
Submitted:
04 August 2024
Posted:
05 August 2024
You are already at the latest version
Abstract
Background
The aims of this study were to assess the peri-operative morbidity, mortality and long-term survival of octogenarians undergoing ATAAD repair, and to compare open and closed distal anastomosis techniques.
Methods
This was a single-centre retrospective study (2007-2021). Open versus closed distal anastomosis were compared. Uni and multi-variable logistic regression analyses were performed to identify independent predictors of in-hospital mortality. Kaplan-Meier and Cox proportional hazards methods were used to compare long-term survival.
Results
Fifty octogenarians patients were included (median age - 82 years, closed distal – 22, open distal - 28). Median CPB time was 187 minutes (open distal vs closed distal group; 219 minutes vs 115.5 minutes, p30 days or return to theatre; HR; 4.1, p=0.02) predicted adverse survival. Open distal anastomosis did no impact survival.
Conclusions –
ATAAD repair in selected octogenarians has favourable short and long-term survival. There is no significant difference between open versus closed distal anastomosis strategies.
Keywords:
acute aortic dissection
; octogenarians
; type A aortic dissection
; perioperative outcomes
Background
The United Kingdom (UK) population is ageing, with >15.5 million people over 60 years old, and 3.2 million octogenarians (4.7%) [1]. The largest increase in population is predicted to be in the older age groups while fraction over 85 years is predicted to double to 3 million by 2041. The proportion of octogenarians undergoing coronary artery bypass grafting has risen 3-fold to 7.2% in UK from 2002 to 2016[2]. With increasing life expectancy and increasing proportion of elderly patients fit for cardiac surgery and cardiology interventions, number of octogenarians with acute Stanford type A aortic dissection (ATAAD) requiring operative intervention is expected to rise over the coming decades. This may also include a new class of more frequent iatrogenic dissections. Outcomes following surgical ATAAD repair have continued to improve over the last decade with large volume aortic centres consistently reporting mortalities of <10%. However, age is perceived as a negative survival predictor and a deterrent for surgical intervention due to poor outcomes[3]. A resource and cost intensive, high-risk emergency surgery for octogenarians remains controversial from a medical and social perspective in overstretched health care systems. The aims of this study were to assess the peri-operative morbidity, mortality and long-term survival outcomes of octogenarians undergoing ATAAD repair, and to compare open and closed distal anastomosis surgical repair techniques.
Methods
Data Collection
This was a single-centre retrospective study (2007-2021) performed at the University Hospital Southampton (UHS). Data for all octogenarian patients who underwent surgical repair of AAATD was collected from the hospital database (Patient Administration System, PAS, e-CAMIS (Electronic Clinical and Management Information System, Yeadon, Leeds, UK). Institutional approvals were obtained for the use of data in compliance with the local data protection policies (Safeguard approval number 7373, 15/11/2022). Consent for individual use of data was waived due to retrospective nature of study and prior approvals at the time of consent for procedures. Inclusion criteria included all octogenarians who underwent emergency/salvage ATAAD repair within 14 days of onset of symptoms. Iatrogenic and intraoperative aortic dissections during cardiac surgery were included. Patients who died without definitive surgery (at or prior to anesthetic induction or prior during the transfer) were excluded.
Baseline demographics included data used for the NICOR (National Institute of Cardiac Outcomes Research, UK) database (Table 1). Operative and postoperative data included type (open versus closed distal anastomosis) and extent of surgery, other concomitant procedures, cannulation technique, cardiopulmonary bypass time (CPB), cross clamp time (XCT), total circulatory arrest time (TCA) and neuroprotection strategy. Postoperative data included return to theatre, new cerebrovascular accident (CVA) , length of hospital stay (LOS), renal replacement therapy (RRT), in-hospital mortality and a composite endpoint consisting of RRT, new CVA, LOS≥30 days, re-exploration and in-hospital mortality.
Long term survival was obtained from PAS, e-CAMIS and the electronic database of General Practitioners’ medical records linked to the hospital database on National Healthcare Service Spine Portal Summary Care Records (SCR) system.
Surgical Techniques
ATAAD was confirmed by preoperative computed tomography in all cases and echocardiography was performed intraoperatively. Surgeons participating in the aortic dissection rota performed the procedures. Cannulation technique, cerebral protection strategy, open versus closed distal anastomosis and degree of hypothermia were selected primarily by the surgeon’s preference and their individual techniques. Our standard surgical procedure consisted of median sternotomy with standard CPB established via femoral/axillary arterial cannulation with systemic hypothermia. Myocardial protection was achieved with antegrade or retrograde cold blood cardioplegia at 4⁰C. All repairs included replacement of the ascending aorta using an interposition graft with open or closed distal anastomosis, with or without extension into the arch/hemiarch and any other concomitant procedures deemed necessary. A tear-oriented surgical strategy was employed. Ascending aortic replacement was performed if the primary tear was in the ascending aorta or in the case it was not identified. Extended aortic resection and repair (hemiarch/arch) were performed if an arch tear was identified. ATAAD involving aortic root was either repaired using Bioglue or aortic root repair/replacement was performed. All open distal procedures were performed under deep hypothermic circulatory arrest (DHCA) at 24-28◦C (nasopharangeal) with/without antegrade selective/non-selective cerebral perfusion depending on cannulation strategy. Near-infrared spectroscopy (NIRS) was used in all cases for neurocerebral monitoring. In the case of significant bilateral discrepancy between NIRS readings, a selective cannulation strategy through the arch was used for cerebral perfusion.
Statistical Analysis
All clinical data were analysed retrospectively through a review of prospectively collected electronic and archived medical records. Postoperative survival was calculated from the time of surgery to death from any cause. Continuous variables are presented as mean ± standard deviation. Categorical variables are presented as counts and percentages. Categorical data were compared with the chi-square test whereas continuous data were compared with the student’s t-test. Demographic data and operative strategies of open versus closed distal anastomosis were compared including preoperative variables. Uni and multi-variable logistic regression analyses were performed to identify independent predictors of in-hospital mortality. Variables with a P-value <0.05 were entered into a multivariable model. Kaplan-Meier and Cox proportional hazards methods were used to compare long-term survival. Statistical analyses were performed using the Stata statistical software v17 (StataCorp. College Station, 2021). P-value of <0.05 was considered statistically significant.
Results
Preoperative Characteristics
Fifty octogenarians underwent surgery for ATAAD (22 with closed distal and 28 with open distal anastomosis). Median age was 82 years (IQR; 80.3-83.4 years) with a female predominance (58%). Five (10%) patients presented with iatrogenic ATAAD either during cardiac catherization or intraoperatively during cardiac surgery. There were no significant differences in preoperative characteristics between patients with open or closed distal anastomosis (Table 1). However, the closed distal group had more commonly preoperative neurological deficit as compared to open distal group (9.3% vs 0%, p=0.10, respectively). Patients in the open distal group had more commonly extracardiac arteriopathy (14.3% vs 4.5%, p=0.25), cardiogenic shock (32.1% vs 13.6%, p=0.13) and lower preoperative haemoglobin 120 vs 127 g/L, p= 0.05). The closed distal group had a higher proportion of patients with previous sternotomy as compared to the open distal group, although the difference was not statistically significant (13.6% vs 3.6%, p=0.19, respectively).
Operative Characteristics
Operative characteristics are demonstrated in Table 2. Femoral artery cannulation was performed most commonly (62%). Median CPB time was 187 minutes (IQR; 121-245 minutes). CPB time was significantly higher in the open distal as compared to the closed distal group (median 219 minutes vs 115.5 minutes, p<0.01, respectively). Median cross-clamp time (XCT) was 93 minutes (IQR; 76-130 minutes). Median TCA time was 26 minutes IQR; 20-39 minutes) in the open-distal group.
Nonselective antegrade cerebral circulation was used for neuroprotection in 22% of all cases and 35.7% of all open-distal anastomosis cases. Concomitant procedures were performed in additional 28%.
Postoperative Characteristics
In-hospital mortality was 18% (14.2% in the open distal vs 22.7% in the closed distal group, p=0.44). We observed higher postoperative CVA rate in the open distal group (39.3% vs closed distal, 22.7%, p=0.21). Intraoperatively, 3 patients (6%) died after failure to wean off CPB. All these 3 patients had iatrogenic ATAAD (cardiac catherization, intraoperative mitral valve replacement and a redo sternotomy) with involvement of the coronary ostia. There was no significant difference in the composite endpoint of RRT, CVA, LOS ≥30 days, re-exploration, and in-hospital mortality (open distal 45.5% vs closed distal 57.1%, p=0.41) (Table 2). LVEF<30, NHYA class 3/4, XCT, LOS, preoperative creatinine, CPB time, concomitant cardiac procedure and male gender were independent predictors of in-hospital mortality on univariate regression, but not multivariate regression (Table 3).
The mean follow-up was 8.5 years and the completion of follow-up was 100%. Median survival was 7.2 years (IQR; 4.5-11.6 years). Long-term survival was comparable between open and closed distal groups (median 10.6 vs 7.2 years, p=0.35, respectively) (Figure 1). Critical preoperative status (preoperative neurological deficit, preoperative renal failure, requirement for intravenous inotropes, cardiogenic shock, or preoperative mechanical ventilation; HR; 3.2, p=0.03) and composite endpoint (RRT, new CVA, LOS>30 days or return to theatre; HR; 4.1, p=0.02) were predictors for adverse long-term survival (Table 4). Open distal anastomosis did no impact survival.
Thirty four percent of the patients were discharged home and the others were sent to a convalescent home (32%) or another hospital (16%) for recuperation. Survival was 75.8 ± 6.1% at 1 year (76.7% for closed distal vs 75.0% for open distal anastomosis, p=0.16) and 55.1 ± 7.7% (7.7%) at 5 years (56.3% for closed distal vs 52.9% for open distal anastomosis, p<0.01).
Discussion
International Registry for Aortic Dissection (IRAD) data demonstrated that surgical repair of ATAAD in octogenarians is associated with improved 5-year survival when compared to medical treatment [4]. IRAD data showed that early postoperative mortality rates appeared similar between septuagenarians and octogenarians (25.1% vs 21.7%, P = 0.205), yet a significantly smaller proportion of octogenarians were operated upon (68.1% vs 85.9%, P< 0.001). Furthermore, comparable rates of postoperative complications demonstrated that surgical repair in selected octogenarians can provide satisfactory outcomes [5,6]. In our series, we demonstrated satisfactory in-hospital mortality and 5-year survival among octogenarians undergoing ATAAD repair, and our results were comparable to IRAD data. However, octogenarians still represent a high-risk group and reported in-hospital mortality after ATAAD repair is generally higher than in younger patients [7,8,9,10,11,12]. Another important finding was that critical preoperative status including preoperative neurological deficit, renal failure, requirement for intravenous inotropes, cardiogenic shock or mechanical ventilation were factors negatively associated with long-term survival of octogenarians (HR; 3.2, p=0.03).
Open distal anastomosis is advocated as the preferred surgical technique [13]. It allows resection of much of the dissected aorta, an easier distal anastomosis even into the hemiarch/arch and arch tears can be inspected. Since prolonged surgery and CPB time may be deleterious in octogenarians, conservative procedures including closed distal anastomosis may be believed to improve outcomes. However, we have previously showed that there was no difference in late survival between patients receiving an open or a closed distal anastomosis [14]. Our mean CPB times and XCT times were comparable to IRAD data: (181.0 mins (142.3–236.8) and 117.0 mins (87.0–156.0) respectively). Although CPB times was significantly longer in our open distal anastomosis group, this did not increase in-hospital mortality (14.2% in open distal vs 22.7% in closed distal anastomosis group. The 5-year survival was comparable in both groups. Such findings suggest that open distal anastomosis with extended resection into the arch in selected octogenarian patients can be performed with satisfactory outcomes. On the other hand, a strategy to do a quicker and less complex operation may be advisable in high risk octogenarians in compromised circumstances of hemodynamic instability, malperfusion or general debility and frailty.
Interestingly, octogenarians account for up to 20% of patients undergoing ATAAD repair in Japan due to an elderly population. Several Japanese studies consistently showed low mortality rates (4.8%-14.3%) and excellent outcomes in octogenarians with both conservative and extended resection techniques [15,16,17,18]. Data from the Japanese Registry of Aortic Dissection (JRAD) for 2011 -2016 however showed that age older than 80 years was a risk factor for in-hospital mortality (odds ratio, 2.37; P < .01) [19]. Other studies, outside of Japan have shown good outcomes of ATAAD repair in octogenarians albeit with higher mortality compared to non-octogenarians [20,21]. A large meta-analysis of 16 retrospective studies by Eranki et al with 16,641 patients showed that octogenarians displayed significantly higher in-hospital mortality than non-octogenarians (OR 1.93; 95% CI 1.33–2.81; P<0.001) [22]. Surprisingly, a 5-year survival in the octogenarian cohort of 54% was significantly lower compared to 76% in the non-octogenarian cohort (P<0.001). Similarly, the meta-analysis by Biancari et al showed in-patient mortality of 18.4% (4%-56%); 20.7% in non-Japanese studies (7%-56%) and 16.3% in Japanese studies (4%-21%). Mean XCT and TCA times were comparable to our study, although their CPB times were shorter 167 versus 187 minutes.
Concerns regarding quality of life (QOL) and resource utilisation after ATAAD repair means that octogenarians are more likely to be managed conservatively [23]. Mean hospital LOS in our study was 16.5 days which is longer than that reported by IRAD (13.0 days). This may represent differences in hospital and intensive care unit discharge policies, and country-based discharge policies; and detailed comparison was not possible. Wide variation is reported in the international literature ranging from hospital LOS of 12-41 days. Although there is an argument for a simpler, more conservative repair technique with a closed distal anastomosis in the elderly to expedite postoperative recuperation, we did not observe a significant difference in LOS in the open distal as compared to the closed distal anastomosis group; (14.6 days versus 13.8 days, p=1.00). Ghazy et al demonstrated that an aggressive surgical strategy did not improve the quality of life in midterm follow-up compared to a defensive strategy [24]. In their short prospective study of 39 patients, a “defensive” strategy had shorter operative times; (184 ± 54 versus 276 ± 110 minutes, P = 0.001) and superior mid-term QOL scores. Only 34% of our patients were fit enough to be discharged home and others were discharged to a convalescence home or another hospital for ongoing recuperation. There was no difference between the surgical strategies.
Iatrogenic dissections from cardiac catherization and intraoperatively are not uncommon in octogenarians. Although no data exist about incidence of these dissections, these are likely to be more common with increased interventions (both cardiological and vascular catherizations and interventions and cardiac surgeries in elderly). These are also likely to carry a worse prognosis as a result of an added life threatening complication of another major procedure in elderly high risk patients. The mortality associated with iatrogenic dissections was higher (4/5, 80%) than for spontaneous dissections (5/45, 11.1%) in our series.
Evidence is growing that QOL after surgery is significantly diminished, particularly in the elderly compared to age-matched general population [25,26,27]. However, equivalent mid-term QOL scores between octogenarian and younger non-octogenarians undergoing ATAAD repair have also been demonstrated. Few studies have precisely addressed QOL following ATAAD repair. Well-designed prospective studies using standardised QOL questionnaires, are needed to make reliable conclusions on the health-related QOL outcomes following ATAAD in octogenarians. This will better guide future appropriate management in this high-risk population.
Limitations
This study has the inherent limitations of a retrospective, single-centre study, and is limited by a relatively small sample size and wide confidence intervals. Because of the limited number of patients and perioperative events, variables for multivariable models were also limited. Results should therefore be cautiously interpreted. Inherent selection bias may confound results as only those who were offered surgery were evaluated. Those who died at transfer or were moribund and not offered surgery were excluded from this analysis. Direct comparison with results of a younger non-octogenarian cohort may have provided better perspective for outcomes. Unfortunately, further comparisons between surgical techniques, extent of surgical repair, cannulation technique and neurocerebral protection strategies were not possible due to small number of patients. Lastly, postoperative QOL and level of physical activity was not evaluated quantitatively and merits further future study since these are critical factors in the ongoing debate surrounding appropriateness of intervention for ATAAD in the elderly.
Conclusions
Despite relatively high-risk of morbidity and mortality, ATAAD repair in selected octogenarians has favourable short and long-term survival and surgical repair may be justified. Age per se, should not be considered an exclusion criterion for surgical repair of ATAAD. There is no significant difference in short and long-term survival of octogenarians between open versus closed distal anastomosis strategies.
Funding
none.
IRB
Safeguard approval number 7373, 15/11/2022.
Consent statement
Consent for individual use of data was waived due to retrospective nature of study and prior approvals at the time of consent for procedures.
Acknowledgments
We thank Mr Bradley Yee, Senior Data Manager for help with the collection of data. We also acknowledge the contributions of other surgeons, anesthetists and the wider team involved in the complex surgeries.
Conflicts of Interest
The authors declare no conflict of interests.
References
- www.mha.org.uk. Accessed 18th May 2023.
- Ohri, S.K.; Benedetto, U.; Luthra, S. , et al. Coronary artery bypass surgery in the UK, trends in activity and outcomes from a 15-year complete national series. Eur J Cardiothorac Surg. 2021, 61, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Biancari, F.; Vasques, F.; Benenati, V.; Juvonen, T. Contemporary results after surgical repair of type A aortic dissection in patients aged 80 years and older: a systematic review and meta-analysis. Eur J Cardiothorac Surg 2011, 40, 1058–1063. [Google Scholar] [CrossRef] [PubMed]
- Hemli, J.M.; Pupovac, S.S.; Gleason, T.G.; Sundt, T.M.; Desai, N.D.; Pacini, D.; Ouzounian, M.; Appoo, J.J.; Montgomery, D.G.; Eagle, K.A.; Ota, T.; et al. Management of acute type A aortic dissection in the elderly: an analysis from IRAD. European Journal of Cardio-Thoracic Surgery 2022, 61, 838–846. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Asai, T.; Kinoshita, T. Emergency surgery for acute type A aortic dissection in octogenarians without patient selection. Ann Thorac Surg 2019, 107, 1146–53. [Google Scholar] [CrossRef]
- Kawahito, K.; Kimura, N.; Yamaguchi, A.; Aizawa, K.; Misawa, Y.; Adachi, H. Early and late surgical outcomes of acute type A aortic dissection in octogenarians. Ann Thorac Surg 2018, 105, 137–43. [Google Scholar] [CrossRef] [PubMed]
- Atsushi Omura, A.; Matsuda, H.; Minami, H.; et al. Early and late outcomes of operation for acute type A aortic dissection in patients aged 80 years and older. Ann Thorac Surg 2017, 103, 131–6. [Google Scholar] [CrossRef] [PubMed]
- Hata, M.; Sezai, A.; Niino, T.; et al. Should emergency surgical intervention be performed for an octogenarian with type A acute aortic dissection? J Thorac Cardiovasc Surg 2008, 135, 1042–6. [Google Scholar] [CrossRef]
- Rampoldi, V.; Trimarchi, S.; Eagle, K.M.; et al. ; Trimarchi, S.; Eagle, K.M.; et al. on behalf of the International Registry of Acute Aortic Dissection (IRAD) Investigators. Simple risk models to predict surgical mortality in acute type A aortic dissection: The international of acute aortic dissection score. Ann Thorac Surg 2007, 83, 55–61. [Google Scholar]
- Piccardo, A.; Regesta, T.; Zannis, K.; et al. Outcomes after surgical treatment for type A acute aortic dissection in octogenarians: a multicenter study. Ann Thorac Surg 2009, 88, 491–7. [Google Scholar] [CrossRef]
- Jonker, F.H.; Schlosser, F.J.; Indes, J.E.; et al. Management of type A aortic dissections: a meta-analysis of the literature. Ann Thorac Surg 2010, 89, 2061–6. [Google Scholar] [CrossRef]
- Ahmad, A.E.S.; Papadopoulos, N.; Detho, F.; et al. Surgical repair for acute type A aortic dissection in octogenarians. Ann Thorac Surg 2015, 99, 547–51. [Google Scholar] [CrossRef]
- Isselbacher, E.M.; Preventza, O.; Hamilton Black, J. , 3rd Augoustides, J.G.; Beck, A.W.; Bolen, M.A.; Braverman, A.C.; Bray, B.E.; Brown-Zimmerman, M.M.; Chen, E.P.; Collins, T.J.; DeAnda AJr Fanola, C.L.; Girardi, L.N.; Hicks, C.W.; Hui, D.S.; Schuyler Jones, W.; Kalahasti, V.; Kim, K.M.; Milewicz, D.M.; Oderich, G.S.; Ogbechie, L.; Promes, S.B.; Gyang Ross, E.; Schermerhorn, M.L.; Singleton Times, S.; Tseng, E.E.; Wang, G.J., Woo. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. YJ. Circulation. 2022, 146, e334–e482. [Google Scholar]
- Malvindi, P.G.; Modi, A.; Miskolczi, S.; Kaarne, M.; Velissaris, T.; Barlow, C.; Ohri, S.K.; Tsang, G.; Livesey, S. Open and closed distal anastomosis for acute type A aortic dissection repair. Interact Cardiovasc Thorac Surg. 2016, 22, 776–83. [Google Scholar] [CrossRef] [PubMed]
- Kawahito, K.; Kimura, N.; Yamaguchi, A.; Aizawa, K.; Misawa, Y.; Adachi, H. Early and late surgical outcomes of acute type A aortic dissection in octogenarians. Ann Thorac Surg 2018, 105, 137–43. [Google Scholar] [CrossRef] [PubMed]
- Omura, A.; Matsuda, H.; Minami, H.; Nakai, H.; Henmi, S.; Murakami, H.; et al. Early and late outcomes of operation for acute type A aortic dissection in patients aged 80 years and older. Ann Thorac Surg 2017, 103, 131–8. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, A.; Tabata, M.; Fukui, T.; Sato, Y.; Matsuyama, S.; Shimokawa, T.; et al. Outcomes of contemporary emergency open surgery for type A acute aortic dissection in elderly patients. J Thorac Cardiovasc Surg 2014, 147, 290–4. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Yamamoto, H.; Miyata, H.; Motomura, N.; Tokuda, Y.; Tanemoto, K.; Usui, A.; Takamoto, S. Patient trends and outcomes of surgery for type A acute aortic dissection in Japan: an analysis of more than 10 000 patients from the Japan Cardiovascular Surgery Database. Eur J Cardiothorac Surg. 2020, 57, 660–667. [Google Scholar] [CrossRef]
- Inoue, Y.; Matsuda, H.; Uchida, K.; Komiya, T.; Koyama, T.; Yoshino, H.; Ito, T.; Shiiya, N.; Saiki, Y.; Kawaharada, N.; Nakai, M.; Iba, Y.; Minatoya, K.; Ogino, H. Analysis of Acute Type A Aortic Dissection in Japan Registry of Aortic Dissection (JRAD). Ann Thorac Surg. 2020, 110, 790–798. [Google Scholar] [CrossRef] [PubMed]
- Bojko, M.M.; Suhail, M.; Bavaria, J.E.; Bueker, A.; Hu, R.W.; Harmon, J.; Habertheuer, A.; Milewski, R.K.; Szeto, W.Y.; Vallabhajosyula, P. Midterm outcomes of emergency surgery for acute type A aortic dissection in octogenarians. J Thorac Cardiovasc Surg. 2022, 163, 2–12. [Google Scholar] [CrossRef]
- Dumfarth, J.; Peterss, S.; Luehr, M.; Etz, C.D.; Schachner, T.; Kofler, M.; Ziganshin, B.A.; Ulmer, H.; Grimm, M.; Elefteriades, J.A.; Mohr, F.W. Acute type A dissection in octogenarians: does emergency surgery impact in-hospital outcome or long-term survival? Eur J Cardiothorac Surg. 2017, 51, 472–477. [Google Scholar] [CrossRef]
- Eranki, A.; Merakis, M.; Williams, M.L.; Flynn, C.D.; Villanueva, C.; Wilson-Smith, A.; Lee, Y.; Mejia, R. Outcomes of surgery for acute type A dissection in octogenarians versus non-octogenarians: a systematic review and meta analysis. J Cardiothorac Surg 2022, 17, 222. [Google Scholar] [CrossRef] [PubMed]
- Aoyama, T.; Kunisawa, S.; Fushimi, K.; Sawa, T.; Imanaka, Y. Comparison of surgical and conservative treatment outcomes for type a aortic dissection in elderly patients. J Cardiothorac Surg. 2018, 13, 129. [Google Scholar] [CrossRef] [PubMed]
- Ghazy, T.; Eraqi, M.; Mahlmann, A.; Hegelmann, H.; Matschke, K.; Kappert, U.; Weiss, N. Quality of Life after Surgery for Stanford Type A Aortic Dissection: Influences of Different Operative Strategies. Heart Surg Forum. 2017, 20, E102–E106. [Google Scholar] [CrossRef]
- Jussli-Melchers, J.; Panholzer, B.; Friedrich, C.; et al. Long-term outcome and quality of life following emergency surgery for acute aortic dissection type A: a comparison between young and elderly adults. Eur J Cardiothorac Surg. 2017, 51, P465–P471. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.H.; Malekan, R.; Yu, C.J.; et al. Surgery for acute type A aortic dissection in octogenarians is justifed. J Thorac Cardiovasc Surg. 2013, 145(3 Suppl), P186–90. 21. [Google Scholar] [CrossRef]
- Tashima, Y.; Toyoshima, Y.; Chiba, K.; et al. Physical activities and surgical out-comes in elderly patients with acute type A aortic dissection. J Card Surgery. 2021, 36, 2754–64. [Google Scholar] [CrossRef]
Figure 1.
Kaplan Meier survival curves comparing open vs closed distal anastomosis technique.
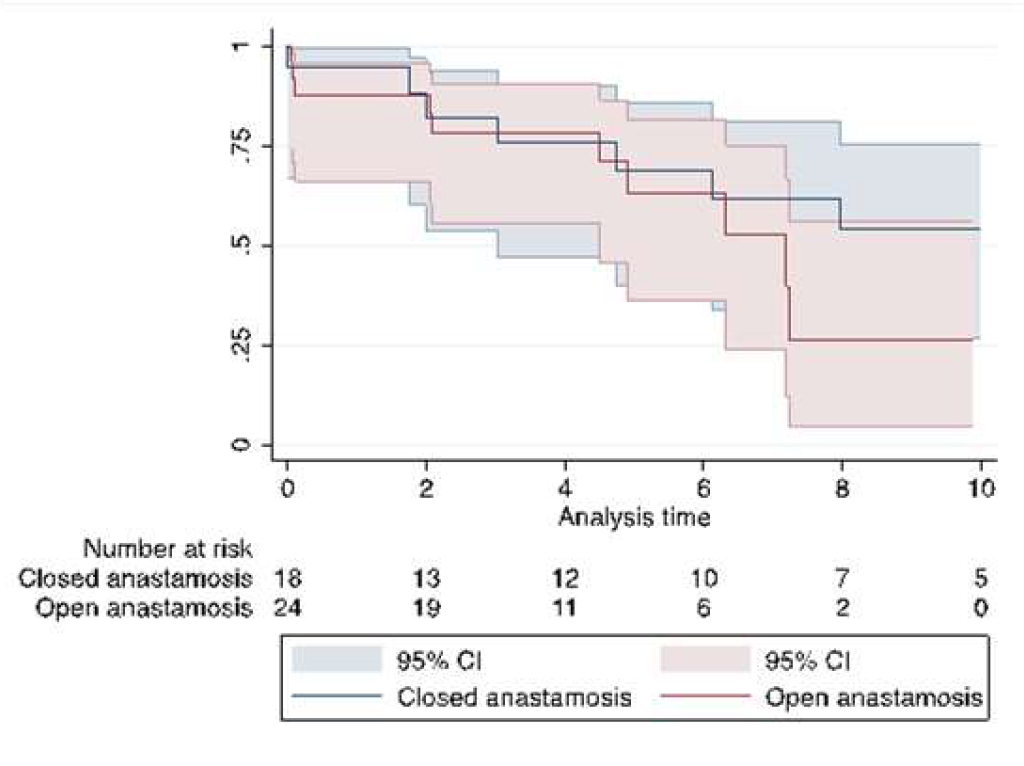

Table 1.
Preoperative demographic and clinical characteristics.
| Variable | Total | Closed (n=22) | Open (n=28) | P value |
|---|---|---|---|---|
| Age, years (IQR) | 82 (80.3-83.4) | 82.8 (80.3-85) | 81.9(80.4-82.9) | 0.23 |
| Male gender | 21 (42%) | 9 (40.9%) | 12 (42.9%) | 0.89 |
| Log EuroSCORE, % (IQR) | 40.6 (35.6- 59.2) | 40.6 (35.9-57.3) | 39.8 (34.3-59.8%) | 0.95 |
| Angina class 3-4 | 11 (22%) | 4 (18.2%) | 7 (25%) | 0.56 |
| NYHA class 3-4 | 3 (6%) | 0 (0%) | 3 (10.7%) | 0.11 |
| Previous cardiac surgery | 4 (8%) | 3 (13.6%) | 1 (3.6%) | 0.19 |
| Previous MI | 2 (4%) | 1 (4.5%) | 1 (3.6%) | 0.86 |
| Diabetes mellitus | 2 (4%) | 1 (4.5%) | 1 (3.6%) | 0.86 |
| Hypertension | 36 (72%) | 16 (72.7%) | 20 (71.4%) | 0.92 |
| Smoking history | 15 (30%) | 7 (31.8%) | 8 (28.6%) | 0.80 |
| Preop renal failure | 3 (6%) | 1 (4.5%) | 2 (7.1%) | 0.70 |
| Preop Hb, g/L (IQR) | 120 (110-133) | 127 (113-137) | 120 (110-124) | 0.05 |
| Preop COPD | 5 (10%) | 2 (9.1%) | 3 (10.7%) | 0.85 |
| Preop neurogical deficit | 2 (4%) | 2 (9.1%) | 0 (0%) | 0.10 |
| Extracardiac arterioathy | 5 (10%) | 1 (4.5%) | 4 (14.3%) | 0.25 |
| LVEF ≤30 | 2 (4%) | 1 (4.5%) | 1 (3.6%) | 0.86 |
| Cardiogenic shock | 12 (24%) | 3 (13.6%) | 9 (32.1%) | 0.13 |
| Preop inotropes | 3 (6%) | 1 (4.5%) | 2 (7.1%) | 0.70 |
| Cause of dissection | ||||
| Hypertension | 44 (88%) | 19 (86.4%) | 25 (89.3%) | |
| Aneurysm | 1 (0.2%) | 1 (0.5%) | 0 | |
| Iatrogenic | 5 (10%) | 2 (0.9%) | 3 (10.7%) | |
|
Data are presented as median (quartiles; minimum–maximum) or count (percent). Abbreviations: NYHA – New York Heart Association, MI – myocardial infarction, COPD – chronic obstryctive pulmonary disease, Hb – haemoglobin, LVEF – left ventricular ejection fraction, LOS – length of stay | ||||
Table 2.
Operative and postoperative characteristics.
| Variable | Total (50) | Closed (n=22) | Open (n=28) | P value |
|---|---|---|---|---|
| OPERATIVE CHARACTERISTICS | ||||
| Cannulation technique | ||||
| Femoral | 31 (62.0%) | 14 (63.6%) | 17 (60.7%) | |
| Subclavian | 10 (20..0%) | 3 (13.6%) | 7 (25.0%) | |
| Central | 7 (14.0%) | 3 13.6%) | 4 (14.3%) | |
| Unknown | 2 (4.0%) | 2 (9.1%) | 0 | |
| XCT, mins (IQR) | 93 (76-130) | 81 (69-112) | 101 (79-146) | 0.31 |
| CPB, mins (IQR) | 187 (121-245) | 115.5 (102-205) | 219 (184-282) | <0.01 |
| TCA, mins (IQR) | n/a | n/a | 26 (20-39) | |
| Neuroprotection | ||||
| Antegrade | 11 (22%) | 1 (4.6%) | 10 (35.7%) | |
| Retrograde | 3 (6.0%) | 0 | 3 (10.7%) | |
| None | 36 (72%) | 21 (95.4%) | 15 (53.6%) | |
| Aortic procedures | ||||
| 1. Interposition tube graft without extension into the arch | 31 (62%) | 19 (86.4%) | 12 (42.9%) | |
| 2. Interposition tube graft with extension into the arch | 13 (26%) | 1 (0.45%) | 12 (42.9%) | |
| 3. Interpositional graft + separate valve | 6 (12%) | 2 (0.9%) | 4 (14.3%) | |
| Other concomitant procedures 1. Aortic valve/root repair/replacement 2. Coronary artery bypass |
10 (20%) 4 (8%) |
5 (22.7 %) 2 (9.1%) |
5 (17.9%) 2 (7.1%) |
0.28 |
| POSTOPERATIVE CHARACTERISTICS | ||||
| Return to theatre | 3 (6%) | 1 (4.5%) | 2 (7.1%) | 0.70 |
| New TIA | 3 (6%) | 0 (0%) | 3 (10.7%) | 0.11 |
| New Stroke | 13 (26%) | 5 (22.7%) | 8 (28.6%) | 0.64 |
| New CVA | 16 (32%) | 5 (22.7%) | 11 (39.3%) | 0.21 |
| RRT | 4 (8%) | 2 (9.1%) | 2 (7.1%) | 0.80 |
| LOS, days (IQR) | 14.6 (8.0-20.7) | 13.8 (3.3-19.4) | 14.6 (8.8-20.9) | 1.00 |
| LOS ≥ 30 days | 5 (10%) | 1 (4.5%) | 4 (14.3%) | 0.25 |
| In-hospital mortality | 9 (18%) | 5 (22.7%) | 4 (14.3%) | 0.44 |
| Composite endpoint* | 26 (52%) | 10 (45.5%) | 16 (57.1%) | 0.41 |
| Discharge destination | ||||
| Home | 17 (34%) | 7 (31.8%) | 10 (35.7%) | |
| Convalescence | 16 (32%) | 7 (31.8%) | 9 (32.1%) | |
| Other hospital | 8 (16%) | 3(13.6%) | 5 (17.9%) | |
| Median survival, years (IQR) | 7.2 (4.5-11.6) | 10.6 (4.7-11.6) | 7.2 (4.5-8.1) | 0.35 |
| Survival | ||||
| 6 months | 76 ± 6.0% | 77.3 ± 8.9% | 85.7 ± 6.6% | 0.08 |
| 1 year | 75.8 ± 6.1% | 76.7 ± 9.1% | 75.0 ± 8.2% | 0.61 |
| 5 years | 55.1 ± 7.7% | 56.3 ± 11.0% | 52.9 ± 11.2% | 0.18 |
|
Data are presented as median (IQR – Inter quartile Range) or count (percent). Abbreviations: CBP – cardiopulmonary bypass time, CVA – cerebrovascular accident,TCA – total circulatory arrest time, LOS – length of stay, RRT – renal replacement therapy, TIA – transient ischemic attack, XCT - cross clamp time. *Composite endpoint of:RRT, new CVA, LOS≥30 days, return to theatre, in-hospital mortality | ||||
Table 3.
Logistic regression model for predictors of in-hospital mortality (<0.05 entered into the multivariable model).
Table 3.
Logistic regression model for predictors of in-hospital mortality (<0.05 entered into the multivariable model).
| Univariable | Multivariable | ||||||
|---|---|---|---|---|---|---|---|
| Variable | Odds Ratio (95% CI) | 95% Confidence interval | P value | Included in multivariable model? | Odds Ratio (95% CI) | 95% Confidence interval | P value |
| Preoperative | |||||||
| Age | 1.03 | 0.75, 1.40 | 0.87 | N | |||
| Female gender | 0.18 | 0.035, 0.84 | 0.03 | Y | 0.35 | 0.03 – 3.5 | 0.37 |
| Log EuroSCORE | 9.69 | 0.20, 458.1 | 0.25 | N | |||
| Angina class 3-4 | 1.14 | 0.23, 5.67 | 0.87 | N | |||
| NHYA class ≥3 | 9.0 | 1.03, 78.7 | 0.047 | Y | 0.24 | 0.004, 14.8 | 0.50 |
| Previous cardiac surgery | 3.24 | 1.11, 9.49 | 0.03 | Y | 1.4 | 0.35, 5.8 | 0.62 |
| Diabetes mellitus | 4.76 | 0.44, 51.52 | 0.20 | N | |||
| Hypertension | 2.68 | 0.42, 17.12 | 0.30 | N | |||
| Smoking history | 0.81 | 0.25, 2.70 | 0.74 | N | |||
| Preop creatinine | 1.02 | 1.00, 1.03 | 0.05 | Y | 1.03 | 0.99, 1.1 | 0.17 |
| Preop Hemoglobin | 1.01 | 0.97, 1.06 | 0.62 | N | |||
| Preop COPD | 3.67 | 0.61, 22.22 | 0.16 | N | |||
| Preop neurology Hx | 0.83 | 0.04, 18.8 | 0.91 | N | |||
| Extracardiac arteriopathy | 1.47 | 0.20, 10.78 | 0.70 | N | |||
| LVEF <30 | 27.67 | 1.20, 635.62 | 0.038 | Y | 1.39 | 0.03, 81.2 | 0.87 |
| Critical preop state* | 1.27 | 0.30, 5.46 | 0.75 | N | |||
| Operative | |||||||
| Additional procedures | 6.68 | 1.49, 29.93 | 0.01 | Y | 1.41 | 0.12, 15.8 | 0.78 |
| Open distal anastomosis | 0.58 | 0.15, 2.34 | 0.45 | N | |||
| CPB time (mina) | 1.01 | 1.00, 1.03 | 0.008 | Y | 1.01 | 0.99, 1.03 | 0.44 |
| Postoperative | |||||||
| Re-exploration for bleeding | 0.58 | 0.03, 13.19 | 0.725 | N | |||
| RRT | 5.27 | 0.77, 35.89 | 0.09 | N | |||
| New CVA | 0.63 | 0.13, 3.03 | 0.57 | N | |||
| Composite endpoint | 0.75 | 0.18, 3.17 | 0.70 | N | |||
| LOS | 0.85 | 0.76, 0.96 | 0.01 | Y | 0.88 | 0.75, 1.03 | 0.12 |
|
Abbreviations: COPD – chronic obstructive pulmonary disease, LVEF – left ventricular ejection fraction, CPB – cardiopulmonary bypass time, CVA – cerebrovascular accident, LOS – length of stay, NYHA - New York Heart Association, RRT – renal replacement therapy *Critical pre-op: pre-op neuro deficit, pre-op renal failure, inotropes, shock or mechanical ventilation | |||||||
Table 4.
Cox regression model for predictors of long-term survival.
| Variable | Hazard ratio | 95% CI | P-value |
|---|---|---|---|
| Critical Pre-opa | 3.17 | 1.1, 8.9 | 0.03 |
| Open distal anastomosis | 1.00 | 0.3, 3.1 | 1.00 |
| Concomitant procedure | 1.30 | 0.4, 4.3 | 0.67 |
| Composite endpointb | 4.06 | 1.3, 12.7 | 0.02 |
| Hypertension | 0.40 | 0.1, 1.1 | 0.08 |
|
aCritical pre-op: pre-op neuro deficit, pre-op renal failure, inotropes, shock or mechanical ventilation bComposite endpoint of RRT, new CVA, LOS>=30 days, return to theatre | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



