
Submitted:
18 July 2024
Posted:
19 July 2024
You are already at the latest version
Abstract
Placenta accreta spectrum (PAS) disorders are characterized by abnormal trophoblastic invasion into the myometrium, leading to significant maternal health risks. PAS includes placenta accreta (invasion <50% of the myometrium), increta (invasion >50%), and percreta (invasion through the entire myometrium). The condition is most associated with previous cesarean deliveries, and its incidence increases with the number of cesareans. Other risk factors include advanced maternal age, multiparity, and various uterine surgeries. The increasing global cesarean rates heighten the importance of early PAS diagnosis and management. The study reviewed molecular mechanisms driving PAS, focusing on signaling pathways, genetic expression, biomarkers, and non-coding RNAs involved in trophoblastic invasion. It explored genetic expression and key regulatory processes such as apoptosis, cell proliferation, invasion, and inflammation. The manuscript was compiled from recent scientific literature (2014 – 2024) from the Scopus, PubMed, Google Scholar, and Web of Science databases. Placenta Acreta Spectrum; acreta; increta; percreta; trophoblast invasion; miRNAs, lncRNAs; genetic expression; biomarkers; signaling pathways were the employed keywords to compile relevant literature. The PAS is an important obstetric health problem that challenges maternal health risks associated with abnormal trophoblastic invasion that relies on abnormal placentation, uterine scarring, and impaired decidualization. Identifying new biomarkers like AFP, sFlt-1, β-hCG, PlGF, and PAPP-A aids early detection and management. Understanding genetic expression and non-coding RNAs is crucial for unraveling PAS complexities. Besides, aberrant signaling pathways like Notch, PI3K/Akt, STAT3, and TGF-β offer potential therapeutic targets to modulate trophoblastic invasion. This review underscores the need for interdisciplinary care, early diagnosis, and ongoing research into PAS biomarkers and molecular mechanisms to improve prognosis and quality of life for affected women.
Keywords:
placenta accreta spectrum
; trophoblast invasion
; placenta acreta
; placenta increta
; placenta percreta
Introduction
The placenta accreta spectrum (PAS) corresponds to a range of conditions characterized by abnormal trophoblastic invasion into the myometrium, which carries significant risks to maternal health. The PAS is categorized based on the extent of invasion into the uterine wall. Placenta accreta is characterized by an invasion of less than 50% of the myometrium, increta by an invasion greater than 50%, and percreta by invasion through the entire myometrium [1]. The PAS is considered a high-risk condition with serious associated morbidities; therefore, the American College of Obstetricians and Gynecologists (ACOG) and the Society for Maternal-Fetal Medicine recommend these patients receive level III (subspecialty) or higher care with consistent access to interdisciplinary staff with expertise in critical care [2].
The most prevalent risk factor for PAS is a previous cesarean delivery, with the incidence of PAS increasing with the number of prior cesarean deliveries [2,3]. According to a systematic review, the rate of PAS increases from 0.3% in women with one previous cesarean delivery to 6.74% in women with five or more cesarean deliveries [4]. Additional risk factors include advanced maternal age, multiparity, prior uterine surgeries or curettage, manual delivery of the placenta, Asherman syndrome, postpartum endometritis, and, more recently, hysteroscopic surgery, endometrial ablation, and uterine artery embolization have all been associated with PAS disorders in subsequent pregnancies [2,5,6].
In this regard, cesarean delivery rates have risen substantially globally, increasing from less than 7% in the 1990s to exceeding the World Health Organization's (WHO) recommended upper limit of 10-15% at the population level in the past two decades [7,8]. Therefore, early diagnosis is essential for management and a favorable outcome for the binomial.
This review aims to describe the molecular mechanisms driving PAS by exploring the pathological signaling pathways implicated in this disease. We will delve into the roles of critical proteins, chemokines, and other biomarkers and the role of non-coding RNAs in trophoblastic invasion. Additionally, we will examine the contributions of epigenetic modifications and genes to the involvement of key regulatory processes, including apoptosis, cell proliferation, invasion, and inflammation.
Methodology
To identify relevant information on the placenta accreta spectrum, this review was compiled based on recent scientific literature (2014-2024) from the Scopus, PubMed, Google Scholar, and Web of Science databases. The keywords used for the literature research were “Placenta Acreta Spectrum; acreta; increta; percreta; trophoblast invasion; miRNAs, lncRNAs; genetic expression; biomarkers; signaling pathways“. We only included literature in the English language. Using these criteria, this review is composed of 74 papers.
Placenta Accreta Spectrum Classification and Physiopathological Features
The International Federation of Gynecology and Obstetrics (FIGO) Committee first recognized the PAS classification for the Ethical Aspects of Human Reproduction and Women's Health in Clinical distinction of morbid adherence of the placenta is associated with comprehensive prenatal diagnosis, clinical approach, correlation of treatment methods, and the frequency of severe obstetric complications [9]. Later, several retrospective and prospective studies made specifically to determine the classification influence on the results of the PAS treatment showed its significant impact on the choice of management [10].
In this regard, the classification of the PAS is based on the depth of the placental invasion within the uterine wall and its extension of involvement. The Society for Maternal-Fetal Medicine (SMFM) developed a widely accepted classification system [11], dividing PAS into three categories: placenta accreta (PA), placenta increta (PI), and placenta percreta (PP), which their features are presented in Figure 1.
The physiopathological features of PAS involve a complex interplay of factors, including abnormal placentation, uterine scarring, and impaired decidualization. In normal pregnancies, the placenta separates easily from the uterine wall during childbirth due to the formation of a specialized layer called the decidua. However, in the PAS, this process is disrupted, leading to abnormal adherence of the placenta [12,13].
Concerning the developmental behavior on the severity in this spectrum, it comprises abnormal placentation, which allows trophoblast to develop and adhere by cellular invasion. Angiogenesis is another necessary cellular process, allowing correct endometrial growth, embryonic growth, and placentation. Regarding invasion, it is pivotal for blastocyst differentiation into villous and extravillous trophoblasts (EVT), which acquire pathological characteristics when they reach decidua and myometrium [14]. Once implanted by migration, maternal uterine artery and vascular smooth muscle cells are replaced by trophoblasts through apoptosis [15]. Herein, cellular and molecular processes involved in the PAS are discussed.
Biomarkers Associated with Placenta Accreta Development
The Placenta accreta spectrum (PAS) encompasses the disorders of abnormal placental adherence, including placenta accreta, increta, and percreta [16]. Clinical suspicion is based on the risk factors for PAS and the imaging findings [17]. However, the PAS is sometimes diagnosed only at the time of delivery or by pathology since placental findings may not be visualized until the delivery time [18,19]. There is interest in identifying potential biomarkers for the PAS, particularly those that may be clinically useful and non-invasive.
Some researchers suggested combining serum biomarker values with imaging and clinical data to improve the diagnostic performance of ultrasonography and MRI-based methods for PAS disorders. The medical literature has shown that certain peripheral blood biomarkers, including those related to angiogenesis, the immune system, beta-human chorionic gonadotropin (β-hCG), and placental-derived cell-free DNA, may increase in patients with placental invasion disorders compared to normal pregnancies [20,21]. The most relevant biomarkers for the spectrum diagnosis are presented in Table 1.
Molecular Mechanisms Involved in the Placenta Acreta Spectrum
The placenta accreta spectrum comprehends several mechanisms that involve multifactorial processes, which highlight proliferation and invasion into local tissues, similar to a tumor. Other characteristics involved in PAS physiopathology include angiogenesis induction and cell death resistance, including epithelial-to-mesenchymal transition (EMT) [12,37,38]. Despite the several reports of placental pathologies, the precise molecular mechanisms of the placenta accreta spectrum are still poorly understood. Here, we enlist the most relevant to date molecular mechanisms involved in the spectrum.
5.Gene Expression
In the process of invasion, proliferation, and migration, excessive trophoblast invasion and decidual deficiency are the main pathophysiological mechanisms of PA, these processes in combination with other mechanisms such as endometrial invasion, migration through the myometrium, among others, trigger the spectrum [39].
In this regard, the chemokine CXCL12 and its receptors, CXCR4 and CXCR7, are known to play pivotal roles in the invasion process of trophoblast cells. Consequently, the mechanisms underlying the excessive invasion of trophoblasts in patients diagnosed with PAS present an upregulation of CXCL12 and CXCR4/CXCR7 in extravillous trophoblastic cells in a dose-dependent manner. Moreover, it was noted that the regulation of trophoblast migration, invasion, and migration is related to CXCL12 and CXCR4/CXCR7 expression in the same manner, suggesting the participation of these chemokines in the PAS development [40]. On the other hand, a study conducted by Arakaza, Liu, Zhu and Zou [29] indicated that the expression of insulin-like growth factor 1 (IGF-1), fibroblast growth factor 2 (bFGF), and placental growth factor (PlGF) are important for PAS development since their expression was found higher in PAS placental tissue in comparison to normal placental samples. Interestingly, IGF-1 expression increased among them related to disease severity. This phenomenon might be associated with the function of IGF-1 in the trophoblastic invasion due to it acts as an angiogenic growth factor [41]. This last might explain the behavior of IGF-1 expression related to severity since it is relative to invasion rates.
The role of β-catenin has been studied regarding placental disparities, β-catenin plays important roles in the maintenance of cellular homeostasis as well as intercellular connections, which consolidate cell adhesion [42]. Concerning placental affections, in accreta tissues β-catenin expression is downregulated, which might be an important cause that leads to excessive trophoblastic invasion [43]. Besides, EMT in trophoblasts has been linked with BAP1 high expression; this mechanism was elucidated by observing Bap1-null mouse trophoblast stem cells (mTSCs) by CRISPR/Cas9, resulting in the augmenting ETM rates, which in turn regulates differentiation, invasion, and proliferation capacities [44].
Inflammation is another mechanism involved in the PAS since an interaction exists between the trophoblast and the uterine tissue, resulting in the exacerbated release of proinflammatory mediators [45]. In this regard, in a recent study conducted by Abdel-Hamid, et al. [46], the expression of tumor necrosis factor-alpha (TNF-α), interleukin-1 beta (IL-1β), and IL6 were overexpressed in placentas of patients with invasive placentation (creta placentas) interestingly, their expression levels were associated with the number of EVT, which also are greater in comparison to normal placentation tissue’s samples. It is argued that it might be mainly TNF-α due to its ability to inhibit trophoblastic invasion. Besides, their increased co-expression, TNF-α, IL-1β, and IL6 suggest their pivotal role of these pro-inflammatory mediators in creta pathogenesis.
5.The Roles of Non-Coding RNAs in the PAS
Non-coding RNAs play a pivotal role in the regulation of biological processes, including pathologic development. ncRNAs comprise regulatory molecules, of which micro RNAs (miRNAs) and long non-coding RNAs (lncRNAs) are mainly addressed in the context of biological regulation [47]. Concerning placenta-related illness, there have been identified several ncRNAs and their roles in these pathologic disorders, mainly in intrauterine growth retardation, preeclampsia, and the placenta accreta spectrum stages [48]. Several research has identified valuable information about how ncRNAs present differential expression levels and their roles in the regulation of the PAS [49]. Nonetheless, physiopathological regulation coffered by both, miRNAs and lncRNAs is still limited. In this regard, we next condensate the most relevant pathological roles of ncRNA based on placenta accreta spectrum patients.
5.2.microRNAs
One of the key functions of miRNAs is regulating genes by mediating the degradation of mRNAs. miRNAs influence transcription and translation through two primary mechanisms: the canonical pathway, which has been briefly described earlier, involves the degradation of mRNAs based on the miRNA seed sequence [50]. Furthermore, circulating microRNAs have been demonstrated to play crucial roles in research and clinical settings, particularly in disease monitoring. Changes in circulating miRNAs have been linked to pathological processes, including chronic diseases, cancer, as well as the PAS [51,52].
Concerning miRNA behavior in the PAS development, they are still poorly explored. Nonetheless, there is evidence that their roles are related to cellular processes that accompany pathological development. In this regard, miR-7-5p plays an important role in trophoblast invasion since its overexpression converged in a significant diminution of cell invasion in HTR-8/SVneo cells, moreover, its downregulation results in the increase of SNAIL, SLUG, TWIST, and vimentin expression, promoting EMT and this trophoblast invasion [53]. In extravillous trophoblast cells, miR-519d is highly expressed, and its main activity is to control migration by suppressing CXCL6, FOXL2, and NR4A2; besides MMP2 is a target gene of miR-519d, which suggests that it is involved in trophoblast invasiveness [54]. Murrieta-Coxca, et al. [55] identified a plethora of deregulated expressed miRNAs in placenta accreta tissue, miR-24-3p, miR-193b-3p, miR-331-3p, miR-376c-3p, miR-382-3p, miR-495-3p, miR-519d-3p, and miR-3074-5p were overexpressed in PAS tissue while miR-106b-3p, miR-222-3p, miR-370-3p, miR-454-5p, and miR-3615-3p presented downregulation in PAS tissue, prior biological pathway analysis identified a significant reduction in NF-kB mRNA was confirmed in PAS samples suggesting their roles in a high invasive capacities, presumable by miR-382-3p and miR-495-3p. On the other hand, miR-106b-3p, miR-222-3p, and miR-519d-3p target PTEN, which controls the cell cycle, mainly in trophoblasts proliferation and migration. The microRNA 1296-5p is overexpressed in the tissue of the PAS patient; its roles are presumed to provide regulation of apoptosis since its overexpression affected AGGF1, which, in turn, inhibits P53 and Bax expression, also increasing the expression of Bcl-2 protein [56]. In placenta accreta tissues, overexpression of miR-518b was positively associated with OPN and VEGF, playing important roles in regulating villous trophoblast cell migration, invasion, and adhesion [57]. In creta sites, MCL1 expression is higher than non-creta, specifically in intermediate trophoblast cells, which inhibits apoptosis. The gene MCL1 has been reported as a target gene for both miR-29a/b/c and miR-125a; their cellular role resulted in the promotion of the apoptosis of trophoblast cells, whereby downregulation of MCL1 expression [58,59].
5.2.Long Non-Coding RNAs
Long non-coding RNAs (lncRNAs) are s crucial because they play a vital role in maintaining homeostasis in biological processes. However, lncRNAs also contribute significantly to the development of diseases. Their biogenesis involves a comprehensive genomic system, including promoters, enhancers, and intergenic regions in eukaryotic genomes [60].
The roles exerted by lncRNAs are also pivotal in regulating cellular processes concerning placental invasive behaviors. In this regard, H19 downregulation can sponge microRNA let-7, as a consequence, TβR3 (type III TGF-β receptor) expression is negatively affected, promoting the invasion of extravillous trophoblast (EVT) by increasing migration and invasion rates [61]. High expression of lncRNA SNHG6 enhances invasion of the human extravillous trophoblast HTR-8/SVneo cell line, the mechanism is argued to occur by SNHG6/miR-101-3p/OTUD3 regulatory axis [62]. Another regulatory axis in the PAS has been linked to lncRNA SNHG16 since its expression was diminished in placental affections, like preeclampsia. Nonetheless, its behavior has been evaluated in HTR-8/SVneo cells, after overexpressed, resulting in the creation of cell proliferation, migration, and invasion as well as inhibition of apoptosis, thus by sponging miR-218-5p which in turn suppresses LASP1, a protein that facilitates cell invasion in diverse types of malignancies [63].
Besides, lncRNA uc.187 aberrant expression had been linked with higher proliferation rates, invasion, and lower apoptotic activities in HTR-8/SVneo cells, regarding these mechanisms, they are prompted to act by increasing expression of MMP-2/-9 and PCNA/Ki-67 proteins, enhancing invasion and proliferation respectively, on the contrary, uc.187 overexpression affected Bcl-2 protein, converging in a reduction of cell death in trophoblast cells [64].
Another study found that lncZBTB39 was upregulated in pre-eclampsia-complicated human placentas and that its overexpression could inhibit invasion and migration. However, the expression pattern of lncZBTB39 is unknown and is required for the further use of this biomarker in predictive tests [65].
Several reports indicate the cellular behavior of ncRNAs in placental pathologies. Since placenta accreta is an emerging pathology, many aspects are still unknown. Comprehending molecular mechanisms would aid in developing early diagnostics and treatment in affected women.
Aberrant Signaling Pathways in the Placenta Accreta Spectrum
Several signaling pathways have been involved in the etiology of the PAS, such as the Notch signaling pathway, which is essential in regulating angiogenesis. Regarding the PAS, it is activated through the overexpression of periostin (POSTN), which in turn provokes an increase in the expression of Notch1, HES1, and Hey1, thus activating Notch signaling in the HUVEC cell line during the neovascularization process [66]. The above-mentioned has been linked to an exacerbated hemorrhage in the PAS, mainly attributed to hypervascularity in the uteroplacental and utero-bladder interfaces [67].
Interestingly, AGGF1 has been found to be downregulated in PAS samples, and its deletion in human trophoblast HTR8/SVneo cells enhances mechanisms related to the invasive phenotype of PAS, such as proliferation, invasion, and migration. It also represses apoptosis by downregulating P53 and Bax and stimulating Bcl-2 overexpression, highlighting AGGF1 as a regulator of the P53 signaling axis [56].
Furthermore, the invasive trait of trophoblastic cells has been related to YKL-40 enhancer activity since it is overexpressed in PAS samples and in vitro using HTR8/SVneo cells has promoting proliferation, migration, and invasion, but also inhibits apoptosis through the activation of Akt/MMP9 signaling pathway [68]. Additionally, STAT3, p38, and JNK pathways have been related to trophoblast invasion in the PAS, since FYN stimulates the activation of STAT3, p38, and JNK through phosphorylation [69]. Besides, LAMC2 is overexpressed in placental, and in vitro has shown an increase in cell proliferation, invasion, and migration but inhibited apoptosis, accompanied by elevated protein expression of MMP2, MMP9, and phosphorylated Akt (pAkt) which means that LAMC2 is implicated in the pathogenesis of PAS by activating the PI3K/Akt/MMP2/9 signaling pathway to stimulate trophoblast over-invasion [70].
Duan, et al. [71] found by immunoblotting and qPCR analysis in abnormally invasive placentas (AIP), including PA, PI, or PP, showed that CCN3 overexpression is accompanied by high levels of p53, p16, p21, cyclin D1, Notch-1 cleaved, pFAK, pAkt, and pmTOR, as well as low levels of pRb, suggesting that CCN3 mediates senescence by cell cycle arrest through activation of the FAK-Akt-mTOR pathway and cleaved Notch-1/p21, contributing to increasing the invasion properties of EVT.
Furthermore, growth factor signaling pathways, such as the macrophage-induced netrin-1/DCC/VEGF signaling pathway, have been implicated in trophoblastic angiogenesis in the PAS tissues through netrin-1, DCC receptors, VEGF overexpression, and high recruitment of macrophages compared to normal placental tissue [72]. Likewise, by in vitro assays using the gestational choriocarcinoma cell line JEG-3 and the trophoblast cell line HTR-8/SVneo, it was found that the non-canonical TGF-β-UCHL5-Smad2 signaling pathway is essential for invasion of the EVTs, a critical step in placental development, in which Smad1/5/9 are governing factors. In addition, the TGF-β-UCHL5-Smad2 pathway is also regulated by the ERK signaling pathway since it promotes angiogenesis and vascularization, and alteration of these signaling pathways can cause abnormal placental invasion and angiogenesis, which leads to triggering PA. [73]. Another novel mechanism described involved in the development of the PAS consists of suppressing Wnt-β-catenin/VEGF signaling through pigment epithelium-derived factor (PEDF), downregulated in PAS tissues. In vitro studies revealed that PEDF overexpression inhibits EVTs proliferation, invasion, and angiogenesis, and induces ferroptosis, a newly described form of regulated cell death [74].
Perspectives and Conclusions
We provide an extensive overview of available therapeutic strategies that could aid in early diagnosing the placenta acreta spectrum. It is important to comprehend the molecular mechanisms underlying the PAS, particularly the signaling pathways involved in the early stages accompanying this pathology, which is addressed by trophoblastic invasiveness and angiogenesis. Thus, researchers aim to develop specific biomarkers that can effectively prevent PAS. Besides, exploring the signaling pathways involved would provide valuable tools to develop targeted therapies that can effectively manage PAS are mainly attributed to TGF-β-UCHL5-Smad2, ERK, and Wnt-β-catenin/VEGF pathways, which play significant roles in the development and progression of PAS. Therapeutic strategies targeting these pathways could potentially inhibit abnormal placental invasion and angiogenesis.
Additionally, implementing other molecules as novel biomarkers, such as PDEF, is pivotal to reducing the severity of PAS since it is downregulated in pathological tissues. Otherwise, overexpression of PEDF in vitro has been shown to inhibit proliferation, invasion, and angiogenesis of EVTs and induce ferroptosis, suggesting a promising therapeutic strategy.
The placenta acreta spectrum (PAS) represents a significant obstetric challenge due to its pathologic complexity, as well as it represents severe maternal health risks. The PAS encompasses abnormal trophoblastic invasion that can vary in degrees, which is determined by the depth of myometrial invasion, classifying it in placenta accreta, increta, and percreta. The rise in cesarian delivery rates is a phenomenon that has contributed to increasing the incidence of PAS, underestimating the necessity the need for heightened awareness and early diagnosis [11,13].
Physiopathology accompanying the spectrum is a multifactorial interplay of abnormal placentation, uterine scarring, and impaired decidualization, resulting in abnormal placental adherence [16]. Promising advances in identifying new biomarkers, such as AFP, sFlt-1, β-hCG, PlGF, and PAPP-A, would aid in the early detection and correct management of affected women[22,25,34]. Besides, comprehension of molecular mechanisms, such as genetic expression and the roles of non-coding RNAs, is pivotal for unraveling the complexities of PAS [39,48,49].
Besides, identifying aberrant signaling pathways, such as Notch, PI3K/Akt, STAT3, and TGF-β, offers potential targets for therapeutic interventions to modulate trophoblastic invasion and improve patient outcomes. Since they play pivotal roles in the invasiveness of trophoblastic cells contributing to the PAS pathogenesis [66,69]
Overall, this review highlights the importance of interdisciplinary care, early diagnosis, and a comprehensive understanding of the molecular underpinnings of PAS. Continued research into PAS's biomarkers and molecular mechanisms is crucial for developing effective diagnostic and therapeutic strategies, ultimately improving the prognosis and quality of life for affected women.
Author Contributions
E.L.V. and C.E.M.P. conceived and designed the content of this review, E.L.V., S.A.B.O., E.P.G.G., M.M.M., P.Y.G.A., M.M.A.F., K.P.G.C., D.E.C.L., P.G.Q., and C.E.M.P. wrote the paper, E.L.V., S.A.B.O., and E.P.G.G. conceived supervision and visualization of manuscript, C.E.M.P., E.L.V., and E.P.G.G contributed to revising and editing the paper critically for important intellectual content. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Carrillo, A.P.; Chandraharan, E. Placenta accreta spectrum: Risk factors, diagnosis and management with special reference to the Triple P procedure. Women's Health 2019, 15. [Google Scholar] [CrossRef]
- Cahill, A.G.; Beigi, R.; Heine, P.; Silver, R.M.; Wax, J.R. Obstetric Care Consensus No. 7: Placenta Accreta Spectrum. Obstet. Gynecol. 2018, 132, e259–e275. [Google Scholar] [CrossRef]
- Eller, A.G.; Bardsley, T.R.; Greene, T.; Varner, M.W.; Silver, R.M.; Bowman, Z.S. Risk Factors for Placenta Accreta: A Large Prospective Cohort. Am. J. Perinatol. 2013, 31, 799–804. [Google Scholar] [CrossRef] [PubMed]
- Marshall, N.E.; Fu, R.; Guise, J.-M. Impact of multiple cesarean deliveries on maternal morbidity: a systematic review. Am. J. Obstet. Gynecol. 2011, 205, 262.e1–262.e8. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Jurkovic, D. Placenta accreta: Pathogenesis of a 20th century iatrogenic uterine disease. Placenta 2012, 33, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Jauniaux, E.; Chantraine, F.; Silver, R.M.; Langhoff-Roos, J. for the FIGO Placenta Accreta Diagnosis and Management Expert Consensus Panel FIGO consensus guidelines on placenta accreta spectrum disorders: Epidemiology. Int. J. Gynecol. Obstet. 2018, 140, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Betrán, A.P.; Ye, J.; Moller, A.-B.; Zhang, J.; Gülmezoglu, A.M.; Torloni, M.R. The Increasing Trend in Caesarean Section Rates: Global, Regional and National Estimates: 1990-. PLOS ONE 2016, 11, e0148343. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Zhang, J.; Mikolajczyk, R.; Torloni, M.R.; Gülmezoglu, A.; Betran, A. Association between rates of caesarean section and maternal and neonatal mortality in the 21st century: a worldwide population-based ecological study with longitudinal data. BJOG: Int. J. Obstet. Gynaecol. 2015, 123, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Calagna, G.; Polito, S.; Labate, F.; Guiglia, R.A.; De Maria, F.; Bisso, C.; Cucinella, G.; Calì, G. Placenta Accreta Spectrum Disorder in a Patient with Six Previous Caesarean Deliveries: Step by Step Management. Case Rep. Obstet. Gynecol. 2021, 2021, 1–4. [Google Scholar] [CrossRef]
- van Beekhuizen, H.J.; Stefanovic, V.; Schwickert, A.; Henrich, W.; Fox, K.A.; Gziri, M.M.; Sentilhes, L.; Gronbeck, L.; Chantraine, F.; Morel, O.; et al. A multicenter observational survey of management strategies in 442 pregnancies with suspected placenta accreta spectrum. Acta Obstet. et Gynecol. Scand. 2021, 100, 12–20. [Google Scholar] [CrossRef]
- Zheng, W.; Zhang, H.; Ma, J.; Dou, R.; Zhao, X.; Yan, J.; Yang, H. Validation of a scoring system for prediction of obstetric complications in placenta accreta spectrum disorders. J. Matern. Neonatal Med. 2021, 35, 4149–4155. [Google Scholar] [CrossRef] [PubMed]
- Bartels, H.C.; Postle, J.D.; Downey, P.; Brennan, D.J. Placenta Accreta Spectrum: A Review of Pathology, Molecular Biology, and Biomarkers. Dis. Markers 2018, 2018, 1–11. [Google Scholar] [CrossRef] [PubMed]
- AlQasem, M.H.; Shaamash, A.H.; Al Ghamdi, D.S.; Mahfouz, A.A.; Eskandar, M.A. Incidence, risk factors, and maternal outcomes of major degree placenta previa. SciVee 2023, 44, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Jansen, C.H.J.R.; Kastelein, A.W.; Kleinrouweler, C.E.; Van Leeuwen, E.; De Jong, K.H.; Pajkrt, E.; Van Noorden, C.J.F. Development of placental abnormalities in location and anatomy. Acta Obstet. et Gynecol. Scand. 2020, 99, 983–993. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; A Lorca, R.; Su, E.J. Molecular and cellular underpinnings of normal and abnormal human placental blood flows. J. Mol. Endocrinol. 2018, 60, R9–R22. [Google Scholar] [CrossRef] [PubMed]
- Morlando, M.; Collins, S. Placenta Accreta Spectrum Disorders: Challenges, Risks, and Management Strategies. Int. J. Women's Heal. 2020; 12, 1033–1045. [Google Scholar] [CrossRef]
- Romeo, V.; Verde, F.; Sarno, L.; Migliorini, S.; Petretta, M.; Mainenti, P.P.; D’armiento, M.; Guida, M.; Brunetti, A.; Maurea, S. Prediction of placenta accreta spectrum in patients with placenta previa using clinical risk factors, ultrasound and magnetic resonance imaging findings. La Radiol. medica 2021, 126, 1216–1225. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Wang, Y.; Wu, Y.; Zeng, J.; Yuan, X.; Tong, C.; Qi, H. What we know about placenta accreta spectrum (PAS). Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 259, 81–89. [Google Scholar] [CrossRef]
- Hecht, J.L.; Baergen, R.; Ernst, L.M.; Katzman, P.J.; Jacques, S.M.; Jauniaux, E.; Khong, T.Y.; Metlay, L.A.; Poder, L.; Qureshi, F.; et al. Classification and reporting guidelines for the pathology diagnosis of placenta accreta spectrum (PAS) disorders: recommendations from an expert panel. Mod. Pathol. 2020, 33, 2382–2396. [Google Scholar] [CrossRef]
- Shainker, S.A.; Silver, R.M.; Modest, A.M.; Hacker, M.R.; Hecht, J.L.; Salahuddin, S.; Dillon, S.T.; Ciampa, E.J.; D'Alton, M.E.; Otu, H.H.; et al. Placenta accreta spectrum: biomarker discovery using plasma proteomics. In Proceedings of the Am J Obstet Gynecol, 2020/9//, 2020; pp. 433.e431-433.e414.
- Zhang, T.; Wang, S. Potential Serum Biomarkers in Prenatal Diagnosis of Placenta Accreta Spectrum. Front. Med. 2022, 9, 860186. [Google Scholar] [CrossRef]
- Berezowsky, A.; Pardo, J.; Ben-Zion, M.; Wiznitzer, A.; Aviram, A. Second Trimester Biochemical Markers as Possible Predictors of Pathological Placentation: A Retrospective Case-Control Study. Fetal Diagn. Ther. 2019, 46, 187–192. [Google Scholar] [CrossRef]
- Oztas, E.; Ozler, S.; Caglar, A.T.; Yucel, A. Analysis of first and second trimester maternal serum analytes for the prediction of morbidly adherent placenta requiring hysterectomy. Kaohsiung J. Med Sci. 2016, 32, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Lumbanraja S; Yaznil MR; Siahaan AM; Berry Eka Parda B. Soluble FMS-Like Tyrosine Kinase-1: Role in placenta accreta spectrum disorder. 2022, 10. [CrossRef]
- Zhang, F.; Gu, M.; Chen, P.; Wan, S.; Zhou, Q.; Lu, Y.; Li, L. Distinguishing placenta accreta from placenta previa via maternal plasma levels of sFlt-1 and PLGF and the sFlt-1/PLGF ratio. Placenta 2022, 124, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Büke, B.; Akkaya, H.; Demir, S.; Sağol, S.; Şimşek, D.; Başol, G.; Barutçuoğlu, B. Relationship between first trimester aneuploidy screening test serum analytes and placenta accreta. J. Matern. Neonatal Med. 2017, 31, 59–62. [Google Scholar] [CrossRef]
- Zhou, J.; Li, J.; Yan, P.; Ye, Y.; Peng, W.; Wang, S.; Wang, X.T. Maternal plasma levels of cell-free β-HCG mRNA as a prenatal diagnostic indicator of placenta accrete. Placenta 2014, 35, 691–695. [Google Scholar] [CrossRef]
- Faraji, A.; Akbarzadeh-Jahromi, M.; Bahrami, S.; Gharamani, S.; Shahraki, H.R.; Kasraeian, M.; Vafaei, H.; Zare, M.; Asadi, N. Predictive value of vascular endothelial growth factor and placenta growth factor for placenta accreta spectrum. J. Obstet. Gynaecol. 2021, 42, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Arakaza, A.; Liu, X.; Zhu, J.; Zou, L. Assessment of serum levels and placental bed tissue expression of IGF-1, bFGF, and PLGF in patients with placenta previa complicated with placenta accreta spectrum disorders. J. Matern. Neonatal Med. 2024, 37, 2305264. [Google Scholar] [CrossRef]
- Wang, F.; Chen, S.; Wang, J.; Wang, Y.; Ruan, F.; Shu, H.; Zhu, L.; Man, D. First trimester serum PAPP-A is associated with placenta accreta: a retrospective study. Arch. Gynecol. Obstet. 2021, 303, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Desai, N.; Krantz, D.; Roman, A.; Fleischer, A.; Boulis, S.; Rochelson, B. Elevated first trimester PAPP-A is associated with increased risk of placenta accreta. Prenat. Diagn. 2013, 34, 159–162. [Google Scholar] [CrossRef]
- Thompson, O.; Otigbah, C.; Nnochiri, A.; Sumithran, E.; Spencer, K. First trimester maternal serum biochemical markers of aneuploidy in pregnancies with abnormally invasive placentation. BJOG: Int. J. Obstet. Gynaecol. 2015, 122, 1370–1376. [Google Scholar] [CrossRef]
- Lyell, D.J.; Faucett, A.M.; Baer, R.J.; Blumenfeld, Y.J.; Druzin, M.L.; El-Sayed, Y.Y.; Shaw, G.M.; Currier, R.J.; Jelliffe-Pawlowski, L.L. Maternal serum markers, characteristics and morbidly adherent placenta in women with previa. J. Perinatol. 2015, 35, 570–574. [Google Scholar] [CrossRef]
- Penzhoyan, G.A.; Makukhina, T.B. Significance of the routine first-trimester antenatal screening program for aneuploidy in the assessment of the risk of placenta accreta spectrum disorders. jpme 2019, 48, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, A.; Sekizawa, A.; Ventura, W.; Koide, K.; Hori, K.; Okai, T.; Masashi, Y.; Furuya, K.; Mizumoto, Y. Increased Levels of Cell-Free Human Placental Lactogen mRNA at 28–32 Gestational Weeks in Plasma of Pregnant Women With Placenta Previa and Invasive Placenta. Reprod. Sci. 2014, 21, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhang, N.; Zhang, Y.; Hu, X.; Gao, G.; Ye, Y.; Peng, W.; Zhou, J. Human placental lactogen mRNA in maternal plasma play a role in prenatal diagnosis of abnormally invasive placenta: yes or no? Gynecol. Endocrinol. 2019, 35, 631–634. [Google Scholar] [CrossRef] [PubMed]
- Shainker, S.A.; Dannheim, K.; Gerson, K.D.; Neo, D.; Zsengeller, Z.K.; Pernicone, E.; Karumanchi, S.A.; Hacker, M.R.; Hecht, J.L. Down-regulation of soluble fms-like tyrosine kinase 1 expression in invasive placentation. Arch. Gynecol. Obstet. 2017, 296, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Goh, W.; Yamamoto, S.Y.; Thompson, K.S.; Bryant-Greenwood, G.D. Relaxin, Its Receptor (RXFP1), and Insulin-Like Peptide 4 Expression Through Gestation and in Placenta Accreta. Reprod. Sci. 2013, 20, 968–980. [Google Scholar] [CrossRef] [PubMed]
- Illsley, N.P.; DaSilva-Arnold, S.C.; Zamudio, S.; Alvarez, M.; Al-Khan, A. Trophoblast invasion: Lessons from abnormally invasive placenta (placenta accreta). Placenta 2020, 102, 61–66. [Google Scholar] [CrossRef]
- Long, Y.; Jiang, Y.; Zeng, J.; Dang, Y.; Chen, Y.; Lin, J.; Wei, H.; Xia, H.; Long, J.; Luo, C.; et al. The expression and biological function of chemokine CXCL12 and receptor CXCR4/CXCR7 in placenta accreta spectrum disorders. J. Cell. Mol. Med. 2020, 24, 3167–3182. [Google Scholar] [CrossRef]
- He, X.; Zhao, L.; Yue, L.; Zhang, W.; Wang, W.; Fu, Y.; Feng, Y.; Fu, F. The relationship between IGF1 and the expression spectrum of miRNA in the placenta of preeclampsia patients. Ginekol. Polska 2019, 90, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Pedone, E.; Marucci, L. Role of β-Catenin Activation Levels and Fluctuations in Controlling Cell Fate. Genes 2019, 10, 176. [Google Scholar] [CrossRef] [PubMed]
- Han, Q.; Zheng, L.; Liu, Z.; Luo, J.; Chen, R.; Yan, J. Expression of β-catenin in human trophoblast and its role in placenta accreta and placenta previa. J. Int. Med Res. 2018, 47, 206–214. [Google Scholar] [CrossRef]
- Perez-Garcia, V.; Lea, G.; Lopez-Jimenez, P.; Okkenhaug, H.; Burton, G.J.; Moffett, A.; Turco, M.Y.; Hemberger, M. BAP1/ASXL complex modulation regulates epithelial-mesenchymal transition during trophoblast differentiation and invasion. eLife 2021, 10. [Google Scholar] [CrossRef]
- Cheng, S.-B.; Nakashima, A.; Huber, W.J.; Davis, S.; Banerjee, S.; Huang, Z.; Saito, S.; Sadovsky, Y.; Sharma, S. Pyroptosis is a critical inflammatory pathway in the placenta from early onset preeclampsia and in human trophoblasts exposed to hypoxia and endoplasmic reticulum stressors. Cell Death Dis. 2019, 10, 1–15. [Google Scholar] [CrossRef]
- Abdel-Hamid, A.M.; Mesbah, Y.; Soliman, M.; Firgany, A.-D.L. Dominance of pro-inflammatory cytokines over anti-inflammatory ones in placental bed of creta cases. J. Microsc. Ultrastruct. 2023, 12, 14–20. [Google Scholar] [CrossRef]
- Mattick, J.S.; Amaral, P.P.; Carninci, P.; Carpenter, S.; Chang, H.Y.; Chen, L.-L.; Chen, R.; Dean, C.; Dinger, M.E.; Fitzgerald, K.A.; et al. Long non-coding RNAs: definitions, functions, challenges and recommendations. Nat. Rev. Mol. Cell Biol. 2023, 24, 430–447. [Google Scholar] [CrossRef]
- Monteiro, L.J.; Peñailillo, R.; Sánchez, M.; Acuña-Gallardo, S.; Mönckeberg, M.; Ong, J.; Choolani, M.; Illanes, S.E.; Nardocci, G. The Role of Long Non-Coding RNAs in Trophoblast Regulation in Preeclampsia and Intrauterine Growth Restriction. Genes 2021, 12, 970. [Google Scholar] [CrossRef]
- Kannampuzha, S.; Ravichandran, M.; Mukherjee, A.G.; Wanjari, U.R.; Renu, K.; Vellingiri, B.; Iyer, M.; Dey, A.; George, A.; Gopalakrishnan, A.V. The mechanism of action of non-coding RNAs in placental disorders. Biomed. Pharmacother. 2022, 156, 113964. [Google Scholar] [CrossRef]
- He, L.; Hannon, G.J. MicroRNAs: Small RNAs with a big role in gene regulation. Nat. Rev. Genet. 2004, 5, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.-S.; Su, J.-L.; Hung, M.-C. Dysregulation of MicroRNAs in cancer. J. Biomed. Sci. 2012, 19, 90–90. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Ding, Y.; Liang, B.; Lin, J.; Kim, T.-K.; Yu, H.; Hang, H.; Wang, K. A Systematic Study of Dysregulated MicroRNA in Type 2 Diabetes Mellitus. Int. J. Mol. Sci. 2017, 18, 456. [Google Scholar] [CrossRef]
- Tsai, S.; Shih, J.-C.; Lin, H.-H.; Hsiao, A.-C.; Su, Y.-T.; Chien, C.-L.; Kung, H.-N. Unveiling the role of microRNA-7 in linking TGF-β-Smad-mediated epithelial-mesenchymal transition with negative regulation of trophoblast invasion. FASEB J. 2019, 33, 6281–6295. [Google Scholar] [CrossRef]
- Xie, L.; Sadovsky, Y. The function of miR-519d in cell migration, invasion, and proliferation suggests a role in early placentation. Placenta 2016, 48, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Murrieta-Coxca, J.M.; Barth, E.; Fuentes-Zacarias, P.; Gutiérrez-Samudio, R.N.; Groten, T.; Gellhaus, A.; Köninger, A.; Marz, M.; Markert, U.R.; Morales-Prieto, D.M. Identification of altered miRNAs and their targets in placenta accreta. Front. Endocrinol. 2023, 14, 1021640. [Google Scholar] [CrossRef]
- Wang, R.; Zhao, J.; Liu, C.; Li, S.; Liu, W.; Cao, Q. Decreased AGGF1 facilitates the progression of placenta accreta spectrum via mediating the P53 signaling pathway under the regulation of miR-1296–5p. Reprod. Biol. 2023, 23, 100735. [Google Scholar] [CrossRef] [PubMed]
- Long, Y.; Chen, Y.; Fu, X.-Q.; Yang, F.; Chen, Z.-W.; Mo, G.-L.; Lao, D.-Y.; Li, M.-J. Research on the expression of MRNA-518b in the pathogenesis of placenta accreta. 2019, 23, 23–28.
- Gu, Y.; Meng, J.; Zuo, C.; Wang, S.; Li, H.; Zhao, S.; Huang, T.; Wang, X.; Yan, J. Downregulation of MicroRNA-125a in Placenta Accreta Spectrum Disorders Contributes Antiapoptosis of Implantation Site Intermediate Trophoblasts by Targeting MCLI. Reprod. Sci. 2019, 26, 1582–1589. [Google Scholar] [CrossRef]
- Gu, Y.; Bian, Y.; Xu, X.; Wang, X.; Zuo, C.; Meng, J.; Li, H.; Zhao, S.; Ning, Y.; Cao, Y.; et al. Downregulation of miR-29a/b/c in placenta accreta inhibits apoptosis of implantation site intermediate trophoblast cells by targeting MCLPlacenta 2016, 48, 13–19. [CrossRef]
- Ha, M.; Kim, V.N. Regulation of microRNA biogenesis. Nat. Rev. Mol. Cell Biol. 2014, 15, 509–524. [Google Scholar] [CrossRef]
- Zuckerwise, L.; Li, J.; Lu, L.; Men, Y.; Geng, T.; Buhimschi, C.S.; Buhimschi, I.A.; Bukowski, R.; Guller, S.; Paidas, M.; et al. H19 long noncoding RNA alters trophoblast cell migration and invasion by regulating TβR3 in placentae with fetal growth restriction. Oncotarget 2016, 7, 38398–38407. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Liu, X.; Ren, C.; Zhang, H.; Gao, L. Silencing of LncRNA SNHG6 protects trophoblast cells through regulating miR-101-3p/OTUD3 axis in unexplained recurrent spontaneous abortion. Histochem. J. 2022, 53, 871–882. [Google Scholar] [CrossRef]
- Yu, Z.; Zhang, Y.; Zheng, H.; Gao, Q.; Wang, H. LncRNA SNHG16 regulates trophoblast functions by the miR-218-5p/LASP1 axis. Histochem. J. 2021, 52, 1021–1033. [Google Scholar] [CrossRef] [PubMed]
- Cao, C.; Li, J.; Li, J.; Liu, L.; Cheng, X.; Jia, R. Long Non-Coding RNA Uc.187 Is Upregulated in Preeclampsia and Modulates Proliferation, Apoptosis, and Invasion of HTR-8/SVneo Trophoblast Cells. J. Cell. Biochem. 2017, 118, 1462–1470. [Google Scholar] [CrossRef]
- Tian, J.; Liu, Y.; Hu, M.; Zheng, Y.; Xu, P.; Zhang, L.; Liao, J.; Wu, Y.; Wen, L.; Tong, C.; et al. Upregulated LncZBTB39 in pre-eclampsia and its effects on trophoblast invasion and migration via antagonizing the inhibition of miR-210 on THSD7A expression. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 248, 164–171. [Google Scholar] [CrossRef]
- Li, R.; Wang, W.; Qiu, X.; He, M.; Tang, X.; Zhong, M. Periostin promotes extensive neovascularization in placenta accreta spectrum disorders via Notch signaling. J. Matern. Neonatal Med. 2023, 36, 2264447. [Google Scholar] [CrossRef] [PubMed]
- Calì, G.; D'Antonio, F.; Forlani, F.; Timor-Tritsch, I.E.; Palacios-Jaraquemada, J.M. Ultrasound Detection of Bladder-Uterovaginal Anastomoses in Morbidly Adherent Placenta. Fetal Diagn. Ther. 2016, 41, 239–240. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Wang, R.; Liu, S.; Yin, X.; Huo, Y.; Zhang, R.; Li, J. YKL-40 promotes proliferation and invasion of HTR-8/SVneo cells by activating akt/MMP9 signalling in placenta accreta spectrum disorders. J. Obstet. Gynaecol. 2023, 43, 2211681. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Su, C.; Zhu, L.; Dong, F.; Shu, H.; Zhang, H.; Wang, M.; Wang, F.; Man, D. Highly expressed FYN promotes the progression of placenta accreta by activating STAT3, p38, and JNK signaling pathways. Acta Histochem. 2023, 125, 151991. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Liu, W.; Zhao, J.; Liu, L.; Li, S.; Duan, Y.; Huo, Y. Overexpressed LAMC2 promotes trophoblast over-invasion through the PI3K/Akt/MMP2/9 pathway in placenta accreta spectrum. J. Obstet. Gynaecol. Res. 2022, 49, 548–559. [Google Scholar] [CrossRef] [PubMed]
- Duan, L.; Schimmelmann, M.; Wu, Y.; Reisch, B.; Faas, M.; Kimmig, R.; Winterhager, E.; Köninger, A.; Gellhaus, A. CCN3 Signaling Is Differently Regulated in Placental Diseases Preeclampsia and Abnormally Invasive Placenta. Front. Endocrinol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Badary, D.M.; Elsaied, H.; Abdel-Fadeil, M.R.; Ali, M.K.; Abou-Taleb, H.; Iraqy, H.M. Possible Role of Netrin-1/Deleted in Colorectal Cancer/Vascular Endothelial Growth Factor Signaling Pathway in the Pathogenesis of Placenta Accreta Spectrum: A Case-control Study. Int. J. Gynecol. Pathol. 2024. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, K.; Miyagawa, Y.; Watanabe, S.; Takasaki, K.; Nishizawa, M.; Yatsuki, K.; Takahashi, Y.; Kamata, H.; Kihira, C.; Hiraike, H.; et al. The TGF-β/UCHL5/Smad2 Axis Contributes to the Pathogenesis of Placenta Accreta. Int. J. Mol. Sci. 2023, 24, 13706. [Google Scholar] [CrossRef]
- Li, R.; Weng, X.; Hu, X.; Wang, J.; Zheng, L. Pigment epithelium-derived factor inhibits proliferation, invasion and angiogenesis, and induces ferroptosis of extravillous trophoblasts by targeting Wnt-β-catenin/VEGF signaling in placenta accreta spectrum. Mol. Med. Rep. 2024, 29. [Google Scholar] [CrossRef]
Figure 1.
The placenta accreta spectrum classification. The invasive cells start at the uterine wall (1), severity of the spectrum is relative to the invasive depth, affecting the myometrium layer (2) and subsequently invading the serosa layer (3).
Figure 1.
The placenta accreta spectrum classification. The invasive cells start at the uterine wall (1), severity of the spectrum is relative to the invasive depth, affecting the myometrium layer (2) and subsequently invading the serosa layer (3).
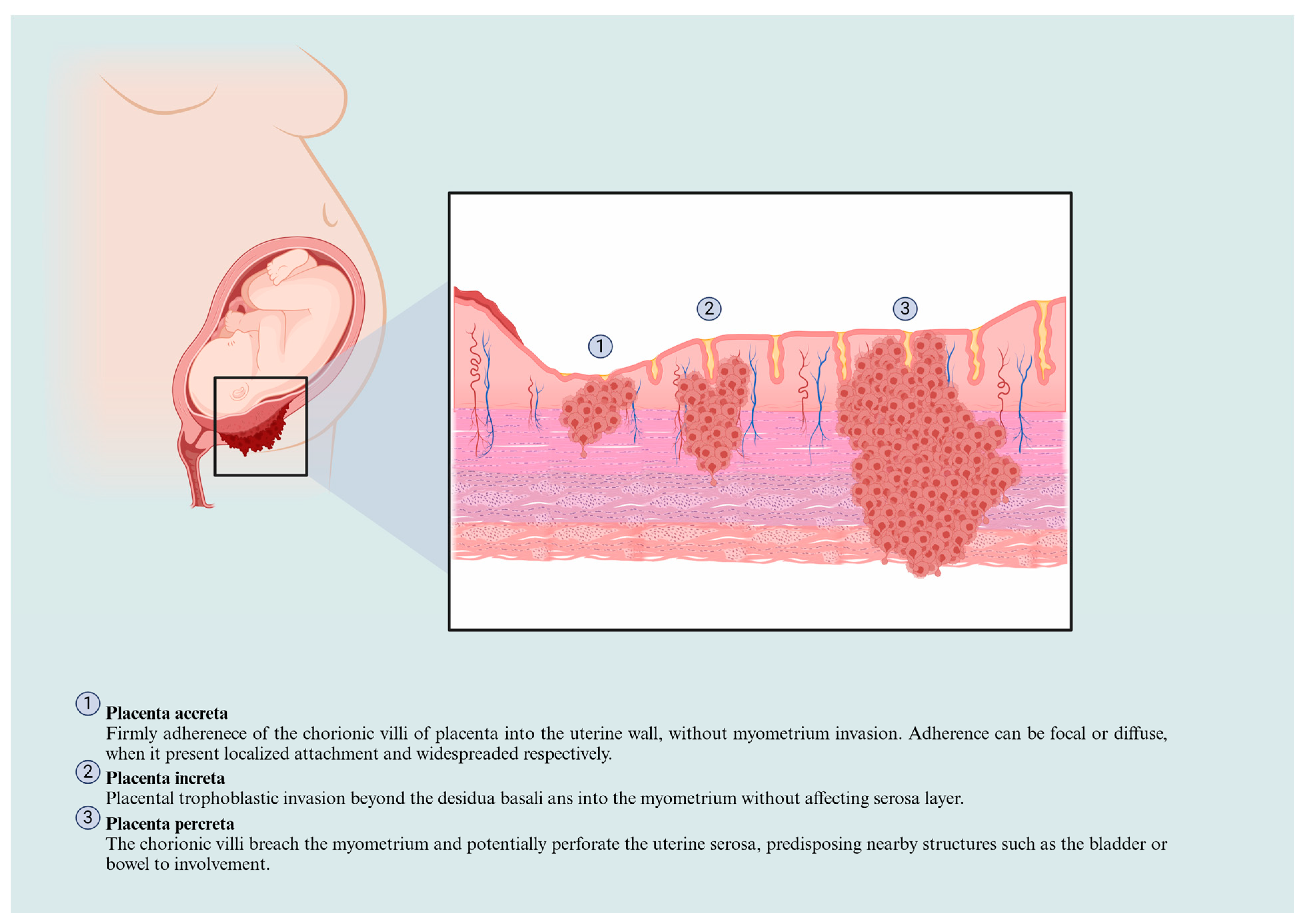

Table 1.
Biomarkers related to placenta accreta spectrum.
| Biomarker | Source | Findings | References |
|---|---|---|---|
| Alpha-fetoprotein(AFP) | Maternal serum | APF showed a sensitivity and specificity of 71 and 46%, respectively to serve as a biomarker for pathological placentation, specifically in women with placenta previa and acreta in the second trimester. Thus, a high level of AFP can be used as suspicion in high-risk pathological placentation. | [22] |
| Maternal serum AFP levels were associated with PAS patients. Nonetheless, was establishedAs a predictor for PAS patients that require hysterectomy with 85.94% sensitivity and 71.43% specificity. | [23] | ||
| Soluble fms-like tyrosine kinase-1(sFlt-1) | Maternal serum | Third-trimester sFlt-1 serum levels are decreased in those PAS-affected women, respectively with its pathological severity. | [24] |
| Maternal plasma | Concentrations of sFlt-1 were lower in patients with PAS than those with normal placentation, with 90.0% sensitivity and 82.0 % specificity. The lower concentrations were also associated with intraoperative blood loss. | [25] | |
| β human chorionic gonadotrophin(β-hCG) | Maternal plasma or serum | The elevated concentration of β-HCG in serum may be appropriate to the prenatal diagnosis of placenta accreta, which suggests the relationship between the risk of PAS in the first trimester. | [26] |
| Maternal serum | hCG showed a sensitivity and specificity of 53 and 68%, respectively, to serve as a biomarker for pathological placentation. Higher levels of hCG can be used as suspicion in high-risk pathological placentation. | [22] | |
| Maternal plasmacell-free β-hCG mRNA | Cell-free β-hCG mRNA concentrations were significantly elevated in women with placenta accreta. This suggests that β-hCG mRNA levels might be a marker for identifying women with placenta accreta likely to require hysterectomy. | [27] | |
| Placental growth factor(PlGF) | Maternal plasma | Concentrations of PLGF were higher in patients with PAS than those with normal placentation, with 86.0% sensitivity and 93.0 % specificity. Higher concentrations were also associated with intraoperative bleeding. | [25] |
| Maternal serum | PIGF serum levels are higher in PAS severity groups than normal placentation patients, including, placenta previa patients. Suggesting it as a predictor criterion exclusive for PAS patients with an 83% sensitivity and 82% specificity. | [28] | |
| Maternal serum and placental bed tissues | High serum levels and high placental bed expression in placenta previa patients with PAS disorders. PlGF serum levels might predict PAS affection, excepting the severity grade based on FIGO. | [29] | |
| Pregnancy-associated plasma protein-A (PAPP-A) | Maternal serum | Increased first-trimester serum was positively associated with placenta accreta, suggesting the potential role of PAPP-A as a biomarker in identifying pregnancies at high risk for placenta accreta. | [26,30-33] |
| A significant correlation was found between PAPP-A levels and blood loss volume. This suggests that first-trimester PAPP-A levels may be thoughtful for the early prediction of pathological blood loss at delivery in pregnant women with PAS and for recognizing a high-risk group for PAS. | [34] | ||
| Human placental lactogen mRNA(hPL mRNA) | Maternal plasma | The expression of hPL mRNA is elevated in the plasma of women diagnosed with placenta previa and invasive placenta between 28 and 32 weeks of gestation. | [35] |
| The multiple of the median (MoM) for hPL mRNA was significantly higher in the placenta accreta group compared to the control and placenta previa groups. | [36] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



