
Submitted:
07 August 2024
Posted:
09 August 2024
You are already at the latest version
Abstract
Background: Historically, a large gender-related disparity in vascular access (AV) has been demonstrated, with a lower prevalence of women with arteriovenous fistula (AVF) compared to men and worse maturity rates. The cause of this difference is not entirely clear, although several reasons that could contribute to it have been hypothesized. The emergence of new percutaneous FAV (pFAV) systems could be an alternative for reducing these differences.
Objective: The study aims to determine if there is a gender difference in the creation of AVFs using the new percutaneous systems.
Material and Methods: A systematic review of the literature was conducted by searching PubMed and Google Scholar using the following terms: "percutaneous arteriovenous fistula", "endovascular arteriovenous fistula", and "hemodialysis". All clinical trials, comparative studies, and descriptive studies involving patients who underwent a pAVF were included.
Results: Finally, the review includes 19 studies, comprising 14 retrospective and 5 prospective studies. Of these, 6 studies are comparative, 5 of which compare pAVF with surgically created AVFs (sAVF), and 1 comparing pAVFs performed using different systems with each other.
A total of 1,269 patients were included in the review. Of the total number of patients, only 414 were women, representing 32.62%.
Conclusion: The number of women included in the various studies analyzing pAVF remains very low, representing less than one-third of all patients. Although the causes of this difference are not entirely clear, several reasons have been hypothesized such as socio-economic factors, anatomical factors, or even patients' preferences. Given these results, further studies are needed to try to clarify the reasons for this gender disparity and to establish different strategies to mitigate the barriers faced by women in accessing the creation of an AVF.
Keywords:
percutaneous arteriovenous fistula
; endovascular arteriovenous fistula
; hemodialysis
; Ellypsis
; WavelinQ
; EverlinQ
1. Introduction
According to the United States Renal Data System (USRDS) and the European Renal Association (ERA) registry, in 2021, 135,972 people in the United States and 76,240 in Europe respectively started renal replacement therapy (RRT) [1,2]. Of these, 84.2% and 83% began with hemodialysis (HD). In Spain, according to the 2023 Spanish Registry of Renal Patients (REER), 7,119 patients started RRT, of whom 78.4% started on HD [3]. Vascular access (VA) through which HD sessions are performed is crucial for these patients. It affects both the quality of treatment and associated morbidity and mortality [4,5]. Following the recommendations of clinical guidelines, native AVFs remain the first option to consider as VA when a patient needs to start HD, ahead of central venous catheters (CVCs) and prosthetic AVFs [6,7]. This is due to their lower complication rate, lower associated morbidity and mortality, and higher long-term patency rate [8,9,10,11,12]. Despite these recommendations, the number of incidents and prevalent patients using CVCs as vascular access remains very high. According to the USRDS, in 2021, 85.4% of patients initiated HD through a CVC, reducing this percentage to 23% in prevalent patients [2].
Similarly, the latest data from the DOPPS 5 study shows that 29% of patients use a CVC [13]. This issue is even more pronounced in certain minority groups such as women, the elderly, or vulnerable populations. Thus, there is multiple evidence showing that women are less likely to receive an AVF than men and that they also have a higher probability of AV maturation failure [14,15,16]. However, there is limited evidence explaining the reason for this disparity, making it difficult to study different methods to reduce it.
In 2018, the United States Food and Drug Administration (FDA) approved two new endovascular systems for creating native AVFs using minimally invasive techniques [17,18]. These systems are the WavelinQ®TM EndoAVF System (Becton, Dickinson, and Company) and the Ellipsys®TM EndoAVF System (Avenu Medical).
The WavelinQ®TM EndoAVF System used to perform a pAVF consists of two 4 French magnetic catheters The venous catheter contains a radiofrequency (RF) electrode, connected via an electrocautery pencil to an electrocautery unit that delivers RF energy. Conversely, the arterial catheter contains a ceramic stop that receives the electrode once both catheters are attracted. Both catheters have rotational indicators to ensure they are in the correct position The arterial catheter is introduced through the artery (US approval was given for brachial artery only; brachial, radial, or ulnar artery insertion was approved in Europe), and a venous catheter (with an electrode) placed through the brachial, radial, or ulnar vein. Fluoroscopic guidance with contrast imaging is used to position and align the catheters. At the same time, magnets hold the artery and vein together as a radio-frequency electrode incises a channel between proximal forearm vessels, resulting in AVF flow. Coil embolization of the brachial vein increases superficial pAVF flow through the DCV and completes the procedure [19].
The Ellipsys device is inserted over a single superficial venous guidewire, advanced through the deep communicating vein, and introduced through the vein wall into the proximal radial artery. The entire procedure is performed with duplex ultrasonographic guidance; no fluoroscopy or contrast is used. The device is advanced over the wire, capturing both arterial and venous walls and, when closed and activated, generates a secure anastomosis through thermal resistance and pressure. A balloon dilation of the anastomosis completes the procedure, removing spasms and establishing outflow through the deep communicating vein to the superficial venous system [20].
Multiple publications have demonstrated the benefits of using these minimally invasive systems, which could increase the number of both incident and prevalent women with an AVF as their VA by providing a solution to some problems such as smaller vessel caliber or lower maturation rate [19,20,21,22,23].
The main objective of this study is to analyze whether there is a gender disparity in access to the performance of an AVF using these minimally invasive systems to determine if it is an alternative to classic surgical methods and could contribute to reducing these differences.
2. Material and Methods
2.1. Research Question
At the beginning of the study, the following research question was formulated as the main objective of this review: Is there a sex disparity in VA for hemodialysis with the new percutaneous systems?
2.2. Search Strategy
To answer the above question, information was searched in two databases (PUBMED and GOOGLE SCHOLAR) using the following key terms: percutaneous arteriovenous fistula, endovascular arteriovenous fistula, and hemodialysis. Additionally, a manual review of the bibliographic references of the selected articles was conducted to find any potential articles that could be included in the review.
2.3. Selection Criteria and Information Analysis
For this review, randomized clinical trials, comparative studies, and observational studies, both retrospective and prospective, were considered for inclusion if they involved patients who underwent pAVF creation. There were no limitations regarding the year of publication or language. Articles that did not differentiate gender in the results were excluded.
This review followed the methodological guidelines recommended by the PRISMA statement (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [24]. The selection of articles is shown in Figure 1.
For the present work, the full text of the selected articles was read based on their publication date, starting from the oldest to the most recent. After completing the full-text reading, a table was created including the main characteristics of the finally selected articles, information related to the authors, year of publication, sex, age, type of studies, and system used to perform the pAVF (Table 1]. For those articles comparing percutaneously or surgically created AVFs, only the data of patients with pAVFs were collected.
3. Results
Finally, the review included 19 studies, 14 retrospective and 5 prospective. Of these, 6 studies are comparative. 5 compares pAVFs with sAVFs, and 1 compares pAVFs performed using different systems. 5 studies include data from pAVFs performed using the EverlinQ system (TVA Medical Inc., Austin, TX, USA), 10 include data from pAVFs performed using the Ellipsys system (Medtronic), and 6 using the Wavelin Q system (TVA Medical Inc., Austin, TX, USA).
A total of 1269 patients were included in the review. Of these, only 414 were women, representing 32.62% of the total patients (Figure 2).
None of the studies included differences by sex in the results regarding maturation, patency, or complication rate.
4. Discussion
The main finding of our study is that despite the overwhelming evidence supporting the use of the AVF as the preferred vascular access in hemodialysis patients due to lower complication rates, lower costs, and lower mortality rates [6,7], only a third of the patients selected for this endovascular technique are women, revealing a gender disparity. Many other studies have shown a significant gender disparity in VA, demonstrating a lower prevalence of AVFs in women compared to men. [16,25,26,27,28,29,30,31]. The cause of this disparity is not entirely clear, although several reasons have been hypothesized that could contribute to it.
One reason for this difference could be related to vessel diameter, as vein size is the main predictor of AVF maturation failure [32]. Some authors have hypothesized that the lower maturation rates observed in women might be related to the smaller diameter of both veins and arteries [14,33,34,35]. These findings could contribute to a clinical bias, leading nephrologists and surgeons to consider women as less suitable candidates for AVF creation due to their anatomy and higher likelihood of maturation failure. However, evidence suggests that these differences are not significant in clinical practice and that variations in maturation rates are due to other factors [26,28,29,36,37]. This hypothesis regarding smaller vessel sizes in women might contribute to the significant gender disparity observed in percutaneous arteriovenous fistulas (pAVFs) studies, for both currently available systems, Ellipsys and WavelinQ, a vein and artery diameter greater than 2 mm is required to insert the catheters.
Similarly, numerous studies have shown the impact of obesity on AVFs, with lower maturation rates and a higher number of reinterventions. This could be due to various causes, such as lower intraoperative blood flow or higher leptin levels and inflammatory markers related to myointimal hyperplasia [38,39,40]. It has been hypothesized that these factors could be related to the lower maturation rate of AVFs in women, due to the greater accumulation of fatty tissue in the arms [41]. However, pAVFs could be a good option for this patient profile as they are minimally invasive systems that reduce inflammatory markers and myointimal hyperplasia. Being performed in the deep venous system and increasing possible puncture sites, they could minimize cannulation problems due to the greater depth of veins in obese individuals.
Other potential causes for the women’s lower AVF maturation rates have been studied, such as venous dilation capacity or different inflammation mechanisms [42]. In this regard, a study by Dember LM et al. analyzed different markets of vascular function before AVF creation. However, the lower maturation rates of AVF in women were not explained by preoperative vascular function tests [43].
At the hormonal level, certain factors could contribute to these differences in maturation rate. Sex hormones and their receptors play a significant role in the progression of chronic kidney disease (CKD) through various pathophysiological pathways. However, these hormones may play an unclear role in inflammation during AVF maturation [44]. To address these uncertainties, Satam K et al. studied the role of sex hormones in AVF maturation in mice, demonstrating that estrogens can lead to early failure due to increased recruitment of immune cells [45].
Another reason that could explain the lower rate of women with AVFs is the patients’ preferences. In this regard, The Dialysis Outcomes and Practice Patterns Study data (DOPPS) showed that when patients were asked to indicate their preferences for VA, 58% of women preferred a fistula compared to 69% of men [13]. Although the two main reasons for this choice were to avoid needles and bleeding, it has been hypothesized that one of the reasons could be aesthetic [16]. In the case of pAVFs, the lower number of women included in the studies should not be justified by aesthetic reasons. One of the main advantages is that these minimally invasive techniques do not involve surgery, sutures, or surgical scars. It has also been shown that there is a lower rate of aneurysms in the cannulation area [46,47].
Another reason that could lead to a lower number of women using an AVF as a VA could be certain socioeconomic factors and access to healthcare. There is evidence showing that a smaller percentage of women start renal replacement therapy (RRT), opting for conservative treatment and that those who do start it, start it later than men [48,49]. This could be justified by the slower progression of CKD in women, although certain factors such as lower access to specialized medical care in certain regions could contribute [50,51]. Additionally, there may be a lack of awareness about the impact of gender on the presentation of certain diseases such as chronic kidney disease (CKD) [50,52].
One limitation of our review is that it is purely descriptive. It also includes studies with a very limited number of patients, and several of them are retrospective, which could lead to selection biases. Another important limitation to consider is that none of the studies included in the review distinguish by sex in terms of outcomes. The final important limitation to note is that this review only considers the percentage of selected women who underwent AVF, rather than the total population from which the sample was drawn. This is due to several articles not providing this information.
5. Conclusions
Historically, there has been a significant gender disparity in the use of AVFs as VA, despite the substantial benefits demonstrated compared to the use of CVCs. Although the causes of this difference are not entirely clear, several reasons have been hypothesized, including socioeconomic factors, anatomical factors, and even patient preferences. The emergence of new percutaneous and minimally invasive systems for creating AVFs could provide a good opportunity to reduce these differences and increase the number of women undergoing dialysis through an AVF. However, in the various studies published in the literature, the low number of women included remains striking.
Given the gender disparity in the studies, further research is necessary to examine the differences in results between the sexes. Additionally, it is important to work on identifying and mitigating the barriers women face in accessing AVF creation, ensuring that medical decisions are based on individual needs, and avoiding assumptions or biases.
Funding
The authors did not receive support from any organization for the submitted work.
Conflicts of Interest
The authors have no conflicts of interest to declare.
References
- ERA-Registry-Annual-Report-2021_231206.pdf.
- nited States Renal Data System. 2023 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2023.
- Registro Español de Enfermos Renales. Informe de Diálisis y Trasplante 2023. Sociedad Española de Nefrología [INTERNET]. Available from: https://www.senefro.org/contents/webstructure/SEN_2023_REER_V2_1_.pdf.
- Domenick Sridharan N, Fish L, Yu L, Weisbord S, Jhamb M, Makaroun MS, et al. The associations of hemodialysis access type and access satisfaction with health-related quality of life. J Vasc Surg. 2018 Jan;67(1):229–35.
- de Arriba G, Gutiérrez Avila G, Torres Guinea M, Moreno Alia I, Herruzo JA, Rincón Ruiz B, et al. La mortalidad de los pacientes en hemodiálisis está asociada con su situación clínica al comienzo del tratamiento. Nefrología. 2021 Jul 1;41(4):461–6.
- Ibeas J, Roca-Tey R, Vallespín J, Moreno T, Moñux G, Martí-Monrós A, et al. Spanish Clinical Guidelines on Vascular Access for Haemodialysis. Nefrologia. 2017 Nov;37 Suppl 1:1–191.
- Lok CE, Huber TS, Lee T, Shenoy S, Yevzlin AS, Abreo K, et al. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. Am J Kidney Dis. 2020 Apr;75(4 Suppl 2):S1–164. [CrossRef]
- Poinen K, Quinn RR, Clarke A, Ravani P, Hiremath S, Miller LM, et al. Complications From Tunneled Hemodialysis Catheters: A Canadian Observational Cohort Study. Am J Kidney Dis. 2019 Apr;73(4):467–75. [CrossRef]
- Ravani P, Palmer SC, Oliver MJ, Quinn RR, MacRae JM, Tai DJ, et al. Associations between hemodialysis access type and clinical outcomes: a systematic review. J Am Soc Nephrol. 2013 Feb;24(3):465–73.
- Murea M, Gardezi AI, Goldman MP, Hicks CW, Lee T, Middleton JP, et al. Study protocol of a randomized controlled trial of fistula vs. graft arteriovenous vascular access in older adults with end-stage kidney disease on hemodialysis: the AV access trial. BMC Nephrol. 2023 Feb 24;24(1):43. [CrossRef]
- Nassar GM, Ayus JC. Infectious complications of the hemodialysis access. Kidney Int. 2001 Jul;60(1):1–13. [CrossRef]
- Ng Y-Y, Hung Y-N, Wu S-C, Ko P-J. Characteristics and 3-year mortality and infection rates among incident hemodialysis patients with a permanent catheter undergoing a first vascular access conversion. Clin Exp Nephrol. 2014 Apr;18(2):329–38. [CrossRef]
- Pisoni RL, Zepel L, Port FK, Robinson BM. Trends in US Vascular Access Use, Patient Preferences, and Related Practices: An Update From the US DOPPS Practice Monitor With International Comparisons. Am J Kidney Dis. 2015 Jun 1;65(6):905–15. [CrossRef]
- Shah S, Leonard AC, Meganathan K, Christianson AL, Thakar CV. Gender and Racial Disparities in Initial Hemodialysis Access and Outcomes in Incident End-Stage Renal Disease Patients. Am J Nephrol. 2018 Jul 10;48(1):4–14. [CrossRef]
- MacRae JM, Clarke A, Ahmed SB, Elliott M, Quinn RR, James M, et al. Sex differences in the vascular access of hemodialysis patients: a cohort study. Clin Kidney J. 2021 May;14(5):1412–8. [CrossRef]
- Beaumier M, Ficheux M, Couchoud C, Lassalle M, Launay L, Courivaud C, et al. Is there sex disparity in vascular access at dialysis initiation in France? A mediation analysis using data from the Renal Epidemiology and Information Network registry. Clin Kidney J. 2022 Nov;15(11):2144–53. [CrossRef]
- Lok CE, Rajan DK, Clement J, Kiaii M, Sidhu R, Thomson K, et al. Endovascular Proximal Forearm Arteriovenous Fistula for Hemodialysis Access: Results of the Prospective, Multicenter Novel Endovascular Access Trial (NEAT). Am J Kidney Dis. 2017 Oct 1;70(4):486–97. [CrossRef]
- Hull JE, Jennings WC, Cooper RI, Waheed U, Schaefer ME, Narayan R. The Pivotal Multicenter Trial of Ultrasound-Guided Percutaneous Arteriovenous Fistula Creation for Hemodialysis Access. J Vasc Interv Radiol. 2018 Feb;29(2):149-158.e5. [CrossRef]
- Kitrou PM, Balta L, Papachristou E, Papasotiriou M, Katsanos K, Theofanis M, Papadoulas S, Anagnostopoulos F, Georgopoulou GA, Goumenos D, Karnabatidis D. Percutaneous Arteriovenous Fistula Creation with the WavelinQ 4-French EndoAVF System: A Single-Center Retrospective Analysis of 30 Patients. J Vasc Interv Radiol [Internet]. Available from: http://dx.doi.org/10.1016/j.jvir.2021.09.021. [CrossRef]
- Shahverdyan R, Beathard G, Mushtaq N, Litchfield TF, Nelson PR, Jennings WC. Comparison of Outcomes of Percutaneous Arteriovenous Fistulae Creation by Ellipsys and WavelinQ Devices. J Vasc Interv Radiol. 2020 Sep;31(9):1365–72. [CrossRef]
- Zemela MS, Minami HR, Alvarez AC, Smeds MR. Real-World Usage of the WavelinQ EndoAVF System. Ann Vasc Surg. 2021 Jan;70:116–22. [CrossRef]
- Berland TL, Clement J, Griffin J, Westin GG, Ebner A. Endovascular Creation of Arteriovenous Fistulae for Hemodialysis Access with a 4 Fr Device: Clinical Experience from the EASE Study. Ann Vasc Surg. 2019 Oct;60:182–92. [CrossRef]
- Inston N, Khawaja A, Tullett K, Jones R. WavelinQ created arteriovenous fistulas versus surgical radiocephalic arteriovenous fistulas? A single-centre observational study. J Vasc Access. 2020 Sep;21(5):646–51. [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;372:n71.
- Hecking M, Bieber BA, Ethier J, Kautzky-Willer A, Sunder-Plassmann G, Säemann MD, et al. Sex-specific differences in hemodialysis prevalence and practices and the male-to-female mortality rate: the Dialysis Outcomes and Practice Patterns Study (DOPPS). PLoS Med. 2014 Oct;11(10):e1001750. [CrossRef]
- Caplin N, Sedlacek M, Teodorescu V, Falk A, Uribarri J. Venous access: women are equal. Am J Kidney Dis. 2003 Feb;41(2):429–32. [CrossRef]
- Silpe J, Koleilat I, Yu J, Kim YH, Taubenfeld E, Talathi S, et al. Sex disparities in hemodialysis access outcomes: A systematic review. Semin Vasc Surg. 2023 Dec;36(4):560–70. [CrossRef]
- Hoffstaetter T, Silpe J, Delijani D, Landis GS, Etkin Y. Sex Disparities in Arteriovenous Fistula Maturation Outcomes. Ann Vasc Surg. 2023 Sep;95:197–202. [CrossRef]
- Miller CD, Robbin ML, Allon M. Gender differences in outcomes of arteriovenous fistulas in hemodialysis patients. Kidney Int. 2003 Jan;63(1):346–52. [CrossRef]
- Angelici L, Marino C, Umbro I, Bossola M, Calandrini E, Tazza L, et al. Gender Disparities in Vascular Access and One-Year Mortality among Incident Hemodialysis Patients: An Epidemiological Study in Lazio Region, Italy. J Clin Med Res [Internet]. 2021 Oct 30;10(21). Available from: http://dx.doi.org/10.3390/jcm10215116. [CrossRef]
- Arhuidese IJ, Faateh M, Meshkin RS, Calero A, Shames M, Malas MB. Gender-Based Utilization and Outcomes of Autogenous Fistulas and Prosthetic Grafts for Hemodialysis Access. Ann Vasc Surg. 2020 May;65:196–205. [CrossRef]
- Lauvao LS, Ihnat DM, Goshima KR, Chavez L, Gruessner AC, Mills JL Sr. Vein diameter is the major predictor of fistula maturation. J Vasc Surg. 2009 Jun;49(6):1499–504. [CrossRef]
- Marcus RJ, Marcus DA, Sureshkumar KK, Hussain SM, McGill RL. Gender differences in vascular access in hemodialysis patients in the United States: developing strategies for improving access outcome. Gend Med. 2007 Sep;4(3):193–204. [CrossRef]
- McGill RL, Lacson E. Sex, race, and hemodialysis vascular access processes. J Vasc Access. 2017 Mar 21;18(2):132–8. [CrossRef]
- Allon M, Lockhart ME, Lilly RZ, Gallichio MH, Young CJ, Barker J, et al. Effect of preoperative sonographic mapping on vascular access outcomes in hemodialysis patients. Kidney Int. 2001 Nov;60(5):2013–20. [CrossRef]
- Lee T, Barker J, Allon M. Associations with predialysis vascular access management. Am J Kidney Dis. 2004 Jun;43(6):1008–13. [CrossRef]
- Peterson WJ, Barker J, Allon M. Disparities in fistula maturation persist despite preoperative vascular mapping. Clin J Am Soc Nephrol. 2008 Mar;3(2):437–41. [CrossRef]
- Kim J-K, Jeong JH, Song YR, Kim HJ, Lee WY, Kim KI, et al. Obesity-related decrease in intraoperative blood flow is associated with maturation failure of radiocephalic arteriovenous fistula. J Vasc Surg. 2015 Oct;62(4):1010-1017.e1. [CrossRef]
- Kats M, Hawxby AM, Barker J, Allon M. Impact of obesity on arteriovenous fistula outcomes in dialysis patients. Kidney Int. 2007 Jan;71(1):39–43. [CrossRef]
- Raulli SJ, Sather K, Dicken QG, Farber A, Kalish JA, Eslami MH, et al. Higher body mass index is associated with reinterventions and lower maturation rates after upper extremity arteriovenous access creation. J Vasc Surg. 2021 Mar;73(3):1007–15. [CrossRef]
- Delgado Ramírez A, Latorre López LI, Ruiz García E, Crespo Montero R. Factores que influyen en la supervivencia de la fístula arteriovenosa interna y su relación con la técnica de punción. Enferm Nefrol. 2016 Sep 15;19(3):215–30.
- Chan SM, Weininger G, Langford J, Jane-Wit D, Dardik A. Sex Differences in Inflammation During Venous Remodeling of Arteriovenous Fistulae. Front Cardiovasc Med. 2021 Jul 21;8:715114. [CrossRef]
- Dember LM, Imrey PB, Duess M-A, Hamburg NM, Larive B, Radeva M, et al. Vascular Function at Baseline in the Hemodialysis Fistula Maturation Study. J Am Heart Assoc [Internet]. 2016 Jul 22;5(7). Available from: http://dx.doi.org/10.1161/JAHA.116.003227. [CrossRef]
- Valdivielso JM, Jacobs-Cachá C, Soler MJ. Sex hormones and their influence on chronic kidney disease. Curr Opin Nephrol Hypertens. 2019 Jan;28(1):1–9. [CrossRef]
- Satam K, Ohashi Y, Thaxton C, Gonzalez L, Setia O, Bai H, et al. Sex hormones impact early maturation and immune response in the arteriovenous fistula mouse model. AMERICAN JOURNAL OF PHYSIOLOGY HEART AND CIRCULATORY PHYSIOLOGY [ISSN: 0363-6135] [ISSN: 1522-1539] [Internet]. 2023; Available from: http://dx.doi.org/10.1152/ajpheart.00049.2023. [CrossRef]
- Mallios A, Bourquelot P, Franco G, Hebibi H, Fonkoua H, Allouache M, et al. Midterm results of percutaneous arteriovenous fistula creation with the Ellipsys Vascular Access System, technical recommendations, and an algorithm for maintenance. J Vasc Surg. 2020 Dec;72(6):2097–106. [CrossRef]
- Beathard GA, Litchfield T, Jennings WC. Two-year cumulative patency of endovascular arteriovenous fistula. J Vasc Access. 2020 May;21(3):350–6. [CrossRef]
- Morton RL, Turner RM, Howard K, Snelling P, Webster AC. Patients who plan for conservative care rather than dialysis: a national observational study in Australia. Am J Kidney Dis. 2012 Mar;59(3):419–27. [CrossRef]
- Yong DSP, Kwok AOL, Wong DML, Suen MHP, Chen WT, Tse DMW. Symptom burden and quality of life in end-stage renal disease: a study of 179 patients on dialysis and palliative care. Palliat Med. 2009 Mar;23(2):111–9. [CrossRef]
- García GG, Iyengar A, Kaze F, Kierans C, Padilla-Altamira C, Luyckx VA. Sex and gender differences in chronic kidney disease and access to care around the globe. Semin Nephrol. 2022 Mar;42(2):101–13. [CrossRef]
- Gasparini A, Evans M, Coresh J, Grams ME, Norin O, Qureshi AR, et al. Prevalence and recognition of chronic kidney disease in Stockholm healthcare. Nephrol Dial Transplant. 2016 Dec;31(12):2086–94. [CrossRef]
- Kausz AT, Obrador GT, Arora P, Ruthazer R, Levey AS, Pereira BJG. Late initiation of dialysis among women and ethnic minorities in the United States. J Am Soc Nephrol. 2000 Dec;11(12):2351-2357. [CrossRef] [PubMed]
- Berland T, Clement J, Inston N, Kreienberg P, Ouriel K, WavelinQ 4 French Investigators. Percutaneous arteriovenous fistula creation with the 4F WavelinQ EndoAVF System. J Vasc Surg. 2022 Mar;75(3):1038-1046.e3. [CrossRef]
- Harika G, Mallios A, Allouache M, Costanzo A, de Blic R, Boura B, et al. Comparison of surgical versus percutaneously created arteriovenous hemodialysis fistulas. J Vasc Surg. 2021 Jul;74(1):209–16. [CrossRef]
- Habib SG, Jano A, Ali AA, Phillips A, Pinter J, Yuo TH. Early clinical experience and comparison between percutaneous and surgical arteriovenous fistula. J Vasc Surg. 2023 Sep;78(3):766–73. [CrossRef]
- Hebibi H, Achiche J, Franco G, Rottembourg J. Clinical hemodialysis experience with percutaneous arteriovenous fistulas created using the Ellipsys® vascular access system. Hemodial Int. 2019 Apr;23(2):167–72. [CrossRef]
- Hull JE, Elizondo-Riojas G, Bishop W, Voneida-Reyna YL. Thermal Resistance Anastomosis Device for the Percutaneous Creation of Arteriovenous Fistulae for Hemodialysis. J Vasc Interv Radiol. 2017 Mar;28(3):380–7. [CrossRef]
- Mordhorst A, Clement J, Kiaii M, Faulds J, Hsiang Y, Misskey J. A comparison of outcomes between open and endovascular arteriovenous access creation for hemodialysis. J Vasc Surg. 2022 Jan;75(1):238-247.e1. [CrossRef]
- Osofsky R, Byrd D, Reagor J, Das Gupta J, Clark R, Argyropoulos C, et al. Initial Outcomes Following Introduction of Percutaneous Arteriovenous Fistula Program with Comparison to Historical Surgically Created Fistulas. Ann Vasc Surg. 2021 Jul;74:271–80. [CrossRef]
- Radosa CG, Radosa JC, Weiss N, Schmidt C, Werth S, Hofmockel T, et al. Endovascular Creation of an Arteriovenous Fistula (endoAVF) for Hemodialysis Access: First Results. Cardiovasc Intervent Radiol. 2017 Oct;40(10):1545–51. [CrossRef]
- Rajan DK, Ebner A, Desai SB, Rios JM, Cohn WE. Percutaneous creation of an arteriovenous fistula for hemodialysis access. J Vasc Interv Radiol. 2015 Apr;26(4):484–90. [CrossRef]
- Shahverdyan R, Beathard G, Mushtaq N, Litchfield TF, Vartanian S, Konner K, et al. Comparison of Ellipsys Percutaneous and Proximal Forearm Gracz-Type Surgical Arteriovenous Fistulas. Am J Kidney Dis. 2021 Oct;78(4):520-529.e1. [CrossRef]
- Sultan S, Langsfeld M, Chavez L, Fabre A, Osofsky R, Argyropoulos C, et al. Initial 6-month quality review of a percutaneous endovascular arteriovenous fistula program. J Vasc Access. 2021 Jul;22(4):540–6. [CrossRef]
Figure 1.
flow diagram for study selection.
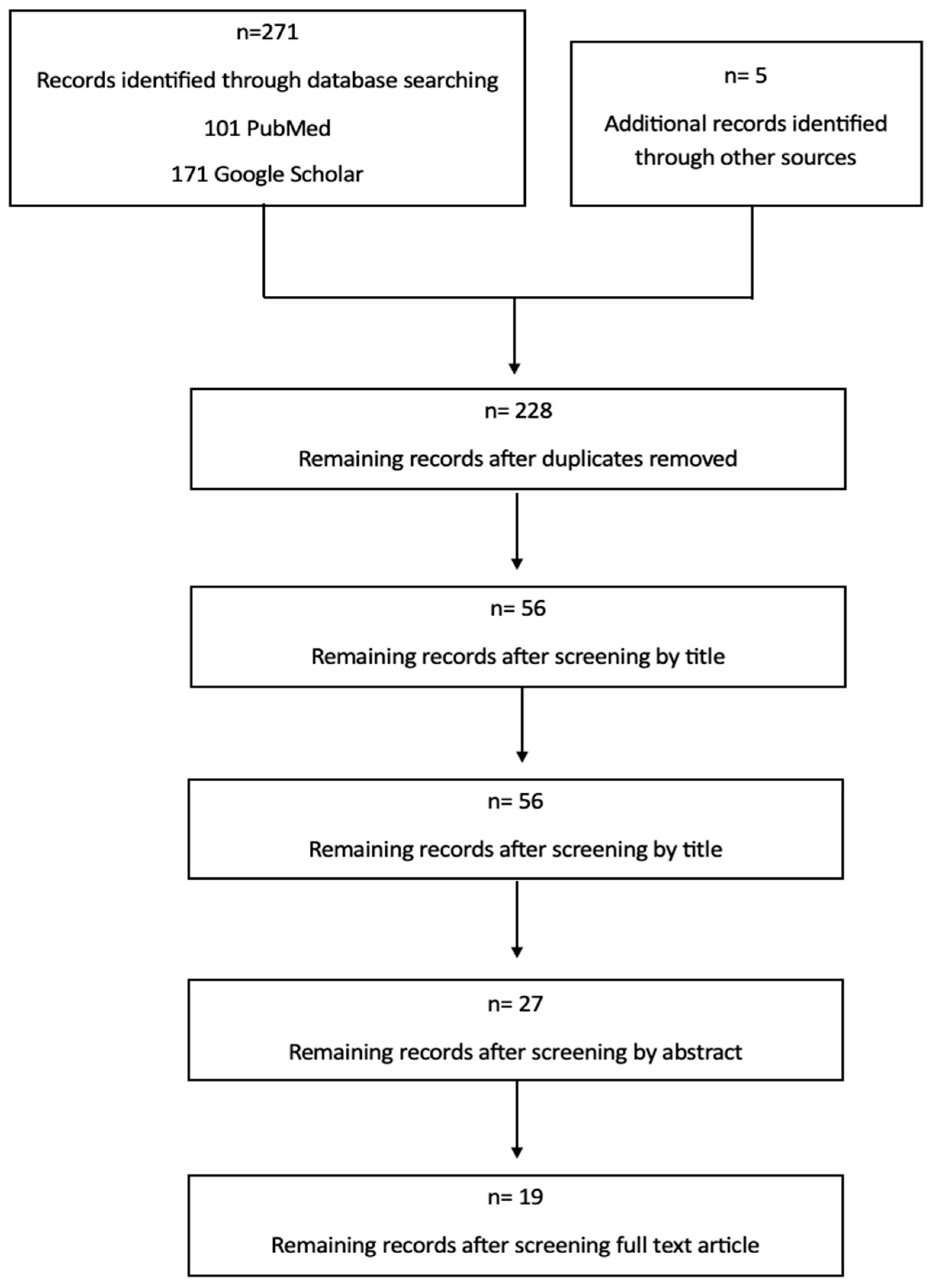
Figure 2.
Percentage of women with pAVFs included in the review.

Table 1.
Main Characteristics of the Studies.
| Autor/year | Study Type | Number of participants | Mean Age | Gender N (%) |
Device |
|---|---|---|---|---|---|
| Beathard et al [47], 2020 | Retrospective Cohort Study | 105 | 56,2 | Male: 77 (73,3) Female: 28 (26,3) |
Ellipsys Vascular Access System |
| Berland et al [53], 2022 | Retrospective Cohort Study | 120 | 55,6±15,9 | Male: 97 (80,8) Female: 23 (19,2) |
Wavelin Q EndoAVF System |
| Harika et al [54] | Retrospective comparative study | 107 | 63,6±15,41 | Male: 66 (61,7) Female: 41 (38,3) |
Ellipsys Vascular Access System/ Surgical AVF |
| Habib et al [55], 2023 | Retrospective comparative study | 51 | 58 ± 13,5 | Male 40 (78) Female: 11 (22) |
Ellipsys Vascular Access System/ Wavelin Q EndoAVF System / Surgical AVF |
| Hebibi et al [56], 2019 | Retrospective Cohort Study | 34 | 62 | Male: 20 (58) Female: 34 (42) |
Ellipsys Vascular Access System |
| Hull, et al [57], 2017 | Prospective Cohort Study | 26 | 45,5±13,6 | Male: 10 (38,46) Female: 16 (61,54) |
Ellipsys Vascular Access System |
| Hull et al [18], 2018 | Prospective Cohort Study | 107 | 56,7±12 | Male: 78 (72,9) Female: 29 (27,1) |
Ellipsys Vascular Access System |
| Inston et al[23], 2019 | Prospective comparative study | 30 | 57±15 | Male: 25 (75) Female: 5 (30) |
Wavelin Q EndoAVF System/Surgical AVF |
| Kitrou et al [19], 2022 | Retrospective Cohort Study | 30 | 55,3±13,6 | Male: 30 (100) Female: 0 (0). |
Wavelin Q EndoAVF System |
| Lok et al [17], 2017 | Prospective Cohort Study | 60 | 59 ±13,6 | Male: 39 (65) Female: 21 (35) |
Everlin Q EndoAVF System |
| Mallios et al[46] , 2020 | Retrospective Cohort Study | 234 | 64 | Male: 148 (63,24) Female: 86 (36,76) |
Ellipsys Vascular Access System |
| Mordhorst et al[58], 2022 | Retrospective comparative study | 61 | 64 | Male: 46 (75,4) Female: 15 (24,6) |
Everlin Q EndoAVF/Surgical AVF |
| Osofsky et al[59], 2021 | Retrospective comparative study | 24 | 56,7±22,6 | Male: 12 (50) Female: 12 (50) |
Ellipsys Vascular Access System/ Surgical AVF |
| Radosa et al [60], 2017 | Retrospective Cohort Study | 8 | 57 | Male: 6 (75) Female: 2 (25) |
Everlin Q EndoAVF System |
| Rajan et al [61], 2015 | Prospective Cohort Study | 33 | 51±11,4 | Male: 20 (61) Female: 13 (39) |
Everlin Q EndoAVF System |
| Shahverdyan et al [20], 2020 | Retrospective comparative study | 100 | 64,18 ± 14,18 | Male: 69 (69) Female: 31 (31) |
Ellipsys Vascular Acces System/ Wavelin Q EndoAVF System |
| Shahverdyan et al [62], 2021 | Restrospective comparative study | 89 | 67,9 | Male: 58 (65,2) Female: 31 (34,8) |
Ellipsys Vascular Access System/ Surgical AVF |
| Sultan et al [63] | Retrospective Cohort Study | 18 | 63,8 | Male: 10 (55,6) Female: 8 (44,4) |
Everlin Q EndoAVF System |
| Zemela et al [21], 2021 | Retrospective Cohort Study | 32 | 60,2 | Male: 23 (71,9) Female: 8 (28,1) |
Wavelin Q EndoAVF System |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



