
Submitted:
03 July 2024
Posted:
06 July 2024
You are already at the latest version
Abstract
(1) Background: LUS has emerged as a simple, rapid and non-invasive method for the dynamic assessment of pulmonary congestion, a major prognostic factor and a therapeutic target in AHF. (2) Methods: In the single-center prospective observational study, 42 patients hospitalized for AHF in the post-emergency polyvalent medicine department of CHU Grenoble were successively included between May 2021 and July 2022. Clinical examination, LUS and electrolyte panel results were collected daily. Vital status was assessed 30 days after the last LUS. The primary endpoint was the evolution of the number of B-lines according to the dose of diuretic administered ; (3) Results: We performed 188 LUS. Our patients were elderly (85.8 [SD 8.1]) and comorbid. The median number of B-lines decreased from 17 at admission to 7 in the middle of the hospital stay, then stagnated until discharge. Simultaneously, the median dose of diuretics, initially stable at a maximum of 40 mg/d IV, decreased to 20mg/d IV by the end of hospital stay. Patients with CKD had a higher mean number of B-lines at entry (24.2 [SD 11.6]) compared to those without CKD (8.2 [SD 8.8]). However, the evolution of B-lines number was independent of creatinine levels. 30-day all-causes mortality was significantly related to the number of B-lines at discharge (15.2 [SD 10.1] in deceased patients versus 3.9 [SD 5.4] in living patients, p
Keywords:
acute heart failure
; pulmonary congestion
; lung ultrasound
1. Introduction
The Heart failure is a major public health problem. In France, this frequent and growing pathology affects 2.3% of the adult population and is responsible for 70,000 deaths per year. Acute heart failure (AHF) is one of the leading cause of hospitalization in patients over 65 years old, with hospital stays that are often long and expensive [1].
Pulmonary congestion appears as a major prognostic factor in AHF [2,3], and therefore represents an important therapeutic target [4]. However, it is poorly evaluated by the usual methods used in the medical ward. Clinical evaluation is not very sensitive for its detection [5], even by experienced physicians, and pulmonary auscultation is poorly reproducible. These clinical evaluation is not standardized, yet it represents the usual patient monitoring and is used to adapt diuretic therapy. Studies are currently underway to standardize this care, such as the CARESS protocol within the PRODUCT HF study [6].
LUS is an easy-to-use, rapid, reproducible and non-invasive method that offers bedside evaluation of pulmonary congestion status [7]. Minimal training is required and reproductible results are obtained after 30 minutes to 1 hour of practice [8]. A B-line, or comet tail, is an ultrasound artefact characterized by a vertical hyperechogenic line starting from the pleural line, not fading, and moving synchronously with the lung sliding. It reflects the presence of engorged interlobular septa, areas where air is in close contact with water, leading to decreased air content and increased lung density due to differences in acoustic impedance. The number of B-lines increases with the reduction in air content. They are correlated with the presence of an alveolar-interstitial syndrome, with a sensitivity and a specificity of 93% [9,10].
The value of LUS for the diagnosis of AHF has already been proven, particularly in patients admitted to the emergency department (ED) for acute dyspnea [8,9,10]. Monitoring B-lines could be interesting for tracking pulmonary congestion, allowing for treatment in AHF patients and improving their prognosis. Additionally, diuretic administration is followed by a rapid decrease in the number of B-lines [11].
In this prospective observational study, we will correlate the evolution of B-lines with diuretic posology and clinic and biologic signs of pulmonary congestion in patients admitted with AHF in a polyvalent medicine unit.
2. Materials and Methods
2.1. Study Design
We conducted this single-center prospective cohort study in the internal medicine department of Grenoble Alpes University Hospital (CHUGA). This department admits a large number of patients directly from the ED and with any type of medical pathologies.
The senior doctors working in this department are emergency physicians, general practitioners, geriatrics and internists.
2.2. Population
Patients admitted to the internal medicine department from ED between May 18, 2021, and July 15, 2022, were screened for inclusion. Patients are eligible if they are over 18 years-old and present an AHF at admission. The diagnosis is assessed by two senior physicians, according to the diagnostic criteria of the European Society of Cardiology (ESC) guidelines [12]. Patients undergoing hemodialysis, those with pneumonectomy or lung fibrosis and those under guardianship or deprived of freedom are excluded.
2.3. Heart Failure Treatment and Protocol
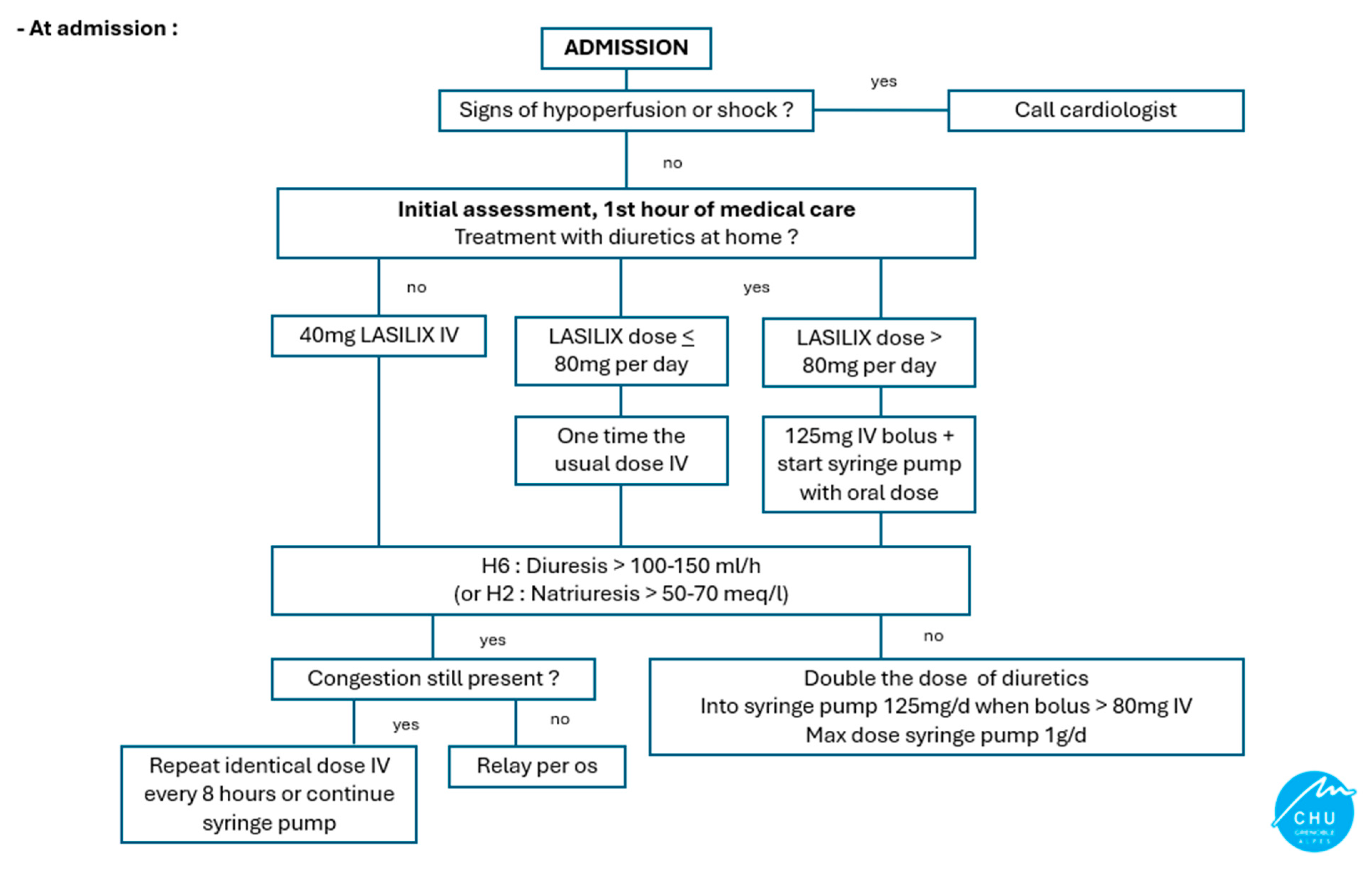
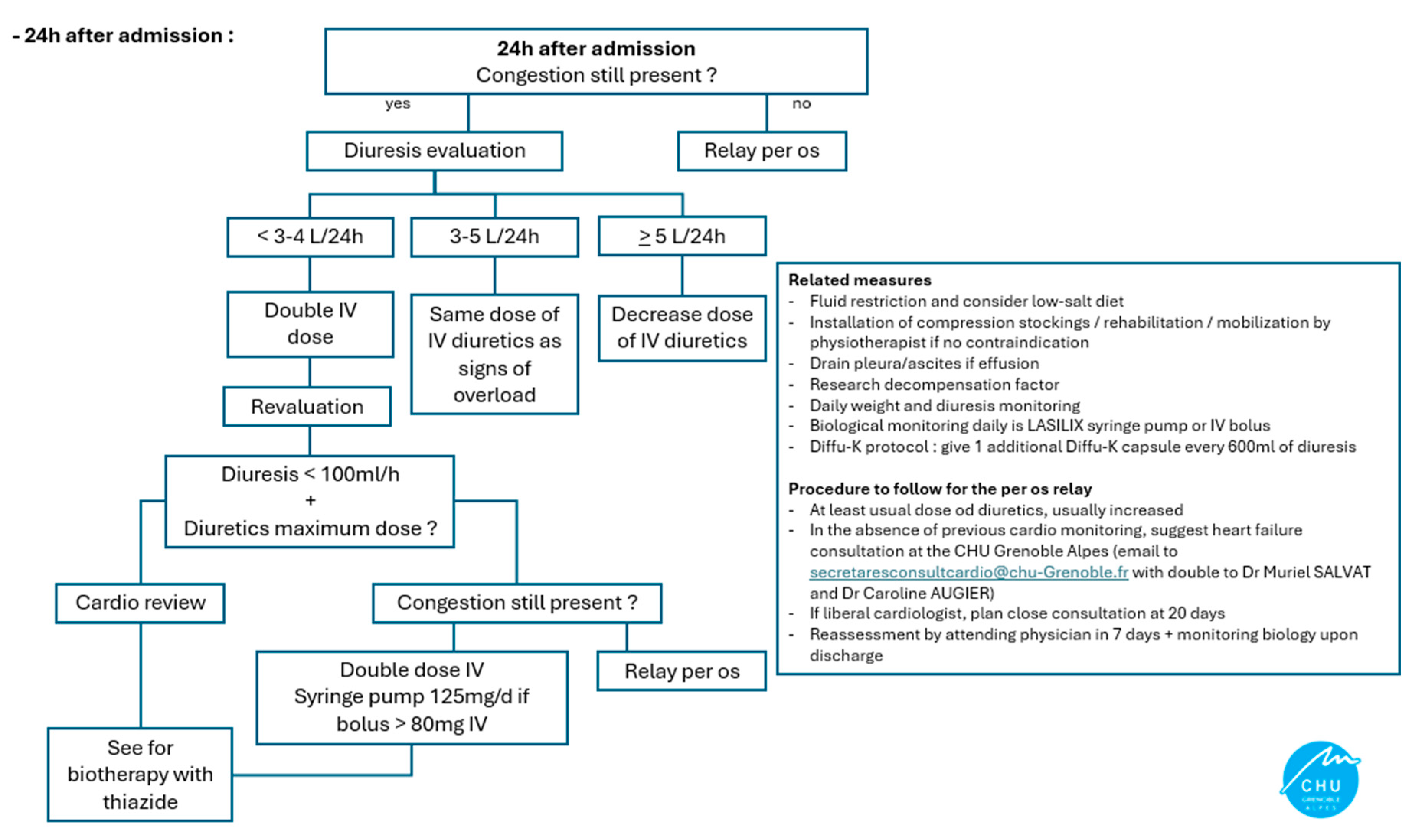
Patients are treated for AHF according to usual practices and with the help of a protocol created by the cardiologists at CHUGA, which summarize the guidelines of the ESC [Appendix A]. This protocol uses clinical assessment, weight and diuresis to guide therapeutic adjustments, ultrasound techniques are not available in the department. The protocol has been in use for several months before the start of the study and physicians were encouraged to follow it. However, adaptation of diuretic posology were left to their discretion.
2.4. Lung Ultrasound Protocol
For each patient, LUS is performed at admission and daily by a senior physician from the department who is not in charge of the patient and is blinded to clinical and biological findings.
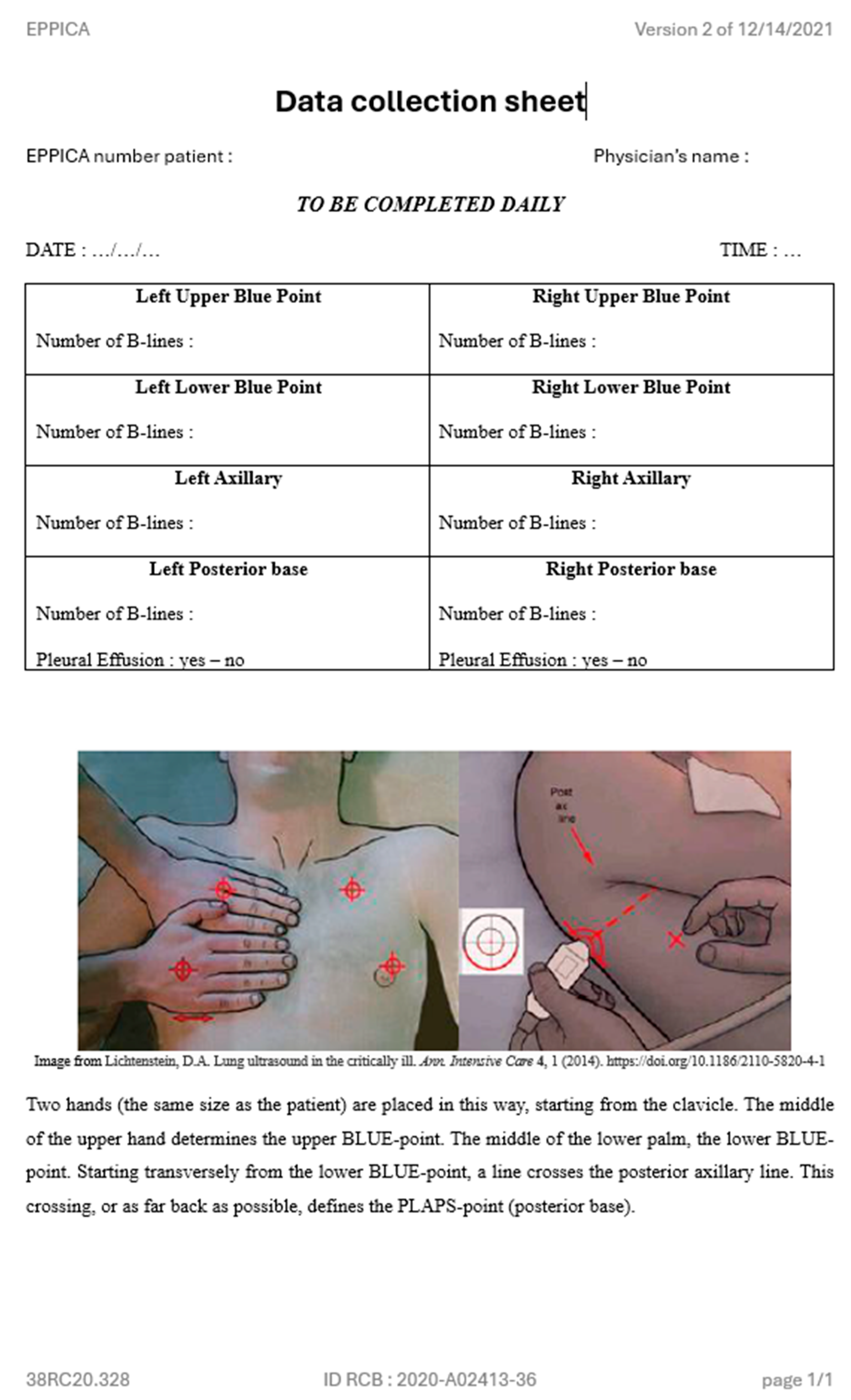
The patient’s position can influence the number of B-lines [7,13], raison why, for each LUS at bedside, we positioned our patients in a 30° supine position using adjustable beds. Inspired by the BLUE-protocol of Lichtenstein [10,14] and according to the expert consensus document [15], four points on each hemithorax are analyzed : two anterior points, between the sternum and the anterior axillary line, one under the clavicle and one under the nipple ; and two lateral points, between the anterior and posterior axillary lines, one superior and one inferior.
For each area, the number of B-lines is counted, and the presence of pleural effusion is recorded. In areas where pleural effusion is present, the number of B lines is not counted. Results are reported on a paper form [Appendix B], completed by the physician for each exam, and kept sealed.
GE Healthcare Vivid T8 echograph device is used, with a 3.5-5 MHz phased array transducer at an imaging depth of four to six centimeters. The depth is set according to the department’s standard practices to ensure standardized image reading, it could be adjusted according to the patient’s size.
Most of the physicians already had an echography certification, while others completed a theoretical and practical course before starting the inclusions.
2.5. Follow-Up / Data Collection
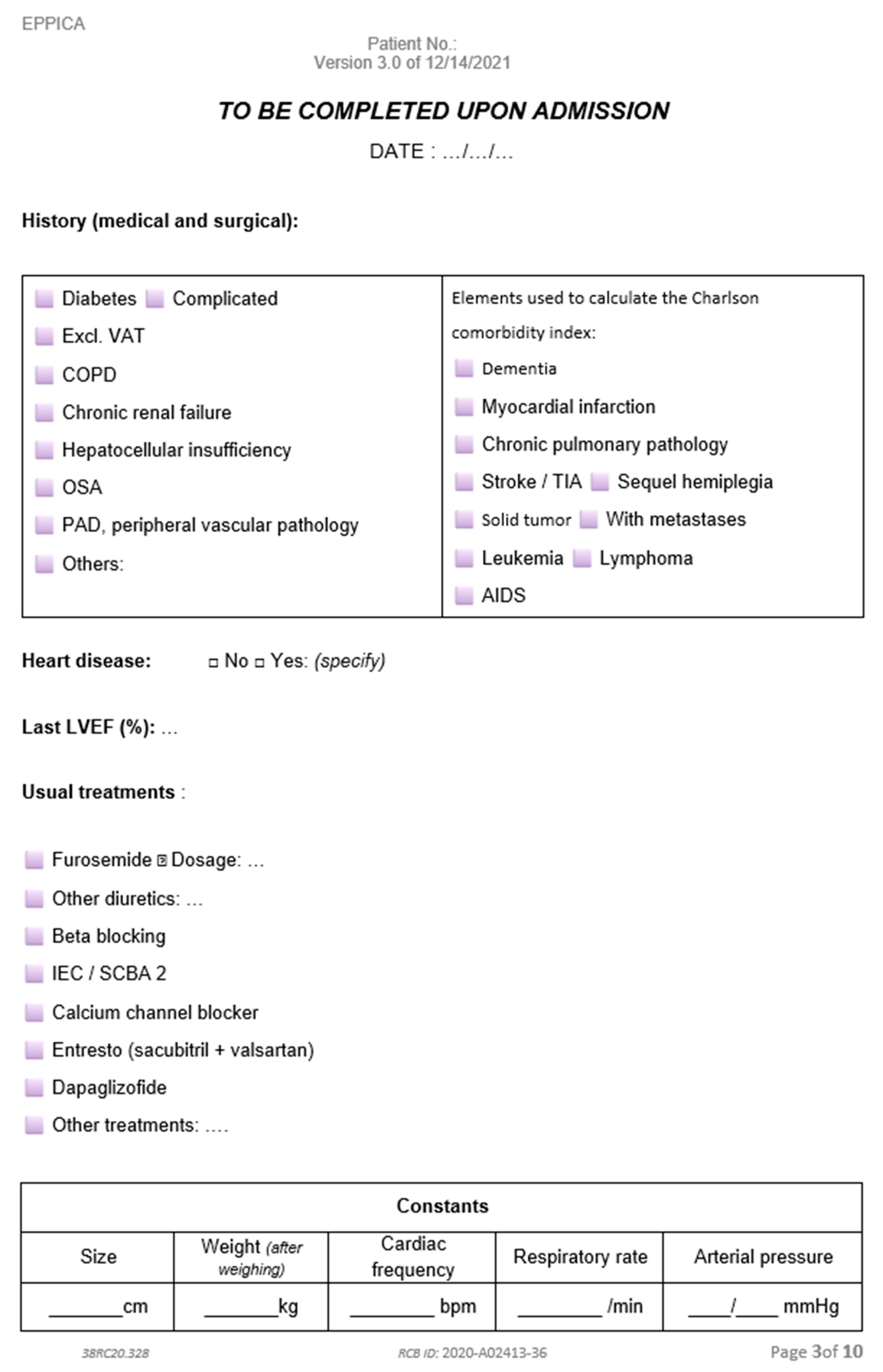
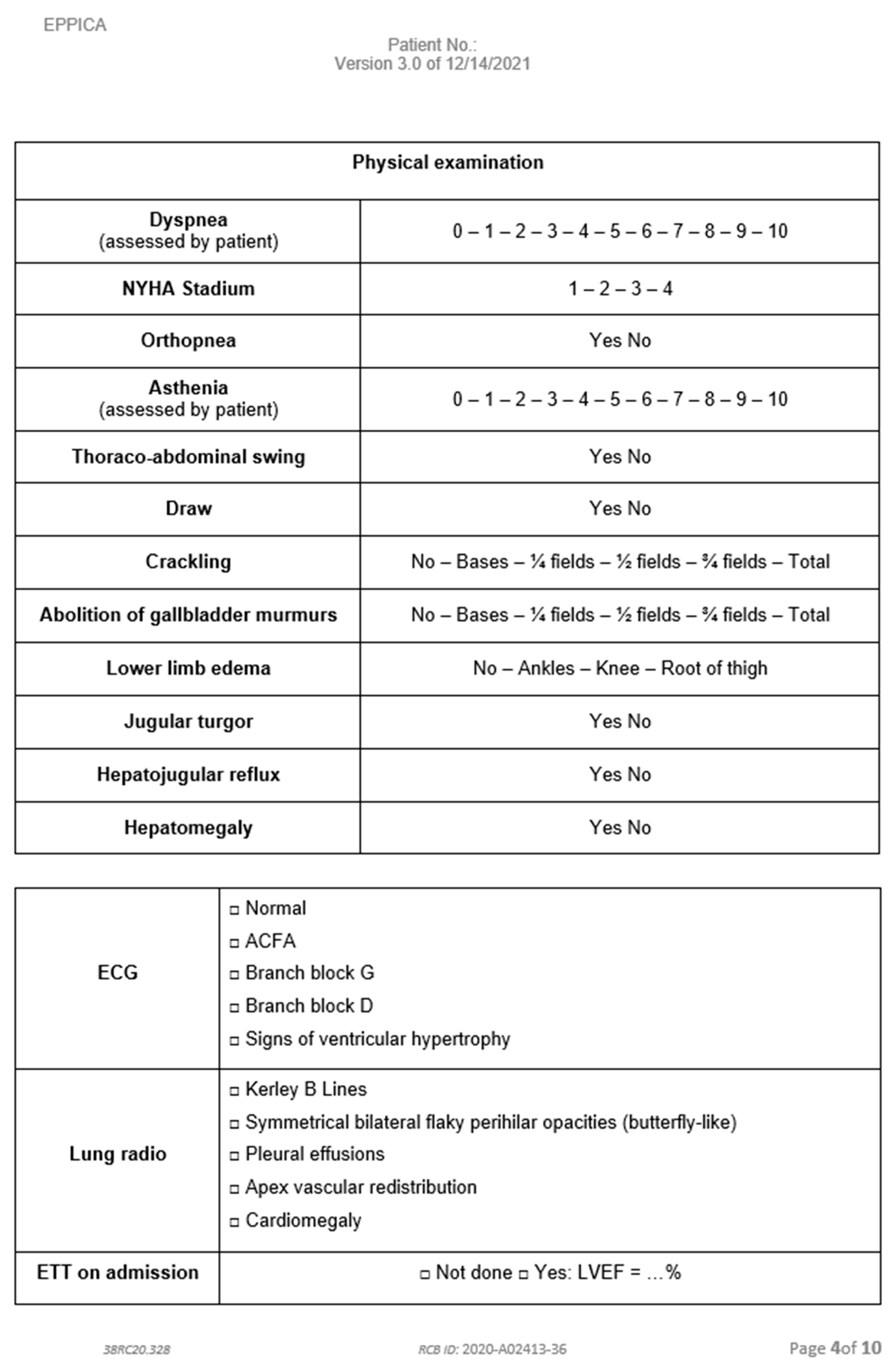
Medical information about the patient's status is recorded at admission and updated daily by the physician responsible for the patient [Appendix C] in a nominative data collection notebook [Appendix D].
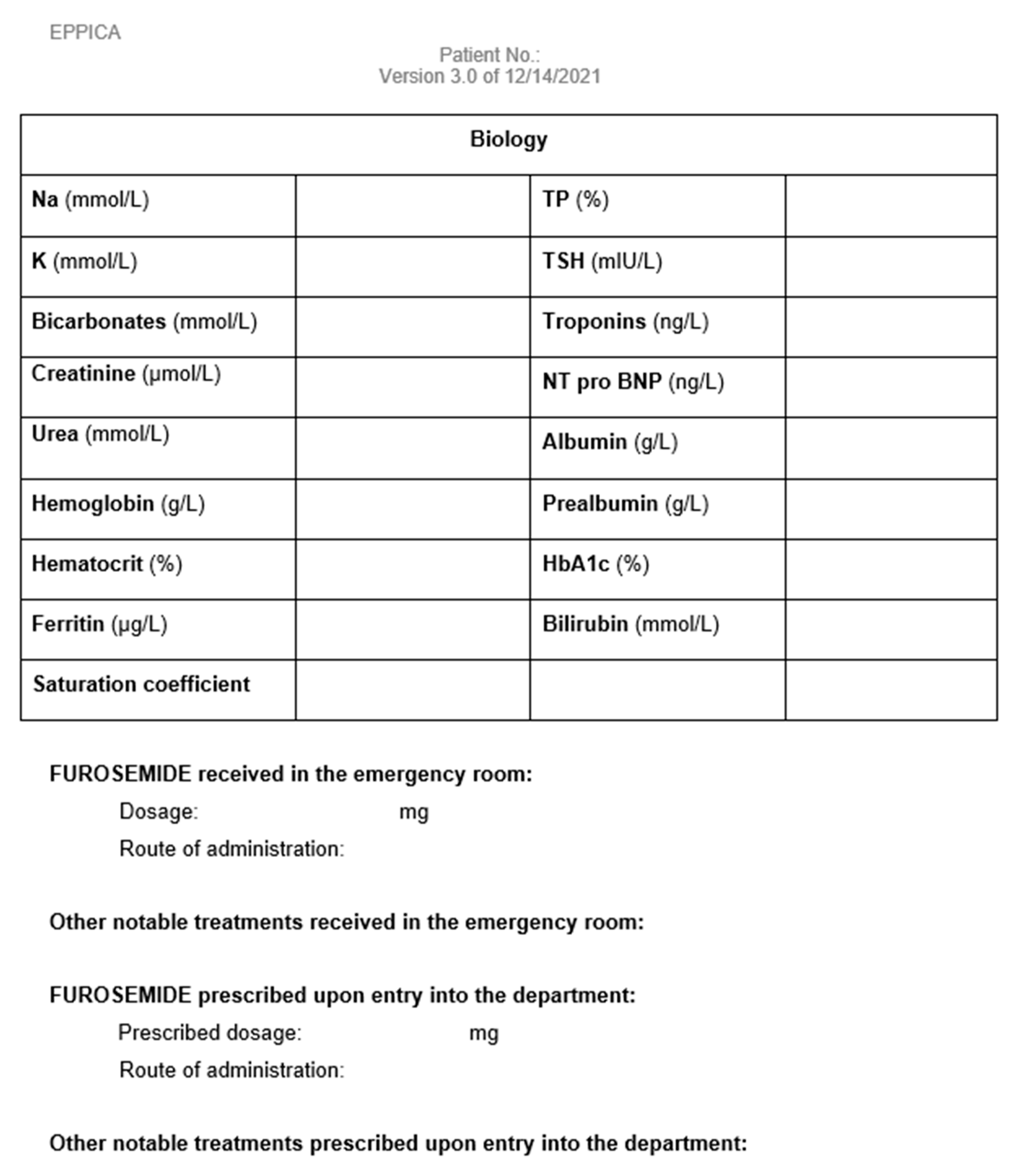
Demographic variables (age, sex), past medical history and comorbidities (Modified Charlson score), usual treatments, heart failure characteristics (aetiology, ejection fraction), physical examination findings and clinical variables (height, weight, vital signs, heart failure signs and symptoms), as well as results of electrocardiogram, chest radiography and biological test (hemogram, electrolyte panel and renal function, martial assessment, liver function test, natriuretic peptides, troponin, and nutritional status) are recorded at admission.
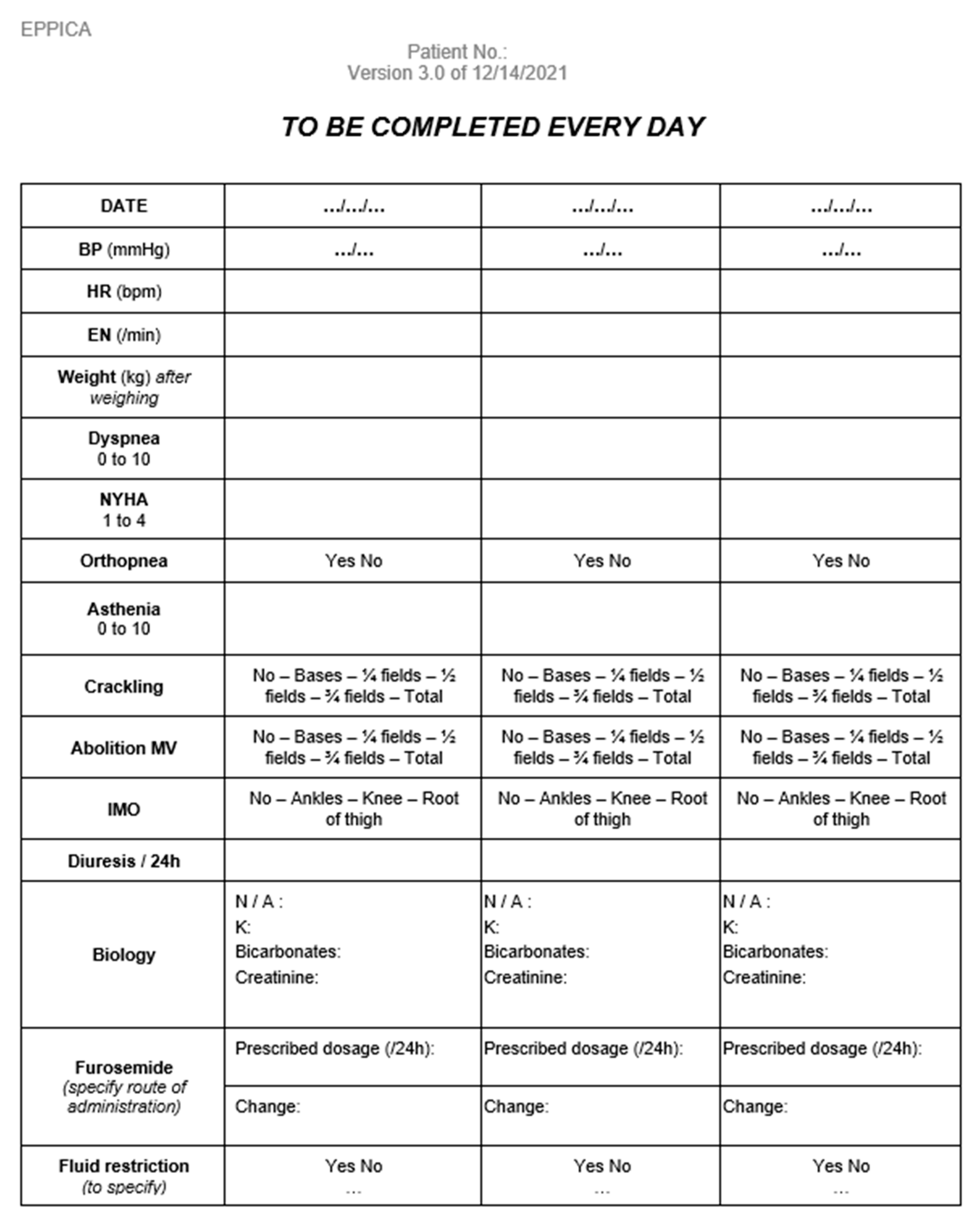
Every day, including the day of discharge, clinical signs and symptoms of heart failure, vital parameters, administered diuretic treatment, and available electrolyte panel are recorded.
On the day of discharge, we collect information on the triggering factor of cardiac decompensation, whether iron was administered during hospitalization, nutritional and kinetic assessment, and planned follow-up (both biological and medical). Patients who remain in the hospital after the resolution of AFH for a social issue (institutionalization or implementation of home help) or secondary medical issue are considered discharged after 48 hours of stable diuretic treatment.
Vital status and possible rehospitalization are enquired 30 days after the last LUS by reviewing hospital medical records or via phone calls to the patient, their family, or their attending physician.
2.6. Study Outcomes
The primary endpoint examined is the daily measurement of the number of B-lines in LUS compared to the evolution of diuretic doses.
Several secondary outcomes are assessed : the evolution of the number of B-lines according to clinical signs of cardiac overload (crackles and lower limbs oedemas) and the agreement between them at hospital discharge ; the evolution of the number of B-lines according to plasma creatinine level; and the prognostic value of LUS at discharge in predicting readmission for AHF and all-causes mortality at 30 days.
We also aim to assess the feasibility of daily monitoring of LUS during working days, as well as the interobserver reproducibility of LUS by two doctors on the same group of patients, on the same day.
2.7. Statistical Analysis
We calculated that with a sample size of 42, a two-sided 95% confidence interval for a single mean will extend one from the observed mean, assuming that the standard deviation is known to be 3,28 and the confidence interval is based on the large sample z statistic.
For the statistical analysis, the duration of follow-up for each patient was divided into four parts, with 100% representing the total time of hospitalization. A descriptive statistical analysis was performed on the baseline characteristics of the population. Continuous variables are reported as median (interquartile range [IQR]) or mean value (standard deviation [SD]), as appropriate. Categorical variables are expressed as percentage (%).
In the analysis of the primary endpoint, we first used a Join Point regression model describing B-lines and diuretic posology. Then, a temporal trend analysis was performed on the evolution of the number of B-lines and posology of diuretics. A linear regression model was employed to model the linear trend and to compare trends according to the hospitalization duration threshold defined as 0% (admission), 25%, 50%, 75% et 100% (discharge). Adjustment for patient age was performed.
The assessment of the evolution of the number of B-lines according to clinical signs of cardiac overload, the relationship between B-lines and crackles at discharge and the evolution of B-lines count according to plasma creatinine level was performed using the same analysis as the primary endpoint.
The prognostic value of LUS at discharge for predicting readmission or all-causes mortality at 30 days was analyzed using a linear regression model.
For the reproducibility study, we calculated a correlation coefficient : an intraclass correlation coefficient for the quantitative variable (B-lines) and a Kappa coefficient for the qualitative variable (pleural effusion).
Statistical significance was set at p < 0.05. All analysis was performed using the programs RStudio (Version 2022.07.1, PBC, Boston, MA) and Jamovi (Version 2.3.13.0, Sydney, Australia).
2.8. Ethical Aspects
The study protocol and its review were approved by an institution review board (Comité de Protection des Personnes Est III), on November the 4th of 2020 [Appendix F] and on March the 3rd of 2022 [Appendix G], respectively. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Patients received oral and written information about the nature of the study, its objectives and expected benefits. Their non-opposition was recorded by one of the senior physicians involved in the research project, in accordance with the French law for observational study with usual care. If patients were unable to decide for themself, the consent was obtained from their support person.
3. Results
3.1. General Characteristics
From May 25, 2021, to July 14, 2022, 57 patients hospitalized for AHF were screened, and 43 were included in the study. Finally, 42 patients were analyzed due to the loss of a file (Figure 1). No patients were lost for follow-up.
The population was elderly (average age, 85.8 + 8.2 years), mainly masculine (61.9%) and had multiple comorbidities (Charlson Comorbidity Index (CCI) 8.5 + 2.3). Additionally, 73.8% of patients had a known heart disease and received an average daily dose of 135,5 mg of furosemide at home (range 0-1000mg). (Table 1).
The Table 2 presents the clinical examination findings, creatinine level, as well as the furosemide posology and number of B-lines at different times during hospitalization.
3.2. Reproducibility and Feasibility
After comparing 17 exams conducted by two different physicians, the intraclass correlation coefficient obtained for the total number of B lines was 0,809 (IC 95% : 0.556 – 0.955) and the Cohen’s kappa coefficient for the presence of pleural effusion was 0,764 (IC 95% : 0.403 – 1.00).
The 42 patients analyzed accumulated 237 working days of hospitalization. A total of 188 LUS were performed, representing 79,3% of the working days. In other words, 20,7% of the LUS were missing during patient follow-up.
3.3. LUS B-Lines, Posology Diuretics, Clinical and Biological Parameters
The number of B-lines decreases promptly and importantly at the beginning of hospitalization with the diuretic therapy, then stabilizes in the middle and remains so until discharge. Diuretic posology remains stable at beginning of hospitalization, then decreases towards the middle and until discharge (Figure 2).
The crackles also decrease during hospitalization, without any significant relationship to the number of B-lines (Table 3).
At discharge, there is no significant connection between the number of B-lines and the presence or intensity of crackles. (Table 4).
Twenty-two patients (52%) had a known history of chronic kidney disease (CKD) with a baseline average creatinine value of 155.7 µmol/l. Their average value was 174.2 µmol/l at hospital admission and remained relatively stable throughout the hospital stay (Figure 3). Among them, 15 (68%) suffered acute kidney injury (AKI). AKI was present in 11 patients (50%) at admission and 4 patients (18%) developed it during hospitalization. The 20 patient (48%) without a history ok CKD had an average creatinine level at admission of 91.8 µmol/l, which also remained stable throughout their hospital stay (Figure 4). Among them, seven patients (35%) suffered from AKI with 2 patients (10% having AKI at admission and an additional 5 patients (25%) developing it during hospitalization. Table 5 shows that, at admission, patients with a history of CKD had a significantly higher number of B-lines than those without a history of CKD. There was no relationship observed between the evolution of the number of B-lines and creatinine levels.
Within one month of hospitalization, 5 patients (12%) died and 7 patients (20%) were re-hospitalized for AHF. Only one of the deceased patients died after readmission for AHF. The relationship between the number of B-lines and the vital status at 30-days discharge is statistically significant with a p-value < 0.001 (Table 6).
4. Discussion
In this prospective monocentric study conducted in a post-urgence ward, we interested the relationship between the number of B-lines on LUS, the administrated diuretic posology, and the clinical and biological signs of cardiac overload in hospitalized patients with AHF. We observed an important decrease in the number of B-lines during the first half of hospitalization, followed by a stabilization trend, and a stabilization trend then, while the diuretic posology decreased during the second part of hospitalization. At discharge, some of the patients presented subclinical pulmonary overload without crackles but with the persistence of B-lines. The presence of B-lines at discharge is significantly associated with a higher risk of mortality at 30-days.
Previous studies examining the relationship between LUS B-lines and diuretic posology in hospitalized patients outside cardiology and intensive care unit are limited. Pang et al [16] conducted a pilot trial wherein patients consulting for AHF and pulmonary congestion in the ED were divided into two groups to compare standard care and a LUS-guided strategy-of-care in the first six hours. Patients in the intervention group showed a consistent numerical reduction in B-lines during hospitalization, suggesting that protocol driven therapy may facilitate a faster congestion reduction. Panuccio et al [17] conducted a pilot study in hospitalization patients for AKI in nephrology ward. They showed that LUS is superior to clinical examination for detecting interstitial lung edema, notably in preclinical stages of congestion. Cardiology groups have also assess the utility of LUS in adjusting diuretic treatment in outpatient settings. For example, Rivas-Lasarte et al. [18] used LUS to monitor patients after a hospitalization for AHF and showed that patients with LUS-guided adjustment of diuretic treatment had fewer urgent visit, fewer hospitalization for lower all-cause mortality rates (HR = 0.518 [CI 95% : 0.268-0.998 ; p = 0.049]) compared to those with standard follow-up.
Our results are consistent with previous studies that report a discrepancy between clinical pulmonary congestion, notably crackles, and LUS B-lines. This discrepancy can occur at both admission and discharge, as some patients may have subclinical pulmonary fluid overload that is not detectable through clinical examination. LUS can identify this clinically silent pulmonary edema. In the study by Platz and al. [7], 35% of patients with acute heart failure did not have crackles at admission, whereas only 6% did not have B-lines. At discharge, Rivas-Lasarte and al. [19] found that 40% of their patients who were “lung dry” to auscultation still had subclinical fluid overload detected by LUS, which seems to have similarly poor prognosis as overt clinical pulmonary congestion. The poor interobserver agreement of crackles at lung auscultation can also participate to this discrepancy. For Panuccio et al [17], in patients with AKI, the agreement between lung crackles and LUS-B lines was poor (κ = 0.02, p = 0.63). Ramos-Hernandez et al [20] compared the interobserver agreement of LUS and lung auscultation, finding good reproducibility for B-lines (κ = 0.81 [CI 95% : 0.81 – 0.83]) but poor repoducibility for crackles (κ = 0.18 [CI 95% : 0.16 – 0.20]).
Evaluating lung congestion in patients with AKI is a challenging task. Panuccio et al [17] showed that in patients with AKI hospitalized in nephrology ward, hidden lung congestion is more frequent in apparently euvolemic and hypovolemic patients. Approximately 30% of their euvolemic and hypovolemic patients presented clear-cut cardiovascular congestion. For Ruggenenti et al [21], patients with AHF and concomitant AKI require urgent and effective therapy, as the combination of both is a stronger predictor of mortality. The emphasize that the priority must be pulmonary decongestion without being limited by altered renal markers. Blair et al [22] noted that AKI appearing in-hospital reflects aggressive decongestion, as it is frequently associated with reductions in natriuretic peptides, blood pressure and body weight, which are good prognostic factors. We did not find studies focusing on LUS and the clinical or biological signs of AKI during episodes of AHF. In our study, patients with a history of CKD had more B-lines at admission than those with healthy kidneys. This relationship was significant only at admission. During hospitalization, creatinine levels remained steady in both groups while the number of B-lines decrease.
The lack of clearance of B-lines at the discharge seems to be associated with a high risk of adverse events, such as ED consultation, readmission for AHF, and all-causes mortality. Our results of 30-day all-cause mortality and readmission for AFH are consistent with data of the American Heart Association, which reports rates of 10% and 20-25% respectively, in patients older than 65 years following an episode of AHF [23]. Cogliati et al [3] who studied in-patients in an internal medicine department, found that the sonographic score was significantly associated with adverse events at 100days, with a hazard ratio (HR) of 1.19 (IC 95% : 1.05-1.14 ; p = 0.005). Similarly, E. Platz et al [24] found a strong relationship between the risk of adverse event and a high number of B-lines at discharge, with an unadjusted HR at 60 days of 3.30 (IC 95 % CI : 1.52-7.17 ; p = 0.002). In our study, we found a significant relationship between the number of B-lines and 30-days all-causes mortality. However, we did not find a connection between the number of B-lines and the risk of readmission, which is inconsistent with literature.
Gargani et al [4] and Miglioranza et al [25] concluded that the presence of fewer than 15 B-lines at discharge identifies a subgroup at extremely low risk of adverse event. Using this threshold to determine prognosis, we observed that among our deceased patients, four out of five had ≥ 15 B-lines, whereas among the surviving patients, only two out of 37 had ≥ 15 B-lines.
We focused on all-cause mortality and did not collect the cause of death. Other Several factors may contribute to explain this high mortality rate. The average age in the aforementioned studies were 70, 53 and 71 years respectively. Like us, only Cogliati et al [3] were interested in elderly patients. The mean age of our patient was 85.6 years (range : 71.7 – 98.8), and age is a known strong and independent predictor of mortality in patients with HF [26]. Furthermore CCI is an independent predictor of mid-term post-discharge mortality among elderly HF patients [27]. A CCI ≥ 5 is associated with an age-adjusted HR of 77.3 (IC 95% 74.7-79.8) for 1-year mortality [28] and our average CCI was 8.5 (range : 5 – 17). The prognosis seems to be influenced not only by pulmonary edema but also by the triggering factors and underlaying conditions [29,30].
4.1. Strenghs
Our study has several strengths. First, we performed 8-zones LUS according to recommendations by international consensus statement [15] and interpreted in real time. LUS were performed with patients in the same position, using the same ultrasound device and configuration.
Second, although the extrapolation of our results may be limited by the small sample size and the single center approach, we performed a large number of LUS (188). Two main factors may explain the low number of patients included : first, the Covid-19 pandemic (the department only admitted Covid-19 patients during the months of December 2021 and January 2022, and three covid-19 clusters slowed down admissions); second, other departments in our hospital also admitted these patients (cardiology, geriatrics and short-stay hospitalization unit).
Third, most studies evaluating LUS are conducted in a cardiology or an intensive care units, with few are conducted in a polyvalent medicine ward. Our patients are mainly elder and have multiple comorbidities, bringing our study population closer to a geriatric population than to cardiology patients, who are often younger.
Fourth, practitioners performing the LUS were blinded to the clinical examination. Even though LUS was not performed by the same physician every day, the intraclass correlation coefficient for the number of B-lines was excellent (0,809 [IC 95%: 0.556 – 0.955]) and comparable to that found in other studies. For instance, Russel et al [31] reported a coefficient of 0,74 after a trial of approximately 11 exams and two hours of theoretical class. Miglioranza et al [25] reported a coefficient of 0.98 (95% IC : 0.98-0.99 ; p < 0.0001) in a set of 20 consecutive patients, M. Mazzola et al [32] found a coefficient of 0.98 (p < 0.0001) in 50 LUS videos evaluated by an expert reader.
Fifth, although doctors were free to prescribe treatment doses based on their assessment, our study positively impacted the implementation of standardized care protocols for AHF treatment in the department.
4.2. Limitations
To our knowledge, our study had some limitations. First, the absence of a consensus definition of cardiac congestion and the lack of a gold standard to verify its presence are significant limitation for the diagnosis of AFH. Consequently, physicians relied on a set of clinical, biological and imaging criteria to establish the diagnosis before including a patient, as recommend by the ESC [12]. There is also no consensus on the definition of ultrasound pulmonary congestion, which is why we decided to count the number of B-lines without setting a specific cut-off. We did not exclude patients with pleural effusion. We decided to record "0" when a pleural effusion prevented the counting of B-lines, which likely leads to an underestimation of congestion. This is also one of the limitations of our study.
Second, we did not perform daily LUS on each patient during working days as planned, we completed 79,3% of the intended exams. This can be explained by the high workload and the need for sufficient senior doctors to hold the blind. We did not find other studies that performed daily LUS, making this an original feature. Gargani et al [4] performed LUS at admission and discharge with 100% feasibility, Mazzola et al [32] conducted LUS at admission, and 24 and 48 hours after admission, and before discharge.
Third, during their stay in the ED, our patient received furosemide (an average of 122 mg IV). Some patients stayed for several hours, and we have no ultrasound data from this period. B-lines are dynamic and quickly impacted by diuretic treatment [7]. Consequently, our clinical and ultrasound examination may have shown fewer signs of congestion than when patients first arrived at ED. Pang et al [16] showed that patients with LUS-guided therapy in the ED had a significantly greater reduction in B-lines in the first 48 hours compared to those receiving usual care (p = 0.04).
Fourth, the detection of B-lines does not necessarily imply the cardiogenic origin. Other pathologies can also cause of B-lines. None of our patients presented with ARDS and we excluded patients with fibrosis and pneumonectomy. However, we included patients with infectious pneumonia, which is a common trigger for AHF. We used the total number of B-lines for our analysis, which can be increased in such cases and may constitute a confounding factor. Nevertheless, according to Mazzola et al [32], LUS can monitor pulmonary decongestion in patients with AHF, whether they have associated pneumonia or not.
Fifth, we conducted the study without considering the left ventricular ejection fraction. Yang et al [33] did not find significant differences in the B-lines between heart failure with preserved ejection fraction (HFpEF) and reduced ejection fraction (HFrEF) groups. Conversely, Palazzuoli et al [34] found that patients with HErEF had more B-lines compare to them with HEpEF at admission (p-value = 0.04) and at discharge (p-value = 0.009). These studies are discordant, indicating a need for further research.
5. Conclusions
Over the last decade, pleuropulmonary ultrasound has emerged as an additional tool for diagnosing and monitoring patients who suffer from heart failure.
In this prospective observational study conducted in a multidisciplinary medical ward, we observed a trend towards stagnation in the number of B-lines at the end of hospitalization, while the administered diuretic posology continued to decrease. At the time of discharge, some of our patients presented a subclinical pulmonary overload. Subject to small patient numbers and the limitations describe above, we found a significant relationship between the number of B-lines at discharge and the risk of death at 30 days.
In the absence of a gold standard for the quantitative assessment of cardiac overload, LUS is an valuable tool that could help optimize the management of congestion, particularly when it becomes subclinical, thereby improving the 30-days prognosis. A randomized interventional study is needed to assess the value of echo-guided therapeutic management in conventional non-cardiology hospital settings.
Author Contributions
Conceptualization, A. Grember, C. Cheval and P. Dumanoir ; methodology, A. Grember, C. Cheval, P. Dumanoir and A. Bellier ; software, A. Bellier ; validation, P. Dumanoir and L. Bouillet ; formal analysis, A. Bellier, P. Dumanoir and E. Bel Alonso; investigation, R. Papillon, L. Mairot, A. Deroux and P. Dumanoir; resources, P. Dumanoir and L. Bouillet ; data curation, E. Bel Alonso, A. Grember and C. Cheval; writing—original draft preparation, E. Bel Alonso; writing—review and editing, P. Dumanoir and L. Bouillet .; visualization, E. Bel Alonso.; supervision, P. Dumanoir; project administration, P. Dumanoir. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study protocol and its review were approved by an institution review board (Comité de Protection des Personnes Est III), on November the 4th of 2020 (Appendix 6) and on March the 3rd of 2022 (Appendix 7) respectively. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Informed Consent Statement
Patients received oral and written information about the nature of the study, its objectives and expected advantage. Their non-opposition was recorded by one of the senior physicians implied in the research project, according with the French law for observational study with usual care. If patients were unable to decide for themself, consent from the support person was collected.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A. Diuretic Adaptation Protocol
Appendix B. Paper Form to Report LUS Results
Appendix C. Follow-Up Table

| Description of the data collected |
Pre inclusion J0 (entry into service) |
Inclusion T0 |
Daily during hospitalization |
Follow-up visit 30 days (+/- 3 days) after the last ultrasound |
| Subject Information | ✔ | |||
| Checking eligibility criteria | ✔ | ✔ | ||
| Collection of clinical data | ✔ | ✔ | ||
| Collection of biological data | ✔ | ✔* | ||
| Ultrasound | ✔ | ✔ | ||
| Collection of rehospitalizations or vital status | ✔ | |||
| Medical record review | ✔ |
Appendix D. Data Collection Notebook
Appendix E. Notice of the Committee for the Protection of Persons – November the 3rd 2020
Appendix G. Notice of the Committee for the Protection of persons – Review of protocol on March the 1rd 2022
References
- L’état de santé de la population en France - Rapport 2017 | Direction de la recherche, des études, de l’évaluation et des statistiques [Internet]. [cité 18 mars 2022]. Disponible sur: https://drees.solidarites-sante.gouv.fr/publications-documents-de-reference/rapports/letat-de-sante-de-la-population-en-france-rapport-2017.
- Coiro S, Rossignol P, Ambrosio G, Carluccio E, Alunni G, Murrone A, et al. Prognostic value of residual pulmonary congestion at discharge assessed by lung ultrasound imaging in heart failure. Eur J Heart Fail. nov 2015;17(11):1172-81. [CrossRef]
- Cogliati C, Casazza G, Ceriani E, Torzillo D, Furlotti S, Bossi I, et al. Lung ultrasound and short-term prognosis in heart failure patients. Int J Cardiol. 1 sept 2016;218:104-8. [CrossRef]
- Gargani L, Pang PS, Frassi F, Miglioranza MH, Dini FL, Landi P, et al. Persistent pulmonary congestion before discharge predicts rehospitalization in heart failure: a lung ultrasound study. Cardiovasc Ultrasound. 4 sept 2015;13:40. [CrossRef]
- Torino C, Gargani L, Sicari R, Letachowicz K, Ekart R, Fliser D, et al. The Agreement between Auscultation and Lung Ultrasound in Hemodialysis Patients: The LUST Study. Clin J Am Soc Nephrol. 7 nov 2016;11(11):2005-11. [CrossRef]
- Riocreux CAM. Thèse de médecine : Optimisation des diurétiques dans la décompensation de l’insuffisance cardiaque chronique : rationnel e tdescription de l’étude ProDUCT-HF. 2019;134.
- Platz E, Merz AA, Jhund PS, Vazir A, Campbell R, McMurray JJ. Dynamic changes and prognostic value of pulmonary congestion by lung ultrasound in acute and chronic heart failure: a systematic review. Eur J Heart Fail. sept 2017;19(9):1154-63. [CrossRef]
- Girerd N, Seronde MF, Coiro S, Chouihed T, Bilbault P, Braun F, et al. Integrative Assessment of Congestion in Heart Failure Throughout the Patient Journey. JACC Heart Fail. avr 2018;6(4):273-85. [CrossRef]
- Martindale JL, Wakai A, Collins SP, Levy PD, Diercks D, Hiestand BC, et al. Diagnosing Acute Heart Failure in the Emergency Department: A Systematic Review and Meta-analysis. Acad Emerg Med. mars 2016;23(3):223-42. [CrossRef]
- Lichtenstein DA, Mezière GA. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest. juill 2008;134(1):117-25. [CrossRef]
- Öhman J, Harjola VP, Karjalainen P, Lassus J. Focused echocardiography and lung ultrasound protocol for guiding treatment in acute heart failure. ESC Heart Fail. févr 2018;5(1):120-8. [CrossRef]
- 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure | European Heart Journal | Oxford Academic [Internet]. [cité 1 juin 2022]. Disponible sur: https://academic.oup.com/eurheartj/article/42/36/3599/6358045?login=true.
- Frasure SE, Matilsky DK, Siadecki SD, Platz E, Saul T, Lewiss RE. Impact of patient positioning on lung ultrasound findings in acute heart failure. Eur Heart J Acute Cardiovasc Care. août 2015;4(4):326-32. [CrossRef]
- Buessler A, Chouihed T, Duarte K, Bassand A, Huot-Marchand M, Gottwalles Y, et al. Accuracy of Several Lung Ultrasound Methods for the Diagnosis of Acute Heart Failure in the ED: A Multicenter Prospective Study. Chest. janv 2020;157(1):99-110.
- Platz E, Jhund PS, Girerd N, Pivetta E, McMurray JJV, Peacock WF, et al. Expert consensus document: Reporting checklist for quantification of pulmonary congestion by lung ultrasound in heart failure. Eur J Heart Fail. juill 2019;21(7):844-51. [CrossRef]
- Pang PS, Russell FM, Ehrman R, Ferre R, Gargani L, Levy PD, et al. Lung Ultrasound-Guided Emergency Department Management of Acute Heart Failure (BLUSHED-AHF): A Randomized Controlled Pilot Trial. JACC Heart Fail. sept 2021;9(9):638-48.
- Panuccio V, Tripepi R, Parlongo G, Mafrica A, Caridi G, Catalano F, et al. Lung ultrasound to detect and monitor pulmonary congestion in patients with acute kidney injury in nephrology wards: a pilot study. J Nephrol. avr 2020;33(2):335-41. [CrossRef]
- Rivas-Lasarte M, Álvarez-García J, Fernández-Martínez J, Maestro A, López-López L, Solé-González E, et al. Lung ultrasound-guided treatment in ambulatory patients with heart failure: a randomized controlled clinical trial (LUS-HF study). Eur J Heart Fail. déc 2019;21(12):1605-13. [CrossRef]
- Rivas-Lasarte M, Maestro A, Fernández-Martínez J, López-López L, Solé-González E, Vives-Borrás M, et al. Prevalence and prognostic impact of subclinical pulmonary congestion at discharge in patients with acute heart failure. ESC Heart Fail. oct 2020;7(5):2621-8. [CrossRef]
- Ramos-Hernández C, Botana-Rial M, Núñez-Fernández M, Lojo-Rodríguez I, Mouronte-Roibas C, Salgado-Barreira Á, et al. Validity of Lung Ultrasound: Is an Image Worth More Than a Thousand Sounds? J Clin Med. 25 mai 2021;10(11):2292.
- Ruggenenti P, Remuzzi G. Worsening kidney function in decompensated heart failure: treat the heart, don’t mind the kidney. Eur Heart J. oct 2011;32(20):2476-8. [CrossRef]
- Blair JEA, Pang PS, Schrier RW, Metra M, Traver B, Cook T, et al. Changes in renal function during hospitalization and soon after discharge in patients admitted for worsening heart failure in the placebo group of the EVEREST trial. Eur Heart J. oct 2011;32(20):2563-72. [CrossRef]
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, et al. Heart Disease and Stroke Statistics—2021 Update. Circulation. 23 févr 2021;143(8):e254-743. [CrossRef]
- Platz E, Campbell RT, Claggett B, Lewis EF, Groarke JD, Docherty KF, et al. Lung Ultrasound in Acute Heart Failure: Prevalence of Pulmonary Congestion and Short- and Long-Term Outcomes. JACC Heart Fail. oct 2019;7(10):849-58.
- Miglioranza MH, Gargani L, Sant’Anna RT, Rover MM, Martins VM, Mantovani A, et al. Lung ultrasound for the evaluation of pulmonary congestion in outpatients: a comparison with clinical assessment, natriuretic peptides, and echocardiography. JACC Cardiovasc Imaging. nov 2013;6(11):1141-51.
- Komajda M, Hanon O, Hochadel M, Lopez-Sendon JL, Follath F, Ponikowski P, et al. Contemporary management of octogenarians hospitalized for heart failure in Europe: Euro Heart Failure Survey II. Eur Heart J. févr 2009;30(4):478-86. [CrossRef]
- Formiga F, Moreno-Gonzalez R, Chivite D, Franco J, Montero A, Corbella X. High comorbidity, measured by the Charlson Comorbidity Index, associates with higher 1-year mortality risks in elderly patients experiencing a first acute heart failure hospitalization. Aging Clin Exp Res. août 2018;30(8):927-33. [CrossRef]
- Bannay A, Chaignot C, Blotière PO, Basson M, Weill A, Ricordeau P, et al. The Best Use of the Charlson Comorbidity Index With Electronic Health Care Database to Predict Mortality. Med Care. févr 2016;54(2):188-94. [CrossRef]
- Freund Y, Cachanado M, Delannoy Q, Laribi S, Yordanov Y, Gorlicki J, et al. Effect of an Emergency Department Care Bundle on 30-Day Hospital Discharge and Survival Among Elderly Patients With Acute Heart Failure: The ELISABETH Randomized Clinical Trial. JAMA. 17 nov 2020;324(19):1948-56.
- Teixeira A, Parenica J, Park JJ, Ishihara S, AlHabib KF, Laribi S, et al. Clinical presentation and outcome by age categories in acute heart failure: results from an international observational cohort. Eur J Heart Fail. nov 2015;17(11):1114-23. [CrossRef]
- Russell FM, Ferre R, Ehrman RR, Noble V, Gargani L, Collins SP, et al. What are the minimum requirements to establish proficiency in lung ultrasound training for quantifying B-lines? ESC Heart Fail. oct 2020;7(5):2941-7.
- Mazzola M, Pugliese NR, Zavagli M, De Biase N, Bandini G, Barbarisi G, et al. Diagnostic and Prognostic Value of Lung Ultrasound B-Lines in Acute Heart Failure With Concomitant Pneumonia. Front Cardiovasc Med. 2021;8:693912. [CrossRef]
- Yang F, Wang Q, Zhi G, Zhang L, Huang D, Shen D, et al. The application of lung ultrasound in acute decompensated heart failure in heart failure with preserved and reduced ejection fraction. Echocardiography. oct 2017;34(10):1462-9. [CrossRef]
- Palazzuoli A, Ruocco G, Beltrami M, Nuti R, Cleland JG. Combined use of lung ultrasound, B-type natriuretic peptide, and echocardiography for outcome prediction in patients with acute HFrEF and HFpEF. Clin Res Cardiol. juill 2018;107(7):586-96. [CrossRef]
Figure 1.
Flow chart.
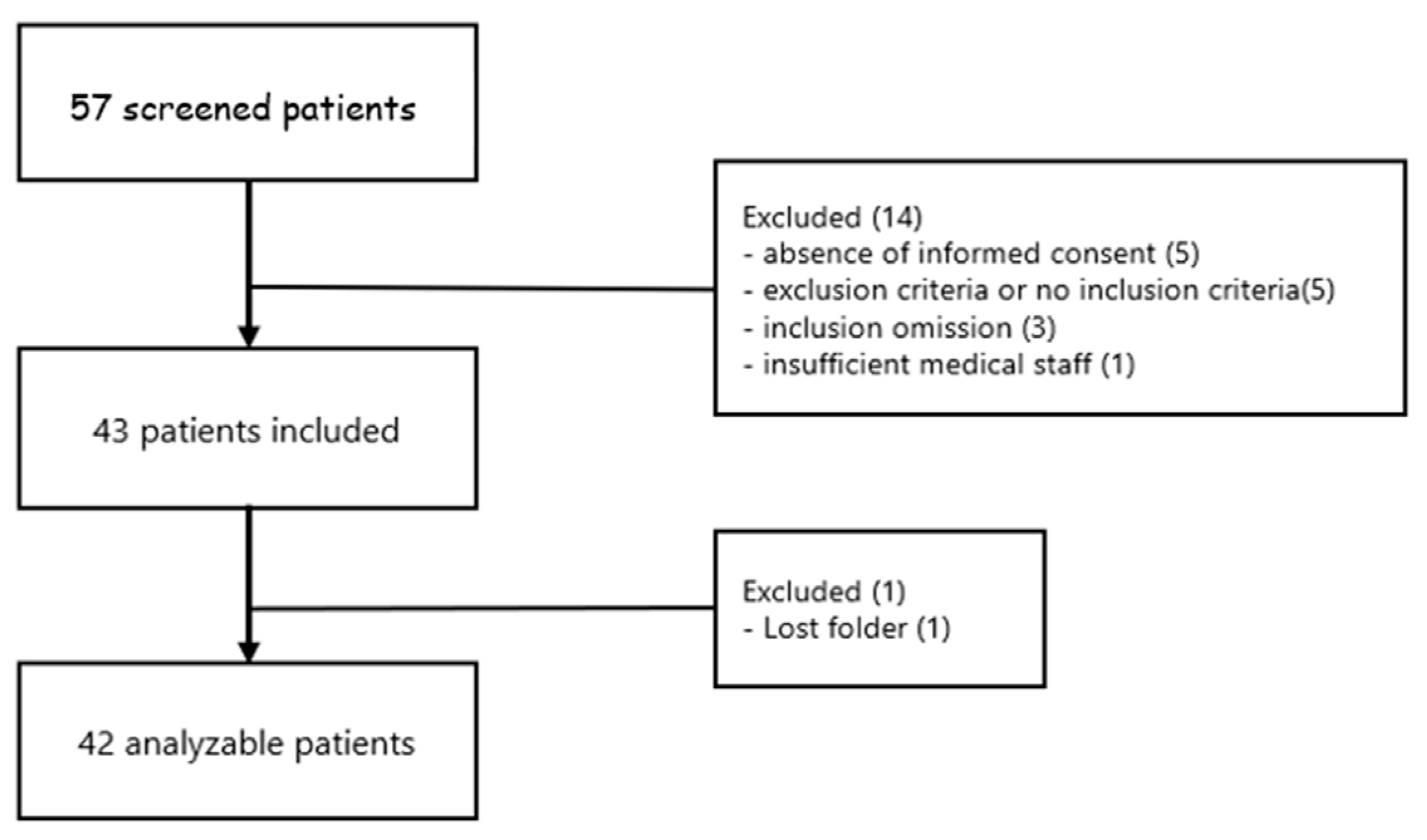
Figure 2.
Evolution of median B-lines and median diuretic posology according to time.
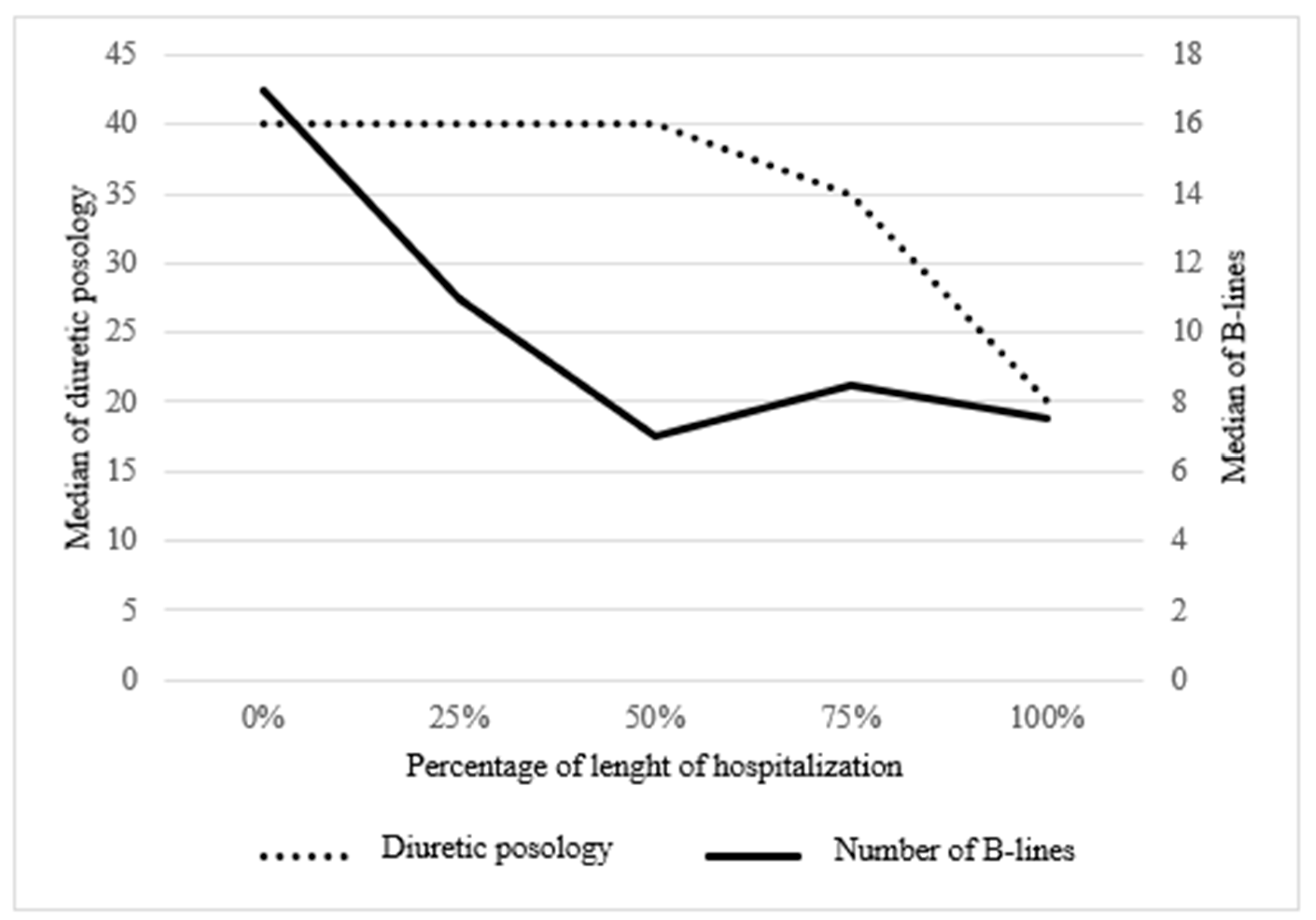
Figure 3.
Evolution of number of B-lines and creatinine levels according to time in patients with a history of CKD. CKD = Chronic kidney disease.
Figure 3.
Evolution of number of B-lines and creatinine levels according to time in patients with a history of CKD. CKD = Chronic kidney disease.
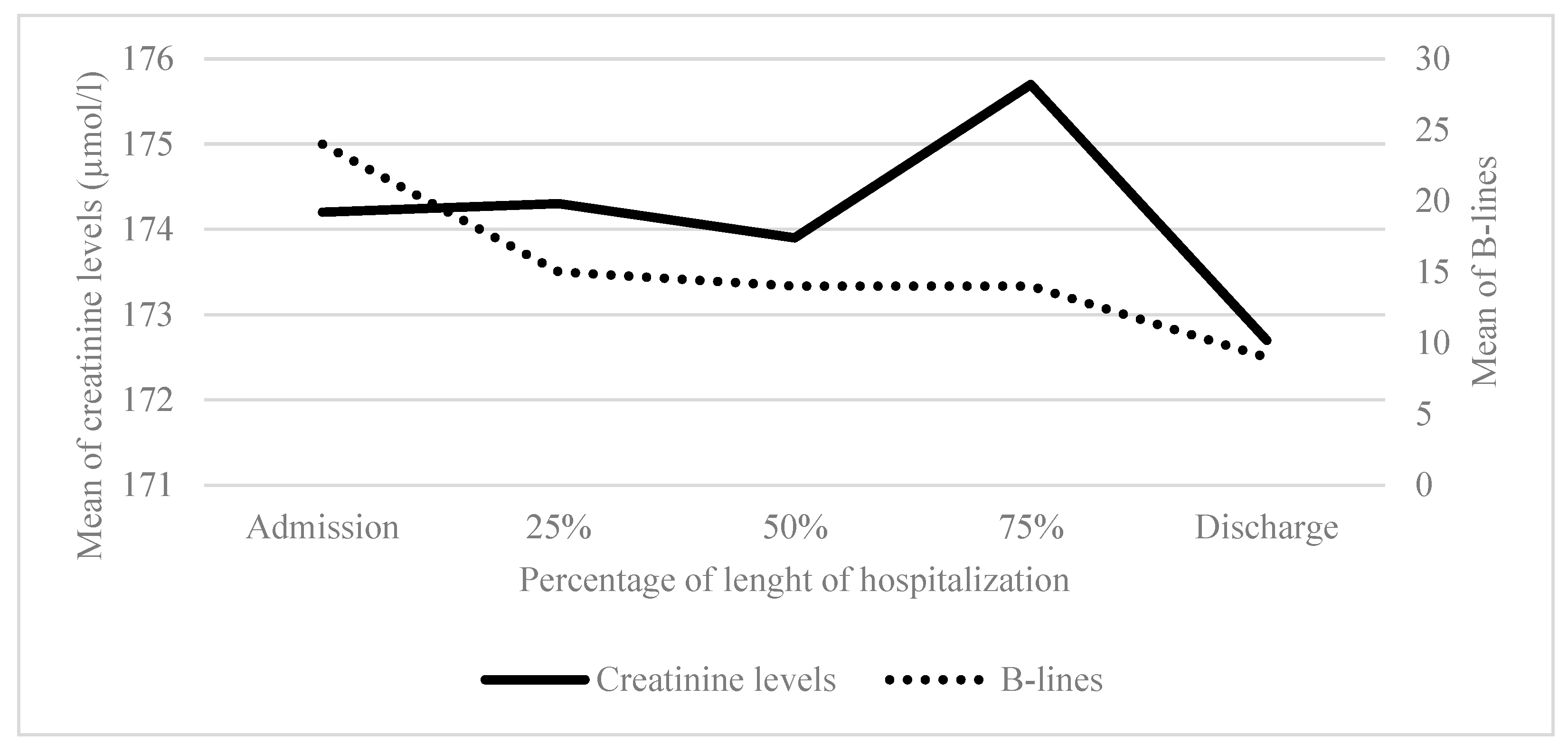
Figure 4.
Evolution of number of B-lines and creatinine levels according to time in patients without a history of CKD. CKD = Chronic kidney disease.
Figure 4.
Evolution of number of B-lines and creatinine levels according to time in patients without a history of CKD. CKD = Chronic kidney disease.
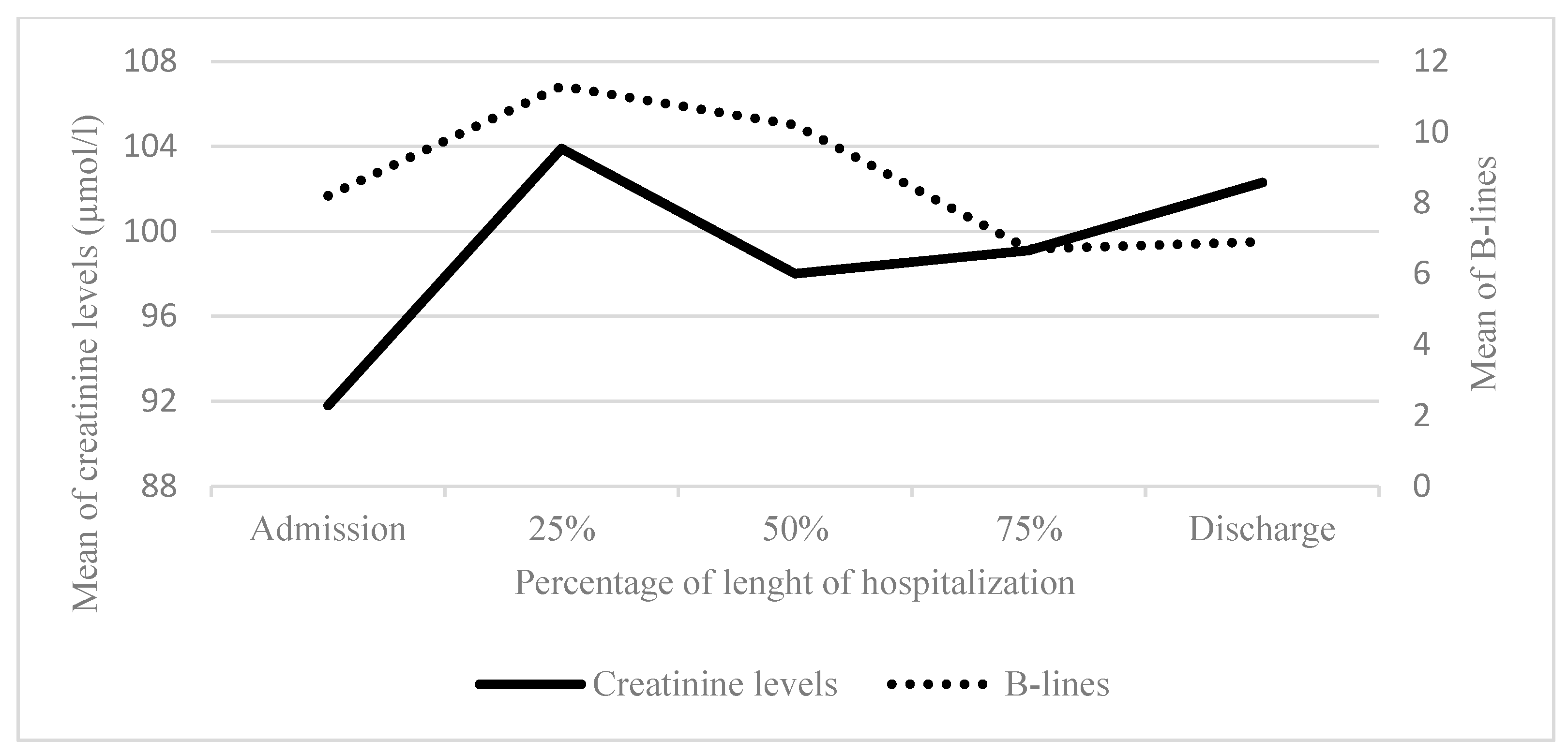
Table 1.
Characteristics of the study population.
| No | Mean (SD) or No. (%) | |
| Baseline characteristics | ||
| Age, years (extremes) | 42 | 85.8 (SD 8.2) (71.7 - 98.8) |
| Male gender | 42 | 26 (61.9%) |
| BMI (kg/m2) | 39 | 26.5 (SD 6.2) |
| Charlson Comorbidity Index | 42 | 8.5 (SD 2.3) |
| Chronic kidney disease | 42 | 22 (52%) |
| Hypertension | 42 | 32 (76%) |
| Diabetes | 42 | 18 (43%) |
| Previous cardiac history | ||
| Know heart disease | 42 | 31 (73.8%) |
| LVEF | 25 | 49.8 (SD 13.5) |
| Daily per os furosemide posology (mg) | 42 | 132.5 (SD 231.5) |
| Triggering factor of AHF | ||
| Unknown | 42 | 8 (19,0%) |
| Anaemia | 42 | 9 (21,4%) |
| Pneumopathy | 42 | 8 (21,4%) |
| Atrial fibrillation | 42 | 5 (11,9%) |
| Other bacterial infections (pyelonephritis, erysipelas) | 42 | 4 (9,5%) |
| Recent decrease in diuretic treatment | 42 | 2 (4,8%) |
| Non-compliance in healthcare | 42 | 2 (4,8%) |
| Pulmonary embolism | 42 | 1 (2,4%) |
| Altitude hypoxemia | 42 | 1 (2,4%) |
| Covid-19 | 42 | 1 (2,4%) |
| Biological and radiography characteristics at admission | ||
| Haemoglobin (g/dL) | 42 | 11.2 ( SD 1.9) |
| Ferritin (ng/ml) | 30 | 167.1 (SD 199.2) |
| Transferrin saturation (%) | 30 | 12.4 (SD 9.1) |
| Creatinine (µmol/L) | 42 | 134.9 (SD 55.0) |
| Urea (mmol/L) | 42 | 14.7 (SD 9.5) |
| Natremia (mmol/L) | 42 | 139.8 (SD 3.8) |
| Kalemia (mmol/L) | 41 | 4.2 (SD 0.7) |
| NT-pro BNP (ng/L) | 41 | 9041 (SD 8770.6) |
| Albumin (g/L) | 35 | 32.1 (SD 5.6) |
| Signs of pulmonary oedema on chest radiography | 36 | 30 (83.3%) |
| During hospitalization | ||
| Length of hospitalization (days) | 42 | 8.0 (5.1) |
| Furosemide posology IV received in ED (mg) | 42 | 122.4 (SD 214.5) |
| Furosemide posology IV/24h on admission (mg) | 42 | 159.2 (SD 256.5) |
| Intra-venous iron supplementation | 42 | 24 (57.1%) |
| Dietetic consultation | 42 | 15 (35,7%) |
| Physiotherapy | 42 | 25 (59,5%) |
| Therapeutic patient education | 42 | 5 (11,9%) |
| At discharge | ||
| Daily per os furosemide posology (mg) | 42 | 153.9 (SD 268.5) |
| Biological check-up at 7 days | 42 | 22 (52,4%) |
| Consultation with attending physician at 7 days | 42 | 18 (42,9%) |
| Consultation with cardiologist at 20 days | 42 | 20 (47,6%) |
BMI = body mass index ; LEVF = left ventricular ejection fraction ; AHF = acute heart failure ; NYHA = New York Heart Association ; BNP = brain natriuretic peptide ; ED = emergency department ; IV = intra venous.
Table 2.
Characteritics evolution of the patients during hospitalization.
| Admission (0%) | 25% | 50% | 75% | Discharge (100%) | ||
|---|---|---|---|---|---|---|
|
Weight loss Mean (SD) [count] |
- | -0,8 (-0,4) [24] | -1,7 (-0,8) [22] | -1,6 (-1,2) [21] | -2,7 (-1,6) [20] | |
|
Dyspnoea (self-evaluation) Mean (SD) [count] |
5.1 (3.2) [34] | 3.3 (2.9) [25] | 2.1 (2.5) [26] | 1.8 (2.3) [25] | 1.7 (2.2) [28] | |
|
NHYA Mean (SD) [count] |
3.1 (1.0) [35] | 2.3 (1.0) [27] | 2.2 (1.0) [27] | 2.1 (0.9) [23] | 2.2 (0.9) [27] | |
|
Orthopnoea % of total [count] |
Yes | 36.6% [15] | 14.7% [5] | 9.7% [3] | 7.4% [2] | 2.6% [1] |
| No | 63.4% [26] | 85.3% [29] | 90.3% [28] | 92.6% [25] | 97.4% [37] | |
|
Asthenia (self-evaluation) Mean (SD) [count] |
5.6 (3.0) [31] | 4.4 (2.7) [23] | 3.9 (3.0) [20] | 3.3 (3.2) [18] | 3.2 (2.6) [21] | |
|
Crackles % of total [count] |
No | 24.4% [10] | 32.3% [10] | 35.5% [11] | 30.0% [9] | 44.7% [17] |
| Base | 26.8% [11] | 38.7% [12] | 48.4% [15] | 53.3% [16] | 31.6% [12] | |
| 1/4 lung | 12.2% [5] | 6.5% [2] | 6.5% [2] | 10.0% [3] | 21.1% [8] | |
| 1/2 lung | 29.3% [12] | 22.6% [7] | 9.7% [3] | 6.7% [2] | 2.6% [1] | |
| 3/4 lung | 7.3% [3] | 0.0% [0] | 0.0% [0] | 0.0% [0] | 0.0% [0] | |
|
VM abolition % of total [count] |
No | 61.0% [25] | 75.0% [24] | 63.3% [19] | 63.3% [19] | 84.2% [32] |
| Base | 22.0% [9] | 9.4% [3] | 23.3% [7] | 26.7% [8] | 10.5% [4] | |
| 1/4 lung | 4.9% [2] | 6.2% [2] | 3.3% [1] | 3.3% [1] | 5.3% [2] | |
| 1/2 lung | 7.3% [3] | 6.2% [2] | 6.7% [2] | 6.7% [2] | 0.0% [0] | |
| 3/4 lung | 2.4% [1] | 3.1% [1] | 3.3% [1] | 0.0% [0] | 0.0% [0] | |
| All lung | 2.4% [1] | 0.0% [0] | 0.0% [0] | 0.0% [0] | 0.0% [0] | |
|
Lower limbs oedema % of total [count] |
No | 33.3% [14] | 50.0% [16] | 14 (46.7%) | 48.3% [14] | 56.8% [21] |
| Ankle | 28.6% [12] | 21.9% [7] | 12 (40.0%) | 44.8% [13] | 45.1% [13] | |
| Knee | 28.6% [12] | 25.0% [8] | 3 (10.0%) | 6.9% [2] | 5.4% [2] | |
| Thigh | 9.5% [4] | 3.1% [1] | 1 (3.3%) | 0.0% [0] | 2.7% [1] | |
|
Creatinine (µmol/l) Mean (SD) [count] |
133.7 (55.1) [42] | 139.1 (51.8) [30] | 139.8 (54.0) [26] | 144.1 (58.5) [21] | 142.8 (57.5) [30] | |
|
Furosemide posology (IV, mg) Mean (SD) [count] |
162.1 (SD 259.0) [42] | 147.4 (224.7) [35] | 124.0 (220.2) [36] | 80.5 (137.4) [34] | 77.0 (134.2) [42] | |
|
Pleural effusion % of total [count] |
Yes | 61.5% [8] | 60.0% [15] | 48.0% [12] | 46.2% [12] | 35.7% [10] |
| No | 38.5% [5] | 40.0% [10] | 52.0% [13] | 53.8% [14] | 64.3% [18] | |
|
B-lines left Mean (SD) [count] |
9.1 (7.5) [13] | 6.8 (5.1) [25] | 5.6 (5.1) [25] | 4.8 (4.1) [26] | 4.5 (3.5) [28] | |
|
B-lines right Mean (SD) [count] |
9.8 (7.1) [13] | 8.2 (6.9) [25] | 6.3 (4.8) [25] | 6.0 (4.2) [26] | 3.9 (4.0) [28] | |
|
Total B-lines Mean (SD) [count] |
18.1 (13.0) [13] | 13.4 (10.2) [25] | 11.9 (9.4) [25] | 10.8 (7.8) [26] | 8.4 (6.8) [28] | |
NYHA = New York Heart Association ; VM = vesicular murmur ; IV = intra venous.
Table 3.
Evolution of number of B-lines according to crackeles.
| Hospitalization time | Intensity of clinic sign | No. | B-lines mean (SD) [count] | p value1 |
|---|---|---|---|---|
| Admission (0%) | Absent | 13 | 14.7 (9.1) [3] | 0.295 |
| Moderate a | 12.8 (14.4) [5] | |||
| Severe b | 25.4 (12.3) [5] | |||
| 25% | Absent | 31 | 10.3 (11.4) [10] | 0.824 |
| Moderate a | 8.7 (9.9) [14] | |||
| Severe b | 11.7 (11.1) [7] | |||
| 50% | Absent | 31 | 9.8 (11.8) [11] | 0.539 |
| Moderate a | 9.1 (8.3) [17] | |||
| Severe b | 3.0 (3.6) [3] | |||
| 75% | Absent | 30 | 12.8 (9.4) [9] | 0.223 |
| Moderate a | 7.4 (7.9) [19] | |||
| Severe b | 4.5 (6.4) [2] | |||
| At discharge (100%) | Absent | 39 | 6.6 (7.1) [17] | 0.055 |
| Moderate a | 3.9 (6.4) [21] | |||
| Severe b | 20.0 (NA) [1] |
a Crackles in bases and 1/4 lung b Crackles in 1/2 , 3/4 and all lung. 1 Linear Model ANOVA.
Table 4.
Correlation between crackles intensity and the number of B-lines at discharge.
| At discharge | No crackles | Bases crackles | ¼ lung crackles | ½ lung crackles | ¾ lung crackles | All lung crackles | p-value1 |
|---|---|---|---|---|---|---|---|
|
B lines Mean (SD) [count] |
6.6 (7.1) [17] | 4.1 (7.2) [13] | 3.6 (5.4) [8] | 20.0 (NA) [1] | 0.0 (NA) [0] | 0.0 (NA) [0] | 0.124 |
1 Linear Model ANOVA.
Table 5.
B-lines evolution according to creatinine measurement.
| Hospitalization time | CDK history | No. | Creatinine in µmol/l mean (SD) [count] | B-lines mean (SD) [count] | p value1 |
|---|---|---|---|---|---|
| Admission (0%) | Yes | 22 | 174.2 (43.1) [22] | 24.2 (11.6) [8] | 0.023 |
| No | 20 | 91.8 (26.9) [20] | 8.2 (8.8) [5] | ||
| 25% | Yes | 22 | 174.3 (43.8) [15] | 14.6 (9.4) [16] | 0.450 |
| No | 20 | 103.9 (31.4) [15] | 11.3 (11.7) [9] | ||
| 50% | Yes | 22 | 170.5 (49.8) [15] | 13.7 (10.2)[12] | 0.373 |
| No | 20 | 98.0 (21.7) [11] | 10.2 (8.7) [13] | ||
| 75% | Yes | 22 | 171.8 (56.6) [13] | 14.4 (8.5) [14] | 0.008 |
| No | 20 | 99.1 (23.3) [8] | 6.7 (3.9) [12] | ||
| At discharge (100%) | Yes | 22 | 169.8 (57) [18] | 9.2 (7.5) [18] | 0.406 |
| No | 20 | 102.3 (26.9) [12] | 6.9 (5.2) [10] |
1 Linear Model ANOVA.
Table 6.
B-lines at discharge according to vital and hospital status 30-days after discharge.
| At 30-days after discharge | B-lines mean (SD) [count] at discharge | p-value1 | |
|---|---|---|---|
| Vital status | Death (all causes) | 15.2 (10.1) [5] | <0.001 |
| Alive | 3.9 (5.4) [37] | ||
| Hospital status for AHF | Readmission | 4.9 (5.4) [8] | 0.469 |
| No readmission | 4.1 (5.7) [30] | ||
1 Linear Model ANOVA.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



