
Submitted:
08 August 2024
Posted:
09 August 2024
You are already at the latest version
Abstract
Objectives: To rate the effects of low molecular weight hyaluronic acid (LMWHA) solution and high concentration oxygen (HCO) through a specific medical device (Caress Flow©), compared to topical administration of hyaluronic acid (HA) alone on symptoms of mild and moderate stress and mixed urinary incontinence in women with genitourinary syndrome of menopause (GSM).
Methods: A total of 68 postmenopausal women were enrolled (from October 2021 to September 2023). Patients were separated in two groups: one group used therapy with LMWHA solution and HCO combined and the second group used therapy with HA alone. Patient Global Impres-sion of Improvement (PGI-I) as the first outcome was used. As secondary outcomes International Consultation on Incontinence Questionnaire - short form (ICIQ-SF) questionnaire and Internation-al Quality of Life (IQoL) questionnaire were used.
Results: Sixty-eight (68) women, 35 (51%) and 33 (49%), were treated with LMWHA solution and HCO combined and HA alone for 10 weeks, respectively. 28 (80%) versus 7 (20%) women reported an improvement (PGI-I score ≤3) of the symptoms in LMWHA solution and HCO com-bined group versus HA alone group. According to the ICIQ-SF, a statistically significant differ-ence was recorded after treatment between the two groups (median, 7 [5-11] vs 10 [8-11]; P = 0.03). According to the IQoL questionnaire, a statistically significantly lower median score was recorded in the LMWHA solution and HCO combined compared with the HA group, before (71 [IQR 55-81] vs 89 [IQR 67-94]; P < 0.01) and after (78 [IQR 65-86] vs 88 [IQR 72-99]; P = 0.04) treatment.
Conclusions: LMWHA solution and HCO combined might improve the mild and moderate stress and mixed urinary incontinence in this set of women and that it is superior to HA therapy alone. However, these results need to be confirmed in further studies with a controlled design and a larger population.
Keywords:
hyaluronic acid and high concentration oxygen
; menopause
; genitourinary syndrome
; stress incontinence
; mixed urinary incontinence
1. Introduction
“Genitourinary Syndrome of Menopause” (GSM) is a chronic condition characterized by the set of signs and symptoms associated with absence of estrogens (ER) and other sex steroids caused by the cessation of ovarian function, involving lower genital structures (labia majora/minora, clitoris, vestibule, vagina and vulva) and the lower part of the urinary tract (specifically bladder trigone and proximal urethra) [1]. GSM is a common disorder (affecting approximately 50 to 70% of post-menopausal women), but at the same time it is frequently under-diagnosed and consequently under-treated. Symptoms related to GSM, especially those at the vulvo-vaginal level, interfere with sexual satisfaction (74%), sexual spontaneity (70%) and relationship with one’s own partner (66%) [2], therefore they are the main cause of discomfort in sexual intercourse, which consequently are often avoided, with further worsening of the condition atrophy and consequent negative impact on the couple’s relationship, with a strong impact on life quality [3]. In Italy the prevalence is comparable to the average of other European countries. In “The AGATA Study” by F. Palma and collaborators, 79.1% of post-menopausal women involved in the study is affected by GSM, with a prevalence varying from 64.7% one year from menopause, to 84.2% in the following six years [4]. Hypoestrogenism following menopause represents the main pathogenetic cause of GSM, but there are several concomitant risk factors [5]. Regarding the pathophysiology of urinary signs and symptoms of GSM, it was seen that the urethra becomes atrophic and prominent with a relative increase of transitional cells and a reduction of intermediate and superficial squamous cells. There is a remodeling of the bladder with reduction of the tropism of smooth muscle tissue and collagen. This involves a reduction in the contractile force of the detrusor, bladder capacity and sensitivity, urethral closure pressure and urinary flow [6,7]. The absence of ER receptors at the trigone level determines a reduction in the bladder sensory threshold with a reduction in pressure to the point of leakage, leading to urgency incontinence and bladder hyperactivity [8]. Furthermore, the loss of collagen is also responsible for the greater laxity of the structures support of the pelvic floor thus contributing to the genesis of the clinical pictures of prolapse genitals and urinary incontinence characterizing GSM. There are currently various therapeutic options to choose, based on the patient’s clinical history and the severity of the symptoms: non hormonal therapy, hormonal therapy, and laser therapy [9]. Several studies have highlighted how topical oxygen therapy is useful in counteract inflammatory dermatological diseases, androgenic alopecia, and dry eyes [10,11,12]. In the literature it is indicate that oxygen, in addition to having an anti-inflammatory and antibacterial, would appear to induce the stimulation of collagen synthesis and would promote hydroxylation. Increasing oxygen could promote release of VEGF (Vascular Endothelial Growth Factor)2, increasing the angiogenic stimulus and tropism of tissues [13,14]. Hyaluronic acid is a polymer that is normally found in the connective tissue known for its supporting, hygroscopic, re-epithelizing, viscoelastic, antioxidant, bacteriostatic and anti-inflammatory. Its administration has proven effective in improving dryness, dyspareunia and tropism of the vaginal epithelium in women affected by GSM has also proven to be a valid alternative to conjugated estrogen therapy also having effects on the symptoms of incontinence [15].
2. Materials and Methods
2.1. Study Design
The current study is a double center, retrospective study conducted at the gynecological clinic of the Hospital “Pugliese-Ciaccio” in Catanzaro and ‘’Umberto I ‘’ in Enna. The protocol was approved by the Ethical Committee of the Calabria Region (nr 342, October 2021). Menopausal patients suffering from genitourinary syndrome of menopause with mild and moderate stress and mixed urinary incontinence were enrolled from October 2021 to September 2023. Patients were divided into two groups. The first group received combined therapy with low molecular weight hyaluronic acid (LMWHA) solution and high concentration oxygen (HCO) through a specific device (Caress Flow©). The second group had received topical daily therapy with vaginal tables of hyaluronic acid (HA) for 10 weeks daily.
2.2. Inclusion Criteria and Validated Questionnaire
We enrolled only women with mild or moderate stress and mixed urinary incontinence, after verifying inclusion criteria (good general health; aged between 45 and 70 years; natural or surgical menopause at least 12 months before enrollment, absence of lower urinary tract infections (UTI); absence of pre-existing prolapse; absence of incontinence due to neurological damage; absence of neoplasm affecting the genitourinary system; absence of contraindications to local therapy with high oxygen concentration and hyaluronic acid) and exclusion criteria (prolapse; incontinence due to neurological damage; genitourinary cancer; previous radio/brachytherapy; systemic intake of estrogens, progestins, androgens, selective modulators of estrogen receptor (SERM), intrauterine progestins or vaginal lubricants and moisturizers within 8 weeks, alternatively taking transdermal or vaginal hormonal products within 4 weeks; signs and symptoms of severe urinary incontinence or absence of signs and/or symptoms of urinary incontinence).
The patients were selected based on the score obtained on the questionnaires administered during the first outpatient visit. The questionnaires that we used were approved by the International Consultation on Incontinence (ICI), validated for the Italian language. With the Overactive Bladder Screener (OAB-S) we evaluated the presence of urge incontinence symptoms and with the International Consultation on Incontinence Questionnaire- Short Form (ICIQ-SF) we identified the frequency and entity of urinary leakages, how much these leaks impacted daily activities, and when they appeared. It is composed of three questions plus a multiple-choice question about urine leaks. The total score allows classifying incontinence as mild (scores 1-5), moderate (scores 6-12), severe (scores 13-18), and very severe (scores 19-21). Only women with mild or moderate stress or mixed incontinence (ICIQ-SF score ≤12) were enrolled. The OAB-S is composed of eight questions, with scores ranging from 8 to 48, with a score >8 representative of the presence of incontinence. This questionnaire was repeated at the end of the 5 sessions treatment to verify symptomatic improvements. Also, we administered the International Quality of Life (IQoL) questionnaire. The IQoL is a validated tool composed of 22 questions that evaluate the impact of incontinence on quality of life. Total scores range from 22 to 110. The lower score indicates the stronger impact of urinary incontinence on quality of life. At the end of the 5 sessions of treatment, the Patient Global Impression of Improvement (PGI-I) questionnaire was administered. The PGI-I questionnaire is composed of a single question evaluating the perceived improvement by the patient of a specific symptom after treatment, with scores ranging from 1 (meaning “very much better”) to 7 (meaning “very much worse”). An improvement is defined when the PGI-I score is ≤3. At this point, the women were also asked to answer the ICIQ-SF and the IQoL questionnaires again.
2.3. Treatment Administration
The patients underwent, under medical prescription, combined therapy with low molecular weight hyaluronic acid (LMWHA) solution and high concentration oxygen (HCO) for 15 minutes a session, for a total of 5 sessions at 14-day intervals (for a total of 10 weeks), using the X2 self-cooling device (Caress Flow©) or hyaluronic acid (HA) vaginal tablet therapy (dose is the same of one vaginal tablet each evening for 10 weeks).
2.4. Effectiveness Evaluation Procedures
For both groups, LMWHA solution and HCO combined and HA alone, 30 days after the treatments a follow-up visit was done and in that occasion the following questionnaires were administered to evaluate the possible improvement of urinary symptoms: the first outcome was used Patient Global Impression of Improvement (PGI-I) to investigate the degree of improvement perceived by the patient following the 5-session treatment in the LMWHA solution and HCO combined group in the comparation with local HA group . As secondary outcomes, Overactive Bladder Screener - (OAB-S); International Consultation on Incontinence Questionnaire Short Form (ICIQ-SF); International Quality of Life Questionnaire (IQoL) were administered to both groups. During each session, any adverse event was noted and reported according to the criteria CTGAE.
2.5. Statistical Analyses
The primary endpoint was the difference in the proportion of women who reported improvements (PGI-I scores ≤3) between the two groups. Secondary endpoints were ICIQ-SF and IQoL scores at the end of the 5 sessions of treatment. Descriptive statistics were presented as means and SDs, medians, and interquartile ranges (IQRs) for continuously coded variables or counts and percentages for categorically coded variables. t Test, Kruskal-Wallis test, and χ2 test examined the statistical significance in differences between means, medians, and proportions. Wilcoxon signed ranks test for the paired sample was used to compare continuous nonparametric variables. In all statistical analyses, the R software (University of Toronto, Canada) environment for statistical computing and graphics (R version 4.0.0) was used. All tests were two-sided with a level of significance set at P < 0.05.
3. Results
From October 2021 to September 2023 a total of 68 postmenopausal women were enrolled. Among them, 35 (51,5 %) had started and finished combined therapy with LMWHA solution and HCO combined and 33 (48,5 %) had used therapy with HA alone. In the overall population (Table 1), the median age was 59,7 years (IQR, 45-66 years), and the median menopause age was 58,5 years (IQR, 45-64 years). There was no statistically significant difference in age (P = 0.4) and age at menopause (P = 0.4) between the two groups. All women enrolled reported an OAB-S score >8 (overall median score, 28 [IQR, 22.5-34], and no statistically significant difference was recorded between the two groups, P = 0.9). All women were Caucasian of Italian ancestry.
3.1. Primary Endpoint: PGI-I Questionnaire at 10 Weeks after Treatment
According to the PGI-I questionnaire (Figure 1), a significantly higher percentage of women reported an improvement (score ≤3) in the LMWHA solution and HCO combined group than in the hyaluronic acid (HA) alone group (P < 0.001). Indeed, 28 women (80%) in LMWHA solution and HCO combined group reported an improvement at the end of treatment (2 [7,1%] very much better, 7 [25%] much better, 19 [67.9%] a little better). Conversely, 18 (55%) women in the HA group reported no improvement at the end of the treatment (15 [83,4%] no change, 2 [11,1%] a little worse, 1 [5,5%] much worse).
3.2. Secondary Endpoint I: ICIQ-SF Questionnaire
According to the ICIQ-SF questionnaire (Figure 2), in the between group analysis, no statistically significant difference was recorded before treatment administration between the LMWHA solution and HCO combined and HA alone groups (median score, 12 [6,7,8,9,10,11,12] vs 10 [8,9,10,11,12]; P = 0.8). Conversely, a statistically significant difference was recorded after treatment administration between the two groups (median score, 7 [5,6,7,8,9,10,11] vs 10 [8,9,10,11]; P = 0.03).
3.3. Secondary Endpoint II: IQoL Questionnaire
According to the IQoL questionnaire (Figure 3), in the between group analysis, a statistically significantly lower median score was recorded in the LMWHA solution and HCO combined group than the HA alone group, before (71 [IQR 55-81] vs 89 [IQR 67-94]; P < 0.01) and after (78 [IQR 65-86] vs 88 [IQR 72-99]; P = 0.04) treatment.
4. Discussion
The prevalence of bladder symptoms, such as frequency, urgency, and incontinence, tends to increase around the menopause, although it is still debated whether these disorders are due to menopause, or aging, or a combination of the two. Urinary symptoms are associated with the genitourinary syndrome of menopause (GSM) which is characterized by physical and hormonal modifications. It has been seen that hormonal therapies improve the symptoms of GSM, but to date their time of use/dose and the type of effect on long-term systemic levels are still unclear. Local estrogen therapy has played and plays an important role in maintaining good tropism of the vaginal mucosa, but even in this case not all patients accept it, and, in some situations, the effectiveness might not be optimal. Furthermore, it must be considered the impossibility of hormonal therapies’ use in some categories of women with high risk factors like previous breast cancer or thromboembolic diseases [16]. The use of non-hormonal therapies that significantly improve the symptoms of GSM and the quality of life of affected patients is successful, but many topical, non-hormonal products on the market have demonstrated a temporary positive action in promoting only lubrication but are often not sufficient to solve all the problems related to mild and moderate stress or mixed urinary incontinence of GSM but allow only transient benefits about vaginal tropism, with the consequent need for repeated treatments [17,18]. Several studies support the use of non-hormonal therapies for the treatment of stress and mixed incontinence in postmenopausal women, particularly, several studies have highlighted how topical oxygen therapy is useful in counteract inflammatory diseases, because the oxygen reactivates the microcirculation of the urogenital epithelium favoring neo angiogenesis, stimulates cellular turnover, improving trophism and conveys nutrients to the epithelial cells. A study published in 2018 by Condemi et All. demonstrated how the treatment with LMWHA solution and HCO combined by a specific medical device is useful in the treatment of urinary symptoms related to GSM [11]. In the diagnosis and management of mild and moderate stress or mixed urinary incontinence of GSM, the gynecological evaluation includes accurate medical history and the use of validated questionnaires that investigate the presence, frequency, and the impact of the symptoms on the quality of life, accurate objective examination that searches for signs at the vulvar, vaginal level, request for tests and/or diagnostic procedures that confirm the diagnosis. Once the patients were selected, they were followed for 10 weeks of treatment and at the end they were re-evaluated with the same questionnaires administered at the beginning of the treatment. In this retrospective study, we did not consider patients with severe stress urinary incontinence. The use of the medical device Caress Flow© appears to constitute a valid treatment for GSM, especially useful for urinary symptoms of mild and moderate stress and mixed incontinence, being completely natural, well tolerated by patients with immediate therapeutic effects, with statistically significant improvement in symptoms before and after treatment, with recovery of one’s sexuality, urinary control and without side effects. In our study, the fist endpoint, according to the between-group analyses of the PGI-I questionnaire postmenopausal women with vulvovaginal atrophy, suffering from symptoms of mild and moderate stress or mixed urinary incontinence, reported a subjective improvement of their symptoms at a significantly higher percentage when treated with LMWHA solution and HCO combined than only HA. In our opinion, as there is no biological or pharmacological reason for believing that hyaluronic acid could exert any significant positive or negative effect on stress and mixed urinary incontinence symptoms, its use alone for this indication may be comparable to a placebo, unless it is associated with a combined treatment with HCO, in which an improvement in all questionnaires score was seen used in the post-treatment. Therefore, our data suggest that Caress Flow© device might exert a beneficial effect on the symptoms of urinary urge incontinence in postmenopausal women with vulvovaginal atrophy. In our experience the medical device Caress Flow© had no contraindications or immediate side effects, had effective results perceivable from the first treatment, was pleasant and non-invasive device, the sessions were very lasts (15 minutes) and did not require recovery time. The evaluation of our secondary endpoints led to interesting observations. No difference in the AOB-S and ICIQ-SF total score was detected between the two groups at the beginning of the study, whereas after 10 weeks it was significantly lower for the ICIQ-SF in the LMWHA solution and HCO combined group and HA group. Women using combined LMWHA and HCO solution had a significantly better quality of life at the end of the study. However, this observation is hardly relevant, as the IQoL questionnaire score was already significantly higher at the beginning of the study in women who would use LMWHA and HCO combined solution. In conclusion, our study showed a significantly superior effect of LMWHA solution and HCO combined with the medical device Caress Flow© over the use only HA in improving the symptoms of mild and moderate stress or mixed urinary incontinence, the functional and inflammatory state of the vaginal mucosa and above all the quality of life, which agrees with the previous literature. Also, the union of LMWHA solution and HCO represents one of the better alternatives for patients who do not want to take hormones, which they have contraindications or who have had negative experiences with hormone therapies.
Furthermore, patients must be enrolled to increase the sample number and increase the statistical power of our preliminary data or confirmed in a controlled design study, but these first results are encouraging.
5. Conclusions
The current multicenter retrospective study supports the hypothesis that combined therapy with LMWHA solution and HCO with Caress Flow© device might improve the severity of mild or moderate stress and mixed urinary incontinence in this set of women. However, these results need to be confirmed in further studies with a controlled design and a larger population.
Author Contributions
Conceptualization, P.M. and F.Z.; methodology, P.M.; software, D.M.; validation, P.S. and G.S.; formal analysis, B.P.; investigation, B.P.; resources, P.F.; data curation, D.M.; writing—original draft preparation, P.F.; writing—review and editing, B.P..; visualization, P.M.; supervision, F.Z. and P.S.; project administration, P.M.; funding acquisition, P.M.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethical Committee of the Calabria Region (nr 342, October 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Angelou K, Grigoriadis T, Diakosavvas M, Zacharakis D, Athanasiou S. The Genitourinary Syndrome of Menopause: An Overview of the Recent Data. Cureus. 2020 Apr 8;12(4):e7586. [CrossRef]
- Lukacz ES, Santiago-Lastra Y, Albo ME, Brubaker L. Urinary Incontinence in Women: A Review JAMA. 2017 Oct 24;318(16):1592-1604. [CrossRef]
- Palma F, Volpe A, Villa P, Cagnacci A; Writing group of AGATA study. Vaginal atrophy of women in postmenopause. Results from a multicentric observational study: The AGATA study. Maturitas. 2016 Jan;83:40-44. [CrossRef]
- Mitchell CM, Waetjen LE. Genitourinary Changes with Aging. Obstet Gynecol Clin North Am. 2018 Dec;45(4):737-750. [CrossRef]
- Gandhi J, Chen A, Dagur G, Suh Y, Smith N, Cali B, Khan SA. Genitourinary syndrome of menopause: an overview of clinical manifestations, pathophysiology, etiology, evaluation, and management. Am J Obstet Gynecol. 2016 Dec;215(6):704-711. [CrossRef]
- Sturdee DW, Panay N; International Menopause Society Writing Group. Recommendations for the management of postmenopausal vaginal atrophy. Climacteric. 2010 Dec;13(6):509-22. [CrossRef]
- Traish AM, Vignozzi L, Simon JA, Goldstein I, Kim NN. Role of Androgens in Female Genitourinary Tissue Structure and Function: Implications in the Genitourinary Syndrome of Menopause. Sex Med Rev. 2018 Oct;6(4):558-571. [CrossRef]
- Nappi RE, Particco M, Biglia N, Cagnacci A, Di Carlo C, Luisi S, Paoletti AM. Attitudes and perceptions towards vulvar and vaginal atrophy in Italian post-menopausal women: Evidence from the European REVIVE survey. Maturitas. 2016 Sep;91:74-80. [CrossRef]
- Claudia Collà Ruvolo, MD,1 Olimpia Gabrielli, MD,1 Carmen Formisano, MD,1 Gianluigi Califano, MD,1 Paolo Manna, MD,2 Roberta Venturella, MD,2 and Costantino Di Carlo, MD1 Prasterone in the treatment of mild to moderate urge incontinence: an observational study , The Journal of The North American Menopause Society 2022. [CrossRef]
- Piovella et al. Effects of high concentration oxygen in combination with sodium hyaluronate, in the meibomites secondary to chronic blepharitis and palpebral tonicity. Euvision 2017; 2/17 p. 5.
- Condemi L. et al. Vaginal Natural Oxygenation Device (VNOD): concomitant administration of hyaluronic acid and topical hyperbaric oxygen to treat vulvo-vaginal atrophy. European Review for Medical and Pharmacological Sciences 2018. Accepted publication.
- Patel et al. Oxygen: from the benefits of inducing VEGF expression to managing the risk of hyperbaric stress. Antioxid Redox Signal. 2005 Sep-Oct;7(9- 10):1377-87. [CrossRef]
- Jokar A, Davari T, Asadi N, Ahmadi F, Foruhari S. Comparison of the Hyaluronic Acid Vaginal Cream and Conjugated Estrogen Used in Treatment of Vaginal Atrophy of Menopause Women: A Randomized Controlled Clinical Trial. Int J Community Based Nurs Midwifery. 2016 Jan;4(1):69-78.
- Tubaro A, Zattoni F, Prezioso D, Scarpa RM, Pesce F, Rizzi CA, Santini AM, Simoni L, Artibani W; Flow Study Group. Italian validation of the International Consultation on Incontinence Questionnaires. BJU Int. 2006 Jan;97(1):101-8. [CrossRef]
- McKown S, Abraham L, Coyne K, Gawlicki M, Piault E, Vats V. Linguistic validation of the NQOL (ICIQ), OAB-q (ICIQ), PPBC, OAB-S and ICIQ-MLUTSsex questionnaires in 16 languages. Int J Clin Pract. 2010 Nov;64(12):1643-52. [CrossRef]
- Lethaby A, Ayeleke RO, Roberts H. Local oestrogen for vaginal atrophy in postmenopausal women. Cochrane Database Syst Rev 2016; 2016: CD001500. [CrossRef]
- Sinha A, Ewies AA. Non-hormonal topical treatment of vulvovaginal atrophy: an up-to-date overview. Climacteric 2013; 16: 305-31. [CrossRef]
- Teodoro, M.C., Scibilia, G., Lomeo, E., ...Scollo, P., Pecorino, B. Carbon dioxide laser as a new valid treatment of lichen sclerosus. Clinical and Experimental Obstetrics and Gynecology, 2019, 46(2), pp. 206–210. [CrossRef]
Figure 1.
The Patient Global Impression of Improvement (PGI-I) questionnaire was administered to 35 women (51%) who received LMWHA solution and HCO combined and 33 women (49%) who received HA alone after 10 weeks of treatment. (A) The PGI-I questionnaire stratified in ≤3 and >3 scores. (B) The PGI-I questionnaire reports all possible answer results.
Figure 1.
The Patient Global Impression of Improvement (PGI-I) questionnaire was administered to 35 women (51%) who received LMWHA solution and HCO combined and 33 women (49%) who received HA alone after 10 weeks of treatment. (A) The PGI-I questionnaire stratified in ≤3 and >3 scores. (B) The PGI-I questionnaire reports all possible answer results.
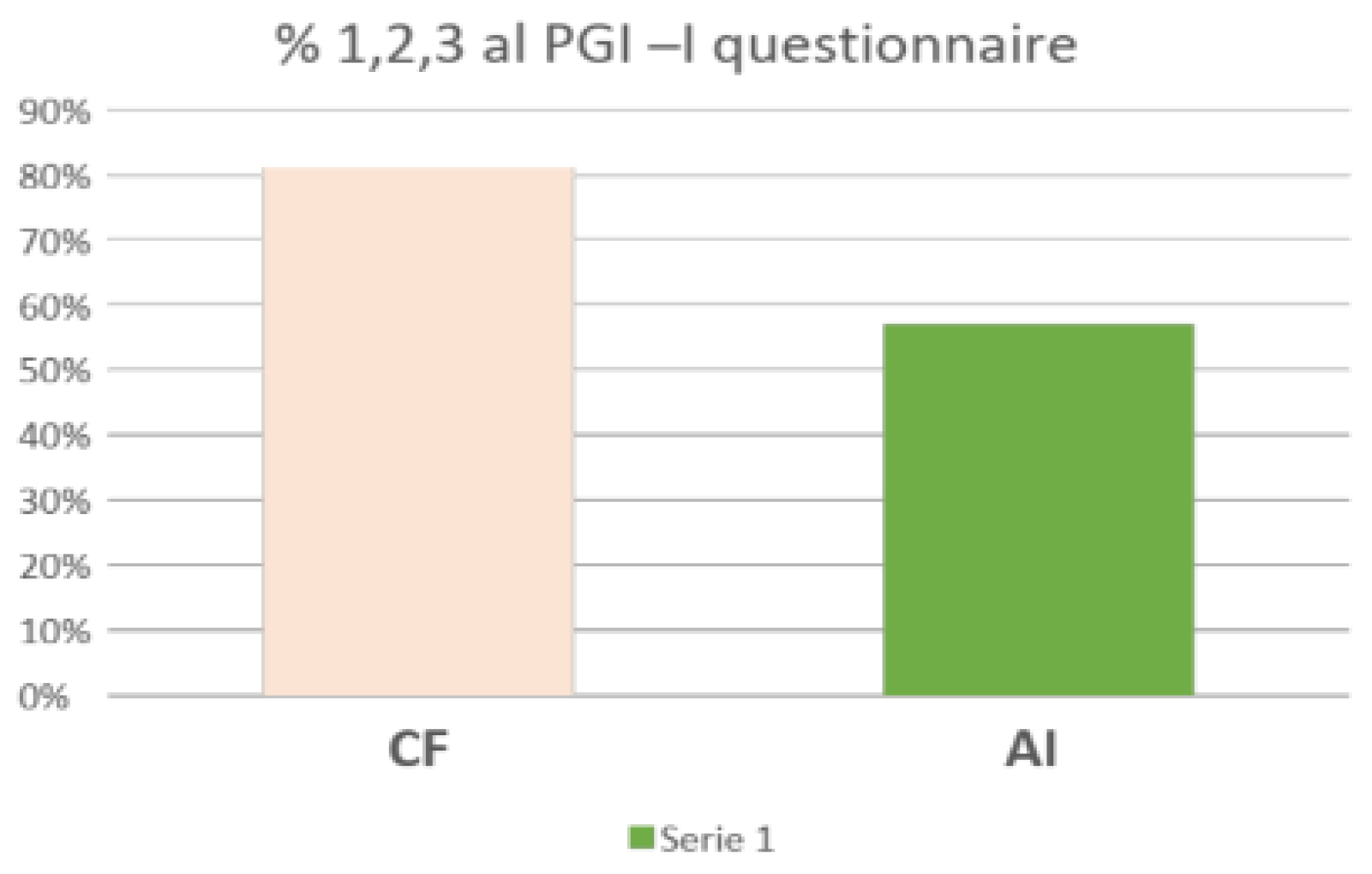
Figure 2.
The International Consultation on Incontinence Questionnaire - short form (ICIQ-SF) questionnaire before (T0, A) and after (T1, B) starting treatment, between LMWHA solution and HCO combined and HA group. Boxes denote the interquartile range. The solid black horizontal bar denotes the median score. Whiskers denote 95% range of the distribution of the ICIQ-SF score. The open circles denote outlier values.
Figure 2.
The International Consultation on Incontinence Questionnaire - short form (ICIQ-SF) questionnaire before (T0, A) and after (T1, B) starting treatment, between LMWHA solution and HCO combined and HA group. Boxes denote the interquartile range. The solid black horizontal bar denotes the median score. Whiskers denote 95% range of the distribution of the ICIQ-SF score. The open circles denote outlier values.
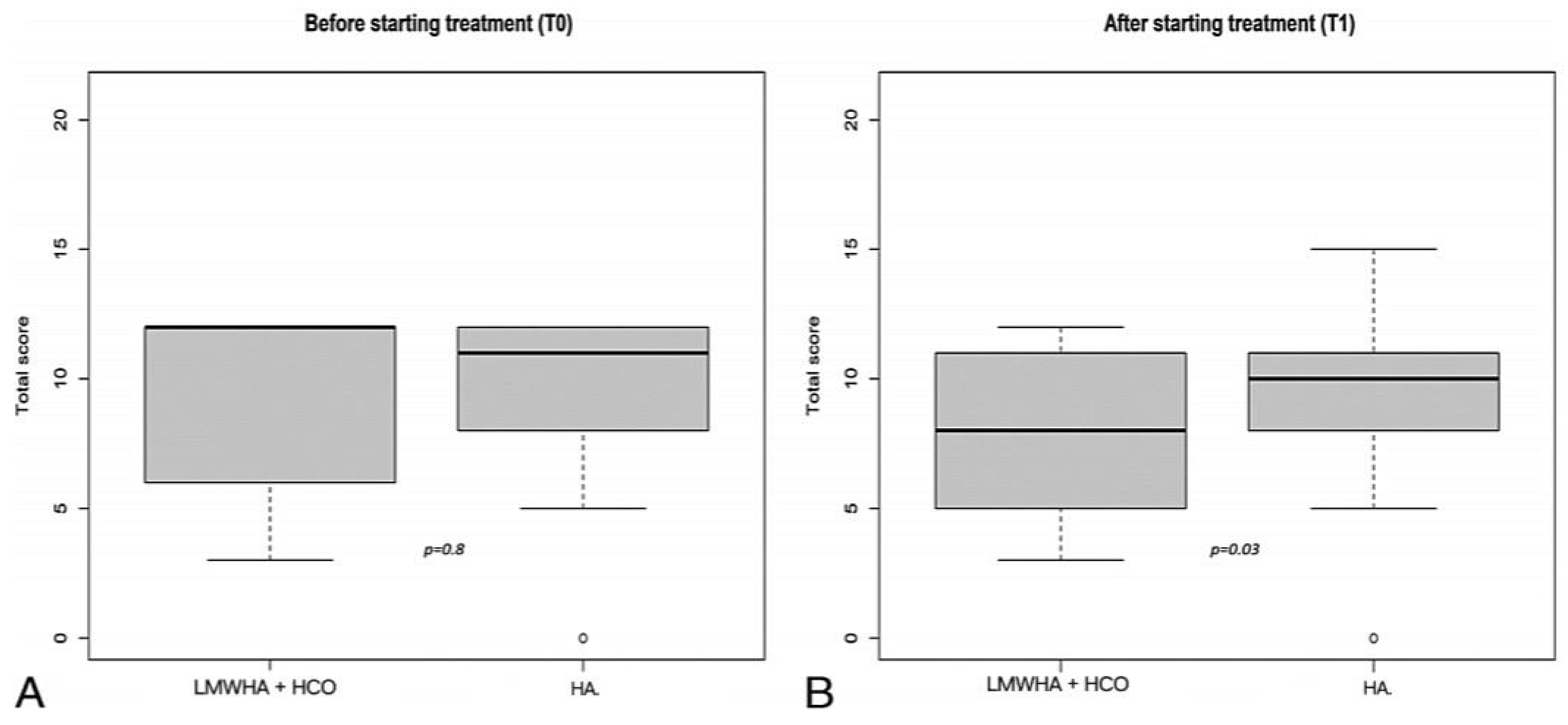
Figure 3.
The International Quality of Life (IQoL) questionnaire before (T0, A) and after (T1, B) starting treatment, between LMWHA solution and HCO combined group and HA group. Boxes denote the interquartile range. The solid black horizontal bar denotes the median score. Whiskers denote 95% range of the distribution of IQoL score.
Figure 3.
The International Quality of Life (IQoL) questionnaire before (T0, A) and after (T1, B) starting treatment, between LMWHA solution and HCO combined group and HA group. Boxes denote the interquartile range. The solid black horizontal bar denotes the median score. Whiskers denote 95% range of the distribution of IQoL score.
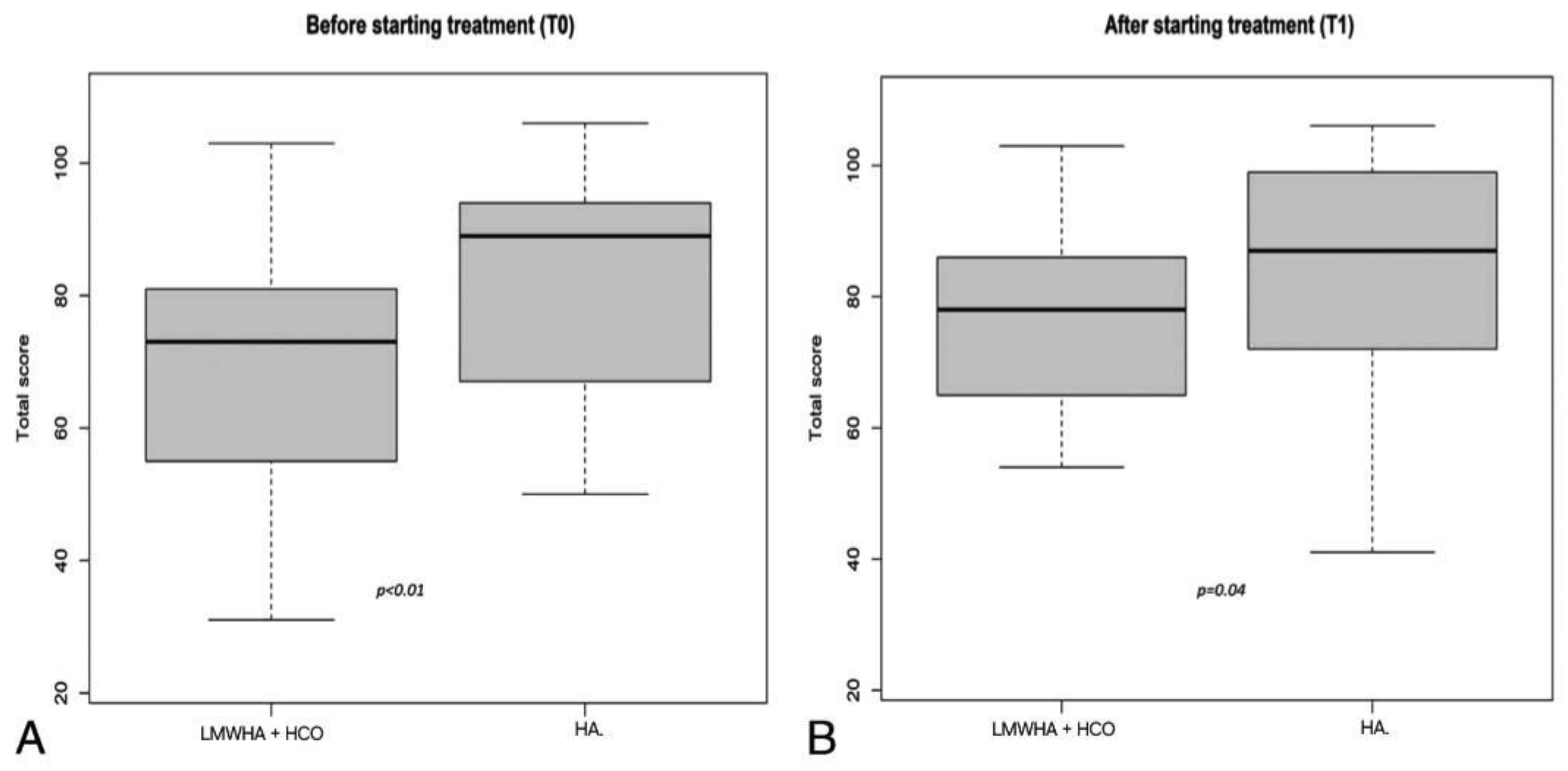

Table 1.
Selection criteria and study population characteristics.
| HCO + LMWH Combined | HA Topically Alone | |
|---|---|---|
| Age | 59,7 | 58,5 |
| BMI | 24,7 | 25,0 |
| Parity | 2,1 | 1,8 |
| LMP (y) | 50,2 | 51,2 |
| Distance from LMP (y) | 5,5 | 6,0 |
| IQoL score pre-treatment | 73 | 89 |
| OAB score pre treatment | 27 | 26 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



