
Submitted:
21 August 2024
Posted:
22 August 2024
You are already at the latest version
Abstract
Background: The Advanced Lung Cancer Inflammation Index (ALI) is a novel, comprehensive index that integrates inflammation and nutritional status, incorporating parameters such as albumin, body mass index (BMI), and the neutrophil-to-lymphocyte ratio (NLR). Unlike traditional inflammation biomarkers, this study aims to evaluate the prognosis of IPF patients by considering both inflammation and nutritional status. Method: A total of 102 patients with IPF were included in the study. Clinical data were obtained from the patients’ medical records. NLR and ALI score were calculated based on data collected at the initiation of antifibrotic treatment using the following formula: Neut/Lym and albumin × BMI / NLR. Results: IPF subject subgroups in terms of ALI based on gender–age–physiology (GAP) stages (1,2,3), FVC (median split, <70% vs ≥70%), DLCO (<51% vs ≥51%), 6-Minute Walk Test (6MWT) (<350 vs ≥350) and CCI (≤1 vs >1). ALI showed significant difference depending on the categories of GAP stage, FVC, DLCO, and 6MWT but these differences were not observed based on the charlson comorbidity index (CCI) categories (sırasıyla p=0.000, p=0.000, p=0.000, p=0.001, p=0.233). Receiver Operating Characteristic (ROC) curve analysis was performed to evaluate the sensitivity and specificity of ALI, albumin, NLR, and BMI in determining the mortality risk in IPF patients. ALI demonstrated a sensitivity of 63.6% and a specificity of 98.9% at a threshold of 11.2 (AUC = 0.945, 95% CI 0.892–0.998, p < 0.000). Conclusion: We determined that ALI levels are significantly associated with disease severity and mortality in patients with IPF.
Keywords:
idiopathic pulmonary fibrosis
; advanced lung cancer inflammation index
; albümin
; body mass index
; neutrophil‐to‐lymphocyte ratio
Background
Idiopathic Pulmonary Fibrosis (IPF) is a chronic and progressive lung disease characterized by irreversible deterioration of lung function and a short median survival time. It is associated with an age-standardized mortality rate ranging from 0.5 to 12 deaths per 100,000 individuals [1].
IPF is unpredictable. While some cases exhibit a rapid decline, others progress more slowly. Additionally, some cases may experience exacerbations, leading to shorter survival times. Various lung function parameters have been proposed to distinguish between patients with different prognoses. Furthermore, there are scores that incorporate clinical, functional, radiological, and hematological data [2,3,4]. In recent years, there has been increasing interest in blood cell-derived inflammation indices. Although it remains unclear whether inflammation is a cause or a consequence of the fibrotic process, recent studies have indicated that inflammation plays a role in several stages of IPF pathogenesis [5].
Body mass index (BMI) and weight change are important features of nutritional status. BMI has also been recognized as a clinical indicator for assessing malnutrition in IPF, although its significance in IPF patients has not been fully established [6]. Previous studies have suggested that low BMI and weight loss are predictive of rapid decline in lung function [7]. The Advanced Lung Cancer Inflammation Index (ALI) is a novel, comprehensive index that integrates inflammation and nutritional status, incorporating parameters such as albumin, BMI, and the neutrophil-to-lymphocyte ratio (NLR). Initially used to assess prognosis in cancer patients, ALI has gained attention for its ability to simultaneously evaluate both inflammation and nutritional status, and its role in inflammation-related conditions such as heart failure, coronary artery disease, hypertension, and diabetes [8]. These studies have demonstrated that a decreased ALI value (i.e., low BMI and albumin, high NLR) indicates poorer nutritional status and more severe inflammatory response in patients [9,10]. Consequently, inflammation may influence the prognosis of IPF patients not only directly but also indirectly through albumin and BMI. Therefore, relying solely on inflammation markers may not be sufficient to assess the prognosis of IPF patients, and there is an urgent need for new predictive indicators for a comprehensive evaluation. To date, no study has validated the prognostic value of ALI in IPF patients. In this study, we aimed to evaluate the prognostic impact of ALI and hypothesized that it could be useful in predicting mortality.
Materials and Methods
A retrospective review of medical records was conducted for 123 patients diagnosed with IPF at Antalya Training and Research Hospital between June 2020 and July 2024. IPF diagnosis was based on the identification of the usual interstitial pneumonia (UIP) pattern or possible UIP pattern using high-resolution computed tomography (HRCT), in accordance with the 2022 international consensus guidelines that exclude other interstitial lung diseases or overlapping conditions [11]. All patients were over 18 years old, and clinical findings, hemogram results, and albumin levels were available within 24 hours of hospital admission. Exclusion criteria were: 1) missing data; 2) severe, life-threatening disease in another system unrelated to IPF; and 3) confirmed lung cancer prior to admission. Based on these criteria, a total of 21 patients were excluded. Ultimately, 102 patients were included in the final analysis.
Clinical data were obtained from the patients’ medical records. Laboratory findings and results of pulmonary function tests (PFTs) were recorded with timestamps from the initiation of antifibrotic treatment. The Gender-Age-Physiology (GAP) score for diagnosis and the Charlson Comorbidity Index (CCI), used to classify comorbid conditions that might affect mortality risk, were calculated as previously described [12,13]. The date of diagnosis for each patient was designated as the date of the PFT. The observation period was calculated from the start date of antifibrotic treatment to the date of the last visit. The follow-up period ended in July 2024. Survival time was defined as the duration from the PFT date to the date of death or, if the patient was still alive at that time, to July 2024. When the final status could not be obtained from records, phone calls were made to determine survival status. NLR and ALI scores were calculated based on data from the initiation of antifibrotic treatment using the following formulae: Neut/Lym and albumin × BMI / NLR. When peripheral leukocytes were assessed, no patients were experiencing active infections.
This study was approved by the Antalya Training and Research Hospital Human Research Ethics Committee on 13/06/2024 under decision no: 9/16. Since it was a retrospective study, the requirement for informed consent was waived. The study was conducted in accordance with institutional and/or national research committee ethical standards, as well as the Declaration of Helsinki and its subsequent amendments or similar ethical standards.
Statistical Analysis
Statistical analysis of the study data was performed using SPSS version 23.0. The normality of variable distributions was assessed using visual (histograms and probability plots) and analytical methods (Kolmogorov-Smirnov/Shapiro-Wilk tests). Descriptive statistics for normally distributed variables are reported as mean and standard deviation, while median and interquartile range (IQR) values are provided for non-normally distributed variables. Differences between groups were evaluated using t-tests/Mann-Whitney U tests and ANOVA/Kruskal-Wallis H tests, as appropriate. For categorical variables, frequencies and percentages are reported, and differences between groups were assessed using the Chi-square test. Pearson/Spearman correlation analyses were conducted to evaluate relationships between variables. The predictive performance of ALI and NLR levels for mortality was analyzed using Receiver Operating Characteristic (ROC) curves. Sensitivity and specificity values for significant cutoff points were calculated. Statistical significance was considered for p-values less than 0.05, with a Type I error rate below 5% deemed statistically significant.
Results
Baseline Characteristics of the Study Population
The demographic and clinical characteristics of the 102 IPF patients are summarized in Table 1. The average age of the study cohort at diagnosis was 70.4 ± 7.39 years, with an average BMI of 24.1 ± 1.79 kg/m². The cohort comprised 78.4% male participants, and the majority were former smokers (71.6%). When categorized by GAP stages, 44 patients (43.1%) were in GAP stage 1, 32 patients (31.4%) were in GAP stage 2, and 26 patients (25.5%) were in GAP stage 3. The mean observation period was 33.4 ± 8.61 months, during which 11 patients (10.8%) died. Additionally, 15 patients (14.7%) experienced acute exacerbations of IPF (Table 1).
We also compared IPF subject subgroups in terms of ALI based on GAP stages (1,2,3), with Forced Vital Capacity (FVC) (median split, <70% vs ≥70%), Diffusing Capacity for Carbon Monoxide (DLCO) (<51% vs ≥51%), 6-Minute Walk Test (6MWT) (<350 vs ≥350) and CCI (≤1 vs >1). ALI showed significant difference depending on the categories of GAP stage, FVC, DLCO, and 6MWT but these differences were not observed based on the CCI categories (sırasıyla p=0.000, p=0.000, p=0.000, p=0.001, p=0.233) (Table 2). Additionally, significant differences in NLR, BMI, and albumin levels were observed when individuals were grouped according to GAP stages (sırasıyla p=0.000, p=0.000, p=0.000). These significant differences were also observed when IPF patients were categorized into three groups based on their ALI levels (Quantile1 group (< 21,2), Quantile 2 group (21,3-31,4) and Quantile 3 group (>31,5). There were significant differences in albümin, BMI and NLR values between the subjects in Quantile1 groups and Quantile 2 groups (p=0.000), Quantile1 groups and Quantile3 groups (p=0.000), Quantile 2 groups and Quantile 3 groups (sırasıyla p=0.000, p=0.000, p=0.000) (Table 2).
Association Between ALI/GAP/NLR/BMI/FVC/DLCO/6MWT and Albumin
Pearson correlation analysis revealed that the ALI was significantly negatively correlated with the GAP stage (r = -0.815, p = 0.000) and significantly positively correlated FVC, DLCO, and the 6MWT (r = 0.498, p = 0.000; r = 0.637, p = 0.000; r = 0.445, p = 0.000, respectively). Albumin and BMI also showed correlations with the GAP stage and lung function parameters similar to those of ALI. Specifically, as the GAP stage increased, ALI, BMI, and albumin values decreased, while FVC, DLCO, and 6MWT decreased in parallel. NLR was found to be significantly positively correlated with the GAP stage (r = 0.638, p = 0.000) and significantly negatively correlated with FVC and DLCO (r = -0.348, p = 0.000; r = -0.525, p = 0.000, respectively) (Table 3).
Survival Curve Based on Predictors of IPF Mortality
Receiver Operating Characteristic (ROC) curve analysis was performed to evaluate the sensitivity and specificity of ALI, albumin, NLR, and BMI in determining the mortality risk in IPF patients (Table 4). All Area Under the Curve (AUC) values were found to be significant. ALI demonstrated a sensitivity of 63.6% and a specificity of 98.9% at a threshold of 11.2 (AUC = 0.945, 95% CI 0.892–0.998, p < 0.000) (Figure 1).
Discussion
To the best of our knowledge, this retrospective study is the first to evaluate the ALI in patients with IPF undergoing antifibrotic treatment, integrating both inflammation and nutritional status. ALI levels showed statistically significant differences when patients were grouped according to their GAP stages and functional parameters. Additionally, a key finding is that ALI, along with albumin, NLR, and BMI, has been identified as predictors of IPF mortality in this cohort.
It is widely accepted that the fibrogenesis in IPF results from an abnormal healing process due to continuous micro-injuries to alveolar epithelial cells. Excessive healing and tissue remodeling lead to chronic inflammation and ultimately fibrosis. Inflammation may play a role in the pathogenesis and progression of pulmonary fibrosis. However, recent data suggest that the pathophysiology of IPF may be more a result of fibroblast dysfunction rather than persistent inflammation. Consequently, it has been proposed that inflammation could be an epiphenomenon rather than a key driver in IPF [14].
ALI includes the NLR as a marker of inflammation. Neutrophils are complex cells activated by the immune response and possess the capacity to perform numerous specialized functions. Excessively activated neutrophils can contribute to chronic inflammation and promote the expansion of both innate and adaptive immune responses [15]. It has been shown that all stages of fibrosis in IPF are associated with both innate and adaptive responses [16]. Previous studies have indicated that high neutrophil counts signal non-specific inflammation, while decreased lymphocyte levels reflect weakened immunity. Therefore, NLR represents an individual’s immunological status and inflammatory response [17]. In our study, the mean NLR level in IPF cases was 3.3, which is higher than the average levels found in healthy individuals (1.65–2.11) [18,19]. However, different NLR values have been reported in the literature using various methods across different populations (neoplastic or non-neoplastic). Currently, there is no universal value available.
In a study evaluating combined blood cell count indices, including NLR, it was demonstrated that NLR is a reliable index of systemic inflammation in IPF cases and is significantly associated with functional lung parameters [20]. Another study assessing NLR in bronchoalveolar lavage (BAL) samples isolated from IPF patients found that NLR showed a negative correlation with FVC and FEV1 and was associated with the composite physiological index measured at the time of BAL sample collection [21]. In studies examining the relationship between NLR and clinical outcomes in IPF patients, a poor prognosis has been observed in those with high NLR. Similarly, in our study, we observed a significant negative correlation between NLR and FVC and DLCO. These results are consistent with previous studies indicating that NLR can predict the prognosis of various chronic inflammatory diseases [22,23,24,25].
The GAP model, which integrates the effects of age, sex, FVC, and DLCO, is the most commonly used prognostic model in IPF and other chronic interstitial lung diseases [12]. Studies have been conducted that incorporate peripheral leukocyte analyses into the GAP model to predict mortality risk. In one such study, it was reported that a median NLR ≥ 2.9 was associated with increased mortality in IPF patients, and the combined assessment of GAP and NLR classified mortality risk [26]. In another study, a risk scoring system associated with inflammation was developed by incorporating the CCI and monocytes into the GAP model for IPF patients. This study demonstrated that patients with lower FVC, lower DLCO, comorbidities, and higher monocyte levels had the poorest survival outcomes [27]. In another study, high NLR was found to be associated with an increased risk of mortality in patients with progressive fibrotic interstitial lung diseases undergoing antifibrotic treatment. Although subgroup analyses in this study indicated that NLR may not be suitable for advanced disease stages and non-IPF patients, the combined assessment of the GAP index and NLR successfully classified mortality risk both at the initiation of antifibrotic therapy and during long-term follow-up [28]. In our study, the GAP model and CCI were not assessed in combination with ALI. However, when categorizing cases according to GAP stages, we found statistically significant differences in NLR and ALI values. Specifically, there was a significant negative correlation between GAP stage and ALI, and a significant positive correlation between GAP stage and NLR. This indicates that as the GAP stage increased, NLR levels rose and ALI values decreased. However, we did not observe this significant difference when categorizing based on CCI.
Studies evaluating the relationship between NLR and mortality in patients with IPF and idiopathic pleuropulmonary fibroelastosis have shown that NLR levels did not significantly change one year after the initiation of treatment. Patients who continued to have high NLR levels were at a higher risk of mortality compared to others. These findings support the pathological effects of NLR on the progression of pulmonary fibrosis and suggest that NLR may indicate disease severity regardless of the timing of assessment [29,30]. In our study cohort, NLR and ALI were assessed at a single time point, and high NLR and low ALI were associated with shorter overall survival. ROC analysis showed that the AUROC value for NLR in predicting overall survival was 0.768, while ALI had an AUROC value of 0.945. These results indicate that both NLR and ALI could be potential prognostic biomarkers for overall survival in IPF patients.
Another parameter included in ALI is albumin, which can be affected by inflammation and malnutrition, leading to decreased albumin levels and weight loss. Albumin is a sensitive nutritional marker. A study conducted in IPF cases has demonstrated that lower albumin levels are associated with shorter survival times in patients [31]. Similarly, in our study, when grouping ALI values by percentiles, we observed that albumin levels were also low in the Quantile 1 (low ALI) group, and there was a significant positive correlation between ALI and albumin. ROC analysis indicated that the AUROC value for albumin in predicting mortality was 0.952. Therefore, we suggest that there is a consistent trend between albumin levels and mortality risk in IPF patients, with a decrease in albumin being associated with a concurrent increase in mortality risk.
Malnutrition is closely associated with the progression of conditions such as sarcopenia and cachexia, which are commonly observed in patients with advanced lung disease [32,33]. Recent studies have shown that malnutrition and reduced food intake increase the risk of hospitalization and mortality in IPF patients, suggesting that nutritional status may have a negative impact on the prognosis of IPF [34]. BMI is another indicator commonly used to assess nutritional status and is included in ALI. Independent of antifibrotic drug use, it may potentially serve as an indicator for predicting mortality, disease progression, and hospitalization risk in IPF patients [35]. The second analysis of the placebo group in the INPULSIS study showed that the rate of decline in FVC was numerically greater in patients with a BMI < 25 kg/m² compared to those with a BMI ≥ 25 kg/m², and in those who experienced more than 5% weight loss compared to those with less than 5% weight loss. This suggests that low BMI and weight loss in patients may be important clinical indicators of poor prognosis in IPF [7]. In a study evaluating the risk associated with malnutrition in IPF patients using serum albumin, body weight, and ideal body weight, it was reported that this risk is an independent poor prognostic factor regardless of age, sex, FVC, or GAP index. The study demonstrated that patients with malnutrition-related risk had significantly shorter survival times compared to those without this risk, both in separate and combined cohorts [36]. In our study cohort, we observed that individuals with low BMI had lower ALI values, and there was a significant positive correlation between them. ROC analysis results indicated that the AUROC value for BMI in predicting overall survival was 0.885, suggesting that low BMI, similar to ALI, could be predictive of mortality risk in IPF patients. These observations imply that, independent of sex, age, or lung physiology, nutritional status is critically important for the progression and outcomes of IPF patients. These findings suggest that ALI assessments could be a valuable tool for evaluating disease severity, prognosis, and mortality.
Unlike traditional inflammation biomarkers, the ALI examined in this study is an innovative inflammation biomarker that considers both inflammation and nutritional status. To date, no studies have evaluated the relationship between ALI and prognosis and mortality in patients with IPF. Our research identified a significant association between ALI levels and disease severity and mortality in IPF patients. Disease severity classification is typically based on physiological parameters, primarily FVC and/or DLCO, at baseline and/or their temporal changes. However, physiological assessments have some limitations; for example, they may be influenced by patient effort, can be challenging to complete in critically ill patients, and may fail to predict mortality accurately. Routine peripheral blood parameters can overcome these disadvantages and are readily accessible. In this study, we demonstrated the prognostic utility of ALI, a simple and routinely derived biomarker. Consequently, we argue that evaluating both inflammation and nutritional status simultaneously is essential for accurately and comprehensively assessing the prognosis of IPF patients.
However, the present study has several limitations. Specifically, the relatively small sample size and the single-center nature of the study restrict the generalizability of the findings, especially given the low prevalence of the disease. Additionally, the cross-sectional design did not allow for establishing a definitive cause-and-effect relationship between the examined indices and the presence of IPF or pulmonary function parameters. Future research will require larger sample sizes and prospective designs to clarify causality. Furthermore, despite using various statistical methods to reduce bias, it may not be possible to completely eliminate unknown confounding factors. This study is a retrospective observational study and thus may be subject to some selection bias and missing data. It assessed a group of patients who did not have serious, life-threatening conditions in other systems, liver and kidney dysfunction, infections, or confirmed lung cancer prior to admission, rather than including all IPF patients. The data collected were limited to those who presented to the hospital, and most subjects had only basic data available. The BMI reference value used to calculate ALI varies by race and country. While the average BMI in Western countries is approximately 26-28 kg/m², in Asian countries it is around 23-24 kg/m². Therefore, ALI may not be directly applicable across all races and countries. Our data indicated that patients with low ALI levels had shorter survival times; however, the sample size was too small to perform stratified analyses.
In summary, prognosis assessment is crucial for patient counseling, disease management, and referral for lung transplantation. Our research identifies, for the first time, a significant association between an increase in ALI and a notable reduction in mortality risk among IPF patients. These findings underscore the importance of managing ALI within an appropriate range for the long-term survival of IPF patients (e.g., weight management, maintaining albumin within normal ranges, and antifibrotic treatments). Dynamic changes in ALI may assist clinicians in establishing personalized ALI standards, which could help optimize the long-term survival of IPF patients.
Author Contributions
F.B. and O.K. contributed to the conceptual design and planning of the study, data collection, and its interpretation. F.B. and O.K. performed the statistical analyses. The main manuscript was drafted by F.B. All authors reviewed and approved the final version of the manuscript, taking full responsibility for the integrity of the reported data and their analysis. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
This study was conducted in accordance with the guidelines of the Declaration of Helsinki and was approved by the Institutional Review Board of Antalya Training and Research Hospital in Antalya, Turkey (Decision No: 9/16, dated 13/06/2024).
Conflicts of Interest
The authors declare no conflict of interest
References
- Zheng, Q.; Cox, I.A.; Campbell, J.A.; Xia, Q.; Otahal, P.; Graaff, B.; Corte, T.J.; Teoh, A.K.; Walters, E.H.; Palmer, A.J. Mortality and survival in idiopathic pulmonary fibrosis: a systematic review and meta-analysis. ERJ Open Res. 2022, 14, 8, 00591-2021. [CrossRef]
- Nathan, S.D; Reffett, T.; Brown, A.W.; Fischer, C.P.; Shlobin, O.A.; Ahmad, S.; Weir, N.; Sheridan, M.J. The Red Cell Distribution Width as a Prognostic Indicator in Idiopathic Pulmonary Fibrosis. Chest 2013, 143, 1692–1698. [CrossRef] [PubMed]
- Wells, A.U.; Desai, S.R.; Rubens, M.B.; Goh, N.S.; Cramer, D.; Nicholson, A.G.; Colby, T.V.; du Bois, R.M.; Hansell, D.M. Idiopathic pulmonary fibrosis: A composite physiologic index derived from disease extent observed by computed tomography. Am. J. Respir. Crit. Care Med. 2003, 167, 962–969. [CrossRef] [PubMed]
- Collard, H.R.; King, T.E., Jr.; Bartelson, B.B.; Vourlekis, J.S.; Schwarz, M.I.; Brown, K.K. Changes in clinical and physiologic variables predict survival in idiopathic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 2003, 168, 538–542. [CrossRef]
- Desai, O.; Winkler, J.; Minasyan, M.; Herzog, E.L. The Role of Immune and Inflammatory Cells in Idiopathic Pulmonary Fibrosis. Front. Med. 2018, 5, 43. [CrossRef]
- Jouneau, S.; Kerjouan, M.; Rousseau, C.; Lederlin, M.; Llamas-Guttierez, F.; De.; Latour, B.; Guillot, S.; Vernhet, L.; Desrues, B; Thibault, R. What are the best indicators to assess malnutrition in idiopathic pulmonary fibrosis patients? A cross-sectional study in a referral center. Nutrition 2019, 62, 115–121. [CrossRef]
- Jouneau, S.; Crestani, B.; Thibault, R.; Lederlin, M.; Vernhet, L.; Valenzuela, C.; Wijsenbeek, M.; Kreuter, M.; Stansen, W.; Quaresma, M,; et. al. Analysis of body mass index, weight loss and progression of idiopathic pulmonary fibrosis. Respir. Res. 2020, 21, 312. [CrossRef]
- Chen, X.; Hong, C.; Guo, Z.; Huang, H.; Ye, L. Association between advanced lung cancer inflammation index and all-cause and cardiovascular mortality among stroke patients: NHANES, 1999–2018. Front. Public Health 2024, 12, 1370322. [CrossRef]
- Maeda, D.; Kanzaki, Y.; Sakane, K.; Ito, T.; Sohmiya, K.; Hoshiga, M. Prognostic impact of a novel index of nutrition and inflammation for patients with acute decompensated heart failure. Heart Vessels 2020, 35, 1201–8. [CrossRef]
- Yuan, X.; Huang, B.; Wang, R.; Tie, H.; Luo, S. The prognostic value of advanced lung cancer inflammation index (ALI) in elderly patients with heart failure. Front. Cardiovasc. Med. 2022, 9, 934551. [CrossRef]
- Raghu, G.; Remy-Jardin, M,; Richeldi, L.; Thomson, C.C.; Inoue, Y.; Johkoh, T.; Kreuter, M.; Lynch, D.A.; Maher, T.M.; Martinez, F.J.; et. al. Idiopathic Pulmonary Fibrosis (an Update) and Progressive Pulmonary Fibrosis in Adults: An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline Am. J. Respir. Crit. Care Med. 2022, 205, 18-47. [CrossRef]
- Ley, B.; Ryerson, C.J.; Vittinghoff, E.; Ryu, J.H.; Tomassetti, S.; Lee, J.S.; Poletti, V,; Buccioli, M.; Elicker, B.M.; Jones, K.D.; et. al. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann. Intern. Med. 2012, 156, 684–9. [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic. Dis. 1987, 40, 373-83. [CrossRef] [PubMed]
- Wuyts, W.A.; Agostini, C.; Antoniou, K.M.; Bouros, D.; Chambers, R.C.; Cottin, V.; Egan, J.J.; Lambrecht, B.N.; Lories, R.; Parfrey, H.; Prasse A.; et. al. The pathogenesis of pulmonary fibrosis: a moving target. Eur. Respir. J. 2013, 41, 1207–18. [CrossRef]
- Mantovani, A.; Cassatella, M.A.; Costantini, C.; Jaillon, S. Neutrophils in the activation and regulation of innate and adaptive immunity. Nat. Rev. Immunol. 2011, 11, 519–31. [CrossRef]
- Wynn, T.A. Integrating mechanisms of pulmonary fibrosis. J. Exp. Med. 2011, 208, 1339–50. [CrossRef] [PubMed]
- Adane, T.; Melku, M.; Worku, Y.B.; Fasil, A., Aynalem, M.; Kelem, A.; Geteva, S. The association between neutrophil-to-lymphocyte ratio and Glycemic control in type 2 diabetes mellitus: a systematic review and meta-analysis. J. Diabetes Res. 2023, 2023, 1-11. [CrossRef]
- Azab, B.; Camacho-Rivera, M.; Taioli, E. Average values and racial differences of neutrophil lymphocyte ratio among a nationally representative sample of United States subjects. PLoS One. 2014, 9, e112361. [CrossRef] [PubMed]
- Lee, J.S.; Kim, N.Y.; Na, S.H.; Youn, Y.H.; Shin, C.S. Reference values of neutrophil lymphocyte ratio, lymphocyte-monocyte ratio, platelet-lymphocyte ratio, and mean platelet volume in healthy adults in South Korea. Medicine 2018, 97, e11138. [CrossRef] [PubMed]
- Zinellu, A.; Paliogiannis, P.; Sotgiu, E.; Mellino, S.; Mangoni, A.A.; Zinellu, E.; Negri, S.; Collu, C.; Pintus, G.; Serra, A.; et .al. Blood Cell Count Derived Inflammation Indexes in Patients With Idiopathic Pulmonary Fibrosis. Lung 2020, 198, 821–827. [CrossRef]
- D’Alessandro, M.; Bergantini, L.; Carleo, A.; Cameli, P.; Perrone, A.; Fossi, A.; Sestini, P.; Bargagli, B. Neutrophil-To-Lymphocyte Ratio in Bronchoalveolar Lavage From IPF Patients: A Novel Prognostic Biomarker? Minerva Med. 2022, 113, 526-531. [CrossRef]
- Paliogiannis, P.; Satta, R.; Deligia, G.; Farina, G.; Bassu, S.; Mangoni, A.A.; Carru, C.; Zinellu, A. Associations between the neutrophil-to-lymphocyte and the platelet-to-lymphocyte ratios and the presence and severity of psoriasis: a systematic review and meta-analysis. Clin. Exp. Med. 2019, 19, 37–45. [CrossRef]
- Paliogiannis, P.; Fois, A.G.; Sotgia, S.; Mangoni, A.A.; Zinellu, E.; Pirina, P.; Carru, C.; Zinellu, A. The neutrophil-to-lymphocyte ratio as a marker of chronic obstructive pulmonary disease and its exacerbations: a systematic review and meta-analysis. Eur. J. Clin. Invest. 2018, 48, e12984. [CrossRef] [PubMed]
- Paliogiannis, P.; Fois, A.G.; Sotgia, S.; Mangoni, A.A.; Zinellu, E.; Pirina, P.; Negri, S.; Carru, C.; Zinellu, A. Neutrophil to lymphocyte ratio and clinical outcomes in COPD: recent evidence and future perspectives. Eur. Respir. Rev. 2018, 27, 170113. [CrossRef]
- Mochimaru, T.; Ueda, S.; Suzuki, Y.; Asano, K.; Fukunaga, K. Neutrophil-to-lymphocyte ratio as a novel independent predictor of severe exacerbation in patients with asthma. Ann. Allergy Asthma Immunol. 2019, 122, 337–339. [CrossRef]
- Mikolasch, T.A.; George, P.M.; Sahota, J.; Nancarrow, T.; Barratt, S.L.; Woodhead, F.A.; Kouranos, V.; Cope, V.S.A.; Creamer, A.W.; Fidan S.; et. al. Multi-center evaluation of baseline neutrophil-to-lymphocyte (NLR) ratio as an independent predictor of mortality and clinical risk stratifier in idiopathic pulmonary fibrosis. EClinicalMedicine 2023, 55, 101758. [CrossRef]
- Zhang, X.; Ren, Y.; Xie, B.; Ye, O.; Ban, C.; Zhang, S.; Zhu, M.; Liu, Y.; Wang, S.; Geng, J.; et. al. Blood monocyte counts as a prognostic biomarker andpredictor in Chinese patients with idiopathic pulmonary fibrosis. Front. Med. 2022, 9, 955125. [CrossRef] [PubMed]
- Takuma, S.; Suzuki, Y.; Kono, M.; Hasegawa, H.; Hashimoto, D.; Yokomura, K.; Mori, K.; Shimizu, M.; Inoue, Y.; Yasui, H.; et.al. Neutrophil-lymphocyte ratio being associated with mortality risk in patients receiving antifibrotic therapy. Respir. Med. 2024, 223, 107542. [CrossRef]
- Achaiah, A.; Rathnapala, A.; Pereira, A.; Bothwell, H.; Dwivedi, K.; Barker, R.; Iotchkova, V.; Benamore, R.; Hoyles, R.K.; Ho, L.P. Neutrophil lymphocyte ratio as an indicator for disease progression in Idiopathic Pulmonary Fibrosis. BMJ Open Respir. Res. 2022, 9, e001202. [CrossRef]
- Suzuki, Y.; Kono, M.; Hasegawa, H.; Hashimoto, D.; Yokomura, K.; Imokawa, S.; Inoue, Y.; Hozumi, H.; Karayama, M.; Furuhashi, K.; et. al. Neutrophil-lymphocyte ratio in patients with idiopathic pleuroparenchymal fibroelastosis, BMJ Open Respir Res 2023, 10, e001763. [CrossRef]
- Li, B.; Zhang, X.; Xu, G.; Zhang, S.; Song, H.; Yang, K.; Dai, H.; Wang, C. Serum prealbumin is a prognostic indicator in idiopathic pulmonary fibrosis. Clin. Respir. J. 2019, 13, 493-8. [CrossRef] [PubMed]
- Suzuki, Y.; Mori, K.; Aono, Y.; Kono, M.; Hasegawa, H.; Yokomura, K.; Hozumi, H.; Karayama, M.; Furuhashi, K.; Enomoto, N.; et. al. Cause of mortality and sarcopenia in patients with idiopathic pulmonary fibrosis receiving antifibrotic therapy. Respirology 2021, 26, 171–9. [CrossRef] [PubMed]
- Suzuki, Y.; Mori, K.; Aono, Y.; Kono, M.; Hasegawa, H.; Yokomura, K.; Naoi, H.; Hozumi, H.; Karayama, M.; Furuhashi, K.; et. al. Combined assessment of the GAP index and body mass index at antifibrotic therapy initiation for prognosis of idiopathic pulmonary fibrosis. Sci. Rep. 2021, 11, 18579. [CrossRef] [PubMed]
- Jouneau, S.; Rousseau, C.; Lederlin, M.; Lescoat, A.; Kerjouan, M.; Chauvin, P.; Luque-Paz, D.; Guillot, S.; Oger, E.; Vernhet, L.; et. al. Malnutrition and decreased food intake at diagnosis are associated with hospitalization and mortality of idiopathic pulmonary fibrosis patients. Clin. Nutr. 2022, 41, 1335–1342. [CrossRef]
- Jouneau, S.; Crestani, B.; Thibault, R.; Lederlin, M.; Vernhet, L.; Yang, M.; Morgenthien, E.; Kirchgaessler, K.; Cottin, V. Post hoc analysis of clinical outcomes in placebo- and Pirfenidone-treated patients with iPF stratified by BMi and weight loss. Respiration 2022, 101, 142–154. [CrossRef]
- Mochizuka, Y.; Suzuki, Y.; Kono, M.; Hasegawa, H.; Hashimoto, D.; Yokomura, K.; Inoue, Y.; Yasui, H.; Hozumi, H.; Karayama, M.; Furuhashi, K.; et. al. Respirology 2023, 28, 775–783. [CrossRef] [PubMed]
Figure 1.
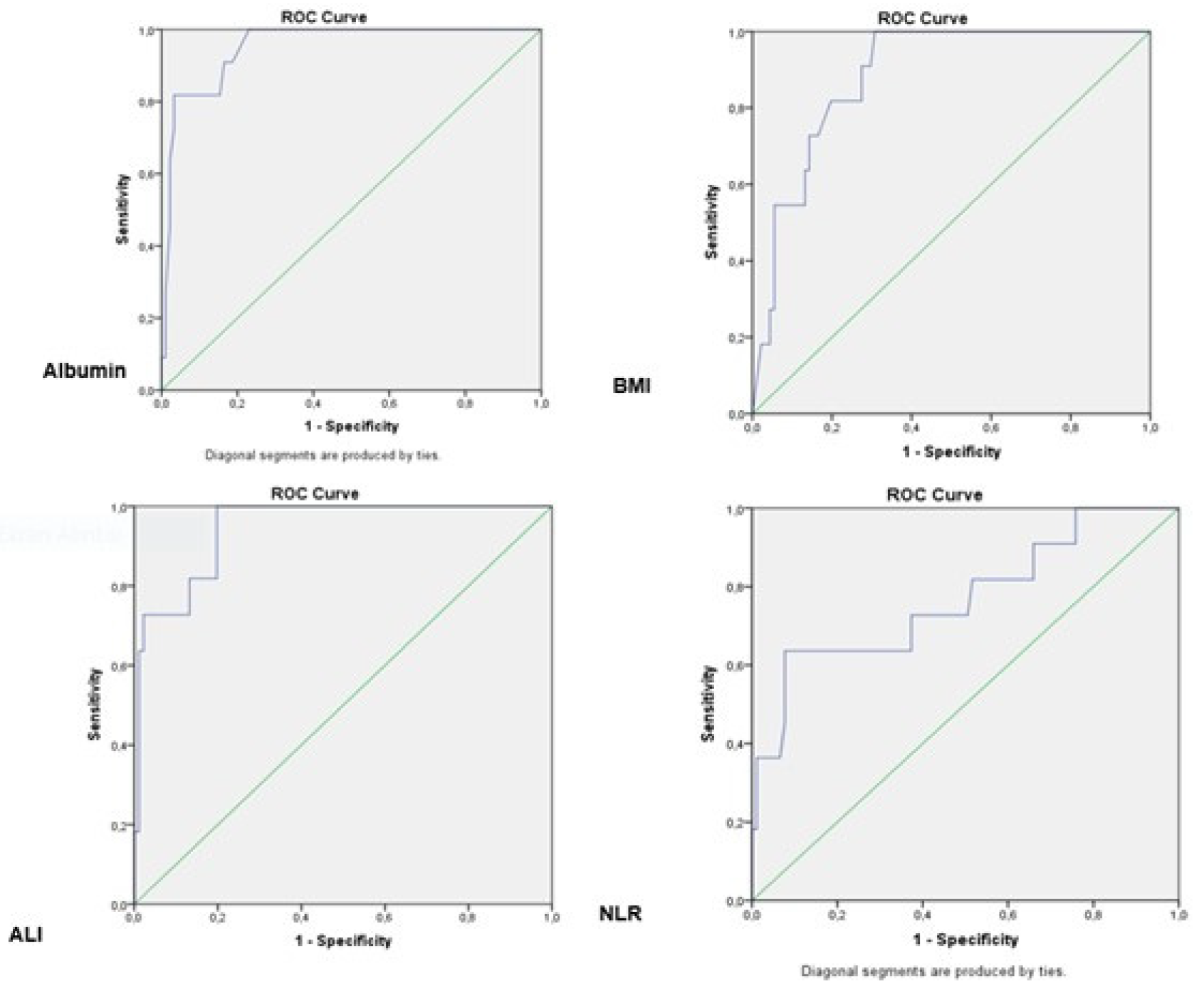

Table 1.
Characteristics of the study population.
| Subjects | |
|---|---|
| Gender, M/F(n/%) | 80 (78.4) /22 (21.6) |
| Age, years | 70.4±7.39 |
| Smokers, never/current/ex (n) | 13 (12.7)/ 16 (15.7)/ 73 (71.6) |
| BMI (kg/m2) | 24.1±1.79 |
| Disease duration (months) | 33.4±8.61 |
| AE (n,%) | 15 (14.7) |
| Charlson Comorbidity Index | 1.4±0.62 |
| GAP Stages | |
| I | 44 (43.1) |
| II | 32 (31.4) |
| III | 26 (25.5) |
| GAP index (1/2/3/4/5/6/7) | 2 (2.0)/12 (11.8)/30 (29.4)/16 (15.7)/16 (15.7)/19(18.6)/7(6.9) |
| Pulmonary function test | |
| FVC, %-pred | 70.2±7.54 |
| FEV1, %-pred | 74.7±7.43 |
| DLCO, % | 49.7±11.82 |
| 6MWT (meters) | 359.2±49.42 |
| Laboratory variables | |
| Neutrophils (10^9/L) | 5.50±1.26 |
| Lymphocytes (10^9/L) | 1.7 ±0.35 |
| Monocytes (10^9/L) | 1.7 ±0.35 |
| Albumin, g/dL | 3.5±0.69 |
| LDH, U/L | 212.9±65.90 |
| ALT (U/L) | 22.8±28.70 |
| AST (U/L) | 20.8±7.11 |
| NLR | 3.3±1.05 |
| ALI | 29.6±15.32 |
| Survivor/Nonsurvivor (n/%) | 91 (89.2)/ 11 (10.8) |
Data are expressed as mean ± standard deviation, median (interquartile range], or n (%). Abbreviations: BMI: body mass index, AE: acute exacerbation, GAP: gender, age and two lung physiology variables index, FVC :forced vital capacity, DLCO: diffusion capacity for carbon monoxide, 6MWT:six-minute walk test, AST:aspartate aminotransferase; ALT:alanine aminotransferase; LDH:lactate dehydrogenase NLR, neutrophil-lymphocyte ratio, ALI: advanced lung cancer inflammation index.
Table 2.
Comparison of the clinical parameters and blood cell count indexes of the groups.
| ALI | ||||
|---|---|---|---|---|
| n | Median (IQR) | p | ||
| GAP stages | 1 (0-3) | 44 | 38.5 (18.60)a |
0.000 |
| 2 (4-5) | 32 | 21.6 (7.35)b | ||
| 3 (6-8) | 26 | 17.5 (10.72)c | ||
| FVC(median split) | <70 | 44 | 21.1 (9,58) | 0.000 |
| ≥70 | 58 | 31,3 (20,05 | ||
| DLCO | <51 | 49 | 20.3 (10.75) | 0.000 |
| ≥51 | 53 | 32.0 (20.04) | ||
| 6MWT (meters) | <350 | 36 | 19.6 (11.63) | 0.001 |
| ≥350 | 66 | 29.7 (17.65) | ||
| Charlson Comorbidity Index | ≤1 | 65 | 27,5 (19,96) | 0.233 |
| >1 | 37 | 22,1 (12,59) | ||
| GAP stage 1 (n=44) | GAP stage 1 (n=44) | GAP stage 3 (n=26) | ||
| BMI | 25.2±1.30a | 23.7±1.50b | 22.5±1.42c | 0,000 |
| NLR | 2.5±0.71a | 3.6±0.70b | 4.1±1.15b,c | 0,000 |
| Albumin | 4.0±0.53a | 3.36±0.45b | 2.93±0.11c | 0,000 |
| Neutrophils (10^9/L) | 4.5±0.84a | 6.1±0.76b | 6.5±1.08b,c | 0,000 |
| Lymphocytes (10^9/L) | 1,6 (0) | 1.7 (0) | 1.6 (0) | 0,070 |
| Monocytes (10^9/L) | 0.8 (0) | 0.7 (0) | 0.9 (0) | 0,114 |
| ALI | 38 (16,59)a | 25,1 (7.43)b | 17.6 (4.27)c | 0,000 |
|
ALI Quantile 1 [< 21,2] (n=36) |
ALI Quantile 2 [21,3-31,4] (n=33) |
ALI Quantile 3 [>31,5] (n=33) |
||
| BMI | 22.9±1.38a | 24.1±1.73b | 25.2±1.43c | 0,000 |
| NLR | 4.2±0.96a | 3,3±0.45b | 2.3±0.56c | 0,000 |
| Albumin | 2.8±0.48a | 3.7±0.41b | 4.0±0.55c | 0,000 |
| Neutrophils (10^9/L) | 6.4±0,96a | 5.7±0.86b | 4.2±0.76c | 0,000 |
| Lymphocytes (10^9/L) | 1.6 (0)a | 1.7 (0)b | 1.9 (1)b,c | 0,000 |
| Monocytes (10^9/L) | 0,9 (0) | 0,8 (0) | 0.8 (0) | 0,534 |
Data are expressed as mean ± standard deviation, median (interquartile range], or n (%). Abbreviations: ALI: advanced lung cancer inflammation index, GAP: gender, age and two lung physiology variables index, FVC:forced vital capacity, DLCO: diffusion capacity for carbon monoxide, 6MWT:six-minute walk test. BMI: body mass index, NLR, neutrophil-lymphocyte ratio.
Table 3.
Relationships between simple blood cell count indexes and clinical parameters.
| Gap stage | FVC | DLCO | 6MWT | ||
|---|---|---|---|---|---|
| ALI | r | -0.815 | 0.498 | 0.637 | 0.445 |
| p | 0.000 | 0.000 | 0.000 | 0.000 | |
| BMI | r | -0.634 | 0.406 | 0.493 | 0.499 |
| p | 0.000 | 0.000 | 0.000 | 0.000 | |
| NLR | r | 0.638 | -0.348 | -0.525 | -0.257 |
| p | 0.000 | 0.000 | 0.000 | 0.009 | |
| Albumin | r | -0.636 | 0.410 | 0.431 | 0.412 |
| p | 0.000 | 0.000 | 0.000 | 0.000 |
Abbreviations: BMI: body mass index, GAP: gender, age and two lung physiology variables index, FVC:forced vital capacity, DLCO: diffusion capacity for carbon monoxide,; NLR, neutrophil-lymphocyte ratio, ALI: advanced lung cancer inflammation index, 6MWT six-minute walk test.
Table 4.
Receiver operating characteristics (ROC) curves albümin, BMI, ALI, and NLR for mortality in ipf patients.
Table 4.
Receiver operating characteristics (ROC) curves albümin, BMI, ALI, and NLR for mortality in ipf patients.
| AUC (%95) | Cut off | p | sensitivity (%) | specifity (%) | |
|---|---|---|---|---|---|
| Albumin | 0.952 (0.904-1,000) | 2.45 | 0.000 | 63,6 | 97,8 |
| BMI | 0.885 (0.811-0.959) | 21,84 | 0,000 | 54,5 | 94,5 |
| ALI | 0.945 (0.892-0.998) | 11,20 | 0,000 | 63,6 | 98,9 |
| NLR | 0.768 (0.600-0.936) | 5,25 | 0,004 | 36,4 | 98,9 |
Abbreviations: BMI: body mass index, NLR, neutrophil-lymphocyte ratio, ALI: advanced lung cancer inflammation index, AUC area under the curve, CI confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



