
Submitted:
09 June 2024
Posted:
11 June 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The COVID-19 pandemic struck unexpectedly, emergency services and chronic care institutions, including dialysis centers, were overloaded.
An important problem was the care of positive COVID patients, but also the care of chronically dialyzed patients who presented emergencies.
In our Hospital, which has become a COVID support for dialysis patients with severe forms of the disease, we had to care for PD patients with dialysis-related emergencies.
We presented 2 cases of patients managed on an outpatient basis or 1 day hospitalization, treated successfully and without compromising the quality of the care provided. We used remote monitoring, we worked in a multidiscipli-nary team, we shortened the hospitalization of patients (and implicitly the risk of contact).
In pandemic conditions, the advantage of PD was represented by the possibility of patient isolation, so that in the first 6 months of the pandemic, we recorded no deaths in this category of patients. In case of hemodialysis patients, in-fection and mortality rates were high.
Although we expected an increase in the number of peritoneal dialysis patients in the post-pandemic period, this did not happen. We continue to plead for the popularization of the PD method among patients and doctors, which has proven its advantages under the conditions of the pandemic.
Keywords:
peritoneal dialysis emergencies
; covid pandemia
; telemonitoring
1. Introduction
The respiratory disease caused by the new coronavirus, declared a pandemic by the WHO on March 11 2020, overturned medical systems all over the world, including Romania [1].
The advantage of Romania was the fact that the epidemic started later (the first case was confirmed on February 26), giving our country the necessary time to prepare and be inspired by the experience of the previously severely affected countries.
In 1974, the first iterative hemodialysis center in the country was established at the “Dr. Carol Davila” Nephrology Clinical Hospital which has had an uninterrupted activity to this day.
The modernization of the hospital was an ongoing process, holding today 215 beds, a nephrology department, a surgical department (including vascular surgery), allergology, urology, and an intensive care unit.
In essence, our facility is a comprehensive centralized center for the care of renal patients and not only.
In 2020, by the order of the Minister of Health, our hospital was declared a support hospital for dialysis cases seriously affected by COVID 19.
As a consequence, the organizational structure of the hospital was changed, and separate functional circuits for patients, staff and patients infected with COVID had to be created. [2]
The major advantage of our facility is represented by the pavilion type of architectural structure - 2 separate buildings, making possible the complete separation of the circuits for the patients infected with Covid 19.
At the time, under the conditions of the restrictions of the current medical personnel and medical activity, we had to face new challenges -the uninterrupted care of peritoneal dialysis patients so that they continue to benefit from dialysis but also from the management of possible associated urgencies and emergencies. [3,4,5,6]
2. Materials and Methods
According to the recommendations, a telemonitoring system was implemented, so that hospital visits were transformed into audio-video conferences using platforms for remote communication (WhatsApp, Zoom, Smartphone) [7,8,9,10].
Following the experience of other centers, we limited the access of peritoneal dialysis patients to the hospital.
They were instead contacted every 3 days by a medical staff person, who ensured that they had the necessary supplies at home, they checked on their state of health and offered advice for in-home care.
The hospital’s dialysis center directly cares for 42 hemodialysis patients and 13 peritoneal dialysis patients, but the real total number of dialysis patients who are dependent on “Dr Carol Davila” Hospital is a few hundred a year, serving practically the entire southern area of the country.
However, even under these conditions, emergency situations arose that required hospitalization.
The results of the implementation of the new protocols were verified by evaluating the first 2 cases that required emergency patient care.
Our previous experience from the successful collaboration of the surgical team with the team of nephrologists and the intensive care unit (ICU) led to these results.
3. Results
3.1. Case 1
A 71-year-old patient has been in our evidence since October 2018, at that time with dialysis-dependent acute kidney injury, not recovered.
As the patient was diabetic and presented significant cardiovascular morbidity (cerebral lacunar disease, ischemic cardiomyopathy with chronic heart failure (CHF) NYHA class III, peripheral arteriopathy of the lower limbs stage IV, arterial fibrillation permanently on anticoagulant treatment), our team proposed peritoneal dialysis as chronic renal replacement therapy, an option that the patient and his wife have accepted.
A straight PD Tenckhoff catheter was implanted in the left flank and continuous ambulatory peritoneal dialysis (CAPD) with four exchanges daily, cleaning and dressing of the exit site every other day, local antibiotic therapy with mupirocin and intranasal application of mupirocin, 5 days/month (nasal carrier of Staphylococcus aureus).
The clinical and biological evolution was favorable.
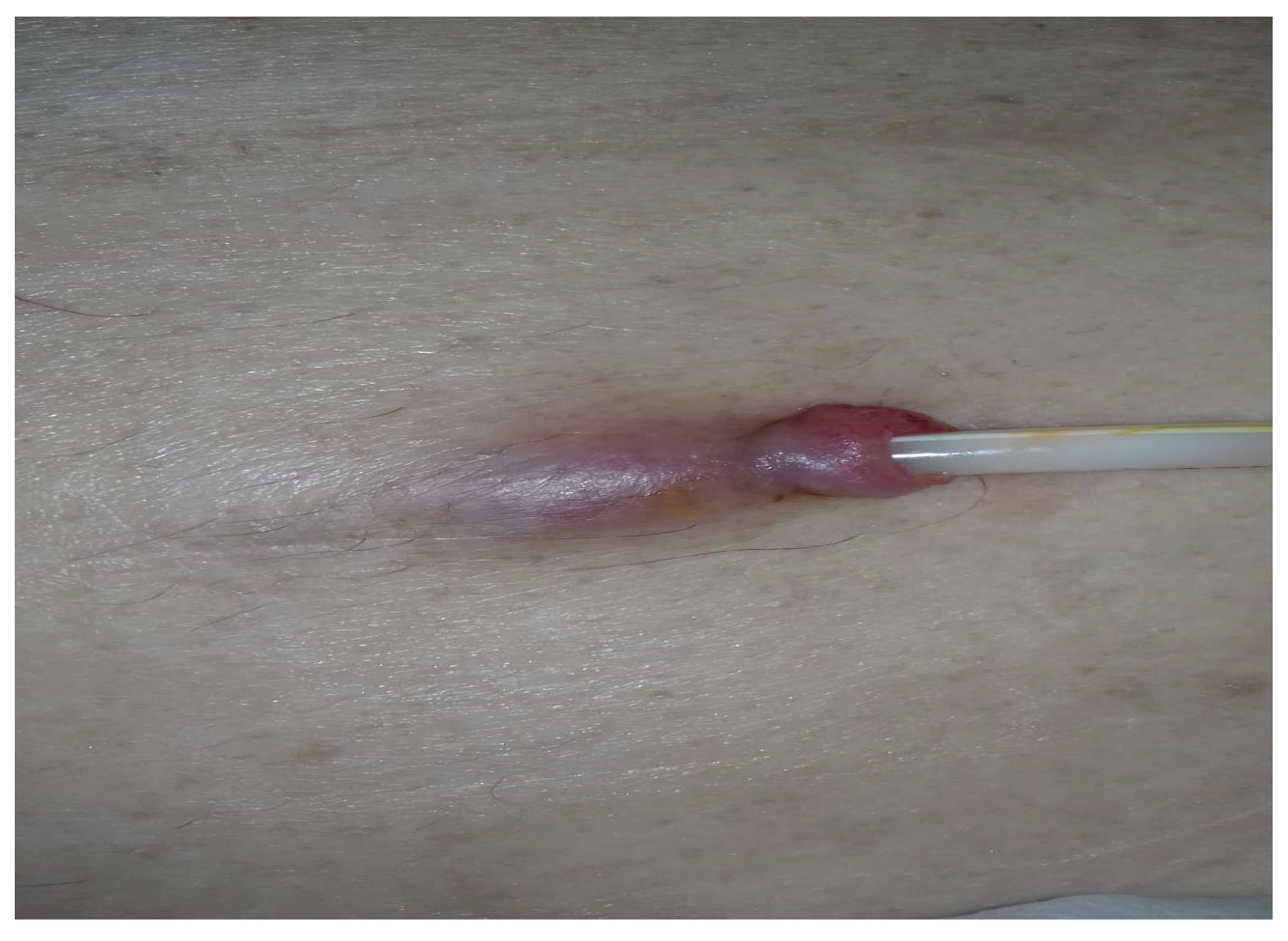
At the beginning of March 2020, the patient presented with erythema, purulent secretion and pain at the level of the catheter exit site.
He was diagnosed with exit site infection associated with tunnel infection (Figure 1).
We initiated empiric antibiotherapy with oral levofloxacin 250 mg/day and rifampicin 600 mg/day and intensified the local treatment (washing and disinfection with hydrogen peroxide and hypertonic saline solution and antibiotic therapy with kanamycin ointment).
Since there was no improvement after a week, we augmented the treatment with vancomycin 2 g intraperitoneally, every 5 days without response at 3 weeks. We decided to extract the catheter and to proceed with contralateral implantation, at the same operative time, with the aim of minimizing the length of hospitalization.
We talked to his family and wife agreed to take responsibility for wound dressing and home peritoneal dialysis treatment, according to our instructions.
Following a telephone consultation, the therapeutic plan for the patient was established, being scheduled on 04/07/2020 for hospital admission.
The medical recommendations were:
- to interrupt oral anticoagulant and antiplatelet administration one week prior to admission,
prevention being ensured by in-house administration of low molecular weight heparin
- to monitor the temperature twice a day
- to monitor the appearance of the peritoneal fluid
- to monitor the wound from the catheter exteriorization opening
- to maintain complete isolation at home throughout the period, without outside contact
The hospitalization was scheduled so that both, the extraction of the infected catheter as well as the implantation of a new peritoneal dialysis catheter in the contralateral flank can be performed in the same surgical session.
The pre-anesthesia consultation was initially carried out remotely.
Taking into account the patient’s medical history, local anesthesia and intravenous sedation were recommended (we avoided anesthesia general with orotracheal intubation, which carried increased risks for both the patient and the medical staff).
On the day of admission, biological samples were collected and anesthesia and surgical consultations were performed.
After obtaining the results, the patient was transported to the operating room where the staff was equipped with increased means of protection.
During the same surgical session, the infected catheter was extracted (the surgical wound of the exit point was left open) and the insertion, without incident, of a new dialysis catheter in the right flank, via open method.
The patient was discharged the next day, being transported home by ambulance. Postoperatively, he required daily telephone monitoring by the surgeon and the nephrologist.
We recommended a stringent restricted diet for fluids, fresh fruits and vegetables due to his minimal residual renal function (diuresis 500 mL, eGFR 4 mL/min).
The washing of the peritoneal cavity was performed once every two days. Wound dressing was performed daily.
The culture results taken intraoperatively from the tip of the catheter, revealed the presence of Staphylococcus aureus, sensitive to Clarithromycin, Gentamicin, Linezolid, Vancomycin, which justified the continuation of antibiotic therapy with vancomycin administered intraperitoneally in a liter of 1.5% glucose solution overnight, every 5 days for two more weeks postoperatively.
From the 5th postoperative day, we progressively restarted the peritoneal dialysis treatment, initially, 2 exchanges/day with 1 liter of dialysis solution each, with the patient in supine position.
From the 8th postoperative day, we increased the dialysis dose by adding two more volume exchanges of 500 mL.
The volumes were gradually increased every two days, until the patient reached the stable schedule he has had prior to the surgery.
The evolution was favorable, both from a surgical point of view (primary healing of wounds, without signs of local complications) as well as nephrological (early resumption of peritoneal exchanges, clear appearance of the liquid without leakage at the suture points).
2.2. The Particularities of the Case
-Patient with multiple associated co-morbidities, which required preoperative preparation and postoperative care. The advantage was that the patient was already present in the records of the clinic and having his medical conditions already known, the treatment and care recommendations could be easily transmitted and applied.
- Patient dependent at home on care provided by another person (wife).
2.3. Case 2
A 63-years old male patient presented himself at the emergency room on 04/05/2020, requesting consultation for diffuse abdominal pain and dialysis effluent turbidity in the last 48 hours.
The renal replacement therapy by peritoneal dialysis was initiated in 2019.
About 2 weeks prior to this visit at our clinic, he observed pus purulent secretion at the catheter exit site for which he was succesfully treated with levofloxacin.
At presentation, the patient was in good general condition, without fever. He accused spontaneous and on palpation diffuse abdominal pain which did not require administration of analgesics and without signs of peritoneal irritation, the intestinal transit was delayed, the peritoneal effluent appeared cloudy and ultrafiltration was negative (-200 mL) for the last two days. Systemic inflammation and high effluent cellularity were present (reactive protein C 230 mg/L, 6 800 cells/mm3, 92% PMN).
A diagnosis of peritoneal dialysis associated peritonitis (first episode) was established.
Bacteriology samples were collected from the exit site and from the dialysis effluent. Empiric antibiotherapy with levofloxacin 250 mg/day orally and vancomycin 2 g intraperitoneally, every 5 days was initiated.
The patient was monitored by telephone daily by the attending nephrologist.
His evolution was favorable with the clearing of the dialysis liquid after 2 days of treatment.
The total treatment duration was three weeks.
2.4. The Particularities of the Case
It was a patient newly initiated on peritoneal dialysis (approximately 6 months prior) who presented with a severe complication - peritonitis. The patient was not known to our clinic, but following the instructions of treatment received, the evolution of the case was uneventful and without the appearance of other complications requiring hospitalization/presentation to the hospital.
Under normal circumstances, the patient would have been hospitalized, but in the context of the spread of Sars Cov 2, we decided on treatment and follow-up at home.
The two cases emphasize one of the advantages of peritoneal dialysis, namely the independence from hospital management and, in special conditions, the possibility for the treatment of complications.
4. Discussion
The Sars Cov 2 epidemic has caused up to the present time over 704 million infections in the world, of which over 7 million deaths.
In Romania on May 11, 2020, 15,362 positive cases and 952 deaths were registered, only 2 and half months since the start of the COVID 19 pandemic. [2]
Similar to situations in other countries, more than half of the contaminations occurred in closed communities -nursing homes for the elderly, institutions for disabled people, hemodialysis centers, centers for palliative care.
In these places, the number of infections increased exponentially, more than half of the deaths in the country being represented by these categories of people. [4,11,12,13]
In particular, hemodialysis patients are at high risk of contracting the disease, mortality being increased in this category .[14,15,16]
Comparatively, in the private hemodialysis centers there were mass outbreaks of illness with COVID 19, involving both patients, medical and auxiliary personnel, with 100 deaths recorded among hemodialysis patients infected with Sars Cov2, in 6 months since the start of the pandemic. [17]
Regarding the deaths caused by the SARS Cov2 epidemic in our country, no deaths of a peritoneal dialysis patient were recorded, compared to approximately 100 deaths among hemodialyzed patients in the first 6 mounts. This is another pleading for increasing the number of peritoneal dialyzed patients – not only in Romania, but also in the world. [18,19,20,21]
In 2022, in our country, there were 18,253 dialysis patients, of which 326 were treated by peritoneal dialysis. [21]
Although Romania had a success story related to peritoneal dialysis, just like in all the countries of the world, once the introduction of private dialysis centers, the number of peritoneal dialysis patients decreased steadily compared to the number of hemodialysis patients.
Although in 2012 a prediction from the RRR (Romanian Renal Registry) showed that if the trend would have been maintained, in 5 years, Romania would have reached a 60% decrease in the number of peritoneal dialysis patients, in 2020 Romania had the same number of PD patients. [21] But the data from the RRR sown in 2020 an increase of the new patients in peritoneal dialysis by 60%. 2021 continues with decrease of new patients in peritoneal dialysis by 44% and increase again in 2022 with 18% [21) The main issue of the decrease of patients in peritoneal dialysis is the low reimbursement.
But the pandemic years have shown more advantages of this dialysis method and it is a reason for gaining more and more trust from the patients.
Studies prior to the COVID 19 pandemic tried to demonstrate the utility of remote control for peritoneal dialysis patients confirmed by Milana Manai et al. and later by Virizi et al. Studies also indicated that remote control increases patient’s trust in this dialysis modality. [22,23,24]
In 2024 WHO indicated the tremendous importance of the digital technologies that are already part of the people’s life for the scope of health and well-being. [25]
5. Conclusions
The therapeutic success in unfavorable medical support conditions is equally due to the multidisciplinary team involved in the treatment of the dialysis patients and the close patient adherence to treatment along with his family support.
Each type of dialysis has advantages and disadvantages, indications and contraindications, but the reality of the recent pandemia has emphasized a new advantage of PD both in Romania and worldwide – it allowed social distance and remote follow-up of the patients, so that no deaths were recorded among these patients in the first 6 months of SARS Cov2 pandemic.
Author Contributions
Conceptualization, C.I. and C.R.I.; methodology, I.A.; software, I.A.; validation, C.I., S.H.S. and V.S.; formal analysis, I.B.; investigation, T.C; resources, C.R.I. and I.A..; data curation, V.S.; writing—original draft preparation, C.R.I.; writing—review and editing, C.I.; visualization, C.I..; supervision, S.H.S..; project administration, C.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study was performed in accordance with the Declaration of Helsinki and was approved by the local Ethics Committee: Dr Carol Davila Clinical Nephrology Hospital,
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper
Data Availability Statement
Not applicable
Acknowledgments
Publication of this paper was supported by the University of Medicine and Pharmacy Carol Davila, through the institutional program Publish not Perish.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization Coronavirus disease (COVID-19) 2022. [cited 2022 MAR]. Available from: https://www.who.int/health-topics/coronavirus.
- www.ms.
- Perez-Moran D, Perez-Cuevas R, Doubova SV. Challenges for Peritoneal Dialysis Centers Before and During the COVID-19 Pandemic in Mexico. Arch Med Res. 2022 Jun;53(4):431-440 Epub 2022 Apr 29. [CrossRef] [PubMed]
- Yang Z, Dong J. Operational considerations for peritoneal dialysis management during the COVID-19 pandemic. Clin Kidney J. 2020 Jul 4;13(3):322-327. [CrossRef] [PubMed]
- Htay H, Wong PMPK, Choo RR, Dawood US, Foo MWY, Jayaballa M, Lee G, Lee MB, Liu YLA, Low S, Ng AKH, Oei EL, See YP, Tagore R, Tai Y, Liew A. Strategies for Management of Peritoneal Dialysis Patients in Singapore during COVID-19 Pandemic. Ann Acad Med Singap. 2020 Dec;49(12):1025-1028. [CrossRef] [PubMed]
- de Sequera P, Quiroga B, Goicoechea M; en representación de la Junta Directiva de la Sociedad Española de Nefrología (S.E.N.). Actualización de las recomendaciones de medidas de prevención y aislamiento frente al SARS-CoV-2 en las unidades de diálisis: un posicionamiento de la Sociedad Española de Nefrología [Update of the prevention and isolation measure recommendations against SARS-COV-2 in dialysis units of Spain: A position paper of the Spanish Society of Nephrology Council]. Nefrologia. 2022 Nov-Dec;42(6):714-721. Spanish Epub 2022 Oct 12. [CrossRef] [PubMed]
- https://ispd.org/wp-content/uploads/ISPD-PD-management-in-COVID-19_ENG.
- Ronco C, Manani SM, Giuliani A, Tantillo I, Reis T, Brown EA. Remote patient management of peritoneal dialysis during COVID-19 pandemic. Perit Dial Int. 2020 Jul;40(4):363-367. Epub 2020 Jun 29. [CrossRef] [PubMed]
- Car J, Koh GC, Foong PS, Wang CJ. Video consultations in primary and specialist care during the covid-19 pandemic and beyond. BMJ. 2020 Oct 20;371:m3945. [CrossRef] [PubMed]
- El Shamy O, Tran H, Sharma S, Ronco C, Narayanan M, Uribarri J. Telenephrology with Remote Peritoneal Dialysis Monitoring during Coronavirus Disease 19. Am J Nephrol. 2020;51(6):480-482. Epub 2020 Apr 28. [CrossRef] [PubMed]
- Maldonado M, Ossorio M, Del Peso G, Santos C, Álvarez L, Sánchez-Villanueva R, Rivas B, Vega C, Selgas R, Bajo MA. COVID-19 incidence and outcomes in a home dialysis unit in Madrid (Spain) at the height of the pandemic. Nefrologia (Engl Ed). 2021 May-Jun;41(3):329-336. English, Spanish. Epub 2020 Nov 5. [CrossRef] [PubMed]
- Alfano G, Fontana F, Giovanella S, Morisi N, Amurri A, Ligabue G, Guaraldi G, Ferrari A, Cappelli G, Magistroni R, Gregorini M, Donati G. Prevalence, clinical course and outcomes of COVID-19 in peritoneal dialysis (PD) patients: a single-center experience. Clin Exp Nephrol. 2023 Feb;27(2):171-178. Epub 2022 Nov 3. [CrossRef] [PubMed]
- Geetha D, Kronbichler A, Rutter M, Bajpai D, Menez S, Weissenbacher A, Anand S, Lin E, Carlson N, Sozio S, Fowler K, Bignall R, Ducharlet K, Tannor EK, Wijewickrama E, Hafidz MIA, Tesar V, Hoover R, Crews D, Varnell C, Danziger-Isakov L, Jha V, Mohan S, Parikh C, Luyckx V. Impact of the COVID-19 pandemic on the kidney community: lessons learned and future directions. Nat Rev Nephrol. 2022 Nov;18(11):724-737. Epub 2022 Aug 24. Erratum in: Nat Rev Nephrol. 2022 Sep 20. [CrossRef] [PubMed]
- Yavuz D, Karagöz Özen DS, Demirağ MD. COVID-19: mortality rates of patients on hemodialysis and peritoneal dialysis. Int Urol Nephrol. 2022 Oct;54(10):2713-2718. Epub 2022 Apr 5. [CrossRef] [PubMed]
- Perl, Jeffrey; Thomas, Doneal; Tang, Yiwen; Yeung, Angie; Ip, Jane; Oliver, Matthew J.; Blake, Peter G.. COVID-19 among Adults Receiving Home versus In-Center Dialysis. CJASN 16(9):p 1410-1412, September 2021. [CrossRef]
- https://cnscbt.
- Naljayan, Mihran V. ; Schiller, Brigitte; Watnick, Suzanne, Weinhandl, Eric D., Eds.; Perl, Jeffrey How the COVID-19 Pandemic Hit Home in North America Lessons Learned in Improving Home Dialysis Utilization and Outcomes linical Journal of the American Society of Nephrology 18(7): p 957-960, July 2023. [Google Scholar] [CrossRef]
- Perl, Jeffrey; Thomas, Doneal; Tang, Yiwen; Yeung, Angie; Ip, Jane; Oliver, Matthew J.; Blake, Peter G.. COVID-19 among Adults Receiving Home versus In-Center Dialysis. CJASN 16(9):p 1410-1412, September 2021. [CrossRef]
- Yeter HH, Gok Oguz E, Akcay OF, Karaer R, Yasar E, Duranay M, Ayli MD, Guz G. The reliability and success of peritoneal dialysis during the COVID-19 pandemic. Semin Dial. 2021 Mar;34(2):147-156. Epub 2020 Nov 19. [CrossRef] [PubMed]
- Rombolà G, Brunini F. COVID-19 and dialysis: why we should be worried. J Nephrol. 2020 Jun;33(3):401-403. [CrossRef] [PubMed]
- www.registrulrenal.
- Milan Manani S, Rosner MH, Virzì GM, Giuliani A, Berti S, Crepaldi C, Ronco C. Longitudinal Experience with Remote Monitoring for Automated Peritoneal Dialysis Patients. Nephron. 2019;142(1):1-9. Epub 2019 Jan 30. [CrossRef] [PubMed]
- Virzì GM, Morisi N, Milan Manani S, Tantillo I, Gonzàlez Barajas JD, Villavicencio BD, Castiglione C, Alfano G, Donati G, Zanella M. Scheduling of Remote Monitoring for Peritoneal Dialysis Patients. J Clin Med. 2024 Jan 11;13(2):406. [CrossRef] [PubMed]
- Centellas-Pérez FJ, Ortega-Cerrato A, Vera M, Devesa-Buch RJ, Muñoz-de-Bustillo E, Prats M, Alonso-Valente R, Morais JP, Cara-Espada PJ, Yuste-Lozano C, Montomoli M, González-Rico M, Díez-Ojea B, Barbosa F, Iriarte M, Flores C, Quirós-Ganga PL, Espinel L, Paraíso V, Peña-Ortega M, Manzano D, Cancho B, Pérez-Martínez J. Impact of Remote Monitoring on Standardized Outcomes in Nephrology-Peritoneal Dialysis. Kidney Int Rep. 2023 Nov 5;9(2):266-276. [CrossRef] [PubMed]
- World Health Organization Health topics. [cited 2024 mar]. Available from: www.who.int/health-topics/digital-health.
Figure 1.
Tumefaction, erythema of the exit site and the initial part of the subcutaneous tunnel.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



