Submitted:
15 August 2024
Posted:
19 August 2024
You are already at the latest version
Abstract
Psoriasis is a multifactorial, chronic, and inflammatory disease that severely impacts patients’ quality of life. The disease is caused by genetic irregularities affected by the epigenetic and environmental factors. Some of these factors may include the seasonal changes, such as solar radiation, air pollution and humidity, and changes in circadian rhythm, especially in the temporal and polar zones. Thus, some psoriasis patients report seasonal variability of symptoms. Through a comprehensive review, we aim to delve deeper into the intricate interplay between seasonality, environmental factors, and the genetic and epigenetic landscape of psoriasis. By elucidating these complex relationships, we strive to provide insights that may inform targeted interventions and personalized management strategies for individuals living with psoriasis.
Keywords:
psoriasis
; environmental factors
; genetics
; epigenetics
; solar radiation
; humidity
; air pollution
; circadian rhythm
; geoepidemiology
; seasonality
1. Introduction
Psoriasis vulgaris (PsV) is a chronic systemic inflammatory disease that significantly impacts patients' quality of life [1,2]. Depending on the geographic region, PsV affects from 0.27 to 11.4% of the worldwide population. Ten to forty percent of psoriatic patients are affected with psoriatic arthritis (PsA) [3,4,5,6]. PsV, due to its inflammatory background, is linked with an increased risk of several comorbidities, such as cardiovascular disorders (CVD), metabolic syndrome, nonalcoholic fatty liver disease, and inflammatory bowel disease. Comorbidities in psoriasis may lead to a shortened lifespan for affected patients [7,8,9]. Due to visible skin lesions and a proinflammatory background, psoriasis is associated with a lower quality of life and psychiatric disorders such as depression and anxiety [10,11,12,13]. Patients affected by PsV experience reduced levels of employment and income [1,10,14]. Beyond geographic differences psoriasis is affected by environmental factors and presents different seasonal patterns [6,15]. Understanding the seasonal patterns of psoriasis is important for patients and healthcare providers, fostering tailored treatment approaches, optimizing outcomes, and improving patient-clinician relationships. This review aims to elucidate the seasonality of psoriasis vulgaris (PsV), exploring potential molecular mechanisms underpinning this phenomenon, and evaluating its implications on treatment strategies and patient adherence.
1.1. Material and Methods
The PubMed, Embase, and Google Scholar databases were searched for the following keywords: “environmental factors”, “genetics”, “epigenetics”, “solar radiation”, “humidity,”, “air pollution”, “circadian rhythm”, “geoepidemiology”, “seasonal” and “seasonality” related to psoriasis vulgaris. Original studies and review papers in the English language, published until 10th of March 2024, were taken into consideration. The authors reviewed each paper. Articles that did not mention terms related to the possible seasonal severity of psoriatic symptoms were excluded from further review. The remaining articles’ abstracts were read, and the relevant articles relating to seasonality and environmental factors have been read in full and included in the analysis. The authors also screened the references in the selected articles and included relevant publications. Figures were prepared with BioRender© (www.biorender.com) software.
2. Molecular Background of Psoriasis
2.1. Genetics of Psoriasis
Psoriasis vulgaris is a multifactorial disorder in which the genetic background takes major impact on the course of the symptoms. [16]. About 30 to 35 percent of PsV patients are also affected by psoriatic arthritis. PsV and PsA share strong hereditary component. Genes responsible for symptoms may be inherited dominantly or recessively [17]. PsA occurs at a high rate in close relatives, more likely in mono- compared to dizygotic twins [18]. Genome-wide association studies (GWAS) revealed more than eighty loci associated with psoriasis, including IL-23/NF-κB/epidermal differentiation signaling. [17]. Genes associated with PsA include HLA-B/C, HLA-B, IL-12B, IL-23R, TNP1, TRAF3IP3, and REL [17,19]. These genes are associated with the maintenance of cutaneous barrier functioning, control of innate immune-mediated by nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB), and interferon signaling, but also adaptive responses linked to the activity of CD8 lymphocytes and Th17 [17,19]. There are at least fifteen regions that contribute to psoriatic disorders, known as Psoriasis Susceptibility (PSORS) numbered from 1 to 15 [20].
The PSORS1 maps to the Major Histocompatibility Complex (MHC) on chromosome 6p21 and encompasses nine genes, alleles, or haplotypes of human leukocyte antigen (HLA) class I [20,21]. HLA-C, Coiled-Coil Alpha-Helical Rod Protein 1 (CCHCR1), and corneodesmosin (CDSN) genes are highly polymorphic in patients with PsV [22,23]. The HLA-B*27, HLA-B*39, HLA-B*38, and HLA-B*08 are associated with a higher risk of PsA with HLA-B27 and HLA-B*39 earlier onset of PsV and PsA. The HLA phenotypes are also associated with different clinical manifestations of PsA; whereas HLA-B*08 with asymmetric sacroiliitis, peripheral arthritis ankylosis, and increased joint damage, the HLA-B*27 is associated with symmetric sacroiliitis, dactylitis and enthesitis [24]. The HLA-C encodes a receptor that participates in immune responses by presentation of antigens to CD8+ T lymphocytes [25]. HLA-Cw6 allele can present specific melanocyte auto-antigen (ADAMTS-like protein 5) to CD8+ T-cells [22]. The HLA-C*06:02 is associated with an earlier onset of PsV and a later onset of PsA [26]. Corneodesmosin (CDSN) is involved in the production of the protein responsible for skin desquamation; however, its association with PsV is inconclusive [20,25,27,28]. PSORS2 locus contains the Caspase Recruitment Domain Family Member 14 (CARD14) gene, which is highly expressed in keratinocytes [29]. CARD14 is an adaptive protein that takes part in NF-κB signaling, leading to the production of proinflammatory cytokines [29]. Gain of function mutations in the CARD14 gene are associated not only with psoriasis but also with other inflammatory skin diseases: pityriasis rubra pilaris (PRP) and generalized pustular psoriasis (GPP) [17,30,31].
Other PSORS4 region maps to chromosome 1q21 includes the Epidermal Differentiation Cluster (EDC), which participates in definitive keratinocyte differentiation [20,32]. Deletion of two genes from the EDC region, LCE3B, and LCE3C, is associated with psoriasis and disruption of epidermal barrier function [32,33,34].
Polymorphisms associated with PsV are reported in IL-12B, IL-13, RUNX1, IL-23 receptor (il23r), TNF-regulated protein A20 (TNFAIP3), tyrosine-protein phosphatase non-receptor type 22 (PTPN22) genes [35,36,37,38]. Another polymorphisms in FTO, CALCR, AC003006.7 genes were found in patients with PsV are also related to obesity [39].
2.2. Epigenetics of Psoriasis
For many years, epigenetic factors have been investigated in the context of skin diseases, including psoriasis. The epigenetic modifications influence the genetic expression through methylation, histone modifications, and microRNA (miRNA).
3.2.1. DNA Methylation
OAS2 (2′-5′-oligoadenylate synthetase 2) gene is an antiviral enzyme activated by innate immune system and its overexpression has been reported in patients with inflammatory diseases. Study by Gu et al. [40] revealed that OAS2 gene was hypomethylated in PsV skin samples from 39 psoriatic patients. In another study by Roberson et al. [41], over 1300 genes transcripts were altered in 20 skin samples of the patients with PsV (12 biopsies of skin affected with psoriasis, and 8 of uninvolved skin) compared to 10 samples from healthy volunteers. Out of 1108 differed gene’s expression, 674 gene’s CpG site were hypermethylated and 444 hypomethylated. The altered CpG sites methylation was observed and associated with transcriptional upregulation of genes such as KYNU, OAS2, S100A12, and SERPINB3 which are associated with PsV. Authors also reported that after one month therapy with TNF-α inhibitors in psoriatic patients, the methylation reversed toward the non-psoriatic state observed in healthy subjects. Verma et al. [42] performed genome-wide analysis using epidermal samples to investigate global DNA methylation in patients with psoriasis. Authors mapped over thirty-five thousand differently methylated sites in patients with PsV compared to healthy volunteers. Additionally, a large number of differently methylated sites were present in clinically uninvolved skin samples versus healthy epidermidis, suggested the presence of pre-lesion state in clinically healthy skin with no psoriatic symptoms. Chandra et al. [43] profiled the methylation of psoriatic lesions and adjacent normal skin tissues of 24 patients with PsV (48 pairs) and comparing to a cohort of 30 skin samples of 15 healthy participants. Genome-wide methylation profiling revealed inverse correlation between methylation and overlapping genes activity located in PSORs regions, including 100A9, SELENBP1, CARD14, KAZN and PTPN.
3.2.2. Histone Modification
Zhang et al. [44] analysed histone methylation of psoriatic lesions and peripheral blood mononuclear cells (PBMCs) in thirty patients with PsV and twenty healthy volunteers. The mean total 5mC levels of psoriatic PBMC’s were significantly increased compared to normal controls and positively correlated with disease activity assessed with PASI scores. Ovejero-Benito et al. [45] analysed PBMCs samples of 39 PsV patients treated with biologics (ustekinumab, secukinumab, adalimumab, ixekizumab) before and after start of the therapy, and from forty-two healthy subjects. Psoriasis patients presented reduced levels of acetylated H3 and H4 and increased levels of methylated H3K4 when compared to controls. There were no statistically significant changes of methylation level between pre- and post-treatment samples, however changes in methylated H3K27 level were found between responders and non-responders to biological medications after 3 months therapy. Eleven patients in this group also suffered from psoriatic arthritis. Patients without PsA presented significant differences in H3K4 methylation level between responders and non-responders to biological drugs at 3 and 6 months. Those results indicate that histone methylation may be used as a biomarker of treatment response to biological agents among patients with PsV.
3.2.3. Non-Coding RNA
Psoriasis is associated with multiple chromosome loci and majority of signals in genome-wide association studies (GWAS) are found in non-coding regions of the human genome [46,47]. Non-coding RNAs (ncRNAs) are RNA molecules which are not translated into proteins but are playing a key role in transcriptional and post-transcriptional DNA activity [46,47,48]. Long non-coding RNAs (lncRNA) are ncRNAs which are longer than two hundred nucleotides while micro RNAs (miRNA) are composed of 18-23 nucleotides. These two major classes of ncRNAs have a significant role in PsV pathogenesis [46,47,48].
Micro RNAs primarily regulate gene expression by binding to the 3’ UTR of mRNA, forming a miRNA-mRNA complex and leading to mRNA degradation [49]. These molecules modulate gene expression by influencing epigenetic modifications. MiRNAs can influence gene silencing and may contribute to human diseases by modulating DNA methylation in CpG islands. Additionally, miRNAs target enzymes that are important for DNA methylation and histone modifications. Patients with psoriasis have significantly higher levels of miRNA expression than healthy individuals, and these molecules may be involved in the pathogenesis of psoriasis. In several, studies miRNA-146a, miRNA-203, miRNA-21, miRNA-31, miRNA-184, miRNA-221, and miRNA-222 were upregulated, whereas miRNA-99a, miRNA-424, and miRNA-125b were downregulated in patients with psoriasis when compared to healthy subjects [43,48,50,51].
LncRNAs act as epigenetic modulators through the recruitment of transcription factors and chromatin modifying proteins to transcriptionally active loci [52,53,54]. Studies have identified over four thousand lncRNAs that are differently expressed in psoriatic skin compared to non-lesional or healthy skin [8,54].
3.2.4. Seasonality of Epigenetics
While the topic on seasonal epigenetic changes in plants and animals are well explored, the literature of seasonality of epigenetic factors in human immunology is still limited. Dopico et al. [55] found that 23% of the genome (5.136 unique genes out of 22.822 genes tested) show significant seasonal differences in expression. Moreover, they observed an inverted pattern of those expressions when comparing Europeans to Oceanian people. Among others, during winter months in Europe, a proinflammatory profile with high levels of soluble IL-6 receptor and C-reactive protein was observed. The proinflammatory drive of the immune system may be an evolutionary adaptation of humans to difficult environmental conditions during autumn, winter, and early spring. Furthermore, the daily variables of mean ambient temperature and mean sunlight hours both served as linear predictors of seasonality, which suggests human environmental adaptation [55].
3.3. Cellular Pathomechanisms in Psoriatic Disease
Psoriasis is considered a T-cell mediated condition affecting macrophages, dendritic cells, neutrophiles, keratocytes and other cells, leading to hyperproliferation of keratocytes [56,57,58,59]. The process consists of two phases. The first phase is triggered by external factors such as trauma, stress, and infections, which cause the release of deoxyribonucleic acid (DNA) and antimicrobial peptides (AMPs) such as cathelicidin (antimicrobial peptide LL-37), S100 and human β-defensins [59,60,61,62]. These molecules can create a complex binding to toll-like receptor nine (TLR9) on plasmacytoid dendritic cells in the dermis causing the release of proinflammatory factors: interferons INF-α and INF-β, tumor necrosis factor alpha (TNF-α), interleukins (IL) 6 and 1β. Further reactions lead to involvement and activation of naïve T-cells which secrete TNF-α, IL-12 and IL-23 and cause differentiation into mature T-cells. Th17, Th1, and Th22 conduct the further release of proinflammatory cytokines (TNF-α, INF-γ, IL-17, and IL-22) and activation of JAK/STAT pathway, which further creates self-generating positive loop causing proliferation of the keratinocytes, acanthosis, and then scaling of the epidermis [63,64,65]. It is also hypothesized that because of the polyspecificity of T-cell receptor (TCR), a variety of environmental antigens that align with previously identified potential psoriasis risk factors may interact with a pathogenic psoriatic TCR [66,67]. This interaction could potentially trigger an autoimmune response against melanocytes in psoriasis. Steering clear of these environmental risk factors could aid in the control and management of psoriasis [66,67].
4. Environmental Factors Effecting Psoriasis
4.1. Sunlight
The Sun is a natural source of electromagnetic energy, from gamma radiation to radio waves. Due to the atmosphere filtering effect, a range between 280 and 2 500 nm reaches the surface of the Earth, consisting of 4% of ultraviolet radiation (UV, 280–400 nm), 43 % of visible light (400–760 nm) and 53 % of infrared radiation (IR, 760–1000 nm) [68,69] (Table 1).
Approximately 95 % of terrestrial UV is UV-A radiation, while the rest is UV-B radiation. The mechanisms of UV-R on the skin are represented on the Figure 1.
The significancy of sunlight and its impact on psoriasis is well established. Phototherapy is one of the most common treatment options for children and adults [85,86]. Exposure to solar radiation in skin influences several epidermis functions due to apoptosis, DNA damage responses and cell cycle control, innate and acquired immune regulation and inflammation, redox response and angiogenesis, circadian rhythmicity, and keratinocyte differentiation [87]. In keratinocytes of psoriatic skin, UV-B 311 nm wavelength exposure causes upregulation of pro-apoptotic genes leading to the apoptosis and suppression of the keratinocyte differentiation. UV-B also causes increased levels of reactive oxygen species (ROS) which can result in oxidative damage to proteins, DNA, and lipids. Excessive production of ROS can disrupt redox homeostasis and cause DNA damage [87]. Due to above mechanisms, phototherapy (especially UV-B 311 nm) is one of the treatments for patients with PsV [68,85,87,88]. Photochemotherapy with psolaren and UV-A irradiation (PUVA) used both locally (e.g., PUVA baths) and orally are another standard phototherapy used in psoriasis treatment [68,85]. Lately, the spectra of visible light, the blue and red light, were used in psoriasis treatment; however, the results of the clinical studies are inconclusive [89,90,91,92,93,94].
Heliotherapy is defined as medical therapy involving exposure to natural sunlight [95]. It was reported that heliotherapy may be an alternative to other treatments for psoriasis in low- and mid-latitude regions of the Eaarth, including cold and cloudy countries such as Poland [69,96,97]. In Italy [98] and Israel [99,100], heliotherapy has been used in practice. However, UV radiation, despite its therapeutic effect in patients with psoriasis, has many negative effects on the skin. Exposure to ultraviolet radiation is a major risk factor for the development of solar lentigines and, more significantly, skin neoplasms [72,101,102,103]. The practical application of heliotherapy can be realized using UV intensity at the ground-level from weather forecasting models [97,104] and/or measurements with standard UV monitoring instruments placed at the tanning site [105].
However, exposure to UV is not beneficial for all PsV patients. Photosensitive psoriasis (P-PsV) refers to a group of patients who may experience a worsening of their psoriasis symptoms when exposed to sunlight [106]. This phenomenon affects between 5.5% and 24% of psoriatic patients with female predominance and low age of disease onset [106,107]. The main cause of this phenomenon is Koebnerization, which is the development of new psoriasis lesions due to local trauma, such as UV radiation and sunburns [106,108]. Other factors that can exacerbate symptoms include coexisting conditions like polymorphic light eruption, systemic erythematous lupus, porphyria, and chronic actinic dermatitis. HLA-CW*0602 and CARD14 mutations have been linked to P-PsV [106,107,109]. The innate immune response, triggered by UV-induced damage-related molecular patterns (DAMP), impaired self-coding RNA, or possible inflammasome formation and activation, creates a skin microenvironment that is conducive to psoriasis [106,110]. This environment is characterized by an abundance of IL-17, IFN-γ, and TNF-α, and a deficiency of IL-4 and IL-10, leading to worsening psoriatic symptoms [106,111].
4.2. Humidity
Psoriasis is associated with increased transepidermal water loss (TEWL) and decreased subcutaneous water content [112]. The reduced water content in epidermis was reported to be related to the papulosquamous skin features of PsV [112,113,114]. In the study conducted by Nakahigashi et al. [113] comparing aquaporin 3 (AQP3) expression via immunofluorescence and skin hydration in the epidermis (stratum corneum hydration - SCH) in 19 PsV patients and ten healthy volunteers were investigated. Results of the study indicated that patients with PsV when compared to healthy subjects had significantly increased TEWL and decreased SCH. Voss et al. [115] evaluated ten healthy and 10 PsV skin samples by immunohistochemistry using antibodies recognizing AQP3 and enzyme phospholipase D2, which also interact functionally in normal skin by inhibiting keratinocytes' hyperproliferation. In psoriasis samples, APQ3 was mainly observed in the cytoplasm rather than the cellular membrane, and PLD2 staining revealed decreased immunoreactivity and aberrant localization. Another cross-sectional study by Montero-Vilchez et al. [114], which included 157 healthy individuals, ninety-two psoriasis and sixty-five atopic dermatitis (AD) patients, compared TEWL, SCH, and temperature values between healthy skin, psoriatic skin, and AD skin. The results of the study revealed statistically decreased values of TEWL and temperature, with increased values for SCH in patients with PsV compared to healthy volunteers. Thus, the authors stated that TEWL and skin temperature measurement can be helpful in the assessment of disease severity and treatment intensity. Similar conclusions were presented in the research paper by Nikam et al. (2011). Denda et al. [116] on mice models (HR-1) demonstrated the influence of prolonged dry and moist environments on the skin. Exposure to low humidity for 48 hours led to increased inflammatory markers and skin barrier disruption, resulting in marked epidermal hyperplasia. Cravello and Ferri [117] measured TEWL changes in the skin of young six female participants who were affected by different environmental factors in the climate chamber. Authors demonstrated correlation between TEWL and ambient temperature, while the relative humidity had a weaker effect on TEWL in the temperature range under investigation. Mean skin temperature showed a higher correlation with ambient temperature compared with relative humidity.
On the other hand, according to Liang et al. [118] the incidence of biologic therapy initiation in patients with psoriasis appeared to be higher in low humidity regions of the South and Midwest USA, than in other regions.
4.3. Air Pollution
Particulate matter (PM2.5: ≤2.5 μm; PM10: ≤10 μm) and nitrogen dioxide (NO2) cause oxidative damage to the epithelial cells by production of volatile organic compounds, increasing TEWL [103,119,120,121]. According to the available data PM2.5, PM10, and surface ozone (O3) may play essential roles in psoriasis development via aryl hydrocarbon receptor (AHR) activation, leading to increased Th-17 differentiation [122,123,124,125]. AHR is a ligand-dependent transcriptional factor that plays a crucial role in Th17 functioning, influencing the production of IL-22 and taking part in chemical sensing of the circadian rhythm and the skin’s adaptive response to environmental stimuli by controlling the Treg and Th17 cell differentiation [103,120,121,123,126]. This ligand regulates the Treg and Th17 cell differentiation, playing a vital role in the development of psoriasis. AHR receptor is modulated by the novel drug, tapinarof, which recently has been approved by FDA in the topical treatment for psoriasis [127]. Other outdoor pollutants such as carbon monoxide (CO) and sulfur dioxide (SO2) also cause epidermal damage due to ROSs [103,128]. Air pollutants present seasonal distribution [129,130]. It was shown that increased concentrations of air pollutants cause flares of PsV [131,132]. Liaw et al. [132] reported that blood concentration of cadmium was statistically significantly higher in patients with psoriasis and correlated with the disease severity.
Air pollution may influence psoriasis flare ups due to its seasonal pattern caused by indoor heating and decrease beneficial UV exposure for psoriatic patients [103,133].
Another air pollutant, cigarette smoke, is strongly associated with incidence and severity of psoriasis [122,134]. Nicotine causes an increased secretion of proinflammatory cytokines IL-2, IL-12, INF-γ, and granulocyte-monocyte colony-stimulating factor, which also participate in the keratinocyte’s differentiation [135]. Shan et al. [136] showed that CD1a+ antigen-presenting cells (APCs) from the lungs of patients with emphysema could induce autoreactive, pathological T helper 1 (Th1) and Th17 cell responses and cause overexpression for INF-γ and IL-17A which take crucial role in psoriasis pathogenesis. Smoking is also related to two single nucleotide polymorphisms at the CSMD1 gene (rs7007032 and rs10088247), which effect epithelial cell turnover and influence the differentiation of keratinocytes [37].
PsV patients have an increased risk of pulmonary diseases such as asthma, chronic obstructive pulmonary disease (COPD), obstructive sleep apnea (OSA), and pulmonary hypertension [137]. Similarly, pulmonary disorders, such as COPD [138,139], asthma [140], OSA [141], are related with the higher risk of psoriasis susceptibility. Smoking is also strongly associated with psoriasis [142]. Zhou et al. [143] conducted meta-analysis of the relationship between smoking and treatment efficacy in PsV patients. Authors concluded that smoking negatively affects the efficacy of psoriasis treatment and smokers are exposed to more immune regulators compared to non-smokers. This results indicate that smoking cause worse improvement to conventional and biological treatment. On the other hand, smoking is associated with increased incidence of psoriasiform lesions in inflammatory bowel disease patients undergoing anti-TNF therapy [144].
4.4. Circadian Rhythm
Li et al. [145] reported higher risk of incidence of psoriasis and psoriatic comorbidities in rotating night shift healthcare workers. This phenomenon can be explained by lower exposure to sunlight, decreased vitamin D levels, reduced production of melatonin, or a tendency to behavioral disruptions, but also by the circadian rhythm’s disturbance. A similar study by Huang et al. [146] had comparable results in urticaria incidence.
The circadian rhythm is regulated by the so-called master clock located in the suprachiasmatic nucleus (SCN) and affects molecular clocks in peripheral tissues [147,148,149]. The molecular mechanism of the circadian rhythms is based on the transcription-translation positive and negative feedback loops of circadian clock genes and their proteins [150]. The positive arm of the cire clock gene network consists of the transcription factor Brain and Muscle ANT-like 1 (BMAL1) and Circadian Locomotor output Circle (CLOCK), which form heterodimers binding the enhancer box to active transcription of Period (Per) 1, 2 and 3 and Cryptochrome (CRY) 1 and 2. PER and CRY drive the negative arm by inhibiting the expression of BMAL1-CLOCK genes, leading to the impediment of their transcription. Decreased levels of PER and CRY factors conduct the BMAL1-CLOCK activation, completing the circle within 24 hours. Other clock-controlled genes associated with circadian rhythms within the SCN are RAR-related orphan receptors (RORs) and REV-ERBS-response elements (RORE), which form a secondary feedback loop influencing the oscillatory expression of the BMAL1 gene [149].
The light causes the retina's neuronal and hormonal signaling, activating the SCN [147]. Neurotransmitters involved in this process, vasoactive intestinal peptide (VIP) and arginine vasopressin (AVP), along with the astrocytes, stabilize the circadian clocks within the SNC [147,148,149]. Peripheral tissues’ clocks, for example, skin, are also influenced by environmental factors, such as temperature, activity, and food intake [151,152].
The increased risk of psoriasis appears to be linked to disturbances in circadian rhythms [145,149,153,154,155,156,157]. The direct link between Th17 cells differentiation and the circadian clock was firstly described by Yu et al. in 2013 [158]. Expression of NFIL3 suppresses Th17 cell development by repressing orphan receptor RORγt transcription. CLOCK, PER2, and BMAL1 genes also play a significant part in the transcription of IL-23R in γ/β+ T-cells. Mutations in these regions are associated with induction of psoriatic symptoms [154]. BMAL1, CRY, RORα, and REV-ERBα proteins are positive regulators of the anti-inflammatory reactions [154]. Downregulation of these proteins enhances inflammation. CLOCK protein, however, can promote inflammation via the NF-κB pathway. Circadian genes such as CRY2, PER3, NR1D1, and RORC are downregulated in psoriatic lesions and the adjacent normal skin compared to the skin from non-psoriatic individuals [159]. The mRNA expression for IL-17A, IL-22, and IL-23 is strongly associated with circadian genes and elevates at night, decreases at dawn, and then increases during the day [154]. The disruption of the REV-ERBα gene, which suppresses RORγt-driven Th17 cell differentiation, also seems to be involved in developing psoriasis and psoriatic arthritis symptoms [160].
The study conducted by Hirotsu et al. [161] on the mice Balb/C which went through selective paradoxical sleep deprivation led to immunological disturbances. Authors observed increased levels of proinflammatory cytokines IL-1, IL-6, and IL-12 and decreased levels of anti-inflammatory cytokine IL-10 in tested mice. Another study investigated the potential reciprocal relationship between the circadian clock, feeding time, and skin inflammation exacerbation [162]. Mice lacking circadian rhythms had more significant epidermal hyperplasia and more robust activation of the INF pathway. Also, the daytime-restricted feeding shifted the phase of INF-sensitive gene expression in mouse skin.
Németh et al. compared the expression of core clock genes in six human lesional and six non-lesional skin samples, and in human low calcium temperature (HaCaT) keratinocytes after stimulation with pro-inflammatory cytokines [163]. Authors also assessed the CLOCK proteins in skin biopsies from PsV patients by immunohistochemistry. Altered CLOCK gene expression was observed in non-lesional psoriatic skin, with increased CRY1, BMAL1, PER1 and PER2 gene expression and decreased REV-ERBα expression. Moreover, cytokine treatment affected the circadian oscillation and relative mRNA expression of clock gene in HaCaT keratinocytes. In lesional psoriatic skin REV-ERBα and CRY1 genes showed altered rhythmicity and reduced relative mRNA expression compared to healthy skin.
Melatonin (MLT) has a crucial impact on the circadian clock and is also related to psoriasis etiopathogenesis [164,165]. Some studies showed that patients with psoriasis, compared to non-PsV volunteers presented lower MTL levels [166,167,168].
Nguyen et al. [169] performed a prospective randomized study comparing the efficacy of topical corticosteroids in forty-six psoriasis patients based on the time of their application, one group applied medications between 5pm and 6pm, and the second group between 8am and 9am. In the group of patients who applied the treatment in the evening, the response to the therapy was faster compared to the patients who applied the medication in the morning. However, these differences were statistically irrelevant after five days of the treatment.
5. Geoepidemiology of Psoriasis
The seasons are different depending on the latitude. In the latitudes of tropic and subtropic climate zones, the weather is usually less dynamic and variable than in temperate zones. Those differences connected to exposure to different humidity, temperature, sunlight, etc., may also influence the severity and seasonality of psoriasis. Reports on the geoepidemiological profile of PsV are limited, with only 19% of the countries having epidemiological data on the disease [170]. Most studies were conducted in Europe, North America, and Australasia. In 2020, The Global Burden of Disease (GBD) analyzed the prevalence and impact of skin conditions [171]. Among the fifteen most common skin diseases, psoriasis was assigned the sequelae of itch and disfigurement. The authors also emphasized the concern about the pathogenic association between PsV and cardiovascular disorders. A study by GBD showed increased number of psoriasis diagnoses between 1990 and 2017. In addition, the risk of psoriasis assessed in the above study increased with age, which is consistent with literature data. Parisi et al. [170] conducted a meta-analysis and systemic review of the worldwide epidemiology of psoriasis based on 159 studies. The studies differed in the prevalence of PsV regionally and nationally. Regionally, the occurrence of the disease in the overall population varied from 0.11% in East Asia to 1.58% (from 0.50% to 5.73%) in Australasia and 1.52% (from 0.87% to 2.74%) in Western Europe. Country-specific prevalence of psoriasis varied substantially. Considering the estimate for the overall population, Australia 1.88% (from 0.59% to 6.10%), Norway 1.86% (from 0.94% to 3.97%), Israel 1.81% (from 0.83% to 4.44%), and Denmark 1.79% (from 0.91% to 3.61%) had the highest estimates of the prevalence of PsV. The estimated prevalence of psoriasis in countries in East Asia is significantly lower. Taiwan, with a PsV prevalence of 0.05% (0.02% to 0.16%) seems to be the country with the lowest country with cases of psoriasis per 100 000 people worldwide. The prevalence was highest in high-income countries, which may also have influenced the study results due to better healthcare systems, disease awareness, and better data quality. Another interesting study conducted by Lecaros et al. [172] described that the incidence of psoriasis in Chile depended on the latitude. The data revealed gradual elevation of prevalence in the population living in the country's Southern parts when compared to Northern areas. Among many factors that could have impacted this phenomenon, the authors mention environmental ones.
6. Seasonality of Psoriasis
Clinically observed seasonality of medical conditions is a well-known phenomenon [173]. The differences in the activity scores of the diseases seen among different countries during the year may not solely be influenced by environmental factors but also the cultural activities and festivities. For example, intermittent circadian fasting (Ramadan), a common Muslim practice, seemed beneficial in patients with psoriasis and psoriatic arthritis [174,175].
There is a common belief that in most patients with psoriasis, skin lesions improve in warmer months of the year [173,176,177,178,179,180,181,182]. However, not all literature data supports this statement (see Table 1 for more details) [179,183,184,185].
Brito et al. [177] examined the seasonality of the hospitalizations at a dermatological ward, with no differences observed regarding patients with psoriasis. The study by Ferguson et al. [178] revealed that 77% of patients with psoriasis reported seasonal changes in the disease activity with exacerbations in winter (67%) and summer months (24%). Mrowietz et al. [186] conducted a questionnaire study in Northern Germany. Five hundred thirty-six patients were self-classifying into four types of psoriasis intensity during a year: type 1- stable disease course with no variation depending on the season (40.86%), type 2 - unstable disease course with no variation depending on the season (22.57%), type 3 – increased flares incident rate in winter (30.6%) and type 4 - increased flares incident rate in summer (5.97%). In a retrospective study of 20 270 Chinese patients with psoriasis, the disease duration, hyperlipidemia, and smoking were associated with severe psoriasis in autumn and winter [187]. In this study, age and occupations with extensive sunlight exposure were negatively associated with seasonal psoriasis exacerbation. Considering the findings of Jensen et al. [188], only 30% of psoriatic patients in Northern and Central Europe reported improvement in their disease activity in summer months, however, other factors could be responsible for the results obtained in the study.
A survey study conducted on 1080 Polish patients with PsV revealed that seasonal changes were reported to have a considerable impact on the psoriasis disease course in 45.09% patients [142].
Internet searches connected with psoriasis and its treatment also showed statistically significant seasonality peak in late winter [185]. On the other hand, Kubota et al. [184] did not observe any difference in seasonal frequency in the number of patients with psoriasis using health services in Japan.
Outdoor conditions for the mid-autumn/winter and mid-spring/summer seasons are very different in Europe, with higher temperatures and stronger solar radiation in the latter period [189]. In mid-spring/summer, it is evident that the patients have a chance to synthesize large amounts of vitamin D during outdoor activities due to UV-B exposure. They also receive more solar radiation in UV-A (315-400 nm) and visible spectrum (400-700 nm), and prolonged outdoor exposures until late evening could interfere with melatonin production.
However, studies do not support the positive effect of possible higher levels of vitamin D on psoriatic patients in summer months. Theodoridis et al. [190] performed a meta-analysis of the influence of vitamin D supplementation on the severity of psoriasis, which could not confirm its beneficial effect. The Medical Board of the National Psoriasis Foundation in the USA does not recommend oral vitamin D in psoriatic patients with normal vitamin D levels [191].
Considering other environmental factors, it was reported that humidity significantly influenced the epidermis structure that can contribute to seasonal deteriorations and improvements of inflammatory dermatoses such as atopic dermatitis and psoriasis [116].
Another possible explanation for the phenomenon is the seasonally fluctuating expressions of several genes. Ruano et al. [192] analyzed a group of patients with moderate to severe plaque psoriasis treated with etanercept or adalimumab who, after achieving a significant response to the treatment, had a temporary suspension of the treatment. The authors found that the risk of relapse and duration of the remission was related to the time of the year the treatment was stopped. Figure 3
The seasonality of psoriasis activity may also affect the time when the systemic treatment is started. Liang et al. [118] evaluated initiation, discontinuation, and switching biologics and systemic non-biologics (drugs in 74 960 patients with psoriasis between 2016 and 2019 in the United States. The initiation of the treatment peaked in spring months, followed by the summer, fall and winter. Discontinuation of biologic drugs peaked in summer, and switching of biologics was highest in spring. The authors underlined that the initiation, discontinuation, and switching the biologics treatment for psoriasis was associated with season, although seasonality pattern is less clear for nonbiologic systemic medications. The question remains whether the environmental factors may influence the treatment course. In preliminary study by Niedźwiedź et al. [193] sixty-two patients with moderate to severe psoriasis were evaluated at the beginning of the biological treatment, after 1, 4 and 7 months of the therapy. The study involved categorizing patients into two distinct groups: those who initiated treatment during the colder months (from November to March) and those who began therapy in the warmer period (from May to September). After 1 and 4 months of treatment, it was observed that patients on IL-12/23 and IL-17 inhibitors had better improvement when the therapy was started in summer months. Interestingly, the course of psoriasis improvement remained consistent for patients using TNF-α inhibitors, irrespective of the season. The treatment outcomes after 7 months of therapy were comparable between both seasonal groups and across various types of biologics used.
7. Conclusion
Psoriasis activity and severity is affected by epigenetic and environmental factors such as sun exposure, humidity, air pollution and circadian rhythm. The seasonality of psoriasis may be related to a different expression of genes with a more proinflammatory immune system and various environmental changes observed as the evolutionary adaptation of humans to more difficult environmental conditions during autumn, winter, and early spring in temperate and subpolar climate regions. Patients who are exposed to a lower UV dose, higher amount of air pollutants or lower humidity may be more prone to deterioration of skin lesions. Also, disturbances in the circadian rhythm, such as changes in sleep pattern, variable day length during the year and shift working, may influence the skin symptoms of psoriasis. The differences in the psoriasis activity scores during the year in different countries can be not only influenced by environmental factors but also by cultural activities. The role of vitamin D level in PsV patients is still questionable. New data is emerging investigating the possible connection between the season of starting the therapy and the effectiveness of treatment. Further understanding of seasonality of psoriasis may improve healthcare resource planning in the disease management.
Author Contributions
Conceptualization, M.Nie.; investigation, M.Nie. and M.S.; resources, M.Nie.; data curation, M.Nie. and M.S.; writing—original draft preparation, M.Nie. and M.S.; writing—review and editing, M.Nie., M.S., M.C., M.Now., A.C., J.K., J.N. and A.L.; visualization, M.Nie.; supervision, M.C., A.C., J.K., J.N, and A.L.; project administration, M.Nie., J.N., and A.L.; funding acquisition, J.N. and A.L. All authors have read and agreed to the published version of the manuscript.
Funding
The research was supported by statutory activities of Medical University of Lodz, Poland, (no. 503/5-064-04/503-01) and Institute of Geophysics, Polish Academy of Sciences (no. 3841/E-41/S/2020). The APC was funded by statutory activities of Medical University of Lodz, Poland, no. 503/5-064-04/503-01.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Figures were prepared with the BioRender© (www.biorender.com) software.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Nestle, F.O.; Kaplan, D.H.; Barker, J. Psoriasis. N Engl J Med 2009, 361, 496–509. [Google Scholar] [CrossRef]
- Ritchlin, C.T.; Colbert, R.A.; Gladman, D.D. Psoriatic Arthritis. N Engl J Med 2017, 376, 957–970. [Google Scholar] [CrossRef]
- Parisi, R.; Symmons, D.P.; Griffiths, C.E.; Ashcroft, D.M.; Identification; Management of, P. ; Associated ComorbidiTy project, t. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol 2013, 133, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Villani, A.P.; Rouzaud, M.; Sevrain, M.; Barnetche, T.; Paul, C.; Richard, M.A.; Beylot-Barry, M.; Misery, L.; Joly, P.; Le Maitre, M.; et al. Prevalence of undiagnosed psoriatic arthritis among psoriasis patients: Systematic review and meta-analysis. J Am Acad Dermatol 2015, 73, 242–248. [Google Scholar] [CrossRef]
- Alinaghi, F.; Calov, M.; Kristensen, L.E.; Gladman, D.D.; Coates, L.C.; Jullien, D.; Gottlieb, A.B.; Gisondi, P.; Wu, J.J.; Thyssen, J.P.; et al. Prevalence of psoriatic arthritis in patients with psoriasis: A systematic review and meta-analysis of observational and clinical studies. J Am Acad Dermatol 2019, 80, 251–265 e219. [Google Scholar] [CrossRef] [PubMed]
- Ogdie, A.; Weiss, P. The Epidemiology of Psoriatic Arthritis. Rheum Dis Clin North Am 2015, 41, 545–568. [Google Scholar] [CrossRef]
- Springate, D.A.; Parisi, R.; Kontopantelis, E.; Reeves, D.; Griffiths, C.E.; Ashcroft, D.M. Incidence, prevalence and mortality of patients with psoriasis: a U.K. population-based cohort study. Br J Dermatol 2017, 176, 650–658. [Google Scholar] [CrossRef]
- Patrick, M.T.; Li, Q.; Wasikowski, R.; Mehta, N.; Gudjonsson, J.E.; Elder, J.T.; Zhou, X.; Tsoi, L.C. Shared genetic risk factors and causal association between psoriasis and coronary artery disease. Nat Commun 2022, 13, 6565. [Google Scholar] [CrossRef]
- Salahadeen, E.; Torp-Pedersen, C.; Gislason, G.; Hansen, P.R.; Ahlehoff, O. Nationwide population-based study of cause-specific death rates in patients with psoriasis. J Eur Acad Dermatol Venereol 2015, 29, 1002–1005. [Google Scholar] [CrossRef]
- Gelfand, J.M.; Feldman, S.R.; Stern, R.S.; Thomas, J.; Rolstad, T.; Margolis, D.J. Determinants of quality of life in patients with psoriasis: a study from the US population. J Am Acad Dermatol 2004, 51, 704–708. [Google Scholar] [CrossRef]
- Fabrazzo, M.; Cipolla, S.; Signoriello, S.; Camerlengo, A.; Calabrese, G.; Giordano, G.M.; Argenziano, G.; Galderisi, S. A systematic review on shared biological mechanisms of depression and anxiety in comorbidity with psoriasis, atopic dermatitis, and hidradenitis suppurativa. Eur Psychiatry 2021, 64, e71. [Google Scholar] [CrossRef] [PubMed]
- Jalenques, I.; Bourlot, F.; Martinez, E.; Pereira, B.; D'Incan, M.; Lauron, S.; Rondepierre, F. Prevalence and Odds of Anxiety Disorders and Anxiety Symptoms in Children and Adults with Psoriasis: Systematic Review and Meta-analysis. Acta Derm Venereol 2022, 102, adv00769. [Google Scholar] [CrossRef] [PubMed]
- Marek-Jozefowicz, L.; Czajkowski, R.; Borkowska, A.; Nedoszytko, B.; Zmijewski, M.A.; Cubala, W.J.; Slominski, A.T. The Brain-Skin Axis in Psoriasis-Psychological, Psychiatric, Hormonal, and Dermatological Aspects. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef] [PubMed]
- Horn, E.J.; Fox, K.M.; Patel, V.; Chiou, C.F.; Dann, F.; Lebwohl, M. Association of patient-reported psoriasis severity with income and employment. J Am Acad Dermatol 2007, 57, 963–971. [Google Scholar] [CrossRef]
- Griffiths, C.E.; Barker, J.N. Pathogenesis and clinical features of psoriasis. Lancet 2007, 370, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Babaie, F.; Omraninava, M.; Gorabi, A.M.; Khosrojerdi, A.; Aslani, S.; Yazdchi, A.; Torkamandi, S.; Mikaeili, H.; Sathyapalan, T.; Sahebkar, A. Etiopathogenesis of Psoriasis from Genetic Perspective: An updated Review. Current Genomics 2022, 23, 163–174. [Google Scholar] [CrossRef]
- Queiro, R.; Coto, P.; Gonzalez-Lara, L.; Coto, E. Genetic Variants of the NF-kappaB Pathway: Unraveling the Genetic Architecture of Psoriatic Disease. Int J Mol Sci 2021, 22. [Google Scholar] [CrossRef]
- Lonnberg, A.S.; Skov, L.; Skytthe, A.; Kyvik, K.O.; Pedersen, O.B.; Thomsen, S.F. Heritability of psoriasis in a large twin sample. Br J Dermatol 2013, 169, 412–416. [Google Scholar] [CrossRef]
- Rahmati, S.; Li, Q.; Rahman, P.; Chandran, V. Insights into the pathogenesis of psoriatic arthritis from genetic studies. Semin Immunopathol 2021, 43, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Capon, F. The Genetic Basis of Psoriasis. Int J Mol Sci 2017, 18. [Google Scholar] [CrossRef]
- Azuaga, A.B.; Ramirez, J.; Canete, J.D. Psoriatic Arthritis: Pathogenesis and Targeted Therapies. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef]
- Arakawa, A.; Siewert, K.; Stohr, J.; Besgen, P.; Kim, S.M.; Ruhl, G.; Nickel, J.; Vollmer, S.; Thomas, P.; Krebs, S.; et al. Melanocyte antigen triggers autoimmunity in human psoriasis. J Exp Med 2015, 212, 2203–2212. [Google Scholar] [CrossRef]
- International Psoriasis Genetics, C. The International Psoriasis Genetics Study: assessing linkage to 14 candidate susceptibility loci in a cohort of 942 affected sib pairs. Am J Hum Genet 2003, 73, 430–437. [Google Scholar] [CrossRef]
- Haroon, M.; Winchester, R.; Giles, J.T.; Heffernan, E.; FitzGerald, O. Clinical and genetic associations of radiographic sacroiliitis and its different patterns in psoriatic arthritis. Clin Exp Rheumatol 2017, 35, 270–276. [Google Scholar]
- Capon, F.; Munro, M.; Barker, J.; Trembath, R. Searching for the major histocompatibility complex psoriasis susceptibility gene. J Invest Dermatol 2002, 118, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Perez-Chada, L.M.; Balak, D.; Cohen, J.M.; Ogdie, A.; Merola, J.F.; Gottlieb, A.B. Measurement properties of instruments assessing psoriatic arthritis symptoms for psoriasis clinical trials: a systematic literature review. Expert Rev Clin Immunol 2020, 16, 267–283. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, B.; Liu, J.L.; Gao, X.H.; Chen, H.D.; Li, Y.H. Association of -619C/T polymorphism in CDSN gene and psoriasis risk: a meta-analysis. Genet Mol Res 2011, 10, 3632–3640. [Google Scholar] [CrossRef] [PubMed]
- Jonca, N.; Leclerc, E.A.; Caubet, C.; Simon, M.; Guerrin, M.; Serre, G. Corneodesmosomes and corneodesmosin: from the stratum corneum cohesion to the pathophysiology of genodermatoses. Eur J Dermatol 2011, 21 Suppl 2, 35–42. [Google Scholar] [CrossRef]
- Jordan, C.T.; Cao, L.; Roberson, E.D.; Pierson, K.C.; Yang, C.F.; Joyce, C.E.; Ryan, C.; Duan, S.; Helms, C.A.; Liu, Y.; et al. PSORS2 is due to mutations in CARD14. Am J Hum Genet 2012, 90, 784–795. [Google Scholar] [CrossRef]
- Fuchs-Telem, D.; Sarig, O.; van Steensel, M.A.; Isakov, O.; Israeli, S.; Nousbeck, J.; Richard, K.; Winnepenninckx, V.; Vernooij, M.; Shomron, N.; et al. Familial pityriasis rubra pilaris is caused by mutations in CARD14. Am J Hum Genet 2012, 91, 163–170. [Google Scholar] [CrossRef]
- Sugiura, K.; Muto, M.; Akiyama, M. CARD14 c.526G>C (p.Asp176His) is a significant risk factor for generalized pustular psoriasis with psoriasis vulgaris in the Japanese cohort. J Invest Dermatol 2014, 134, 1755–1757. [Google Scholar] [CrossRef] [PubMed]
- Oh, I.Y.; de Guzman Strong, C. The Molecular Revolution in Cutaneous Biology: EDC and Locus Control. J Invest Dermatol 2017, 137, e101–e104. [Google Scholar] [CrossRef] [PubMed]
- de Cid, R.; Riveira-Munoz, E.; Zeeuwen, P.L.; Robarge, J.; Liao, W.; Dannhauser, E.N.; Giardina, E.; Stuart, P.E.; Nair, R.; Helms, C.; et al. Deletion of the late cornified envelope LCE3B and LCE3C genes as a susceptibility factor for psoriasis. Nat Genet 2009, 41, 211–215. [Google Scholar] [CrossRef]
- Riveira-Munoz, E.; He, S.M.; Escaramis, G.; Stuart, P.E.; Huffmeier, U.; Lee, C.; Kirby, B.; Oka, A.; Giardina, E.; Liao, W.; et al. Meta-analysis confirms the LCE3C_LCE3B deletion as a risk factor for psoriasis in several ethnic groups and finds interaction with HLA-Cw6. J Invest Dermatol 2011, 131, 1105–1109. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Meng, X.; Liu, Y.; Ma, X.; Zhang, Q.; Li, C.; Li, C.; Ren, L. Association Between Protein Tyrosine Phosphatase Non-Receptor Type 22 (PTPN22) Polymorphisms and Risk of Ankylosing Spondylitis: A Meta-analysis. Med Sci Monit 2017, 23, 2619–2624. [Google Scholar] [CrossRef] [PubMed]
- Huraib, G.B.; Al Harthi, F.; Arfin, M.; Aljamal, A.; Alrawi, A.S.; Al-Asmari, A. Association of Functional Polymorphism in Protein Tyrosine Phosphatase Nonreceptor 22 (PTPN22) Gene with Vitiligo. Biomark Insights 2020, 15, 1177271920903038. [Google Scholar] [CrossRef]
- Yin, X.; Low, H.Q.; Wang, L.; Li, Y.; Ellinghaus, E.; Han, J.; Estivill, X.; Sun, L.; Zuo, X.; Shen, C.; et al. Genome-wide meta-analysis identifies multiple novel associations and ethnic heterogeneity of psoriasis susceptibility. Nat Commun 2015, 6, 6916. [Google Scholar] [CrossRef]
- Jiang, Y.; Wang, W.; Zheng, X.; Jin, H. Immune Regulation of TNFAIP3 in Psoriasis through Its Association with Th1 and Th17 Cell Differentiation and p38 Activation. J Immunol Res 2020, 2020, 5980190. [Google Scholar] [CrossRef]
- Kisielnicka, A.; Sobalska-Kwapis, M.; Purzycka-Bohdan, D.; Nedoszytko, B.; Zabłotna, M.; Seweryn, M.; Strapagiel, D.; Nowicki, R.J.; Reich, A.; Samotij, D.; et al. The Analysis of a Genome-Wide Association Study (GWAS) of Overweight and Obesity in Psoriasis. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef]
- Gu, X.; Boldrup, L.; Coates, P.J.; Fahraeus, R.; Nylander, E.; Loizou, C.; Olofsson, K.; Norberg-Spaak, L.; Garskog, O.; Nylander, K. Epigenetic regulation of OAS2 shows disease-specific DNA methylation profiles at individual CpG sites. Sci Rep 2016, 6, 32579. [Google Scholar] [CrossRef]
- Roberson, E.D.; Liu, Y.; Ryan, C.; Joyce, C.E.; Duan, S.; Cao, L.; Martin, A.; Liao, W.; Menter, A.; Bowcock, A.M. A subset of methylated CpG sites differentiate psoriatic from normal skin. J Invest Dermatol 2012, 132, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Verma, D.; Ekman, A.K.; Bivik Eding, C.; Enerback, C. Genome-Wide DNA Methylation Profiling Identifies Differential Methylation in Uninvolved Psoriatic Epidermis. J Invest Dermatol 2018, 138, 1088–1093. [Google Scholar] [CrossRef] [PubMed]
- Chandra, A.; Senapati, S.; Roy, S.; Chatterjee, G.; Chatterjee, R. Epigenome-wide DNA methylation regulates cardinal pathological features of psoriasis. Clinical Epigenetics 2018, 10. [Google Scholar] [CrossRef]
- Zhang, P.; Su, Y.; Zhao, M.; Huang, W.; Lu, Q. Abnormal histone modifications in PBMCs from patients with psoriasis vulgaris. Eur J Dermatol 2011, 21, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Ovejero-Benito, M.C.; Reolid, A.; Sanchez-Jimenez, P.; Saiz-Rodriguez, M.; Munoz-Aceituno, E.; Llamas-Velasco, M.; Martin-Vilchez, S.; Cabaleiro, T.; Roman, M.; Ochoa, D.; et al. Histone modifications associated with biological drug response in moderate-to-severe psoriasis. Exp Dermatol 2018, 27, 1361–1371. [Google Scholar] [CrossRef]
- Dopytalska, K.; Ciechanowicz, P.; Wiszniewski, K.; Szymanska, E.; Walecka, I. The Role of Epigenetic Factors in Psoriasis. Int J Mol Sci 2021, 22. [Google Scholar] [CrossRef]
- Ghosh, D.; Ganguly, T.; Chatterjee, R. Emerging roles of non-coding RNAs in psoriasis pathogenesis. Funct Integr Genomics 2023, 23, 129. [Google Scholar] [CrossRef] [PubMed]
- Antonatos, C.; Grafanaki, K.; Asmenoudi, P.; Xiropotamos, P.; Nani, P.; Georgakilas, G.K.; Georgiou, S.; Vasilopoulos, Y. Contribution of the Environment, Epigenetic Mechanisms and Non-Coding RNAs in Psoriasis. Biomedicines 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Shi, R.; Ma, R.; Tang, X.; Gong, Y.; Yu, Z.; Shi, Y. The role of microRNA in psoriasis: A review. Exp Dermatol 2023, 32, 1598–1612. [Google Scholar] [CrossRef]
- Mateu-Arrom, L.; Puig, L. Genetic and Epigenetic Mechanisms of Psoriasis. Genes (Basel) 2023, 14. [Google Scholar] [CrossRef]
- Ghafouri-Fard, S.; Eghtedarian, R.; Taheri, M.; Rakhshan, A. The eminent roles of ncRNAs in the pathogenesis of psoriasis. Noncoding RNA Res 2020, 5, 99–108. [Google Scholar] [CrossRef]
- Liu, S.; Shi, G.; Pan, Z.; Cheng, W.; Xu, L.; Lin, X.; Lin, Y.; Zhang, L.; Ji, G.; Lv, X.; et al. Integrated Bioinformatics Analysis for the Identification of Key lncRNAs, mRNAs, and Potential Drugs in Clear Cell Renal Cell Carcinomas. Int J Gen Med 2023, 16, 2063–2080. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Yang, C.; Zhang, J.; Zhong, W.; Zhu, L.; Chen, Y. Identification of potential key mRNAs and LncRNAs for psoriasis by bioinformatic analysis using weighted gene co-expression network analysis. Mol Genet Genomics 2020, 295, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Mercer, T.R.; Shearwood, A.M.; Siira, S.J.; Hibbs, M.E.; Mattick, J.S.; Rackham, O.; Filipovska, A. Mapping of mitochondrial RNA-protein interactions by digital RNase footprinting. Cell Rep 2013, 5, 839–848. [Google Scholar] [CrossRef]
- Dopico, X.C.; Evangelou, M.; Ferreira, R.C.; Guo, H.; Pekalski, M.L.; Smyth, D.J.; Cooper, N.; Burren, O.S.; Fulford, A.J.; Hennig, B.J.; et al. Widespread seasonal gene expression reveals annual differences in human immunity and physiology. Nat Commun 2015, 6, 7000. [Google Scholar] [CrossRef]
- Brembilla, N.C.; Boehncke, W.H. Revisiting the interleukin 17 family of cytokines in psoriasis: pathogenesis and potential targets for innovative therapies. Front Immunol 2023, 14, 1186455. [Google Scholar] [CrossRef] [PubMed]
- Reinhardt, A.; Prinz, I. Whodunit? The Contribution of Interleukin (IL)-17/IL-22-Producing gammadelta T Cells, alphabeta T Cells, and Innate Lymphoid Cells to the Pathogenesis of Spondyloarthritis. Front Immunol 2018, 9, 885. [Google Scholar] [CrossRef]
- Reali, E.; Ferrari, D. From the Skin to Distant Sites: T Cells in Psoriatic Disease. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef]
- Zhou, X.Y.; Chen, K.; Zhang, J.A. Mast cells as important regulators in the development of psoriasis. Front Immunol 2022, 13, 1022986. [Google Scholar] [CrossRef]
- Zielke, C.; Nielsen, J.E.; Lin, J.S.; Barron, A.E. Between good and evil: Complexation of the human cathelicidin LL-37 with nucleic acids. Biophys J 2023. [Google Scholar] [CrossRef]
- Uzuncakmak, T.K.; Karadag, A.S.; Ozkanli, S.; Akbulak, O.; Ozlu, E.; Akdeniz, N.; Oguztuzun, S. Alteration of tissue expression of human beta defensin-1 and human beta defensin-2 in psoriasis vulgaris following phototherapy. Biotech Histochem 2020, 95, 243–248. [Google Scholar] [CrossRef]
- Liang, H.; Li, J.; Zhang, K. Pathogenic role of S100 proteins in psoriasis. Front Immunol 2023, 14, 1191645. [Google Scholar] [CrossRef]
- Hu, P.; Wang, M.; Gao, H.; Zheng, A.; Li, J.; Mu, D.; Tong, J. The Role of Helper T Cells in Psoriasis. Front Immunol 2021, 12, 788940. [Google Scholar] [CrossRef] [PubMed]
- Schon, M.P.; Erpenbeck, L. The Interleukin-23/Interleukin-17 Axis Links Adaptive and Innate Immunity in Psoriasis. Front Immunol 2018, 9, 1323. [Google Scholar] [CrossRef]
- Tonel, G.; Conrad, C.; Laggner, U.; Di Meglio, P.; Grys, K.; McClanahan, T.K.; Blumenschein, W.M.; Qin, J.Z.; Xin, H.; Oldham, E.; et al. Cutting edge: A critical functional role for IL-23 in psoriasis. J Immunol 2010, 185, 5688–5691. [Google Scholar] [CrossRef]
- Schön, M.P. Adaptive and Innate Immunity in Psoriasis and Other Inflammatory Disorders. Front Immunol 2019, 10, 1764. [Google Scholar] [CrossRef] [PubMed]
- Ishimoto, T.; Arakawa, Y.; Vural, S.; Stohr, J.; Vollmer, S.; Galinski, A.; Siewert, K.; Ruhl, G.; Poluektov, Y.; Delcommenne, M.; et al. Multiple environmental antigens may trigger autoimmunity in psoriasis through T-cell receptor polyspecificity. Front Immunol 2024, 15, 1374581. [Google Scholar] [CrossRef]
- Kurz, B.; Berneburg, M.; Baumler, W.; Karrer, S. Phototherapy: Theory and practice. J Dtsch Dermatol Ges 2023, 21, 882–897. [Google Scholar] [CrossRef]
- Krzyscin, J.W.; Jaroslawski, J.; Rajewska-Wiech, B.; Sobolewski, P.S.; Narbutt, J.; Lesiak, A.; Pawlaczyk, M. Effectiveness of heliotherapy for psoriasis clearance in low and mid-latitudinal regions: a theoretical approach. J Photochem Photobiol B 2012, 115, 35–41. [Google Scholar] [CrossRef]
- Finlayson, L.; Barnard, I.R.M.; McMillan, L.; Ibbotson, S.H.; Brown, C.T.A.; Eadie, E.; Wood, K. Depth Penetration of Light into Skin as a Function of Wavelength from 200 to 1000 nm. Photochem Photobiol 2022, 98, 974–981. [Google Scholar] [CrossRef] [PubMed]
- Knak, A.; Regensburger, J.; Maisch, T.; Baumler, W. Exposure of vitamins to UVB and UVA radiation generates singlet oxygen. Photochem Photobiol Sci 2014, 13, 820–829. [Google Scholar] [CrossRef]
- von Thaler, A.K.; Kamenisch, Y.; Berneburg, M. The role of ultraviolet radiation in melanomagenesis. Exp Dermatol 2010, 19, 81–88. [Google Scholar] [CrossRef]
- Zhang, Y.; Dood, J.; Beckstead, A.A.; Li, X.B.; Nguyen, K.V.; Burrows, C.J.; Improta, R.; Kohler, B. Photoinduced Electron Transfer in DNA: Charge Shift Dynamics Between 8-Oxo-Guanine Anion and Adenine. J Phys Chem B 2015, 119, 7491–7502. [Google Scholar] [CrossRef] [PubMed]
- Wagener, F.A.; Carels, C.E.; Lundvig, D.M. Targeting the redox balance in inflammatory skin conditions. Int J Mol Sci 2013, 14, 9126–9167. [Google Scholar] [CrossRef]
- Bernard, J.J.; Gallo, R.L.; Krutmann, J. Photoimmunology: how ultraviolet radiation affects the immune system. Nat Rev Immunol 2019, 19, 688–701. [Google Scholar] [CrossRef] [PubMed]
- Berthier-Vergnes, O.; Bermond, F.; Flacher, V.; Massacrier, C.; Schmitt, D.; Péguet-Navarro, J. TNF-alpha enhances phenotypic and functional maturation of human epidermal Langerhans cells and induces IL-12 p40 and IP-10/CXCL-10 production. FEBS Lett 2005, 579, 3660–3668. [Google Scholar] [CrossRef]
- Bernard, J.J.; Cowing-Zitron, C.; Nakatsuji, T.; Muehleisen, B.; Muto, J.; Borkowski, A.W.; Martinez, L.; Greidinger, E.L.; Yu, B.D.; Gallo, R.L. Ultraviolet radiation damages self noncoding RNA and is detected by TLR3. Nat Med 2012, 18, 1286–1290. [Google Scholar] [CrossRef]
- Wille, J.J.; Kydonieus, A.F.; Murphy, G.F. cis-urocanic acid induces mast cell degranulation and release of preformed TNF-alpha: A possible mechanism linking UVB and cis-urocanic acid to immunosuppression of contact hypersensitivity. Skin Pharmacol Appl Skin Physiol 1999, 12, 18–27. [Google Scholar] [CrossRef]
- Chacón-Salinas, R.; Chen, L.; Chávez-Blanco, A.D.; Limón-Flores, A.Y.; Ma, Y.; Ullrich, S.E. An essential role for platelet-activating factor in activating mast cell migration following ultraviolet irradiation. J Leukoc Biol 2014, 95, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Guo, Q.; Jin, Y.; Chen, X.; Ye, X.; Shen, X.; Lin, M.; Zeng, C.; Zhou, T.; Zhang, J. NF-kappaB in biology and targeted therapy: new insights and translational implications. Signal Transduct Target Ther 2024, 9, 53. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Wu, S.B.; Hong, C.H.; Yu, H.S.; Wei, Y.H. Molecular Mechanisms of UV-Induced Apoptosis and Its Effects on Skin Residential Cells: The Implication in UV-Based Phototherapy. Int J Mol Sci 2013, 14, 6414–6435. [Google Scholar] [CrossRef]
- Zhou, L.; Jiang, A.; Veenstra, J.; Ozog, D.M.; Mi, Q.S. The Roles of Skin Langerhans Cells in Immune Tolerance and Cancer Immunity. Vaccines (Basel) 2022, 10. [Google Scholar] [CrossRef]
- Fukunaga, A.; Khaskhely, N.M.; Ma, Y.; Sreevidya, C.S.; Taguchi, K.; Nishigori, C.; Ullrich, S.E. Langerhans cells serve as immunoregulatory cells by activating NKT cells. J Immunol 2010, 185, 4633–4640. [Google Scholar] [CrossRef]
- Mizoguchi, A.; Mizoguchi, E.; Takedatsu, H.; Blumberg, R.S.; Bhan, A.K. Chronic intestinal inflammatory condition generates IL-10-producing regulatory B cell subset characterized by CD1d upregulation. Immunity 2002, 16, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Nast, A.; Smith, C.; Spuls, P.I.; Avila Valle, G.; Bata-Csorgo, Z.; Boonen, H.; De Jong, E.; Garcia-Doval, I.; Gisondi, P.; Kaur-Knudsen, D.; et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris - Part 1: treatment and monitoring recommendations. J Eur Acad Dermatol Venereol 2020, 34, 2461–2498. [Google Scholar] [CrossRef]
- Nast, A.; Smith, C.; Spuls, P.I.; Avila Valle, G.; Bata-Csorgo, Z.; Boonen, H.; De Jong, E.; Garcia-Doval, I.; Gisondi, P.; Kaur-Knudsen, D.; et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris - Part 2: specific clinical and comorbid situations. J Eur Acad Dermatol Venereol 2021, 35, 281–317. [Google Scholar] [CrossRef]
- Addison, R.; Weatherhead, S.C.; Pawitri, A.; Smith, G.R.; Rider, A.; Grantham, H.J.; Cockell, S.J.; Reynolds, N.J. Therapeutic wavelengths of ultraviolet B radiation activate apoptotic, circadian rhythm, redox signalling and key canonical pathways in psoriatic epidermis. Redox Biol 2021, 41, 101924. [Google Scholar] [CrossRef] [PubMed]
- Myers, E.; Kheradmand, S.; Miller, R. An Update on Narrowband Ultraviolet B Therapy for the Treatment of Skin Diseases. Cureus 2021, 13, e19182. [Google Scholar] [CrossRef]
- Sadowska, M.; Narbutt, J.; Lesiak, A. Blue Light in Dermatology. Life (Basel) 2021, 11. [Google Scholar] [CrossRef]
- Falcone, D.; Uzunbajakava, N.E.; van Abeelen, F.; Oversluizen, G.; Peppelman, M.; van Erp, P.E.J.; van de Kerkhof, P.C.M. Effects of blue light on inflammation and skin barrier recovery following acute perturbation. Pilot study results in healthy human subjects. Photodermatol Photoimmunol Photomed 2018, 34, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Weinstabl, A.; Hoff-Lesch, S.; Merk, H.F.; von Felbert, V. Prospective randomized study on the efficacy of blue light in the treatment of psoriasis vulgaris. Dermatology 2011, 223, 251–259. [Google Scholar] [CrossRef]
- Kleinpenning, M.M.; Otero, M.E.; van Erp, P.E.; Gerritsen, M.J.; van de Kerkhof, P.C. Efficacy of blue light vs. red light in the treatment of psoriasis: a double-blind, randomized comparative study. J Eur Acad Dermatol Venereol 2012, 26, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Maari, C.; Viau, G.; Bissonnette, R. Repeated exposure to blue light does not improve psoriasis. J Am Acad Dermatol 2003, 49, 55–58. [Google Scholar] [CrossRef]
- Pfaff, S.; Liebmann, J.; Born, M.; Merk, H.F.; von Felbert, V. Prospective Randomized Long-Term Study on the Efficacy and Safety of UV-Free Blue Light for Treating Mild Psoriasis Vulgaris. Dermatology 2015, 231, 24–34. [Google Scholar] [CrossRef]
- Jarrett, P.; Scragg, R. A short history of phototherapy, vitamin D and skin disease. Photochem Photobiol Sci 2017, 16, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Krzyscin, J.W.; Guzikowski, J.; Czerwinska, A.; Lesiak, A.; Narbutt, J.; Jaroslawski, J.; Sobolewski, P.S.; Rajewska-Wiech, B.; Wink, J. 24 hour forecast of the surface UV for the antipsoriatic heliotherapy in Poland. J Photochem Photobiol B 2015, 148, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Krzyscin, J.W.; Narbutt, J.; Lesiak, A.; Jaroslawski, J.; Sobolewski, P.S.; Rajewska-Wiech, B.; Szkop, A.; Wink, J.; Czerwinska, A. Perspectives of the antipsoriatic heliotherapy in Poland. J Photochem Photobiol B 2014, 140, 111–119. [Google Scholar] [CrossRef]
- Melandri, D.; Albano, V.M.; Venturi, M.; Flamigni, A.; Vairetti, M. Efficacy of combined liman peloid baths and heliotherapy in the treatment of psoriasis at Cervia spa, Emilia, Italy. Int J Biometeorol 2020, 64, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Emmanuel, T.; Lybaek, D.; Johansen, C.; Iversen, L. Effect of Dead Sea Climatotherapy on Psoriasis; A Prospective Cohort Study. Front Med (Lausanne) 2020, 7, 83. [Google Scholar] [CrossRef]
- Emmanuel, T.; Petersen, A.; Houborg, H.I.; Ronsholdt, A.B.; Lybaek, D.; Steiniche, T.; Bregnhoj, A.; Iversen, L.; Johansen, C. Climatotherapy at the Dead Sea for psoriasis is a highly effective anti-inflammatory treatment in the short term: An immunohistochemical study. Exp Dermatol 2022, 31, 1136–1144. [Google Scholar] [CrossRef]
- Slavinsky, V.; Helmy, J.; Vroman, J.; Valdebran, M. Solar ultraviolet radiation exposure in workers with outdoor occupations: a systematic review and call to action. Int J Dermatol 2024, 63, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Shraim, R.; Farran, M.Z.; He, G.; Marunica Karsaj, J.; Zgaga, L.; McManus, R. Systematic review on gene-sun exposure interactions in skin cancer. Mol Genet Genomic Med 2023, 11, e2259. [Google Scholar] [CrossRef] [PubMed]
- Belzer, A.; Parker, E.R. Climate Change, Skin Health, and Dermatologic Disease: A Guide for the Dermatologist. Am J Clin Dermatol 2023, 24, 577–593. [Google Scholar] [CrossRef] [PubMed]
- Krzyscin, J.W.; Lesiak, A.; Narbutt, J.; Sobolewski, P.; Guzikowski, J. Perspectives of UV nowcasting to monitor personal pro-health outdoor activities. J Photochem Photobiol B 2018, 184, 27–33. [Google Scholar] [CrossRef]
- Czerwinska, A.; Krzyscin, J. Measurements of biologically effective solar radiation using erythemal weighted broadband meters. Photochem Photobiol Sci 2024, 23, 479–492. [Google Scholar] [CrossRef]
- Wolf, P.; Weger, W.; Patra, V.; Gruber-Wackernagel, A.; Byrne, S.N. Desired response to phototherapy vs photoaggravation in psoriasis: what makes the difference? Exp Dermatol 2016, 25, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Rutter, K.J.; Watson, R.E.; Cotterell, L.F.; Brenn, T.; Griffiths, C.E.; Rhodes, L.E. Severely photosensitive psoriasis: a phenotypically defined patient subset. J Invest Dermatol 2009, 129, 2861–2867. [Google Scholar] [CrossRef] [PubMed]
- Camargo, C.M.; Brotas, A.M.; Ramos-e-Silva, M.; Carneiro, S. Isomorphic phenomenon of Koebner: facts and controversies. Clin Dermatol 2013, 31, 741–749. [Google Scholar] [CrossRef]
- Tsoi, L.C.; Spain, S.L.; Knight, J.; Ellinghaus, E.; Stuart, P.E.; Capon, F.; Ding, J.; Li, Y.; Tejasvi, T.; Gudjonsson, J.E.; et al. Identification of 15 new psoriasis susceptibility loci highlights the role of innate immunity. Nat Genet 2012, 44, 1341–1348. [Google Scholar] [CrossRef] [PubMed]
- Gallo, R.L.; Bernard, J.J. Innate immune sensors stimulate inflammatory and immunosuppressive responses to UVB radiation. J Invest Dermatol 2014, 134, 1508–1511. [Google Scholar] [CrossRef]
- Tan, G.; Niu, J.; Shi, Y.; Ouyang, H.; Wu, Z.H. NF-κB-dependent microRNA-125b up-regulation promotes cell survival by targeting p38α upon ultraviolet radiation. J Biol Chem 2012, 287, 33036–33047. [Google Scholar] [CrossRef]
- Camilion, J.V.; Khanna, S.; Anasseri, S.; Laney, C.; Mayrovitz, H.N. Physiological, Pathological, and Circadian Factors Impacting Skin Hydration. Cureus 2022, 14, e27666. [Google Scholar] [CrossRef]
- Nakahigashi, K.; Kabashima, K.; Ikoma, A.; Verkman, A.S.; Miyachi, Y.; Hara-Chikuma, M. Upregulation of aquaporin-3 is involved in keratinocyte proliferation and epidermal hyperplasia. J Invest Dermatol 2011, 131, 865–873. [Google Scholar] [CrossRef]
- Montero-Vilchez, T.; Segura-Fernandez-Nogueras, M.V.; Perez-Rodriguez, I.; Soler-Gongora, M.; Martinez-Lopez, A.; Fernandez-Gonzalez, A.; Molina-Leyva, A.; Arias-Santiago, S. Skin Barrier Function in Psoriasis and Atopic Dermatitis: Transepidermal Water Loss and Temperature as Useful Tools to Assess Disease Severity. J Clin Med 2021, 10. [Google Scholar] [CrossRef]
- Voss, K.E.; Bollag, R.J.; Fussell, N.; By, C.; Sheehan, D.J.; Bollag, W.B. Abnormal aquaporin-3 protein expression in hyperproliferative skin disorders. Arch Dermatol Res 2011, 303, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Denda, M.; Sato, J.; Tsuchiya, T.; Elias, P.M.; Feingold, K.R. Low humidity stimulates epidermal DNA synthesis and amplifies the hyperproliferative response to barrier disruption: implication for seasonal exacerbations of inflammatory dermatoses. J Invest Dermatol 1998, 111, 873–878. [Google Scholar] [CrossRef]
- Cravello, B.; Ferri, A. Relationships between skin properties and environmental parameters. Skin Res Technol 2008, 14, 180–186. [Google Scholar] [CrossRef]
- Liang, H.; Kirk, B.; Polinski, J.M.; Yue, X.; Kilpatrick, R.D.; Gelfand, J.M. Impact of Season and Other Factors on Initiation, Discontinuation, and Switching of Systemic Drug Therapy in Patients with Psoriasis: A Retrospective Study. JID Innov 2023, 3, 100171. [Google Scholar] [CrossRef] [PubMed]
- Green, M.; Kashetsky, N.; Feschuk, A.; Maibach, H.I. Transepidermal water loss (TEWL): Environment and pollution-A systematic review. Skin Health Dis 2022, 2, e104. [Google Scholar] [CrossRef] [PubMed]
- Parker, E.R. The influence of climate change on skin cancer incidence - A review of the evidence. Int J Womens Dermatol 2021, 7, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Parker, E.R.; Mo, J.; Goodman, R.S. The dermatological manifestations of extreme weather events: A comprehensive review of skin disease and vulnerability. The Journal of Climate Change and Health 2022, 8. [Google Scholar] [CrossRef]
- Abolhasani, R.; Araghi, F.; Tabary, M.; Aryannejad, A.; Mashinchi, B.; Robati, R.M. The impact of air pollution on skin and related disorders: A comprehensive review. Dermatol Ther 2021, 34, e14840. [Google Scholar] [CrossRef]
- Cella, M.; Colonna, M. Aryl hydrocarbon receptor: Linking environment to immunity. Semin Immunol 2015, 27, 310–314. [Google Scholar] [CrossRef]
- van Voorhis, M.; Knopp, S.; Julliard, W.; Fechner, J.H.; Zhang, X.; Schauer, J.J.; Mezrich, J.D. Exposure to atmospheric particulate matter enhances Th17 polarization through the aryl hydrocarbon receptor. PLoS One 2013, 8, e82545. [Google Scholar] [CrossRef] [PubMed]
- Afaq, F.; Zaid, M.A.; Pelle, E.; Khan, N.; Syed, D.N.; Matsui, M.S.; Maes, D.; Mukhtar, H. Aryl hydrocarbon receptor is an ozone sensor in human skin. J Invest Dermatol 2009, 129, 2396–2403. [Google Scholar] [CrossRef] [PubMed]
- Quintana, F.J.; Basso, A.S.; Iglesias, A.H.; Korn, T.; Farez, M.F.; Bettelli, E.; Caccamo, M.; Oukka, M.; Weiner, H.L. Control of T(reg) and T(H)17 cell differentiation by the aryl hydrocarbon receptor. Nature 2008, 453, 65–71. [Google Scholar] [CrossRef]
- Nogueira, S.; Rodrigues, M.A.; Vender, R.; Torres, T. Tapinarof for the treatment of psoriasis. Dermatol Ther 2022, 35, e15931. [Google Scholar] [CrossRef]
- Kantor, R.; Silverberg, J.I. Environmental risk factors and their role in the management of atopic dermatitis. Expert Rev Clin Immunol 2017, 13, 15–26. [Google Scholar] [CrossRef]
- Siudek, P. Chemical composition and source apportionment of ambient PM2.5 in a coastal urban area, Northern Poland. Chemosphere 2024, 356, 141850. [Google Scholar] [CrossRef]
- Ayinde, B.O.; Musa, M.R.; Ayinde, A.O. Application of machine learning models and landsat 8 data for estimating seasonal pm 2.5 concentrations. Environ Anal Health Toxicol 2024, 39, e2024011–2024010. [Google Scholar] [CrossRef]
- Bellinato, F.; Adami, G.; Vaienti, S.; Benini, C.; Gatti, D.; Idolazzi, L.; Fassio, A.; Rossini, M.; Girolomoni, G.; Gisondi, P. Association Between Short-term Exposure to Environmental Air Pollution and Psoriasis Flare. JAMA Dermatol 2022, 158, 375–381. [Google Scholar] [CrossRef]
- Liaw, F.Y.; Chen, W.L.; Kao, T.W.; Chang, Y.W.; Huang, C.F. Exploring the link between cadmium and psoriasis in a nationally representative sample. Sci Rep 2017, 7, 1723. [Google Scholar] [CrossRef] [PubMed]
- European Environmental Agency. Available online: https://www.eea.europa.eu/en (accessed on 10th of March 2024).
- Armstrong, A.W.; Harskamp, C.T.; Dhillon, J.S.; Armstrong, E.J. Psoriasis and smoking: a systematic review and meta-analysis. Br J Dermatol 2014, 170, 304–314. [Google Scholar] [CrossRef]
- Armstrong, A.W.; Armstrong, E.J.; Fuller, E.N.; Sockolov, M.E.; Voyles, S.V. Smoking and pathogenesis of psoriasis: a review of oxidative, inflammatory and genetic mechanisms. Br J Dermatol 2011, 165, 1162–1168. [Google Scholar] [CrossRef]
- Shan, M.; Yuan, X.; Song, L.Z.; Roberts, L.; Zarinkamar, N.; Seryshev, A.; Zhang, Y.; Hilsenbeck, S.; Chang, S.H.; Dong, C.; et al. Cigarette smoke induction of osteopontin (SPP1) mediates T(H)17 inflammation in human and experimental emphysema. Sci Transl Med 2012, 4, 117ra119. [Google Scholar] [CrossRef] [PubMed]
- Mleczko, M.; Gerkowicz, A.; Krasowska, D. Chronic Inflammation as the Underlying Mechanism of the Development of Lung Diseases in Psoriasis: A Systematic Review. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef]
- Ungprasert, P.; Srivali, N.; Thongprayoon, C. Association between psoriasis and chronic obstructive pulmonary disease: A systematic review and meta-analysis. J Dermatolog Treat 2016, 27, 316–321. [Google Scholar] [CrossRef]
- Brinch Hyttel, C.; Ghazanfar, M.N.; Zhang, D.G.; Thomsen, S.F.; Ali, Z. The association between psoriasis and chronic obstructive pulmonary disease: a systematic review and meta-analysis. Ital J Dermatol Venerol 2024. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Ke, R.; Shi, W.; Yan, X.; Wang, Q.; Zhang, Q.; Chai, L.; Li, M. Association between psoriasis and asthma risk: A meta-analysis. Allergy Asthma Proc 2018, 39, 103–109. [Google Scholar] [CrossRef]
- Ger, T.Y.; Fu, Y.; Chi, C.C. Bidirectional Association Between Psoriasis and Obstructive Sleep Apnea: A Systematic Review and Meta-Analysis. Sci Rep 2020, 10, 5931. [Google Scholar] [CrossRef]
- Purzycka-Bohdan, D.; Kisielnicka, A.; Zabłotna, M.; Nedoszytko, B.; Nowicki, R.J.; Reich, A.; Samotij, D.; Szczęch, J.; Krasowska, D.; Bartosińska, J.; et al. Chronic Plaque Psoriasis in Poland: Disease Severity, Prevalence of Comorbidities, and Quality of Life. J Clin Med 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Wu, R.; Kong, Y.; Zhao, M.; Su, Y. Impact of smoking on psoriasis risk and treatment efficacy: a meta-analysis. J Int Med Res 2020, 48, 300060520964024. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.; Xiao, S.; Huang, H.; Zhang, Z. Incidence of and Risk Factors for Paradoxical Psoriasis or Psoriasiform Lesions in Inflammatory Bowel Disease Patients Receiving Anti-TNF Therapy: Systematic Review With Meta-Analysis. Front Immunol 2022, 13, 847160. [Google Scholar] [CrossRef] [PubMed]
- Li, W.Q.; Qureshi, A.A.; Schernhammer, E.S.; Han, J. Rotating night-shift work and risk of psoriasis in US women. J Invest Dermatol 2013, 133, 565–567. [Google Scholar] [CrossRef]
- Huang, Y.; Jing, D.; Su, J.; Huang, Z.; Liu, H.; Tao, J.; He, M.; Chen, X.; Shen, M.; Xiao, Y. Association of Night Shift Work With Chronic Spontaneous Urticaria and Effect Modification by Circadian Dysfunction Among Workers. Front Public Health 2021, 9, 751579. [Google Scholar] [CrossRef] [PubMed]
- Cox, K.H.; Takahashi, J.S. Circadian clock genes and the transcriptional architecture of the clock mechanism. J Mol Endocrinol 2019, 63, R93–R102. [Google Scholar] [CrossRef] [PubMed]
- Hastings, M.H.; Maywood, E.S.; Brancaccio, M. Generation of circadian rhythms in the suprachiasmatic nucleus. Nat Rev Neurosci 2018, 19, 453–469. [Google Scholar] [CrossRef]
- Duan, J.; Greenberg, E.N.; Karri, S.S.; Andersen, B. The circadian clock and diseases of the skin. FEBS Lett 2021, 595, 2413–2436. [Google Scholar] [CrossRef]
- Takahashi, J.S. Transcriptional architecture of the mammalian circadian clock. Nat Rev Genet 2017, 18, 164–179. [Google Scholar] [CrossRef]
- Koronowski, K.B.; Kinouchi, K.; Welz, P.S.; Smith, J.G.; Zinna, V.M.; Shi, J.; Samad, M.; Chen, S.; Magnan, C.N.; Kinchen, J.M.; et al. Defining the Independence of the Liver Circadian Clock. Cell 2019, 177, 1448–1462 e1414. [Google Scholar] [CrossRef]
- Sinturel, F.; Gos, P.; Petrenko, V.; Hagedorn, C.; Kreppel, F.; Storch, K.F.; Knutti, D.; Liani, A.; Weitz, C.; Emmenegger, Y.; et al. Circadian hepatocyte clocks keep synchrony in the absence of a master pacemaker in the suprachiasmatic nucleus or other extrahepatic clocks. Genes Dev 2021, 35, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Clarkson-Townsend, D.A.; Everson, T.M.; Deyssenroth, M.A.; Burt, A.A.; Hermetz, K.E.; Hao, K.; Chen, J.; Marsit, C.J. Maternal circadian disruption is associated with variation in placental DNA methylation. PLoS One 2019, 14, e0215745. [Google Scholar] [CrossRef] [PubMed]
- Nemeth, V.; Horvath, S.; Kinyo, A.; Gyulai, R.; Lengyel, Z. Expression Patterns of Clock Gene mRNAs and Clock Proteins in Human Psoriatic Skin Samples. Int J Mol Sci 2021, 23. [Google Scholar] [CrossRef]
- Plikus, M.V.; Van Spyk, E.N.; Pham, K.; Geyfman, M.; Kumar, V.; Takahashi, J.S.; Andersen, B. The circadian clock in skin: implications for adult stem cells, tissue regeneration, cancer, aging, and immunity. J Biol Rhythms 2015, 30, 163–182. [Google Scholar] [CrossRef]
- Ando, N.; Nakamura, Y.; Aoki, R.; Ishimaru, K.; Ogawa, H.; Okumura, K.; Shibata, S.; Shimada, S.; Nakao, A. Circadian Gene Clock Regulates Psoriasis-Like Skin Inflammation in Mice. J Invest Dermatol 2015, 135, 3001–3008. [Google Scholar] [CrossRef] [PubMed]
- Narasimamurthy, R.; Hatori, M.; Nayak, S.K.; Liu, F.; Panda, S.; Verma, I.M. Circadian clock protein cryptochrome regulates the expression of proinflammatory cytokines. Proc Natl Acad Sci U S A 2012, 109, 12662–12667. [Google Scholar] [CrossRef]
- Yu, X.; Rollins, D.; Ruhn, K.A.; Stubblefield, J.J.; Green, C.B.; Kashiwada, M.; Rothman, P.B.; Takahashi, J.S.; Hooper, L.V. TH17 cell differentiation is regulated by the circadian clock. Science 2013, 342, 727–730. [Google Scholar] [CrossRef]
- Yu, Z.; Gong, Y.; Cui, L.; Hu, Y.; Zhou, Q.; Chen, Z.; Yu, Y.; Chen, Y.; Xu, P.; Zhang, X.; et al. High-throughput transcriptome and pathogenesis analysis of clinical psoriasis. J Dermatol Sci 2020, 98, 109–118. [Google Scholar] [CrossRef]
- Chang, C.; Loo, C.S.; Zhao, X.; Solt, L.A.; Liang, Y.; Bapat, S.P.; Cho, H.; Kamenecka, T.M.; Leblanc, M.; Atkins, A.R.; et al. The nuclear receptor REV-ERBalpha modulates Th17 cell-mediated autoimmune disease. Proc Natl Acad Sci U S A 2019, 116, 18528–18536. [Google Scholar] [CrossRef]
- Hirotsu, C.; Rydlewski, M.; Araujo, M.S.; Tufik, S.; Andersen, M.L. Sleep loss and cytokines levels in an experimental model of psoriasis. PLoS One 2012, 7, e51183. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, E.N.; Marshall, M.E.; Jin, S.; Venkatesh, S.; Dragan, M.; Tsoi, L.C.; Gudjonsson, J.E.; Nie, Q.; Takahashi, J.S.; Andersen, B. Circadian control of interferon-sensitive gene expression in murine skin. Proc Natl Acad Sci U S A 2020, 117, 5761–5771. [Google Scholar] [CrossRef] [PubMed]
- Németh, V.; Horváth, S.; Kinyó, Á.; Gyulai, R.; Lengyel, Z. Expression Patterns of Clock Gene mRNAs and Clock Proteins in Human Psoriatic Skin Samples. Int J Mol Sci 2021, 23. [Google Scholar] [CrossRef] [PubMed]
- Karaaslan, C.; Suzen, S. Antioxidant properties of melatonin and its potential action in diseases. Curr Top Med Chem 2015, 15, 894–903. [Google Scholar] [CrossRef]
- Nakao, A.; Nakamura, Y. Time will tell about mast cells: Circadian control of mast cell activation. Allergol Int 2022, 71, 425–431. [Google Scholar] [CrossRef]
- Kartha, L.B.; Chandrashekar, L.; Rajappa, M.; Menon, V.; Thappa, D.M.; Ananthanarayanan, P.H. Serum melatonin levels in psoriasis and associated depressive symptoms. Clin Chem Lab Med 2014, 52, e123–125. [Google Scholar] [CrossRef]
- Tohid, H.; Aleem, D.; Jackson, C. Major Depression and Psoriasis: A Psychodermatological Phenomenon. Skin Pharmacol Physiol 2016, 29, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Scuderi, S.A.; Cucinotta, L.; Filippone, A.; Lanza, M.; Campolo, M.; Paterniti, I.; Esposito, E. Effect of Melatonin on Psoriatic Phenotype in Human Reconstructed Skin Model. Biomedicines 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, S.; Bahakeem, H.; Alkhalifah, A.; Cavalie, M.; Boukari, F.; Montaudie, H.; Lacour, J.P.; Passeron, T. Topical corticosteroids application in the evening is more effective than in the morning in psoriasis: results of a prospective comparative study. J Eur Acad Dermatol Venereol 2017, 31, e263–e264. [Google Scholar] [CrossRef]
- Parisi, R.; Iskandar, I.Y.K.; Kontopantelis, E.; Augustin, M.; Griffiths, C.E.M.; Ashcroft, D.M.; Global Psoriasis, A. National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study. BMJ 2020, 369, m1590. [Google Scholar] [CrossRef]
- Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [CrossRef]
- Lecaros, C.; Dunstan, J.; Villena, F.; Ashcroft, D.M.; Parisi, R.; Griffiths, C.E.M.; Hartel, S.; Maul, J.T.; De la Cruz, C. The incidence of psoriasis in Chile: an analysis of the National Waiting List Repository. Clin Exp Dermatol 2021, 46, 1262–1269. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; Azrielant, S.; Bragazzi, N.L.; Sharif, K.; David, P.; Katz, I.; Aljadeff, G.; Quaresma, M.; Tanay, G.; Adawi, M.; et al. Seasonality and autoimmune diseases: The contribution of the four seasons to the mosaic of autoimmunity. J Autoimmun 2017, 82, 13–30. [Google Scholar] [CrossRef] [PubMed]
- Adawi, M.; Damiani, G.; Bragazzi, N.L.; Bridgewood, C.; Pacifico, A.; Conic, R.R.Z.; Morrone, A.; Malagoli, P.; Pigatto, P.D.M.; Amital, H.; et al. The Impact of Intermittent Fasting (Ramadan Fasting) on Psoriatic Arthritis Disease Activity, Enthesitis, and Dactylitis: A Multicentre Study. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Damiani, G.; Bragazzi, N.L.; Garbarino, S.; Chattu, V.K.; Shapiro, C.M.; Pacifico, A.; Malagoli, P.; Pigatto, P.D.M.; Conic, R.R.Z.; Tiodorovic, D.; et al. Psoriatic and psoriatic arthritis patients with and without jet-lag: does it matter for disease severity scores? Insights and implications from a pilot, prospective study. Chronobiol Int 2019, 36, 1733–1740. [Google Scholar] [CrossRef] [PubMed]
- Bedi, T.R. Psoriasis in North India. Geographical variations. Dermatologica 1977, 155, 310–314. [Google Scholar] [CrossRef]
- Brito, L.D.A.R.; Nascimento, A.C.M.D.; Marque, C.D.; Miot, H.A. Seasonality of the hospitalizations at a dermatologic ward (2007-2017). Anais Brasileiros de Dermatologia 2018, 93, 755–758. [Google Scholar] [CrossRef]
- Ferguson, F.J.; Lada, G.; Hunter, H.J.A.; Bundy, C.; Henry, A.L.; Griffiths, C.E.M.; Kleyn, C.E. Diurnal and seasonal variation in psoriasis symptoms. J Eur Acad Dermatol Venereol 2021, 35, e45–e47. [Google Scholar] [CrossRef] [PubMed]
- Hancox, J.G.; Sheridan, S.C.; Feldman, S.R.; Fleischer, A.B., Jr. Seasonal variation of dermatologic disease in the USA: a study of office visits from 1990 to 1998. Int J Dermatol 2004, 43, 6–11. [Google Scholar] [CrossRef]
- Hellgren, L. Psoriasis. A statistical, clinical and laboratory investigation of 255 psoriatics and matched healthy controls. Acta Derm Venereol 1964, 44, 191–207. [Google Scholar]
- Park, B.S.; Youn, J.I. Factors influencing psoriasis: an analysis based upon the extent of involvement and clinical type. J Dermatol 1998, 25, 97–102. [Google Scholar] [CrossRef]
- Pascoe, V.L.; Kimball, A.B. Seasonal variation of acne and psoriasis: A 3-year study using the Physician Global Assessment severity scale. J Am Acad Dermatol 2015, 73, 523–525. [Google Scholar] [CrossRef]
- Harvell, J.D.; Selig, D.J. Seasonal variations in dermatologic and dermatopathologic diagnoses: a retrospective 15-year analysis of dermatopathologic data. Int J Dermatol 2016, 55, 1115–1118. [Google Scholar] [CrossRef] [PubMed]
- Kubota, K.; Kamijima, Y.; Sato, T.; Ooba, N.; Koide, D.; Iizuka, H.; Nakagawa, H. Epidemiology of psoriasis and palmoplantar pustulosis: a nationwide study using the Japanese national claims database. BMJ Open 2015, 5, e006450. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Xu, Z.; Dan, Y.L.; Zhao, C.N.; Mao, Y.M.; Liu, L.N.; Pan, H.F. Seasonality and global public interest in psoriasis: an infodemiology study. Postgrad Med J 2020, 96, 139–143. [Google Scholar] [CrossRef]
- Mrowietz, U.; Dieckmann, T.; Gerdes, S.; Szymczak, S.; von Spreckelsen, R.; Korber, A. ActiPso: definition of activity types for psoriatic disease: A novel marker for an advanced disease classification. J Eur Acad Dermatol Venereol 2021, 35, 2027–2033. [Google Scholar] [CrossRef]
- Zheng, X.; Wang, Q.; Luo, Y.; Lu, W.; Jin, L.; Chen, M.; Zhu, W.; Kuang, Y. Seasonal Variation of Psoriasis and Its Impact in the Therapeutic Management: A Retrospective Study on Chinese Patients. Clin Cosmet Investig Dermatol 2021, 14, 459–465. [Google Scholar] [CrossRef]
- Jensen, K.K.; Serup, J.; Alsing, K.K. Psoriasis and seasonal variation: A systematic review on reports from Northern and Central Europe-Little overall variation but distinctive subsets with improvement in summer or wintertime. Skin Res Technol 2022, 28, 180–186. [Google Scholar] [CrossRef]
- Air quality in Europe 2022. Available online: https://www.eea.europa.eu/publications/air-quality-in-europe-2022 (accessed on 10th March 2024).
- Theodoridis, X.; Grammatikopoulou, M.G.; Stamouli, E.M.; Talimtzi, P.; Pagkalidou, E.; Zafiriou, E.; Haidich, A.B.; Bogdanos, D.P. Effectiveness of oral vitamin D supplementation in lessening disease severity among patients with psoriasis: A systematic review and meta-analysis of randomized controlled trials. Nutrition 2021, 82, 111024. [Google Scholar] [CrossRef]
- Ford, A.R.; Siegel, M.; Bagel, J.; Cordoro, K.M.; Garg, A.; Gottlieb, A.; Green, L.J.; Gudjonsson, J.E.; Koo, J.; Lebwohl, M.; et al. Dietary Recommendations for Adults With Psoriasis or Psoriatic Arthritis From the Medical Board of the National Psoriasis Foundation: A Systematic Review. JAMA Dermatology 2018, 154, 934–950. [Google Scholar] [CrossRef] [PubMed]
- Ruano, J.; Velez, A.; Casas, E.; Rodriguez-Martin, A.; Salido, R.; Isla-Tejera, B.; Espejo-Alvarez, J.; Gomez, F.; Jimenez-Puya, R.; Moreno-Gimenez, J.C. Factors influencing seasonal patterns of relapse in anti-TNF psoriatic responders after temporary drug discontinuation. J Eur Acad Dermatol Venereol 2014, 28, 516–518. [Google Scholar] [CrossRef]
- Niedźwiedź, M.; Noweta, M.; Narbutt, J.; Owczarek, W.; Ciążyńska, M.; Czerwińska, A.; Krzyścin, J.; Lesiak, A.; Skibińska, M. Does the effectiveness of biological medications in the treatment for psoriasis depend on the moment of starting therapy? A preliminary study. Postepy Dermatol Alergol 2024, 41, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Lane Guy, C.; Crawford, G. Psoriasis: a statistical study of two hundred and thirty-one cases. Archives of Dermatology and Syphilology 1937, 35, 1051–1061. [Google Scholar] [CrossRef]
- Lomholt, G. Psoriasis on the Faroe Islands; a preliminary report. Acta Derm Venereol 1954, 34, 92. [Google Scholar]
- Kononen, M.; Torppa, J.; Lassus, A. An epidemiological survey of psoriasis in the greater Helsinki area. Acta Derm Venereol Suppl (Stockh) 1986, 124, 1–10. [Google Scholar] [PubMed]
- Knopf, B.; Geyer, A.; Roth, H.; Barta, U. [The effect of endogenous and exogenous factors on psoriasis vulgaris. A clinical study]. Dermatol Monatsschr 1989, 175, 242–246. [Google Scholar]
- Kardeş, S. Seasonal variation in the internet searches for psoriasis. Arch Dermatol Res 2019, 311, 461–467. [Google Scholar] [CrossRef]
Figure 1.
Influence of UV-R on the skin. When UV electromagnetic waves reach the skin, a small part of them are reflected, while the majority penetrate the skin and are absorbed by different molecules [68]. UV-B penetrates the skin to a depth of about 0.1 mm and UV-A to a depth of about 0.8 mm [70]. While UV-B is absorbed by most of the molecules within the skin, UV-A is not absorbed by DNA and most proteins but can be absorbed by endogenous porphyrins, oxidized fatty acids, and B vitamins [68,71]. The energy of absorbed UV is converted into heat, fluorescence, and chemical changes in the absorbing molecules causing formation of reactive oxygen species (ROS) such as superoxide anions, singlet oxygen, and hydroxyl radicals [68,71]. ROS can damage DNA components through formation of 8-oxo-guanine [72,73]. Singlet oxygen promotes T-cell apoptosis and mitochondrial DNA deletions, activation of signal transduction by p38, heme oxygenase, and collagenase genes [68,74]. Damaged keratinocytes produce and release several immunomodulators, such as tumor necrosis factors (TNF), 6-formylindolo[3,2-b]carbazole (FICZ), receptor activator of NF-κB ligand (RANKL), platelet- activating factors (PAFs), cis-urocanic acid (cis-UCA), IL-10 [75,76,77]. TNFs, FICZ and RANKL cause activation and migration of Langerhans cells to local lymph nodes [75,76,78,79]. PAFs and cis-UCA induce further release TNFs IL-10 and IL-4 which supports recruiting of cells such as Natural Killers (NKT) cells, regulatory B (Breg) and T (Treg) cells, which promote humoral and cell-mediated immunosuppression [75,80,81,82,83,84]. Figure was created with BioRender.com.
Figure 1.
Influence of UV-R on the skin. When UV electromagnetic waves reach the skin, a small part of them are reflected, while the majority penetrate the skin and are absorbed by different molecules [68]. UV-B penetrates the skin to a depth of about 0.1 mm and UV-A to a depth of about 0.8 mm [70]. While UV-B is absorbed by most of the molecules within the skin, UV-A is not absorbed by DNA and most proteins but can be absorbed by endogenous porphyrins, oxidized fatty acids, and B vitamins [68,71]. The energy of absorbed UV is converted into heat, fluorescence, and chemical changes in the absorbing molecules causing formation of reactive oxygen species (ROS) such as superoxide anions, singlet oxygen, and hydroxyl radicals [68,71]. ROS can damage DNA components through formation of 8-oxo-guanine [72,73]. Singlet oxygen promotes T-cell apoptosis and mitochondrial DNA deletions, activation of signal transduction by p38, heme oxygenase, and collagenase genes [68,74]. Damaged keratinocytes produce and release several immunomodulators, such as tumor necrosis factors (TNF), 6-formylindolo[3,2-b]carbazole (FICZ), receptor activator of NF-κB ligand (RANKL), platelet- activating factors (PAFs), cis-urocanic acid (cis-UCA), IL-10 [75,76,77]. TNFs, FICZ and RANKL cause activation and migration of Langerhans cells to local lymph nodes [75,76,78,79]. PAFs and cis-UCA induce further release TNFs IL-10 and IL-4 which supports recruiting of cells such as Natural Killers (NKT) cells, regulatory B (Breg) and T (Treg) cells, which promote humoral and cell-mediated immunosuppression [75,80,81,82,83,84]. Figure was created with BioRender.com.
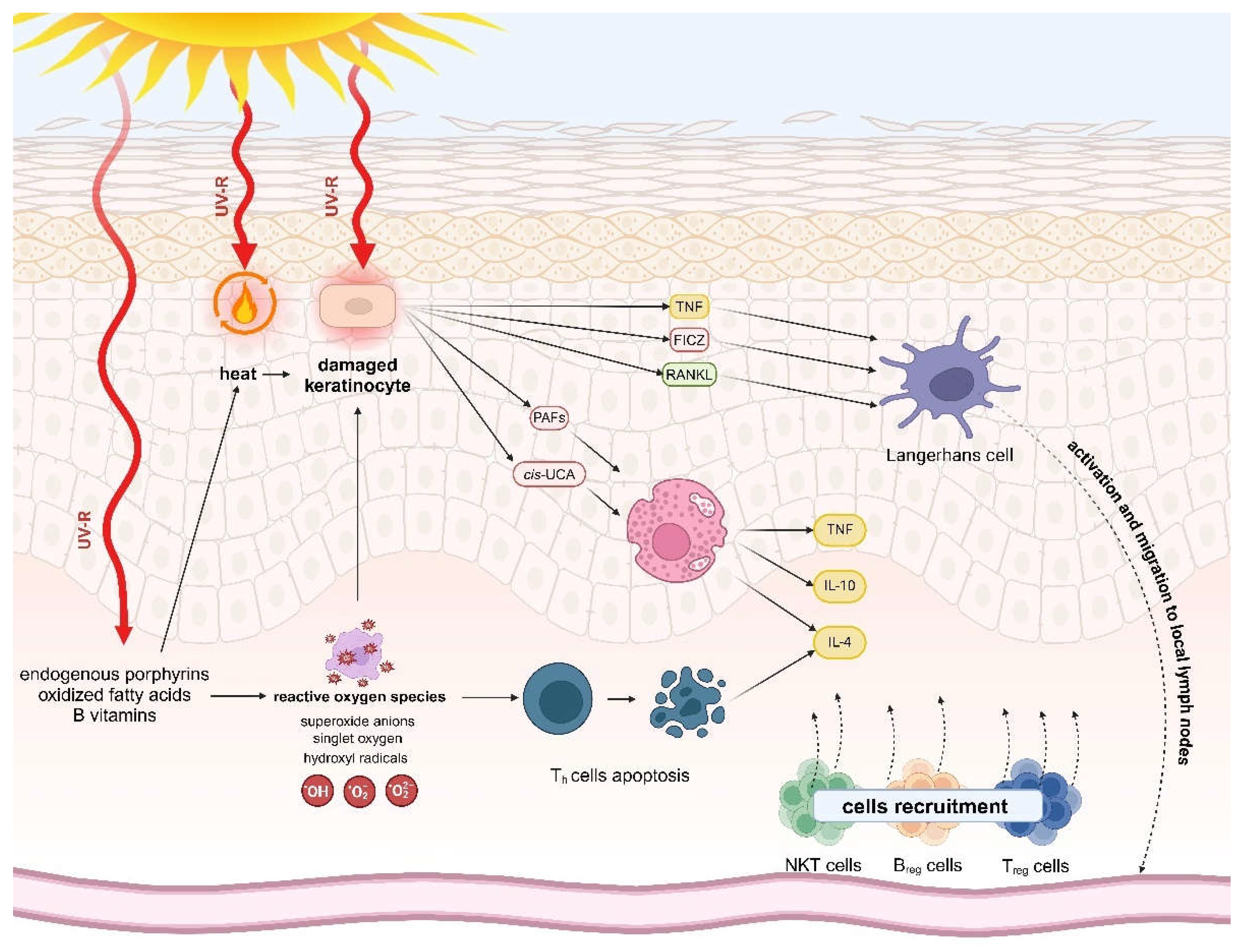
Figure 2.
Relation between environmental factors, genetics background, epigenetic modifications, and inflammatory reactions leading to development of psoriatic skin symptoms. Figure was created with BioRender.com.
Figure 2.
Relation between environmental factors, genetics background, epigenetic modifications, and inflammatory reactions leading to development of psoriatic skin symptoms. Figure was created with BioRender.com.
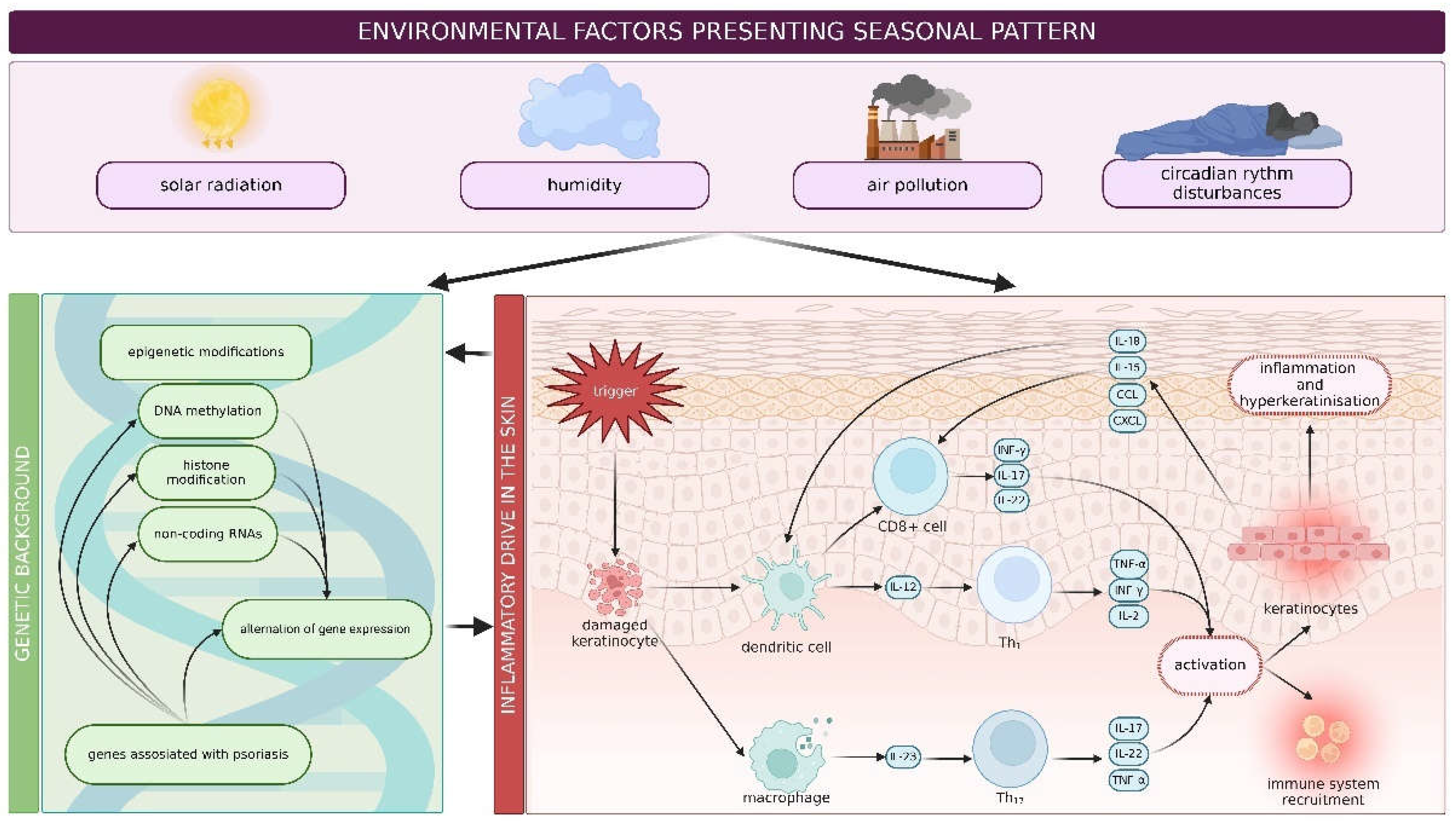
Figure 3.
Factors leading to seasonal pattern of clinical deteriorations and improvements in patients with psoriasis. Figure was created with BioRender.com.
Figure 3.
Factors leading to seasonal pattern of clinical deteriorations and improvements in patients with psoriasis. Figure was created with BioRender.com.
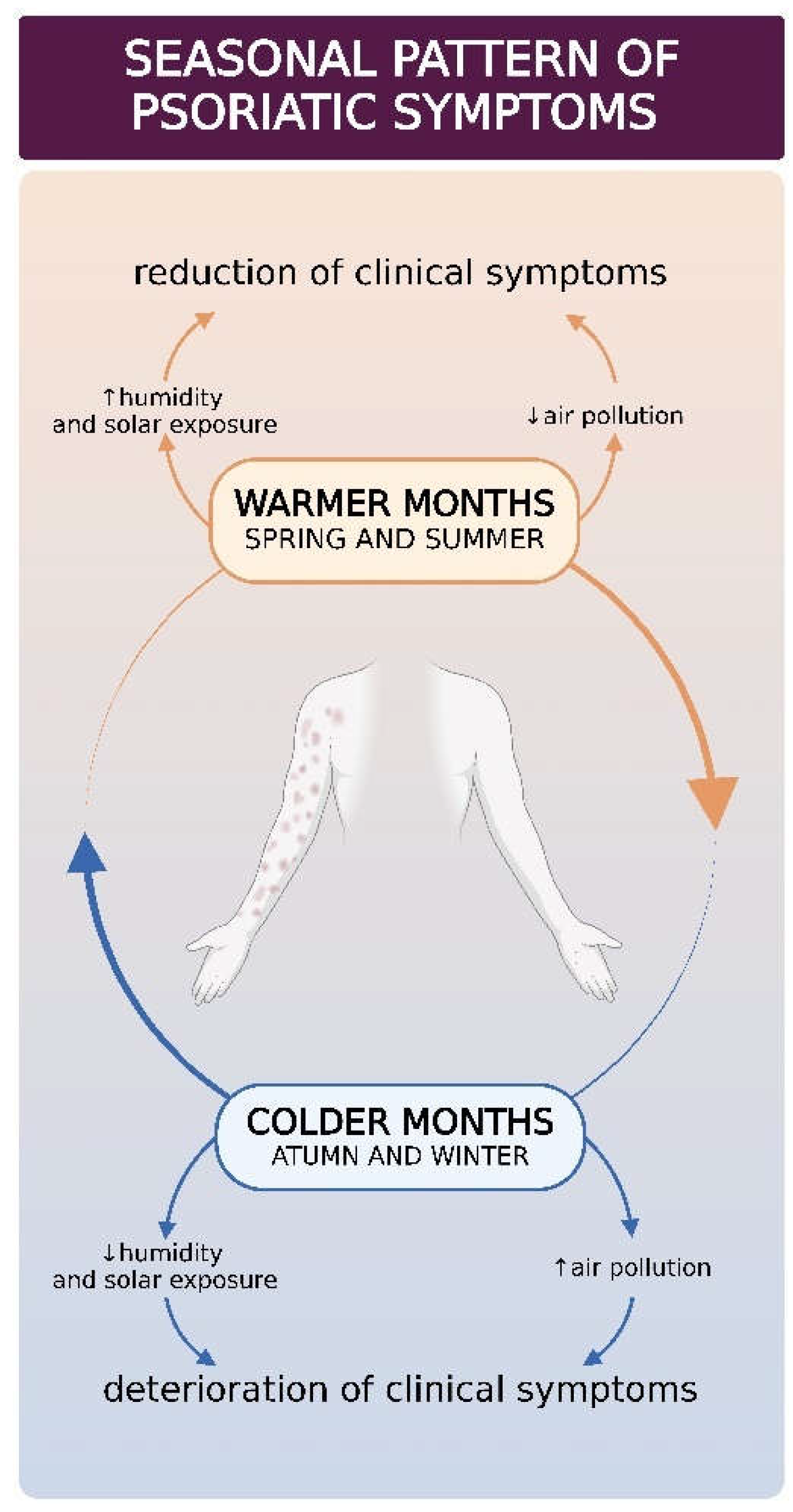

Table 1.
Examples of genes polymorphisms associated with psoriasis and their clinical implications.
| Described polymorphism | Clinical features/implication |
|---|---|
|
HLA-B*27 HLA-B*39 HLA-B*38 HLA-B*08 |
Higher risk of PsA development. |
| HLA-B*08 | Asymmetric sacroiliitis, peripheral arthritis ankylosis, and increased joint damage. |
| HLA-B*27 | Symmetric sacroiliitis, dactylitis and enthesitis development. |
| HLA-C*06:02 | An earlier onset of PsV and a later onset of PsA. Photosensitive psoriasis. |
| CARD14 | Psoriasis and/or features of PRP and GPP. Photosensitive psoriasis. |
|
FTO CALCR AC003006.7 |
PsV associated with obesity. |
Table 1.
Spectrum of Solar radiation.
| Light type | Abbreviation | Wavelength [nm] |
|---|---|---|
| UV-radiation | UV-R | 100-400 |
| UV-C | 100-280 | |
| UV-B | 280-315 | |
| UV-A | 315-400 | |
| UV-A2 | 315-340 | |
| UV-A1 | 340-400 | |
| visible light | VIS | 400-780 |
| infrared radiation | IR | 780-1000 |
Table 1.
Research on seasonality of psoriasis.
| Author(s) | Year of publication | Study design | Region | Number of analysed PsV patients | Conclusion |
|---|---|---|---|---|---|
|
Lane and Crawford [194] |
1937 | retrospective analysis of clinic visits | USA | 231 | Seasonal pattern in 75% of patients. Deterioration of psoriasis in 14.3% of patients in summer, improvement in 60.2% in summer. |
|
Lomholt [195] |
1954 | personal interview by the investigator | Faroe Islands | 206 | Seasonal pattern of psoriasis in about 50% of cases. Patients with seasonal pattern observed deterioration in winter and spring (25% and 52% respectively) and improvement in summer (63%). |
|
Hellgren [180] |
1964 | analysis of inpatients with psoriasis | Sweden | 255 | Seasonal pattern of psoriasis in about 50%. Patients observed improvement in winter and summer (7.9% and 22.6% respectively). |
|
Bedi [176] |
1977 | analysis of outpatients with psoriasis | Northern India | 162 | No seasonal pattern in 54% patients. Twenty-five percent patients reported deterioration in winter and improvement in summer. Twelve percent patients reported improvement in winter and deterioration in summer. |
|
Könönen et al. [196] |
1986 | survey/questionnaires | Finland | 1 517 | Deterioration of psoriasis in 54% of patients in winter, 18% in spring and 2% in summer. |
|
Knopf et al. [197] |
1989 | survey/questionnaires | Germany | 390 | Deterioration of psoriasis in 37.4% of patients in winter, 42.3% in spring; improvement in 60.5% of patients in summer. |
|
Park and Youn [181] |
1998 | survey/questionnaires | South Korea | 870 | Deterioration in winter reported by 65% of patients and no seasonality or improvement reported by 35%. |
|
Hancox [179] |
2004 | retrospective analysis of office visits | USA | no data | No seasonality observed by using astronomical calendar. Significant differences observed by using meteorological calendar with majority of visits in spring. |
|
Kubota et al. [184] |
2015 | statistical analysis of the data in Japanese national database of health insurance claims (JNDB) | Japan | 429 679 | No seasonal pattern observed. |
|
Pascoe and Kimball [182] |
2015 | analysis of dermatologists’ billing sheets based on PGA scores | USA | 5 468 | The percentage of patients with clear/almost clear disease was highest in summer at 20.4% and the lowest in winter at 15.3%. Number of patients with moderate/severe psoriasis was highest in winter at 40.5% and the lowest in summer at 34.1%. |
|
Harvell and Selig [183] |
2016 | retrospective analysis of dermatopathological data | USA | 223 | No seasonal pattern in histopathological diagnosis observed. |
|
Brito [177] |
2018 | retrospective analysis of ward admissions | Brazil | 155 | Twenty-nine percent of admissions of patients with psoriasis in autumn, 27% in winter, 25% in spring and 19% in summer. |
|
Kardeş [198] |
2019 | analysis of Google Trends queries for psoriasis | United States; United Kingdom; Canada; Ireland; Australia; New Zealand | no data | Statistically significant seasonal pattern of searches for psoriasis with peaks in winter/early spring and troughs in summer/early fall. Peaks in late winter/early spring and troughs in late summer/early fall presented approximately with 6-month difference between hemispheres. |
|
Wu [185] |
2020 | analysis of Google Trends queries for psoriasis | Australia, New Zealand, USA, Canada, United Kingdom, Ireland | ND | Significant seasonal pattern for psoriasis, with peaks in late winter/early spring and troughs in late summer/early autumn. |
|
Ferguson et al. [178] |
2020 | cross-sectional online survey | world-wide | 186 | Seventy-seven percent of respondents reported seasonal pattern of psoriasis exacerbation. Deterioration of psoriasis reported by 67.1% of patients in winter, 23.8% in summer, 7% in spring and 2.1% in autumn. |
|
Jensen [188] |
2021 | systematic review | Northern and Central Europe | 12 900 | Thirteen publications: nine published before 1958 and including four reported above (Lomholt, Hellgren, Könönen et al, Knopf et al.). No seasonality in 50% of patients. Approximately 30% improved in summer, and 20% performed better in winter. |
|
Purzycka-Bohdan et al. [142] |
2022 | national survey study | Poland | 1080 | Seasonal changes were reported by 45.09% to have a considerable impact on the psoriasis disease course. |
|
Liang et al. [118] |
2023 | retrospective ecological study of individuals with psoriasis identified in the Optum Clinformatics Data Mart. | USA | 74 960 | The initiation of the treatment peaked in spring months, followed by the summer, fall and winter. Discontinuation of biologic drugs peaked in summer, and switching of biologics was highest in spring. Season was associated with initiation, discontinuation, and switching, although seasonality pattern is less clear for nonbiologic systemic drugs. |
|
Niedźwiedź et al. [193] |
2024 | retrospective analysis of patients treated with biologics depend on starting point of the therapy | Poland | 62 | Seasonality appeared in the effectiveness of IL12/23 and IL17 inhibitors therapy in moderate to severe psoriasis with better results obtained within first months of treatment in patients starting therapy in the warm period of the year (May-September). No seasonality was observed in patients treated with TNF-α inhibitors. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



