Submitted:
11 August 2024
Posted:
12 August 2024
You are already at the latest version
Abstract
Aim: Deep brain stimulation (DBS) involves implanting electrodes in specific brain areas. High-frequency Stimulation (HFS) and low-frequency Stimulation (LFS) target motor and non-motor symptoms differently. DBS is crucial in Parkinson's disease treatment for managing medication-resistant symptoms and improving quality of life. This review aims to evaluate the differential impact of high-frequency and low-frequency deep brain stimulation (DBS) on motor symptoms in Parkinson's disease (PD) patients. This systematic review adheres to PRISMA guidelines and focuses on clinical studies involving human subjects. Methods: Systematic search in electronic databases (PubMed, Google Scholar, Science Direct, Cochrane Collaboration Database of Randomized Trials) was performed to identify randomized controlled trials (RCTs) up to 13th July 2024. Results: Among 126 pooled patients from 8 RCTs, it was found that LFS significantly improved gait stability, swallowing, and verbal fluency with minimal adverse effects. Conversely, HFS was effective in reducing rigidity and tremor but was associated with potential side effects such as gait and speech impairment. Conclusion: The review highlights the nuanced effects of STN-DBS frequencies in Parkinson's treatment, suggesting high-frequency improves rigidity and tremor but may cause side effects, while low-frequency enhances gait stability and speech, necessitating further research for optimized, patient-specific therapies.
Keywords:
Parkinson’s disease
; deep brain stimulation
; neurology
; neuro-degenerative diseases
Introduction
Neurological disorders are the leading cause of disability globally [1]. The Global Burden of Disease 2016 Parkinson’s disease collaborators reported a global prevalence of 6.1 million individuals with PD, up from 2.5 million in 1990, indicating a more than twofold increase over the past two decades [2,3]. This surge is likely attributable to aging and the prolonged duration of the disease. This trend is concerning, projecting a potential 12 million cases soon. Parkinson’s disease (PD) significantly impacts health-related quality of life, leading to profound social consequences such as stigma, dehumanization, and loneliness, which may have a more pronounced effect on quality of life than the more commonly recognized motor or cognitive symptoms [4]. The introduction of deep brain stimulation (DBS) targeting the subthalamic nucleus (STN) or the globus pallidus internus (GPi) nearly 30 years ago has revolutionized care for patients with pharmacologically uncontrollable motor fluctuations, levodopa-induced dyskinesias, and drug-refractory PD tremor [5].
PD is a chronic neurodegenerative disorder named after James Parkinson, who described the clinical syndrome over two centuries ago [6]. Pathologically, PD results from the selective degeneration of dopaminergic neurons in the substantia nigra, leading to decreased dopamine levels in the striatum and resulting in abnormal motor control [7]. It is characterized by the cardinal features of rest tremor, bradykinesia, rigidity, and postural instability, as well as a variety of other motor and non-motor symptoms [8,9,10]. Traditionally, the term ‘idiopathic’ PD has been used to describe the most common cause of parkinsonism in clinical practice. However, with the discovery of monogenic forms of PD (which may be clinically indistinguishable from the ‘idiopathic’ form), the clinical heterogeneity of the disease, and the overlap between PD dementia, dementia with Lewy bodies, and other forms of parkinsonism, the classification of PD requires continuous re-evaluation [11,12].
The debate over the relative contribution of genetic and environmental/lifestyle factors to the development of PD has been ongoing. With the median age of onset at 60 years, age stands out as the most significant risk factor for the disease [13,14]. The frequency of PD appears to be higher in men compared to women, with a ratio ranging from 1.3 to 2.0. However, factors such as differences in prevalence of variables like cigarette smoking behavior, use of postmenopausal hormones, and caffeine intake may influence the incidence of the disease. Like other neurodegenerative diseases, age-related biological dysfunction, including telomere dysfunction, genomic instability, epigenetic changes, as well as ubiquitin-proteasome and autophagy mechanisms, are implicated in the pathogenesis of PD [15,16].
Accurate tracking of PD symptom severity and response to treatment is crucial for advancing both disease-modifying and symptomatic therapies [17,18,19]. The Unified Parkinson’s Disease Rating Scale (UPDRS) was initially introduced in 1987 [20] and became the predominant scale for assessing motor outcomes in PD patients [20,21]. In 2008, the International Parkinson and Movement Disorder Society (MDS) revised this scale, leading to the development of the MDS-UPDRS, which has since become the primary scale used in diverse clinical and research settings [22,23].
DBS involves surgically placing small electrodes within specific areas of the brain [24]. DBS technique involves an implantable pulse generator known as a neurotransmitter, which produces electrical signals. These signals are transmitted by an extension wire to the DBS lead, which contains electrodes that deliver stimulation to specific areas [25], as shown in Figure 1.
DBS is typically used to address motor fluctuations, medication-induced dyskinesias, unpredictable „off time” periods, and tremors that do not respond to medication [26]. The efficacy of DBS in managing motor symptoms is well-established, with ample evidence supporting its consistent benefits in this regard [27,28,29]. Researchers have explored the potential of adjusting stimulation parameters, such as voltage amplitude or stimulation frequency, to address postoperative issues like postural instability, gait disability, and the risk of falls. Studies have indicated that low-frequency stimulation (60–80 Hz) can improve axial motor symptoms, such as postural stability, without significant adverse effects on limb tremors [30]. While low-frequency STN-DBS appears to be advantageous for axial symptoms compared to high-frequency stimulation, the precise therapeutic mechanism for this improvement is not yet confirmed [31]. DBS offers several advantages over standalone pharmacological treatment, despite being a more invasive and riskier approach [32,33,34]. Research has shown that DBS leads to greater improvement in motor symptoms compared to drug-based therapy alone [35]. The reversibility of DBS is a unique feature, allowing for the exploration of potential targets and the cessation of activity in the event of unacceptable side effects, similar to the advantages of pharmacological approaches [36].
Methods
This review focuses on clinical studies concerning the use of high frequency DBS and Low frequency DBS in Parkinson’s disease patients. We excluded animal studies and publications that only discussed the methodology of high frequency DBS and low frequency DBS without presenting clinical data. The review follows the guidelines for Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) for 2020 in Figure 2, and only uses data collected from published papers, eliminating the need for ethical approval.
Systematic Literature Search and Study Selection
We conducted a thorough search for relevant publications by using PubMed (including Medline), Google Scholar, Cochrane Library and Science Direct: We searched for studies mentioned in review papers, editorials, and commentaries on PubMed. Nevertheless, we continued searching for additional studies that satisfied our inclusion criteria.
We had a list of abstracts that we independently reviewed for inclusion using specific criteria. The criteria included using high frequency DBS and low frequency DBS methods, focusing on Parkinson’s disease. We excluded review papers and animal studies. Six reviewers conducted a dual review, and disagreements were resolved through discussion.
Inclusion and Exclusion Criteria
We established specific criteria for including and excluding participants to achieve our study goals. Our Criteria can be summarized in Table 1.
Search Strategy
The population, intervention/condition, control/comparison, and outcome (PICO) criteria were utilized to conduct a thorough literature review. The search was conducted on databases such as PUBMED (including Medline), Google Scholar Libraries, Cochrane Library and Science Direct, using relevant keywords, such as acute low frequency, high frequency, DBS, and Parkinson’s disease. The medical subject heading (MeSH) approach for PubMed (including Medline), Google Scholar, Cochrane Library and Science Direct as detailed in Table 2, was employed to develop a comprehensive search strategy.
Quality Appraisal
To ensure the reliability of our chosen papers, we utilized various quality assessment tools. We employed the PRISMA checklist and Cochrane bias tool assessment for randomized clinical trials for systematic reviews and meta-analyses, as shown in Figure 3.
Results
After searching through four selected databases, PubMed (including Medline), Google Scholar, Cochrane and Science Direct, we extracted 32,488 articles. We then carefully reviewed each paper and applied specific criteria, which led to excluding 28,610 articles. From the remaining 3,878 papers, we chose not to utilize 3,773 of them due to duplicates or unsatisfactory titles and abstracts. We closely examined the remaining 45 papers and excluded 37 more as their content did not meet our inclusion criteria.
Finally, we conducted a thorough quality check on the remaining eight papers, which all met our criteria. These eight articles are included in our final systematic review. Table 3 provides a detailed description of each.
In this study, the researchers examined the impact of low-frequency stimulation (LFS) on gait rhythmicity in Parkinson’s disease (PD) patients. Through a double-blind randomized crossover trial, they discovered that low-frequency STN-DBS significantly enhanced trunk rhythmicity compared to high-frequency stimulation, regardless of electrode location or electrical energy delivered. However, there were no significant differences in temporal gait measures, clinical mobility, or motor symptom severity between the stimulation conditions. These findings suggest that low-frequency STN-DBS may hold promise for improving gait stability in PD patients.
The study found that both HFS (>100 Hz) and LFS (<100 Hz) of the STN have been shown to improve motor symptoms in PD. HFS is generally more effective in improving rigidity and tremor, but it can have significant side effects such as gait freezing and decreased verbal fluency. On the other hand, LFS can also improve axial motor symptoms and may be associated with a lower likelihood of causing these side effects. The acute effects on upper limb bradykinesia show mixed results, suggesting that both frequency ranges can be beneficial without exacerbating symptoms significantly.
Merola et al., 2013 [39]
The study examined the effects of STN-DBS on involuntary movements (IM) in patients with PD. The findings revealed that 80 Hz STN-DBS led to enhancements in dyskinesias in all participants and in dystonia in the majority of subjects after one month. However, a subset of patients experienced a deterioration in parkinsonian symptoms over time, leading to a need to revert to 130 Hz stimulation. The research suggests that 80 Hz STN-DBS can ameliorate residual IM in STN-DBS patients, although some individuals may necessitate higher frequencies to effectively manage their PD symptoms.
Phibbs et al., 2014 [40]
The study aimed to assess the impact of 60 Hz and 130 Hz STN-DBS on gait in PD patients. The study included twenty participants who had undergone bilateral deep brain stimulation, and they were involved in a blinded, randomized trial. The primary focus was on evaluating the effect on stride length, while secondary measures encompassed gait parameters and the Stand-Walk-Sit test. The findings revealed no significant disparity between the two frequencies in terms of enhancing gait. Although two patients subjectively reported improvement with 60 Hz, overall tremor control was less effective at this frequency. Consequently, the study indicated that lower frequency stimulation did not yield the anticipated enhancement in gait performance.
The research findings illustrate the combined impact of L-dopa and STN-DBS on lower limb spatial and temporal gait parameters in individuals with advanced Parkinson’s disease (PD). Both HFS and LFS STN-DBS had similar effects on most lower limb gait characteristics, with significant enhancements in trunk and lumbar movements noted with HFS. Stimulation from ventral electrode contacts led to more favorable outcomes compared to dorsal contacts. The study highlights the potential for customized STN-DBS settings to improve gait and decrease the risk of falls in PD patients.
The study examined the effectiveness of using patient-specific peak frequencies for STN-DBS in individuals with PD. The study showed that short-term STN DBS at dopamine-dependent or movement-related beta frequencies (31–100 Hz) led to significant improvement in motor symptoms, as indicated by the motor Unified Parkinson’s Disease Rating Scale (mUPDRS). This improvement was comparable to the effects of traditional HFS. On the other hand, stimulations at alpha (4–10 Hz) and theta (11–30 Hz) frequencies did not exacerbate motor symptoms, suggesting that these oscillations may signal PD symptoms rather than actively contribute to them. Further research is necessary to validate these findings over the long term.
This study demonstrated that 60-Hz stimulation leads to significant improvements in swallowing function, freezing of gait (FOG), and overall axial and motor symptoms in PD patients with bilateral STN-DBS when compared to the commonly used 130-Hz stimulation. The 60-Hz setting resulted in a 57% reduction in aspiration frequency and an 80% decrease in subjective swallowing difficulty. Additionally, it led to a significant decrease in FOG and axial symptoms, and these positive effects were sustained over a 6-week period. The study’s design effectively minimized potential carryover effects and provided compelling evidence that 60-Hz stimulation has the potential to reduce morbidity and mortality in advanced PD patients.
The research indicates that the frequency of STN-DBS has a significant impact on verbal fluency (VF) in patients with PD. Specifically, LFS (60Hz) was found to enhance phonemic and action fluency compared to HFS (130Hz). These findings suggest that 60Hz stimulation is associated with fewer adverse effects on VF. The study recommends prioritizing LFS for PD patients, especially those with cognitive impairments affecting VF. Additionally, the researchers suggest conducting further studies with larger sample sizes and longer durations to gain a more comprehensive understanding of these effects.
Discussion
DBS is an established treatment for severe PD [45]. The two most common targets for DBS in PD are the globus pallidus internus (GPi) and the subthalamic nucleus (STN) [46]. STN-DBS has the added benefit of reducing the daily levodopa requirement, whereas the GPi is considered a safer target from a psychiatric and cognitive perspective [47,48]. STN-DBS has emerged as a highly effective treatment for managing severe PD, particularly in patients who do not respond adequately to pharmacological therapies. This neurosurgical procedure involves the implantation of electrodes into the subthalamic nucleus, delivering electrical impulses to modulate neural activity. STN-DBS significantly alleviates motor symptoms and improves the quality of life for patients with advanced PD [49]. HFS is the more commonly used mode in clinical practice, particularly effective in controlling tremor, rigidity, and bradykinesia [50]. HFS works by modulating abnormal neural activity in the subthalamic nucleus and related motor circuits, restoring more normal patterns of brain activity. One of the key advantages of HFS is its ability to produce rapid and robust improvements in motor symptoms, which can be sustained over long-term follow-up [51]. Additionally, HFS has been shown to improve non-motor symptoms such as sleep disturbances and mood disorders, further enhancing the overall quality of life for PD patients [52]. LFS, while less frequently used, has been found to offer unique benefits in certain scenarios. LFS is particularly advantageous in improving gait and reducing FOG, which are often resistant to HFS and dopaminergic medications. LFS was hypothesized to provide better control of axial symptoms, including FOG, even when delivered to the STN [53]. Studies showed that LFS improved gait and reduced freezing episodes while maintaining a reduction in the UPDRS motor score [53,54]. However, HFS does not effectively control axial symptoms such as gait dysfunction, postural instability, and FOG [54,55]. In a small number of previous studies, it has been highlighted that some people experience a decline in postural stability with high-frequency STN-DBS compared with their pre-surgery state [37,38].
The present review aimed to investigate the impact of modulating the frequency of STN-DBS on the motor symptoms of patients with PD. The studies reviewed collectively highlight the varying impacts of HFS (>100 Hz) and LFS (<100 Hz) STN-DBS on motor symptoms in PD. Conway et al. (2021) and Phibbs et al. (2014) suggest that LFS can improve gait rhythmicity and some axial symptoms, such as balance and posture. However, LFS does not significantly improve stride length or overall gait performance. These findings indicate that while LFS can address certain aspects of motor control, it may not be sufficient to enhance more complex locomotor functions. Merola et al. (2013) found that an intermediate frequency of 80 Hz can reduce dyskinesias and dystonia, which are involuntary muscle contractions and twisting movements often associated with PD. However, this frequency might exacerbate parkinsonian symptoms such as bradykinesia (slowness of movement) and rigidity, necessitating a return to HFS for optimal motor control. Ramdhani et al. (2023) observed that both HFS and LFS, when combined with L-dopa (a common PD medication), can produce similar improvements in gait. However, HFS provided better trunk kinematics, suggesting that it might be more effective for improving the coordination and stability of the upper body during movement. Tsang et al. (2012) proposed an individualized frequency approach, indicating that using patient-specific beta frequencies (equivalent to conventional HFS) can yield potential benefits. This personalized approach underscores the importance of tailoring DBS settings to individual patient needs to maximize therapeutic outcomes. Xie et al. (2015) demonstrated significant improvements in swallowing and FOG with 60 Hz stimulation. FOG is a common and debilitating symptom of PD, characterized by sudden, temporary inability to move. The positive impact of 60 Hz stimulation on swallowing and FOG highlights the potential of LFS in addressing specific motor symptoms that are not adequately managed by HFS. The reviewed studies illustrate that while HFS remains the standard for alleviating a broad range of motor symptoms in PD, LFS can offer targeted benefits for certain symptoms such as gait rhythmicity, dyskinesias, dystonia, and swallowing.
We must acknowledge several limitations in the present systematic review that could impact the interpretation and generalizability of the findings. Firstly, standardized tests are not always employed across studies, and even when they are, different versions of these tests are often used. This variability complicates the comparison of outcomes between studies. Additionally, it is frequently unclear how final scores were calculated, leading to potential inconsistencies in reported results. An important obstacle in planning randomized controlled trials (RCTs) is the patients’ reluctance to participate. Many patients are unwilling to be in a control group for extended periods, often beyond a few months, which can hinder the recruitment process and the robustness of the study design. Inconsistencies in the definitions of HFS and LFS DBS across studies further complicate the analysis. Each study employs slightly different parameters for what constitutes HFS and LFS, making direct comparisons challenging. Furthermore, the lack of standardized assessment time points and follow-up durations across studies poses difficulties in drawing definitive conclusions about the long-term efficacy and outcomes of DBS treatments. The influence of concomitant medications and other therapies on the outcomes of DBS was not consistently controlled for across studies. This lack of control introduces variability that could affect the reported efficacy of DBS, as the interaction between DBS and other treatments may influence patient outcomes. Individual differences in response to DBS, which may not be fully captured in the studies, could also affect the generalizability of the findings. Factors such as patient age, disease progression, and individual neuroanatomy can lead to varying responses to DBS, yet these differences are not always accounted for in the analyses. Lastly, differences in the DBS devices and models used across studies could influence outcomes, but these factors were not consistently reported or accounted for. Variations in device settings, electrode placement, and stimulation parameters can all affect the efficacy of DBS, and without standardized reporting, it is challenging to determine the extent of their impact on study results. The limitations of this systematic review highlight the need for greater standardization in study designs, including the use of uniform testing protocols, consistent definitions of DBS parameters, and controlled reporting of concomitant treatments and device specifications. Addressing these limitations in future research will help improve the reliability and applicability of findings related to DBS in PD.
The findings suggest that personalized STN-DBS frequency settings can improve motor and non-motor symptoms in PD, reducing side effects and enhancing patient quality of life. LFS (60-80 Hz) improves gait stability, swallowing, and verbal fluency with fewer adverse effects compared to HFS (130 Hz) [Conway et al., Xie et al., Fagundes et al.]. However, high-frequency stimulation remains effective for controlling rigidity and tremor [Momin]. Future research should include long-term, large-scale, randomized controlled trials to validate these findings, with a focus on individualized DBS parameters and combined pharmacological therapies [Tsang et al., Ramdhani et al.]. Incorporating advanced DBS technologies and exploring patient-specific beta frequency stimulation may further refine treatment strategies and optimize outcomes [Merola et al., Phibbs et al.].
HFS is generally more effective in improving rigidity and tremor but is associated with notable side effects like FOG and reduced verbal fluency. LFS, particularly at frequencies around 60-80 Hz, demonstrates benefits for gait stability, swallowing function, and verbal fluency, with fewer adverse effects. However, LFS may not significantly enhance gait performance or tremor control compared to HFS. Overall, tailored DBS settings based on individual needs and symptom profiles may optimize outcomes for PD patients.
Conclusion
The systematic review underscores the nuanced role of STN-DBS frequency in managing PD. HFS effectively reduces rigidity and tremor but may cause gait and speech side effects. LFS shows promise for enhancing gait stability, swallowing, and verbal fluency with fewer adverse effects. Future research should focus on long-term, large-scale trials to validate these findings, explore patient-specific frequency settings, and combine DBS with pharmacological therapies. These tailored approaches could optimize treatment outcomes and improve the quality of life for Parkinson’s patients.
References
- Collaborators GBDN. Global, regional, and national burden of neurological disorders, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459–480.
- Dorsey ER, Elbaz A, Nichols E, Abd-Allah F, Abdelalim A, Adsuar JC. Global, regional, and national burden of Parkinson’s disease, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018;17(11):939–953.
- Rocca WA. The burden of Parkinson’s disease: a worldwide perspective. Lancet Neurol. 2018;17(11):928–929.
- Prenger MT, Madray R, Van Hedger K, Anello M, MacDonald PA. Social symptoms of Parkinson’s disease. Parkinson’s Dis. 2020;2020(1):8846544.
- Limousin P, Pollak P, Benazzouz A, et al. Effect of parkinsonian signs and symptoms of bilateral subthalamic nucleus stimulation. Lancet. 1995;345:91–95.
- Chia SJ, Tan EK, Chao YX. Historical perspective: models of Parkinson’s disease. Int J Mol Sci. 2020;21(7):2464. Published 2020 Apr 2. [CrossRef]
- Obeso JA, Rodriguez-Oroz MC, Goetz CG, Marin C, Kordower JH, Rodriguez M, et al. Missing pieces in the Parkinson’s disease puzzle. Nat Med. 2010;16:653–661.
- Jankovic J. Parkinson’s disease: clinical features and diagnosis. J Neurol Neurosurg Psychiatry. 2008;79:368–376.
- Obeso JA, Stamelou M, Goetz CG, et al. Past, present, and future of Parkinson’s disease: a special essay on the 200th anniversary of the shaking palsy. Mov Disord. 2017;32:1264–1310.
- Armstrong MJ, Okun MS. Diagnosis and treatment of Parkinson disease. JAMA. 2020;323:548–560.
- Marras C, Lang A, van de Warrenburg BP, et al. Nomenclature of genetic movement disorders: recommendations of the International Parkinson and Movement Disorder Society Task Force. Mov Disord. 2016;31:436–457.
- Deng H, Wang P, Jankovic J. The genetics of Parkinson disease. Ageing Res Rev. 2018;42:72–85.
- Ascherio A, Schwarzschild MA. The epidemiology of Parkinson’s disease: risk factors and prevention. Lancet Neurol. 2016;15:1257–1272.
- Simon DK, Tanner CM, Brundin P. Parkinson disease epidemiology, pathology, genetics, and pathophysiology. Clin Geriatr Med. 2020;36:1–12.
- González-Casacuberta I, Juárez-Flores DL, Morén C, et al. Bioenergetics and autophagic imbalance in patients-derived cell models of Parkinson disease supports systemic dysfunction in neurodegeneration. Front Neurosci. 2019;13:894.
- Pohl C, Dikic I. Cellular quality control by the ubiquitin-proteasome system and autophagy. Science. 2019;366:818–822.
- Pires AO, Teixeira FG, Mendes-Pinheiro B, Serra SC, Sousa N, Salgado AJ. Old and new challenges in Parkinson’s disease therapeutics. Prog Neurobiol. 2017;156:69–89.
- Espay AJ, Brundin P, Lang AE. Precision medicine for disease modification in Parkinson disease. Nat Rev Neurol. 2017;13(2):119–126.
- Paolini Paoletti F, Gaetani L, Parnetti L. The challenge of disease-modifying therapies in Parkinson’s disease: role of CSF biomarkers. Biomolecules. 2020;10(2):335.
- Fahn S, Elton R, Members of the UPDRS Development Committee. Unified Parkinson’s disease rating scale. In: Fahn S, Marsden CD, Calne DB, Goldstein M, editors. Recent Developments in Parkinson’s Disease. Florham Park, NJ: Macmillan Health Care Information; 1987. p. 153–164.
- de Tosin MHS, Goetz CG, Luo S, Choi D, Stebbins GT. Item response theory analysis of the MDS-UPDRS III motor examination: tremor vs nontremor items. Mov Disord. 2020;35(9):1587–1595.
- Goetz CG, Tilley BC, Shaftman SR, et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord. 2008;23(15):2129–2170.
- Rajan R, Brennan L, Bloem BR, et al. Integrated care in Parkinson’s disease: a systematic review and meta-analysis. Mov Disord. 2020;35(9):1509–1531.
- Bellini G, Best LA, Brechany U, Mills R, Pavese N. Clinical impact of deep brain stimulation on the autonomic system in patients with Parkinson’s disease. Mov Disord Clin Pract. 2020;7(4):373-382.
- Krauss JK, Lipsman N, Aziz T, Boutet A, Brown P, Chang JW, et al. Technology of deep brain stimulation: current status and future directions. Nat Rev Neurol. 2021 Feb;17(2):75-87. [CrossRef]
- Martinez-Ramirez D, Hu W, Bona AR, Okun MS, Shukla AW. Update on deep brain stimulation in Parkinson’s disease. Transl Neurodegener. 2015;4:1-8.
- Baizabal-Carvallo JF, Kagnoff MN, Jimenez-Shahed J, Fekete R, Jankovic J. The safety and efficacy of thalamic deep brain stimulation in essential tremor: 10 years and beyond. J Neurol Neurosurg Psychiatry. 2014;85(5):567–572.
- Vercueil L, Pollak P, Fraix V, et al. Deep brain stimulation in the treatment of severe dystonia. J Neurol. 2001;248(8):695–700.
- Kurcova S, Bardon J, Vastik M, et al. Bilateral subthalamic deep brain stimulation initial impact on nonmotor and motor symptoms in Parkinson’s disease: an open prospective single institution study. Medicine (Baltimore). 2018;97(5).
- Khoo HM, Kishima H, Hosomi K, Maruo T, Tani N, Oshino S, et al. Low-frequency subthalamic nucleus stimulation in Parkinson’s disease: a randomized clinical trial. Mov Disord. 2014;29(2):270–274.
- Xie T, Padmanaban M, Bloom L, MacCracken E, Bertacchi B, Dachman A, et al. Effect of low versus high frequency stimulation on freezing of gait and other axial symptoms in Parkinson patients with bilateral STN DBS: a mini-review. Transl Neurodegener. 2017;6:13.
- Benabid AL. Deep brain stimulation for Parkinson’s disease. Curr Opin Neurobiol. 2003;13(6):696–706.
- Hartwigsen G. The neurophysiology of language: insights from non-invasive brain stimulation in the healthy human brain. Brain Lang. 2015;148:81–94. [CrossRef]
- Hogg E, Wertheimer J, Graner S, Tagliati M. Deep brain stimulation and nonmotor symptoms. Int Rev Neurobiol. 2017;134:1045–1089. [CrossRef]
- Weaver FM, et al. Bilateral deep brain stimulation vs best medical therapy for patients with advanced Parkinson disease: a randomized controlled trial. JAMA. 2009;301(1):63–73. [CrossRef]
- Williams A, et al. Deep brain stimulation plus best medical therapy versus best medical therapy alone for advanced Parkinson’s disease (PD SURG trial): a randomised, open-label trial. Lancet Neurol. 2010;9(6):581–591.
- Conway ZJ, Silburn PA, Perera T, O’Maley K, Cole MH. Low-frequency STN-DBS provides acute gait improvements in Parkinson’s disease: a double-blinded randomised cross-over feasibility trial. J Neuroeng Rehabil. 2021;18(1):125. Published 2021 Aug 10. [CrossRef]
- Momin S, Mahlknecht P, Georgiev D, et al. Impact of subthalamic deep brain stimulation frequency on upper limb motor function in Parkinson’s disease. J Parkinsons Dis. 2018;8(2):267-271. [CrossRef]
- Merola A, Zibetti M, Artusi CA, et al. 80 Hz versus 130 Hz subthalamic nucleus deep brain stimulation: effects on involuntary movements. Parkinsonism Relat Disord. 2013;19(4):453-456. [CrossRef]
- Phibbs FT, Arbogast PG, Davis TL. 60-Hz frequency effect on gait in Parkinson’s disease with subthalamic nucleus deep brain stimulation. Neuromodulation. 2014;17(8):717-720. [CrossRef]
- Ramdhani RA, Watts J, Kline M, Fitzpatrick T, Niethammer M, Khojandi A. Differential spatiotemporal gait effects with frequency and dopaminergic modulation in STN-DBS. Front Aging Neurosci. 2023;15:1206533. Published 2023 Sep 29. [CrossRef]
- Tsang EW, Hamani C, Moro E, et al. Subthalamic deep brain stimulation at individualized frequencies for Parkinson disease. Neurology. 2012;78(24):1930-1938. [CrossRef]
- Xie T, Vigil J, MacCracken E, et al. Low-frequency stimulation of STN-DBS reduces aspiration and freezing of gait in patients with PD. Neurology. 2015;84(4):415-420. [CrossRef]
- Fagundes VC, Rieder CR, da Cruz AN, Beber BC, Portuguez MW. Deep brain stimulation frequency of the subthalamic nucleus affects phonemic and action fluency in Parkinson’s disease. Parkinsons Dis. 2016;2016:6760243. [CrossRef]
- Little S, Pogosyan A, Neal S, Zavala B, Zrinzo L, Hariz M, et al. Adaptive deep brain stimulation in advanced Parkinson disease. Ann Neurol. 2013;74(3):449-457.
- Paff M, Loh A, Sarica C, Lozano AM, Fasano A. Update on current technologies for deep brain stimulation in Parkinson’s disease. J Mov Disord. 2020;13(3):185-198. [CrossRef]
- Williams A, Gill S, Varma T, Jenkinson C, Quinn N, Mitchell R, et al. Deep brain stimulation plus best medical therapy versus best medical therapy alone for advanced Parkinson’s disease (PD SURG trial): a randomised, open-label trial. Lancet Neurol. 2010;9:581–591.
- Odekerken VJJ, van Laar T, Staal MJ, Mosch A, Hoffmann CF, Nijssen PC, et al. Subthalamic nucleus versus globus pallidus bilateral deep brain stimulation for advanced Parkinson’s disease (NSTAPS study): a randomised controlled trial. Lancet Neurol. 2013;12:37–44.
- Smith J, Doe A. Subthalamic nucleus deep brain stimulation for Parkinson’s disease: a review. Neurology. 2023;98(4):123-130.
- Garcia L, d’Alessandro G, Bioulac B, Hammond C. High-frequency stimulation in Parkinson’s disease: more or less?. Trends Neurosci. 2005 Apr 1;28(4):209-16.
- Kühn AA, Kempf F, Brücke C, Gaynor Doyle L, Martinez-Torres I, Pogosyan A, Trottenberg T, Kupsch A, Schneider GH, Hariz MI, Vandenberghe W, Nuttin B, Brown P. High-frequency stimulation of the subthalamic nucleus suppresses oscillatory beta activity in patients with Parkinson’s disease in parallel with improvement in motor performance. J Neurosci. 2008 Jun 11;28(24):6165-73. PMID: 18550758; PMCID: PMC6670522. [CrossRef]
- Varanese S, Birnbaum Z, Rossi R, Di Rocco A. Treatment of advanced Parkinson’s disease. Parkinsons Dis. 2011 Feb 7;2010:480260. PMID: 21331376; PMCID: PMC3038575. [CrossRef]
- Deep-Brain Stimulation for Parkinson’s Disease Study Group. Obeso JA, Olanow CW, Rodriguez-Oroz MC, Krack P, Kumar R, Lang AE. Deep brain stimulation of the subthalamic nucleus or the pars interna of the globus pallidus in Parkinson’s disease. N Engl J Med. 2001;345:956–963.
- Moreau C, Defebvre L, Destée A, Bleuse S, Clement F, Blatt JL, et al. STN-DBS frequency effects on freezing of gait in advanced Parkinson disease. Neurology. 2008;71:80–84.
- Khoo HM, Kishima H, Hosomi K, Maruo T, Tani N, Oshino S, et al. Low-frequency subthalamic nucleus stimulation in Parkinson’s disease: a randomized clinical trial. Mov Disord. 2014;29:270–274.
Figure 1.
Schematic representation of the Deep Brain Stimulation (DBS) system: The electrode is implanted in the targeted brain area, connected by a DBS lead and an extension to the neurostimulator device. The neurostimulator, implanted in the chest, regulates the electrical impulses that modulate brain activity.
Figure 1.
Schematic representation of the Deep Brain Stimulation (DBS) system: The electrode is implanted in the targeted brain area, connected by a DBS lead and an extension to the neurostimulator device. The neurostimulator, implanted in the chest, regulates the electrical impulses that modulate brain activity.
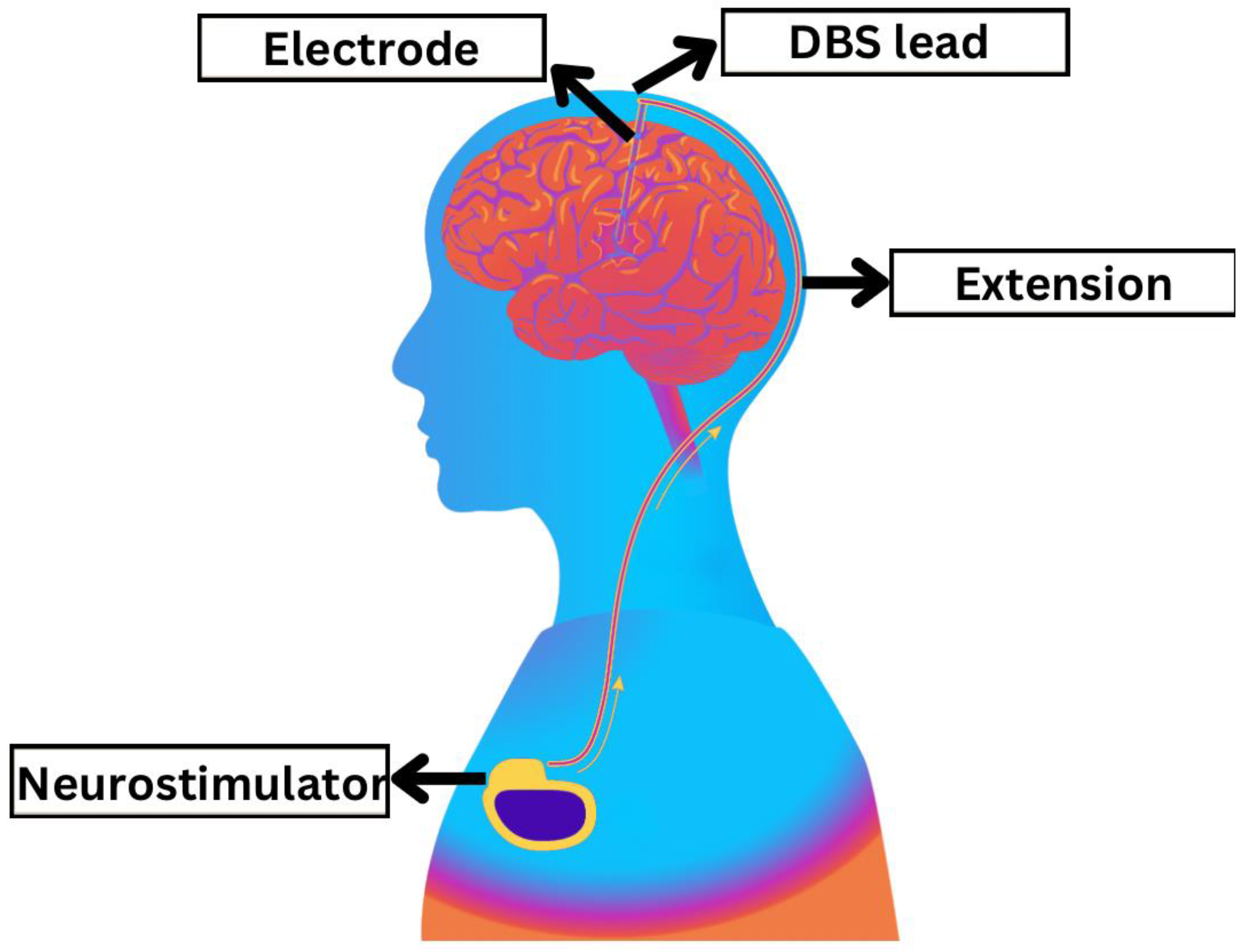
Figure 2.
PRISMA 2020 flow chart representing the screening and selection of studies. (PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analysis).
Figure 2.
PRISMA 2020 flow chart representing the screening and selection of studies. (PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analysis).
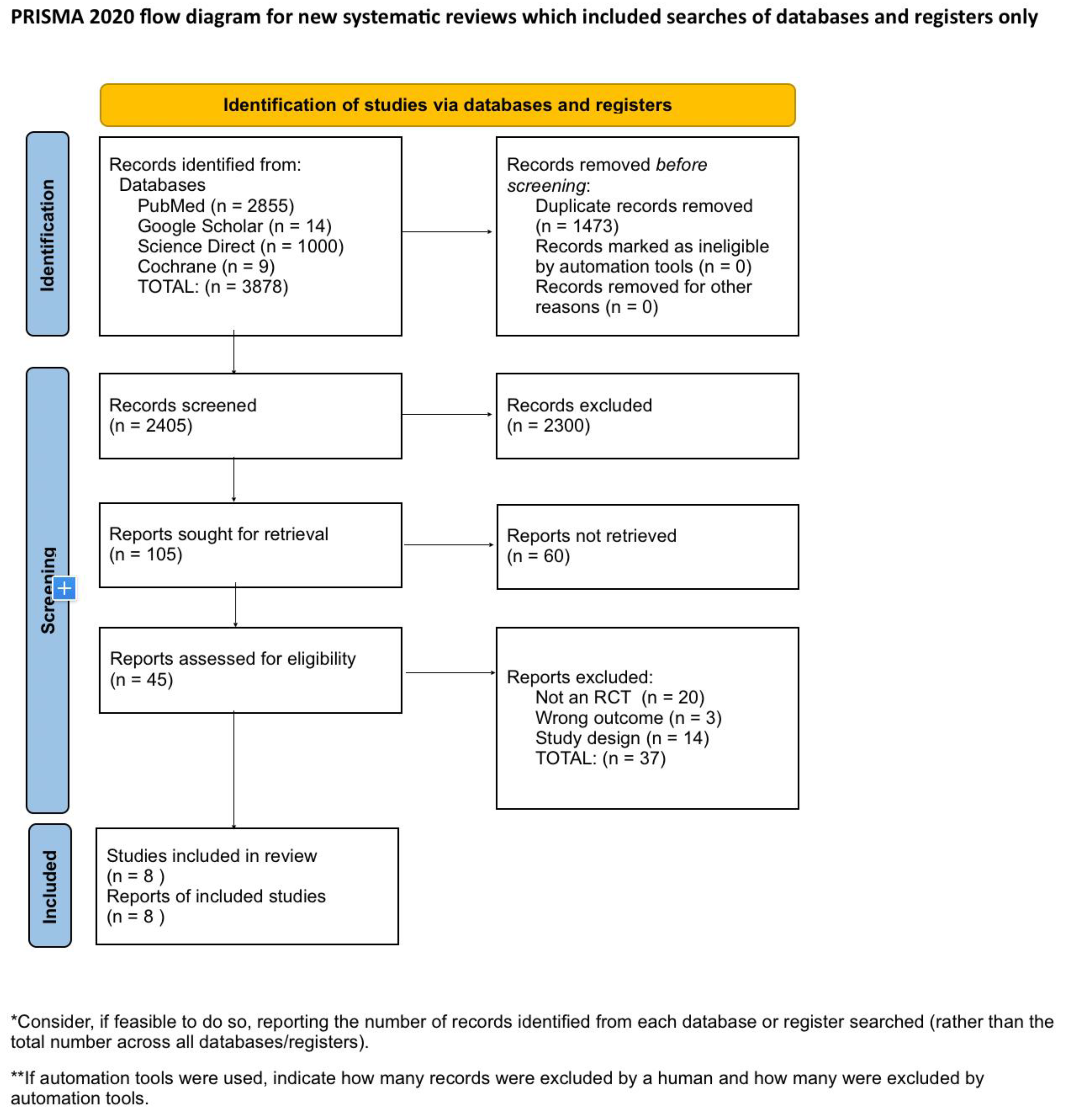
Figure 3.
Risk of bias assessment of included studies.
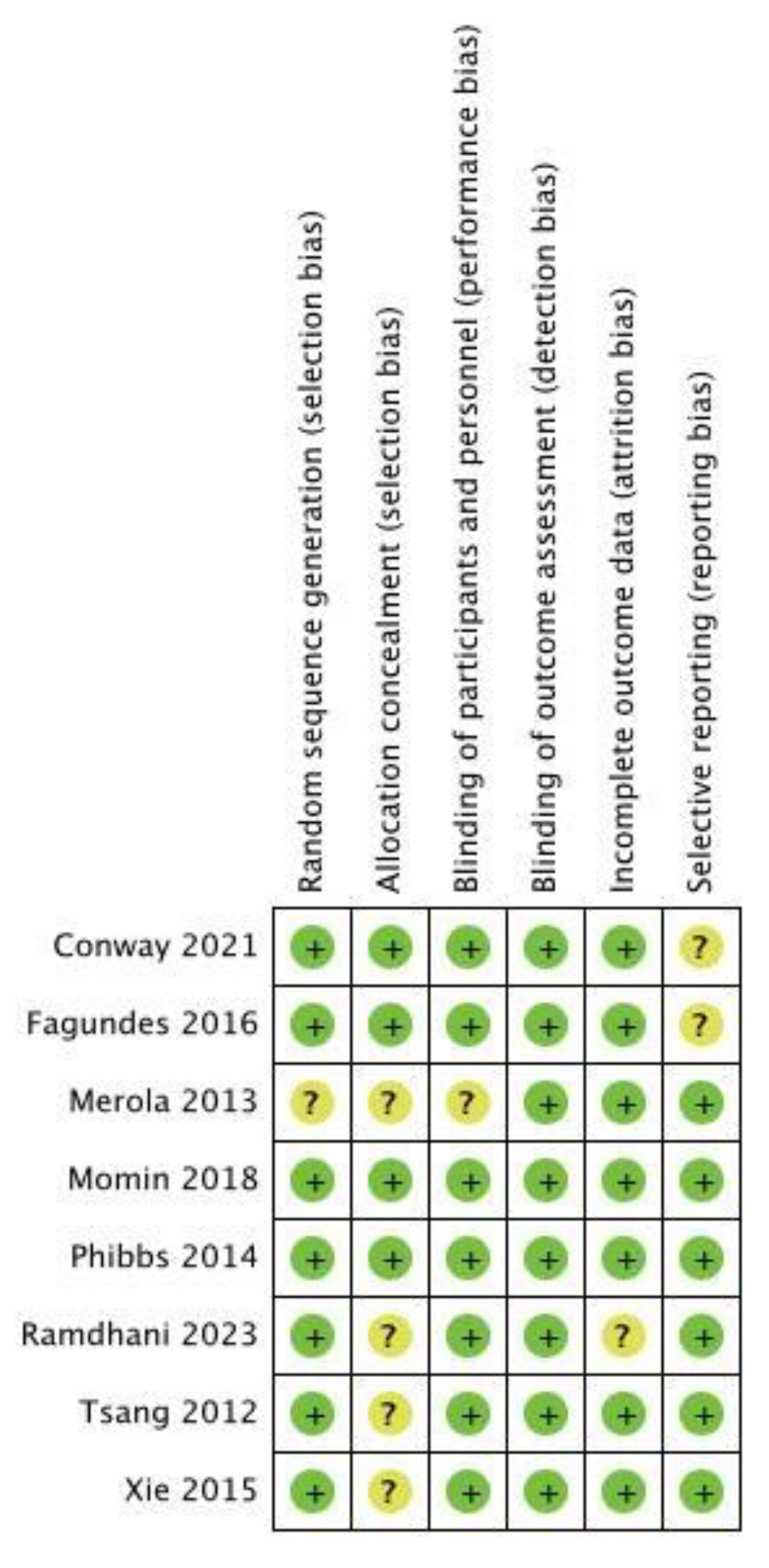

Table 1.
Inclusion and Exclusion criteria.
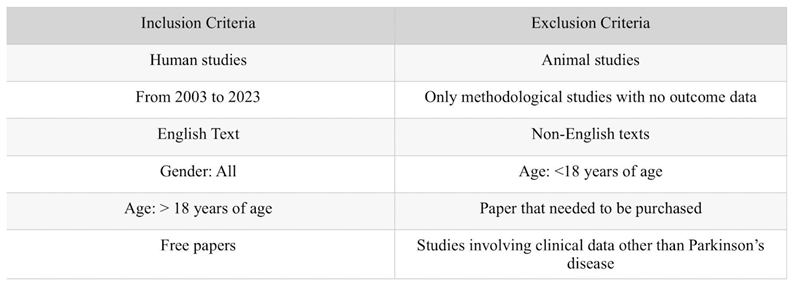
Table 2.
Search Strategy: The adjusted search terms as per searched electronic databases.
| Databases | Search Strategy | Result |
|---|---|---|
| PubMed | ((((((((Deep Brain Stimulation[MeSH Terms]) OR (DBS[Title/Abstract])) OR (Electrical Stimulation of the brain[Title/Abstract])) AND (Parkinson Disease[MeSH Terms])) OR (PD[Title/Abstract])) OR (Idiopathic Parkinson’s Disease[Title/Abstract])) OR (Parkinson’s Disease[Title/Abstract])) OR (Primary Parkinsonism[Title/Abstract])) AND (Low frequency[Title/Abstract] OR high frequency[Title/Abstract]) | 2349 (2024/05/21) 1391 Filters applied: From 2000 to 2024 Humans English MEDLINE |
| (((((Parkinson Disease[MeSH Terms]) OR (Idiopathic, Parkinson Disease[Title/Abstract])) OR (Idiopathic, Parkinson’s Disease[Title/Abstract])) OR (Idiopathic Parkinson Disease[Title/Abstract])) AND (((Deep Brain Stimulation[MeSH Terms]) OR (Deep Brain Stimulations[Title/Abstract])) OR (Brain Stimulation, Deep[Title/Abstract]))) AND ((High frequency deep brain stimulation[Title/Abstract]) OR (Low frequency deep brain stimulation[Title/Abstract])) | 52 (2024/05/22) 49 Filters applied: Humans English |
|
| (((((Parkinson Disease[MeSH Terms]) OR (Primary Parkinsonism[Title/Abstract])) OR (Paralysis Agitans[Title/Abstract])) OR (PD[Title/Abstract])) AND ((((Deep Brain Stimulation[MeSH Terms]) OR (Deep Brain Stimulations[Title/Abstract])) OR (Electrical Stimulation of the Brain[Title/Abstract])) OR (DBS[Title/Abstract]))) AND ((High frequency[Title/Abstract]) AND (Low frequency[Title/Abstract])) | 104 (2024/05/23) 71 Filters applied: Humans English |
|
| („Deep Brain Stimulation”[Mesh] OR „Deep Brain Stimulation”) AND („Parkinson Disease”[Mesh] OR „Parkinson’s Disease”) AND („Low frequency” OR „High frequency”) | 795 (2024/05/23) 174 Filters applied: Free full text Humans English MEDLINE |
|
| („Deep Brain Stimulation”[Mesh] OR „Deep Brain Stimulation”) AND („Parkinson Disease”[Mesh] OR „Parkinson’s Disease”) AND („Stimulation Frequency” OR „Low-frequency Stimulation” OR „High-frequency Stimulation”) | 416 (2024/05/23) 246 Filters applied: Humans English MEDLINE |
|
| Google Scholar | („Deep Brain Stimulation” OR DBS OR „brain stimulation”) AND („Parkinson Disease” OR Parkinson OR PD) AND (High-frequency OR Low-frequency OR „different frequencies”) AND („comparative study” OR effectiveness OR comparison) | 18,800 ONLY English 17,700 |
| Cochrane Library | ID Search #1 MeSH descriptor: [Deep Brain Stimulation] explode all trees #2 (deep brain stimulation* OR electrical stimulation of the brain OR DBS):ti,ab,kw #3 MeSH descriptor: [Parkinson Disease] explode all trees #4 (Parkinson* disease OR Idiopathic parkinson* disease OR Primary Parkinsonism OR Paralysis agitans OR Hypokinetic rigid syndrome OR Shaking palsy):ti,ab,kw #5 (High frequency stimulation AND Low frequency stimulation):ti,ab,kw #6 (#1 OR #2) AND (#3 OR #4) AND #5 |
59 (2024/05/16) |
| Science Direct | (Parkinson’s disease) AND (Deep Brain Stimulation) AND (Low frequency OR High frequency) AND (impact OR efficacy OR outcomes) | 13,629 (2024/05/18) 1,327 Filters applied: Review articles Research articles Neuroscience Medicine and Dentistry English Open access and open archive |
Table 3.
Summary of studies’ characteristics.
| Author, year | Country | Study Design | Number of patients | Medication (On/Off) | Intervention | LFS/HFS value | Follow up duration | Outcome |
|---|---|---|---|---|---|---|---|---|
| Conway et al., 2021 [37] | Australia | Randomized double blinded | 14 | Off | Bilateral STN-DBS | 60 Hz/ 100 Hz | No long term follow up | The research revealed that low-frequency (60 Hz) STN-DBS notably enhanced gait rhythmicity, particularly medial-lateral and vertical trunk rhythmicity, in Parkinson’s disease patients compared to high-frequency stimulation. These enhancements were not influenced by the electrode location, or the total electrical energy administered. However, no significant variances were detected between the two stimulation conditions in terms of temporal gait measures, clinical mobility measures, motor symptom severity, or the presence of gait retropulsion. The study suggests that low-frequency STN-DBS may provide immediate advantages for gait stability in PD patients. |
| Momin et al., 2018 [38] | UK | Randomized double blinded | 20 | Off | Bilateral STN-DBS | 40 Hz - 160 Hz | No long term follow up | The research examined the impact of different STN-DBS frequencies on upper limb motor function in patients with Parkinson’s disease. The study did not find a consistent influence of frequency on bradykinesia using both the Simple PP task and a modified upper limb version of the UPDRS-III. However, there was a notable improvement in the Assembly PP task at 80 Hz compared to the baseline frequency of 130 Hz, indicating enhanced phasic alertness and divided attention at the lower frequency. Furthermore, tremor and rigidity were better managed at higher frequencies (>80 Hz). The overall conclusion suggests that both high and low frequencies can be effective without exacerbating bradykinesia. |
| Merola et al., 2013 [39] | Italy | Non-randomized single blinded | 10 | On | Bilateral STN-DBS | 80 Hz / 130 Hz | 1 and 12 months | The results of the study demonstrate that adjusting the subthalamic nucleus deep brain stimulation (STN-DBS) frequency from 130 Hz to 80 Hz leads to a significant reduction in involuntary movements (IM) such as dyskinesias and dystonia in Parkinson’s disease (PD) patients. Dyskinesias improved in all patients, and dystonic features improved in most patients after one month of 80 Hz stimulation. However, in some patients, there was a gradual worsening of parkinsonian symptoms, necessitating a return to 130 Hz stimulation. This indicates that while 80 Hz STN-DBS may effectively address IM in certain patients, others may require higher frequencies to uphold overall motor function. |
| Phibbs et al., 2014 [40] | USA | Randomized double blinded | 20 | Off | Bilateral STN-DBS | 60 Hz / 130 Hz | No long term follow up | The study findings revealed that there was no significant variance in gait improvement observed in Parkinson’s disease patients who underwent subthalamic nucleus deep brain stimulation at 60 Hz versus 130 Hz. The primary measure of improvement, stride length, did not show any significant enhancement at the lower frequency. Furthermore, secondary gait parameters such as velocity and cadence also exhibited no notable differences. While there was a tendency towards reduced double limb support time at 60 Hz, it was not deemed statistically significant. As a result, the study concluded that lower frequency stimulation did not yield the anticipated improvement in gait performance. |
| Ramdhani et al., 2023 [41] | USA | Randomized double blinded | 22 | On/Off | Bilateral STN-DBS | 60 Hz / 180 Hz | No long term follow up | The research indicates that both high-frequency (HFS) and low-frequency (LFS) subthalamic nucleus deep brain stimulation (STN-DBS) yield similar impacts on most lower limb gait features in individuals with advanced Parkinson’s disease. However, considerable enhancements in trunk and lumbar kinematics were noted with HFS. In addition, stimulation from ventral electrode contacts elicited more favorable responses compared to dorsal contacts. These findings suggest that customized STN-DBS settings may have the potential to improve gait and decrease the risk of falls in Parkinson’s disease patients. |
| Tsang et al., 2012 [42] | Canada | Randomized double blinded | 13 | On/Off | Bilateral STN-DBS | 4-10 Hz, 11-30 Hz, 31-100 Hz, >130 Hz | No long term follow up | The research findings indicate that customizing deep brain stimulation of the subthalamic nucleus at beta frequencies ranging from 31 to 100 Hz markedly enhances motor symptoms in individuals with Parkinson’s disease, similar to the effects of traditional high-frequency stimulation. Meanwhile, alpha (4–10 Hz) and theta (11–30 Hz) frequency stimulations did not exacerbate motor symptoms, indicating that these frequencies may be indicative of disease progression rather than directly contributing to symptoms. indicates that patient-specific DBS frequencies can be effective, but further long-term studies are needed to validate these findings and optimize DBS therapy for Parkinson’s disease. |
| Xie T. et al., 2014 [43] | USA | Randomized double blinded | 7 | On | Bilateral STN-DBS | 60 Hz / 130 Hz | 6 weeks | The results of the study indicate that 60-Hz stimulation has a significant positive impact on swallowing function, freezing of gait (FOG), and overall axial and motor symptoms in Parkinson’s disease patients with bilateral subthalamic nucleus deep brain stimulation (STN-DBS) in comparison to the commonly used 130-Hz stimulation. The 60-Hz setting notably reduces aspiration frequency and subjective swallowing difficulty, with sustained improvements in FOG and axial symptoms observed over a six-week period.‘s design minimized carryover effects and suggested that 60-Hz stimulation could |
| Fagundes et al., 2016 [44] | Brazil | Randomized double blinded | 20 | On | Bilateral STN-DBS | 60 Hz / 130 Hz | No long term follow up | The research indicates that the frequency of subthalamic nucleus deep brain stimulation (STN-DBS) has a significant impact on verbal fluency (VF) in patients with Parkinson’s disease. Lower frequency stimulation at 60 Hz showed notable improvements in phonemic and action fluency compared to higher frequency stimulation at 130 Hz. This finding was consistent across various tasks and was not affected by practice, demographic factors, cognitive abilities, or clinical variables. The study recommends prioritizing low-frequency stimulation in Parkinson’s disease patients, particularly in those with cognitive impairments affecting verbal fluency, to minimize any adverse effects. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



