Submitted:
08 August 2024
Posted:
08 August 2024
You are already at the latest version
Abstract
Background: Telemonitoring systems in cardiology have shown potential in improving chronic cardiovascular disease (CVD) management. This study aims to evaluate the impact of telemonitoring, mainly through mobile applications, on patient outcomes such as self-care, blood pressure control, quality of life, and hospitalization. Methods: We systematically reviewed studies assessing telemonitoring methods for patients with chronic CVD. The analysis included studies from various geographic regions and healthcare settings, focusing on qualitative outcomes without performing a meta-analysis. Results: Telemonitoring was found to aid in maintaining blood pressure and significantly enhance self-care abilities. Improvements in quality of life were observed in some studies, though results varied. Most studies indicated telemonitoring could effectively manage blood pressure and reduce hypertension-related complications. However, the heterogeneity of interventions and outcomes measured across trials posed challenges for a comprehensive meta-analysis. Conclusions: Integrating telemonitoring systems into routine care can significantly improve disease management and patient outcomes for chronic CVD patients. Future research should standardize telemonitoring interventions and outcome measures, conduct long-term studies, and evaluate the cost-effectiveness of these systems. Greater blindness in future randomized controlled trials and more studies on atrial fibrillation are also necessary. Significant potential exists for telemonitoring to improve patient outcomes and assist in managing chronic illnesses.
Keywords:
Telemedicine
; Heart failure
; Atrial fibrillation
; Hypertension
; Telemonitoring
1. Introduction
In recent years, the adoption of telemonitoring systems in cardiology has shown significant potential in improving the management of chronic cardiovascular diseases [1]. Telemedicine, defined as using technology to provide healthcare services remotely [2], has become crucial in treating conditions such as hypertension, atrial fibrillation, and heart failure. This approach allows for constant monitoring of patient’s vital parameters, enhancing the timeliness and effectiveness of care.
The benefits of telemonitoring have been documented in various systematic reviews [3,4], which have highlighted how the implementation of such technologies can lead to a significant reduction in hospitalizations and mortality rates, as well as an overall improvement in patient quality of life. However, it is important to note that this systematic review does not include a meta-analysis but focuses on the qualitative analysis of available studies.
The universal definitions of the diseases considered in this review are crucial for contextualizing the results and effectively comparing studies. Hypertension is commonly defined as a systolic blood pressure of at least 140 mmHg and/or a diastolic pressure of at least 90 mmHg [5]. Heart failure is characterized by the heart’s inability to pump sufficient blood to meet the body’s needs [6,7], while atrial fibrillation is a cardiac arrhythmia that results in an irregular and often rapid heartbeat [8].
The rapid development of telemedicine has been further accelerated by the COVID-19 pandemic, highlighting the need for innovative and remote healthcare solutions [9]. During this period, a significant increase in telemedicine services was observed, making it essential to evaluate the effectiveness and efficiency of these interventions in emergency health contexts. Telemedicine facilitated the continuity of care during the pandemic and opened new perspectives for managing chronic diseases, reducing the need for in-person visits, and improving accessibility to healthcare services [10].
The primary objective of this systematic review is to assess whether the use of telemonitoring systems for patients with chronic cardiovascular diseases can improve their quality of life, including psychological and physical health, and increase their awareness of the disease and management methods. Specifically, the focus is on the effectiveness of these systems in improving disease-specific parameters, quality of life, and patients’ ability to self-manage their condition.
In this context, telemonitoring presents a promising solution to address the challenges posed by cardiovascular diseases. Several studies [11,12,13,14,15,16] have demonstrated that using remote monitoring devices and mobile applications can lead to better blood pressure control, reduced heart failure symptoms, and improved patients’ quality of life. Moreover, the real-time monitoring of vital parameters allows physicians to intervene promptly in case of a deterioration in the patient’s condition, thereby enhancing the effectiveness of prescribed therapies.
Despite the numerous advantages, there are still some barriers to the widespread adoption of telemedicine, including the need for adequate technological and secure infrastructure, training of medical personnel, and resistance to change from older patients [17,18,19]. However, with continuous technological advancement and the increasing integration of these solutions into healthcare systems, telemonitoring will likely become an integral part of cardiovascular disease management in the near future.
This systematic review aims to provide a comprehensive overview of the current state of telemonitoring for cardiovascular diseases. It analyzes the results of recent studies and identifies best practices and areas needing further research. The ultimate goal is to provide evidence-based recommendations for effectively implementing these technologies to improve clinical outcomes and the quality of life for patients with chronic cardiovascular diseases.
2. Materials and Methods
This systematic review was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework [20,21,22]. The review aims to answer the following research question: does the use of telemonitoring systems for patients with chronic cardiovascular diseases (CVD) allow for improving their living conditions, including psychological and physical health, and improve their awareness of the disease and management methods?
2.1. Eligibility Criteria
As observed in other studies [23], the PICOS (Population, Intervention, Comparator, Outcomes, Study design) [24] strategy was adopted to perform the research and the selection of the studies to determine the inclusion criteria of articles in the review. In the following subsections, the eligibility criteria for each of the categories of the PICOS strategy are explained in detail.
2.1.1. Population
All studies between 2020 and 2024 analyzing the effects of a telemedicine intervention on patients aged 18 years or older were considered eligible for inclusion if they had one or more of the following cardiovascular diseases: hypertension, heart failure, or atrial fibrillation.
2.1.2. Intervention
The considered trials concerned the use of systems enabling medical practitioners to remotely monitor disease-specific parameters of intervention group participants. Only trials in which patients in the intervention group received a telemonitoring device to collect disease-related parameter values or a smartphone app to send their data to the medical center were included. The remote patient monitoring devices must be able to transmit the collected data to the medical team so that the latter can make appropriate changes to the therapy.
2.1.3. Comparator
Studies in which the usual care (UC) or a more limited intervention (e.g., a version of the app with fewer functionalities concerning the app used in the intervention) was used in the control group were considered eligible for inclusion in the systematic review.
2.1.4. Outcomes
Consideration was given to trials in which the results being measured are related to the improvement of the patient’s living condition, understood both as physical or psychological health and as a better awareness of the disease and the techniques for managing it, i.e., improvement in quality of life, disease-specific parameters, ability to measure these parameters, self-care, etc.
2.1.5. Study Design
Only randomized controlled trials (RCTs) were included, while non-randomized or non-controlled trials, study protocols and designs, cross-sectional, retrospective, qualitative, observational, and pilot studies, conference proceedings, feasibility, cost, ancillary, and secondary analyses, and all studies not reporting the use of a telemonitoring system were excluded.
2.2. Search Strategy
The literature search covered articles in the PubMed, Scopus, and Web of Science databases and published in English from January 1st, 2020 to February 2nd, 2024. The choice to analyze the period between 2020 and 2024 is motivated by the significant increase in telemedicine services found during the COVID-19 pandemic [25,26,27]. It will be interesting to see whether this topic of research and application is exclusively related to the early times of pandemic-related emergencies or whether it has become common in healthcare. The Supplemental Appendix contains a description of the entire search approach and terms.
All records found were exported in Research Information Systems (RIS) formats, which are fed to EndNote 1, the reference manager used for this review.
All English-language studies were included. The terms used as keywords for the search were ’telemedicine’, ’heart failure’, ’hypertension’, ’atrial fibrillation’, and their synonyms and combinations obtained using Boolean operators. In particular, the following combination of terms was used: (“telemedicine*” AND (“hypertension*” OR “heart failure*” OR “atrial fibrillation*”)).
Prior to the screening stage by study title, all duplicate papers were eliminated via a reference management tool.
2.3. Study Selection
The studies were selected using the appropriate tool produced by Clarivate Analytics, EndNote. In the first step, the title and abstract of the papers from the database search were analyzed, eliminating all articles that did not meet the inclusion criteria. Subsequently, full texts were examined to exclude all articles that did not include remote monitoring of disease-specific parameters in their interventions.
2.4. Data Extraction
We performed independent data extraction and obtained the following information for each trial: authors, year, country, and reference; number of participants and their age and sex; health condition; type of intervention (how the data are transmitted, follow-up duration, etc.); comparator (usual care, different interventions, etc.); outcomes (primary and secondary); impact of telemonitoring intervention on outcomes, compared to the control group.
2.5. Risk of Bias Assessment
We performed an independent risk of bias assessment of all papers using the Cochrane Risk of Bias 2 [28,29], the standard de facto for the evaluation of bias in studies 2. All included studies were classified into five different domains according to three levels of bias: low, medium, and high. Some outcomes, such as hospitalizations and mortality, are unlikely to be influenced by the lack of blindness. In contrast, others, such as improvement in quality of life (QoL), disease-specific knowledge, or self-care, are likely influenced by patient subjectivity.
3. Results
3.1. Study Selection and Characteristics
There were 866 articles found in all. The remaining 831 records were assessed for inclusion/exclusion criteria based on their title and abstract after 35 duplicates were removed. According to this screening, 793 works that did not fit the inclusion requirements were dropped. After reading 38 whole texts in all, 22 of them [30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51] were considered appropriate after the selection process since they met all the standards (Figure 1).
Table 1, Table 2, and Table 3 show the characteristics of the studies included in the analysis, respectively, for the three diseases reviewed, i.e., hypertension, atrial fibrillation, and heart failure. Less than 100 patients were included in each arm of a large number (12/22, 54.5%) of RCTs, and sample sizes range from 40 [49] to 3628 [38]. Most of the included studies were carried out in China (5/22, 22.7%), with a smaller number of studies carried out in Sweden, Germany, and the USA (2/22, 9.1%). Additionally, 4.5% (1/22) of the investigations were conducted in each of the following nations: Iran [31], Jordan [36], Spain [37], UK [45], Greece [41], South Korea [32], Denmark [33], Belgium (in combination with Italy) [34], Australia [35], Singapore [39] and Argentina [49]. The average age ranged from 48 to 80, with a greater percentage of males. Patients in the majority of trials (16/22, 72.7%) were followed for fewer than a year, and follow-up time ranges from 8 weeks [36] to 24 months [37,40]. The variables that were most frequently monitored were blood pressure, quality of life (9/22, 40.91%), self-care (6/22, 27.27%), and hospitalization (4/22, 18.2%). In particular, QoL was measured through SF-36 (consisting of MCS and PCS) [52], EQ-5D-5L [53], MLHFQ [54], AFEQT (2/22, 9.1%) [55], SF-12 [56] and MacNew Heart Disease HRQoL (1/22, 4.5%) [57]. Furthermore, current European recommendations [58] state that a mean office systolic blood pressure (SBP) of at least 140 mmHg and/or a diastolic blood pressure (DBP) of at least 90 mmHg constitute uncontrolled blood pressure. Manual input was the most common data entry method (14/22, 63.6%). At the same time, eight of the strategies under study (36.36%) stated automatic interface using external devices that were wirelessly connected (e.g., scales, blood pressure monitors, etc.). Most trials (18/22, 81.8%) compared the intervention with standard care, which included in-person meetings with general practitioners or the hospital care team and routine visits (outpatient clinics).
3.2. Interventions
For hypertension, Andersson et al. [30] provided participants with a Microlife BP A6 BT monitor and nightly reminders to measure and report blood pressure and other vital signs via a web portal accessible to both patients and healthcare providers. Bozorgi et al. [31] used an app for blood pressure logging, medication reminders, and informational support, alerting family and clinicians if readings were abnormal. Dwairej et al. [36] also offered an app for blood pressure recording and access to educational materials, with data available to clinicians through a web tool. Echeazarra et al. [37] implemented a Telegram bot for twice-daily blood pressure reminders and recording, with data available to healthcare providers. Leupold et al. [42] used a BOSO medicus family 4 monitor, an app, and an online eLearning system for data transmission and graphical analysis. Liu et al. [43] provided an app for logging blood pressure and other health metrics, such as heart rate and medication intake, viewable by healthcare providers. McManus et al. [45] had participants measure blood pressure with an Omron M3 monitor twice each morning for a week each month, with out-of-range values alerting clinicians via email. Meng et al. [46] equipped participants with a sphygmomanometer that automatically uploaded readings to an app accessible by patients and clinicians. Yuting et al. [50] provided a wrist blood pressure monitor that sent daily readings via Bluetooth to a website. Zhang et al. [51] used a Sanjian Tech Co. digital bracelet and app for patients and healthcare providers to log and monitor data automatically.
In atrial fibrillation studies, Guo et al. [38] used an app and photoplethysmography (PPG) smart devices for heart rhythm monitoring, allowing remote or hospital-based management of critical events. Lazaridis et al. [41] had both intervention and control groups use an app to log heart rate, with the intervention group logging additional parameters like blood pressure, weight, glucose levels, oxygen saturation, and therapy adherence. Marcus et al. [44] provided an app for selecting and statistically analyzing triggers for atrial fibrillation episodes, offering probabilistic feedback on potential triggers.
For heart failure, Choi et al. [32] offered an app for daily logging of blood pressure, weight, medication, meals, and exercise, including informational content and direct Q&A with clinicians. Cichosz et al. [33] provided a Samsung Galaxy Tab2, a UA-767 blood pressure monitor, and a precision scale, with data transmitted to a central system and alerts for out-of-range values. Clays et al. [34] used a comprehensive system with a blood pressure monitor, scale, pill organizer, and wristband sensor, with data processed by a decision support system and displayed via a smartphone app installed on a Nokia 6 TA-1021 smartphone. Ding et al. [35] used a digital scale and Samsung Galaxy Tab A to transmit weight data to an online decision support system, generating six possible alerts about weight fluctuation or low-level battery. Jiang et al. [39] combined educational and self-management toolkits with three home visits and an app, only available for experimental group B, for reminders, symptom logging, and communication with medical staff. Koehler et al. [40] provided devices for collecting blood pressure, weight, and electrocardiogram (ECG), which were connected via Bluetooth to a digital assistant transmitting data to a medical center. Sahlin et al. [47] offered the OPTILOGG device, a tablet connected to a scale featuring symptom monitoring, interactive education, and diuretic adjustments, with data shareable to medical practitioners at the patient’s discretion. Upshaw et al. [48] used an app for daily logging of weight, heart rate, blood pressure, and symptoms, with healthcare provider alerts for concerning data. Yanicelli et al. [49] provided a system that included an app for daily logging of health metrics, processing data online, and sending risk alerts to medical staff, with additional educational features and interactive content.
3.3. Risk of bias assessment
Each included study’s RoB2 domain scores are displayed in Supplemental Figure 1. Twenty-one (95.5%) RCTs raised at least some concerns about bias. At the same time, only one (4.5%) was classified as having minimal risk of bias [51].
In particular, two studies (9.1%) showed some concerns about bias in the randomization process. Because of the deviations from the intended interventions, most of the findings (19/22, 86.36%) either raised some concerns or demonstrated a significant risk of bias. Due to incomplete outcome data, three RCTs (13.6%) had problems or a high risk of bias. Of the 22 studies, thirteen (59.1%) have some issues or a significant risk of bias in measuring outcomes. Lastly, only a small number of RCTs (5/22, 22.73%) revealed significant issues or a high risk of bias in the reported outcome selection.
3.4. Outcomes
Most of the involved studies in blood pressure (8/9, 88.9%) showed a positive effect of telemonitoring intervention on the BP control ratio of patients. Concerning quality of life, it must be remembered that the studies do not use a unique metric to measure it, so it is impossible to compare the various trials objectively. However, four out of nine studies (44.4%) monitoring QoL show improvements compared to the control group due to the telemedicine intervention. Most studies (5/6, 83.3%) focusing on self-care demonstrate increases in this variable due to the telemedicine intervention with the control group. Finally, studies concerning hospitalization showed, for the biggest part (3/4, 75%), a positive impact of telemedicine on these outcomes when compared to the control patients.
4. Discussion
4.1. Principal Findings
The impact of telemonitoring methods with mobile applications on patients with chronic cardiovascular illnesses was assessed in this systematic review. Using them enhances self-care and blood pressure control ratios. Some effects varied between the RCTs concerning quality of life. The majority of studies raised at least some bias-related issues. For some of the papers analyzed, the analysis of the risk of bias raised discordant opinions among reviewers and was, therefore, subject to further evaluation.
Most studies showed that telemonitoring helped CVD patients maintain their blood pressure. These results imply that telemonitoring can be very helpful in controlling blood pressure and possibly lowering complications associated with hypertension. Improvements in quality of life were found in four out of nine trials (44.4%), suggesting that telemonitoring approaches could benefit patients’ mental and emotional health. In 83.3% of the trials, improved self-care abilities were observed, highlighting the potential of telemonitoring to enable patients to manage their health conditions better.
4.2. Comparison with Prior Works
Our results are consistent with earlier studies showing the advantages of telemonitoring in treating chronic illnesses. We discovered substantial improvements in blood pressure control [4,12,13,14], and capacity for self-care [15,16], which is in agreement with the findings reported by other authors. Our research reveals a significant influence on quality of life, in contrast to certain previous studies [3,4], and suggests that recent developments in telemonitoring technology may contribute to these good outcomes.
4.3. Strengths and Limitations
This review’s inclusion of a broad range of research from various geographic regions and healthcare settings is one of its strongest points; it offers a thorough summary of the current state of telemonitoring in CVD management. This review does have some limitations, though. Doing a meta-analysis was challenging due to the heterogeneity of the interventions and outcomes measured across trials. Furthermore, there might have been a language bias due to the reliance on studies published in English.
4.4. Practical Implications and Future Developments
Our findings indicate that integrating telemonitoring systems into routine care for patients with CVD could improve disease management and patient outcomes. Healthcare providers should consider adopting telemonitoring technologies to empower patients to manage their conditions more effectively. Policymakers should support the inclusion of telemonitoring into healthcare policies and funding models in order to ensure that patients have access to these beneficial interventions.
Future research should aim to standardize telemonitoring intervention and outcome measures to facilitate meta-analyses and more robust conclusions. It is necessary to lead long-term studies to assess the sustained impact of telemonitoring on patient outcomes. Furthermore, the next studies should focus on the cost-effectiveness of telemonitoring systems to inform policy decisions and healthcare funding allocations, and they could include other RCTs that may have been published after our article’s research.
Further research should ensure greater blindness among healthcare practitioners to reduce bias and improve the reliability of the results. The absence of a substantial number of papers on atrial fibrillation highlights the need for more RCTs focused on this condition to provide a clearer understanding of the benefits and limitations of telemonitoring in this specific patient group.
5. Conclusions
In summary, the findings from this systematic review highlight the considerable benefits of using telemonitoring systems in managing chronic cardiovascular conditions. The evidence points towards notable improvements in patients’ ability to manage their disease, including better control of disease-specific parameters, enhanced quality of life, and stronger self-care practices. Integrating telemonitoring into routine care practices can enhance patient outcomes and support chronic disease management significantly. It is essential for future research to explore further and leverage the full potential of these technologies to maximize their benefits for patients and the healthcare system at large.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, File S1: Search strategy; Figure S1: Risk of bias assessment for included studies undertaken using the RoB2 tool; Table S1: PRISMA checklist.
Funding
This work was supported by the European Union - NextGenerationEU - National Recovery and Resilience Plan (Piano Nazionale di Ripresa e Resilienza, PNRR) - Project: “SoBigData.it - Strengthening the Italian RI for Social Mining and Big Data Analytics” - Prot. IR0000013 - Avviso n. 3264 del 28/12/2021.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We thank Simona Sada and Giuseppe Trerotola for the administrative and technical support they provided.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AF | Atrial fibrillation |
| AFEQT | Atrial Fibrillation Effect on Quality-of-Life |
| BMI | Body-mass index |
| BP | Blood pressure |
| CVD | Cardiovascular disease |
| DBP | Diastolic blood pressure |
| DOAJ | Directory of open access journals |
| ECG | Electrocardiogram |
| EQ-5D-5L | 5-level EuroQol EQ-5D |
| HF | Heart failure |
| HT | Hypertension |
| HRQoL | Health-related Quality-of-life |
| MCS | Mental component summary |
| MDPI | Multidisciplinary Digital Publishing Institute |
| MLHFQ | Minnesota Living with Heart Failure Questionnaire |
| NYHA | New York Heart Association |
| PCS | Physical component summary |
| PPG | Photoplethysmography |
| RCT | Randomized controlled trial |
| QoL | Quality-of-Life |
| SBP | Systolic blood pressure |
| SF-12 | 12-item Short-Form |
| SF-36 | 36-item Short-Form |
| TM | Telemonitoring |
| TTE | Transthoracic echocardiogram |
| UC | Usual care |
References
- Kuan, P.X.; Chan, W.K.; Ying, D.K.F.; Rahman, M.A.A.; Peariasamy, K.M.; Lai, N.M.; Mills, N.L.; Anand, A. Efficacy of telemedicine for the management of cardiovascular disease: A systematic review and meta-analysis. The Lancet Digital Health 2022, 4, e676–e691. [Google Scholar] [CrossRef] [PubMed]
- Bashshur, R.L. On the definition and evaluation of telemedicine. Telemedicine Journal 1995, 1, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Rebolledo Del Toro, M.; Herrera Leaño, N.M.; Barahona-Correa, J.E.; Muñoz Velandia, O.M.; Fernández Ávila, D.G.; García Peña, Á.A. Effectiveness of mobile telemonitoring applications in heart failure patients: Systematic review of literature and meta-analysis. Heart Failure Reviews 2023, 28, 431–452. [Google Scholar] [CrossRef] [PubMed]
- Leo, D.G.; Buckley, B.J.R.; Chowdhury, M.; Harrison, S.L.; Isanejad, M.; Lip, G.Y.H.; Wright, D.J.; Lane, D.A. Interactive Remote Patient Monitoring Devices for Managing Chronic Health Conditions: Systematic Review and Meta-analysis. J Med Internet Res 2022, 24, e35508. [Google Scholar] [CrossRef] [PubMed]
- Giles, T.D.; Berk, B.C.; Black, H.R.; Cohn, J.N.; Kostis, J.B.; Izzo, J.L., Jr.; Weber, M.A. Expanding the definition and classification of hypertension. J Clin Hypertens (Greenwich) 2005, 7, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Coats, A.J.; Tsutsui, H.; Abdelhamid, C.M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Böhm, M.; Butler, J.; et al. Universal definition and classification of heart failure: A report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure. European Journal of Heart Failure 2021, 23, 352–380. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. European Heart Journal 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; Fauchier, L.; Filippatos, G.; Kalman, J.M.; La Meir, M.; Lane, D.A.; Lebeau, J.P.; Lettino, M.; Lip, G.Y.H.; Pinto, F.J.; Thomas, G.N.; Valgimigli, M.; Van Gelder, I.C.; Van Putte, B.P.; Watkins, C.L.; ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2021, 42, 373–498. [Google Scholar]
- KÄdzierski, K.; Radziejewska, J.; SÅawuta, A.; WawrzyÅska, M.; Arkowski, J. Telemedicine in Cardiology: Modern Technologies to Improve Cardiovascular Patientsâ OutcomesâA Narrative Review. Medicina 2022, 58. [Google Scholar] [CrossRef]
- Colbert, G.B.; Venegas-Vera, A.V.; Lerma, E.V. Utility of telemedicine in the COVID-19 era. Reviews in Cardiovascular Medicine 2020, 21, 583–587. [Google Scholar]
- Alvarez, P.; Sianis, A.; Brown, J.; Ali, A.; Briasoulis, A. Chronic disease management in heart failure: Focus on telemedicine and remote monitoring. Reviews in Cardiovascular Medicine 2021, 22, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.S.; Kim, N.S.; Kim, A.Y.; Woo, H.S. Nurse-Coordinated Blood Pressure Telemonitoring for Urban Hypertensive Patients: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health 2021, 18. [Google Scholar] [CrossRef] [PubMed]
- AbuDagga, A.; Resnick, H.E.; Alwan, M. Impact of blood pressure telemonitoring on hypertension outcomes: A literature review. Telemed J E Health 2010, 16, 830–838. [Google Scholar] [CrossRef]
- Duan, Y.; Xie, Z.; Dong, F.; Wu, Z.; Lin, Z.; Sun, N.; Xu, J. Effectiveness of home blood pressure telemonitoring: A systematic review and meta-analysis of randomised controlled studies. J Hum Hypertens 2017, 31, 427–437. [Google Scholar] [CrossRef]
- Nick, J.M.; Roberts, L.R.; Petersen, A.B. Effectiveness of telemonitoring on self-care behaviors among community-dwelling adults with heart failure: A quantitative systematic review. JBI Evid Synth 2021, 19, 2659–2694. [Google Scholar] [CrossRef] [PubMed]
- Strandberg, S.; Backåberg, S.; Fagerström, C.; Ekstedt, M. Self-care management and experiences of using telemonitoring as support when living with hypertension or heart failure: A descriptive qualitative study. International Journal of Nursing Studies Advances 2023, 5, 100149. [Google Scholar] [CrossRef]
- Haleem, A.; Javaid, M.; Singh, R.P.; Suman, R. Telemedicine for healthcare: Capabilities, features, barriers, and applications. Sensors International 2021, 2, 100117. [Google Scholar] [CrossRef] [PubMed]
- Ciampi, M.; Sicuranza, M.; Silvestri, S. A Privacy-Preserving and Standard-Based Architecture for Secondary Use of Clinical Data. Information 2022, 13. [Google Scholar] [CrossRef]
- Silvestri, S.; Islam, S.; Amelin, D.; Weiler, G.; Papastergiou, S.; Ciampi, M. Cyber threat assessment and management for securing healthcare ecosystems using natural language processing. International Journal of Information Security 2024, 23, 31–50. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLOS Medicine 2009, 6, 1–6. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; Chou, R.; Glanville, J.; Grimshaw, J.M.; Hróbjartsson, A.; Lalu, M.M.; Li, T.; Loder, E.W.; Mayo-Wilson, E.; McDonald, S.; McGuinness, L.A.; Stewart, L.A.; Thomas, J.; Tricco, A.C.; Welch, V.A.; Whiting, P.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, https. [Google Scholar] [CrossRef]
- Muka, T.; Glisic, M.; Milic, J.; Verhoog, S.; Bohlius, J.; Bramer, W.; Chowdhury, R.; Franco, O.H. A 24-step guide on how to design, conduct, and successfully publish a systematic review and meta-analysis in medical research. European Journal of Epidemiology 2020, 35, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Ãlvarez Hernández, S.; Castillo, D.; Villa-Vicente, J.G.; Yanci, J.; Marqués-Jiménez, D.; Rodrà guez-Fernández, A. Analyses of Physical and Physiological Responses during Competition in Para-Footballers with Cerebral Palsy: A Systematic Review. Applied Sciences 2024, 14. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Medical Informatics and Decision Making 2007, 7. [Google Scholar] [CrossRef] [PubMed]
- Mann, D.M.; Chen, J.; Chunara, R.; Testa, P.A.; Nov, O. COVID-19 transforms health care through telemedicine: Evidence from the field. Journal of the American Medical Informatics Association 2020, 27, 1132–1135. [Google Scholar] [CrossRef] [PubMed]
- Omboni, S.; Padwal, R.S.; Alessa, T.; Benczúr, B.; Green, B.B.; Hubbard, I.; Kario, K.; Khan, N.A.; Konradi, A.; Logan, A.G.; Lu, Y.; Mars, M.; McManus, R.J.; Melville, S.; Neumann, C.L.; Parati, G.; Renna, N.F.; Ryvlin, P.; Saner, H.; Schutte, A.E.; Wang, J. The worldwide impact of telemedicine during COVID-19: Current evidence and recommendations for the future. Connect Health 2022, 1, 7–35. [Google Scholar] [CrossRef] [PubMed]
- Hincapié, M.A.; Gallego, J.C.; Gempeler, A.; Piñeros, J.A.; Nasner, D.; Escobar, M.F. Implementation and Usefulness of Telemedicine During the COVID-19 Pandemic: A Scoping Review. Journal of Primary Care & Community Health 2020, 11, 2150132720980612. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; Emberson, J.R.; Hernán, M.A.; Hopewell, S.; Hróbjartsson, A.; Junqueira, D.R.; Jüni, P.; Kirkham, J.J.; Lasserson, T.; Li, T.; McAleenan, A.; Reeves, B.C.; Shepperd, S.; Shrier, I.; Stewart, L.A.; Tilling, K.; White, I.R.; Whiting, P.F.; Higgins, J.P.T. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, https. [Google Scholar] [CrossRef] [PubMed]
- Di Francesco, F.; Lanza, A.; Di Blasio, M.; Vaienti, B.; Cafferata, E.A.; Cervino, G.; Cicciù, M.; Minervini, G. Application of Botulinum Toxin in Temporomandibular Disorders: A Systematic Review of Randomized Controlled Trials (RCTs). Applied Sciences 2022, 12. [Google Scholar] [CrossRef]
- Andersson, U.; Nilsson, P.M.; Kjellgren, K.; Hoffmann, M.; Wennersten, A.; Midlöv, P. PERson-centredness in Hypertension management using Information Technology: A randomized controlled trial in primary care. J Hypertens 2023, 41, 246–253. [Google Scholar] [CrossRef]
- Bozorgi, A.; Hosseini, H.; Eftekhar, H.; Majdzadeh, R.; Yoonessi, A.; Ramezankhani, A.; Mansouri, M.; Ashoorkhani, M. The effect of the mobile "blood pressure management application" on hypertension self-management enhancement: A randomized controlled trial. Trials 2021, 22, 413. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.Y.; Park, J.S.; Min, D.L.; Ahn, S.; Ahn, J.A. Heart Failure-Smart Life: A randomized controlled trial of a mobile app for self-management in patients with heart failure. BMC CARDIOVASCULAR DISORDERS 2023, 23. [Google Scholar] [CrossRef] [PubMed]
- Cichosz, S.L.; Udsen, F.W.; Hejlesen, O. The impact of telehealth care on health-related quality of life of patients with heart failure: Results from the Danish TeleCare North heart failure trial. J Telemed Telecare 2020, 26, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Clays, E.; Puddu, P.E.; LuÅ¡trek, M.; Pioggia, G.; Derboven, J.; Vrana, M.; De Sutter, J.; Le Donne, R.; Baert, A.; Bohanec, M.; Ciancarelli, M.C.; Dawodu, A.A.; De Pauw, M.; De Smedt, D.; Marino, F.; Pardaens, S.; Schiariti, M.S.; ValiÄ, J.; Vanderheyden, M.; Vodopija, A.; Tartarisco, G. Proof-of-concept trial results of the HeartMan mobile personal health system for self-management in congestive heart failure. Sci Rep 2021, 11, 5663. [Google Scholar] [CrossRef]
- Ding, H.; Jayasena, R.; Chen, S.H.; Maiorana, A.; Dowling, A.; Layland, J.; Good, N.; Karunanithi, M.; Edwards, I. The Effects of Telemonitoring on Patient Compliance With Self-Management Recommendations and Outcomes of the Innovative Telemonitoring Enhanced Care Program for Chronic Heart Failure: Randomized Controlled Trial. J Med Internet Res 2020, 22, e17559. [Google Scholar] [CrossRef]
- Dwairej, L.; Ahmad, M. Hypertension and mobile application for self-care, self-efficacy and related knowledge. Health Educ Res 2022, 37, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Echeazarra, L.; Pereira, J.; Saracho, R. TensioBot: A Chatbot Assistant for Self-Managed in-House Blood Pressure Checking. J Med Syst 2021, 45, 54. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Lane, D.A.; Wang, L.; Zhang, H.; Wang, H.; Zhang, W.; Wen, J.; Xing, Y.; Wu, F.; Xia, Y.; Liu, T.; Liang, Z.; Liu, F.; Zhao, Y.; Li, R.; Li, X.; Zhang, L.; Guo, J.; Burnside, G.; Chen, Y.; Lip, G.Y.H. Mobile Health Technology to Improve Care for Patients With Atrial Fibrillation. J Am Coll Cardiol 2020, 75, 1523–1534. [Google Scholar] [CrossRef]
- Jiang, Y.; Koh, K.W.L.; Ramachandran, H.J.; Nguyen, H.D.; Lim, S.; Tay, Y.K.; Shorey, S.; Wang, W. The effectiveness of a nurse-led home-based heart failure self-management programme (the HOM-HEMP) for patients with chronic heart failure: A three-arm stratified randomized controlled trial. Int J Nurs Stud 2021, 122, 104026. [Google Scholar] [CrossRef]
- Koehler, J.; Stengel, A.; Hofmann, T.; Wegscheider, K.; Koehler, K.; Sehner, S.; Rose, M.; Deckwart, O.; Anker, S.D.; Koehler, F.; Laufs, U. Telemonitoring in patients with chronic heart failure and moderate depressed symptoms: Results of the Telemedical Interventional Monitoring in Heart Failure (TIM-HF) study. Eur J Heart Fail 2021, 23, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Lazaridis, C.; Bakogiannis, C.; Mouselimis, D.; Tsarouchas, A.; Antoniadis, A.P.; Triantafyllou, K.; Fragakis, N.; Vassilikos, V.P. The usability and effect of an mHealth disease management platform on the quality of life of patients with paroxysmal atrial fibrillation - The emPOWERD-AF study. Health Informatics J 2022, 28, 14604582221139053. [Google Scholar] [CrossRef]
- Leupold, F.; Karimzadeh, A.; Breitkreuz, T.; Draht, F.; Klidis, K.; Grobe, T.; Weltermann, B. Digital redesign of hypertension management with practice and patient apps for blood pressure control (PIA study): A cluster-randomised controlled trial in general practices. ECLINICALMEDICINE 2023, 55. [Google Scholar] [CrossRef]
- Liu, F.; Song, T.; Yu, P.; Deng, N.; Guan, Y.; Yang, Y.; Ma, Y. Efficacy of an mHealth App to Support Patients’ Self-Management of Hypertension: Randomized Controlled Trial. J Med Internet Res 2023, 25, e43809. [Google Scholar] [CrossRef] [PubMed]
- Marcus, G.M.; Modrow, M.F.; Schmid, C.H.; Sigona, K.; Nah, G.; Yang, J.; Chu, T.C.; Joyce, S.; Gettabecha, S.; Ogomori, K.; Yang, V.; Butcher, X.; Hills, M.T.; McCall, D.; Sciarappa, K.; Sim, I.; Pletcher, M.J.; Olgin, J.E. Individualized Studies of Triggers of Paroxysmal Atrial Fibrillation: The I-STOP-AFib Randomized Clinical Trial. JAMA Cardiology 2022, 7, 167–174. [Google Scholar] [CrossRef] [PubMed]
- McManus, R.J.; Little, P.; Stuart, B.; Morton, K.; Raftery, J.; Kelly, J.; Bradbury, K.; Zhang, J.; Zhu, S.; Murray, E.; May, C.R.; Mair, F.S.; Michie, S.; Smith, P.; Band, R.; Ogburn, E.; Allen, J.; Rice, C.; Nuttall, J.; Williams, B.; Yardley, L. Home and Online Management and Evaluation of Blood Pressure (HOME BP) using a digital intervention in poorly controlled hypertension: Randomised controlled trial. Bmj 2021, 372, m4858. [Google Scholar] [CrossRef] [PubMed]
- Meng, W.W.; Bai, Y.Y.; Yan, L.; Zheng, W.; Zeng, Q.; Zheng, Y.S.; Zha, L.; Pi, H.Y.; Sai, X.Y. Effect of Home Blood Pressure Telemonitoring Plus Additional Support on Blood Pressure Control: A Randomized Clinical Trial. Biomed Environ Sci 2023, 36, 517–526. [Google Scholar] [CrossRef]
- Sahlin, D.; Rezanezad, B.; Edvinsson, M.L.; Bachus, E.; Melander, O.; Gerward, S. Self-care Management Intervention in Heart Failure (SMART-HF): A Multicenter Randomized Controlled Trial. J Card Fail 2022, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Upshaw, J.N.; Parker, S.; Gregory, D.; Koethe, B.; Vest, A.R.; Patel, A.R.; Kiernan, M.S.; DeNofrio, D.; Davidson, E.; Mohanty, S.; Arpin, P.; Strauss, N.; Sommer, C.; Brandon, L.; Butler, R.; Dwaah, H.; Nadeau, H.; Cantor, M.; Konstam, M.A. The effect of tablet computer-based telemonitoring added to an established telephone disease management program on heart failure hospitalizations: The Specialized Primary and Networked Care in Heart Failure (SPAN-CHF) III Randomized Controlled Trial. Am Heart J 2023, 260, 90–99. [Google Scholar] [CrossRef]
- Yanicelli, L.M.; Goy, C.B.; González, V.D.C.; Palacios, G.N.; Martà nez, E.C.; Herrera, M.C. Non-invasive home telemonitoring system for heart failure patients: A randomized clinical trial. J Telemed Telecare 2021, 27, 553–561. [Google Scholar] [CrossRef]
- Yuting, Z.; Xiaodong, T.; Qun, W. Effectiveness of a mHealth intervention on hypertension control in a low-resource rural setting: A randomized clinical trial. Front Public Health 2023, 11, 1049396. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Tao, Y.; Zhong, Y.; Thompson, J.; Rahmani, J.; Bhagavathula, A.S.; Xu, X.; Luo, J. Feedback based on health advice via tracing bracelet and smartphone in the management of blood pressure among hypertensive patients: A community-based RCT trial in Chongqing, China. Medicine (Baltimore) 2022, 101, e29346. [Google Scholar] [CrossRef] [PubMed]
- Ware, Jr, J. E.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Quality of Life Research 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed]
- Rector, T.S.; Cohn, J.N. Assessment of patient outcome with the Minnesota Living with Heart Failure questionnaire: Reliability and validity during a randomized, double-blind, placebo-controlled trial of pimobendan. Pimobendan Multicenter Research Group. Am Heart J 1992, 124, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Spertus, J.; Dorian, P.; Bubien, R.; Lewis, S.; Godejohn, D.; Reynolds, M.R.; Lakkireddy, D.R.; Wimmer, A.P.; Bhandari, A.; Burk, C. Development and Validation of the Atrial Fibrillation Effect on QualiTy-of-Life (AFEQT) Questionnaire in Patients With Atrial Fibrillation. Circulation: Arrhythmia and Electrophysiology 2011, 4, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Ware, Jr, J. ; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Höfer, S.; Lim, L.; Guyatt, G.; Oldridge, N. The MacNew Heart Disease health-related quality of life instrument: A summary. Health and Quality of Life Outcomes 2004, 2, 3. [Google Scholar] [CrossRef]
- Stergiou, G.S.; Palatini, P.; Parati, G.; O’Brien, E.; Januszewicz, A.; Lurbe, E.; Persu, A.; Mancia, G.; Kreutz, R.; on behalf of the European Society of Hypertension Council and the European Society of Hypertension Working Group on Blood Pressure Monitoring and Cardiovascular Variability. 2021 European Society of Hypertension practice guidelines for office and out-of-office blood pressure measurement. Journal of Hypertension 2021, 39. [Google Scholar] [CrossRef]
- Russell, S.D.; Saval, M.A.; Robbins, J.L.; Ellestad, M.H.; Gottlieb, S.S.; Handberg, E.M.; Zhou, Y.; Chandler, B.; HF-ACTION Investigators. New York Heart Association functional class predicts exercise parameters in the current era. Am Heart J 2009, 158, S24–30. [Google Scholar] [CrossRef]
| 1 | |
| 2 |
Figure 1.
PRISMA diagram depicting the screening and study selection process
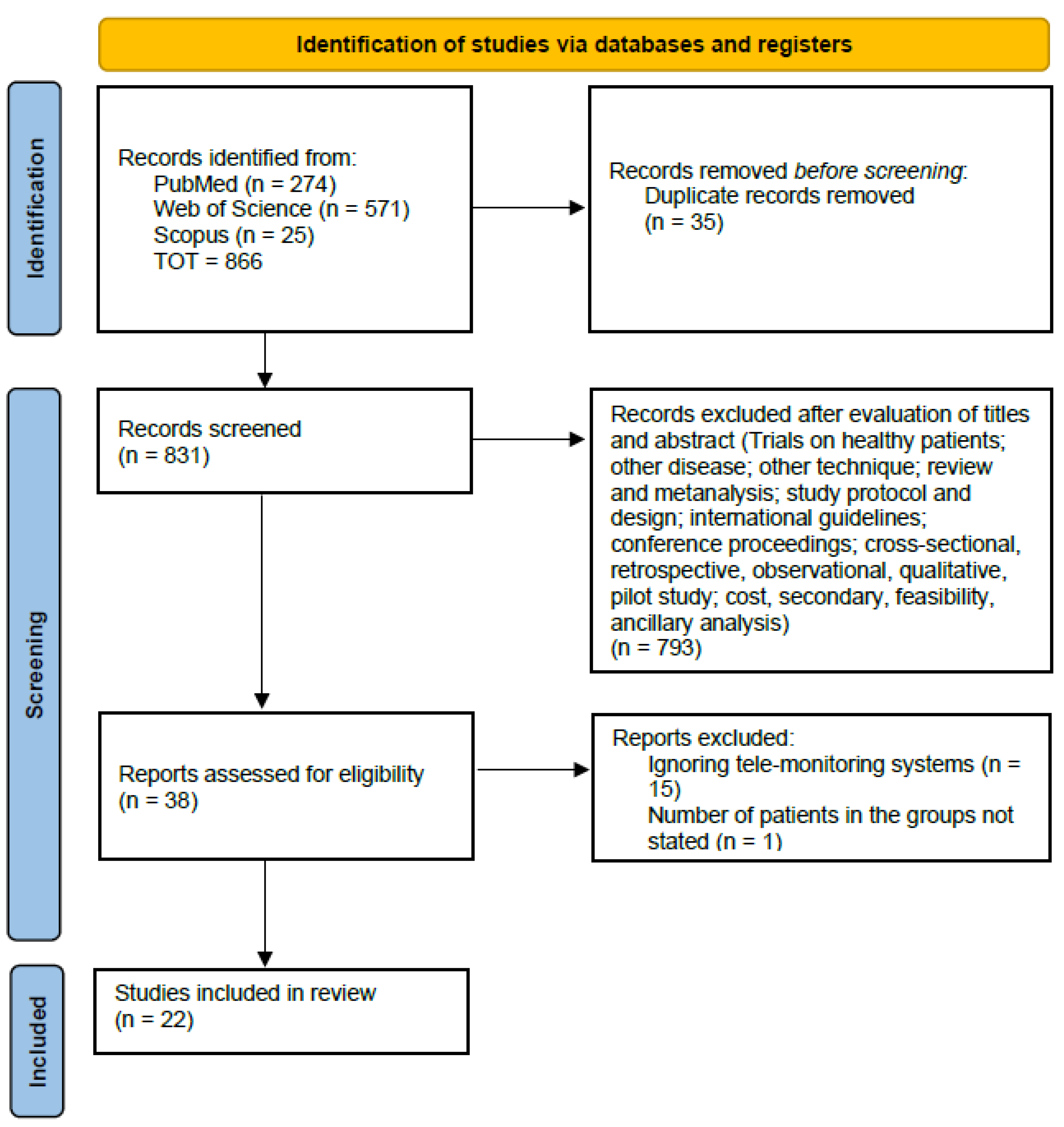

Table 1.
Description of the studies relative to hypertension.
| Study | Intervention / comparator (patients) | Mean age in years (SD), men (%) | Follow-up, patients after | Outcomes | Impact |
|---|---|---|---|---|---|
| Andersson et al., 2023, Sweden [30] | Web-based TM system (482); UC (467) | I: 62.8 (9.8), 283 (58.7); C: 63.0 (10.0), 259 (55.5) at baseline | 12 months; I: 442, C: 420 | % patients with a controlled BP | Positive effect, with uncertain long-term effect |
| Bozorgi et al., 2021, Iran [31] | Mobile app (60); UC (60) | I: 52.0 (8.1), 35 (58.3); C: 51.6 (9.4), 36 (60.0) at baseline | 24 weeks; I: 58, C: 60 | Adherence to treatment; adherence to DASH diet, regular monitoring of BP, physical activity | Positive effect |
| Dwairej et al., 2022, Jordan [36] | Mobile app (75); UC (75) | I: 50.0 (7.3), 32 (56.1); C: 51.0 (5.1), 31 (52.5) after follow-up | 8 weeks; I: 57, C: 59 | Self-care, self-efficacy, knowledge, % patients with a controlled BP | Positive effect |
| Echeazarra et al., 2021, Spain [37] | Telegram chatbot (55); UC (57) | I: 50.2, 32 (58.2); C: 53.9, 33 (57.9) at baseline | 24 months; 88 | Adherence to checking schedule, knowledge and skills on BP checking best practices, satisfaction with intervention | No change on adherence, positive effect on knowledge and skills |
| Leupold et al., 2023, Germany [42] | Patient app connected with a practice management centre (331); UC (305) | I: 56.9 (8.7), 181 (54.7); C: 59.2 (9.7), 154 (50.5) at baseline | 6 months; I: 311, C: 305 | BP control rate, BP changes, satisfaction with intervention | Positive effect |
| Liu et al., 2023, China [43] | Mobile app (148); UC (149) | I: 48.58 (9.54), 78 (52.7); C: 50.64 (8.72), 70 (47) at baseline | 6 months; I: 111, C: 115 | BP control rate, knowledge, changes in lifestyle behavior, blood glucose levels, blood lipid levels, waist-hip ratio, BMI | Positive effect |
| McManus et al., 2021, UK [45] | Self monitoring of BP (305); UC (317) | I: 65.2 (10.3), 160 (52.46); C: 66.7 (10.2), 174 (54.89) at baseline | 12 months; I: 271, C: 282 | Change in BP, drug adherence, HRQoL (EQ-5D-5L) | Positive effect |
| Meng et al., 2023, China [46] | Smart device and a mobile app (95); UC (95) | I: 50.96 (10.50), 50 (59.5); C: 51.45 (12.22), 51 (58.0) after follow-up | 12 weeks; I: 84, C: 88 | BP reduction, % patients achieving the target BP | Positive effect |
| Yuting et al., 2023, China [50] | Smart device and a mobile app (74); UC (74) | I: 61.37 (11.73), 45 (68.18); C: 62.09 (10.66), 38 (55.88) after follow-up | 12 weeks; I: 66, C: 68 | Change in BP, in waist and hip circumference, height and weight; HT adherence, change in self-efficacy and QoL (SF-12) | No change in diastolic BP, positive effect on diastolic BP, HT compliance, mental health |
| Zhang et al., 2022, China [51] | Smart device and a mobile app (164); UC (143) | I: 56.7 (9.3), 44 (42.3); C: 62.6 (10.1), 31 (35.2) after follow-up | 6 months; I: 104, C: 88 | Reduction in BP and weight | Positive effect |
Table 2.
Description of the studies relative to atrial fibrillation.
| Study | Intervention / comparator (patients) | Mean age in years (SD), men (%) | Follow-up, patients after follow-up | Outcomes | Impact |
|---|---|---|---|---|---|
| Guo et al., 2020, China [38] | Mobile app (1786); UC (1842) | I: 67.0 (15.0), 1021 (62.0); C: 70.0 (12.0), 1041 (62.0) after follow-up | 286 days (mean); I: 1646, C: 1678 | Composite of stroke / thromboembolism, all-cause death, hospitalization | Positive effect |
| Lazaridis et al., 2022, Greece [41] | Mobile app (40); Limited version of the app (40) | I: 58.8 (7.9), 27 (68); C: 57.5 (9.4), 26 (65) at baseline | 6 months; I: 40, C: 40 | QoL (AFEQT, EQ-5D-5L) | Positive effect |
| Marcus et al., 2021, USA [44] | Trigger testing with a mobile app (251); Monitoring only with a mobile app (248) | I: 58 (14), 149 (59); C: 58 (14), 140 (56) at baseline | 10 weeks; I: 136, C: 184 | QoL (AFEQT) | No change |
Table 3.
Description of the studies relative to heart failure.
| Study | Intervention / comparator (patients) | Mean age in years (SD), men (%) | Follow-up, patients after follow-up | Outcomes | Impact |
|---|---|---|---|---|---|
| Choi et al., 2023, South Korea [32] | Mobile app (38); UC (38) | I: 70.31 (10.55), 19 (52.8); C: 79.42 (7.59), 16 (42.1) after follow-up | 3 months; I: 36, C: 38 | Differences in BMI, waist circumference, BP, NYHA functional classes [59], TTE, depression, QoL (MacNew), medication adherence | Positive effect on physical factors, no change in psychosocial and behavioral factors |
| Cichosz et al., 2020, Denmark [33] | Tablet and smart devices (145); UC (154) | I: 70, 83 (57.24); C: 69, 79 (51.3) | 12 months; I: 93, C: 100 | Change in HRQoL (SF-36) | Positive effect on MCS, no change on PCS |
| Clays et al., 2021, Belgium & Italy [34] | Smart devices (38); UC (23) | I: 61.8 (11.0), 26 (76.47); C: 65.2 (9.6), 17 (77.27) after follow-up | 6 months; I: 34, C: 22 | Change in HRQoL (MLHFQ), self-management, exercise capacity, illness perception, mental and sexual health | Further studies required |
| Ding et al., 2020, Australia [35] | Smart devices (91); UC (93) | I: 69.5 (12.3), 66 (73); C: 70.8 (12.4), 75 (81) at baseline | 6 months; I: 67, C: 81 | Patient compliance with self-monitoring | Positive effect |
| Jiang et al., 2021, Singapore [39] | A: toolkit for self-care (71); B: additional mobile app (70); C: UC (72) | A: 69.08 (10.51), 35 (71.4); B: 66.82 (11.81), 40 (70.2); C: 68.82 (13.14), 37 (66.1) after follow-up | 6 months; A: 49, B: 57, C: 56 | HF self-care, cardiac self-efficacy, anxiety and depression, HRQoL (MLHFQ), perceived social support | Positive effect |
| Koehler et al., 2020, Germany [40] | Smart devices (339); UC (335) | I: 67.13 (10.92), 272 (80.2); C: 66.88 (10.56), 276 (82.4) at baseline | 24 months; I: 198, C: 210 | Change in depression and HRQoL (SF-36) | Positive effect |
| Sahlin et al., 2022, Sweden [47] | Home-based medical device (62); UC (62) | I: 80 (8), 39 (67.24); C: 77 (11), 32 (53.3) after follow-up | 240 days; I: 58, C: 60 | HF self-care, # HF-related in-hospital days | Positive effect |
| Upshaw et al., 2023, USA [48] | Remote monitoring of parameters and symptoms via a tablet (159); telephone-based management (53) | I: 68, 115 (72); C: 74, 35 (66) at baseline | 90 days; I: 156, C: 52 | # days hospitalized for HF | Further studies required |
| Yanicelli et al., 2020, Argentina [49] | Mobile app (20); UC (20) | 52 y.o., I: 14 (93); C: 10 (66) after follow-up | 90 days; I: 15, C: 15 | Change in HF self-care, treatment adherence, re-hospitalizion | Positive effect |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



