155. [PubMed]
- Mecocci, P.; MacGarvey, U.; Beal, M.F. Oxidative damage to mitochondrial DNA is increased in Alzheimer's disease. Ann Neurol 1994, 36, 747-751. [CrossRef]
- Gao, R.; Ma, S.L. Is Mitochondria DNA Variation a Biomarker for AD? Genes (Basel) 2022, 13. [CrossRef]
- Chen, Z.; Zhong, C. Oxidative stress in Alzheimer's disease. Neurosci Bull 2014, 30, 271-281. [CrossRef] [PubMed]
- Wang, Y.; Shi, Y.; Wei, H. Calcium Dysregulation in Alzheimer's Disease: A Target for New Drug Development. J Alzheimers Dis Parkinsonism 2017, 7. [CrossRef]
- Görlach, A.; Bertram, K.; Hudecova, S.; Krizanova, O. Calcium and ROS: A mutual interplay. Redox Biol 2015, 6, 260-271. [CrossRef]
- Wang, C.; Youle, R.J. The role of mitochondria in apoptosis*. Annu Rev Genet 2009, 43, 95-118. [CrossRef] [PubMed]
- Bernardi, P.; Di Lisa, F. The mitochondrial permeability transition pore: molecular nature and role as a target in cardioprotection. J Mol Cell Cardiol 2015, 78, 100-106. [CrossRef]
- Wang, W.; Zhao, F.; Ma, X.; Perry, G.; Zhu, X. Mitochondria dysfunction in the pathogenesis of Alzheimer's disease: recent advances. Mol Neurodegener 2020, 15, 30. [CrossRef]
- Van der Paal, J.; Neyts, E.C.; Verlackt, C.C.W.; Bogaerts, A. Effect of lipid peroxidation on membrane permeability of cancer and normal cells subjected to oxidative stress. Chem Sci 2016, 7, 489-498. [CrossRef] [PubMed]
- Kehm, R.; Baldensperger, T.; Raupbach, J.; Höhn, A. Protein oxidation - Formation mechanisms, detection and relevance as biomarkers in human diseases. Redox Biol 2021, 42, 101901. [CrossRef]
- Davies, M.J. The oxidative environment and protein damage. Biochimica et Biophysica Acta (BBA)-Proteins and Proteomics 2005, 1703, 93-109.
- Gonos, E.S.; Kapetanou, M.; Sereikaite, J.; Bartosz, G.; Naparło, K.; Grzesik, M.; Sadowska-Bartosz, I. Origin and pathophysiology of protein carbonylation, nitration and chlorination in age-related brain diseases and aging. Aging (Albany NY) 2018, 10, 868-901. [CrossRef] [PubMed]
- Ayala, A.; Muñoz, M.F.; Argüelles, S. Lipid peroxidation: production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenal. Oxid Med Cell Longev 2014, 2014, 360438. [CrossRef]
- Singh, M.; Dang, T.N.; Arseneault, M.; Ramassamy, C. Role of by-products of lipid oxidation in Alzheimer's disease brain: a focus on acrolein. J Alzheimers Dis 2010, 21, 741-756. [CrossRef]
- Butterfield, D.A.; Bader Lange, M.L.; Sultana, R. Involvements of the lipid peroxidation product, HNE, in the pathogenesis and progression of Alzheimer's disease. Biochim Biophys Acta 2010, 1801, 924-929. [CrossRef]
- Montine, T.J.; Peskind, E.R.; Quinn, J.F.; Wilson, A.M.; Montine, K.S.; Galasko, D. Increased cerebrospinal fluid F2-isoprostanes are associated with aging and latent Alzheimer's disease as identified by biomarkers. Neuromolecular Med 2011, 13, 37-43. [CrossRef]
- Dang, T.N.; Arseneault, M.; Murthy, V.; Ramassamy, C. Potential role of acrolein in neurodegeneration and in Alzheimer's disease. Curr Mol Pharmacol 2010, 3, 66-78. [PubMed]
- Ali, J.; Aziz, M.A.; Rashid, M.M.O.; Basher, M.A.; Islam, M.S. Propagation of age-related diseases due to the changes of lipid peroxide and antioxidant levels in elderly people: A narrative review. Health Sci Rep 2022, 5, e650. [CrossRef]
- Mark, R.J.; Lovell, M.A.; Markesbery, W.R.; Uchida, K.; Mattson, M.P. A role for 4-hydroxynonenal, an aldehydic product of lipid peroxidation, in disruption of ion homeostasis and neuronal death induced by amyloid β-peptide. Journal of neurochemistry 1997, 68, 255-264. [CrossRef]
- Selley, M.; Close, D.; Stern, S. The effect of increased concentrations of homocysteine on the concentration of (E)-4-hydroxy-2-nonenal in the plasma and cerebrospinal fluid of patients with Alzheimer’s disease. Neurobiology of aging 2002, 23, 383-388. [CrossRef] [PubMed]
- Tamagno, E.; Robino, G.; Obbili, A.; Bardini, P.; Aragno, M.; Parola, M.; Danni, O. H2O2 and 4-hydroxynonenal mediate amyloid β-induced neuronal apoptosis by activating JNKs and p38MAPK. Experimental neurology 2003, 180, 144-155. [CrossRef] [PubMed]
- Butterfield, D.A. Brain lipid peroxidation and alzheimer disease: Synergy between the Butterfield and Mattson laboratories. Ageing Res Rev 2020, 64, 101049. [CrossRef]
- Abdul, H.M.; Sultana, R.; St Clair, D.K.; Markesbery, W.R.; Butterfield, D.A. Oxidative damage in brain from human mutant APP/PS-1 double knock-in mice as a function of age. Free Radic Biol Med 2008, 45, 1420-1425. [CrossRef]
- Butterfield, D.A.; Castegna, A.; Lauderback, C.M.; Drake, J. Evidence that amyloid beta-peptide-induced lipid peroxidation and its sequelae in Alzheimer’s disease brain contribute to neuronal death. Neurobiology of aging 2002, 23, 655-664. [CrossRef]
- Butterfield, D.A.; Drake, J.; Pocernich, C.; Castegna, A. Evidence of oxidative damage in Alzheimer's disease brain: central role for amyloid β-peptide. Trends in molecular medicine 2001, 7, 548-554. [CrossRef]
- Butterfield, D.A.; Swomley, A.M.; Sultana, R. Amyloid β-peptide (1-42)-induced oxidative stress in Alzheimer disease: importance in disease pathogenesis and progression. Antioxid Redox Signal 2013, 19, 823-835. [CrossRef]
- Yin, H.; Xu, L.; Porter, N.A. Free radical lipid peroxidation: mechanisms and analysis. Chemical reviews 2011, 111, 5944-5972. [PubMed]
- Lovell, M.A.; Markesbery, W.R. Oxidative DNA damage in mild cognitive impairment and late-stage Alzheimer's disease. Nucleic acids research 2007, 35, 7497-7504. [PubMed]
- Collins, A.R.; Dusinska, M.; Gedik, C.M.; Stĕtina, R. Oxidative damage to DNA: do we have a reliable biomarker? Environmental health perspectives 1996, 104, 465-469. [PubMed]
- Gabbita, S.P.; Lovell, M.A.; Markesbery, W.R. Increased nuclear DNA oxidation in the brain in Alzheimer's disease. Journal of neurochemistry 1998, 71, 2034-2040.
- Mattson, M.P.; Chan, S.L. Neuronal and glial calcium signaling in Alzheimer’s disease. Cell calcium 2003, 34, 385-397.
- Nunomura, A.; Perry, G.; Pappolla, M.A.; Wade, R.; Hirai, K.; Chiba, S.; Smith, M.A. RNA oxidation is a prominent feature of vulnerable neurons in Alzheimer’s disease. Journal of Neuroscience 1999, 19, 1959-1964.
- Lovell, M.A.; Gabbita, S.P.; Markesbery, W.R. Increased DNA oxidation and decreased levels of repair products in Alzheimer's disease ventricular CSF. Journal of neurochemistry 1999, 72, 771-776.
- Mecocci, P.; MacGarvey, U.; Beal, M.F. Oxidative damage to mitochondrial DNA is increased in Alzheimer's disease. Annals of Neurology: Official Journal of the American Neurological Association and the Child Neurology Society 1994, 36, 747-751.
- Maynard, S.; Schurman, S.H.; Harboe, C.; de Souza-Pinto, N.C.; Bohr, V.A. Base excision repair of oxidative DNA damage and association with cancer and aging. Carcinogenesis 2009, 30, 2-10. [CrossRef]
- Cannan, W.J.; Pederson, D.S. Mechanisms and Consequences of Double-Strand DNA Break Formation in Chromatin. J Cell Physiol 2016, 231, 3-14. [CrossRef] [PubMed]
- Chen, J.; Potlapalli, R.; Quan, H.; Chen, L.; Xie, Y.; Pouriyeh, S.; Sakib, N.; Liu, L.; Xie, Y. Exploring DNA Damage and Repair Mechanisms: A Review with Computational Insights. BioTech (Basel) 2024, 13. [CrossRef]
- Alexandrov, N.; Alexandrov, V. Computational science research methods for science education at PG level. Procedia Computer Science 2015, 51, 1685-1693.
- Milanowska, K.; Rother, K.; Bujnicki, J.M. Databases and bioinformatics tools for the study of DNA repair. Molecular biology international 2011, 2011.
- Lei, T.; Du, S.; Peng, Z.; Chen, L. Multifaceted regulation and functions of 53BP1 in NHEJ-mediated DSB repair (Review). Int J Mol Med 2022, 50. [CrossRef]
- Zentout, S.; Smith, R.; Jacquier, M.; Huet, S. New methodologies to study DNA repair processes in space and time within living cells. Frontiers in Cell and Developmental Biology 2021, 9, 730998.
- Mohandas, E.; Rajmohan, V.; Raghunath, B. Neurobiology of Alzheimer's disease. Indian J Psychiatry 2009, 51, 55-61. [CrossRef]
- Tamagno, E.; Guglielmotto, M.; Vasciaveo, V.; Tabaton, M. Oxidative Stress and Beta Amyloid in Alzheimer's Disease. Which Comes First: The Chicken or the Egg? Antioxidants (Basel, Switzerland) 2021, 10. [CrossRef]
- Reiss, A.B.; Arain, H.A.; Stecker, M.M.; Siegart, N.M.; Kasselman, L.J. Amyloid toxicity in Alzheimer’s disease. Reviews in the Neurosciences 2018, 29, 613-627.
- Butterfield, D.A. The 2013 discovery award from the society for free radical biology and medicine: Selected discoveries from the Butterfield Laboratory of oxidative stress and its sequelae in brain in cognitive disorders exemplified by Alzheimer disease and chemotherapy induced cognitive impairment. Free radical biology & medicine 2014, 157.
- Boutte, A.M.; Woltjer, R.L.; Zimmerman, L.J.; Stamer, S.L.; Montine, K.S.; Manno, M.V.; Cimino, P.J.; Liebler, D.C.; Montine, T.J. Selectively increased oxidative modifications mapped to detergent-insoluble forms of Aβ and β-III tubulin in Alzheimer's disease. The FASEB journal 2006, 20, 1473-1483. [CrossRef]
- Allan Butterfield, D. Amyloid β-peptide (1-42)-induced oxidative stress and neurotoxicity: implications for neurodegeneration in Alzheimer's disease brain. A review. Free radical research 2002, 36, 1307-1313. [CrossRef] [PubMed]
- Dean, R.T.; FU, S.; Stocker, R.; Davies, M.J. Biochemistry and pathology of radical-mediated protein oxidation. Biochemical Journal 1997, 324, 1-18. [CrossRef] [PubMed]
- Takuma, K.; Yao, J.; Huang, J.; Xu, H.; Chen, X.; Luddy, J.; Trillat, A.-C.; Stern, D.M.; Arancio, O.; Yan, S.S. ABAD enhances Aβ-induced cell stress via mitochondrial dysfunction. The FASEB Journal 2005, 19, 1-25. [CrossRef]
- Persson, T.; Popescu, B.O.; Cedazo-Minguez, A. Oxidative stress in Alzheimer’s disease: why did antioxidant therapy fail? Oxidative medicine and cellular longevity 2014, 2014, 427318. [CrossRef] [PubMed]
- Akterin, S.; Cowburn, R.F.; Miranda-Vizuete, A.; Jiménez, A.; Bogdanovic, N.; Winblad, B.; Cedazo-Minguez, A. Involvement of glutaredoxin-1 and thioredoxin-1 in β-amyloid toxicity and Alzheimer's disease. Cell Death & Differentiation 2006, 13, 1454-1465.
- Cenini, G.; Sultana, R.; Memo, M.; Butterfield, D.A. Elevated levels of pro-apoptotic p53 and its oxidative modification by the lipid peroxidation product, HNE, in brain from subjects with amnestic mild cognitive impairment and Alzheimer's disease. Journal of cellular and molecular medicine 2008, 12, 987-994. [CrossRef]
- Sharma, A.; Sharma, R.; Chaudhary, P.; Vatsyayan, R.; Pearce, V.; Jeyabal, P.V.; Zimniak, P.; Awasthi, S.; Awasthi, Y.C. 4-Hydroxynonenal induces p53-mediated apoptosis in retinal pigment epithelial cells. Archives of biochemistry and biophysics 2008, 480, 85-94. [CrossRef]
- Mandelkow, E.M.; Mandelkow, E. Biochemistry and cell biology of tau protein in neurofibrillary degeneration. Cold Spring Harb Perspect Med 2012, 2, a006247. [CrossRef]
- Alavi Naini, S.M.; Soussi-Yanicostas, N. Tau Hyperphosphorylation and Oxidative Stress, a Critical Vicious Circle in Neurodegenerative Tauopathies? Oxid Med Cell Longev 2015, 2015, 151979. [CrossRef]
- Liu, Z.; Li, T.; Li, P.; Wei, N.; Zhao, Z.; Liang, H.; Ji, X.; Chen, W.; Xue, M.; Wei, J. The Ambiguous Relationship of Oxidative Stress, Tau Hyperphosphorylation, and Autophagy Dysfunction in Alzheimer's Disease. Oxid Med Cell Longev 2015, 2015, 352723. [CrossRef]
- Dhapola, R.; Beura, S.K.; Sharma, P.; Singh, S.K.; HariKrishnaReddy, D. Oxidative stress in Alzheimer's disease: current knowledge of signaling pathways and therapeutics. Mol Biol Rep 2024, 51, 48. [CrossRef] [PubMed]
- Lee, K.Y.; Koh, S.H.; Noh, M.Y.; Park, K.W.; Lee, Y.J.; Kim, S.H. Glycogen synthase kinase-3beta activity plays very important roles in determining the fate of oxidative stress-inflicted neuronal cells. Brain Res 2007, 1129, 89-99. [CrossRef]
- Morel, M.; Authelet, M.; Dedecker, R.; Brion, J.P. Glycogen synthase kinase-3beta and the p25 activator of cyclin dependent kinase 5 increase pausing of mitochondria in neurons. Neuroscience 2010, 167, 1044-1056. [CrossRef] [PubMed]
- Mudher, A.; Shepherd, D.; Newman, T.A.; Mildren, P.; Jukes, J.P.; Squire, A.; Mears, A.; Drummond, J.A.; Berg, S.; MacKay, D.; et al. GSK-3beta inhibition reverses axonal transport defects and behavioural phenotypes in Drosophila. Mol Psychiatry 2004, 9, 522-530. [CrossRef]
- Ibáñez-Salazar, A.; Bañuelos-Hernández, B.; Rodríguez-Leyva, I.; Chi-Ahumada, E.; Monreal-Escalante, E.; Jiménez-Capdeville, M.E.; Rosales-Mendoza, S. Oxidative Stress Modifies the Levels and Phosphorylation State of Tau Protein in Human Fibroblasts. Front Neurosci 2017, 11, 495. [CrossRef]
- Sanacora, G.; Rothman, D.L.; Mason, G.; Krystal, J.H. Clinical studies implementing glutamate neurotransmission in mood disorders. Annals of the New York Academy of Sciences 2003, 1003, 292-308.
- Krystal, J.H.; Tolin, D.F.; Sanacora, G.; Castner, S.A.; Williams, G.V.; Aikins, D.E.; Hoffman, R.E.; D'Souza, D.C. Neuroplasticity as a target for the pharmacotherapy of anxiety disorders, mood disorders, and schizophrenia. Drug discovery today 2009, 14, 690-697.
- Pekny, M.; Nilsson, M. Astrocyte activation and reactive gliosis. Glia 2005, 50, 427-434. [CrossRef] [PubMed]
- Lipton, S.A.; Rosenberg, P.A. Excitatory amino acids as a final common pathway for neurologic disorders. New England Journal of Medicine 1994, 330, 613-622.
- Meldrum, B.S. The role of glutamate in epilepsy and other CNS disorders. Neurology 1994, 44, S14-23.
- Maragakis, N.J.; Rothstein, J.D. Mechanisms of disease: astrocytes in neurodegenerative disease. Nature clinical practice Neurology 2006, 2, 679-689.
- Kew, J.N.; Kemp, J.A. Ionotropic and metabotropic glutamate receptor structure and pharmacology. Psychopharmacology 2005, 179, 4-29. [PubMed]
- Gjessing, L.; Gjesdahl, P.; Sjaastad, O. The free amino acids in human cerebrospinal fluid. 1972.
- Danbolt, N.C. Glutamate uptake. Progress in neurobiology 2001, 65, 1-105. [PubMed]
- Görlach, A.; Bertram, K.; Hudecova, S.; Krizanova, O. Calcium and ROS: A mutual interplay. Redox biology 2015, 6, 260-271. [PubMed]
- Girouard, H.; Wang, G.; Gallo, E.F.; Anrather, J.; Zhou, P.; Pickel, V.M.; Iadecola, C. NMDA receptor activation increases free radical production through nitric oxide and NOX2. Journal of Neuroscience 2009, 29, 2545-2552. [CrossRef]
- Mattson, M.P.; Magnus, T. Ageing and neuronal vulnerability. Nature reviews neuroscience 2006, 7, 278-294.
- Szule, J.A.; Jung, J.H.; McMahan, U.J. The structure and function of ‘active zone material’at synapses. Philosophical Transactions of the Royal Society B: Biological Sciences 2015, 370, 20140189.
- DeKosky, S.T.; Scheff, S.W. Synapse loss in frontal cortex biopsies in Alzheimer's disease: correlation with cognitive severity. Annals of Neurology: Official Journal of the American Neurological Association and the Child Neurology Society 1990, 27, 457-464.
- Jang, S.-S.; Chung, H.J. Emerging link between Alzheimer’s disease and homeostatic synaptic plasticity. Neural plasticity 2016, 2016, 7969272.
- Chen, T.S.; Huang, T.H.; Lai, M.C.; Huang, C.W. The Role of Glutamate Receptors in Epilepsy. Biomedicines 2023, 11. [CrossRef]
- Bliss, T.V.; Cooke, S.F. Long-term potentiation and long-term depression: a clinical perspective. Clinics (Sao Paulo) 2011, 66 Suppl 1, 3-17. [CrossRef]
- Srivastava, A.; Das, B.; Yao, A.Y.; Yan, R. Metabotropic Glutamate Receptors in Alzheimer's Disease Synaptic Dysfunction: Therapeutic Opportunities and Hope for the Future. J Alzheimers Dis 2020, 78, 1345-1361. [CrossRef] [PubMed]
- Tönnies, E.; Trushina, E. Oxidative Stress, Synaptic Dysfunction, and Alzheimer's Disease. J Alzheimers Dis 2017, 57, 1105-1121. [CrossRef]
- Newcomer, J.W.; Farber, N.B.; Olney, J.W. NMDA receptor function, memory, and brain aging. Dialogues in clinical neuroscience 2000, 2, 219-232. [CrossRef] [PubMed]
- Frankland, P.W.; Bontempi, B. The organization of recent and remote memories. Nature reviews neuroscience 2005, 6, 119-130. [PubMed]
- Trushina, E.; McMurray, C. Oxidative stress and mitochondrial dysfunction in neurodegenerative diseases. Neuroscience 2007, 145, 1233-1248.
- Bezprozvanny, I.; Mattson, M.P. Neuronal calcium mishandling and the pathogenesis of Alzheimer's disease. Trends Neurosci 2008, 31, 454-463. [CrossRef]
- Parsons, M.P.; Raymond, L.A. Extrasynaptic NMDA receptor involvement in central nervous system disorders. Neuron 2014, 82, 279-293. [CrossRef]
- Lipton, S.A. Paradigm shift in neuroprotection by NMDA receptor blockade: memantine and beyond. Nat Rev Drug Discov 2006, 5, 160-170. [CrossRef]
- Hsieh, H.; Boehm, J.; Sato, C.; Iwatsubo, T.; Tomita, T.; Sisodia, S.; Malinow, R. AMPAR removal underlies Abeta-induced synaptic depression and dendritic spine loss. Neuron 2006, 52, 831-843. [CrossRef]
- Shichiri, M. The role of lipid peroxidation in neurological disorders. J Clin Biochem Nutr 2014, 54, 151-160. [CrossRef]
- Westra, M.; Gutierrez, Y.; MacGillavry, H.D. Contribution of Membrane Lipids to Postsynaptic Protein Organization. Front Synaptic Neurosci 2021, 13, 790773. [CrossRef] [PubMed]
- Tolar, M.; Hey, J.; Power, A.; Abushakra, S. Neurotoxic Soluble Amyloid Oligomers Drive Alzheimer's Pathogenesis and Represent a Clinically Validated Target for Slowing Disease Progression. International journal of molecular sciences 2021, 22. [CrossRef]
- McDaid, J.; Mustaly-Kalimi, S.; Stutzmann, G.E. Ca(2+) Dyshomeostasis Disrupts Neuronal and Synaptic Function in Alzheimer's Disease. Cells 2020, 9. [CrossRef]
- Wang, R.; Reddy, P.H. Role of Glutamate and NMDA Receptors in Alzheimer's Disease. J Alzheimers Dis 2017, 57, 1041-1048. [CrossRef]
- Birben, E.; Sahiner, U.M.; Sackesen, C.; Erzurum, S.; Kalayci, O. Oxidative stress and antioxidant defense. World Allergy Organ J 2012, 5, 9-19. [CrossRef] [PubMed]
- Joe, E.; Ringman, J.M. Cognitive symptoms of Alzheimer's disease: clinical management and prevention. Bmj 2019, 367, l6217. [CrossRef]
- Söderberg, L.; Johannesson, M.; Nygren, P.; Laudon, H.; Eriksson, F.; Osswald, G.; Möller, C.; Lannfelt, L. Lecanemab, Aducanumab, and Gantenerumab - Binding Profiles to Different Forms of Amyloid-Beta Might Explain Efficacy and Side Effects in Clinical Trials for Alzheimer's Disease. Neurotherapeutics 2023, 20, 195-206. [CrossRef]
- Barthold, D.; Joyce, G.; Ferido, P.; Drabo, E.F.; Marcum, Z.A.; Gray, S.L.; Zissimopoulos, J. Pharmaceutical Treatment for Alzheimer's Disease and Related Dementias: Utilization and Disparities. J Alzheimers Dis 2020, 76, 579-589. [CrossRef] [PubMed]
- Arias-Sánchez, R.A.; Torner, L.; Fenton Navarro, B. Polyphenols and Neurodegenerative Diseases: Potential Effects and Mechanisms of Neuroprotection. Molecules 2023, 28. [CrossRef]
- Alkhalifa, A.E.; Al-Ghraiybah, N.F.; Kaddoumi, A. Extra-Virgin Olive Oil in Alzheimer's Disease: A Comprehensive Review of Cellular, Animal, and Clinical Studies. International journal of molecular sciences 2024, 25. [CrossRef]
- Rathod, N.B.; Elabed, N.; Punia, S.; Ozogul, F.; Kim, S.K.; Rocha, J.M. Recent Developments in Polyphenol Applications on Human Health: A Review with Current Knowledge. Plants (Basel) 2023, 12. [CrossRef]
- Bucciantini, M.; Leri, M.; Nardiello, P.; Casamenti, F.; Stefani, M. Olive Polyphenols: Antioxidant and Anti-Inflammatory Properties. Antioxidants (Basel, Switzerland) 2021, 10. [CrossRef]
- Zhang, Y.H.; Wang, D.W.; Xu, S.F.; Zhang, S.; Fan, Y.G.; Yang, Y.Y.; Guo, S.Q.; Wang, S.; Guo, T.; Wang, Z.Y.; Guo, C. α-Lipoic acid improves abnormal behavior by mitigation of oxidative stress, inflammation, ferroptosis, and tauopathy in P301S Tau transgenic mice. Redox Biol 2018, 14, 535-548. [CrossRef]
- Afzal, O.; Dalhat, M.H.; Altamimi, A.S.A.; Rasool, R.; Alzarea, S.I.; Almalki, W.H.; Murtaza, B.N.; Iftikhar, S.; Nadeem, S.; Nadeem, M.S.; Kazmi, I. Green Tea Catechins Attenuate Neurodegenerative Diseases and Cognitive Deficits. Molecules 2022, 27. [CrossRef]
- Cassidy, L.; Fernandez, F.; Johnson, J.B.; Naiker, M.; Owoola, A.G.; Broszczak, D.A. Oxidative stress in alzheimer's disease: A review on emergent natural polyphenolic therapeutics. Complement Ther Med 2020, 49, 102294. [CrossRef]
- Kim, J.H.; Ju, I.G.; Kim, N.; Huh, E.; Son, S.R.; Hong, J.P.; Choi, Y.; Jang, D.S.; Oh, M.S. Yomogin, Isolated from Artemisia iwayomogi, Inhibits Neuroinflammation Stimulated by Lipopolysaccharide via Regulating MAPK Pathway. Antioxidants (Basel, Switzerland) 2022, 12. [CrossRef]
- Zhou, X.; Li, Y.; Shi, X.; Ma, C. An overview on therapeutics attenuating amyloid β level in Alzheimer's disease: targeting neurotransmission, inflammation, oxidative stress and enhanced cholesterol levels. Am J Transl Res 2016, 8, 246-269. [PubMed]
- Ekert, J.O.; Gould, R.L.; Reynolds, G.; Howard, R.J. TNF alpha inhibitors in Alzheimer's disease: A systematic review. Int J Geriatr Psychiatry 2018, 33, 688-694. [CrossRef]
- Lương, K.; Nguyen, L.T. The role of Beta-adrenergic receptor blockers in Alzheimer's disease: potential genetic and cellular signaling mechanisms. Am J Alzheimers Dis Other Demen 2013, 28, 427-439. [CrossRef]
- Qin, J.; Ma, Z.; Chen, X.; Shu, S. Microglia activation in central nervous system disorders: A review of recent mechanistic investigations and development efforts. Front Neurol 2023, 14, 1103416. [CrossRef]
- Kisby, B.; Jarrell, J.T.; Agar, M.E.; Cohen, D.S.; Rosin, E.R.; Cahill, C.M.; Rogers, J.T.; Huang, X. Alzheimer's Disease and Its Potential Alternative Therapeutics. J Alzheimers Dis Parkinsonism 2019, 9. [CrossRef]
- Ouyang, Y.; Chen, Z.; Tan, M.; Liu, A.; Chen, M.; Liu, J.; Pi, R.; Fang, J. Carvedilol, a third-generation β-blocker prevents oxidative stress-induced neuronal death and activates Nrf2/ARE pathway in HT22 cells. Biochem Biophys Res Commun 2013, 441, 917-922. [CrossRef] [PubMed]
- Khalaf, S.S.; Hafez, M.M.; Mehanna, E.T.; Mesbah, N.M.; Abo-Elmatty, D.M. Combined vildagliptin and memantine treatment downregulates expression of amyloid precursor protein, and total and phosphorylated tau in a rat model of combined Alzheimer's disease and type 2 diabetes. Naunyn Schmiedebergs Arch Pharmacol 2019, 392, 685-695. [CrossRef] [PubMed]
- Shukla, M.; Govitrapong, P.; Boontem, P.; Reiter, R.J.; Satayavivad, J. Mechanisms of Melatonin in Alleviating Alzheimer's Disease. Curr Neuropharmacol 2017, 15, 1010-1031. [CrossRef]
- Sun, T.C.; Liu, X.C.; Yang, S.H.; Song, L.L.; Zhou, S.J.; Deng, S.L.; Tian, L.; Cheng, L.Y. Melatonin Inhibits Oxidative Stress and Apoptosis in Cryopreserved Ovarian Tissues via Nrf2/HO-1 Signaling Pathway. Front Mol Biosci 2020, 7, 163. [CrossRef]
- Merlo, S.; Spampinato, S.F.; Sortino, M.A. Early compensatory responses against neuronal injury: A new therapeutic window of opportunity for Alzheimer's Disease? CNS Neurosci Ther 2019, 25, 5-13. [CrossRef]
- Perez Ortiz, J.M.; Swerdlow, R.H. Mitochondrial dysfunction in Alzheimer's disease: Role in pathogenesis and novel therapeutic opportunities. Br J Pharmacol 2019, 176, 3489-3507. [CrossRef]
- Salman, M.; Akram, M.; Shahrukh, M.; Ishrat, T.; Parvez, S. Effects of pramipexole on beta-amyloid(1-42) memory deficits and evaluation of oxidative stress and mitochondrial function markers in the hippocampus of Wistar rat. Neurotoxicology 2022, 92, 91-101. [CrossRef]
- Wang, J.; Jia, Y.; Li, G.; Wang, B.; Zhou, T.; Zhu, L.; Chen, T.; Chen, Y. The Dopamine Receptor D3 Regulates Lipopolysaccharide-Induced Depressive-Like Behavior in Mice. Int J Neuropsychopharmacol 2018, 21, 448-460. [CrossRef]
- Chen, J.Y.; Zhu, Q.; Zhang, S.; OuYang, D.; Lu, J.H. Resveratrol in experimental Alzheimer's disease models: A systematic review of preclinical studies. Pharmacol Res 2019, 150, 104476. [CrossRef]
- Wang, N.; He, J.; Pan, C.; Wang, J.; Ma, M.; Shi, X.; Xu, Z. Resveratrol Activates Autophagy via the AKT/mTOR Signaling Pathway to Improve Cognitive Dysfunction in Rats With Chronic Cerebral Hypoperfusion. Front Neurosci 2019, 13, 859. [CrossRef] [PubMed]
- Schweiger, S.; Matthes, F.; Posey, K.; Kickstein, E.; Weber, S.; Hettich, M.M.; Pfurtscheller, S.; Ehninger, D.; Schneider, R.; Krauß, S. Resveratrol induces dephosphorylation of Tau by interfering with the MID1-PP2A complex. Sci Rep 2017, 7, 13753. [CrossRef]
- Detrait, E.R.; Danis, B.; Lamberty, Y.; Foerch, P. Peripheral administration of an anti-TNF-α receptor fusion protein counteracts the amyloid induced elevation of hippocampal TNF-α levels and memory deficits in mice. Neurochem Int 2014, 72, 10-13. [CrossRef] [PubMed]
- Lee, I.T.; Luo, S.F.; Lee, C.W.; Wang, S.W.; Lin, C.C.; Chang, C.C.; Chen, Y.L.; Chau, L.Y.; Yang, C.M. Overexpression of HO-1 protects against TNF-alpha-mediated airway inflammation by down-regulation of TNFR1-dependent oxidative stress. Am J Pathol 2009, 175, 519-532. [CrossRef] [PubMed]
- Ortí-Casañ, N.; Wu, Y.; Naudé, P.J.W.; De Deyn, P.P.; Zuhorn, I.S.; Eisel, U.L.M. Targeting TNFR2 as a Novel Therapeutic Strategy for Alzheimer's Disease. Front Neurosci 2019, 13, 49. [CrossRef]
- Thakur, S.; Dhapola, R.; Sarma, P.; Medhi, B.; Reddy, D.H. Neuroinflammation in Alzheimer's Disease: Current Progress in Molecular Signaling and Therapeutics. Inflammation 2023, 46, 1-17. [CrossRef]
- Yang, M.; Chen, J.; Zhao, J.; Meng, M. Etanercept attenuates myocardial ischemia/reperfusion injury by decreasing inflammation and oxidative stress. PloS one 2014, 9, e108024. [CrossRef]
- Khalatbary, A.R.; Khademi, E. The green tea polyphenolic catechin epigallocatechin gallate and neuroprotection. Nutr Neurosci 2020, 23, 281-294. [CrossRef]
- Han, J.; Wang, M.; Jing, X.; Shi, H.; Ren, M.; Lou, H. (-)-Epigallocatechin gallate protects against cerebral ischemia-induced oxidative stress via Nrf2/ARE signaling. Neurochem Res 2014, 39, 1292-1299. [CrossRef]
- Pierzynowska, K.; Podlacha, M.; Gaffke, L.; Majkutewicz, I.; Mantej, J.; Węgrzyn, A.; Osiadły, M.; Myślińska, D.; Węgrzyn, G. Autophagy-dependent mechanism of genistein-mediated elimination of behavioral and biochemical defects in the rat model of sporadic Alzheimer's disease. Neuropharmacology 2019, 148, 332-346. [CrossRef]
- Devi, K.P.; Shanmuganathan, B.; Manayi, A.; Nabavi, S.F.; Nabavi, S.M. Molecular and Therapeutic Targets of Genistein in Alzheimer's Disease. Mol Neurobiol 2017, 54, 7028-7041. [CrossRef] [PubMed]
- Guo, J.; Yang, G.; He, Y.; Xu, H.; Fan, H.; An, J.; Zhang, L.; Zhang, R.; Cao, G.; Hao, D.; Yang, H. Involvement of α7nAChR in the Protective Effects of Genistein Against β-Amyloid-Induced Oxidative Stress in Neurons via a PI3K/Akt/Nrf2 Pathway-Related Mechanism. Cell Mol Neurobiol 2021, 41, 377-393. [CrossRef] [PubMed]
Figure 1.
Various pathophysiological mechanisms involved in Alzheimer's disease. These include but are not limited to interconnected processes such as OS and neurotoxicity that directly and indirectly contribute to the initiation and progression of the disease in addition to pathological hallmarks of AD, Aβ, and NFTs. Abbreviations: acetylcholinesterase (AChE), AMP-activated protein kinase (AMPK), amyloid precursor protein (APP), autophagy-related (ATG), beta-site amyloid precursor protein cleaving enzyme 1 (BACE-1), choline acetyltransferase (ChAT), cy-clooxygenase-2 (COX-2), glutathione peroxidase (GPx), glutathione (GSH), glycogen syn-thase kinase-3 beta (GSK-3β), interleukin-1 beta (IL-1β), interleukin-6 (IL-6), microtu-bule-associated protein 1A/1B-light chain 3 (LC3), malondialdehyde (MDA), matrix met-alloproteinase-9 (MMP-9), mechanistic target of rapamycin (mTOR), muscarinic acetyl-choline receptor (mAChR), nicotinic acetylcholine receptor (nAChR), nuclear factor kappa B (NF-kB), p62/sequestosome 1 (p62/SQSTM1), presenilin 1/2 (PSEN1/2), superoxide dismutase (SOD), tumor necrosis factor-alpha (TNF-α), vesicu-lar acetylcholine transporter (VAChT), and zonula occludens-1 (ZO-1).
Figure 1.
Various pathophysiological mechanisms involved in Alzheimer's disease. These include but are not limited to interconnected processes such as OS and neurotoxicity that directly and indirectly contribute to the initiation and progression of the disease in addition to pathological hallmarks of AD, Aβ, and NFTs. Abbreviations: acetylcholinesterase (AChE), AMP-activated protein kinase (AMPK), amyloid precursor protein (APP), autophagy-related (ATG), beta-site amyloid precursor protein cleaving enzyme 1 (BACE-1), choline acetyltransferase (ChAT), cy-clooxygenase-2 (COX-2), glutathione peroxidase (GPx), glutathione (GSH), glycogen syn-thase kinase-3 beta (GSK-3β), interleukin-1 beta (IL-1β), interleukin-6 (IL-6), microtu-bule-associated protein 1A/1B-light chain 3 (LC3), malondialdehyde (MDA), matrix met-alloproteinase-9 (MMP-9), mechanistic target of rapamycin (mTOR), muscarinic acetyl-choline receptor (mAChR), nicotinic acetylcholine receptor (nAChR), nuclear factor kappa B (NF-kB), p62/sequestosome 1 (p62/SQSTM1), presenilin 1/2 (PSEN1/2), superoxide dismutase (SOD), tumor necrosis factor-alpha (TNF-α), vesicu-lar acetylcholine transporter (VAChT), and zonula occludens-1 (ZO-1).
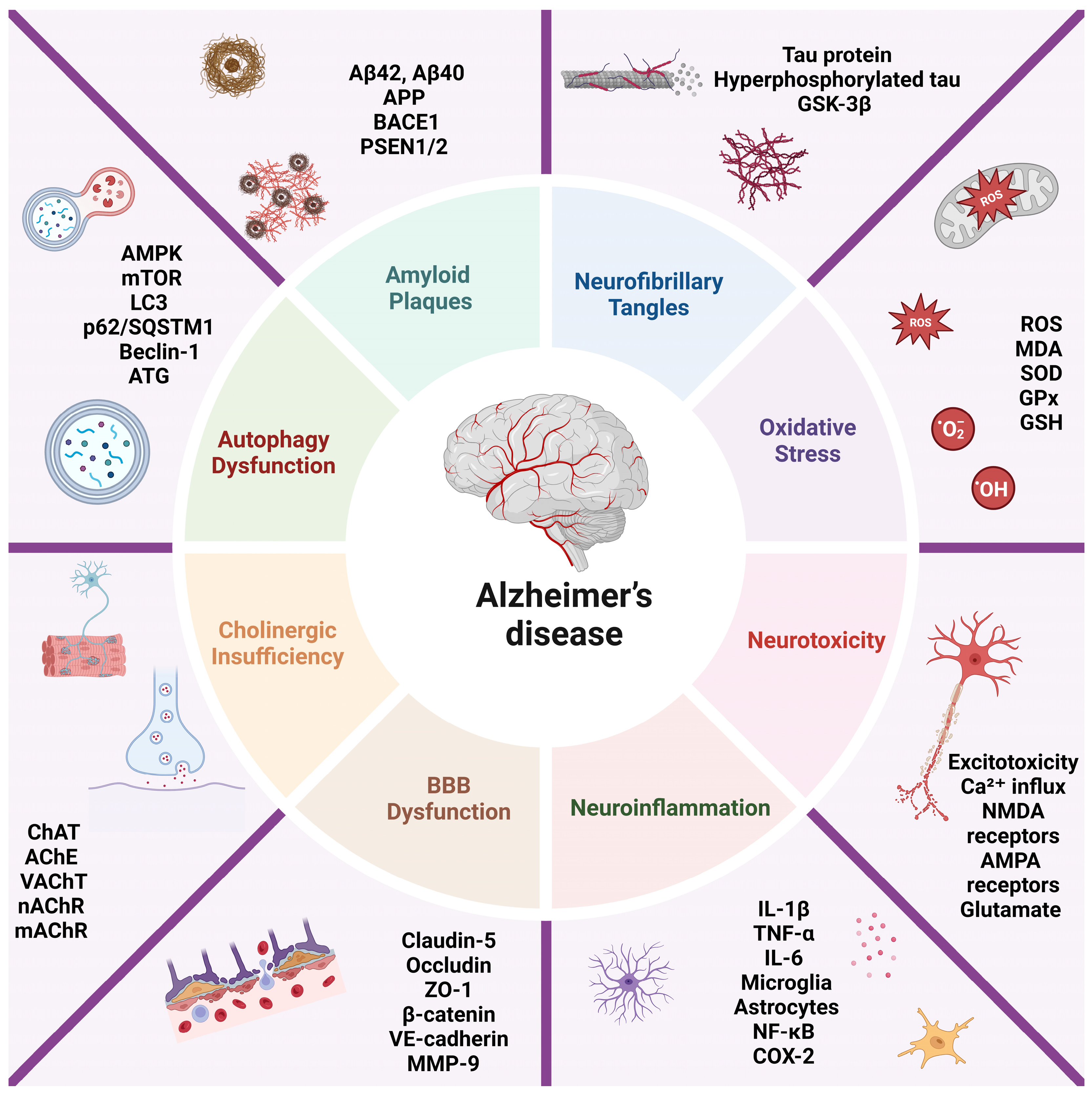
Figure 2.
PRISMA diagram illustrating the selection process of the articles included in the review.
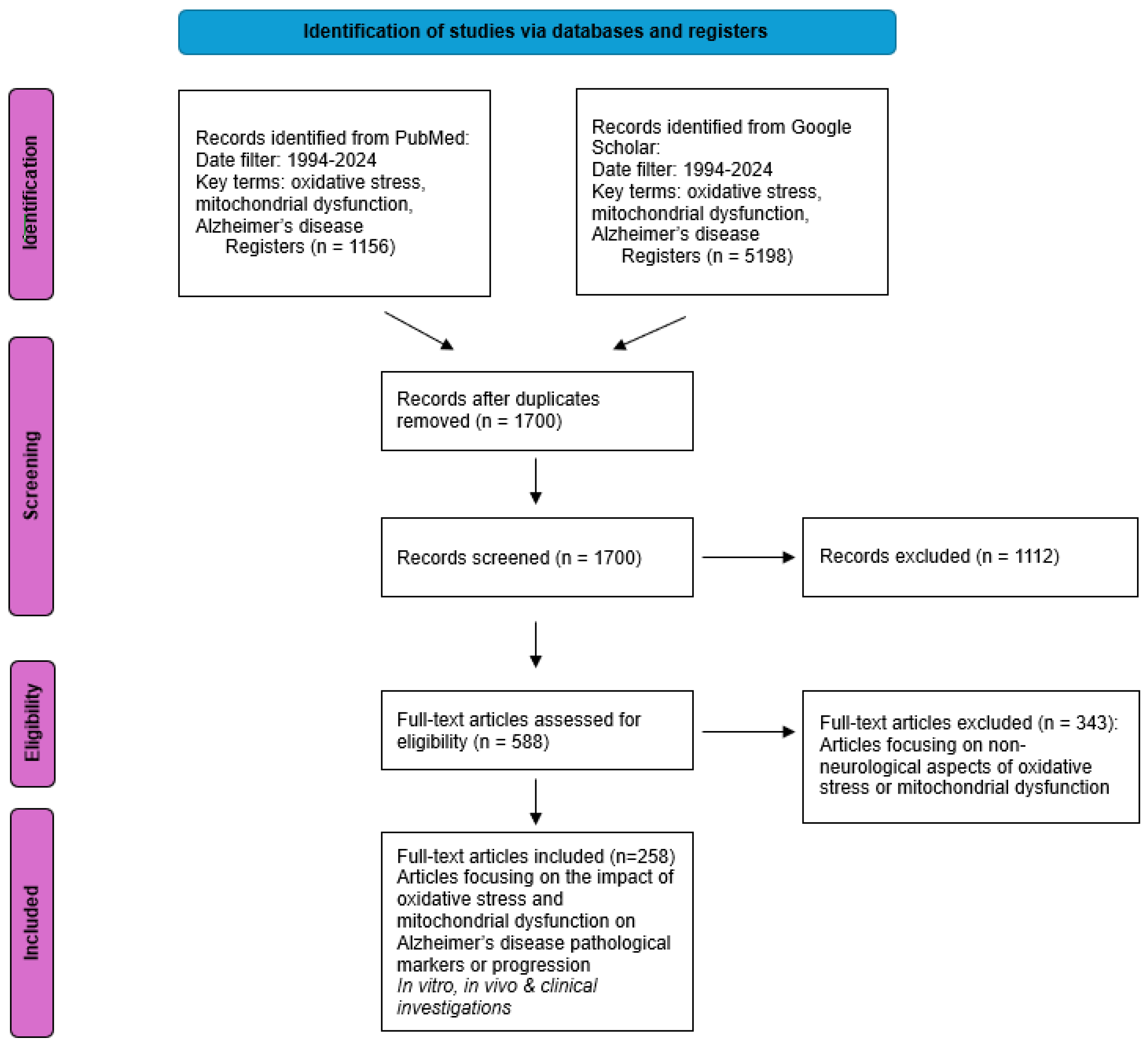
Figure 3.
The relationship between mitochondrial dysfunction, OS, and AD. At the core of cellular metabolism, mitochondria generate energy through the electron transport chain (ETC), a series of protein complexes embedded in the inner mitochondrial membrane. The ETC facilitates the transfer of electrons from nicotinamide adenine dinucleotide (NADH) and flavin adenine dinucleotide (FADH2) through complexes I to IV, culminating in the reduction of oxygen to water and the synthesis of ATP via ATP synthase. During this process, ROS are generated as by-products. Excessive ROS production, as indicated in the figure, leads to OS, damaging cellular components such as lipids, proteins, and DNA. This oxidative damage is particularly detrimental to neuronal cells, contributing to the pathogenesis of AD. The schematic highlights how metabolic intermediates like glucose and pyruvate fuel the tricarboxylic acid (TCA) cycle, producing substrates for the ETC. However, dysregulation in these pathways exacerbates ROS production, ultimately promoting neurodegenerative processes associated with AD, as depicted by the brain image showing areas affected by the disease.
Figure 3.
The relationship between mitochondrial dysfunction, OS, and AD. At the core of cellular metabolism, mitochondria generate energy through the electron transport chain (ETC), a series of protein complexes embedded in the inner mitochondrial membrane. The ETC facilitates the transfer of electrons from nicotinamide adenine dinucleotide (NADH) and flavin adenine dinucleotide (FADH2) through complexes I to IV, culminating in the reduction of oxygen to water and the synthesis of ATP via ATP synthase. During this process, ROS are generated as by-products. Excessive ROS production, as indicated in the figure, leads to OS, damaging cellular components such as lipids, proteins, and DNA. This oxidative damage is particularly detrimental to neuronal cells, contributing to the pathogenesis of AD. The schematic highlights how metabolic intermediates like glucose and pyruvate fuel the tricarboxylic acid (TCA) cycle, producing substrates for the ETC. However, dysregulation in these pathways exacerbates ROS production, ultimately promoting neurodegenerative processes associated with AD, as depicted by the brain image showing areas affected by the disease.
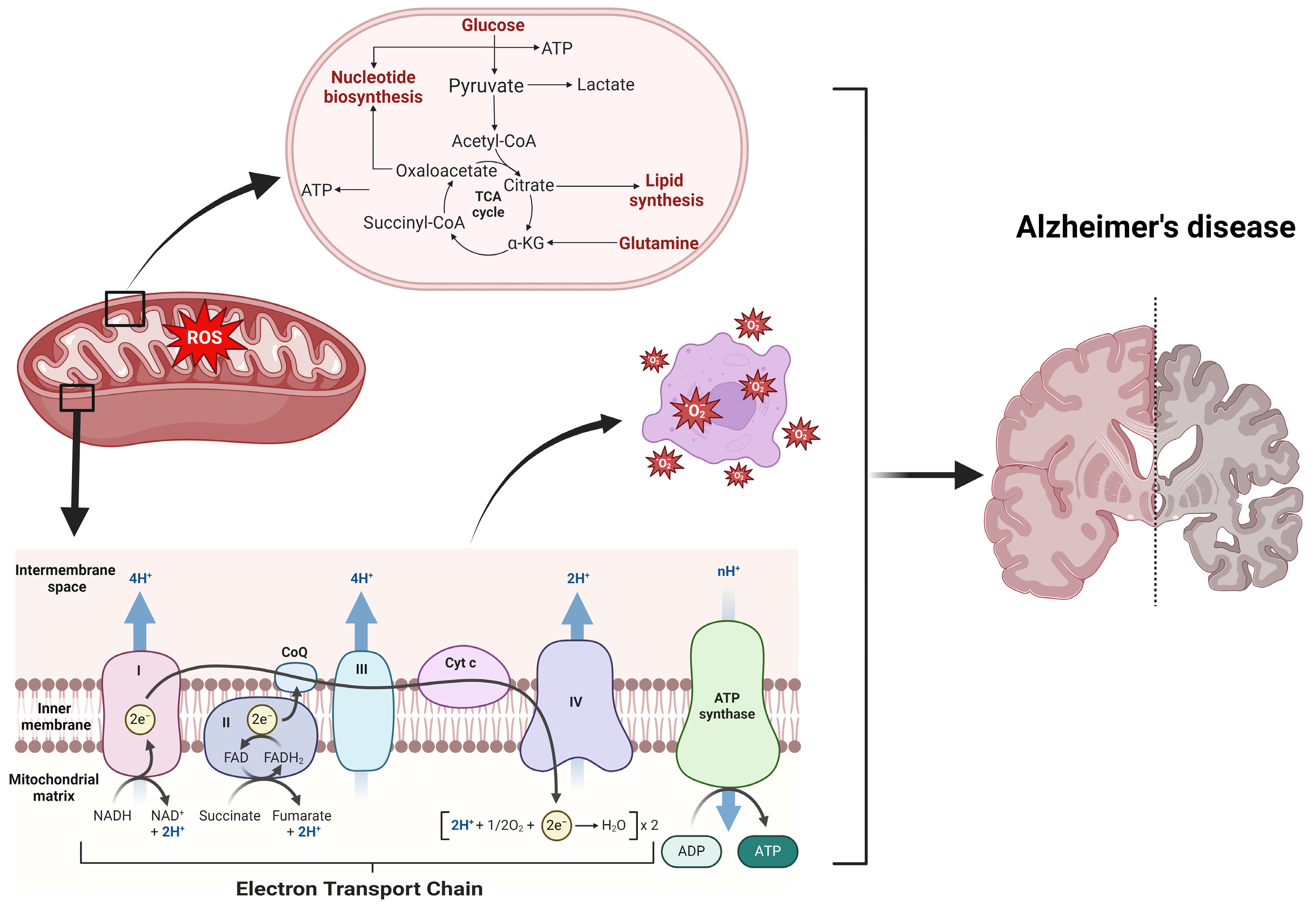
Figure 4.
Summary of the primary exogenous and endogenous antioxidant defenses for ROS/RNS elimination.
Figure 4.
Summary of the primary exogenous and endogenous antioxidant defenses for ROS/RNS elimination.
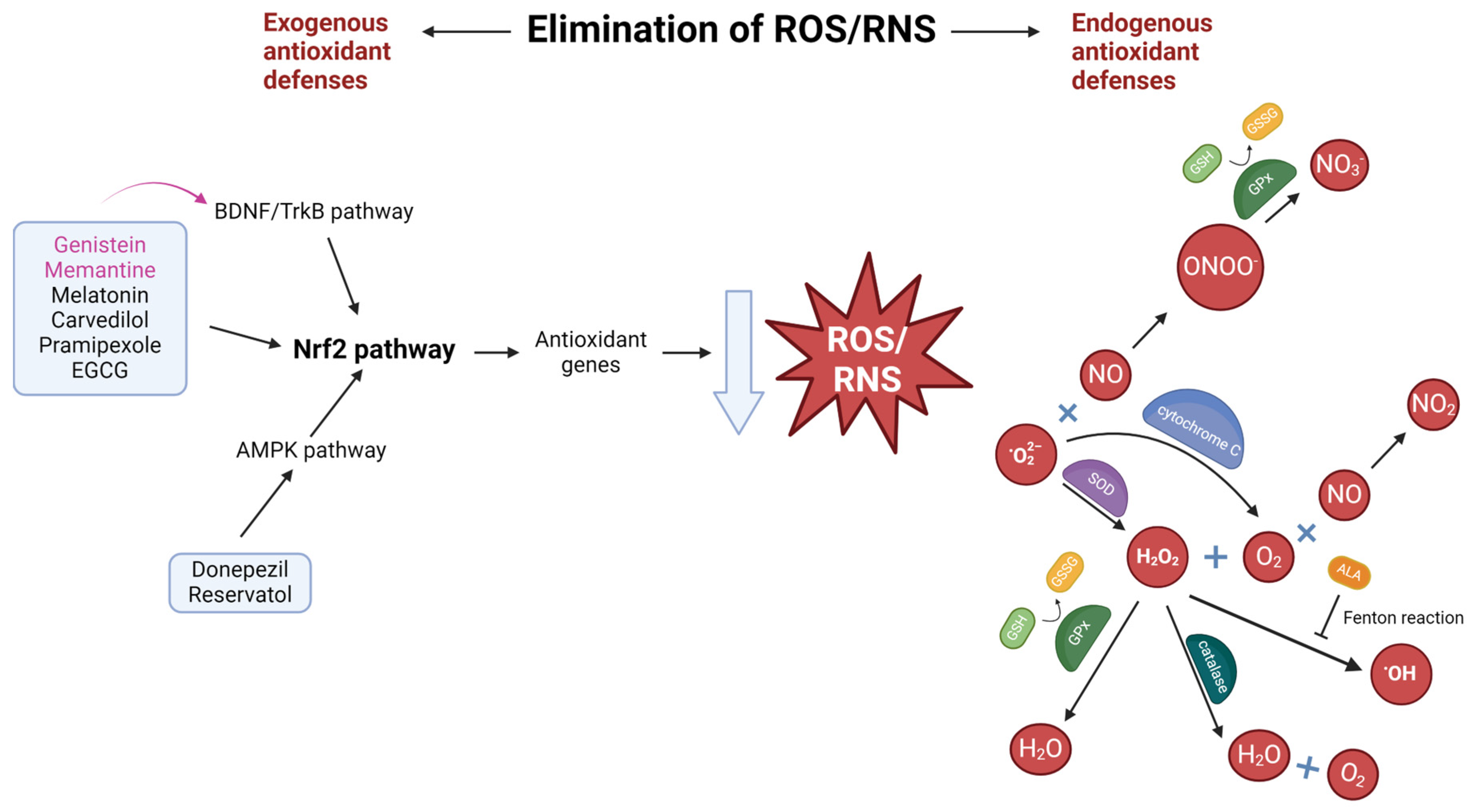
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



