Submitted:
14 December 2024
Posted:
16 December 2024
You are already at the latest version
Abstract
Dengue fever, caused by the dengue virus (DENV), presents a significant global health challenge, especially in tropical and subtropical regions. The exponential increase in native DENV cases in Europe is concerning, indicating a significant rise in incidence. As climate change intensifies, it is crucial to implement proactive measures to address the presence of Aedes albopictus (Asian tiger mosquito) in Europe to prevent dengue and other tropical diseases from becoming endemic in temperate regions. In 2024, Brazil experienced a dramatic surge in dengue cases, reporting an incidence rate four times higher than that of 2023, accompanied by a notable rise in mortality. This alarming trend underscores the urgent need for heightened surveillance and preventive measures, as it may signal the potential for new dengue outbreaks in non-tropical regions. Herein, we explored various aspects of DENV transmission, clinical manifestations, epidemiological trends, and management strategies. DENV transmission depends on Aedes mosquitoes as vectors and humans as hosts. The Aedes species is easily identified by its distinctive black-and-white striped legs. Factors such as temperature, humidity, and precipitation significantly influence mosquito proliferation, and these factors are increasingly affected by climate change. Additionally, the rise in global travel is facilitating the spread of viruses across borders, particularly arboviruses like DENV. Understanding these dynamics is crucial for effective public health interventions. DENV presents a spectrum of clinical manifestations, ranging from asymptomatic cases to severe conditions such as dengue hemorrhagic fever and dengue shock syndrome, influenced by viral serotype and host factors. We explored various diagnostic approaches that integrate clinical symptoms with serological and molecular testing. In Brazil, prevention strategies including vector control, community engagement, and vaccination programs have been implemented. However, these measures have proven insufficient to avert the outbreak in 2024. Climate change drives the geographical expansion of dengue-endemic areas, with recent outbreaks in Europe highlighting the evolving epidemiological landscape. Vigilant global collaboration is essential to mitigate the impact of dengue and other emerging arboviruses, including West Nile virus, Zika virus, Chikungunya virus, Oropouche virus, and Yellow Fever virus.
Keywords:
Dengue
; outbreak
; vaccines
; pandemic
; epidemiology
Introduction
Dengue is a viral disease transmitted by mosquitoes, which are a type of arthropod, and it is considered a zoonotic disease [1]. Over the past three decades, the incidence of arthropod-borne diseases (arboviruses) has risen significantly, largely due to climate change, population growth and travel, which creates conditions that favor the spread of these viruses [2]. Heatwaves and floods are among the factors responsible for the geographic expansion of mosquitoes, which are vectors of various viruses infectious diseases like Dengue, Chikungunya, Yellow Fever, Rift Valley Fever, West Nile Fever, Japanese Encephalitis, and Zika [2,3]. Additionally, with the worsening of global warming, mosquitoes have been migrating to regions in Africa, Asia, Europe, and Americas [4,5,6]. Arboviruses, which include a diverse range of viruses, follow a transmission cycle involving arthropod vectors and vertebrate hosts [7]. The human-mosquito cycle occurs primarily in urban environments [8]. The transmission of the virus from a human to a mosquito depends on the viral load in the human host. The closer the human is to the peak of the viral phase, the higher the viral load, which increases the likelihood that the mosquito will acquire enough virus during feeding to subsequently transmit it [8]. The primary vectors of the disease are female mosquitoes of the species Aedes aegypti and Aedes albopictus. While most dengue infections are associated with A. aegypti, the geographic range of A. albopictus is rapidly expanding [9].
In addition to mosquitoes, other vectors such as ticks, sandflies, and biting midges also play significant roles in transmitting various arboviruses [10,11]. However, the families of viruses that encompass arboviruses include: Flaviviridae (genus Flavivirus), Bunyaviridae (genera Nairovirus, Orthobunyavirus, Phlebovirus, and Tospovirus), Togaviridae (genus Alphavirus), Rhabdoviridae (genus Vesiculovirus), Orthomyxoviridae (genus Thogotovirus), and Reoviridae (genera Orbivirus and Coltivirus) [12,13]. Among these, the most significant viruses causing diseases in humans and animals belong to the Togaviridae and Flaviviridae families [12,14]. Flaviviruses are a group of enveloped, (+)ssRNA viruses [15,16] that includes Dengue Virus (DENV), Japanese Encephalitis Virus (JEV), West Nile Virus (WNV), Zika Virus (ZIKV), Yellow Fever Virus (YFV), and Tick-Borne Encephalitis Virus (TBEV) [15]. Other virus present in the Americas are Chikungunya Virus (CHIKV) and Mayaro Virus (MAYV) that have (+)ssRNA, which belong to the Alphavirus genus of the Togaviridae family [17,18]. Another virus of concern is the Oropouche Virus (OROV), a segmented (-)ssRNA virus belonging to the genus Orthobunyavirus in the Peribunyaviridae family, which causes symptoms similar to dengue fever [18,19].
Dengue is an endemic disease prevalent in over 100 countries worldwide, particularly in tropical and subtropical regions of Southeast Asia, Africa, the West Pacific, and the Americas [20,21], where temperature and humidity conditions favor the proliferation of mosquito vectors [22,23]. Additionally, cases of the disease have been observed in some regions of Europe and the United States of America [21]. It is widely believed that climate change, population growth, and increased global travel will lead to a rise in dengue incidence, particularly in areas where the disease is already endemic. Moreover, the spread of Aedes vectors, which primarily originate from Asia, is likely to further expand the geographic range of the virus, pushing its borders into new, previously unaffected regions [9,24,25]. In particular, in Brazil, dengue epidemics are intensified by temperature variations and rainy periods. Mosquito populations increase significantly during warm and wet periods, as these conditions provide ideal environments for their proliferation. Most cases of dengue fever occur after humid and hot periods, particularly in urban areas. High temperatures (26 ºC to 29 ºC) significantly influence the spread of dengue by affecting mosquito development rates, reproduction, survival, biting rates, and viral replication within the vector [26].
The DENV has four distinct serotypes, each exhibiting genetic diversity and because each has different interactions with the antibodies in human blood serum [27]. These serotypes are classified into various genotypes based on samples collected from different geographic regions: (1) DENV-1 includes I, II, III, and IV genotypes; (2) DENV-2 is categorized into Asian genotype I, Asian genotype II, Cosmopolitan genotype, American genotype V, and Sylvatic genotype; (3) DENV-3 comprises I, II, III, and IV genotypes; (4) DENV-4 encompasses I, II, III, and IV genotypes [28]. Recently, a fifth serotype, DENV-5, was identified in Malaysia [29,30]. Human infection occurs through the bite of a female mosquito, particularly A. aegypti [31,32] or A. albopictus [33], affecting approximately 390 million people annually. While A. aegypti is commonly associated with most infections. The geographic range of Aedes albopictus continues to expand, driven by its ecological plasticity, which allows it to tolerate colder climates. Its competitive feeding behavior and the lack of effective control strategies further contribute to the increasing number of dengue cases in previously colder regions [8,34,35].
When a person infected with DENV is bitten by an A. aegypti or A. albopictus a complex sequence of events allows the virus to replicate and spread within the mosquito [33,36] (Figure 1). Inside the female mosquito the virus infects the midgut epithelial cells, where it binds to specific receptors and replicates [37]. After replication, the virus exits the midgut and spreads throughout the haemocoel, infecting various secondary tissues, such as the fat body, nervous system, and salivary glands. Infection of the salivary glands is essential for the virus’s transmission to new hosts [38,39,40]. When the mosquito bites another person, DENV is transmitted through the saliva injected during blood feeding, introducing the virus into the new host’s bloodstream and initiating a new cycle of infection [38]. This entire process, from the ingestion of the virus to the mosquito’s ability to transmit it to a new host, typically takes around 8-12 days, depending on environmental factors such as temperature and humidity. Given Brazil’s tropical climate, where dengue is a concern, these environmental factors are especially relevant, as warmer temperatures can shorten the time needed for the virus to become transmissible [36,38]. This period is known as the extrinsic incubation period [22]. Understanding these steps is crucial for developing strategies to interrupt the transmission cycle of DENV and reduce the incidence of dengue worldwide. Vertical transmission from human to human in the case of dengue from mother to child has been reported, although there is no evidence of such transmission in early pregnancy. It can occur in late pregnancy, with studies showing an increased risk of low birth weight and preterm births among infected pregnant women. However, the significance of vertical transmission as a risk factor for adverse pregnancy outcomes remains inconclusive [41], and congenital dengue infection is regarded as rare in the literature [42]. Notably, natural vertical transmission in Aedes aegypti and Aedes albopictus is regarded as a maintenance mechanism for the dengue virus during unfavorable conditions, potentially contributing to the emergence of dengue outbreaks. The detection of DENV-3 during years when no human autochthonous cases of this serotype were recorded suggests the silent circulation of DENV-3, indicating that green areas may sustain serotypes not currently circulating in the human population, possibly through vertical transmission mechanisms [43].
Once inside the human host, the dengue virus infects a range of cells and tissues, such as macrophages, lymphocytes, and endothelial cells, as well as organs like the lymph nodes, lungs, liver, kidneys, stomach, and the central nervous system. These diverse targets contribute to the virus’s systemic impact throughout the body as described in more detail below. [46]. Dengue infection progresses through three phases: the febrile phase, the critical phase, and the recovery phase [47]. The febrile phase lasts about a week, characterized by high fever, severe headache, muscle and joint pain, eye pain, fatigue, nausea, vomiting, loss of appetite, and minor bleeding [48,49]. The critical phase involves more severe symptoms such as plasma leakage and internal hemorrhage [7]. The recovery phase is marked by the gradual reabsorption of fluid from the extravascular compartment, improvement in general well-being, return of appetite, and stabilization of the haemodynamic state [7]. Additionally, neurological complications such as encephalopathy, myelopathy, myositis, and peripheral neuropathy are frequently identified following dengue infection [50].
Herein, we examined dengue fever as an escalating global health challenge, particularly in tropical and subtropical regions. Latin America is a region of critical importance in the global context of dengue transmission, as environmental conditions, rapid urbanization, and socio-economic factors create a highly conducive environment for A. aegypti, the primary mosquito vector. Notably, the surge in cases in Latin America in 2024 is striking, with reported instances more than four times higher than those in 2023 in Brazil. This region’s susceptibility is compounded by climate variability, which intensifies mosquito breeding cycles, and by varying levels of access to healthcare, which hinder effective disease management and control. Our focus on Latin America reflects both the substantial burden of dengue in this region and the urgent need for strengthened and targeted public health interventions to curb transmission and mitigate the severe socio-economic impacts of these outbreaks.
We explored various aspects, including its transmission by Aedes mosquitoes, which is influenced by climate factors such as temperature and precipitation due to climate change. Clinical manifestations of dengue fever vary widely, ranging from asymptomatic cases to severe forms, including dengue hemorrhagic fever and dengue shock syndrome. These variations are influenced by factors such as the viral serotype and the host’s immune response. We emphasized the diagnostic approaches based on clinical symptoms and laboratory tests. Prevention efforts encompass various strategies, including vector control and community engagement initiatives, such as wearing long-sleeved, light-colored clothing and installing mosquito screens on windows. In tropical regions with high humidity, wearing long clothes is challenging due to elevated temperatures. While this consideration is important, there are currently no government recommendations supporting such initiatives in Latin America. Vaccination campaigns also play a crucial role; however, challenges like insecticide resistance remain a significant hurdle. Additionally, we discussed the spread of dengue into new regions, including Europe, underscoring the evolving epidemiological landscape and the urgent need for global collaboration to implement effective mitigation strategies.
The impact of global warming on dengue outbreaks in the Latin America
As global warming becomes more evident with the increasing frequency of climate disasters, one significant impact is the intensification of rainfall [51]. The Brazilian National Institute for Space Research (INPE) reports that in 2024, the southern part of Brazil will experience up to a 30% increase in average annual rainfall compared to the last three decades [52]. This increase in rainfall will lead to more standing water in urban areas, which are the primary habitats for the main vectors of dengue [53]. The proliferation of Aedes mosquitoes is directly related to precipitation, humidity, and high temperatures, with Latin America providing an ideal environment. Global warming leads to higher temperatures in subtropical and temperate areas, which often have high urban population densities, creating ideal conditions for proliferation of mosquitoes. These observations suggest that global warming and climate change are directly influencing the spread of tropical diseases. In developing countries, which are experiencing an increase in natural disasters such as floods, tsunamis, and storms, these events exacerbate the formation of standing water in large urban areas. This, in turn, facilitates the spread of dengue and other mosquito-borne diseases.
The data on dengue cases in Latin America shows significant variation between 2023 and 2024 (Figure 2 and Table 1). Brazil leads with an increase in the number of cases, changing from 3,064,739 in 2023 to 7,253,599 in 2024 (Table 1). These data represent 83.4% of total cases in 2024, a notable increase compared to 66.7% in 2023 (Table 1 and Figure 2). Argentina also experienced a significant increase, going from 146,876 cases in 2023 to 498,091 in 2024, which increased the proportion from ~3 to ~6%. Conversely, Mexico decreased the number of cases from 277,963 to 73,532, from 2023 to 2024, representing a proportion from 6.0 to 0.8 %. Other countries presented a considerable increase in the number of cases such as Paraguay, from 63,216 to 278,827, and Colombia, from 131,784 to 157,097. In contrast, countries such as Nicaragua and Bolivia presented significant reductions in cases (Table 1). These data indicate that dengue continues to be a major public health problem in Latin America. The significant outbreak of DENV cases in Central and South America signals potential for similar outbreaks not only in Latin America but also in colder regions. A study published in 2024 concluded that climate change has facilitated the spatial spread of West Nile Virus (WNV) in Europe. Additionally, warm and wet days contribute to the movement of mosquitoes into higher latitudes and altitudes. In 2024, Italy and France reported 22 locally transmitted dengue cases, and a locally transmitted chikungunya case was detected in France. Therefore, the increasing DENV cases in some countries in Latin America may be just the tip of the iceberg, foreshadowing what could happen in the coming years regarding the spread of arboviruses worldwide.
The observed temperature anomalies in South America have shown a notable upward trend, increasing by approximately 1°C over a span of two years, from 0.75°C in 2022 to 1.75°C in 2024 (Figure 2b). In 2024, Latin America reported the highest incidence of dengue cases, likely driven by increased vector proliferation resulting from warmer temperatures and heightened precipitation. This trend underscores the direct correlation between rising temperatures, humidity, and the frequency of dengue outbreaks. A recent study demonstrated a positive correlation between El Niño events and an increased A. aegypti larval index in São Paulo State, Brazil. The larval index was notably higher when seasonal rainfall exceeded 153.12 mm and temperatures rose above 23.30°C [54]. These findings suggest that the combination of climate change and the El Niño event in 2024 likely amplified mosquito proliferation, potentially contributing to the dengue outbreak in Brazil.
Brazil, in particular, saw an approximate tenfold increase in Oropouche virus (OROV) fever cases from 2023 to 2024, underscoring the role of mosquitoes in the spread of arboviruses under favorable climatic conditions. Dengue-related deaths in Latin America highlight significant regional disparities, with Brazil also experiencing the highest number of deaths from January 1st to May 5th, 2024, with 3,086 cases (Table 2). Argentina, Paraguay, and Peru also reported substantial deaths (343, 100, and 192, respectively), underscoring vulnerabilities in healthcare systems amid expanding outbreaks. Even smaller nations, such as Panama, Uruguay, and Grenada, may reflect underreporting of cases compared to countries with the highest numbers, such as Brazil, Argentina, Paraguay, and Peru (Table 2).

Table 1.
Confirmed and under investigation Dengue cases in Latin American countries (2023 and May of 2024). This table presents the number of dengue reported cases by country in Latin America in the period of 2023 and until May of 2024. These data were obtained from the Pan American Health Organization (PAHO).
Table 1.
Confirmed and under investigation Dengue cases in Latin American countries (2023 and May of 2024). This table presents the number of dengue reported cases by country in Latin America in the period of 2023 and until May of 2024. These data were obtained from the Pan American Health Organization (PAHO).
| Country |
Cases (2023) |
Cases (from January to May 2024) |
|---|---|---|
| Brazil | 3,064,739 | 7,253,599 |
| Argentina | 146,876 | 498,091 |
| Mexico | 277,963 | 73,532 |
| Paraguay | 63,216 | 278,827 |
| Nicaragua | 181,096 | 17,339 |
| Peru | 274,227 | 242,742 |
| Colombia | 131,784 | 157,097 |
| Bolivia | 158,744 | 36,747 |
| Ecuador | 27,838 | 27,063 |
| Guatemala | 72,358 | 21,991 |
| Chile | ND | 148 |
| Uruguay | 48 | 701 |
| Venezuela | 4,809 | ND |
| French Guiana | 2,684 | 14,084 |
| Guyana | 27,438 | 12,929 |
| Suriname | 282 | 95 |
| Nicaragua | 181,096 | 17,339 |
| Costa Rica | 30,649 | 8,851 |
| Panama | 20,924 | 6,774 |
| Cuba | ND | ND |
| Honduras | 34,050 | 20,563 |
| El Salvador | 5,788 | 2,056 |
| ND, not disclosed. | ||
Figure 2.
Distribution of confirmed and under investigation dengue fever cases in Latin America (2023-2024) and average temperature (2022-2024). a) The cases of dengue in Latin America exhibited significant regional variation between 2023 and from January to May 2024, with marked increases in several countries. Brazil presented a largest proportion of cases, with a notable escalation from 3,064,739 cases in 2023 to 7,253,599 cases until May of 2024. Similarly, Argentina reported an increase of dengue cases from 146,876 in 2023 to 498,091 in 2024, while Paraguay experienced an increase from 63,216 to 278,827. Nicaragua showed substantial decrease in case numbers. This figure was performed using data obtained from Pan American Health Organization (PAHO). Graph colored based on the dengue fever cases shown in Table 1. b) Temperature anomalies in South America in the period of 2022-2024.
Figure 2.
Distribution of confirmed and under investigation dengue fever cases in Latin America (2023-2024) and average temperature (2022-2024). a) The cases of dengue in Latin America exhibited significant regional variation between 2023 and from January to May 2024, with marked increases in several countries. Brazil presented a largest proportion of cases, with a notable escalation from 3,064,739 cases in 2023 to 7,253,599 cases until May of 2024. Similarly, Argentina reported an increase of dengue cases from 146,876 in 2023 to 498,091 in 2024, while Paraguay experienced an increase from 63,216 to 278,827. Nicaragua showed substantial decrease in case numbers. This figure was performed using data obtained from Pan American Health Organization (PAHO). Graph colored based on the dengue fever cases shown in Table 1. b) Temperature anomalies in South America in the period of 2022-2024.
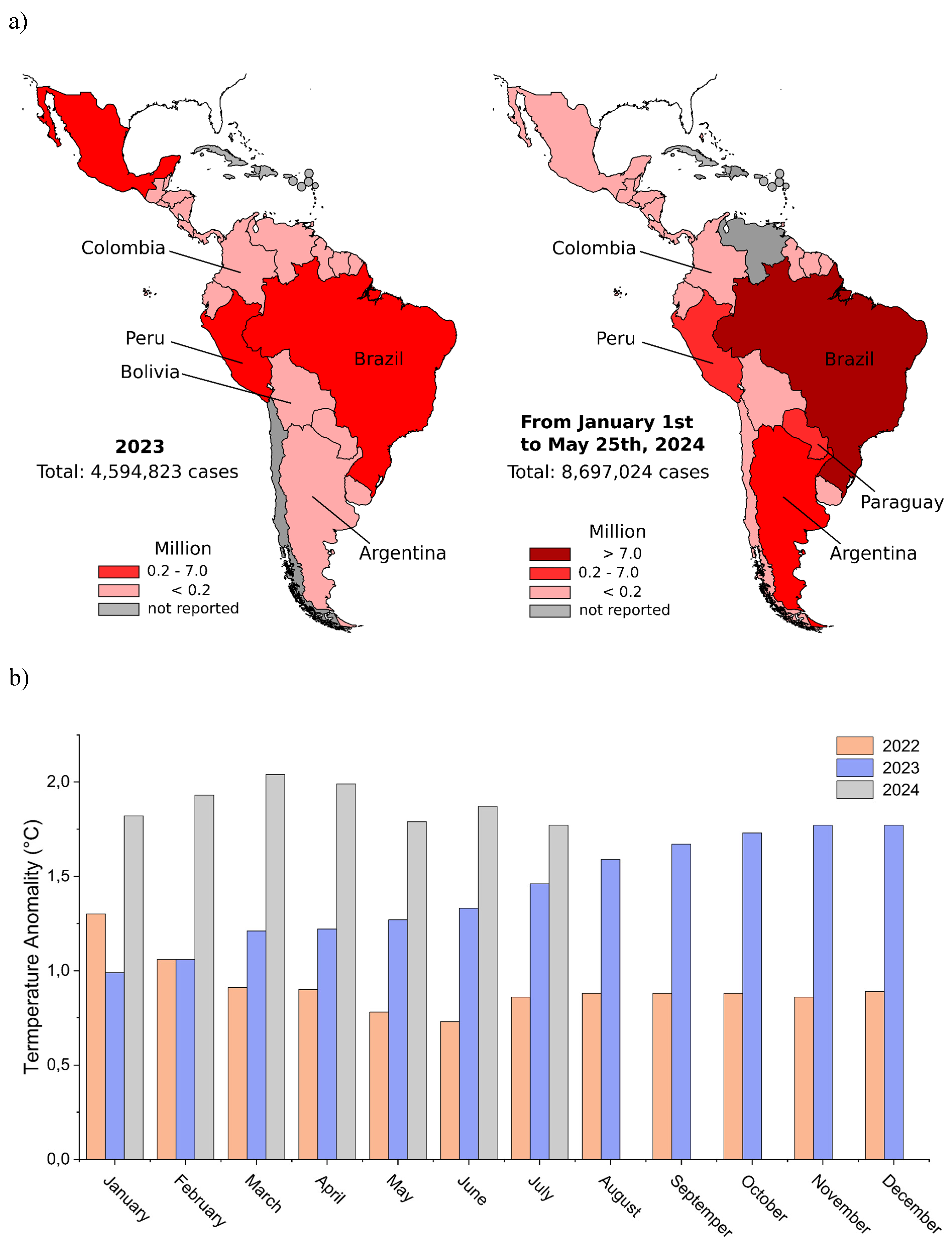
Table 2.
Dengue-related deaths by country in Latin America from January to May 2024. This table presents the number of dengue-related deaths in various Latin American countries from January to May 2024.
Table 2.
Dengue-related deaths by country in Latin America from January to May 2024. This table presents the number of dengue-related deaths in various Latin American countries from January to May 2024.
| Country | Deaths caused by Dengue from January to May 2024 |
Rate of death (death/cases) (%) |
|---|---|---|
| Brazil | 3086 | 0.04 |
| Argentina | 343 | 0.07 |
| Paraguay | 100 | 0.04 |
| Nicaragua | ND | ND |
| Peru | 192 | 0.08 |
| Colombia | 70 | 0.05 |
| Mexico | 26 | 0.04 |
| Bolivia | 14 | 0.04 |
| Ecuador | 31 | 0.12 |
| Guatemala | 10 | 0.05 |
| Chile | ND | ND |
| Honduras | 10 | 0.05 |
| El Salvador | ND | ND |
| Guyana | 2 | 0.02 |
| Panama | 12 | 0.18 |
| Uruguay | 2 | 0.29 |
| Venezuela | ND | ND |
| French Guiana | ND | ND |
| Suriname | 3 | 3.16 |
| Costa Rica | ND | ND |
| Cuba | ND | ND |
ND, not disclosed.
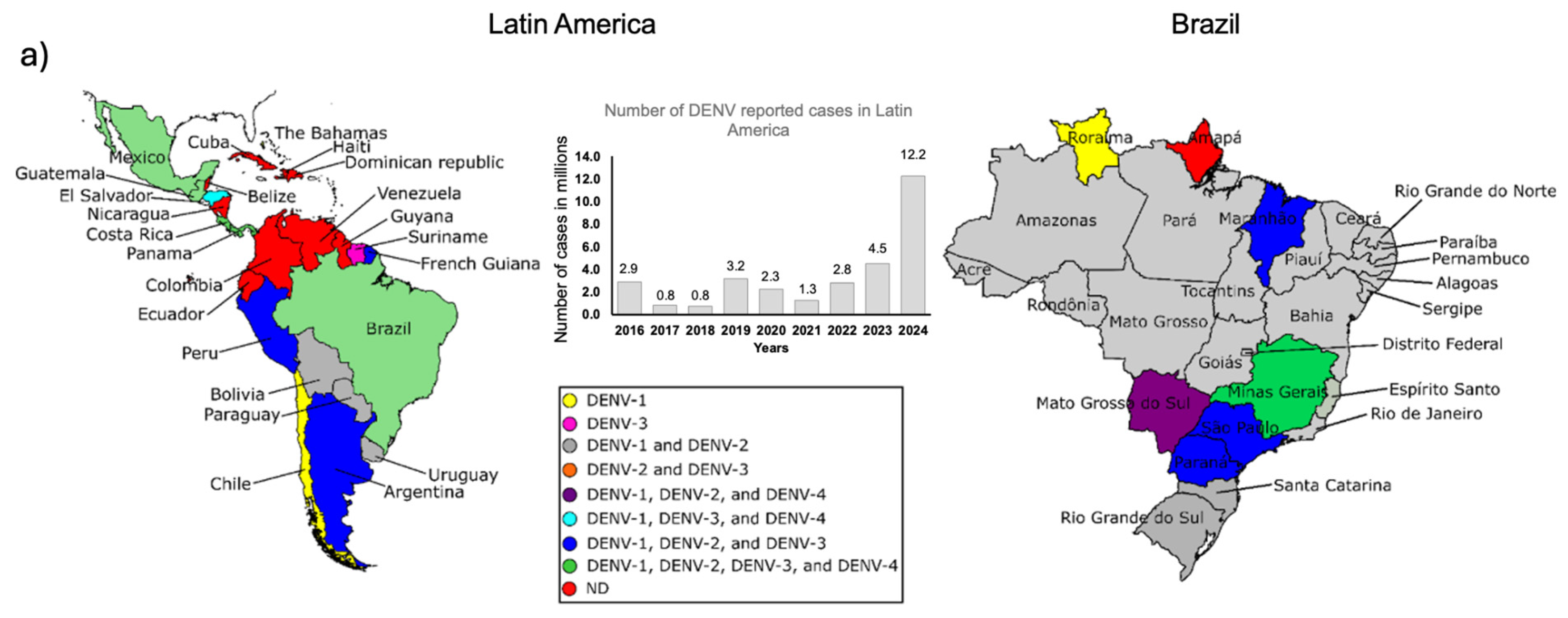
In 2023 and 2024, the distribution of DENV serotypes in Latin America varied significantly among countries [55] (Figure 3a). In 2023, most countries, including Antigua and Barbuda, Argentina, Barbados, and Brazil, reported the circulation of DENV-1, DENV-2, and DENV-3, with DENV-4 being less common. By 2024, there was an increase in the diversity of serotypes in many countries, with Brazil, Costa Rica, Guatemala, and El Salvador maintaining the presence of all four serotypes. Argentina and Mexico also reported all four serotypes but Guyana and Trinidad and Tobago exhibited sporadic presence of some serotypes. Saint Barthelemy and Saint Vincent and the Grenadines reported only one serotype, predominantly DENV1. The data highlights a notable increase in serotype diversity in many Latin America countries in 2024 compared to 2023 [55]. Since 2021, dengue cases in Latin America have shown an exponential increase, with 2024 reporting 2.7 times more cases than the previous year (Figure 3a).
Dengue is a notifiable disease in Brazil, meaning that all suspected and/or confirmed cases must be reported to the Epidemiological Surveillance Service of the Municipal Health Department (SMS). Suspected dengue cases can be confirmed through either laboratory criteria or clinical-epidemiological linkage. Patient history, clinical symptoms, and additional medical record information support epidemiological surveillance in the investigation and closure of cases within the official reporting system. Laboratory confirmation is based on serological tests (IgG and/or IGM), detection of NS1 antigen and RT-PCR (Reverse Transcription Polymerase Chain Reaction). The criteria applied are as follows: detection of reactive NS1 protein, positive viral isolation, detectable RT-PCR (within five days of symptom onset), IgM detection by ELISA (from the sixth day onwards), and a ≥4-fold increase in antibody titers in PRNT (Plaque reduction neutralization tests) with paired samples (acute and convalescent phases, with at least a 14-day interval). Due to cross-reactivity between the dengue and Zika viruses, serological tests may yield inconclusive results. When laboratory confirmation is not feasible or results are inconclusive, epidemiological linkage to a confirmed case, supported by spatial distribution analysis, should be used for diagnosis [56].
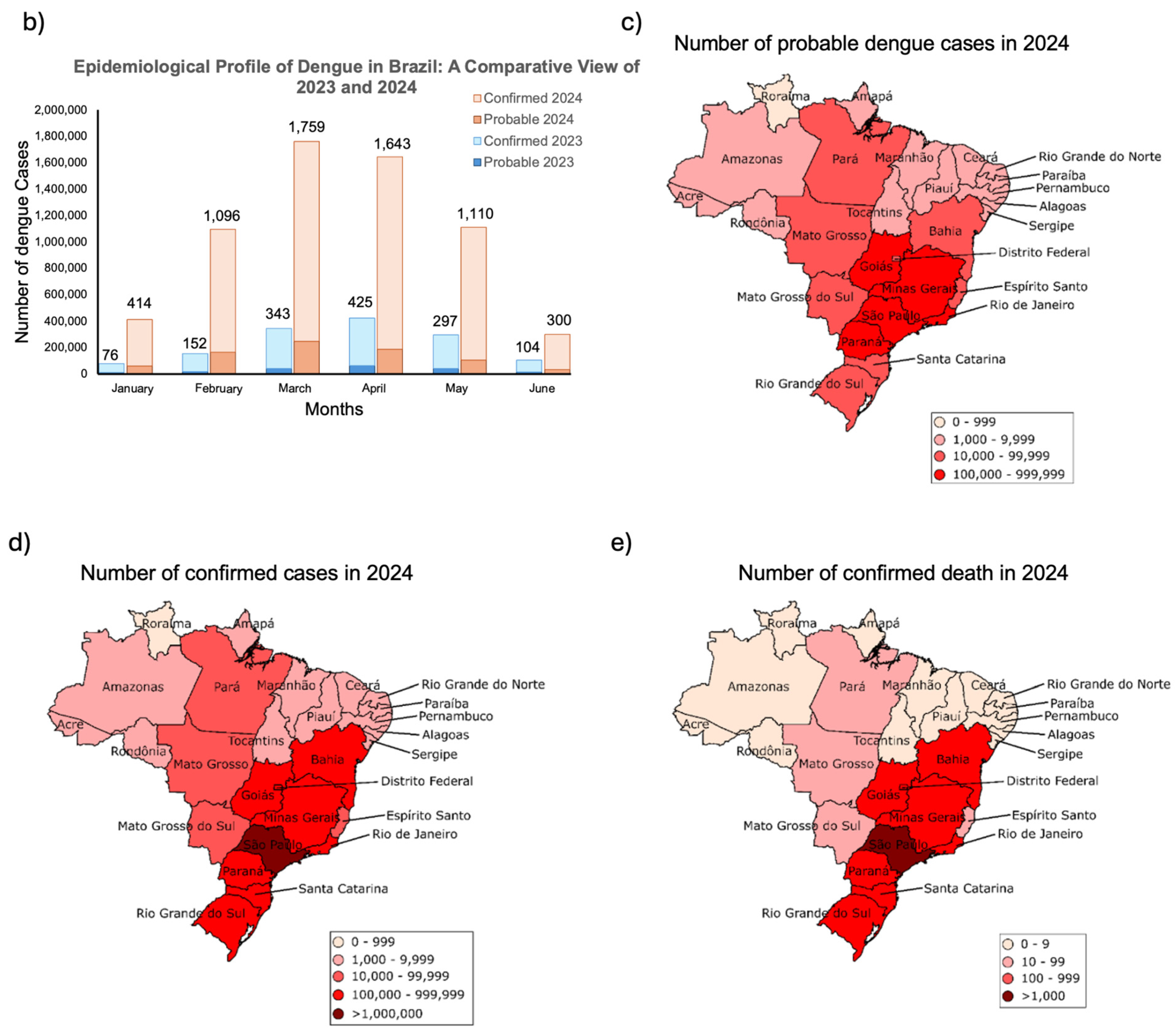
In March of 2024 the number of probable and confirmed cases of DENV in Brazil was five times higher than 2023, with higher cases and deaths in the southeast and south regions (Figure 3 b-e). The cases of DENV may be underestimated due to economic factors and limited diagnostic tests, especially in the north and northeast regions of Brazil. In 2023, Brazil recorded 1.4 million confirmed dengue cases, with an additional 240,462 cases under investigation and 1,179 deaths. [57]. The fatality rate for dengue cases under investigation is 0.07 %, while for severe dengue cases, it rises to 4.8 % [57]. Until September 26, 2024, Brazil had reported a total of ~5.5 million confirmed dengue cases and 5,428 deaths [57]. Additionally, ~1.0 million dengue cases and over 1,200 deaths are still under investigation [57]. The fatality rate for dengue cases under investigation is 0.1%, while for severe dengue cases, it rises to 5.5% [57]. The dengue outbreak in Brazil in 2024 occurred between February and May, with more than 300,000 cases under investigation each week. This period corresponds to the late summer and early autumn. The unprecedented rise in dengue cases in Brazil in 2024 is likely due to multiple factors, including conditions that favored mosquito proliferation and an extended period of warm, humid weather. With the onset of autumn and winter, we expect a decrease in dengue cases in Brazil, as the cooler temperatures are less favorable to mosquito reproduction. However, continued vigilance and preventive measures remain crucial to controlling the spread of dengue.
Figure 3.
Geographic distribution of serotypes and dengue cases in different regions of the Americas and Brazil, 2024. a) Distribution of the serotypes by country in Latin America from 2016 to November 2024 [57,58]. Latin America comprises 20 countries: Argentina, Bolivia, Brazil, Chile, Colombia, Costa Rica, Cuba, Ecuador, El Salvador, Guatemala, Haiti, Honduras, Mexico, Nicaragua, Panama, Paraguay, Peru, the Dominican Republic, Uruguay, and Venezuela. Twenty-five countries and territories reported the circulation of dengue serotypes in the Americas. Brazil, Costa Rica, Guatemala, Honduras, Mexico, and Panama reported the simultaneous circulation of DENV-1, DENV-2, DENV-3, and DENV-4 [59,60]. In Brazil, Minas Gerais state reported the simultaneous circulation of DENV-1, DENV-2, DENV-3, and DENV-4 [61]. ND = Not divulged. b) Number of probable (under investigation) and confirmed dengue cases in Brazil from January to June 2023 (blue) and 2024 (orange). Values above each column represent the combined total of cases in thousands [57]. The maps display the number of probable (panel c) and confirmed (panel d) dengue cases across Brazilian states in 2024 [57]. e) Number of deaths caused by dengue in Brazil in 2024. Confirmed DENV cases in Brazil are determined through laboratory testing and clinical-epidemiological criteria. In 2024, 37% of cases were confirmed via laboratory tests, while 63% were based on clinical-epidemiological assessment. The number of confirmed deaths was determined based on laboratory and/or clinical-epidemiological criteria. The number of dengue cases under investigation refers to those that have been officially reported.
Figure 3.
Geographic distribution of serotypes and dengue cases in different regions of the Americas and Brazil, 2024. a) Distribution of the serotypes by country in Latin America from 2016 to November 2024 [57,58]. Latin America comprises 20 countries: Argentina, Bolivia, Brazil, Chile, Colombia, Costa Rica, Cuba, Ecuador, El Salvador, Guatemala, Haiti, Honduras, Mexico, Nicaragua, Panama, Paraguay, Peru, the Dominican Republic, Uruguay, and Venezuela. Twenty-five countries and territories reported the circulation of dengue serotypes in the Americas. Brazil, Costa Rica, Guatemala, Honduras, Mexico, and Panama reported the simultaneous circulation of DENV-1, DENV-2, DENV-3, and DENV-4 [59,60]. In Brazil, Minas Gerais state reported the simultaneous circulation of DENV-1, DENV-2, DENV-3, and DENV-4 [61]. ND = Not divulged. b) Number of probable (under investigation) and confirmed dengue cases in Brazil from January to June 2023 (blue) and 2024 (orange). Values above each column represent the combined total of cases in thousands [57]. The maps display the number of probable (panel c) and confirmed (panel d) dengue cases across Brazilian states in 2024 [57]. e) Number of deaths caused by dengue in Brazil in 2024. Confirmed DENV cases in Brazil are determined through laboratory testing and clinical-epidemiological criteria. In 2024, 37% of cases were confirmed via laboratory tests, while 63% were based on clinical-epidemiological assessment. The number of confirmed deaths was determined based on laboratory and/or clinical-epidemiological criteria. The number of dengue cases under investigation refers to those that have been officially reported.
Dengue symptoms and determinants for recurrence and disease severity
Patients infected with dengue are asymptomatic or exhibit a range of symptoms from mild to severe, which can sometimes progress to fatal outcomes [62,63]. Dengue is considered an acute, systemic, dynamic, debilitating, and self-limiting febrile illness. While most patients recover, some can progress to severe forms and even death. Nearly all dengue-related deaths are preventable, often depending on the quality of healthcare provided [64]. Anyone presenting with a sudden onset of fever (39°C to 40°C) accompanied by at least two of the following symptoms such as strong headache, prostration, muscle and/or joint pain, and pain behind the eyes, should seek medical attention immediately to receive timely treatment [64]. However, vigilance is necessary after the febrile period. As the fever subsides (between the 3rd and 7th day of illness), warning signs may appear, indicating a potential deterioration of the patient’s condition. These signs, which suggest plasma leakage from blood vessels and/or hemorrhaging, that may include severe and continuous abdominal pain, persistent vomiting, fluid accumulation in body cavities (ascites, pleural effusion, pericardial effusion), postural hypotension and/or fainting, lethargy and/or irritability, enlarged liver (hepatomegaly) > 2 cm, mucosal bleeding and progressive increase in hematocrit [64]. After the critical phase of dengue, the patient enters the recovery phase. However, the disease can still progress to severe forms, characterized by significant plasma leakage, severe hemorrhages, or severe organ impairment, potentially leading to death [64]. Dengue in children can begin with severe abdominal pain, accompanied by diarrhea and vomiting, before progressing to the classic symptoms of dengue. The warning signs of dengue in infants and children may not be as evident, increasing the risk of severe illness. All age groups are equally susceptible to dengue. However, individuals with preexisting conditions, pregnant women, infants, young children (up to 2 years old), and people over 65 years old are at higher risk of developing complications [64]. Even in mild cases of dengue, patients often experience severe weakness, which affects their daily activities and, consequently, their work performance, leading to a financial impact on society. In some cases, dengue-infected patients, in addition to reporting nausea and loss of appetite, also experience changes in taste, such as a metallic flavour in the mouth [65].
Although the clinical manifestations of dengue are similar across age groups with symptoms such as fever and headache, a Brazilian study found notable age-related differences in symptom prevalence. Specifically, only 69% of children aged 6–10 and 56% of those aged 1–5 reported experiencing myalgia, compared to over 80% of individuals aged 11 and above. Similarly, arthralgia was observed more frequently in older individuals than in children under 10 years [66]. Interestingly, children under 10 years have an increased risk of hospitalization [67]; however, mortality rates are significantly higher in patients aged 15 years and older, particularly among those over 80 years of age [68].
Common symptoms for all dengue serotypes include abdominal pain, drowsiness, and sometimes bleeding mucous membranes (Figure 4) [69]. However, the presence and severity of other symptoms may vary depending on the serotype involved in the infection. While the majority of primary DENV infections are asymptomatic, they contribute to the force of infection, transmission, and overall epidemiological burden [70,71]. An analysis of symptomatic versus asymptomatic and severe versus non-severe outcomes in Nicaragua from 2004 to 2022 revealed that DENV-3 was significantly more likely to cause symptomatic and severe infections compared to other serotypes. Symptomatic infections were recorded in 23.2% of DENV-1, 20.1% of DENV-2, and 36.1% of DENV-3 cases. Among primary infections, severe disease was observed in 2.5% of DENV-1, 1.4% of DENV-2, and 7.4% of DENV-3 cases. These findings underscore the variability in clinical outcomes associated with different dengue virus serotypes [72]. Between 2009 and 2013 in Vitória, Brazil, 485 dengue cases were analysed: DENV-1 caused 77.3% of cases, DENV-4 16.1%, DENV-2 6.4%, and DENV-3 only 0.2%. Among all cases, 6.6% developed into severe dengue, with DENV-2 showing a significantly higher association with severe outcomes [73]. This trend could relate to DENV-2’s relatively high prevalence compared to DENV-3 in this study. Thus, the relationship between DENV serotype and disease severity is complex and influenced by multiple factors such as age, genetic variability, and alterations in the patient’s immune response are significant indicators of potential disease severity [74]. Studies have demonstrated that elderly patients often require longer hospital stays and have a higher likelihood of developing severe dengue due to preexisting comorbidities and infections with specific serotypes [75,76]. Adults are at increased risk of developing dengue hemorrhagic fever, while children and teenagers are particularly susceptible to severe plasma leakage and shock [77]. These severe manifestations are associated to the elevated expression of chemokines and pro-inflammatory cytokines such as CCL-2, CCL-5, TNF-α, IFN-γ, and IL-6, which act on endothelial cells to promote plasma extravasation and the escape of pro-inflammatory factors [74,78].
Another critical aspect is that secondary dengue infections are generally more severe than primary infections. This increased severity is believed to occur because a primary infection induces permanent immunity against the initial serotype and short-term immunological memory to other serotypes. During a secondary infection by a different serotype, pre-existing antibodies form complexes with the virus that are then captured by receptors on immune cells, leading to internalization and replication of the virus within host cells [62,79]. Recent studies have also indicated that a primary infection with Zika virus followed by a subsequent dengue virus infection poses a significant risk for developing severe dengue fever, comparable to the severity observed in heterologous primary and secondary dengue infections [80].
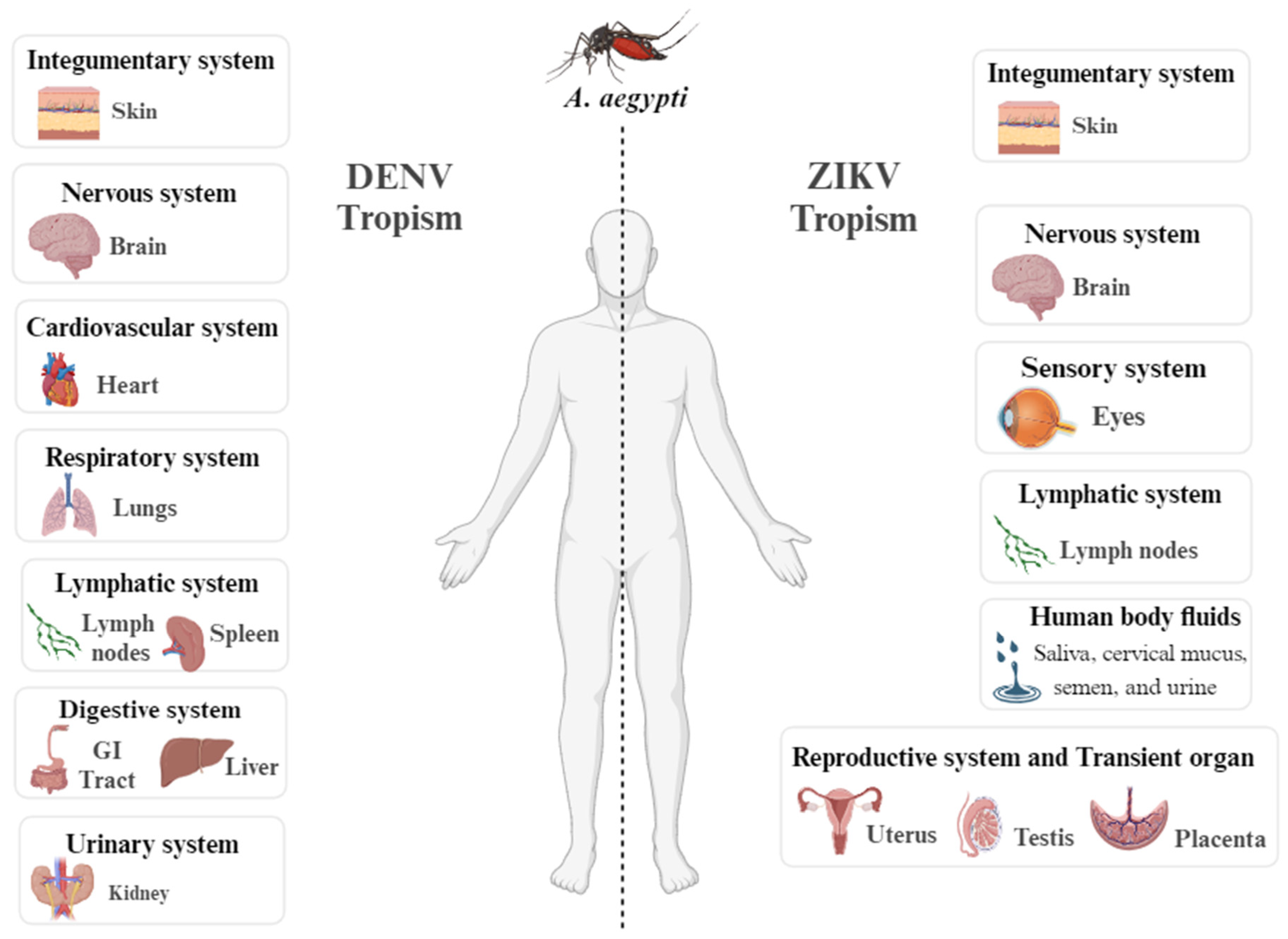
Dengue and Zika are related viruses transmitted by the same species of mosquitoes. While dengue has been well-documented and has affected people worldwide for many years, Zika has only recently caused outbreaks. Despite the similarities between viruses, the tropism of the viruses is different (Figure 5). Complication due to Zika virus infection during pregnancy may cause microcephaly and other congenital malformations in the infant referred to as congenital Zika syndrome [81]. Another neglected arbovirus, with symptoms similar to dengue are chikungunya and Oropouche fever (OF) [19,82]. The Oropouche virus (OROV) is one of the most common orthobunyaviruses and has in recent months spread to several countries in Central and South America, alerting the Pan American Health Organization (PAHO, WHO) on February 2, 2024 [83,84].
Figure 4.
Development and evolution of dengue symptoms in humans. Dengue progresses through three distinct clinical phases: (1) febrile phase that begins after the incubation period and is characterized by classic symptoms such as high fever, rash, myalgia, retro-orbital pain, nausea, and diarrhea (depicted on the left side of the figure). (2) Critical phase that occurs as the fever starts to subside. During this period, symptoms may worsen, indicating a potential progression to a more severe condition. Symptoms include plasma leakage through capillaries, hemorrhages, shock, and liver or kidney impairment (depicted on the right side of the figure). (3) Recovery phase, where the extravasated fluid is reabsorbed, and gastrointestinal symptoms gradually reduce. This image was created based on data from references [85,86].
Figure 4.
Development and evolution of dengue symptoms in humans. Dengue progresses through three distinct clinical phases: (1) febrile phase that begins after the incubation period and is characterized by classic symptoms such as high fever, rash, myalgia, retro-orbital pain, nausea, and diarrhea (depicted on the left side of the figure). (2) Critical phase that occurs as the fever starts to subside. During this period, symptoms may worsen, indicating a potential progression to a more severe condition. Symptoms include plasma leakage through capillaries, hemorrhages, shock, and liver or kidney impairment (depicted on the right side of the figure). (3) Recovery phase, where the extravasated fluid is reabsorbed, and gastrointestinal symptoms gradually reduce. This image was created based on data from references [85,86].
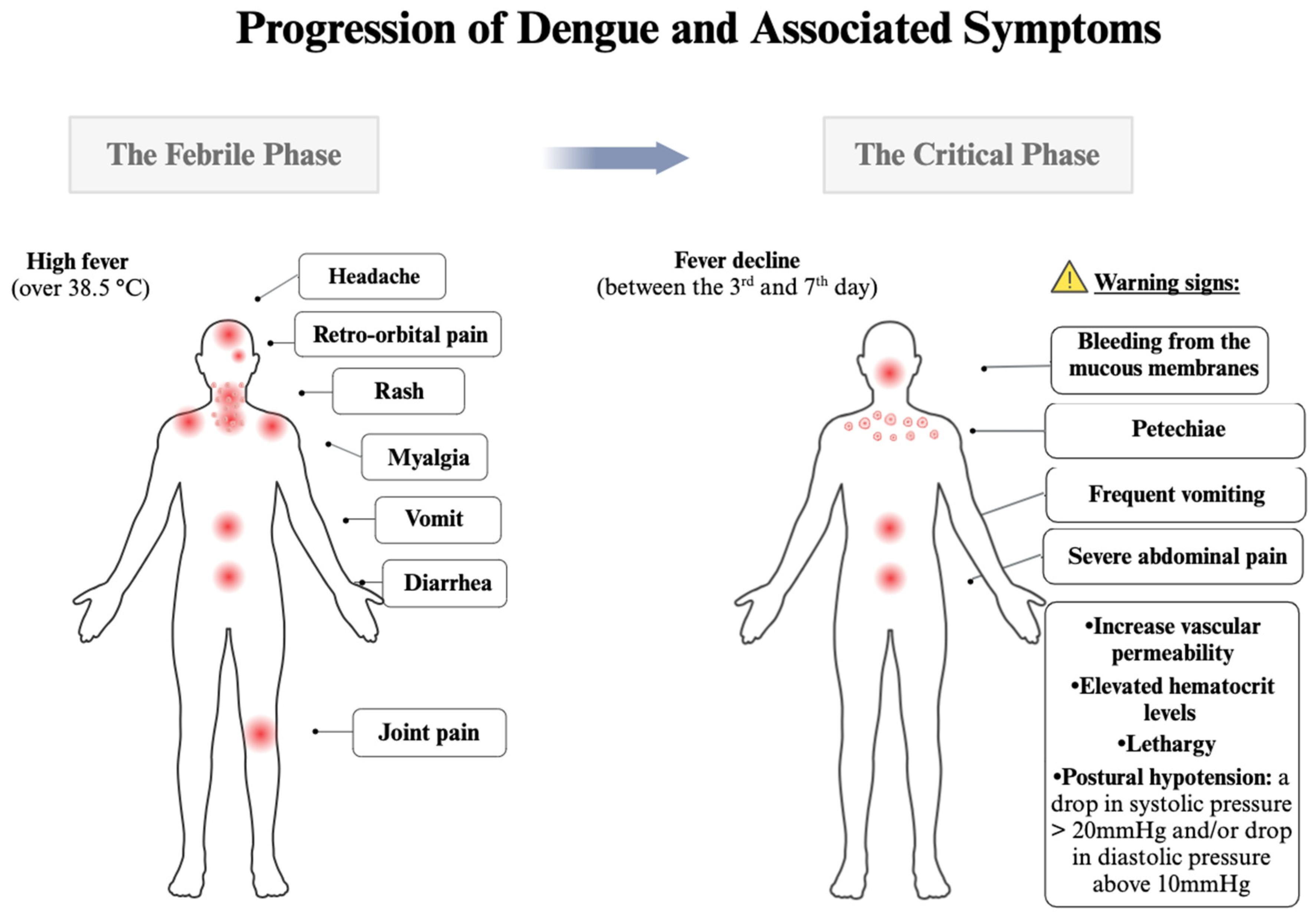
Figure 5.
Tissue tropism of Dengue (DENV) and Zika (ZIKV) viruses detected in humans. The organs and body fluids where Dengue virus (DENV, left side) and Zika virus (ZIKV, right side) have been detected in humans bitten by A. aegypti mosquitoes carrying these viruses. The figure is based on data obtained from references [87,88,89,90].
Figure 5.
Tissue tropism of Dengue (DENV) and Zika (ZIKV) viruses detected in humans. The organs and body fluids where Dengue virus (DENV, left side) and Zika virus (ZIKV, right side) have been detected in humans bitten by A. aegypti mosquitoes carrying these viruses. The figure is based on data obtained from references [87,88,89,90].
Clinical management and therapeutic intervention in Dengue infection in Brazil
The severity of the infection is a key factor in choosing the better treatment. The Federal Government Organization responsible for promoting, protecting and recovering the health of the population in Brazil, the Ministério da Saúde (MS), emphasizes through the National Dengue Control Guidelines the importance of risk classification of patients, for treatment and reduction of fatalities. The following classification model is indicated as shown in Table 3 based on "National Guidelines for the Prevention and Control of Dengue Epidemics" [91]. The classification system ensures that patients receive appropriate care based on the severity of their symptoms, aiming to reduce mortality and improve outcomes. By following these guidelines, healthcare providers can effectively manage dengue cases, prioritize resources, and deliver timely interventions to those in need. Proper adherence to this structured approach is essential for controlling the impact of dengue and other arboviruses in the Americas [92,93]. In this regard, the following classification model is indicated: Group A: Intended for patients with classic symptoms of Dengue. In this case, care is provided at Primary Health Care Units (Urgent Care), and the patient is advised to undergo home treatment with oral hydration, and if symptomatic, the doctor may recommend the use of the analgesics and antipyretics Dipyrone and Paracetamol. It is important to note that during the treatment of Dengue fever, drugs from Salicylate class and other non-steroidal anti-inflammatory drugs, as well as corticosteroid anti-inflammatory drugs, are not prescribed due to the increased risk of gastrointestinal bleeding. Group B: For patients presenting two or more clinical signs of the acute phase in addition to spontaneous bleeding, which can be indicated by petechiae, gingival bleeding and ecchymosis. The patient is attended to at a Secondary Health Care Unit equipped with an on-observation bed, where they are required to stay hospitalized for a minimum of 12 h. During this time, they receive oral or intravenous hydration and undergo a complete blood count to monitor their hematocrit levels. Group C: when fever begins to subside (between the 3rd and 7th day), the symptoms may arise that may indicate the progression of the disease to a more serious clinical condition, with lethargy, severe abdominal pain, postural hypotension, frequent vomiting, bleeding from the mucous membranes, progressive increase in the hematocrit levels, and decrease of the platelets levels. In this case, the patient should be transferred to a Tertiary Health Care Unit (Reference Hospital with greater technical support) where they will receive more rigorous intravenous hydration with physiological saline or Ringer Lactate 1 to 3 times a day, and clinical reassessment should occur hourly with hematocrit evaluation after 2 h. Group D: intended for patients presenting signs of shock: convergent blood pressure (Differential BP <20mm Hg), arterial hypotension, cyanosis, rapid pulse, and slow capillary refill. Therefore, the patient should receive more rigorous intravenous hydration at any healthcare facility and be immediately transferred to a Tertiary Health Care Unit (Reference Hospital with ICU beds). Immediate intravenous hydration with an isotonic solution is advised (procedure may be repeated up to 3 times as needed), followed by clinical reassessment (every 15-30 min), hematocrit reassessment after 2 h, and evaluation of BP, pulse and urinary output. If there is improvement, the patient will undergo treatment designated for group C. If the treatment is ineffective, the patient will undergo hematocrit evaluation, assessment for signs of congestive heart failure, metabolic acidosis, and monitoring of platelet levels, liver enzymes, serum albumin, assessment of renal function, and imaging tests. In this group, depending on the symptoms, there may be medical indications for analgesics and antipyretics, synthetic colloids or albumin, and diuretics for symptom reversal.
To enhance healthcare systems in a coordinated manner across the Americas and to prevent the progression of diseases and deaths caused by dengue fever, chikungunya, and Zika, the Pan American Health Organization (PAHO) developed a document in 2022 titled “Guidelines for the Clinical Diagnosis and Treatment of Dengue, Chikungunya, and Zika”. In creating this document, PAHO received support from the World Health Organization (WHO), the International Technical Group of Experts on Arboviral Diseases (GT-Arbovirus International), and specialists in the GRADE methodology. The update of the guidelines is based on systematic reviews of published papers and the specialized knowledge of these professionals regarding these arboviruses.
Table 3.
Risk group classification and clinical approaches for Dengue treatment. Patients with DENV are classified into distinct severity groups based on clinical signs, hypotension, and bleeding. It guides healthcare professionals with indicators for patient management. Treatment strategies vary according to each group. Group A - receives care at Primary Health Care Units with home-based treatments, Group B is observed in Secondary Health Care Units with intensified hydration, Group C undergoes intravenous hydration in Tertiary Health Care Units, and Group D requires immediate intensive care [91].
Table 3.
Risk group classification and clinical approaches for Dengue treatment. Patients with DENV are classified into distinct severity groups based on clinical signs, hypotension, and bleeding. It guides healthcare professionals with indicators for patient management. Treatment strategies vary according to each group. Group A - receives care at Primary Health Care Units with home-based treatments, Group B is observed in Secondary Health Care Units with intensified hydration, Group C undergoes intravenous hydration in Tertiary Health Care Units, and Group D requires immediate intensive care [91].
| Signs of shock | Clinical approach | Reference | |
|---|---|---|---|
| Group A |
- | • Care is provided at Primary Health Care Units (Urgent Care); • The patient is advised to undergo home treatment with oral hydration, and if symptomatic, the doctor may recommend the use of the analgesics and antipyretics Dipyrone and Paracetamol. It is important to note that during the treatment of Dengue fever, drugs from Salicylate class and other non-steroidal anti-inflammatory drugs, as well as corticosteroid anti-inflammatory drugs, are not prescribed due to the increased risk of gastrointestinal bleeding. |
[85,87,91,94] |
| Group B |
Patients presenting two or more clinical signs of the acute phase in addition to spontaneous bleeding, which can be indicated by petechiae, gingival bleeding and ecchymosis. |
The care occurs in a Secondary Health Care Unit equipped with an on-observation bed, where they are required to stay hospitalized for a minimum of 12 h. During this time, they receive oral or intravenous hydration and undergo a complete blood count to monitor their hematocrit levels. |
[85,94] |
| Group C |
Here symptoms may arise that may indicate the progression of the disease to a more serious clinical condition that includes lethargy, severe abdominal pain, postural hypotension, frequent vomiting, bleeding from the mucous membranes, progressive increase in the hematocrit levels and decrease of the platelets levels. |
• The patient should be transferred to a Tertiary Health Care Unit (Reference Hospital with greater technical support); • Will receive more rigorous intravenous hydration with physiological saline or Ringer Lactate 1 to 3 times a day, and clinical reassessment should occur hourly with hematocrit evaluation after 2 h. |
[85,94] |
| Group D |
Intended for patients presenting signs of shock: convergent blood pressure (Differential BP <20mm Hg), arterial hypotension, cyanosis, rapid pulse, and slow capillary refill. |
• The patient should receive more rigorous intravenous hydration at any healthcare facility and be immediately transferred to a Tertiary Health Care Unit (Reference Hospital with ICU beds). • Immediate intravenous hydration with an isotonic solution is advised (the procedure may be repeated up to three times as needed), followed by clinical reassessment every 15-30 min, hematocrit reassessment after two hours, and evaluation of blood pressure, pulse, and urinary output. • If there is improvement, the patient will undergo treatment designated for group C. • If the treatment is ineffective, the patient will undergo hematocrit evaluation, assessment for signs of congestive heart failure, metabolic acidosis, and monitoring of platelet levels, liver enzymes, serum albumin, assessment of renal function, and imaging tests. In this group, depending on the symptoms, there may be medical indications for analgesics and antipyretics, and diuretics for symptom reversal. |
[85,91,94] |
Measures adopted in Brazil to mitigate DENV cases
Dengue fever exhibits distinct seasonal contamination patterns, with a notable surge in cases and heightened epidemic risks typically observed between October and May of the following year [95].The precariousness of basic sanitation services, uncontrolled urban expansion, and improper waste disposal are factors that impact the proliferation of the vector and the disease [91,95]. In 2024, global dengue cases exploded, particularly in the Americas, where 80% of global cases are concentrated. In the first weeks of this year, case notifications increased in eleven countries, including Brazil, which has also recorded the simultaneous circulation of the four dengue serotypes (Figure 3) [96]. Climate change-induced alterations have accelerated mosquito breeding and virus dissemination, contributing significantly to this scenario [97]. Effective year-round prevention hinges on intersectoral policies involving community engagement and healthcare professionals as pivotal actors. Strategies include mechanical, biological, and chemical control methods, along with governmental regulations and legal measures [87,91,98].
In Brazilian territory, it is up to each citizen to adopt preventive measures in their homes and surroundings, avoiding: (a) the accumulation of containers that can store standing water and later become breeding grounds for the mosquito, (b) the accumulation of leaves and impurities in gutters and drains, (c) open water reservoirs, (d) the accumulation of trash and debris; and adopting individual protective measures such as installing protective screens on windows (mechanical control) and using repellents that are registered in Agência Nacional de Vigilância Sanitária (Anvisa), and the contain in their formulation any of these compounds: N,N-DIETIL-3-Methylbenzamide (DEET), Hydroxyethyl Isobutyl piperidine carboxylate (Icaridin or Picaridin), Ethyl butylacetylaminopropionate (EBAAP or IR3535), or oil of the Cymbopogon (Citronella) [99]. Endemic Disease Control (EDC) professionals and Community Health Agents (CHA) complement these efforts by visiting homes in order to educate and guide their residents on mosquito prevention and overseeing preventive measures [91].
Interestingly, female Aedes aegypti detect ultraviolet light at the shorter wavelength end of the human-visible spectrum but are unable to perceive red light at the longer wavelength end. Their dichromatic vision likely limits their color discrimination ability. Additionally, A. aegypti exhibit eye parameters optimized for low-light conditions, aligning with their preference for activity in dim environments. This adaptation enhances their capacity to detect hosts and navigate effectively during dawn and dusk, when ambient light levels are low. [100]. Photocontrol has been proposed as an effective method for managing mosquito populations. Specifically, blue light with a wavelength of approximately 420 nm has been identified as a promising method for controlling populations of Aedes albopictus and Culex pipiens f. molestus [101]. Capture assays with Aedes aegypti demonstrated that traps using various LED intensities and color combinations achieved different capture rates, with the tricolored trap capturing 100% of female mosquitoes. Although statistical differences between the experimental groups were not significant, the tricolored trap appears to enhance female capture rates by accommodating variations in mosquito vision. This green technology-based trap shows promise as an effective, safe tool for reducing mosquito populations and potentially curbing the spread of mosquito-borne diseases [102].
Chemical control entails World Health Organization (WHO)-approved insecticides, including aerosol sprays, called in Brazil as “fumacê”, an insecticide composed of Prallethrin, Imidacloprid, and solvents, which acts on the mosquitoes nervous system, causing their death. Because it is a method that generates environmental impact and can induce increased mosquito resistance, it should be used sparingly [91,103]. As an alternative to the use of Chemical insecticides, the MS it incorporated the use of the biological larvicide Bacillus thuringiensis israelensis (Bti) into the vector control program, which kills the larvae of A. aegypti that ingest its endotoxins. Another highly effective strategy used by the MS has been the Wolbachia Method, which involves the release of A. aegypti mosquitoes infected with the Wolbachia bacteria. By reproducing with local mosquitoes, new populations of mosquitoes with the bacteria are formed, which in turn, prevents the development of the virus in the mosquito, interrupting arbovirus transmission. The method has been used in some Brazilian cities that have achieved an important reduction in dengue, chikungunya, and Zika cases. For instance, cities like Niterói and parts of Rio de Janeiro observed reductions of 69% and 71%, respectively, following Wolbachia deployments in A. aegypti mosquitoes [104,105]. In Yogyakarta, Indonesia, Wolbachia reduced dengue incidence by 77.1% [106,107], while in Colombia’s Aburra Valley, it decreased cases by 95-97% during the 2–4 years compared to the 10 years pre-intervention [108]. These outcomes confirm Wolbachia as a powerful tool for reducing dengue in high-risk areas. Recently, it was inaugurated in Belo Horizonte city The Wolbachia Bio Factory, result of a partnership between the MS, the Fundação Oswaldo Cruz (Fiocruz), the patent owner World Mosquito Program (WMP), the government of Minas Gerais and the Belo Horizonte city [109,110]. This will allow expanding the Wolbachia method to additional Brazilian cities and could significantly reduce dengue cases nationwide, as it has already shown promising results in a few test locations.
Alternative strategies for controlling mosquito populations include the development of RNAi-based bioinsecticides, which can be used independently or in conjunction with conventional insecticides. A promising low-cost bioinsecticide has been proposed for direct application to breeding water, derived from lysates of recombinant E. coli expressing double-stranded RNA. This bioproduct disrupts the chitinous structures of mosquito larvae, which are critical for their survival. Furthermore, this RNAi-based approach has demonstrated an insecticidal adjuvant effect when combined with diflubenzuron, a chitin synthesis inhibitor, enhancing overall efficacy in mosquito control [106].
Legal measures enforce cleanliness norms on vacant or abandoned properties, facilitating access for health agents in inactive or resistant premises [91]. Brazil’s Unified Health System (SUS) incorporated the Qdenga vaccine (Takeda Laboratory) against Dengue into the National Vaccination Schedule in December 2023, as an additional form of disease progression control. The immunizations for the first dose began in February 2024 and covered 521 municipalities across the national territory. Initially, the priority for vaccinations was children and teenagers between the ages of 10 and 14, who will receive two doses of the vaccine over a three-month period [111]. Despite supply challenges, subsequent vaccine shipments are ongoing, with nearly 1 million doses distributed by late May 2024 to 405 municipalities [97,112]. And although the MS has acquired a large quantity of vaccines, they will not be enough to vaccinate the entire population.
In general, combating dengue fever in Brazil requires a multidisciplinary approach that integrates community involvement, robust healthcare strategies, and coordinated efforts across various sectors. Addressing the environmental, social, and health-related determinants of Dengue transmission is essential for reducing the DENV circulation. Despite implementing various control efforts, Brazil has achieved modest progress in reducing dengue incidence, with mosquito proliferation increasingly driven by climate change. To prevent another outbreak during the upcoming seasonal cycle, expected from December to May, additional proactive strategies are urgently needed.
Dengue vaccines
In Brazil, the search for an effective vaccine against dengue has been a public health priority due to the high incidence of the disease in various regions. Currently, two live attenuated tetravalent dengue vaccines have been licensed [113]. The first is Dengvaxia (CYD-TDV), developed by Sanofi Pasteur. Approved by Anvisa in 2015 and subsequently in several countries [114] it is recommended for individuals aged 9 to 45 who have had previous exposure to the dengue virus and is administered in three doses [115]. Dengvaxia primarily induces a CD8+ response targeting NS3 and neutralizing antibodies mainly against DENV-4 [116]. This vaccine is a chimeric live attenuated tetravalent vaccine, which means it contains weakened forms of the dengue virus that stimulate the immune system without causing the disease [117]. It is based on a vaccine strain of the yellow fever virus (YFV) known as 17D. In this technology, the pre-membrane (prM) and envelope (E) genes of YFV were replaced by the corresponding genes of each of the four DENV serotypes, derived from DENV isolates collected in Thailand and Indonesia between 1978 and 1988. Four chimeric YF-DEN viruses were generated and used in the formulation of the tetravalent vaccine, called ChimeriVax™ DENV 1-4 [118,119,120]. The vaccine offers varying levels of protection for each serotype DENV-1 (50.3%), DENV-2 (42.3%), DENV-3 (74.0%), and DENV-4 (77.74%) [121]. Studies also have shown that seronegative individuals vaccinated with Dengvaxia have an increased risk of developing more severe forms of the disease if they become infected after vaccination, leading to more restricted recommendations for its use [122].
Although Dengvaxia marked a significant advancement in dengue prevention, its implementation requires careful evaluation of the risks and benefits, particularly in populations without previous exposure to the virus. The vaccine remains a milestone in dengue prevention but highlights the need for ongoing development of safer and more effective vaccines to protect all at-risk populations.
The second licensed vaccine is TAK-003, also known as Qdenga or Takeda. Developed by the Takeda Pharmaceuticals in Rionegro, Colombia [123,124], it is a live attenuated tetravalent Dengue vaccine based on the structure of serotype 2 (DENV-2) [125,126], with recombinant strains that express surface proteins for the other serotypes (DENV1, DENV3, and DENV4) [127]. Qdenga stimulates a response against all four Dengue serotypes, with a more robust response for DENV-2 [127].
Qdenga is considered a safe vaccine for both seropositive and seronegative individuals, making it appropriate for use in non-endemic regions for dengue and in both adults and children living in dengue-endemic areas such as Asia and Latin America [128]. Countries including Brazil, Argentina, Thailand, Indonesia, the European Union, and Great Britain have authorized the use of Qdenga [123]. Clinical studies have demonstrated that TAK-003 may reduce the risk of severe disease and hospitalization. However, it does not completely prevent Dengue infection [129,130].
Achieving high vaccination coverage, particularly in endemic regions, remains a key challenge in the deployment of dengue vaccines. This coverage is critical to curbing viral transmission. The cost of vaccines further complicates widespread adoption, especially among vulnerable populations. While several other dengue vaccines are in development, including some in advanced clinical stages, much study remains to ensure their safety and effectiveness across diverse populations. Given the elevated risk of severe disease following a first partial DENV infection, the Laboratory of Infectious Diseases (LID) at the National Institute of Allergy and Infectious Diseases (NIAID), U.S., has employed recombinant DNA technologies to produce a tetravalent live-attenuated dengue vaccine [131]. Among their developments is TV003, which incorporates non-structural proteins from three Dengue serotypes, contrasting with the CYD™ vaccine that lacks non-structural proteins in its formulation. Preliminary clinical trials demonstrated that TV003 provided significant protection following a second dose administered after 6 or 12 months [131]. Research has revealed that vaccination with TV003 activates both CD4+ and CD8+ T cells, with distinct target preferences: CD8+ T cells largely recognize non-structural (NS) proteins, while CD4+ T cells are responsive to the C and NS2A proteins. Notably, NS3 and NS5 antigens elicit responses from both T cell populations, whereas prM and E proteins trigger lower immune responses. It is plausible that the Butantan-DV vaccine, sharing similarities with TV003, could induce a comparable immunological mechanism [132,133,134].
The Butantan-DV vaccine stems from attenuated strains produced by the NIH and has undergone phase 1 clinical trials in the U.S. The Butantan Institute subsequently selected tetravalent formulations, including TV003, for further development and manufacturing. Currently, the vaccine is in the final stage of clinical trials. Phase 2 trials were conducted in healthy Brazilian volunteers aged 18 to 59, both DENV-naive and previously exposed individuals. Randomized participants received the Butantan-DV vaccine, TV003, or a placebo. The immune responses and neutralizing antibody titers elicited by the Butantan-DV vaccine and TV003 showed no significant differences. Pre-exposure to DENV was correlated with higher neutralizing antibody levels, except for DENV-4. Among DENV-naive individuals, 64% developed an immune response against all four serotypes, while 55% of previously exposed participants achieved a response post-vaccination with Butantan-DV [133].
Phase 3 trials initiated in 2016, enrolling 16,235 healthy participants in a double-blind study. Subjects were divided into three age cohorts: 2–6 years, 7–17 years, and 18–59 years, receiving either the Butantan-DV vaccine or a placebo. Follow-up assessments over subsequent years evaluated the vaccine’s safety and efficacy, particularly against serotypes 1 (89.5%) and 2 (69.6%). Notably, serotypes DENV-3 and DENV-4 were not detected in the trials. The efficacy of Butantan-DV was 80.1% in participants aged 2–6, 77.8% in those aged 7–17, and 90.0% in those aged 18–59. Among DENV-naive participants, vaccine efficacy was 79.6%, compared to 89.2% in those previously exposed. A crucial outcome of the trial was the vaccine’s capacity to prevent severe dengue cases and reduce progression to more serious forms of the disease [113,135].
Diagnosis test
Different strategies are employed for dengue diagnosis depending on the stage of the disease and the clinical history of the infection [136] (Table 4). Despite the significant advancements in biomolecular approaches and lateral flow rapid tests, simpler techniques such as the tourniquet test (TT) are widely used in regions with a high incidence of cases and in poor areas where these methods are not affordable or laboratories cannot achieve the demand [137],[138]. A positive TT (≥10 petechiae per square inch) is usually observed in patients with dengue hemorrhagic fever and severe forms of the disease due to capillary fragility and thrombocytopenia [139]. However, due to its low sensitivity and specificity, the TT alone is not accepted as a diagnostic criterion and must complement other biomolecular, antigenic, and immunogenic assays [140,141].
When deciding which test to use, previous exposure to Flaviviridae viruses must be considered. In primary infections, a longer viraemia and an extended presence of non-structural protein (NS1) in the bloodstream and body fluids are found. IgM typically emerges around the third day of symptom onset, while IgG is absent until the tenth day. In contrast, immunological memory from past infections allows early production of IgG, creating an effective antiviral response that limits the circulating amount of NS1 [46,142,143,144,145]. Reverse-transcriptase polymerase chain reaction (RT-PCR) is considered a gold standard technique by the World Health Organization for confirming the presence of viral particles, known for its high sensitivity and specificity, which can reach up to 100%. This method is capable of differentiating flavivirus species and even the five DENV subtypes [46,146,147]. However, appropriate sample conservation strategies are essential for reliable RT-PCR results. Samples should be stored at 4-8°C for no more than 24 h to avoid false-negative results due to the fast degradation of viral RNA in vitro [148]. Furthermore, the timing of sample collection during the infection course can impact sensitivity. Viral loads tend to decline as the disease progresses, especially after the fifth day of infection, which may affect detection depending on primer choice, sample processing conditions and type of commercial kits used [149,150].
For NS1 detection using Enzyme-Linked Immunosorbent Assay (ELISA), samples can be stored at 4-8°C for 24 h and at -30°C or -70°C for 15 days or longer periods [47,148]. NS1 is a conserved glycoprotein produced by flaviviruses and found in serum and body fluids, making it an interesting target for diagnostic tests. However, saliva and urine samples have shown much lower sensitivity and specificity compared to plasma samples [151,152,153,154].
Serological tests are essential for interpreting disease progression and differentiating between primary and secondary infections. These tests can vary significantly depending on infection history and are susceptible to cross-reactions in individuals previously infected by other flaviviruses, such as a secondary Zika virus infection in patients once exposed to dengue virus [155]. Positive IgM and negative IgG during the first week of infection indicates a recent primary infection, while positive IgM and IgG in a 1.10 ratio reveals a recent secondary infection (sensitivity (Se) = 100 % and specificity (Sp) = 97.4 %) [156]. Negative IgM and positive IgG results indicate an infection from the past few months [46,48]. Combining two or more tests (e.g., NS1 and IgM or NS1 and IgM/IgG detections) is strongly recommended to improve sensitivity and specificity (up to 100%), thereby providing a more reliable diagnosis.
In addition to the aforementioned techniques, some older methods, though largely replaced by new technological systems for clinical diagnosis, still hold importance for specific investigations. For example, the plaque reduction neutralization test (PRNT) and virus cultivation require specialized laboratories capable of growing the virus in cell tissues, often taking more than a week to obtain results. PRNT provides information about the presence of antibodies in the patient’s serum that can inactivate specific virus species, while virus cultivation allows for the laboratory culture of viruses from different sources, including autopsy tissues [157,158,159].
Overall, accurate dengue fever diagnosis requires a combination of diagnostic strategies tailored to the disease stage and patient history. Advanced biomolecular techniques and rapid tests have improved diagnostic capabilities, but simpler methods like the tourniquet test are still vital in resource-limited settings. Biomolecular assays, such as RT-PCR and NS1 detection, confirm viral presence and differentiate dengue subtypes, though careful management is needed to ensure accuracy. Serological tests distinguish between primary and secondary infections, despite potential cross-reactions with other flaviviruses. Combining multiple diagnostic methods enhances reliability. Older techniques such as plaque reduction neutralization tests and virus cultivation remain important for specific research. An integrated approach using both advanced and traditional methods is crucial for effective dengue management, with ongoing innovation and improved accessibility key to controlling the disease globally. Table 4 presents recommended diagnostic tests for dengue based on the number of days since symptom onset and the time required to obtain results. It is important to note that the sensitivity (Se) and specificity (Sp) of each test can vary depending on the specific protocols, reagents, and equipment employed for analysis.
Following the incorporation of the Qdenga vaccine (developed by Takeda Laboratories) into Brazil’s National Vaccination Schedule by the SUS in December 2023, individuals vaccinated have shown IgM antibodies for the NS1 protein for over 3 months and IgG antibodies for over a year. This renders traditional serological dengue tests ineffective for this group. The only reliable method for detecting the presence of DENV in these individuals will be through the NS1 antigen test during the period of dengue viraemia or/and RT-PCR. In Brazil, suspected dengue cases can be confirmed through laboratory criteria or clinical-epidemiological linkage. The primary diagnostic tests accepted for confirmation include serological tests (IgG and/or IgM antibodies), detection of the NS1 antigen, and RT-PCR (Reverse Transcription Polymerase Chain Reaction) [56].
Table 4.
Diagnostic tests based on days after symptom onset. Primary infection (PI) refers to a patient experiencing their first dengue infection, while secondary infection (SI) pertains to a patient who has had a previous Dengue infection. DF stands for dengue fever, DHF for dengue hemorrhagic fever, Se for sensitivity, Sp for specificity, and RDT for rapid diagnostic test.
Table 4.
Diagnostic tests based on days after symptom onset. Primary infection (PI) refers to a patient experiencing their first dengue infection, while secondary infection (SI) pertains to a patient who has had a previous Dengue infection. DF stands for dengue fever, DHF for dengue hemorrhagic fever, Se for sensitivity, Sp for specificity, and RDT for rapid diagnostic test.
| Diagnostic test timeline (days after symptom onset) | |||||
|---|---|---|---|---|---|
| Method principle | Primary Infection (PI) | Secondary Infection (SI) | Time to obtain the result | ||
| Capillary fragility | Tourniquet Test | - from 0 to 7 days • Se = 11.9 to 19.1 % in DF and 63 to 83% in DHF [140,160] • Sp = 86.4 to 88.9 % [140,160] in DF and 60 % in DHF [161] |
min | ||
| Virus or virus product detection | Virus isolation | - from 0 to 4 days • Se = 85.3 % [162] - from 4 days onwards • Se = 65.4 % [162] |
≥ one week | ||
| • Se = 91.0 % [162] | • Se = 77.6 % [162] | ||||
| RT-PCR or RT-qPCR | - from 0 to 5 days • Se = 90 to 100 % [150,147,147,149] • Sp = 100 % [150] - from 5 days onwards • Se = 38 to 100 % [150] • Sp = 100 % [150] |
around one day | |||
| NS1 protein detection | ELISA (serum) | - from 0 to 7 days • Se = 93.9 to 100 % [154] - from 7 to 9 days • Se = 85.7 to 93.9 % [154] |
- from 0 to 3 days • Se = 88.6 % [154] -from 3 to 5 days • Se = 54.1 % [154] |
around one day | |
| RDT (serum) | • Se = 80.3 % [163] • Sp = 100 % [163] |
• Se = 55.1 % [163] • Sp = 100 % [163] |
min | ||
| - from 0 to 3 days • Se = 76.7 to 83.3 % [164] - from 4 days onwards • Se = 47.6 to 76.2 % [164] | |||||
| Antibody detection | IgM detection | ELISA (serum) | - from 4 to 7 days • Se = 55 % [165] - from 7 days onwards • Se = 94 % [165] |
- from 4 to 7 days • Se = 47 % [165] - from 7 days onwards • Se = 78 % [165] (SI patients have a lower concentration of IgM than PI) |
around one day |
| RDT (serum) | - from 0 to 3 days • Se = 3.3 % [164] • Sp = 100 % [164] - from 4 days onwards • Se = 23.8 to 38.1 % [164] • Sp = 100 % [164] |
min | |||
| IgG detection | RDT (serum) | - From 3 to 7 days • Se = 31.82 to 40.91 % [166] • Sp = 95.24 to 100 % [166] |
- From 3 to 7 days • Se = 82.76 to 95.4 % [166] • Sp = 95.24 to 100 % [166] |
min | |
Oropouche Fever in Latin America: Rising Incidence, Clinical Overlap with Dengue, and Emerging Public Health Challenges
Oropouche fever was first identified in forestry workers in Trinidad in 1955, with its initial detection in Brazil occurring in 1960 [19,167]. The disease is endemic to several Latin American countries, including Brazil, Panama, Argentina, Bolivia, Ecuador, Peru, and Venezuela, with the Amazon region being particularly affected [19,168]. Prior to the emergence of chikungunya and Zika viruses in 2013, Oropouche virus (OROV) was recognized as the second most prevalent arbovirus in Brazil [169]. Between January 1 and September 26, 2024, Brazil reported 8,174 cases of oropouche fever, a sharp increase compared to 831 cases in 2023, including two deaths. This marks the highest number of cases recorded since the 1961 outbreak, which saw approximately 11,000 cases [167,170]. Other Latin American countries also experienced an increase in cases during this period, including Bolivia (356), Peru (290), Colombia (74), and Cuba (74). Previous studies in the Brazilian states of Acre and Pará have identified four cases of newborns with microcephaly; however, study limitations prevent establishing a causal link between OROV infection and neurological malformations [167,170]. Another study in Brazil detected OROV IgM in six of 68 newborns with unexplained microcephaly, with OROV RNA and antigen present in multiple tissues, including the brain, of one deceased infant [171]. Recently a case of OROV infection in pregnancy that was associated with a no apparent malformation stillbirth was reported in Brazil as the first case of vertical transmission. The presence of OROV RNA was detected in the cerebrospinal fluid, brain, lungs, liver, umbilical cord, and placenta with signs of infarction [172]. These findings highlight the need for urgent investigation into OROV’s potential role in fetal harm.
The OROV, a member of the Peribunyaviridae family, is an arbovirus transmitted primarily by mosquitoes and is the causative agent of oropouche fever [82]. The transmission of OROV is mainly associated with forested regions and proximity water bodies, with the virus sustained in nature through both urban and sylvatic cycles [173]. The OROV outbreak can be divided into: (1) sylvatic, transmitted by the mosquitoes Coquilletti diavenezuelensis, Aedes serratus and, the most important, Culicoides paraenses, through various hosts, such as sloths (Bradypus tridactylus), rodents, birds, and non-human primates; (2) urban, transmitted by the mosquitoes Culicoides paraenses and Culex quinquefasciatus through humans as the amplifying host [19,82,83,174]. The genus Culicoides constitutes a global public health concern, acting as a vector for various arboviruses [82]. Furthermore, climate changes may also contribute to expanding the distribution of OROV vectors to other continents [82,175].
Clinical manifestations of OROV infection include high fever, headache, myalgia, arthralgia, nausea, vomiting, chills, and photophobia symptoms that are often indistinguishable from other arboviral diseases such as Dengue, West Nile, Zika, Chikungunya, and even Influenza, which may contribute to underreporting [175,176,177,178]. OF symptoms usually disappear within two weeks. A minority of patients may develop severe complications, including hemorrhagic manifestations and neurological involvement [179,180] such as meningitis or encephalitis [19,82,181]. Currently, no specific antiviral treatment or vaccine is currently available for OROV; thus, patient care remains symptomatic and supportive [181]. Prevention efforts are focused on minimizing mosquito exposure through personal protective measures such as insect repellents, appropriate clothing, and vector control strategies as described for preventing dengue infections. The overlap in symptoms caused by different arboviruses, combined with the dengue outbreak in Brazil in 2024, underscores significant challenges for the healthcare system. With limited capacity for RT-qPCR testing across all samples, most cases were confirmed based on clinical presentation, as previously mentioned. This approach can lead to an overestimation of dengue cases, particularly in endemic regions where new arboviruses may also emerge.
Therefore, the development and implementation of rapid diagnostic tests capable of distinguishing between different arboviruses are essential during outbreak scenarios. Such tools would provide a clearer picture of the etiological agents in circulation, enabling more accurate public health responses and resource allocation.
Dengue’s emergence in Europe: a changing epidemiological landscape
Dengue outbreaks are becoming more frequent in tropical regions, with increasing reports from colder climates where such events were previously rare. While the majority of dengue cases have historically been associated with international travel [182], there is a growing shift in this pattern. Anthropogenic climate change has facilitated the expansion of invasive mosquito species into regions where they were once unable to persist. Since May 2024, non-native Aedes species, including A. aegypti, A. albopictus, A. atropalpus, A. japonicus, and A. koreicus, have been reported as well-established in multiple European countries [183]. This poses a concern for the potential adaptation of native European Aedes species as vectors of dengue and other arboviruses. Notably, A. geniculatus, a species indigenous to Europe [184], has been implicated in the transmission of chikungunya virus. As arboviruses continue to adapt to the local mosquito population [185], there is a growing risk of their permanent establishment in these new environments.
Among the Aedes species, A. aegypti and A. albopictus are recognized as primary vectors of DENV. In this regard, A. albopictus is expected to play a dominant role in the spread of dengue within Europe (Figure 6) [186]. The northward expansion of A. albopictus, extending into southern Sweden, raises significant public health concerns. Established populations in the Mediterranean region suggest that these areas may serve as endemic hotspots for dengue transmission, driven by climate conditions increasingly favorable for Aedes spp. proliferation. Another arbovirose under concern in Europe is West Nile virus (WNV). In 2024, the European Centre for Disease Prevention and Control (ECDC) reported 715 locally acquired cases of WNV across 15 European countries. As of September 4, 51 deaths have been attributed to the infection. Around 20% of WNV cases develop into West Nile fever, characterized by symptoms such as fever, headaches, vomiting, and fatigue. In less than 1% of cases, the virus leads to severe neurological complications, including potentially life-threatening swelling of the brain (encephalitis) [187].
The establishment of non-native Aedes mosquitoes in Europe highlights the urgent need for preparedness within healthcare systems and communities. The European Centre for Disease Prevention and Control [186] has documented an upward trend in autochthonous dengue cases across the continent in recent years (Figure 7) [183]. Europe’s climate is undergoing progressive tropicalization, marked by rising temperatures and increased flooding, mirroring environmental conditions in Latin America and other dengue-endemic regions. These climatic changes are closely linked to the introduction and persistence of Aedes mosquitoes in flood-prone areas, facilitating their establishment and reproductive success. The growing presence of Aedes spp. thus heightens the risk of dengue, other arboviruses, and other tropical diseases becoming endemic in Europe.
The exponential profile in DENV native cases is alarming, suggesting a significant increase in cases in Europe (Figure 7a). This underscores the urgent need for European lifestyles and healthcare systems to prepare for managing large numbers of arbovirus cases. With intensifying climate change, proactive measures are crucial to address the presence of A. albopictus in Europe before dengue and other tropical diseases become endemic in temperate regions. As shown in Latin America, a parallel trend has emerged in Europe, where temperature anomalies similarly increased by approximately 1°C over two years, rising from 1.75°C in 2022 to 2.75°C in 2024 (Figure 7b). The expanding geographical range of mosquitoes in the region highlights the potential risk of future dengue outbreaks driven by favourable climatic shifts. This possibility is further supported by Singh et al., who demonstrated a robust correlation between seasonal temperature rises and annual dengue incidence in India [188].
Therefore, Figure 7 illustrates a concerning rise in autochthonous dengue cases across Europe, highlighting the increasing risk of locally acquired outbreaks. These changes emphasize the urgent need for preparedness, as Europe’s climate is undergoing a ’tropicalization,’ which enhances the likelihood of further mosquito proliferation and the potential establishment of other tropical diseases, including dengue and arboviruses previously undetected in the region. This situation suggests that Europe may not yet be fully equipped to handle the challenges posed by such emerging threats.
Figure 7.
Annual count of total autochthonous cases in Europe. a) Annual count of total dengue autochthonous cases in Europe. The curve represents the exponential regression, showing an increase in total autochthonous cases in Europe in function of time (in year). b) Temperature anomalies in Europe in the period of 2023 to 2024.
Figure 7.
Annual count of total autochthonous cases in Europe. a) Annual count of total dengue autochthonous cases in Europe. The curve represents the exponential regression, showing an increase in total autochthonous cases in Europe in function of time (in year). b) Temperature anomalies in Europe in the period of 2023 to 2024.
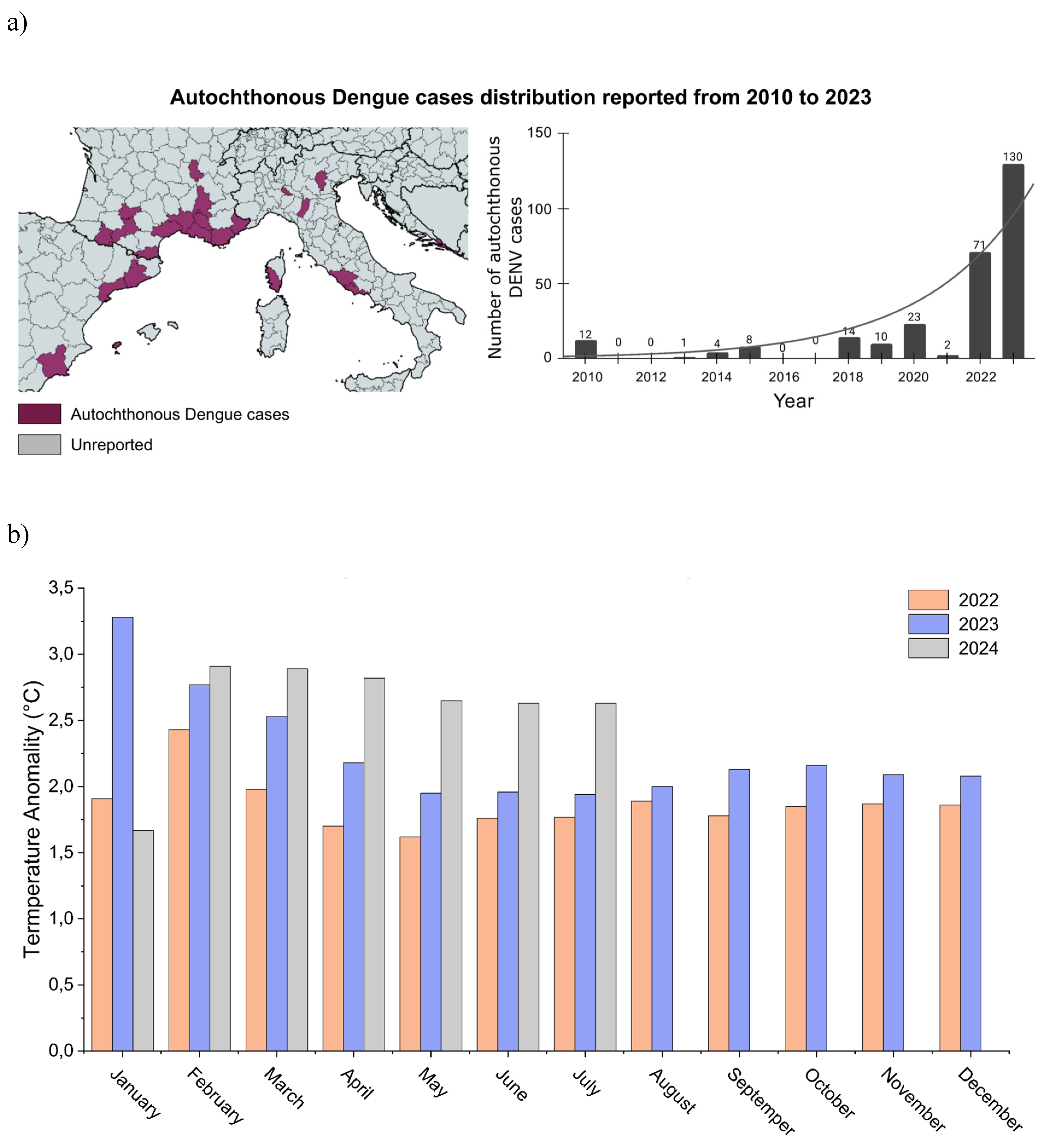
Conclusion
Dengue fever, a prominent arboviral disease transmitted by Aedes mosquitoes, presents an increasingly significant global public health challenge. Its spread is driven by factors such as climate change, urbanization, and globalization, all of which facilitate mosquito vector proliferation and the movement of infected individuals across borders. This trend is particularly evident in Latin America, where rising temperatures and increased rainfall create ideal breeding conditions for mosquitoes. In 2024, Brazil experienced a severe dengue outbreak, with approximately 5.7 million confirmed cases and 5,792 deaths, compared to around 1.4 million cases and 1,179 deaths in 2023 [57]. Furthermore, the spread of Aedes mosquito vectors is expanding the virus’s geographic range, pushing into previously unaffected areas and raising concerns for non-tropical countries about the potential emergence of arboviruses like dengue.
This study highlights the shifting epidemiology of dengue, as evidenced by its emergence in traditionally non-endemic regions such as Europe. The establishment of Aedes albopictus and other invasive mosquito species in new territories signals a critical shift in DENV transmission dynamics, fueled by climate change and vector adaptation [183,186]. The presence of these vectors in temperate zones raises serious public health concerns, underscoring the need for coordinated surveillance, vector control strategies, and preparedness efforts.
Global warming has accelerated the proliferation of various mosquito species that act as vectors for the transmission of several arboviruses, including dengue, Zika, chikungunya, oropouche, and West Nile virus. These mosquitoes thrive in warm, humid environments, resulting in higher infection rates. The dramatic rise in dengue cases in Latin American countries such as Brazil and Argentina in 2024 serves as a warning of what may soon occur in Europe and other regions. Consequently, while arboviruses are typically endemic to tropical areas, they must now be considered emerging threats in non-tropical countries as well. Addressing these challenges will require interdisciplinary approaches and international collaboration to mitigate the global spread of dengue and other arboviruses.
Informed Consent Statement
not applicable.
Data Availability Statement
not applicable.
Acknowledgments
The authors acknowledge the National Council for Scientific and Technological Development (CNPq), the Coordination for the Improvement of Higher Education Personnel (CAPES, grant 88887.374931/2019-00 and 88887.600105/2021-00, Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Finance Code 01), and the São Paulo Research Foundation (FAPESP, 2021/10577-0, 2022/08730-7, 2021/05262-0, 2023/13894-1, 2023/07366-2, 2023/18211-0), FINEP grant 29794 (FINEP/UFMG/PRPQ/CT VACINAS/SARS-CoV-2), for financial support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- FAO-WHO Expert Committee on Zoonoses Zoonoses: Report of the FAO-WHO Expert Committee on Zoonoses, 3rd, Geneva, 1966; 1967; ISBN 9789241203784.
- George, A.M.; Ansumana, R.; de Souza, D.K.; Niyas, V.K.M.; Zumla, A.; Bockarie, M.J. Climate Change and the Rising Incidence of Vector-Borne Diseases Globally. Int. J. Infect. Dis. 2024, 139, 143–145. [CrossRef]
- Wong, C. Climate Change Is Also a Health Crisis - These 3 Graphics Explain Why. Nature 2023, 624, 14–15. [CrossRef]
- Alied, M.; Endo, P.T.; Aquino, V.H.; Vadduri, V.V.; Huy, N.T. Latin America in the Clutches of an Old Foe: Dengue. Braz. J. Infect. Dis. 2023, 27, 102788. [CrossRef]
- Akhtar, N.; Gupta, S.K.; Singh, H. Surveillance of Zika and Dengue Viruses in Field-Collected Aedes Aegypti Mosquitoes from Different States of India. Virology 2022, 574, 96–101. [CrossRef]
- Laverdeur, J.; Desmecht, D.; Hayette, M.-P.; Darcis, G. Dengue and Chikungunya: Future Threats for Northern Europe? Front Epidemiol 2024, 4, 1342723. [CrossRef]
- Harapan, H.; Michie, A.; Sasmono, R.T.; Imrie, A. Dengue: A Minireview. Viruses 2020, 12. [CrossRef]
- Schaefer, T.J.; Panda, P.K.; Wolford, R.W. Dengue Fever. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2024.
- Paz-Bailey, G.; Adams, L.E.; Deen, J.; Anderson, K.B.; Lc., K. Website. Lancet 2024, 403, 667–682. [CrossRef]
- Arthropod-Borne and Rodent-Borne Viral Diseases. Report of a WHO Scientific Group. World Health Organ. Tech. Rep. Ser. 1985, 719, 1–116.
- Young, P.R. Arboviruses: A Family on the Move. Adv. Exp. Med. Biol. 2018, 1062, 1–10. [CrossRef]
- Go, Y.Y.; Balasuriya, U.B.R.; Lee, C.-K. Zoonotic Encephalitides Caused by Arboviruses: Transmission and Epidemiology of Alphaviruses and Flaviviruses. Clin. Exp. Vaccine Res. 2014, 3, 58–77. [CrossRef]
- Hollidge, B.S.; González-Scarano, F.; Soldan, S.S. Arboviral Encephalitides: Transmission, Emergence, and Pathogenesis. J. Neuroimmune Pharmacol. 2010, 5, 428–442. [CrossRef]
- Weaver, S.C.; Reisen, W.K. Present and Future Arboviral Threats. Antiviral Res. 2010, 85, 328–345. [CrossRef]
- Liu, Y.; Guan, W.; Liu, H. Subgenomic Flaviviral RNAs of Dengue Viruses. Viruses 2023, 15. [CrossRef]
- Murugesan, A.; Manoharan, M. Dengue Virus. In Emerging and Reemerging Viral Pathogens; Elsevier, 2020; pp. 281–359 ISBN 9780128194003.
- Drugs Targeting Structural and Nonstructural Proteins of the Chikungunya Virus: A Review. Int. J. Biol. Macromol. 2024, 262, 129949. [CrossRef]
- Caicedo, E.-Y.; Charniga, K.; Rueda, A.; Dorigatti, I.; Mendez, Y.; Hamlet, A.; Carrera, J.-P.; Cucunubá, Z.M. The Epidemiology of Mayaro Virus in the Americas: A Systematic Review and Key Parameter Estimates for Outbreak Modelling. PLoS Negl. Trop. Dis. 2021, 15, e0009418. [CrossRef]
- Martins-Filho, P.R.; Soares-Neto, R.F.; de Oliveira-Júnior, J.M.; Alves Dos Santos, C. The Underdiagnosed Threat of Oropouche Fever amidst Dengue Epidemics in Brazil. Lancet Reg Health Am 2024, 32, 100718. [CrossRef]
- Cattarino, L.; Rodriguez-Barraquer, I.; Imai, N.; Cummings, D.A.T.; Ferguson, N.M. Mapping Global Variation in Dengue Transmission Intensity. Sci. Transl. Med. 2020, 12. [CrossRef]
- Kularatne, S.A.; Dalugama, C. Dengue Infection: Global Importance, Immunopathology and Management. Clin. Med. 2022, 22, 9–13. [CrossRef]
- Ferreira-de-Lima, V.H.; Lima-Camara, T.N. Natural Vertical Transmission of Dengue Virus in Aedes Aegypti and Aedes Albopictus: A Systematic Review. Parasit. Vectors 2018, 11, 77. [CrossRef]
- Tauil, P.L. [Critical aspects of dengue control in Brazil]. Cad. Saude Publica 2002, 18, 867–871. [CrossRef]
- Xu, Z.; Bambrick, H.; Frentiu, F.D.; Devine, G.; Yakob, L.; Williams, G.; Hu, W. Projecting the Future of Dengue under Climate Change Scenarios: Progress, Uncertainties and Research Needs. PLoS Negl. Trop. Dis. 2020, 14, e0008118. [CrossRef]
- Morin, C.W.; Comrie, A.C.; Ernst, K. Climate and Dengue Transmission: Evidence and Implications. Environ. Health Perspect. 2013, 121, 1264–1272. [CrossRef]
- Combined Effects of Hydrometeorological Hazards and Urbanisation on Dengue Risk in Brazil: A Spatiotemporal Modelling Study. The Lancet Planetary Health 2021, 5, e209–e219. [CrossRef]
- Dengue Overview: An Updated Systemic Review. J. Infect. Public Health 2023, 16, 1625–1642. [CrossRef]
- Chen, R.; Vasilakis, N. Dengue--Quo Tu et Quo Vadis? Viruses 2011, 3, 1562–1608. [CrossRef]
- Bashyam, H.S.; Green, S.; Rothman, A.L. Dengue Virus-Reactive CD8+ T Cells Display Quantitative and Qualitative Differences in Their Response to Variant Epitopes of Heterologous Viral Serotypes. J. Immunol. 2006, 176, 2817–2824. [CrossRef]
- Parveen, S.; Riaz, Z.; Saeed, S.; Ishaque, U.; Sultana, M.; Faiz, Z.; Shafqat, Z.; Shabbir, S.; Ashraf, S.; Marium, A. Dengue Hemorrhagic Fever: A Growing Global Menace. J. Water Health 2023, 21, 1632–1650. [CrossRef]
- Brathwaite Dick, O.; San Martín, J.L.; Montoya, R.H.; del Diego, J.; Zambrano, B.; Dayan, G.H. The History of Dengue Outbreaks in the Americas. Am. J. Trop. Med. Hyg. 2012, 87, 584–593. [CrossRef]
- Juan, C. Dengue Fever: Strategies for Preventing Dengue and Bite Transmission Via Mosquitoes; Independently Published, 2024; ISBN 9798876916952.
- Cristodulo, R.; Luoma-Overstreet, G.; Leite, F.; Vaca, M.; Navia, M.; Durán, G.; Molina, F.; Zonneveld, B.; Perrone, S.V.; Barbagelata, A.; et al. Dengue Myocarditis: A Case Report and Major Review. Glob. Heart 2023, 18, 41. [CrossRef]
- Aedes Albopictus - Current Known Distribution: October 2023 Available online: https://www.ecdc.europa.eu/en/publications-data/aedes-albopictus-current-known-distribution-october-2023 (accessed on 28 May 2024).
- Gamez, S.; Antoshechkin, I.; Mendez-Sanchez, S.C.; Akbari, O.S. The Developmental Transcriptome of , a Major Worldwide Human Disease Vector. G3 2020, 10, 1051–1062. [CrossRef]
- Weerakoon, K.G.; Kularatne, S.A.; Edussuriya, D.H.; Kodikara, S.K.; Gunatilake, L.P.; Pinto, V.G.; Seneviratne, A.B.; Gunasena, S. Histopathological Diagnosis of Myocarditis in a Dengue Outbreak in Sri Lanka, 2009. BMC Res. Notes 2011, 4, 268. [CrossRef]
- Sinha, S.; Singh, K.; Ravi Kumar, Y.S.; Roy, R.; Phadnis, S.; Meena, V.; Bhattacharyya, S.; Verma, B. Dengue Virus Pathogenesis and Host Molecular Machineries. J. Biomed. Sci. 2024, 31, 43. [CrossRef]
- Madhry, D.; Pandey, K.K.; Kaur, J.; Rawat, Y.; Sapra, L.; Y S, R.K.; Srivastava, R.K.; Bhattacharyya, S.; Verma, B. Role of Non-Coding RNAs in Dengue Virus-Host Interaction. Front. Biosci. 2021, 13, 44–55. [CrossRef]
- Guzman, M.G.; Gubler, D.J.; Izquierdo, A.; Martinez, E.; Halstead, S.B. Dengue Infection. Nature Reviews Disease Primers 2016, 2, 1–25. [CrossRef]
- Gubler, D.J.; Ooi, E.E.; Vasudevan, S.; Farrar, J. Dengue and Dengue Hemorrhagic Fever, 2nd Edition; CABI, 2014; ISBN 9781845939649.
- Tan, P.C.; Rajasingam, G.; Devi, S.; Omar, S.Z. Dengue Infection in Pregnancy: Prevalence, Vertical Transmission, and Pregnancy Outcome. Obstet Gynecol 2008, 111, 1111–1117. [CrossRef]
- Kaur, G.; Soni, S.; Aggarwal, S.; Saini, A.S. Vertical Transmission of Dengue—A Case Report. The Journal of Obstetrics and Gynecology of India 2013, 64, 1–2. [CrossRef]
- Ferreira-de-Lima, V.H.; Andrade, P.D.S.; Thomazelli, L.M.; Marrelli, M.T.; Urbinatti, P.R.; Almeida, R.M.M. de S.; Lima-Camara, T.N. Silent Circulation of Dengue Virus in Aedes Albopictus (Diptera: Culicidae) Resulting from Natural Vertical Transmission. Sci Rep 2020, 10, 3855. [CrossRef]
- Joshi, V.; Mourya, D.T.; Sharma, R.C. Persistence of Dengue-3 Virus through Transovarial Transmission Passage in Successive Generations of Aedes Aegypti Mosquitoes. Am J Trop Med Hyg 2002, 67, 158–161. [CrossRef]
- Shroyer, D.A. Vertical Maintenance of Dengue-1 Virus in Sequential Generations of Aedes Albopictus. J Am Mosq Control Assoc 1990, 6, 312–314.
- Kok, B.H.; Lim, H.T.; Lim, C.P.; Lai, N.S.; Leow, C.Y.; Leow, C.H. Dengue Virus Infection - a Review of Pathogenesis, Vaccines, Diagnosis and Therapy. Virus Res. 2023, 324, 199018. [CrossRef]
- Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control: New Edition; World Health Organization: Geneva, 2009; ISBN 9789241547871.
- Zerfu, B.; Kassa, T.; Legesse, M. Epidemiology, Biology, Pathogenesis, Clinical Manifestations, and Diagnosis of Dengue Virus Infection, and Its Trend in Ethiopia: A Comprehensive Literature Review. Trop. Med. Health 2023, 51, 11. [CrossRef]
- Kalayanarooj, S. Clinical Manifestations and Management of Dengue/DHF/DSS. Trop. Med. Health 2011, 39, 83–87. [CrossRef]
- Verma, R.; Sharma, P.; Garg, R.K.; Atam, V.; Singh, M.K.; Mehrotra, H.S. Neurological Complications of Dengue Fever: Experience from a Tertiary Center of North India. Ann. Indian Acad. Neurol. 2011, 14, 272–278. [CrossRef]
- Marengo, J.A. Água e mudanças climáticas. Estud. av. 2008, 22, 83–96. [CrossRef]
- Southern Brazil Has Seen an Increase of up to 30% in Average Annual Rainfall over the Last Three Decades Available onlinhttps://www.gov.br/planalto/en/latest-news/2024/05/southern-brazil-has-seen-an-increase-of-up-to-30-in-average-annual-rainfall-over-the-last-three-decades (accessed on 3 June 2024).
- Diallo, D.; Diouf, B.; Gaye, A.; NDiaye, E.H.; Sene, N.M.; Dia, I.; Diallo, M. Dengue Vectors in Africa: A Review. Heliyon 2022, 8, e09459. [CrossRef]
- Pirani, M.; Lorenz, C.; de Azevedo, T.S.; Barbosa, G.L.; Blangiardo, M.; Chiaravalloti-Neto, F. Effects of the El Niño-Southern Oscillation and Seasonal Weather Conditions on Aedes Aegypti Infestation in the State of São Paulo (Brazil): A Bayesian Spatio-Temporal Study. PLOS Neglected Tropical Diseases 2024, 18, e0012397. [CrossRef]
- Website Available online: (https://www.paho.org/pt/topicos/dengue).
- Dengue: diagnóstico e manejo clínico: adulto e criança Available online: https://www.gov.br/saude (accessed on 8 November 2024).
- BRASIL Painel de Monitoramento das Arboviroses Available online: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/a/aedes-aegypti/monitoramento-das-arboviroses/painel (accessed on 18 June 2024).
- Dengue Available online: https://www3.paho.org/data/index.php/en/mnu-topics/indicadores-dengue-en.html (accessed on 7 November 2024).
- PAHO Situation Report No 20 - Dengue Epidemiological Situation in the Region of the Americas - Epidemiological Week 20, 2024 Available online: https://www.paho.org/en/documents/situation-report-no-20-dengue-epidemiological-situation-region-americas-epidemiological (accessed on 17 June 2024).
- Gutiérrez, L.A. PAHO/WHO Data - Dengue serotypes by country Available online: https://www3.paho.org/data/index.php/en/mnu-topics/indicadores-dengue-en/dengue-nacional-en/517-dengue-serotypes-en.html (accessed on 7 November 2024).
- BRASIL Centro de Operações de Emergências (COE) Available online: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/a/arboviroses/informe-semanal/informe-semanal-no-02-coe (accessed on 17 June 2024).
- Khanam, A.; Gutiérrez-Barbosa, H.; Lyke, K.E.; Chua, J.V. Immune-Mediated Pathogenesis in Dengue Virus Infection. Viruses 2022, 14. [CrossRef]
- Waickman, A.T.; Lu, J.Q.; Fang, H.; Waldran, M.J.; Gebo, C.; Currier, J.R.; Ware, L.; Van Wesenbeeck, L.; Verpoorten, N.; Lenz, O.; et al. Evolution of Inflammation and Immunity in a Dengue Virus 1 Human Infection Model. Sci. Transl. Med. 2022, 14, eabo5019. [CrossRef]
- Dengue Available online: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/d/dengue/dengue (accessed on 3 July 2024).
- Scully, C. Persistent Metallic Taste. Br. Dent. J. 2013, 214, 217–218. [CrossRef]
- Sansone, N.M.S.; Boschiero, M.N.; Marson, F.A.L. Dengue Outbreaks in Brazil and Latin America: The New and Continuing Challenges. Int J Infect Dis 2024, 147, 107192. [CrossRef]
- Burattini, M.N.; Lopez, L.F.; Coutinho, F.A.B.; Siqueira, J.B., Jr; Homsani, S.; Sarti, E.; Massad, E. Age and Regional Differences in Clinical Presentation and Risk of Hospitalization for Dengue in Brazil, 2000-2014. Clinics (Sao Paulo) 2016, 71, 455–463. [CrossRef]
- Paixão, E.S.; Costa, M. da C.N.; Rodrigues, L.C.; Rasella, D.; Cardim, L.L.; Brasileiro, A.C.; Teixeira, M.G.L.C. Trends and Factors Associated with Dengue Mortality and Fatality in Brazil. Rev Soc Bras Med Trop 2015, 48, 399–405. [CrossRef]
- Yung, C.-F.; Lee, K.-S.; Thein, T.-L.; Tan, L.-K.; Gan, V.C.; Wong, J.G.X.; Lye, D.C.; Ng, L.-C.; Leo, Y.-S. Dengue Serotype-Specific Differences in Clinical Manifestation, Laboratory Parameters and Risk of Severe Disease in Adults, Singapore. Am. J. Trop. Med. Hyg. 2015, 92, 999–1005. [CrossRef]
- Ten Bosch, Q.A.; Clapham, H.E.; Lambrechts, L.; Duong, V.; Buchy, P.; Althouse, B.M.; Lloyd, A.L.; Waller, L.A.; Morrison, A.C.; Kitron, U.; et al. Contributions from the Silent Majority Dominate Dengue Virus Transmission. PLoS Pathog 2018, 14, e1006965. [CrossRef]
- Duong, V.; Lambrechts, L.; Paul, R.E.; Ly, S.; Lay, R.S.; Long, K.C.; Huy, R.; Tarantola, A.; Scott, T.W.; Sakuntabhai, A.; et al. Asymptomatic Humans Transmit Dengue Virus to Mosquitoes. Proceedings of the National Academy of Sciences 2015, 112, 14688–14693. [CrossRef]
- Bos, S.; Zambrana, J.V.; Duarte, E.; Graber, A.L.; Huffaker, J.; Montenegro, C.; Premkumar, L.; Gordon, A.; Kuan, G.; Balmaseda, A.; et al. Serotype-Specific Epidemiological Patterns of Inapparent versus Symptomatic Primary Dengue Virus Infections: A 17-Year Cohort Study in Nicaragua. Lancet Infect Dis 2024. [CrossRef]
- Vicente, C.R.; Herbinger, K.-H.; Fröschl, G.; Malta Romano, C.; de Souza Areias Cabidelle, A.; Cerutti Junior, C. Serotype Influences on Dengue Severity: A Cross-Sectional Study on 485 Confirmed Dengue Cases in Vitória, Brazil. BMC Infect Dis 2016, 16, 320. [CrossRef]
- Henrique Ferreira Sucupira, P.; Silveira Ferreira, M.; Santos Coutinho-da-Silva, M.; Alves Bicalho, K.; Carolina Campi-Azevedo, A.; Pedro Brito-de-Sousa, J.; Peruhype-Magalhães, V.; Rios, M.; Konduru, K.; Teixeira-Carvalho, A.; et al. Serotype-Associated Immune Response and Network Immunoclusters in Children and Adults during Acute Dengue Virus Infection. Cytokine 2023, 169, 156306. [CrossRef]
- Rowe, E.K.; Leo, Y.-S.; Wong, J.G.X.; Thein, T.-L.; Gan, V.C.; Lee, L.K.; Lye, D.C. Challenges in Dengue Fever in the Elderly: Atypical Presentation and Risk of Severe Dengue and Hospital-Acquired Infection [corrected]. PLoS Negl. Trop. Dis. 2014, 8, e2777. [CrossRef]
- Lin, C.-H.; Schiøler, K.L.; Jepsen, M.R.; Ho, C.-K.; Li, S.-H.; Konradsen, F. Dengue Outbreaks in High-Income Area, Kaohsiung City, Taiwan, 2003-2009. Emerg. Infect. Dis. 2012, 18, 1603–1611. [CrossRef]
- Paz-Bailey, G.; Sánchez-González, L.; Torres-Velasquez, B.; Jones, E.S.; Perez-Padilla, J.; Sharp, T.M.; Lorenzi, O.; Delorey, M.; Munoz-Jordan, J.L.; Tomashek, K.M.; et al. Predominance of Severe Plasma Leakage in Pediatric Patients With Severe Dengue in Puerto Rico. J. Infect. Dis. 2022, 226, 1949–1958. [CrossRef]
- Hober, D.; Poli, L.; Roblin, B.; Gestas, P.; Chungue, E.; Granic, G.; Imbert, P.; Pecarere, J.L.; Vergez-Pascal, R.; Wattre, P. Serum Levels of Tumor Necrosis Factor-Alpha (TNF-Alpha), Interleukin-6 (IL-6), and Interleukin-1 Beta (IL-1 Beta) in Dengue-Infected Patients. Am. J. Trop. Med. Hyg. 1993, 48, 324–331. [CrossRef]
- Soo, K.-M.; Khalid, B.; Ching, S.-M.; Chee, H.-Y. Meta-Analysis of Dengue Severity during Infection by Different Dengue Virus Serotypes in Primary and Secondary Infections. PLoS One 2016, 11, e0154760. [CrossRef]
- Estofolete, C.F.; Versiani, A.F.; Dourado, F.S.; Milhim, B.H.G.A.; Pacca, C.C.; Silva, G.C.D.; Zini, N.; Santos, B.F.D.; Gandolfi, F.A.; Mistrão, N.F.B.; et al. Influence of Previous Zika Virus Infection on Acute Dengue Episode. PLoS Negl. Trop. Dis. 2023, 17, e0011710. [CrossRef]
- Musso, D.; Ko, A.I.; Baud, D. Zika Virus Infection - After the Pandemic. N. Engl. J. Med. 2019, 381, 1444–1457. [CrossRef]
- Zhang, Y.; Liu, X.; Wu, Z.; Feng, S.; Lu, K.; Zhu, W.; Sun, H.; Niu, G. Oropouche Virus: A Neglected Global Arboviral Threat. Virus Res. 2024, 341, 199318. [CrossRef]
- Mohapatra, R.K.; Mishra, S.; Satapathy, P.; Kandi, V.; Tuglo, L.S. Surging Oropouche Virus (OROV) Cases in the Americas: A Public Health Challenge. New Microbes New Infect 2024, 59, 101243. [CrossRef]
- Public Health Risk Assessment Related to Oropouche Virus (OROV) in the Region of the Americas, 9 February 2024 Available online: https://reliefweb.int/report/world/public-health-risk-assessment-related-oropouche-virus-orov-region-americas-9-february-2024 (accessed on 18 June 2024).
- B A Seixas, J.; Giovanni Luz, K.; Pinto Junior, V. [Clinical Update on Diagnosis, Treatment and Prevention of Dengue]. Acta Med. Port. 2024, 37, 126–135. [CrossRef]
- Rajapakse, S.; de Silva, N.L.; Weeratunga, P.; Rodrigo, C.; Fernando, S.D. Prophylactic and Therapeutic Interventions for Bleeding in Dengue: A Systematic Review. Trans. R. Soc. Trop. Med. Hyg. 2017, 111, 433–439. [CrossRef]
- Jasamai, M.; Yap, W.B.; Sakulpanich, A.; Jaleel, A. Current Prevention and Potential Treatment Options for Dengue Infection. J. Pharm. Pharm. Sci. 2019, 22, 440–456. [CrossRef]
- Silva, N.M.; Santos, N.C.; Martins, I.C. Dengue and Zika Viruses: Epidemiological History, Potential Therapies, and Promising Vaccines. Trop Med Infect Dis 2020, 5. [CrossRef]
- Miner, J.J.; Diamond, M.S. Zika Virus Pathogenesis and Tissue Tropism. Cell Host Microbe 2017, 21, 134–142. [CrossRef]
- Begum, F.; Das, S.; Mukherjee, D.; Mal, S.; Ray, U. Insight into the Tropism of Dengue Virus in Humans. Viruses 2019, 11. [CrossRef]
- BRASIL Diretrizes Nacionais Para a Prevenção E Controle de Epidemias de Dengue. Brasília, DF: MS, 2009 Available online: http://bvsms.saude.gov.br/bvs/publicacoes/diretrizes_nacionais_prevencao_controle_dengue (accessed on 16 June 2024).
- PAHO Guidelines for the Clinical Diagnosis and Treatment of Dengue, Chikungunya, and Zika Available online: https://iris.paho.org/handle/10665.2/55867 (accessed on 9 September 2024).
- WHO Dengue Guias Para El Diagnóstico, Tratamiento, Prevención Y Control: Nueva Edición Available online: https://iris.who.int/handle/10665/44504 (accessed on 9 September 2024).
- Stanley, S.M.; Khera, H.K.; Chandrasingh, S.; George, C.E.; Mishra, R.K. A Comprehensive Review of Dengue with a Focus on Emerging Solutions for Precision and Timely Detection. Int. J. Biol. Macromol. 2024, 254, 127613. [CrossRef]
- BRASIL Ministério da Saúde-Saúde de A a Z-Dengue Available online: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/d/dengue/dengue (accessed on 16 June 2024).
- OPAS Alerta Epidemiológico-Aumento de casos de dengue na Região das Américas Available online: https://www.paho.org/pt/documentos/alerta-epidemiologico-aumento-casos-dengue-na-regiao-das-americas-16-fevereiro-2024 (accessed on 16 June 2024).
- BRASIL Ministério da Saúde entrega nova remessa de vacinas da dengue Available online: https://www.gov.br/saude/pt-br/assuntos/noticias/2024/maio/ministerio-da-saude-entrega-nova-remessa-de-vacinas-da-dengue (accessed on 16 June 2024).
- BRASIL Ministério da Saúde elabora plano para enfrentamento da dengue 2024/2025 Available online: https://www.gov.br/saude/pt-br/assuntos/noticias/2024/maio/ministerio-da-saude-elabora-plano-para-enfrentamento-da-dengue-2024-2025 (accessed on 16 June 2024).
- Website Available online: BRASIL. Combate ao mosquito. Ministério da Saúde https://www.gov.br/saude/pt-br/campanhas-da-saude/2023/combate-ao-mosquito/combate-ao-mosquito (2023).
- Muir, L.E.; Thorne, M.J.; Kay, B.H. Aedes Aegypti (Diptera: Culicidae) Vision: Spectral Sensitivity and Other Perceptual Parameters of the Female Eye. J Med Entomol 1992, 29, 278–281. [CrossRef]
- Taniyama, K.; Hori, M. Lethal Effect of Blue Light on Asian Tiger Mosquito, Aedes Albopictus (Diptera: Culicidae). Sci. Rep. 2022, 12, 10100. [CrossRef]
- Salles, T.; Corrêa, I.; Guimarães-Ribeiro, V.; Carvalho, E.; Moreira, M. LED Colour Trap for Aedes Aegypti Control. Recent Pat Biotechnol 2021, 15, 227–331. [CrossRef]
- BRASIL Saiba como é utilizado o fumacê no combate ao mosquito da dengue Available online: https://www.gov.br/saude/pt-br/assuntos/noticias/2024/marco/saiba-como-e-utilizado-o-fumace-no-combate-ao-mosquito-da-dengue (accessed on 16 June 2024).
- Pinto, S.B.; Riback, T.I.S.; Sylvestre, G.; Costa, G.; Peixoto, J.; Dias, F.B.S.; Tanamas, S.K.; Simmons, C.P.; Dufault, S.M.; Ryan, P.A.; et al. Effectiveness of Wolbachia-Infected Mosquito Deployments in Reducing the Incidence of Dengue and Other Aedes-Borne Diseases in Niterói, Brazil: A Quasi-Experimental Study. PLoS Negl Trop Dis 2021, 15, e0009556. [CrossRef]
- Ribeiro Dos Santos, G.; Durovni, B.; Saraceni, V.; Souza Riback, T.I.; Pinto, S.B.; Anders, K.L.; Moreira, L.A.; Salje, H. Estimating the Effect of the wMel Release Programme on the Incidence of Dengue and Chikungunya in Rio de Janeiro, Brazil: A Spatiotemporal Modelling Study. Lancet Infect Dis 2022, 22, 1587–1595. [CrossRef]
- Lopez, S.B.G.; Guimarães-Ribeiro, V.; Rodriguez, J.V.G.; Dorand, F.A.P.S.; Salles, T.S.; Sá-Guimarães, T.E.; Alvarenga, E.S.L.; Melo, A.C.A.; Almeida, R.V.; Moreira, M.F. RNAi-Based Bioinsecticide for Aedes Mosquito Control. Sci Rep 2019, 9, 4038. [CrossRef]
- Utarini, A.; Indriani, C.; Ahmad, R.A.; Tantowijoyo, W.; Arguni, E.; Ansari, M.R.; Supriyati, E.; Wardana, D.S.; Meitika, Y.; Ernesia, I.; et al. Efficacy of Wolbachia-Infected Mosquito Deployments for the Control of Dengue. N Engl J Med 2021, 384, 2177–2186. [CrossRef]
- Velez, I.D.; Tanamas, S.K.; Arbelaez, M.P.; Kutcher, S.C.; Duque, S.L.; Uribe, A.; Zuluaga, L.; Martínez, L.; Patiño, A.C.; Barajas, J.; et al. Reduced Dengue Incidence Following City-Wide wMel Wolbachia Mosquito Releases throughout Three Colombian Cities: Interrupted Time Series Analysis and a Prospective Case-Control Study. PLoS Negl Trop Dis 2023, 17, e0011713. [CrossRef]
- BRASIL Você sabe o que é o Método Wolbachia? Available online: https://www.gov.br/saude/pt-br/assuntos/saude-com-ciencia/noticias/2024/maio/voce-sabe-o-que-e-o-metodo-wolbachia (accessed on 16 June 2024).
- World Mosquito Program Sobre O Método Wolbachia Available online: https://www.worldmosquitoprogram.org/sobre-o-metodo-wolbachia (accessed on 16 June 2024).
- BRASIL Ministério da Saúde incorpora vacina contra a dengue no SUS Available online: https://www.gov.br/saude/pt-br/assuntos/noticias/2023/dezembro/ministerio-da-saude-incorpora-vacina-contra-a-dengue-no-sus (accessed on 16 June 2024).
- Butantan, I. Instituto Butantan-Portal Do Butantan Available online: https://butantan.gov.br/covid/butantan-tira-duvida/tira-duvida-noticias/vacina-da-dengue-deve-proteger-de-todos-os-subtipos-da-doenca--entenda-a-complexidade-do-ensaio-clinico (accessed on 2024).
- Kallás, E.G.; Cintra, M.A.T.; Moreira, J.A.; Patiño, E.G.; Braga, P.E.; Tenório, J.C.V.; Infante, V.; Palacios, R.; de Lacerda, M.V.G.; Batista Pereira, D.; et al. Live, Attenuated, Tetravalent Butantan-Dengue Vaccine in Children and Adults. N. Engl. J. Med. 2024, 390, 397–408. [CrossRef]
- Buerano, C.C.; Morita, K. Single Dose of Dengvaxia Vaccine: Is It a Cause for Alarm? Lancet Infect. Dis. 2024, 24, 670–671. [CrossRef]
- Forrat, R.; Dayan, G.H.; DiazGranados, C.A.; Bonaparte, M.; Laot, T.; Capeding, M.R.; Sanchez, L.; Coronel, D.L.; Reynales, H.; Chansinghakul, D.; et al. Analysis of Hospitalized and Severe Dengue Cases Over the 6 Years of Follow-up of the Tetravalent Dengue Vaccine (CYD-TDV) Efficacy Trials in Asia and Latin America. Clin. Infect. Dis. 2021, 73, 1003–1012. [CrossRef]
- Turner, M.; Papadimitriou, A.; Winkle, P.; Segall, N.; Levin, M.; Doust, M.; Johnson, C.; Lucksinger, G.; Fierro, C.; Pickrell, P.; et al. Immunogenicity and Safety of Lyophilized and Liquid Dengue Tetravalent Vaccine Candidate Formulations in Healthy Adults: A Randomized, Phase 2 Clinical Trial. Hum. Vaccin. Immunother. 2020, 16, 2456–2464. [CrossRef]
- Thomas, S.J.; Yoon, I.-K. A Review of Dengvaxia®: Development to Deployment. Hum. Vaccin. Immunother. 2019, 15, 2295–2314. [CrossRef]
- Guirakhoo, F.; Weltzin, R.; Chambers, T.J.; Zhang, Z.X.; Soike, K.; Ratterree, M.; Arroyo, J.; Georgakopoulos, K.; Catalan, J.; Monath, T.P. Recombinant Chimeric Yellow Fever-Dengue Type 2 Virus Is Immunogenic and Protective in Nonhuman Primates. J. Virol. 2000, 74, 5477–5485. [CrossRef]
- Guirakhoo, F.; Arroyo, J.; Pugachev, K.V.; Miller, C.; Zhang, Z.X.; Weltzin, R.; Georgakopoulos, K.; Catalan, J.; Ocran, S.; Soike, K.; et al. Construction, Safety, and Immunogenicity in Nonhuman Primates of a Chimeric Yellow Fever-Dengue Virus Tetravalent Vaccine. J. Virol. 2001, 75, 7290–7304. [CrossRef]
- Torres-Flores, J.M.; Reyes-Sandoval, A.; Salazar, M.I. Dengue Vaccines: An Update. BioDrugs 2022, 36, 325–336. [CrossRef]
- Villar, L.; Dayan, G.H.; Arredondo-García, J.L.; Rivera, D.M.; Cunha, R.; Deseda, C.; Reynales, H.; Costa, M.S.; Morales-Ramírez, J.O.; Carrasquilla, G.; et al. Efficacy of a Tetravalent Dengue Vaccine in Children in Latin America. N. Engl. J. Med. 2015, 372, 113–123. [CrossRef]
- Mendoza, R.U.; Dayrit, M.M.; Alfonso, C.R.; Ong, M.M.A. Public Trust and the COVID-19 Vaccination Campaign: Lessons from the Philippines as It Emerges from the Dengvaxia Controversy. Int. J. Health Plann. Manage. 2021, 36, 2048–2055. [CrossRef]
- Patel, S.S.; Winkle, P.; Faccin, A.; Nordio, F.; LeFevre, I.; Tsoukas, C.G. An Open-Label, Phase 3 Trial of TAK-003, a Live Attenuated Dengue Tetravalent Vaccine, in Healthy US Adults: Immunogenicity and Safety When Administered during the Second Half of a 24-Month Shelf-Life. Hum. Vaccin. Immunother. 2023, 19, 2254964. [CrossRef]
- Jain, S.; Vimal, N.; Angmo, N.; Sengupta, M.; Thangaraj, S. Dengue Vaccination: Towards a New Dawn of Curbing Dengue Infection. Immunol. Invest. 2023, 52, 1096–1149. [CrossRef]
- Sáez-Llorens, X.; Biswal, S.; Borja-Tabora, C.; Fernando, L.; Liu, M.; Wallace, D.; Folschweiller, N.; Reynales, H.; LeFevre, I.; TIDES Study Group Effect of the Tetravalent Dengue Vaccine TAK-003 on Sequential Episodes of Symptomatic Dengue. Am. J. Trop. Med. Hyg. 2023, 108, 722–726. [CrossRef]
- Bengolea, A.; Scigliano, C.; Ramos-Rojas, J.T.; Rada, G.; Catalano, H.N.; Izcovich, A. Effectiveness and Safety of the Tetravalent TAK-003 Dengue Vaccine: A Systematic Review. Medicina 2024, 84, 689–707.
- Angelin, M.; Sjölin, J.; Kahn, F.; Ljunghill Hedberg, A.; Rosdahl, A.; Skorup, P.; Werner, S.; Woxenius, S.; Askling, H.H. Qdenga® - A Promising Dengue Fever Vaccine; Can It Be Recommended to Non-Immune Travelers? Travel Med. Infect. Dis. 2023, 54, 102598. [CrossRef]
- Sirivichayakul, C.; Barranco-Santana, E.A.; Esquilin-Rivera, I.; Oh, H.M.L.; Raanan, M.; Sariol, C.A.; Shek, L.P.; Simasathien, S.; Smith, M.K.; Velez, I.D.; et al. Safety and Immunogenicity of a Tetravalent Dengue Vaccine Candidate in Healthy Children and Adults in Dengue-Endemic Regions: A Randomized, Placebo-Controlled Phase 2 Study. J. Infect. Dis. 2016, 213, 1562–1572. [CrossRef]
- Thomas, S.J. Is New Dengue Vaccine Efficacy Data a Relief or Cause for Concern? NPJ Vaccines 2023, 8, 55. [CrossRef]
- Flacco, M.E.; Bianconi, A.; Cioni, G.; Fiore, M.; Calò, G.L.; Imperiali, G.; Orazi, V.; Tiseo, M.; Troia, A.; Rosso, A.; et al. Immunogenicity, Safety and Efficacy of the Dengue Vaccine TAK-003: A Meta-Analysis. Vaccines (Basel) 2024, 12. [CrossRef]
- Whitehead, S.S. Development of TV003/TV005, a Single Dose, Highly Immunogenic Live Attenuated Dengue Vaccine; What Makes This Vaccine Different from the Sanofi-Pasteur CYDTM Vaccine? Expert Rev. Vaccines 2016, 15, 509–517. [CrossRef]
- Weiskopf, D.; Angelo, M.A.; Bangs, D.J.; Sidney, J.; Paul, S.; Peters, B.; de Silva, A.D.; Lindow, J.C.; Diehl, S.A.; Whitehead, S.; et al. The Human CD8+ T Cell Responses Induced by a Live Attenuated Tetravalent Dengue Vaccine Are Directed against Highly Conserved Epitopes. J. Virol. 2015, 89, 120–128. [CrossRef]
- Kallas, E.G.; Precioso, A.R.; Palacios, R.; Thomé, B.; Braga, P.E.; Vanni, T.; Campos, L.M.A.; Ferrari, L.; Mondini, G.; da Graça Salomão, M.; et al. Safety and Immunogenicity of the Tetravalent, Live-Attenuated Dengue Vaccine Butantan-DV in Adults in Brazil: A Two-Step, Double-Blind, Randomised Placebo-Controlled Phase 2 Trial. Lancet Infect. Dis. 2020, 20, 839–850. [CrossRef]
- Angelo, M.A.; Grifoni, A.; O’Rourke, P.H.; Sidney, J.; Paul, S.; Peters, B.; de Silva, A.D.; Phillips, E.; Mallal, S.; Diehl, S.A.; et al. Human CD4 T Cell Responses to an Attenuated Tetravalent Dengue Vaccine Parallel Those Induced by Natural Infection in Magnitude, HLA Restriction, and Antigen Specificity. J. Virol. 2017, 91. [CrossRef]
- Nogueira, M.L.; Cintra, M.A.T.; Moreira, J.A.; Patiño, E.G.; Braga, P.E.; Tenório, J.C.V.; de Oliveira Alves, L.B.; Infante, V.; Silveira, D.H.R.; de Lacerda, M.V.G.; et al. Efficacy and Safety of Butantan-DV in Participants Aged 2-59 Years through an Extended Follow-up: Results from a Double-Blind, Randomised, Placebo-Controlled, Phase 3, Multicentre Trial in Brazil. Lancet Infect. Dis. 2024. [CrossRef]
- Muller, D.A.; Depelsenaire, A.C.I.; Young, P.R. Clinical and Laboratory Diagnosis of Dengue Virus Infection. J. Infect. Dis. 2017, 215, S89–S95. [CrossRef]
- Gregory, C.J.; Lorenzi, O.D.; Colón, L.; García, A.S.; Santiago, L.M.; Rivera, R.C.; Bermúdez, L.J.C.; Báez, F.O.; Aponte, D.V.; Tomashek, K.M.; et al. Utility of the Tourniquet Test and the White Blood Cell Count to Differentiate Dengue among Acute Febrile Illnesses in the Emergency Room. PLoS Negl. Trop. Dis. 2011, 5, e1400. [CrossRef]
- Kalayanarooj, S.; Vaughn, D.W.; Nimmannitya, S.; Green, S.; Suntayakorn, S.; Kunentrasai, N.; Viramitrachai, W.; Ratanachu-eke, S.; Kiatpolpoj, S.; Innis, B.L.; et al. Early Clinical and Laboratory Indicators of Acute Dengue Illness. J. Infect. Dis. 1997, 176, 313–321. [CrossRef]
- Montes y Gómez, M.; Escalante, H.J.; Segura, A.; de Dios Murillo, J. Advances in Artificial Intelligence - IBERAMIA 2016: 15th Ibero-American Conference on AI, San José, Costa Rica, November 23-25, 2016, Proceedings; Springer, 2016; ISBN 9783319479552.
- Furlan, N.B.; Tukasan, C.; Estofolete, C.F.; Nogueira, M.L.; da Silva, N.S. Low Sensitivity of the Tourniquet Test for Differential Diagnosis of Dengue: An Analysis of 28,000 Trials in Patients. BMC Infect. Dis. 2016, 16, 627. [CrossRef]
- Mayxay, M.; Phetsouvanh, R.; Moore, C.E.; Chansamouth, V.; Vongsouvath, M.; Sisouphone, S.; Vongphachanh, P.; Thaojaikong, T.; Thongpaseuth, S.; Phongmany, S.; et al. Predictive Diagnostic Value of the Tourniquet Test for the Diagnosis of Dengue Infection in Adults. Trop. Med. Int. Health 2011, 16, 127–133. [CrossRef]
- St John, A.L.; Rathore, A.P.S. Adaptive Immune Responses to Primary and Secondary Dengue Virus Infections. Nat. Rev. Immunol. 2019, 19, 218–230. [CrossRef]
- Tang, K.F.; Ooi, E.E. Diagnosis of Dengue: An Update. Expert Rev. Anti. Infect. Ther. 2012, 10, 895–907. [CrossRef]
- Avrami, S.; Hoffman, T.; Meltzer, E.; Lustig, Y.; Schwartz, E. Comparison of Clinical and Laboratory Parameters of Primary vs Secondary Dengue Fever in Travellers. J. Travel Med. 2023, 30. [CrossRef]
- Fisher, R.; Lustig, Y.; Sklan, E.H.; Schwartz, E. The Role of NS1 Protein in the Diagnosis of Flavivirus Infections. Viruses 2023, 15. [CrossRef]
- Lanciotti, R.S.; Calisher, C.H.; Gubler, D.J.; Chang, G.J.; Vorndam, A.V. Rapid Detection and Typing of Dengue Viruses from Clinical Samples by Using Reverse Transcriptase-Polymerase Chain Reaction. J. Clin. Microbiol. 1992, 30, 545–551. [CrossRef]
- Chien, L.-J.; Liao, T.-L.; Shu, P.-Y.; Huang, J.-H.; Gubler, D.J.; Chang, G.-J.J. Development of Real-Time Reverse Transcriptase PCR Assays to Detect and Serotype Dengue Viruses. J Clin Microbiol 2006, 44, 1295–1304. [CrossRef]
- Iani, F.C. de M.; Caetano, A.C.B.; Cocovich, J.C.W.; Amâncio, F.F.; Pereira, M.A.; Adelino, T.É.R.; Caldas, S.; Silva, M.V.F.; Pereira, G. de C.; Duarte, M.M. Dengue Diagnostics: Serious Inaccuracies Are Likely to Occur If Pre-Analytical Conditions Are Not Strictly Followed. Mem. Inst. Oswaldo Cruz 2021, 115, e200287. [CrossRef]
- Najioullah, F.; Viron, F.; Césaire, R. Evaluation of Four Commercial Real-Time RT-PCR Kits for the Detection of Dengue Viruses in Clinical Samples. Virol J 2014, 11, 164. [CrossRef]
- Monitoring and Improving the Sensitivity of Dengue Nested RT-PCR Used in Longitudinal Surveillance in Thailand. J. Clin. Virol. 2015, 63, 25–31. [CrossRef]
- Cecchetto, J.; Fernandes, F.C.B.; Lopes, R.; Bueno, P.R. The Capacitive Sensing of NS1 Flavivirus Biomarker. Biosens. Bioelectron. 2017, 87, 949–956. [CrossRef]
- Rastogi, M.; Sharma, N.; Singh, S.K. Flavivirus NS1: A Multifaceted Enigmatic Viral Protein. Virol. J. 2016, 13, 131. [CrossRef]
- Peeling, R.W.; Artsob, H.; Pelegrino, J.L.; Buchy, P.; Cardosa, M.J.; Devi, S.; Enria, D.A.; Farrar, J.; Gubler, D.J.; Guzman, M.G.; et al. Evaluation of Diagnostic Tests: Dengue. Nat. Rev. Microbiol. 2010, 8, S30–S38. [CrossRef]
- Andries, A.-C.; Duong, V.; Ong, S.; Ros, S.; Sakuntabhai, A.; Horwood, P.; Dussart, P.; Buchy, P. Evaluation of the Performances of Six Commercial Kits Designed for Dengue NS1 and Anti-Dengue IgM, IgG and IgA Detection in Urine and Saliva Clinical Specimens. BMC Infect. Dis. 2016, 16, 1–9. [CrossRef]
- Lanciotti, R.S.; Kosoy, O.L.; Laven, J.J.; Velez, J.O.; Lambert, A.J.; Johnson, A.J.; Stanfield, S.M.; Duffy, M.R. Genetic and Serologic Properties of Zika Virus Associated with an Epidemic, Yap State, Micronesia, 2007. Emerg. Infect. Dis. 2008, 14, 1232–1239. [CrossRef]
- Changal, K.H.; Raina, A.H.; Raina, A.; Raina, M.; Bashir, R.; Latief, M.; Mir, T.; Changal, Q.H. Differentiating Secondary from Primary Dengue Using IgG to IgM Ratio in Early Dengue: An Observational Hospital Based Clinico-Serological Study from North India. BMC Infect. Dis. 2016, 16, 1–7. [CrossRef]
- Bäck, A.T.; Lundkvist, A. Dengue Viruses - an Overview. Infect. Ecol. Epidemiol. 2013, 3. [CrossRef]
- Ayukekbong, J.A.; Oyero, O.G.; Nnukwu, S.E.; Mesumbe, H.N.; Fobisong, C.N. Value of Routine Dengue Diagnosis in Endemic Countries. World J Virol 2017, 6, 9–16. [CrossRef]
- Thomas, S.J.; Nisalak, A.; Anderson, K.B.; Libraty, D.H.; Kalayanarooj, S.; Vaughn, D.W.; Putnak, R.; Gibbons, R.V.; Jarman, R.; Endy, T.P. Dengue Plaque Reduction Neutralization Test (PRNT) in Primary and Secondary Dengue Virus Infections: How Alterations in Assay Conditions Impact Performance. Am. J. Trop. Med. Hyg. 2009, 81, 825–833. [CrossRef]
- Antunes, A.C.; Oliveira, G.L.; Nunes, L.I.; Guedes Filho, L.A.; Prado, R.S.; Henriques, H.R.; Vieira, A.J.C. Evaluation of the Diagnostic Value of the Tourniquet Test in Predicting Severe Dengue Cases in a Population from Belo Horizonte, State of Minas Gerais, Brazil. Rev. Soc. Bras. Med. Trop. 2013, 46, 542–546. [CrossRef]
- Grande, A.J.; Reid, H.; Thomas, E.; Foster, C.; Darton, T.C. Tourniquet Test for Dengue Diagnosis: Systematic Review and Meta-Analysis of Diagnostic Test Accuracy. PLoS Negl. Trop. Dis. 2016, 10. [CrossRef]
- Jarman, R.G.; Nisalak, A.; Anderson, K.B.; Klungthong, C.; Thaisomboonsuk, B.; Kaneechit, W.; Kalayanarooj, S.; Gibbons, R.V. Factors Influencing Dengue Virus Isolation by C6/36 Cell Culture and Mosquito Inoculation of Nested PCR-Positive Clinical Samples. Am. J. Trop. Med. Hyg. 2011, 84, 218. [CrossRef]
- Tricou, V.; Vu, H.T.T.; Quynh, N.V.N.; Nguyen, C.V.V.; Tran, H.T.; Farrar, J.; Wills, B.; Simmons, C.P. Comparison of Two Dengue NS1 Rapid Tests for Sensitivity, Specificity and Relationship to Viraemia and Antibody Responses. BMC Infect. Dis. 2010, 10, 1–8. [CrossRef]
- Luvira, V.; Thawornkuno, C.; Lawpoolsri, S.; Thippornchai, N.; Duangdee, C.; Ngamprasertchai, T.; Leaungwutiwong, P. Diagnostic Performance of Dengue NS1 and Antibodies by Serum Concentration Technique. Tropical Medicine and Infectious Disease 2023, 8. [CrossRef]
- Laboratory Diagnosis of Primary and Secondary Dengue Infection. J. Clin. Virol. 2004, 31, 179–184. [CrossRef]
- Jang, W.S.; Kwak, S.Y.; May, W.L.; Yang, D.J.; Nam, J.; Lim, C.S. Comparative Evaluation of Three Dengue Duo Rapid Test Kits to Detect NS1, IgM, and IgG Associated with Acute Dengue in Children in Myanmar. PLoS One 2019, 14, e0213451. [CrossRef]
- Sah, R.; Srivastava, S.; Kumar, S.; Golmei, P.; Rahaman, S.A.; Mehta, R.; Ferraz, C.; Apostolopoulos, V.; Rodriguez-Morales, A.J. Oropouche Fever Outbreak in Brazil: An Emerging Concern in Latin America. Lancet Microbe 2024. [CrossRef]
- Sciancalepore, S.; Schneider, M.C.; Kim, J.; Galan, D.I.; Riviere-Cinnamond, A. Presence and Multi-Species Spatial Distribution of Oropouche Virus in Brazil within the One Health Framework. Trop Med Infect Dis 2022, 7. [CrossRef]
- Emergence of Oropouche Fever in Latin America: A Narrative Review. Lancet Infect. Dis. 2024, 24, e439–e452. [CrossRef]
- PAHO Epidemiological Alert Oropouche in the Region of the Americas: Vertical Transmission Event under Investigation in Brazil - 17 July 2024 Available online: https://www.paho.org/en/documents/epidemiological-alert-oropouche-region-americas-vertical-transmission-event-under (accessed on 8 September 2024).
- das Neves Martins, F.E.; Chiang, J.O.; Nunes, B.T.D.; Ribeiro, B. de F.R.; Martins, L.C.; Casseb, L.M.N.; Henriques, D.F.; de Oliveira, C.S.; Maciel, E.L.N.; Azevedo, R. da S.; et al. Newborns with Microcephaly in Brazil and Potential Vertical Transmission of Oropouche Virus: A Case Series. Lancet Infect Dis 2024. [CrossRef]
- Garcia Filho, C.; Lima Neto, A.S.; Maia, A.M.P.C.; da Silva, L.O.R.; Cavalcante, R. da C.; Monteiro, H. da S.; Marques, K.C.A.; Oliveira, R. de S.; Gadelha, S. de A.C.; Nunes de Melo, D.; et al. A Case of Vertical Transmission of Oropouche Virus in Brazil. N Engl J Med 2024. [CrossRef]
- Feitoza, L.H.M.; de Carvalho, L.P.C.; da Silva, L.R.; Meireles, A.C.A.; Rios, F.G.F.; Silva, G.S.; de Paulo, P.F.M.; Pessoa, F.A.C.; de Medeiros, J.F.; Julião, G.R. Influence of Meteorological and Seasonal Parameters on the Activity of Culicoides Paraensis (Diptera: Ceratopogonidae), an Annoying Anthropophilic Biting Midge and Putative Vector of Oropouche Virus in Rondônia, Brazilian Amazon. Acta Trop. 2023, 243, 106928. [CrossRef]
- Febre do Oropouche Available online: https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/f/febre-do-oropouche (accessed on 18 June 2024).
- Silva-Júnior, E.F. da Oropouche Virus - The “Newest” Invisible Public Enemy? Bioorg. Med. Chem. 2024, 109, 117797. [CrossRef]
- Parra Barrera, E.L.; Reales-González, J.; Salas, D.; Reyes Santamaría, E.; Bello, S.; Rico, A.; Pardo, L.; Parra, E.; Rodriguez, K.; Alarcon, Z.; et al. Fatal Acute Undifferentiated Febrile Illness among Clinically Suspected Leptospirosis Cases in Colombia, 2016-2019. PLoS Negl. Trop. Dis. 2023, 17, e0011683. [CrossRef]
- Gaillet, M.; Pichard, C.; Restrepo, J.; Lavergne, A.; Perez, L.; Enfissi, A.; Abboud, P.; Lambert, Y.; Ma, L.; Monot, M.; et al. Outbreak of Oropouche Virus in French Guiana. Emerg. Infect. Dis. 2021, 27, 2711–2714. [CrossRef]
- Romero-Alvarez, D.; Escobar, L.E. Oropouche Fever, an Emergent Disease from the Americas. Microbes Infect. 2018, 20, 135–146. [CrossRef]
- Bastos, M. de S.; Figueiredo, L.T.M.; Naveca, F.G.; Monte, R.L.; Lessa, N.; Pinto de Figueiredo, R.M.; Gimaque, J.B. de L.; Pivoto João, G.; Ramasawmy, R.; Mourão, M.P.G. Identification of Oropouche Orthobunyavirus in the Cerebrospinal Fluid of Three Patients in the Amazonas, Brazil. Am. J. Trop. Med. Hyg. 2012, 86, 732–735. [CrossRef]
- Cardoso, B.F.; Serra, O.P.; Heinen, L.B. da S.; Zuchi, N.; Souza, V.C. de; Naveca, F.G.; Santos, M.A.M. dos; Slhessarenko, R.D. Detection of Oropouche Virus Segment S in Patients and inCulex Quinquefasciatus in the State of Mato Grosso, Brazil. Mem. Inst. Oswaldo Cruz 2015, 110, 745–754. [CrossRef]
- Sakkas, H.; Bozidis, P.; Franks, A.; Papadopoulou, C. Oropouche Fever: A Review. Viruses 2018, 10. [CrossRef]
- Dengue- Global Situation Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2023-DON498#:~:text=Dengue%20is%20not%20endemic%20in,%2C%20Italy%2C%20Portugal%20and%20Spain. (accessed on 28 May 2024).
- Aedes Invasive Mosquitoes - Current Known Distribution: October 2023 Available online: https://www.ecdc.europa.eu/en/publications-data/aedes-invasive-mosquitoes-current-known-distribution-october-2023 (accessed on 28 May 2024).
- Prudhomme, J.; Fontaine, A.; Lacour, G.; Gantier, J.-C.; Diancourt, L.; Velo, E.; Bino, S.; Reiter, P.; Mercier, A. The Native European Mosquito Species Can Transmit Chikungunya Virus. Emerg. Microbes Infect. 2019, 8, 962–972. [CrossRef]
- LaTourrette, K.; Garcia-Ruiz, H. Determinants of Virus Variation, Evolution, and Host Adaptation. Pathogens 2022, 11. [CrossRef]
- Autochthonous Vectorial Transmission of Dengue Virus in Mainland EU/EEA, 2010-Present Available online: https://www.ecdc.europa.eu/en/all-topics-z/dengue/surveillance-and-disease-data/autochthonous-transmission-dengue-virus-eueea (accessed on 28 May 2024).
- Naddaf, M. Mosquito-Borne Diseases Are Surging in Europe - How Worried Are Scientists? Nature 2024, 633, 749. [CrossRef]
- Singh, P.S.; Chaturvedi, H.K. A Retrospective Study of Environmental Predictors of Dengue in Delhi from 2015 to 2018 Using the Generalized Linear Model. Sci. Rep. 2022, 12, 8109. [CrossRef]
Figure 1.
Reproduction cycle of Aedes spp. and dengue transmission cycle. The reproduction cycle of Aedes spp. mosquitoes and the dengue transmission cycle involve several stages. Male and female mosquitoes mate (step 1), and female mosquitoes go for blood feeding for egg development (step 2). A female mosquito then bites an infected individual, acquiring the dengue virus (step 3 and 4). This infected mosquito subsequently bites multiple healthy individuals, transmitting the virus to them (step 5). These newly infected individuals then transmit the virus to additional mosquitoes that bite them. The female mosquito lays her eggs in stagnant water sources (step 6), where the eggs hatch into larvae and develop into new mosquitoes, perpetuating the cycle (step 7). Two types of vertical DENV transmission may occur: from an infected pregnant woman to her baby, which is rare [41], and natural vertical transmission of DENV in A. aegypti and A. albopictus mosquito populations serves as a mechanism for viral persistence in the environment during periods unfavorable for horizontal transmission [22,43,44,45]. This last process is an important maintenance strategy for DENV circulation, ensuring the virus remains within mosquito populations even when conditions limit transmission between mosquitoes and human hosts.
Figure 1.
Reproduction cycle of Aedes spp. and dengue transmission cycle. The reproduction cycle of Aedes spp. mosquitoes and the dengue transmission cycle involve several stages. Male and female mosquitoes mate (step 1), and female mosquitoes go for blood feeding for egg development (step 2). A female mosquito then bites an infected individual, acquiring the dengue virus (step 3 and 4). This infected mosquito subsequently bites multiple healthy individuals, transmitting the virus to them (step 5). These newly infected individuals then transmit the virus to additional mosquitoes that bite them. The female mosquito lays her eggs in stagnant water sources (step 6), where the eggs hatch into larvae and develop into new mosquitoes, perpetuating the cycle (step 7). Two types of vertical DENV transmission may occur: from an infected pregnant woman to her baby, which is rare [41], and natural vertical transmission of DENV in A. aegypti and A. albopictus mosquito populations serves as a mechanism for viral persistence in the environment during periods unfavorable for horizontal transmission [22,43,44,45]. This last process is an important maintenance strategy for DENV circulation, ensuring the virus remains within mosquito populations even when conditions limit transmission between mosquitoes and human hosts.
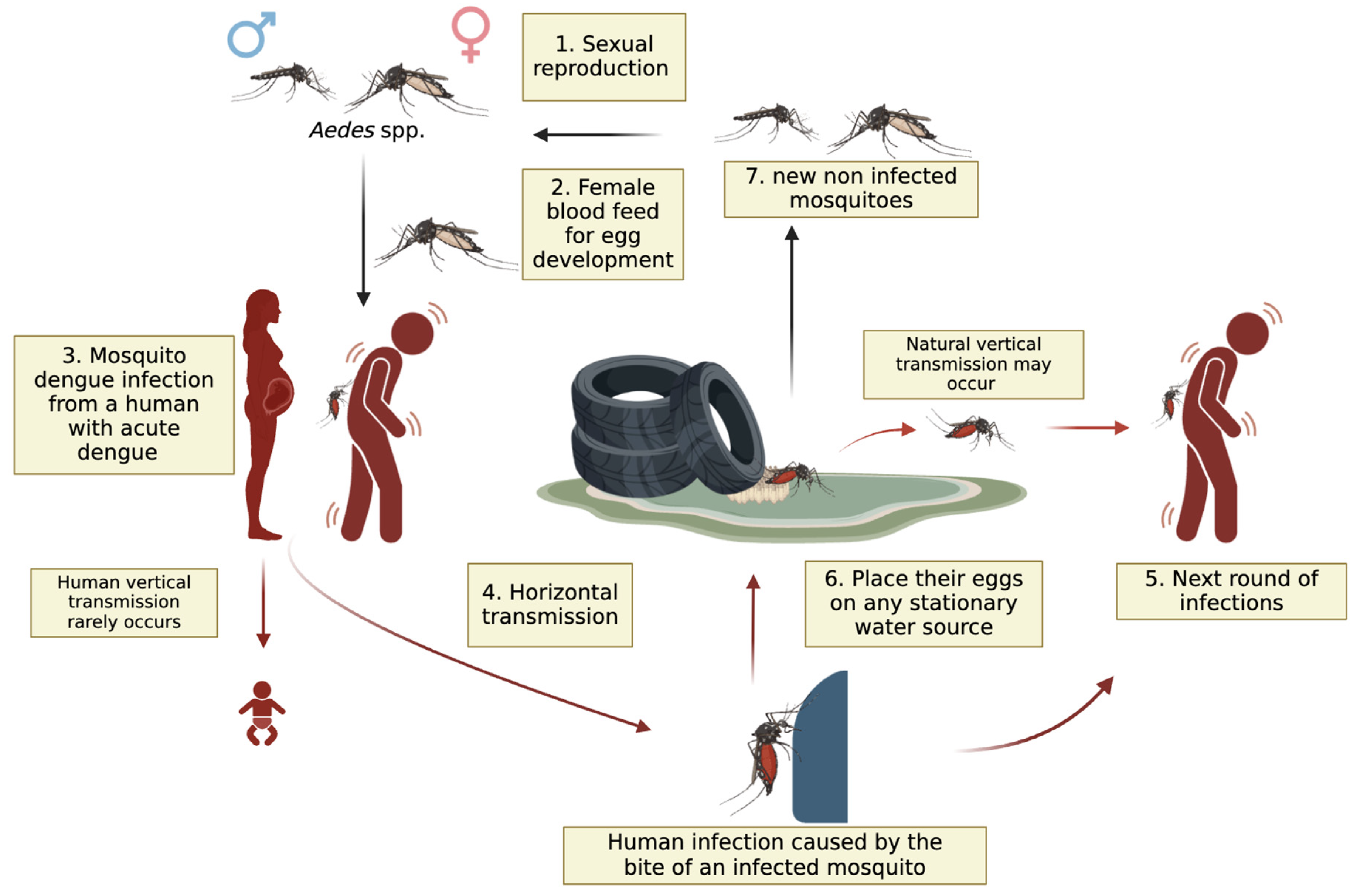
Figure 6.
Aedes albopictus distribution in Europe. Established populations in the Mediterranean region highlight potential endemic hotspots for dengue transmission, driven by increasingly favourable climate conditions for the proliferation of Aedes species [155].
Figure 6.
Aedes albopictus distribution in Europe. Established populations in the Mediterranean region highlight potential endemic hotspots for dengue transmission, driven by increasingly favourable climate conditions for the proliferation of Aedes species [155].
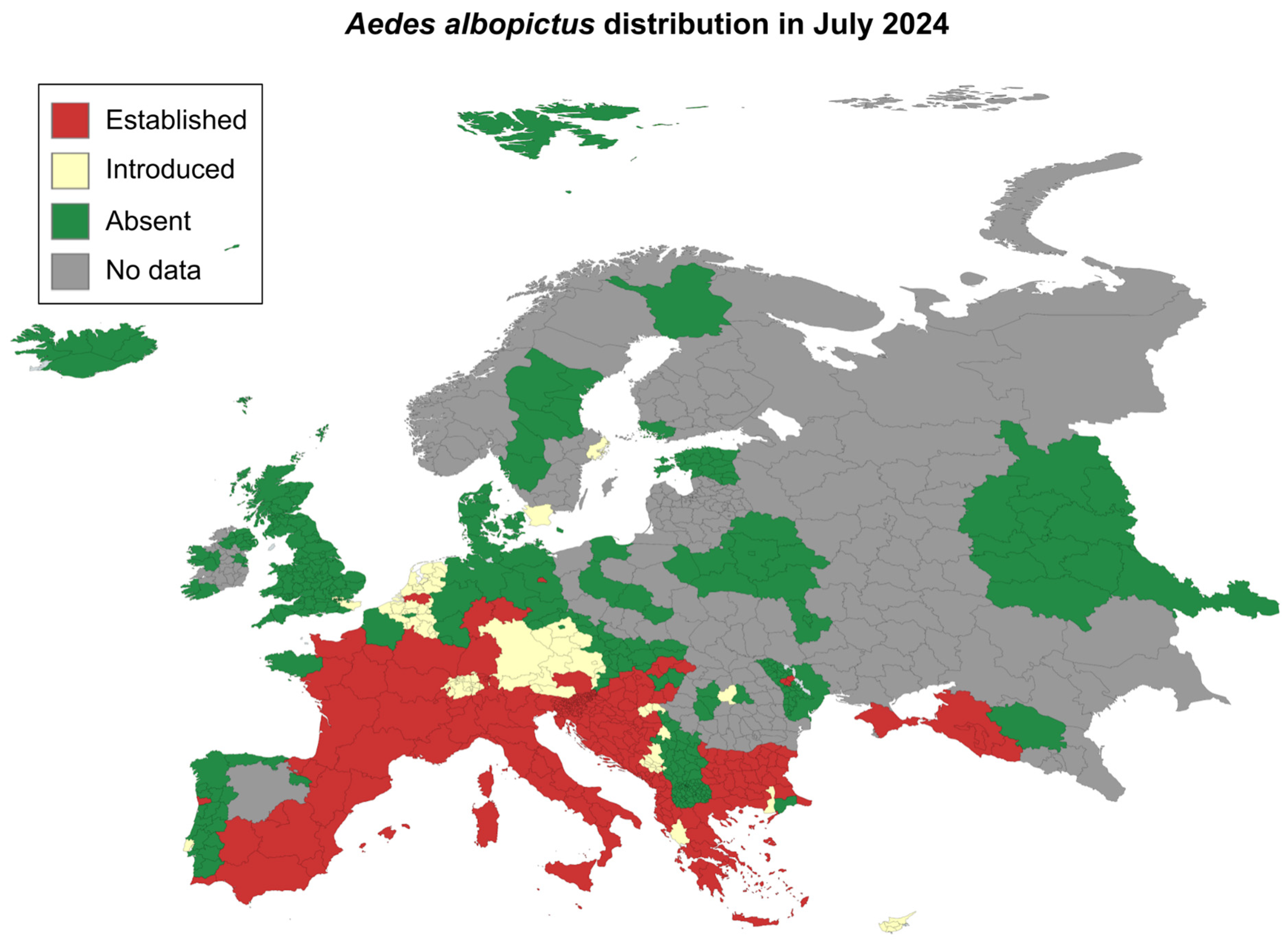
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



