
Submitted:
16 July 2024
Posted:
24 July 2024
You are already at the latest version
Abstract
Background: Breast cancer incidence and mortality exhibit a rising trend globally among both premenopausal and postmenopausal women suggesting that there are serious errors in our preventive and therapeutic measures.Purpose: Providing a series of valuable, but misunderstood inventions highlighting the role of increasing estrogen signaling in prevention and therapy of breast cancer instead of its inhibition. Results: 1. Breast cells and breast cancer cells with germline BRCA1/2 mutations similarly show defect in liganded estrogen receptor (ER) signaling demonstrating its role in genomic instability and cancer initiation. 2. In breast cancers, the increased expression of certain receptor family is an effort for self directed improvement of genomic defects, while the weakness or loss of receptors indicates a defect requiring medical repair. 3. ER overexpression in breast cancer cells is capable of strengthening estrogen signaling and DNA repair, while in ER negative tumors, HER2 overexpression tries to upregulate unliganded ER activation and genome stabilization. 4. ER positive breast cancers responsive to endocrine therapy may show a compensatory ER overexpression resulting in a transient tumor response. Breast tumors, non responsive to endocrine therapy, show HER2 overexpression for compensation the complete blockade of liganded ER activation. 5. In breast tumors, somatic mutations serve upregulation of liganded or unliganded activation of ERs helping genome stabilization and apoptotic death. 6. The dynamic communication between breast cancer and its microenvironment is a wonderful collaboration among molecular players fighting for genomic repair and apoptosis in the tumor. 7. In breast cancers, there is no resistance to genotoxic or immune blocker therapies, but rather the non responsive tumor cells exhausted all compensatory possibilities against therapeutic damages. Conclusion: Understanding the behavior and ambition of breast cancer cells may achieve a turn in therapy via applying a supportive care instead of genotoxic measures.
Keywords:
antiestrogen
; breast cancer
; cancer therapy
; DNA damage
; DNA repair
; endocrine disruptor
; estrogen receptor
; growth factor receptor
; immune reaction
; mutation
Introduction
Breast cancer constitutes a major public health problem globally, as it is the most commonly diagnosed cancer in the world. The recent global cancer burden data estimate that there were near 2.3 million diagnosed breast cancer cases in 2020 and this disease is the leading cause of cancer mortality worldwide among women [1]. The therapy of breast cancer is a great challenge even today illuminating that there are serious shortcomings in our preventive and therapeutic measures.
Breast cancer incidence and mortality exhibit a rising trend globally among both premenopausal and postmenopausal women [2]. Incidence trends for 1998-2012 were assessed by calculating the annual average percent change. In 2018, 645 000 premenopausal and 1·4 million postmenopausal breast cancer cases were diagnosed worldwide, with more than 130 000 and 490 000 breast cancer related deaths occurring in the pre- and postmenopausal groups, respectively. Proportionally, countries with a low human development index (HDI) faced a higher burden of premenopausal breast cancer concerning both incidence and mortality as compared with higher income countries. Surprisingly, countries with a very high HDI had the highest premenopausal and postmenopausal breast cancer incidence; 30 and 253 cases per 100 000, respectively. By contrast, countries with low and medium HDI showed the highest mortality among both premenopausal (8/100 000) and postmenopausal (53/100 000) breast cancer cases.
In five continents, country-specific data and trends of breast cancer incidence and mortality were analyzed up to 2018 [3]. Most countries showed an increasing trend in breast cancer incidence. For the older population aged ≥ 50 years, Japan, Slovakia and China reported the most prominent increase in incidence rate. For young females (<50 years), Japan, Germany and Slovakia reported the most drastic rise in breast cancer incidence. In addition, 12 countries showed an increasing incidence rate of breast cancer among women aged <40 years. As for breast cancer related mortality, the Philippines, Thailand, Colombia and Brazil reported a significantly high increase. In conclusion, the disease burden of breast cancer showed an increasing trend in a large number of populations.
Global increasing trend in breast cancer mortality underlines that the wide spread introduction of early diagnosis via mammographic screening could not keep under control the most frequently diagnosed cancer in women. In a large prospective study including more than 100 000 women with ductal carcinoma in situ (DCIS)) diagnosis, it was established that DCIS carries a higher risk of breast cancer-related death than previously thought [4]. Women diagnosed with DCIS are twice as likely to die as compared with the general female population in US. The high risk for invasive breast cancer development from DCIS suggests that our standard surgical and adjuvant therapeutic measures require rethinking as being inappropriate for ensuring a tumor-free life [5].
The presented study illuminates the crucial role of breast cancer studies in the progress of overall cancer research. Understanding the unique sensitivity of female breasts to genomic imbalance and the recognition of DNA damage repairing activity in breast cancer cells justify that our currently used modern strategies targeting the DNA damage responses of tumors are erroneous.
Historical Survey of Omitted Opportunities for Understanding Breast Cancer Behavior
At the end of the 19th century, pulsation of breast cancers was observed parallel with the menstrual cycle of premenopausal patients. Misunderstanding of this observation led to the erroneous idea of estrogen withdrawal as a breast cancer therapy via oophorectomy [6]. Later, farther results were published on achieving a tumor regression rate of <30% in breast cancer patients via therapeutic oophorectomy [7]. From that time onwards, estrogen withdrawal as a means for breast cancer prevention and therapy has become a fundamental medical principle defining a unique pathway for breast cancer care till now. Breast cancer with its presumably recognized causal factor estrogen, has become the pioneer of oncological research fairly dominating the therapeutic investigations.
In 1960, the discovery of estrogen receptor (ER) was a milestone in medical research [8]. Estrogen binding proteins proved to be transcription factors inducing DNA replication and protein synthesis in the targeted tissues. This invention apparently illuminated the mechanism of estrogen induced breast cancer via liganded ER activation. From that time onwards, molecular studies tried to find causal correlations between excessive estrogen signaling and breast cancer induction [9,10,11,12].
Extragonadal estrogen synthesis in adipose tissue was first described in 1974 [13]. In adipocytes, androgen hormones were converted to estrogens via aromatase enzyme activity. The great physiological significance of this phenomenon and the crucial role of estrogen signal in the regulatory functions of adipose tissue were clarified much later [14]. Local aromatase activity parallel with high estrogen concentration in mammary adipose tissue was erroneously evaluated as a fuel for initiation and proliferation of breast cancer [15].
In the early 1950s, menopausal hormone therapy (MHT) became widely used among menopausal women. Synthetic estrogen, ethinylestradiol (EE) and CEE extracted from pregnant equine urine were prescribed for the care of menopausal complaints and for prophylaxis of cardiovascular diseases and thromboembolic complications [16]. In MHT user women, increased risks for cardiovascular and pulmonary thromboembolic events and for breast tumor were established [17]. Concerning the risks and benefits of synthetic and natural hormone treatments, there were no comparative studies.
Synthetic estrogen, ethinylestradiol became the standard estrogenic component of oral contraceptive (OC) pills developed in the 1960s [18]. In OC users, thromboembolic diseases and increased risk for some cancers including tumors of the female breast were rare but serious complications [19,20]. Moreover OC use increased the risk for glucose intolerance and type 2 diabetes as the chemically modified synthetic estrogen proved to be an endocrine disruptor [21]. In laboratory investigations, ethinylestradiol proved to be a histone modifying genotoxic compound [22].
Despite the complications of MHT and OC use in women, synthetic hormones were not withdrawn from medical practice; their prescription was supported by the Food and Drug Administration [16]. In addition, the toxic and carcinogenic effects of human estrogen hormones were included into medical school-books, world while.
In the early 1970s, antiestrogen compounds were developed for ER positive breast cancer therapy. Blockers of liganded ER activation and aromatase enzyme inhibitors were introduced so as to spare tumors from excessive estrogen signaling [23]. In tumors, the blockade of liganded estrogen signal was regarded as a single pathway targeting DNA damage response, while it seemed to spare healthy cells being protected by the complexity of their different routes leading to DNA repair. Conversely, liganded estrogen signaling is the fundamental regulator of mammalian cells and its blockade is genotoxic provoking desperate counteractions in both patients and their tumors [24].
The initial enthusiasm rapidly turned into frustration as about 50% of even the targeted breast tumors with ER expression proved to be non responders to endocrine therapy, it was nominated as primary resistance [25]. Moreover, following a long term therapy, all patients showing previously good tumor response, turned to secondary endocrine resistance resulting in metastatic tumor spread and lethal outcome. Molecular studies on ER positive tumors under endocrine therapy mistakenly suggested, that in responsive tumors the overexpression of ERs is an effort for survival [26]. By contrast, in non responsive tumors, the increased expression of growth factor receptors seemed to be a survival technique [27].
Studying the endocrine resistance of breast cancers illuminated that responsive tumors successfully counteract the endocrine disruptor therapy via overexpression of ERs, restoring estrogen signaling and improving genomic regulation [28]. Conversely, when the liganded activation of ERs is completely blocked in tumors, growth factor receptor overexpression desperately targets ER activation via unliganded pathway. Non responsive breast cancers are not fighting for their survival against antiestrogen therapy, but rather they are incapable of genomic repair via counteracting the endocrine blockade.
In the 1990s, correlations between obesity and increased risk for breast cancer were reported in postmenopausal women [29]. Later, a paradoxical and controversial relationship was established between obesity and breast cancer, defined by the menopausal status [30]. In obese postmenopausal women, the increased aromatase activity and estrogen synthesis of abundant adipose tissue was mistakenly regarded as a causal factor of increased risk for breast cancer. By contrast, in premenopausal patients, the obesity associated hormonal defects and amenorrhoea seemed to be protective for female breasts via reduced estrogen signaling. In reality, in obese postmenopausal women, estrogen loss and the associated insulin resistance promotes breast cancer development. Conversely, in obese, cycling premenopausal cases, a moderately declining estrogen signal may counteract the obesity associated insulin resistance providing protection for the female breast [31].
In 1992, report on a case control study established that hyperinsulinemia, which is a compensatory reaction against insulin resistance, is a significant risk factor for breast cancer independent of general adiposity or body fat distribution [32]. Analyzing the role of insulin in breast cancer development, its complex interaction with estrogen was described [33]. Insulin induces aromatase synthesis in mammary adipose cells and ER expression in tumor cells. In addition, insulin suppresses sex hormone binding globulin level, increasing the concentration of accessible estrogen. Authors established that excessive insulin level increases estrogen synthesis and bioactivity that equivocally support the development of estrogen-dependent breast cancer. In reality, insulin resistance develops as a consequence of defective estrogen signaling [34]. Compensatory hyperinsulinemia tries to restore genome stabilization via upregulation of estrogen signaling in both healthy breast cells and breast cancers [35].
Breast cancer incidence and progression shows strong disparities between African American (AA) and white American (WA) women. Among AA women, breast cancers exhibit a higher prevalence and are more often diagnosed in young age [36]. In AA women, the progression of mammary tumors is rapid, more frequently exhibit lower differentiation and triple negative receptor subtype as compared with white women [37]. Studying these ethnic/racial differences in breast cancer incidence and mortality clarified that excessive pigmentation of dark skinned women in US results in a relative light-deficiency. In AA women, poor light exposure may promote estrogen deficiency, insulin resistance, hypothyroidism and low vitamin-D level conferring excessive breast cancer incidence and mortality [38]. In AA women, a thorough care of hormonal and metabolic imbalances may reduce their overall health disparity. Nevertheless, the continuous growth of the Black-White breast cancer mortality gap justifies that the current approaches to eliminating racial/ethnic disparities in breast cancer are not appropriate [39].
Studying the receptor landscape of breast cancers, ER positive and ER negative tumors were sharply separated [40]. Increased ER expression was regarded as a survival technique of estrogen dependent tumors, whilst the much more aggressive ER negative ones were kept to be entirely hormone independent having quite different etiology, clinical picture and therapeutic possibility. Considering the high prevalence of ER positive breast tumors in postmenopausal women, increased ER expression indicates a compensatory action asking for estrogen from the estrogen deficient milieu [41]. Conversely, the lack of hormone receptors in breast tumors reflects the serious defect of estrogen signaling attributed to the defect of compensatory ER expression.
Discovery of BRCA1 [42] and BRCA2 [43] genes proved to be a breakthrough in cancer research. Germline mutation of these genome safeguarding genes resulted in genomic instability and high risk for cancer, specifically for breasts and ovaries in women. Nevertheless, appropriate BRCA proteins play essential roles in all human cell types ensuring genomic stability [44,45].
Molecular investigations on tumor cells with BRCA mutation revealed the weakness of hormonal activation of ERs, while increased compensatory unliganded ER activation also was experienced [46]. In patients with BRCA gene mutation, compensatory increased aromatase enzyme expression and activation as well as elevated estrogen synthesis were experienced. These findings mistakenly justified the presumed estrogen induced genomic instability [47]. Breast cancers exhibiting BRCA gene mutation are predominantly basal type ER negative; HER2 overexpressed and triple negative breast cancers (TNBCs) [48,49]. These hormone receptor negative breast cancer subtypes are familiar with their independence of hormonal influences
Both molecular and clinical findings on BRCA gene mutation carrier tumors oppose the role of estrogen in genomic instability and breast cancer development [50]. Tumors with BRCA gene defect may hardly be under excessive estrogen activation as they lost their liganded ER activation and ER expression. In BRCA gene mutation carriers, the defect of liganded ER activation clearly showed a causal correlation with the instability of genome and the high risk for breast cancer. Studying patients and their tumors with BRCA mutation helped to reveal the technique of genomic stabilization via regulatory circuits of ERs.
Studies on healthy and cancer cells with BRCA1/2 mutation, undoubtedly revealed the hard work for compensatory upregulation of estrogen signaling and genome stabilization via somatic mutations [51]. These observations suggested that somatic mutations in healthy cells try to maintain genomic stability, while in tumor cells constitutive mutations serve the inhibition of further genomic damages, rather than stimulating the proliferation. Nevertheless, reports on patients and tumors with BRCA gene mutation, concordantly blame excessive estrogen signaling for genomic instability and breast tumor growth.
In the early 2000s, investigations on the liganded and unliganded activation of ERs fairly promoted the development of human genetics and understanding the rules of the whole genomic machinery [52,53]. Estradiol regulated signaling network maintains genomic integrity and drives DNA damage repair in both men and women. Recently, the vision of E2 as a pro-carcinogenic hormone seems to be somewhat questionable [54].
In 2004, a large, Women’s Health Initiative (WHI) study was reported on a strikingly decreased risk of breast cancer in CEE (Premarin) treated women compared to the placebo control cases [55]. Authors could not believe in their unusual findings and suggested strengthening investigations. In 2002, a similar WHI study found increased incidence of cardiovascular and thromboembolic complications and an increased risk for breast cancer among women taking Premarin plus MPA (medroxyprogesterone acetate) [17]. In this examination, the beneficial Premarin treatment was counteracted by using a genotoxic synthetic progestin, MPA [56].
The WHI study, resulting in breast cancer prevention by Premarin alone was repeated several times on women remaining alive [57,58,59]. The genome safeguarding effect was justified in the Premarin treated group in all repeated studies; however, authors could not explain their unusual findings. In 2019, a global meta-analysis study was published on the worldwide epidemiological evidences of MHT induced breast cancer, associated with all used hormone formulas [60]. Nevertheless, WHI studies justifying the breast cancer prophylaxis by Premarin treatment were not included into this examination.
Despite our developing knowledge concerning the complex roles of estrogen signaling in the genomic regulation and health maintenance of mammalians, breast cancer has been considered an estrogen induced disease till now [61].
Estrogen Deficiency and ER Resistance Proved to Be Newly Recognized Cancer Risk Factors
In 2007, estrogen deficiency was revealed as a risk for oral cancer based on the findings of a Hungarian clinical-epidemiological study [62]. Age and gender related analysis of oral cancer cases revealed that men are increasingly affected by this aggressive tumor during their whole life, attributed to their smoking and drinking habits. By contrast, women, in their premenopausal period are near completely protected from this disease. Above 50; a steeply increasing oral cancer incidence may be observed among non smoker, non drinker older women parallel with their estrogen loss.
Estrogen deficiency emerged as a risk factor for further malignancies and the principle of “estrogen induced breast cancer” became fairly questionable. Since genomic instability may not develop via quite opposite pathways at different sites, the defect of estrogen signaling emerged as a risk factor even for breast cancer [63]. In postmenopausal women, estrogen loss maybe an obvious risk factor for breast cancer as compared with premenopausal patients. In premenopausal patients, inherited or acquired gene mutations may result in weak estrogen signaling, genetic instability and increased breast cancer risk. Among breast cancer cases, about 80% are above 50, being predominantly postmenopausal, while only 20% of them are younger, premenopausal women [64].
Thorough investigations could not find direct correlations between increased serum estrogen levels and breast cancer development in either young or postmenopausal breast cancer cases [65,66]. Epidemiological studies suggested that the better the reproductive capacity of a woman the lower is her breast cancer risk. In premenopausal women having healthy ovulatory cycles, the breast cancer risk is much lower as compared with postmenopausal cases with extremely low serum estrogen concentrations [67]. Strikingly decreased breast cancer risk may be observed in correlation with parity and particularly multiparity as compared with nulliparous women [68]. Conversely, anovulatory disorders and nulliparity increase the risk for breast tumors and further female cancers [69,70]. These epidemiological studies support the pathogenic role of defective estrogen signaliing in breast cancer development.
Immunohistochemical imaging of estrogen receptors (ERs), progesterone receptors (PRs) and human epidermal growth factor receptors (HER2s) in breast cancers provided further possibilities to clarify the risk factors and therapeutic possibilities of variously differentiated tumors [40]. In postmenopausal breast cancer cases, tumors predominantly showed high differentiation with abundant ER expression compensating the decreasing level of serum estrogen [71]. There was an erroneous concept suggesting the hormone dependence of ER positive tumors and estrogen seemed to be a fuel for their growth and metastatic spread. In reality, in tumors, a compensatory increased ER expression upregulates estrogen signaling and helps DNA stabilization in an estrogen deficient milieu [41].
In contrast, premenopausal patients with breast cancer have predominantly poorly differentiated ER- PR- negative or TNBC type tumors, while their serum estrogen levels maybe normal or compensatory increased attributed to the defect of ERs [72]. In young patients, the predominance of poorly differentiated, hormone receptor negative tumors may be associated with germline or acquired weakness of their liganded ER activation [41].
Germline BRCA gene mutation carriers exhibit high risk for both ER-negative and TNBC type tumors in correlation with their defect of ER expression and activation. Female breasts require a balanced ER activation via liganded and unliganded pathways consequently, they are uniquely vulnerable to the fault of estrogen signaling in BRCA gene mutation carriers. In young women with weak estrogen signaling and ER negative breast cancer, a deceiving high estrogen level may be experienced associated with clinical signs of menstrual disorders and anovulatory infertility [73].
In conclusion, either estrogen deficiency or defective liganded ER activation may lead to genomic instability increasing the risk for breast cancer.
Genes Activated by Estrogen Upregulate DNA Stabilization and Silence cell Proliferation in Breast Cancer Cells
Estrogen liganded ERs are transcriptional factors regulating the genomic machinery as hubs in the network of regulatory circuits. DNA stabilization, cell proliferation/silencing and fuel supply are the main regulatory circuits of ERs orchestrating all genomic processes in mammalian cells [74].
The DNA stabilization circuit of ERs enjoys the primacy over all other regulatory functions and requires continuous estrogen activation of ERs. Three regulatory proteins: ER alpha, BRCA1 and aromatase enzyme (A450) create a signaling network via triangular partnership. Liganded ER-alpha is capable of occupying the promoter regions of ESR1, BRCA1 and Cyp19A aromatase genes and driving messenger RNA (mRNA) expressions. The next step is the expression of ER-alpha, BRCA1 protein and aromatase enzyme via translation. Abundant aromatase expression increases estrogen synthesis and the newly formed estrogen activates ERs again closing the regulatory circuit. Estrogen paralelly drives the genome stabilizer circuit and estrogen signaling according to the requirements. Decreased estrogen supply or weakness of any of the three regulatory proteins endangers genomic stability and promotes emergency measures.
In the cell proliferation circuit liganded ERs regulate and supervise the rapidity and quality of cell proliferation via upregulation or downregulation adapting to the necessities. ERs exhibit mutual interaction with membrane associated growth factor receptors (GFRs). The expression and activation of growth factors (GFs) and their receptors (GFRs) are also regulated under estrogen control. Growth factor signal (GFS) transduction upregulates kinase cascades via PI3- K/AKT/mTOR and RAS/RAF/MEK/MAPK pathways. Kinase cascades mediate nuclear ER activation via unliganded pathway facilitating further expression of specific genes.
Through the fuel supply circuit, estrogen liganded ERs regulate all phases of glucose uptake and orchestrate all players participating in glucose homeostasis. Estrogen activated genes drive insulin synthesis in the pancreatic islands and the expression of insulin receptors (IRs) in all human cells. Liganded ERs stimulate glucose transporter 4 (GLUT4) gene expressions and GLUT4 translocation to the cell membrane so as to mediate glucose uptake. Plasma membrane associated ERs activate insulin receptor substrate 1 (IRS-1) stimulating the kinase cascade through PI3-K/AKT/mTOR pathway. Kinase cascade confers unliganded activation for nuclear ERs closing the regulatory circuit and upgrading glucose uptake.
Genomic instability is a crisis situation even for cancer cells moving the activation of available DNA protecting mechanisms [51]. Breast cancer cells use and strengthen their genome stabilizer pathways via gene amplifications and activating mutations. Highly differentiated breast tumors show increased expression of ERs and estrogen synthesis driving liganded ER activation and genome stabilization. In case of moderately differentiated breast cancers, the loss of hormone receptors upregulates the expression of HER2 receptors and kinase cascade members, strengthening the unliganded activation of scarcely occurring ERs. In triple-receptor negative, poorly differentiated tumors, there is no possibility for either liganded or unliganded ER activation, resulting in unrestrained proliferation.
In Breast Cancer Cells, Estrogen Upregulates the Genome Stabilizer Circuit Counteracting Pro-Oncogenic Processes
In tumor cells, estradiol treatment stimulates the liganded ER activation. Four types of estrogens; estrone, estradiol, estriol and estetrol significantly increased the ER-expression of ER-positive breast cancer cell lines as compared with the untreated controls [75]. This activation of ERs is an effort for upregulation of genome stabilization and stopping cell proliferation, rather than a survival technique.
In breast cancer cells, estrogen treatment facilitated the expression of membrane associated growth factor receptors, both EGFR and HER2, upregulating even the unliganded activation of ERs [27]. In addition, estradiol treatment enhances the activity of phosphatidylinositol 3-kinase (PI 3-K)/Akt system in tumor cells [76]. Estrogen promoted the activation of membrane associated growth factor receptors (GFRs) and kinase cascades serving DNA stabilization through increased unliganded ER activation [24]. In tumor cells, crosstalk between overexpressed ERs and GFRs targets the improvement of genomic stability leading to apoptotic death.
In breast tumor cells, estrogen treatment frequently induces an amplification of ESR1 gene at 6q25 locus upregulating ER protein synthesis [77]. During breast cancer treatment with estrogen, a cluster of non coding RNAs was experienced activating the appropriate ESR1 locus [78]. A longer disease-free survival was experienced in patients showing ESR1 gene amplification in breast tumors compared to those without this alteration [79]. These clinical observations justify that in tumors an estrogen induced amplification of ESR1 gene is not a pro-oncogenic adaptation but rather, an abundant expression of ERs may facilitate tumor responses.
In estradiol treated tumor cells, activated ERs confer the transcription and an increased expression of lncRNAs, such as HOTAIR [80]. Increased HOTAIR expression induces epigenetic changes both on ESR1 and BRCA1 genes, promoting increased expression of ER-alpha, strengthening DNA stabilization and tumor regression [81]. Increased HOTAIR expression in tumors of breast cancer cases was associated with lower risks of relapse and mortality compared to those having low expression of HOTAIR in their cancers [82].
In breast tumor cells, estrogen activation of ERs is capable of increasing aromatase enzyme expression and estrogen synthesis, facilitating the liganded activation of ERs. ER-negative tumor cells were transfected with exogenous ER alpha and estradiol treatment enhanced the aromatase activity in a dose-dependent manner [83]. In breast cancer cells, estradiol may enhance the expression of aromatase enzyme through ER-alpha activation and increases aromatase activity via an enhanced tyrosine phosphorylation of the enzyme [84].
High aromatase activity and an increased in situ estrogen concentration were experienced at the invasive front of breast cancers, where interaction between the tumor and neighboring tissues may define the expansion or regression of cancer [85]. Aromatase activity of surgically removed tumor samples and patient’s survival time after surgery showed a direct correlation in breast cancer cases [86,87].
In MCF-7 breast cancer cell line, estrogen treatment stimulated increased BRCA1 protein expression [88]. In turn, BRCA1 protein promotes ESR1-gene activation leading to an increased expression of ER-alpha mRNA and ER protein in breast cancer cell lines [89]. In hypoxia, that is an important factor of solid tumor progression, a decrease of both BRCA1 and ERα expression was demonstrated in MCF-7 cells [90]. These observations support that ligand activated ER alpha and BRCA1 protein together upregulate the circuit of genome stabilization leading to self directed death of tumor cells [50].
In tumor cells, estradiol treatment increases insulin assisted glucose uptake. In MCF-7 tumor cell lines, estradiol facilitates insulin signaling through an increased expression of insulin receptor substrate-1 (IRS-1) [91]. In MCF-7 cell lines, estradiol helps the entrance of glucose through the cell membrane via increasing GLUT4 expression. Estradiol treatment increases PI3K/Akt kinase cascade activation helping the translocation of GLUT4 into the plasma membrane driven by ER-alpha [92]. These results reveal that estrogen increases insulin assisted glucose uptake even into cancer cells ensuring energy for the improvement of DNA stability, rather than increasing proliferative activity.
Molecular Classification of Breast Cancer Subtypes Is a Mirror Reflecting the Defect of Estrogen Signaling and Genomic Damage in Patients
Breast cancer is apparently a multifaceted disease originating from the excessive proliferation of either lobular or ductal breast epithelium [93]. The molecular profile is the most important factor for breast cancer categorization [94]. Molecular heterogeneity of breast cancers was exposed through the expression of various gene panels. Four main groups of breast cancers were established; luminal A, luminal B, HER2 overexpression, and basal-like triple-negative breast cancers (TNBCs). Moreover, a highly differentiated subgroup of breast cancer also was described morphologically resembling the tumors of luminal A group but it is associated with a poor outcome of the disease.
Breast cancer subgroups are recognized by immunohistochemical staining of receptors. In clinical practice, ER-alpha, progesterone (PR) and human epidermal growth factor receptor (HER2) expressions are evaluated [93]. The increased expression of certain receptor groups in tumors is erroneously evaluated as aggressive effort for survival leading to unrestrained proliferation. According to current therapeutic principles, the targeted inhibition of highly expressed receptors, such as ERs or HER2 proteins may inhibit the altered DNA damage response of tumors. Conversely, in tumors, the overexpression of certain receptors reflects the upregulation of pathways serving the improvement of defective genomic processes and DNA repair [81].
In breast cancer cells, lack or low expression of certain receptors is associated with aggressive growth and at the same time reveals the critical points of serious genomic defects to be repaired [41]. Currently, poorly differentiated basal type triple negative breast cancers are treated with chemotherapy or immune therapy as they do not have receptors to be targeted [95].
Luminal A subtype of breast cancers are highly differentiated tumors exhibiting increased expression of hormone receptors, ER alpha, and progesterone receptor (PR and showing good prognosis. In breast cancer, increased ER expression is erroneously regarded as a pivotal player in tumor initiation and growth conferring excessive estrogen signaling. In the clinical practice, ER expression in breast cancer is a prerequisite for the efficacy of antiestrogen treatment; however, near half of ER-rich tumors prove to be endocrine resistant [25]. In ER positive breast cancers, ESR1 gene amplification and point mutation are the supposed causal factors for increased aggressivity and endocrine resistance of tumors [96]. In reality, mutational changes of ESR1 gene are desperate efforts counteracting the endocrine disruptor therapy so as to save estrogen signaling in the absence of estrogen [28].
Various studies have published different ESR1 amplification frequencies in breast cancers ranging from 0% to 75 %. [77]. These various results show different capacities of tumors for the genome repairing activation of estrogen signaling. Recently, in tamoxifen responsive early stage breast cancers, focal ESR1 gene amplification was a powerful predictor for long term tumor free survival of patients [97]. These results suggest that in the early stage of tumor, somatic mutations of ESR1 gene may effectively facilitate genomic stabilization. Conversely, in advanced breast cancers, even extensive ESR1 gene mutation and ER protein modification are incapable of counteracting the excessive genomic damage.
In metastatic breast cancers, specific ESR1 mutations were identified inducing estrogen independent activation of ERs. These mutations led to constitutive activation of ERs and reduced sensitivity to ER antagonists [98]. Authors suggested the development of new ER antagonists with appropriate efficacy against certain ESR1 mutants. In reality, the development of estrogen independent ER activation in tumors is an ultimate refuge against the exhaustive endocrine disruptor treatment, rather than pro-oncogenic alteration.
Early diagnosis and treatment of ER positive breast cancer does not ensure long term tumor free survival for patients [5]. Tamoxifen treatment of early ER-positive tumors could result in late tumor recurrence after 10-15 years [99]. These findings highlight that antiestrogen therapy is not a right routine against the targeted ER positive breast cancers. The source of tumor recurrence is a persistent genomic instability of the female breast rather than survival of residual tumor cells. Both endocrine treatment and chemotherapy further deteriorate the genomic defect in the targeted breast tissue helping new tumor initiation.
Luminal B subtype of breast cancer shows some dedifferentiation and the disease has worse prognosis as compared with luminal A type tumors. They exhibit decreased expression of ER alpha and PR and in some cases a lack of PR may be observed in association with the declining estrogen signal [100]. In certain luminal B tumors, somatic mutations of TP53 and HER2 expression may also be experienced [101]. In these tumors, somatic TP53 mutations are not cancer driver alterations, but rather they provide an additional DNA safeguarding via changes in p53 protein. In luminal B cancers, increasing genomic damage induces HER2 expression strengthening ER activation via unliganded pathway [24].
Tamoxifen therapy in women with ER positive, PR negative and HER2 positive tumors resulted in more frequent tumor recurrence and higher mortality rate compared to patients without tamoxifen treatment [102]. This experience justifies that the declining ER signal in type B breast cancers is further damaged by the ER blockade. Conversely, against ER positive, PR negative luminal B type tumors, natural estrogen (Premarin) therapy achieved significant tumor regression and improved the survival of patients via genome stabilization [103].
ER/HER2 co-expression may presumably disturb responses to both anti-HER2–directed and endocrine therapy due to crosstalk between ER and HER2 pathways. For type B breast cancers that are both ER and HER2 positive, a combined HER2/ER blockade was recommended as an effective treatment strategy [104]. This double blockade on HER2 and ER may be catastrophic for patients as in B-type tumors these regulatory pathways together provide restoring the altered ER signaling and genomic defects.
In HER2-enriched subtype of breast cancer, the lack of ER/PR expression and overexpression of HER2 are characteristic findings. HER2-enriched breast tumors show faster growth than luminal types and patients have poorer prognosis. Loss of ER and PR expression in HER2 enriched tumors reflect the failure of estrogen signaling and serious errors in genomic functions [24]. In ER/PR negative breast cancers, HER2 overexpression is erroneously taken for a stimulator of tumor growth, similarly like increased expression of other growth factor receptors [93]. In reality, cognition of DNA damage promotes HER2 overexpression as an adaptive response serving compensatory unliganded ER activation, even when ERs are not detectable [24]. Therapies, targeting HER2 protein in these tumor types achieve ambiguous results as only a successful counteraction may produce transient tumor response in the minority of cases [28].
Genomic analysis on HER2-enriched breast cancer revealed higher expression of ERBB3 gene, while lower expression of ESR1 gene compared to the non HER2 enriched subtype [105]. These findings are concordant with the compensatory increased expression of HER2 protein and the apparently missing expression of ERs in HER2 enriched breast cancer subtype.
Triple-negative or basal-like subtype of breast cancer is characterized by the lack of ER, PR and HER2. Triple-negative breast cancer (TNBC) is frequently associated with germline gene mutation, genomic instability and defective estrogen signaling [41]. TNBC type breast cancers exhibit low grade differentiation and they are more aggressive than any other breast cancer subtype.
In TNBC type tumors, the missing estrogen- progesterone- and HER-2 receptors reflect a severe damage of the whole genome. TNBCs clinically exhibit rapid growth and poor prognosis. Self directed DNA repair is impossible for TNBCs as ERs seem to be absent and the liganded and non liganded activation of ERs are missing [41]. Development of a TNBC type tumor in women indicates a seriously defective estrogen signaling. Increased prevalence of TNBCs among black American women may be associated with their light deficiency associated hormonal disorders as dark pigmentation, is incongruent with a light deficient northern milieu. [38].
Basal type hormone receptor negative and TNBC type breast cancers with serious genomic damage are regarded as being refractory to antiestrogen therapy. Chemotherapy remains the standard for TNBC treatment; however, new drug delivery methods are compulsory as the signaling pathways within these tumors are not clarified [95]. Since hormone receptor negative breast tumors are “immune hot” showing strong inflammatory infiltration, immune checkpoint inhibitors (ICPis) were introduced targeting the presumably pro-oncogenic immune competent cells [106]. Despite the promising results of IPCi therapy, these drugs may induce immune-related endocrine dysfunction that could lead life threatening complications. Authors suggest continuing the IPCi therapy as the adverse endocrine complications may be treated with hormone replacement.
In conclusion, molecular classification of breast tumor subtypes is a mirror reflecting the defect of estrogen signaling and genomic damage in cancer patients. In women, robust estrogen signaling may repress breast cancer initiation and the accidentally developing tumors are highly ER positive in these cases. By contrast, in women with a weak estrogen signaling, the associated genomic instability liberates breast cancer development and their tumors are predominantly aggressive, hormone receptor negative or triple negative breast cancers.
Dynamic Communication between Breast Cancers and Their Microenvironment during Anticancer Fight
From the 2000s, the microenvironment of cancers is taken for essential participant in tumor growth and aggressive metastatic extension [107]. According to recent aspect, cancer is a combined lesion comprising a tumor lump and an altered cellular microenvironment [108,109]. Tumor and cellular infiltration of microenvironment exhibit an active communication mistakenly suggesting collaboration serving unrestrained tumor invasion as well as escape from immune reactions and anticancer therapies.
Highly elevated expression of certain regulatory proteins and signaling molecules in cancers and in their neighboring cellular environment are mistakenly regarded as pro-oncogenic factors strengthening the concept of pro-tumorigenic conspiration [109,110,111]. Moreover, when genes having role in genome stabilization are amplified, or altered by mutation, they are regarded as pro-oncogenic changes instead of self directed labors for genomic repair [96,112,113,114,115]. In breast cancers, the upregulation of estrogen synthesis and the ER activation via various pathways are taken for crucial conditions helping tumor growth. Conversely, in cancers, intensifying signaling pathways and the accumulation of somatic mutations do not product cancer driver factors, but rather they facilitate estrogen signaling, DNA repair and apoptotic death [81].
In case of solid tumors, cancer associated fibroblasts (CAFs) are the major players of tumor microenvironment [108]. In the peritumoral cellular infiltration, CAFs and all kinds of immune proficient cells are in mutual connection with tumor cells [109]. Membrane bordered extracellular vesicles (EVs) are carrying intercellular messages comprising different signaling molecules, regulatory proteins and nucleotide templates. Intercellular communication between tumors and their microenvironment are mistakenly regarded as help for tumor growth and invasion.
CAF secretome frequently comprises growth factors and growth factor receptors. Growth factor signaling cascade is regarded as pro-tumorigenic stimulus upregulating tumor growth and invasion [116], while this regulatory pathway confers possibility for unliganded ER activation.
Cytokine secretion of CAFs, monocytes and macrophages regulates the inflammatory and immunological reactions in the peritumoral region [117]. Pro-inflammatory cytokines recruit inflammatory immune competent cells and activate aromatase expression leading to increased estrogen synthesis [118]. Appropriate estrogen concentration is not a cancer driver factor, but rather it orchestrates the anticancer combat of immune competent cells. When the fight was successful, anti-inflammatory cytokines alleviate inflammatory response and allow decreasing estrogen concentration [119].
Numerous tumors induce increased aromatase synthesis in both tumor cells and peritumoral stroma via high proinflammatory cytokine secretion [120]. In breast cancers, abundant expression of aromatase was observed in tumor cells, in fibrous cells and in adjacent adipocytes suggesting a pro-carcinogenic activity of increased estrogen synthesis [121]. Conversely, a parallel clinical and genetic investigation on breast cancer cases justified significant correlation between missing aromatase level in surgically removed tumors and high local recurrence rate [87]. In conclusion, there is no causal correlation between high estrogen concentration and rapid tumor growth, but rather the lack of estrogen production in tumors is linked with poor prognosis of the disease.
Recently, mammary adipocytes are particularly blamed for the growth and invasion of breast cancer, since female breast comprises abundant fatty tissue. Cancer associated adipocytes (CAAs) are specific players in the microenvironment of breast tumors presumably helping progression and metastatic spread [122]. Activated CAAs show dedifferentiation and their copious secretome comprises different cytokines and adipokines. CAAs comprise tiny lipid droplets serving the rapid energy supply of adjacent tumor cells. They participate in remodeling the extracellular matrix, increasin aromatase expression and modulating the immune cell functions. In reality, activated CAAs serve the anticancer fight via adipokine secretion, energy supply and regulatory commands for all neighboring cells similarly, like activated CAFs.
In summary, cancers and their peritumoral cellular infiltration are allies in the combat against DNA damage and uncontrolled proliferation of tumor. The graver the DNA damage in tumors, the stronger is the cellular infiltration of microenvironment. The aim is the restoration of DNA stability compelling apoptotic death. Intensive peritumoral cellular infiltration coupled with invasive tumor growth may not be regarded as a victory of conspirator partners, but rather it is a collective defeat of cancer and its microenvironment.
Correlations between Breast Cancer Subtypes and the Characteristics of Their Cellular Microenvironment
Recently, correlations between the receptor status of breast cancers and peritumoral inflammatory reaction are thoroughly investigated. Abundant immune cell infiltration was experienced around “immune hot” hormone receptor negative breast cancers with a predominance of B cells, Th1 T cells, and cytotoxic T lymphocytes (CTLs), while ER-positive cancers proved to be immune cold [123].
Extensive analysis was conducted on the features of tumor microenvironment in each breast cancer subtypes [124]. Basal-like and HER2 enriched tumors were associated with high immune scores expressing most immune regulatory targets and abundant immune cell infiltration. These poorly differentiated breast cancer subtypes could be defined as “immune hot” tumors (Figure 1.)
In contrast, luminal A and luminal B subtypes showing ER expression were associated with low immune scores and weak immune cell infiltration suggesting that these subtypes may be regarded as “immune cold” cancers [124]. Highly differentiated ER-positive tumors do not require strong immune cell support for their anticancer fight as cancer associated fibroblasts (CAFs) and cancer associated adipocytes (CAAs) are capable of cytokine secretion facilitating aromatase expression and estrogen synthesis. Estrogen activation on abundant ERs upregulates estrogen signaling and DNA repair in ER-positive tumors without dense inflammatory reaction [Figure 2.].
In ER-positive breast cancer cases, gene expression analysis revealed that aromatase inhibitor (letrozole) treatment persistently increases the density of immune cells around tumors comprising subsets of B cells and T helper lymphocytes [110]. This observation underlines that inhibition of estrogen signaling is an emergency state even for tumors. In ER-positive “immune cold” breast cancers, letrozole attack against estrogen regulation caused a rapid recruiting of dense immune cell infiltration and copious cytokine secretion upregulating aromatase expression and estrogen synthesis.
In conclusion, hormone receptor positive tumors are capable of fighting for increased aromatase expression and estrogen synthesis with the assistance of bordering CAFs and CAMs aiming genomic repair. By contrast, hormone receptor negative and TNBC type cancers, as well as tumors exhaustively treated by antiestrogens, are in emergency condition requiring the help of immune competent cells.
Estrogen Prevention and Therapy of Breast Cancer
Experiments on carcinogen induced mammary tumor models justified that pregnancy, either before or soon after exposure to a chemical carcinogen proved to be highly protective against breast cancer development in rodents [125,126,127]. Short term treatment with high, pregnancy mimicking levels of estradiol with or without progesterone also was highly protective against mammary carcinogenesis in rodents [128,129]. Synthetic estrogen (ethinylestradiol) plus synthetic progesterone (megesterol acetate) treatment for 3 weeks resulted in significantly lower mammary cancer incidence in rats as compared with untreated controls after 6 months of the exposure of chemical carcinogen [130].
The mechanism of breast cancer preventive hormonal activity was examined in genetically challenged mouse models [131]. High dose estrogen/progesterone treatment reduced the incidence of mammary tumors by more than 60% in mice with oncogenic overexpression of the HER2/neu. Considering that growth factor overexpression is not oncogenic action but rather an unliganded activation of weak, E2-refractory ERs, estrogen treatment helps ER activation and genome stabilization [24]. Moreover, in mice with homozygous deletions of Tp53 gene, exogenous estrogen/progesterone treatment reduced mammary tumor development by at least 70% [131]. These results justify that hormone-mediated protection of breast tissue may also have altering pathways independent of p53 protein activation [132].
In clinical practice, parity reduces breast cancer risk even among germline BRCA1/2 mutation carrier women [133]. Sky-high estrogen level in pregnancy drives the genome stabilizer circuit and the increased expression of estrogen regulated genes compensates the weakness of genome safeguarding BRCA proteins [50].
Hormone induced breast cancer prevention experienced in animal studies was not similarly successful in the human practice. In MHT studies, the application of endocrine disruptor synthetic estrogens and synthetic progestins resulted in deregulation of ERs leading to increased risk for thromboembolic complications and breast cancer [56]. Moreover, in breast cancer cases, high dose synthetic estrogen treatment resulted in modest tumor regression and high toxicity [18]. Using Premarin in high doses, seemed to be risky in human practice. In contrast, the endocrine disruptor ethinylestradiol was regarded as a bioidentical hormone appropriate for human therapy even in high doses.
WHI investigators published horse urine derived CEE (Premarin) alone in a great prospective, placebo controlled MHT study and a shocking breast cancer preventive effect was published affecting the hormone treated group [55]. This investigation was repeated several times on the participating women remaining alive. Long term genome stabilizer effect of Premarin was justified by the decreased breast cancer incidence in the hormone treated group even after 16 years [59].
In patients with ER-positive, PR-negative luminal B type tumor, Premarin treatment induced a significant reduction of cancer growth and decreased tumor associated mortality [103]. In contrast, worsening results of tamoxifen therapy were experienced on ER/HER2-positive luminal B type tumors as compared with the untreated controls [102].
In HER2 overexpressed, apparently hormone receptor negative tumors, E2 refractory ERs occur in the background as the activated HER2 an kinase cascade pathways serve increased unliganded ER activation. High dose estrogen treatment may upregulate the activation and expression of hidden E2-resistant ERs driving the genome stabilizer circuit [134]. At the same time, high dose estrogen silences the peritumoral immune cell infiltration as an appropriate estrogen concentration facilitates the beneficial anticancer effects of immune competent cells.
The conviction that TNBC is completely hormone-independent tumor is quite incorrect. Although, TNBCs are apparently deficient in both hormone receptors and growth factor receptors, some hidden components of the liganded or unliganded pathway of ER activation may arise in them. Interestingly, 5-10% of the ER-negative breast cancers have shown response to tamoxifen treatment [135]. In a subtype of TNBCs, a specific isoform of estrogen receptor-alpha (ER-α36) was observed. Icaritin, a prenylflavonoid derivate affected ER-α36-mediated pathways and tumor growth showing a possibility for the development of a novel therapeutic agent against TNBC.
In some primary TNBC cases, arising ER, PR or HER2 expression were observed in the metastatic lesions [136]. In a systematic review and meta-analysis, average percentages of negative to positive receptor conversion in metastatic tumors were 21.5% for ERs, 15.9% for PRs and 9.5% for HER2s. Among patients with ER negative primary tumors, conversion to a positive ER status in their metastatic lesion was associated with a prolonged survival compared to those without conversion in their metastasis [137]. Appearance of ERs in the metastatic lesion of TNBC increases the possibility of successful high dose estrogen therapy.
Tumors, exhaustively treated with tamoxifen, the achieved ER blockade may be regarded as an artificially created ER negative status as estrogen signaling suffered an irreparable damage. Among patients with tamoxifen resistant advanced breast cancer, estrogen treatment dramatically decreased breast cancer related mortality [138]. In tumors, with tamoxifen blocked ERs, estrogen treatment induces abundant new ER expression and drives the genome stabilization. In patients with aromatase inhibitor resistant tumors, estrogen treatment induced regression of metastatic cancers and extended the survival [139]. In tumors exhaustively treated with aromatase inhibitor, therapeutic estrogen is bound by the overexpressed ERs driving the genome stabilization circuit. These findings help to reevaluate the belief of estrogen induced breast cancer and the role of antiestrogens in breast cancer therapy [140].
Medical stimulation of ER protein expression would be a promising new method for the therapy of ER negative and TNBC type tumors. Receptor negative breast cancer cell line was transfected with exogenous estrogen receptor and the following estrogen treatment reduced the proliferative and metastatic capacity of cancer cells [141]. This experiment justified that induction of ER expression in ER-negative cancers may increase their vulnerability to estrogen therapy.
In 1989, results of a milestone experiment were published on the induction of protein synthesis in cells by transfecting them with exogenous mRNA template. The expression of an appropriate protein was stimulated via translation. [142]. Later, artificially synthesized mRNA was injected into the muscle of mice as a direct gene transfer so as to generate the expression of the most wanted muscular protein [143]. Authors recommended the use of mRNA technology for vaccination against pathogenic microbes. These experiments provided the earliest trials towards the development of mRNA vaccination during the outbreak of COVID-19 epidemic [144].
Beyond vaccination, the mRNA technology may have enormous potential in medical practice. Malone’s technology is an appropriate method for inducing expressions of various transcriptional factors or enzymes in patients via a direct gene transfer technique. In genetically challenged women with decreased ER expression and/or E2-refractory ERs, the facilitation of ER production via ESR1 mRNA treatment increases the expression of estrogen regulated genes preventing the development of cancer in the breasts and ovaries.
Preoperative ESR1 mRNA therapy in cases with advanced stage of ER negative or TNBC kind breast cancer may result in an obvious tumor response coupled with stimulated immune competent cells in the neighboring tissues. In the postoperative period, local ESR1 mRNA therapy and the associated ER expression improves all genomic functions in the residual breast tissue inhibiting cancer recurrence.
In conclusion, estrogen treatment is the adequate therapy of ER positive breast tumors, whereas high estrogen doses may be efficient even against ER negative breast cancers. In the future, the medical motivation of ER expression would be an excellent cure and secondary prevention for breast cancer patients with inherited or acquired defects of ERs.
Conclusions
Breast cancer care developed through centuries from estrogen withdrawal by surgical oophorectomy to the current use of radiological and chemical targeting of estrogen signaling. There were major inventions providing possibilities for the evaluation of estrogen’s great role in human health, while at the same time unfortunate failures and misunderstandings distracted breast cancer research from the right way.
The therapeutic use of estrogen withdrawal against breast cancer has been an erroneous route; however, the compensatory upregulation of estrogen signaling could achieve deceiving tumor responses in <30% of patients. Major mistakes may be established based on the therapeutic experiences seriously delaying the progress of both breast cancer care and overall cancer therapy.
The first, principal error is the therapeutic attack against the regulatory pathways of breast cancer cells supposing that tumor killing is the right way of recovery. In reality, cancer cell recognizes its genomic defect and shows adaptive responses so as to achieve DNA repair and apoptotic death. The therapeutic blockade of DNA damage responses in breast cancer strengthens genomic failures in both tumors and patients.
The second mistake is evaluating a tumor response rate under 30% as a therapeutic success of endocrine disruptor treatment. This modest response rate may be attributed to the counteraction of breast cancer against genotoxic treatment; however, in the majority of cases, the genome defending efforts of tumors remain unsuccessful.
The third mistake is the establishment of tumor resistance in case of therapeutic failures. There is no resistance against genotoxic therapy, but rather tumors may be incapable of counteracting the excessive genomic damage caused by endocrine disruptor therapy. In cancers refractory to endocrine treatment, the genomic regulation breaks down leading to unrestrained proliferation.
Chemotherapy, radiotherapy and excessive mutilation are methods for radical killing even the last tumor cell, mistakenly believing that residual tumor cells cause tumor recurrence after years or decades. In reality, in cancer patients, the persisting genomic instability causes new tumor initiation in their highly vulnerable organs. The genome damaging and immune blocking modern therapies assist the recurrence of tumors even after a longer period of recovery.
Breast cancer cells are capable of cognition the crisis of genomic damage and exhibit adaptive rectifying responses via their genomic plasticity. This hard labor is generally unsuccessful without medical supports of genomic stability and immune reactions. Understanding the efforts for DNA repair in breast cancer cells requires a turn in tumor therapy; we should help the genome stabilizer responses of breast tumors and the immune system, rather than provoking additional genomic damages.
Conflicts of Interest
The author declares no conflict of interest.
References
- Wilkinson, L.; Gathani, T. Understanding breast cancer as a global health concern. Br J Radiol. 2022, 95, 20211033. [Google Scholar] [CrossRef]
- Heer, E.; Harper, A.; Escandor, N.; Sung, H.; McCormack, V.; et al. Global burden and trends in premenopausal and postmenopausal breast cancer: A population-based study. The Lancet Global Health 2020, 8, e1027–e1037. [Google Scholar] [CrossRef]
- Huang, J.; Chan, P.S.F.; Lok, V.; Chen, X.; Ding, H.; Jin, Y.; et al. Global incidence and mortality of breast cancer: A trend analysis. Aging 2021, 13, 5748–5803. [Google Scholar] [CrossRef]
- Narod, S.A.; Iqbal, J.; Giannakeas, V.; Sopik, V.; Sun, P. Breast cancer mortality after a diagnosis of ductal carcinoma in situ. JAMA Oncol 2015, 1, 888–896. [Google Scholar] [CrossRef]
- Esserman, L.; Yau, C. Rethinking the standard for ductal carcinoma in situ treatment. JAMA Oncol. 2015, 1, 881–883. [Google Scholar] [CrossRef]
- Beatson, G.T. On the treatment of inoperable cases of carcinoma of the mamma: Suggestions for a new method of treatment, with illustrative cases. Lancet 1986, 2, 104–107. [Google Scholar]
- Boyd, S. On oophorectomy in cancer of the breast. BMJ 1900, 2, 1161–1187. [Google Scholar] [CrossRef]
- Jensen, E.V.; Jacobson, H.I. Biological Activities of Steroids in Relation to Cancer; Pincus, G., Vollmer, E.P., Eds.; Academic Press: New York, 1960; p. 161. [Google Scholar]
- Liehr, J.G. Genotoxic effects of estrogens. Mutat Res. 1990, 238, 269–276. [Google Scholar] [CrossRef]
- Yager, D.J. Endogenous estrogens as carcinogens through metabolic activation. Natl Cancer Inst Monogr. 2000, 27, 67–73. [Google Scholar] [CrossRef]
- Cavalieri, E.; Rogan, E. Catechol quinones of estrogens in the initiation of breast, prostate, and other human cancers: Keynote lecture. Ann N Y Acad Sci. 2006, 1089, 286–301. [Google Scholar] [CrossRef]
- Russo, J.; Russo, I.H. The role of estrogen in the initiation of breast cancer. J Steroid Biochem Mol Biol 2006, 102, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Hemsell, D.L.; Grodin, J.M.; Brenner, P.F.; Siiteri, P.K.; MacDonald, P.C. Plasma precursors of estrogen. II. Correlation of the extent of conversion of plasma androstenedione to estrone with age. The Journal of Clinical Endocrinology and Metabolism. 1974, 38, 476–479. [Google Scholar] [CrossRef] [PubMed]
- Mahboobifard, F.; Pourgholami, M.H.; Jorjani, M.; Dargahi, L.; et al. Estrogen as a key regulator of energy homeostasis and metabolic health. Biomed Pharmacother 2022, 156, 113808. [Google Scholar] [CrossRef] [PubMed]
- Simpson, E.R.; Mahendroo, M.S.; Nichols, J.E.; Bulun, S.E. Aromatase gene expression in adipose tissue: Relationship to breast cancer. Int J Fertil Menopausal Stud. 1994, 39 (Suppl. S2), 75–83. [Google Scholar] [PubMed]
- Stefanick, M.L. Estrogens and progestins: Background and history, trends in use, and guidelines and regimens approved by the US Food and Drug Administration. Am J Med 2005, 118 (Suppl. S12), 64–73. [Google Scholar] [CrossRef] [PubMed]
- Rossouw, J.E.; Anderson, G.L.; Prentice, R.L.; et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: Principal results from the Women’s Health Initiative randomized controlled trial. JAMA 2002, 288, 321–333. [Google Scholar] [PubMed]
- Coelingh-Bennink, H.J.; Verhoeven, C.; Dutman, A.E.; Thijssen, J. The use of high-dose estrogens for the treatment of breast cancer. Maturitas 2017, 95, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Lidegaard, Ø.; Løkkegaard, E.; Jensen, A.; Skovlund, C.W.; Keiding, N.; et al. Thrombotic stroke and myocardial infarction with hormonal contraception. N Engl J Med 2012, 366, 2257–2266. [Google Scholar] [CrossRef] [PubMed]
- Mørch, L.S.; Skovlund, C.W.; Hannaford, P.C.; Iversen, L.; Fielding, S.; Lidegaard, Ø. Contemporary Hormonal Contraception and the Risk of Breast Cancer. N Engl J Med 2017, 377, 2228–2239. [Google Scholar] [CrossRef]
- Cortés, M.E.; Alfaro, A.A. The effects of hormonal contraceptives on glycemic regulation. Linacre Q 2014, 81, 209–218. [Google Scholar] [CrossRef]
- Hilakivi-Clarke, L.; de Assis, S.; Warri, A. Exposures to Synthetic Estrogens at Different Times During the Life, and Their Effect on Breast Cancer Risk. J Mammary Gland Biol Neoplasia. 2013, 18, 25–42. [Google Scholar] [CrossRef]
- Bentrem, D.J.; Jordan, V.C. Role of antiestrogens and aromatase inhibitors in breast cancer treatment. Curr Opin Obstet Gynecol. 2002, 14, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Suba, Z. Amplified crosstalk between estrogen binding and GFR signaling mediated pathways of ER activation drives responses in tumors treated with endocrine disruptors. Recent Pat Anticancer Drug Discov 2018, 13, 428–444. [Google Scholar] [CrossRef]
- Hayes, D.F. Tamoxifen: dr. Jekyll and mr. Hyde? J Natl Cancer Inst 2004, 96, 895–897. [Google Scholar] [CrossRef] [PubMed]
- Osborne, C.K.; Schiff, R. Mechanisms of endocrine resistance in breast cancer. Annu Rev Med. 2011, 62, 233–247. [Google Scholar] [CrossRef]
- Massarweh, S.; Osborne, C.K.; Creighton, C.J.; Qin, L.; Tsimelzon, A.; Huang, S.; Weiss, H.; Rimawi, M.; Schiff, R. Tamoxifen resistance in breast tumors is driven by growth factor receptor signaling with repression of classic estrogen receptor genomic function. Cancer Res. 2008, 68, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Suba, Z. Compensatory estrogen signal is capable of DNA repair in antiestrogen-responsive cancer cells via activating mutations. J Oncol 2020, 2020, 5418365. [Google Scholar] [CrossRef] [PubMed]
- Pujol, P.; Galtier-Dereure, F.; Bringer, J. Obesity and breast cancer risk. Human Reproduction 1997, 12, 116–125. [Google Scholar] [CrossRef]
- García-Estévez, L.; Cortés, J.; Pérez, S.; Calvo, I.; Gallegeos, I.; Moreno-Bueno, G. Obesity and Breast Cancer: A Paradoxical and Controversial Relationship Influenced by Menopausal Status. Front Oncol. 2021, 11, 705911. [Google Scholar] [CrossRef]
- Suba, Z. Circulatory Estrogen Level Protects against Breast Cancer in Obese Women. Recent Patents Anti-Cancer Drug Discov 2013, 8, 154–167. [Google Scholar] [CrossRef]
- Bruning, P.F.; Bonfrèr, J.M.G.; van Noord, P.A.H.; Hart, A.A.M.; et al. Insulin resistance and breast-cancer risk. Int J Cancer 1992, 52, 511–516. [Google Scholar] [CrossRef]
- Rose, D.P.; Vona-Davis, L. The cellular and molecular mechanisms by which insulin influences breast cancer risk and progression. Endocrine-Related Cancer 2012, 19, R225–R241. [Google Scholar] [CrossRef] [PubMed]
- Suba, Z. Interplay between insulin resistance and estrogen deficiency as coactivators in carcinogenesis. Pathol Oncol Res 2012, 18, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Suba, Z. Low estrogen exposure and/or defective estrogen signaling induces disturbances in glucose uptake and energy expenditure. J Diabet Metab 2013, 4, 272–281. [Google Scholar] [CrossRef]
- Amend, K.; Hicks, D.; Ambrosone, C.B. Breast cancer in AfricanAmerican women: Differences in tumor biology from EuropeanAmerican women. Cancer Res 2006, 66, 8327–8330. [Google Scholar] [CrossRef] [PubMed]
- Amirikia, K.C.; Mills, P.; Bush, J.; Newman, L.A. Higher populationbased incidence rates of triple-negative breast cancer among young African-American women: Implications for breast cancer screening recommendations. Cancer 2011, 117, 2747–2753. [Google Scholar] [CrossRef] [PubMed]
- Suba, Z. Light deficiency confers breast cancer risk by endocrine disorders. Recent Pat Anticancer Drug Discov. 2012, 7, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Yedjou, C.G.; Sims, J.N.; Miele, L.; Noubissi, F.; Lowe, L.; et al. Health and Racial Disparity in Breast Cancer. Adv Exp Med Biol. 2019, 1152, 31–49. [Google Scholar] [PubMed]
- Phipps, A.I.; Chlebowski, R.T.; Prentice, R.; McTiernan, A.; Stefanick, M.L.; Wactawski-Wende, J.; Kuller, L.H.; Adams-Campbell, L.L.; Lane, D.; Vitolins, M.; et al. Body size, physical activity, and risk of triple-negative and estrogen receptor-positive breast cancer. Cancer Epidemiol Biomarkers Prev 2011, 20, 454–463. [Google Scholar] [CrossRef]
- Suba, Z. Triple-negative breast cancer risk in women is defined by the defect of estrogen signaling: Preventive and therapeutic implications. Onco Targets Ther. 2014, 7, 147–164. [Google Scholar] [CrossRef]
- Miki, Y.; Swensen, J.; Shattuck-Eidens, D.; Futreal, P.A.; Harshman, K.; Tavtigian, S.; et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science 1994, 266, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Wooster, R.; Bignell, G.; Lancaster, J.; Swift, S.; Seal, S.; Mangion, J.; et al. Identification of the breast cancer susceptibility gene BRCA2. Nature 1995, 378, 789–792. [Google Scholar] [CrossRef] [PubMed]
- Gorski, J.J.; Kennedy, R.D.; Hosey, A.M.; Harkin, D.P. The complex relationship between BRCA1 and ERalpha in hereditary breast cancer. Clin Cancer Res 2009, 15, 1514–1518. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Di, L.J. BRCA1 and estrogen/estrogen receptor in breast cancer: Where they interact? Int J Biol Sci 2014, 10, 566–575. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Annab, L.A.; Afshari, C.A.; Lee, W.H.; Boyer, T.G. BRCA1 mediates ligand-independent transcriptional repression of the estrogen receptor. Proc Natl Acad Sci USA. 2001, 98, 9587–9592. [Google Scholar] [CrossRef] [PubMed]
- Chand, A.L.; Simpson, E.R.; Clyne, C.D. Aromatase expression is increased in BRCA1 mutation carriers. BMC Cancer 2009, 9, 148. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, S.R.; Van De Vijver, M.J.; Jacquemier, J.; et al. The pathology of familial breast cancer: Predictive value of immunohistochemical markers estrogen receptor, progesterone receptor, HER-2, and p53 in patients with mutations in BRCA1 and BRCA2. J Clin Oncol. 2002, 20, 2310–2318. [Google Scholar] [CrossRef] [PubMed]
- Sorlie, T.; Perou, C.M.; Tibshirani, R.; et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci U S A. 2001, 98, 10869–10874. [Google Scholar] [CrossRef]
- Suba, Z. DNA stabilization by the upregulation of estrogen signaling in BRCA gene mutation carriers. Drug Des Devel Ther 2015, 9, 2663–2675. [Google Scholar] [CrossRef]
- Suba, Z. DNA damage responses in tumors are not proliferative stimuli, but rather they are DNA repair actions requiring supportive medical care. Cancers 2024, 16, 1573. [Google Scholar] [CrossRef]
- Björnström, L.; Sjöberg, M. Mechanisms of estrogen receptor signaling: Convergence of genomic and nongenomic actions on target genes. Mol Endocrinol 2005, 19, 833–842. [Google Scholar] [CrossRef]
- Maggi, A. Liganded and unliganded activation of estrogen receptor and hormone replacement therapies. Biochim Biophys Acta 2011, 1812, 1054–1060. [Google Scholar] [CrossRef]
- Pescatori, S.; Berardinelli, F.; Albanesi, J.; Ascenzi, P.; et al. A Tale of Ice and Fire: The Dual Role for 17β-Estradiol in Balancing DNA Damage and Genome Integrity. Cancers 2021, 13, 1583. [Google Scholar] [CrossRef]
- Anderson, G.L.; Limacher, M.; Assaf, A.R.; et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: The Women’s Health Initiative randomized controlled trial. JAMA 2004, 291, 1701–1712. [Google Scholar]
- Suba, Z. Synthetic Estrogens Deregulate Estrogen Receptors Inducing Thromboembolic Complications and Cancer. In: Topics in Anti-Cancer Research. Vol. 8. Eds: Atta-ur-Rahman and Khurshid Zaman. Bentham Science Publishers 2019, Chapter 2, pp. 44–73. [CrossRef]
- LaCroix, A.Z.; Chlebowski, R.T.; Manson, J.E.; Aragaki, A.K.; Johnson, K.C.; Martin, L.; et al. Health Outcomes after Stopping Conjugated Equine Estrogens Among Postmenopausal Women with Prior Hysterectomy: A Randomized Controlled Trial. JAMA 2011, 305, 1305–1314. [Google Scholar] [CrossRef] [PubMed]
- Manson, J.E.; Chlebowski, R.T.; Stefanick, M.L.; Aragaki, A.K.; Rossouw, J.E.; Prentice, R.L.; et al. Menopausal Hormone Therapy and Health Outcomes during the Intervention and Extended Poststopping Phases of the Women’s Health Initiative Randomized Trials. JAMA 2013, 310, 1353–1368. [Google Scholar] [CrossRef] [PubMed]
- Chlebowski, R.T.; Anderson, G.L.; Aragaki, A.K.; Manson, J.E.; Stefanick, M.L.; Pan, K.; et al. Association of Menopausal Hormone Therapy with Breast Cancer Incidence and Mortality during Long-Term Follow-Up of the Women’s Health Initiative Randomized Clinical Trials. JAMA 2020, 324, 369–380. [Google Scholar] [CrossRef]
- Collaborative Group on Hormonal Factors in Breast Cancer. Type and timing of menopausal hormone therapy and breast cancer risk: Individual participant meta-analysis of the worldwide epidemiological evidence. Lancet 2019, 394, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Al-Shami, K.; Awadi, S.; Khamees, A.; Alsheikh, A.A.; Sumaiya Al-Sharif, S.; et al. Estrogens and the risk of breast cancer: A narrative review of literature. Heliyon 2023, 9, e20224. [Google Scholar] [CrossRef]
- Suba, Z. Gender-related hormonal risk factors for oral cancer. Pathol Oncol Res 2007, 13, 195–202. [Google Scholar] [CrossRef]
- Suba, Z. Common soil of smoking-associated and hormone-related cancers: Estrogen deficiency. Oncol Rev 2010, 4, 73–87. [Google Scholar] [CrossRef]
- McGuire, A.; Brown, J.A.L.; Malone, C.; McLaughlin, R.; Kerin, M.J. Effects of Age on the Detection and Management of Breast Cancer. Cancers 2015, 7, 908–929. [Google Scholar] [CrossRef]
- Kaaks, R.; Berrino, F.; Key, T.; Rinaldi, S.; Dossus, L.; Biessy, C.; Secreto, G.; et al. Serum Sex Steroids in Premenopausal Women and Breast Cancer Risk Within the European Prospective Investigation into Cancer and Nutrition (EPIC). J Natl Cancer Inst 2005, 97, 755–765. [Google Scholar] [CrossRef] [PubMed]
- Baglietto, L.; Severi, G.; English, D.R.; Krishnan, K.; Hopper, J.L.; McLean, C.; Morris, H.A.; Tilley, W.D.; Giles, G.G. Circulating steroid hormone levels and risk of breast cancer for postmenopausal women. Cancer Epidemiol Biomarkers Prev 2010, 19, 492–502. [Google Scholar] [CrossRef] [PubMed]
- Hartley, M.C.; McKinley, B.P.; Rogers, E.A.; Kalbaugh, C.A.; Messich, H.S.; Blackhurst, D.W.; Lokey, J.S.; Trocha, S.D. Differential expression of prognostic factors and effect on survival in young (< or =40) breast cancer patients: A case-control study. Am Surg 2006, 72, 1189–1194. [Google Scholar]
- Britt, K.; Ashworth, A.; Smalley, M. Pregnancy and the risk of breast cancer. Endocrine-Related Cancer 2007, 14, 907–933. [Google Scholar] [CrossRef]
- Papaioannou, S.; Tzafettas, J. Anovulation with or without PCO, hyperandrogenaemia and hyperinsulinaemia as promoters of endometrial and breast cancer. Best Practice Res Clin Obstet Gynaecol 2010, 24, 19–27. [Google Scholar] [CrossRef]
- Gleicher, N. Why are reproductive cancers more common in nulliparous women? Reprod Biomed Online 2013, 26, 416–419. [Google Scholar] [CrossRef]
- Talley, L.I.; Grizzle, W.E.; Waterbor, J.W.; Brown, D.; Weiss, H.; Frost, A.R. Hormone receptors and proliferation in breast carcinomas of equivalent histologic grades in pre- and postmenopausal women. Int J Cancer 2002, 98, 118–127. [Google Scholar] [CrossRef]
- Dolle, J.M.; Daling, J.R.; White, E.; Brinton, L.A.; Doody, D.R.; Porter, P.L.; Malone, K.E. Risk factors for triple-negative breast cancer in women under the age of 45 years. Cancer Epidemiol Biomarkers Prev 2009, 18, 1157–1166. [Google Scholar] [CrossRef]
- Suba, Z. Diverse pathomechanisms leading to the breakdown of cellular estrogen surveillance and breast cancer development: New therapeutic strategies. Drug Design Devel Ther 2014, 8, 1381–1390. [Google Scholar] [CrossRef] [PubMed]
- Suba, Z. Rosetta Stone for Cancer Cure: Comparison of the Anticancer Capacity of Endogenous Estrogens, Synthetic Estrogens and Antiestrogens. Oncol Rev 2023, 17, 10708. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Ruan, X.; Schultz, S.; Neubauer, H.; Fehm, T.; Seeger, H.; et al. Oestetrol stimulates proliferation and oestrogen receptor expression in breast cancer cell lines: Comparison of four oestrogens. Eur J Contracept Reprod Health Care 2015, 20, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Stoica, G.E.; Franke, T.F.; Moroni, M.; Mueller, S.; Morgan, E.; Iann, M.C.; et al. Effect of estradiol on estrogen receptor-alpha gene expression and activity can be modulated by the ErbB2/PI 3-K/Akt pathway. Oncogene 2003, 22, 7998–8011. [Google Scholar] [CrossRef] [PubMed]
- Holst, F.; Stahl, P.R.; Ruiz, C.; Hellwinkel, O.; Jehan, Z.; Wendland, M.; et al. Estrogen receptor alpha (ESR1) gene amplification is frequent in breast cancer. Nat Genet 2007, 39, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Tomita, S.; Abdalla, M.O.; Fujiwara, S.; Matsumori, H.; Maehara, K.; Ohkawa, Y.; et al. A cluster of noncoding RNAs activates the ESR1 locus during breast cancer adaptation. Nat Commun 2015, 6, 6966. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, P.; Wang, L.; Piao, H.L.; Ma, L. Long non-coding RNA HOTAIR in carcinogenesis and metastasis. Acta Biochim Biophys Sin (Shanghai) 2014, 46, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Bhan, A.; Mandal, S.S. Estradiol-Induced Transcriptional Regulation of Long Non-Coding RNA, HOTAIR. Methods Mol Biol 2016, 1366, 395–412. [Google Scholar] [PubMed]
- Suba, Z. Activating mutations of ESR1, BRCA1 and CYP19 aromatase genes confer tumor response in breast cancers treated with antiestrogens. Recent Pat Anticancer Drug Discov 2017, 12, 136–147. [Google Scholar] [CrossRef]
- Lu, L.; Zhu, G.; Zhang, C.; Deng, Q.; Katsaros, D.; Mayne, S.T.; et al. Association of large noncoding RNA HOTAIR expression and its downstream intergenic CpG island methylation with survival in breast cancer. Breast Cancer Res Treat 2012, 136, 875–883. [Google Scholar] [CrossRef]
- Kinoshita, Y.; Chen, S. Induction of aromatase (CYP19) expression in breast cancer cells through a nongenomic action of estrogen receptor alpha. Cancer Res 2003, 63, 3546–3555. [Google Scholar] [PubMed]
- Catalano, S.; Giordano, C.; Panza, S.; Chemi, F.; Bonofiglio, D.; Lanzino, M.; et al. Tamoxifen through GPER upregulates aromatase expression: A novel mechanism sustaining tamoxifen-resistant breast cancer cell growth. Breast Cancer Res Treat 2014, 146, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Sasano, H.; Miki, Y.; Nagasaki, S.; Suzuki, T. In situ estrogen production and its regulation in human breast carcinoma: From endocrinology to intracrinology. Pathology International 2009, 59, 777–789. [Google Scholar] [CrossRef] [PubMed]
- Evans, T.R.J.; Rowlands, M.G.; Silva, M.C.; Law, M.; Coombes, R.C. Prognostic significance of aromatase and estrone sulfatase enzymes in human breast cancer. J Steroid Biochem Mol Biol 1993, 44, 583–587. [Google Scholar] [CrossRef] [PubMed]
- Bollet, M.A.; Savignoni, A.; De Koning, L.; Tran-Perennou, C.; Barbaroux, C.; Degeorges, A.; et al. Tumor aromatase expression as a prognostic factor for local control in young breast cancer patients after breast-conserving treatment. Breast Cancer Res 2009, 11, R54. [Google Scholar] [CrossRef]
- Kininis, M.; Chen, B.S.; Diehl, A.G.; Isaacs, G.D.; Zhang, T.; Siepel, A.C.; et al. Genomic analyses of transcription factor binding, histone acetylation, and gene expression. Mol Cell Biol 2007, 27, 5090–5104. [Google Scholar] [CrossRef]
- Hosey, A.M.; Gorski, J.J.; Murray, M.M.; Quinn, J.E.; Chung, W.Y.; Stewart, G.E.; et al. Molecular basis for estrogen receptor alpha deficiency in BRCA1-linked breast cancer. J Natl Cancer Inst 2007, 99, 1683–1694. [Google Scholar] [CrossRef] [PubMed]
- Scherbakov, A.M.; Shestakova, E.A.; Galeeva, K.E.; et al. BRCA1 and Estrogen Receptor α Expression Regulation in Breast Cancer Cells. Mol Biol 2019, 53, 442–451. [Google Scholar] [CrossRef]
- Mauro, L.; Salerno, M.; Panno, M.L.; Bellizzi, D.; Sisci, D.; Miglietta, A.; et al. Estradiol increases IRS-1 gene expression and insulin signaling in breast cancer cells. Biochem Biophys Res Commun. 2001, 288, 685–689. [Google Scholar] [CrossRef]
- Garrido, P.; Morán, J.; Alonso, A.; González, S.; González, C. 17β-estradiol activates glucose uptake via GLUT4 translocation and PI3K/Akt signaling pathway in MCF-7 cells. Endocrinology 2013, 154, 1979–8. [Google Scholar] [CrossRef]
- Clusan, L.; Ferrière, F.; Flouriot, G.; Pakdel, F. A Basic Review on Estrogen Receptor Signaling Pathways in Breast Cancer. Int J Mol Sci 2023, 24, 6834. [Google Scholar] [CrossRef] [PubMed]
- Perou, C.M.; Sørlie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular Portraits of Human Breast Tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Mandapati, A.; Lukong, K.E. Triple negative breast cancer: Approved treatment options and their mechanisms of action. J Cancer Res Clin Oncol 2023, 149, 3701–3719. [Google Scholar] [CrossRef] [PubMed]
- Lei, J.T.; Gou, X.; Seker, S.; Ellis, M.J. ESR1 alterations and metastasis in estrogen receptor positive breast cancer. J Cancer Metastasis Treat. 2019, 5, 38. [Google Scholar] [CrossRef] [PubMed]
- Singer, C.F.; Holst, F.; Steurer, S.; Eike, C.; Burandt, E.C.; Lax, S.F.; et al. Estrogen Receptor Alpha Gene Amplification Is an Independent Predictor of Long-Term Outcome in Postmenopausal Patients with Endocrine-Responsive Early Breast Cancer. Clin Cancer Res. 2022, 28, 4112–4120. [Google Scholar] [CrossRef] [PubMed]
- Toy, W.; Weir, H.; Razavi, P.; Lawson, M.; Goeppert, A.U.; Mazzola, A.M.; Smith, A.; Wilson, J.; et al. Activating ESR1 Mutations Differentially Affect the Efficacy of ER Antagonists. Cancer Discov 2017, 7, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Munzone, E.; Colleoni, M. Optimal management of luminal breast cancer: How much endocrine therapy is long enough? Ther Adv Med Oncol. 2018, 10, 1758835918777437. [Google Scholar] [CrossRef] [PubMed]
- Arpino, G.; Weiss, H.; Lee, A.V.; Schiff, R.; De Placido, S.; Osborne, C.K.; et al. Estrogen receptor-positive, progesterone receptor-negative breast cancer: Association with growth factor receptor expression and tamoxifen resistance. J Natl Cancer Inst 2005, 97, 1254–1261. [Google Scholar] [CrossRef] [PubMed]
- Parker, J.S.; Mullins, M.; Cheang, M.C.U.; Leung, V.D.; Vickery, T.; Davies, S.; Fauron, C.; He, X.; Hu, Z.; et al. Supervised Risk Predictor of Breast Cancer Based on Intrinsic Subtypes. J Clin Oncol Off J Am Soc Clin Oncol 2009, 27, 1160–1167. [Google Scholar] [CrossRef]
- Rouanet, P.; Roger, P.; Rousseau, E.; Thibault, S.; Romieu, G.; et al. HER2 overexpression a major risk factor for recurrence in pT1a-bN0M0 breast cancer: Results from a French regional cohort. Cancer Med. 2014, 3, 134–142. [Google Scholar] [CrossRef]
- Chlebowski, R.T.; Aragaki, A.K.; Pan, K. Breast Cancer Prevention: Time for Change. JCO Oncol Pract 2021, 17, 709–716. [Google Scholar] [CrossRef] [PubMed]
- Pegram, M.; Jackisch, C.; Johnston, S.R.D. Estrogen/HER2 receptor crosstalk in breast cancer: Combination therapies to improve outcomes for patients with hormone receptor-positive/HER2-positive breast cancer. npj Breast Cancer 2023, 9, 45. [Google Scholar] [CrossRef] [PubMed]
- Ju, J.; Du, F.; Gao, S.L.; Si, Y.R.; Hu, N.L.; Liu, D.X. Combined analysis of receptor expression reflects inter-and intra-tumor heterogeneity in HR+/HER2+ breast cancer. Breast Cancer Research and Treatment 2022, 194, 221–230. [Google Scholar] [CrossRef]
- Deligiannis, N.G.; Sosa, S.; Danilowicz, K.; Rizzo, L.F. Endocrine dysfunction induced by immune checkpoint inhibitors. Medicina (B Aires) 2021, 81, 269–278. [Google Scholar] [PubMed]
- Chew, V.; Toh, H.; Abastado, J. Immune Microenvironment in Tumor Progression: Characteristics and Challenges for Therapy. Journal of Oncology 2012, 2012, 608406. [Google Scholar] [CrossRef]
- Wang, Q.; Shao, X.; Zhang, Y.; Zhu, M.; Wang, F.X.C.; et al. Role of tumor microenvironment in cancer progression and therapeutic strategy. Cancer Med. 2023, 12, 11149–11165. [Google Scholar] [CrossRef] [PubMed]
- Linares, J.; Marín-Jiménez, J.A.; Badia-Ramentol, J.; Calon, A. Determinants and Functions of CAFs Secretome during Cancer progression and Therapy. Front Cell Dev Biol 2021, 8, 621070. [Google Scholar] [CrossRef]
- Mantovani, A.; Allavena, P.; Marchesi, F.; Garlanda, C. Macrophages as tools and targets in cancer therapy. Nat Rev Drug Discov 2022, 21, 799–820. [Google Scholar] [CrossRef]
- Chen, Y.; McAndrews, K.M.; Kalluri, R. Clinical and therapeutic relevance of cancer-associated fibroblasts. Nat Rev Clin Oncol 2021, 18, 792–804. [Google Scholar] [CrossRef]
- Pejerrey, S.M.; Dustin, D.; Kim, J.A.; Gu, G.; Rechoum, Y.; et al. The impact of ESR1 mutations on the treatment of metastatic breast cancer. Horm Cancer 2018, 9, 215–228. [Google Scholar] [CrossRef]
- Caizzi, L.; Ferrero, G.; Cutrupi, S.; Cordero, F.; Ballaré, C.; Miano, V.; et al. Genome-wide activity of unliganded estrogen receptor-α in breast cancer cells. Proc Natl Acad Sci USA 2014, 111, 4892–4897. [Google Scholar] [CrossRef] [PubMed]
- Stellato, C.; Porreca, I.; Cuomo, D.; Tarallo, R.; Nassa, G.; Ambrosino, C. The “busy life” of unliganded estrogen receptors. Proteomics 2016, 16, 288–300. [Google Scholar] [CrossRef] [PubMed]
- Fan, P.; Jordan, V.C. New insights into acquired endocrine resistance of breast cancer. Cancer Drug Resist 2019, 2, 198–209. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Wu, K.; Wang, X.; Zhang, J.; Wang, L.; Jiang, Y.; et al. Periostin secreted by cancer-associated fibroblasts promotes cancer stemness in head and neck cancer by activating protein tyrosine kinase 7. Cell Death Dis 2018, 9, 1082. [Google Scholar] [CrossRef] [PubMed]
- Rothenberger, N.J.; Somasundaram, A.; Stabile, L.P. The Role of the Estrogen Pathway in the Tumor Microenvironment. Int J Mol Sci 2018, 19, 611. [Google Scholar] [CrossRef] [PubMed]
- Purohit, A.; Newman, S.P.; Reed, M.J. The role of cytokines in regulating estrogen synthesis: Implications for the etiology of breast cancer. Breast Cancer Research 2002, 4, 65. [Google Scholar] [CrossRef] [PubMed]
- Suba, Z. Crossroad between obesity and cancer: A defective signaling function of heavily lipid laden adipocytes (Online First). In Crosstalk in Biological Processes; El-Esawi, M.A., Ed.; InTechOpen: London, 2019. [Google Scholar] [CrossRef]
- Dannenfelser, R.; Nome, M.; Tahiri, A.; Ursini-Siegel, J.; Vollan, H.K.M.; Haakensen, V.D.; Helland, A.; Naume, B.; Caldas, C.; Borresen-Dale, A.L.; et al. Data-driven analysis of immune infiltrate in a large cohort of breast cancer and its association with disease progression, er activity, and genomic complexity. Oncotarget 2017, 8, 57121–57133. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Miki, Y.; Akahira, J.I.; Moriya, T.; Ohuchi, N.; Sasano, H. Review: Aromatase in human breast carcinoma as a key regulator of intratumoral sex steroid concentrations. Endocrine J 2008, 55, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Dong, S.; Huang, R.; Chen, X. Cancer-Associated Adipocytes and Breast Cancer: Intertwining in the Tumor Microenvironment and Challenges for Cancer Therapy. Cancers 2023, 15, 726. [Google Scholar] [CrossRef]
- Ali, H.R.; Provenzano, E.; Dawson, S.J.; Blows, F.M.; Liu, B.; Shah, M.; et al. Association between cd8+ t-cell infiltration and breast cancer survival in 12,439 patients. Ann. Oncol. 2014, 25, 1536–1543. [Google Scholar] [CrossRef]
- Li, J.; Wu, J.; Han, J. Analysis of Tumor Microenvironment Heterogeneity among Breast Cancer Subtypes to Identify Subtype-Specific Signatures. Genes 2022, 14, 44. [Google Scholar] [CrossRef]
- Sinha, D.K.; Pazik, J.E.; Dao, T.L. Prevention of mammary carcinogenesis in rats by pregnancy: Effect of full-term and interrupted pregnancy. Br J Cancer 1988, 57, 390–394. [Google Scholar] [CrossRef] [PubMed]
- Medina, D.; Smith, G.H. Chemical carcinogen-induced tumorigenesis in parous, involuted mouse mammary glands. J Natl Cancer Inst. 1999, 91, 967–969. [Google Scholar] [CrossRef]
- Yang, J.; Yoshizawa, K.; Nandi, S.; Tsubura, A. Protective effects of pregnancy and lactation against N-methyl-N-nitrosourea-induced mammary carcinomas in female Lewis rats. Carcinogenesis 1999, 20, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Guzman, R.C.; Yang, J.; Rajkumar, L.; Thordarson, G.; Chen, X.; Nandi, S. Hormonal prevention of breast cancer: Mimicking the protective effect of pregnancy. Proc Natl Acad Sci USA. 1999, 96, 2520–2525. [Google Scholar] [CrossRef]
- Rajkumar, L.; Guzman, R.C.; Yang, J.; Thordarson, G.; Talamantes, F.; Nandi, S. Short-term exposure to pregnancy levels of estrogen prevents mammary carcinogenesis. Proc Natl Acad Sci USA 2001, 98, 11755–11759. [Google Scholar] [CrossRef]
- Rajkumar, L.; Guzman, R.C.; Yang, J.; Thordarson, G.; Talamantes, F.; Nandi, S. Prevention of mammary carcinogenesis by short-term estrogen and progestin treatments. Breast Cancer Res 2004, 6, R31–R37. [Google Scholar] [CrossRef]
- Rajkumar, L.; Kittrell, F.S.; Guzman, R.C.; Brown, P.H.; Nandi, S.; Medina, D. Hormone-induced protection of mammary tumorigenesis in genetically engineered mouse models. Breast Cancer Res. 2007, 9, R12. [Google Scholar] [CrossRef]
- Jerry, J. Roles for estrogen and progesterone in breast cancer prevention. Breast Cancer Res 2007, 9, 102. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, A.C.; Shenton, A.; Maher, E.R.; Watson, E.; Woodward, E.; et al. Parity and breast cancer risk among BRCA1 and BRCA2 mutation carriers. Breast Cancer Res 2006, 8, R72. [Google Scholar] [CrossRef] [PubMed]
- Quaynor, S.D.; Stradtman, E.W.; Kim, H.G.; Shen, Y.; Chorich, L.P.; Schreihofer, D.A.; Layman, L.C. Delayed puberty and estrogen resistance in a woman with estrogen receptor α variant. N Engl J Med 2013, 369, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Manna, S.; Holz, M.K. Tamoxifen action in ER-negative breast cancer. Sign Transduct Insight 2016, 5, 1–7. [Google Scholar] [CrossRef] [PubMed]
- van Barele, M.; Heemskerk-Gerritsen, B.A.M.; Louwers, Y.V.; Vastbinder, M.B.; et al. Estrogens and Progestogens in Triple Negative Breast Cancer: Do They Harm? Cancers 2021, 13, 2506. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Qarmali, M.; Siegal, G.P.; Wei, S. Receptor conversion in metastatic breast cancer: Analysis of 390 cases from a single institution. Mod Pathol. 2020, 33, 2499–2506. [Google Scholar] [CrossRef] [PubMed]
- Jordan, V.C. Linking estrogen induced apoptosis with decreases in mortality following long term adjuvant tamoxifen therapy. Journal of the National Cancer Institute 2014, 106, dju296. [Google Scholar] [CrossRef]
- Jordan, V.C. The new biology of estrogen induced apoptosis applied to treat and prevent breast cancer. Endocr. Relat. Cancer 2015, 22, R1–R31. [Google Scholar] [CrossRef] [PubMed]
- Abderrahman, B.; Jordan, V.C.C. Estrogen for the Treatment and Prevention of Breast Cancer: A Tale of 2 Karnofsky Lectures. Cancer, J. 2022, 28, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.; Derocq, D.; Freiss, G.; Rochefort, H. Activation of estrogen receptor transfected into a receptor-negative breast cancer cell line decreases the metastatic and invasive potential of the cells. Proc Natl Acad Sci USA 1992, 89, 11538–11542. [Google Scholar] [CrossRef]
- Malone, R.W.; Felgner, P.L.; Verma, I.M. Cationic liposome-mediated RNA transfection. Proceedings of the National Academy of Sciences 1989, 86, 6077–6081. [Google Scholar] [CrossRef]
- Wolff, J.A.; Malone, R.; Williams, P.; Chong, W.; Acsadi, G.; Jani, A.; et al. Direct gene transfer into mouse muscle in vivo. Science 1990, 247, 1465–1468. [Google Scholar] [CrossRef]
- Dolgin, E. The tangled history of mRNA vaccines. Nature News Feature. 14 September 2021. Correction 22 October 2021.
Figure 1.
HER2 overexpressed immune hot breast cancer cell.In the nucleus, numerous transcriptional factors (TFs) and their cofactors (Cs) are working on the expression of various genes. without estrogen regulation. Estrogen receptors are undetectable. In the cytoplasm, intensive protein synthesis produces HER2 and the members of its kinase cascades: PI3-K, Akt, mTOR and, R.A.S.; RAF, MEK, Mapk, for rectifying cell proliferation via unliganded ER activation. At the cell membrane, numerous HER2 wait for finding ERs appropriate for activation and improving genomic damages. In the peritumoral ring, cancer associated adipocytes (CAAs), cancer-associated fibroblasts (CAFs) and dense immune cell infiltration helps the genomic repair and apoptosis of tumor cell. The cytokine secretome promotes aromatase enzyme (AE) expression and estradiol (E2) synthesis. CAM: cancer-associated monocyte, Bly: b lymphocyte, TLy: t lymphocyte, DC: dendritic cell, EV: extracellular vesicle, N: nucleus.
Figure 1.
HER2 overexpressed immune hot breast cancer cell.In the nucleus, numerous transcriptional factors (TFs) and their cofactors (Cs) are working on the expression of various genes. without estrogen regulation. Estrogen receptors are undetectable. In the cytoplasm, intensive protein synthesis produces HER2 and the members of its kinase cascades: PI3-K, Akt, mTOR and, R.A.S.; RAF, MEK, Mapk, for rectifying cell proliferation via unliganded ER activation. At the cell membrane, numerous HER2 wait for finding ERs appropriate for activation and improving genomic damages. In the peritumoral ring, cancer associated adipocytes (CAAs), cancer-associated fibroblasts (CAFs) and dense immune cell infiltration helps the genomic repair and apoptosis of tumor cell. The cytokine secretome promotes aromatase enzyme (AE) expression and estradiol (E2) synthesis. CAM: cancer-associated monocyte, Bly: b lymphocyte, TLy: t lymphocyte, DC: dendritic cell, EV: extracellular vesicle, N: nucleus.
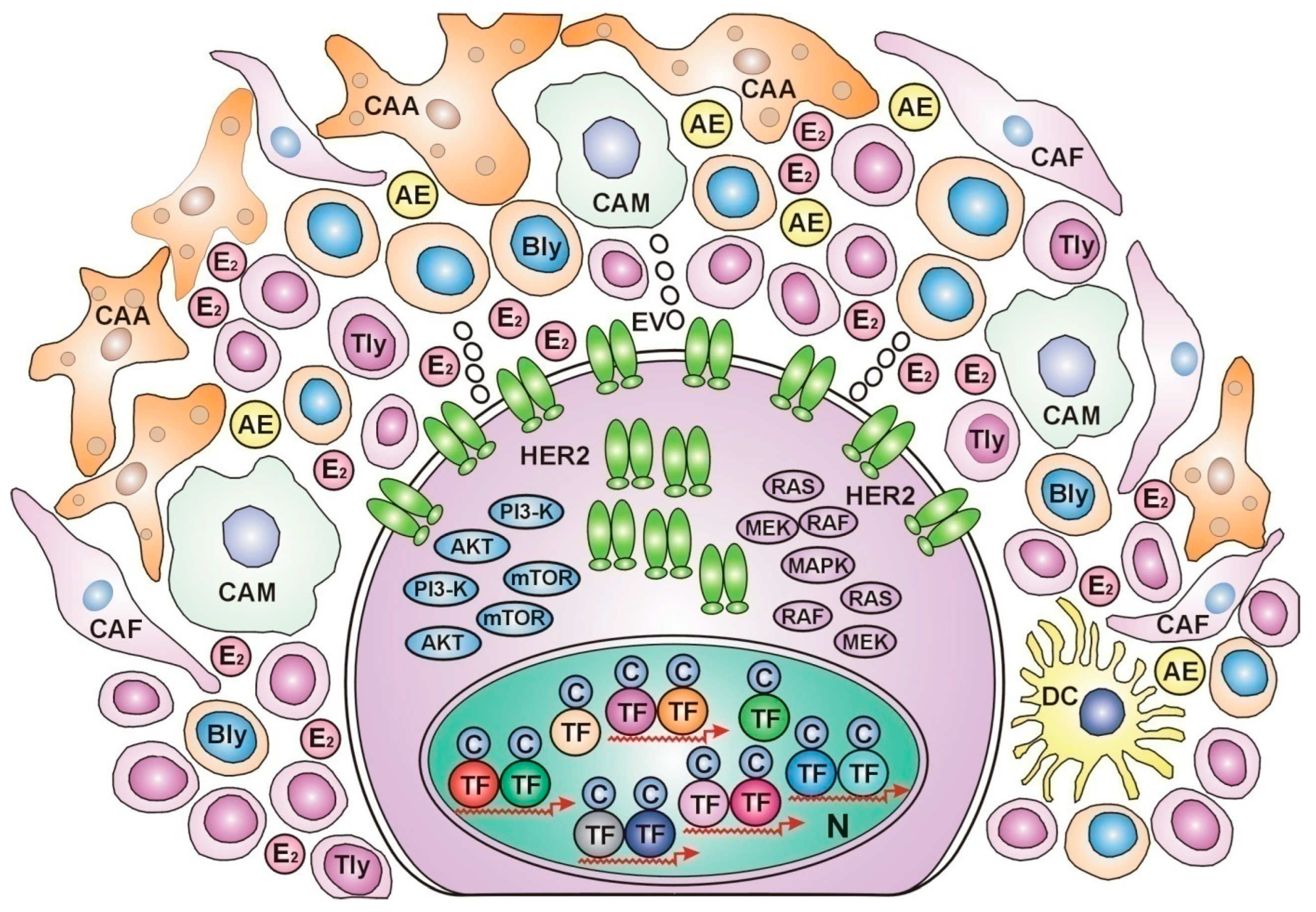
Figure 2.
ER-positive immune cold breast cancer cell.The nucleus is crowded with estrogen (E2) activated estrogen receptors (ERs) showing busy transcriptional activity. In the cytoplasm, intensive protein synthesis produces the players of genome stabilizer circuit: estrogen receptors (ERs), BRCA proteins and aromatase enzyme (AE) completed with estrogen (E2) synthesis. In the peritumoral ring, lipid laden adipocytes (As) border the actively helping cells; cancer-associated adipocytes (CAAs) and cancer-associated fibroblasts (CAFs). The cytokine secretome activates aromatase enzyme (AE) expression and estrogen (E2) synthesis, EV: extracellular vesicle, N: nucleus.
Figure 2.
ER-positive immune cold breast cancer cell.The nucleus is crowded with estrogen (E2) activated estrogen receptors (ERs) showing busy transcriptional activity. In the cytoplasm, intensive protein synthesis produces the players of genome stabilizer circuit: estrogen receptors (ERs), BRCA proteins and aromatase enzyme (AE) completed with estrogen (E2) synthesis. In the peritumoral ring, lipid laden adipocytes (As) border the actively helping cells; cancer-associated adipocytes (CAAs) and cancer-associated fibroblasts (CAFs). The cytokine secretome activates aromatase enzyme (AE) expression and estrogen (E2) synthesis, EV: extracellular vesicle, N: nucleus.
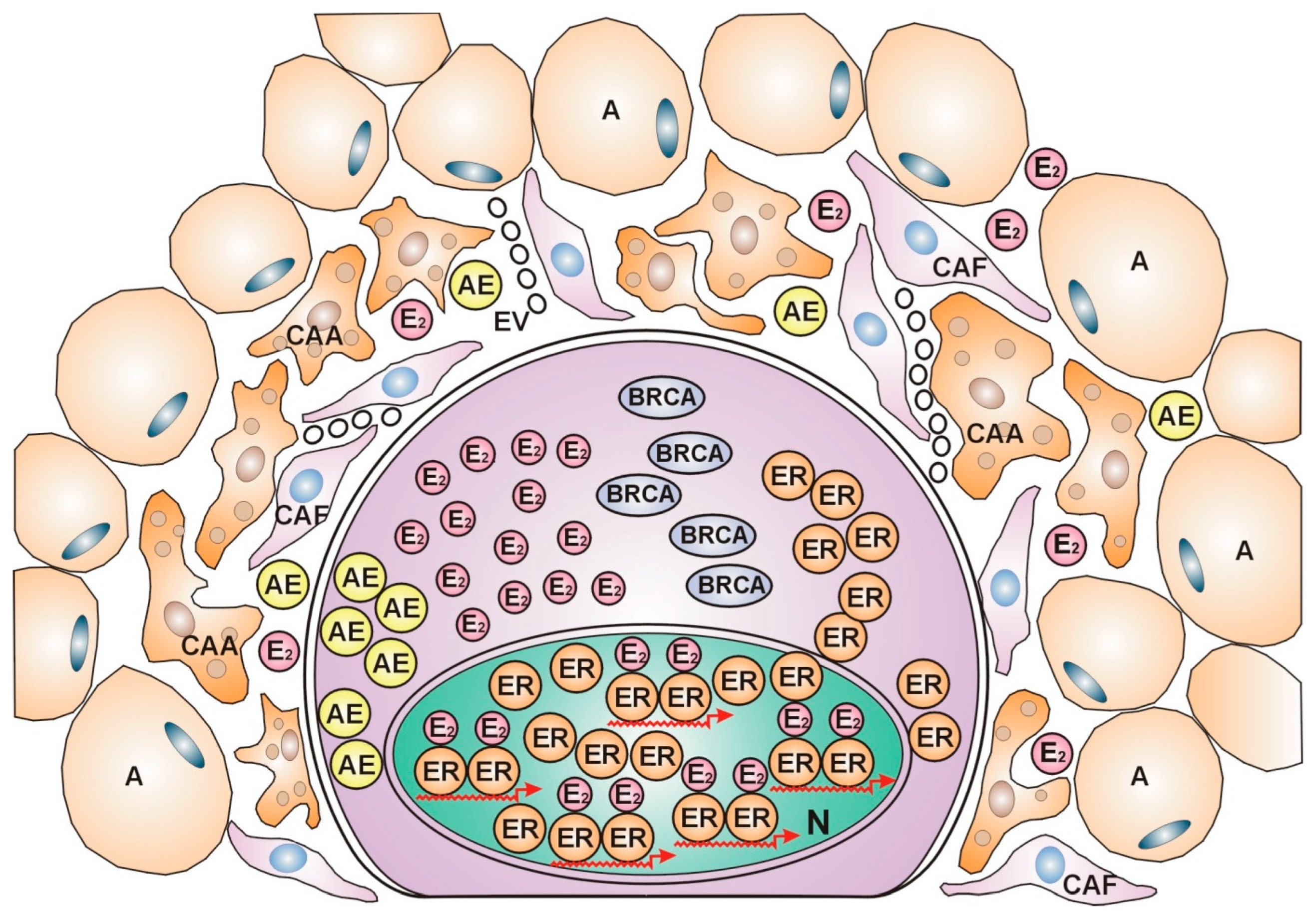
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



