
Submitted:
18 August 2024
Posted:
19 August 2024
You are already at the latest version
Abstract
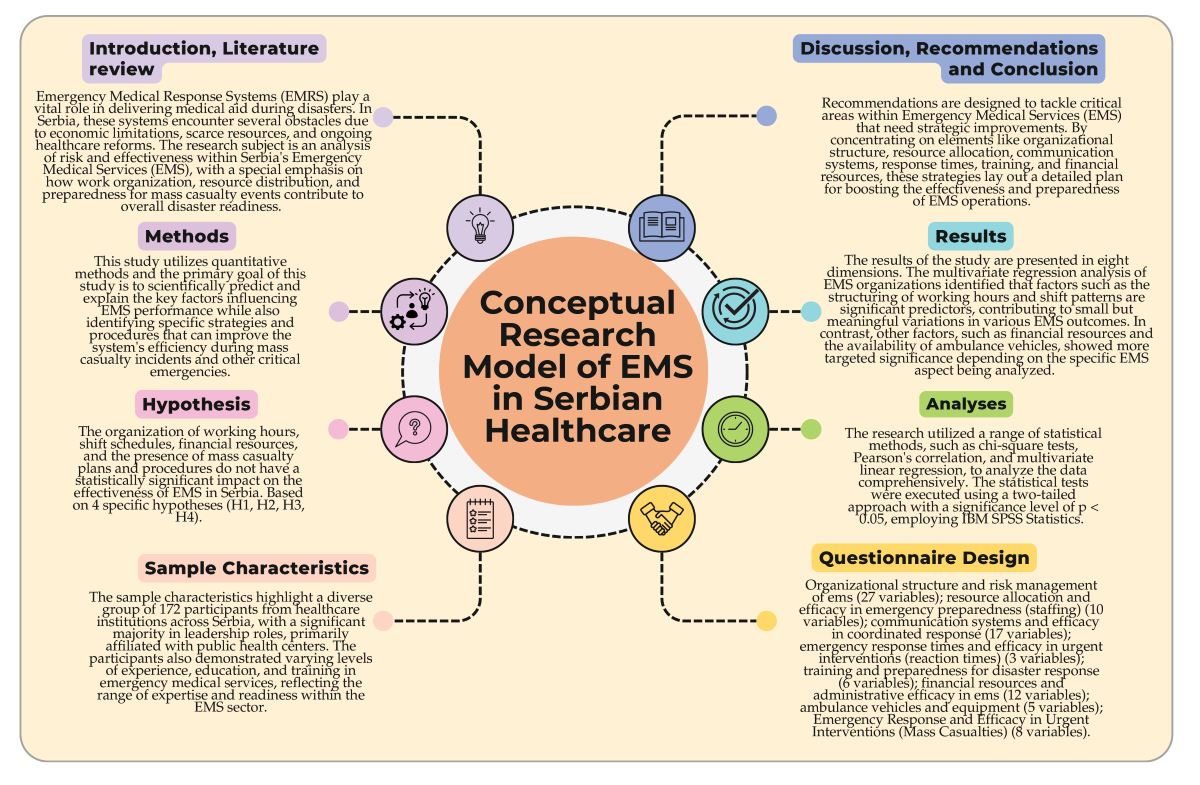
Emergency Medical Response Systems (EMRS) play a vital role in delivering medical aid during disasters. In Serbia, these systems encounter several obstacles due to economic limitations, scarce resources, and ongoing healthcare reforms, all of which affect their performance. This study focuses on examining the risk factors and effectiveness of Serbia's EMRS, identifying systemic issues, and proposing enhancements to improve emergency preparedness for disasters. A survey was conducted across healthcare institutions in Serbia to gather comprehensive insights. The survey explored various aspects, including organizational structures, resource distribution, communication systems, and the speed of emergency responses. Statistical methods such as Pearson's correlation, multivariate regression analysis and chi-square tests were utilized to interpret data collected from 172 healthcare institutions. The multivariate regression analysis of EMS organization identified that factors such as the structuring of working hours and shift patterns are significant predictors, contributing to small but meaningful variations in various EMS outcomes. In contrast, other factors, such as financial resources and the availability of ambulance vehicles, showed more targeted significance depending on the specific EMS aspect being analyzed. Institutions with written mass casualty plans and procedures demonstrate superior effectiveness in EMS activities, excelling in resource allocation, operational continuity, and emergency preparedness, particularly through enhanced coordination and specialized systems for managing large-scale emergencies. The findings highlighted notable disparities in how EMRS are organized, with only 46% of institutions having specific emergency departments. Resource limitations were evident, as many facilities operated with minimal staff and outdated equipment. The communication systems revealed weaknesses, with just 54% having established protocols for handling emergency calls. Response times frequently surpassed international standards, which negatively affected patient outcomes. Additionally, the study found training deficiencies, with 68% of participants expressing a need for further education. Serbia’s EMRS are significantly impacted by systemic issues such as insufficient funding, disjointed service delivery, and inadequate training. Overcoming these challenges necessitates a comprehensive approach that includes boosting financial support, implementing standardized protocols, and fostering enhanced collaboration across different sectors.
Keywords:
risk
; disaster
; emergency preparedness
; efficacy
; comprehensive survey
; emergency medical response systems
; vulnerabilities
; Serbian healthcare
1. Introduction
Emergency Medical Response Systems (EMRS) are vital components of healthcare, providing crucial medical assistance to individuals in urgent need, such as natural and man-made (technological) disasters [1,2,3]. The effectiveness of these systems can have a profound impact on patient outcomes, especially in critical, life-threatening situations [4,5]. In Serbia, the healthcare sector has encountered numerous obstacles, such as economic limitations, resource scarcity, and ongoing reform transitions, which influence the performance of its EMRS [6,7,8,9]. The evolution of emergency medical services (EMS) in Serbia has progressed alongside the country’s broader healthcare system, reflecting significant socio-economic and political shifts [10,11,12]. The EMS framework in Serbia has historically been shaped by the Yugoslavian healthcare model, which emphasized accessibility and comprehensiveness [13,14]. However, the disintegration of Yugoslavia and the ensuing conflicts in the 1990s caused substantial disruptions in healthcare delivery, including emergency services [14].
Reforms initiated post-2000 aimed to align Serbian EMS with European standards and have met with varying degrees of success. Initial reform efforts concentrated on restructuring organizational frameworks, boosting funding, and enhancing training programs for medical personnel [15,16,17]. Despite these reforms, ongoing issues such as inadequate infrastructure and an insufficient workforce continue to challenge the system’s ability to deliver timely and effective emergency care [18]. Serbia’s EMRS is currently organized into several key components: pre-hospital care, hospital emergency departments, and specialized emergency units [12,19]. Pre-hospital care involves dispatch centers and ambulance services, which are crucial for ensuring rapid response times. Nonetheless, research indicates that response times in Serbia frequently surpass international benchmarks due to logistical challenges and resource limitations [20].
Hospital emergency departments in Serbia grapple with issues such as overcrowding, understaffing, and outdated equipment [21]. These problems are exacerbated by the limited presence of specialized emergency units, like trauma and cardiac care centres, particularly in rural regions [1,4,8,12,15,21]. The effectiveness of EMRS in Serbia is further hampered by uneven distribution of healthcare resources and disparities in access to emergency care between urban and rural populations [22,23,24].
Several risk factors impact the performance of EMRS in Serbia, including systemic, organizational, and operational challenges [25]. The Serbian healthcare system is plagued by chronic underfunding, affecting all levels of healthcare delivery, including emergency services [26]. Limited financial resources result in inadequate investment in infrastructure, technology, and human resources, leading to subpar EMRS performance [9,15,24]. Inefficiencies such as fragmented service delivery and lack of coordination between different healthcare sectors impede the effectiveness of EMRS. Furthermore, the absence of standardized national protocols for emergency medical care leads to inconsistencies in service quality and patient outcomes [27]. Operational risks include delays in response times, insufficient training for EMS personnel, and lack of access to advanced medical equipment. These factors contribute to increased morbidity and mortality rates among emergency patients [28]. Additionally, emergency medical technicians and paramedics often experience high levels of occupational stress and burnout, which can adversely affect their performance and decision-making abilities [6,29].
The efficacy of EMRS in Serbia is assessed through various indicators, including response times, patient outcomes, and system efficiency. Response time is a crucial indicator of EMRS efficacy, as it directly influences patient survival rates, especially in cases of cardiac arrest, trauma, and stroke [30]. Studies reveal that response times in Serbia often exceed recommended international standards, mainly due to logistical challenges and resource constraints [6]. Patient outcomes in emergency scenarios are affected by the quality of pre-hospital and in-hospital care. Research suggests that patient outcomes in Serbia are frequently suboptimal due to delays in care, inadequate medical interventions, and limited access to specialized emergency services [31,32]. System efficiency is influenced by resource allocation, coordination among healthcare sectors, and the implementation of evidence-based protocols [33]. Efforts to improve system efficiency in Serbia have focused on enhancing communication systems, optimizing resource allocation, and implementing training programs for EMS personnel [1,2,21,34].
Addressing the risks and enhancing the efficacy of EMRS in Serbia requires a multifaceted approach involving policy, organizational, and operational interventions [35,36,37,38,39,40]. Policy initiatives should focus on increasing funding for emergency services, developing standardized national protocols for emergency care, and promoting inter-sectoral collaboration to improve coordination between healthcare sectors [41,42]. Organizational strategies should aim to enhance service delivery by improving communication systems [43,44], optimizing resource allocation, and implementing evidence-based protocols for emergency care [42]. Efforts to decentralize healthcare services and encourage regional collaboration can also help address disparities in access to emergency care [45]. Operational measures should concentrate on improving response times, enhancing training and education for EMS personnel, and ensuring access to advanced medical equipment. Initiatives to reduce occupational stress and burnout among EMS personnel can also enhance performance and patient outcomes [46,47,48].
Regarding that, this study delves into the analysis of risk and effectiveness within Serbia’s Emergency Medical Services (EMS), with a special emphasis on how work organization, resource distribution, and preparedness for mass casualty events contribute to overall disaster readiness. Also, the primary goal of this study is to scientifically predict and explain the key factors influencing EMS performance while also identifying specific strategies and procedures that can im-prove the system’s efficiency during mass casualty incidents and other critical emergencies.
1.1. Literature Review
Emergency Medical Response Systems (EMRS) worldwide have been extensively analyzed, providing valuable insights into their strengths, challenges, and best practices across various regions [5,6,33,42,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64]. Studies from outside Serbia have identified common themes, such as the necessity for well-organized protocols [45,65], efficient resource distribution [51,66,67,68], and ongoing EMS personnel training [69,70,71,72]. Research from countries like Germany and the United Kingdom highlights the significance of standardized national protocols in ensuring consistent, high-quality care [10,73,74,75]. In Germany, nationwide protocols have enhanced coordination among emergency services and reduced response times, leading to better patient outcomes [76]. Similarly, the UK’s National Health Service (NHS) emphasizes standardized training and procedures, which have contributed to high survival rates in critical emergencies like cardiac arrests [77,78].
Effective resource allocation and infrastructure are key to EMRS’s success [19,79]. A U.S. studies found that urban EMS systems with access to advanced medical technologies and well-equipped ambulances achieved shorter response times and better outcomes compared to rural areas with fewer resources [73,80,81,82]. Conversely, in countries with weaker infrastructure, longer response times have been linked to lower survival rates in trauma and cardiac emergencies [83]. Ongoing training is critical for effective EMS systems [81]. In Canada and Australia, EMS personnel regularly participate in simulation exercises and refresher courses, improving their ability to make decisions under pressure and reducing medical errors [84,85]. Japan’s EMS training integrates disaster preparedness, which has proven effective in large-scale emergencies such as natural disasters [86,87].
Technology plays a crucial role in enhancing EMRS effectiveness [88,89]. In South Korea, advanced telemedicine systems allow EMS teams to provide real-time medical consultations, improving pre-hospital care quality [90]. Similarly, Scandinavian countries use GPS-based dispatch systems to optimize emergency vehicle deployment, reducing response times, particularly in rural areas [91]. In low-middle-income countries, resource limitations hinder EMRS efficiency. For example, sub-Saharan Africa struggles with inadequate training, poor infrastructure, and limited access to essential equipment [92]. However, community-based EMS models have shown promise in expanding access to care in remote areas [93]. Innovations like motorcycle ambulances have also helped overcome transportation challenges in urban areas with poor road infrastructure [94].
Furthermore, the presence of written mass casualty plans has been shown to significantly improve the performance of EMRS [50,82,95,96]. Institutions with such plans demonstrate better resource allocation, operational continuity, and overall preparedness during large-scale emergencies [97]. However, in Serbia, only 46% of institutions have dedicated emergency departments, and many lack specialized units for trauma and cardiac care [12].
Regarding Serbia, Emergency Medical Response System (EMRS) has seen substantial transformation, particularly driven by the need to modernize and adapt following past disasters. Events such as the 1999 NATO bombings, the devastating 2014 floods, and the COVID-19 pandemic revealed both the system’s strengths and significant weaknesses. In the context of post-conflict and post-disaster settings, Nelson et al. [7] discuss how health-system reforms are often complicated by unforeseen obstacles, frequently arising from inadequate initial evaluations. Expanding on this, Nelson et al. [12] conducted a comprehensive multimodal analysis of Serbia’s emergency medical services, blending both quantitative and qualitative methods. Their findings illuminated critical challenges, including fragmented systems, outdated equipment, inadequate training, and insufficient financial support, all of which hinder the system’s effectiveness.
Further exploration into the health sector’s disaster management by Radović and Ćurčić [9]highlighted the pressing need for improved crisis communication between healthcare providers and emergency services. Their study emphasized that enhanced coordination, along with the development of academic programs, targeted training, and more robust financial investment, is essential for redefining the role of the health workforce within society. The researchers also noted that the dedication and expertise of healthcare professionals are pivotal in rebuilding public trust—an element crucial for effective disaster response.
Comparing EMRS in Serbia with those in other countries provides insights into potential areas for improvement [58]. Countries with well-established EMRS, such as Germany and the United Kingdom, demonstrate several best practices, including standardized national protocols, advanced training programs, and efficient resource allocation [73,74]. Conversely, Serbia faces challenges related to the lack of standardized protocols, limited access to advanced training, and insufficient funding. However, recent initiatives aimed at aligning Serbian EMS with European standards have shown promise, indicating potential for future improvements [62,74].
The urgency of these issues became even more apparent during the COVID-19 pandemic. Madić-Rajćević et al. underscored the necessity for adjustments in workforce planning, education, training, and workload management, particularly for healthcare workers directly involved in patient care. These challenges mirror the findings of Lapčević et al. [98], who evaluated a primary healthcare center’s preparedness following the 2014 floods in Obrenovac using the Hospital Safety Index (HSI). Despite a general level of preparedness, significant gaps were identified, especially in emergency power supply and communication systems, which are vital for maintaining functionality during crises. However, operational challenges are only part of the problem. Inconsistent government funding and frequent political shifts have further impeded long-term disaster preparedness and the effective implementation of policies. According to the World Bank’s 2021 Serbia Emergency COVID-19 Response Project [99], the Serbian healthcare system remains overly focused on curative care, with insufficient emphasis on preventive strategies. This, combined with inefficient use of hospital infrastructure and staffing, has only deepened the system’s vulnerabilities during emergencies.
These systemic weaknesses are reflected in Serbia’s Global Health Security Index (GHSI) rankings [100]. Despite being ranked 59th globally, Serbia shows particularly weak performance in specific areas such as disaster response and health system capacity. In emergency preparedness and response planning, Serbia ranks 72nd, while its health capacity in clinics and hospitals is ranked 84th. The country’s lowest scores are found in categories like political and security risk (148th), financing (146th), risk communication (142nd), and environmental risks (122nd) [99,100].
The World Bank’s Emergency Preparedness and Response Assessment [101] further illustrates the strain on Serbia’s medical response capabilities during disasters. The report highlights limited emergency medical services’ ability to provide advanced life support, as well as the absence of prehospital mass casualty incident structures like organized triage zones, advanced medical posts, and transport staging areas. The lack of regional reserves for emergency medical response, similar to regional fire and rescue reserves, is also a significant shortfall [101].
Serbia’s healthcare system and workforce play an indispensable role in disaster response. Ongoing reforms, along with targeted improvements in communication, coordination, and infrastructure, are crucial for building a more resilient system that can effectively protect public health in future emergencies. Beside that, Vukosavljević et al. [102] emphasize that strategic reforms are not only necessary but also critical for improving public health and disaster preparedness in Serbia. These reforms must be implemented urgently, with well-defined strategies aimed at strengthening the population’s health culture and disaster resilience. Similarly, Cvetković et al. [103] identified significant disparities in public risk perception and behavior during the COVID-19 pandemic, underscoring the need for community-based strategies that encourage behavioral change and improve risk management to bolster national preparedness.
2. Methods
This research delves into the analysis of risk and effectiveness within Serbia’s Emergency Medical Services (EMS), with a special emphasis on how work organization, resource distribution, and preparedness for mass casualty events contribute to overall disaster readiness (see Figure 1).
The primary goal of this study is to scientifically predict and explain the key factors influencing EMS performance while also identifying specific strategies and procedures that can improve the system’s efficiency during mass casualty incidents and other critical emergencies.
Regarding that, this study utilizes quantitative methods, including Pearson’s correlation, multivariate regression analysis and chi-square tests to identify key predictors of risk and efficacy in EMS performance. Additionally, it assesses how mass casualty plans and procedures impact the overall effectiveness of EMS, particularly during large-scale emergencies.
General Hypothesis (H₀):
The organization of working hours, shift schedules, financial resources, and the presence of mass casualty plans and procedures do not have a statistically significant impact on the effectiveness of EMS in Serbia.
Specific Hypotheses:
- H₁ − The organization of working hours and shift schedules significantly improves EMS organization and performance in Serbia.
- H₂ − Financial resources allocated to EMS play a critical role in enhancing the system’s preparedness and operational efficiency during disaster response.
- H₃ − The implementation of mass casualty plans and procedures significantly strengthens EMS readiness and response capabilities in large-scale emergencies.
- H₄ − The availability of ambulance vehicles and specialized equipment significantly enhances the overall effectiveness of EMS, particularly in handling mass casualty incidents.
2.1. Study Area
This research delves into the evaluation of emergency medical response systems within Serbia’s healthcare sector. Situated in Southeast Europe, Serbia occupies the heart of the Balkan Peninsula (see Map 1). The country, home to around 7 million inhabitants, features a varied landscape that includes fertile plains in the north and mountainous terrain in the south, each posing distinct challenges to emergency medical services (EMS) [1,2].
Serbia’s healthcare system is a hybrid model that combines state-run public healthcare with private medical services. Public healthcare operates on three levels: primary, secondary, and tertiary care. Emergency medical services, which are essential to this system, are primarily handled by the public sector. These services are designed to deliver urgent care both before patients reach the hospital and once they are within the hospital setting. The effectiveness and promptness of these services become especially crucial during disasters, whether natural, such as floods or earthquakes, or human-made [6,13,16,17,25,30,42,104,105,106,107].
The study encompasses a broad range of regions across Serbia, including major urban centers like Belgrade and Novi Sad, as well as rural and isolated areas where access to emergency services might be more restricted. This regional diversity facilitates a thorough evaluation of EMS across various environments, addressing the risks and evaluating the efficiency of the existing emergency preparedness and response strategies [7,12].
2.2. Sample Characteristics
The study included 172 participants drawn from various healthcare institutions actively involved in emergency medical services (EMS) across Serbia. A significant portion, 81.4%, were in leadership roles within their institutions, while 13.37% comprised medical staff. The remaining participants were administrative personnel (4.07%) and operational medical staff (1.16%). As for the type of institution, the majority (70.93%) were affiliated with public health centers, 22.67% worked in private healthcare facilities, and 6.40% were connected to hospitals (Table 1).
Participants’ experience levels showed diversity, with nearly half (49.42%) having worked in EMS for 5 to 10 years, 26.16% for less than 5 years, and 24.42% for more than 10 years. Gender distribution was fairly even, with 55.23% male and 44.77% female participants. Regarding education, 58.14% held a bachelor’s degree, 24.42% had earned a master’s degree, and 17.44% had completed high school (Table 1).
A notable 70.93% of participants had undergone one or more training sessions related to emergency medical services, while 29.07% had not received any such training. In their roles, 46.51% of participants identified as coordinators, 29.07% as first responders, and 24.42% as support staff. Additionally, 63.95% of the institutions reported having established mass casualty plans or procedures, while 36.05% did not have such measures in place. This diverse group underscores the varied levels of experience, roles, and readiness among healthcare institutions engaged in emergency medical services throughout Serbia (Table 1).
2.3. Questionnaire Design
A communication was sent to the offices of all city mayors and municipal leaders, requesting that it be relayed to the appropriate healthcare institutions within their areas, specifically those responsible for providing Emergency Medical Services (EMS), such as EMS centers and health clinics. In response, 172 healthcare institutions (Public Health Centers, Hospitals and Private Healthcare Facilities) successfully completed the survey.
The survey questionnaire is crafted to collect in-depth insights into how emergency medical services (EMS) in Serbia are organized and operate. This extensive questionnaire is divided into seven primary sections, each targeting a different aspect of EMS, with a varying number of questions designed to extract precise information. The first section "Organizational structure and Risk Management of Emergency Medical Services" delves into how EMS is structured and managed within institutions. With 27 questions, it aims to shed light on the setup of shifts, the makeup of teams, the operational scope, and how these services cover different territories and demographics. The next section "Resource allocation (staffing) and efficacy in emergency preparedness" focuses on human resources. This section comprises 10 questions intended to gather data on staffing levels, gender and age demographics, educational backgrounds, and the training of EMS personnel. Additionally, it explores staff capacity and adherence to mandatory examinations and legal requirements.
To examine the "Communication systems and efficacy in coordinated response", 17 questions investigate the communication infrastructure’s effectiveness in emergency coordination. This section looks into how calls are managed, the protocols followed, and the technologies employed to facilitate communication between EMS teams and other emergency services. The section about "Reaction time for first order emergencies section", containing 3 questions, is dedicated to evaluating how EMS monitors and reports on reaction times during initial emergency interventions, focusing specifically on the activation and pre-hospital intervention periods.
Exploring the educational aspect, the "Training (education) and preparedness for disaster response" section includes 6 questions that assess EMS staff participation in training centers and the perceived necessity for further education to boost disaster response preparedness. Additional "Funding for Emergency Medical Services (EMS)" features 12 questions that scrutinize the financial resources available to EMS, identifying their sources and how they are allocated for staffing and operational needs. This section evaluates the support from local government and other funding mechanisms. Lastly, the section on "Ambulance Vehicles and Equipment" consists of 5 questions that look into the availability, condition, and functionality of ambulance vehicles and medical equipment, as well as the potential need for additional or updated equipment to ensure operational readiness. In addition, there is a section on "Emergency response and efficacy in urgent interventions, mass casualties", which includes 8 questions to assess EMS preparedness for mass casualty events. It examines the existence of written plans and procedures, along with the frequency and type of training exercises conducted with other rescue services.
Each section is meticulously designed to provide a holistic overview of EMS capabilities and challenges, ensuring that all critical aspects of emergency preparedness and response are comprehensively addressed. Before the study commenced, a dedicated group of experts conducted an in-depth review of all the questions in the questionnaire. This panel was comprised of professionals from various fields pertinent to emergency medical services and disaster preparedness, including specialists in healthcare management, public health policy, and disaster risk management. Their analysis aimed to guarantee that the questions were not only comprehensive and relevant but also reflective of the current socio-economic and political landscape.
Drawing on their expertise, the panel offered numerous suggestions to refine the questionnaire. Their input was geared toward enhancing the clarity and specificity of the questions, ensuring they effectively captured the complexities inherent in emergency medical response systems. The experts also advised updating the questions to align with recent changes in healthcare policies and practices, acknowledging the dynamic nature of disaster risk management. In addition to considering contemporary socio-economic and political factors, the panel conducted a thorough review of existing literature and previous research on emergency medical response to pinpoint gaps and opportunities for improvement. Their insights were pivotal in fine-tuning the questionnaire to more accurately assess the risk and effectiveness of emergency medical response systems within Serbian healthcare.
After the expert review, a pilot study was undertaken to test the revised questionnaire. This preliminary study engaged a small group of participants from various healthcare institutions. Its goal was to evaluate the questionnaire’s functionality, uncover any issues with question interpretation, and assess the overall coherence and flow of the survey. The pilot study yielded valuable insights into the questionnaire’s practical application, highlighting areas where further refinement was needed. Feedback from participants was instrumental in enhancing the language and structure of the questions, ensuring they were clear and pertinent to the respondents’ experiences.
The combination of expert analysis and pilot testing ensured that the final questionnaire was robust, comprehensive, and well-equipped to capture the critical data needed to evaluate the risk and efficacy of emergency medical response systems in the context of disaster preparedness in Serbia.
2.4. Analyses
The research utilized a range of statistical methods, such as chi-square tests, Pearson’s correlation, and multivariate linear regression, to analyze the data comprehensively. Initially, the analysis revealed a breach of the equal variance assumption, prompting the application of the Welch and Brown–Forsythe tests, which are well-suited for handling such deviations. To provide a clear overview of the dataset, descriptive statistical analysis was also carried out. The statistical tests were executed using a two-tailed approach with a significance level of p < 0.05, employing IBM SPSS Statistics (Version 26, New York, NY, USA). Additionally, the study assessed internal consistency across various subscales utilizing Likert scales, yielding promising outcomes. The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the In-stitutional Review Board of the Scientific–Professional Society for Disaster Risk Management and the International Institute for Disaster Research (protocol code 005/2024, 15 July 2024).
3. Results
The results of the study are presented in three dimensions: the predictors of risk and efficacy analysis of emergency medical response systems in Serbian healthcare; correlations and influences of demographic and socioeconomic factors on the perception of risk and efficacy analysis of emergency medical response systems in Serbian healthcare; and descriptive analysis parts: organizational structure and risk management of emergency medical services; resource allocation and efficacy in emergency (disaster) preparedness; communication systems and efficacy in coordinated response; emergency response times and efficacy in urgent interventions; training and preparedness for disaster response; financial resources and administrative efficacy in emergency medical services.
3.1. The Predictors of Risk and Efficacy Analysis of Emergency Medical Response Systems in Serbian Healthcare
The results from the multivariate regression analysis regarding the organization of EMS reveal that both the organization of working hours (β = 0.035) and shift work (β = 0.042) are the most significant predictors, together explaining 1.9% of the variance. Other factors, such as EMS teams working only in the clinic and financial resources, did not show statistically significant effects on EMS organization. This model (R² = 0.019, Adj. R² = 0.006, F = 2.78, t = 59.87, p < 0.05) explains 1.9% of the variance in the organization of EMS, considering all the independent variables included in the analysis (Table 2).
For the number of EMS points performed, the analysis indicates that the organization of shift work (β = −0.045) and working hours (β = −0.037) are significant predictors, accounting for 2.0% of the variance. In contrast, other variables like ambulance vehicles and financial resources did not contribute significantly to the model. This regression model (R² = 0.020, Adj. R² = 0.008, F = 3.15, t = 62.14, p < 0.05) explains 2.0% of the variance in the number of EMS points performed (Table 2).
When it comes to service area coverage, the regression results suggest that none of the predictors were statistically significant. Although the model (R² = 0.027, Adj. R² = 0.015, F = 3.50, t = 63.21, p ≥ 0.05) explains 2.7% of the variance in service area coverage, this relationship was not found to be statistically significant (Table 2).
In the case of the EMS doctors, the presence of EMS teams working only in the clinic (β = 0.07) emerged as a significant predictor, explaining 3.5% of the variance. However, other factors, such as shift work and financial resources, did not show statistical significance. This model (R² = 0.035, Adj. R² = 0.022, F = 3.88, t = 64.45, p < 0.05) accounts for 3.5% of the variance in the total number of EMS doctors (Table 2).
Lastly, the regression analysis related to Plan/procedures for mass casualties indicates that ambulance vehicle availability (β = 0.075) and financial resources (β = 0.033) are significant predictors, explaining 4.1% of the variance. Other variables, such as the organization of working hours, were not significant in this context. This model (R² = 0.041, Adj. R² = 0.030, F = 4.25, t = 65.72, p < 0.05) explains 4.1% of the variance in the presence of plans or procedures for mass casualties (Table 2).
3.2. Correlations and Influences of Demographic and Socioeconomic Factors on the Perception of Risk and Efficacy Analysis of Emergency Medical Response Systems in Serbian Healthcare
Based on Pearson’s correlation results, there is a statistically significant correlation between the EMS organization and several key variables. These include the total number of EMS doctors (p = 0.000), the number of emergency medicine specialists (p = 0.000), the number of doctors in emergency medicine training (p = 0.000), the number of general practitioners in EMS (p = 0.001), the number of permanent EMS ambulance drivers (p = 0.000), the number of day shift teams on weekdays (p = 0.000), the number of night shift teams on weekdays (p = 0.000), the maximum distance from EMS headquarters to the hospital (p = 0.002), the gender distribution of male doctors (p = 0.000), the gender distribution of female doctors (p = 0.009), the number of male emergency medicine specialists (p = 0.000), and the number of female emergency medicine specialists (p = 0.000) (see Table 3).
On the other hand, Pearson’s correlation analysis revealed no statistically significant correlation between EMS organization and other variables such as the average time spent by medical teams at higher-level centers (p = 0.817), the average time spent by transport teams at higher-level centers (p = 0.732), the number of general medicine specialists (p = 0.161), the number of doctors with verified limited working capacity (p = 0.068), standby readiness for doctors (p = 0.059), standby readiness for nurses-technicians (p = 0.088), and the maximum diameter of the EMS service area (p = 0.423) (Table 3).
Furthermore, a statistically significant correlation was identified between the number of EMS points performed and the variable "Doctors with verified limited working capacity" (p = 0.033). However, no significant correlations were found with other variables such as the total number of EMS doctors (p = 0.139), the number of emergency medicine specialists (p = 0.213), the number of doctors in emergency medicine training (p = 0.203), the number of general medicine doctors (p = 0.199), the number of permanent EMS ambulance drivers (p = 0.244), or standby readiness for nurses-technicians (p = 0.299). When it comes to the EMS service area coverage, the analysis did not reveal any statistically significant correlations with any variables, including the average time spent by medical teams (p = 0.232), the average time spent by transport teams (p = 0.338), or any other analyzed factors (Table 3).
Further analyses revealed that as the total number of EMS doctors grows, the organization of EMS services tends to become more structured and effective. A similar pattern is observed with the increase in emergency medicine specialists, where their presence boosts both specialization and the system’s ability to respond swiftly to emergencies. As more doctors enter emergency medicine training, the EMS organization gains strength, which signals a clear emphasis on preparing for the future. Additionally, having more general practitioners involved in EMS correlates with improved coverage and a more solid organizational structure, while a greater number of permanent EMS ambulance drivers leads to noticeable gains in operational efficiency and the overall organization of EMS.
Moreover, adding more day shift teams during weekdays results in better resource management and a more organized EMS system. Similarly, an increase in night shift teams enhances the system’s flexibility, allowing it to meet nighttime demands more effectively. The analysis also pointed out that as the distance between EMS headquarters and the hospital increases, the organization becomes more structured to ensure a timely response and smooth patient transfer.
Regarding gender distribution, a higher percentage of male doctors is linked to a more structured EMS organization, which might be influenced by staffing patterns. On the other hand, an increase in female doctors brings balance to the organization, possibly reflecting a more diverse range of roles within the staff. When the number of male emergency medicine specialists rises, the organization becomes more specialized, focusing on emergency care, and a similar effect is seen with female specialists, where their growing presence contributes to improved preparedness and organization within EMS.
In addition, the data indicates that as the number of doctors with verified limited working capacity increases, there is also an increase in the number of EMS points performed, suggesting that staffing adjustments have been made to accommodate these limitations.
The results of the Chi-square test highlight a statistically significant corelation between the organization of emergency medical services (EMS) and several critical variables. Notably, there is a strong relationship between EMS organization and how EMS activities are conducted (p = 0.001), the number of points where these activities take place (p = 0.005), and the structure of working hours (p = 0.001). The organization of shift work (p = 0.001) and the presence of a dedicated EMS team working exclusively in the clinic (p = 0.004) also show significant correlations (Table 4).
In addition, the number of ambulance transport teams per shift during the day (p = 0.001), night (p = 0.001), and weekends (p = 0.001) is significantly tied to EMS organization. Other relevant factors include the composition of the ambulance transport team (p = 0.001), on-call duties in cases where the team needs to leave the territory (p = 0.003), and whether the regular shift workload includes additional responsibilities (p = 0.001). Further significant correlations emerged regarding the number of doctors in EMS (p = 0.006), the regularity of annual medical examinations for doctors (p = 0.002), limited work capacity (p = 0.005), and the number of ambulance drivers (p = 0.001). Communication-related aspects such as having a separate phone number for ambulance transport (p = 0.007), call identification features (p = 0.018), the presence of a call recorder (p = 0.003), and recording calls on this system (p = 0.001) also demonstrated significant relationships (Table 4).
Moreover, the condition of radio repeaters (p = 0.008), the installation of radio stations in ambulances (p = 0.001), and having a power supply backup for the radio system in case of outages (p = 0.001) were all significantly correlated with EMS organization. Lastly, factors such as maintaining a dedicated communication channel with the police (p = 0.005) and firefighters-rescuers (p = 0.003), monitoring response times during interventions (p = 0.001), and training for emergency medicine doctors (p = 0.004) and nurses (p = 0.003) also showed significant associations (Table 4).
Further analysis show that institutions with well-organized EMS systems exhibit a higher level of efficiency in conducting emergency medical activities, particularly when operating across multiple locations (27.3%) compared to single-point operations (20.3%). This ability to manage multiple service points ensures that resources are distributed evenly, reducing response times and enhancing the quality of care provided. The flexibility that comes from organizing EMS across various points (41.1%) further strengthens these institutions, enabling them to allocate staff and resources more effectively to meet community needs.
The organization of working hours, including structured shifts, plays a crucial role in maintaining continuous service and adapting to varying demands. Institutions that implement structured 8-hour shifts (24.4%) or other types of shifts (55.8%) can ensure that trained personnel are always available to respond to emergencies. A focus on shift work (42.4%) also helps institutions keep EMS teams well-rested and ready for emergencies at all times, reducing burnout and improving the overall quality of service provided. Specialized EMS teams working exclusively in clinics (28.9%) enhance clinic-based interventions, with staff trained to handle specific medical scenarios more effectively. Similarly, institutions that allocate more teams for ambulance transport during day shifts (43.5%) or night shifts (43.0%) can manage high-demand periods with greater efficiency, ensuring prompt responses to emergency calls. This flexibility extends to weekends and holidays, where well-organized EMS teams (47.1%) maintain uninterrupted service even during peak times.
Effective resource management is vital for institutions with dedicated ambulance transport teams (34.7%) and well-organized on-call duty systems (42.4%), particularly when teams must leave their designated areas. By balancing regular shift workloads (48.6%), these institutions ensure that EMS teams are not overwhelmed and can continue delivering consistent care. Moreover, institutions with a higher number of doctors in their EMS teams (42.4%) and those that conduct regular medical examinations for staff (26.2%) are better equipped to maintain a healthy, capable workforce.
Also, reliable communication systems are essential for EMS operations. Institutions with separate phone lines for ambulance transport (23.3%) and call identification capabilities (45.3%) are better organized, enabling them to handle emergency calls efficiently. Established protocols for receiving calls (53.2%) and call recording capabilities (42.0%) further enhance the quality of service by ensuring that communications are documented and reviewed. Additionally, equipping ambulances with radio stations (58.4%) and maintaining functional radio repeaters (26.2%) guarantees that communication channels remain operational during emergencies.
Institutions that foster collaboration with other emergency services demonstrate improved coordination during crises. Those with dedicated communication channels with police (26.2%) and firefighters (26.2%) can work more effectively with these agencies during joint operations, ensuring timely medical support in various emergency scenarios. Regular monitoring of intervention reaction times (39.5%) and specialized training for emergency medicine doctors and nurses (42.4%) also contribute to the institution’s ability to handle a wide range of medical emergencies.
Finally, institutions that receive additional financial resources for healthcare (40.7%) are better positioned to expand services, hire more staff, and maintain well-equipped ambulance vehicles (42.4%). This financial support, coupled with vehicles for mass casualty incidents (34.7%) and written plans for handling such events (48.8%), ensures that EMS teams are prepared for large-scale emergencies. Regular exercises and drills (41.8%) with other first responders also help these institutions refine their response strategies, ensuring that all personnel are ready to act efficiently during real-world crises.
The results from the Chi-square test reveal statistically significant correlations between EMS employee training and a range of key variables. Notably, there is a strong correlation between EMS employee training and the conducting of EMS activities (p = 0.001), as well as with the organization of working hours (p = 0.002) and shift work (p = 0.001). Additionally, significant correlations were identified between EMS employee training and the number of ambulance transport teams working both day (p = 0.001) and night (p = 0.003) shifts, along with those working on weekends (p = 0.001). The data also shows significant relationships between EMS employee training and the organization of on-call duty when teams are outside their designated areas (p = 0.001), the implementation of protocols and procedures for receiving calls (p = 0.000), and the monitoring of response times during interventions (p = 0.000). Moreover, there are strong correlations with the availability of dedicated communication channels with the police (p = 0.000) and firefighters (p = 0.002), as well as with the financial resources allocated to healthcare (p = 0.003). EMS employee training also shows significant correlations with the presence of triage tags (p = 0.002), exercises for responding to mass casualty incidents (p = 0.001), and joint exercises with other first responders (p = 0.005). For the remaining variables, no statistically significant correlations were found (Table 4).
Further analysis show that carrying out EMS activities is notably more effective in institutions where employees have undergone formal training at recognized centers. These institutions exhibit a higher level of operational readiness, ensuring their staff is well-prepared to handle various medical emergencies. This preparation is evident in their ability to allocate tasks more efficiently, reducing the risk of errors during critical incidents. Also, when it comes to organizing working hours, institutions with formally trained staff are more likely to implement structured shifts (41.9%). This structured approach allows for better shift management, ensuring that trained personnel are available around the clock to handle emergencies. This leads to more consistent and dependable service delivery.
Similarly, institutions with trained EMS personnel are more likely to utilize shift work (42.4%), which supports continuous service provision. This systematic organization of shifts allows them to respond effectively to increased demand during peak periods, ensuring that qualified professionals are always present. For teams working exclusively in clinics, training in established centers correlates with better organizational efficiency (28.9%). Such institutions are more adept at handling clinic-based interventions, as their specialized training equips staff with the necessary skills to manage specific medical scenarios. Resource allocation during day shifts, particularly for ambulance transport, is more efficient in institutions with trained EMS staff (43.5%). This allows for more effective use of teams during busy hours, facilitating quicker responses to emergency situations.
At night, these institutions also excel in organizing shifts for ambulance transport (43.0%), ensuring adequate staffing during off-peak hours. This ability to maintain round-the-clock coverage helps meet emergency transport needs effectively. During weekends and holidays, institutions with trained staff are better equipped to manage ambulance transport services (47.1%), ensuring they can handle high demand without sacrificing care quality. When it comes to on-call duties, particularly when teams need to leave their designated areas, institutions with trained EMS staff demonstrate better management (42.4%). These organizations can maintain sufficient coverage, even when on-call teams are deployed to other locations.
Regular shift workloads are more effectively managed in institutions with trained personnel (48.6%). This allows them to balance emergency response with routine medical tasks without overwhelming their teams. In terms of staffing, institutions with more trained EMS personnel tend to have a more balanced distribution of doctors across teams (42.4%), ensuring that medical expertise is available whenever needed, thereby enhancing the quality of care provided. Institutions with dedicated ambulance transport phone lines (55.0%) are also more common where staff have received formal training. This specialization enhances their ability to coordinate emergency responses and streamline communication.
The implementation of call identification systems is more prevalent in institutions with trained EMS staff (45.3%), improving their ability to direct resources efficiently to where they are most needed, which shortens response times. Furthermore, institutions with trained personnel are more likely to have established protocols for handling emergency calls (53.2%). These protocols ensure standardized call handling, minimizing the risk of miscommunication or delays in critical situations. The presence of call recording devices is another feature more commonly seen in institutions with trained EMS staff (42.0%). These devices provide valuable documentation and allow for quality review, which can be essential for both performance assessment and legal purposes.
Reliable communication with teams in the field is another advantage seen in institutions with trained personnel, where the use of radio systems is more frequent (46.6%). This ensures real-time coordination and response adaptability in the field. Ambulances in institutions with trained staff are more likely to be equipped with radio stations (58.4%), which facilitates continuous communication and improves the speed of coordination during emergency responses. Moreover, institutions with trained employees are more likely to have backup power systems for their radio equipment (42.4%), ensuring uninterrupted communication even during power outages, which is vital for maintaining service continuity in emergencies. Dedicated communication channels with the police are another feature more commonly found in institutions with trained staff (56.7%). This enhances coordination during joint operations, ensuring effective collaboration between EMS teams and law enforcement during emergencies.
Monitoring reaction times to interventions is also more common in institutions with trained EMS employees (47.9%). This practice enables these organizations to evaluate and improve their response times, enhancing overall service delivery. Dedicated communication lines with firefighters are prevalent in institutions with trained EMS personnel (56.7%), facilitating better coordination during fire-related emergencies and ensuring that medical support is promptly provided. Institutions that prioritize training for their emergency medicine doctors tend to have better-prepared staff overall (42.4%), with the latest medical skills and knowledge needed to address a wide range of emergency situations effectively. The same is true for institutions that invest in the training of emergency medicine nurses (42.4%). This ensures nursing staff are well-equipped to handle high-pressure situations and deliver high-quality care during emergencies.
Additional financial resources allocated to healthcare are more common in institutions with trained EMS personnel (40.7%). This funding supports investment in training programs, leading to an expanded workforce and improved service delivery. Ambulance fleets in institutions with trained EMS staff are more likely to be well-maintained (42.4%), ensuring their readiness for immediate deployment in emergency scenarios and enhancing the overall responsiveness of the institution. Specialized vehicles for mass casualty events are also more common in institutions with trained EMS personnel (34.7%). This training enables staff to effectively manage large-scale emergencies, particularly in terms of the logistics of transporting multiple patients.
Institutions with trained staff are more likely to have written plans and procedures in place for mass casualty incidents (48.8%). These protocols ensure that all personnel are well-prepared for large-scale emergencies, enhancing their readiness and response capabilities. Triage tags, used to prioritize patients in mass casualty situations, are more readily available in institutions with trained EMS personnel (34.7%). This ensures that patients in the most critical condition receive attention first, improving the overall efficiency of care during such events. Regular drills and exercises for responding to mass casualty situations are more common in institutions with trained staff (41.8%). These exercises help teams refine their procedures and ensure they are ready to act quickly and effectively in real emergencies. Joint exercises with other first responders, such as police and firefighters, are also more frequently conducted in institutions with trained EMS personnel (41.8%). These collaborative exercises improve the coordination between different emergency services, enhancing the overall effectiveness of joint responses during major incidents.
Similarly, the Chi-square test results demonstrate statistically significant correlations between plans and procedures for mass casualty events and several critical variables. These include conducting EMS activities (p = 0.001), the organization of working hours (p = 0.000), and the presence of ambulance transport teams working during both day (p = 0.000) and night (p = 0.000) shifts. Additionally, significant correlations were observed between mass casualty event planning and the organization of on-call duty (p = 0.000), as well as the existence of protocols and procedures for receiving calls (p = 0.000). There is also a strong correlation with the presence of radio communication equipment in ambulances (p = 0.000) and the monitoring of response times during interventions (p = 0.005). Finally, plans for mass casualty events are significantly associated with the availability of vehicles for such incidents (p = 0.000), the presence of triage tags (p = 0.045), and the organization of joint exercises with other first responders (p = 0.000). No statistically significant correlations were identified for the remaining variables (Table 4).
Furhtermore, results show that institutions that have written plans and procedures for mass casualty events demonstrate greater success in conducting EMS activities. These institutions are more likely to provide services from multiple dislocated points (55.9% for 47 institutions with plans) compared to those without such plans (55.3% for 21 institutions). The structured approach afforded by these plans helps streamline operations across various locations, ensuring a broader reach and better preparedness for emergencies.
The organization of working hours also benefits from the existence of mass casualty plans. Institutions with these plans are more inclined to implement shift work (52.4% for 44 institutions) compared to those without plans (60.5% for 23 institutions). This structure facilitates continuous service provision, allowing institutions to maintain operational efficiency and ensure staff availability at all times, particularly during high-demand periods.
When it comes to ambulance transport teams, institutions with mass casualty plans excel in organizing both day and night shifts. These institutions effectively allocate resources during peak times (58.3% for day shifts and 51.2% for night shifts), compared to those without plans. Additionally, the existence of such plans enables better management of on-call duties (60.7% for 51 institutions with plans), especially when teams need to operate outside their designated territories, ensuring uninterrupted coverage.
Institutions with mass casualty plans are also more likely to have established protocols and procedures for receiving emergency calls (78.6% for 66 institutions). This formalized process enables them to manage critical situations more effectively than institutions without plans (39.5% for 15 institutions). Furthermore, these institutions are better equipped with radio communication systems in ambulances (79.8% for 67 institutions), which enhances coordination during interventions and ensures seamless communication between teams.
Monitoring response times is another area where institutions with mass casualty plans outperform. By tracking response times (63.1% for 53 institutions), they can evaluate their efficiency and make necessary adjustments to improve overall performance. Moreover, these institutions are more likely to have specialized vehicles for mass casualty incidents (10.7% for 9 institutions), making them better prepared to handle large-scale emergencies compared to institutions without plans (2.6% for 1 institution).
Lastly, the presence of mass casualty plans correlates with the availability of triage tags (40.5% for 34 institutions) and the organization of joint exercises with other first responder services (58.3% for 49 institutions). These factors contribute to enhanced coordination and preparedness during emergencies, ensuring that all agencies involved are well-equipped to respond effectively to mass casualty events.
3.3. Organizational Structure and Risk Management of Emergency Medical Services (EMS)
The study uncovers a variety of approaches to structuring Emergency Medical Services (EMS), each influencing the efficiency and effectiveness of emergency response capabilities in distinct ways. To be specific, the organizational structure of EMS within healthcare facilities shows notable diversity. A substantial portion, 46.04%, is integrated within dedicated EMS departments in health centers, a model that supports focused management of emergency care. Another 33.81% operates within general medical services, where regular medical staff, including doctors and health workers, manage emergency situations as part of their routine duties. In contrast, 15.11% of facilities have established EMS as separate organizational units within the broader medical framework, emphasizing the allocation of specific resources for emergency services. A smaller fraction, 3.60%, functions as specialized entities like Institutes for Emergency Medical Services, while only 1.44% lack an organized EMS system, indicating areas that may require service expansion (Table 5).
Most EMS activities occur within healthcare facilities (45.3%), utilizing existing infrastructure to facilitate emergency operations. Meanwhile, 26.7% of EMS activities are centralized in a single location, and 7.6% are distributed across multiple sites, aiming to enhance coverage and accessibility. The data also show that EMS activities are predominantly concentrated in one or two locations, accounting for 88.89% of operations, reflecting a centralized management approach. A smaller percentage of facilities operate across multiple locations, with 4.44% having 3 to 10 points and 1.11% reporting more than 11 points, showcasing varying degrees of decentralization to meet regional needs (Table 5).
Regarding working hours, 55.2% of facilities employ shift work to ensure continuous service delivery, while 44.8% use rotating shifts to balance workloads among staff. Among these, 80.2% of services operate on 12-hour shifts, the most common scheduling model, whereas 11.6% and 8.1% adhere to 8-hour shifts or alternative configurations, respectively, illustrating adaptability to operational demands and workforce preferences. In terms of specific shift patterns, 51.85% of facilities follow a schedule with a day shift, a subsequent 24-hour rest, and a night shift with 72 hours off, balancing work demands with adequate rest. Other patterns include a day shift followed by 48 hours off (24.44%) and a 48-hour rest period after each shift (23.70%) (Table 5).
During daytime shifts on weekdays, a single team configuration is prevalent in 50.6% of cases, facilitating streamlined operations. Conversely, 16.9% of facilities employ two teams, and 3.5% use three or more teams to address higher demand or specific challenges. Additionally, 27.9% of services utilize special configurations tailored to unique needs. For nighttime shifts on weekdays, 48.3% of facilities operate with one team, a common practice for maintaining service readiness. Meanwhile, 16.3% use two teams, 11.0% deploy three or more teams, and 23.2% implement special configurations to meet nighttime requirements. Only 1.2% report having no teams during night shifts, possibly due to low demand or reliance on on-call staff. Regarding healthcare management plans, 28.5% of facilities have teams dedicated solely to clinic operations, focusing on non-emergency services. In contrast, 49.4% do not differentiate between clinic and EMS teams, suggesting an integrated approach, while 22.1% report varied organizational structures that preclude direct comparison (Table 5).
Clinic team configurations for daytime shifts predominantly involve one team (64.0%), optimizing resource allocation for clinic operations. A smaller segment employs two teams (8.1%) or three or more teams (7.0%), reflecting complex operational demands. At nighttime, 72.1% of clinics maintain operations with one team, whereas 15.1% report no teams, possibly relying on emergency services for critical care during these hours. Finally, transport by a team composed of a medical nurse-technician and driver accounts for 19.2% of facilities, emphasizing a lean team setup designed for specific transport needs while balancing resource efficiency with the ability to address urgent situations (Table 5).
This next analysis delves into the operational capabilities and strategic readiness of emergency medical services (EMS), examining medical transport teams, geographical coverage, and how seasonal population changes affect service delivery. It highlights the configurations and logistical strategies that define the efficiency of medical transport services and their adaptability to fluctuating population needs.
Medical transport teams are typically organized with a single team, as reported by 43.0% of responses, allowing for streamlined patient transport operations. A smaller segment, 14.0%, deploys two teams, while configurations involving three (4.1%) and four teams (4.1%) indicate facilities with higher demand or specific operational requirements. A few facilities use five teams (1.2%) or more (1.7%), reflecting substantial transport capabilities. On the other side, the reliance on single-team configurations increases to 47.7% for overnight transport needs. In 19.8% of cases, no teams are reported, suggesting minimal demand or alternative staffing strategies, such as on-call services. Only 5.8% utilize two teams, indicating a targeted approach to nighttime operations (Table 6).
The composition of medical transport teams often includes a vehicle driver (33.1%) or a nurse-technician paired with a driver (29.7%), highlighting the lean operational structures in place. However, 37.8% of teams are more comprehensive, consisting of a doctor, nurse/technician, and driver, ensuring thorough patient care during transport. Other configurations, such as driver-only or driver with occasional medical staff (16.9%), and teams assembled based on specific needs (14.0%), reflect flexibility in adapting to different patient conditions. Teams vary depending on patient needs (20.9%), showcasing the adaptability necessary for appropriate care (Table 6).
Across facilities, 43.0% report established emergency readiness, while 57.0% lack specific plans, indicating a need for improved strategic planning. Similarly, 48.3% of facilities have organized preparedness for vehicle drivers, whereas 51.7% do not, highlighting an opportunity to enhance emergency transport efficiency. The average holding time for medical teams in higher-level centers varies, with most teams spending 61-120 minutes (18.0%) or 31-60 minutes (15.7%) at these locations, reflecting the time needed for patient handovers and administrative tasks. Transport teams usually spend 31-60 minutes (18.6%) at centers, indicating efficient turnover for prompt service resumption (Table 6).
Healthcare service coverage (HMP) ranges widely, with the most common area being 300-400 km² (20.3%). Many facilities cover areas between 100-200 km² (10.5%) and 400-500 km² (10.5%), demonstrating varying regional service demands. The typical territory diameter is 30-60 km (60.5%), indicating broad reach within the healthcare system. Also, the maximum distance from HMP headquarters to hospitals is primarily 25-50 km (31%), suggesting strategic facility placement for timely patient transport. For tertiary centers, the most common distances are 60-90 km (23.8%), reflecting the distribution of specialized services. Institutions covering parts of a highway report mixed responses: 50.0% indicate no coverage, 26.2% confirm coverage, and 23.8% find it non-applicable. Highway access is crucial for efficient logistics and rapid emergency site access (Table 6).
Population changes in HMP jurisdictions are noted by 48.8% of respondents, emphasizing the impact of seasonal influxes on healthcare demand. Increases typically involve fewer than 1,000 people (40.7%) or 1,000-5,000 people (37.2%), often due to tourism and migration (37.8%) or temporary residents (19.8%). Beyond urgent care, 65.1% of facilities report regular shift workloads that encompass various healthcare services, managed primarily by regular staff (75.0%) rather than on-call duty (25.0%). During night shifts for urgent care, transport teams mainly consist of a full medical team (73.8%), emphasizing comprehensive care during critical transport operations. This configuration reflects a commitment to delivering high-quality patient care in emergencies at all times (Table 6).
3.4. Resource Allocation and Efficacy in Emergency (Disaster) Preparedness
In emergency medical services (EMS) facilities, a significant number, precisely 25.58%, function with a moderate staffing model of 3 to 5 doctors. This configuration appears to be common for handling emergency care effectively. Following this, 18.02% of facilities have teams of 6 to 8 doctors, with another 18.02% maintaining 9 to 11 doctors. These figures suggest a preference for medium-sized teams capable of efficiently managing disasters. Notably, 11.63% of EMS facilities operate with a smaller team of just 0 to 2 doctors, which could indicate challenges in staffing for some institutions. On the other hand, 11.05% boast a slightly larger team of 12 to 15 doctors, and a smaller fraction, 8.72%, have over 15 doctors, likely reflecting those with a higher capacity for complex cases (Table 7).
When it comes to specialists, a large portion, 51.74%, of EMS facilities have only 0 to 2 specialists, highlighting the difficulty in hiring specialized personnel. A moderate number, 15.70%, report having 3 to 5 specialists, while fewer institutions fall into the categories of 6 to 8, 9 to 11, 12 to 15, and over 15 specialists, at 4.07%, 1.74%, 1.16%, and 2.33%, respectively. This distribution indicates that specialists, while present, are generally concentrated in a limited number of facilities (Table 7).
Among doctors undergoing emergency medicine training, most EMS institutions (67.44%) have 0 to 2 doctors in training, pointing to opportunities for growth in workforce development. A smaller segment, 4.65%, reports 3 to 5 doctors in training, with even fewer institutions having 6 to 8 doctors at 1.16% and 9 to 11 doctors at 0.58%. Looking at EMS doctors who are specialists in general medicine, 58.14% of institutions are staffed with 0 to 2 specialists, indicating a tendency toward employing generalists. Another 13.37% have 3 to 5 specialists, while a minor segment, 2.33%, employs 6 to 10 specialists. Only 0.58% have more than 10 specialists, underscoring the scarcity of high specialization within EMS (Table 7).
The distribution of general medicine doctors in EMS is such that 43.02% of institutions operate with 0 to 4 doctors, followed by 24.42% with 5 to 9 doctors. This suggests a balanced staffing approach, with fewer facilities (6.40%) maintaining 10 to 19 doctors and none exceeding 20, reflecting a structured limitation on general practitioners. In terms of additional medical specialties, 54.7% of institutions incorporate these to broaden the range of services offered. Conversely, 25.0% report that such integration is not applicable, possibly due to strategic decisions or institutional focus. An additional 20.3% lack other specialties entirely, which might indicate limitations in diversifying services (Table 7).
Among medical specialties, 49.4% of institutions are dedicated to specialized fields, including gynecology and pediatrics, showcasing the breadth of available expertise. General medicine makes up 17.4% of specialties, playing a crucial role in foundational healthcare. Diagnostics and laboratory services represent 23.3%, emphasizing their importance in medical facilities. Surgical specialties are found in 5.8% of institutions, with other less common specialties making up 4.1%, highlighting the varied medical landscape in these settings (Table 7). These findings underscore the diverse distribution of medical staff and specialties within EMS, with a strong focus on moderate-sized teams and generalists, while also identifying potential areas for specialist expansion and service diversification.
This analysis sheds light on staffing patterns within emergency medical services (EMS), revealing strengths and potential gaps in gender representation and specialization. In terms of male doctors, most institutions (41.3%) employ between 0 and 5 doctors, indicating a prevalent staffing level. Meanwhile, 15.7% of institutions have 6 to 10 male doctors, and 12.2% maintain 11 to 20, reflecting moderate staffing levels across many facilities. A smaller segment of institutions, 2.3%, employs 21 to 30 male doctors, with only 2.9% exceeding 30, suggesting that larger teams of male doctors are relatively uncommon (Table 8).
Regarding female doctors, 30.2% of institutions have 0 to 5 doctors, marking the most common staffing range for women in the field. Meanwhile, 19.2% employ 6 to 10 female doctors, and 17.4% have 11 to 20, showing a somewhat more balanced distribution compared to male doctors. Only 4.1% of institutions have 21 to 30 female doctors, while 3.5% have more than 30, highlighting a slightly more constrained presence of female doctors in larger numbers.
For male specialists in emergency medicine, 62.2% of institutions employ 0 to 2 specialists, emphasizing a significant reliance on a minimal number of male specialists. Only 9.3% have 3 to 5 male specialists, with even smaller proportions, 2.9%, 0.6%, and 0.6%, in the categories of 6 to 10, 11 to 15, and over 15 male specialists, respectively. Female specialists in emergency medicine predominantly fall within the 0 to 2 category as well, with 65.7% of institutions reporting this number. About 5.8% of institutions employ 3 to 5 female specialists, and even smaller percentages, 1.2%, 0.6%, and 0.6%, report having 6 to 10, 11 to 20, and more than 20 female specialists, respectively, suggesting limited presence at higher levels (Table 8).
In terms of male doctors specializing in emergency medicine, 56.4% of institutions report having no specialists, indicating a lack of specialization in many facilities. A smaller group, 14.0%, has 1 to 2 male specialists, and only 3.5% have 3 to 5, pointing to potential areas for growth. Female doctors specializing in emergency medicine show similar trends, with 54.1% of institutions lacking specialists. About 16.3% have 1 to 2 female specialists, while only 2.9% report having 3 or more, suggesting that specialization among female doctors is similarly limited (Table 8).
For male general medicine specialists, 44.8% of institutions report no specialists, and 24.4% have 1 to 2 specialists, indicating a trend toward low specialization in this area. Only 4.7% of institutions have 3 or more male specialists, suggesting room for increased specialization. Female general medicine specialists are slightly more prevalent, with 35.5% of institutions having no specialists and 23.8% employing 1 to 2. Approximately 9.9% of institutions employ 3 to 5 female specialists, while 4.1% have 6 or more, indicating a more significant presence compared to their male counterparts (Table 8).
For male general medicine doctors, 48.8% of institutions have 0 to 2 doctors, highlighting a primary staffing level. Meanwhile, 19.2% of institutions employ 3 to 5 male doctors, and only 5.2% have 6 to 10, with a minimal 0.6% exceeding 10, reflecting limited higher staffing levels. On the other side, for female general medicine doctors, 29.1% of institutions employ 0 to 2 doctors, showing a slightly lower presence than male doctors in this category. About 20.3% have 3 to 5 doctors, and 14.0% employ 6 to 10, with 9.9% reporting 11 or more female doctors, indicating a broader distribution among female general practitioners (Table 8).
Among male nursing staff with higher education, 60.5% of institutions employ 0 to 1 staff, indicating limited numbers of highly educated male nurses. Only 9.9% have 2 to 4 male nurses, and 2.9% employ 5 or more, suggesting potential areas for expansion. Female nursing staff with higher education show a similar trend, with 55.2% of institutions having 0 to 2 staff. About 9.3% employ 3 to 5, and another 9.3% have 6 or more, reflecting a slightly higher presence compared to their male counterparts (Table 8).
For male nursing technicians with secondary education, 44.2% of institutions employ 0 to 5 technicians, indicating a common staffing range. Meanwhile, 12.8% have 6 to 10, with smaller percentages of 7.6% and 9.3% employing 11 to 20 and 21 or more technicians, respectively. Female nursing technicians with secondary education are less prevalent, with 20.3% of institutions having 0 to 5 technicians. A higher proportion, 23.8%, have 6 to 10, while 20.3% employ 11 to 20, and smaller percentages employ more, indicating a more even distribution of female nursing technicians across different staffing levels (Table 8). Overall, these data suggest that while gender distribution in EMS is generally balanced, opportunities exist to enhance specialization, particularly among male and female specialists in emergency and general medicine. Additionally, increasing the presence of both male and female nursing staff could further support comprehensive healthcare delivery.
For doctors under the age of 30, a substantial majority of institutions, about 61.0%, report having just 0 to 1 doctor. This suggests a relatively low presence of younger doctors within the workforce. A smaller portion, 11.0%, employs between 2 and 5 doctors, while only 1.2% have 6 or more, indicating challenges in recruiting or retaining young doctors. In contrast, among doctors aged 30 to 55, there is a more balanced distribution. Here, 22.7% of institutions report having 0 to 5 doctors and another 22.7% have 6 to 10. The largest group, 27.9%, has 11 to 20 doctors, reflecting that mid-career professionals are the most prevalent in this age group. Smaller proportions, 8.1% and 4.1% have 21 to 30 and 31 or more doctors, respectively, indicating a decline in higher numbers. For doctors over the age of 55, 49.4% of institutions have 0 to 5 doctors, suggesting a transition toward retirement. Approximately 11.0% of institutions report having 6 to 10 doctors, while 13.4% have 11 or more, underscoring the continued presence of experienced doctors nearing the end of their careers (Table 9).
Among nursing technicians under 30 with secondary education, 51.7% of institutions employ 0 to 1 technician, highlighting limited entry-level opportunities. Meanwhile, 15.7% employ 2 to 4 technicians and only 5.8% have 5 or more, indicating a focus on retaining more experienced staff. Nursing technicians aged 30 to 55 show a diverse distribution. Around 16.9% of institutions have 0 to 5 technicians, while 19.2% have 6 to 10. Notably, 14.0% employ 11 to 15 technicians, and 17.4% have 21 or more, reflecting a strong presence of mid-career professionals. For those over the age of 55, 34.9% of institutions employ 0 to 2 technicians, suggesting a trend toward retirement. Meanwhile, 21.5% have 3 to 5 technicians, with smaller percentages, 10.5% and 6.4%, employing 6 to 10 and 11 or more, respectively, highlighting the retention of experienced staff (Table 9).
Among doctors, 61.6% report no verified limitations in work capacity, indicating a generally healthy workforce. However, 10.5% have minor limitations, and 1.7% have significant ones, suggesting areas for intervention to maintain productivity. Compliance with annual medical examinations is relatively high among doctors, with 47.1% meeting the requirements. However, 26.7% do not comply, revealing potential gaps in regulatory adherence. For medical nurses and technicians, 45.3% comply with annual examinations, while 28.5% do not, indicating similar compliance challenges as seen with doctors (Table 9).
Among ambulance drivers, compliance with annual medical examination requirements is strong, with 64.5% adhering to standards. Nonetheless, 9.3% do not comply, highlighting areas for improvement. Regarding work capability, 69.2% of ambulance drivers report no verified limitations, indicating a robust workforce. However, 4.1% have minor limitations, and 0.6% face significant limitations, underscoring the need for ongoing health assessments (Table 9).
The age distribution of ambulance drivers shows that 50.0% are under 30, indicating a youthful workforce. However, 17.4% are aged 30 to 55, while 63.4% are over 55, highlighting a significant proportion nearing retirement age (Table 9).
3.5. Communication Systems and Efficacy in Coordinated Response
The evaluation of communication infrastructure within emergency medical services reveals significant insights into system readiness and adherence to established protocols, which are vital for gauging the operational effectiveness of these services. Notably, a designated phone number for urgent responses is in place in 59 instances (34.3%), suggesting that just over one-third of the analyzed entities have a direct line for emergencies. Nevertheless, the reliance on various other numbers by 39.5% of the units could potentially complicate the efficiency of call handling during emergencies (Table 10).
The ability to identify incoming calls—a crucial factor in prioritizing emergency responses—is implemented in 45.3% of the units. This feature substantially boosts the responsiveness of services, facilitating the swift identification of repeat or critical calls. In contrast, the absence of this capability in 28.5% of the units might hinder timely responses, necessitating manual verification of calls.
Variability is also evident in the assignment of call reception responsibilities: doctors are directly engaged in this task in only 14.0% of cases, whereas nurses or technicians assume this role in another 14.0% of instances, occasionally requiring consultation with a doctor, as noted in 10.5% of the cases. The most common arrangement involves a mixed model where both nurses and doctors participate, observed in 35.5% of the responses. This arrangement likely offers a balanced approach, ensuring that skilled medical personnel are involved early in the triage process (Table 10).
Furthermore, protocols for managing calls, essential for the standardization and efficiency of operations, are in place in 54.1% of the units. This demonstrates a predominant compliance with structured communication protocols, which are critical for upholding high standards of service. However, the lack of established protocols in 19.8% of the units may result in inconsistent management of incoming calls. The data underscores both the strengths and potential areas for enhancement in the communication frameworks of emergency medical services. By promoting more standardized call-handling practices and advancing the technological infrastructure for call identification, there could be substantial improvements in service delivery, especially in scenarios characterized by high urgency and stress (Table 10).
When examining the capabilities and technological backbone of emergency medical services, several key factors stand out, particularly in the areas of communication tools, response protocols, and direct lines of communication. This analysis delves deeply into the hardware and operational dynamics crucial for swift and efficient disaster management. Regarding that, about 35.5% of services report having operational dictation machines, which play a vital role in documenting interactions accurately and maintaining accountability. However, 9.3% have machines that aren’t working, potentially hampering effective record-keeping and follow-up on emergency calls. Furthermore, 29.1% of the services lack a dictation machine entirely, which could affect the quality of data retention and retrieval (Table 11).
In 41.3% of cases, phone conversations with patients are recorded, aiding in thorough documentation and review of emergency calls, essential for training and quality control. However, 32.6% of services do not adopt this practice, and for 26.2%, it is not applicable, possibly due to privacy concerns or technical limitations. Moreover, only 8.7% record radio communications, with a significant 65.1% not doing so, which might impact the review and enhancement of dispatch and on-field communication protocols (Table 11).
A mere 12.2% have a direct telephone line to the police, and only 11.6% connect with the Alert and Notification Center, indicating limited direct liaisons with these crucial emergency services. This limitation could delay response times during incidents that require police or centralized alert services. A majority (62.2%) of communications with field teams happen via mobile phones, highlighting reliance on cellular networks for coordination. The combined use of mobile phones and radios is seen in only 8.1% of cases, while exclusive use of radios is minimal at 3.5%, showing a shift towards more accessible and potentially more reliable mobile technology (Table 11).
While 15.7% of ambulances have a radio station, a significant 58.1% do not, which may impede communication during critical transfers or remote interventions. Radio repeaters, vital for extending the range of radio communications, are operational in just 16.9% of cases, with a worrying 57.0% reported as non-operational, highlighting a critical need for improvement to ensure robust communication during emergencies. Only 17.4% of services have devices to power their radio systems during outages, revealing a vulnerability in maintaining communication continuity during infrastructure failures. Direct channels to communicate with police and firefighter-rescuers are exceptionally rare, at just 1.7% each, pointing to a significant gap in establishing dedicated and efficient communication lines with these critical emergency response entities (Table 11).
Tracking reaction times during first-order emergency interventions occurs in 39.5% of cases, a crucial metric for assessing the responsiveness and efficiency of emergency services. However, nearly one-third (34.3%) do not monitor these times, potentially missing out on valuable data that could drive improvements in service delivery. These insights collectively underscore both the strengths and significant areas for improvement in enhancing the effectiveness, speed, and reliability of emergency medical services. Advancing technological infrastructure, ensuring the functionality of communication tools, and setting up solid protocols for direct communication with other emergency services are vital steps towards optimizing emergency response outcomes.
3.6. Emergency Response Times and Efficacy in Urgent Interventions
An analysis of response times in different emergency medical service scenarios sheds light on how effectively and swiftly interventions are carried out. By categorizing these times into distinct ranges, we can better understand how well services are delivered across various operational contexts. The data indicate that a significant 20.3% of activation times fall within the 0 to 1-hour range, demonstrating a quick response in a fifth of the cases. As the activation time lengthens, however, the percentage of cases decreases, with only 6.4% taking between 1 and 3 hours and an even smaller 4.1% extending from 3 to 10 hours. Alarmingly, 8.7% of activation times exceed 10 hours, raising questions about delays in certain emergency responses and pointing to either complex cases or underlying inefficiencies that merit closer scrutiny (Table 12).
On the other side, reaction times offer another critical measure of responsiveness. In 8.7% of cases, services manage to react within an hour, indicating that immediate action is possible, though not consistently achieved across all services. The largest proportion, 23.3%, falls within the 1 to 10-hour range, revealing a wide variation in response timeliness. Reaction times that extend beyond 10 hours—5.8% of cases up to 20 hours and 1.7% surpassing 20 hours—highlight possible operational or logistical challenges (Table 12).
This metric (prehospital intervention time) breaks down the responsiveness from the onset of an emergency to the point of medical intervention. About 15.7% of prehospital interventions occur within 0 to 10 hours, reflecting quicker activation periods. The percentage rises to 16.3% for interventions taking 10 to 30 hours, suggesting that many interventions fall within this range. Longer intervention times—between 30 to 60 hours and those exceeding 60 hours—are less common, at 5.2% and 2.3%, respectively, indicating areas where intervention delays are significant. These various timeframes—across activation, reaction, and prehospital intervention—provide a detailed view of the operational dynamics in emergency medical services. The data reveal both the potential for rapid action and areas where delays impact overall emergency response effectiveness. Understanding these dynamics is essential for pinpointing where improvements are needed, enhancing training and resources, and ultimately improving patient outcomes in critical situations such as disasters (Table 12).
A notable number of institutions have developed written plans or procedures for disaster response, with nearly half (48.8%) confirming their existence. This statistic indicates a moderate level of preparedness, as almost 50% of the surveyed institutions have established and shared their disaster response strategies with their teams. On the flip side, only 5.8% reported having vehicles equipped specifically for mass casualty incidents, pointing to a considerable gap in physical readiness for large-scale emergencies. Similarly, only 9.3% of institutions had triage cards, which are essential for the efficient allocation of resources during such incidents. This limited availability suggests there could be delays and inefficiencies during the initial response phases.
In terms of mass casualty response drills, just 14% of institutions conducted these exercises in the past two years, with most of them doing so once a year or even less frequently. This lack of regular training could impact the readiness and ability of institutions to effectively manage disaster situations. Furthermore, only 15.7% of institutions participated in joint drills with other emergency services, such as the police, military, and fire departments, over the past two years. This could hamper coordinated response efforts in real disaster scenarios.
Looking at response times as another key measure of preparedness, only 8.7% of services managed to respond within an hour, showing that while immediate action is sometimes possible, it is not consistently achieved across all services. The largest group, 23.3%, responded within 1 to 10 hours, illustrating a wide variation in timeliness. Some response times exceeded 10 hours, with 5.8% taking up to 20 hours and 1.7% taking even longer, highlighting potential operational or logistical challenges.
3.6. Training and Preparedness for Disaster (Emergency) Response
Regarding training compliance and needs within an EMS system, results show that 32.0% of newly hired doctors and 30.8% of nursing technicians have undergone specialized emergency medicine training soon after being hired, reflecting strong initial training programs for these essential staff members. However, there are notable gaps, as 41.9% of doctors and 43.0% of nursing technicians reported not receiving this training, highlighting a need to improve training coverage (Table 9). A closer look reveals that 42.4% of EMS personnel have received training at established centers, yet 31.4% have not, and 26.2% are marked as not applicable, indicating potential disparities in training access or inconsistent requirements across the organization. Alarmingly, while a significant 68.0% of respondents recognize the need for more training for all EMS staff, 5.8% do not see this necessity, pointing to a perception gap that could affect service delivery (Table 9).
When asked to prioritize training needs, 57.0% of respondents believe doctors require the most training, compared to only 5.2% for nursing technicians and ambulance drivers. This suggests a focused need for advanced training for physicians who often handle the most complex medical emergencies (Table 9). Specific training needs identified include CPR and trauma management, prioritized by 26.2% of responses, underscoring the importance of these skills in emergency settings. Other areas such as urgent medical conditions, emergency protocols and equipment use, safety and operational training, and specialized medical fields like obstetrics and cardiology also receive significant attention. This indicates a broad spectrum of training needs that align with the diverse challenges faced in emergency medical services (Table 13).
A significant majority, 57%, emphasized the importance of establishing clear norms for operations, including aspects like equipment, staffing, space, vehicles, and education. This highlights a strong belief in the necessity for standardized and well-defined operational guidelines. Similarly, 47.1% of participants stress the importance of strict adherence to established standards and procedures, underscoring the critical role of regulatory compliance and structured protocols in disaster management (Table 13).
Moreover, continuous education is considered crucial, with 56.4% of respondents acknowledging its importance in keeping EMS personnel updated with the latest medical practices and emergency response techniques. However, opinions differ on the value of physical expansions like new training centers; only 34.3% see this as beneficial, while a larger portion, 39.5%, disagrees, suggesting concerns about the effectiveness or resource allocation for such initiatives. Support for equipment renewal is notably strong, with 61.6% of respondents affirming that modern and efficient equipment is vital for enhancing EMS functionality and service quality.
Similarly, 59.3% of respondents favor adding more staff, pointing to a recognized need for additional personnel to meet increasing service demands and ensure prompt emergency responses (Table 13). These perspectives collectively highlight a consensus on the need to improve operational standards, continuous professional development, and resource upgrades to advance the quality and efficiency of emergency medical services. However, the perceived value of expanding training facilities remains a point of contention.
3.8. Financial Resources and Administrative Efficacy in Emergency Medical Services
A significant 69.2% of Emergency Medical Services (EMS) are primarily funded by the National Health Insurance Fund (RFZO), showing a heavy reliance on national health insurance to keep their operations running smoothly. In stark contrast, just 4.1% of EMS do not receive any funding from RFZO, underscoring the fund’s crucial role in supporting EMS activities. On the other hand, municipal or city budgets are a source of funding for 39% of EMS, while 34.3% receive no financial support from their local governments, illustrating differing levels of local government involvement in various areas (Table 14).
When it comes to generating their own revenue or receiving donations, these sources play a smaller role. Only 24.4% and 20.3% of EMS rely on self-generated revenue and donations, respectively. Notably, 48.8% do not depend on their own revenue, and 52.9% do not rely on donations, pointing to potential financial vulnerabilities and challenges in maintaining stable operations. Additionally, 40.7% of healthcare institutions benefit from extra funding from local governments for staffing, which is vital for enhancing their ability to respond effectively to emergencies (Table 14).
In terms of staffing, about half of the EMS units operate with a modest number of 0-5 doctors, indicating that many services manage with minimal medical personnel. This pattern is similar for medical nursing technicians and ambulance drivers, suggesting that numerous EMS units work with limited staff. The data on service length and working conditions reveals that a significant number of doctors and medical technicians/nurses have considerable experience, suggesting good retention rates. However, almost as many lack this longevity, which could indicate staff turnover or the presence of newer team members. Compensation for working unsociable hours is well recognized, with around 69.8% of medical staff receiving payment for night shifts and work on Sundays. This highlights the demanding nature of EMS work schedules and the importance of compensating staff for their night and weekend shifts (Table 14).
The assessment of the ambulance vehicle fleet shows a diverse range of ages. Notably, 18.6% of the vehicles were manufactured between 2011 and 2015, suggesting that part of the fleet is relatively modern. However, older vehicles from 1989 to 2000 and 2001 to 2005 make up smaller portions, 6.4% and 11.0% respectively. This highlights a potential need to update older vehicles to maintain reliability and efficiency in emergency responses (Table 15).
When looking at how much these vehicles have been used, we see that 22.1% have traveled between 400,000 to 1,000,000 kilometers, indicating heavy use. This high mileage suggests that maintaining these vehicles could be costly, and their reliability might be compromised. Other mileage ranges also reflect significant usage, underscoring the demanding nature of these vehicles’ operational duties. Regarding the availability of critical medical equipment, the functionality rate is quite high for essential items like EKG machines and biphasic defibrillators, at 70.9% and 64.0%, respectively. This suggests that most EMS services are well-prepared to handle cardiac emergencies. However, there’s a noticeable gap in more advanced equipment like portable mechanical respirators with CPAP mode, which are functional in only 11.0% of services. This indicates a need for improvement in respiratory support capabilities. Basic emergency equipment, such as cardiopulmonary resuscitation sets and 10-liter oxygen bottles, is generally well-stocked, with functionality rates of 61.6% and 68.6%, respectively. This suggests strong readiness for basic life-saving interventions. However, more specialized equipment, like vacuum mattresses and cervical collars for spinal immobilization, show varied availability at 33.1% and 62.8%, respectively, indicating differences in preparedness for specific emergencies (Table 11).
Communication equipment is another critical area for EMS operations. Fixed radio stations are available in 25% of ambulances, while handheld radios are present in only 9.3% of cases. This highlights a significant opportunity to enhance communication capabilities during emergencies. There are also significant shortages in essential medical supplies, such as thrombolytic medications and emergency cricothyrotomy kits, which are available in only 4.7% and 8.7% of cases, respectively. Similarly, the availability of infusion solution heaters and protective helmets with lamps is extremely limited, at just 0.6% each. These shortages emphasize the challenges EMS face in being fully equipped. Overall, these findings point to critical needs and gaps within emergency medical services. There’s an urgent requirement for investment in equipment and vehicle updates to boost the effectiveness and responsiveness of EMS operations (Table 11).
4. Discussion
The study sheds light on the diverse organizational structures of Emergency Medical Services (EMS) in Serbian healthcare institutions. Approximately 46% of health centers have EMS integrated into specialized departments, which helps focus efforts on managing emergencies through targeted training and resource allocation. This setup can potentially lead to better patient outcomes by making emergency care more efficient and organized [54,118]. However, implementing this model requires significant resource investment, which may not be practical for every facility [119].
For about 34% of centers, EMS operates within general medical services, allowing existing medical staff to handle emergencies alongside their regular duties. This flexible approach can maximize resource use but also poses challenges in juggling routine care with emergency demands, possibly affecting the quality of emergency responses [120]. Staff in these settings may need additional training to be adequately prepared for emergencies [121,122]. A small portion, 15% of facilities, have set up EMS as separate units, specifically dedicating resources to emergencies. This can enhance the efficiency and effectiveness of emergency responses by ensuring specialized training and equipment are available [123]. However, the limited adoption of this model suggests there are barriers, such as financial or administrative hurdles, to its wider use [70,124].
Specialized entities like Institutes for Emergency Medical Services, present in just 3.6% of cases, highlight the potential benefits of concentrated expertise and resources. These institutions can act as centers of excellence, offering advanced emergency care and serving as models for best practices [125]. Meanwhile, the lack of an organized EMS system in 1.44% of facilities points to a critical gap in emergency healthcare coverage, indicating a need for policy interventions and investments to extend EMS services [54].
EMS activities are mainly centralized, with nearly 89% of operations taking place in one or two locations. While this centralization can enhance efficiency by leveraging economies of scale, it might restrict access for remote areas, particularly in rural or underserved regions [96,126]. Some facilities are trying to improve coverage with limited decentralization (4.44% having 3 to 10 points and 1.11% with more than 11 points), but further expansion is needed to ensure equitable access to emergency services across the country [80]. Centralization may also create bottlenecks during high-demand periods, stressing the importance of strategic planning and resource allocation to increase capacity and responsiveness [127].
Shift work predominates in EMS staffing, with 55.2% of operations using this approach over rotating shifts (44.8%) to ensure continuous service delivery, which is crucial for emergency healthcare. The widespread use of 12-hour shifts (80.2%) aims to balance operational efficiency with staff well-being, though these shifts can lead to fatigue and decreased performance over time. Alternative shift models, including 8-hour shifts and flexible schedules, could help reduce burnout and enhance staff satisfaction [128,129].
Single-team configurations are common during both daytime (50.6%) and nighttime (48.3%) shifts, streamlining operations but potentially creating challenges during peak times or complex emergencies [130]. Facilities employing multiple teams (16.9% during the day and 16.3% at night) or special configurations (27.9% during the day and 23.2% at night) show adaptability to varying demands, suggesting tailored staffing models could improve EMS effectiveness [61].
The composition and deployment of medical transport teams show notable variation, with 43.0% of facilities relying on single teams for daytime transport operations. While this lean setup emphasizes resource efficienc [131], it may limit the ability to handle multiple emergencies or complex cases simultaneously [51]. Comprehensive team configurations (37.8%), including doctors, nurses/technicians, and drivers, ensure thorough patient care but require significant resources.
Healthcare facilities typically cover areas of 300-400 km², reflecting a broad reach, though the lack of highway coverage in 50.0% of institutions highlights logistical challenges that could delay rapid responses [132]. Strategic placement of facilities and enhancements in infrastructure [79], such as road networks and communication systems, are vital to improving EMS accessibility and efficiency [133]. Also, the study identifies major gaps in strategic readiness, with 57.0% of facilities lacking specific emergency preparedness plans. This gap underscores the need for better planning and coordination to improve EMS effectiveness [75,134,135,136,137,138]. The absence of preparedness plans could lead to inconsistent response strategies and suboptimal patient outcomes, especially in large-scale emergencies and disasters [72,103,106,107,114,115,139,140,141].
Seasonal population changes, reported by 48.8% of respondents, further emphasize the need for flexible and adaptive EMS strategies. Facilities must be prepared to adjust resources and staffing in response to fluctuations caused by tourism, migration, or temporary residents [64,142].
Furthermore, the study highlights notable differences in staffing models among Emergency Medical Services (EMS) facilities in Serbia, which points to both strengths and challenges in meeting the demands of emergency care. In 25.58% of these facilities, there is a moderate staffing model with 3 to 5 doctors, reflecting a balanced strategy that can efficiently handle emergencies without stretching resources too thin. This setup provides a good mix of cost efficiency and operational capacity, ensuring there is enough medical expertise for handling routine emergencies [49,143]. However, there are challenges in some facilities where 11.63% operate with just 0 to 2 doctors. Such limited staffing can pose significant challenges in delivering timely and comprehensive care, especially during high-demand situations or complex emergencies and disasters [50]. On the other hand, facilities with larger teams of 12 to 15 doctors (11.05%) or more than 15 doctors (8.72%) suggest an ability to manage more complex cases, likely indicating strategic investments in areas with greater emergency needs or larger populations [53].
The availability of specialists in EMS facilities is generally limited, with 51.74% of facilities employing only 0 to 2 specialists. This lack highlights the challenges in recruiting and retaining specialized personnel, which can affect the quality of care in complex or specialized emergency situations [66]. Facilities with 3 to 5 specialists (15.70%) can offer more comprehensive care, but the scarcity of larger numbers of specialists suggests systemic barriers, like funding constraints or limited training opportunities, to developing specialization [82]. Also, training for doctors in emergency medicine is also sparse, with 67.44% of institutions reporting only 0 to 2 doctors in training. This situation indicates a significant opportunity for growth in workforce development [144], highlighting the need for targeted training programs to enhance specialization and improve emergency care capabilities [68,71,113,145,146,147]. The trend toward employing generalists (58.14% with 0 to 2 specialists in general medicine) shows a pragmatic approach to staffing but underscores the need for greater specialization to effectively manage diverse medical emergencies.
The gender distribution among doctors and specialists in EMS facilities shows a reasonably balanced representation of female doctors, with 30.2% of institutions having 0 to 5 female doctors, compared to 41.3% with 0 to 5 male doctors. This suggests a relatively equitable gender distribution in smaller teams, though larger teams of female doctors are less common [148]. While opportunities exist for women in EMS, there is room for improvement in achieving gender parity, especially in higher-level or specialized roles [56,116,117].
The age distribution among doctors shows a low presence of younger doctors under 30, with 61.0% of institutions employing just 0 to 1 doctor in this age group. This indicates challenges in attracting and retaining young medical professionals, which could have long-term implications for workforce sustainability [60]. Meanwhile, the prevalence of doctors aged 30 to 55 points to a more stable mid-career workforce, but the significant proportion of doctors over 55 suggests potential retirements on the horizon, necessitating proactive recruitment and succession planning [149].
The evaluation of communication infrastructure in Emergency Medical Services (EMS) facilities in Serbia provides critical insights into their preparedness and protocol adherence, which are vital for effective disaster management [150]. In 34.3% of the facilities, having a designated phone number for urgent responses indicates a structured method of handling emergencies. This setup facilitates faster response times and boosts overall system efficiency [151]. However, the use of multiple other numbers by 39.5% of units suggests potential inefficiencies in call management, which could lead to delays during critical emergencies. Streamlining communication channels with a standardized direct line for emergencies across all facilities could improve efficiency and reduce confusion during high-stress scenarios [57]. The capability to identify incoming calls, implemented in 45.3% of units, is a crucial feature that enhances responsiveness by allowing quick identification of critical or repeat calls [152]. This ability is essential for prioritizing emergencies and ensuring timely intervention. The absence of this feature in 28.5% of units highlights a gap that could hinder prompt responses, pointing to the need for technological upgrades to support real-time call identification and prioritization [153].
The study shows variability in the assignment of call reception responsibilities, with a mixed model involving both nurses and doctors being the most common arrangement (35.5%). This approach likely provides a balanced method, ensuring skilled medical personnel are involved early in the triage process [55]. The involvement of nurses or technicians in 14.0% of cases and doctors in another 14.0% suggests a flexible approach that can be tailored to the specific needs and resources of each facility. However, the requirement for consultation with doctors in some cases (10.5%) indicates potential delays in decision-making [154]. Empowering nurses and technicians through enhanced training could streamline operations and improve response times [155].
The existence of protocols for managing calls in 54.1% of units reflects adherence to structured communication frameworks, which are essential for maintaining high service standards [5,61,80,153]. However, the absence of established protocols in 19.8% of units may lead to inconsistent call management and potential delays in emergency responses. Promoting standardized call handling practices and implementing comprehensive protocols across all facilities are critical steps toward improving operational consistency and service quality [156]. The technological infrastructure of EMS facilities, including communication tools and response protocols, is crucial for effective disaster management [38,39,40,138,146]. The operational status of dictation machines in 35.5% of services is important for accurate documentation and accountability. However, the lack of functional machines in 9.3% and their absence in 29.1% of services indicate significant gaps in data retention and retrieval capabilities. Addressing these deficiencies through investments in functional communication tools and technologies is vital to support efficient record-keeping and follow-up on emergency calls [89]. Regarding communication with other emergency services, the study highlights limited direct communication channels with other emergency services, such as the police and the Alert and Notification Center, with only 12.2% and 11.6% of facilities having such connections, respectively. This limitation could delay responses during incidents requiring coordination with police or centralized alert services [104,157,158,159]. This for sure underscoring the need for integrated communication systems that facilitate seamless interaction among different emergency responders [160]. The reliance on mobile phones for field communication in 62.2% of cases reflects a shift towards more accessible and reliable technology [161,162,163,164]. However, the minimal use of radios (3.5%) and the lack of combined mobile and radio communication (8.1%) suggest that facilities could benefit from leveraging multiple communication platforms to ensure redundancy and reliability during emergencies. The lack of operational radio stations in ambulances (58.1%) and non-functional radio repeaters (57.0%) further emphasizes the need for technological upgrades to maintain robust communication during critical situations [165,166].
Analyzing response times in various emergency medical service scenarios provides valuable insights into how well these services operate and respond during emergencies and disasters [63]. Activation time, which is the interval from receiving an emergency call to the start of a response, is a critical measure of system readiness [167]. The data show that 20.3% of activation times are within the 0 to 1-hour range, indicating a strong ability to quickly respond in a significant number of cases. This performance suggests that when conditions are favorable, services are well-prepared for rapid deployment [168]. Nonetheless, there are instances of longer activation times, with 6.4% of cases taking between 1 and 3 hours and 8.7% exceeding 10 hours. These delays highlight areas that need improvement, possibly due to logistical hurdles, resource constraints, or complex disasters [84]. Addressing these inefficiencies is vital for reducing delays and enhancing the overall responsiveness of emergency medical services [169].
Reaction time, which tracks the period from activation to when emergency personnel arrive at the scene, is another key indicator of responsiveness [20,159]. Although 8.7% of cases achieve a reaction time within an hour, this suggests that immediate response is not always the norm. The largest share of cases, 23.3%, falls within the 1 to 10-hour range, indicating variability in how effectively different services and scenarios are handled [133]. Extended reaction times, with 5.8% of cases taking up to 20 hours and 1.7% surpassing 20 hours, point to notable operational or logistical hurdles. These delays may be due to traffic congestion [170], geographic challenges, or inadequate staffing during peak times [95]. Tackling these issues requires a comprehensive approach, including infrastructure upgrades, better resource management, and improved communication systems to optimize response times.
Prehospital intervention time, which covers the span from the onset of an emergency to the point of medical intervention, provides a full picture of EMS efficiency [171]. The data show that 15.7% of interventions occur within 0 to 10 hours, reflecting quick activation and response. However, a notable 16.3% of interventions occur within the 10 to 30-hour range, indicating room for improvement. Longer intervention times, with 5.2% of cases taking 30 to 60 hours and 2.3% exceeding 60 hours, underscore the need for strategic enhancements in EMS operations [80]. These delays might stem from complex emergencies, limited resources [172], or coordination issues, stressing the importance of continuously evaluating and optimizing EMS processes to shorten intervention times and improve patient outcomes [65].
Preparedness for mass casualty incidents such as disasters is a vital aspect of EMS readiness [105,173,174]. About 48.8% of institutions have written plans or procedures for disaster response, indicating a moderate level of preparedness. However, the limited availability of vehicles equipped for mass casualty incidents (5.8%) and triage cards (9.3%) reveals significant gaps in physical readiness. These deficiencies could lead to delays and inefficiencies in the initial phases of a large-scale emergency, highlighting the need for better planning and resource allocation. The infrequency of mass casualty response drills, with only 14% of institutions conducting such exercises in the past two years, points to a lack of regular training that could affect readiness and response effectiveness [69]. Additionally, limited participation in joint drills with other emergency services (15.7%) indicates potential barriers to coordinated response efforts. This underscores the need for increased collaboration and training to ensure a unified and effective approach during actual disaster scenarios [175].
The data reveals that a significant number of new Emergency Medical Services (EMS) employees receive initial training. Specifically, 32% of newly hired doctors and 30.8% of nursing technicians are provided with specialized emergency medicine training soon after they join. This reflects a strong commitment to ensuring essential staff are equipped with the necessary skills from the start [176]. However, there are notable gaps, with 41.9% of doctors and 43% of nursing technicians not receiving this training. This underscores the need to broaden training programs to ensure comprehensive coverage for all new hires [176]. Consistent training for all new EMS personnel is vital for maintaining high standards of emergency care [177]. About 42.4% of EMS personnel receive training at established centers, but 31.4% report lacking access, and for 26.2%, it is deemed not applicable. This suggests disparities in training access or inconsistencies in training requirements throughout the EMS system [91]. Notably, while 68% of staff acknowledge the need for more training, 5.8% do not perceive this necessity. This gap in perception could impact service delivery quality if not addressed, as it indicates differing levels of awareness about the importance of ongoing training [69,70].
When considering training priorities, 57% of respondents believe that doctors need the most training compared to just 5.2% for nursing technicians and ambulance drivers. This highlights a demand for advanced training for physicians, who frequently manage complex emergencies and disasters [178]. Key areas of training identified include CPR and trauma management (26.2%), emphasizing the importance of these skills in disasters [38,68,177]. Other essential areas include training in urgent medical conditions, emergency protocols, equipment use, and specialized fields like obstetrics and cardiology, reflecting the wide range of challenges faced in EMS [38,68,177]. A significant majority (57%) highlight the importance of establishing clear operational standards, covering aspects like equipment, staffing, space, vehicles, and education. This reflects a strong belief in the value of standardized and well-defined guidelines to enhance EMS operations [179]. Similarly, 47.1% stress the importance of adhering strictly to established standards and procedures, emphasizing the crucial role of regulatory compliance and structured protocols in disaster management. Continuous education is seen as vital by 56.4% of respondents, underscoring its role in keeping EMS personnel updated with the latest practices and techniques [180].
Opinions are divided regarding the expansion of physical training facilities, with only 34.3% seeing it as beneficial, while 39.5% disagree. This suggests concerns about the effectiveness or resource allocation of such initiatives [67]. However, there is strong support for equipment renewal, with 61.6% affirming that modern and efficient equipment is essential for improving EMS functionality and service quality. Additionally, 59.3% of respondents support adding more staff, highlighting a recognized need for additional personnel to meet growing service demands and ensure prompt disasaster responses [35,72,122,141,146,166].
The Emergency Medical Services (EMS) system predominantly depends on the National Health Insurance Fund (RFZO), which funds 69.2% of its services, highlighting its critical role. In contrast, only 39% of EMS services receive support from municipal or city budgets, and 34.3% do not receive any funding from local governments, indicating a significant variation in regional financial backing. This underscores the need for greater municipal involvement to ensure consistent quality across services [181].
Self-generated revenue and donations are relatively minor funding sources, with only 24.4% and 20.3% of EMS units relying on them, respectively. This limited diversification of funding highlights potential financial vulnerabilities [182] and underscores the necessity for varied funding strategies to maintain stable operations [183]. A significant number of EMS units operate with minimal staffing, with about half employing only 0-5 doctors, a trend that is also reflected in the number of nursing technicians and ambulance drivers. This staffing level could impact the quality of emergency response and underscores the need for additional personnel to meet the growing demand for services [184]. The workforce comprises a mix of experienced and newer staff, indicating both retention and potential turnover. Compensation for night shifts and weekends is provided, with 69.8% of medical staff receiving additional pay, highlighting the demanding nature of EMS work and the importance of fair compensation.
The ambulance fleet includes a modest proportion of modern vehicles (18.6% from 2011-2015), while many vehicles are outdated, suggesting a pressing need for upgrades to ensure reliability [88]. High mileage in 22.1% of vehicles indicates heavy usage, which could compromise efficiency and dependability. Most EMS units are equipped with essential tools such as EKG machines (70.9%) and defibrillators (64.0%), but there is a notable gap in advanced equipment like portable respirators (11.0%). The limited availability of communication tools, such as fixed radio stations (25%) and handheld radios (9.3%), highlights a need to improve communication capabilities [59]. There are significant shortages in crucial supplies, such as thrombolytic medications (4.7%) and cricothyrotomy kits (8.7%), pointing to preparedness gaps. This indicates a need for enhanced inventory management to ensure comprehensive emergency support [52].
The study faced several limitations, which are outlined below: a) the participant sample was drawn exclusively from healthcare institutions within Serbia, limiting the ability to generalize the findings to other countries or healthcare systems; b) since the research depends on participants’ self-assessments, there is a possibility of subjectivity in their responses, which could introduce bias into the results; c) the absence of longitudinal data makes it challenging to monitor changes in the efficiency of the emergency medical response system over time, thus potentially obscuring long-term trends; d) resource and equipment shortages in certain institutions may have influenced the depth of the data collected, especially in facilities with smaller capacities; e) differences in emergency preparedness levels across healthcare institutions could make it more difficult to compare results from different regions or organizations; f) the lack of standardized national protocols might have affected the uniformity and reliability of the collected data, posing difficulties for accurate analysis of the system’s overall efficiency.
5. Recommendations
The recommendations in Table 16 are designed to tackle critical areas within Emergency Medical Services (EMS) that need strategic improvements. By concentrating on elements like organizational structure, resource allocation, communication systems, response times, training, and financial resources, these strategies lay out a detailed plan for boosting the effectiveness and preparedness of EMS operations.
Each recommendation is evaluated based on factors like duration, feasibility, cost, and priority to ensure that the actions taken are well-suited to the varied needs and challenges faced by EMS units. Through these focused efforts, the aim is to strengthen EMS capabilities, make better use of resources, and ensure a strong response to emergencies.
6. Conclusions
The analysis of Emergency Medical Response Systems (EMRS) in Serbian healthcare paints a picture of a system with both strengths and areas needing attention. This study pulls together key findings, giving us a full view of how things currently stand and offering ways to make improvements. When we look at how EMRS is organized in Serbia, there’s a lot of variation. This diversity comes from the country’s unique historical and economic shifts. Many emergency services operate within specialized departments in health centers, which helps focus on managing emergency care effectively. However, some are set up as independent units or are part of general medical services, showing that there’s a mix in how services are delivered. This variety highlights the need for standardized procedures and centralized management to boost coordination and efficiency.
Even though there have been efforts to match European standards, challenges like outdated infrastructure, not enough staff, and logistical hurdles still slow down quick responses. This study emphasizes the need to establish clear operational guidelines, improve communication systems, and adopt evidence-based procedures to tackle these issues. By fostering cooperation between different agencies and regions, Serbia can better manage risks and address unequal access to emergency care. The study also finds significant gaps in resource distribution, with many emergency facilities struggling with minimal staff and outdated equipment. Reliance on the National Health Insurance Fund (RFZO) as the main funding source highlights financial constraints. Meanwhile, municipal budgets and self-generated revenue contribute less, pointing to a need for more varied funding approaches.
To improve service delivery, conducting targeted resource audits and setting up funds for state-of-the-art EMS equipment are crucial. Deploying mobile resource units and forming strategic partnerships with technology providers can enhance resource distribution and ensure underserved areas get the support they need. Sharing resources among EMS agencies can further optimize usage and improve efficiency. Effective communication is key to a coordinated emergency response, yet the study finds significant gaps in this area. The absence of standardized communication protocols and limited direct links to crucial emergency services, like the police and alert centers, hinder efficient responses. While mobile phones are increasingly used for field communication, the lack of backup channels poses risks during outages.
Upgrading to digital radio systems, setting up regional communication centers, and investing in AI-driven communication tools are recommended to improve coordination and responsiveness. Training programs on communication technologies can also help equip EMS personnel with the skills needed to handle complex emergency scenarios. Analyzing response times reveals variability, with some services exceeding international benchmarks. While some services can respond within an hour, delays in activation and reaction times point to inefficiencies. Improving these times requires streamlined processes and infrastructure upgrades.
Strategies for rapid deployment, infrastructure improvements, and expanding emergency medical facilities are essential for reducing response times and improving patient outcomes. Performance tracking and data analytics can provide valuable insights, allowing targeted interventions to address bottlenecks. Training and preparedness are crucial for effective disaster response, yet gaps in training access and specialized programs remain. Continuous education and advanced training for EMS personnel, particularly in CPR, trauma management, and specialized medical fields, are necessary. Establishing new training centers and digital hubs for disaster response can help disseminate knowledge and develop skills. Collaborating with international agencies and integrating simulation-based training can enhance readiness and resilience in disaster scenarios.
Financial constraints and administrative inefficiencies pose significant challenges to the sustainability of EMS. Reliance on national and municipal funding highlights the need for strategic financial planning and resource optimization. Streamlining administrative processes and developing financial partnerships can reduce overhead and improve efficiency. Big data analytics can help predict funding needs and optimize resource allocation. Securing more governmental and international support is crucial for advancing EMS capabilities.
Serbia’s Emergency Medical Response Systems face a range of challenges, including organizational diversity, resource constraints, communication gaps, and variable response times. Addressing these requires a comprehensive approach that includes policy changes, organizational improvements, and operational interventions. Standardizing protocols, enhancing communication systems, optimizing resource allocation, and investing in training and infrastructure are vital steps toward improving EMRS effectiveness and resilience. By leveraging technology and fostering collaboration, Serbia can enhance its emergency medical services and ensure all citizens have access to timely and effective care in emergencies.
These findings offer a roadmap for policymakers, healthcare administrators, and EMS personnel to prioritize strategic interventions and build a robust emergency medical response system. With concerted efforts and sustained investment, Serbia can align its EMS with international standards, improving health and safety for its population.
Author Contributions
V.M.C. conceived the original idea for this study and developed the study design and questionnaire. V.M.C. and J.T. contributed to the dissemination of the questionnaire, while V.M.C. analyzed and interpreted the data. R.R. made a significant contribution by drafting the introduction; V.M.C., J.T., and V.R. drafted the discussion, and V.M.C., R.R., and J.T. composed the conclusions. V.M.C., H.R., and H.B. critically reviewed the data analysis and contributed to revising and finalizing the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Scientific–Professional Society for Disaster Risk Management, Belgrade (https://upravljanje-rizicima.com/, accessed on 18 August 2024) and the International Institute for Disaster Research (https://idr.edu.rs/, accessed on 18 August 2024), Belgrade, Serbia.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the Scientific–Professional Society for Disaster Risk Management and the International Institute for Disaster Research (protocol code 005/2024, 15 July 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
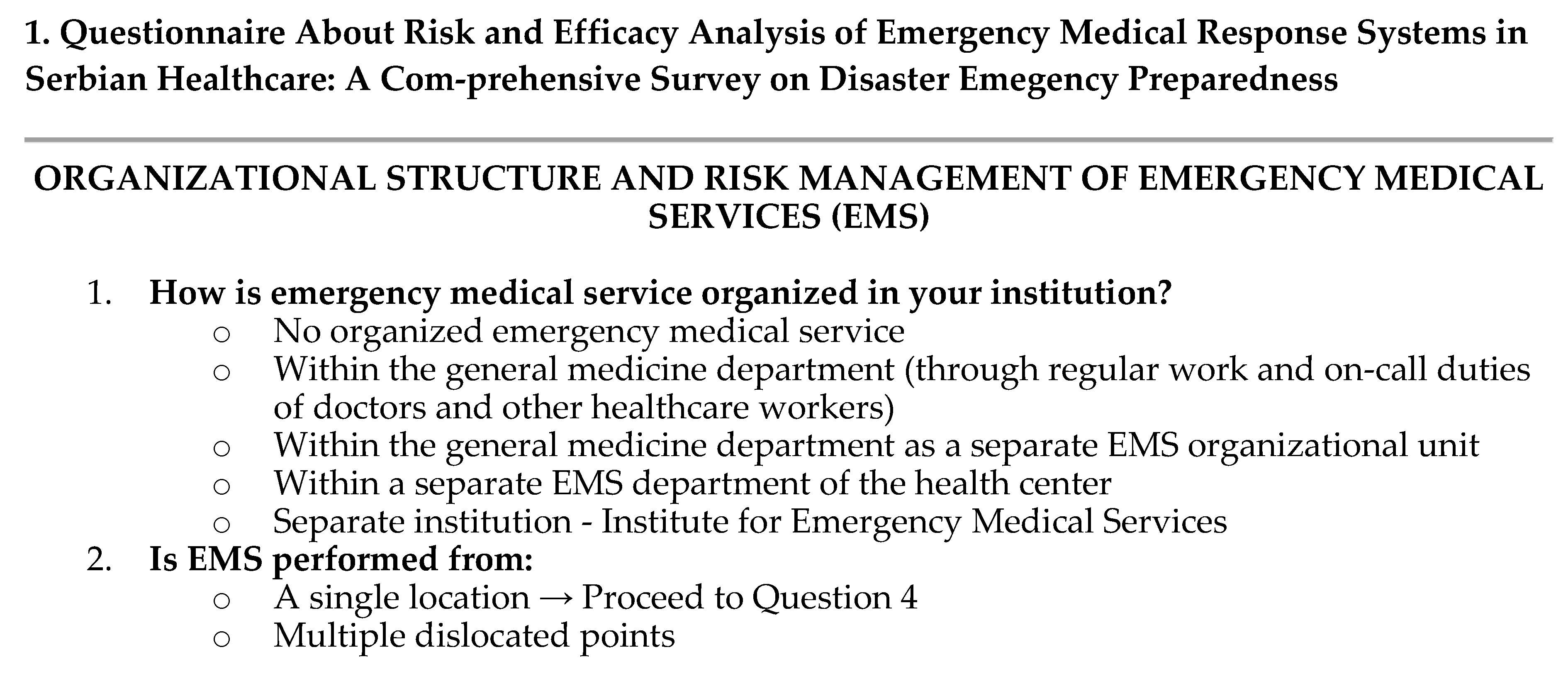
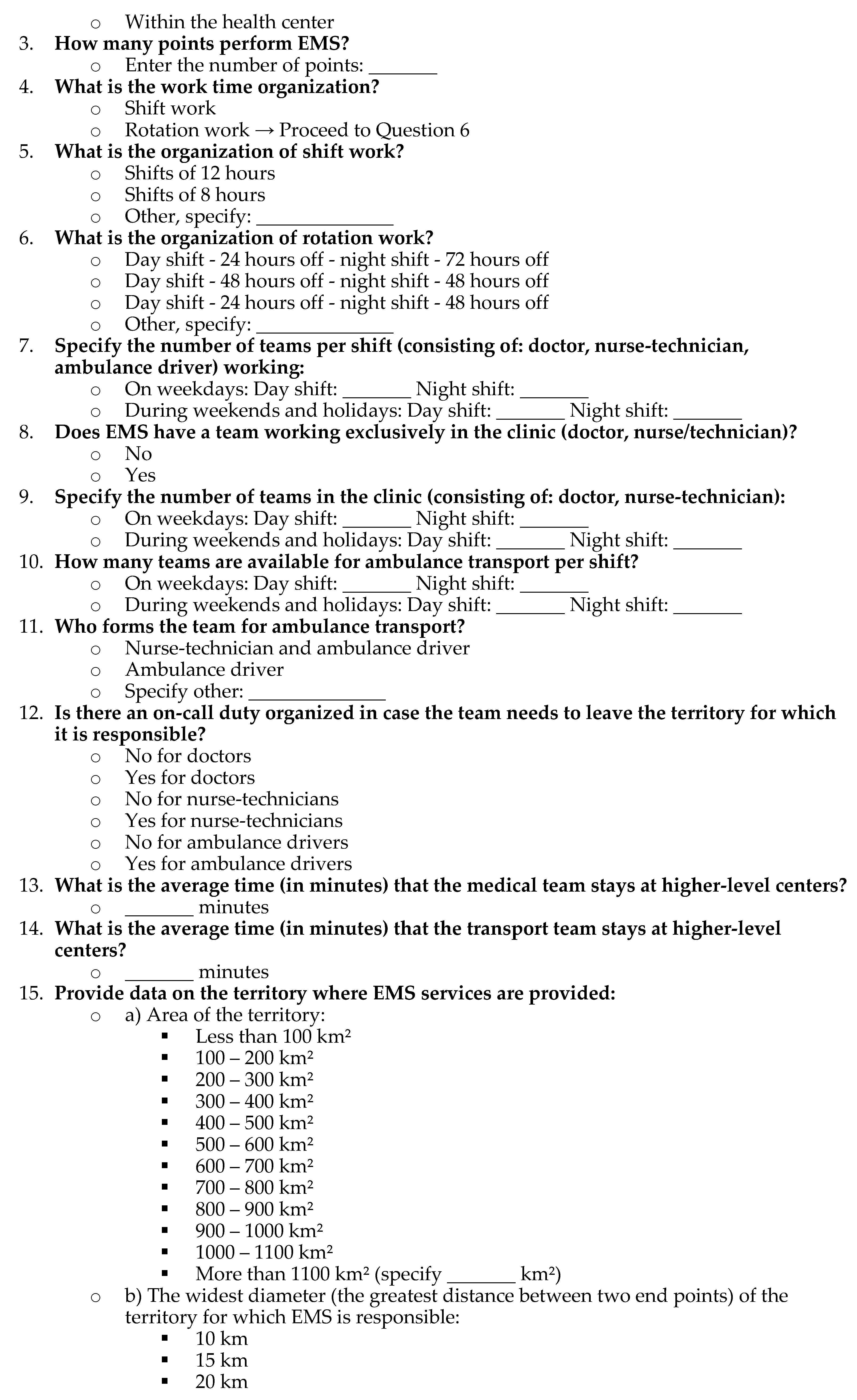
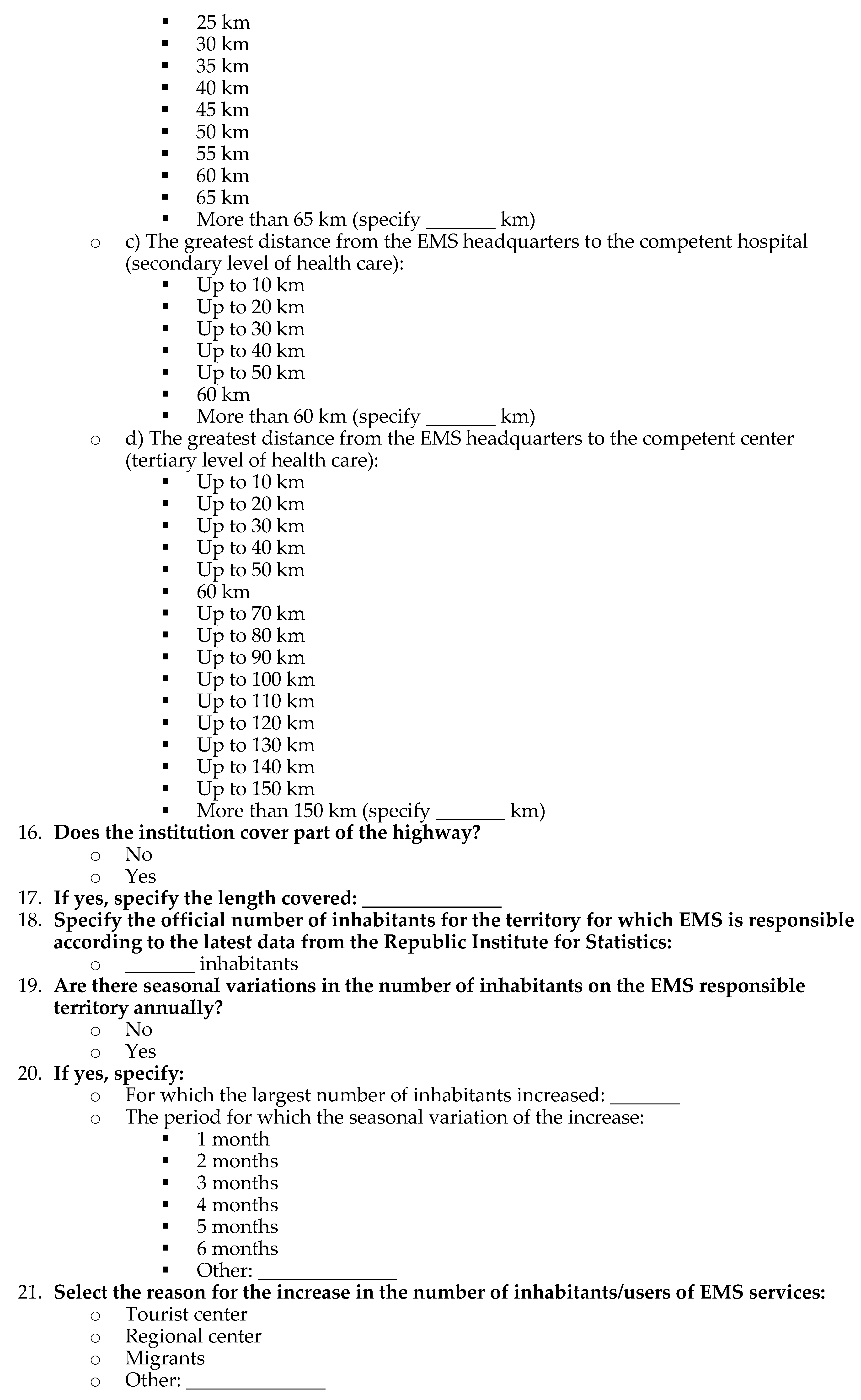
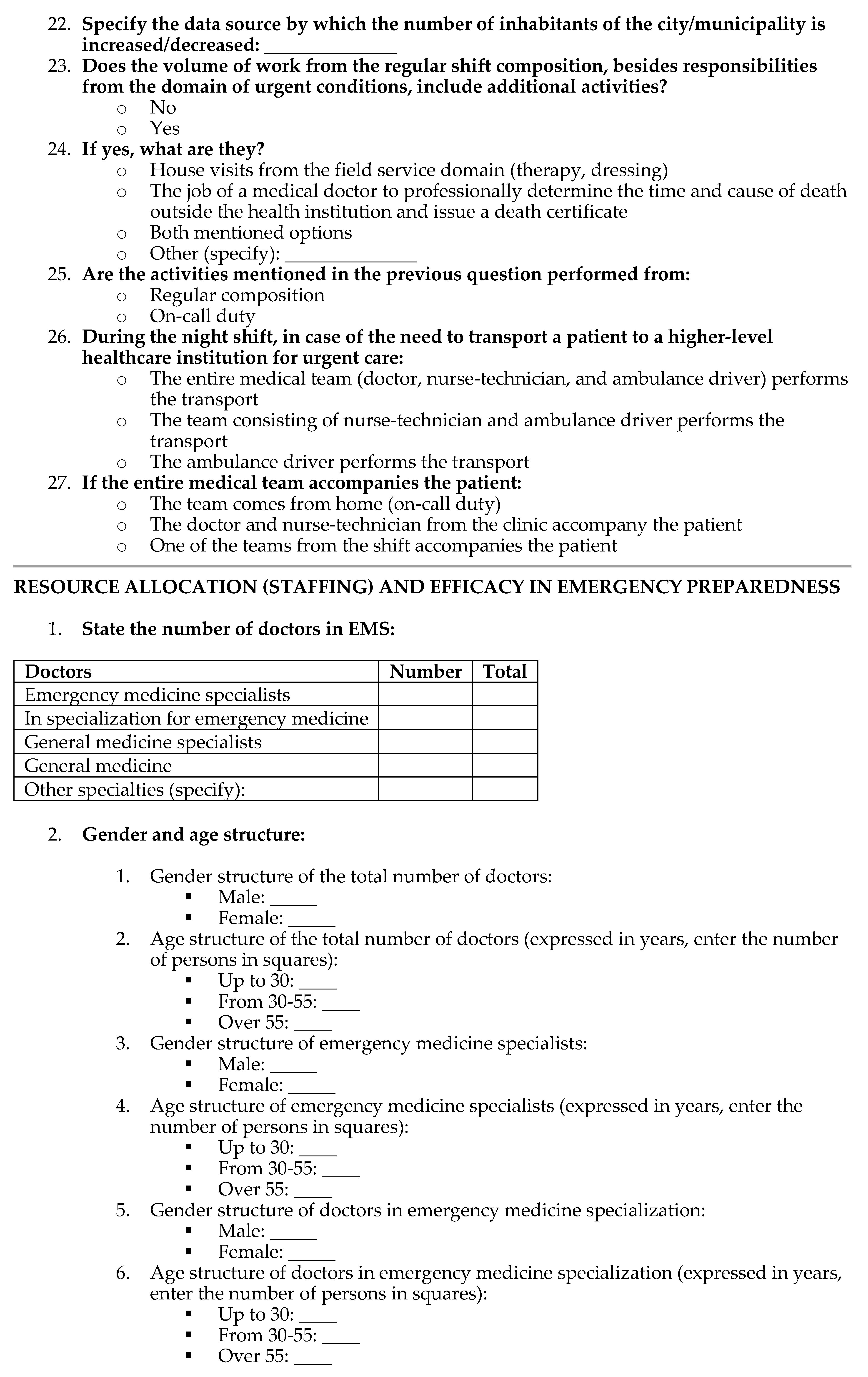
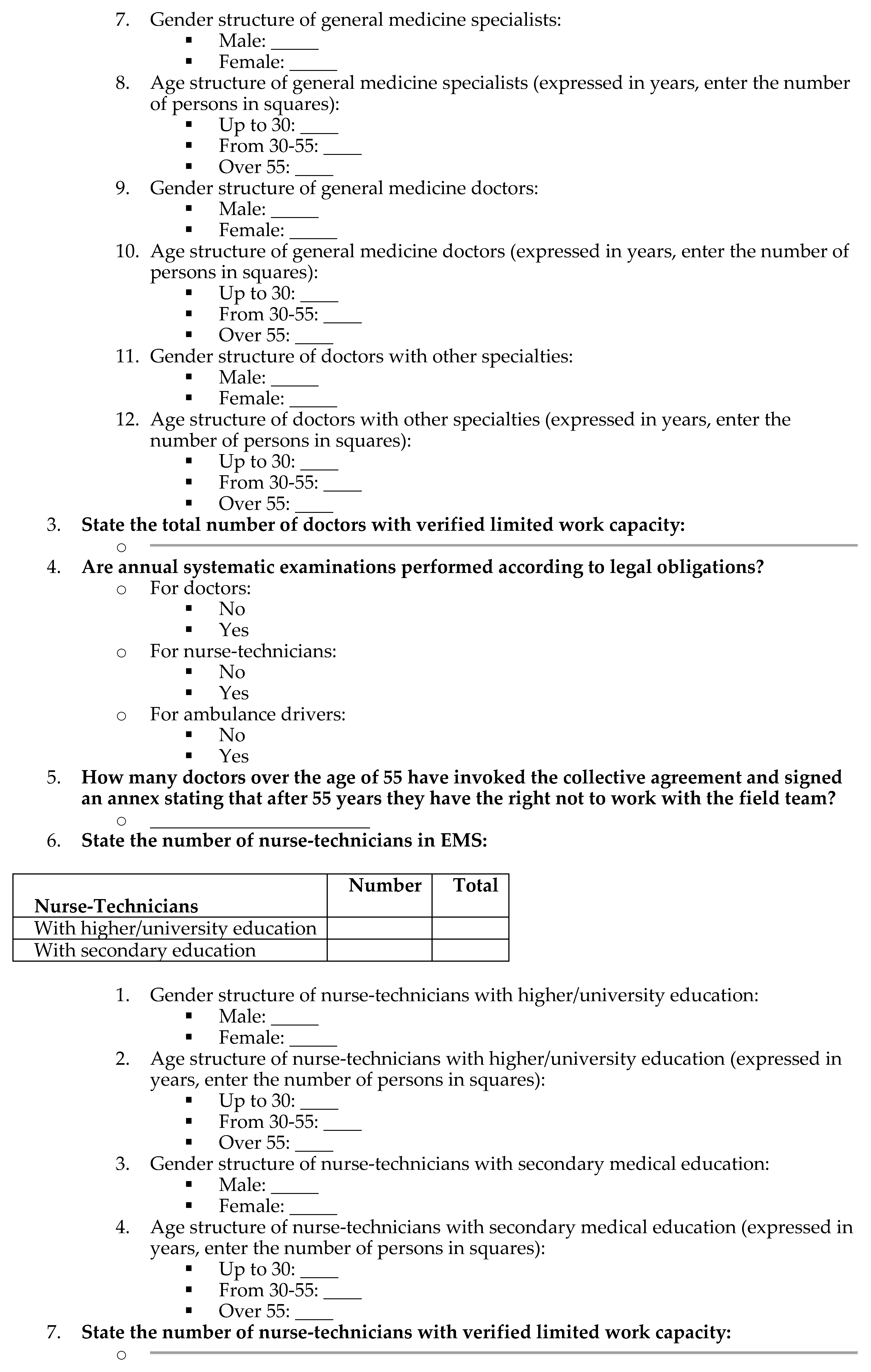
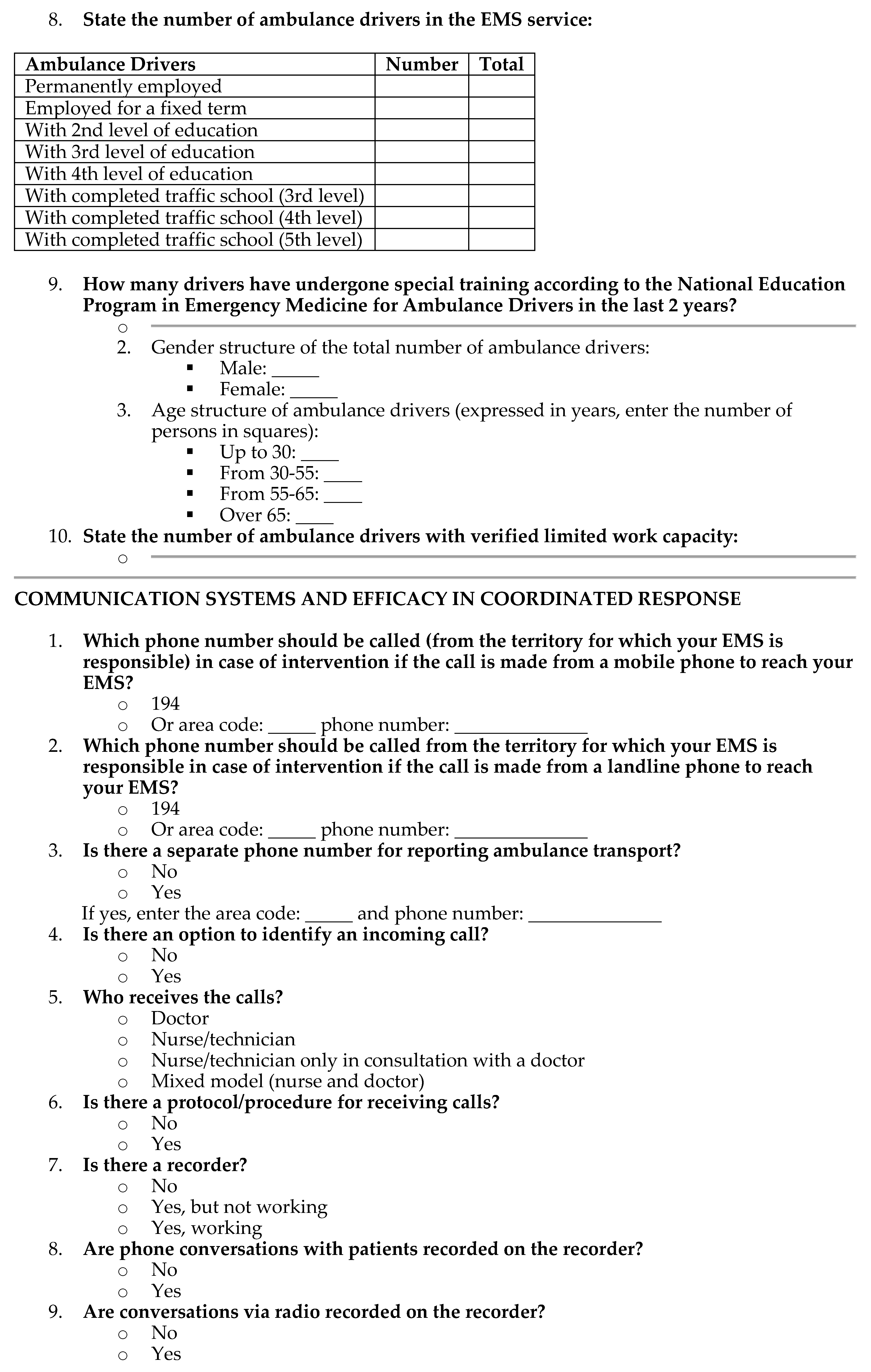
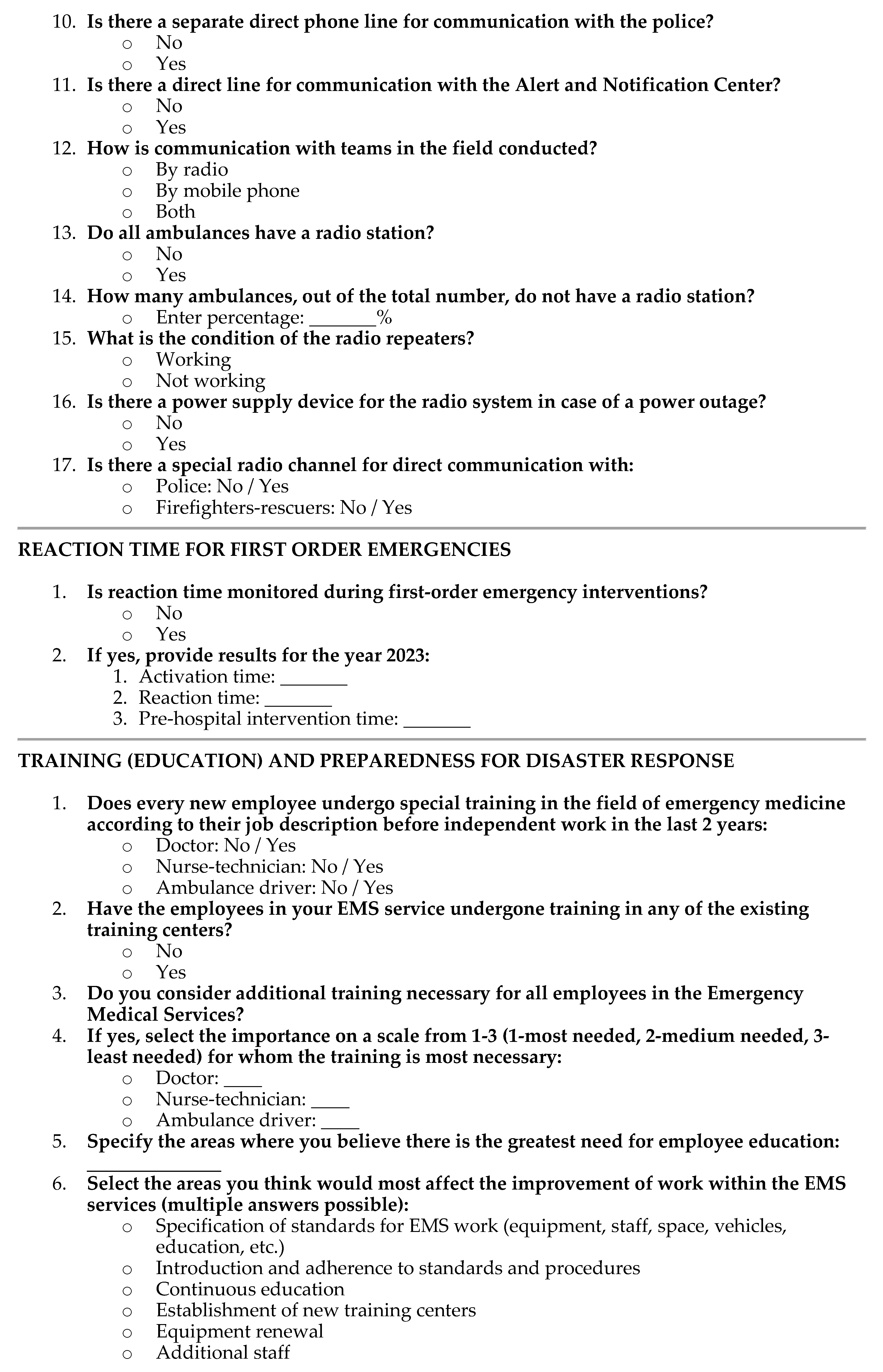
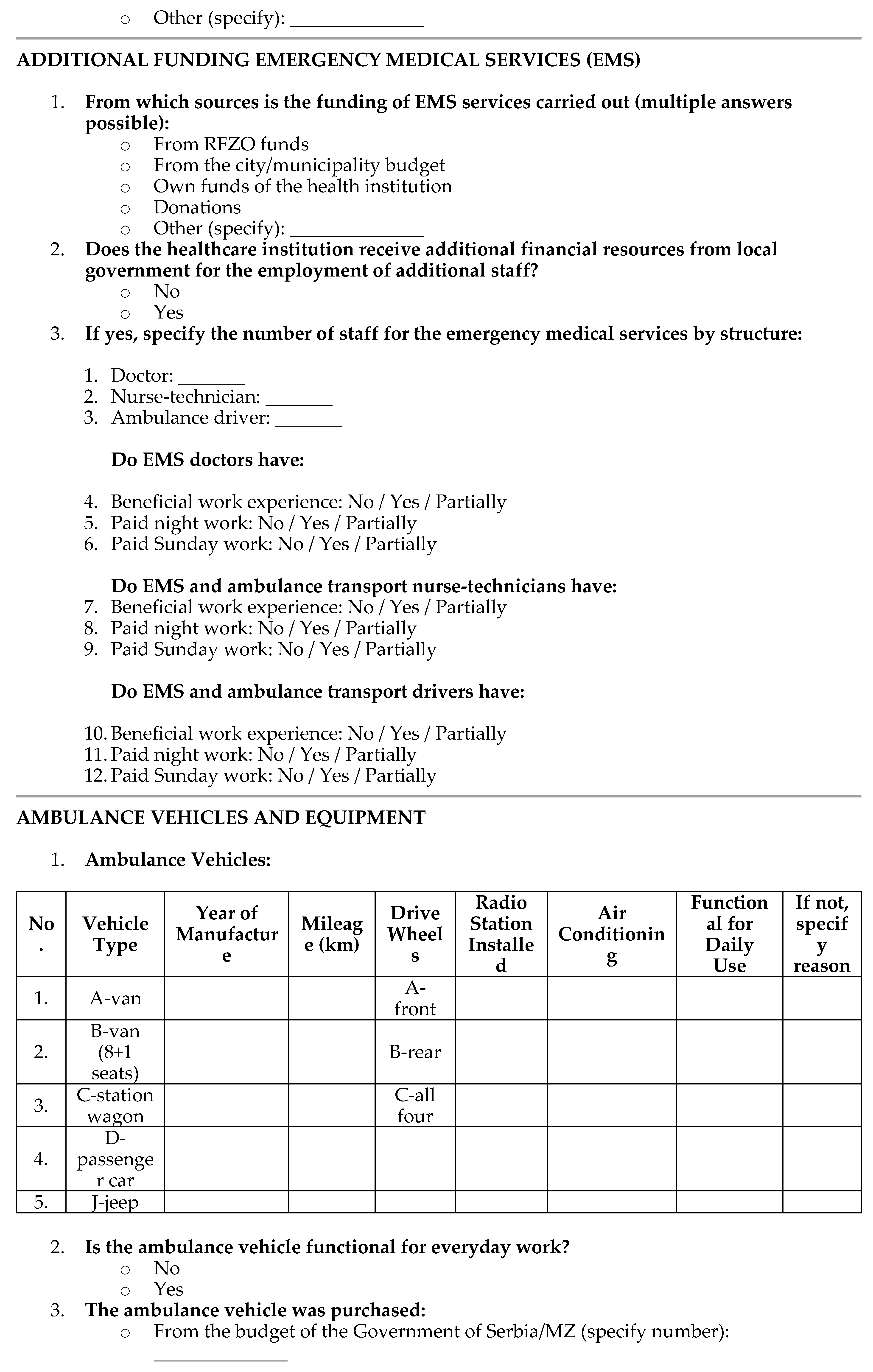
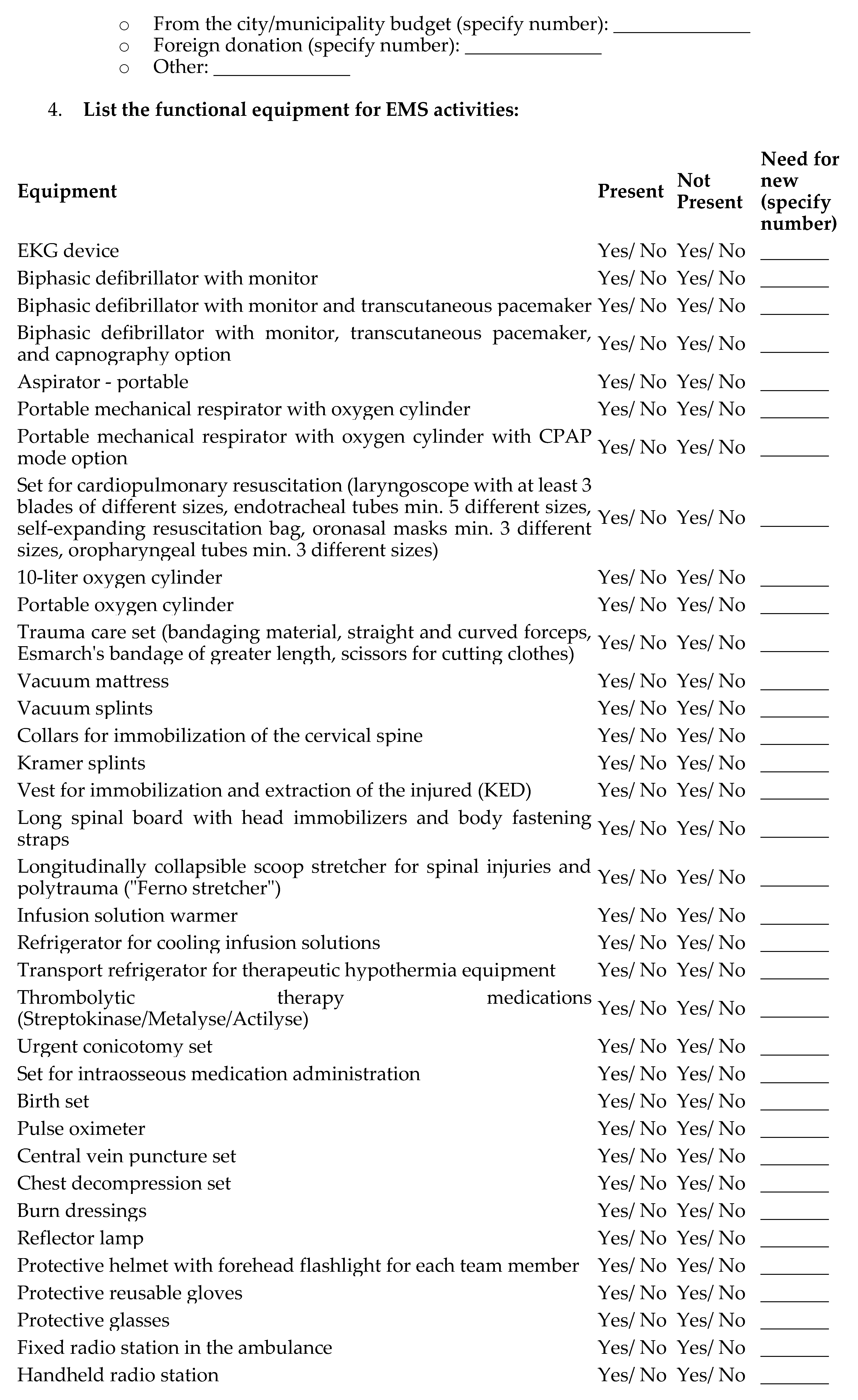
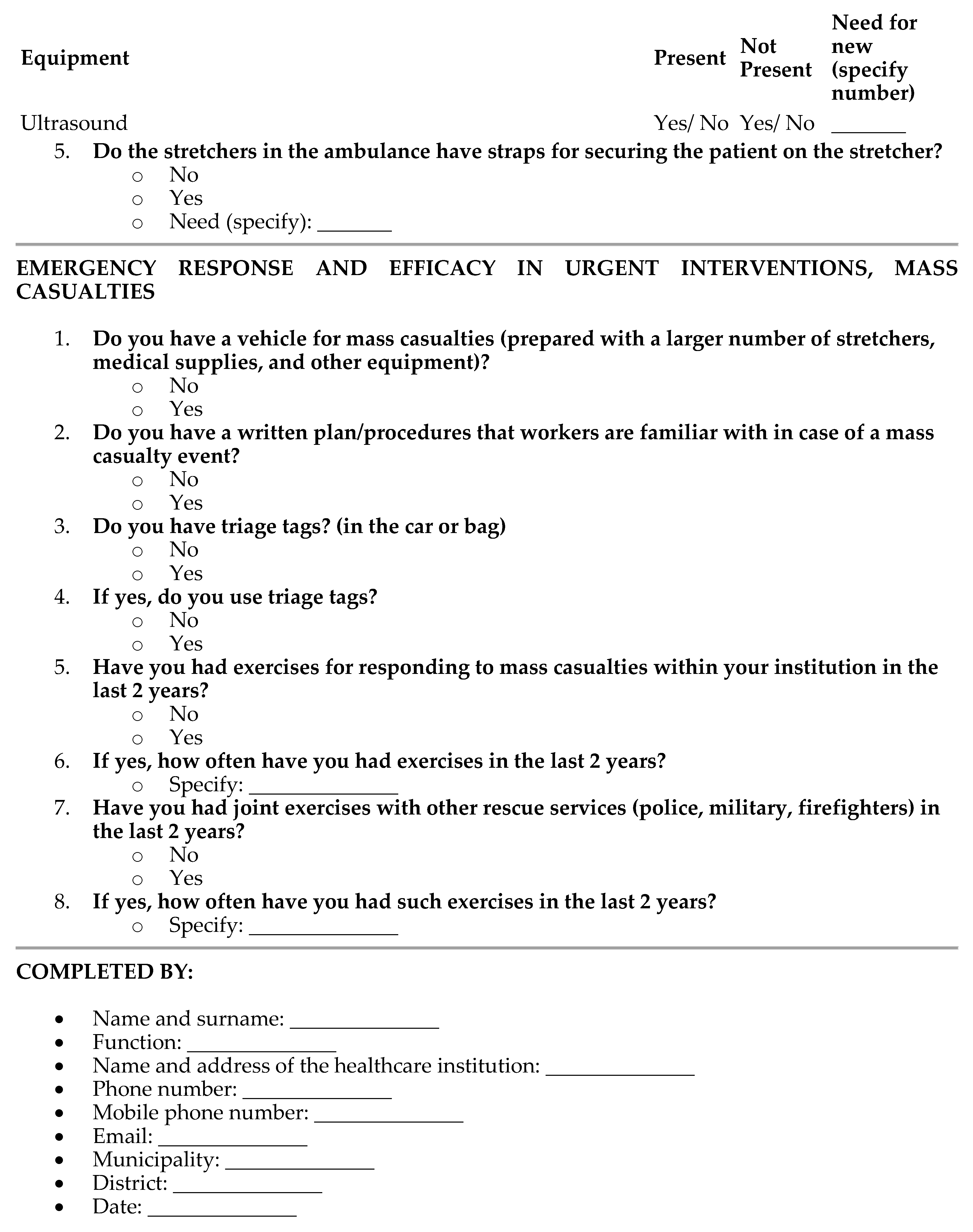
References
- Cvetković, V.; Tanasić, J.; Ocal, A.; Živković-Šulović, M.; Ćurić, N.; Milojević, S.; Knežević, S. The Assessment of Public Health Capacities at Local Self-Governments in Serbia. Lex localis - Journal of Local Self Government 2023, 21, 1201–1234. [Google Scholar] [CrossRef] [PubMed]
- Cvetković, V.M.; Tanasić, J.; Ocal, A.; Kešetović, Ž.; Nikolić, N.; Dragašević, A. Capacity Development of Local Self-Governments for Disaster Risk Management. International Journal of Environmental Research and Public Health 2021, 18, 10406. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Liu, J.; Han, Z.; Jiang, J. Stochastic Petri net based modeling of emergency medical rescue processes during earthquakes. Journal of systems science and complexity 2021, 34, 1063–1086. [Google Scholar] [CrossRef]
- Usoro, A.; Mehmood, A.; Rapaport, S.; Ezeigwe, A.K.; Adeyeye, A.; Akinlade, O.; Dias, J.; Barnett, D.J.; Hsu, E.B.; Tower, C. A scoping review of the essential components of emergency medical response systems for mass casualty incidents. Disaster medicine and public health preparedness 2023, 17, e274. [Google Scholar] [CrossRef]
- Billhardt, H.; Lujak, M.; Sánchez-Brunete, V.; Fernández, A.; Ossowski, S. Dynamic coordination of ambulances for emergency medical assistance services. Knowledge-Based Systems 2014, 70, 268–280. [Google Scholar] [CrossRef]
- Hernandez-Quevedo, C.; Bjegovic-Mikanovic, V.; Vasic, M.; Vukovic, D.; Jankovic, J.; Jovic-Vranes, A.; Santric-Milicevic, M.; Terzic-Supic, Z. How accessible is the Serbian health system? Main barriers and challenges ahead. European Journal of Public Health 2020, 30, ckaa166-1397. [Google Scholar] [CrossRef]
- Nelson, B.D.; Simic, S.; Beste, L.; Vukovic, D.; Bjegovic, V.; VanRooyen, M.J. Multimodal assessment of the primary healthcare system of Serbia: a model for evaluating post-conflict health systems. Prehospital and disaster medicine 2003, 18, 6–13. [Google Scholar] [CrossRef]
- Gacevic, M.; Milicevic, M.S.; Vasic, M.; Horozovic, V.; Milicevic, M.; Milic, N. The relationship between dual practice, intention to work abroad and job satisfaction: A population-based study in the Serbian public healthcare sector. Health Policy 2018, 122, 1132–1139. [Google Scholar] [CrossRef]
- Radović, V.; Ćurčić, L. The opportunities of crises and emergency risk communication in activities of Serbian public health workforce in emergencies. Iranian journal of public health 2012, 41, 15. [Google Scholar] [PubMed]
- Tiede, W.; Simon, C. Comparative analysis of the Serbian and German legislation on emergency medical services. SEER Journal for Labour and Social Affairs in Eastern Europe 2010, 12, 263–293. [Google Scholar] [CrossRef]
- Alavanja, V.A. (81) Reform of the Emergency Medical Services System in Serbia. Prehospital and Disaster Medicine 2007, 22, S48–S49. [Google Scholar]
- Nelson, B.D.; Dierberg, K.; Šćepanović, M.; Mitrović, M.; Vuksanović, M.; Milić, L.; VanRooyen, M.J. Integrating quantitative and qualitative methodologies for the assessment of health care systems: emergency medicine in post-conflict Serbia. BMC health services research 2005, 5, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Mihailovic, N.; Simic-Vukomanovic, I.; Sunjka, M.L.; Zivanovic, S.; Milicic, B.; Milicic, V. Self-Assessment of Health among the Citizens of Serbia in the Transition Period. Iranian Journal of Public Health 2021, 50, 756. [Google Scholar] [CrossRef]
- Masic, I.; Hadziahmetovic, M.; Donev, D.; Pollhozani, A.; Ramadani, N.; Skopljak, A.; Pasagic, A.; Roshi, E.; Zunic, L.; Zildzic, M. Public health aspects of the family medicine concepts in South eastern europe. Materia socio-medica 2014, 26, 277. [Google Scholar] [CrossRef]
- Simić, S.; Milićević, M.Š.; Matejić, B.; Marinković, J.; Adams, O. Do we have primary health care reform? The story of the Republic of Serbia. Health policy 2010, 96, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Mihailovic, N.M.; Kocic, S.S.; Trajkovic, G.; Jakovljevic, M. Satisfaction with health services among the citizens of Serbia. Frontiers in pharmacology 2017, 8, 50. [Google Scholar] [CrossRef]
- Krstic, K.; Janicijevic, K.; Timofeyev, Y.; Arsentyev, E.V.; Rosic, G.; Bolevich, S.; Reshetnikov, V.; Jakovljevic, M.B. Dynamics of health care financing and spending in Serbia in the XXI Century. Frontiers in public health 2019, 7, 381. [Google Scholar] [CrossRef] [PubMed]
- Paunović, I.; Apostolopoulos, S.; Miljković, I.B.; Stojanović, M. Sustainable Rural Healthcare Entrepreneurship: A Case Study of Serbia. Sustainability 2024, 16, 1143. [Google Scholar] [CrossRef]
- Winkelmann, J.; Webb, E.; Williams, G.A.; Hernández-Quevedo, C.; Maier, C.B.; Panteli, D. European countries’ responses in ensuring sufficient physical infrastructure and workforce capacity during the first COVID-19 wave. Health Policy 2022, 126, 362–372. [Google Scholar] [CrossRef]
- Ilic, B.S.; Stankovic, S.S. Analysis of the Sustainability of Supply Chains and Value Chain Management: Economy in the Republic of Serbia. In Government Impact on Sustainable and Responsible Supply Chain Management; IGI Global, 2023; pp. 282–306. [Google Scholar]
- Djukanovic, V.; Mach, E.P.; World Health, O. Alternative approaches to meeting basic health needs in developing countries: a joint UNICEF/WHO study; World Health Organization, 1975. [Google Scholar]
- Vekić, B.; Pilipović, F.; Dragojević-Simić, V.; Živić, R.; Radovanović, D.; Rančić, N. Implementation of the nationwide electronic health record system in Serbia: challenges, lessons learned, and early outcomes. Acta Clinica Croatica 2022, 61, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Vucetic, M.; Uzelac, A.; Gligoric, N. E-health transformation model in Serbia: Design, architecture and developing; 2011; pp. 566–573. [Google Scholar]
- Rajković, P.; Janković, D.; Milenković, A. Developing and deploying medical information systems for Serbian public healthcare: Challenges, lessons learned and guidelines. Computer Science and Information Systems 2013, 10, 1429–1454. [Google Scholar] [CrossRef]
- Bjegovic-Mikanovic, V.; Vasic, M.; Vukovic, D.; Jankovic, J.; Jovic-Vranes, A.; Santric-Milicevic, M.; Terzic-Supic, Z.; Hernández-Quevedo, C.; World Health, O. Serbia: Health system review. 2019. [Google Scholar]
- Veličković, J.; Lutovac, M.; Jokić, M. Integrated health information system in the Republic of Serbia. Annals of Nursing 2023, 2, 24–39. [Google Scholar] [CrossRef]
- Iezzoni, L.I.; Dorner, S.C.; Ajayi, T. Community paramedicine—addressing questions as programs expand. New England Journal of Medicine 2016, 374, 1107–1109. [Google Scholar] [CrossRef] [PubMed]
- Gligorovic, P.; Knezevic, V.; Stojanovic, Z.; Pavicevic, D.; Karlicic, I.S. International models of emergency psychiatric care: the Republic of Serbia. Models of Emergency Psychiatric Services That Work 2020, 243–251. [Google Scholar]
- Zabuha, Y.Y.; Mykhailichenko, T.О.; Morochkovska, O.V. Overview and analysis of occupational risks in healthcare of eastern europe countries. Wiadomości Lekarskie 2019, 72, 2. [Google Scholar]
- Mihic, M.M.; Obradovic, V.L.; Todorovic, M.L.; Petrovic, D.C. Analysis of implementation of the strategic management concept in the healthcare system of Serbia. HealthMED 2012, 6, 34–48. [Google Scholar]
- Bogdanović, R.; Lozanović, D.; Milovančević, M.P.; Jovanović, L.S. The child health care system of Serbia. The Journal of Pediatrics 2016, 177, S156–S172. [Google Scholar] [CrossRef]
- Atanasković-Marković, Z.; Bjegović, V.; Janković, S.; Kocev, N.; Laaser, U.; Marinković, J.; Marković-Denić, L.; Pejin-Stokić, L.; Penev, G.; Stanisavljević, D. The burden of disease and injury in Serbia; Ministry of health of the Republic of Serbia: Belgrade, Serbia, 2003. [Google Scholar]
- Bhattarai, H.K.; Bhusal, S.; Barone-Adesi, F.; Hubloue, I. Prehospital emergency care in low-and middle-income countries: a systematic review. Prehospital and Disaster Medicine 2023, 1–18. [Google Scholar] [CrossRef]
- Jakovljevic, M.; Jovanovic, M.; Lazic, Z.; Jakovljevic, V.; Radovanovic-Velickovic, R.; Antunovic, M. Current efforts and proposals to reduce healthcare costs in Serbia. 2011. [Google Scholar]
- Cvetković, V.; Šišović, V. Understanding the Sustainable Development of Community (Social) Disaster Resilience in Serbia: Demographic and Socio-Economic Impacts. Sustainability 2024, 16, 2620. [Google Scholar] [CrossRef]
- Cvetković, V.; Nikolić, N.; Lukić, T. Exploring Students’ and Teachers’ Insights on School-Based Disaster Risk Reduction and Safety: A Case Study of Western Morava Basin, Serbia. Safety 2024, 10, 2024040472. [Google Scholar] [CrossRef]
- Cvetković, V.M. In-Depth Analysis of Disaster (Risk) Management System in Serbia: A Critical Examination of Systemic Strengths and Weaknesses. 2024. [Google Scholar]
- Sudar, S.; Cvetković, V.; Ivanov, A. Harmonization of Soft Power and Institutional Skills: Montenegro’s Path to Accession to the European Union in the Environmental Sector. International Journal of Disaster Risk Management 2024, 6, 41–74. [Google Scholar] [CrossRef]
- Cvetković, V. Disaster Risk Management; Scientific-Professional Society for Disaster Risk Management. 2024. [Google Scholar]
- Tanasić, J.; Cvetković, V. The Efficiency of Disaster and Crisis Management Policy at the Local Level: Lessons from Serbia; Scientific-Professional Society for Disaster Risk Management: Belgrade, Serbia, 2024. [Google Scholar]
- Lončar, D.; Stojanović, F. Gap analysis of the health system in Serbia compared to the developed health systems in Europe. Ekonomika preduzeća 2017, 65, 216–228. [Google Scholar] [CrossRef]
- Buch Mejsner, S.; Eklund Karlsson, L. Informal payments and health system governance in serbia: A pilot study. Sage Open 2017, 7, 2158244017728322. [Google Scholar] [CrossRef]
- Cvetković, V.M.; Radovanović, M.P.; Milašinović, S.M. Disaster risk communication: Attitudes of Serbian citizens. Sociološki pregled 2021, 55, 1610–1647. [Google Scholar] [CrossRef]
- Cvetković, V.M.; Radovanović, M. Disaster risk communication: attitudes of Serbian citizens-Komunikacija o rizicima od katastrofa: stavovi građana Srbije.
- Ebben, R.H.A.; Siqeca, F.; Madsen, U.R.; Vloet, L.C.M.; Van Achterberg, T. Effectiveness of implementation strategies for the improvement of guideline and protocol adherence in emergency care: a systematic review. BMJ open 2018, 8, e017572. [Google Scholar] [CrossRef] [PubMed]
- Gačić, J.; Jović, S.J.; Terzić, N.S.; Cvetković, V.M.; Terzić, M.T.; Stojanović, D.G.; Stojanović, G.R. Gender differences in stress intensity and coping strategies among students, future emergency relief specialists. Vojnosanitetski pregled 2021, 78, 635–641. [Google Scholar] [CrossRef]
- Cvetković, V.; Aksentijević, V.; Ivović, M. Uloga službe hitne medicinske pomoći u vanrednim situacijama izazvanim terorističkim aktima - The role of emergency medical service in disaster caused by terrorism. 2015; 355–367. [Google Scholar]
- Cvetković, V. Essential Tactics for Disaster Protection and Resque. Belgrade: Scientific-Professional Society for Disaster Risk Management 2022, 1–794. [Google Scholar]
- Hopp, W.J.; Lovejoy, W.S. Hospital operations: Principles of high efficiency health care; FT Press, 2012. [Google Scholar]
- Hick, J.L.; Hanfling, D.; Wynia, M.K.; Pavia, A.T. Duty to plan: health care, crisis standards of care, and novel coronavirus SARS-CoV-2. Nam Perspectives 2020, 2020. [Google Scholar] [CrossRef] [PubMed]
- Hick, J.L.; Hanfling, D.; Cantrill, S.V. Allocating scarce resources in disasters: emergency department principles. Annals of emergency medicine 2012, 59, 177–187. [Google Scholar] [CrossRef]
- Heng, L.; Kaiyou, Y. Research on Smart Warehouse of Emergency Supplies Based on Cloud Computing and IoT. 2022; 693–697. [Google Scholar]
- Connolly, M.A.; Gayer, M.; Ryan, M.J.; Salama, P.; Spiegel, P.; Heymann, D.L. Communicable diseases in complex emergencies: impact and challenges. The Lancet 2004, 364, 1974–1983. [Google Scholar] [CrossRef] [PubMed]
- Committee on the Future of Emergency Care in the United States Health, S. Hospital-based emergency care: at the breaking point; National Academies Press, 2007. [Google Scholar]
- Cameron, P.A.; Gabbe, B.J.; Smith, K.; Mitra, B. Triaging the right patient to the right place in the shortest time. British journal of anaesthesia 2014, 113, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Butkus, R.; Serchen, J.; Moyer, D.V.; Bornstein, S.S.; Hingle, S.T.; Health; Public Policy Committee of the American College of, P. Achieving gender equity in physician compensation and career advancement: a position paper of the American College of Physicians. Annals of internal medicine 2018, 168, 721–723.
- Bogdan, G.M.; Scherger, D.L.; Keller, D.; Wruk, K.M.; Peterson, J.; Swanson, B.S.N.D.D.; Ammon, K.; Daley, D.W.; Dart, R.C.; Gabow, P.A. Health Emergency Assistance Line and Triage Hub (HEALTH) Model. Prepared by Denver Health—Rocky Mountain Poison and Drug Center under Contract 2005, 5–0040. [Google Scholar]
- Besciu, C.D. The Paradoxes of European Medical System Regarding the Performance Management. International Journal of Economic Practices & Theories 2015, 5. [Google Scholar]
- Beamon, B.M.; Kotleba, S.A. Inventory modelling for complex emergencies in humanitarian relief operations. International Journal of Logistics: research and applications 2006, 9, 1–18. [Google Scholar] [CrossRef]
- Barriball, L.; Bremner, J.; Buchan, J.; Craveiro, I.; Dieleman, M.; Dix, O.; Dussault, G.; Jansen, C.; Kroezen, M.; Rafferty, A.M. Recruitment and retention of the health workforce in Europe; European Commission: Brussels, Belgium, 2015. [Google Scholar]
- Aringhieri, R.; Bruni, M.E.; Khodaparasti, S.; van Essen, J.T. Emergency medical services and beyond: Addressing new challenges through a wide literature review. Computers & Operations Research 2017, 78, 349–368. [Google Scholar]
- Anđelić, S.; Vidanović, V.; Milutinović, O. View on health care system of the Republic of Serbia. Annals of Nursing 2023, 2, 13–23. [Google Scholar] [CrossRef]
- Aboueljinane, L.; Sahin, E.; Jemai, Z. A review on simulation models applied to emergency medical service operations. Computers & Industrial Engineering 2013, 66, 734–750. [Google Scholar]
- Abella, M. Policies and best practices for management of temporary migration. 2006. [Google Scholar]
- Wennlund, K.T. Emergency medical dispatching: protocols, experiences and priorities; Karolinska Institutet (Sweden). 2023. [Google Scholar]
- Snow, R.C.; Asabir, K.; Mutumba, M.; Koomson, E.; Gyan, K.; Dzodzomenyo, M.; Kruk, M.; Kwansah, J. Key factors leading to reduced recruitment and retention of health professionals in remote areas of Ghana: a qualitative study and proposed policy solutions. Human resources for health 2011, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hutchison-Krupat, J.; Kavadias, S. Strategic resource allocation: Top-down, bottom-up, and the value of strategic buckets. Management Science 2015, 61, 391–412. [Google Scholar] [CrossRef]
- Dubois, C.-A.; Singh, D. From staff-mix to skill-mix and beyond: towards a systemic approach to health workforce management. Human resources for health 2009, 7, 1–19. [Google Scholar] [CrossRef]
- Mathieu, J.E.; Tannenbaum, S.I.; Salas, E. Influences of individual and situational characteristics on measures of training effectiveness. Academy of management journal 1992, 35, 828–847. [Google Scholar] [CrossRef]
- Harrington, I.C. Improving public safety emergency response efficiency amid uncertainty through crisis leadership training. 2011. [Google Scholar]
- Cvetković, V.M.; Öcal, A.; Ivanov, A. Young adults’ fear of disasters: A case study of residents from Turkey, Serbia and Macedonia. International Journal of Disaster Risk Reduction 2019. [Google Scholar] [CrossRef]
- Cvetković, V.M.; Dragašević, A.; Protić, D.; Janković, B.; Nikolić, N.; Milošević, P. Fire safety behavior model for residential buildings: Implications for disaster risk reduction. International Journal of Disaster Risk Reduction 2022. [Google Scholar] [CrossRef]
- Moran, M. Governing the health care state: a comparative study of the United Kingdom, the United States, and Germany. Manchester University Press, 1999. [Google Scholar]
- Kuhlmann, E.; Allsop, J.; Saks, M. Professional governance and public control: a comparison of healthcare in the United Kingdom and Germany. Current Sociology 2009, 57, 511–528. [Google Scholar] [CrossRef]
- Cvetković, V.; Andrić, K. Comparative Analysis of Disaster Risk Management Systems in Germany, USA, Russia and China. Preprints 2023, arXiv:2023020267. [Google Scholar] [CrossRef]
- Roessler, M.; Zuzan, O. EMS systems in Germany. Resuscitation 2006, 68, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Heyworth, J. Emergency medicine—quality indicators: the United Kingdom perspective. Academic emergency medicine 2011, 18, 1239–1241. [Google Scholar] [CrossRef] [PubMed]
- Mason, S. Keynote address: United Kingdom experiences of evaluating performance and quality in emergency medicine. Academic Emergency Medicine 2011, 18, 1234–1238. [Google Scholar] [CrossRef]
- Mavalankar, D.V.; Ramani, K.V.; Patel, A.; Sankar, P. Building the Infrastructure to Reach and Care for the Poor: Trends, Obstacles and Strategies to overcome them. 2005. [Google Scholar]
- Committee on the Future of Emergency Care in the United States Health, S. Emergency medical services: at the crossroads; National Academies Press, 2007. [Google Scholar]
- Pozner, C.N.; Zane, R.; Nelson, S.J.; Levine, M. International EMS systems: The United States: past, present, and future. Resuscitation 2004, 60, 239–244. [Google Scholar] [CrossRef]
- Pierce, L.G.; Williams, C.A.; Byrne, C.L.; McCauley, D. Planning for organization development in operations control centers; United States. Office of Aerospace Medicine, 2012. [Google Scholar]
- Alanazy, A.R.M.; Wark, S.; Fraser, J.; Nagle, A. Factors impacting patient outcomes associated with use of emergency medical services operating in urban versus rural areas: a systematic review. International journal of environmental research and public health 2019, 16, 1728. [Google Scholar] [CrossRef]
- Boutilier, J.J. Emergency Medical Services Response Optimization; University of Toronto: Toronto, ON, Canada, 2018. [Google Scholar]
- Oostlander, S.A.; Bournival, V.; O’Sullivan, T.L. The roles of emergency managers and emergency social services directors to support disaster risk reduction in Canada. International journal of disaster risk reduction 2020, 51, 101925. [Google Scholar] [CrossRef] [PubMed]
- Parmar, P.; Arii, M.; Kayden, S. Learning from Japan: Strengthening US emergency care and disaster response. Health Affairs 2013, 32, 2172–2178. [Google Scholar] [CrossRef]
- Edgington, D.W. Local Government Emergency Response Following the Great East Japan Earthquake Disaster. JAPAN: Facing Major Natural and International Challenges in the 21st Century, 2014. [Google Scholar]
- Ismail, E.; Naidoo, M.R.; Prakaschandra, D.R. Preparedness of Western Cape ALS providers to provide clinical stabilisation and intensive care for neonates during the patient journey. 2017. [Google Scholar]
- Geisler, E.; Wickramasinghe, N. The role and use of wireless technology in the management and monitoring of chronic diseases. IBM Center for The Business of Government, Tech. Rep 2009. [Google Scholar]
- Oh, J.-Y.; Park, Y.-T.; Jo, E.C.; Kim, S.-M. Current status and progress of telemedicine in Korea and other countries. Healthcare Informatics Research 2015, 21, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Langhelle, A.; Lossius, H.M.; Silfvast, T.; Björnsson, H.M.; Lippert, F.K.; Ersson, A.; Søreide, E. International EMS systems: the Nordic countries. Resuscitation 2004, 61, 9–21. [Google Scholar] [CrossRef]
- Jawhari, B.; Ludwick, D.; Keenan, L.; Zakus, D.; Hayward, R. Benefits and challenges of EMR implementations in low resource settings: a state-of-the-art review. BMC medical informatics and decision making 2016, 16, 1–12. [Google Scholar] [CrossRef]
- Silva, A.L.; Poggioli, S. A81 Emergency Transport experiences from Sub-Saharan Africa: public involvement in transport innovations to improve access to healthcare. Journal of Transport & Health 2015, 2, S47. [Google Scholar]
- Apiratwarakul, K.; Suzuki, T.; Celebi, I.; Tiamkao, S.; Bhudhisawasdi, V.; Pearkao, C.; Ienghong, K. “Motorcycle Ambulance” policy to promote health and sustainable development in large cities. Prehospital and Disaster Medicine 2022, 37, 78–83. [Google Scholar] [CrossRef]
- Saaiman, T.; Filmalter, C.J.; Heyns, T. Important factors for planning nurse staffing in the emergency department: a consensus study. International Emergency Nursing 2021, 56, 100979. [Google Scholar] [CrossRef]
- Abimbola, S.; Baatiema, L.; Bigdeli, M. The impacts of decentralization on health system equity, efficiency and resilience: a realist synthesis of the evidence. Health policy and planning 2019, 34, 605–617. [Google Scholar] [CrossRef] [PubMed]
- Baker, D.; Refsgaard, K. Institutional development and scale matching in disaster response management. Ecological Economics 2007, 63, 331–343. [Google Scholar] [CrossRef]
- Lapčević, Z.; Mandić-Rajčević, S.; Lepić, M.; Jovanović, M. Evaluating a primary healthcare centre’s preparedness for disasters using the hospital safety index: lessons learned from the 2014 floods in Obrenovac, Serbia. International journal of disaster risk reduction 2019, 34, 436–442. [Google Scholar] [CrossRef]
- The World Bank, GFDRR. Serbia – Ready 2 Respond: Emergency Preparredness and Response Assesment - Country Report. 2022. Available online: https://documents1.worldbank.org/curated/en/099350008252228932/pdf/P16537706f45a60ba0898302ebcf92314b2.pdf?_gl=1*14k0evo*_gcl_au*MjExOTU3MDcwMC4xNzE2ODkxNzE0.
- GHS Index. "2021 GHS Index Country Profile for Serbia". 2021. Available online: https://ghsindex.org/country/serbia/.
- Nguyen, H.T.H. Disclosable Restructuring Paper-Serbia Emergency COVID-19 Response Project-P173892. 2021. [Google Scholar]
- Vukosavljević, I.; Vukosavljević, I.; Milutinović, S.; Krivokapić, L.; Cvetković-Jovanović, M.; Ivanović, S. Analysis of the health care system in the Republic of Serbia: Cross-sectional study for the year 2021. Medicinski pregled 2023, 76, 338–343. [Google Scholar] [CrossRef]
- Cvetković, V.M.; Nikolić, N.; Radovanović Nenadić, U.; Öcal, A.; K Noji, E.; Zečević, M. Preparedness and Preventive Behaviors for a Pandemic Disaster Caused by COVID-19 in Serbia. International Journal of Environmental Research and Public Health 2020, 17, 4124. [Google Scholar] [CrossRef]
- Cvetković, M.V. The impact fo demographic factors on the expetation of assistance from the police inn natural disaster. Serbian Science Today 2016, 1, 8–17. [Google Scholar]
- Cvetković, V.; Andrejević, T. Qualitative research on the readiness of citizens to respond to natural disasters. Serbian Science Today 2016, 1. [Google Scholar]
- Cvetković, V.; Kevin, R.; Shaw, R.; Filipović, M.; Mano, R.; Gačić, J.; Jakovljević, V. Household earthquake preparedness in Serbia – a study from selected municipalities. Acta Geographica 2019, 59, In. [Google Scholar]
- Cvetković, V.; Roder, G.; Öcal, A.; Tarolli, P.; Dragićević, S. The Role of Gender in Preparedness and Response Behaviors towards Flood Risk in Serbia. International Journal of Environmental Research and Public Health 2018, 15, 2761. [Google Scholar] [CrossRef]
- Cvetković, V. Essential Tactics for Disaster Protection and Resque. Scientific-Professional Society for Disaster Risk Management, Belgrade: 2024.
- Cvetković, V.M.; Gačić, J.; Jakovljević, V. Geospatial and temporal distribution of forest fires as natural disasters. Vojno delo 2016, 68, 108–127. [Google Scholar] [CrossRef]
- Cvetković, V.; Renner, R.; Lukić, T.; Aleksova, B. Geospatial and Temporal Patterns of Natural and Man-made (Technological) Disasters (1900-2024): Insights from Different Perspectives. Preprints 2024, 2024080175. [Google Scholar]
- Cvetković, V.; Stojković, D. Analysis of geospatial and temporal distribution of storms as a natural disaster. In International scientific conference - Criminalistic education, situation and perspectives 20 years after Vodinelic, Faculty of security, University St. Kliment Ohridski - Bitola in collaboration with Faculty of detectives and security, FON University: Skopje, 2015.
- Cvetković, V.; Milojković, B.; Stojković, D. Analysis of geospatial and temporal distribution of earthquakes as natural disasters. Vojno delo 2014, 66, 166–185. [Google Scholar] [CrossRef]
- Cvetković, V. The relationship between educational level and citizen preparedness for responding to natural disasters. Journal of the Geographical Institute “Jovan Cvijić” SASA 2016, 66, 237–253. [Google Scholar] [CrossRef]
- Cvetković, V.; Gačić, J.; Babić, S. Religiousness level and citizen preparedness for natural disasters. Vojno delo 2017, 69, 253–262. [Google Scholar] [CrossRef]
- Cvetković, V.; Janković, B. Private security preparedness for disasters caused by natural and anthropogenic hazards. International Journal of Disaster Risk Management 2020, 2, 23–33. [Google Scholar] [CrossRef]
- Cvetković, V.; Roder, G.; Tarolli, P.; Öcal, A.; Ronan, K.; Dragićević, S. Flood risk perception and preparedness: a gendered perspective in Serbia. Disasters 2017. [Google Scholar]
- Cvetković, V.; Roder, G.O.A.; Tarolli, P.; Dragićević, S. The Role of Gender in Preparedness and Response Behaviors towards Flood Risk in Serbia. Int. J. Environ. Res. Public Health 2018, 15, 2761. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Nam, M.-Y.; Choi, J.; Kirlik, A.; Sha, L.; Berlin, R.B. Supporting emergency medical care teams with an integrated status display providing real-time access to medical best practices, workflow tracking, and patient data. Journal of medical systems 2017, 41, 1–19. [Google Scholar] [CrossRef]
- Risser, D.T.; Rice, M.M.; Salisbury, M.L.; Simon, R.; Jay, G.D.; Berns, S.D.; MedTeams Research, C. The potential for improved teamwork to reduce medical errors in the emergency department. Annals of emergency medicine 1999, 34, 373–383. [Google Scholar] [CrossRef]
- McKelvie, S.E. Clinical decision making in uncertainty; an ethnography of a complex intervention in the ambulatory emergency care setting. 2021.
- Gowing, J.R.; Walker, K.N.; Elmer, S.L.; Cummings, E.A. Disaster preparedness among health professionals and support staff: what is effective? An integrative literature review. Prehospital and disaster medicine 2017, 32, 321–328. [Google Scholar] [CrossRef]
- Chapman, K.; Arbon, P. Are nurses ready?: Disaster preparedness in the acute setting. Australasian Emergency Nursing Journal 2008, 11, 135–144. [Google Scholar] [CrossRef]
- Gao, L.; Wu, Q.; Li, Y.; Ding, D.; Hao, Y.; Cui, Y.; Kang, Z.; Jiao, M.; Liang, L.; Ferrier, A. How prepared are hospitals’ emergency management capacity? Factors influencing efficiency of disaster rescue. Disaster medicine and public health preparedness 2018, 12, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Waugh Jr, W.L.; Streib, G. Collaboration and leadership for effective emergency management. Public administration review 2006, 66, 131–140. [Google Scholar] [CrossRef]
- Crane, J.; Noon, C. The definitive guide to emergency department operational improvement: employing lean principles with current ED best practices to create the “no wait” department; Productivity Press: 2019.
- MacDonald, S.; Winner, B.; Smith, L.; Juillerat, J.; Belknap, S. Bridging the rural efficiency gap: expanding access to energy efficiency upgrades in remote and high energy cost communities. Energy Efficiency 2020, 13, 503–521. [Google Scholar] [CrossRef]
- Jack, E.P.; Powers, T.L. Volume flexible strategies in health services: A research framework. Production and Operations Management 2004, 13, 230–244. [Google Scholar] [CrossRef]
- Smith, L.; Folkard, S.; Tucker, P.; Macdonald, I. Work shift duration: a review comparing eight hour and 12 hour shift systems. Occupational and environmental medicine 1998, 55, 217–229. [Google Scholar] [CrossRef]
- Stimpfel, A.W.; Sloane, D.M.; Aiken, L.H. The longer the shifts for hospital nurses, the higher the levels of burnout and patient dissatisfaction. Health affairs 2012, 31, 2501–2509. [Google Scholar] [CrossRef]
- Hamilton-Fairley, D.; Coakley, J.; Moss, F. Hospital at night: an organizational design that provides safer care at night. BMC Medical Education 2014, 14, 1–10. [Google Scholar] [CrossRef]
- Souza, D.L.; Korzenowski, A.L.; Alvarado, M.M.; Sperafico, J.H.; Ackermann, A.E.F.; Mareth, T.; Scavarda, A.J. A systematic review on lean applications’ in emergency departments. 2021; p. 763.
- Dolinskaya, I.; Besiou, M.; Guerrero-Garcia, S. Humanitarian medical supply chain in disaster response. Journal of Humanitarian Logistics and Supply Chain Management 2018, 8, 199–226. [Google Scholar] [CrossRef]
- Yang, Y.; Yin, J.; Ye, M.; She, D.; Yu, J. Multi-coverage optimal location model for emergency medical service (EMS) facilities under various disaster scenarios: a case study of urban fluvial floods in the Minhang district of Shanghai, China. Natural Hazards and Earth System Sciences 2020, 20, 181–195. [Google Scholar] [CrossRef]
- Khakali, S. Assessment of Pre-Hospital Emergency Medical Services Using a Systemic Approach. 2023.
- Cvetković, V.; Nikolić, A. The Role of Social Media in the Process of Informing the Public About Disaster Risks. Preprint 2023. [Google Scholar] [CrossRef]
- Cvetković, V. A Predictive Model of Community Disaster Resilience based on Social Identity Influences. Preprint 2023. [Google Scholar] [CrossRef]
- Cvetkovic, V.; Ivanov, A. Knowledge and perceptions of students of the Academy of criminalistic and police studies about natural disasters. 2015; pp. 181-195.
- Cvetković, V.; Ivković, T. Social Resilience to Flood Disasters: Demographic, Socio-economic and Psychological Factors of Impact. 2022.
- Grozdanić, G.; Cvetković, V.; Lukić, T.; Ivanov, A. Sustainable Earthquake Preparedness: A Cross-Cultural Comparative Analysis in Montenegro, North Macedonia, and Serbia. Sustainability 2024, 16, 3138. [Google Scholar] [CrossRef]
- Carla S, R.G. School-community collaboration: disaster preparedness towards building resilient communities. International Journal of Disaster Risk Management 2019, 1, 45–59. [Google Scholar]
- Mano, R.; A, K.; Rapaport, C. Earthquake preparedness: A Social Media Fit perspective to accessing and disseminating earthquake information. International Journal of Disaster Risk Management 2019, 1, 19–31. [Google Scholar] [CrossRef]
- Gössling, S.; Scott, D.; Hall, C.M. Pandemics, tourism and global change: a rapid assessment of COVID-19. Journal of sustainable tourism 2020, 29, 1–20. [Google Scholar] [CrossRef]
- Reuter-Oppermann, M.; van den Berg, P.L.; Vile, J.L. Logistics for emergency medical service systems. Health Systems 2017, 6, 187–208. [Google Scholar] [CrossRef]
- Koo, D.; Miner, K. Outcome-based workforce development and education in public health. Annual Review of Public Health 2010, 31, 253–269. [Google Scholar] [CrossRef]
- Cvetković, V.M.; Šišović, V. Capacity Building in Serbia for Disaster and Climate Risk Education. Available at SSRN 4575350 2023. [Google Scholar] [CrossRef]
- Cruz, R.D.D.; Ormilla, R.C.G. Disaster Risk Reduction Management Implementation in the Public Elementary Schools of the Department of Education, Philippines. International Journal of Disaster Risk Management 2022, 4, 1–15. [Google Scholar] [CrossRef]
- Cvetković, V.; Tarolli, P.; Roder, G.; Ivanov, A.; Ronan, K.; Ocam, A.; Kutub, R. Citizens education about floods: a Serbian case study. Proceedings of the VII International scientific conference Archibald Reiss days; p. In press.
- Bickel, J. Gender equity in undergraduate medical education: a status report. Journal of women’s health & gender-based medicine 2001, 10, 261–270. [Google Scholar]
- Bickel, J.; Brown, A.J. Generation X: Implications for faculty recruitment and development in academic health centers. Academic Medicine 2005, 80, 205–210. [Google Scholar] [CrossRef] [PubMed]
- World Health, O.; Netherlands Institute for Health Services, R. Evaluation of structure and provision of primary care in Romania: a survey-based project; World Health Organization. Regional Office for Europe: 2012.
- Aunger, J.; Ross Millar, P.; Greenhalgh, J.; Russell Mannion, P.; Rafferty, A.M.; Faulks, M.D.; McLeod, H. How, Why, and When Do Inter-Organisational Collaborations in Healthcare Improve Performance? A Realist Evaluation. 2022. [Google Scholar]
- Van Bruggen, V.; Barendrecht, P.; Geense, A.; Van Dijk, E.; Achilleos, M.; Saris, I.; Meijer, M.; Deijkers, A.; Verwoerd, G.; Taks, M. Continuously improving patient safety by a rapid response system. Critical Care 2010, 14, 1. [Google Scholar] [CrossRef]
- Clawson, J.J. EMS dispatch. Emergency medical services: clinical practice and systems oversight 2015, 94–112. [Google Scholar]
- Taneja, A. Better Elective Waiting Times For The Surgical Outpatient Clinic. 2017.
- Prince, A.W.; Armstrong, E. Empowering nurses to help reduce the rate of primary cesarean births. Journal of Obstetric, Gynecologic, & Neonatal Nursing 2015, 44, S23. [Google Scholar]
- Eitel, D.R.; Rudkin, S.E.; Malvehy, M.A.; Killeen, J.P.; Pines, J.M. Improving service quality by understanding emergency department flow: a White Paper and position statement prepared for the American Academy of Emergency Medicine. The Journal of emergency medicine 2010, 38, 70–79. [Google Scholar] [CrossRef]
- Cvetković, V. Innovative solutions for disaster early warning and alert systems: a literary review. Proceedings of XI International scientific conference Archibald Reiss days, November 9-10, 2021At: Belgrade, University of Criminal Investigation and Police Studies 2021.
- Vladimir, C.M. Policija i prirodne katastrofe - Police and natural disasters. Beograd: Zadužbina Andrejević: 2016.
- Cvetković, V.M.; Milojković, B. The influence of demographic factors on the level of citizen awareness of police responsibilities in natural disasters. Bezbednost, Beograd 2016, 58, 5–31. [Google Scholar] [CrossRef]
- Brooke, K. Sharing Information between Public Safety and Transportation Agencies for Traffic Incident Management; Transportation Research Board: 2004; Vol. 520.
- Cvetković, V.; Filipović, M. Information systems and disaster risk management. Proceedings of International scientific and professional conference – 40 years of higher education in the field of security – Theory and Practice, Skopje, Republic of Macedonia; 2017. [Google Scholar]
- Svrdlin, M.; Cvetković, V.J.V.d. Mobilni komunikacioni sistemi i aplikacije od značaja za integrisano upravljanje katastrofama -Mobile communications systems and relevant applications for integrated disaster risk management. 2019, In press.
- Cvetković, V.; Nikolić, M. The role of social networks in disaster risk reduction: a case study Belgrade - Uloga društvenih mreža u smanjenju rizika od katastrofa: studija slučaja Beograd. Bezbednost 2021, 61, 25–42. [Google Scholar] [CrossRef]
- Cvetković, V.M.; Filipović, M.; Dragićević, S.; Novković, I. The role of social networks in disaster risk reduction. 2018; pp. 311-321.
- Cvetković, V. First aid disaster kit for a family: a case study of Serbia - Porodični pribor za pružanje prve pomoći u katastrofama: studija slučaja Srbije. In Proceedings of the IX International scientic conference Archibald Reiss days November 6-7, 2019. University of Criminal Investigation and Police Studies, Belgrade 2019.
- Cvetković, V.M. First aid disaster kit for a family: A case study of Serbia. Archibald Reiss Days 2019, 9. [Google Scholar]
- Lanyero, B.; Edea, Z.A.; Musa, E.O.; Watare, S.H.; Mandalia, M.L.; Livinus, M.C.; Ebrahim, F.K.; Girmay, A.; Bategereza, A.K.; Abayneh, A. Readiness and early response to COVID-19: achievements, challenges and lessons learnt in Ethiopia. BMJ global health 2021, 6, e005581. [Google Scholar] [CrossRef]
- Yen, H.R.; Wang, W.; Wei, C.-P.; Hsu, S.H.-Y.; Chiu, H.-C. Service innovation readiness: Dimensions and performance outcome. Decision Support Systems 2012, 53, 813–824. [Google Scholar] [CrossRef]
- Valente, J.T. From Crash to Care: A Road Towards Improved Safety and Efficiency of Emergency Medical Response. 2024.
- McKinnon, A. The impact of Traffic congestion on logistical efficiency; Citeseer: 1998.
- Nichol, G.; Detsky, A.S.; Stiell, I.G.; O’Rourke, K.; Wells, G.; Laupacis, A. Effectiveness of emergency medical services for victims of out-of-hospital cardiac arrest: a metaanalysis. Annals of emergency medicine 1996, 27, 700–710. [Google Scholar] [CrossRef] [PubMed]
- Elamir, H. Improving Patient Flow in the Emergency Department of a General Hospital Providing Secondary Healthcare Services. 2015.
- Cvetković, V.M. Crises: Readiness of state, local community and citizens. Vojno delo 2017, 69, 122–136. [Google Scholar] [CrossRef]
- Cvetković, V.M. Prepreke unapređenju spremnosti za reagovanje u prirodnim katastrofama - Obstacles to improving readiness for responding in natural disasters. Vojno delo 2017, 69, 132–150. [Google Scholar] [CrossRef]
- Weiner, B.J. A theory of organizational readiness for change. In Handbook on implementation science, Edward Elgar Publishing: 2020; pp. 215-232.
- Meyer, J.P.; Becker, T.E.; Vandenberghe, C. Employee commitment and motivation: a conceptual analysis and integrative model. Journal of applied psychology 2004, 89, 991. [Google Scholar] [CrossRef]
- Latman, N.S.; Wooley, K. Knowledge and skill retention of emergency care attendants, EMT-As, and EMT-Ps. Annals of emergency medicine 1980, 9, 183–189. [Google Scholar] [CrossRef]
- Gostin, L.O.; Hanfling, D.; Hanson, S.L.; Stroud, C.; Altevogt, B.M. Guidance for establishing crisis standards of care for use in disaster situations: a letter report. 2009.
- Takahashi, T.; Nakamura, M. The impact of operational characteristics on firms’ EMS decisions: strategic adoption of ISO 14001 certifications. Corporate Social Responsibility and Environmental Management 2010, 17, 215–229. [Google Scholar] [CrossRef]
- Stewart, R.D. Medical direction in emergency medical services: the role of the physician. Emergency Medicine Clinics of North America 1987, 5, 119–132. [Google Scholar] [CrossRef]
- Masiya, T.; Mazenda, A.; Davids, Y.D. Effective public participation in municipal service delivery. Administratio publica 2019, 27, 27–47. [Google Scholar]
- Williamson, S.M.; Prybutok, V. The Era of Artificial Intelligence Deception: Unraveling the Complexities of False Realities and Emerging Threats of Misinformation. Information 2024, 15, 299. [Google Scholar] [CrossRef]
- Molinari, C.; Alexander, J.; Morlock, L.; Lyles, A.C. Does the hospital board need a doctor?: The influence of physician board participation on hospital financial performance. Medical care 1995, 33, 170–185. [Google Scholar] [CrossRef] [PubMed]
- Kelen, G.D.; Wolfe, R.; D’Onofrio, G.; Mills, A.M.; Diercks, D.; Stern, S.A.; Wadman, M.C.; Sokolove, P.E. Emergency department crowding: the canary in the health care system. NEJM Catalyst Innovations in Care Delivery 2021, 2. [Google Scholar]
Figure 1.
Conceptual research model of the emergency medical response system in Serbian healthcare.
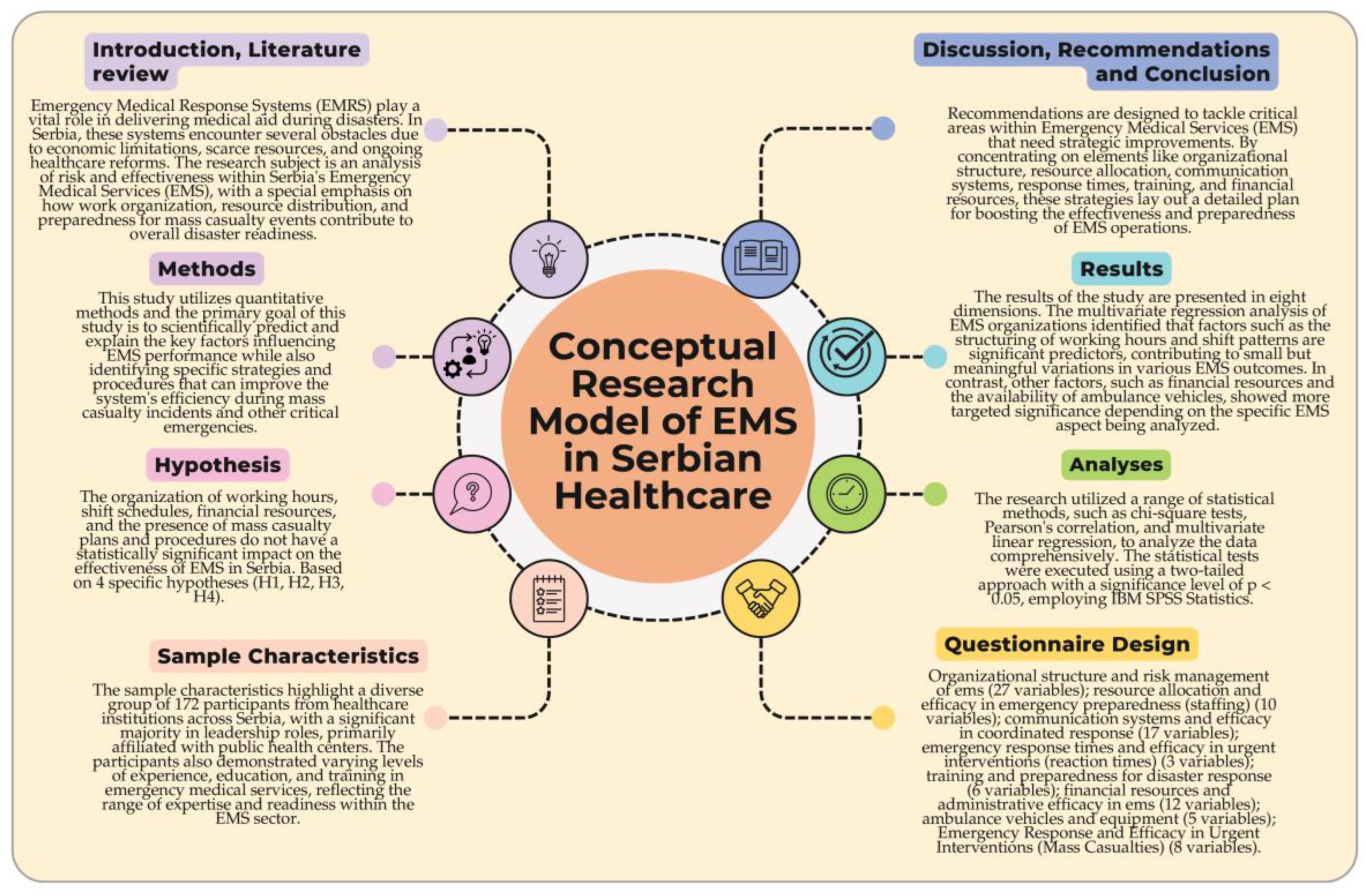
Map 1.
Map of municipalities in Serbia showing municipal and national borders.
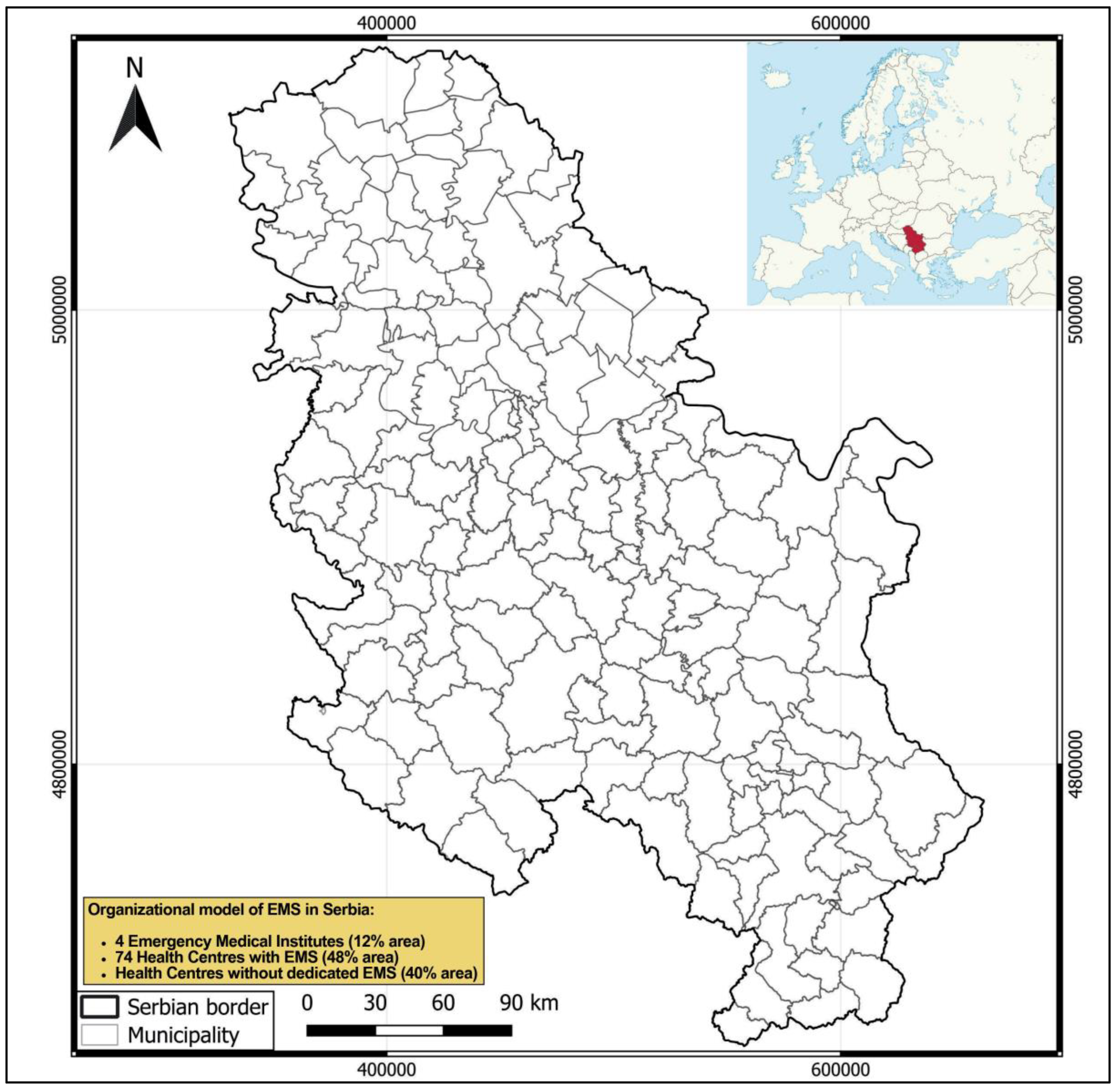

Table 1.
Demographic and Institutional Characteristics of Participants Involved in Emergency Medical Response Services in Serbia.
Table 1.
Demographic and Institutional Characteristics of Participants Involved in Emergency Medical Response Services in Serbia.
| Variables | Category | n | % |
|---|---|---|---|
| Function in EMS | Medical personnel | 23 | 13.37 |
| Leadership positions within a medical institution | 140 | 81.4 | |
| Administrative medical personnel | 7 | 4.07 | |
| Operational medical personnel | 2 | 1.16 | |
| Type of Institution EMS | Public Health Center | 122 | 70.93 |
| Hospital | 11 | 6.40 | |
| Private Healthcare Facility | 39 | 22.67 | |
| Experience in EMS | Less than 5 years | 45 | 26.16 |
| 5-10 years | 85 | 49.42 | |
| More than 10 years | 42 | 24.42 | |
| Gender | Male | 95 | 55.23 |
| Female | 77 | 44.77 | |
| Education Level | High School | 30 | 17.44 |
| Bachelor’s Degree | 100 | 58.14 | |
| Master’s Degree | 42 | 24.42 | |
| Participation in Training | No participation in training | 50 | 29.07 |
| Participated in one or more training sessions | 122 | 70.93 | |
| Emergency Response Role | First responder | 50 | 29.07 |
| Coordinator | 80 | 46.51 | |
| Support staff | 42 | 24.42 | |
| Mass Casualty Plans/Procedures | Yes, institution has a plan | 110 | 63.95 |
| No, institution does not have a plan | 62 | 36.05 | |
| Total | 172 | 100 |
Table 2.
Results of a multivariate regression analysis concerning predictors for EMS organization, number of ems points performed, service area coverage, ems doctors, and mass casualty plans/procedures.
Table 2.
Results of a multivariate regression analysis concerning predictors for EMS organization, number of ems points performed, service area coverage, ems doctors, and mass casualty plans/procedures.
| Predictor Variable |
Organization of EMS | Number of EMS points performed | Service area coverage | EMS doctors |
Plan/procedures mass casualty | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | β | B | SE | β | B | SE | β | B | SE | β | B | SE | β | |
| Organization of working hours |
0.03 | 0.01 | 0.035* | −0.032 | 0.011 | −0.037* | 0.029 | 0.012 | 0.032 | 0.038 | 0.012 | 0.042 | 0.041 | 0.013 | 0.045 |
| Organization of shift work |
0.04 | 0.012 | 0.042* | −0.041 | 0.013 | −0.045* | 0.039 | 0.014 | 0.043* | 0.047 | 0.015 | 0.048 | 0.049 | 0.016 | 0.051 |
| Organization of work in shifts |
0.027 | 0.009 | 0.029 | −0.028 | 0.01 | −0.031* | 0.026 | 0.011 | 0.028 | 0.034 | 0.011 | 0.035 | 0.036 | 0.012 | 0.037 |
| EMS team working only in the clinic |
0.065 | 0.015 | 0.062 | −0.065 | 0.016 | −0.063 | 0.067 | 0.017 | 0.064 | 0.072 | 0.018 | 0.07* | 0.075 | 0.019 | 0.073 |
| Teams per day shift for amb. tran. |
0.058 | 0.014 | 0.058 | −0.062 | 0.015 | 0.059 | 0.061 | 0.016 | 0.06 | 0.066 | 0.017 | 0.065* | 0.07 | 0.018 | 0.069 |
| Teams per night shift for amb. tran. |
0.049 | 0.013 | 0.053 | −0.051 | 0.014 | −0.055 | 0.05 | 0.015 | 0.054 | 0.055 | 0.016 | 0.057 | 0.059 | 0.017 | 0.061 |
| Teams per shift during weekends |
0.034 | 0.01 | 0.038 | −0.036 | 0.011 | −0.039 | 0.035 | 0.012 | 0.037 | 0.041 | 0.012 | 0.043 | 0.044 | 0.013 | 0.046 |
| Financial resources for the healthcare |
0.023 | 0.009 | 0.029 | −0.026 | 0.01 | −0.028 | 0.025 | 0.011 | 0.027 | 0.031 | 0.012 | 0.031 | 0.033 | 0.013 | 0.033 |
| Ambulance vehicles | 0.06 | 0.012 | 0.06 | −0.065 | 0.013 | −0.065 | 0.067 | 0.014 | 0.067 | 0.072 | 0.015 | 0.072* | 0.075 | 0.016 | 0.075 |
| Vehicle for mass casualties (disasters) |
0.044 | 0.011 | 0.041 | −0.048 | 0.012 | −0.046 | 0.047 | 0.013 | 0.045 | 0.052 | 0.014 | 0.05 | 0.055 | 0.015 | 0.053 |
| Plan/procedures | 0.071 | 0.016 | 0.073 | −0.071 | 0.017 | -0.074 | 0.073 | 0.018 | 0.075 | 0.078 | 0.019 | 0.078 | 0.08 | 0.02 | 0.08 |
| 0.019 (0.006) | 0.020 (0.008) | 0.027 (0.015) | 0.035 (0.022) | 0.041 (0.030) | |||||||||||
* p ≤ 0.05; B: unstandardized (B) coefficients; SE: std. error; β: standardized (β) coefficients. Note: Note: EMS organized as a separate institution (Institute for Emergency Medical Services), multiple dislocated points for EMS, service area coverage of more than 1100 km², higher total number of EMS doctors, presence of a plan/procedure for mass casualties, shift work for working hours, shifts of 12 hours, presence of an EMS team working only in the clinic, adequate financial resources for healthcare, ambulance vehicles functional for daily use, availability of a vehicle for mass casualties, availability and usage of triage tags, participation in exercises for responding to mass casualties, and joint exercises with other first responders have all been coded as 1. All other values have been coded as 0.
Table 3.
Pearson’s correlation results for the relationship between various variables and EMS organization, number of ems points performed, and service area coverage (n = 172).
Table 3.
Pearson’s correlation results for the relationship between various variables and EMS organization, number of ems points performed, and service area coverage (n = 172).
| Variables | Organization of EMS | Number of EMS points performed |
Service area coverage |
|||
|---|---|---|---|---|---|---|
| Sig. | r | Sig. | r | Sig. | r | |
| Average time spent by medical teams (minutes) | 0.817 | −0.020 | −0.057 | 0.597 | 0.232 | 0.654 |
| Average time spent by transport teams (minutes) | 0.732 | −0.030 | −0.060 | 0.582 | 0.338 | −0.549 |
| Total number of EMS doctors | 0.000** | −0.340 | 0.139 | 0.199 | 0.190 | −0.698 |
| EMS doctors specialized in emergency medicine | 0.000** | −0.424 | 0.135 | 0.213 | 0.909 | 0.072 |
| EMS doctors in emergency medicine training | 0.000** | −0.430 | 0.139 | 0.203 | 0.857 | 0.112 |
| EMS doctors specialized in general medicine | 0.161 | −0.125 | 0.042 | 0.702 | 0.750 | 0.197 |
| EMS doctors practicing general medicine | 0.001** | −0.286 | 0.140 | 0.199 | 0.874 | −0.126 |
| Permanent EMS ambulance drivers | 0.000** | −0.344 | 0.128 | 0.244 | 0.905 | 0.074 |
| Doctors with verified limited working capacity | 0.068 | −0.162 | 0.033* | 0.762 | 0.981 | 0.015 |
| Day shift teams on weekdays | 0.000** | −0.326 | 0.115 | 0.297 | 0.942 | 0.046 |
| Night shift teams on weekdays | 0.000** | −0.409 | 0.124 | 0.257 | 0.992 | 0.006 |
| Standby readiness for doctors | 0.059 | 0.164 | 0.120 | 0.269 | 0.892 | 0.007 |
| Standby readiness for nurses-techn | 0.088 | 0.149 | 0.113 | 0.299 | 0.321 | 0.08 |
| Maximum diameter of the EMS service area | 0.423 | 0.147 | 0.366 | 0.112 | 0.213 | 0.09 |
| Max distance EMC to hospital | 0.002** | 0.275 | 0.132 | 0.228 | 0.163 | 0.837 |
| Gender distribution of male doctors | 0.000** | −0.346 | 0.079 | 0.472 | 0.995 | 0.004 |
| Gender distribution of female doctors | 0.009** | −0.231 | 0.103 | 0.343 | 0.866 | 0.105 |
| Male emergency medicine specialists | 0.000** | −0.473 | 0.072 | 0.505 | 0.919 | 0.063 |
| Female emergency medicine specialists | 0.000** | −0.338 | 0.066 | 0.404 | 0.435 | 0.460 |
Table 4.
Chi-square test results examine the relationship between different variables and the organization of EMS, employees (EMS) training, and plan/procedures regarding mass casualty.
Table 4.
Chi-square test results examine the relationship between different variables and the organization of EMS, employees (EMS) training, and plan/procedures regarding mass casualty.
| Variable | Organization of EMS |
Employees (EMS) training |
Plan/procedures mass casualty |
|||
|---|---|---|---|---|---|---|
| p | X2 | p | X2 | |||
| Conducting EMS Activities | 0.001** | 190.38 | 0.001** | 126.64 | 0.001** | 110.05 |
| Number of points EMS | 0.005** | 86.99 | 0.107 | 25.68 | 0.526 | 16.56 |
| Organization of working hours | 0.000** | 194.06 | 0.002** | 134.01 | 0.000** | 113.90 |
| Organization of shift work | 0.001** | 76.13 | 0.001** | 34.58 | 0.055 | 14.49 |
| Organization of work in shifts | 0.006** | 85.40 | 0.065 | 23.13 | 0.000** | 42.14 |
| EMS team working only in the clinic | 0.004** | 165.43 | 0.005** | 147.07 | 0.060 | 18.23 |
| Teams per day shift for amb. transport | 0.001** | 265.23 | 0.001** | 154.02 | 0.000** | 140.43 |
| Teams per night shift for amb. transport | 0.000** | 185.06 | 0.003** | 127.23 | 0.000** | 126.24 |
| Teams per shift during weekends | 0.000** | 223.92 | 0.001** | 143.07 | 0.000** | 124.43 |
| Ambulance transport team | 0.001** | 142.18 | 0.056 | 16.98 | 0.000** | 133.37 |
| On-call duty, leave the territory | 0.003** | 154.18 | 0.001** | 142.88 | 0.000** | 123.21 |
| Regular shift workload | 0.001** | 140.29 | 0.006** | 153.06 | 0.000** | 131.61 |
| Number of doctors in EMC | 0.006** | 236.17 | 0.007** | 160.02 | 0.000** | 138.07 |
| Systematic medical examinations | 0.002** | 126.85 | 0.285 | 53.05 | 0.313 | 52.24 |
| Verified limited work capacity | 0.005** | 115.26 | 0.320 | 68.18 | 0.000** | 148.73 |
| Number of ambulance drivers | 0.000** | 211.04 | 0.160 | 34.30 | 0.909 | 9.128 |
| Separate phone number for amb. transport | 0.007** | 129.06 | 0.000** | 179.29 | 0.875 | 35.75 |
| Call identification capability | 0.018* | 159.62 | 0.004** | 175.19 | 0.453 | 28.07 |
| Protocol/procedure for receiving calls | 0.023* | 116.4 | 0.000** | 176.43 | 0.000** | 154.63 |
| Presence of a call recorder | 0.003* | 169.14 | 0.001** | 174.02 | 0.000** | 150.10 |
| Recording conversations | 0.001** | 153.06 | 0.065 | 43.65 | 0.232 | 46.01 |
| Communication with teams in the field | 0.005** | 151.13 | 0.001** | 179.06 | 0.000** | 152.96 |
| Presence of radio stations in ambulances | 0.001** | 124.43 | 0.003** | 172.02 | 0.000** | 148.92 |
| Condition of radio repeaters | 0.008** | 134.18 | 0.204 | 34.01 | 0.000** | 18.56 |
| Power supply device for the radio system | 0.001** | 123.02 | 0.001** | 183.02 | 0.000** | 145.05 |
| Dedicated communication: police | 0.005** | 127.01 | 0.000** | 172.14 | 0.001** | 124.04 |
| Monitoring reaction time of interventions | 0.001** | 174.44 | 0.000** | 185.93 | 0.005** | 162.87 |
| Dedicated communication firefighers | 0.003** | 119.02 | 0.002** | 172.14 | 0.003** | 148.73 |
| Training for emergency medicine doctors | 0.004** | 105.01 | 0.001** | 187.01 | 0.005** | 139.01 |
| Training for emergency medicine nurses | 0.003** | 102.07 | 0.002** | 175.01 | 0.001** | 23.08 |
| Financial resources for the healthcare | 0.001** | 156.07 | 0.003* | 165.45 | 0.000** | 211.76 |
| Ambulance vehicles | 0.765 | 15.06 | 0.001** | 197.32 | 0.005** | 175.20 |
| Vehicle for mass casualties (disasters) | 0.005** | 130.52 | 0.001** | 159.67 | 0.000** | 172.45 |
| Plan/procedure: mass casualties | 0.001** | 110.30 | 0.005** | 149.32 | 0.000** | 215.65 |
| Triage tags | 0.003** | 118.01 | 0.002** | 150.2 | 0.045 | 35.53 |
| Exercises for responding to mass casualties | 0.001** | 103.32 | 0.001** | 149.01 | 0.000** | 178.34 |
| Joint exercises with other first responders | 0.003** | 109.11 | 0.005** | 139.04 | 0.000** | 160.14 |
* p ≤ 0.05; ** p ≤ 0.01.
Table 5.
Organizational and operation of emergency medical services (EMS).
| Variables | Category | n | % |
|---|---|---|---|
| Organization of EMS in Facility | No organized emergency medical service | 2 | 1.44 |
| Special institution – Institute for Emergency Medical Services | 5 | 3.60 | |
| Within a special Emergency Medical Service department of a health center | 64 | 46.04 | |
| Within the general medical service (through regular work and duty of doctors and other health workers) | 47 | 33.81 | |
| Within the general medical service, as a separate organizational unit for emergency medical services | 21 | 15.11 | |
| Conducting EMS Activities | From a single location | 46 | 26.7 |
| Within a healthcare facility | 78 | 45.3 | |
| From multiple dislocated points | 13 | 7.6 | |
| Number of points where EMS activities are conducted | From 0 to 2 points | 80 | 88.89 |
| From 3 to 5 points | 4 | 4.44 | |
| From 6 to 10 points | 4 | 4.44 | |
| From 11 to 50 points | 1 | 1.11 | |
| From 51+ points | 1 | 1.11 | |
| Organization of working hours | Shift work | 95 | 55.2 |
| Rotating shifts | 77 | 44.8 | |
| Organization of shift work | In shifts of 12 hours | 138 | 80.2 |
| Other | 14 | 8.1 | |
| In shifts of 8 hours | 20 | 11.6 | |
| Organization of work in shifts | Day shift - 24h off – night shift - 48h off | 33 | 24.44 |
| Day shift – 24h off – night shift – 72h off | 70 | 51.85 | |
| Day shift – 48h off – night shift - 48h off | 32 | 23.70 | |
| Team configurations during daytime shifts on weekdays | 1 team (all variations) | 87 | 50.6 |
| 2 teams (all variations) | 29 | 16.9 | |
| 3 or more teams | 6 | 3.5 | |
| Special configurations | 48 | 27.9 | |
| Team configurations during nighttime shifts on weekdays | 0 teams | 2 | 1.2 |
| 1 team (all variations) | 83 | 48.3 | |
| 2 teams (all variations) | 28 | 16.3 | |
| 3 or more teams | 19 | 11.0 | |
| Special configurations | 40 | 23.2 | |
| Healthcare Management Plan have a team that only works in the clinic | Yes | 49 | 28.5 |
| N/A | 38 | 22.1 | |
| No | 85 | 49.4 | |
| Teams in the clinic during the daytime on weekdays | 1 team (including various descriptions) | 110 | 64.0 |
| 2 teams | 14 | 8.1 | |
| 3 or more teams (special configurations) | 12 | 7.0 | |
| Teams in the clinic during the nighttime on weekdays | 0 teams | 26 | 15.1 |
| 1 team (including various descriptions) | 124 | 72.1 | |
| Transport by a team of medical nurse-technician and driver | 33 | 19.2 |
Table 6.
Comprehensive overview of emergency medical services (EMS) structure, operations, and geographical coverage.
Table 6.
Comprehensive overview of emergency medical services (EMS) structure, operations, and geographical coverage.
| Variables | Category | n | % |
|---|---|---|---|
| Medical transport teams during daytime shifts on weekdays | No teams reported | 9 | 5.2 |
| 1 team configurations | 106 | 43.0 | |
| 2 teams configurations | 39 | 14.0 | |
| 3 teams configurations | 7 | 4.1 | |
| 4 teams configurations | 7 | 4.1 | |
| 5 teams configurations | 2 | 1.2 | |
| More than 5 teams configurations | 3 | 1.7 | |
| Medical transport teams during nighttime shifts on weekdays | No teams reported | 34 | 19.8 |
| 1 team (including all 1 team variations) | 126 | 47.7 | |
| 2 teams (including all 2 teams variations) | 10 | 5.8 | |
| Composition of medical transport teams | Nurse-technician and vehicle driver | 67 | 29.7 |
| Other | 31 | 13.4 | |
| Vehicle driver | 74 | 33.1 | |
| Medical transport team configurations | Standard team (doctor, nurse/technician, driver) | 65 | 37.8 |
| Driver only or driver with occasional medical staff | 29 | 16.9 | |
| Teams formed based on specific needs | 24 | 14.0 | |
| No specific team required for transport only | 17 | 9.9 | |
| Variable teams depending on patient condition | 36 | 20.9 | |
| Other unspecified configurations | 1 | 0.6 | |
| Organization of preparedness for medical teams | Yes | 74 | 43.0 |
| No | 98 | 57.0 | |
| Organization of preparedness for vehicle drivers | Yes | 83 | 48.3 |
| No | 89 | 51.7 | |
| Average holding time of medical teams (in minutes) | 0 - 10 | 27 | 15.7 |
| 11 - 30 | 25 | 14.5 | |
| 31 - 60 | 27 | 15.7 | |
| 61 - 120 | 31 | 18.0 | |
| 121 - 240 | 22 | 12.8 | |
| 241 mins and above | 16 | 9.3 | |
| Average Holding Time of Transport Teams (in minutes) | Under 10 | 19 | 11.0 |
| 10 - 30 | 26 | 15.1 | |
| 31 - 60 | 32 | 18.6 | |
| 61 - 120 | 30 | 17.4 | |
| 121 - 240 | 19 | 11.0 | |
| 241 mins and above | 6 | 3.5 | |
| Area covered by health services (HMP) | Less than 100 km² | 12 | 7.0 |
| 100 – 200 km² | 18 | 10.5 | |
| 200 – 300 km² | 18 | 10.5 | |
| 300 – 400 km² | 35 | 20.3 | |
| 400 – 500 km² | 18 | 10.5 | |
| 500 – 600 km² | 14 | 8.1 | |
| 600 – 700 km² | 14 | 8.1 | |
| 700 – 800 km² | 13 | 7.6 | |
| 800 – 900 km² | 10 | 5.8 | |
| 900 – 1000 km² | 1 | 0.6 | |
| 1000 – 1100 km² | 9 | 5.2 | |
| Other | 8 | 4.7 | |
| The largest diameter of territory covered by health services (HMP) | Under 30 km | 32 | 18.6 |
| 30 - 60 km | 104 | 60.5 | |
| Over 60 km | 37 | 21.5 | |
| Maximum distance from HMP headquarters to corresponding hospital | 0 - 25 km | 50 | 29 |
| 25 - 50 km | 53 | 31 | |
| 50 - 75 km | 28 | 16 | |
| Over 75 km | 41 | 24 | |
| Maximum distance from HMP headquarters to the corresponding tertiary healthcare center | Under 30 km | 27 | 15.7 |
| 30 to 60 km | 39 | 22.7 | |
| 60 to 90 km | 41 | 23.8 | |
| Over 90 km | 49 | 28.5 | |
| Institution cover part of the highway | Yes | 45 | 26.2 |
| N/A | 41 | 23.8 | |
| No | 86 | 50.0 | |
| Distances that institutions cover part of a highway | Under 25 km | 40 | 23.3 |
| 25 to 50 km | 35 | 20.3 | |
| 50 to 75 km | 30 | 17.4 | |
| Over 75 km | 22 | 12.8 | |
| Seasonal variations in the population numbers within the HMP’s jurisdiction | Yes | 84 | 48.8% |
| N/A | 41 | 23.8% | |
| No | 47 | 27.3% | |
| Specific population increases reported during seasonal variations within the HMP’s jurisdiction | Under 1,000 | 70 | 40.7% |
| 1,000 to 5,000 | 64 | 37.2% | |
| 5,001 to 10,000 | 18 | 10.5% | |
| 10,001 to 30,000 | 33 | 19.2% | |
| Over 30,000 | 7 | 4.1% | |
| Seasonal population increases reported by institutions | Short-Term (1-3 months) | 92 | 53.5 |
| Mid-Term (4-5 months) | 41 | 23.8 | |
| Long-Term (6 months) | 39 | 22.7 | |
| Reasons for the increase in the population or users of HMP services | Seasonal Tourism and Migration | 65 | 37.8 |
| Returnees and Temporary Residents | 34 | 19.8 | |
| Local Events and Activities | 25 | 14.5 | |
| Migrants | 11 | 6.4 | |
| Regional Center | 5 | 2.9 | |
| Tourist Center | 32 | 18.6 | |
| Regular shift’s workload, beyond the scope of managing urgent care, includes additional activities | Yes | 112 | 65.1 |
| N/A | 41 | 23.8 | |
| No | 19 | 11.0 | |
| Extent of Additional Activities by Staff Type | From On-Call Duty | 43 | 25.0 |
| From Regular Staff | 129 | 75.0 | |
| Organization of transport teams during the night shift for urgent medical care | Transport by a team of medical nurse-technician and driver | 33 | 19.2 |
| Transport by a complete medical team (doctor, nurse-technician, driver) | 127 | 73.8 | |
| Transport by a medical vehicle driver only | 12 | 7.0 | |
| Transport by a team of medical nurse-technician and driver | 33 | 19.2 |
Table 7.
Distribution of Doctors and Specialists in Emergency Medical Services.
| Variables | Category | n | % |
|---|---|---|---|
| Doctors in emergency medical services | 0-2 doctors | 20 | 11.63 |
| 3-5 doctors | 44 | 25.58 | |
| 6-8 doctors | 31 | 18.02 | |
| 9-11 doctors | 31 | 18.02 | |
| 12-15 doctors | 19 | 11.05 | |
| More than 15 doctors | 15 | 8.72 | |
| Specialists in emergency medical services | 0-2 doctors | 89 | 51.74 |
| 3-5 doctors | 27 | 15.70 | |
| 6-8 doctors | 7 | 4.07 | |
| 9-11 doctors | 3 | 1.74 | |
| 12-15 doctors | 2 | 1.16 | |
| More than 15 doctors | 4 | 2.33 | |
| Doctors in emergency medical services (EMS) specialists who are in training for emergency medicine | 0-2 doctors | 116 | 67.44 |
| 3-5 doctors | 8 | 4.65 | |
| 6-8 doctors | 2 | 1.16 | |
| 9-11 doctors | 1 | 0.58 | |
| 12-15 doctors | 1 | 0.58 | |
| More than 15 doctors | 0 | 0.00 | |
| Doctors in emergency medical services (EMS) who are specialists in general medicine | 0-2 doctors | 100 | 58.14 |
| 3-5 doctors | 23 | 13.37 | |
| 6-10 doctors | 4 | 2.33 | |
| More than 10 doctors | 1 | 0.58 | |
| General medicine doctors in emergency medical services (EMS) | 0-4 doctors | 74 | 43.02 |
| 5-9 doctors | 42 | 24.42 | |
| 10-19 doctors | 11 | 6.40 | |
| 20 or more doctors | 0 | 0.00 | |
| Institutions have other specialties | Yes | 94 | 54.7 |
| Not Applicable | 43 | 25.0 | |
| No | 35 | 20.3 | |
| Medical specialties in institutions | General medicine (general practitioners) | 30 | 17.4 |
| Specialized medicine (all specialized fields like gynecology, pediatrics, etc.) | 85 | 49.4 | |
| Diagnostics and lab (radiology, biochemistry, etc.) | 40 | 23.3 | |
| Surgical specialties (surgery-related fields) | 10 | 5.8 | |
| Other specialties (less common specialties) | 7 | 4.1 |
Table 8.
Distribution of Doctors and Nursing Staff by Gender and Specialization.
| Variables | Category | n | % |
|---|---|---|---|
| Gender distribution of male doctors | 0-5 doctors | 71 | 41.3 |
| 6-10 doctors | 27 | 15.7 | |
| 11-20 doctors | 21 | 12.2 | |
| 21-30 doctors | 4 | 2.3 | |
| More than 30 doctors | 5 | 2.9 | |
| Gender distribution of female doctors | 0-5 Doctors | 52 | 30.2 |
| 6-10 Doctors | 33 | 19.2 | |
| 11-20 Doctors | 30 | 17.4 | |
| 21-30 Doctors | 7 | 4.1 | |
| More than 30 Doctors | 6 | 3.5 | |
| Male specialists in emergency medicine | 0-2 doctors | 107 | 62.2 |
| 3-5 doctors | 16 | 9.3 | |
| 6-10 doctors | 5 | 2.9 | |
| 11-15 doctors | 1 | 0.6 | |
| more than 15 doctors | 1 | 0.6 | |
| Female specialists in emergency medicine | 0-2 doctors | 113 | 65.7 |
| 3-5 doctors | 10 | 5.8 | |
| 6-10 doctors | 2 | 1.2 | |
| 11-20 doctors | 1 | 0.6 | |
| more than 20 doctors | 1 | 0.6 | |
| Male doctors in specialization for emergency medicine | 0 doctors | 97 | 56.4 |
| 1-2 doctors | 24 | 14.0 | |
| 3-5 doctors | 6 | 3.5 | |
| Female doctors in specialization for emergency medicine | 0 doctors | 93 | 54.1 |
| 1-2 doctors | 28 | 16.3 | |
| 3 or more doctors | 5 | 2.9 | |
| Male general medicine specialists | 0 doctors | 77 | 44.8 |
| 1-2 doctors | 42 | 24.4 | |
| 3 or more doctors | 8 | 4.7 | |
| Female general medicine specialists | 0 doctors | 61 | 35.5 |
| 1-2 doctors | 41 | 23.8 | |
| 3-5 doctors | 17 | 9.9 | |
| 6 or more doctors | 7 | 4.1 | |
| Male general medicine doctors | 0-2 doctors | 84 | 48.8 |
| 3-5 doctors | 33 | 19.2 | |
| 6-10 doctors | 9 | 5.2 | |
| more than 10 doctors | 1 | 0.6 | |
| Female general medicine doctors | 0-2 doctors | 50 | 29.1 |
| 3-5 doctors | 35 | 20.3 | |
| 6-10 doctors | 24 | 14.0 | |
| 11 or more doctors | 17 | 9.9 | |
| Male nursing staff with higher education | 0-1 | 104 | 60.5 |
| 2-4 | 17 | 9.9 | |
| 5 or more | 5 | 2.9 | |
| Female nursing staff with higher education | 0-2 | 95 | 55.2 |
| 3-5 | 16 | 9.3 | |
| 6 or more | 16 | 9.3 | |
| Male nursing technicians with secondary education | 0-5 | 76 | 44.2 |
| 6-10 | 22 | 12.8 | |
| 11-20 | 13 | 7.6 | |
| 21 or more | 16 | 9.3 | |
| 0-5 | 76 | 44.2 | |
| Female nursing technicians with secondary education | 0-5 | 35 | 20.3 |
| 6-10 | 41 | 23.8 | |
| 11-20 | 35 | 20.3 | |
| 21-30 | 11 | 6.4 | |
| 31 or more | 5 | 2.9 |
Table 9.
Age distribution and work capability in medical and emergency services.
| Variables | Category | n | % |
|---|---|---|---|
| Age structure data for doctors under the age of 30 | 0-1 | 105 | 61.0 |
| 2-5 | 19 | 11.0 | |
| 6 or more | 2 | 1.2 | |
| Doctors aged 30-55 | 0-5 | 39 | 22.7 |
| 6-10 | 39 | 22.7 | |
| 11-20 | 48 | 27.9 | |
| 21-30 | 14 | 8.1 | |
| 31 or more | 7 | 4.1 | |
| Doctors over the age of 55 | 0-5 | 85 | 49.4 |
| 6-10 | 19 | 11.0 | |
| 11 or more | 23 | 13.4 | |
| Nursing technicians under the age of 30 with secondary education | 0-1 | 89 | 51.7 |
| 2-4 | 27 | 15.7 | |
| 5 or more | 10 | 5.8 | |
| Nursing technicians aged 30-55 | 0-5 | 29 | 16.9 |
| 6-10 | 33 | 19.2 | |
| 11-15 | 24 | 14.0 | |
| 16-20 | 11 | 6.4 | |
| 21 or more | 30 | 17.4 | |
| Nursing technicians over the age of 55 | 0-2 | 60 | 34.9 |
| 3-5 | 37 | 21.5 | |
| 6-10 | 18 | 10.5 | |
| 11 or more | 11 | 6.4 | |
| Doctors with verified limited work capacity | No limitation | 106 | 61.6 |
| Minor limitation | 18 | 10.5 | |
| Significant limitation | 3 | 1.7 | |
| Doctors comply with the legal requirement to undergo annual systematic medical examinations | Yes | 81 | 47.1 |
| No | 46 | 26.7 | |
| Medical nurses and technicians comply with the legal requirement for annual systematic examinations | Yes | 78 | 45.3 |
| No | 49 | 28.5 | |
| Ambulance drivers regarding compliance with the legal requirement for annual systematic examinations | Yes | 111 | 64.5 |
| No | 16 | 9.3 | |
| Medical nurses and technicians with verified limited work capacity | No Limitation | 92 | 53.5 |
| Minor Limitation | 31 | 18.0 | |
| Significant Limitation | 4 | 2.3 | |
| Ambulance drivers per vehicle in the Emergency Medical Service (HMP) | 0-5 | 77 | 44.77 |
| 6-15 | 34 | 19.77 | |
| 16-30 | 10 | 5.81 | |
| 31-70 | 5 | 2.91 | |
| 71+ | 1 | 0.58 | |
| Ambulance drivers in HMP service (permanent employees) | 0-16 | 115 | 66.9 |
| 17-33 | 11 | 6.4 | |
| 34-66 | 1 | 0.6 | |
| Ambulance drivers in the Emergency Medical Service by contract type (Fixed-term Employees) | 0–1 | 89 | 51.7 |
| 2–3 | 26 | 15.1 | |
| 4–10 | 11 | 6.4 | |
| Ambulance drivers on fixed-term contracts with secondary education | 0–1 | 97 | 56.4 |
| 2–6 | 25 | 14.5 | |
| 8–20 | 5 | 2.9 | |
| Ambulance drivers based on their shifts per month with completed traffic school education | 0 | 115 | 66.9 |
| 1–3 | 10 | 5.8 | |
| 10 | 1 | 0.6 | |
| Ambulance drivers who have undergone special training under the National Emergency Medicine Education Program in the past two years | 0 | 104 | 60.5 |
| 1–6 | 16 | 9.3 | |
| 8–71 | 7 | 4.1 | |
| Male ambulance drivers | 0–9 | 98 | 57.0 |
| 10–29 | 24 | 14.0 | |
| 30–69 | 5 | 2.9 | |
| 70 and above | 1 | 0.6 | |
| Female ambulance drivers | 0 | 123 | 71.5 |
| 1–2 | 2 | 1.2 | |
| 6 | 1 | 0.6 | |
| Ambulance drivers under the age of 30 | 0 | 86 | 50.0 |
| 1–2 | 30 | 17.4 | |
| 3–6 | 9 | 5.2 | |
| 20 | 1 | 0.6 | |
| Ambulance drivers aged 30 to 55 | 0–5 | 82 | 47.7 |
| 6–15 | 33 | 19.2 | |
| 17–33 | 10 | 5.8 | |
| 50 and above | 3 | 1.7 | |
| Ambulance drivers over the age of 55 | 0–3 | 109 | 63.4 |
| 4–10 | 15 | 8.7 | |
| 12 and above | 3 | 1.7 | |
| Ambulance drivers with verified limited work capability | 0 | 119 | 69.2 |
| 1–3 | 7 | 4.1 | |
| 6 | 1 | 0.6 |
Table 10.
Communication channels and call management in emergency services.
| Variables | Category | n | % |
|---|---|---|---|
| Phone number to call (from the territory under your HMP jurisdiction) in case of intervention | 194 | 59 | 34.3% |
| Other | 68 | 39.5% | |
| The specific phone number for registering for ambulance transport? | Yes | 40 | 23.3% |
| N/A | 45 | 26.2% | |
| No | 87 | 50.6% | |
| Capability to identify incoming calls | Yes | 78 | 45.3% |
| N/A | 45 | 26.2% | |
| No | 49 | 28.5% | |
| Who receives calls | Doctor | 24 | 14.0% |
| Nurse/Technician | 24 | 14.0% | |
| Nurse/Technician only with doctor consultation | 18 | 10.5% | |
| Mixed model (nurse, doctor) | 61 | 35.5% | |
| Protocol/procedure for receiving calls | Yes | 93 | 54.1% |
| N/A | 45 | 26.2% | |
| No | 34 | 19.8% |
Table 11.
Technical Equipment and Recording Capabilities.
| Variables | Category | n | % |
|---|---|---|---|
| Presence and condition of a dictation machine | Yes, functional | 61 | 35.5% |
| Yes, non-functional | 16 | 9.3% | |
| No | 50 | 29.1% | |
| Phone conversations with patients are recorded on a dictation machine | Yes | 71 | 41.3% |
| N/A | 45 | 26.2% | |
| No | 56 | 32.6% | |
| Radio communications recorded on a dictation machine | Yes | 15 | 8.7% |
| N/A | 45 | 26.2% | |
| No | 112 | 65.1% | |
| Special direct telephone line for communication with the police | Yes | 21 | 12.2% |
| N/A | 45 | 26.2% | |
| No | 106 | 61.6% | |
| Direct line for communication with the Alert and Notification Center | Yes | 20 | 11.6% |
| N/A | 45 | 26.2% | |
| No | 107 | 62.2% | |
| Communication conducted with teams in the field | Both methods | 14 | 8.1% |
| Via mobile phone | 107 | 62.2% | |
| Via radio | 6 | 3.5% | |
| Ambulance vehicles have a radio station | Yes | 27 | 15.7% |
| N/A | 45 | 26.2% | |
| No | 100 | 58.1% | |
| Ambulance Vehicles Without a Radio Station | 0-5 | 64 | 37.2% |
| 6-10 | 11 | 6.4% | |
| 11-15 | 1 | 0.6% | |
| 16-20 | 24 | 13.9% | |
| Condition of the radio repeaters | Operational | 29 | 16.9% |
| Not Operational | 98 | 57.0% | |
| Device to power the radio communication system in case of a power outage | Yes | 30 | 17.4% |
| N/A | 45 | 26.2% | |
| No | 97 | 56.4% | |
| Special radio communication channel for direct communication with the police | Yes | 3 | 1.7% |
| No | 124 | 72.1% | |
| Special radio communication channel for direct communication with firefighters-rescuers | Yes | 3 | 1.7% |
| No | 124 | 72.1% | |
| Reaction time monitored during first-order emergency interventions | Yes | 68 | 39.5% |
| N/A | 45 | 26.2% | |
| No | 59 | 34.3% |
Table 12.
Analysis of response times in emergency medical services.
| Variables | Category | n | % |
|---|---|---|---|
| Activation times | 0 to 1 hour | 35 | 20.3 |
| >1 to 3 hours | 11 | 6.4 | |
| >3 to 10 hours | 7 | 4.1 | |
| >10 hours | 15 | 8.7 | |
| Reaction time | 0 to 1 hour | 15 | 8.7 |
| >1 to 10 hours | 40 | 23.3 | |
| >10 to 20 hours | 10 | 5.8 | |
| >20 hours | 3 | 1.7 | |
| Prehospital intervention time results | 0 to 10 hours | 27 | 15.7 |
| 10 to 30 hours | 28 | 16.3 | |
| 30 to 60 hours | 9 | 5.2 | |
| More than 60 hours | 4 | 2.3 | |
| A written plan/procedure known to workers in case of disasters | Yes | 84 | 48.8 |
| N/A | 50 | 29.1 | |
| No | 38 | 22.1 | |
| Vehicle for mass casualty incidents equipped with stretchers and medical supplies? | Yes | 10 | 5.8 |
| N/A | 50 | 29.1 | |
| No | 112 | 65.1 | |
| Availability of triage cards (either in vehicles or bags) | Yes | 16 | 9.3 |
| N/A | 50 | 29.1 | |
| No | 106 | 61.6 | |
| Mass casualty response drills in the last 2 years at your institution | Yes | 24 | 14.0 |
| N/A | 50 | 29.1 | |
| No | 98 | 57.0 | |
| Frequently drills for mass casualty incidents | One time per year or less | 20 | 80.0 |
| Twice a year | 4 | 16.0 | |
| More than twice a year | 1 | 4.0 | |
| Joint drills with other emergency services in the last 2 years? | Yes | 27 | 15.7 |
| N/A | 50 | 29.1 | |
| No | 95 | 55.2 |
Table 13.
Training and Compliance in Emergency Medical Services.
| Variables | Category | n | % |
|---|---|---|---|
| Newly hired employee doctors undergone special training in emergency medicine | Yes | 55 | 32.0 |
| No | 72 | 41.9 | |
| Newly hired employee nursing technician undergone special training in emergency medicine | Yes | 53 | 30.8 |
| No | 74 | 43.0 | |
| Employees in EMS service undergone training at any of the existing training centers | Yes | 73 | 42.4 |
| N/A | 45 | 26.2 | |
| No | 54 | 31.4 | |
| Additional training is necessary for all employees in the EMS | Yes | 117 | 68.0 |
| N/A | 45 | 26.2 | |
| No | 10 | 5.8 | |
| Importance of who needs training the most | Doctor | 98 | 57.0 |
| Nursing Technician | 9 | 5.2 | |
| Ambulance Driver | 9 | 5.2 | |
| Categories of training needs | CPR and Trauma Management (Cardiopulmonary resuscitation, trauma management, polytrauma handling) | 45 | 26.2% |
| Urgent Medical Conditions (Emergency response, urgent medical and pediatric care) | 35 | 20.3% | |
| Emergency Protocols and Equipment (Equipment use, triage, protocols, communication) | 32 | 18.6% | |
| Safety and Operational Training (Safety protocols, personal safety, psychological support) | 30 | 17.4% | |
| Specialized Medical Training (Obstetrics, toxicology, neurology, cardiology) | 30 | 17.4% | |
| Specification of norms for operations (equipment, staff, space, vehicles, education, etc.) as key area for enhancing EMC services | Yes | 98 | 57.0 |
| N/A | 45 | 26.2 | |
| No | 29 | 16.9 | |
| Implementation and adherence to standards and procedures as key area for enhancing emc services | Yes | 81 | 47.1 |
| N/A | 45 | 26.2 | |
| No | 46 | 26.7 | |
| Continuous education as key area for enhancing EMC services | Yes | 97 | 56.4 |
| N/A | 45 | 26.2 | |
| No | 30 | 17.4 | |
| Establishing new training centers as key area for enhancing EMC services | Yes | 59 | 34.3 |
| N/A | 45 | 26.2 | |
| No | 68 | 39.5 | |
| Equipment renewal as key area for enhancing EMC services | Yes | 106 | 61.6 |
| N/A | 45 | 26.2 | |
| No | 21 | 12.2 | |
| Additional Staff as key area for enhancing EMC services | Yes | 102 | 59.3 |
| N/A | 45 | 26.2 | |
| No | 25 | 14.5 |
Table 14.
Funding Sources and Staffing in Emergency Medical Services (EMS).
| Variables | Category | n | % |
|---|---|---|---|
| National health insurance fund (RFZO) resources: source of funding EMS | Yes | 119 | 69.2 |
| N/A | 46 | 26.7 | |
| No | 7 | 4.1 | |
| Municipal/City Budget Resources: source of funding EMS | Yes | 67 | 39.0 |
| N/A | 46 | 26.7 | |
| No | 59 | 34.3 | |
| Own Revenue: source of funding EMS | Yes | 42 | 24.4 |
| N/A | 46 | 26.7 | |
| No | 84 | 48.8 | |
| Donations: source of funding EMS | Yes | 35 | 20.3 |
| N/A | 46 | 26.7 | |
| No | 91 | 52.9 | |
| Healthcare institution receive additional financial resources from local government to employ additional staff | Yes | 70 | 40.7 |
| N/A | 47 | 27.3 | |
| No | 55 | 32.0 | |
| Doctors in Emergency Medical Services | 0-5 | 86 | 50.0% |
| 6-10 | 14 | 8.1% | |
| 11-15 | 8 | 4.7% | |
| 16-20 | 8 | 4.7% | |
| 21+ | 9 | 5.2% | |
| Medical Nursing Technicians in Emergency Medical Services | 0-5 | 83 | 48.3% |
| 6-10 | 18 | 10.5% | |
| 11-15 | 11 | 6.4% | |
| 16-20 | 8 | 4.7% | |
| 21+ | 5 | 2.9% | |
| Ambulance Drivers in Emergency Medical Services | 0-5 | 84 | 48.8% |
| 6-10 | 16 | 9.3% | |
| 11-20 | 15 | 8.7% | |
| 21-30 | 7 | 4.1% | |
| 30+ | 3 | 1.7% | |
| Doctors in Emergency Medical Services have credited service years | Yes | 56 | 32.6 |
| No | 66 | 38.4 | |
| Undecided | 3 | 1.7 | |
| Doctors in Emergency Medical Services have paid night shifts? | Yes | 120 | 69.8 |
| No | 2 | 1.2 | |
| Undecided | 3 | 1.7 | |
| Doctors in Emergency Medical Services have paid work on Sundays? | Yes | 120 | 69.8 |
| No | 5 | 2.9 | |
| Medical technicians/nurses in Emergency Medical Services and ambulance transport have credited service years? | Yes | 57 | 33.1 |
| No | 66 | 38.4 | |
| Undecided | 2 | 1.2 | |
| Medical technicians/nurses in Emergency Medical Services and ambulance transport have paid night shifts? | Yes | 120 | 69.8 |
| No | 2 | 1.2 | |
| Medical technicians/nurses in Emergency Medical Services and ambulance transport have paid work on Sundays | Yes | 120 | 69.8 |
| No | 5 | 2.9 |
Table 15.
Availability of Medical Equipment and Emergency Personnel in EMS.
| Variables | Category | n | % |
|---|---|---|---|
| Ambulance Vehicles by Year of Manufacture | 1989-2000 | 11 | 6.4% |
| 2001-2005 | 19 | 11.0% | |
| 2006-2010 | 21 | 12.2% | |
| 2011-2015 | 32 | 18.6% | |
| 2016-2018 | 20 | 11.6% | |
| Medical Vehicles - number of kilometers traveled | 0 - 57,200 | 21 | 20.2 |
| 57,200 - 125,354 | 19 | 18.3 | |
| 125,354 - 285,564 | 20 | 19.2 | |
| 285,564 - 400,000 | 21 | 20.2 | |
| 400,000 - 1,000,000 | 23 | 22.1 | |
| Presence of radio stations in medical vehicles | Yes | 38 | 22.0 |
| No | 70 | 40.7 | |
| Functionality of EKG machines for activities within the healthcare service | Does not exist | 2 | 1.2 |
| Exists | 122 | 70.9 | |
| Biphasic defibrillators with monitors for activities within the healthcare service | Does not exist | 13 | 7.6 |
| Exists | 110 | 64.0 | |
| Functionality of portable aspirators for activities within the healthcare service | Does not exist | 17 | 9.9 |
| Exists | 106 | 61.6 | |
| Portable Mechanical Respirator with Oxygen Tank Functionality in HMP Activities | Does not exist | 59 | 34.3 |
| Exists | 64 | 37.2 | |
| Functionality of portable mechanical respirators with oxygen tanks that have the CPAP mode | Does not exist | 104 | 60.5 |
| Exists | 19 | 11.0 | |
| Availability of cardiopulmonary resuscitation sets | Does not exist | 17 | 9.9 |
| Exists | 106 | 61.6 | |
| Availability of 10-liter oxygen bottles for activities within the healthcare service | Does not exist | 5 | 2.9 |
| Exists | 118 | 68.6 | |
| Vacuum mattresses for activities within the healthcare service | Does not exist | 66 | 38.4 |
| Exists | 57 | 33.1 | |
| Cervical collars for spinal immobilization | Does not exist | 15 | 8.7 |
| Exists | 108 | 62.8 | |
| Kramer splints for activities within the healthcare service | Does not exist | 39 | 22.7 |
| Exists | 84 | 48.8 | |
| Infusion Solution Heater Functionality in HMP Activities | Does not exist | 122 | 70.9 |
| Exists | 1 | 0.6 | |
| Medications for thrombolytic therapy | Does not exist | 115 | 66.9 |
| Exists | 8 | 4.7 | |
| Emergency cricothyrotomy kits | Does not exist | 108 | 62.8 |
| Exists | 15 | 8.7 | |
| Availability of childbirth kits | Does not exist | 38 | 22.1 |
| Exists | 85 | 49.4 | |
| Protective Helmets with Lamps Availability in HMP Activities | Does not exist | 122 | 70.9 |
| Exists | 1 | 0.6 | |
| Fixed Radio Station Availability in Ambulance | Does not exist | 80 | 46.5 |
| Exists | 43 | 25.0 | |
| Handheld Radio Availability | Does not exist | 107 | 62.2 |
| Exists | 16 | 9.3 | |
| Ultrasound Device Availability | Does not exist | 112 | 65.1 |
| Exists | 11 | 6.4 |
Table 16.
Strategic Recommendations for Enhancing Emergency Medical Services: Addressing Structural, Resource, and Operational Challenges.
Table 16.
Strategic Recommendations for Enhancing Emergency Medical Services: Addressing Structural, Resource, and Operational Challenges.
| Aspect | Recommendations | Term | Feasibility | Cost | Priority |
|---|---|---|---|---|---|
| Organizational Structure and Risk Management | Standardize risk assessments across all EMS units. | Short | High | Low | High |
| Introduce dynamic updating protocols for emergency response strategies. | Short | High | Medium | High | |
| Establish a centralized authority for EMS management. | Long | Medium | Medium | High | |
| Integrate new technology platforms for real-time risk management. | Long | Low | High | High | |
| Develop inter-agency agreements for risk management best practices. | Long | Medium | Medium | Medium | |
| Resource Allocation and Efficacy | Conduct targeted resource audits in high-demand locations. | Short | High | Low | High |
| Deploy mobile resource units in underserved areas. | Short | Medium | High | High | |
| Establish a fund for state-of-the-art EMS equipment. | Long | Medium | High | Medium | |
| Develop partnerships with technology providers. | Long | Low | High | Medium | |
| Implement a resource sharing protocol among EMS agencies. | Long | High | Low | Low | |
| Communication Systems and Efficacy | Upgrade to digital radio systems and secure networks. | Short | High | Medium | High |
| Establish regional communication centers. | Short | Medium | High | High | |
| Create redundant communication channels. | Long | Medium | High | High | |
| Launch training programs for communication technologies. | Long | Medium | Medium | Medium | |
| Invest in AI-driven communication tools. | Long | Low | High | Medium | |
| Emergency Response Times and Efficacy | Enhance GPS and dispatch technologies. | Short | High | Medium | High |
| Develop rapid deployment strategies. | Short | Medium | High | High | |
| Invest in infrastructure improvements at EMS stations. | Long | Medium | High | High | |
| Expand the network of emergency medical facilities. | Long | Low | High | Medium | |
| Implement performance tracking for response times. | Long | High | Medium | Medium | |
| Training and Preparedness for Disaster Response | Increase frequency and complexity of disaster response simulations. | Short | High | Medium | High |
| Develop specialized units for specific disaster scenarios. | Short | High | Medium | High | |
| Collaborate with international disaster response agencies. | Long | Medium | High | Medium | |
| Create a digital training hub for disaster response. | Long | Medium | Medium | High | |
| Mandate disaster preparedness certifications. | Long | High | Medium | High | |
| Financial Resources and Administrative Efficacy | Optimize financial planning for high-priority needs. | Short | High | Low | High |
| Streamline administrative processes to reduce overhead. | Short | High | Low | High | |
| Develop strategic financial partnerships. | Long | Medium | Low | Medium | |
| Use big data analytics for predictive funding needs. | Long | Medium | Medium | Low | |
| Lobby for increased governmental and international funding. | Long | Low | Low | High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



