
Submitted:
04 August 2024
Posted:
06 August 2024
You are already at the latest version
Abstract
Asthma is a chronic inflammatory disease for which the main anti-inflammatory drugs for better disease control are steroids or corticosteroids. The use of steroids in asthma patients, in particular in uncontrolled asthma patients, is associated with an increased risk of osteoporosis and fragility fractures. A single oral corticosteroids course increases the risk of osteoporosis and continual use of inhaled corticosteroids is correlated over time to an increased risk for both bone conditions. With the use of new, available biologic therapies for asthma, perhaps even anticipating the times of their use in what are the steps of therapeutic management, in the current guidelines and with targeted strategies of prevention it may be possible to improve asthma management, preventing some comorbidities, such as osteoporosis.
Keywords:
severe asthma
; biologics
; corticosteroids
; inflammation
; interleukins
; osteoporosis
Introduction
Asthma and osteoporosis are two medical conditions that might appear distinct, but which are interconnected through a series of pathophysiological mechanisms and shared risk factors. This article explores the links between asthma and osteoporosis, focusing on how chronic inflammation, glucocorticoid use, and other common risk factors contribute to the development of both diseases. Additionally, therapeutic implications and management strategies for patients suffering from both conditions are discussed. Asthma is a chronic inflammatory disease of the airways characterized by reversible bronchial obstruction, bronchial hyperreactivity, and recurring symptoms of wheezing, dyspnoea, chest tightness, and cough. Asthma management is based on international guidelines that include the use of bronchodilators and inhaled corticosteroids to control inflammation and prevent exacerbations [1]. Osteoporosis is a systemic skeletal disease characterized by reduced bone mass and deterioration of bone microarchitecture, leading to increased bone fragility and fracture risk. Risk factors for osteoporosis include advanced age, menopause, calcium and vitamin D deficiency, and prolonged use of glucocorticoids [2]. Chronic inflammation present in asthma can negatively impact bone health. Pro-inflammatory cytokines such as IL-6 and TNF-α, elevated in asthma, can stimulate bone resorption, reducing bone mineral density (BMD) [3]. Glucocorticoids, frequently used in asthma treatment, are well-known for their adverse effects on bone mass. Chronic use of glucocorticoids can decrease intestinal calcium absorption and inhibit bone formation, significantly increasing the risk of osteoporosis and fractures [4]. Studies have shown that both oral (OCS) and inhaled (ICS) corticosteroids can contribute to bone loss, although the effects are more pronounced with oral corticosteroids [5,6]. A sedentary lifestyle is a risk factor for both conditions. Regular physical activity, particularly weight-bearing and resistance exercises, can improve both pulmonary function and bone health [7]. A diet poor in calcium and vitamin D can contribute to osteoporosis and worsen general health, negatively affecting asthma management. Proper nutrition is essential for maintaining good bone health and preventing chronic inflammation [8]. Some genetic factors may predispose individuals to both conditions. Ongoing research continues to explore the genetic links between asthma and osteoporosis, aiming to identify common genes that may influence the development of these diseases [9]. Asthma management should include the prudent use of glucocorticoids, balancing respiratory benefits with the risk of osteoporosis. Using inhalers at the minimal effective dose and introducing alternative medications where possible can help mitigate this risk. Additionally, the use of drugs such as bisphosphonates may be indicated to prevent bone loss in patients requiring long-term glucocorticoids [10]. For asthma patients using glucocorticoids, supplementation with calcium and vitamin D may be indicated. This approach can help maintain bone mineral density and reduce the risk of osteoporosis. Tailored exercise programs will help. Exercise not only helps maintain good bone health but can also improve asthma control, reducing the frequency and severity of exacerbations. The use of biological therapies has revolutionized the treatment of severe asthma. These therapies target specific pathways involved in the inflammatory process, offering a more personalized approach to asthma management. Biologics such as monoclonal antibodies against IgE (omalizumab), IL-5 (mepolizumab, reslizumab, benralizumab) and IL-4/IL-13 (dupilumab) have shown significant efficacy in reducing asthma exacerbations, improving lung function, and enhancing the quality of life for patients with severe asthma. The introduction of these biologics also has implications for bone health. By potentially reducing the need for systemic glucocorticoids, biologics may help mitigate the associated risk of osteoporosis [11] (Table 1). The pharmacoeconomic impact of biological therapies in asthma management is substantial. While these treatments are often more expensive upfront compared to traditional therapies, they can reduce healthcare costs in the long term by decreasing the frequency of severe asthma exacerbations, hospitalizations, and the overall burden of the disease. Furthermore, by potentially reducing the need for systemic glucocorticoids, biologics may lower the incidence of glucocorticoid-induced osteoporosis, thereby reducing costs related to osteoporosis management and fracture treatment [12]. It is crucial to regularly monitor bone mineral density in asthmatic patients undergoing long-term glucocorticoid therapy. This can be done through exams such as dual-energy X-ray absorptiometry (DEXA), which allows early identification of bone loss and intervention with preventive measures. Integrated management of asthma and osteoporosis requires a multidisciplinary approach that considers the interconnection between the two conditions. A thorough understanding of the common mechanisms and preventive strategies can improve the quality of life for patients affected by both diseases. Collaboration between pulmonologists, endocrinologists, and other specialists is essential to develop personalized treatment plans that address the specific needs of patients. Ultimately, the management of asthma and osteoporosis must consider the interplay between these conditions. Ensuring optimal asthma control while minimizing the adverse effects of treatment on bone health requires careful consideration of medication choices, lifestyle modifications, and regular monitoring. The advent of biological therapies provides new opportunities for managing severe asthma more effectively and with potentially fewer side effects, highlighting the importance of ongoing research and innovation in the treatment of these chronic conditions.

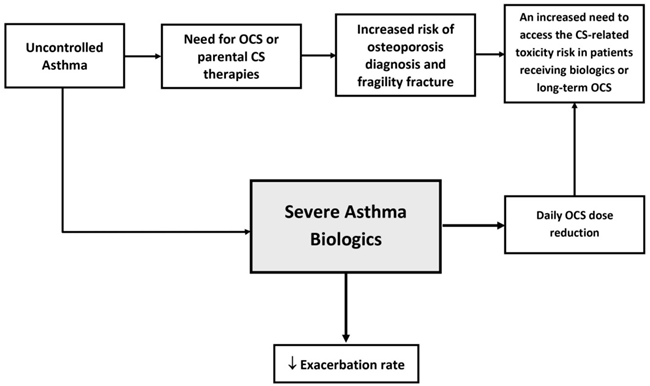
Table 1.
Flow chart for severe asthma management.
Osteoporosis and the IL-31/33 Axis
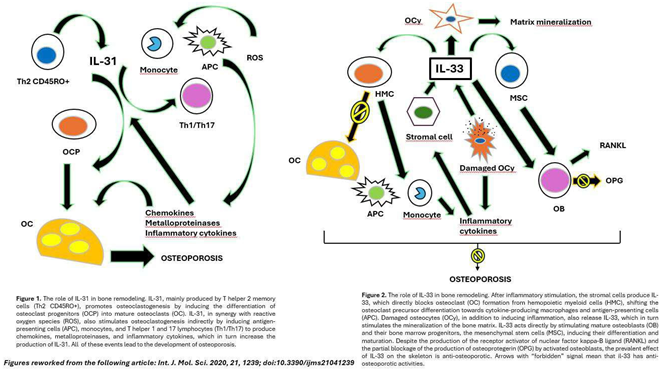
Bronchial asthma is a chronic respiratory disease characterized by inflammation and hyperreactivity of the airways. The interleukins IL-31 and IL-33 play a crucial role in the pathological mechanisms that govern this condition [13]. IL-31, produced mainly by T helper 2 (Th2) cells, is involved in modulating the inflammatory response. This cytokine is known to promote the activation of mast cell and basophil cells, facilitating allergic inflammation and contributing to the production of other pro-inflammatory cytokines and chemokines, which in turn amplify asthma symptoms [14]. Its secretion is increased in conditions of severe asthma, suggesting a direct link between elevated IL-31 levels and disease severity [15]. On the other hand, IL-33, a high alarmin released by damaged epithelial cells, plays a critical role in the activation of immune system cells, including T cells and mast cells [16]. Activation occurs in situations of environmental stress or tissue injury, stimulating a robust inflammatory response. IL-33 induces the production of other Th2 cytokines, such as IL-4 and IL-13, which are important for the allergic response and chronic inflammation in the airways. Interactions between IL-31 and IL-33 lead to further amplification of inflammation, contributing to the pathogenesis of asthma [17]. This chronic inflammation is not limited to the airways, but also causes systemic effects that can affect bone metabolism. Pro-inflammatory cytokines, activated by mediators of the IL-31/IL-33 axis, can stimulate osteoclastogenesis, i.e., the formation of osteoclasts, cells responsible for bone resorption. As a result, asthma patients with sustained inflammation may be at increased risk of developing osteoporosis [18]. Furthermore, prolonged use of corticosteroids for asthma control further compromises bone mineral density, making patients vulnerable to bone fractures [19]. Therefore, it is critical for pulmonary physicians to integrate an osteoporosis risk assessment into the management of asthma patients, as chronic inflammation and corticosteroid treatment may interact negatively to impact bone health. Identification of the IL-31/IL-33 axis as a risk factor for osteoporosis not only improves understanding of the pathophysiology of asthma, but also highlights the importance of therapeutic strategies that consider both respiratory and systemic symptoms. Preventive strategies such as the adoption of a healthy lifestyle, combined with scrupulous pharmacological management, can have their say in mitigating the side effects linked to osteoporosis in these patients [20,21]. Continued research on the effects of IL-31 and IL-33 in asthma may lead to new therapeutic innovations, thus improving the quality of life of asthma patients and reducing the risk of associated complications (Figure 1 and Figure 2) [22].
Overview of OCS Available and Conversion of Doses of OCS
The main treatment in asthma is the use of corticosteroids given their capacity to act on inflammation which is typical of asthma. It is important to understand the correct use of corticosteroids available and their pharmacokinetics. An OCS conversion table can be found at the end of the paragraph (Table 2) [23].
Cortisone: This hormone acts on the intermediate metabolism, increasing the availability of glucose, inducing proteolysis and lipolysis, thus placing the organism in an energetically active state, useful for overcoming any stressful conditions; it alters the normal fluid and electrolyte balance, increasing the reabsorption of sodium and the excretion of potassium and calcium. Finally, it induces vasoconstriction at the microcirculation level. Indicated in the treatment of acute and chronic inflammatory pathologies that require systemic therapies with OCS, it can also be useful in the management of symptoms in allergic and neoplastic conditions [24].
Table 2.
Corticosteroids conversion table drawn up from the available literature with clinical studies of sufficiently homogeneous enrolled populations.
Table 2.
Corticosteroids conversion table drawn up from the available literature with clinical studies of sufficiently homogeneous enrolled populations.
| CORTICOSTEROIDS (OCS) |
APPROXIMATE EQUIVALENT DOSE (MILLIGRAMS) |
|---|---|
| Cortisone | 25 mg |
| Hydrocortisone | 20mg |
| Deflazacort | 7,5mg |
| Prednisolone | 5mg |
| Prednisone | 5mg |
| Methylprednisolone | 4mg |
| Triamcinolone | 4mg |
| Betamethasone | 0,75mg |
| Dexamethasone | 0,75mg |
Hydrocortisone: Hydrocortisone is the main glucocorticoid produced by the adrenal cortex. It works by binding to its receptors present inside the cells, promoting the expression of some specific genes with consequent activation of molecules with anti-inflammatory action and the simultaneous inhibition of molecules with pro-inflammatory activity. It is used against inflammation, allergic reactions, diseases involving collagen, asthma, adrenal insufficiency, some forms of cancer and Addison’s disease and autoimmune diseases such as arthritis, lupus, psoriasis, ulcerative colitis and Crohn’s disease [25].
Deflazacort: This is a corticosteroid which, after oral intake, is absorbed rapidly and completely in the intestine with peak plasma levels reached in 1-2 hours. Subsequently, the original compound is deacetylated at position 21 to be transformed into an active metabolite characterized by high binding affinity for tissue glucocorticoid receptors. The absolute oral bioavailability is 68%, the binding to plasma proteins is 39.8%, while the almost complete elimination of the active metabolite occurs within 24 hours mainly through urine. It is a drug that has indications in the treatment of various pathologies including sarcoidosis, juvenile chronic arthritis, polymyalgia rheumatica, rheumatoid arthritis [26].
Prednisolone: This works by preventing the release of molecules that trigger inflammation. It is used in the treatment of many different disorders associated with inflammation, for example, allergies, ulcerative colitis, arthritis, lupus, psoriasis or respiratory problems [27].
Prednisone: This is a synthetic hormone that belongs to the corticosteroid group, and has properties to reduce pain, swelling, stiffness, redness and heat in affected tissues. It is used in some rheumatological conditions such as rheumatoid arthritis, acute gouty arthritis, Still’s disease, ankylosing spondylitis, systemic lupus erythematosus, dermatomyositis, bronchial asthma, atopic and contact dermatitis, in sarcoidosis, to treat some diseases of the blood, as palliative therapy for some tumours, in addition to therapies for gastrointestinal pathologies [28].
Methylprednisolone: Methylprednisolone is a powerful anti-inflammatory which, similarly to other corticosteroid drugs, appears to inhibit the release of arachidonic acid, the precursor of important inflammatory mediators. Oral methylprednisolone is used in the treatment of adrenal insufficiency, joint pathologies, such as psoriatic arthritis, rheumatoid arthritis, skin conditions such as severe psoriasis, pemphigus, allergic diseases, eye disorders such as diffuse posterior uveitis, optic neuritis, iritis and iridocyclitis, lung diseases such as sarcoidosis and emphysema, blood pathologies and tumours such as leukaemia, intestinal diseases such as ulcerative colitis and regional enteritis, brain disorders (e.g., tuberculous meningitis) and other pathologies [29].
Triamcinolone: This acts from a molecular point of view, determining expression of the lipocortin enzyme, capable of inhibiting phospholipase A2 and consequently reducing the availability of arachidonic acid. The reduced concentration of the starting substrate translates into a modest synthesis of inflammatory mediators such as leukotrienes, prostaglandins and prostacyclins with consequent control of the entire inflammatory process and related tissue damage. Once its activity is complete, the active ingredient is metabolised in the liver, mainly through hydroxylation processes and subsequently excreted via the kidneys. It can be used to treat many different conditions: allergies, disorders of the skin and related tissues (hair, nails) such as psoriasis, rheumatic diseases, ulcerative colitis (chronic inflammatory bowel disease) and some respiratory diseases [30].
Betamethasone: This belongs to the class of long-acting glucocorticoids. The main indications are for the treatment of bronchial asthma, severe allergic diseases, rheumatoid arthritis, collagenopathies, inflammatory skin diseases, tumours of the lymphatic system such as acute and chronic malignant hemolymphopathies, Hodgkin’s disease, nephrotic syndrome, ulcerative colitis and Crohn’s disease, pemphigus, sarcoidosis, rheumatic carditis, ankylosing spondylitis, haemolytic anaemia, agranulocytosis, thrombocytopenic purpura [31].
Dexamethasone: This is a synthetic hormone with an anti-inflammatory activity approximately 7 times more powerful than prednisolone and 30 times more powerful than hydrocortisone. The molecule exerts its action on the hypothalamic-pituitary-adrenal (HPA) axis by binding to specific receptors on the cellular plasma membrane. In other tissues, the molecule passes cell membranes and diffuses into the cytosol, combining with specific cytoplasmic receptors, the glucocorticoid receptor (GR). The complex that is formed enters the cell nucleus and stimulates protein synthesis. Like other adrenocortical steroids, dexamethasone has anti-allergic, anti-shock, antitoxic, antifebrile and immunosuppressive properties. Characteristically this molecule predominantly presents a glucocorticoid activity; its ability to determine renal retention of sodium and water (i.e., mineralocorticoid activity) is vastly lower than that of other molecules of the same class. After oral administration, dexamethasone is rapidly absorbed from the gastrointestinal tract. Following intravenous injection, peak plasma levels are reached in 5 minutes. Its half-life in plasma is approximately 190 minutes. It may be more interesting to consider the biological half-life of the molecule, which is equal to 36-54 hours, which makes dexamethasone a substance that is indicated for the treatment of those pathologies that require prolonged glucocorticoid action such as patients suffering from rheumatoid arthritis, bronchial asthma, purpura, undergoing chemotherapy, etc. [32].
The Impact of Severe Asthma Biologics in Sparing Steroid Therapy
Severe asthma biologics that act on the different steps of Type 2 inflammation are a revolutionary strategy to treat the disease. When the diagnosis of asthma is confirmed and comorbidities have been addressed, such as rhinitis, rhinosinusitis, nasal polyps, and gastroesophageal reflux, severe asthma is classified as “asthma which requires treatment with high dose ICSs plus a second controller (and/or systemic corticosteroids) to prevent it from becoming ‘uncontrolled’ or which remains ‘uncontrolled’ despite this therapy.” Patients affected by uncontrolled asthma present high rates of exacerbations with the need for glucocorticoid therapy [33].
There are now several monoclonal antibody (mAb) therapies (“biologics”) available to treat severe asthma. These drugs all reduce the exacerbation rate.“Severe asthma” describes asthma that is dependent upon high-dose ICS plus a second controller (and/or systemic corticosteroids) to maintain symptom control, or which remains “uncontrolled” despite these therapies [34]. Once comorbidities have been addressed, and excluding those patients who are poorly adherent to inhaled therapy, the prevalence of severe asthma affects approximately 3.7% of the asthma population [35], resulting in significant asthma-related healthcare costs, frequent exacerbations, impairment of quality of life, missed work/school days, and frequent healthcare utilization. Severe asthma exacerbations need OCS or may need maintenance oral corticosteroids (mOCS) to control the disease. Long term use of OCS is associated with relevant long-term morbidity, such as adrenal suppression, osteopenia and osteoporosis, increased risk of type II diabetes, cataracts, and obesity [36]. Asthma can be considered the result of the combination of genetic susceptibility with external factors such as allergens, microbes, pollutants and other triggers that, acting on the airway epithelium, induce the release of “alarmins”, including interleukin (IL)-25, IL-33 and thymic stromal lymphopoietin (TSLP), which result in the production of T2 cytokines from cells including Th2 cells and type 2 innate lymphoid cells (ILC2) [37]. Severe asthma biologics that are essential in the exacerbation pathogenesis in asthma act on one or more mediators or cells within this pathway. Type 2 cytokines that play a key role in asthma disease include IL-4, related to IgE production from B-cells, IL-5, related to eosinophil cycle, and IL-13, related to mucus hypersecretion and airway hyperresponsiveness [38].
Omalizumab (“Xolair”), the first monoclonal antibody (mAb) approved to treat severe asthma, with an antiviral response and a reduction of virus-induced exacerbations, binds to free circulating IgE, inducing an inhibition of attachment to its receptor (FCεRI) and a reduction of downstream effects, including mast cell degranulation and the expression of inflammatory cytokines such as IL-3, IL-4, IL-5, IL-6 and IL-13. [39]. Various real-world, observational trials reported mOCS dose reduction in patients treated with omalizumab [40,41,42,43,44]. In a systematic review of 42 observational or registry trials, the authors highlighted a mean OCS dose reduction of 68% at 12 months, with a broad range from −78% to −12% [45]. The large “eXpeRience” registry reported on over 260 patients on baseline OCS and reported that 57% either reduced or stopped mOCS by 1 year of omalizumab treatment. Moreover, it was reported that the mean prednisolone dose at the end of 1 year was 7.7 mg compared to 15.5 mg at baseline [46]. In a randomized trial a major reduction or interruption of mOCS in patients treated with omalizumab rather than with optimal standard care was described [47].
Mepolizumab (“Nucala”), the first mAb introduced for severe eosinophilic asthma, acts on the IL-5 cytokine involved in the development, migration and survival of eosinophils [43,45]. The phase 3 MENSA trial reported a reduction of exacerbations (52%) in patients treated with mepolizumab compared to patients treated with placebo [46] and, moreover, a significant reduction of OCS dose in patient’s dependent on daily OCS to maintain asthma control. The SIRIUS trial reported that at 24 weeks, 14% of asthma patients in mepolizumab treatment were able to stop prednisolone with a general median reduction of 50% OCS use [47].
A retrospective analysis of 99 patients in mepolizumab treatment reported a 50% reduction of exacerbation rate, with a reduction in prednisolone dose of at least 50% [48]. Regarding Reslizumab (“Cinqaero”), a recombinant humanized IgG4 mAb that acts on IL-5, the efficacy in terms of reduction of mOCS use has not been formally reported. Indeed, mepolizumab, benralizumab and dupilumab are the only severe asthma biologics for which a significant reduction in daily OCS use has been reported.
Benralizumab (“Fasenra”) that acts on the IL-5 pathway through ligation to the α subunit of the IL-5 receptor (IL-5R-α), induces a cell mediated cytotoxicity, and consequent cell apoptosis (eosinophils and basophils) on which IL-5R-α is expressed [49,50]. In the ZONDA study, which enrolled OCS-dependent asthma patients, a 50% reduction in OCS dose in benralizumab treated patients was reported compared with placebo. Moreover, a reduction of 70% in exacerbations was described [51]. In the open-label PONENTE study, it was reported that in 598 OCS-dependent patients treated with benralizumab over 80% were able to stop the use, or achieved a dosage, of 5 mg or less if the reason for stopping the reduction was adrenal insufficiency rather than asthma [52].
Dupilumab (“Dupixent”), an mAb targeted against the α subunit of the IL-4 receptor, has also reported a significant reduction of mOCS use in asthma. The LIBERTY ASTHMA VENTURE trial [53] reported an overall median prednisolone dose reduction of 50% compared to placebo and 69% reduced their dose below 5 mg•day 1, compared with 33% of the placebo group. Moreover, in this trial a significant reduction in corticosteroid dose in both low (<300 cells•μL−1) and high (≥300 cells•μL−1) blood eosinophil groups were seen, although the greatest response was reported in asthma patients with higher baseline blood eosinophil counts [54].
Tezepelumab is an mAb that targets the epithelial alarmin TSLP, which is released by epithelial cells in response to various pro-inflammatory stimuli and is related to both T2 cytokine expression and asthma severity in asthma [55,56]. In the SOURCE trial, with patients with OCS-dependent asthma, randomized to tezepelumab or placebo, the investigators reported that the trial did not meet the primary endpoint of reducing daily OCS whilst maintaining asthma control [57,58].
Conclusions
Asthma patients are characterized by an increased risk for osteoporosis and fragility fractures, of vertebra and forearm/wrist fractures, compared with the general population [59]. Knowledge of the risk of CS-related toxicities correlated to OCS or parenteral CS therapies for the management of acute severe asthma exacerbations is an important factor to consider in terms of asthma management and safety. It has been reported that the risk of osteoporosis diagnosis and fracture increases per 1-g in systemic CS exposure in asthma patients [60]. Therefore, the use of anti-osteoporotic treatment is essential in adult patients with high cumulative CS exposure (>5 g/year) [61,62]. Moreover, an analysis published in 2021 highlighted how there is an inter-person variability in the risk of OCS-related toxicity among severe asthma patients, as measured by the Glucocorticoid Toxicity Index (GTI), with only a modest correlation between recent OCS exposure and GTI score [63]. This inter-variability appears to be part of the heterogeneity of patients suffering from asthma, with their different phenotypes and endotypes and varying response to treatments, including biological therapies, which have shown a more favourable safety profile compared to therapies the use of which correlates to multi-comorbidities [64,65]. Indeed, as reported by Cutroneo PM et al., conducting an overview of safety data of severe asthma biologics in VigiBase, the World Health Organization global pharmacovigilance database, the most frequently reported suspected adverse drug reactions (ADRs) are the well-known adverse effects such as general disorders, injection-site reactions, nasopharyngitis, headache and hypersensitivity, while others, such as asthma exacerbation or therapeutic failure, may be related to the indication of use [66]. An important aspect to consider in asthma management is that often, despite asthma guidelines recommending biological therapies for severe asthma, patients cannot eliminate the need for OCS during exacerbations [1,67,68]. Physicians managing severe asthma should remain vigilant in assessing the CS-related toxicity risk in patients receiving biologics or long-term OCS, especially in patients with additional osteoporotic risk factors. Therefore, increasing patient awareness, especially in younger populations, as well as physicians’ knowledge on bone condition comorbidities in asthma, particularly in uncontrolled asthma patients that need OCS, may represent the key of all the players involved in asthma management at every level for a better safety profile and for the prevention of comorbidities.
Author Contributions
Conceptualization, F.F.; resources, M.U.S., C.P., and F.F.; writing—original draft preparation, F.F., and M.U.S.; writing—review and editing, F.F., G.R.T.,M.U.S.,C.P. and C.G.G., drawing of figure, F.F., G.R.T., M.U.S; project administration, C.P., and F.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention 2024. Update May 2024. Available online: http://www.ginasthma.org/.
- Kearney, D.M.; Lockey, R.F. Osteoporosis and asthma. Ann Allergy Asthma Immunol. 2006, 96, 769–74. [Google Scholar] [CrossRef] [PubMed]
- Chalitsios, C.V.; Shaw, D.E.; McKeever, T.M. Corticosteroids and bone health in people with asthma: A systematic review and meta-analysis. Respir Med. 2021, 181, 106374. [Google Scholar] [CrossRef] [PubMed]
- Chalitsios, C.V.; McKeever, T.M.; Shaw, D.E. Incidence of osteoporosis and fragility fractures in asthma: a UK population-based matched cohort study. Eur Respir J. 2021, 57, 2001251. [Google Scholar] [CrossRef] [PubMed]
- Heffler, E.; Madeira, L.N.G.; Ferrando, M.; Puggioni, F.; Racca, F.; Malvezzi, L.; Passalacqua, G.; Canonica, G.W. Inhaled Corticosteroids Safety and Adverse Effects in Patients with Asthma. J Allergy Clin Immunol Pract. 2018, 6, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.J.; Phillips, P.J.; Heller, R.F. Asthma and chronic obstructive airway diseases are associated with osteoporosis and fractures: a literature review. Respirology. 1999, 4, 101–9. [Google Scholar] [CrossRef] [PubMed]
- Chalitsios, C.V.; Shaw, D.E.; McKeever, T.M. Risk of osteoporosis and fragility fractures in asthma due to oral and inhaled corticosteroids: two population-based nested case-control studies. Thorax. 2021, 76, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Cardet, J.C.; Bulkhi, A.A.; Lockey, R.F. Nonrespiratory Comorbidities in Asthma. J Allergy Clin Immunol Pract. 2021, 9, 3887–3897. [Google Scholar] [CrossRef] [PubMed]
- Weare-Regales, N.; Hudey, S.N.; Lockey, R.F. Practical Guidance for Prevention and Management of Glucocorticoid-Induced Osteoporosis for the Allergist/Immunologist. J Allergy Clin Immunol Pract. 2021, 9, 1841–1850. [Google Scholar] [CrossRef] [PubMed]
- Carpaij, O.A.; van den Berge, M. The asthma-obesity relationship: underlying mechanisms and treatment implications. Curr Opin Pulm Med. 2018, 24, 42–49. [Google Scholar] [CrossRef]
- Maslan, J.; Mims, J.W. What is asthma? Pathophysiology, demographics, and health care costs. Otolaryngol Clin North Am. 2014, 47, 13–22. [Google Scholar] [CrossRef]
- González-Barcala, F.J.; Muñoz-Gall, X.; Mariscal, E.; García, A.; Yang, S.; van de Wetering, G.; Izquierdo-Alonso, J.L. Cost-effectiveness analysis of anti-IL-5 therapies of severe eosinophilic asthma in Spain. J Med Econ. 2021, 24, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Virchow, J.C.; Barnes, P.J. Asthma. Semin Respir Crit Care Med. 2012, 33, 577. [Google Scholar] [PubMed]
- Barnes, P.J. Cellular and molecular mechanisms of asthma and COPD. Clin Sci (Lond). 2017, 131, 1541–1558. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.J.; Adcock, I.M. How do corticosteroids work in asthma? Ann Intern Med. 2003, 139, 359–70. [Google Scholar] [CrossRef] [PubMed]
- Ginaldi, L.; De Martinis, M.; Ciccarelli, F.; Saitta, S.; Imbesi, S.; Mannucci, C.; Gangemi, S. Increased levels of interleukin 31 (IL-31) in osteoporosis. BMC Immunol. 2015, 16, 60. [Google Scholar] [CrossRef] [PubMed]
- De Martinis, M.; Sirufo, M.M.; Suppa, M.; Ginaldi, L. IL-33/IL-31 Axis in Osteoporosis. Int J Mol Sci. 2020, 21, 1239. [Google Scholar] [CrossRef] [PubMed]
- Sirufo, M.M.; Suppa, M.; Ginaldi, L.; De Martinis, M. Does Allergy Break Bones? Osteoporosis and Its Connection to Allergy. Int J Mol Sci. 2020, 21, 712. [Google Scholar] [PubMed]
- Malerba, M.; Romanelli, G.; Grassi, V. Glucocorticoid-induced osteoporosis in asthma and respiratory diseases. Front Horm Res. 2002, 30, 86–93. [Google Scholar] [PubMed]
- Barnes, P.J. Pathophysiology of asthma. Br J Clin Pharmacol. 1996, 42, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.J.; Phillips, P.J.; Heller, R.F. Asthma and chronic obstructive airway diseases are associated with osteoporosis and fractures: a literature review. Respirology. 1999, 4, 101–9. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.F.; Barnes, P.J. Role of inflammatory mediators in asthma. Br Med Bull. 1992, 48, 135–48. [Google Scholar] [CrossRef] [PubMed]
- Parente, L. Deflazacort therapeutic index, relative potency and equivalent doses versus other corticosteroids, BMC Pharmacology and Toxicology. 2017, 18,1.
- RCP Cortisone.
- RCP Hydrocortisone.
- RCP Deflazacort.
- RCP Prednisolone.
- RCP Prednisone.
- RCP Methylprednisolone.
- RCP Triamcinolone.
- RCP Betamethasone.
- RCP Dexamethasone.
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014, 43, 343–373. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J 2014, 43, 343–373. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Asthma. Difficult-to-treat and severe asthma in adolescent and adult patients. 2019. Available online: https://ginasthma.org/wp-content/uploads/2019/04/GINA-Severe-asthma-Pocket-Guide-v2.0-wms-1.pdf.
- Price, D.B.; Trudo, F.; Voorham, J.; Xu, X.; Kerkhof, M.; Ling, Zhi Jie, J.; Tran, T.N. Adverse outcomes from initiation of systemic corticosteroids for asthma: long-term observational study. J Asthma Allergy. 2018, 11, 193–204. [CrossRef] [PubMed]
- Fahy, J.V. Type 2 inflammation in asthma—present in most, absent in many. Nat Rev Immunol. 2015, 15, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Lambrecht, B.N.; Hammad, H.; Fahy, J.V. The cytokines of asthma. Immunity. 2019, 50, 975–991. [Google Scholar] [CrossRef] [PubMed]
- Teach, S.J.; Gill, M.A.; Togias, A.; Sorkness, C.A.; Arbes, S.J. Jr.; Calatroni, A.; Wildfire, J.J.; Gergen, P.J.; Cohen, R.T.; Pongracic, J.A.; et al. Preseasonal treatment with either omalizumab or an inhaled corticosteroid boost to prevent fall asthma exacerbations. J Allergy Clin Immunol. 2015, 136, 1476–1485. [Google Scholar] [CrossRef] [PubMed]
- Adachi, M.; Kozawa, M.; Yoshisue, H.; Milligan, K.L.; Nagasaki, M.; Sasajima, T.; Miyamoto, T.; Ohta, K. Real-world safety and efficacy of omalizumab in patients with severe allergic asthma: a long-term post-marketing study in Japan. Respir Med. 2018, 141, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Gevaert, P.; Omachi, T.A.; Corren, J.; Mullol, J.; Han, J.; Lee, S.E.; Kaufman, D.; Ligueros-Saylan, M.; Howard, M.; Zhu, R. Efficacy and safety of omalizumab in nasal polyposis: 2 randomized phase 3 trials. J Allergy Clin Immunol. 2020, 146, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Cox, L.; Platts-Mills, T.A.; Finegold, I.; Schwartz, L.B.; Simons, F.E.R.; Wallace, D.V. American Academy of Allergy, Asthma & Immunology/American College of Allergy; Asthma and Immunology joint task force report on omalizumab-associated anaphylaxis. J Allergy Clin Immunol. 2007, 120, 1373–1377. [Google Scholar] [PubMed]
- Sanderson, C. Interleukin-5, eosinophils, and disease. Blood. 1992, 79, 3101–3109. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.A.; Minthorn, E.A.; Beerahee, M. Pharmacokinetics and pharmacodynamics of mepolizumab, an anti-interleukin-5 monoclonal antibody. Clin Pharmacokinet. 2011, 50, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Flood-Page, P.T.; Menzies-Gow, A.N.; Kay, A.B.; Robinson, D.S. Eosinophil’s role remains uncertain as anti–interleukin-5 only partially depletes numbers in asthmatic airway. Am J Respir Crit Care Med. 2003, 167, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Ortega, H.G.; Liu, M.C.; Pavord, I.D.; Brusselle, G.G.; FitzGerald, J.M.; Chetta, A.; Humbert, M.; Katz, L.E.; Keene, O.N.; Yancey, S.W.; Chanez, P.; MENSA Investigators. Mepolizumab treatment in patients with severe eosinophilic asthma. N Engl J Med. 2014, 371, 1198–1207. [Google Scholar] [PubMed]
- Bel, E.H.; Wenzel, S.E.; Thompson, P.J.; Prazma, C.M.; Keene, O.N.; Yancey, S.W.; Ortega, H.G.; Pavord, I.D. SIRIUS Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. N Engl J Med. 2014, 371, 1189–1197. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, J.E.; d’Ancona, G.; Elstad, M.; Green, L.; Fernandes, M.; Thomson, L.; Roxas, C.; Dhariwal, J.; Nanzer, A.M.; Kent, B.D.; Jackson, D.J. Real-world effectiveness and the characteristics of a ‘super-responder’ to mepolizumab in severe eosinophilic asthma. Chest 2020, 158, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Ghazi, A.; Trikha, A.; Calhoun, W.J. Benralizumab – a humanized mAb to IL-5Rα with enhanced antibody-dependent cell-mediated cytotoxicity – a novel approach for the treatment of asthma. Expert Opin Biol Ther. 2012, 12, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Kolbeck, R.; Kozhich, A.; Koike, M.; Peng, L.; Andersson, C.K.; Damschroder, M.M.; Reed, J.L.; Woods, R.; Dall’acqua, W.W.; Stephens, G.L. MEDI-563, a humanized anti-IL-5 receptor alpha mAb with enhanced antibody-dependent cell-mediated cytotoxicity function. J Allergy Clin Immunol 2010, 125, 1344–1353. [Google Scholar] [CrossRef] [PubMed]
- Nair, P.; Wenzel, S.; Rabe, K.F.; Bourdin, A.; Lugogo, N.L.; Kuna, P.; Barker, P.; Sproule, S.; Ponnarambil, S.; Goldamn, M.; Zonda Trial Investigators. Oral glucocorticoid–sparing effect of benralizumab in severe asthma. N Engl J Med. 2017, 376, 2448–2458. [Google Scholar] [PubMed]
- Menzies-Gow, A.; Gurnell, M.; Heaney, L.G.; Corren, J.; Bel, E.H.; Maspero, J.; Harrison, T.; Jackson, D.J.; Price, D.; Lugogo, N.; et al. Oral corticosteroid elimination via a personalised reduction algorithm in adults with severe, eosinophilic asthma treated with benralizumab (PONENTE): a multicentre, open-label, single-arm study. Lancet Respir Med. 2022, 10, 47–58. [Google Scholar] [CrossRef]
- Rabe, K.F.; Nair, P.; Brusselle, G.; Maspero, J.F.; Castro, M.; Sher, L.; Zhu, H.; Hamilton, J.D.; Swanson, B.N.; Khan, A.; et al. Efficacy and safety of dupilumab in glucocorticoid-dependent severe asthma. N Engl J Med. 2018, 378, 2475–2485. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, J.E.; Hearn, A.P.; Jackson, D.J. A pragmatic guide to choosing biologic therapies in severe asthma. Breathe (Sheff). 2021, 17, 210144. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, S.F.; Roan, F.; Bell, B.D.; Stoklasek, T.A.; Kitajima, M.; Han, H. The biology of thymic stromal lymphopoietin (TSLP). Adv Pharmacol. 2013, 66, 129–155. [Google Scholar]
- Ying, S.; O’Connor, B.; Ratoff, J.; Meng, Q.; Mallett, K.; Cousins, D.; Robinson, D.; Zhang, G.; Lee, T.H.; Corrigan, C. Thymic stromal lymphopoietin expression is increased in asthmatic airways and correlates with expression of Th2-attracting chemokines and disease severity. J Immunol. 2005, 174, 8183–8190. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, M.E.; Colice, G.; Griffiths, J.M.; Almqvist, G.; Skärby, T.; Piechowiak, T.; Kaur, P.; Bowen, K.; Hellqvist, A.; Mo, M.; Garcia Gil, G. SOURCE: a phase 3, multicentre, randomized, double-blind, placebo-controlled, parallel group trial to evaluate the efficacy and safety of tezepelumab in reducing oral corticosteroid use in adults with oral corticosteroid dependent asthma. Respir Res. 2020, 21, 264. [Google Scholar] [CrossRef]
- AstraZeneca. Update on SOURCE Phase III trial for tezepelumab in patients with severe, oral corticosteroid-dependent asthma. Date date last updated: 22 December 2020. 2020. Available online: https://www.astrazeneca.com/media-centre/press-releases/2020/update-on-source-phase-iii-trial-for-tezepelumab-in-patients-with-severe-oral-corticosteroid-dependent-asthma.html (accessed on 14 September 2021).
- Chalitsios, C.V.; McKeever, T.M.; Shaw, D.E. Incidence of osteoporosis and fragility fractures in asthma: a UK population-based matched cohort study. Eur Respir J. 2021, 57, 2001251. [Google Scholar] [CrossRef] [PubMed]
- Price, D. B.; Trudo, F.; Voorham, J.; Xu, X.; Kerkhof, M.; Ling Zhi Jie, J.; Tran, T.N. Adverse outcomes from initiation of systemic corticosteroids for asthma: Long-term observational study. J. Asthma Allergy. 2018, 11, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Buckley, L.; Guyatt, G.; Fink, H. A.; Cannon, M.; Grossman, J.; Hansen, K. E.; Humphrey, M.B.; Lane, N.E.; Magrey, M.; Miller, M.; et al. American college of rheumatology guideline for the prevention and treatment of glucocorticoid-induced osteoporosis. Arthritis Rheumatol. 2017, 69, 1521–1537. [Google Scholar] [CrossRef] [PubMed]
- Naranjo Hernández, A.; Díaz Del Campo Fontecha, P.; Aguado Acín, M.P.; Arboleya Rodríguez, L.; Casado Burgos, E.; Castañeda, S.; Arestè, J.F.; Gifre, L.; Gòmez Vaquero, C.; Rodrìguez, G.C.; et al. Recommendations by the Spanish society of rheumatology on osteoporosis. Reumatol. Clin. Engl. 2019, 15, 188–210. [Google Scholar] [CrossRef] [PubMed]
- McDowell, P. J.; Stone, J. H.; Zhang, Y.; Honeyford, K.; Dunn, L.; Logan, R. J.; Butler, C.A.; McGarvey, L.P.A.; Heaney, L.G. Quantification of glucocorticoid-associated morbidity in severe asthma using the Glucocorticoid Toxicity Index. J. Allergy Clin Immunol Pract. 2021, 9, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Portacci, A.; Dragonieri, S.; Carpagnano, G.E. Super-Responders to Biologic Treatment in Type 2-High Severe Asthma: Passing Fad or a Meaningful Phenotype? J Allergy Clin Immunol Pract. 2023, 11, 1417–1420. [Google Scholar] [CrossRef] [PubMed]
- Caminati, M.; Vaia, R.; Furci, F.; Guarnieri, G.; Senna, G. Uncontrolled Asthma: Unmet Needs in the Management of Patients. J Asthma Allergy. 2021, 14, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Cutroneo, P.M.; Arzeton, E.; Furci, F.; Scapini, F.; Bulzomì, M.; Luxi, N.; Caminati, M.; Senna, G.; Moretti, U.; Trifirò, G. Safety of Biological Therapies for Severe Asthma: An Analysis of Suspected Adverse Reactions Reported in the WHO Pharmacovigilance Database. BioDrugs. 2024, 38, 425–448. [Google Scholar] [CrossRef] [PubMed]
- Weare-Regales, N.; Hudey, S. N.; Lockey, R. F. Practical guidance for prevention and management of glucocorticoid-induced osteoporosis for the allergist/immunologist. J. Allergy Clin. Immunol Pract. 2021, 9, 1841–1850. [Google Scholar] [CrossRef] [PubMed]
- Lommatzsch, M.; Buhl, R.; Canonica, G.W.; Ribas, C.D.; Nagase, H.; Brusselle, G.G.; Jackson, D.J.; Pavord, I.D.; Korn, S.; Milger, K.; et al. Pioneering a paradigm shift in asthma management: remission as a treatment goal. Lancet Respir Med. 2024, 12, 96–99. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



