Submitted:
18 July 2024
Posted:
22 July 2024
You are already at the latest version
Abstract
Urinary incontinence after Radical prostatectomy (RALRP) has been associated with older age, longer operative time, higher BMI, short membranous urethral length and preoperative erectile function. We sought to assess the association between the neuromuscular characteristics and postoperative urinary incontinence. Methods: RALRP specimens from 29 men who underwent bilateral nerve sparing were reanalyzed. Urinary incontinence was evaluated using the International Consultation on Questionnaire-Short Form (ICIQ-SF) at 6 weeks post surgery and last follow-up. Linear and logistic regression analyses were performed to assess neuromuscular characteristics and incontinence. Results: At a median follow-up of 11 months (IQR 9-12), 11 patients (38%) reported on severe incontinence (>12 ICIQ-SF score). Median number of peripheral nerves observed at the base and apex of the specimens were 52 (IQR 13-139) and 59 (IQR: 28-129), respectively. Ganglia were present in 19 patients (65%) at the base and 12 patients (41%) at the apex. Additionally, the median proportional area of detrusor smooth muscle fibers at the base was 0.54 (IQR 0.31-1), while the median proportional area of striated muscle fibers at the apex was 0.13 (IQR 0.08-0.24). No statistical significant associations were found. Conclusion: Histologic neuromuscular characteristics were not associated with postoperative urinary incontinence. Enhanced intraoperative evaluation and larger scale studies may prove useful for prediction of post prostatectomy incontinence.
Keywords:
incontinence
; radical prostatectomy
; neuromuscular features
Introduction
Robotic-assisted radical prostatectomy (RALRP) is considered a major treatment alternative for intermediate and high-risk prostate cancer. Accumulating experience over the past 2 decades has led to improved postoperative outcomes in terms of recovery of urinary continence and erectile dysfunction (ED) [1,2]. However, postoperative urinary incontinence (UI) which has a profound impact on patients' quality of life and social well-being remains a significant burden [1,3].
Despite substantial progress in surgical technique, the prevalence of postoperative incontinence remains high, estimated to range from 2% to 66% [4,5]. Numerous studies have established potential predictors of postoperative UI namely increased patient age, longer operative time, higher body mass index (BMI), shorter membranous urethral length, and preoperative erectile dysfunction [6,7,8]. While some suggested that adequate preservation of the neurovascular bundles may expedite the recovery of postoperative urinary continence [9,10,11,12], the relationship between the two remains elusive.
The objective of this study was to quantify the amount of retained neurovascular tissue on radical prostatectomy specimens as a surrogate for the quality of neurovascular bundles preservation and assess its association with recovery of postoperative UI.
Materials and Methods
After institutional review board approval, our departmental database was queried to retrieve the medical records of 50 consecutive male patients who underwent bilateral nerve sparing RALRP between October 2021 and March 2022.Based on their clinical evaluation and disease features, bilateral intrafascial dissection technique was employedin all patients [13]. Clinical and pathological data were collected and reviewed, including age and comorbidities, performance status, Prostate-Specific Antigen [PSA] levels and imaging (MRI and PET-PSMA) findings. Pathological analysis included tumor stage and grade (TMN), margin status and tumor size.
Urinary functional outcomes were assessed at 2 consecutivepoints in time during follow-up: immediately (6 weeks) after surgery and at last follow-up. The former included the number of pads used per day and IPSS score, whereas the latter involved a formal interview where patients were asked to complete the International Consultation on Incontinence Questionnaire-Short Form (ICIQ-SF) [14].
The ICIQ-SF is comprised of 3 questions, and the total ICIQ score ranges from 0 to 21. A score of zero indicates no urine leakage and no impact on quality of life. Question 1 (Q1) assesses the frequency of urinary leakage, question 2 (Q2) evaluates the amount of leakage, and question 3 (Q3) measures the extent to which UI affects daily life. The scoring categories for incontinence are further stratified into slight (1-5), moderate (6-12), severe (13-18), and very severe (19-21). Of the 50 patients, 29 responded and provided consent to be included in the study.
A dedicated genitourinary pathologist reanalyzed all RP specimens,evaluating the neuromuscular characteristics at the base and apex of the specimen. Six explicit neuromuscular features were investigated, including (1) the presence of ganglions at the base of the prostate, (2) the presence of ganglions at the apex of the prostate, (3) the proportional area of detrusor muscle fibers at the base, (4) the proportional area of sphincteric striated muscle fibers at the apex, (5) the number of nerves at the base, and the (6) number of nerves at the apex. (Figure 1). A score was generated for each specimen based on these findings and its relationship with the severity of incontinence was analyzed.
Descriptive statistics were used to summarize the patients’ characteristics. Continuous variables were reported as median and inter-quartile range (IQR), and categorical variables were reported as proportion(%). Linear and logistic regression analyses were conducted to assess the relationship between the specimen neuromuscular characteristics and the severity of UI, controlling for clinical and pathological variables including age, prostate size, and pathological stage.
All statistical analyses were two-sided, and significance was defined as p < 0.05. The SPSS software (IBM SPSS Statistics, Version 25, IBM Corp., Armonk, NY, USA) was used.
Results
Of the 50 patients who underwent RALRP in our medical facilitybetween October 2021 and March 2022, 29 responded and provided consent to be included in the study.
At6 weeks post-surgery, 7 patients (24%) reported onfull urinary continence (day and night continence and no protectivepads used).
At a median follow-up of 11 months (IQR 9,12) patients were interviewed and stratified into 3 groups based on their ICIQ scores. Nine patients (31%) were categorized as slight UI (ICIQ-SF score<6),9 patients (31%) were categorized as moderate UI (ICIQ-SF scores 6-12), and 11 patients (38%) were categorized as severe and very severe UI (ICIQ-SF score>12). There was nostatistically significant association between the early continence rate and the severity of UIat last follow-up (p=0.182). Of the 12 patients with adequate preoperative potency, recovery of erectile function 1 year after surgery was documented in 3 based on their IIEF score (Table 1).
Based on the median and average ICIQ scores, the patients were restratified into two groups: 1 – ICIQ scores 1-12 - slight to moderate UI, 2 – ICIQ scores 13-21 - severe to very severe UI. While there was no difference in patients' age between the groups, a statistically significant correlation was found between severity of incontinence and the risk of disease progression. Compared to patients with lower ICIQ scores, those with higher ICIQ scores had significantly higher preoperative PSA levels (Table 2). However, number of patients with preoperative lower urinary tract symptoms (LUTS)( IPSS>7), prostate size, early continence rates and pathological stage did not demonstrated significant difference between the groups (Table 2).
Discussion
Rapid return of urinary control is a critical step in achieving overall satisfaction after radical prostatectomy [1,9]. UI is considered one of the most distressing side effects following surgery and strategies to improve continence outcomes have been a focus of research in this field [10].While the importance of neurovascular preservation to improve early postoperative urinary continence has been demonstrated repeatedly [15], most studies have evaluated the adequacy of nerve sparing based on subjective surgeon reported notes. Within this context we endeavored to study the relationship between the amount of neurovascular tissue found on the pathological specimen in men undergoing bilateral nerve preservation as a surrogate of inadequate nerve sparing and possibly postoperative urinary incontinence. The addition of useful information to a standard pathology report might potentially allow a more aggressive approach treating postprostatectomy incontinence.
Our findings demonstrate that post-operative incontinence was more common among higher risk tumors, however, no associations were found between the pathological neuromuscular characteristics of the specimens and postoperative UI.
Traditionally, intraoperative damage to the external urethral sphincter or its innervation was considered the main root of incontinence after radical prostatectomy [16]. However, the true mechanism has not been completely understood, and currently, it is thought to be multifactorial. Factors potentially affecting post-surgery incontinence include patient’s age and comorbidities, obesity, preoperative lower urinary tract dysfunction, prostate size, membranous urethra length, bladder neck preservation and preservation of the membranous urethra supporting structures [17].
A urodynamic study before and after RP reported that the maximum urethral closure pressure at rest immediately after RP was reduced to roughly 40% of its preoperative level [18,19,20,21]. At 1 year postoperatively, the maximal urethral closure pressure had improved, but not to its preoperative point. [19,20,21].
The presence of neuromuscular tissue on the outer surface of the prostate specimen might not just be an anatomical observation. It holds potential significance in predicting functional outcomes, including recovery of urinary continence [22]. While a preserved denser nerve network might theoretically offer better functional outcomes, its presence on the excised specimen suggests it was not adequately secured during surgery, which might be deleterious [23]. Moreover, the observed association between cancer stage and incontinence might reflect the tendency to sacrifice, at least in part, the neurovascular tissue surrounding the gland in locally advanced tumors [24]. Kaye et al. have shown that sparing at least 1 neurovascular bundle along with its supportive tissues has a dramatic effect on recovery of urinary continence and quality of life in preoperatively potent men [25]. The cavernous nerve (CN) is the main autonomic nerve regulating penile erection but is also involved in the voiding reflex by innervating the urethral transverse muscle on the anterior aspect of the prostate through designated branches [26].
Meticulous nerve preservation during radical prostatectomy has been linked with enhanced postoperative erectile function outcomes [27]. However the relationship between nerve sparing, and urinary incontinence is less clear, pointing towards possible overlapping anatomical or physiological pathways [28]. Due to its small size and small number of men with documented erectile function recovery, our study could not corroborate the previously observed association between the two. Nonetheless, in the absence of any association between retained specimen neuromuscular components and urinary function outcomes, our findings might suggest that a non-nerve sparing operation in locally advanced tumors (extrafascial dissection) might not be inevitably deleterious for rapid recovery of urinary continence.
Two limitations need to be emphasized. The high prevalence of preoperative erectile dysfunction in our study impedes our ability to study the association between nerve-sparing, postoperative ED and UI. Additionally, the modest cohort size might have limited our ability to provide definitive proof of an association between neuromuscular specimen characteristics and urinary incontinence [29]. There is clear need for more extensive research to better comprehend these interconnections and improve surgical practices and patient outcomes [30].
Conclusions
Histologic neuromuscular characteristics in radical prostatectomy specimens were not associated with postoperative continence outcomes. Further studies that incorporate additional assessments such as myelin staining mightprovide different insights regarding the integrity of the neurovascular bundles and of its association with incontinence outcomes.
References
- Sood, A.; Jeong, W.; Palma-Zamora, I.; Abdollah, F.; Butaney, M.; Corsi, N.; et al. Description of Surgical Technique and Oncologic and Functional Outcomes of the Precision Prostatectomy Procedure (IDEAL Stage 1-2b Study). Eur Urol. 2022, 81, 396–406. [Google Scholar] [CrossRef]
- Du, Y.; Long, Q.; Guan, B.; Mu, L.; Tian, J.; Jiang, Y.; Bai, X.; Wu, D. Robot-Assisted Radical Prostatectomy Is More Beneficial for Prostate Cancer Patients: A System Review and Meta-Analysis. Med SciMonit. 2018, 24, 272–287. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Amano, K.; Suzuki, K.; Ito, Y. Changes in quality of life and lower urinary tract symptoms over time in cancer patients after a total prostatectomy: Systematic review and meta-analysis. Support Care Cancer. 2022, 30, 2959–2970. [Google Scholar] [CrossRef]
- Pinkhasov, R.M.; Lee, T.; Huang, R.; Berkley, B.; Pinkhasov, A.M.; Dodge, N.; et al. Prediction of Incontinence after Robot-Assisted Radical Prostatectomy: Development and Validation of a 24-Month Incontinence Nomogram. Cancers (Basel) 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- MacDiarmid, S.A. Incontinence after radical prostatectomy: Pathophysiology and management. Curr. Urol. Rep. 2001, 2, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Hagens, M.J.; Veerman, H.; de Ligt, K.M.; Tillier, C.N.; van Leeuwen, P.J.; van Moorselaar, R.J.A.; et al. Functional outcomes rather than complications predict poor health-related quality of life at 6 months after robot-assisted radical prostatectomy. J Robot Surg. 2022, 16, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Hikita, K.; Honda, M.; Shimizu, R.; Teraoka, S.; Kawamoto, B.; Yumioka, T.; et al. Longitudinal, 5-year long-term outcomes for urinary continence and quality of life after robot-assisted radical prostatectomy in Japanese patients. Low Urin Tract Symptoms. 2022, 14, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Gondoputro, W.; Thompson, J.; Evans, M.; Bolton, D.; Frydenberg, M.; Murphy, D.G.; et al. How Does Age Affect Urinary Continence following Robot-Assisted Radical Prostatectomy? A Prospective Multi-Institutional Study Using Independently Collected, Validated Questionnaires. J Urol. 2022, 207, 1048–1056. [Google Scholar] [CrossRef]
- Ko, W.J.; Truesdale, M.D.; Hruby, G.W.; Landman, J.; Badani, K.K. Impacting factors for recovery of erectile function within 1 year following robotic-assisted laparoscopic radical prostatectomy. J Sex Med. 2011, 8, 1805–1812. [Google Scholar] [CrossRef] [PubMed]
- Haga, N.; Miyazaki, T.; Tsubouchi, K.; Okabe, Y.; Shibayama, K.; Emoto, D.; Matsuoka, W.; Maruta, H.; Aoyagi, C.; Matsuzaki, H.; Irie, S.; Nakamura, N.; Matsuoka, H. Comprehensive approach for preserving cavernous nerves and erectile function after radical prostatectomy in the era of robotic surgery. Int J Urol. 2021, 28, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Reeves, F.; Preece, P.; Kapoor, J.; Everaerts, W.; Murphy, D.G.; Corcoran, N.M.; Costello, A.J. Preservation of the neurovascular bundles is associated with improved time to continence after radical prostatectomy but not long-term continence rates: Results of a systematic review and meta-analysis. Eur Urol. 2015, 68, 692–704. [Google Scholar] [CrossRef] [PubMed]
- Haglind, E.; Carlsson, S.; Stranne, J.; Wallerstedt, A.; Wilderäng, U.; Thorsteinsdottir, T.; Lagerkvist, M.; Damber, J.E.; Bjartell, A.; Hugosson, J.; Wiklund, P.; Steineck, G.; LAPPRO steering committee. Urinary Incontinence and Erectile Dysfunction After Robotic Versus Open Radical Prostatectomy: A Prospective, Controlled, Nonrandomised Trial. Eur Urol. 2015, 68, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wu, Y.; Guo, J.; Chen, H.; Weng, X.; Liu, X. Intrafascial nerve-sparing radical prostatectomy improves patients' postoperative continence recovery and erectile function: A pooled analysis based on available literatures. Medicine (Baltimore). 2018, 97, e11297. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grøn Jensen, L.C.; Boie, S.; Axelsen, S. International consultation on incontinence questionnaire - Urinary incontinence short form ICIQ-UI SF: Validation of its use in a Danish speaking population of municipal employees. PLoS ONE. 2022, 17, e0266479. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sanchez-Salas, R.; Tourinho-Barbosa, R.; Sivaraman, A.; Borges, R.C.; Candela, L.; Cathala, N.; Mombet, A.; Marra, G.; Sanchez, L.R.; Boumezrag, C.B.; Lanz, C.; Macek, P.; Korkes, F.; Cathelineau, X. Assessing the efficacy of pelvic floor muscle training and duloxetine on urinary continence recovery following radical prostatectomy: A randomized clinical trial. Prostate. 2024, 84, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Gacci, M.; Ierardi, A.; Rose, A.D.; Tazzioli, S.; Scapaticci, E.; Filippi, S.; Maggi, M.; Nicita, G.; Carini, M.; Montorsi, F. Vardenafil can Improve Continence Recovery after Bilateral Nerve Sparing Prostatectomy: Results of a Randomized, Double Blind, Placebo-Controlled Pilot Study. J. Sex. Med. 2010, 7, 234–243. [Google Scholar] [CrossRef]
- Gacci, M.; De Nunzio, C.; Sakalis, V.; Rieken, M.; Cornu, J.N.; Gravas, S. Latest Evidence on Post-Prostatectomy Urinary Incontinence. J Clin Med. 2023, 12, 1190. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kadono, Y.; Ueno, S.; Yaegashi, H.; Ofude, M.; Izumi, K.; Maeda, Y.; Mizokami, A.; Miwa, S.; Miyagi, T.; Namiki, M. Urodynamic evaluation before and immediately after robot-assisted radical prostatectomy. Urology. 2014, 84, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Kadono, Y.; Ueno, S.; Iwamoto, D.; Takezawa, Y.; Nohara, T.; Izumi, K.; Mizokami, A.; Namiki, M. ChronologicalUrodynamic Evaluation of ChangingBladder and UrethralFunctionsAfter Robot-assisted Radical Prostatectomy. Urology. 2015, 85, 1441–1447. [Google Scholar] [CrossRef]
- Kadono, Y.; Ueno, S.; Kadomoto, S.; Iwamoto, H.; Takezawa, Y.; Nakashima, K.; Nohara, T.; Izumi, K.; Mizokami, A.; Gabata, T.; et al. Use of pre-operativefactorsincludingurodynamicevaluations and nerve-sparingstatus for predictingurinary continence recoveryafter robot-assisted radical prostatectomy: Nerve-sparing technique contributes to the reduction of postprostatectomy incontinence. Neurourol. Urodyn. 2016, 35, 1034–1039. [Google Scholar] [CrossRef]
- Kadono, Y.; Nohara, T.; Kawaguchi, S.; Naito, R.; Urata, S.; Nakashima, K.; Iijima, M.; Shigehara, K.; Izumi, K.; Gabata, T.; et al. Investigating the mechanismunderlyingurinary continence recoveryafter radical prostatectomy:Effectiveness of a longer urethralstump to preventurinary incontinence. BJU Int. 2018, 122, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Hefermehl, L.; Bossert, K.; Ramakrishnan, V.M.; Seifert, B.; Lehmann, K. A Prospective Analysis of the Effects of Nerve-Sparing Radical Prostatectomy on Urinary Continence Based on Expanded Prostate Cancer Index Composite and International Index of Erectile FunctionScoringSystems. Int Neurourol J. 2018, 22, 123–132. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Secin, F.P.; Serio, A.; Bianco FJJr Karanikolas, N.T.; Kuroiwa, K.; Vickers, A.; Touijer, K.; Guillonneau, B. Preoperative and intraoperativeriskfactors for side-specific positive surgicalmargins in laparoscopic radical prostatectomy for prostate cancer. EurUrol. 2007, 51, 764–771. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.R.; Sivaraman, A.; Coelho, R.F.; Chauhan, S.; Palmer, K.J.; Orvieto, M.A.; Camacho, I.; Coughlin, G.; Rocco, B. Pentafecta:a new concept for reportingoutcomes of robot-assistedlaparoscopic radical prostatectomy. EurUrol. 2011, 59, 702–707. [Google Scholar] [CrossRef] [PubMed]
- Kaye, D.R.; Hyndman, M.E.; Segal, R.L.; Mettee, L.Z.; Trock, B.J.; Feng, Z.; Su, L.M.; Bivalacqua, T.J.; Pavlovich, C.P. Urinaryoutcomes are significantlyaffected by nerve sparingqualityduring radical prostatectomy. Urology. 2013, 82, 1348–1353. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Wu, C.; Zhou, X.; Zhai, G.; Wu, J. Cavernous Nerve InjuryResulted Erectile Dysfunction and Regeneration. J ImmunolRes. 2021, 2021, 5353785. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Walsh, P.C.; Donker, P.J. Impotence following radical prostatectomy: Insight intoetiology and prevention. J Urol. 1982, 128, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Ficarra, V.; Novara, G.; Rosen, R.C.; Artibani, W.; Carroll, P.R.; Costello, A.; Menon, M.; Montorsi, F.; Patel, V.R.; Stolzenburg, J.U.; Van der Poel, H.; Wilson, T.G.; Zattoni, F.; Mottrie, A. Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy. Eur Urol. 2012, 62, 405–417. [Google Scholar] [CrossRef] [PubMed]
- Sanda, M.G.; Dunn, R.L.; Michalski, J.; Sandler, H.M.; Northouse, L.; Hembroff, L.; Lin, X.; Greenfield, T.K.; Litwin, M.S.; Saigal, C.S.; Mahadevan, A.; Klein, E.; Kibel, A.; Pisters, L.L.; Kuban, D.; Kaplan, I.; Wod, D.; Ciezki, J.; Shah, N.; Wei, J.T. Quality of life and satisfaction withoutcomeamong prostate-cancer survivors. N Engl J Med. 2008, 358, 1250–1261. [Google Scholar] [CrossRef] [PubMed]
- Litwin, M.S.; Lubeck, D.P.; Henning, J.M.; Carroll, P.R. Differences in urologist and patient assessments of healthrelatedquality of life in men with prostate cancer:results of the CaPSUREdatabase. J Urol. 1998, 159, 1988–1992. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Representative images of pathologic specimens: A. Ganglions spread. B. Peripheral nerves, C. Skeletal muscles, D. Tumor involvement within skeletal muscle.
Figure 1.
Representative images of pathologic specimens: A. Ganglions spread. B. Peripheral nerves, C. Skeletal muscles, D. Tumor involvement within skeletal muscle.
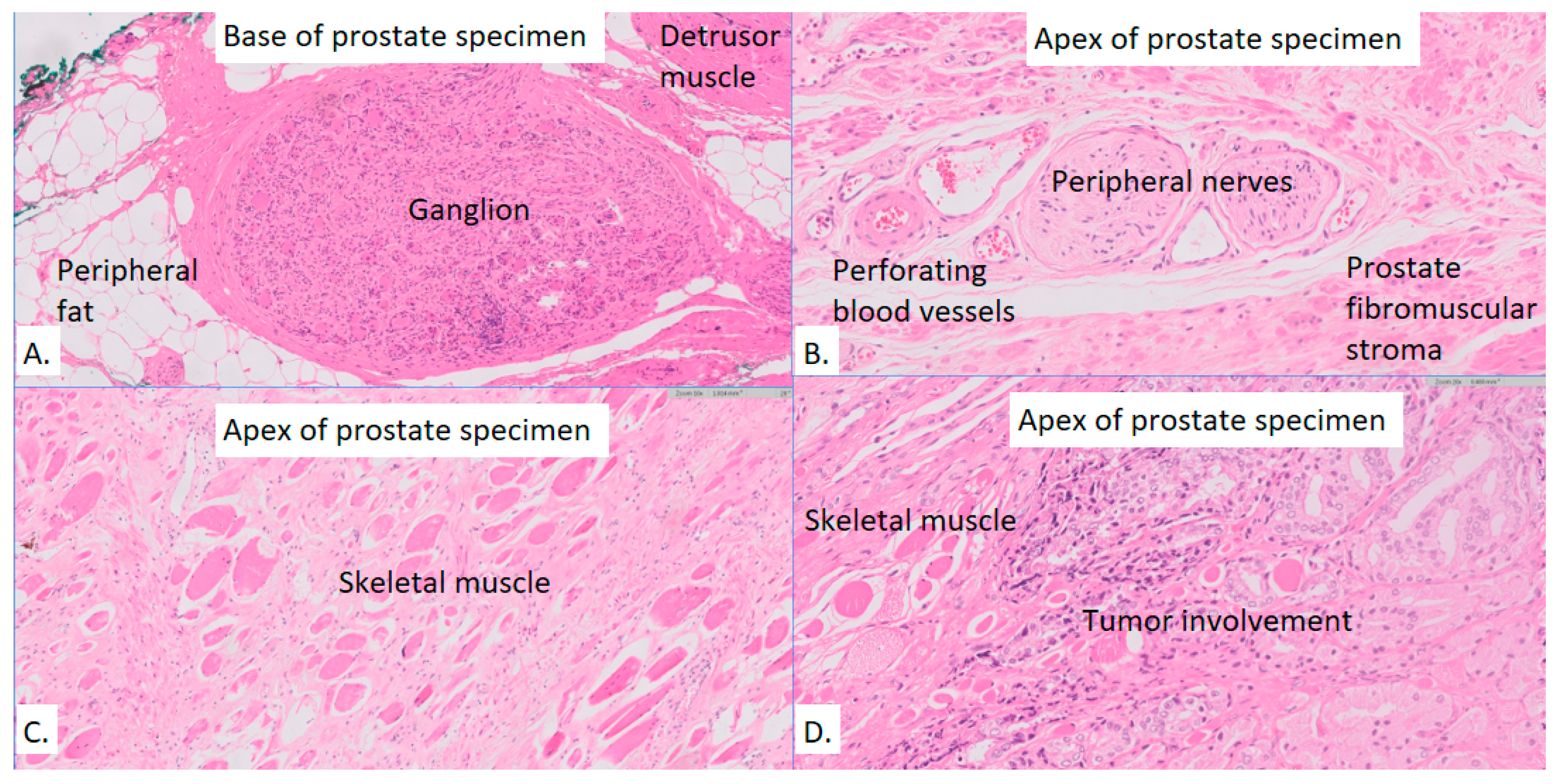

Table 1.
Patients' post-op continence and erectile preservation based on ICIQ score.
| ICIQ category (11 months post surgery (IQR 9,12) | Number of patients (percentage) | Early full continence -number of patients (6 weeks post surgery) (percentage from the group) | Erectile preservation (number of patient with pre-op erectile function) |
|---|---|---|---|
| Slight (1-5) | 9 (31%) | 4 (44%) | 2 (4) |
| Moderate (6-12) | 9 (31%) | 2 (22%) | 1 (4) |
| Severe and very severe (13-21) | 11 (38%) | 1 (9%) | 0 (4) |
Table 2.
Comparison between 11 months (9-12) post op continence score.
| ICIQ<=12 (n=18) | ICIQ > 12 (n=11) | P value | |
|---|---|---|---|
| Average ICIQ(IQR) | 6.5(2.25-10.75) | 16.4(14.5-18) | |
| Age (IQR) | 67.3(63.9-73.3) | 69.4(67-72.7) | 0.44 |
| Pre op PSA(ng/ml) (IQR) | 9.1(6.6-9.9) | 16(9-22.2) | 0.02 |
| Number of patients withpre op LUTS (IPSS>7) | 8 (45%) | 5 (45%) | 0.96 |
|
ISUP score 1 2 3 4 5 |
1 (5.5%) 8 (44.4%) 5 (27.7%) 2 (11.1%) 2 (11.1%) |
0 (0%) 3 (27.2%) 4 (36.3%) 2 (18.1%) 0 (0%) *ISUPx – after hormonal treatment – 2 (18.1%) |
0.302 |
| Prostate size (gram) | 68(55-73) | 63.2(49.5-65.3) | 0.6 |
|
pT stage (2009) T2 T3a T3b |
8 (44.4%) 9 (50%) 1 (5.5%) |
1 (9%) 9 (82%) 1 (9%) |
0.136 |
| Full 6W continence day | 8 (45%) | 3 (27%) | 0.37 |
| Full 6W continence night | 8 (45%) | 2 (18%) | 0.14 |
Table 3.
Neuromuscular characteristics of pathologic specimens stratified by incontinence severity.
| Overall (n=29) |
ICIQ score ≤ 12 (n=18) |
ICIQ score >12 (n=11) |
P value | |
|---|---|---|---|---|
| Presence of ganglion in the base, n (%) | 19 (65%) | 11 (61%) | 8 (72%) | 0.22 |
| Presence of ganglion in the apex, n (%) | 12 (41%) | 8 (44%) | 4 (36%) | 0.11 |
| Proportional area of detrusor muscle in the base, median (IQR) | 0.54 (0.31-1.00) | 0.45 (0.29-0.92) | 0.60 (0.40-1.00) | 0.57 |
| Proportional area of striated muscle at the apex, median (IQR) | 0.13 (0.07-0.24) | 0.13 (0.06-0.24) | 0.13 (0.08-0.24) | 1.00 |
| # of nerves at the base, median (IQR) | 52 (13-139) | 69 (11-152) | 36 (14-108) | 0.65 |
| # of nerves at the apex, median (IQR) | 59 (28-129) | 61 (28-142) | 51 (33-116) | 0.46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



