
Submitted:
16 July 2024
Posted:
17 July 2024
You are already at the latest version
Abstract
Obstructive sleep apnea (OSA) often goes unrecognized despite common symptoms such as excessive daytime sleepiness, fatigue, and impaired quality of life (QoL). CPAP is the gold standard treatment for OSA, but optimal daily usage and time needed for observable effects remain unclear. This study aimed to investigate the short-term effects of CPAP on daytime sleepiness and QoL in patients with severe OSA. Medical records were collected from 87 patients with severe OSA who initiated CPAP therapy. Also, validated questionnaires were used before and after one month of CPAP to analyze QoL - the Calgary Sleep Apnea Quality of Life Index (SAQLI), the Cues to CPAP Use Questionnaire (CCUQ), and daytime sleepiness - the Epworth Sleepiness Scale (ESS). Multiple regression analysis was conducted to identify predictors of CPAP usage. Of the total participants aged 55.6±12.5, 77% were males, and 62% were CPAP adherent. Reductions in daytime sleepiness (ESS) were noted, as well as improvements in both overall QoL (SAQLI) and specifically in the domains of daily functioning, social interactions, emotional well-being, and symptom perception. Important cues for CPAP usage recognized by patients were physicians’ instructions and physicians’ worry regarding patients' condition. Furthermore, multiple regression revealed higher SAQLI scores and lower ESS scores as positive predictors of CPAP usage, along with lower AHI after one month of CPAP being associated with sufficient adherence.
Keywords:
obstructive sleep apnea
; OSA
; severe OSA
; CPAP
; adherence
; quality of life
1. Introduction
It has been estimated that approximately 4.7% of the worldwide population have obstructive sleep apnea (OSA), with 2% of cases being severe [1,2,3]. Characterized by recurrent collapses of the upper airway during sleep, OSA usually presents with snoring and reduced airflow due to decreased activity of the upper airway dilator muscles and narrowed airway [4,5,6]. Due to multiple interruptions of sleep by breathing cessations, signs and symptoms of OSA include non-restorative sleep, excessive daytime sleepiness, fatigue, tiredness, lack of energy, abrupt awakenings, and morning headaches [7,8]. Furthermore, OSA occurs significantly more frequently in patients with conditions such as arterial hypertension, hyperlipidemia, type 2 diabetes mellitus, atrial fibrillation, stroke, obesity, posttraumatic stress disorder, and major depressive disorder [9,10,11].
Several studies have confirmed the significant impairment of the quality of life (QoL) in OSA patients [12,13]. Although the concept of QoL is challenging to define, it encompasses overall well-being involving both objective and subjective determinants related to physical, material, social, and emotional aspects [14]. Furthermore, improving QoL might result in superior patient care and rehabilitation, as well as in reduced disease symptoms [15]. Additionally, the concept of health-related QoL is considered to reflect the impact of illness and treatment on patient disability and daily functioning [14,15]. Due to the complex and comprehensive nature of QoL, numerous instruments are employed to assess it, primarily developed based on empirical considerations [15]. The Calgary Sleep Apnea Quality of Life Index (SAQLI) is specifically designed to examine the health-related QoL in OSA patients, also enabling measurement of changes in patients' conditions following therapeutic interventions [13,16].
In addition to therapeutic recommendations for lifestyle changes, continuous positive airway pressure (CPAP) remains the gold standard treatment for symptomatic OSA patients [8,17]. Furthermore, it has been shown that CPAP reduces daytime sleepiness and improves health-related QoL [18]. However, CPAP adherence in OSA patients often remains unsatisfactory, with some studies revealing that up to 80% of patients use the CPAP for less than 4 hours per night [8,17,18]. The necessary duration of device usage to achieve optimal therapeutic effects is yet to be determined, and most studies have focused on the therapy's effectiveness in improving the QoL after several months of usage [17,18] even though symptoms such as daytime sleepiness may reduce as early as following one month of therapy initiation [19].
Therefore, the aim of our study was to assess the effects of one month of CPAP treatment on the QoL (SAQLI) and daytime sleepiness (Epworth sleepiness scale, ESS) in severe OSA patients. Additionally, using the Cues to CPAP Use Questionnaire (CCUQ), we aimed to identify the reasons contributing the most to patients' initiation of therapy.
2. Materials and Methods
2.1. Ethics
The research followed the principles of the Helsinki Declaration (20) and other relevant guidelines, providing ethical conduct and the participants’ safety. Before study enrollment, all participants signed the informed consent, and confidentiality was maintained throughout the study. The Ethics Committee of the University of Split School of Medicine approved the study (protocol code: 003-08/22-03/0003).
2.2. Patients
A total of 87 consecutive severe OSA patients ranging from 27 to 80 years of age, diagnosed between October 1, 2022, and May 31, 2023, at the Sleep Medicine Center of the University of Split School of Medicine and the University Hospital of Split, were included in the study. Patients were assessed with either whole-night polysomnography (PSG) or polygraphy (PG), and severe OSA was defined as an apnea-hypopnea index (AHI) of ≥30 (8). Additionally, the inclusion criteria were an age of 18 years or older and the necessary physical and mental capability to adhere to the research protocol, assessed by the attending physician.
2.3. Questionnaires
A total of three validated questionnaires were used: the Epworth Sleepiness Scale (ESS) [21,22,23], the Calgary Sleep Apnea Quality of Life Index (SAQLI) [16,24], and the Cues to CPAP Use Questionnaire (CCUQ) [25].
The ESS assesses participants’ possibility of falling asleep in eight common daily situations and is widely used in multiple languages and clinical settings [21,22]. The participants respond on a scale from 0 (never doze) to 3 (high chance of dozing), with a total score ranging from 0 to 24 [23], and a higher score indicates increased daytime sleepiness [23].
The SAQLI evaluates the health-related quality of life in patients with OSA, primarily for research purposes rather than routine clinical practice [16,24]. It consists of 45 questions distributed across distinct domains: daily functioning (A), social interactions (B), emotional functioning (C), patient-selected or nominated symptoms potentially due to OSA (D), and treatment-related symptoms (E). Responses for Domain E are exclusively filled out after therapy implementation. Each question is rated on a scale from 1 (indicating maximum impairment) to 7 (indicating no impairment) [16,24]. The average score is calculated for each specific domain. To determine the overall SAQLI score, the result of Domain E is subtracted from the score of each domain, and the average is subsequently computed. This unique characteristic of the questionnaire incorporates therapy side effects [16,24].
The final questionnaire, CCUQ, aims to identify the primary factors influencing a patient's decision to commence CPAP therapy. The questionnaire consists of nine items or potential reasons, to which respondents provide answers on a scale from 0 (not at all) to 3 (extremely important) [25].
2.4. Data Collection and Statistical Analysis
Before undergoing PSG or PG procedures, demographic data, medical history, and comorbidity information were collected, alongside the completion of the ESS. Following this, all patients underwent either the whole-night PSG (Alice 6, Philips Respironics, Eindhoven, the Netherlands) or PG recording (Alice NightOne, Philips Respironics, Eindhoven, the Netherlands and SOMNOcheck2, Weinmann, Hamburg, Germany). Obtained data were manually scored and OSA was diagnosed according to AASM diagnostic criteria and ESRS guidelines [26].
Before initiating CPAP therapy, all 87 patients were asked to complete the pen-and-paper SAQLI questionnaire. A total of 55 patients (63.2%) agreed to attend a follow-up check-up after one month of CPAP usage, during which data from the CPAP memory cards showing usage were extracted. Participants also completed the CCUQ as well as the follow-ups of ESS and SAQLI questionnaires. Follow-up data was collected in 47 participants for CCUQ, 53 participants for ESS, and 53 participants for the SAQLI (Figure 1).
Data analysis was done in Microsoft Excel, version 13.0 (Microsoft Corporation, Redmond, WA, USA), and SPSS Statistics 23.0 (IBM Corporation, Armonk, NY, USA). Continuous data were presented as mean ± standard deviation (SD), while categorical variables were expressed as absolute numbers and percentages. For the comparison of continuous variables, the t-test for independent samples was used, while the χ²-test was used for nominal scale data. To assess the differences in questionnaire results before and after CPAP therapy, repeated measures ANOVA was conducted. The ANOVA analysis on SAQLI was conducted for 53 patients who completed questionnaires before and after CPAP. However, considering that the initial ESS was filled out by 77 patients, the ANOVA analysis was conducted on the 44 who completed the ESS both before and after one month of CPAP usage (Figure 1). Patients were categorized based on CPAP compliance (percentage of days with CPAP usage ≥4 hours per day). Those who used CPAP ≥4 hours per day on less than 70% of days were classified as non-adherent, whereas those with usage of 70% or more were considered adherent. The odds ratio was calculated for the association between CCUQ and CPAP compliance, with significance assessed using the Fisher exact test. The association of CPAP compliance with the following variables: AHI, ESS score before CPAP initiation, and total SALQI score before CPAP usage was analyzed by multiple regression. A p-value of <0.05 was considered statistically significant.
3. Results
During the study, a total of 87 patients with a mean age of 55.6±12.5 years, were diagnosed with severe OSA and were enrolled in the study. The majority were male (77%) and the body mass index was 33.2±7.4 kg/m2 (Table 1). Polysomnography or polygraphy results revealed an AHI of 50.5±19.1 with a mean oxygen saturation of 92.8%±3.6%.
After one month of CPAP usage, 55 patients consented to a regular follow-up examination, when data from CPAP memory cards were extracted (Table 2). Based on the percentage of days with CPAP usage ≥4 hours per day, 21 of them, or 38.2%, were classified as non-compliant, while 61.8% were compliant. The mean AHI during CPAP usage was found to be 4.7±4.6. AHI among non-compliant patients was significantly higher than among compliant patients (6.5±6.3 vs. 3.5±2.8, respectively, p=0.018).
At the check-up after one month of CPAP therapy, the scores for all domains of SAQLI were significantly lower, including daily functioning (domain A), social interactions (domain B), emotional functioning (domain C), and patient-selected or nominated symptoms potentially due to OSA (domain D), indicating better quality of life (Table 3). Additionally, the total score after one month of CPAP therapy was significantly lower than the pre-CPAP score (3.4±1.1 vs. 1.7±0.9, respectively, p<0.001). Patients exhibited significantly lower check-up ESS score indicating lower daytime sleepiness (7.2±5.1 vs. 4.6±4.2, p=0.004).
As shown in Figure 2, non-compliant patients exhibited higher endorsement rates on all items of the CCUQ except for Q3 ("I started using CPAP because my partner couldn't sleep because of my snoring") and Q6 ("My partner encouraged me to start using CPAP").
Responses to the CCUQ were grouped into two categories: "not at all" and "little important" vs. "moderately important" and "extremely important". The association between CPAP compliance and the relevance of the specific cue is shown in Table 4. It was demonstrated that the statistically significant difference was only observed for Q2 ("I started using CPAP because I was worried about my heart") where answers "moderately or extremely important" were associated with subsequent CPAP non-compliance (OR: 0.263 (95% CI: 0.028-2.443); p=0.022). Therefore, it appears that patients starting to use CPAP due to heart concerns have a low probability of being in the compliant group. Overall, patients most frequently reported the relevance of Q1 indicating the relevance of physicians’ instructions, and Q4 indicating the physicians' worry regarding patients' condition.
Multiple regression analysis confirmed both ESS and SAQLI before CPAP in patients diagnosed with severe OSA were significantly associated with CPAP compliance, explaining 13.7% of the variability, while AHI was not (Table 5).
4. Discussion
The results of this study showed that severe OSA patients had an improvement in OSA-related quality of life and reduced daytime sleepiness following one month of CPAP therapy. This improvement was established in daily functioning, social interactions, emotional well-being, and symptom perception, emphasizing the benefits of effective OSA treatment on patients' quality of life.
It has been shown that CPAP is efficient in mitigating respiratory events during sleep in severe OSA patients, and it also has favorable effects on alleviating symptomatic manifestations of OSA and improving daytime functioning [7,12,13]. This was supported by the results of the present study showing a significant reduction in AHI and daytime sleepiness among compliant patients.
Previous studies reported lower QoL with poor sleep quality, excessive daytime sleepiness, dizziness, headaches, decreased concentration, mood changes, impaired hearing, and voice alteration among OSA patients when compared to the general population [7,12,17,27,28,29,30]. In OSA patients QoL is closely associated with factors such as age, stress, lifestyle, depression, BMI, and overall health status [28]. Numerous studies have investigated the impact of various factors on the broad concept of QoL, yet the distinctive influence of individual factors remains unclear [28]. In recent years, improvement in QoL has become a relevant aim in the OSA treatment [17]. CPAP successfully alleviates symptoms and reduces disease severity [17,28,30,31,32], and improves QoL due to improvement in neurocognitive function, sleep quality and restfulness, emotional well-being, symptoms of depression, and social functioning [28,29,30]. This is in accordance with the results of the current study, showing an improvement across all analyzed domains of QoL, including daily functioning, social interactions, emotional functioning, and patient-selected symptoms.
In the present study, where the QoL was assessed with an OSA-specific SAQLI questionnaire, the overall score significantly decreased within only one month, surpassing the clinically meaningful score change. Improvements were observed in daily functioning, social interactions, emotional well-being, and symptom perception. Differences between SAQLI and other QoL questionnaires include its OSA-specificity, and considering treatment-related symptoms [7,13,16]. Furthermore, SAQLI has a high correlation with the widely used, disease-nonspecific 36-Item Short Form Health Survey [SF-36] [13]. A recent meta-analysis found that SAQLI scores remained improved at both 3 and 12 months with CPAP therapy [7], while previous studies also report improvements at 6 months, but not at 2 months of CPAP therapy [13]. Still, the observed 1.7-point improvement in our study has been recognized within one month of CPAP therapy, and such findings may be attributed to the fact that all patients had severe OSA with an average AHI of 50.
This study included severe OSA patients, predominantly middle-aged men with increased BMI, reflecting previously established OSA risk factors [34]. Based on CPAP usage data, 38.2% of enrolled severe OSA patients were non-compliant, reflecting the world trends [18,35] and highlighting the challenges in achieving optimal CPAP adherence [5,18]. OSA is considered a disease with one of the poorest adherence rates to therapy, with non-adherence rates ranging from 29% to 83% [18]. Consequently, recent research has focused on strategies to increase CPAP adherence, including educational materials, regular check-ups, motivational therapy, telephone calls, online consultations, or home visits [5,18,36,37]. However, the effectiveness of these interventions is questionable [5,18]. Behavioral therapy, such as motivational interviewing, has been proven to be one of the most effective for CPAP compliance [18]. Nevertheless, it requires highly educated staff and considerable one-on-one time with patients [18]. On the other hand, educational materials whether in written or video format, although incomprehensible to some patients, offer a relatively straightforward approach and, according to some authors, significantly increase adherence [18]. Additionally, adherence after just one month serves as a good predictor of future adherence [38], providing an opportunity for targeted interventions in those exhibiting poor adherence in the short term. Nonetheless, additional research is imperative to ascertain the most effective approaches. However, it is favorable that in our study even patients classified as non-compliant still attempted to use CPAP, and they might become compliant users in the coming months. One might presume that just one month of usage was not sufficient for them to adapt to the device, hence they had poorer compliance results.
To provide a comprehensive analysis of CPAP compliance, the current study also assessed the patient attitudes and motivations influencing CPAP compliance using the CCUQ questionnaire. A significant predictor of non-compliance in our study was patients’ concern regarding cardiovascular health. Previous research has presented conflicting views regarding hypertension as an indicator of cardiovascular health concerning CPAP compliance [39]. While some authors consider it a predictor of compliance, others suggest it indicates non-compliance, with certain studies showing no correlation at all [39]. Various other predictors of CPAP compliance have also demonstrated variability depending on the setting and study group [3,39]. Nevertheless, established predictors associated with higher adherence include older age, female sex, ESS>10, severe OSA [AHI>30], health insurance coverage, lower rates of depression and insomnia, lower SpO2 levels, and the use of hypnotics [3,39]. A recent systematic review emphasizes patient personality and their beliefs and cognitions as significant predictors of adherence [40], as well as the value patients place on their health and their self-efficacy, referring to their confidence and ability to self-manage CPAP treatment [40,41].
Our multiple regression analysis revealed lower ESS scores and higher SAQLI domains measured before CPAP initiation as significant predictors of CPAP compliance. Namely, patients' subjective perception of worse QoL was a significant predictor of better adherence. Our finding regarding ESS contrasts with existing literature [19,42], suggesting that in severe OSA patients, domains of QoL would have a stronger impact on better CPAP adherence, rather than daytime sleepiness measured by ESS. Furthermore, AHI levels before CPAP therapy were not significant predictors of CPAP compliance. While it is well-established that CPAP significantly reduces AHI [19], the fact that adherence was not associated with AHI in our patients emphasizes the necessity of considering additional factors that might influence the compliance in this population. These factors might be associated to patient-specific characteristics, such as belonging to a certain OSA phenotype cluster [43], which significantly influences the variability in treatment adherence and thus merits further investigation.
Limitations of the study are a relatively small sample size, and single-center setting, which might limit the generalization of findings. Thus, future research should include larger, multicenter studies and focus on additional determinants of CPAP compliance, such as psychosocial factors, socioeconomic status, and healthcare system-related barriers. Moreover, longitudinal studies with extended follow-up periods could evaluate long-term treatment effects on QoL and adherence patterns among patients undergoing CPAP therapy.
5. Conclusions
In conclusion, this study provides valuable insights into the quality of life, compliance patterns, and reasons relevant for good CPAP adherence among severe OSA patients undergoing CPAP therapy. Furthermore, the study highlights the importance of addressing patient-centered factors in promoting CPAP adherence and the use of disease-specific questionnaires such as SAQLI. Tailored interventions aimed at optimizing CPAP adherence and enhancing treatment outcomes among patients with severe OSA should be used to improve long-term treatment compliance and efficacy.
Author Contributions
Conceptualization, Karla Milinovic, Ivana Pavlinac Dodig, Linda Lusic Kalcina, Renata Pecotic and Zoran Dogas; Formal analysis, Ivana Pavlinac Dodig, Linda Lusic Kalcina and Maja Valic; Investigation, Karla Milinovic, Renata Pecotic, Natalija Ivkovic and Zoran Dogas; Methodology, Karla Milinovic, Ivana Pavlinac Dodig, Linda Lusic Kalcina, Natalija Ivkovic, Maja Valic and Zoran Dogas; Supervision, Renata Pecotic and Zoran Dogas; Validation, Linda Lusic Kalcina, Renata Pecotic, Natalija Ivkovic and Maja Valic; Visualization, Karla Milinovic, Ivana Pavlinac Dodig, Linda Lusic Kalcina, Renata Pecotic, Natalija Ivkovic and Zoran Dogas; Writing – original draft, Karla Milinovic and Ivana Pavlinac Dodig; Writing – review & editing, Ivana Pavlinac Dodig, Linda Lusic Kalcina, Renata Pecotic, Natalija Ivkovic, Maja Valic and Zoran Dogas.All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Biomedical Ethics Committee of the University of Split School of Medicine, Split, Croatia (protocol code: 003-08/22-03/0003 and date of approval: December 9th, 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study, and confidentiality was maintained throughout the study.
Data Availability Statement
The data presented in this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors wish to thank Dijana Radanovic, Vjera Solic, and Jelena Baricevic for technical assistance in data collection.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Benjafield AV, Ayas NT, Eastwood PR, Heinzer R, Ip MSM, Morrell MJ, Nunez CM, Patel SR, Penzel T, Pépin JL, Peppard PE, Sinha S, Tufik S, Valentine K, Malhotra A. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019, 7(8), 687-98. [CrossRef]
- Stradling J. Obstructive sleep apnoea. BMJ. 2007, 335(7615), 313-4. [CrossRef]
- Madbouly, E.M.; Nadeem, R.; Nida, M.; Molnar, J.; Aggarwal, S.; Loomba, R. The Role of Severity of Obstructive Sleep Apnea Measured by Apnea–Hypopnea Index in Predicting Compliance With Pressure Therapy, a Meta-analysis. Am. J. Ther. 2014, 21, 260–264. [CrossRef]
- West SD, Turnbull C. Obstructive sleep apnoea. Eye (Lond). 2018, 32(5), 889-903. [CrossRef]
- Rapelli, G.; Pietrabissa, G.; Manzoni, G.M.; Bastoni, I.; Scarpina, F.; Tovaglieri, I.; Perger, E.; Garbarino, S.; Fanari, P.; Lombardi, C.; et al. Improving CPAP Adherence in Adults With Obstructive Sleep Apnea Syndrome: A Scoping Review of Motivational Interventions. Front. Psychol. 2021, 12. [CrossRef]
- Wang, Y.; Shou, X.; Wu, Y.; Fan, Z.; Cui, J.; Zhuang, R.; Luo, R. Relationships Between Obstructive Sleep Apnea and Cardiovascular Disease: A Bibliometric Analysis (2010-2021). Med Sci. Monit. 2021, 27, e933448–e933448-12. [CrossRef]
- Labarca G, Saavedra D, Dreyse J, Jorquera J, Barbe F. Efficacy of CPAP for Improvements in Sleepiness, Cognition, Mood, and Quality of Life in Elderly Patients With OSA: Systematic Review and Meta-analysis of Randomized Controlled Trials. Chest. 2020, 158(2), 751-64. [CrossRef]
- Gottlieb DJ, Punjabi NM. Diagnosis and Management of Obstructive Sleep Apnea: A Review. JAMA. 2020, 323(14), 1389-400. [CrossRef]
- Labarca, G.; Schmidt, A.; Dreyse, J.; Jorquera, J.; Enos, D.; Torres, G.; Barbe, F. Efficacy of continuous positive airway pressure (CPAP) in patients with obstructive sleep apnea (OSA) and resistant hypertension (RH): Systematic review and meta-analysis. Sleep Med. Rev. 2021, 58, 101446. [CrossRef]
- Zinchuk, A.V.; Gentry, M.J.; Concato, J.; Yaggi, H.K. Phenotypes in obstructive sleep apnea: A definition, examples and evolution of approaches. Sleep Med. Rev. 2017, 35, 113–123. [CrossRef]
- Gupta, M.A.; Simpson, F.C. Obstructive Sleep Apnea and Psychiatric Disorders: A Systematic Review. J. Clin. Sleep Med. 2015, 11, 165–175. [CrossRef]
- Pecotic, R.; Dodig, I.P.; Valic, M.; Galic, T.; Kalcina, L.L.; Ivkovic, N.; Dogas, Z. Effects of CPAP therapy on cognitive and psychomotor performances in patients with severe obstructive sleep apnea: a prospective 1-year study. Sleep Breath. 2018, 23, 41–48. [CrossRef]
- Batool-Anwar, S.; Goodwin, J.L.; Kushida, C.A.; Walsh, J.A.; Simon, R.D.; Nichols, D.A.; Quan, S.F. Impact of continuous positive airway pressure (CPAP) on quality of life in patients with obstructive sleep apnea (OSA). J. Sleep Res. 2016, 25, 731–738. [CrossRef]
- Karimi M, Brazier J. Health, Health-Related Quality of Life, and Quality of Life: What is the Difference? Pharmacoeconomics. 2016, 34(7), 645-9. [CrossRef]
- Haraldstad K, Wahl A, Andenæs R, Andersen JR, Andersen MH, Beisland E, Borge CR, Engebretsen E, Eisemann M, Halvorsrud L, Hanssen TA, Haugstvedt A, Haugland T, Johansen VA, Larsen MH, Løvereide L, Løyland B, Kvarme LG, Moons P, Norekvål TM, Ribu L, Rohde GE, Urstad KH, Helseth S; LIVSFORSK network. A systematic review of quality of life research in medicine and health sciences. Qual Life Res. 2019, 28(10), 2641-50. [CrossRef]
- Flemons, W.W.; Reimer, M.A. Measurement Properties of the Calgary Sleep Apnea Quality of Life Index. Am. J. Respir. Crit. Care Med. 2002, 165, 159–164. [CrossRef]
- Kuhn E, Schwarz EI, Bratton DJ, Rossi VA, Kohler M. Effects of CPAP and Mandibular Advancement Devices on Health-Related Quality of Life in OSA: A Systematic Review and Meta-analysis. Chest. 2017, 151(4), 786-94. [CrossRef]
- Bakker JP, Weaver TE, Parthasarathy S, Aloia MS. Adherence to CPAP: What Should We Be Aiming For, and How Can We Get There? Chest. 2019, 155(6), 1272-87. [CrossRef]
- Battan G, Kumar S, Panwar A, Atam V, Kumar P, Gangwar A, Roy U. Effect of CPAP Therapy in Improving Daytime Sleepiness in Indian Patients with Moderate and Severe OSA. J Clin Diagn Res. 2016;10(11):OC14-OC16. [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013, 310(20), 2191-4.
- Pecotic, R.; Dodig, I.P.; Valic, M.; Ivkovic, N.; Dogas, Z. The evaluation of the Croatian version of the Epworth sleepiness scale and STOP questionnaire as screening tools for obstructive sleep apnea syndrome. Sleep Breath. 2011, 16, 793–802. [CrossRef]
- A Walker, N.; Sunderram, J.; Zhang, P.; Lu, S.-E.; Scharf, M.T. Clinical utility of the Epworth sleepiness scale. Sleep Breath. 2020, 24, 1759–1765. [CrossRef]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [CrossRef]
- Flemons, W.W.; Reimer, M.A. Development of a Disease-specific Health-related Quality of Life Questionnaire for Sleep Apnea. Am. J. Respir. Crit. Care Med. 1998, 158, 494–503. [CrossRef]
- Olsen, S.; Smith, S.; Oei, T.P.S.; Douglas, J. Cues to starting CPAP in obstructive sleep apnea: development and validation of the cues to CPAP Use Questionnaire. J. Clin. Sleep Med. 2010, 6, 229–37. [CrossRef]
- AASM International Classification of Sleep Disorders—Third Edition (ICSD-3) [(accessed on 25 March 2023)]. Available online: https://learn.aasm.org/Listing/a1341000002XmRvAAK.
- Kim, T. Quality of Life in Metabolic Syndrome Patients Based on the Risk of Obstructive Sleep Apnea. Behav. Sci. 2024, 14, 127. [CrossRef]
- Lee W, Lee SA, Ryu HU, Chung YS, Kim WS. Quality of life in patients with obstructive sleep apnea: Relationship with daytime sleepiness, sleep quality, depression, and apnea severity. Chron Respir Dis. 2016, 13(1), 33-9. [CrossRef]
- Hamada, S.; Togawa, J.; Sunadome, H.; Nagasaki, T.; Takahashi, N.; Hirai, T.; Sato, S. Sleep Restfulness in Patients with Obstructive Sleep Apnea Undergoing Continuous Positive Airway Pressure Therapy. Sleep Sci. 2024, 17, e37–e44. [CrossRef]
- Sgaria, V.P.; Cielo, C.A.; Bortagarai, F.M.; Fleig, A.H.D.; Callegaro, C.C. CPAP Treatment Improves Quality of Life and Self-perception of Voice Impairment in Patients with OSA. J. Voice 2024. [CrossRef]
- Singh, A.; Bhat, A.; Saroya, J.; Chang, J.; Durr, M.L. Sociodemographic and Healthcare System Barriers to PAP Alternatives for Adult OSA: A Scoping Review. Laryngoscope 2024. [CrossRef]
- Sun, L.; Chang, Y.-F.; Wang, Y.-F.; Xie, Q.-X.; Ran, X.-Z.; Hu, C.-Y.; Luo, B.; Ning, B. Effect of Continuous Positive Airway Pressure on Blood Pressure in Patients with Resistant Hypertension and Obstructive Sleep Apnea: An Updated Meta-analysis. Curr. Hypertens. Rep. 2024, 26, 201–211. [CrossRef]
- Najafi, A.; Ala, M.; Amali, A.; Hivechi, N.; Heidari, R.; Mokary, Y. An Evaluation of Obstructive Sleep Apnea Patient’s Quality of life Following Continuous Positive Airway Pressure and Uvulopalatopharyngoplasty. Indian J. Otolaryngol. Head Neck Surg. 2023, 76, 1–5. [CrossRef]
- Yeghiazarians Y, Jneid H, Tietjens JR, Redline S, Brown DL, El-Sherif N, Mehra R, Bozkurt B, Ndumele CE, Somers VK. Obstructive Sleep Apnea and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation. 2021, 144(3), e56-e67. [CrossRef]
- Weaver, T.E.; Grunstein, R.R. Adherence to Continuous Positive Airway Pressure Therapy: The Challenge to Effective Treatment. Proc. Am. Thorac. Soc. 2008, 5, 173–178. [CrossRef]
- Franke, C.; Piezonna, F.; Schäfer, R.; Grimm, A.; Loris, L.-M.; Schwaibold, M. Effect of a digital patient motivation and support tool on CPAP/APAP adherence and daytime sleepiness: a randomized controlled trial. Sleep Biol. Rhythm. 2023, 22, 49–63. [CrossRef]
- Schisano, M.; Libra, A.; Rizzo, L.; Morana, G.; Mancuso, S.; Ficili, A.; Campagna, D.; Vancheri, C.; Bonsignore, M.R.; Spicuzza, L. Distance follow-up by a remote medical care centre improves adherence to CPAP in patients with obstructive sleep apnoea over the short and long term. J. Telemed. Telecare 2024. [CrossRef]
- Gabryelska, A.; Sochal, M.; Wasik, B.; Szczepanowski, P.; Białasiewicz, P. Factors Affecting Long-Term Compliance of CPAP Treatment—A Single Centre Experience. J. Clin. Med. 2021, 11, 139. [CrossRef]
- Cho, S.-E.; Jung, J.H.; Kang, J.M.; Cho, M.Y.; Lee, Y.S.; Kang, S.-G.; Kim, S.T. Predictors of Continuous Positive Airway Pressure Adherence and Comparison of Clinical Factors and Polysomnography Findings Between Compliant and Non-Compliant Korean Adults With Obstructive Sleep Apnea. Psychiatry Investig. 2024, 21, 200–207. [CrossRef]
- Kasetti, P.; Husain, N.; Skinner, T.; Asimakopoulou, K.; Steier, J.; Sathyapala, S. Personality traits and pre-treatment beliefs and cognitions predicting patient adherence to continuous positive airway pressure: A systematic review. Sleep Med. Rev. 2024, 74, 101910. [CrossRef]
- Kojima, S.; Saito, A.; Sasaki, F.; Hayashi, M.; Mieno, Y.; Sakakibara, H.; Hashimoto, S. Associations of self-efficacy and outcome expectancy with adherence to continuous positive airway pressure therapy in Japanese patients with obstructive sleep apnea. Fujita Med. J. 2022, 9, 142–146. [CrossRef]
- Laratta, C.R.; Ayas, N.T.; Povitz, M.; Pendharkar, S.R. Diagnosis and treatment of obstructive sleep apnea in adults. Can. Med Assoc. J. 2017, 189, E1481–E1488. [CrossRef]
- Bailly, S.; Grote, L.; Hedner, J.; Schiza, S.; McNicholas, W.T.; Basoglu, O.K.; Lombardi, C.; Dogas, Z.; Roisman, G.; Pataka, A.; et al. Clusters of sleep apnoea phenotypes: A large pan-European study from the European Sleep Apnoea Database (ESADA). Respirology 2020, 26, 378–387. [CrossRef]
Figure 1.
A flowchart diagram of the study.
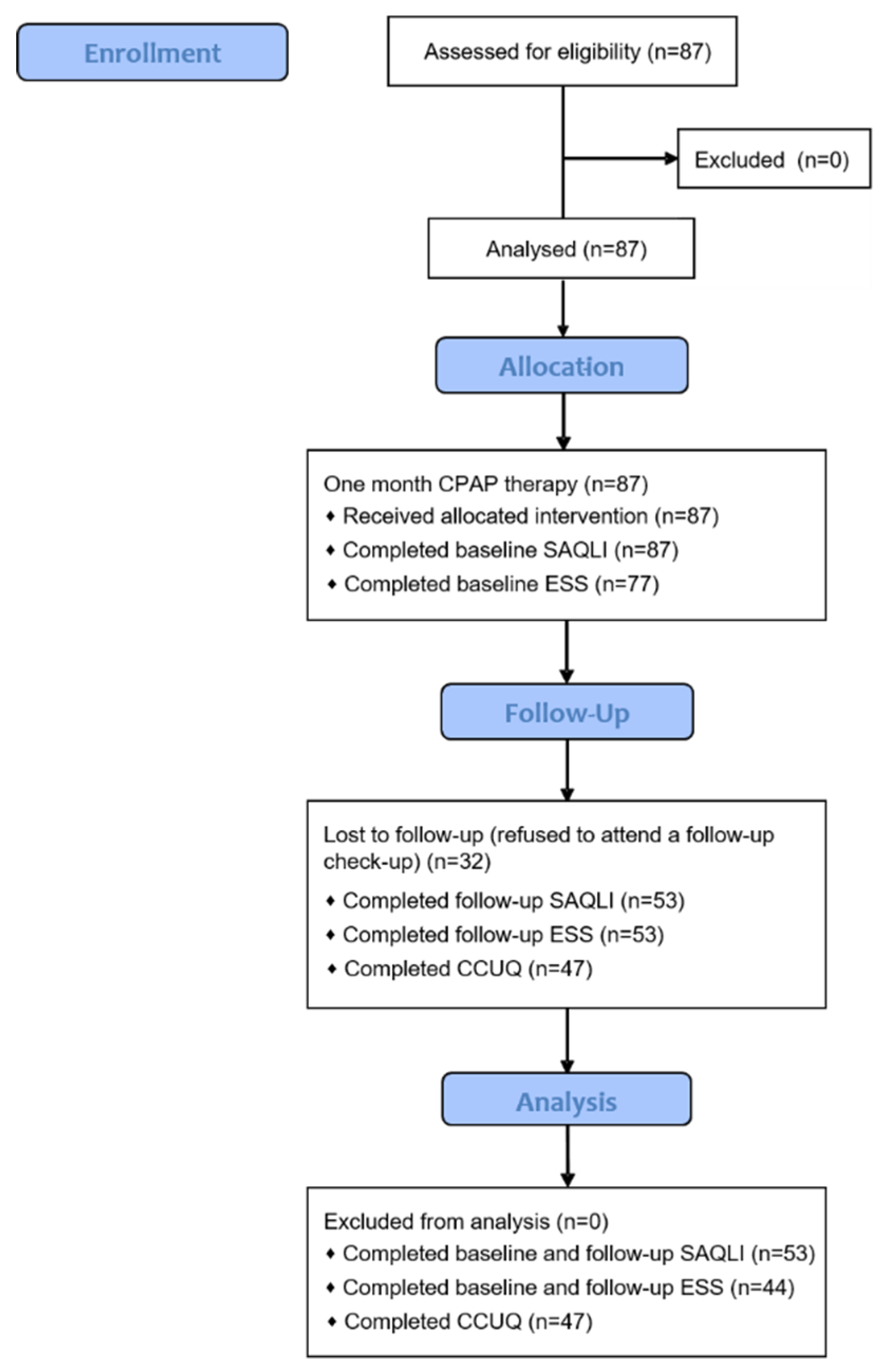
Figure 2.
The frequency of endorsement for each item on the Cues to CPAP Use Questionnaire (CCUQ) concerning CPAP compliance (n=47).
Figure 2.
The frequency of endorsement for each item on the Cues to CPAP Use Questionnaire (CCUQ) concerning CPAP compliance (n=47).
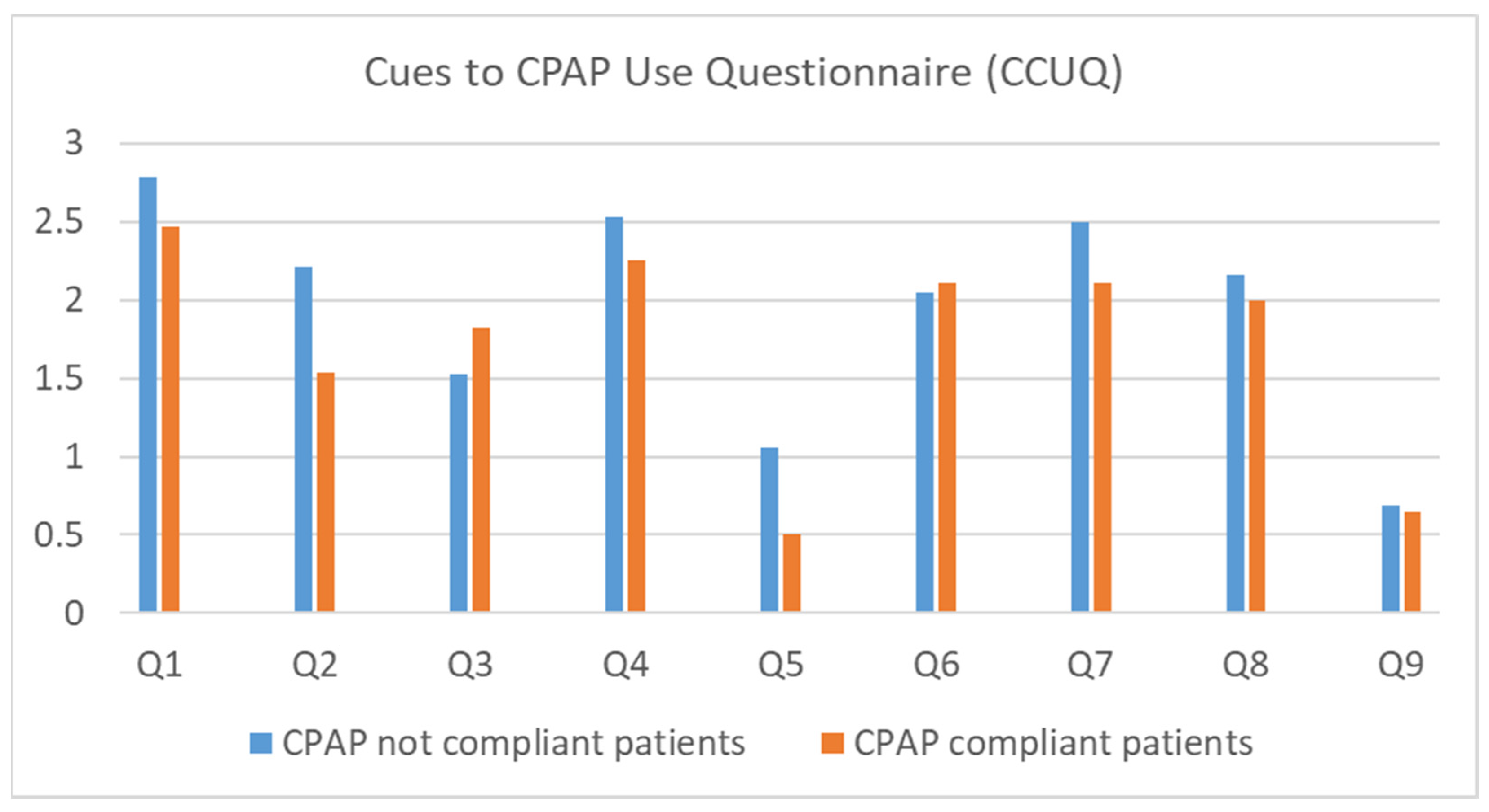

Table 1.
Demographic and anthropometric characteristics of severe Obstructive Sleep Apnea (OSA) patients with polysomnography (PSG) or polygraphy (PG) results.
Table 1.
Demographic and anthropometric characteristics of severe Obstructive Sleep Apnea (OSA) patients with polysomnography (PSG) or polygraphy (PG) results.
| Parameters | Total patients (n=87) |
|---|---|
| Age | 55.6±12.5 |
| Gender | |
| Men | 67 (77) |
| Women | 20 (23) |
| Height (cm) | 179.3±9.2 |
| Weight (kg) | 108.9±24.7 |
| Body mass index (kg/m2) | 33.2±7.4 |
| Neck circumference (cm) | 45.4±5.0 |
| Waist circumference (cm) | 118.0±16.0 |
| Hip circumference (cm) | 115.6±12.4 |
| Apnea-Hypopnea Index (AHI) | 50.5±19.1 |
| Oxygen Desaturation Index (ODI) | 51.0±22.8 |
| Mean saturation (%) | 92.8±3.6 |
| Time below 90% saturation (min) | 80.1±109.2 |
| Lowest saturation (%) | 72.3±11.8 |
Data are shown as mean±standard deviation or n (%).
Table 2.
The data from the CPAP memory cards after one month of usage in compliant and non-compliant patients.
Table 2.
The data from the CPAP memory cards after one month of usage in compliant and non-compliant patients.
| Parameters | Total (n=55) | CPAP non-compliant (n=21) | CPAP compliant (n=34) | p† |
|---|---|---|---|---|
| Average usage (all days, min)* | 305.3±116.5 | 193.6±71.5 | 378.6±74 | <0.001 |
| Average usage (days used, min)* | 341.2±99.9 | 255.3±73.5 | 397.6±70.5 | <0.001 |
| Total days with device usage (n)* | 26.8±7.4 | 23.6±10.3 | 28.8±3.5 | 0.011 |
| Percentage of days with device usage* | 88%±17.8% | 78.3%±23.1% | 94.4%±9% | <0.001 |
| Total days with CPAP usage ≥4h | 20.5±9.3 | 10.7±5.8 | 26.5±4.8 | <0.001 |
| Percentage of days with CPAP usage ≥4h | 69.8%±28.7% | 37.9%±19% | 89.4%±9.5% | <0.001 |
| Average apnea-hypopnea index (AHI) | 4.7±4.6 | 6.5±6.3 | 3.5±2.8 | 0.018 |
Data are shown as mean±standard deviation. * n=53 available data, †Independent Samples T-Test.
Table 3.
Calgary Sleep Apnea Quality of Life Index (SAQLI) and Epworth Sleepiness Scale (ESS) results before and after one month of CPAP usage (n=53).
Table 3.
Calgary Sleep Apnea Quality of Life Index (SAQLI) and Epworth Sleepiness Scale (ESS) results before and after one month of CPAP usage (n=53).
| Parameters | Before CPAP | After one month of CPAP | p* |
|---|---|---|---|
| Domain A | 2.9±1.2 | 2.1±1.2 | <0.001 |
| Domain B | 2.9±1.2 | 2.1±1.2 | <0.001 |
| Domain C | 2.8±1.3 | 2.2±1.1 | <0.001 |
| Domain D† | 5.2±1.7 | 3.3±1.7 | <0.001 |
| Domain E† | - | 2.8±1.5 | - |
| Total SALQI† | 3.4±1.1 | 1.7±0.9 | <0.001 |
| Domain F I† | - | 7.0±2.4 | - |
| Domain F II† | - | 3.6±3.3 | - |
| Epworth Sleepiness Scale‡ | 7.2±5.1 | 4.6±4.2 | 0.004 |
Data are shown as mean±standard deviation. * Repeated measures ANOVA, † n=50 available data, ‡ n=44 available data.
Table 4.
The frequency of moderately or extremely important answers for each item on the Cues to CPAP Use Questionnaire (CCUQ) in relation to CPAP compliance; n (%).
Table 4.
The frequency of moderately or extremely important answers for each item on the Cues to CPAP Use Questionnaire (CCUQ) in relation to CPAP compliance; n (%).
| Parameters | Total (n=50) | CPAP non-compliant (n=20) | CPAP compliant (n=30) | p* | OR (95%CI) | p† |
|---|---|---|---|---|---|---|
| Q1 My sleep physician said that I should | 44 (88.0) | 19 (95.0) | 23 (76.7) | 0.214 | 0.263 (0.028-2.443) | 0.381 |
| Q2 I was worried about my heart | 30 (60.0) | 16 (80.0) | 14 (46.7) | 0.018 | 0.219 (0.059-0.810) | 0.022 |
| Q3 Partner couldn't sleep because of my snoring | 29 (58.0) | 10 (50.0) | 19 (63.3) | 0.349 | 1.727 (0.548-5.448) | 0.393 |
| Q4 My sleep physician was worried about my OSA | 42 (84.0) | 18 (90.0) | 24 (80.0) | 0.345 | 0.444 (0.080-2.465) | 0.450 |
| Q5 Advice from a friend/acquaintance (who does not have OSA) | 11 (22.0) | 7 (35.0) | 4 (13.3) | 0.070 | 0.286 (0.071-1.155) | 0.090 |
| Q6 Partner encouraged me to start CPAP† | 34 (69.4) | 14 (70.0) | 20 (69.0) | 0.938 | 0.952 (0.276-3.286) | 1.000 |
| Q7 I was worried about the health consequences of my sleep problem | 39 (78.0) | 17 (85.0) | 22 (73.3) | 0.329 | 0.485 (0.112-2.111) | 0.489 |
| Q8 I was so tired all of the time | 36 (72.0) | 16 (80.0) | 20 (66.7) | 0.304 | 0.500 (0.132-1.896) | 0.353 |
| Q9 I was worried that I would have a car accident | 10 (20.0) | 5 (25.0) | 5 (16.7) | 0.470 | 0.600 (0.149-0.421) | 0.494 |
Data are shown as n (%). * Chi square test, †Fisher’s exact test, ‡ n=49 available data.
Table 5.
Multiple Regression Analysis for predictors of CPAP compliance.
| Variable | Unstandardized coefficients | Standard Error | Standardized coefficients | T | p-value |
|---|---|---|---|---|---|
| Apnea-hypopnea index* | -0.342 | 0.990 | -0.051 | -0.345 | 0.732 |
| Epworth sleepiness scale* | -8.653 | 3.684 | -0.387 | -2.349 | 0.024 |
| Total SALQI score* | 48.263 | 16.647 | 0.481 | 2.899 | 0.006 |
R2=0.253, Adjusted R2=0.198, F=4.627, p=0.007, * Before CPAP.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



