
Submitted:
13 July 2024
Posted:
15 July 2024
You are already at the latest version
Abstract
Introduction. Autism Spectrum Disorder (ASD) includes different manifestations of an individual’s level of functioning. It is characterised by qualitative alterations in reciprocal social interaction and social communication, and the presence of repetitive behaviours and restricted interests. Based on two dimensions, three levels are differentiated: social communication, restricted interests, and repetitive behaviour. Aim. To gain knowledge of the application and usefulness of BRIEF‐P in the evaluation of Executive Functions (EFs) in people with ASD. Method. Out of a total of 161,773 potentially eligible published articles from different databases. 13 appropriate articles were revised and 4 articles were selected. Studies that were included evaluated samples involving individuals with ASD aged 2 to 8 years, and were published in English or Spanish during the period of 2012‐2022. Results. The executive profile obtained from the application of BRIEF‐P in individuals with ASD was analysed. Conclusion. Results confirm deficits in flexibility, although they are not conclusive. This may be due to aspects related to methodology, whereby the studies (i) include very large and heterogeneous age groups, (ii) do not discriminate based on the level of competence, and (iii) use instruments for evaluating Executive Functions that are not validated or adapted to people with ASD. Another reason is due to the lack of consensus in the very operational definition of the Executive Functions construct, with the studies focusing mainly on the cold dimension while ignoring the hot dimension.
Keywords:
BRIEF-P
; flexibility
; Executive Functions
; inhibition
; Miyake model
; working memory
; Autism Spectrum Disorder
1. Introduction
Executive functions can be likened to an “orchestra conductor” construct that controls, organises, and directs cognitive activity, behavioural activity, and emotional response [1]. Executive functions are not exclusively “cold” cognitive, because they also include processes that reflect “hot” emotional and behavioural control [2].
The first researchers to define Executive Deficits in individuals with ASD were Damasio and Maurer [3], who established that the Executive Deficits which those individuals presented were analogous with damage to the frontal lobe affecting individuals.
Based on this study, we can review other publications [4] that have focused on the study of Executive Deficits in people with ASD: (a) Russell [5], in her classic work “Autism as an executive function disorder”, considers that the neurobiology of autism has characteristics that are very similar to those of the neurobiology of Executive Functioning. That consideration has been defended and maintained by other authors [6]; (b) Hill [7] published “Executive dysfunction in autism”, in which a review of three dimensions was carried out: planning, mental flexibility, and inhibition. The information that was obtained from this review concludes by highlighting the importance of developing more in-depth research on the different dimensions that make up the Executive Functioning construct in people with ASD, as well as knowing the neuroanatomical correlates of the different dimensions throughout the life of an individual; (c) Etchepareborda [8] published the article “Executive functions and autism”. That author, as well as those previously mentioned, agree in highlighting tremendous cognitive rigidity as the most relevant characteristic of ASD. The ‘dysexecutive’ explanation attempts to integrate neurobiological, cognitive, and behavioural data. Thus, individuals with ASD perform poorly in tasks that those studies evaluate: inhibition, flexibility, and planning. Specifically, people with ASD manage to solve second-order mental tasks, but not Executive Function tests; (d) Martos & Paula [9] developed the study “An approach to executive functions in autism spectrum disorder”. They review the behavioural manifestation and the state of the research on Executive Functions in individuals with ASD, and its impact on the abilities of planning, mental and cognitive flexibility, generativity, response inhibition, mental abilities, and sense of activity. The results of this review point to the difficulty of considering the executive hypothesis in people with ASD, as there are not enough intervention programmes with proven efficacy that minimise the effects of Executive Dysfunction in autism; (e) Talero et al. [10] published “Autism Spectrum Disorder and executive function”. This empirical study aimed to evaluate the performance of people with ASD in Executive Function tests. The results of this study show that children with ASD are susceptible to presenting significant alterations in tasks related to Executive Functions. This dysfunction correlates with the severity of autism and varies by age. Finally, those authors consider that this alteration is not a phenomenon, which occurs exclusively in ASD. Executive Functioning is an area that has also been shown to be impaired in children with ASD (for a review see [11] and [12]).
Some of the symptoms presented by people with ASD can be explained by a failure in the efficiency of certain skills linked to the executive system, including: self-control of action and thought, planning, inhibition capacity, working memory, monitoring of action, inhibition of automatic responses, and cognitive flexibility. These alterations tend to be grouped under the name of dysexecutive syndrome [13], observed in individuals with a tendency to act impulsively, while ignoring relevant information for the activity they would wish to perform. Likewise, the individuals show difficulties in finding alternative solutions when they do not achieve the desired objective, and in some cases, they are incapable of realising the mistakes they made or anticipating the consequences of their actions.
Table 1 reviews, non-systematically, various current studies that point to a deficit in the flexibility dimension [8,9,14,15,16,17,18,19] and working memory [17] in individuals with ASD.
Although there is no doubt about the presence of executive dysfunction in ASD, this theory suffers from several problems [36]: (i) Firstly, the presence of Executive Dysfunction is not specific to ASD, for there are many other disorders that share deficits in Executive Functions: ADHD, Tourette Syndrome (TS), schizophrenia, or Parkinson’s disease also present Executive Function disorders [37]; (ii) Secondly, this theory suffers from a fundamental problem, which is the over-extension of the term Executive Function, in order to refer to a wide range of capacities that, in many cases, are not clearly defined and, more importantly, not all of these capacities are affected in ASD [38].
We agree with Di Renzo et al. [39], who highlight both the difficulty of assessing Executive Functioning (a complex and heterogeneous construct) and ASD, while aiming at (i) a multisource research perspective and (ii) an approach that would allow a more accurate and complete assessment of Executive Functioning in ASD, while (iii) differentiating the clinical characteristics, and (iv) considering how the different components of development interact to determine their cognitive and social competence.
BRIEF-P [40] is a questionnaire, with which to assess the Executive Functions of children (aged 2 years to 6 years), and that derives from BRIEF (Gioia et al., 2000), in the context itself and includes the dimension of Self-Regulation. In its development, Isquith et al. [40] relied on a series of models that converge on the idea that Executive Functions are a series of interrelated dimensions or processes, which are responsible for directing behaviour and cognitive activity towards an objective.
Using a Likert-type frequency scale with three response options: never, sometimes, and frequently, parents and teachers (as informants) respond to the question: “How often have these behaviours been a problem compared with other children of the same age?” For this, it is necessary that the informants have known the child for a minimum period of 6 months.
The questionnaire is made up of 63 items under five clinical scales (Inhibition, Emotional Control, Flexibility, Planning and Organization, and Working Memory); three Indices (Inhibitory Self-control, Flexibility and Emerging Metacognition); a Global Executive Function Index; and two validity scales (Negativity and Inconsistency). Its application requires 10-15 minutes.
It is an efficient and valid instrument with which to detect, assess, and monitor the development of Executive Functioning in children, and it is easy to use, brief, and structured.
In this context, we review the findings published in relation to the application of BRIEF-P in individuals with ASD who are of preschool age, in order to analyse the profile of Executive Functioning by answering the question: “Is it possible to obtain an Executive Functioning profile in children with ASD using BRIEF-P?”
2. Method
Non-experimental or ex post facto descriptive.
There are various review studies that have been carried out with individuals who have ASD, and among them, we highlight the following:
i) The study developed by Pennington & Ozonoff [41] is probably the first review study available that is related to ASD. Those authors reviewed 18 studies on ADHD, 9 studies on Conduct Disorder (without ADHD), 14 studies on ASD, and 5 studies on Tourette Syndrome. Executive Function deficits are consistently found in both ADHD and autism, but not in Conduct Disorder (CD) without ADHD, or Tourette Syndrome (TS). Furthermore, both the severity and the profile of EF deficits seem to differ between ADHD and autism. Molar EF deficits are more severe in the latter than in the former. In the few studies of more specific EF tasks, there are deficits in motor inhibition in ADHD but not in autism, while there are deficits in verbal working memory in autism but not in ADHD. We conclude with a discussion of the implications for future research.
ii) Lai et al. [42] conducted a review with the aim of outlining the profile of Executive Functioning deficits in children and adolescents with high-functioning autism spectrum disorder (HFASD). Those authors reviewed 98 case-control studies, involving 5,991 individuals, of which 2,986 had ASD, and 3,005 had normotypical development. This meta-analysis confirmed the presence of Executive Dysfunction in children and adolescents with HFASD.
iii) Kercood et al. [43] analysed 24 studies with individuals having different levels of competence: HFA, Asperger’s (ASP), and Autism. The results suggest that individuals with ASD obtain lower scores in working memory, cognitive flexibility, and planning compared to indiviuals with normotypical development. Low verbal working memory scores were associated with greater problems in adaptive behaviour, and more restrictive and repetitive behaviour.
iv) Leung and Zakzanis [44] conducted a systematic review of 72 studies in order to analyse the sensitivity of measures of cognitive flexibility in individuals with ASD. Impairments in cognitive flexibility do not uniformly characterise all individuals with ASD.
v) Geurts et al. [45] analysed 41 studies, in order to determine whether individuals with ASD have difficulties in inhibitory control: inhibition of the overbearing response and interference control. Those researchers found that individuals with ASD show poorer performance in automatic response inhibition and interference control tasks, compared to individuals with normotypical development. One cannot make a conclusion by affirming that the inhibition of automatic responses is the most characteristic indicator of individuals with ASD, because there are variables related to age and IQ that can differentially influence inhibition.
Procedure
We have followed the guidelines of PRISMA 2020 [46], which were operationalised in a series of stages: (i) formulation of the problem; (ii) literature search; (iii) coding of the studies; (iv) statistical analysis and interpretation, and (v) publication of the results.
We conducted a literature search in Science Direct, NCBI (National Center for Biotechnology Information), Science Direct, APA PsycInfo, and PubMed. The keywords used in the search were: autism or ASD or ASD; Behavior Rating Instrument of Executive Function-Preschool or BRIEF-P.
The search language was primarily English.
The search itineraries focused on the last ten years:
i) Science Direct → 4255 results
Search 1 → 97 results
(autism or ASD) and (Behavior Rating Instrument of Executive Function-Preschool)
Search 2 → 4.158 results
(autism or ASD) and (BRIEF-P)
ii) NCBI → 275 results
Search → NCBI → Total 142
(autism+or+ASD) and (BRIEF-P)
Search NCBI → Total 133
((“autistic disorder”[MeSH Terms] OR (“autistic” [All Fields] AND “disorder”[All Fields]) OR “autistic disorder”[All Fields] OR “autism”[All Fields]) OR “asd”[All Fields]) AND BRIEF-P[All Fields] AND (“2012/02/07"[PDat] : “2022/02/03”[PDat]) (autism+or+ASD) and (BRIEF-P)
iii) APA PsycInfo
Search → autism or ASD and BRIEF-P → 89,143 results
iv) PubMed
Search → autism or ASD and BRIEF-P → 67,379 results
The search strategy is reflected in the PRISMA flow diagram (Figure 1).
Selection Criteria
The criteria were previously decided by considering the objectives of the study:
i) Inclusion criteria: (a) Participants: people with a diagnosis of ASD obtained from the application of standardised tests; (b) Cognitive age that allows the application of BRIEF-P; (c) Cognitive competence: obtained through the application of standardised tests; (d) Executive dimensions: single construct or basic dimensions (flexibility, inhibition, and working memory); (e) Assessment instruments: standardised to assess executive functions: hetero-report and/or self-report; (f) Types of studies: empirical; (g) Language: English and Spanish; (h) Other features: full text
ii) Exclusion criteria: (a) Participants: no diagnosis of ASD; (b) Cognitive age: it does not allow applying BRIEF-P; (c) Cognitive competence: not available; (d) Assessment instruments: not standardised; (e) Types of studies: case study and review; (f) Language: other; (g) Other characteristics: summary.
We carried out a systematic review and considered a series of characteristics that define this type of scientific publication: (i) the preparation process is specified in detail; (ii) it is possible to replicate and verify the results and conclusions; (iii) an issue is dealt with in depth; (iv) the research is useful for obtaining concrete answers to specific clinical questions; (v) the research provides objective data.
3. Results
The search returned 161,773 potentially eligible studies. Finally, 13 works that were published in the last ten years were selected, because they met the necessary criteria to be part of the present study. The selected articles were reviewed and the most relevant information was extracted. The Table 1 includes the reviewed studies.
We have selected 4 studies that have sufficient statistical information to perform the meta-analysis with 6 comparisons (TEA versus Control) that allow us to compare the results in relation to the scores on the Clinical Inhibition and Flexibility and Global Executive Functioning Scales.
The Q test for homogeneity indicates that we cannot reject the null hypothesis that the effect size is the same in all studies.
The study that has the most weight in the meta-analysis is the one developed by Jahromi et al. [2013] [60].
In this case, the overall effect, measures the statistical significance of the result of the meta-analysis. In our study it is observed that it is statistically significant as the value is less than 0.05 (for 95% CI). There are statistically significant differences in BRIEF-P scores between people with ASD and the control group.
Considering a significance level at 0.05, a p-value of 0.015 would be less than this threshold and would be considered statistically significant (see Table 2).
Figure 2 presents the forest plot, which visually summarizes the results of the meta-analysis. Each study is represented by a horizontal line indicating its confidence interval, with a square marker denoting the effect size. The overall effect estimate is illustrated by a diamond at the bottom of the plot, providing a comprehensive view of the combined data. This visualization helps to quickly assess the consistency and significance of the findings across different studies.
4. Discussion and Conclusions
The purpose of this study was to review and analyse the published findings regarding the application of BRIEF-P in individuals with ASD, of preschool age, in order to obtain the characteristic and differential Executive profile.
The scores obtained in BRIEF-P by individuals with ASD show high scores on all clinical scales and indices. The scores are particularly high on the Clinical Flexibility Scale, thus demonstrating an ability, which would constitute a hallmark of Autism Spectrum Disorders.
These results are in line with those obtained by various researchers who have applied BRIEF-P to children with ASD: (i) McClain et al. [61], in comparing children with ASD versus children with Intellectual Disability, found that the latter exhibit more significant deficiencies in EF, regardless of diagnosis, with working memory being the most affected Executive Function ability in both groups; (ii) Godfrey et al. [62] confirm greater difficulty in switching attention between activities, and persistence in interests in individuals with ASD.
Executive Functioning is an affected area in children with ASD (for a review see Best & Miller [11]. Kenworthy et al. [12], in comparing children with and without ASD, found significant improvements in parent-reported general Executive Functioning after Parent-Child Interaction Therapy (PCIT). The changes that were experienced before and after therapy in Emotional Regulation are related to Executive Functioning.
vi) Ratto et al. [63] demonstrated how bilingual students with ASD had significantly fewer Executive Functioning problems and repetitive behaviours when the informants were parents. The bilingual advantage in Executive Functioning may be extended to children with neurodevelopmental disorders.
vii) Otterman et al. [64] suggest a gradual association of Executive Functioning difficulties along the continuum of ASD and ADHD. Further, Executive Functioning problems can be a precursor to ASD and ADHD traits from an early age.
viii) Stephens et al. [2018] [65] provide additional support for ASD risk and show new findings on the relationship between childhood behaviours that are indicative of ASD risk and Executive Functioning in early childhood.
ix) Gorman et al. [2016] [66] link the use of filler phrases that reflect difficulties in planning and delivering speech.
x) Di Renzo et al. [23] conclude that the use of the BRIEF-P which is completed by the parents allows a greater knowledge of the child’s Executive Functioning, but does not add clinical data to the diagnosis.
Based on the results obtained, we can suggest including the BRIEF-P in the protocol for evaluating the Executive Functions of children with ASD, making it necessary to complete the information that is obtained from the informants (parents, caregivers, and teachers) by adding the information gained from the child him/herself, thus evaluating the three nuclear dimensions of Executive Functioning proposed by [67]: working memory, inhibition, and flexibility.
The results are not conclusive. This may be due to various aspects that are related to methodology. In that, a large part of the studies have been carried out with children and adolescents of different ages and IQs below the normal range. Studies with adult samples have used individuals with IQs within the normal range or above. Another reason is that in comparative studies the control groups used are not always the most appropriate to compare with individuals with ASD.
Next, we analyse some future questions [7] that can guide future studies: (i) What is the influence of IQ on Executive Performance in people with ASD?; (ii) What neural mechanisms correspond to specific Executive Functions in individuals with and without ASD?; (iii) What is the profile of Executive Function and Executive Dysfunction in people with ASD throughout their lives?; (iv) In individuals with ASD who do not show clear Executive Deficits in laboratory tasks, how do they perform in naturalistic settings that involve Executive Functions, such as shopping, for example?; (v) Is there a specific profile of Executive Dysfunction that is exclusive to people with ASD, and different from other neurodevelopmental disorders that are associated with Executive Dysfunction?; (vi) What would a cognitive model of Executive Functions in individuals with ASD look like?
References
- Anderson VA, Anderson P, Northam E, Jacobs R, Mikiewicz O. Relationships Between Cognitive and Behavioral Measures of Executive Function in Children With Brain Disease. Child Neuropsychol. diciembre de 2002;8(4):231-40. [CrossRef]
- Zelazo PD, Qu L, Müller U. Hot and cool aspects of executive function: Relations in early development. En: Young children’s cognitive development: Interrelationships among executive functioning, working memory, verbal ability, and theory of mind. Mahwah, NJ, US: Lawrence Erlbaum Associates Publishers; 2005. p. 71-93.
- Damasio AR, Maurer RG. A Neurological Model for Childhood Autism. Arch Neurol. 1 de diciembre de 1978;35(12):777-86. [CrossRef]
- Ozonoff S, Pennington BF, Rogers SJ. Executive Function Deficits in High-Functioning Autistic Individuals: Relationship to Theory of Mind. J Child Psychol Psychiatry. noviembre de 1991;32(7):1081-105. [CrossRef] [PubMed]
- Russell J, editor. Autism as an Executive Disorder (DRAFT) [Internet]. Oxford University Press; 1998 [citado 11 de julio de 2024]. Disponible en: https://academic.oup.com/book/1216.
- Robinson S, Goddard L, Dritschel B, Wisley M, Howlin P. Executive functions in children with Autism Spectrum Disorders. Brain Cogn. diciembre de 2009;71(3):362-8. [CrossRef]
- Hill EL. Executive dysfunction in autism. Trends Cogn Sci. enero de 2004;8(1):26-32. [CrossRef] [PubMed]
- Etchepareborda Simonini MC. Funciones ejecutivas y autismo. Rev Neurol. 2005;41(S01):S155.
- Martos-Pérez J, Paula-Pérez I. [An approach to the executive functions in autism spectrum disorder]. Rev Neurol. 1 de marzo de 2011;52 Suppl 1:S147-153.
- Talero-Gutiérrez C, Echeverría Palacio CM, Quiñones PS, Morales Rubio G, Vélez-van-Meerbeke A. Trastorno del espectro autista y función ejecutiva. Acta Neurológica Colomb. 30 de mayo de 2023;31(3):246-52. [CrossRef]
- Best JR, Miller PH. A Developmental Perspective on Executive Function. Child Dev. noviembre de 2010;81(6):1641-60.
- Kenworthy L, Yerys BE, Anthony LG, Wallace GL. Understanding Executive Control in Autism Spectrum Disorders in the Lab and in the Real World. Neuropsychol Rev. diciembre de 2008;18(4):320-38. [CrossRef] [PubMed]
- Schroeter ML, Eickhoff SB, Engel A. From correlational approaches to meta-analytical symptom reading in individual patients: Bilateral lesions in the inferior frontal junction specifically cause dysexecutive syndrome. Cortex. julio de 2020;128:73-87. [CrossRef]
- Blijd-Hoogewys EMA, Bezemer ML, Van Geert PLC. Executive Functioning in Children with ASD: An Analysis of the BRIEF. J Autism Dev Disord. diciembre de 2014;44(12):3089-100. [CrossRef]
- Brady DI, Schwean VL, Saklofske DH, McCrimmon AW, Montgomery JM, Thorne KJ. Conceptual and Perceptual Set-shifting executive abilities in young adults with Asperger’s syndrome. Res Autism Spectr Disord. diciembre de 2013;7(12):1631-7. [CrossRef]
- Campbell CA, Russo N, Landry O, Jankowska AM, Stubbert E, Jacques S, et al. Nonverbal, rather than verbal, functioning may predict cognitive flexibility among persons with autism spectrum disorder: A preliminary study. Res Autism Spectr Disord. junio de 2017;38:19-25. [CrossRef]
- Chen SF, Chien YL, Wu CT, Shang CY, Wu YY, Gau SS. Deficits in executive functions among youths with autism spectrum disorders: an age-stratified analysis. Psychol Med. junio de 2016;46(8):1625-38. [CrossRef] [PubMed]
- Landry O, Al-Taie S. A Meta-analysis of the Wisconsin Card Sort Task in Autism. J Autism Dev Disord. abril de 2016;46(4):1220-35. [CrossRef] [PubMed]
- Van Eylen L, Boets B, Cosemans N, Peeters H, Steyaert J, Wagemans J, et al. Executive functioning and local-global visual processing: candidate endophenotypes for autism spectrum disorder? J Child Psychol Psychiatry. marzo de 2017;58(3):258-69.
- Blijd-Hoogewys EMA, Bezemer ML, van Geert PLC. Executive Functioning in Children with ASD: An Analysis of the BRIEF. J Autism Dev Disord. 2014;44(12):3089-100. [CrossRef]
- Brady DI, Schwean VL, Saklofske DH, McCrimmon AW, Montgomery JM, Thorne KJ. Conceptual and Perceptual Set-shifting executive abilities in young adults with Asperger’s syndrome. Res Autism Spectr Disord. 2013;7(12):1631-7. [CrossRef]
- Campbell CA, Russo N, Landry O, Jankowska AM, Stubbert E, Jacques S, et al. Nonverbal, rather than verbal, functioning may predict cognitive flexibility among persons with autism spectrum disorder: A preliminary study. Res Autism Spectr Disord. 2017;38:19-25. [CrossRef]
- Chen SFF, Chien YLL, Wu CTT, Shang CYY, Wu YYY, Gau SS. Deficits in executive functions among youths with autism spectrum disorders: An age-stratified analysis. Psychol Med. junio de 2016;46(8):1625-38. [CrossRef]
- Etchepareborda MC. Funciones ejecutivas y autismo. Rev Neurol. 2005;41(1):155-62. [CrossRef]
- Geurts HM, van den Bergh SFWM, Ruzzano L. Prepotent response inhibition and interference control in autism spectrum disorders: Two Meta-Analyses. Vol. 7, Autism Research. 2014. p. 407-20. [CrossRef]
- Hüpen P, Groen Y, Gaastra GF, Tucha L, Tucha O. Performance monitoring in autism spectrum disorders: A systematic literature review of event-related potential studies. Int J Psychophysiol. 2016;102:33-46. [CrossRef] [PubMed]
- Kloosterman PH, Kelley EA, Parker JDA, Craig WM. Executive functioning as a predictor of peer victimization in adolescents with and without an Autism Spectrum Disorder. Res Autism Spectr Disord. 2014;8(3):244-54. [CrossRef]
- Landry O, Al-Taie S. A Meta-analysis of the Wisconsin Card Sort Task in Autism. J Autism Dev Disord. 2016;46(4):1220-35. [CrossRef] [PubMed]
- Martos-Pérez J, Paula-Pérez I. Una aproximación a las funciones ejecutivas en el trastorno del espectro autista. Rev Neurol. 2011;52(Supl 1):147-53. [CrossRef]
- Pellicano E, Kenny L, Brede J, Klaric E, Lichwa H, McMillin R. Executive function predicts school readiness in autistic and typical preschool children. Cogn Dev. 2017;43:1-13. [CrossRef]
- Talero C, Echeverria CMa, Sánchez P, Morales G, Vélez A. Trastorno del espectro autista y función ejecutiva. Acta Neurológica Colomb. 2015;31(3):246-52.
- Van Eylen L, Boets B, Cosemans N, Peeters H, Steyaert J, Wagemans J, et al. Executive functioning and local-global visual processing: candidate endophenotypes for autism spectrum disorder? J Child Psychol Psychiatry. 2017;58(3):258-69.
- Vanegas SB, Davidson D. Investigating distinct and related contributions of Weak Central Coherence, Executive Dysfunction, and Systemizing theories to the cognitive profiles of children with Autism Spectrum Disorders and typically developing children. Res Autism Spectr Disord. 2015;11:77-92. [CrossRef]
- Wu HC, White S, Rees G, Burgess PW. Executive function in high-functioning autism: Decision-making consistency as a characteristic gambling behaviour. Cortex. 2018;1-16. [CrossRef]
- Yi L, Fan Y, Joseph L, Huang D, Wang X, Li J, et al. Event-based prospective memory in children with autism spectrum disorder: The role of executive function. Res Autism Spectr Disord. 2014;8(6):654-60. [CrossRef]
- López B, Leekam SR. Teoría de la coherencia central: una revisión de los supuestos teóricos. Infancia Aprendiz. enero de 2007;30(3):439-57.
- Ozonoff S, Strayer DL, McMahon WM, Filloux F. Executive Function Abilities in Autism and Tourette Syndrome: An Information Processing Approach. J Child Psychol Psychiatry. septiembre de 1994;35(6):1015-32. [CrossRef] [PubMed]
- Griffith EM, Pennington BF, Wehner EA, Rogers SJ. Executive Functions in Young Children with Autism. Child Dev. julio de 1999;70(4):817-32. [CrossRef] [PubMed]
- Di Renzo M, Di Castelbianco FB, Vanadia E. Assessment of Executive Functions in Preschool-Aged Children with Autism Spectrum Disorders: Usefulness and Limitation of BRIEF-P in Clinical Practice. J Child Adolesc Behav [Internet]. 2016 [citado 10 de julio de 2024];04(05). Disponible en: http://www.esciencecentral.org/journals/assessment-of-executive-functions-in-preschoolaged-children-withautism-spectrum-disorders-usefulness-and-limitation-of-briefp-incl-2375-4494-1000313.php?aid=81438.
- Isquith PK, Crawford JS, Espy KA, Gioia GA. Assessment of executive function in preschool-aged children. Ment Retard Dev Disabil Res Rev. agosto de 2005;11(3):209-15. [CrossRef] [PubMed]
- Pennington BF, Ozonoff S. Executive Functions and Developmental Psychopathology. J Child Psychol Psychiatry. enero de 1996;37(1):51-87. [CrossRef]
- Lai CLE, Lau Z, Lui SSY, Lok E, Tam V, Chan Q, et al. Meta-analysis of neuropsychological measures of executive functioning in children and adolescents with high-functioning autism spectrum disorder. Autism Res. mayo de 2017;10(5):911-39. [CrossRef]
- Kercood S, Grskovic JA, Banda D, Begeske J. Working memory and autism: A review of literature. Res Autism Spectr Disord. octubre de 2014;8(10):1316-32. [CrossRef]
- Leung RC, Zakzanis KK. Brief Report: Cognitive Flexibility in Autism Spectrum Disorders: A Quantitative Review. J Autism Dev Disord. octubre de 2014;44(10):2628-45. [CrossRef]
- Geurts HM, Van Den Bergh SFWM, Ruzzano L. Prepotent Response Inhibition and Interference Control in Autism Spectrum Disorders: Two Meta-Analyses. Autism Res. agosto de 2014;7(4):407-20. [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLOS Med. 29 de marzo de 2021;18(3):e1003583.
- Godfrey KJ, Espenhahn S, Stokoe M, McMorris C, Murias K, McCrimmon A, et al. Autism interest intensity in early childhood associates with executive functioning but not reward sensitivity or anxiety symptoms. Autism Int J Res Pract. diciembre de 2021;13623613211064372. [CrossRef] [PubMed]
- Parladé M V., Weinstein A, Garcia D, Rowley AM, Ginn NC, Jent JF. Parent–Child Interaction Therapy for children with autism spectrum disorder and a matched case-control sample. Autism. 2020;24(1):160-76. [CrossRef] [PubMed]
- Nuske HJ, Pellecchia M, Kane C, Seidman M, Maddox BB, Freeman LM, et al. Self-Regulation is Bi-Directionally Associated with Cognitive Development in Children with Autism. J Appl Dev Psychol. 2020;68. [CrossRef]
- Kitzerow J, Hackbusch M, Jensen K, Kieser M, Noterdaeme M, Fröhlich U, et al. Study protocol of the multi-centre, randomised controlled trial of the Frankfurt Early Intervention Programme A-FFIP versus early intervention as usual for toddlers and preschool children with Autism Spectrum Disorder (A-FFIP study). Trials. febrero de 2020;21(1):217. [CrossRef] [PubMed]
- Ratto AB, Potvin D, Pallathra AA, Saldana L, Kenworthy L. Parents report fewer executive functioning problems and repetitive behaviors in young dual-language speakers with autism. Child Neuropsychol J Norm Abnorm Dev Child Adolesc. octubre de 2020;26(7):917-33. [CrossRef] [PubMed]
- Stephens RL, Watson LR, Crais ER, Reznick JS. Infant quantitative risk for autism spectrum disorder predicts executive function in early childhood. Autism Res Off J Int Soc Autism Res. noviembre de 2018;11(11):1532-41. [CrossRef] [PubMed]
- MacFarlane H, Gorman K, Ingham R, Presmanes Hill A, Papadakis K, Kiss G, et al. Quantitative analysis of disfluency in children with autism spectrum disorder or language impairment. PloS One. 2017;12(3):e0173936. [CrossRef] [PubMed]
- Zantinge G, van Rijn S, Stockmann L, Swaab H. Physiological Arousal and Emotion Regulation Strategies in Young Children with Autism Spectrum Disorders. J Autism Dev Disord. septiembre de 2017;47(9):2648-57. [CrossRef]
- Gorman K, Olson L, Hill AP, Lunsford R, Heeman PA, van Santen JPH. Uh and um in children with autism spectrum disorders or language impairment. Autism Res Off J Int Soc Autism Res. agosto de 2016;9(8):854-65.
- Di Renzo M, di Castelbianco FB, Vanadia E. Assessment of Executive Functions in Preschool-Aged Children with Autism Spectrum Disorders: Usefulness and Limitation of BRIEF-P in Clinical Practice. J Child Adolesc Behav. 2016;04(05). [CrossRef]
- Smithson PE, Kenworthy L, Wills MC, Jarrett M, Atmore K, Yerys BE. Real world executive control impairments in preschoolers with autism spectrum disorders. J Autism Dev Disord. agosto de 2013;43(8):1967-75. [CrossRef] [PubMed]
- Jahromi LB, Bryce CI, Swanson J. The importance of self-regulation for the school and peer engagement of children with high-functioning autism. Res Autism Spectr Disord. 2013;7(2):235-46. [CrossRef]
- Drayer JD. Profiles of executive functioning in preschoolers with autism. Diss Abstr Int Sect B Sci Eng. 2009;69(12-B):7834.
- Jahromi LB, Bryce CI, Swanson J. The importance of self-regulation for the school and peer engagement of children with high-functioning autism. Res Autism Spectr Disord. febrero de 2013;7(2):235-46. [CrossRef]
- McClain MB, Golson ME, Murphy LE. Executive functioning skills in early childhood children with autism, intellectual disability, and co-occurring autism and intellectual disability. Res Dev Disabil. marzo de 2022;122:104169. [CrossRef]
- Godfrey KJ, Espenhahn S, Stokoe M, McMorris C, Murias K, McCrimmon A, et al. Autism interest intensity in early childhood associates with executive functioning but not reward sensitivity or anxiety symptoms. Autism. octubre de 2022;26(7):1723-36. [CrossRef]
- Ratto AB, Potvin D, Pallathra AA, Saldana L, Kenworthy L. Parents report fewer executive functioning problems and repetitive behaviors in young dual-language speakers with autism. Child Neuropsychol. 2 de octubre de 2020;26(7):917-33. [CrossRef]
- Otterman DL, Koopman-Verhoeff ME, White TJ, Tiemeier H, Bolhuis K, Jansen PW. Executive functioning and neurodevelopmental disorders in early childhood: a prospective population-based study. Child Adolesc Psychiatry Ment Health. diciembre de 2019;13(1):38. [CrossRef]
- Stephens RL, Watson LR, Crais ER, Reznick JS. Infant quantitative risk for autism spectrum disorder predicts executive function in early childhood. Autism Res. noviembre de 2018;11(11):1532-41. [CrossRef]
- Gorman K, Olson L, Hill AP, Lunsford R, Heeman PA, Van Santen JPH. Uh and um in children with autism spectrum disorders or language impairment. Autism Res. agosto de 2016;9(8):854-65.
- Miyake A, Friedman NP, Emerson MJ, Witzki AH, Howerter A, Wager TD. The Unity and Diversity of Executive Functions and Their Contributions to Complex “Frontal Lobe” Tasks: A Latent Variable Analysis. Cognit Psychol. agosto de 2000;41(1):49-100. [CrossRef] [PubMed]
Figure 1.
PRISMA flow diagram (based on the work of Page et al., 2021) [46].
Figure 1.
PRISMA flow diagram (based on the work of Page et al., 2021) [46].
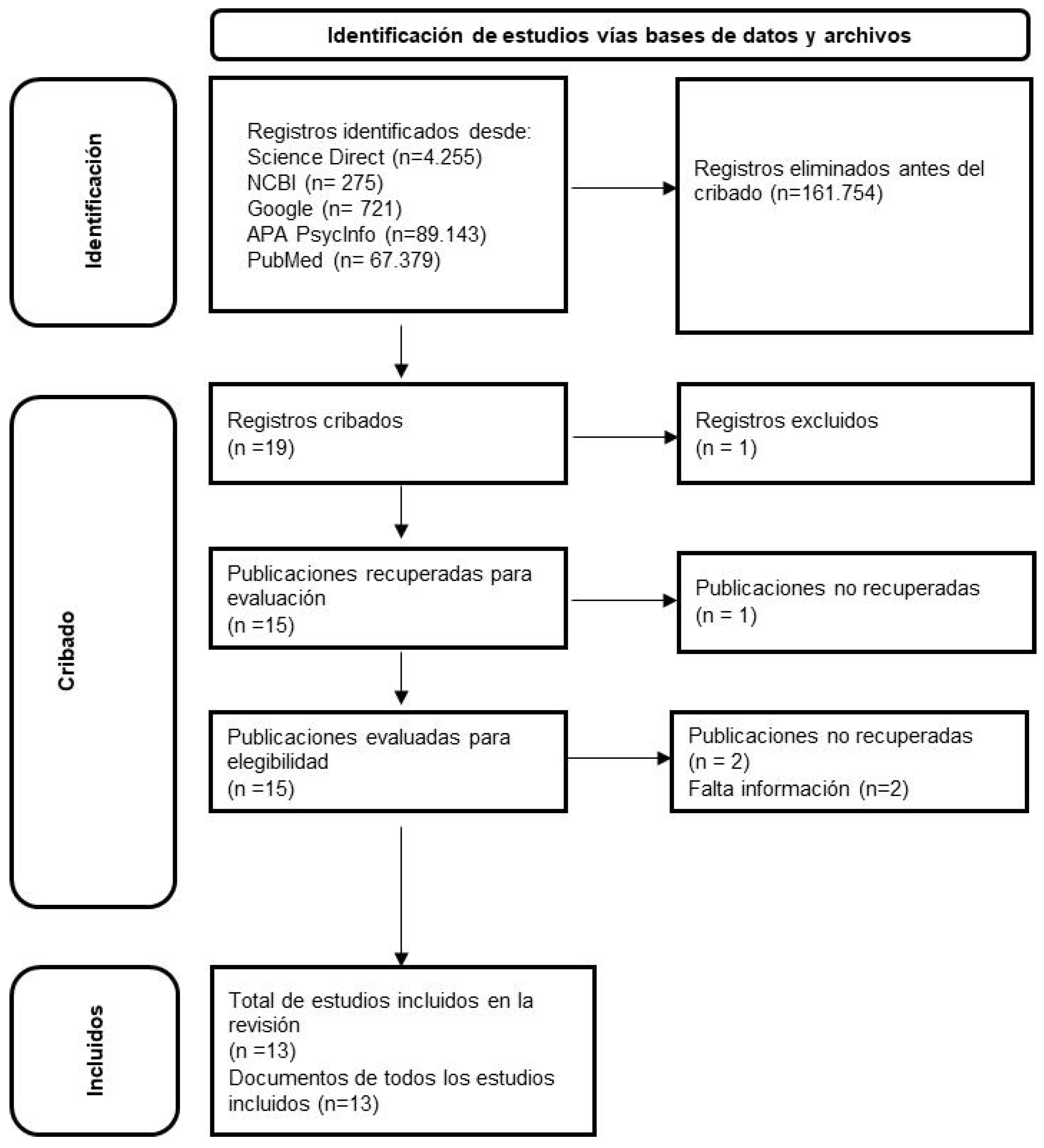
Figure 2.
Forest plot.
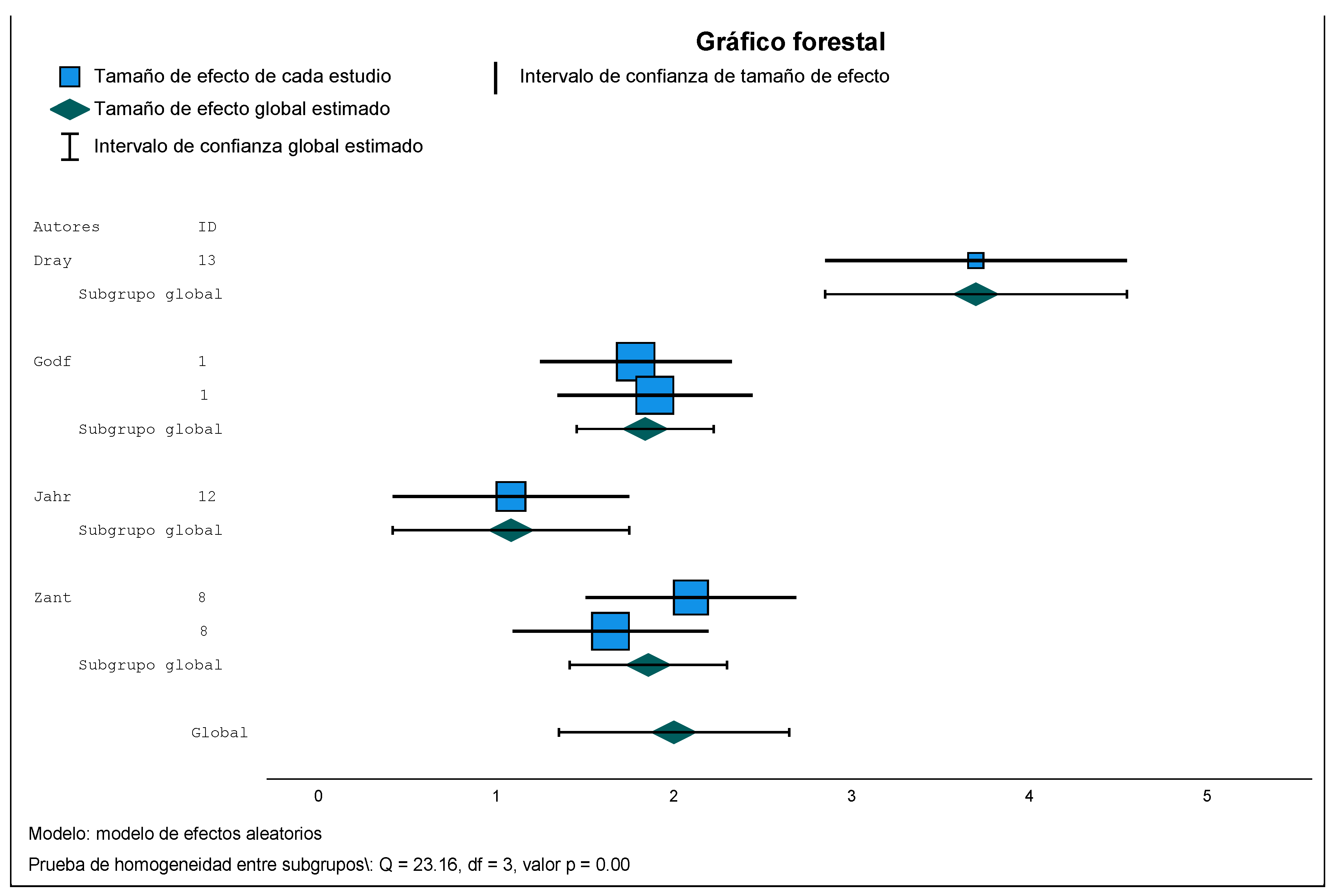

Table 1.
Executive deficits in people with ASD (own elaboration).
| Study | Neurodevelopmental Disorder | Executive Deficits |
|---|---|---|
| [20] | ASD | Flexibility |
| [14,21] | ASD (syndrome de Asperger) | Conceptual flexibility |
| [22] | ASD (no verbal) | Flexibility |
| [23] | ASD | Working memory and planning in youth (13-18 years) Flexibility in children (8-12 years old) |
| [24] | ASD | Inhibition, flexibility and planning |
| [25] | ASD | Inhibition, working memory, cognitive flexibility, and planning |
| [26] | ASD | Self-monitoring of learning |
| [27] | ASD | Emotional control |
| [28] | ASD | Rigidity (not flexibility) |
| [29] | ASD | Planning, mental and cognitive flexibility and response inhibition |
| [30] | ASD | Inhibition and working memory |
| [31] | ASD | Executive Function (unitary construct) |
| [32] | ASD | Flexibility, fluency and inhibition of automatic responses |
| [33] | ASD | Executive Function (unitary construct) |
| [34] | ASD | Repetition, rigidity |
| [35] | ASD | Prospective report |
Note 1: Sorted alphabetically.
Table 1.
Reviewed studies.
| Author/ Year/ Country |
Design | Sample/n | Sample/Median age | Diagnostic instrument_ASD | Assessment instrument for EF | Assessment instrument for other competencies | Executive profile | Included in the meta-analysis |
|---|---|---|---|---|---|---|---|---|
| [47] / Canada |
Non-experimental Descriptive Comparative/Causal 2 groups: -ASD -Comparison |
-ASD= 33 -Comparison = 42 |
3-6 years | >Social Responsiveness Scale–Second Edition (SRS-2) (versión padres) | BRIEF-P | >The Interests Scale (IS) >The Behavioral Inhibition and Behavioral Approach System–Parent Version (BISBAS) >Behavior Assessment System for Children–Third Edition (BASC-3) |
>The group with ASD had greater difficulties on the Flexibility clinical scale and on the Inhibitory control index | YES |
| [48]/ Canada |
Empirical Quasi-experimental Measures: pre-test and post-test 2 groups: -ASD -Control |
-ASD=16 -Comparison= 16 |
3-7 years | > The Autism Diagnostic Observation Schedule, 2nd-edition (ADOS-2) | BRIEF-P | >Differential Abilities Scale, Second Edition (DAS-II) >Picture Vocabulary Test, Fourth Edition (PPVT-4) >Expressive Vocabulary Test, Second Edition (EVT-2) >Peabody Parenting Stress Index, Fourth Edition: Short Form (PSI-4: SF) > ECBI >Behavior Assessment System for Children, Second Edition, Parent Rating Scale (BASC-2 PRS) >Social Responsiveness Scale, Second Edition (SRS-2) |
>There are no statistically significant differences in the BRIEF-P Global Executive Functioning Scale between pre- and post-treatment | NO |
| [49])/ EE.UU |
Non-experimental Descriptive Comparative/Causal 2 groups: -Minimally verbal -Typically verbal |
ASD: -Minimally verbal children= 38 -Typically verbal children=46 |
5-8 years | > Differential Ability Scales-II (DAS-II) | BRIEF-P | >Behavioral Interference Coding Scheme (BICS) | >Children with ASD are at high risk of self-regulation difficulties >Children with ASD who were minimally verbal, compared with typically verbal, had more self-regulation difficulties >Reduction in self-regulation difficulties over one academic year predicted greater gains in cognitive skills and vice versa |
NO |
| [50]/ Germany |
Quasi-experimental 1 group with 6 measurements |
ASD=134 | 24-66 months (2-5.5 years) |
> Autism Diagnostic Interview – Revised (ADI-R) > The Autism Diagnostic Observation Schedule, 2nd-edition (ADOS-2) |
BRIEF-P | > Brief Observation of Social Communication Change (BOSCC) > Social Responsiveness Scale – short versión (SRS-16) > Repetitive Behavior Scale – Revised (RBS-R) > Child Behavior Checklist 1 ½-5 (CBCL 1 ½-5) > Parent sense of competence scale (PSOC) > Depression Anxiety and Stress Scale – short form (DASS-21) > Family quality of Life Survey (FQOLS) > Early Social Communication Scale (ESCS) > Dyadic Communication Measure for Autism (DCMA) > Bayley Scales of Infant and Toddler Development 3rd Edition (Bayley-III) > Parent Adherence to treatment and Competence Scale (PATCS) |
>In preschool children with ASD, EF disturbances were observed in the real world that were not related to ASD symptoms >Given the relevance of EF problems in adulthood, change in EF through early intervention is an important outcome |
NO |
| [51]/ EE.UU |
Non-experimental Descriptive Comparative/Cause 2 groups: - Bilingual -Monolingual |
ASD: -Bilingual= 24 -Monolingual= 31 |
Dual-Language= 4.73 (0.57) Monolingual= 4.76 (0.67) |
> The Autism Diagnostic Observation Schedule, 2nd-edition (ADOS-2) | BRIEF-P | >The Social Responsiveness Scale-2 (SRS-2) >The Vineland-II |
>The bilingual advantage of EF observed in children with normotypical development may also be extended to young children with ASD | NO |
| [52]/ EE.UU |
Non-experimental Descriptive |
ASD= 585 | 42 months (3.5 years) | >The First Year Inventory 2.0 (FYI 2.0) | BRIEF-P | >Social Responsiveness Scale, Second Edition (SRS-2.0) | > Certain childhood behaviours related to ASD are linked to EF difficulties in early childhood | NO |
| [53]/ EE.UU |
Non-experimental Descriptive Comparative/Cause 3 groups: - ASD - Language impairment - Control |
-ASD=47 -Control=32 -Language impairment =18 |
4-8 years | >Autism Diagnostic Observation Schedule (ADOS) | BRIEF-P | >Verbal IQ (VIQ), performance IQ (PIQ) and full-scale IQ (FSIQ) the Wechsler scales tests > CELF Preschool-2 > Communication Checklist (CCC-2) |
> Executive functioning difficulties are more common in individuals with ASD than in children with language disorders | NO |
| [54]/ Netherlands |
Non-experimental Descriptive Comparative/Cause 2 groups: - ASD - Control |
-ASD=27 -Control= 44 |
41-81 months (3,4-6.75 years) |
>Autism Diagnostic Interview-Revised (ADI) |
BRIEF-P | >Dutch Wechsler Nonverbal Scale of Abil-ity (WNV-NL) >Wechsler Preschool and Primary Scale of Intelligence (WPPSI-III-NL) >Nonverbal Intelligence Test (SON-R 2.5–7) >Mullen Scales of Early Learning (MSEL) > Wechsler Nonverbal Scale of Ability (WNV) >Social Skills Rating System (SSRS) >Peabody Picture Vocabulary Test-III-NL (PPVT-III-NL) >Locked Box Task |
>Children with ASD had significantly more problems with inhibitory control and mental flexibility compared to children in the control group | YES |
| [55]/ EE.UU |
Non-experimental Descriptive Comparative/Cause 3 groups: - ASD - Control - Especific Language Impairment |
-ASD=50 -TD=47 -Especific Language Impairment=17 |
4-8 years | >Autism Diagnostic Observation Schedule (ADOS) | BRIEF-P | >Children’s Communication Checklist (CCC-2) >Social Communication Questionnaire |
>There were no reliable associations between um:uh ratio and chronological age, intelligence, or Executive Function | NO |
| [56]/ Italia |
Non-experimental Descriptive Comparative/Cause 4 groups: - ASD -Autistc children -Autism Spectrum Children -Children at risk of autism |
-ASD=46 -AUT=26 -SpD= 7 -Risk= 13 |
24-76 months (2-6.3 years) |
> The Autism Diagnostic Observation Schedule, 2nd-edition (ADOS-2) | BRIEF-P | >The Leiter International Performance Scale-Revised (Leiter-R) | >BRIEF-P administered by professionals is a useful tool to define the profile of individual development in preschool, but it is not indicative of the severity of autistic symptoms. Therefore, in ASD it could be used to define the “specifier” of Executive Functioning, in line with the DSM-5 suggestion. Based on these considerations, the evaluation of EF cannot be left solely in the hands of a questionnaire such as the BRIEF-P, administered by professionals, but must be supported by a clinical diagnosis carried out by professionals with training and experience in autism within a multidisciplinary ASDm. | NO |
| [57]/ EE.UU |
Non-experimental Descriptive Comparative/Cause 2 groups: - ASD -Control |
-ASD= 39 -Control=39 |
2.83–5.83 years | >Autism Diagnostic Observation Schedule (ADOS) | BRIEF-P | >Wechsler Preschool and Primary Scale of Intelligence-Revised (WPPSI-R) >Wechsler Preschool and Primary Scale of Intelligence-Third Edition (WPPSI-III) >WPPSI-III and WPPSI-R |
>Preschoolers with ASD showed generalised deficits in Executive Control when informants were parents. They have greater difficulties in: inhibition, flexibility, emotional control, working memory, and planning/organisation | NO |
| [58]/ EE.UU |
Non-experimental Descriptive Comparative/Cause 2 groups: - ASD -Control |
-ASD_high performance=20 -Control=20 |
54.57 months (4.55 years) |
>Autism Diagnostic Interview-Revised (ADI-R) |
BRIEF-P | >Child Behavior Questionnaire–Short Form (CBQ-SF) | >Emotion regulation was positively related to performance in the Day/Night inhibition task, and was negatively related to deficits on the Inhibitory Control Index in the BRIEF-P | YES |
| [59]/ EE.UU |
Non-experimental Descriptive Comparative/Cause 2 groups: - ASD - Persasive Developmental Disorder |
-ASD=29 -Control=30 |
4-6 years | Schooled in a Special Education center being consulted on the clinical diagnosis. | BRIEF-P | >The Leiter International Performance Scale-Revised (Leiter-R) | >ASDchers in the group of children with ASD reported a higher level of difficulty in Executive Functioning skills in all domains, compared to the group of children without autism. It is noteworthy that the mean Global Executive Functioning Index score was five times higher in the ASD group compared to the non-ASD group. | YES |
Table 2.
Effect size estimates.
| Author/Year/Country | Probabilidad de sesgos | Preocupación sobre la aplicabilidad de los resultados | |||||
| Selección de los individuos | Prueba índice | Prueba de referencia | Flujo y tiempos | Selección de los pacientes | Prueba índice | Prueba de referencia | |
| [47] /Canada | ALTO | BAJO | BAJO | INCIERTO | BAJO | BAJO | BAJO |
| [48]/Canada | BAJO | BAJO | INCIERTO | INCIERTO | BAJO | INCIERTO | INCIERTO |
| [49])/EE.UU | ALTO | INCIERTO | INCIERTO | INCIERTO | ALTO | BAJO | BAJO |
| [50]/Germany | ALTO | BAJO | BAJO | BAJO | ALTO | BAJO | BAJO |
| [51]/EE.UU | ALTO | BAJO | BAJO | ALTO | BAJO | BAJO | BAJO |
| [52]/EE.UU | BAJO | BAJO | BAJO | INCIERTO | BAJO | BAJO | BAJO |
| [53]/EE.UU | ALTO | BAJO | BAJO | INCIERTO | ALTO | BAJO | BAJO |
| [54]/Netherlands | ALTO | BAJO | BAJO | INCIERTO | ALTO | BAJO | BAJO |
| [55]/EE.UU | ALTO | BAJO | BAJO | INCIERTO | BAJO | BAJO | BAJO |
| [56]/Italia | ALTO | ALTO | BAJO | INCIERTO | ALTO | BAJO | BAJO |
| [57]/EE.UU | ALTO | ALTO | BAJO | INCIERTO | ALTO | BAJO | BAJO |
| [58]/EE.UU | ALTO | ALTO | INCIERTO | INCIERTO | BAJO | INCIERTO | ALTO |
| [59]/EE.UU | ALTO | ALTO | BAJO | INCIERTO | ALTO | BAJO | BAJO |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



