
Submitted:
05 August 2024
Posted:
06 August 2024
You are already at the latest version
Abstract
This retrospective study assesses the efficacy and tolerability of anti-CGRP therapy in adolescents and young adults (ages 12-21) with migraines and chronic daily headaches unresponsive to standard treatments. Migraines severely affect school performance, self-esteem, psychological well-being, and cognitive health in this demographic, who are also sensitive to the side effects of conventional medications often prescribed off-label and face high insurance denial rates. Medication overuse, including analgesics, triptans, and NSAIDs, is prevalent due to treatment failures. Elevated plasma CGRP levels during migraines suggest that anti-CGRP therapies, which have shown success in adults, might benefit this age group. Over three years, patients at a specialized headache center were evaluated for the impact of anti-CGRP treatments, including monoclonal antibodies (erenumab, fremanezumab, galcanezumab) and small molecule CGRP receptor antagonists (ubrogepant, rimegepant, atogepant), either alone or in combination with OnabotulinumtoxinA. The study found significant improvements in migraine management, especially among older adolescents, with reduced rescue medication use and emergency visits. Longer treatment courses and combination therapy with traditional medications were more effective than monotherapy, reducing migraine intensity and frequency. Adverse effects were minimal, and no significant medication interactions were noted. Anti-CGRP therapy demonstrates substantial potential in improving outcomes for this age group with chronic and episodic migraines.
Keywords:
pediatric headache
; migraine
; anti- CGRP
; headache
; anti migraine
Main Manuscript
Introduction/ Objective: Migraine is a debilitating neurological condition significantly impacting adolescents and adults alike. This retrospective study evaluates the efficacy and tolerability of anti- calcitonin gene-related peptide (CGRP) therapy—encompassing monoclonal antibodies and small molecule antagonists—in treating resistant migraines in individuals aged 12 to 21. These therapies used either independently or in conjunction with OnabotulinumtoxinA, target migraines and other chronic headache forms that have not responded to conventional treatments.
Background: Migraines are prevalent among children and adolescents, impacting their long-term school performance, self-esteem, psychological well-being, and cognitive health [1,2]. This presents a therapeutic challenge due to the limited availability of evidence-based prevention options [3]. The success of anti- calcitonin gene-related peptide (CGRP) monoclonal antibodies (mAbs) in preventing migraines and episodic cluster headaches in adults, coupled with minimal adverse events, has generated interest [4,5,6,7,8,9,10,11,12,13]. During migraine episodes, increased plasma levels of CGRP are noted in both adult [14] and pediatric patients [15,16], demonstrating a correlation with headache intensity [16,17]. In the pediatric context, elevated plasma CGRP levels not only differentiate migraines from non-migraine headaches but also offer utility as a biomarker for guiding drug therapy strategies [18] Despite CGRP expression in various body systems [13], recent adult trials have shown minimal adverse events, primarily involving injection site reactions, upper respiratory symptoms, and constipation. These treatments offer an advantage by eliminating the need for daily pill consumption, potentially improving adherence, a common issue with oral migraine preventives [19]. However, extending this success to the younger demographic is impeded by the absence of definitive pediatric and adolescent outcome data, prompting a careful examination of potential risks and benefits [20]. The Pediatric & Adolescent Headache special interest group advocates for a nuanced approach, suggesting the consideration of anti-CGRP mAbs in suitable cases [20]. In 2018, Szperka et al. issued recommendations for the use of anti-CGRP monoclonal antibodies (mAbs) in children and adolescents with migraines. [20] In 2020, Greene et al. conducted the initial study reporting on the safety and efficacy of anti-CGRP mAb use in adolescents with chronic headache disorders. The retrospective multi-site cohort study included adolescents under 18 years with chronic migraine, NDPH, or persistent post-traumatic headache, two-thirds of whom experienced continuous headache at baseline. The findings suggest that anti-CGRP mAb treatment benefits a proportion of adolescents with chronic refractory headache disorders, and the observed side effects align with those reported in adult trials [21]. Expanding the scope to include prevalent headache types in children and adolescents, like New Daily Persistent Headache (NDPH) [22,23] and post-traumatic headache (PTH) [22,24], reveals a therapeutic landscape lacking concrete evidence, necessitating cautious exploration [24,25]. For cases of persistent PTH and sometimes NDPH with a migrainous phenotype resistant to conventional therapies, the consideration of anti-CGRP mAbs is deemed reasonable, recognizing potential pathophysiological overlaps [20,21,24,26,27,28]. In addition to monoclonal antibodies targeting the CGRP pathway (e.g., erenumab, eptinezumab, fremanezumab, galcanezumab), another category of anti-CGRP medications includes small molecule CGRP receptor antagonists known as gepants (e.g., rimegepant, ubrogepant, atogepant), which have been introduced to the market [29]. Numerous clinical trials and real-world observational studies consistently affirm their efficacy and tolerability for both acute and preventive treatment of migraines in adults [30]. While randomized controlled trial data for the pediatric population are pending for both types of medications, the American Headache Society (AHS) has provided recommendations for their use in pediatric headache disorders, as discussed previously [20] Furthermore, OnabotulinumtoxinA was effective in reducing monthly headache days, and the addition of an anti-CGRP monoclonal antibody was safe, well-tolerated, and resulted in meaningful reductions in MHD for those continuing the combined treatment, with no new safety concerns identified. [31,32]. While acknowledging therapeutic potential, a prevailing emphasis on caution is maintained due to the absence of long-term safety data for this age group, highlighting the need for further research and judicious clinical decision-making. The importance of robust trials cannot be overstated, both for informed therapeutic decisions and to advocate for improved access and insurance coverage for this age group [20].
Methodology
This study is a retrospective chart review conducted at a dedicated pediatric headache clinic within the Boys Town National Research Hospital, Nebraska, USA. The study period spanned from October 2020 to December 2023. Approval for the study was obtained from the institutional review board of Boys Town National Research Hospital, and the requirement for written informed consent was waived due to the retrospective nature of the research. There was no external funding source for this study. Data were extracted from the hospital’s electronic medical record (EMR) system, specifically from EPIC EMR. A structured template (Figure 1 and Figure 2) was employed for each clinic visit to document key elements pertinent to headache management, such as the duration and intensity of migraines. This template facilitated consistent monitoring of patient progress across visits. Patient satisfaction data were primarily collected using the clinic template and supplemented by telephone calls. Additionally, patient messages and phone calls were reviewed to gather comprehensive information. The results were systematically recorded for analysis. Patients were identified using a spreadsheet that tracked those receiving anti-CGRP therapy and those who underwent OnabotulinumtoxinA injections within the study period. These patients were either treated under the indicated guidelines for anti-CGRP therapy if they were over 18 or under off-label conditions if younger. These included anti-CGRP monoclonal antibodies targeting the CGRP pathway- erenumab, eptinezumab, fremanezumab, galcanezumab and small molecule CGRP receptor antagonists- rimegepant, ubrogepant and atogepant. Some patients also received Onabotulinumtoxin A in combination with anti CGRP therapy.
The primary conditions targeted include episodic and chronic migraines, new daily persistent headache (NDPH), chronic post-traumatic headache (PTH), and chronic daily headache (CDH). Several factors influenced the decision to initiate anti-CGRP therapy, including the duration of therapy usage, a history of unsuccessful first-line preventive migraine medications, prior medical history such as concussions, psychiatric conditions like anxiety, depression, PTSD, and ADHD, the presence of sleep disorders, and other coexisting neurological conditions such as epilepsy and developmental delays. Patients exclusively receiving abortive anti-CGRP therapies, such as rimegepant or ubrogepant for acute migraine attacks, were excluded from the study.
For each patient, demographic and clinical data were collected, including age group, indication for treatment, duration of use, first-line preventive failures, history of concussion, psychiatric conditions, sleep disorders, and other neurological problems. Additionally, data on the type of anti-CGRP therapy were collected, with some patients using monoclonal antibodies (Mabs), others using antagonists, and some using both. Information was also gathered on whether anti-CGRP therapy was combined with traditional therapy and the purpose of anti-CGRP therapy, whether for rescue, prevention, or both. Furthermore, the study tracked the use of anti-CGRP therapy combined with OnabotulinumtoxinA, response to rescue medications, reduction in rescue medication use, reduction in emergency room (ER) visits, reduction in duration and intensity of migraines, improvement in other bothersome symptoms, reduction in the number of headache days after one month and three months, adverse effects, reasons for discontinuation, and patient satisfaction. The collected data were subjected to statistical analysis to evaluate the effectiveness and safety of anti-CGRP therapies and OnabotulinumtoxinA injections. Key outcomes included the reduction in the number and intensity of headache days after 1 and 3 months of therapy, the decrease in the use of rescue medications, and the reduction in ER visits. Adverse effects and reasons for discontinuation were also analyzed to assess the tolerability of the treatments. Patient satisfaction was also evaluated based on survey responses concerning the overall treatment experience.
This methodology outlines a comprehensive approach to evaluating the effectiveness of anti-CGRP therapies and OnabotulinumtoxinA injections in pediatric patients with chronic migraines. The structured data collection and thorough analysis aim to provide valuable insights into treatment outcomes and patient satisfaction, contributing to the optimization of headache management in this population.
Statistical analyses for this study were conducted using R software, version R 3.6.3, available at R Project. The primary objective was to assess the clinical outcomes associated with the use of anti-CGRP therapy (monoclonal antibodies and/or small molecule antagonists) as a treatment for headaches. To achieve this, descriptive statistics summarized patient data, with categorical variables presented in contingency tables featuring counts and percentages, and continuous variables described through means (± standard deviation) or medians (range). For inferential statistics, Fisher’s exact test was applied to categorical data and the Wilcoxon rank-sum test to continuous data to determine differences between groups. A p-value of less than 0.05 was considered statistically significant, guiding the interpretation of the study’s findings.
Results
This study offers a comprehensive analysis of the effectiveness and application of anti-CGRP monoclonal antibodies (mAbs) and antagonists in treating migraines across various age groups and conditions. A total of 23 patients were included in the study, predominantly young; 39.1% were between 12-15 years, 52.2% were aged between 16-18 years, and a smaller segment, 8.7%, were over 18 years old. Most of these patients were treated for chronic migraines, which accounted for 78.3% of the cases, while episodic migraines comprised 13% of the conditions treated. Less common conditions included new daily persistent headaches (NDPH) and combinations of post-traumatic headaches.
The study also highlighted the complex comorbidities within the patient population, with 91.3% of the participants suffering from psychiatric conditions and 69.6% experiencing sleep disorders. Regarding their medication history, more than half of the patients (56.5%) had not found relief with one to two preventive medications, and 30.4% had not seen improvements with three to four medications (Table 1).
The treatment modalities involving anti-CGRP therapy among the patients were distributed as follows: 39.1% received anti -CGRP combined with traditional treatments, 26.1% were treated with anti-CGRP in conjunction with both OnabotulinumtoxinA and traditional treatments, 21.8% received only anti-CGRP therapy, and 13.0% were treated with anti -CGRP and OnabotulinumtoxinA. Anti-CGRP mAbs were the primary therapy used by 65.2% of the patients, while 13% received antagonists, and 21.7% were treated with a combination of both. Most of the patients (60.9%) used anti-CGRP treatments primarily for prevention, and 39.1% used them for both acute and preventive purposes. These treatments were typically utilized long-term, with 78.3% of patients having used them for over six months (Table 2). It was also noted that the patient group with more than 6 months of use had the most response to rescue medications (p= 0.003), significant reduction in ER visits (p= 0.007) due to reduction in duration and intensity of migraines (p= 0.043, p=0.057 respectively).
86.6% of the patients with anti-CGRP along with traditional therapy (n=13) reported significant reduction in duration of migraine (p = 0.058), in intensity of migraine (p = 0.026). This group also had notable reduction in number of headache days after 3 months (p < 0.001).
The effectiveness of the treatments was notable; 91.3% of patients experienced reduced duration and intensity of migraines, and 82.6% reported improvements in other bothersome symptoms. Additionally, the response to rescue medications improved for 73.9% of patients, and 69.6% reported a reduction of more than fifty percent in the use of rescue medications per week due to improvement in response (p=0.08). There was a significant reduction in the number of headache days; 82.6% saw reductions after one month and 87% after three months, with nearly 40% of patients experiencing more than a fifty percent reduction in both periods. Emergency room visits were reduced for 56.5% of patients (p=0.05).
Moreover, adverse reactions were minimal, with 95.7% of patients reporting no side effects.
The high level of patient satisfaction was reflected in the 69.6% of participants expressing strong satisfaction with their treatment outcomes (p= 0.038), including improved response to rescue medications (p= 0.045), reduction in ER visits (p= 0.019), reduction in duration (p=0.021) and intensity (p= 0.056), improvement in other bothersome symptoms (p= 0.006), significant decrease in the number of headache days (more than 50%) after 1 month (p= 0.021) and 3 months (p= 0.004). Similarly, the continuation rate was also high, with 69.6% opting to continue the treatment. These results underscore the significant potential of anti- CGRP therapies in effectively managing migraines, particularly among younger populations with complex comorbidity profiles (Table 3).
Discussion
Migraine remains a debilitating neurological condition that significantly impacts adolescents, often disrupting daily activities and diminishing their quality of life. The prevalence of migraines in adolescents is increasing, leading to significant academic, psychological, and social challenges [1,2]. This age group is often sensitive to the adverse effects and interactions of conventional migraine medications, many of which are prescribed off-label. In the USA, even among traditional antimigraine treatments, only Topiramate has been approved for labeled use for migraine prevention in patients from 12- 18 years. Among rescue medications, only four triptans—Almotriptan, Rizatriptan, Zolmitriptan ODT, and the Sumatriptan/Naproxen combination—are approved for labeled use. Additionally, high insurance denial or cost concerns due to non-coverage are prevalent. Medication overuse is a major issue with analgesics, triptans, and NSAIDs in this patient population due to treatment failures and resistance. The advent of anti-CGRP therapies has revolutionized adult migraine management, yet their efficacy and safety in the pediatric demographic are not well-documented. The limited pediatric-specific trials for these medications highlight the urgent need for evidence-based therapies tailored to this demographic [20].
This retrospective chart review study addresses these gaps by evaluating the application of anti-CGRP therapies in adolescents with chronic migraine (CM), chronic daily headache (CDH), new daily persistent headache (NDPH), and chronic post-traumatic headache (PTH). Over three years, we analyzed treatment-resistant patients aged 12 to 21 at a specialized headache center, assessing the impact of anti-CGRP treatments, both as monotherapies and in combination with OnabotulinumtoxinA. Our findings indicate substantial improvements in migraine management, including reduced headache days, reduced use of rescue medications, fewer emergency room visits, improved functional outcomes in adolescents, and overall increased patient satisfaction. A longer course of therapy appears to be more effective, as indicated by the reduction in migraine burden and improved response to rescue medications. Additionally, we observed a better response with the combination of anti-CGRP and traditional therapy compared to either monotherapy alone. This improvement has led to enhanced school functionality, participation in academic activities, participation in sports, better sleep patterns, and improvements in psychological conditions as well (less stress, better mood, better concentration, and focus), and fewer school absent days. Hence, it highlights the effectiveness of anti-CGRP therapy in managing migraines among adolescents, a demographic notoriously difficult to treat due to the variability in migraine pathology and treatment response. The therapy showed significant efficacy across various migraine types without correlation with psychiatric comorbidities or prior medication failures. These observations suggest that anti-CGRP therapy could be broadly applicable and effective, warranting its consideration in personalized treatment plans for adolescents. Our findings also align with recent studies suggesting the efficacy of anti-CGRP therapies in adolescents. The American Headache Society and various special interest groups have tentatively recommended these therapies, backed by emerging data from cohort studies [20]. For instance, Greene et al. (2020) noted comparable safety and efficacy in a similar demographic [21]. Our study extends these findings by confirming the substantial therapeutic benefits of combining anti-CGRP therapies with traditional migraine medications, emphasizing a synergistic effect that enhances clinical outcomes.
Furthermore, we were able to take this study one step further by also assessing the efficacy of the combination of anti-CGRP therapy along with OnabotulinumtoxinA, so far, the only retrospective review to do so in this age group. We found that OnabotulinumtoxinA was effective in reducing monthly headache days, and the addition of an anti-CGRP monoclonal antibody was well-tolerated and resulted in meaningful reductions in monthly headache days for those continuing the combined treatment, with no new safety concerns identified.
Adolescents are underrepresented in migraine research, yet they stand to benefit significantly from advances in treatment strategies. Effective management of migraines in this age group can positively impact academic performance, social interactions, overall development, and lessen the migraine burden in their adulthood. Our study provides compelling evidence that anti-CGRP therapy can transform migraine management in adolescents, offering a new horizon in personalized medicine for this age group. The data suggest that these therapies, especially when used for extended periods and in combination with other treatments, could significantly improve clinical outcomes, highlighting the necessity for their consideration in routine clinical practice. Additionally, they were well-tolerated with minimal adverse effects, aligning with findings from adult studies.
Despite the promising outcomes, our study stresses the importance of cautious interpretation and the need for further research to establish long-term safety and efficacy. The absence of long-term data in adolescents calls for careful clinical judgment and monitoring. The promising results of this retrospective study advocate for well-designed prospective clinical trials to validate and expand upon our findings. Such research is essential to solidify the role of anti-CGRP therapy in pediatric migraine management and to support its inclusion in treatment guidelines. Expanding research efforts to include this demographic is crucial to developing tailored and effective therapeutic options.
Conclusions
In conclusion, this retrospective study underscores the promising role of anti-CGRP therapy in managing migraine disorders among adolescents and young adults, a group traditionally underrepresented in migraine research. Notably, the therapy has shown beneficial effects in those unresponsive to conventional treatments, with marked improvements in patient satisfaction, reduction in migraine frequency, and overall quality of life. Our findings suggest that the combination of anti-CGRP therapy with traditional treatments or OnabotulinumtoxinA could offer a synergistic benefit, enhancing the therapeutic outcomes and tolerability. This retrospective study contributes valuable insights into the potential of anti-CGRP therapies in managing migraines in this age group.
While the results are promising, they underscore the need for ongoing research and careful clinical application. Future trials are essential to confirm these findings and to advocate for broader access and insurance coverage for effective migraine management in this vulnerable population. The therapeutic potential is substantial but must be approached with prudence due to the current gaps in long-term safety data.
References
- Fuh JL, Wang SJ, Lu SR, Liao YC, Chen SP, Yang CY. Headache disability among adolescents: a student population-based study. Headache. 2010;50(2):210-218.
- Rocha-Filho PA, Santos PV. Headaches, quality of life, and academic performance in schoolchildren and adolescents. Headache. 2014;54(7):1194-1202.
- El-Chammas K, Keyes J, Thompson N, Vijayakumar J, Becher D, Jackson JL. Pharmacologic treatment of pediatric headaches: a meta-analysis. JAMA Pediatr. 2013;167(3):250-258.
- Goadsby PJ, Reuter U, Hallstrom Y, et al. A controlled trial of erenumab for episodic migraine. N Engl J Med. 2017;377(22):2123-2132.
- Tepper S, Ashina M, Reuter U, et al. Safety and efficacy of erenumab for preventive treatment of chronic migraine: a randomized, double-blind, placebo-controlled phase 2 trial. Lancet Neurol. 2017;16(6):425-434.
- Silberstein SD, Dodick DW, Bigal ME, et al. Fremanezumab for the preventive treatment of chronic migraine. N Engl J Med. 2017;377(22):2113-2122.
- Stauffer VL, Dodick DW, Zhang Q, Carter JN, Ailani J, Conley RR. Evaluation of galcanezumab for the prevention of episodic migraine: The EVOLVE-1 randomized clinical trial. JAMA Neurol. 2018.
- Skljarevski V, Matharu M, Millen BA, Ossipov MH, Kim BK, Yang JY. Efficacy and safety of galcanezumab for the prevention of episodic migraine: Results of the EVOLVE-2 Phase 3 randomized controlled clinical trial. Cephalalgia. 2018;38(6):1026-1037.
- Martinez JM, Goadsby PJ, Dodick DW, et al. A placebo-controlled study of galcanezumab in patients with episodic cluster headache: from the 8-week double-blind treatment phase. Headache. 2018;58:1247-1258.
- Dodick DW, Ashina M, Brandes JL, et al. ARISE: A Phase 3 randomized trial of erenumab for episodic migraine. Cephalalgia. 2018;38(6):1026-1037.
- Dodick DW, Silberstein SD, Bigal ME, et al. Effect of fremanezumab compared with placebo for prevention of episodic migraine: a randomized clinical trial. JAMA. 2018;319(19):1999-2008.
- Bigal ME, Edvinsson L, Rapoport AM, et al. Safety, tolerability, and efficacy of TEV-48125 for preventive treatment of chronic migraine: a multicenter, randomized, double-blind, placebo-controlled, phase 2b study. Lancet Neurol. 2015;14(11):1091-1100.
- Deen M, Correnti E, Kamm K, et al. Blocking CGRP in migraine patients - a review of pros and cons. J Headache Pain. 2017;18(1):96.
- Goadsby PJ, Lipton RB, Ferrari MD. Migraine: current understanding and treatment. N Engl J Med. 2002;346:257-270. [CrossRef]
- Gallai V, Sarchielli P, Floridi A, et al. Vasoactive peptide levels in the plasma of young migraine patients with and without aura assessed both interictally and ictally. Cephalalgia. 1995;15(5):384-390. [CrossRef]
- Fan PC, Kuo PH, Chang SH, Lee WT, Wu RM, Chiou LC. Plasma calcitonin gene-related peptide in diagnosing and predicting pediatric migraine. Cephalalgia. 2009;29(8):883-890. [CrossRef]
- Juhasz G, Zsombok T, Modos EA, et al. NO-induced migraine attack: strong increase in plasma calcitonin gene-related peptide (CGRP) concentration and negative correlation with platelet serotonin release. Pain. 2003;106(3):461-470. [CrossRef]
- Fan PC, Kuo PH, Lee MT, et al. Plasma calcitonin gene-related peptide: a potential biomarker for diagnosis and therapeutic responses in pediatric migraine. Front Neurol. 2019;10:10. [CrossRef]
- Berger A, Bloudek LM, Varon SF, Oster G. Adherence with migraine prophylaxis in clinical practice. Pain Pract. 2012;12(7):541-549.
- Szperka CL, VanderPluym J, Orr SL, et al. Recommendations on the use of anti-CGRP monoclonal antibodies in children and adolescents. Headache. 2018;58(10):1658-1669. [CrossRef]
- Greene KA, Gentile CP, Szperka CL, et al. Calcitonin gene-related peptide monoclonal antibody use for the preventive treatment of refractory headache disorders in adolescents. Pediatr Neurol. 2021;114:62-67. [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38:1-211.
- Grengs LR, Mack KJ. New daily persistent headache is most likely to begin at the start of school. J Child Neurol. 2016;31(7):864-868.
- Kacperski J. Pharmacotherapy for persistent posttraumatic headaches in children and adolescents: a brief review of the literature. Paediatr Drugs. 2018.
- Nierenburg H, Newman LC. Update on new daily persistent headache. Curr Treat Options Neurol. 2016;18(6):25.
- Joshi SG, Mathew PG, Markley HG. New daily persistent headache and potential new therapeutic agents. Curr Neurol Neurosci Rep. 2014;14(2):425.
- Dodick DW, Goadsby PJ, Silberstein SD, et al. Safety and efficacy of ALD403, an antibody to calcitonin gene-related peptide, for the prevention of frequent episodic migraine: a randomized, double-blind, placebo-controlled, exploratory phase 2 trial. Lancet Neurol. 2014;13(11):1100-1107.
- Tyburski AL, Cheng L, Assari S, Darvish K, Elliott MB. Frequent mild head injury promotes trigeminal sensitivity concomitant with microglial proliferation, astrocytosis, and increased neuropeptide levels in the trigeminal pain system. J Headache Pain. 2017;18(1):16.
- Al-Hassany L, Goadsby PJ, Danser AHJ, MaassenVanDenBrink A. Calcitonin gene-related peptide-targeting drugs for migraine: how pharmacology might inform treatment decisions. Lancet Neurol. 2022;21(3):284-294. [CrossRef]
- Charles A, Pozo-Rosich P. Targeting calcitonin gene-related peptide: a new era in migraine therapy. Lancet. 2019;394(10210):1765-1774. [CrossRef]
- Mechtler L, Saikali N, McVige J, et al. Real-world evidence for the safety and efficacy of CGRP monoclonal antibody therapy added to onabotulinumtoxinA treatment for migraine prevention in adult patients with chronic migraine. Front Neurol. 2022;12:788159. [CrossRef]
- Blumenfeld AM, Frishberg BM, Schim JD, et al. Real-world evidence for control of chronic migraine patients receiving CGRP monoclonal antibody therapy added to onabotulinumtoxinA: a retrospective chart review. Pain Ther. 2021;10(2):809-826. [CrossRef]
Figure 1.
Headache note template.
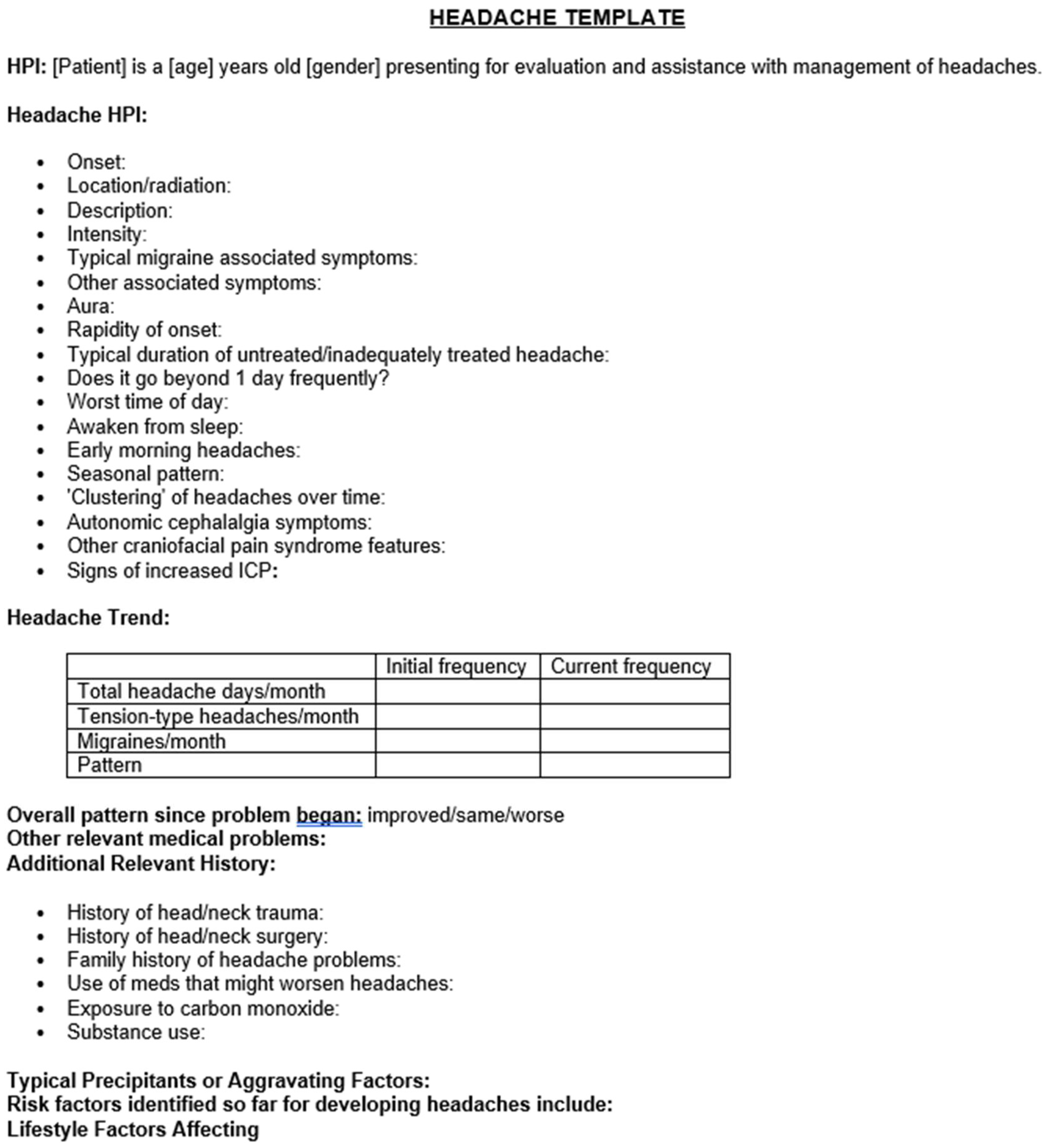
Figure 2.
Headache note template.
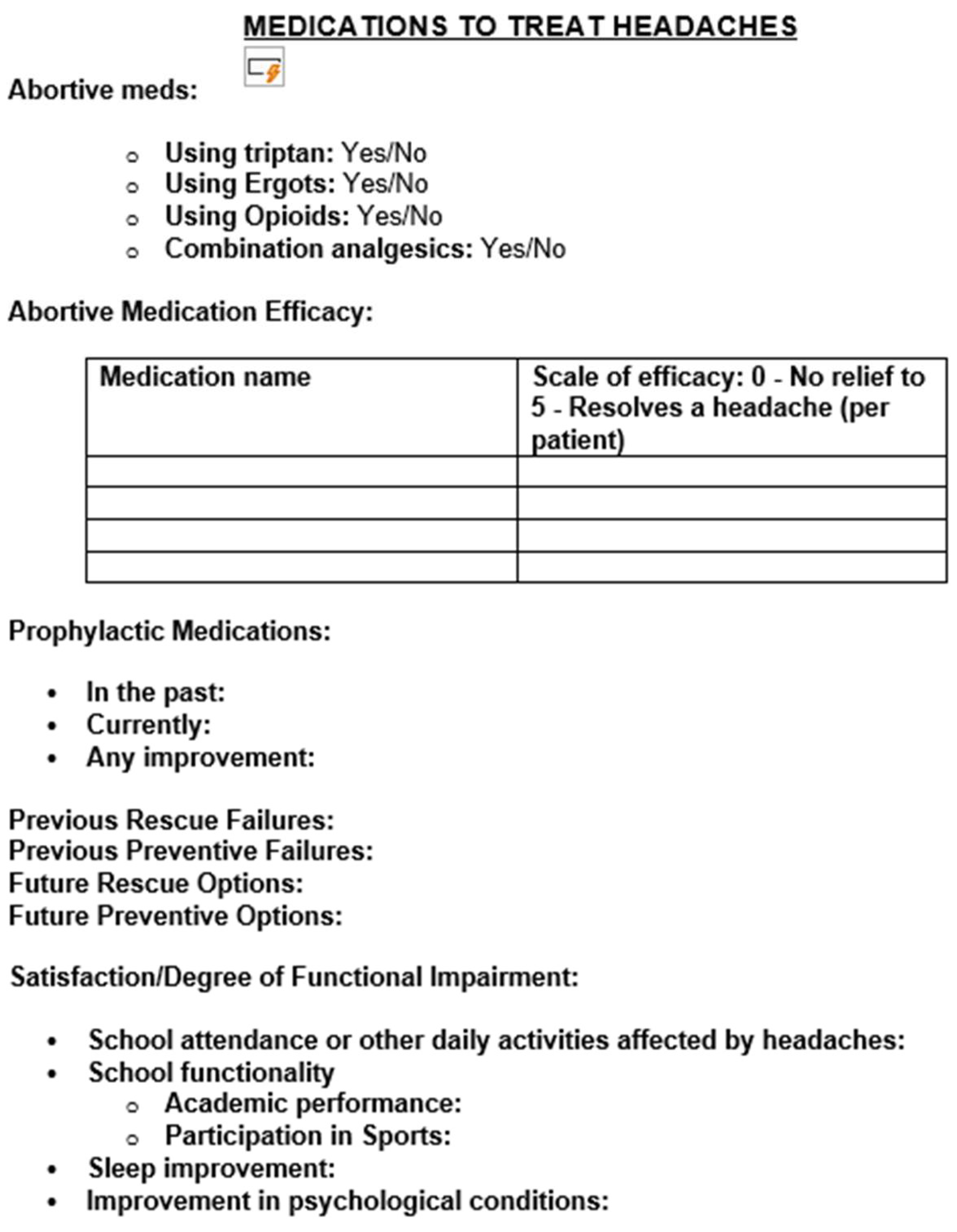

Table 1.
| Table 1 | |
|---|---|
| Column (Variables) | Summary |
| Age Group | n - out of 23 (%) |
| 12-15Y | 9 (39.1) |
| 16-18Y | 12 (52.2) |
| >18 Y | 2 (8.7) |
| Indication | |
| Episodic Migraine | 3 (13) |
| Chronic migraine | 18 (78.3) |
| NDPH | 1 (4.3) |
| Post traumatic (Chronic migraine, NDPH) | 1 (4.3) |
| 1st line preventive failures | |
| 1-2 meds | 13 (56.5) |
| 3-4 meds | 7 (30.4) |
| >4 meds | 3 (13) |
| History of concussion | |
| Yes | 8 (34.8) |
| No | 15 (65.2) |
| Psychiatric conditions | |
| Yes | 21 (91.3) |
| No | 2 (8.7) |
| Sleep disorder | |
| Yes | 16 (69.6) |
| No | 7 (30.4) |
| Other neurological problems | |
| Yes | 5 (21.7) |
| No | 18 (78.3) |
Table 2.
| Table 2 | |
|---|---|
| Column (Variables) | Summary |
| Treatment | n - out of 23 (%) |
| Anti -CGRP + Traditional | 9 (39.1) |
| Anti -CGRP + OnabotulinumtoxinA | 3 (13) |
| Anti -CGRP + OnabotulinumtoxinA + traditional | 6 (26.1) |
| Anti -CGRP alone | 5 (21.8) |
| Months of use | |
| <3 months | 3 (13) |
| 4-6 months | 2 (8.7) |
| >6 months | 18 (78.3) |
| Anti-CGRP therapy for rescue or prevention or both | |
| Rescue | |
| Prevention | 14 (60.9) |
| Both | 9 (39.1) |
Table 3.
| Table 3 | |
|---|---|
| Column (Variables) | Summary |
| Response to rescue meds | n - out of 23 (%) |
| improved | 17 (73.9) |
| no change | 6 (26.1) |
| Reduction in rescue med use in a week | |
| Yes (<50%) | 18 (78.3) |
| No (>50%) | 5 (21.7) |
| ER visits reduction | |
| Yes | 13 (56.5) |
| No | 10 (43.5) |
| Duration of migraines reduced | |
| A lot | 7 (30.4) |
| Some | 14 (60.9) |
| None | 2 (8.7) |
| Intensity of migraines reduced | |
| A lot | 9 (39.1) |
| Some | 12 (52.2) |
| None | 2 (8.7) |
| Other bothersome symptoms improvement | |
| A lot | 9 (39.1) |
| Some | 10 (43.5) |
| None | 4 (17.4) |
| Number of headache days reduction after 1 month | |
| >50% | 9 (39.1) |
| <50% | 10 (43.5) |
| same | 4 (17.4) |
| Number of headache days reduction after 3 months | |
| >50% | 9 (39.1) |
| <50% | 11 (47.8) |
| Same | 3 (13) |
| Adverse effects | |
| Few | 1 (4.3) |
| None | 22 (95.7) |
| Discontinued for any reason | |
| Yes | 7 (30.4) |
| No | 16 (69.6) |
| Patient’s satisfaction | |
| Strongly | 16 (69.6) |
| Doesn’t matter | 5 (21.7) |
| No | 2 (8.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



