
Submitted:
03 June 2024
Posted:
04 June 2024
You are already at the latest version
Abstract
The global centenarian population is expected to reach 3 million by 2050, yet little is known about the health status of centenarians in Sub-Saharan Africa. A case study examined the health conditions and functionality of nine Ethiopian centenarians. In-depth interviews revealed that all nine were Orthodox-Christians and lived with extended family; eight were male. Aside from minor health complaints, centenarians in rural Ethiopia perceived that their sensory/cognitive functionality was normal until their late 90s. Despite a lack of medical care, the centenarians included 2 survivors, 4 delayers, and 3 escapers. Centenarians in rural Ethiopia were embedded in closely-knit, religious, multigenerational households and communities and aspired to live resiliently. Findings call for consideration of the unique health status of centenarians in Global South nations in their own cultural context.
Keywords:
Centenarians
; Ethiopia
; health status
; sensory impairment
1. Introduction
Various studies indicate a growing number of centenarians (older adults who reached 100 years and beyond) particularly in developed countries [1,2,3,4]. The size of the global centenarian population reached 180,000 in 2000 [5], 300,000 in 2010 [6], and 316,000 in 2017 [7]. By 2050 the number of centenarians is estimated to reach up to 4 million [8,9,10]. China is expected to have the highest number of centenarians followed by Japan, the US, Italy, and India [7]. Globally, the centenarian population will grow at a rapid rate and is projected to reach 25 million by 2100 [11,12]. In the developing world including Africa there is a scarcity of information about older adults in general and centenarians in particular [5,13,14,15]. Based on projections of the Central Statistical Agency of Ethiopia [16], 5 to 6 million people in Ethiopia are age 60 or older, or about 5% of the population. This number is expected to reach 11.5 million by 2050. However, there is no documentation about Ethiopian centenarians in any government reports [15].
Old age involves physical, mental, and behavioral changes that have implications for older adults’ health, daily activities, and cognitive status. With the advance of old age, the rate of morbidity increases [17,18] and the level of physical functioning declines [19,20,21]. Clinical tests and self-reports have shown that centenarians experience different types of health conditions. A study of Greek centenarians indicated that of 489 centenarians, 47% (208) experienced urinary incontinence and 23% (102) had fecal incontinence [4]. A study of 93 American centenarians reported a low prevalence rate of hypertension, angina or myocardial infarction, diabetes, and back pain and good mental health status [22]. Among 302 Japanese centenarians (65 men, 237 women), the majority (95%) suffered from hypertension, heart disease, stroke, fractures, and cataracts. However, diabetes mellitus was rarely reported as a health problem [23]. A study in northern Japan found much variability in the health and functional status of centenarians [24].
Australian centenarians identified ocular disease (70%), arthritis (58%) and hypertension (40%) as common health problems [25]. Research findings from two studies in Portugal found that among 127 centenarians, 46.5% rated their health status as good, very good, or excellent [19]. Physical frailty and depression were found to be age-associated health conditions among the Portugese centenarians [26]. The prevalence rate of hypertension among Finish centenarians reached 19%, whereas in Hong Kong 65% of centenarians had hypertension [27].
A study of 424 centenarians in the U.S. and Canada found that 38% (n= 162) were survivors (experienced illness before old age), 43% (n=182) were delayers (did not experience illness until their 80s and 90s), and 19% (n=80) were escapers (did not experience illness before age 100) [28]. Out of 47 Greek centenarians, 15% (n = 7) were escapers [29]. A study of 188 centenarians in Australia similarly ranked survivors (46%, n= 86), delayers (34%, n = 64), and escapers (19%, n = 36) [18].
Older people are susceptible to sensory impairment and deterioration of cognitive functioning [30]. In France, 57.2% (n = 165) of centenarians had hearing defects [31]. Among Costa Rican centenarians (N=43), three-quarters (76.7% n=33) had hearing problems at different levels of severity and 44.2% (n=19) had visual limitations [32]. According to the Italian Multicentric Study on Centenarians [33], among 126 centenarians half had a diminished sense of taste.
The Heidelberg Centenarian Study found that among 90 centenarians, just over half (52%) experienced different levels of cognitive impairment [34]. However, in Greece, researchers found low prevalence rate 4% (n=3) of cognitive problems among centenarians (N=76) [35]. The New England Centenarian Study also found a low prevalence rate of dementia (3%, n=2) among 43 centenarians [36].
While centenarian studies are becoming more common, few if any have focused on centenarians in the African continent. While not focused on centenarians per se, Aladejare’s [37] analysis of macroeconomic indicators in West African nations determined that longevity was lower in nations with higher rates of external debt. Perls [38] advocates for centenarian studies that examine the experiences of older adults of different races and ethnicities as well as those living under varying socioeconomic conditions. In the absence of adequate information about African centenarians, this study aimed to shed light on the health conditions, including sensory and cognitive functionality, of centenarians in Ethiopia. Centenarians are exceptional people who survive illness and various physical and cognitive problems. We conducted this study to explore the health conditions of centenarians in Ethiopia across their life span based on their own perceptions. The findings may serve as a source of information to researchers interested in the health status of centenarians in Global South nations. Accounts of centenarians’ health problems and sensory and cognitive impairment will inform agencies to take measures to improve the lives of the growing number of oldest-old, including centenarians.
This study used a qualitative case study design to explore the health conditions, including sensory and cognitive function, of centenarians. A case study design was a good fit for the purpose of investigating and understanding in-depth the health status of Ethiopian centenarians with consideration of their unique context [39,40,41]. Nine centenarians were selected through snowball sampling from six woredas (local administrative units) in the Amhara Region of Ethiopia. In the process of recruitment, the first author verified ages of centenarians, considered their physical strength, memory, and willingness to participate in in-depth interviews and share their perceptions of their physical condition and sensory and cognitive functioning. Data were collected between December 2015 and January 2019 in the centenarians’ homes. Interviews lasted an average of 142 minutes and were conducted in Amharic. The narrative data were analyzed using descriptive analysis.
Ethical standards were followed throughout the research process. A letter of permission to conduct the study was secured from the Department of Social Work in the Faculty of Social Sciences at Author’s Own University. Centenarians and their family members were informed about the study objective and procedures. Centenarians gave informed consent orally to be interviewed. Study respondents were treated in a respectful manner from the initial recruiting contact through data collection. Pseudonyms were used to protect the confidentiality of study respondents.
3. Results
3.1. Description of Respondents
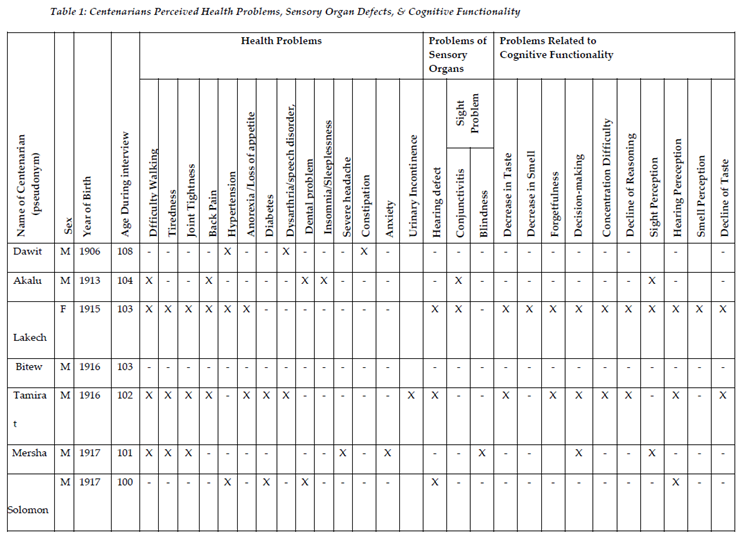
The mean age of the 9 centenarians (8 men, 1 woman) was 102 years and 3 months. There was an eight-year difference between the youngest and oldest centenarians (see Table 1). Dawit, Akalu, Tamirat, Mersha and Demeke lived in rural villages in the community, and the other respondents lived in the towns. The nine centenarians had a total of 67 children, 37 of whom were still living at the time of data collection. Bitew, Solomon, and Nebyou lived with their wives, and the rest lived with their children, grandchildren, and great-grandchildren. All respondents were Orthodox Christians; five were monks (Dawit, Akalu, Tamirat, Mersha and Demeke) and one was a nun (Lakech). Akalu, Lakech, Bitew and Zelalem were non-literate. Mersha, Solomon, and Demeke attended church education and could read and write. Dawit completed eighth grade and earned a certificate for completing a 3-year teachers’ training program. Nebyou dropped out of grade nine. Farming was a lifelong occupation for Akalu, Tamirat, Mersha, and Lakech. The remaining centenarians were engaged in non-farm activities, sometimes combining two or three types of occupations. Dawit (108) served as a schoolteacher for many years and then became a farmer and a priest in a rural parish. Bitew (103) was a shoemaker and business owner; Demeke (100) worked as a “bounty hunter” and ended up as a retired farmer. Solomon (100) was an administrator and secretary of senior officials until his retirement. Nebyu (100) spent half of his life as a mechanic. The main sources of income for centenarians derived from children’s support, rent from small plots of farmland, rental houses, and pension.
3.2. Perceived Health Problems
Centenarians mentioned 14 health conditions that they had experienced based on their self-perceptions and partly considering medical reports. The list comprised of difficulty walking, tiredness, joint tightness, back pain, hypertension, anorexia/loss of appetite, diabetes, dysarthria/speech disorder, dental problems, insomnia/sleeplessness, severe headache, constipation, anxiety, and urinary incontinence. The number of health problems that each respondent noted varied from none to 8. Tamirat (102) struggled with 7 health issues, Lakech (103) noted 6, and Mersha (101) mentioned 5. Akalu (104), Dawit (108) and Solomon noted 3 or 4 health issues. Three respondents (Bitew-103, Demeke-100, Nebyu-100) perceived that they were free from any health problems. Four centenarians mentioned difficulty walking as their health concern. Tiredness, joint tightness, back pain, and hypertension were noted by only three respondents. Anorexia was mentioned as a health problem by two respondents. Sleeplessness, severe headache, constipation, and anxiety were each noted by one respondent.
Two centenarians (Tamirat, Mersha) attributed their difficulty walking with old age and illness, one (Akalu) to wounds from the battlefield in his twenties during the Italo-Ethiopian war of 1936-1941, and one (Lakech) to falling. The severity and duration of difficulty walking varied. Akalu lived with difficulty walking for the last 80 years and shared: “As I got older and thinner, I felt pain on my hip and left leg and became lame as a result of the wound I received in 1936 fighting against the Italians.” Tamirat, Mersha and Lakech experienced difficulty walking for the last three to ten years. Lakech and Tamirat needed the support of other persons to move inside the house. Lakech shared, “I fell in front of the main gate of the house in 2016 and suffered an injury on my left leg and hipfracture. I could not walk a short distance even to the toilet without the support of my daughter and grandchildren.” Tamirat was bedridden for the last three years. In order to receive morning sunlight near his home, he is carried by his children (age 70 and older) and grandchildren. Assisted by family members, Mersha could walk in his compound covering an area of not more than 60-to-70 meter radius where his children, grandchildren, in-laws, close and distant relatives and neighbors reside. Dawit, Bishaw, and Solomon are able to walk far independently in the neighborhoods, to the church, and marketplace. Kebede and Nebyu had difficulty walking and their movements are restricted in the homestead.
Lakech, Tamirat, and Mersha reported tiredness. Different from other respondents, these three centenarians had a poorer health profile and problems of functionality of their sensory organs. Collectively, these three mentioned ten illnesses, each experiencing five to seven. They noted deterioration of their physical strength that resulted in tiredness. Mersha perceived that his experience of tiredness was related to his blindness that restricted his mobility. Akalu, Lakech, Tamirat, and Mersha had joint tightness/joint pain in the young age as vicenarian (Akalu) and in their late nineties as nonagenarians. Centenarians noticed injury from bullets (Akalu), falling (Lakech), and experiencing multiple diseases (Tamirat and Mersha) as causes of joint pain. They felt joint pain in the hip, knees and legs that hindered walking and sitting. Respondents made home treatments washing with warm water and wearing bandages to get relief from joint pain. Akalu, Lakech and Tamirat experienced back pain that created discomfort with movement and sleeping and barred them from doing previous activities. Surprizingly, Dawit, 108, noted that he was free form back pain. He described, “I could walk up right, bend down to pick materials from the ground, and tie shoelaces easily.”
Dawit, Lakech, and Solomon were hypertensive and had physician recommendations to take medication. Dawit (age 108) survived a stroke in 2015 that exposed him to minor dysarthria/speech disorder. Solomon and Lakech were not taking medicine regularly contributing to decline of their health conditions. Lakech and Tamirat had the problem of anorexia or loss of appetite. They associated their loss of appetite with sickness, loss of taste and smell, and restriction from dietary salt intake due to hypertension and diabetes. Lakech and Tamirat excluded some foods from their meals and changed their dietary habits. Lakech skipped meals, sometimes eating only once a day. For Lakech and Tamirat, the loss of appetite contributed to low food intake, weight loss, and reduced physical strength and functional capacity. Tamirat and Solomon suffered from diabetes. Since age 98, Solomon took medication daily as prescribed by a physician. Later on, he became fed up with taking medication and declined to adhere to the advice of the physician including abstaining from alcohol and eating the raw meat that he really enjoyed eating.
Dawit and Tamirat developed minor dysarthria, a type of speech disorder characterized by cessation and slurring of words. Dawit shared, “I had dysarthria after experiencing a stroke in 2015 at the age of 107.” Tamirat was not clear how he became a victim of dysarthria. The problem occurred suddenly when he woke up the morning after a stroke. Akalu and Solomon lost part of their molars and premolars in their late 90s because of tooth decay. They faced difficulty with chewing and took a longer time to finish their meals. The loss of teeth restricted them from eating roasted barely, beans, and corn. They preferred foods that can be chewed easily. Akalu, 104, reflected, “I quit eating roasted cereals after the removal of my teeth. My teeth are not strong. I eat boiled beans and corn.” Solomon substituted some of the missing teeth with gold crowns. The loss of teeth slightly changed the facial appearance of Akalu and Solomon. On the contrary, six centenarians (Dawit, Lakech, Bitew, Tamirat, Alamirew and Nebyou) had strong and intact teeth. They had no problem with chewing cereals, meat, vegetables, and fruits.
Akalu experienced insomnia or sleeping difficulty after the age of 100. Bitew stated, “I didn’t have enough sleep. I went to the bedroom early and slept for a short time and woke up soon. Then, I thought why and how I lost my property till the dawn.” Akalu had a similar sleeping disorder. Bitew and Mersha experienced recurring and painful headaches that lasted 3 to 5 hours about twice a week. Mersha worried about his future life and developed anxiety. Besides difficulty walking, tiredness, dysarthria, joint tightness, back pain, diabetes, and anorexia, Tamirat had challenges with urinary incontinence.
3.3. Decline of Sensory Functioning
Old age is characterized by a decline in sensory functioning. Some respondents mentioned functional problems related to hearing (4), sight (3), taste (2), and smell (1). Lakech, Tamirat, and Solomon experienced mild hearing loss. They had difficulties hearing low pitch sounds from a short distance unless a person sits closely and speaks loudly. During the interview sessions they asked the first author to repeat what he said multiple times. Nebyou (100) faced a severe loss of hearing and used hearing aids for the past six years: “I had hearing problem with my ear. I could hear assisted by hearing aids that my daughter sent me from abroad.” Three centenarians--Dawit (108), Bitew (103) and Demeke (100)--had no sensory functioning problems.
Three respondents had sight limitations. Akalu and Lakech were diagnosed with conjunctivitis at the age of 101 and 98, respectively, and had a partial recovery after receiving medical treatment. Mersha (101) remembered the decline of his sight at age 90 or 91 and became completely blind at age 98. Losing his wife and his sight in the same year was an unbearable tragic time for Mersha. He relied heavily on the assistance of his children, grandchildren, and in-laws to use the traditional toilet room and to go to neighbors’ houses for a coffee ceremony and social occasions. Lakech and Tamirat faced the problem of ageusia, a loss of their sense of taste after the age of 100. They consumed food and drinks without experiencing their real taste. Lakech developed anosmia (loss of sense of smell) at the age of 101.
3.4. Decline of Cognitive Functionality
Five centenarians (Akalu, Lakechc, Tamirat, Mersha and Nebyou) identified cognitive problems including forgetfulness (2), problems with decision-making (3), difficulty with concentration (2), decline of reasoning (2) and decline of sight (3), hearing (4), smell (1), and taste (2). Lakech and Tamirat became forgetful after the age of 100. They forgot where they put items, and sometimes the names of their grandchildren, or exchanged their names and repeated some points. They needed reminders to refresh their memory and to further explain certain ideas. Lakech and Tamirat had concentration difficulty and a decline of reasoning. They had a short span of concentration (about 30 to 40 minutes) on the issue under discussion. During the interview session, they had to take short break of 15 to 20 minutes to refresh their attention. Lakech and Tamirat shared what they knew and could remember but acknowledged a decline of logical reasoning, analyzing, and synthesizing ideas. Lakaech, Tamirat and Mersha had limited cognitive capacity to analyze and interpret information, to conduct a cost and benefit analysis, and to deal with complicated ideas to make decisions. Family members respected the autonomy and dignity of Lakech, Tamirat and Mersha and discussed matters with them in making decisions that affected them.
Impairment of sensory organs affected the respondents’ capacity to perceive what they see, hear, smell and taste to varying degrees. Conjunctivitis reduced the ability of Akalu and Lakech to perceive objects they see precisely. Mersha, a blind centenarian, had severe decline of sight perception. Lakech, Tamirat and Solomon developed mild hearing problems that impacted their hearing. Nebyou, 100, was dependent on hearing devices. Due to his hearing restrictions, he sometimes misunderstands messages. Nebyou spoke loudly and asked the first author to speak louder and repeat the messages whenever necessary. Lakech, 103, was the only respondent who experienced a decline in the sense of smell. She could not perceive odors of foods, drinks, or materials. Lakech and Tamirat found foods and drinks tasteless. Lakech explained how the decline in her sense of smell and taste affected the quality of her life: “I had to eat and drink to live without getting the real flavors of foods and drinks.”
4. Discussion
This study was carried out with nine centenarians (1 woman, 8 men) in Ethiopia in an effort to describe and better understand their health conditions and sensory and cognitive functionality based on their own perceptions. Findings revealed 14 age-related health conditions experienced by centenarians including difficulty walking, tiredness, joint tightness, back pain, hypertension, anorexia /loss of appetite, diabetes, dysarthria/speech disorder, dental problem, insomnia/sleeplessness, severe headache, constipation, anxiety, and urinary incontinence. Variations are visible in the rate of morbidity prevailing among this group of centenarians. One respondent had 8 health conditions, another had 6, and four respondents had three to five health conditions. When we traced the past health history of these six centenarians, two persons experienced illness prior to old age and so are considered Survivors. Four did not develop health limitations until their late eighties and nineties and so are Delayers. Three centenarians reported that they never experienced illness before the age of 100 and hence they are categorized under the Escapers morbidity profile. Demeke, 100, identified himself as an Escaper. He claimed, “I lived a healthy life throughout my life. I have never visited a health center or hospital to get medical treatment in my life. Thanks to God I am healthy!”
Some of the health conditions experienced and perceived by Ethiopian centenarians were similar to those found in studies in Tokyo [23], Greece [4], and France [31]. However, these studies applied different research methods to investigate the health profiles of centenarians and identified several diseases not mentioned by the Ethiopian centenarians such as heart disease, non-skin cancer, skin cancer, osteoporosis, thyroid condition, Parkinson's disease, and chronic obstructive pulmonary disease, depression, and fecal incontinence. Chronic diseases like hypertension frequently appeared among centenarians [23,31] outside of the African continent. Among 445 Greek centenarians, 47% (N= 208) had hypertension [4]. Likewise, Martin and colleagues [27] indicated disparities in the prevalence rate of diseases among centenarians in different countries. The prevalence rate of diseases was 19% among Finnish centenarians and 65% among centenarians in Hong Kong. From a sample of 424 American and Canadian centenarians, 38% (n=162) were survivors, 43% (n=182) were delayers, and 19% (n=80) were escapers [28]. Further study is needed to explain the variations in health conditions of centenarians in different areas of the globe.
The Ethiopian centenarians in this study perceived illness as personal construction attributable to old age and living conditions. For them illness in late life is inevitable, and they worried more about experiencing suffering from illnesses rather than death anxiety. Though centenarians had health and functional limitations, they had limited understanding of the scientific explanations and symptoms of disease processes. Centenarians who perceived themselves as healthy may have hidden diseases that can be detected through medical diagnosis that may change their health profiles which, in turn, may have implications for their morbidity profiles.
Going for medical checkups before illness and post-diagnosis at medical follow-ups is not a common practice among centenarians in Ethiopia. Most of the respondents visited physicians only when they felt sick to the extent of not eating and becoming bedridden for days. Regular medical follow-up and implementing health professionals’ medical advice may improve centenarians’ health conditions; however, many of them were not doing so.
Geographic distance and financial constraint were barriers to centenarians getting further medical treatment at public clinics and hospitals. Rural centenarians and family members with pressing economic problems could not afford transport, medical, and auxiliary costs associated with travelling a long distance to seek medical care. In the Ethiopian context, there are few, if any, physicians with geriatric expertise [15]. Medical self-neglect was observed with one of the respondents who experienced six different health problems. He was not interested in consulting physicians which emanated from his pessimistic belief about the impossibility of recovering from illness at “the climax of human age.” Other respondents had similar tendencies and rarely used health services.
Centenarians had defects on sensory organs (sight, hearing, smelling and taste) with various levels of severity in their late nineties and beginning of centennial age. These sensory functionality problems tended to occur gradually. Respondents had no in-depth understanding about conditions contributing to health problems and sensory and cognitive limitations. Centenarians attributed their health conditions in general terms to old age. Impairment of sensory organs is not unique to Ethiopian centenarians rather it is a prevalent problem across the globe. For instance, findings from studies done among centenarians in Costa Rica, France [32] and Italy [33] show that the prevalence of sight problems reached 44.2 to 50 percent, hearing defect was 57.2 to 76.7 percent, and half of the respondents (N = 126) experienced a loss of taste. Cognitive declines such as forgetfulness, decline of analytical capacity to make decisions, decline of reasoning, and concentration difficulties are experienced by older adults across the globe.
Empirical evidence confirmed that in some cases, sensory and cognitive limitations and health problems may influence each other. Centenarians who have stroke and fractures may experience decline of cognitive and physical functioning [42] Visual and hearing impairment affect cognitive functioning [43]. Visual impairment may engender depression among centenarians [44]. Kuo and colleagues [45] demonstrated the impact of hypertension on logical reasoning. Visual and hearing impairment increased the risk of falls and hip fractures, mortality, decreased cognitive power, and social interaction [46]. Problems with one sensory organ such as vision, hearing, taste, smell or touch may affect proper functioning of another sense organ [30,47].
The relative health of this group of Ethiopian centenarians is remarkable considering the minimal health care they received throughout late life, and especially, the lack of geriatric professionals in Ethiopia. Despite their longevity, poverty, and minimal health care, what stands out about this hearty group of older adults is the lack of chronic disease. Instead of labeling the disease-free respondents as “Escapers,” a more fitting label would be “Thrivers.” Their lives illustrate the possibility of a healthy old age beyond a century within a context of organic foods, regular exercise (e.g., walking, hauling wood for fuel, farming), and strong family support. Future research could help to illuminate the facets of the lives of Global South centenarians that, while seemingly primitive by western standards, are the very things that keep them healthy well into late life.
5. Conclusions
Centenarians in Ethiopia reported experiencing health problems including a decline of sensory and cognitive functionality that affected their quality of life and daily activities and compromised their autonomy and privacy. However, some centenarians aged with proper sensory and cognitive functioning and enjoyed successful aging. Labelling all centenarians as bed-ridden, frail, senile, and fatigued is erroneous. In spite of physical and health problems, centenarians in this study had no feelings of death anxiety. They thanked God for allowing them to live a long life. Likewise, most of the Portuguese centenarians (93.8%) studied by Araújo et al. [48] credited their long life to their religious beliefs. Unless centenarians get proper care and medical treatment, they may experience deterioration of their health or a decline of sensory and cognitive functionality that may diminish their autonomy and contribute to emotional and financial burdens on caregivers. As a limitation, this study was cross-sectional and based on respondents’ self-perceptions.
Generating crystalized knowledge on the health conditions and sensory and cognitive functionality of Ethiopian centenarians necessitates conducting large-scale multi-disciplinary research including mental health, neurology, internal medicine, gerontology, geriatric medicine, gerontological and health social work. Integrating respondents’ self-perceptions with medical reports based on standardized measures and applying different research approaches and models is needed. Medical diagnosis may indicate new results that are not perceived by the centenarians themselves. Just as McCormack [49] recommended “a more expansive and multidisciplinary study of centenarians” (p. 179) in Australia, we likewise call for gerontological scholars to actively engage in research to build a foundation of knowledge on centenarians in Sub-Saharan Africa. Considering that national economic policies can contribute to poverty and subsequently diminish longevity [37], we call for Sub-Saharan nations to step up and provide social protection in the form of basic income support to their aging citizens.
Epilogue. By the end of the data collection period in January 2019, five of the centenarians were still living. Three (Solomon, Demeke and Dawit) lived for a year after their interviews. Dawit, the oldest of all the centenarians who participated in our study, lived for four years after the interview session; he died in November 2019 at the age of 113, reaching the status of super-centenarian. Lakech, the only female respondent, died in 2020 at the age of 104. Tamirat passed away in August 2021 at the age of 105.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by Author’s Own University and followed the National Research Ethics Review Guidelines (2014).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
Raw narrative data available upon request.
Acknowledgments
The authors are grateful to all participants of the study and Author’s Own University.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Cho, J., Martin, P., & Poon, L.W. The older they are, the less successful they become? Findings from the Georgia Centenarian Study. Journal of Aging Research, 2012, 695854. [CrossRef]
- Engberg, H., Christensen, K., Andersen-Ranberg, K., & Jeune, B. Cohort changes in cognitive function among Danish centenarians: A comparative study of 2 birth cohorts born in 1895 and 1905. Dementia & Geriatric Cognitive Disorders, 2008, 26, 153–160. [CrossRef]
- Soriano, J. B., Poulain, M., Grinberg, D., Balcells, S., Busquets, X., Romaguera, D., Alonso-Fernandez, A., Busquets, X., Balcells, S., Gingberg, D. & Poulain, M. Description of extreme longevity in the Balearic Islands: Exploring a potential Blue Zone in Menorca, Spain. Geriatrics & Gerontology International, 2014, 14(3), 620-627. [CrossRef]
- Stathakos, D., Pratsinis, H., Zachos, I., Vlahaki, I., Gianakopoulou, A., Zianni, D., & Kletsas, D. Greek centenarians: Assessment of functional health status and life-style characteristics. Experimental Gerontology, 2005, 40(6), 512–518. [CrossRef]
- Giraldo, G. Counting to 100: A first look at Cuba’s National Centenarian Study. MEDICC Review, 2009 11 (4), 1-19 https://www.medigraphic.com/pdfs/medicreview/mrw-2009/mrw094e.pdf.
- Serra, V., Watson, J., Sinclair, D. & Kneale, D. Living Beyond 100: A Report on Centenarians. London: International Longevity Centre, 2011.
- Green, C. M. Longevity Blue Zone Centenarians: An expository paper. Inquiries Journal, 2021, 13(05). http://www.inquiriesjournal.com/a?id=1899.
- Freeman, S., Garcia, J. & Marston, H.R. Centenarian self-perceptions of factors responsible for attainment of extended health and longevity. Educational Gerontology, 2013, 39(10), 717-728. [CrossRef]
- Sadana, R., Foebel, A. D., Williams, A.N., & Beard, J. R. Population aging, longevity, and the diverse contexts of the oldest old. Public Policy & Aging Report, 2013, 23(20), 18-25. [CrossRef]
- United Nations. Population ageing and development 2009. Department of Economic and Social Affairs, United Nations., 2009.
- Robine, J.M. & Cubaynes, S. Worldwide demography of centenarians. Mechanisms of Ageing and Development, 2017, 165 (Part B), 59-67. [CrossRef]
- Tanprasertsuk, J., Johnson, E.J., Johnson, M.A., Poon, L.W., Nelson, P.T., Davey, A., Martin, P., Barbey, A.K., Barger, K., Wang, X-D., & Scott, T.M. Clinico-neuropathological findings in the oldest old from the Georgia centenarian study. Journal of Alzheimer’s Disease, 70, 2019, 35–49. [CrossRef]
- Aboderin, I. Understanding and Responding to Ageing, Health, Poverty and Social Change in Sub-Saharan Africa: A Strategic Framework and Plan for Research. Outcomes of the Oxford Conference on Research on Ageing, Health and Poverty in Africa: Forging Directions for the Future. Oxford, 2005.
- Ferreira, M. & Kowal., P. Minimum Data Set on Ageing and Older Persons in Sub-Saharan Africa: Process and outcome. African Population Studies, 2013, 21 (1), 19-36. [CrossRef]
- 2021; 15. Author’s Own, 2021.
- Central Statistical Agency of Ethiopia. (CSA). The 2007 Population and Housing Census of Ethiopia-Statistical Report. Addis Ababa, Ethiopia, 2007.
- Jopp, D.S., Boerner, K., Cimarolli, V., Hicks, S., Mirpuri, S., Paggi, M., Cavanagh, A., & Kennedy, E. Challenges experienced at age 100: Findings from the Fordham Centenarian Study. Journal of Aging & Social Policy, 2016, 28, 3, 187-207. [CrossRef]
- Richmond, R.L., Law, J., Kay-Lambkin, F. Morbidity profiles and lifetime health of Australian centenarians. Australian Journal on Ageing, 2012, 31(4), 227–232. [CrossRef]
- Araújo, L., Teixeira, L., Ribeiro, O., & Paúl, C. Objective vs. subjective health in very advanced ages: Looking for discordance in centenarians. Front Medicine, 2018, 5 (189), 1-7. [CrossRef]
- Haslam, A., Hausman, D.B., Davey, A., Cress, E.M., Johnson, M.A., & Poon, L.W. Associations between anemia and physical function in Georgia centenarians. Journal of the American Geriatrics Society, 2012, 60(12): 2362-2363. [CrossRef]
- Sebastião, E. Perceived poor health is positively associated with physical limitations and chronic diseases in Brazilian nonagenarians and centenarians. Geriatrics & Gerontology International, 2015, 16, 1196–1203. [CrossRef]
- Selim, A.J., Fincke, G., Berlowitz, D.R., Miller, D.R., Qian, S.X., Lee, A., Cong, Z., Rogers, W., Selim, B.J., Ren, X.S., Spiro, A., & Kazis, L.E. Comprehensive health status assessment of centenarians: Results from the 1999 Large Health Survey of Veteran Enrollees. Journal of Gerontology: Medical Sciences, 2005, 60A(4), 515–519. [CrossRef]
- Takayama, M., Hirose, N., Arai, Y., Gondo, Y., Shimizu, K., Ebihara, Y., Yamamura, K., Nakazawa, S., Inagaki, H., Masui, Y., & Kitagawa, K. Morbidity of Tokyo-area centenarians and its relationship to functional status. Journal of Gerontology: Medical Science, 62A, 2007 (7), 774–782. [CrossRef]
- Freeman, S., Kurosawa, H., Ebihara, S., & Kohzuki, M. Understanding the oldest old in northern Japan: An overview of the functional ability and characteristics of centenarians. Geriatrics and Gerontology International, 2010, 10 (1), 78-84. [CrossRef]
- Richmond, R.L., Law, J., & Kay-Lambkin, F. Physical, mental, and cognitive function in a convenience sample of centenarians in Australia. American Geriatrics Society, 2011, 59, 1080–1086. [CrossRef]
- Riberio, O., Duarte, N., Teixeira, L., & Paúl, C. Frailty and depression in centenarians. International Psychogeriatrics, 2018, 30, 1, 115–124. [CrossRef]
- Martin, P., Gondo, Y., Arai, Y., Ishioka, Y., Johnson, M.A., Miller, L.S., Woodard, J.L., Poon, L.W., & Hirose, N. Cardiovascular health and cognitive functioning among centenarians: A comparison between the Tokyo and Georgia centenarian studies. International Psychogeriatric, 2019, 31, 4, 455–465. [CrossRef]
- Evert, J., Lawler, E., Bogan, H., & Perls, T. Morbidity profiles of centenarians: Survivors, delayers, and escapers. Journals of Gerontology, 2003, 58, 3, M232-M237. [CrossRef]
- Galanakis, M., Darviri, C., Pelekasis, P., & Tigani, X. Demographic and anthropometric variables related to longevity: Results from a Greek centenarians’ study. Journal of Basic & Applied Sciences, 2015, 11, 381-388. [CrossRef]
- Duran-Badillo, T., Salazar-González, B.C., Cruz-Quevedo, J.E., Sánchez-Alejo, E.J., Gutierrez-Sanchez, G., & Hernández-Cortés, P.L. Sensory and cognitive functions, gait ability and functionality of older adults. Rev. Latino-Am. Enfermagem, 2020; 28:e3282. [CrossRef]
- Herr, M., Arvieu, J.J., Robine, J.M., & Ankri, J. Health, frailty and disability after ninety: Results of an observational study in France: Health after ninety. Archives of Gerontology and Geriatrics, 2016, 66, 166-175. [CrossRef]
- Madrigal-Leer, F., Martìnez-Montandòn, A., Solìs-Umaña, M., Helo-Guzmàn, F., Alfaro-Salas, K., Barrientos-Calvo, I., Camacho-Mora, Z., Jimènez-Porras, V., Estrada-Montero, S., & Morales-Martìnez, F. Clinical., functional., mental and social profile of the Nicoya Peninsula centenarians, Costa Rica, 2017. Aging Clinical and Experimental Research, 2020. [CrossRef]
- Italian Multicentric Study on Centenarians. Assessment of sense of taste in Italian centenarians. Archives of Gerontology and Geriatrics, 1998, 26(2), 177-183. [CrossRef]
- Kliegel, M., Moor, C., & Rott, C. Cognitive status and development in the oldest old: A longitudinal analysis from the Heidelberg Centenarian Study. Archives of Gerontology and Geriatrics, 2004, 39, 143–156. [CrossRef]
- Jopp, D.S., Boerner, K., & Rott, C. Health and disease at age 100: Findings from the Second Heidelberg Centenarian Study. Deutsches Arzteblatt International, 2016, 113, 203–210. [CrossRef]
- Silver, M.H., Jilinskaia, E., & Perls, T.T. Cognitive functional status of age-confirmed centenarians in a population-based study. Journals of Gerontology, B Psychol Sci Soc Sci. 2001, 56(3), 134-40. [CrossRef]
- Aladejare, S. A. Does external debt promote human longevity in developing countries? Evidence from West African countries. Fudan Journal of the Humanities and Social Sciences, 2023, 16, 213–237. [CrossRef]
- Perls, T. Successful aging and its subtypes in centenarians: The Chinese experience. Journal of the American Geriatrics Society, 2023, 71 (5), 1362-1364. [CrossRef]
- Creswell, J.W. Research design: Qualitative, quantitative, and mixed method approaches. Sage. 2003.
- Saldana, J. Fundamentals of qualitative research. Oxford University Press, Oxford, 2011.
- Yin, R. K. Case study research: Design and methods. (3rd Ed.) Sage, 2003.
- Dello Buono, M., Urciuoli, O., & De Leo, D. Quality of life and longevity: A study of centenarians. Age and Ageing, 1998, 27, 207-216. [CrossRef]
- Sun, J., Li, L., & Sun, J. Sensory impairment and all-cause mortality among the elderly adults in China: A population-based cohort study. Aging, 2020, 12(23), 24288-24300. [CrossRef]
- Toyoshima, A., Martin, P., Sato, S. & Poon, L.W. The relationship between vision impairment and well-being among centenarians: Findings from the Georgia Centenarian Study. International Journal of Geriatric Psychiatry, 2018, 33 (2), 414-422. [CrossRef]
- Kuo, H.K., Jones, R.N., Milberg, W.P., Tennstedt, S., Talbot, L., Morris, J.N., & Lipsitz, L.A. Effect of blood pressure and diabetes mellitus on cognitive and physical functions in older adults: A longitudinal analysis of the advanced cognitive training for independent and vital elderly cohort. Journal of the American Geriatrics Society, 2005, 53(7), 1154-1161. [CrossRef]
- Cimarolli, V.R., & Jopp, D.S. Sensory impairments and their associations with functional disability in a sample of the oldest-old. Quality of Life Research, 2014, 23(7), 1977-1984. [CrossRef]
- Liu, C.J., Chang, P.S., Griffith, C.F., Hanley, S.I., & Lu, Y. The nexus of sensory loss, cognitive impairment, and functional decline in older adults: A scoping review. Gerontologist, 2021, 62 (8), 457-467. [CrossRef]
- Araújo, L., Ribeiro, O., Teixeira, L., & Paúl, C. Predicting successful aging at one hundred years of age. Research on Aging, 2016, 38(6), 689-709. [CrossRef]
- McCormack, J. The emergence of centenarians and supercentenarians in Australia. Geriatrics & Gerontology International, 2005, 4 (1), 178-179. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



