
Submitted:
28 July 2024
Posted:
30 July 2024
You are already at the latest version
Abstract
(1) Background: With the rising incidence of life expectancy, obesity, and tumours, understanding the incretory influence of adipose tissue in tumorigenesis becomes increasingly important. As the adipokines leptin and adiponectin are released by fat tissue, we aimed to analyse the expression of their respective receptors in tumours for which an association with obesity is epidemiologically hypothesized; (2) Methods: The expression of leptinR and adipoR1 were analysed in cohorts of renal cell cancer (n = 391), cervical cancer (n = 155), vulvar cancer (n = 107), and endometrial cancer (n = 90) by immunohistochemistry and correlated with clinicopathological parameters including survival times; (3) Results: Expression of leptinR was high in renal cell cancer (62.2% of cases), vulvar carcinoma (50%) and endometrial cancer (80.5% of tissue-samples). High expression was associated with favourable clinicopathological markers and longer overall survival times in renal cell cancer and vulvar cancer. AdipoR1 was only weakly expressed in all four tumor entities and did not show significant associations with clinicopathological parameters or prognosis; (4) Conclusion: High leptinR is a promising biomarker for favourable tumour outcome in renal cell carcinoma and vulvar carcinoma.
Keywords:
Adipokine receptors
; obesity related tumours
; leptinR
; adipoR1
1. Introduction
The rapid and widespread increase of obesity in the western world, starting from the 1980s onwards, marked the emergence of a global epidemic, which caused a rise of obesity-related diseases. In addition to cardiovascular disease, obesity has been linked to higher rates of certain cancers, including renal cell carcinoma, colorectal, oesophageal, endometrial and breast cancer [1,2]. In addition, recent data suggest an association with cervical and vulvar cancer, too [3]. That is because apart from being the main repository of energy in form of triglycerides in the human body, adipose tissue has been recognized to bear important endocrine, metabolic, and inflammatory regulatory functions. One of the factors responsible for the endocrine actions are adipokines, peptide hormones secreted by the adipose tissue into the bloodstream [4]. They provide information about satiety and energy status and influence many physiological processes like reproductive functions and immune response. Adipokines can functionally be divided into pro- and anti-inflammatory players. Expansion of adipose tissue induces a dominance of proinflammatory effects [5]. Adipokine dysregulation is often linked to metabolic disorders, i.e. cardiovascular diseases, and other health conditions. However, in recent years it has become clear that adipokines also play a critical role in cancer development and progression [6]. The first adipokine described in 1994 was leptin [7] that, together with its functional “counterplayer” adiponectin, regulates energy balance by influencing appetite, satiety, and energy expenditure [8,9]. Furthermore, in cancer patients a low adiponectin to leptin ratio has been implemented as an indicator of tumour aggressiveness [10].
In solid tissues, adipokines exert their effects in the target tissue via specific membrane-bound adipokine receptors that are most often ubiquitously expressed [11,12,13,14].
Adipokine binding activates a variety of pathways, such as mitogen-activated protein kinase, leading to cell growth, inflammation and angiogenesis in the case of leptin, and insulin secretion and fatty acid oxidation in the case of adiponectin. In cancer, leptin receptor activation has been associated with proliferation and invasion [15], while adipoR1 has been shown to be overexpressed in both cancer tissue and cancer-associated immune cells, thereby modulating the anti-tumour immune response [11].
For the purpose of this study, we chose to analyse the receptors of two well-characterised adipokines with opposing functions, leptinR and adipoR1, in order to understand their role as potential biomarkers in two types of cancer with an established relationship with obesity, as well as in two types of cancer with a probable relationship with obesity.
2. Materials and Methods
2.1. Patients
Four clinically well characterized tumour cohorts were included in this study (n=391 renal cell, n=155 cervical, n=107 vulvar and n=90 endometrial carcinomas). The patients underwent surgery and histopathological diagnosis at the University Hospital Bonn, Bonn, Germany, between 2002 and 2017. A total of 743 patients were included. For clinicopathological information on patient cohorts see Table S1.
2.2. Methods
2.2.1. Tissue Microarray
Tissue microarrays were constructed as described previously [17]. Core diameter was 1 mm, and every tumour was represented by 1-2 cores. In total 21 TMA plates were included (11 RCC, 4 cervical, 3 vulvar, and 3 endometrial cancer).
2.2.2. Immunohistochemistry
All slides were freshly cut and immunostained in one day. Antibodies used were rabbit monoclonal (GT1233), (GeneTex, Inc., North America, dilution 1:100) for leptinR; for adipoR1, rabbit monoclonal (MAB19531), (abnova, Taiwan, dilution 1:50) was used.
An automated staining system (BenchMark ULTRA; Ventana Medical Systems, Oro Valley, AZ, USA) was applied for deparaffinization, pretreatment with cell conditioning buffer (CC1 buffer, pH8), and primary antibody incubation. For signal detection, the UltraView DAB IHC Detection Kit (Ventana, Ventana Medical Systems, Oro Valley, AZ, USA) was used. The slides were counterstained, dehydrated and coverslipped. Positive controls were performed for each staining (skeletal muscle and liver tissue).
2.2.3. Evaluation of Immunohistochemistry
The slides were scanned with Slide Scanner Panoramic midi (3DHistech, Budapest, Hungary) and read with the open source software for digital pathology image analysis quPath (version 0.5.0) [20]. Staining intensity was scored semiquantitatively. A four-tier scoring system was applied to categorize staining intensities (0: no staining, 1: weak staining, 2: moderate staining, 3: strong staining). If spots from the same patient differed in intensity, the maximum value was used for further analyses.
2.2.4. TCGA PanCancer mRNA Data
An in-silico analysis of leptinR and adipoR1 mRNA expression level from a publicly available database [The Cancer Genome Atlas (TCGA), version: PanCancer available on cBioPortal] was used to complement the immunohistochemistry data. The mRNA expression z-scores relative to all samples were dichotomized by the median. The endpoint used for survival analysis was overall survival [21,22]. The results are based upon data generated by the TCGA Research Network: https://www.cancer.gov/tcga. TCGA PanCancer datasets used were Clear Cell RCC, Cervical Cancer and Endometrial Cancer [23]. No dataset of sufficient size was available for vulvar cancer.
2.2.5. Statistics
Statistical analysis was performed using R (version 4.3.2 The R Foundation for Statistical Computing) and RStudio (version 2023.12.0+369). Patients were dichotomized by the median expression of leptinR and adipoR1. For group comparisons, crossfield-tables, Mann-Whitney-U test, Spearman correlation, and Binomial test were used. Estimated hazard ratios (HR) with 95% confidence intervals were based on univariable Cox regression analyses. Survival analysis was performed using Kaplan-Meier plots, as well as uni- and multivariable Cox regression analysis, and the log-rank test. p-values < 0.05 were considered significant, and p-values between 0.05 and 0.1 were considered indicative of a statistical trend. The Bonferroni correction was applied to correct for multiple testing.
3. Results
3.1. TMA Staining Evaluation
Of 1580 TMA spots on 21 slides, 1303 could be analyzed. This included 801 of 943 spots for the renal cell cancer cohort, 245 of 316 spots for the cervical cancer cohort, 102 of 129 spots for the vulva cancer cohort, and 155 of 192 spots for the endometrial cancer cohort. Control tissue was present on all TMA slides.
3.1.1. Staining Patterns leptinR
LeptinR immunoreactivity was detected in the cytoplasm and membrane of tumour cells, no nuclear staining was noted. Connective tissue cells and lymphocytes were consistently negative. Endothelial and plasma cells were weakly positive. Immunohistochemistry evaluation scheme is depicted in Figure 1.
3.1.2. Staining Patterns adipoR1
AdipoR1 immunoreactivity was detected in the cytoplasm of tumour cells, no nuclear staining was noted. Lymphocytes were consistently negative. Endothelial cells and fibroblasts were weakly positive. Immunohistochemistry evaluation scheme is depicted in Figure 1. Additional images of immunohistochemistry of the other tumour cohorts are given Figure S1.
3.3. Receptor Expression
3.3.1. LeptinR
In RCC 68 cases were negative (17.6%), 78 showed weak staining (20.2%), moderate immunoreactivity was seen in 118 cases (30.6%) and 122 stained strongly (31.6%).
For cervical carcinoma 46 cases were negative (30.7%), 36 showed weak staining (24%), moderate immunoreactivity was seen in 37 cases (24.6%) and 31 stained strongly (20.7%).
In vulvar carcinoma 21 cases were negative (21%), 29 showed weak staining (29%), moderate immunoreactivity was seen in 23 cases (23%) and 27 stained strongly (27%).
In endometrial cancer 2 cases were negative (2.3%), 15 showed weak staining (17.2%), moderate immunoreactivity was seen in 25 cases (28.7%) and 45 stained strongly (51.7%).
For statistics, leptinR staining was dichotomized by the median into low vs. high expression.
3.3.2. AdipoR1
In RCC 124 cases were negative (32.7%), 119 showed weak staining (31.4%), moderate immunoreactivity was seen in 94 cases (24.8%) and 42 stained strongly (11.1%).
In cervical carcinoma 36 cases were negative (24.8%), 52 showed weak staining (35.9%), moderate immunoreactivity was seen in 42 cases (28.9%) and 15 stained strongly (10.4%).
In vulvar carcinoma 28 cases were negative (30.8%), 27 showed weak staining (29.7%), moderate immunoreactivity was seen in 33 cases (36.2%) and 3 stained strongly (3.3%).
In endometrial cancer 18 cases were negative (20.7%), 22 showed weak staining (25.3%), moderate immunoreactivity was seen in 29 cases (33.3%) and 18 stained strongly (20.7%).
Similar to LeptinR, AdipoR1 expression was divided into low and high expression based on the median.
3.4. Associations and Correlations with Clinicopathological Parameters
3.4.1. LeptinR
RCC:
High leptinR expression in RCC was significantly associated with low pathologic stage (66.9%, p < 0.01) and histological subtype (clear cell (57%) and papillary (86.7%), p < 0.01), with a trend toward association with negative lymph nodes (67.4%). No significant association was found for tumour grade, BMI, age, and sex. The association with tumour stage and subtype in RCC was confirmed in Spearman rank correlation analysis. The subtypes that showed a significant high leptinR expression were clear cell RCC (Binomial test p < 0.001) and papillary RCC (p < 0.001) (Tables S2 and S4).
Cervical carcinoma:
In cervical cancer, high leptinR expression was associated significantly with low FIGO stage (59.4%, p < 0.01) and negative lymph nodes (68.8%, p < 0.01). There was a trend towards an association with higher grades (57.4%, p = 0.03) and younger age (<60 years = 50.5%, p = 0.03). It was not significantly associated with BMI and HPV status. Correlation analysis confirmed this: FIGO: CC -0.283, p < 0.001; Lymph node involvement: CC -0.375, p < 0.001 (Tables S2 and S4).
Vulvar carcinoma:
In vulvar cancer high leptinR expression was associated significantly with negative HPV status (57.4%, p < 0.01), but not with pathologic stage, lymph node involvement, grade, BMI or age (Tables S2 and S4).
Endometrial carcinoma:
In endometrial cancer high leptinR expression was associated significantly with lower grades (87.9%, p = 0.002), but not with pathologic stage, lymph node involvement, BMI or age. Correlation analysis confirmed this: Grade: CC -0.332, p = 0.002 (Tables S2 and S4).
3.4.2. AdipoR1RCC:
AdipoR1 expression in RCC was associated with subtype (low expression with clear cell (71.8%) and high expression with papillary (62.7%), p < 0.01), with a trend toward association between high receptor expression and low pathologic stage (39%, p = 0.06). The association with subtype in RCC was confirmed in Spearman rank correlation analysis: Subtype: CC 0.272, p < 0.001. A significant reduction of adipoR1 expression was found in ccRCC (p < 0.001) and a trend in high expression in papillary RCC (p = 0.067). There was no significant association with lymph node involvement, grade, BMI age, or sex (Tables S3 and S4).
Cervical carcinoma:
In cervical cancer, high AdipoR1 expression was significantly associated with low FIGO stage (47.8%, p = 0.02) and higher grades (65.4%, p < 0.01). It was not associated with lymph node involvement, BMI, age, or HPV infection. In correlation analysis, FIGO stage remained a significant parameter: CC -0.201, p = 0.015 (Tables S3 and S4).
Vulvar carcinoma:
Regarding vulvar, the receptor showed no significant association with pathologic stage, lymph node involvement, grade, BMI, age, or HPV status (Tables S3 and S4).
Endometrial carcinoma:
High adipoR1 expression was associated with positive lymph nodes (75%, p = 0.04). Correlation analysis confirmed these results: lymph node involvement: CC 0.296, p = 0.039. The receptor was not associated significantly with pathologic stage, grade, BMI, or age (Tables S3 and S4).
3.5. Survival Analysis of Immunohistochemical Data
3.5.1. LeptinR
Tumours with high leptinR expression showed a significantly longer overall survival in Kaplan-Meier analyses in RCC, cervical and vulvar cancer (RCC: p = 0.004; cervical: p = 0.034 and vulvar: p = 0.029; Figure 2). This was confirmed in multivariable Cox analyses for RCC (p = 0.03, HR = 0.62) and vulvar cancer (p = 0.01, HR = 0.37) but not cervical and endometrial cancer (Table 1). See Table S5 for univariable Cox analyses.
3.5.2. AdipoR1
3.6. Prognostic Value of Receptor mRNA Expression Using TCGA Databases
3.6.1. LeptinR
High expression of LeptinR mRNA was associated with longer overall survival in ccRCC (p = 0.005). Contrarily, for cervical cancer high expression of leptinR mRNA was associated with shorter OS (p = 0.008). The mRNA expression level in endometrial cancer had no significant prognostic value. Kaplan-Meier curves are given in Figure 3.
3.6.2. AdipoR1
AdipoR1 mRNA expression had no prognostic value in any of the three tumour entities. Kaplan-Meier curves are given in Figure 3.
4. Discussion
In recent years, the global surge in obesity rates has emerged as a critical public health concern, transcending mere cosmetic implications [24]. Beyond its well-established association with cardiovascular diseases and metabolic disorders, obesity has been identified as a significant risk factor for the development of various types of cancer, including renal cell carcinoma [25,26] (RCC), cervical cancer [27], vulvar cancer [28], and endometrial cancer [29,30]. The intricate interplay between adipose tissue, metabolic dysregulation, and chronic inflammation creates a microenvironment conducive to tumorigenesis that is, at least in part, influenced by adipokines [31].
Adipokines, furthermore, play a crucial role in signalling of hunger and satiety. Differential expression of adipokines thereby have been linked to obesity and obesity related diseases. The by far best studied adipokine is leptin. Leptin serum levels are higher in obese individuals and have been associated with adverse outcomes in tumour patients meanwhile adiponectin acts in an opposite fashion [32,33]. In the present study, the expression of the adipokine receptors leptinR and adipoR1 was examined in detail in four tumour entities, that have been epidemiologically linked to obesity. We had hypothesized to find a differential expression of these receptors in these tumours in correspondence to the BMI. Data on leptin serum levels were not available for our patients, but as patients with a higher BMI, namely > 30, show statistically higher levels of leptin, we used the BMI as a surrogate parameter. However, in none of the cohorts analysed, BMI and receptor expression did not show any significant association neither for leptinR, nor for adipoR1. Further studies with more detailed serum data of the respective adipokines are warranted to detect more subtle associations.
Regarding our cohorts in detail, high expression of leptinR was associated with longer overall survival both for RCC as well as vulvar carcinoma. In addition, analysis of publicly available mRNA data supported the finding of leptinR presence being associated with longer survival in ccRCC. Our findings, supported by two large cohorts (Bonn cohort, TCGA) and different methodologies are different from previous analyses, that did not identify this prognostic value. In 2006, Horiguchi et al. found no prognostic value of leptinR expression in RCC. Possibly, the small size of their cohort (n=57) precluded a meaningful survival analysis [34]. Nevertheless, a significant association with clinicopathological parameters such as histologic type was found, which is in line with our data, showing a significant correlation between high leptinR expression and clear cell and papillary RCC. Perumal et al. analysed a similarly sized cohort and also found no association of leptinR expression with survival in ccRCC [35]. Although ccRCC has so far been best linked to be causally associated with obesity we found equally high leptinR in papillary RCC [36]. However, the impact of obesity on tumour initiation and progression depends on cofactors and differs between sexes and histologic subtypes of tumours, e.g. the strongest association with obesity was seen in clear cell RCC (ccRCC) [26,37].
Endometrial cancer was one of the first tumours for which an association between obesity and tumour development became evident. Increasing BMI is associated with increased incidence and negative oncologic outcomes [30]. Adipose tissue also synthesizes oestrogen and is the major source of oestrogen in postmenopausal women. Thus it is not surprising, that elevated oestrogen serum levels in obese women have been associated with the development of endometrial cancer [29]. Zhang et al. showed that higher levels of both leptin and leptinR are associated with high BMI, invasion, metastasis, and poor prognosis [38]. Conversely, leptinR expression was also significantly higher when tumour grades were low [38]. Those somewhat contradictory results may, partly, be explained by the small size of the study cohort. Another study with a similarly sized cohort found leptinR overexpression to be correlated with higher grades, and elevated serum leptin levels with BMI and higher grades [39]. In the present cohort, we could not confirm an association between leptinR in tumour tissue and BMI or show a prognostic impact but found that higher leptinR expression was correlated significantly with lower tumour grades. LeptinR mRNA expression in TCGA data did not show a significant impact on survival. As the majority of patients included in the study were > 60 years old (62%, mean 63, SD 12 years), and age and receptor expression were not associated, a possible confounder of endogenous ovarian oestrogen synthesis can be rejected [29]. In addition, the effect of adipokines and steroids hormones does not appear to be mutually exclusive, as presence of progesterone was found to suppress leptinR mRNA expression, an interaction that may be subject to subsequent research activity [40]. Clearly, larger studies are necessary to resolve these discrepancies.
Recently, obesity was suggested to have a negative prognostic impact in vulvar carcinoma [28]. High BMI and metabolic syndrome were found to increase the risk of tumour development [41]. To the best of our knowledge, this study is the first to show a significantly longer survival of patients with vulvar carcinoma with high leptinR expression. This is in line with the data obtained in RCC where high leptinR expression was significantly associated with longer overall survival, too. Unfortunately, it was not possible to prove the results obtained by immunohistochemistry in an independent cohort, as TCGA data did not provide sufficient information on vulvar carcinoma.
In squamous cell carcinomas of the gynaecologic tract, the influence of circulating oestrogen as well as obesity-related hormones and chemokines remains controversial as the impact of human papillomavirus infection is considered to be the most important causative agent. Out of these tumours, the most common is cervical cancer [42]. Although not statistically significant, high leptinR expression showed a strong trend toward a favourable overall survival in patients with cervical squamous cell carcinoma. Additionally, there was a strong and statistically significant association with favourable clinicopathological parameters such as low FIGO stage and absence of lymph node metastasis. Yuan et al. found worse differentiation and disease progression when leptin expression was high, so that one might hypothesize that an inverse relationship between leptin and leptinR exists [43]. However, further research is needed to understand the differential regulation processes. To our knowledge, this is the first study to investigate the relevance of the leptinR in cervical squamous cell carcinoma.
Most cervical cancers, as well as a significant proportion of vulvar cancers are, at least in part, driven by high-risk human papillomavirus (HPV). Given the small number of HPV-negative cervical cancers in our cohort, any conclusions about HPV and leptinR correlations appear speculative. However, as with vulvar carcinoma, HPV-dependent tumours showed significantly lower expression of leptinR, raising the possibility of an interaction. Contrarily to immunohistochemical results, high leptinR mRNA expression in cervical cancer was associated with shorter overall survival. These contradicting results might show that leptinR expression and its regulation on mRNA and proteomic levels act different in this tumour entity or are influenced by other causative agents such as HPV infection. To clarify these opposing associations further investigations are needed.
For adipoR1, no prognostic value could be demonstrated in any of the analysed tumour entities neither immunohistochemically nor on mRNA level in TCGA data. Consistent with previous findings, we confirmed a continuous increase in adipoR1 expression with increasing BMI in all our gynaecologic cancer cohorts. In obese patients adipoR1 expression is reduced in adipose tissue and increased after weight loss. Thereby obese subjects aggravate negative metabolic effects of low serum level adiponectin [44]. In RCC, adipoR1 expression was different depending on subtype with high levels in papillary RCC and low levels in ccRCC. Previously, it was found that patients with ccRCC had lower adiponectin serum levels, and hence the hormone level could be helpful to differentiate ccRCC from non-ccRCC in a non-invasive manner [45]. Moreover, other factors such as insulin-like growth factor or fibroblast growth factor have different secretion rates in different RCC subtypes, so one could argue that differential receptor expression is plausible [45]. In keeping with published data, adipoR1 expression was reduced in ccRCC [46]. Additionally, Kleinmann et al. demonstrated an underactivation of the entire adiponectin hormonal axis in ccRCC [46]. In 2008 Pinthus et al. showed that lower adiponectin levels were associated with tumour aggressiveness [47]. However, the literature is contradictory: Ito et al. postulated high levels of adiponectin were associated with tumour aggressiveness [48]. Regarding this discrepancy, multiple factors were suggested which might affect circulating adiponectin levels, like diabetes, racial background and diurnal variation [49,50]. Secondly, it was pointed out that adipoR1 was not associated with survival which is consistent with our findings [48]. An association between low serum adiponectin levels and the development of RCC and endometrial cancer has also been described [51,52].
Significant correlation of adipoR1 expression with lower FIGO stage but higher grades was found in cervical cancer. To the best of our knowledge, this study is the first to investigate adipoR1 expression in a large cervical cancer cohort. Previous in vitro studies using HeLa cells showed that cells express adipoR1 and that adiponectin can induce apoptosis [53]. Other tumours associated with obesity such as renal and colorectal cancer more frequently express adipoR1 than cervical squamous cell carcinoma, in which the role of obesity remains unclear [54]. Possible factors that determine this uncertain role are reliability and noncompliance of screening test in obese patients [55]. A pan-cancer analysis of a publicly available dataset identified adipoR1 upregulation as a risk factor for shorter disease-free survival in cervical cancer [11]. One might hypothesize that lower levels of adiponectin, which acts as an oncoprotective hormone, could lead to higher expression of adipoR1. However, in the context of our results, we could not confirm an effect of adipoR1 expression on overall survival. Possible confounding factors in tumorigenesis and progression, such as HPV infection as mentioned above and decreased screening compliance with increasing body weight, need to be kept in mind [55].
In both vulvar and endometrial cancers, none of the clinicopathological parameters examined nor the overall survival was significantly associated with the intensity of adipoR1 expression. In prior studies, a high BMI could be associated with shorter disease-free survival in vulvar cancer, suggesting an association with obesity [28].
There is evidence that adiponectin is a potent inhibitor of cell growth in endometrial cancer [56]. AdipoR1 expression is found in non-neoplastic as well as tumour tissues [56]. In addition, Yamauchi et al. demonstrated a strong association between decreased adipoR1/adipoR2 expression and tumour progression in terms of higher grading, growth, invasion, and metastasis [57]. Somewhat contradictorily, we found an increase in adipoR1 expression for both tumour stage and lymph node metastasis as well as shorter survival, although most of our findings did not reach statistical significance.
Strengths of this study are the analysis of multiple tumour types and the careful in-depth statistical evaluation of the protein expression data including patient survival. Weaknesses are the descriptive nature of this analysis and the lack of serum adipokine data.
5. Conclusions
The role of adipokine receptor expression in cancer development and progression has only rarely been investigated. Consistent with leptinR being seen as a protective factor, high expression was associated with favourable clinicopathological parameters namely tumour stage, tumour grade, and absence of lymph node metastasis. Thus, high leptinR expression is a promising biomarker indicating favourable tumour outcome in obesity-related tumours. AdipoR1 did not show significant association with clinicopathological parameters.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Additional information on patient cohorts; Table S2. Associations between clinicopathological parameters and leptinR in RCC, cervical, vulvar, and endometrial carcinoma, Table S3. Associations between clinicopathological parameters and adipoR1 in RCC, cervical, vulvar, and endometrial carcinoma, Table S4. Spearman correlation of receptors with clinicopathological parameters, Table S5. Results of univariable Cox regression survival analysis, Figure S1. Cervical, vulvar and endometrial cancer: Immunohistochemistry evaluation scheme. Magnification: 20x.
Author Contributions
Conceptualization, G.K. and I.B.; methodology, G.K. and I.B.; software, I.B.; validation, G.K., M.B., and I.B.; formal analysis, I.B. and M.B.; investigation, I.B., F.W. and T.T.; resources, G.K., A.T., M.R., A.M., F.W., and T.T.; data curation, F.W., T.T., M.B., and I.B.; writing—original draft preparation, I.B.; writing—review and editing, G.K., M.B., and I.B.; visualization, G.K., M.B., and I.B.; supervision, G.K.; project administration, G.K., M.B., and I.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of the University Bonn (#233/20, #208/21, #228/15, and #233/20).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data may be obtained upon request.
Acknowledgments
The authors thank Susanne Steiner, Carsten Golletz and Kerstin Fuchs (Institute of Pathology, University Hospital Bonn) for their excellent technical assistance.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Aravani, A.; Downing, A.; Thomas, J.D.; Lagergren, J.; Morris, E.J.A.; Hull, M.A. Obesity surgery and risk of colorectal and other obesity-related cancers: An English population-based cohort study. Cancer Epidemiol. 2018, 53, 99–104. [CrossRef]
- Song, M.; Giovannucci, E. Estimating the Influence of Obesity on Cancer Risk: Stratification by Smoking Is Critical. J. Clin. Oncol. 2016, 34, 3237–3239. [CrossRef]
- Da Lee, Y.; Lee, T.S. Associations between metabolic syndrome and gynecologic cancer. Obstet. Gynecol. Sci. 2020, 63, 215–224. [CrossRef]
- Fasshauer, M.; Blüher, M. Adipokines in health and disease. Trends Pharmacol. Sci. 2015, 36, 461–470. [CrossRef]
- Mancuso, P. The role of adipokines in chronic inflammation. Immunotargets Ther. 2016, 5, 47–56. [CrossRef]
- Pergola, G. de; Silvestris, F. Obesity as a major risk factor for cancer. J. Obes. 2013, 2013, 291546. [CrossRef]
- Zhang, Y.; Proenca, R.; Maffei, M.; Barone, M.; Leopold, L.; Friedman, J.M. Positional cloning of the mouse obese gene and its human homologue. Nature 1994, 372, 425–432. [CrossRef]
- Kazeminasab, F.; Behzadnejad, N.; Cerqueira, H.S.; Santos, H.O.; Rosenkranz, S.K. Effects of intermittent fasting combined with exercise on serum leptin and adiponectin in adults with or without obesity: a systematic review and meta-analysis of randomized clinical trials. Front. Nutr. 2024, 11, 1362731. [CrossRef]
- Katsiki, N.; Mantzoros, C.; Mikhailidis, D.P. Adiponectin, lipids and atherosclerosis. Curr. Opin. Lipidol. 2017, 28, 347–354. [CrossRef]
- Grossmann, M.E.; Cleary, M.P. The balance between leptin and adiponectin in the control of carcinogenesis - focus on mammary tumorigenesis. Biochimie 2012, 94, 2164–2171. [CrossRef]
- Chen, Z.; Yang, H.; Ren, Y.; Yang, Z.; Huang, J.; Li, C.; Xiong, Y.; Yu, B. Distinct roles of ADIPOR1 and ADIPOR2: A pan-cancer analysis. Front. Endocrinol. (Lausanne) 2023, 14, 1119534. [CrossRef]
- Booth, A.; Magnuson, A.; Fouts, J.; Foster, M. Adipose tissue, obesity and adipokines: role in cancer promotion. Horm. Mol. Biol. Clin. Investig. 2015, 21, 57–74. [CrossRef]
- Yamauchi, T.; Kamon, J.; Ito, Y.; Tsuchida, A.; Yokomizo, T.; Kita, S.; Sugiyama, T.; Miyagishi, M.; Hara, K.; Tsunoda, M.; et al. Cloning of adiponectin receptors that mediate antidiabetic metabolic effects. Nature 2003, 423, 762–769. [CrossRef]
- Achari, A.E.; Jain, S.K. Adiponectin, a Therapeutic Target for Obesity, Diabetes, and Endothelial Dysfunction. Int. J. Mol. Sci. 2017, 18. [CrossRef]
- Dana, N.; Ferns, G.A.; Nedaeinia, R.; Haghjooy Javanmard, S. Leptin signaling in breast cancer and its crosstalk with peroxisome proliferator-activated receptors α and γ. Clin. Transl. Oncol. 2023, 25, 601–610. [CrossRef]
- Sanders, C.; Hamad, A.S.M.; Ng, S.; Hosni, R.; Ellinger, J.; Klümper, N.; Ritter, M.; Stephan, C.; Jung, K.; Hölzel, M.; et al. CD103+ Tissue Resident T-Lymphocytes Accumulate in Lung Metastases and Are Correlated with Poor Prognosis in ccRCC. Cancers (Basel) 2022, 14, 1541. [CrossRef]
- Condic, M.; Ralser, D.J.; Klümper, N.; Ellinger, J.; Qureischi, M.; Egger, E.K.; Kristiansen, G.; Mustea, A.; Thiesler, T. Comprehensive Analysis of N6-Methyladenosine (m6A) Writers, Erasers, and Readers in Cervical Cancer. Int. J. Mol. Sci. 2022, 23, 7165. [CrossRef]
- Hecking, T.; Thiesler, T.; Schiller, C.; Lunkenheimer, J.-M.; Ayub, T.H.; Rohr, A.; Condic, M.; Keyver-Paik, M.-D.; Fimmers, R.; Kirfel, J.; et al. Tumoral PD-L1 expression defines a subgroup of poor-prognosis vulvar carcinomas with non-viral etiology. Oncotarget 2017, 8, 92890–92903. [CrossRef]
- Hecking, T.; Thiesler, T.; Halbe, J.; Otten, L.; Recker, F.; Gevensleben, H.; Müller, T.; Schiller, C.; Egger, E.K.; Fimmers, R.; et al. Programmed Cell Death Ligand-1 (PDL-1) Correlates With Tumor Infiltration by Immune Cells and Represents a Promising Target for Immunotherapy in Endometrial Cancer. Anticancer Res. 2022, 42, 1367–1376. [CrossRef]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open source software for digital pathology image analysis. Sci. Rep. 2017, 7, 16878. [CrossRef]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The cBio cancer genomics portal: an open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012, 2, 401–404. [CrossRef]
- Gao, J.; Aksoy, B.A.; Dogrusoz, U.; Dresdner, G.; Gross, B.; Sumer, S.O.; Sun, Y.; Jacobsen, A.; Sinha, R.; Larsson, E.; et al. Integrative analysis of complex cancer genomics and clinical profiles using the cBioPortal. Sci. Signal. 2013, 6, pl1. [CrossRef]
- Hoadley, K.A.; Yau, C.; Hinoue, T.; Wolf, D.M.; Lazar, A.J.; Drill, E.; Shen, R.; Taylor, A.M.; Cherniack, A.D.; Thorsson, V.; et al. Cell-of-Origin Patterns Dominate the Molecular Classification of 10,000 Tumors from 33 Types of Cancer. Cell 2018, 173, 291-304.e6. [CrossRef]
- Pi-Sunyer, X. The medical risks of obesity. Postgrad. Med. 2009, 121, 21–33. [CrossRef]
- Lindblad, P.; Wolk, A.; Bergström, R.; Persson, I.; Adami, H.O. The role of obesity and weight fluctuations in the etiology of renal cell cancer: a population-based case-control study. Cancer Epidemiol. Biomarkers Prev. 1994, 3, 631–639.
- Venkatesh, N.; Martini, A.; McQuade, J.L.; Msaouel, P.; Hahn, A.W. Obesity and renal cell carcinoma: Biological mechanisms and perspectives. Semin. Cancer Biol. 2023, 94, 21–33. [CrossRef]
- Urbute, A.; Frederiksen, K.; Thomsen, L.T.; Kesmodel, U.S.; Kjaer, S.K. Overweight and obesity as risk factors for cervical cancer and detection of precancers among screened women: A nationwide, population-based cohort study. Gynecol. Oncol. 2024, 181, 20–27. [CrossRef]
- Klapdor, R.; Hillemanns, P.; Woelber, L.L.; Jueckstock, J.K.; Hilpert, F.; Gregorio, N. de; Hasenburg, A.; Sehouli, J.; Ignatov, A.; Fuerst, S.; et al. The influence of obesity on tumor recurrence in vulvar cancer patients. JCO 2019, 37, e17130-e17130. [CrossRef]
- Lindemann, K.; Vatten, L.J.; Ellstrøm-Engh, M.; Eskild, A. Body mass, diabetes and smoking, and endometrial cancer risk: a follow-up study. Br. J. Cancer 2008, 98, 1582–1585. [CrossRef]
- Kölbl, H.; Bartl, T. Obesity in Gynecologic Oncology. Geburtshilfe Frauenheilkd. 2020, 80, 1205–1211. [CrossRef]
- Park, J.; Morley, T.S.; Kim, M.; Clegg, D.J.; Scherer, P.E. Obesity and cancer--mechanisms underlying tumour progression and recurrence. Nat. Rev. Endocrinol. 2014, 10, 455–465. [CrossRef]
- Considine, R.V.; Sinha, M.K.; Heiman, M.L.; Kriauciunas, A.; Stephens, T.W.; Nyce, M.R.; Ohannesian, J.P.; Marco, C.C.; McKee, L.J.; Bauer, T.L. Serum immunoreactive-leptin concentrations in normal-weight and obese humans. N. Engl. J. Med. 1996, 334, 292–295. [CrossRef]
- Fan, W.-L.; Yeh, Y.-M.; Liu, T.-T.; Lin, W.-M.; Yang, T.-Y.; Lee, C.-W.; Lin, T.-C. Leptin Is Associated with Poor Clinical Outcomes and Promotes Clear Cell Renal Cell Carcinoma Progression. Biomolecules 2021, 11. [CrossRef]
- Horiguchi, A.; Sumitomo, M.; Asakuma, J.; Asano, T.; Zheng, R.; Asano, T.; Nanus, D.M.; Hayakawa, M. Increased serum leptin levels and over expression of leptin receptors are associated with the invasion and progression of renal cell carcinoma. J. Urol. 2006, 176, 1631–1635. [CrossRef]
- Perumal, K.; Mun, K.S.; Yap, N.Y.; Razack, A.H.A.; Gobe, G.C.; Ong, T.A.; Kuppusamy, S.; Rajandram, R. A Study on the Immunohistochemical Expressions of Leptin and Leptin Receptor in Clear Cell Renal Cell Carcinoma. Biomed Res. Int. 2020, 2020, 3682086. [CrossRef]
- Lowrance, W.T.; Thompson, R.H.; Yee, D.S.; Kaag, M.; Donat, S.M.; Russo, P. Obesity is associated with a higher risk of clear-cell renal cell carcinoma than with other histologies. BJU Int. 2010, 105, 16–20. [CrossRef]
- Callahan, C.L.; Hofmann, J.N.; Corley, D.A.; Zhao, W.K.; Shuch, B.; Chow, W.-H.; Purdue, M.P. Obesity and renal cell carcinoma risk by histologic subtype: A nested case-control study and meta-analysis. Cancer Epidemiol. 2018, 56, 31–37. [CrossRef]
- Zhang, Y.; Liu, L.; Li, C.; Ai, H. Correlation analysis between the expressions of leptin and its receptor (ObR) and clinicopathology in endometrial cancer. Cancer Biomark. 2014, 14, 353–359. [CrossRef]
- Boroń, D.; Nowakowski, R.; Grabarek, B.O.; Zmarzły, N.; Opławski, M. Expression Pattern of Leptin and Its Receptors in Endometrioid Endometrial Cancer. J. Clin. Med. 2021, 10. [CrossRef]
- Koshiba, H.; Kitawaki, J.; Ishihara, H.; Kado, N.; Kusuki, I.; Tsukamoto, K.; Honjo, H. Progesterone inhibition of functional leptin receptor mRNA expression in human endometrium. Mol. Hum. Reprod. 2001, 7, 567–572. [CrossRef]
- Nagel, G.; Concin, H.; Bjørge, T.; Rapp, K.; Manjer, J.; Hallmans, G.; Diem, G.; Häggström, C.; Engeland, A.; Almquist, M.; et al. Metabolic syndrome and rare gynecological cancers in the metabolic syndrome and cancer project (Me-Can). Ann. Oncol. 2011, 22, 1339–1345. [CrossRef]
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [CrossRef]
- Yuan, Y.; Zhang, J.; Cai, L.; Ding, C.; Wang, X.; Chen, H.; Wang, X.; Yan, J.; Lu, J. Leptin induces cell proliferation and reduces cell apoptosis by activating c-myc in cervical cancer. Oncol. Rep. 2013, 29, 2291–2296. [CrossRef]
- Rasmussen, M.S.; Lihn, A.S.; Pedersen, S.B.; Bruun, J.M.; Rasmussen, M.; Richelsen, B. Adiponectin receptors in human adipose tissue: effects of obesity, weight loss, and fat depots. Obesity (Silver Spring) 2006, 14, 28–35. [CrossRef]
- Wang, H.; Wu, J.; Gu, W.; Wang, B.; Wan, F.; Dai, B.; Zhang, H.; Shi, G.; Shen, Y.; Zhu, Y.; et al. Serum Adiponectin Level May be an Independent Predictor of Clear Cell Renal Cell Carcinoma. J. Cancer 2016, 7, 1340–1346. [CrossRef]
- Kleinmann, N.; Duivenvoorden, W.C.M.; Hopmans, S.N.; Beatty, L.K.; Qiao, S.; Gallino, D.; Lhotak, S.; Daya, D.; Paschos, A.; Austin, R.C.; et al. Underactivation of the adiponectin-adiponectin receptor 1 axis in clear cell renal cell carcinoma: implications for progression. Clin. Exp. Metastasis 2014, 31, 169–183. [CrossRef]
- Pinthus, J.H.; Kleinmann, N.; Tisdale, B.; Chatterjee, S.; Lu, J.-P.; Gillis, A.; Hamlet, T.; Singh, G.; Farrokhyar, F.; Kapoor, A. Lower plasma adiponectin levels are associated with larger tumor size and metastasis in clear-cell carcinoma of the kidney. Eur. Urol. 2008, 54, 866–873. [CrossRef]
- Ito, R.; Narita, S.; Huang, M.; Nara, T.; Numakura, K.; Takayama, K.; Tsuruta, H.; Maeno, A.; Saito, M.; Inoue, T.; et al. The impact of obesity and adiponectin signaling in patients with renal cell carcinoma: A potential mechanism for the "obesity paradox". PLoS One 2017, 12, e0171615. [CrossRef]
- Gandhi, R.; Sharma, A.; Kapoor, M.; Sundararajan, K.; Perruccio, A.V. Racial Differences in Serum Adipokine and Insulin Levels in a Matched Osteoarthritis Sample: A Pilot Study. J. Obes. 2016, 2016, 8746268. [CrossRef]
- Gavrila, A.; Peng, C.-K.; Chan, J.L.; Mietus, J.E.; Goldberger, A.L.; Mantzoros, C.S. Diurnal and ultradian dynamics of serum adiponectin in healthy men: comparison with leptin, circulating soluble leptin receptor, and cortisol patterns. J. Clin. Endocrinol. Metab. 2003, 88, 2838–2843. [CrossRef]
- Spyridopoulos, T.N.; Petridou, E.T.; Skalkidou, A.; Dessypris, N.; Chrousos, G.P.; Mantzoros, C.S. Low adiponectin levels are associated with renal cell carcinoma: a case-control study. Int. J. Cancer 2007, 120, 1573–1578. [CrossRef]
- Petridou, E.; Mantzoros, C.; Dessypris, N.; Koukoulomatis, P.; Addy, C.; Voulgaris, Z.; Chrousos, G.; Trichopoulos, D. Plasma adiponectin concentrations in relation to endometrial cancer: a case-control study in Greece. J. Clin. Endocrinol. Metab. 2003, 88, 993–997. [CrossRef]
- Xie, L.; Wang, Y.; Wang, S.; Wu, N.; Chen, Y.; Yan, J. Adiponectin induces growth inhibition and apoptosis in cervical cancer HeLa cells. Biologia 2011, 66, 712–720. [CrossRef]
- Chou, S.H.; Tseleni-Balafouta, S.; Moon, H.-S.; Chamberland, J.P.; Liu, X.; Kavantzas, N.; Mantzoros, C.S. Adiponectin receptor expression in human malignant tissues. Horm. Cancer 2010, 1, 136–145. [CrossRef]
- Modesitt, S.C.; van Nagell, J.R. The impact of obesity on the incidence and treatment of gynecologic cancers: a review. Obstet. Gynecol. Surv. 2005, 60, 683–692. [CrossRef]
- Moon, H.-S.; Chamberland, J.P.; Aronis, K.; Tseleni-Balafouta, S.; Mantzoros, C.S. Direct role of adiponectin and adiponectin receptors in endometrial cancer: in vitro and ex vivo studies in humans. Mol. Cancer Ther. 2011, 10, 2234–2243. [CrossRef]
- Yamauchi, N.; Takazawa, Y.; Maeda, D.; Hibiya, T.; Tanaka, M.; Iwabu, M.; Okada-Iwabu, M.; Yamauchi, T.; Kadowaki, T.; Fukayama, M. Expression levels of adiponectin receptors are decreased in human endometrial adenocarcinoma tissues. Int. J. Gynecol. Pathol. 2012, 31, 352–357. [CrossRef]
Figure 1.
Immunohistochemistry evaluation scheme exemplarily in RCC cohort. Magnification: 20x, LeptinR: (A) negative, (B) weak (1+), (C) moderate (2+), (D) strong (3+) positivity. AdipoR1: (E) negative, (F) weak (1+), (G) moderate (2+), (H) strong (3+) positivity.
Figure 1.
Immunohistochemistry evaluation scheme exemplarily in RCC cohort. Magnification: 20x, LeptinR: (A) negative, (B) weak (1+), (C) moderate (2+), (D) strong (3+) positivity. AdipoR1: (E) negative, (F) weak (1+), (G) moderate (2+), (H) strong (3+) positivity.
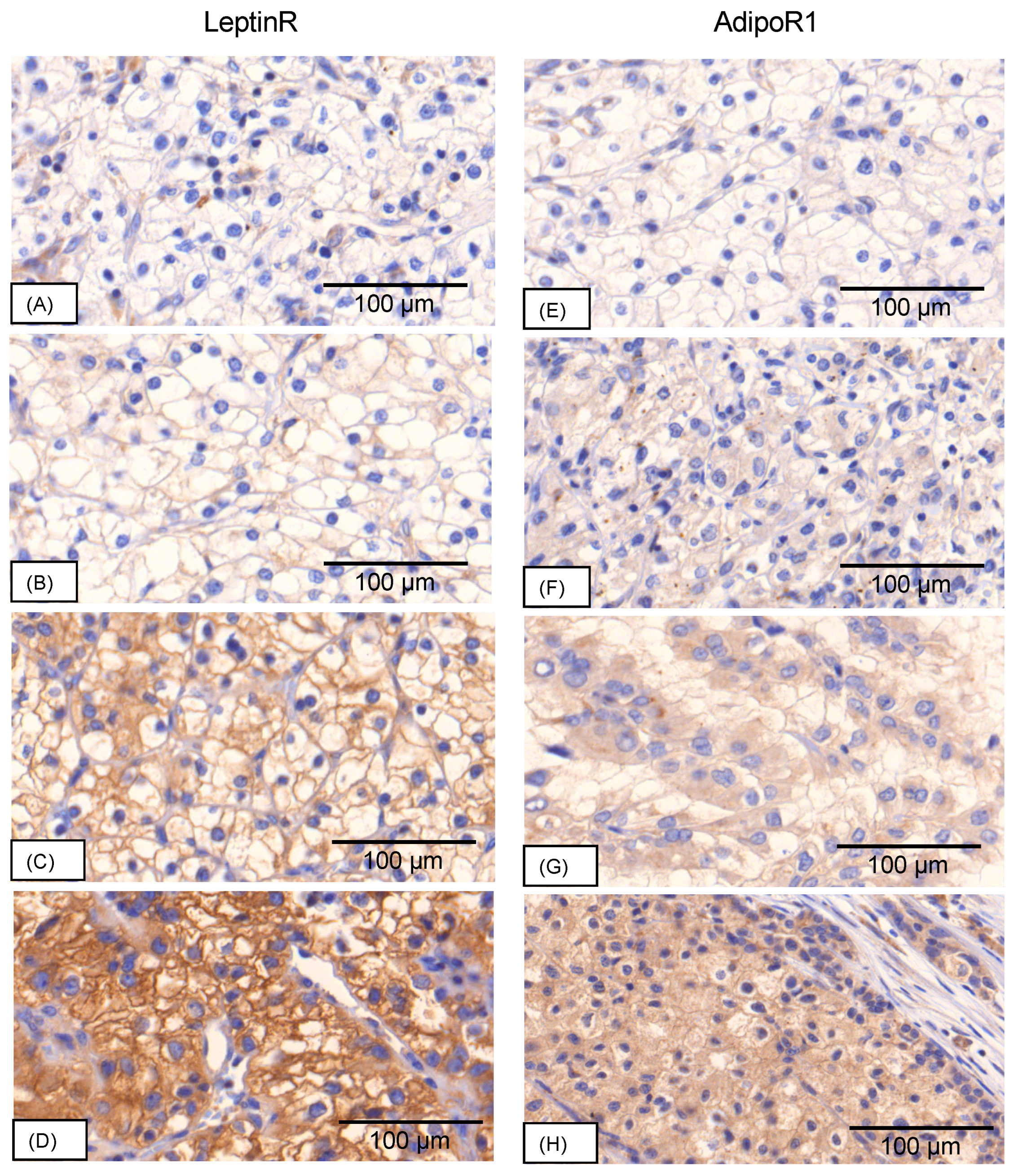
Figure 2.
Prognostic value of receptor expression. Significant longer overall survival was evident with higher leptinR expression in RCC (p = 0.004), cervical (p = 0.034) and vulvar (p = 0.029) carcinoma. AdipoR1 expression showed no prognostic value.
Figure 2.
Prognostic value of receptor expression. Significant longer overall survival was evident with higher leptinR expression in RCC (p = 0.004), cervical (p = 0.034) and vulvar (p = 0.029) carcinoma. AdipoR1 expression showed no prognostic value.
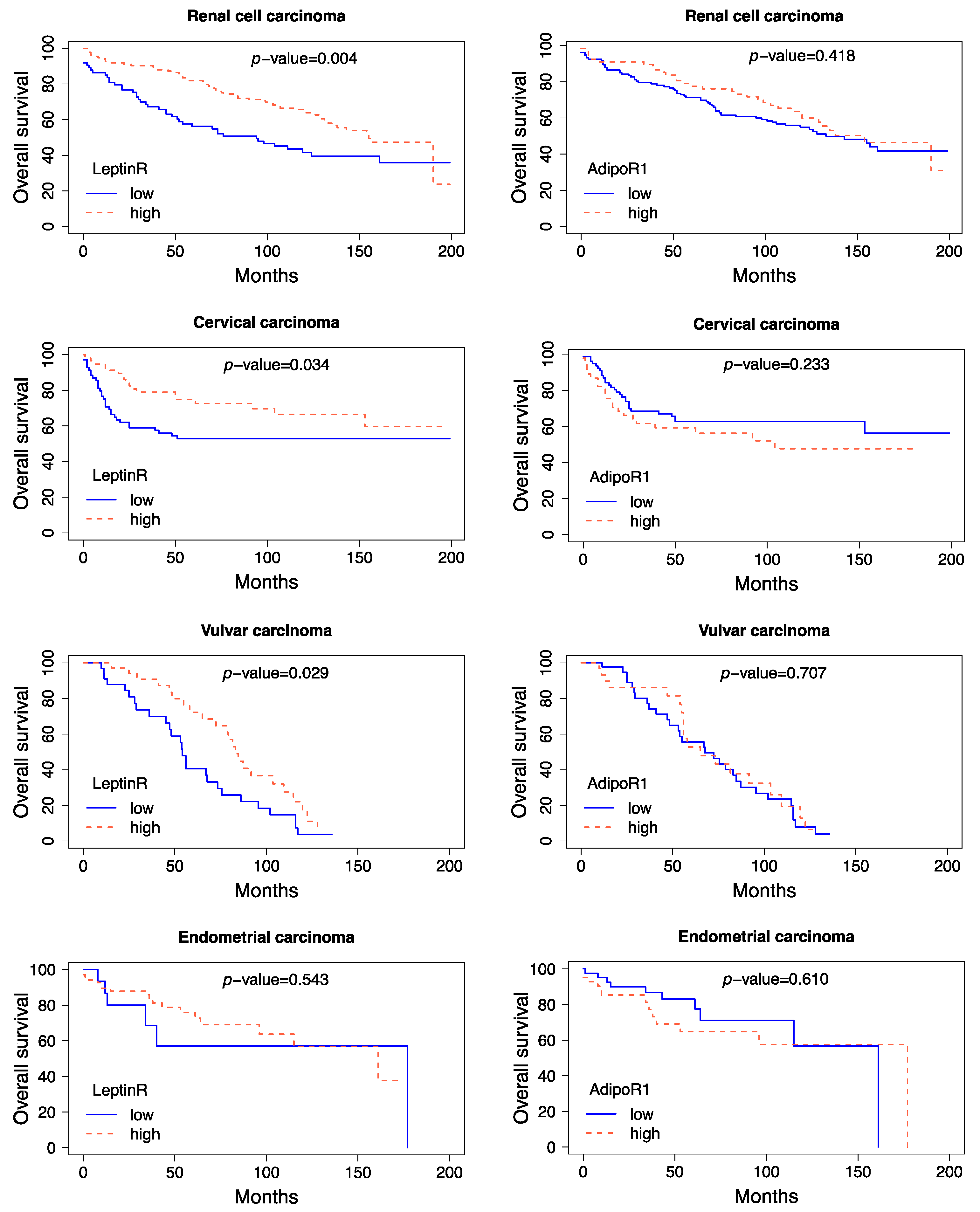
Figure 3.
TCGA Pan cancer survival analyses. Median of leptinR and adipoR1 mRNA expression z-scores relative to all samples. High expression of leptinR mRNA was associated with longer overall survival in ccRCC (p = 0.005). For cervical cancer high expression of leptinR mRNA was associated with shorter OS (p = 0.008). The mRNA expression level in endometrial cancer had no significant prognostic value. AdipoR1 mRNA expression had no prognostic value in any of the three tumour entities.
Figure 3.
TCGA Pan cancer survival analyses. Median of leptinR and adipoR1 mRNA expression z-scores relative to all samples. High expression of leptinR mRNA was associated with longer overall survival in ccRCC (p = 0.005). For cervical cancer high expression of leptinR mRNA was associated with shorter OS (p = 0.008). The mRNA expression level in endometrial cancer had no significant prognostic value. AdipoR1 mRNA expression had no prognostic value in any of the three tumour entities.
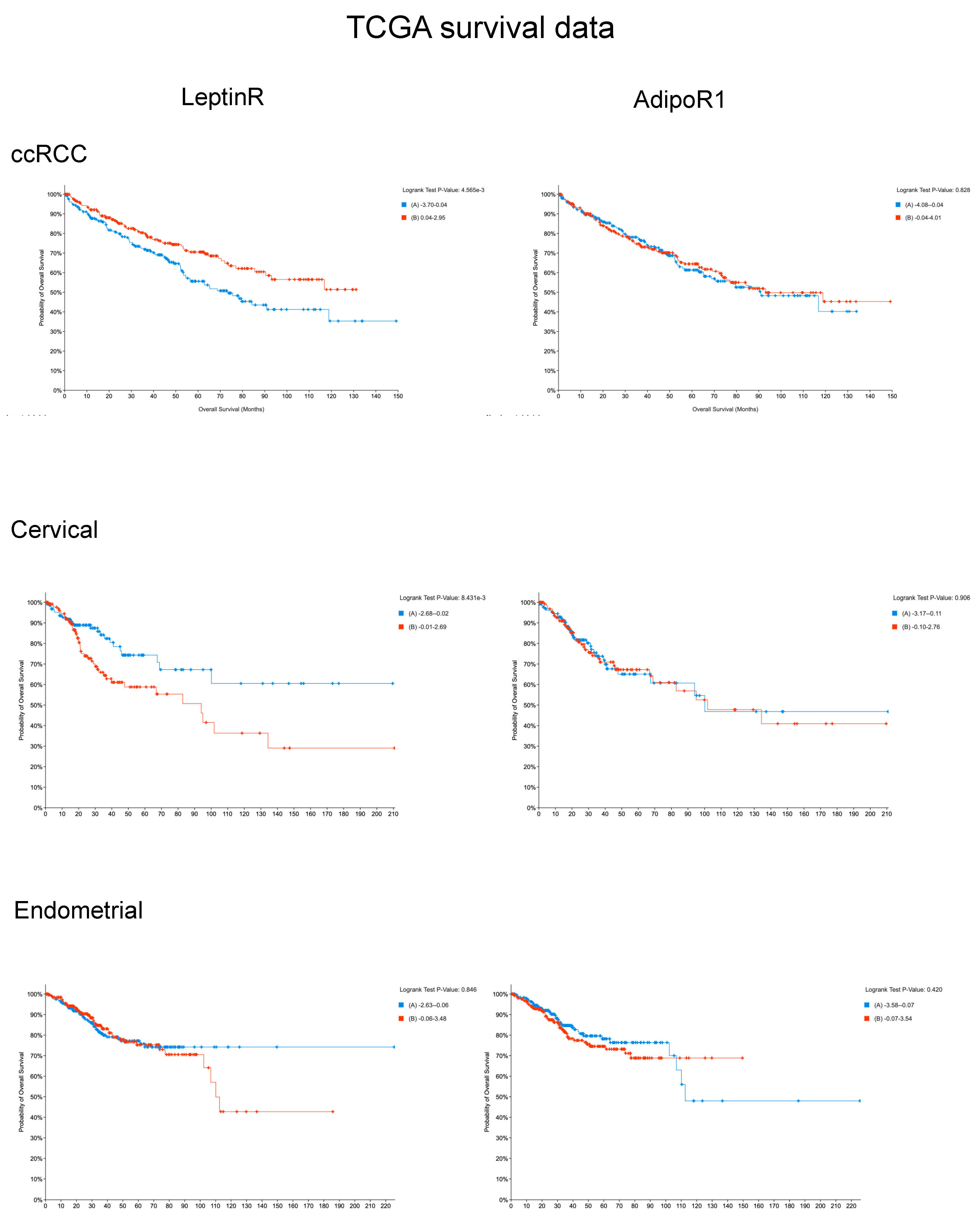

Table 1.
Results of multivariable Cox regression survival analysis. RCC and vulvar carcinoma tissues with high leptinR expression showed a significantly longer overall survival.
Table 1.
Results of multivariable Cox regression survival analysis. RCC and vulvar carcinoma tissues with high leptinR expression showed a significantly longer overall survival.
| Proteins | Staining Intensity | N (Low/High) | Confounders | Hazard Ratio | 95% CI | p-Value (cox) | Likelihood-Ratio-Test | |
|---|---|---|---|---|---|---|---|---|
| RCC | LeptinR | 0–1+/2–3+ | 73/133 | age, BMI, pT, subtype, grade | 0.62 | 0.40 - 0.96 | 0.03 | <0.001 |
| AdipoR1 | 0–1+/2–3+ | 133/67 | age, BMI, pT, subtype, grade | 1.02 | 0.63 - 1.63 | 0.95 | <0.001 | |
| ccRCC | LeptinR | 0–1+/2–3+ | 65/95 | age, BMI, pT, grade | 0.64 | 0.40 - 1.01 | 0.06 | <0.001 |
| AdipoR1 | 0–1+/2–3+ | 116/41 | age, BMI, pT, grade | 0.97 | 0.56 - 1.67 | 0.92 | <0.001 | |
| Cervical cancer | LeptinR | 0–1+/2–3+ | 69/57 | age, BMI, pT, grade | 1.05 | 0.49 - 2.28 | 0.90 | <0.001 |
| AdipoR1 | 0–1+/2–3+ | 73/48 | age, BMI, pT, grade | 0.93 | 0.42 - 2.05 | 0.85 | <0.001 | |
| Vulvar cancer | LeptinR | 0–1+/2–3+ | 42/47 | age, BMI, pT, grade | 0.37 | 0.18 - 0.79 | 0.01 | 0.02 |
| AdipoR1 | 0–1+/2–3+ | 55/36 | age, BMI, pT, grade | 1.13 | 0.52 - 2.45 | 0.76 | 0.6 | |
| Endometrial cancer | LeptinR | 0–1+/2–3+ | 15/67 | age, BMI, pT, grade | 1.52 | 0.36 - 6.39 | 0.56 | 0.004 |
| AdipoR1 | 0–1+/2–3+ | 40/42 | age, BMI, pT, grade | 1.42 | 0.54 - 3.73 | 0.48 | 0.009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



