
Submitted:
02 August 2024
Posted:
06 August 2024
You are already at the latest version
Abstract
(1) Background: This report aims to illustrate the development, progression, diagnosis and treatment of chronically present articular surface lesions; (2) Methods: In this report, two patients are described from the point of initial presentation of symptoms to surgical consultation based on radiologic findings. These patients underwent corrective surgery in the form of mosaicplasty to repair the lesion present at the articular surface and the underlying subchondral bone. (3) Discussion: Diagnosing juvenile OCD remains challenging due to variable clinical presentation and minute radiologic discoveries. X-rays are useful, however, the gold standard remains to be arthroscopy which can be both diagnostic and therapeutic. Future prospects include the use of novel sonographic methods and the use of artificial intelligence within the given modalities. (4) Conclusions: The detailed imaging provided by MRI, combined with the insights from X-rays and potentially other modalities, allows for a nuanced understanding of the disease. This comprehensive approach ensures that treatment decisions are well-informed, optimizing outcomes for young patients with this condition.
Keywords:
osteochondritis dissecans
; OCD
; mosaicplasty
; elbow
; talar
; articular surface
; congruency
1. Introduction
Juvenile osteochondritis dissecans (OCD) is a condition which occurs when the blood supply is diminished in a segment of bone and its surrounding cartilage which may necrotise and separate from the underlying tissues [1]. Primarily the condition affects children and adolescents who are physically active. Towards the end of the 1800s, Franz König described the condition as an inflammatory process which yields loose bodies within the joint. However, novel research methods have revealed that the primary issue is not inflammation but is rather due to the disruption of the blood supply of subchondral bone [2]. As time passed, this shifted the attention regarding the development of OCD towards mechanical and vascular factors. The diagnostic criteria have evolved but the recognition of juvenile OCD is still a significant challenge. Juvenile OCD is much more prevalent than in adults, with no exact number of cases per year, only rough estimates. Most frequently the knee (9-29/100.000), ankle (2-5/100.000), and elbow (2/100.000) are affected with the possibility of smaller joint involvement. The condition is rare under the age of 10, with an increased risk from age 12-19 [1]. Generally, boys are four times more likely to suffer from OCD in the knee and the elbow, however, girls have a 1.5 times higher risk of developing the condition in the ankle. Typically in the knee, the defect will present at the posterior-central medial condyle (63-85%), followed by the lateral condyle inferior-centrally (15-32%), the infero-medial aspect of the patella (1.5-10%), and the trochlea (2%) [3]. Bilateral involvement in 7-29% of cases. In the elbow, the capitulum is affected in an anterolateral or central position (97.5%) tenfold more often than the trochlea (2.5%). Talar OCD lesions are commonly posteromedial (71%), anterolateral (22%) or central (3.5%). Talar bilateral involvement is rare. OCD tends to affect active children and young adults [1,3]. Participation in high-intensity sports activities and athletics is commonly associated with developing the condition in the knee (60%), elbow (84%) and ankle (64%) [3]. The condition is frequently associated with football, basketball, and gymnastics. The risk of developing the condition further increases with obesity. Moderate obesity will increase the risk of developing knee while extreme obesity will increase the risk of talar OCD. A trend of early onset may be associated with early intensive sports activities or severe childhood obesity [3,4].
The condition’s aetiology is not well understood, even though advancements have been made regarding pathogenesis. As the name suggests an inflammatory process should be present, however minimal evidence supports this, either histologically or biochemically [1,3]. Human histochemical studies have shown necrosis in the subchondral bone and the epiphyseal cartilage, cartilage degradation, and matrix metalloproteinase expression linked to chondrocyte apoptosis. The presence of osteonecrosis due to steroids, radiation, hemoglobinopathies or chemotherapy could also potentially provide a pathway for degenerative changes, but the most recent systematic review suggests OCD’s cause likely involves both mechanical and biological factors [1,5]. The microtrauma theory was introduced in the ’50s to describe the pathogenesis of the condition, but since then, the literature has provided arguments for repetitive microtrauma, anatomic variations of the condyles, discoid meniscus, or posterior cruciate ligament [6,7,8]. Incorrect knee positioning, obesity, soft tissue instability and lower limb misalignment have been shown to be part of the biomechanical background of developing the condition [9,10]. Genetic involvement was suggested due to the increased incidence of the disease in monozygotes [8,11]. Hypovitaminosis, namely vitamin D, has been proven to impact disease development significantly [12,13,14].
The susceptibility for ischemic injury can be explained by the vascularity of subchondral bone, which has been demonstrated to be supplied with poor arterial anastomoses, such as in the case of bowel mesentery. Tóth et al. used imaging techniques to demonstrate the involvement of abnormal vascular structure at the predicted sites of OCD in cadavers [2]. The subarticular epiphyseal cartilage shapes adult joint geometry, the survival of which depends on proper blood supply. As the secondary ossification centres expand during growth, these vessels regress [2,15]. The preceding condition called osteochondritis latens, was shown to be caused by premature regression of these vessels, which led to the necrosis of the epiphyseal cartilage in animal samples [5,16]. This lesion will spare the articular surface and the subchondral bone involving only the epiphyseal cartilage. Osteochondritis manifesta results in insufficient mechanical reinforcement to the overlying cartilage. This occurs as growth continues and the ossification reaches the lesion, a necrotic piece of cartilage will be trapped inside the subchondral bone [17]. These lesions may heal on their own as presented in animal studies [18]. Nonetheless, osteochondritis dissecans may develop from these lesions, either due to trauma or repetitive microtrauma [18].
Diagnosis is made difficult due to varying symptoms, depending on severity. Mechanical symptoms, namely locking and catching, are indicative of loose bodies or unstable lesions [1,19]. Those who live an active lifestyle or are involved in sports activities are at a higher risk, with symptoms often surfacing following repetitive microtrauma or a specific injury. Diagnostic delays can occur due to the non-specific nature of early symptoms, underscoring the importance of thorough clinical and radiological evaluation for accurate diagnosis.
The primary diagnostic tools include X-ray and MRI, however novel sonographic methods have been described in recent years, detecting elbow injuries [20]. Many classifications exist based on either the location or severity of the injury, depending on the type of imaging. A summary of these can be viewed in Table 1. However, a simplified staging can be utilised for all OCD lesions characterising the severity of the injury into (I) subchondral defect, (II) surface defect, (III) loose body, (IV)displaced fragment and articular incongruence.
The most important factors determining the treatment plan are lesion stability and skeletal maturity. Generally, non-operative treatment is adequate in case of stable lesions, open physis or in asymptomatic cases. This entails 3-6 months with activity modification and weight-bearing limitations with the possibility of immobilisation, which is controversial [25]. Surgical correction is indicated for unstable lesions or failed conservative management. Options for stable lesions include trans articular or retroarticular drilling [3]. Unstable but salvageable lesions can be treated by aiming to correct the fracture, realign the articular surface and increase blood supply. This can be achieved by headless, partially threaded compression screws, which can be metal or made out of bioabsorbable materials such as PLGA [26]. If a loose body cannot be saved due to fragmentation, necrosis or cartilage degeneration restorative techniques should be applied. Options include osteochondral autograft transplant - also known as mosaicplasty - autologous chondrocyte implantation or allograft transplants, as loose body excision alone leads to poor outcomes [27].
2. Materials and Methods
Patient 1: The first patient arrived at the clinic in October of 2021 with persistent pain which resulted from an injury a month prior. At the initial evaluation, an X-ray was performed which could not identify a fracture, however raised the possibility of OCD (Figure 1).
With proper conservative treatment, the pain persisted throughout the recovery period. Due to this, in suspicion of osteochondral injury, an MRI was requested which revealed the unstable defect of the talar surface, medially (Figure 2).
Due to symptomatic disease progression, surgery was advocated for, which took place on 2023.06.14. Under general anaesthesia, an osteotomy was performed to access the talar surface giving a view of the defect (Figure 3).
The OCD lesion was removed and mosaicplasty was carried out. The graft piece was obtained from the non-weight-bearing surface of the left femoral lateral condyle. After proper positioning and adequate results of the articular surface and its congruency, the osteotomy was repaired and fixed with two absorbable nails, made out of poly-L-lactide-co-glycolic acid (PLGA) (Figure 4). After closure, swathing and bandage took place and the ankle was fixed with an ankle brace.
In the postoperative period, no complications were noted and radiologic control examinations confirmed the proper position of the mosaicplasty as well as the osteotomy (Figure 5). Control examinations took place 2 months after the operation which were unremarkable (Figure 6).
The child underwent physiotherapeutic training in the postoperative period. The ankle was immobilised and no body weight bearing was permitted for the initial …. weeks. The knee was moved with continuous passive motion exercises (CPM) as well as the ankle until the pain threshold was reached during movement. Mobilisation could occur with the help of clutches and further examinations are planned as part of the continued follow-ups. The one-month post-op control evaluation concluded that the implants and the graft were well in place and no complaints or complications were reported during the healing period.
Patient 2: The child is an athlete and performs a continuous active movement in the form of gymnastics on a daily basis. Her complaints started half a year prior to December of 2021 when they presented at the clinic. The patient does not remember a specific injury which might have elicited the original onset, however, she complained of several minor injuries and falls which occur with regular frequency. The ROM of the left elbow has decreased to 20-100 degrees. Neurovascular pathologies could not be identified or elicited with specific tests. An MR examination took place which revealed a loose chondral body (Figure 7).
On 2022.01.07. under general anesthesia the patient underwent surgery. The joint was accessed through a minimally invasive anterolateral incision (about 3 cm) (Figure 8-A). After visualisation, the loose chondral fragment was removed as well as some excess coagulum originating from the synovium (Figure 8-C).
The defect was 10x11mm in space which was corrected by mosaicplasty. The graft piece was obtained from the non-weight-bearing surface of the femur’s lateral condyle and was attached to yield a fresh congruent articular surface (Figure 9). The joint capsule was reconstructed and the wound was closed with 4-0 Vycryl absorbable thread with a continuous intracutaneous technique. Before swathing and bandaging a nerve block was initiated with a sodium-channel blocker and tonogen to lessen the immediate post-op pain.
After congruence was confirmed, the joint capsule was reconstructed and the incision was sutured with 4-0 Vycryl thread and a continuous intracutaneous suture. Following swathing and bandaging an elbow brace was applied in 90 degree position. Control X-ray after surgery confirms the proper congruence (Figure 10-A/B).
The child underwent physiotherapeutic training in the postoperative period. The elbow was immobilised for the first …. weeks. The elbow was trained with continuous passive motion exercises (CPM) until the pain threshold was reached during movement. During the first 8 weeks elbow extension-flexion was limited to 20-120, meaning that extension and flexion were incomplete. The asymmetry between the two extremities can be seen in several different positions (Figure 11). The incongruence was corrected with the help of one year of physiotherapy. The patient gradually returned to sports and gymnastics after one year.
The control MR imaging, at six months, has proved that the lesion was corrected adequately and that the fixation maintained the function and congruency of the joint. However, effectiveness and long-term success should be further evaluated in the patient during adolescence and young adulthood.
After one year, the ROM was complete and could yield 0-130 degrees of movement (Figure 11 A/B/C/D-2). Pronation and supination were painless and no complications or complaints could be noted even with physical activity.
3. Discussion
Variable clinical presentation and subtle radiological findings make the diagnosis of juvenile OCD still challenging. Comprehensive imaging techniques are essential for the proper staging of the condition and for determining the appropriate treatment strategy.
The primary diagnostic modalities for OCD include X-ray and MRI, with each offering distinct advantages. X-rays, being the initial imaging technique, are valuable for identifying gross abnormalities such as lesions or bone fragments. However, their sensitivity is limited, particularly in the early stages of OCD when subchondral bone changes are minimal or absent. MRI, on the other hand, provides a detailed view of both bone and soft tissue, making it the gold standard for diagnosing OCD. It is particularly effective in detecting early subchondral changes, the presence of loose bodies, and cartilage status, which are not visible on X-rays. The use of MRI allows for a more nuanced classification of the lesions, aiding in the assessment of lesion stability and the extent of cartilage involvement. This is crucial for planning treatment, as the choice between conservative management and surgical intervention often hinges on these details. MRI findings such as the presence of high signal changes behind the lesion, indicating fluid or fibrous tissue, can signal instability, thus guiding more aggressive treatment approaches. In today's world, AI programming could also aid the diagnosis of OCD and may be expected to routinely check X-ray images for defects within the near future as it has been used for several conditions [28,29,30].
Accurate staging through radiological evaluation not only helps in the initial diagnosis but also in monitoring disease progression and response to treatment. For instance, conservative management, often preferred in stable lesions, can be monitored for healing or progression through follow-up MRIs. Conversely, surgical intervention, including techniques like mosaicplasty, is considered when imaging shows unstable lesions or significant cartilage damage. Generally, follow-up should be one year minimum, but optimally would last a span of 3-5 years. MRI should be made yearly to properly monitor healing or disease progression to avoid long-term complications. Early on graft rejection, infection, and bleeding. Later joint stiffness, arthritis, graft necrosis, or donor site morbidity [27].
Arthroscopy can be both therapeutic and diagnostic but this procedure requires experience. This should take place if the patient has persistent pain, deficit in the range of motion, and locking or catching [22]. If the arthroscopic findings can support the radiological results a therapeutic approach should take place with debridement, removal if necessary, and restorative approaches, such as mosaicplasty [19].
4. Conclusions
In conclusion, the integration of comprehensive diagnostic and radiological evaluation is indispensable in the management of juvenile OCD. The detailed imaging provided by MRI, combined with the insights from X-rays and potentially other modalities, allows for a nuanced understanding of the disease. This comprehensive approach ensures that treatment decisions are well-informed, optimizing outcomes for young patients with this condition.
Author Contributions
Conceptualization, G.J. and T.K and H.N.; methodology, H.N.; software, A.L.; validation, G.J., H.N., T.K, and A.L.; formal analysis, A.L.; investigation, G.J., T.K., and H.N.; resources, G.J.; data curation, G.J.; writing—original draft preparation, H.N.; writing—review and editing, H.N.; visualization, G.J., and T.K..; supervision, G.J.; project administration, G.J.; funding acquisition, G.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Regional Research Ethics Committee, Clinical Complex, University of Pécs [Pécsi Tudományegyetem, Klinikai Komplex, Regionális és Intézményi Kutatás—Etikai Bizottság] on 9 April 2021 (6138-PTE2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
All data is contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Bruns, J.; Werner, M.; Habermann, C. Osteochondritis Dissecans: Etiology, Pathology, and Imaging with a Special Focus on the Knee Joint. Cartilage 2018, 9, 346–362. [CrossRef]
- Tóth, F.; Nissi, M.J.; Ellermann, J.M.; Wang, L.; Shea, K.G.; Polousky, J.; Carlson, C.S. Novel Application of Magnetic Resonance Imaging Demonstrates Characteristic Differences in Vasculature at Predilection Sites of Osteochondritis Dissecans. Am. J. Sports Med. 2015, 43, 2522–2527. [CrossRef]
- Chau, M.M.; Klimstra, M.A.; Wise, K.L.; Ellermann, J.M.; Tóth, F.; Carlson, C.S.; Nelson, B.J.; Tompkins, M.A. Osteochondritis Dissecans. J. Bone Joint Surg. Am. 2021, 103, 1132–1151. [CrossRef]
- Hefti, F.; Beguiristain, J.; Krauspe, R.; Möller-Madsen, B.; Riccio, V.; Tschauner, C.; Wetzel, R.; Zeller, R. Osteochondritis Dissecans: A Multicenter Study of the European Pediatric Orthopedic Society. J. Pediatr. Orthop. Part B 1999, 8, 231–245.
- Tóth, F.; Nissi, M.J.; Wang, L.; Ellermann, J.M.; Carlson, C.S. Surgical Induction, Histological Evaluation, and MRI Identification of Cartilage Necrosis in the Distal Femur in Goats to Model Early Lesions of Osteochondrosis. Osteoarthr. Cartil. OARS Osteoarthr. Res. Soc. 2015, 23, 300–307. [CrossRef]
- Kamei, G.; Adachi, N.; Deie, M.; Nakamae, A.; Nakasa, T.; Shibuya, H.; Okuhara, A.; Niimoto, T.; Kazusa, H.; Ohkawa, S.; et al. Characteristic Shape of the Lateral Femoral Condyle in Patients with Osteochondritis Dissecans Accompanied by a Discoid Lateral Meniscus. J. Orthop. Sci. Off. J. Jpn. Orthop. Assoc. 2012, 17, 124–128. [CrossRef]
- Ishikawa, M.; Adachi, N.; Yoshikawa, M.; Nakamae, A.; Nakasa, T.; Ikuta, Y.; Hayashi, S.; Deie, M.; Ochi, M. Unique Anatomic Feature of the Posterior Cruciate Ligament in Knees Associated With Osteochondritis Dissecans. Orthop. J. Sports Med. 2016, 4, 2325967116648138. [CrossRef]
- Takigami, J.; Hashimoto, Y.; Tomihara, T.; Yamasaki, S.; Tamai, K.; Kondo, K.; Nakamura, H. Predictive Factors for Osteochondritis Dissecans of the Lateral Femoral Condyle Concurrent with a Discoid Lateral Meniscus. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2018, 26, 799–805. [CrossRef]
- Gonzalez-Herranz, P.; Rodriguez, M.L.; de la Fuente, C. Femoral Osteochondritis of the Knee: Prognostic Value of the Mechanical Axis. J. Child. Orthop. 2017, 11, 1–5. [CrossRef]
- McElroy, M.J.; Riley, P.M.; Tepolt, F.A.; Nasreddine, A.Y.; Kocher, M.S. Catcher’s Knee: Posterior Femoral Condyle Juvenile Osteochondritis Dissecans in Children and Adolescents. J. Pediatr. Orthop. 2018, 38, 410–417. [CrossRef]
- Matching Osteochondritis Dissecans Lesions in Identical Twin Brothers - PubMed Available online: https://pubmed.ncbi.nlm.nih.gov/24025016/ (accessed on 11 July 2024).
- Oberti, V.; Sanchez Ortiz, M.; Allende, V.; Masquijo, J. Prevalencia de Hipovitaminosis D En Pacientes Con Osteocondritis Disecante Juvenil. Rev. Esp. Cir. Ortopédica Traumatol. 2021, 65, 132–137. [CrossRef]
- Bruns, J.; Werner, M.; Soyka, M. Is Vitamin D Insufficiency or Deficiency Related to the Development of Osteochondritis Dissecans? Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2016, 24, 1575–1579. [CrossRef]
- Maier, G.S.; Lazovic, D.; Maus, U.; Roth, K.E.; Horas, K.; Seeger, J.B. Vitamin D Deficiency: The Missing Etiological Factor in the Development of Juvenile Osteochondrosis Dissecans? J. Pediatr. Orthop. 2019, 39, 51–54. [CrossRef]
- Ellermann, J.M.; Ludwig, K.D.; Nissi, M.J.; Johnson, C.P.; Strupp, J.P.; Wang, L.; Zbýň, Š.; Tóth, F.; Arendt, E.; Tompkins, M.; et al. Three-Dimensional Quantitative Magnetic Resonance Imaging of Epiphyseal Cartilage Vascularity Using Vessel Image Features. JBJS Open Access 2019, 4, e0031. [CrossRef]
- Olstad, K.; Ekman, S.; Carlson, C.S. An Update on the Pathogenesis of Osteochondrosis. Vet. Pathol. 2015, 52, 785–802. [CrossRef]
- Tóth, F.; Tompkins, M.A.; Shea, K.G.; Ellermann, J.M.; Carlson, C.S. Identification of Areas of Epiphyseal Cartilage Necrosis at Predilection Sites of Juvenile Osteochondritis Dissecans in Pediatric Cadavers. J. Bone Joint Surg. Am. 2018, 100, 2132–2139. [CrossRef]
- McCoy, A.M.; Toth, F.; Dolvik, N.I.; Ekman, S.; Ellermann, J.; Olstad, K.; Ytrehus, B.; Carlson, C.S. Articular Osteochondrosis: A Comparison of Naturally-Occurring Human and Animal Disease. Osteoarthr. Cartil. OARS Osteoarthr. Res. Soc. 2013, 21, 10.1016/j.joca.2013.08.011. [CrossRef]
- Cabral, J.; Duart, J. Osteochondritis Dissecans of the Knee in Adolescents: How to Treat Them? J. Child. Orthop. 2023, 17, 54–62. [CrossRef]
- Takahara, M.; Ogino, T.; Tsuchida, H.; Takagi, M.; Kashiwa, H.; Nambu, T. Sonographic Assessment of Osteochondritis Dissecans of the Humeral Capitellum. AJR Am. J. Roentgenol. 2000, 174, 411–415. [CrossRef]
- Berndt, A.L.; Harty, M. Transchondral Fractures (Osteochondritis Dissecans) of the Talus. J. Bone Joint Surg. Am. 1959, 41-A, 988–1020.
- Guhl, J.F. Arthroscopic Treatment of Osteochondritis Dissecans. Clin. Orthop. 1982, 65–74.
- Brittberg, M.; Winalski, C.S. Evaluation of Cartilage Injuries and Repair. J. Bone Joint Surg. Am. 2003, 85-A Suppl 2, 58–69. [CrossRef]
- Dipaola, J.D.; Nelson, D.W.; Colville, M.R. Characterizing Osteochondral Lesions by Magnetic Resonance Imaging. Arthrosc. J. Arthrosc. Relat. Surg. Off. Publ. Arthrosc. Assoc. N. Am. Int. Arthrosc. Assoc. 1991, 7, 101–104. [CrossRef]
- Wall, E.J.; Vourazeris, J.; Myer, G.D.; Emery, K.H.; Divine, J.G.; Nick, T.G.; Hewett, T.E. The Healing Potential of Stable Juvenile Osteochondritis Dissecans Knee Lesions. J. Bone Joint Surg. Am. 2008, 90, 2655–2664. [CrossRef]
- Gentile, P.; Chiono, V.; Carmagnola, I.; Hatton, P.V. An Overview of Poly(Lactic-Co-Glycolic) Acid (PLGA)-Based Biomaterials for Bone Tissue Engineering. Int. J. Mol. Sci. 2014, 15, 3640–3659. [CrossRef]
- Sanders, T.L.; Pareek, A.; Obey, M.R.; Johnson, N.R.; Carey, J.L.; Stuart, M.J.; Krych, A.J. High Rate of Osteoarthritis After Osteochondritis Dissecans Fragment Excision Compared With Surgical Restoration at a Mean 16-Year Follow-Up. Am. J. Sports Med. 2017, 45, 1799–1805. [CrossRef]
- Dankelman, L.H.M.; Schilstra, S.; IJpma, F.F.A.; Doornberg, J.N.; Colaris, J.W.; Verhofstad, M.H.J.; Wijffels, M.M.E.; Prijs, J.; Machine Learning Consortium Artificial Intelligence Fracture Recognition on Computed Tomography: Review of Literature and Recommendations. Eur. J. Trauma Emerg. Surg. Off. Publ. Eur. Trauma Soc. 2023, 49, 681–691. [CrossRef]
- Adams, S.J.; Henderson, R.D.E.; Yi, X.; Babyn, P. Artificial Intelligence Solutions for Analysis of X-Ray Images. Can. Assoc. Radiol. J. J. Assoc. Can. Radiol. 2021, 72, 60–72. [CrossRef]
- Kraus, M.; Anteby, R.; Konen, E.; Eshed, I.; Klang, E. Artificial Intelligence for X-Ray Scaphoid Fracture Detection: A Systematic Review and Diagnostic Test Accuracy Meta-Analysis. Eur. Radiol. 2024, 34, 4341–4351. [CrossRef]
Figure 1.
First X-ray taken after the initial injury.

Figure 2.
MR Images A-P (a), side view (b) and T2-weighted (c).

Figure 3.
Intra-op images immediately post osteotomy, revealing the defect.
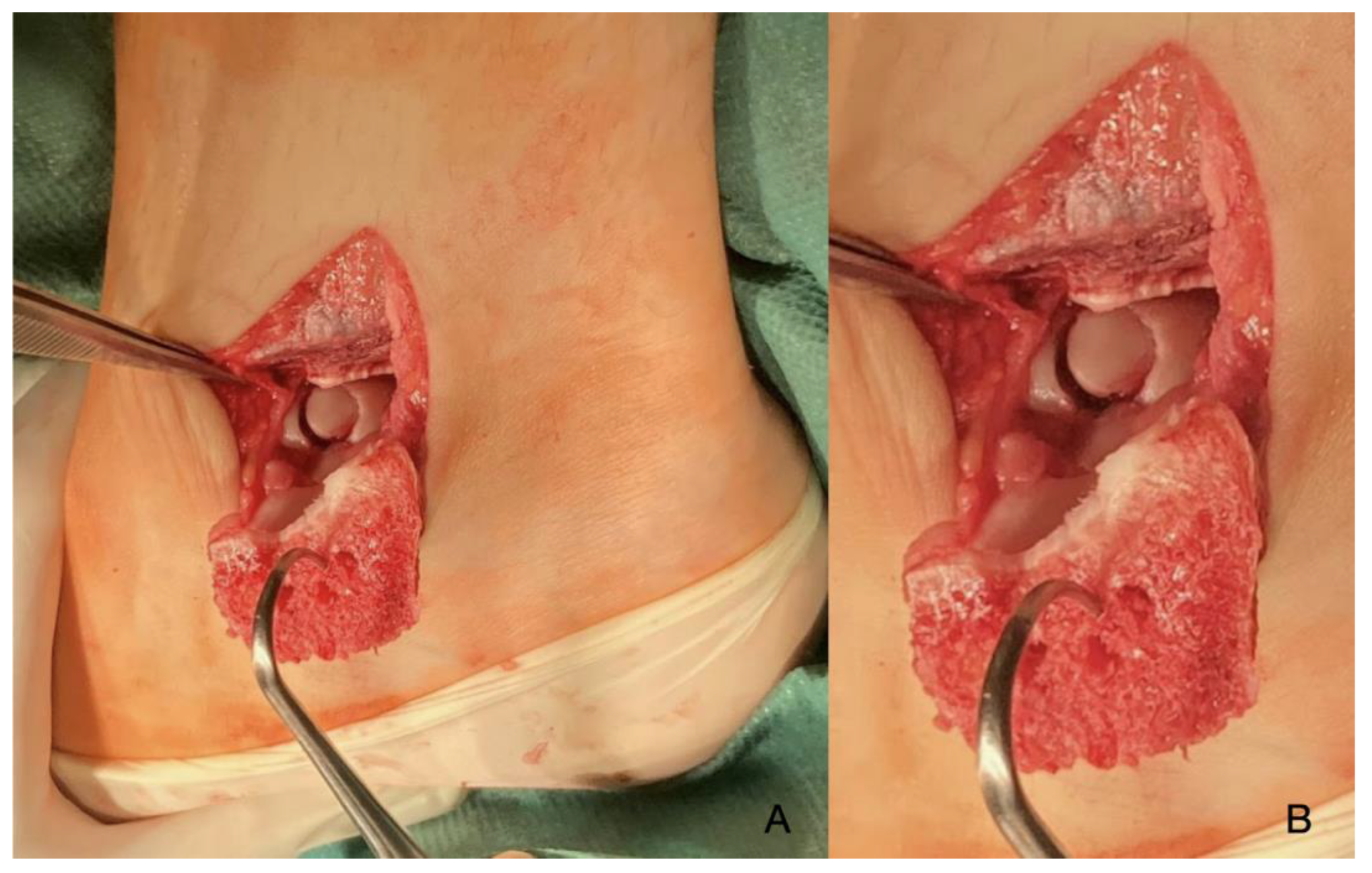
Figure 4.
The defect after the removal of the damaged body(A and B), articuéar surface after mosaicplasty (C), and osteotomy fixed with absorbable nails (D).
Figure 4.
The defect after the removal of the damaged body(A and B), articuéar surface after mosaicplasty (C), and osteotomy fixed with absorbable nails (D).
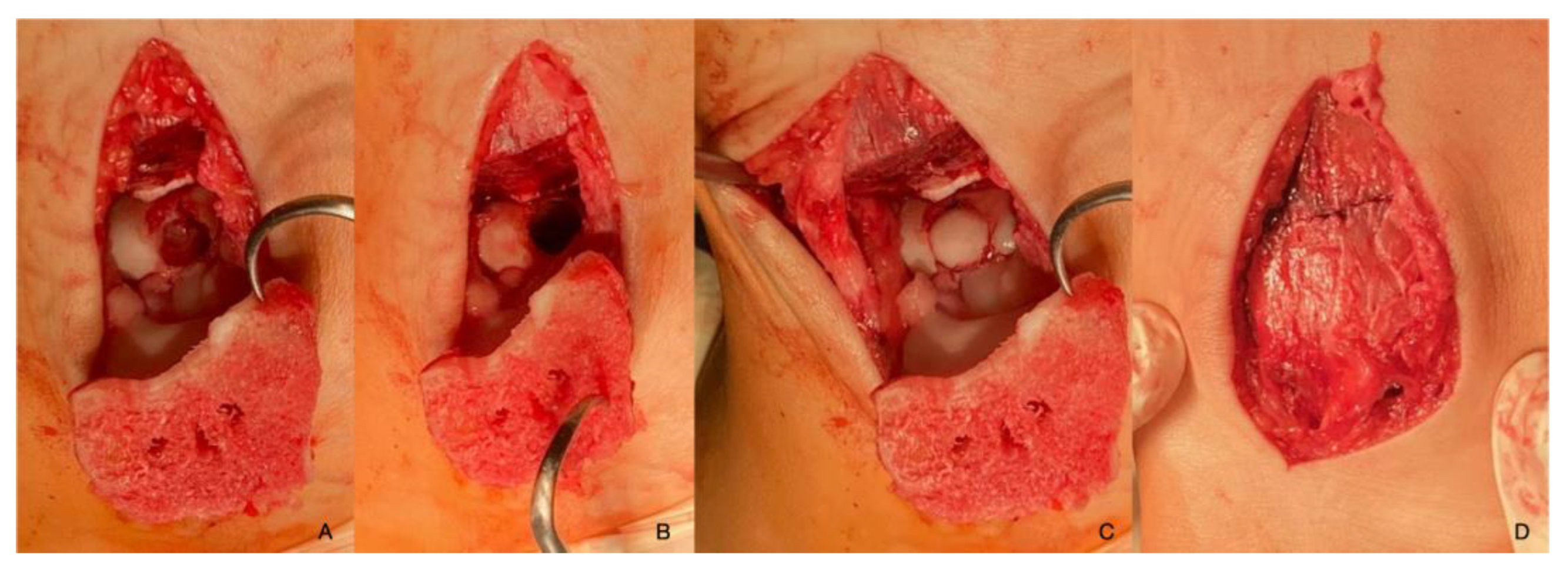
Figure 5.
Post-operative X-ray images showing the proper position of the osteotomy with the nail canal visible and the congruent articular surface after mosaicplasty.
Figure 5.
Post-operative X-ray images showing the proper position of the osteotomy with the nail canal visible and the congruent articular surface after mosaicplasty.

Figure 7.
MR image highlighting the chondral piece of the capitulum humeri.
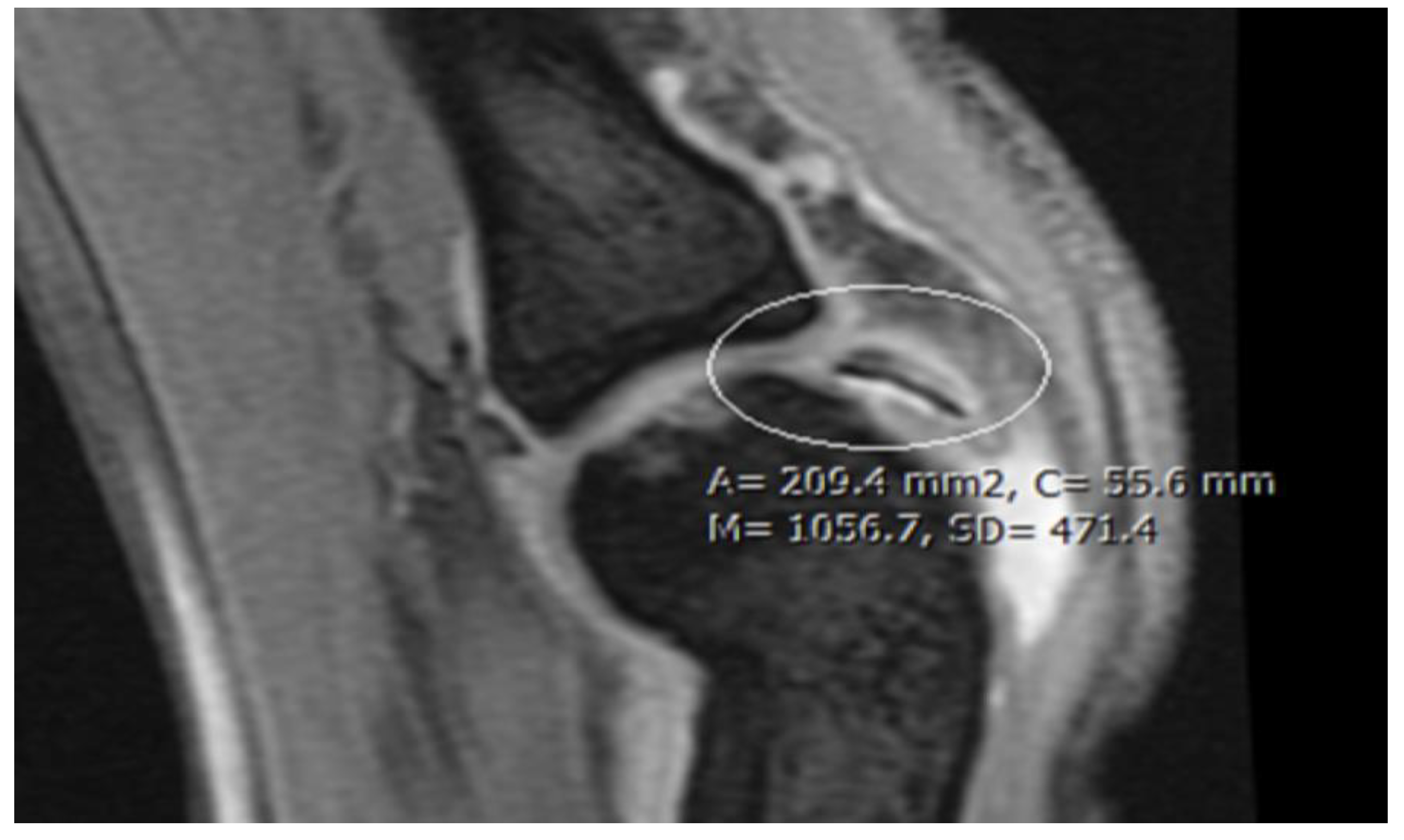
Figure 8.
The defect of the humerus (A and B). The chondral fragment can be seen (black arrow) as well as some synovial coagulum which was removed (C).
Figure 8.
The defect of the humerus (A and B). The chondral fragment can be seen (black arrow) as well as some synovial coagulum which was removed (C).
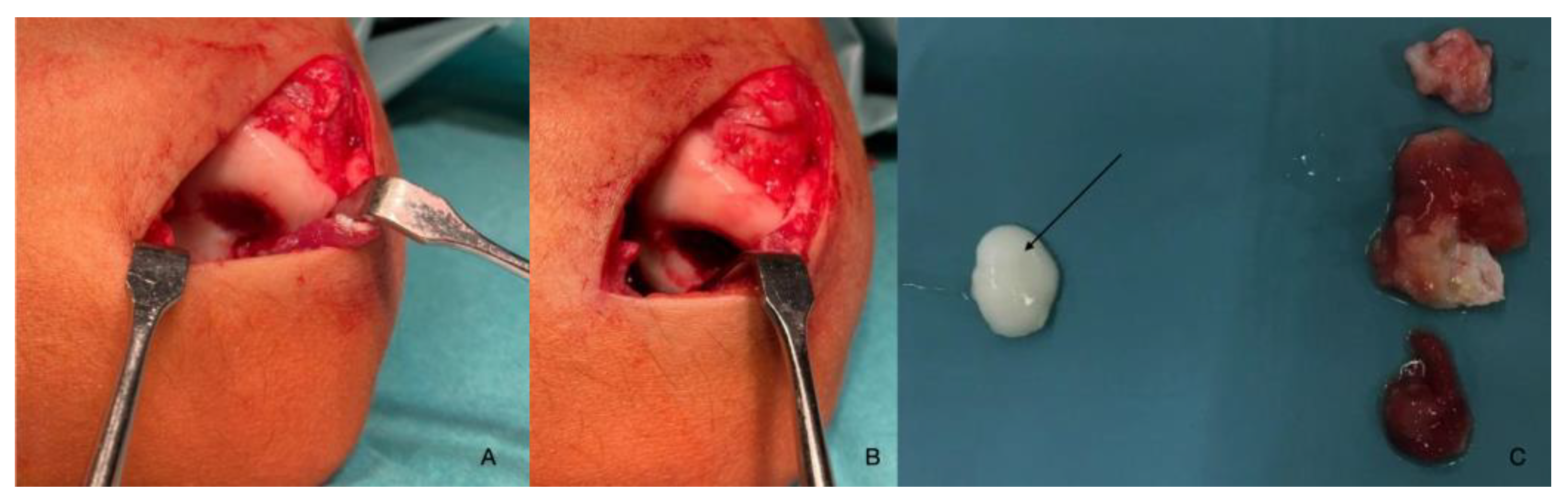
Figure 9.
Intraoperative images of the mosaicplasty from anteroradial (A) and posterior views (B).
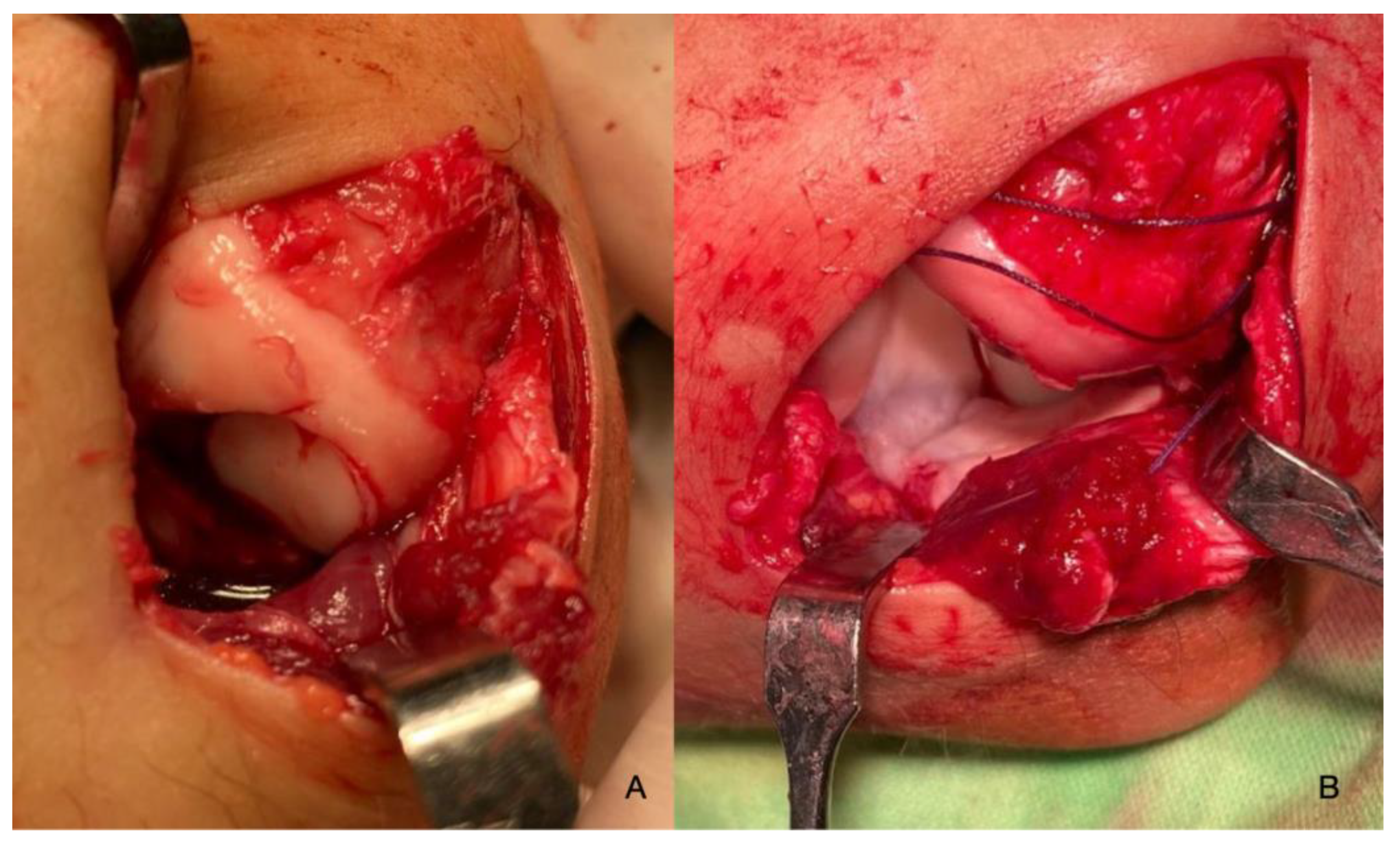
Figure 10.
Control X-rays immediately post-op (A and B). Control X-rays 8 weeks post-op (C and D).
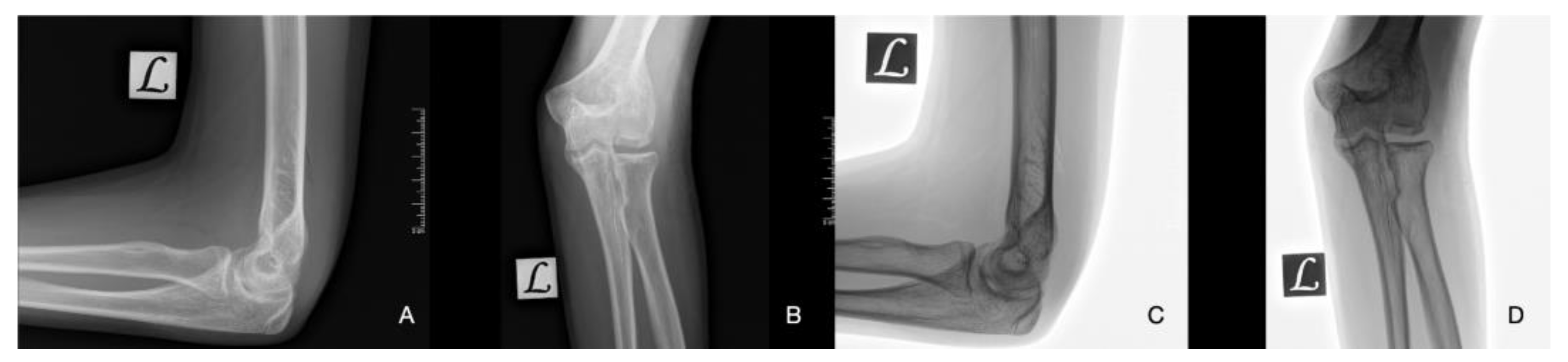
Figure 11.
Functional depiction of the elbow joint at 8 weeks (A/B/C/D-1) where elbow extension is somewhat limited early on and full ROM after one year (A/B/C/D-2).
Figure 11.
Functional depiction of the elbow joint at 8 weeks (A/B/C/D-1) where elbow extension is somewhat limited early on and full ROM after one year (A/B/C/D-2).

Figure 12.
Control MR images six months post-op. The graft can be seen incorporated into the articular surface (orange circles and arrow) on T1 (A and C) and T2 (B) weighted images.
Figure 12.
Control MR images six months post-op. The graft can be seen incorporated into the articular surface (orange circles and arrow) on T1 (A and C) and T2 (B) weighted images.
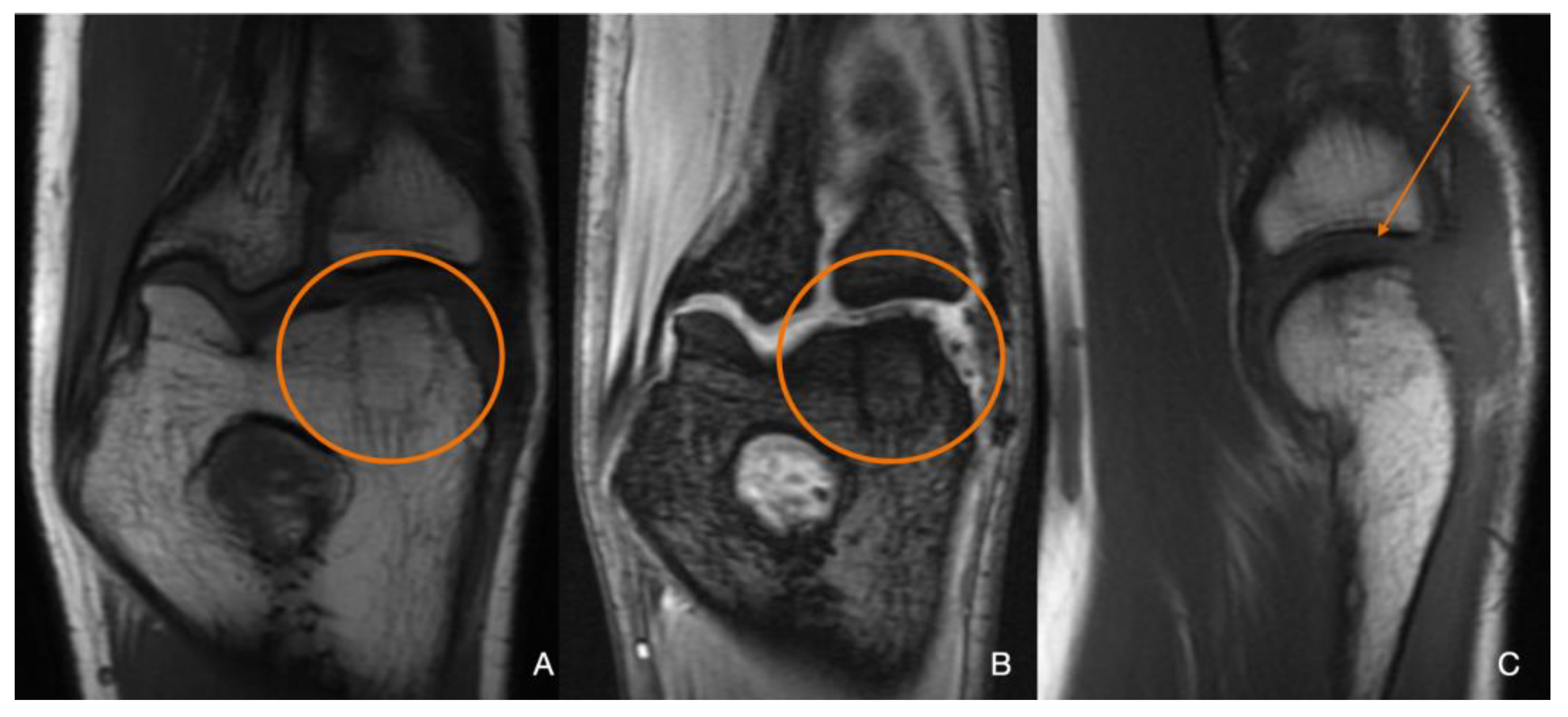

Table 1.
| Imaging: | X-Ray | Arthroscopy | MRI | |||
|---|---|---|---|---|---|---|
| Classification | Berndt and Harty [21] - 1959 | Guhl [22] - 1982 | ICRS by Brittberg and Winalsky [23]- 2003 | DiPaola [24] - 1991 | Hefti [4] - 1999 | Ellerman [15] - 2019 |
| Stage 1 | Small subchondral compression | Intact Lesion | A stable lesion of the softened area covered by intact cartilage. | Thickening of articular cartilage and low signal changes | Small change of signal, without clear fragment margins. | Epiphyseal cartilage lesion with necrotic center |
| Stage 2 | Partially detached osteochondral fragment | A lesion with signs of early separation | Lesions with partial discontinuity which are stable when probed | Articular cartilage has been breached with a low signal rim behind the fragment indicating fibrous attachment | OSteochondral fragment with clear margins, without fluid in between | Epiphyseal cartilage lesion with complete or incomplete rim calcification |
| Stage 3 | Completely detached, non-displaced | Partially detached lesion | Lesions with complete discontinuity which are not dislocated (Dead in situ) | High signal changes behind the fragment indicate synovial fluid between the fragment and the underlying subchondral bone | Fluid is visible partially between the fragment and bone | Partially or completely ossified lesion |
| Stage 4 | Completely detached and displaced - loose body | Craters with loose bodies (salvageable or non-salvageable) | Empty defect bed with loose or dislocated fragment | Loose body | Fluid surrounds the fragment but it is still in situ | A healed osseous lesion with scar |
| Stage 5 | Scranton and McDermott modification : Subchondral Cyst | - | - | - | The fragment is completely detached and displaced | Unhealed, detached osseous lesion (Sequestrum) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



