Submitted:
27 May 2024
Posted:
28 May 2024
You are already at the latest version
Abstract
Greek roots: "phos" (φῶς) - means "light" and "dynamis" (δύναμις) - means "force" or "power". Photodynamic therapy (PDT) is an innovative treatment method based on the ability of photosensitizers to produce reactive oxygen species after exposure to light of a specific wavelength range, either in the visible or near infrared range. This process results in damage to pathological cells, such as cancer cells, while minimizing the impact on healthy tissues. PDT is a promising direction in the treatment of many diseases, with particular emphasis on the fight against cancer and other diseases asso-ciated with excessive cell growth. The power of light contributed to the creation of phototherapy, whose history dates back to ancient times. It was then noticed that some substances exposed to the sun have a negative effect on the body, while others have a therapeutic effect.
This work provides a detailed review of photodynamic therapy, from its origins to the present day. It is surprising how a seemingly simple beam of light can have such a powerful healing effect, which is used not only in dermatology, but also in oncology, surgery, microbiology, virology, and even dentistry. However, despite promising re-sults, photodynamic therapy still faces many challenges. The availability of this thera-py is limited due to the small number of centers offering this type of treatment and the high costs, which may be unaffordable for many patients. Moreover, photodynamic therapy requires further research and improvement.
Keywords:
PDT
; photomedicine
; phototherapy
1. Introduction
Sunlight healing, known as heliotherapy, was practiced by many ancient cultures around the world [1,2]. For example, the Greeks preferred a form of heliotherapy in which participants lay naked in specially designated areas, subjected to total body exposure to the sun, called arenation. The Greek physician Herodotus is considered one of the pioneers of this method. His teaching emphasized the usefulness of sun exposure for restoring health. The Egyptians, Chinese and Indians also believed in the beneficial effects of sunlight on overall health and attempted to cure various diseases using this natural light source, including rickets, psoriasis and psychoses. In addition, light helped the Egyptians mask symptoms of vitiligo - they used juice from the Egyptian amine fruit, which after exposure to solar radiation imitated a natural tan [3,4]. Over time, together with the advent of Christianity, both sun worship and the use of sunlight as a method of healing came to be considered pagan practices, although they continued in various forms.
Figure 1.
Heliotherapy in ancient times.
Important events in the history of phototherapy were the discovery and description of infrared radiation by Herschel in 1800 and ultraviolet radiation by Ritter in 1806 [5]. At the turn of the 18th and 19th centuries, light began to be used in France as a form of therapy to treat various diseases. At that time, light was used to treat diseases such as tuberculosis, psoriasis, scurvy, rheumatism, paralysis and muscle weakness. In the 19th century, the bactericidal properties of ultraviolet radiation were discovered [6]. This discovery was groundbreaking to treat infections, and ultraviolet light therapy became popular. Danish researcher Niels Finsen used this knowledge and used an arc lamp to irradiate patients suffering from cutaneous tuberculosis (lapus vulgaris). His research work and the use of light therapy brought excellent results, for which he was awarded the Nobel Prize in medicine in 1903 [7]. Finsen, born in the Faroe Islands, he was also interested in light contrasts and darkness near the Arctic Circle, which prompted him to study the influence of light on living organisms. He performed experiments on light and published a paper in 1893 on the treatment of smallpox with red light, which it prevented purulent inflammation of pimples [8]. The first report on the photodynamic method dates back to 1900 and was prepared by a medical student, Oscar Raab, who worked in the laboratory of Professor Herman von Tappeiner in Munich [9]. During his research on the use of acridine dyes, Raab noticed that the results of an experiment performed on paramecium colonies varied depending on conditions such as the time of day and the amount of light (in 1902 Ledoux-Lebards discovered that oxygen was also necessary to achieve this effect.) After many attempts, he described the basics of the theory of photodynamic reactions [10]. In the following years Oscar Raab continued his research on the application of photodynamic reactions in collaboration with his teacher, Hermann von Tappeiner. Their research focused, among others, on the use of this method in the treatment of skin lesions associated with tuberculosis and syphilis. In 1903, Tappeiner and a dermatologist named Jesionek used a combination of eosin and light application in the treatment of skin cancer [11]. We also owe Tappeiner the introduction of the term "photodynamic" therapy, i.e. light-dependent therapy. In 1911, Hausmann conducted experiments on mice and described the photosensitizing activity of hematoporphyrin. He injected the animals with this substance and then exposed them to sunlight. The results of these experiments were photosensitizing reactions that had varying degrees of intensity. In 1913, German researcher Friedrich Meyer-Betz decided to investigate whether a similar phenomenon also occurred in humans. He gave himself 200 mg intravenously hematoporphyrin and then exposed his skin to sunlight. The effect of this experiment was increased swelling, pain and itching in the areas that were irradiated [10,11]. One of the most important reports was the selectivity of hematoporphyrin towards cancer cells, described by Palikard in 1924. Subsequent years of experience led to the creation of a derivative of hematoporphyrin, HpD (English: hematoporphyrin derivative), which is a porphyrin ester with even greater selectivity towards cancer cells. In the years 1942-1948, scientists Auler, Banzer, Figge and Weiland conducted research on the use of porphyrins in diagnosis and treatment using the photodynamic method. In 1942, Auler and Banzer studied porphyrins administered to the body, which led to further understanding of their potential use in photodynamic therapy. In 1948, Figge and Weiland continued research on various porphyrin derivatives and searched for their applications in diagnostics and therapy using the photodynamic method. In 1955, Rasmussen-Taxdal and colleagues described the usefulness of a diagnostic method that involved intravenous administration of photosensitizer, enabling tumor localization during the procedure operational. It was not until 1972 that studies conducted in a mouse model of glioma were published, in which tumor growth was inhibited even up to twenty days after the use of photodynamic therapy [12]. In 1975, Kelly and his colleagues performed effective photodynamic therapy in a patient with bladder cancer [13]. At the same time, Thomas Dougherty published a report on the complete cure of cancerous tumors in mice after using photodynamic therapy with a porphyrin derivative. This breakthrough result was the beginning of further research on the use of photodynamic therapy in humans. Just three years later, Dougherty reported successful use of the therapy photodynamic therapy in the treatment of 113 skin tumors (primary and metastatic) in 25 patients. Of these cases, 98 tumors were completely cured, 13 showed a partial response to therapy, and only 2 tumors were completely resistant to therapy [14]. Despite very good therapeutic effects obtained using HpD, due to long-lasting phototoxicity (which lasted from four to six weeks), the search for alternative photosensitizing compounds began. Later, in the 1990s, scientists from Russia developed an innovative vapor-copper laser system, the radiation of which had a significant impact in the field of medicine. An earlier Russian achievement researchers also developed a new photosensitizer called Photogem, which was produced from hematoporphyrins in 1990 by a team led by Professor Andrey F. Mironov in Moscow. Photogem received approval Ministry of Health of Russia and underwent clinical trials from 1992 to 1996. Among 1,500 patients who underwent photodynamic therapy with Photogem, 91 percent showed a clear therapeutic effect and 62 percent of patients achieved complete tumor clearance. In the remaining patients, 29 percent had partial tumor shrinkage, and its reduction was at least half. For patients with a previous diagnosis, 92 percent showed complete tumor clearance [15].

Table 1.
History of photodynamic therapy.
| Year(s) | Researcher(s) | Clinical or experimental work |
|---|---|---|
| 1841 | Scherer | Discovery of hematoporphyrin by removing iron from dried blood |
| 1861-1871 | L.Pasteur, P. Bert | Discovery of phototoxicity |
| 1867 | J.L.W. Thudichum | Spektrum fluorescencji tej czerwonej substancji (hematoporfiryny) oraz fluorescencja |
| 1871 | F. Hoppe-Seyler | Giving a name to the red substance (hematoporphyrin) |
| 1874 | Schultz | Description of a patient with porphyria (errors in heme biosynthesis) |
| 1895-1903 | N.R.Finsen | Phototherapy (Nobel Prize 1903) |
| 1897-1904 | O. Raab, H. von Tappeiner | First reports about phototherapy |
| 1904 | H. von Tappeiner | Introduction of the term "photodynamic action" |
| 1903-1905 | - | The first "before and after" photos of patients (eosin exposure) |
| 1908-1913 | W. Hausmann, F. Meyer-Betz | Many PDT experiments with hematoporphyrin on paramecia, erythrocytes, mice, guinea pigs and humans |
| 1924 | - | A.Policard saw red porphyrin fluorescence in tumors, which was the first observation of tumors |
| 1925 | H. Fisher | The study of porphyrins, for which the Nobel Prize was awarded in 1929. |
| 1945 | S. Scwarz | Radiation hypersensitivity to porphyrins was noted |
| 1959 | D. Harman | A free radical theory of aging and disease has been proposed |
| 1960-1967 | R. Lipson, E. Baldes | HpD synthesis was performed |
| 1970 | H. Kautsky, G. Herzberg | Zauważono rolę aktywnego tlenu |
| 1975 | Z. Malik, M. Djaldetti | ALA was used to induce PpIX |
| 1983-1993 | T. J. Dougherty i inni | Photofrin was used |
| 1990 | J. Kennedy, R.Pottier | ALA has been used in the clinic |
| 1995 | cPDT with Photofrin, the first clinically approved photosensitizer for cancer treatment, was produced by Dougherty and his colleagues. Photofrin, which is a pure formulation of HpD, has received approval from the US Food and Drug Administration (FDA). | |
| 1993 | Photofrin becomes commercially available Representative approval of porphyrin sodium in Canada (bladder cancer) |
|
| 1994 | Representative approval of porphyrin sodium in Japan and the Netherlands (esophageal and lung cancers) | |
| 1995 | Representative approval of porphyrin sodium in the US and Canada (esophageal cancer) | |
| 1996 | Representative approval of porphyrin sodium in France (esophageal cancer) | |
| 1997 | Representative approval of porphyrin sodium in Germany (lung cancer) | |
| 1998 | Representative approval of porphyrin sodium in the US and UK (lung cancer) | |
| 1999 | Photodynamic therapy (PDT) targeting antibody fragments (Neri) has been described. | |
| 2001 | Foscan approved in the EU for head/neck cancer in June, despite Scotia's collapse in January (Scotia/Biolitec) Visudyne as an effective first-line PDT for AMD (QLT). Foscan approved for the treatment of HNSCC in Europe. |
|
| 2003 | Photodynamic therapy (PDT) targeting the HER2 receptor using whole IgG antibodies. Telaporfin (NPe6) approved in Japan for photodynamic therapy of lung cancer |
|
| 2004 | Metwix (methylaminolevulinate, MAL) is approved by the US Food and Drug Administration (FDA) for use in photodynamic therapy (PDT) for the treatment of actinic keratosis (AK) and drug-induced carcinogenesis Polymer complex of chlorin e-6 with polyvinylpyrrolidone approved for photodynamic therapy in Russia |
|
| 2006 | randomized clinical trials of dPDT in northern Europe.. | |
| 2007 | HER2-targeted photodynamic therapy (PDT) using scFv. | |
| 2011 | ALA (10% topical gel) approved by EMA for the treatment of AK | |
| 2012 | Silicone phthalocyanin Pc4 has successfully completed Phase I clinical trials for topical application in photodynamic therapy (PDT). | |
| 2014 | Recommended photodynamic day therapy with MAL (16% topical cream) for the treatment of AK in Australia | |
| 2016 | Sellera published the first clinical study on veterinary photodynamic therapy (PDT) using antibacterial agents for the treatment of infected pododermatitis lesions in penguins EMA has extended the indications for the use of ALA (10% gel for topical use) to include the treatment of BCC and photodynamic day therapy |
|
| 2017 | FDA Approved Oral ALA for Fluorescent Guidance of Brain Tumor Resection (Non-PDT) | |
| 2018 | Padeliporfin is approved by the European Medicines Agency (EMA) for the treatment of prostate cancer. | |
| 2019 | Guided anticancer therapy FA@PDA using PDT | |
| 2020 | Anticancer therapy PTT + PDT | |
| 2021 | The use of chemotherapy in combination with PTT + PDT | |
| 2022 | PTA therapy | |
| 2023 | A group of scientists from the City University of Hong Kong (CityU) have made an important discovery by creating a new type of photo-oxidants that respond to near infrared. These substances are able to effectively eliminate cancer cells without requiring the presence of oxygen. | |
| 2024 | The latest preclinical studies have confirmed the effectiveness of 5-ALA in the treatment of gliomas in brain organoids, leading to the death of cancer cells while not negatively affecting healthy cells. Applying PDT to 3D tumor models |
|
The history of photodynamic therapy is a story of humanity's constant striving to overcome the limits of possibilities. It is a story that does not end with the achievements of 1990, but that is when it gains real momentum. In the following decades, scientists not only developed this technique, but also discovered surprising new applications of light in medicine. In this work, we will look at how a seemingly simple beam of light became a powerful tool in the hands of doctors, enabling the fight against diseases that until recently seemed incurable. We will follow the evolution of photodynamic therapy, which is proof that the human mind knows no limits when it comes to saving lives.
2. Materials and Methods
2.1. Literature Search
The literature search was a key step in developing the history of photodynamic therapy. A systematic analysis of scientific works published until 2023 available on platforms dedicated to scientific papers was used. This process included a careful review of available articles, reviews, clinical trials, and literature reviews related to photodynamic therapy.
2.2. Inclusion and Exclusion Criteria
Inclusion criteria included research papers that focused on photodynamic therapy, both in the context of basic science and clinical applications.
Articles containing information on new scientific discoveries, technological innovations and advances in the field were given priority.
On the other hand, works that did not provide relevant data or were not related with the development of photodynamic therapy, were excluded from the analysis.
2.3. Analysis Process
After screening the papers in accordance with the inclusion and exclusion criteria, an in-depth analysis of the selected articles began. Key information was identified, such as: stages of development of photodynamic therapy, photosensitizers used, imaging techniques, and results of clinical trials. The analysis also included an assessment of the methodological quality of the studies examined.
2.4. Analysis Categories
When analyzing the literature across materials and methods, several key categories were identified. These included:
- History of the development of photodynamic therapy
- Application of photodynamic therapy in various fields of medicine
- Scientific discoveries influencing the development of this method
- Technological innovations and their impact on the effectiveness of therapy photodynamic
2.5. Systematization of Data
The collected information was systematized according to chronological order illustrating the evolution of photodynamic therapy over the years. Additionally, information was grouped thematically, which allowed the identification of key information areas of research and achievements. Carrying out the analysis of materials and methods in accordance with the described criteria allowed us to obtain a comprehensive and in-depth picture of the history of photodynamic therapy and current scientific achievements in this field.
3. Results
3.1. Mechanism of Action of PDT
Photodynamic therapy is a molecular process that involves the interaction of three non-harmful ingredients: a photosensitizer (PS), light of an appropriate wavelength and oxygen dissolved in cells. These ingredients produce the desired effects only in pathological tissues [16]. The two main mechanisms of the photodynamic reaction are strictly dependent on the presence of oxygen molecules in cells. In both mechanisms, the first stage is similar. After entering the cell, the photo-sensitizer is irradiated with light with a wavelength covering the PS absorption spectrum. As a result of photon absorption, the photosensitizer is transformed from the S° ground singlet energy state to the S1 excited singlet state. Part of the energy is emitted as a fluorescence quantum, and the rest of the energy directs the photosensitizer molecule to the excited T1 triplet state, which is the therapeutic form of the compound [17,18]. In the type I mechanism, in the excited triplet T1 state, the photosensitizer transfers energy to biomolecules from its surroundings. A hydrogen or electron transfer occurs between the photosensitizer and the cancer tissue, which leads to the formation of free radicals and anionic radicals of the photosensitizer and the substrate. The electrons interact with the oxygen molecules, which remain in their basic energy state. This process leads to the production of reactive oxygen species (ROS), initially in the form of the anionic superoxide radical (O2•−), which creates further generations of ROS inside cells. The initiated cascade of reactions leads to oxidative stress, resulting in the destruction of cancer cells [19,20]. In the type II mechanism, energy is transferred directly to the oxygen molecule in its ground energy state (ground triplet state) as a result of the photosensitizer's transition to the excited triplet state. Direct energy transfer between particles (PS → O2) is possible because they have the same spins. In this way, excited oxygen particles are created - the so-called singlet oxygen - which are characterized by extremely strong oxidizing properties [21]. Most organic compounds are in the singlet ground state. However, oxygen particles are characterized by a triplet state (as the basis) and excitation to singlet. Thanks to this fact, the excited photosensitizer particles do not damage organic cellular structures and react only with oxygen particles dissolved in the cytoplasm [22]. It is assumed that the type II mechanism is the most important process determining the effectiveness of PDT. However, the ratio of the contribution of both mechanisms depends on many factors, including: oxygen concentration, tissue dielectric constant and pH, and the structure of the photosensitizer. As oxygen is depleted, the type I mechanism begins to predominate. Strongly reactive oxygen species cause photodamage to proteins, fats and other molecules in the photosensitized area. This leads to direct death of cancer cells through apoptosis and/or necrosis [23]. The mutual contribution of different types of cell death depends on the location of the photosensitizer within the cell. Damage to mitochondria may lead to apoptosis, destruction of cell membranes and loss of integrity may induce necrosis, and damage to lysosomes or endoplasmic reticulum may provoke autophagy [24,25].
3.2. Development of PDT Technology
The development of photodynamic therapy (PDT) technology since 1990 has brought numerous innovations and advances that have significantly improved the effectiveness and application of this method in medicine. The main aspects of PDT development include the selection of appropriate photo-sensitizing drugs, improvement of light source technology, adaptation of dosing protocols, development of imaging and miniaturization of devices. Over the years, interest in PDT has grown at a dynamic pace, as evidenced by the number of scientific works published in the years 1980 - 2023. The smallest number of works written falls in 1982 and amounts to 53 works, while their largest number in 2022 reached 3,381. This shows how dynamically this field is developing and how much interest there is among scientists in this treatment method.
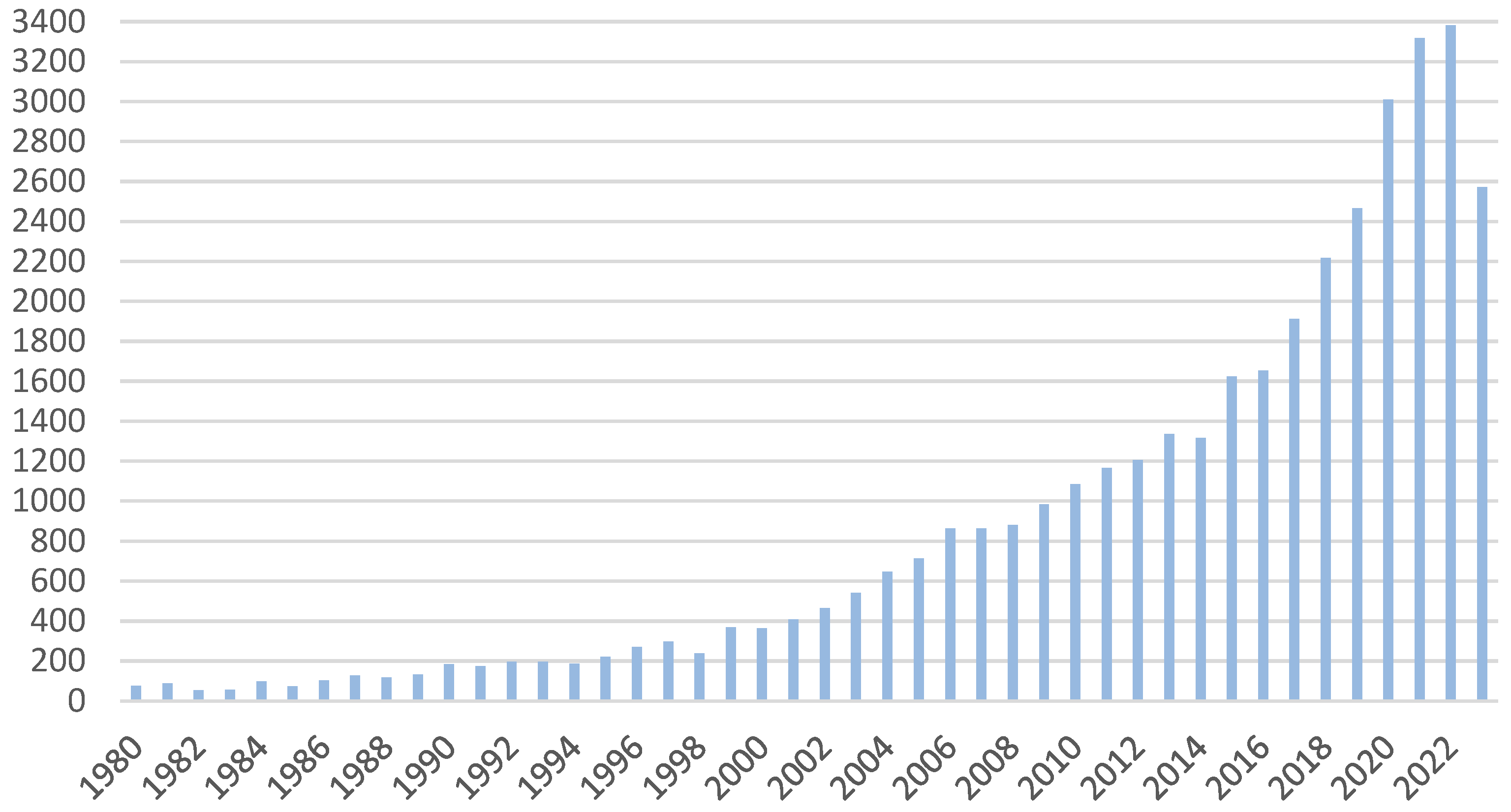
Figure 2.
Number of published scientific papers on PTD according to Pubmed.
3.2.1. Photodynamic Therapy in the Years 1990–1995
The first milestone in the history of PDT treatment (with Photofrin) was achieved in 1993, when Canada became the first country in the world to approve this drug for the preventive treatment of bladder cancer. This event marked the beginning of Photofrin's international expansion. Subsequently, approvals for Photofrin were obtained in the Netherlands and France. In these countries, the drug began to be used to treat advanced esophageal and lung cancer. Germany also recognized Photofrin's potential, approving it for the treatment of early-stage lung cancer. Japan went a step further by approving Photofrin not only for the treatment of early-stage lung cancer, but also for esophageal, stomach and cervical cancers, as well as cervical dysplasia.
In 1993, as a result of a study conducted in Canada, Photofrin-PDT was approved for prophylactic treatment after surgical removal of papillary bladder tumors in patients at high risk of recurrence. Although the full results of this study have not been published, preliminary results were presented in 1991 [26]. After one year of follow-up of 34 patients, disease recurrence was found in 81% of patients who did not receive PDT after surgery and in 39% of patients treated with PDT. The mean time to recurrence was 91 days for the control group and 394 days for the PDT-treated group. Among patients receiving PDT, one third experienced photosensitivity and 93% had urinary symptoms. Due to severe and long-lasting side effects, Nseyo and colleagues [27] suggested the use of multiple therapies at a lower drug dose to reduce the frequency and severity of symptoms after PDT for superficial bladder cancer.
In December 1995, after the completion of phase three clinical trials in the United States, Photofrin received FDA approval [28]. A multi-center study compared PDT with Nd-YAG laser thermal ablation in the treatment of partially obstructive esophageal cancer. The study included 236 patients and showed similar reductions in dysphagia in both groups. However, PDT showed a longer tumor response time (32% at 1 month vs. 20% for Nd-YAG) and more complete responses (negative endoscopic biopsies) than Nd-YAG (9 vs. 2). In some subgroups, PDT showed higher objective responses than Nd-YAG, especially in the upper and lower third of the esophagus, and also for tumors larger than 10 cm. However, the number of patients in these groups was too small to achieve statistical significance. Fewer procedures were required for PDT (mean 1.5) than for Nd-YAG (2.4), and median survival was the same for both groups. There were more adverse reactions in the PDT group (92%) than in the Nd-YAG group (82%), but the rate of withdrawal from the study due to an adverse reaction was similar in both groups. Significantly more esophageal perforations occurred in the Nd-YAG group (7%) than in the PDT group (1%). Sunburn reactions occurred only in the PDT group (19%) and were all mild. The effectiveness of both treatments was equivalent; serious adverse reactions occurred at the same rate in both treatments, except for a higher incidence of perforation in the Nd-YAG treatment. PDT was considered more comfortable for the patient, was easier to perform than Nd-YAG ablation, and was particularly beneficial in situations where Nd-YAG is difficult to perform due to tumor morphology or location.
3.2.2. Photodynamic Therapy in the Years 1996–2000
In 1996, Biel [29] published the results of a study on the treatment of early-stage head and neck cancer with Photofrin. This study included a variety of tumor types, including 29 patients with laryngeal cancer (22 of which were superficial), 32 patients with nasopharyngeal cancer, one patient with nasal cavity cancer, two patients with Kaposi's sarcoma of the palate, three patients with nasopharyngeal cancer, and five patients with laryngotracheal papilloma. Patients received a dose of 2.0 mg/kg Photofrin and 48 hours later were irradiated with 630 nm light using a microlens fiber at 50–75 J/cm2. For tumors larger than 3 cm, diffusion fibers were implanted and a dose of 100 J/cm fiber was delivered interstitally. All 22 patients with superficial laryngeal cancer achieved a complete response, with a mean follow-up of 30 months (up to a maximum of 67 months). Similar results were achieved in patients with oral, intranasal or nasopharyngeal cancer who were followed for a mean of 33 months (up to a maximum of 61 months). Five patients with recurrent laryngeal/tracheal papilloma initially responded to PDT, but disease recurrence was observed 6 months after PDT. Two patients required oral steroids for 5 days due to sunburn. Post-treatment pain ranged from mild to severe but was effectively controlled with oral analgesics.
In 1997, researchers conducted the largest photodynamic therapy (PDT) study using Photofrin on patients with superficial esophageal cancer [30]. This disease often occurs together with Barrett's esophagus, a condition in which the squamous epithelium of the esophagus is replaced by the glandular epithelium of the stomach due to acid reflux. Patients with Barrett's esophagus are at risk of developing esophageal cancer, for which the standard treatment is esophagectomy, a surgical procedure with a high mortality rate. The study included 55 patients and after six months of follow-up after PDT showed that 24 of 36 patients with initial high-grade dysplasia and Barrett's esophagus had no dysplasia and seven had no residual Barrett's esophagus. Three of 36 patients with high-grade dysplasia did not respond to treatment and nine converted to low-grade dysplasia. The technique involved injecting 2.0 mg/kg Photofrin followed by light delivery 48 hours later. In some patients, a 3-, 5-, or 7-cm balloon catheter was used in which the light delivery fiber with a diffuser of the appropriate length was centered. The balloon allowed for proper dilation of the esophagus and provided uniform light delivery to the affected areas. Complications included esophageal stricture in 29 patients, which required dilatation. Photosensitivity was of low frequency. For PDT compared with surgery, the mortality rates were 0% and 6%–14%, respectively. Moreover, PDT was an outpatient procedure with a much shorter recovery time and was associated with much lower procedural costs.
In 1999, a new era began in the United States in the treatment of age-related macular degeneration (AMD), which is the leading cause of irreversible vision loss in people over 50 years of age. This year, photodynamic therapy (PDT) with verteporfin (Visudyne®) was approved by the Food and Drug Administration (FDA) for the treatment of patients with the predominantly classic form of subfoveal neovascularization, which is one of the more serious types of AMD. Results from phase I-II clinical trials showed that PDT with verteporfin could safely stabilize CNV leakage in most patients for up to 3 months. Phase III trials that assessed the long-term prognosis of PDT treatment of CNV in AMD were successful, and several tens of thousands of patients were successfully treated [31].
Also in 1999, the USA saw a groundbreaking use of PDT in dermatology. PDT has gained recognition for its effects in the treatment of solar keratoses - one of the most common skin lesions [32]. These keratoses are characterized as erythematous, flat and scaly lesions, appearing mainly on sun-exposed areas of the skin, especially in people with fair skin. Their diameter may vary from a few millimeters to several centimeters [33]. Traditionally, solar keratosis has been treated with methods such as cryosurgery, laser ablation, dermabrasion, and other techniques. However, the introduction of ALA-PDT (5-aminolevulinic acid-based photodynamic therapy) and MAL-PDT (methyl aminolevulinate-based photodynamic therapy) into clinical practice has yielded breakthrough results. The approval of these treatment methods resulted in high effectiveness, achieving 89-92% elimination of skin lesions, especially those located on the face and scalp [34].
3.2.3. Photodynamic Therapy in 2001–2005
Foscan, also known as temoporfin or m-tetrahydroxyphenylchlorin (mTHPC), is a significant drug used in photodynamic therapy (PDT). In 2001, Foscan received approval from the European Medicines Agency (EMA) for advanced squamous cell carcinoma of the head and neck. In 2000, it was submitted to the US Food and Drug Administration (FDA), but it was not approved there. Foscan has been studied in a variety of clinical contexts, including the treatment of unresectable cholangiocarcinomas, unresectable non-small cell lung cancer, and nasopharyngeal cancer. Initially, Foscan was produced by Scotia Pharmaceuticals in Scotland, but later the rights were taken over by the German company Biolitec. Although Foscan has many advantages, such as high power and a high absorption peak at 652 nm, it also has some disadvantages. Due to its exceptional power, it can damage healthy tissue surrounding the tumor. Furthermore, there is a risk of skin burns due to PS extravasation at the infusion site [35].
In 2003, another study was conducted on photodynamic therapy (PDT) using verteporfin. This study, which was non-randomized and prospective, included 19 patients suffering from symptomatic, limited angiocellular hemangioma. Before starting photodynamic therapy, four patients underwent unsuccessful initial treatment, such as external beam irradiation or laser photocoagulation. Eligibility criteria for the study included the presence of subretinal exudation involving the macula, decreased visual function and additional symptoms such as metamorphopsia. During photodynamic therapy, verteporfin was used at a concentration of 6 mg/m(2) of body surface and a light dose of 100 J/cm(2) with a length of wave 692 nm. The average follow-up time of patients was 10.6 months, and the number of treatment sessions ranged from 1 to 5. The results were promising. Vision improved by at least one line in 73.3% of patients and by at least two lines in 42.1% of patients. Exudation completely resolved in 94.8% of cases, and tumor size decreased in all tumors examined. No recurrences or local or systemic side effects were observed during the follow-up period [36].
In 2004, there were reports of clinical trials using photodynamic therapy (PDT) in the treatment of cholangiocarcinoma (CC). In these studies, almost two-thirds of patients died from progressive CC. Additionally, approximately 5 to 10% of patients died from paraneoplastic pulmonary embolism associated with advanced tumor stage or from gastrointestinal bleeding secondary to tumor invasion into the duodenum or biliary cirrhosis. One quarter of patients died prematurely due to severe infectious complications. Chronic cholangitis led to secondary biliary cirrhosis and fatal complications such as variceal bleeding in two patients with slow tumor progression. Studies have shown that when PDT was used repeatedly to treat progressive disease and resulting segmental biliary tree obstructions, a significant increase in median survival could be expected in the range of >9 to 16.2 months. Even patients in poor condition benefited from PDT [37]. In 2005, scientists from the Weizmann Institute in Israel, Avigdor Scherz and Yoram Salomon, made a breakthrough in the development of Tookadu, a drug used in photodynamic therapy. Struggling with the problems associated with the use of Cremophor in clinical trials, they developed a new, water-soluble derivative of Tookadu. They used a process known as aminolysis, using the amino acid taurine, to create a new compound, which was named WST-11. This compound, later named Stakel and then Padeliporfin, proved to be a key step forward in photodynamic therapy. The production of this new compound was undertaken by Steba Biotech based in Luxembourg. WST-11, like its predecessor WST-09, was found to act very rapidly and was activated in blood vessels, which is characteristic of a type I photochemical process called vascular-targeted PDT or VTP [38].
3.2.4. Photodynamic Therapy in 2006–2010
In 2006, it was announced that photodynamic therapy (PDT) may be effective in the treatment of lung cancer. Studies have shown that PDT with Photofrin increases the expression of vascular endothelial growth factor (VEGF) and prostaglandin E2 in murine tumors. Additionally, it was noticed that the combination of VEGF or cyclooxygenase-2 inhibitors with PDT therapy increases its therapeutic effectiveness. It has also been found that tumors treated with PDT show increased expression of matrix metalloproteinases (MMPs), and pharmacological inhibition of MMPs may enhance the antitumor effects of PDT in vivo [39].
In 2007, photodynamic therapy (PDT) gained importance not only in the fields of dermatology and oncology, but also in microbiology. Research conducted by Smijs' team used an ex vivo human skin model to assess the ability of porphyrins to eliminate T. rubrum. Photosensitizers in liquid carriers were applied to skin that had previously been infected with a dermatophyte. It was found that short incubation periods (8 hours) led to complete destruction of the fungus after irradiation (108 J cm−2, 580–870 nm). However, longer incubation periods (>24 hours) before exposure did not lead to the elimination of the fungus [40].
At the same time, photodynamic therapy (PDT) has been intensively researched in various medical fields. In one study conducted by a team of scientists [41], 15 patients with histologically confirmed actinic cheilitis were treated with PDT using MAL. After two treatment sessions, one week apart, complete clinical remission was observed in almost half of the patients. Nevertheless, histopathological examinations showed signs of dysplasia in most patients, which could suggest that the uneven surface of the lips could lead to uneven absorption of the photosensitizing agent.
Additionally, in a European, randomized, multicenter, placebo-controlled trial [42], the effectiveness of PDT with MAL was compared with cryotherapy and 5-FU in patients with Bowen's disease. The results of this study indicated that PDT with MAL achieved the highest rate of complete remission at 12 months.
Moreover, research conducted by Zane and colleagues [43] showed that PDT can affect collagen fibers, which suggests the possibility of stimulating collagen synthesis. These studies have also shown that PDT can lead to the reorganization or accumulation of new collagen fibers, which may help to improve skin texture.
In 2009, photodynamic therapy (PDT) was described as a potentially effective method of local treatment of nasopharyngeal cancer (NPC), which is not associated with the severe side effects observed in radiotherapy. PDT is effective in eliminating NPC, with effective local inhibition of tumor growth. Many advantages of PDT have been noted, including the possibility of repeating the therapy, lack of cumulative ef-fects and specific effects on cancer cells. The studies used a first-generation photosen-sitizer, hematoporphyrin. Others, in turn, have shown that the second-generation photosensitizer, temoporfin, is more effective. Nasopharyngeal illumination was a challenge, so a new dedicated light delivery applicator was developed [44]. In 2010, a study was conducted on the use of photodynamic therapy (PDT) in the treatment of anal cancer. All study participants went through the PDT process in accordance with the guidelines, without any harm to their health. The procedure was well tolerated with no unforeseen or excessive complications. The entire therapy was performed on an outpatient basis, without the need for hospitalization or visits to the emergency department. No complications were observed after the administration of Photofrin® and none of the patients experienced solar photosensitization. Immediately after PDT treatment, the tumor area became dark and red and began to secrete fluid. Interestingly, none of the patients reported pain at this point. After 24 hours, the tumor area remained dark but was no longer shedding fluid. Healthy tissue appeared clinically unchanged compared to unilluminated regions. The treatment sites were very sensitive to touch. Similar results were observed after 48 hours. All patients controlled their sphincters during this time. Approximately 6-12 hours after PDT, patients experienced an increase in pain around the anus, most noticeable during bowel movements and prolonged sitting. By using additional painkillers, they were able to minimize these symptoms. The intensity of this discomfort decreased significantly after 72-96 hours in all cases. Applying ice to the anal area provided excellent and rapid short-term relief. The use of analgesics was sporadic from the end of the first week and was not necessary 1 month after PDT. Patients were then followed monthly or less frequently. At the first follow-up visit one month later, the tumor was necrotic and appeared to be healing peripherally. No patient had significant pain at this point, and all returned to regular follow-up examinations. Each patient had a repeat biopsy between 3 and 4 months after PDT, and all showed NED. After 6 months, all patients were re-evaluated. None showed local or pelvic recurrence, but two patients had evidence of systemic disease and received chemotherapy. At the last follow-up visit (18–48 months), no patient had local failure, wound healing problems, or sphincter damage caused by PDT [45].
3.2.5. Photodynamic Therapy in 2011–2015
In 2011, a pioneering study was conducted that opened new horizons in the treatment of potentially malignant oral diseases using photodynamic therapy (PDT). In this prospective study, a group of 147 patients underwent PDT with surface illumination using 5-aminolevulinic acid (5-ALA) or meta-tetra(hydroxyphenyl)chlorin (mTHPC) as photosensitizers. The patients, with an average age of 53, did not experience any complications after the procedure. During an average of 7.3 years of follow-up, clinical and histopathological features as well as the rate of recurrence and malignant transformation were compared. The analysis showed that homogeneous leukoplakia occurred in 55 patients, heterogeneous leukoplakia in 73 patients, and 19 patients had erythroplakia. The patients were dominated by former and current lifelong smokers (84.4%). Erythroplakias have mainly been identified in heavy lifelong smokers. The most frequently identified primary anatomical locations are the lateral edge of the tongue, the floor of the mouth and the retromandibular area. Among the patients, 33 were identified as having moderate dysplasia, while 63 patients had severe dysplasia; and 32 patients had a histopathological diagnosis of carcinoma in situ. The recurrence rate for laser surgery was approximately 11.6%. Malignant transformation was observed in 11 patients (7.5%), on the tongue, floor of the mouth and retromandibular area. Recurrence and malignant transformation were mainly identified in erythroplakias and heterogeneous leukoplakias. In conclusion, a 2011 study showed that 5-ALA-PDT and/or mTHPC-PDT offer an effective alternative therapy for potentially malignant oral diseases. Complete response to therapy was identified in 119/147 patients (81%) [46].
Also in 2011, a significant study was conducted to understand the effects of photodynamic therapy (PDT) on papilloma acuminata. The study involved 15 people with histologically confirmed, treatment-resistant acuminal papilloma located in various locations. Patients underwent several cycles of PDT after receiving aminolevulinic acid (ALA). The study showed complete recovery in nine out of fifteen people after five PDT sessions. Lesions in the anal area showed particularly rapid remission. As progress towards complete removal of lesions was observed, dense infiltration of CD4+ T cells was observed in the superficial skin, accompanied by the accumulation of Langerhans cells. At the same time, CD8 began to increase in the lesions of patients responding to treatment, and Langerhans cells appeared to migrate toward the dermis. CD68+ macrophages apparently did not participate in the immune response. In summary, the 2011 study provided valuable information on the effect of ALA-PDT on infiltrating immune cells in acuminal papillomas. The results confirmed previous clinical data, suggesting that rapid activation of specific immunity in the affected skin, CD4+ T cells and dendritic cells could be responsible for healing. This study represented an important step in understanding and treating acuminal papillomas with PDT.
In 2012, a study was conducted on the treatment of warts using photodynamic therapy with aminolevulinic acid (ALA PDT). Unlike previous studies that focused on the use of red PDT light after long-term incubation and occlusion, this study focused on the use of blue light and short-term incubation without occlusion or prior evaporation. The study included adults with at least two resistant warts on the back of the hand or periungual warts. Patients were randomly assigned to receive placebo or 20% ALA. After a 1-hour incubation period, the papillae were exposed to 417-nm blue light for 1,000 seconds. The overall response pattern was not statistically different between the two groups. Only two of the 12 warts treated with cryotherapy disappeared. This response pattern was not statistically different from PDT-treated warts. One patient complained of a burning sensation after ALA application, which was attributed to the acidic solution penetrating through the nipple cracks. All reported moderate to severe pain during cryotherapy and variable discomfort for several days afterwards, but no other adverse effects [47].
In 2013, a study was conducted on the treatment of peri-implantitis, a bacterial complication following the implantation of dental implants. This study was randomized, comparative and included 20 patients and 20 controls. The aim was to compare the antibacterial effectiveness of PDT with surgical therapy in patients with periimplantitis who received dental implants with a rough surface. The surgical group underwent mucoperiosteal flap surgery with scaling on the implant surfaces and removal of granulation tissue. Microbiological testing was assessed before and after interventional treatment, at weeks 12 and 24 in subjects. No significant difference in total anaerobic bacteria was observed between patients treated with PDT and those treated surgically. However, PDT was associated with a significant decrease in bleeding rates and inflammatory secretions, visible even 24 weeks after the procedure [48].
In 2015, a study was conducted on the treatment of actin damage, which is responsible for the development of multiple, recurrent non-melanoma skin cancers (NMSC), including actin keratoses (AK). This study compared the effectiveness and safety of photodynamic therapy with methylaminolevulinate (MAL-PDT) and imiquimod cream (IMIQ) 5% in preventing the development of new NMSCs in patients with field lesions. The study included patients with a tumor field on the face or scalp who were randomly assigned to receive MAL-PDT on one side and IMIQ 5% on the mirror field. The main aim of the study was to examine the number of new lesions in treated fields during a 12-month observation period. No significant difference in the development of new NMSCs was observed between patients treated with MAL-PDT and those treated with IMIQ. Both treatments were safe and well tolerated. Patients showed a preference for MAL-PDT based on procedure, response rates, and future choice. In summary, both MAL-PDT and IMIQ 5% are safe and well-tolerated treatments that effectively prevent the development of new AKs in patients with tumorigenesis. However, MAL-PDT treatment seems to be preferred by patients [49].
3.2.6. Photodynamic Therapy in 2016–2020
In 2016, a study was conducted to assess the safety of photodynamic therapy (PDT) using 3-(1'-hexyloxyethyl) pyropheophorbide-a (HPPH) in the treatment of early stages of laryngeal diseases. This study, conducted in a single center, was open-label and non-comparative. It included patients at high risk for dysplasia, carcinoma in situ, and T1 squamous cell carcinoma (SCC) of the larynx. The primary aim of the study was to determine the safety of therapy and the maximum tolerated dose (MTD), and the secondary aim was to assess the response to treatment. 29 patients participated in the study and 30 lesions were treated. The most common adverse event was transient hoarseness. The most serious adverse event was severe edema requiring tracheostomy, which occurred in two patients within hours of therapy. The maximum tolerated dose was 100 J/cm(2). Patients with T1 squamous cell carcinoma showed a good overall response (82%) to HPPH-PDT therapy at the maximum tolerated dose. The conclusions of the study indicate that HPPH-PDT therapy can be safely used in the treatment of early laryngeal cancer, which suggests its potential effectiveness [50].
Also in 2016, a study was conducted to investigate the effectiveness and safety of photodynamic therapy (PDT) using hemoporfin and a 532 nm laser in the treatment of port-wine stain. This study, carried out in eight hospitals in China, included patients aged 14 to 65 years affected by this mole. In the first phase of the study (day 1 to week 8), patients were randomly assigned to treatment or placebo. The treatment group received 532 nm laser irradiation (96-120 J/cm2) with hemoporfin (5 mg/kg; PDT-hemoporfin, n = 330), while the placebo group received irradiation with placebo (PDT-placebo, n = 110) . In the second phase of the study (from weeks 8 to 16), all patients were offered treatment. The main goal of the study was to determine how many patients achieved at least some improvement at week 8. Additionally, we assessed how many patients achieved almost complete relief of symptoms or at least major improvement at week 8, and how many patients achieved early complete relief, at least major improvement, or at least some improvement at week 16. Investigator and patient satisfaction with treatment was also examined at weeks 8 and 16. The study results showed that the PDT-hemoporfin treatment group achieved significantly better results compared to the placebo group. Nearly 90% of patients in the treatment group achieved at least some improvement at week 8. All secondary efficacy endpoints were also higher in the treatment group. Treatment reactions occurred in almost all patients in the treatment group, and hyperpigmentation occurred in approximately 23 of 100 treated patients. The results of the study allowed us to suggest that PDT using hemoporfin is an effective and safe method of treating port-wine stain in patients of different ages [51].
In 2017, a study was conducted focusing on the chronic and incurable disease lichen sclerosus of the vulva, which causes various unpleasant symptoms and serious consequences. The aim of this study was to investigate the effectiveness of photodynamic therapy (PDT) in the treatment of this disease. The study included 102 patients aged 19 to 85 who suffered from vulvar lichen sclerosus. All patients underwent photodynamic therapy (PDT), which used 5% 5-aminolevulinic acid in the form of a gel. The affected areas were irradiated with a PhotoDyn 501 halogen lamp (590-760nm) during a ten-minute treatment. Treatments were repeated weekly for 10 weeks. The results of the study were promising. Photodynamic therapy showed good therapeutic effects, with an 87.25% improvement rate in patients suffering from lichen sclerosus. The greatest improvement was observed in the reduction of subepithelial petechiae and telangiectasia (78.95%), as well as in the reduction of erosion and cracks (70.97%). Partial resolution of lichenization with hyperkeratosis was observed in 51.61% of cases. The smallest improvement was observed in the reduction of atrophic changes (improvement in 37.36% of cases). These results allowed us to conclude that PDT has excellent effects in the treatment of lichen sclerosus and additionally gives very good cosmetic effects [52].
In 2018, a study was conducted on rosacea, a common chronic skin disease that presents with redness, erythema, pustules and telangiectasia. Due to the tendency of the disease to relapse, a multi-faceted approach to its control is necessary. This study aimed to investigate the effectiveness and safety of photodynamic therapy (PDT) using aminolevulinic acid (ALA) for the treatment of rosacea in Chinese patients with Fitzpatrick skin types III and IV. The study included 20 patients with rosacea, both erythematotelangiectatic and papulopustular types. 5% aminolevulinic acid was used in the form of an oil-in-water emulsion, which was applied to the lesions under occlusion with plastic foil for 2 hours. Then, the lesions were irradiated with red LED light with a power of 100 mW/cm2, 80-90 J/cm2, for 15 minutes in each session. The treatments were repeated every 10 days for 10 weeks. The study results were promising. All patients showed gradual improvement compared to baseline. All clinical inflammatory changes completely disappeared after 24 weeks. Subjective symptoms such as redness, itching, stinging, burning, etc. disappeared and did not recur during the follow-up period. The main side effects are pain, redness, swelling and post-inflammatory hyperpigmentation. All side effects were transient and tolerable in all patients. To sum up, the results of the study showed that photodynamic therapy with aminolevulinic acid is an effective and safe method of treating erythematotelangiectatic or papulopustular rosacea [53].
In 2019, a pioneering study was conducted to investigate the potential benefits of the concomitant use of photodynamic therapy (PDT) as a tumor ablation method in combination with minimally invasive stabilization procedures for pathological vertebral compression fractures (VCF), such as vertebroplasty (VP) and balloon kyphoplasty ( KP). This study aimed to investigate whether PDT could complement the improvement in mechanical stability provided by vertebral cement augmentation (VCA). The study included thirty patients with various primary tumors who were treated with PDT and VP or KP. The study used a single dose of 6 mg/m2 of the clinical photosensitizing agent Visudyne with increasing doses of laser light. After a light-only control group (n = 6), subsequent drug and light treatment groups (n = 6 each) received 50, 100, 150, and 200 J/cm. Cement augmentation of the vertebrae was performed within 15 minutes after PDT. Patients were clinically evaluated at 1 and 6 weeks. The main evaluation criterion was safety from a neurological perspective. The study results were promising. All patients underwent a vertebral PDT procedure, which was technically feasible and provided to all patients in the study. Neither dose group showed a significant increase in pain as defined by the generic SF-36 as well as the disease-specific EORTC-QLQ-BM22 and EORTC-QLQ-C15-PAL questionnaires. The 50 and 100 J/cm groups showed the most significant pain reduction (P < 0.05). Twelve (40%) patients experienced complications during the study, including 3 patients with further progression of vertebral fracture after 6 weeks despite VCA. No complications were directly attributable to PDT. In summary, the study results suggested that vertebral PDT as an adjunct to VCA is safe from a pharmaceutical and neurological point of view. The results of this study motivate a larger-scale study to evaluate the potential effectiveness of PDT in the treatment of vertebral metastases [54].
In 2019, a study was conducted to assess clinical and microbiological periodontal parameters after the use of additional antibacterial photodynamic therapy (APDT) in HIV-infected and uninfected patients suffering from necrotizing ulcerative periodontitis (NUP).
The study included HIV-infected patients (Group-I) and healthy patients (Group-II) suffering from NUP. Patients were randomly divided into two groups that underwent APDT and scaling and root planning (SRP), respectively. Clinical periodontal parameters such as full dental plaque index (FMPI), bleeding on probing (FMBOP), probing depth (PD) and clinical attachment level gain (CAL) were examined. The levels of bacteria, including Aggregatibacter actinomycetem-comitans (Aa), Porphyromonas gingivalis (Pg), and Tannerella forsythia (Tf), were assessed by PCR. All assessments were performed at baseline, 3 months, and 6 months. The study results showed that all periodontal parameters, including FMPI, FMBOP, PD and CAL, significantly improved in both HIV-infected and uninfected patients. The reduction in mean PD was higher only after APDT treatment among patients in group II compared to patients in group I during follow-up (p < 0.05). The gain in mean CAL was higher only after APDT treatment among patients in groups I and II during follow-up (p < 0.05). All bacterial levels decreased from baseline to follow-up after both APDT and SRP treatment in both groups (p < 0.05). APDT showed significantly reduced Aa and Tf levels at 3 months and only Aa at 6 months among HIV positive patients, while Pg and Tf levels were significantly reduced at 3 months and only Aa at 6 months in HIV negative patients (p < 0 .05).In summary, the use of antibacterial photodynamic therapy as an adjunct to scaling and root planning has been effective in improving clinical periodontal parameters and bacterial levels in HIV-infected patients suffering from NUP. However, the improvement was not greater compared to HIV-uninfected patients [55].
In 2020, a prospective, randomized, self-controlled study was conducted to evaluate the effectiveness, pain, and safety of modified photodynamic therapy (M-PDT) in the treatment of genital warts. Papillae were randomly assigned to the M-PDT or C-PDT side. 5-aminolevulinic acid (ALA; 20%) was incubated for 3 hours before exposure of patients to red LED light (100 J/cm2) on the C-PDT side and for 30 minutes before exposure to red LED light (300 J/cm2) on the side M-PDT. Therapy was administered weekly for three weeks. Cure rates were determined at 1 week and recurrence rates at 4, 8, and 12 weeks after treatment. Pain and other side effects were also studied. A total of 24 patients with genital warts participated in the study. Twenty patients completed the study. The cure rates were 98.17% on the M-PDT side and 98.20% on the C-PDT side (P > 0.05). Recurrence rates were 11.11% and 10.53% (P > 0.05). However, M-PDT was almost painless (mean score 0.3 ± 0.47, range 0∼1), which was much less than that of the C-PDT side (mean score 3.6 ± 0.94, range 0∼1) (P < 0.05). Local redness, mild swelling and erosion were observed on both sides. The results of the study established that modified photodynamic therapy is virtually painless and has similar effectiveness to conventional photodynamic therapy. This is a significant breakthrough in pain management in photodynamic therapy [56].
3.2.7. Photodynamic Therapy in 2021–2023
In 2021, another human wart treatment study was conducted and showed significant results. This study, a prospective, randomized, controlled experiment, included eighty patients with warts who were divided into three groups. Group A, consisting of 30 patients, underwent photodynamic therapy (PDT) sessions using endocrine methylene blue (MB) and intense pulsed light (IPL). Group B, also consisting of 30 patients, received only IPL sessions. Group C served as the control group. Response to treatment was assessed based on clinical and dermatoscopic scores, cure rate, and ImageJ analysis, which included the wart surface and hemorrhagic structures or vessels. In group A, subjected to MB/IPL/PDT therapy, clinical and dermatoscopic removal of warts was achieved in 43.3% of patients, which translated into a cure rate of 40.9%. In group B, which received only IPL sessions, these rates were 20% and 23.4%, respectively. ImageJ analysis showed a greater reduction in the area of warts and hemorrhagic or vascular structures in group A. In conclusion, MB/IPL/PDT therapy proved to be an effective treatment option for warts, achieving a success rate of approximately 40% based on clinical and dermatoscopic evaluation. This efficiency was even higher using ImageJ analysis, which took into account both the wart surface and the surface of vessels and hemorrhagic dots. The latter were more affected by treatment [57].
In 2021, a randomized, controlled clinical trial was conducted to compare the effectiveness of photodynamic therapy (PDT) and the use of trichloroacetic acid (TAA) in the treatment of HPV warts around the anus and vulva. This study was conducted at the Women's Health Outpatient Clinic in the city of São Carlos, São Paulo State, Brazil. The study included 36 patients, 31 of whom met the study requirements. Patients were randomly assigned to one of two treatment regimens: photodynamic therapy (PDT) or trichloroacetic acid (TAA). The PDT protocol used the prodrug methylaminolevulinate, which was incubated for 3 hours and then irradiated at a wavelength of 630 nm (100 J/cm²). For TAA, the warts were gently soaked in acid using a cotton swab. Both treatments were repeated weekly until the lesions disappeared completely or until 10 sessions were performed. The main criterion for assessing the effectiveness of treatment was clinical analysis, and patients were followed up for 12 to 30 months after the end of treatment. Among 16 patients treated with PDT and 15 patients treated with TAA, the overall effectiveness was 63% and 60%, respectively. The recurrence rate was 0% for PDT and 33% for TAA. In summary, photodynamic therapy (PDT) not only successfully treated warts by physically destroying lesions and clinical lesions, but also appeared to modulate the immune system and/or reduce local viral load, suggesting a lower recurrence rate compared to the trichloroacetic acid (TAA)-treated group. [58].
A 2022 study aimed to evaluate the effect of antimicrobial photodynamic therapy (aPDT) as an adjunct to topical antiviral therapy in children with herpetic gingivostomatitis. The study involved 45 people aged 12 to 18 years who suffered from herpetic gingivostomatitis (HG). The subjects were divided into three groups depending on the type of treatment used. Group A consisted of 14 people (mean age 17.0 years) who received topical antiviral therapy (TAT). Group B included 15 people (mean age 17.7 years) who underwent antimicrobial photodynamic therapy (aPDT). Group C included 16 people (mean age 18.0 years) who received local antiviral therapy with the addition of aPDT. Pain was assessed using a visual analogue scale (VAS) and the McGill Pain Questionnaire (MPQ), and HSV-1 quantification was performed. Proinflammatory cytokine levels, including interleukin 6 (IL-6) and tumor necrosis factor-alpha (TNF-α), were calculated using ELISA. Analysis of data obtained after clinical assessment showed that all three groups experienced decreases in pain scores, HSV-1 loads, and pro-inflammatory cytokine levels. However, Group C (TAT + aPDT) showed a statistically significant improvement in the observed parameters compared to Group A (TAT) and Group B (aPDT) [59].
A study conducted in 2022 aimed to use photodynamic therapy (PDT) using 5-aminolevulinic acid (5-ALA) in the treatment of nicotine stomatitis in smokers. The study involved 24 patients with this disease, who were divided into two groups: test (n=12) and control (n=12). Patients in the test group were treated with PDT using 5-ALA, while patients in the control group were advised to stop smoking for the duration of the study. PDT treatment was repeated on days 3, 7, and 14, and participants were then monitored at follow-up visits 4, 6, and 8 weeks after completion of treatment. Data analysis was performed using SPSS version 22.0. According to the results, patients in the test group showed statistically significant improvement at all three time points (p < 0.0001). A similar trend was also observed in the control group (p < 0.001), but the difference between both groups was significant. The results of this clinical study suggest that the use of photodynamic therapy with 5-aminolevulinic acid can effectively reduce the clinical symptoms of nicotine stomatitis without negative side effects. Therefore, PDT with 5-ALA seems to be a promising therapeutic option, especially when combined with smoking cessation [60].
A study conducted in 2023 aimed to compare two methods of nasal decolonization in patients undergoing chronic hemodialysis who were carriers of Staphylococcus aureus. Infections in which S. aureus is the etiological agent constitute a significant health problem among this group of patients, and nasal colonization with this pathogen increases the risk of infection. The study used two decolonization approaches: photodynamic therapy and mupirocin treatment. Photodynamic therapy, which does not induce antibiotic resistance, consisted of a single application of light with a wavelength of 660 nm (400 mW/cm2, 300 seconds) using 0.01% methylene blue as a photosensitizer. In turn, mupirocin treatment included the use of this antibiotic topically twice a day for 5 days. The study results showed that both methods were effective in eliminating S. aureus from the nose immediately after treatment. However, within 3 months after completion of photodynamic therapy, 67% of patients who had negative cultures immediately after completion of treatment were recolonized. No adverse events were reported in the photodynamic therapy group. This study is an important step in the search for alternative methods of nasal decolonization in patients undergoing chronic hemodialysis. The study also indicated that larger studies are needed in the future to determine whether photodynamic therapy is equivalent to the standard of care with mupirocin [61].
A scientific study conducted in 2023 focused on analyzing the therapeutic potential of photodynamic therapy (PDT) with indocyanine green (ICG-PDT) in the treatment of keloids, which are a common dermatological problem. As part of the study, patients with keloids were divided into four groups: control, photothermal therapy, photodynamic therapy and combined therapy. The aim of the in vitro study was to understand the mechanism of action of PDT in the context of keloid treatment, which could contribute to the optimization of its clinical application. The study results showed that ICG-PDT effectively inhibited the cellular activity and migration of keloid fibroblasts, and this effect was most visible when the photodynamic mechanism was operating. Additionally, in this experimental group, induction of autophagy and apoptosis and inhibition of collagen synthesis were observed. Moreover, these therapeutic effects could be achieved at relatively low drug concentrations. Based on these results, researchers successfully applied the optimized treatment method to a clinical case with favorable results.
In summary, this study provided valuable information on the mechanism of action of ICG-PDT and allowed for the optimization of the treatment regimen in vivo [62].
A study was also published in 2023, which was a significant contribution to current research on SARS-CoV-2. This study focused on evaluating the effectiveness of intranasal photodynamic therapy (PDT) in the context of SARS-CoV-2 infection. The main aim of the study was to investigate the effect of PDT on shortening the infectious period in SARS-CoV-2 carriers with mild symptoms. Additionally, this study focused on the analysis of SARS-CoV-2-specific effects of immune system stimulation and the safety of therapy.mThe study was conducted as a randomized, placebo-controlled clinical trial. Patients with a positive SARS-CoV-2 PCR within the previous 48 hours were recruited and randomly assigned to receive PDT or placebo. Patients with pneumonia were excluded from the study. The primary outcome of the study was a reduction in in vitro infectivity of nasopharyngeal samples on days 3 and 7 after initiation of therapy. Additional results included safety assessment and quantification of T.m humoral and cellular immune responses. Study results indicate that intranasal PDT is safe in mildly symptomatic COVID-19 patients, reduces SARS-CoV-2 infectivity, and slows the decline in specific immune responses to SARS-CoV-2. CoV-2. These results constitute an important contribution to ongoing research on SARS-CoV-2 and may have a significant impact on future treatment strategies [63].
3.3. Natural Photosensitizers
A photosensitizer, also known as a photosensitizer or photosensitizer, is a chemical or compound that increases the sensitivity of the body or tissues to light, especially ultraviolet (UV) radiation or visible light. The effects of a photosensitizer may include hypersensitivity to light, allergic reactions or damage to skin cells under the influence of light radiation. For this reason, photosensitizers have been used in therapy photodynamic.
Photodynamic therapy is based on triggering a reaction photo biochemical reaction in the presence of oxygen between the photosensitizer and light of a specific wavelength [64]. The photosensitizer is introduced into the body as a substance that appears to have no effect. However, it accumulates in abnormal tissue in a more or less selective manner. The main goal is to lead or induce pathological cells into a programmed death pathway, called apoptosis necrosis process by means of a photooxidative reaction under the influence of light [65]. After a certain period of time, the photosensitizer reaches its highest concentration in the area cancer compared to the surrounding healthy tissue. Then the area containing tumor tissue with a photosensitizer is irradiated with light with a wavelength that corresponds to the maximum of the photosensitizer's absorption spectrum in the spectral range above 500 nm. The choice of light source must be like this adjusted so that its emission band coincides with the absorption band of the dye, which is necessary to induce a photochemical reaction. As a result of photon absorption, the photosensitizer molecule changes from the basic energy state to the singlet excited state. In the context of photodynamic therapy (PDT), there are two important routes to deactivate a molecule from this state to the ground state: A photosensitizer molecule in an excited singlet state can return to the ground state, releasing excess energy in a radiative process, which is called fluorescence. Detecting the fluorescence of a drug accumulated in tumor tissue allows for precise diagnostics, enabling the determination of shape, size and location of the cancer lesion.
As a result of the transition to the triplet state, the photosensitizer molecule excited to a singlet state is converted to a triplet state. The lifetime of a photosensitizer molecule in the triplet state is long (hundreds of microseconds) and interacts with oxygen. In the ground state, the oxygen molecule is in the triplet state and effectively deactivates the triplet state of the drug, generating a strong oxidant – oxygen singlet. In this way, the process of deactivation of the photosensitizer molecule can lead to the generation of singlet oxide, which is a powerful oxidant, particularly effective in the destruction of cancer cells in PDT [66].
For a photosensitizer to be effectively used in the diagnosis or treatment of cancer, it must meet several key conditions:
- Selective accumulation in tumor tissue: The photosensitizer should be able to selectively accumulate in the area of tumor tissue, minimizing the effect on healthy tissues.
- No phototoxic effects in healthy tissues: The photosensitizer should not cause undesirable phototoxic effects in healthy tissues, which means that it cannot damage healthy cells when exposed to light.
- Appropriate absorption bands: The absorption bands of a photosensitizer should not coincide with the absorption bands of the body's natural pigments, such as melanin or hemoglobin, or with the absorption bands of water in the area close to infrared.
- Efficient generation of singlet oxygen and oxidative reactions: The photosensitizer should be able to efficiently generate singlet oxygen and other oxidative reactions that are crucial in the destruction of cancer cells.
- Minimal side effects: The photosensitizer should not cause significant side effects that may be harmful to the patient.
- Low toxicity and easy elimination: The photosensitizer should be low toxic and easily removed from the body after completion of therapy to minimize side effects and burden on the patient's body.
The requirements that photosensitizers must meet are high and therefore no dye has been discovered so far that would meet the above criteria [67]. Most photosensitizers used in anticancer photodynamic therapy are porphyrin compounds (such as protoporphyrin IX), which consist of four pyrrole molecules connected by methine bridges. In the 1970s, hematoporphyrin (Hp) and mixtures of hematoporphyrin derivatives (HpD) were the most commonly used photosensitizers, known as the first generation of photosensitizers. In years
In the 1980s, the second generation of photosensitizers from various chemical families was created, such as: TPPSn - sulfonated tetraphenylporphyrin [68], zinc and aluminum phthalocyanines [69], m-THPC - meso-tetra(hydroxyphenyl) chlorins [70], chlorin e6 [71], m -THPP — meso-tetra(3-hydroxyphenyl) porphyrin [72], merocyanine 540 [73], hypericin [74] or methylene blue derivatives [75]. Chlorites, as one of the chemical groups within porphyrin compounds, are formed by reducing the double bond in one of the four pyrrole rings. This modification causes chlorites to absorb light much more intensively in the long-term spectral range, which is of key importance in anticancer photodynamic therapy. Chlorins can be stimulated with longer wavelength light than porphyrins, which allows deeper penetration of light into tissues compared to porphyrin photosensitizers. For example, light with a wavelength of 630 nm can penetrate tissue to a depth of about 0.5 cm, while light with a wavelength of 700 nm can penetrate to a depth of about 1.5 cm [76]. Chlorites reach their maximum concentration in the tumor area after a few hours, such as chlorin e6, which reaches its maximum after about 3 hours and is then relatively quickly eliminated from the body within 24-48 hours [77].
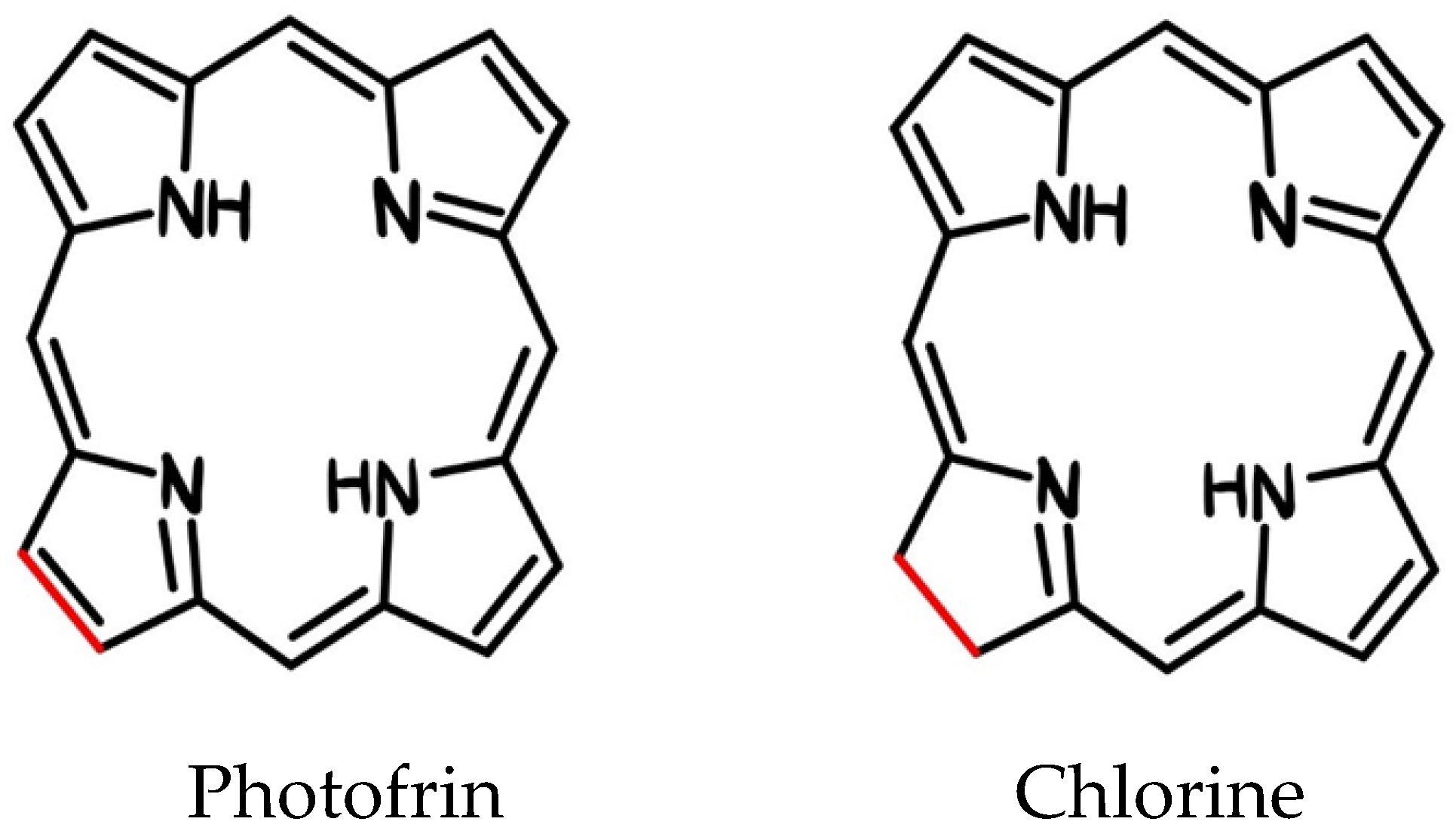
Figure 3.
Structural formula of porphyrin and chlorin.
Table 2.
Examples of in vivo and in vitro experiments on porphyrins and porphyrin derivatives as photosensitizing agents in photodynamic therapy.
Table 2.
Examples of in vivo and in vitro experiments on porphyrins and porphyrin derivatives as photosensitizing agents in photodynamic therapy.
| Photosensitizer | Nanoparticle | Results | In vivo/ In vitro |
|---|---|---|---|
| Photofrin | F3 – Polymer targeted particles | • High rate of uptake of nanoparticles by cells • Significant improvement in survival rate (MDA-MB-435 cell line—breast cancer, 9L rat gliomas) |
In vitro [78] |
| Nanoporous zinc oxide | • Increased ROS generation • Increased cytotoxic effect (Cell line A549 - lung cancer) |
In vitro [79] In vivo |
|
| Liposomy | • Higher phototoxic effect of liposomal photofrin compared to the free drug (Athymic nude rats, Cr:NIH-rna strain with U97 cells) |
In vivo [80] | |
| Photoporphyrin IX | Gold particles | • Increased cytotoxic effect of conjugates (HeLa cell line - cervical cancer) • Increased apoptosis (HeLa cell line - cervical cancer) • Increased single oxygen generation (male Newborn Medical Research Institute [NMRI] mice) |
In vitro [81] In vitro [82] In vivo [83] |
| Polyethyleneimine nanoparticles | • Ability to generate single oxygen upon exposure to light with a wavelength of 635 nm | In vitro [84] | |
| Carbon particles | • Increased single oxygen generation • Additional bioluminescence effect • Increased phototoxic effect (MMC-7721 cell line - hepatocellular carcinoma) |
In vitro [85] | |
| Nanoparticles with a silver core and a silica coating | • Increased single oxygen generation (U251MG cell line - astrocyma glioblastoma, HepG2 cell line - hepatocellular carcinoma) |
In vitro [86] | |
| Polymerosomes | • Increased cytotoxic effect • Selective cytotoxic effect on melanoma cells (Cell line A375 - malignant melanoma) |
In vitro [87] | |
| Micelle poli(etylenoglikolu) - polikaprolaktonu (PEG-PCL) | • Synergistic activity with erlotinib (MDA-MB-231 cell line - breast cancer) |
In vitro [88] |
Table 3.
In vivo and in vitro experiments on chlorites and chlorite derivatives as photosensitizing agents in photodynamic therapy.
Table 3.
In vivo and in vitro experiments on chlorites and chlorite derivatives as photosensitizing agents in photodynamic therapy.
| Photosensitizer | Nanoparticle | Results | In vivo/ In vitro |
|---|---|---|---|
| Chlorine e6 | Lipidots | • Reduced dark toxicity • Retained phototoxicity (CAL-33 cell line - squamous cell carcinoma of the tongue) |
In vitro [89] |
| Superparamagnetic iron oxide partition nanoclusters (SPION) | • High solubility in water • Single oxygen generation preserved • Significant delay in tumor growth (4T1 cell line - breast tumor mice, female nude mice carrying 4T1) |
In vitro [90] In vivo |
|
| Methoxy-poly(ethylene glycol)-poly(D,L-lactide) (mPEG-PLA-Ce6) | • Increased single oxygen generation • Increased cellular internalization (A549 cell line - lung cancer, monolayers and 3D spheres) |
In vitro [91] | |
| Verteporfirin | Poly(D,L-lactide-co-glycolide) | • Size dependent toxicity • Increased phototoxic effect for smaller nanopartitions • Efficiently controlled tumor growth by small nanopartitions loaded with verteporfin (EMT-6 cell line - mammary tumor mice, SKH1 female nude mice) |
In vitro [92] In vivo |
| 2-[1-heksyloksyetylowy]-2-devinyl pyrofeoforbid-a (HPPH) | Functionalized polyacrylamide (AFPAA) | • Efficient en-capsulation, post-loading or HPPH conjugation • Highest phototoxicity and single oxygen production for the post-loaded form • No dark toxicity observed • Tumor location in a murine colorectal cancer model (PC-3 cell line - prostate cancer, MDA-MB-435S cell line - melanoma, Mice carrying human glioblastoma U87MG) |
In vitro [93] In vivo |
An interesting case of a substance used in PDT is acid 5-aminolevulinic acid (ALA). It has been approved for therapeutic use by the US Food and Drug Administration (FDA) in 1999. It is used in the treatment of skin cancer and is applied topically, directly to the tumor area in the form of an ointment. After a few hours in the skin, as a result of natural processes, protoporphyrin is generated, which acts as a photosensitizer. Importantly, ALA is a precursor of hematoporphyrin synthesis in the body, and the resulting porphyrin is not toxic to the body in the absence of light.
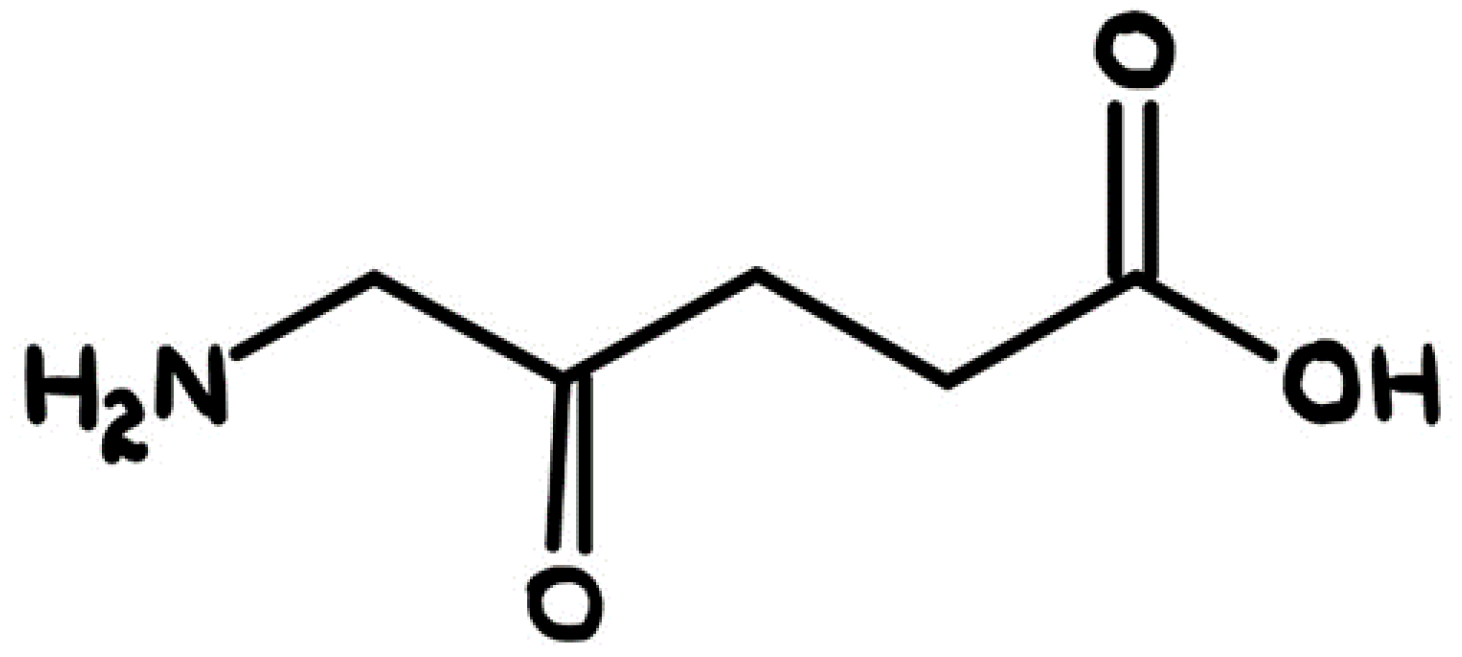
Figure 4.
Structural formula of 5-aminolevulinic acid.
As a result of numerous scientific studies, it has been proven that they are photosensitizers with amphiphilic characteristics show the most favorable properties. These substances have two important features in their structure: lipophilic domains and side domains chains that exhibit hydrophilic properties. The combination of these two different properties makes amphiphilic photosensitizers perfectly adapted to accumulate in cancer cells. Importantly, amphiphilic photosensitizers have the ability to double anchor in cancer cells. One part of the photosensitizer molecule interacts with the lipid structures of the cell, while its side groups are located in the aqueous part of the cell. Thanks to this, they can accumulate effectively in cancer cells, which is crucial in the context of photodynamic therapy.
Table 4.
Properties of some photosensitizing dyes approved for the treatment of PDT and used in PDT-related clinical trials.
Table 4.
Properties of some photosensitizing dyes approved for the treatment of PDT and used in PDT-related clinical trials.
| Compound | Nazwa | Absorption [nm] | Application |
|---|---|---|---|
| Porfimer sodium salt | Photofrin | 632 | Canada (1993) - bladder cancer USA (1995) - esophageal cancer USA (1998) - lung cancer USA (2003) - Barrett's esophagus Japan - cervical cancer Europe, Canada, Japan, USA, Great Britain - endobronchial cancer |
| 5-aminolevulinic acid (ALA) | Levulan | 632 | USA (1999) - actinic keratosis |
| Aminolewulinian metylu (MAL) | Metvixia | - | USA (2004) - actinic keratosis |
| Heksaminolewulinian (HAL) | Cysviev | - | USA (2010) - diagnosis of bladder cancer |
| A derivative of benzoporphyrin Monoacid ring A (BPD-MA) |
Visudine | 689 | USA (age-related macular degeneration 1999) - |
| Meta-tetra(hydroxyphenyl)chlorin (m-THPC) | Foscan | 652 | Europe - neck and head cancer |
| ethyl tin ethiopurpurine | Purlytin | 664 |
Clinical trials - breast adenocarcinoma, basal cell carcinoma, Kaposi's sarcoma, age-related macular degeneration |
| N-aspartylochloryna e6 (NPe6) | Laserphyrin, Litx | 664 | Japan (2003) - lung cancer |
| 2-(1-heksyloksyetylo)-2-dewinyl pirofoforbid (HPPH) | Photochlor | 665 | Clinical trials - esophageal cancer, basal cell carcinoma, lung cancer, Barrett's esophagus |
| Bakteriopheoforbide palladu (WST09) | Tookad | 763 | Clinical trials - prostate cancer |
| WST11 | Stakel | - | Clinical trials - prostate cancer |
| Motexafina lutet (Lu-Tex) | Lutrin, Optrin, Antrin | 732 | Clinical trials - prostate cancer, age-related macular degeneration, breast cancer, cervical cancer, arterial disease |
| Tetrasulfonic aluminum phthalocate (APkS4) | Photosens | 676 | Russia (2001) - stomach, skin, lips, oral cavity, tongue, breast cancer |
| Silicon phthalocyanine (Pc4) | - | 675 | Clinical tests - practical keratosis, Bowen's disease, skin cancer, mycosis |
4. Discussion
4.1. Advances in Imaging Techniques and Diagnostics Supporting PDT
The effectiveness of photodynamic therapy requires accurate diagnostics and monitoring the treatment process, therefore progress in imaging techniques and diagnostics plays a key role in supporting PDT.
- Imaging using fluorescence techniques:
Advanced fluorescence imaging techniques are now available to visualize and monitor the accumulation of photosensitizersbin tissues. An example is fluorescence computed tomography (FLT), which allows three-dimensional reconstruction and localization of photosensitizers in patients' bodies [94].
- Optical imaging:
Optical imaging techniques such as frame spectroscopy enable the identification and assessment of tissue biomarkers. An example is application autofluorescence to detect changes in cancer tissues, which allows for early diagnosis and monitoring of the progress of therapy [95].
- Advanced microscopy imaging:
The use of multi-light and multi-spectral microscopy allows for the analysis of tissue morphology on a microscale and the observation of cell reactions to photodynamic therapy. This helps doctors tailor therapy to the patient's individual needs [96].
- Molecular diagnostics:
The use of molecular biology techniques, such as testing the level of gene expression or protein analysis, allows for the personalization of photodynamic therapy. The appropriate photosensitizer and the optimal time for therapy can be determined [97].
- Imaging using hybrid technologies:
A combination of different imaging techniques, such as computed tomography and magnetic resonance imaging with optical techniques, allows precise localization of areas to be treated and monitoring changes in real time [98].
4.2. The Most Important Centers Specializing in the Treatment of Skin Problems with Photodynamic Therapy in the World
Table 5.
The most important centers specializing in skin PDT in the world.
| Country | Research Centre |
|---|---|
| Austria | Wiener Privatklinik Rudolfinerhaus Privatklinik Döbling Private Clinic Akh Vienna General Hospital Graz Ragnitz Private Clinic Private Clinic Konfraternetat Leech Pivate Clinic |
| China | Fuda Cancer Hospital |
| Czech Republik | Motol University Hospital University Hospital Brno |
| France | American Hospital of Paris Oncological Institut Gustave Roussy |
| Germany | Dermatologikum Berlin Solingen City Hospital University Hospital Rechts der Isar Nuremberg Hospital Helios Medical Group University Hospital of Köln Charité University Hospital Frankfurt University Hospital Essen University Hospital Meoclinic |
| India | Gleneagles Global Hospitals BLK Super Speciality Hospital Apollo Hospitals Fortis Hospital Artemis Hospitals Manipal Hospitals Group Medanta Hospital Wockhardt Hospitals |
| Izrael | Sourasky Medical Center (Ichilov) Assuta Medical Center Sheba Medical Center Rambam Hospital Herzliya Medical Center Hadassah Medical Center Yitzhak Rabin Medical Center Schneider Children’s Medical Center Shaare Zedek Medical Center Ramat Aviv Medical Center Assaf Harofeh Medical Center Meir Medical Center |
| Italy | Salvator Mundi International Hospital |
| Korea | JK Plastic Surgery Clinic Asan Medical Center Severance Hospital Gachon University Gil Medical Center Cheil General Hospital & Women’s Healthcare Center Kyung Hee University Hospital (KUIMS) Seoul National University Hospital Soon Chun Hyang University Hospital Inha University Hospital Chung-Ang University Hospital |
| Litwa | Abromiskes Rehabilitation Center Medical Diagnostic and Treatment Centre |
| Poland | Krakow University Hospital |
| Singapur | Raffles hospital |
| Spain | Hospital Quirónsalud Barcelona Clínica Universidad de Navarra |
| Tajland | Bumrungrad International Hospital |
| Turkey | Medicana Hospitals Group Medistate Hospital Medipol Mega University Hospital Memorial Hospital Medical Park Hospitals Group Koc University Hospital Acibadem Maslak Hospital Liv Hospital Anadolu Medical Center Hisar Intercontinental Hospital Gaziosmanpasa Private Clinic Memorial Şişli Hospital Medical Park Gebze Clinic Memorial Bahçelievler Hospital Memorial Hospital Ataşehir Medical Park Göztepe Hospital Acibadem Taksim Clinic Medical Park Fatih Hospital |
4.3. Side Effects and Complications of PDT
Despite its advantages, photodynamic therapy, like many other medical procedures, may be associated with some side effects and complications. The most common include skin burns in the treated area, especially in the case of excessive exposure or photosensitivity. Patients undergoing PDT may also experience pain and discomfort during the procedure itself procedure and after its completion, they may also be more sensitive to light sun for some time after the procedure, which may lead to burns solar [99]. In addition, the skin may become red and swollen at the treatment site, and may peel and itch. In some cases, PDT may leave permanent scars or skin discoloration. [100]. There is a risk infection at the site of treatment, especially if the wounds are not properly protected and nurtured [101]. Please note that the side effects of PDT may vary depending on the type of disease, area of treatment and individual patient's reaction. There is always a risk of more serious complications, so it is important to carry out therapy under the supervision of an experienced specialist.
4.4. The Future of PDT
There is now a clear and growing interest and international research effort focused on developing new ones photosensitizers, investigating the mechanisms of PDT at the molecular level, increasing its effectiveness through combined therapies, and assessing potential clinical indications [102]. Although there are now regulatory approvals for the clinical use of PDT photosensitizers in many countries around the world and light applicators, the overall number of approved clinical indications is still limited. It is expected that the pharmaceutical industry and research institutes will continue to conduct numerous clinical trials to evaluate the applications of PDT, both as a complement to and as a replacement for traditional oncological treatments and non-oncological. Optical methods and nanotechnology will continue to play a role an important role in the characterization of target tissues, determining the PDT dose and assessing treatment results. Combination therapies, personalized treatment planning and do-simetry will certainly continue to be an important element of photodynamic therapy.
5. Conclusions
New photosensitizers are needed to achieve better therapeutic effects with lower doses and fewer side effects. Despite these challenges, the potential of photodynamic therapy is enormous. We believe that continuous improvement of this method can bring us closer to the world we want to create - a world without pain and suffering. Let this work be a reminder of the extraordinary power of light and how far we have come in using it to treat the most difficult diseases. We hope that the future will bring even more advances in this field, opening new opportunities for patients around the world.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- 1. Dolmans DEJGJ, Fukumura D, Jain RK. Photodynamic therapy for cancer. Nat Rev Cancer. 2003;3:380-387. [CrossRef]
- 2. Agostinis P, Berg K, Cengel KA, Foster TH, Girotti AW, Gollnick SO, Hahn SM, Hamblin MR, Juzeniene A, Kessel D, Korbelik M, Moan J, Mroz P, Nowis D, Piette J, Wilson BC, Golab J. Photodynamic therapy of cancer: an update. CA Cancer J Clin. 2011;61(4):250-281. [CrossRef]
- 3. Podbielska H, Sieroń A, Stręk W, eds. Diagnostyka i terapia fotodynamiczna. Wrocław: Wydawnictwo Medyczne Urban & Partner; 2004.
- 4. Osmałek T, Gośliński T. Rozwój badań dotyczących fotodynamicznej terapii onkologicznej. Farm Pol. 2009;65(8):549–552.
- 5. Herschel W. Experiments on the Refrangibility of the Invisible Rays of the Sun. Philos Trans R Soc Lond. 1800;90:284-292.
- 6. Cauvin JF. Des bienfaits de l’insolation. Rozprawa Ph.D. Thesis, University of Paris, France. 1815.
- 7. Finsen NR. Phototherapy. London: Edward Arnold; 1901.
- 8. Gøtzsche PC. Niels Finsen's treatment for lupus vulgaris. J R Soc Med. 2011;104(1):41–42. [CrossRef]
- 9. Raab O. Uber die Wirkung fluoreszierender Stoffe auf Infusorien. Z Biol. 1900;39:524–546.
- 10. Allison RR, Downie GH, Cuenca R, Hu XH, Jh Childs C, Sibata CH. Photosensitizers in clinical PDT. Photodiagnosis Photodyn Ther. 2004;1(1):27–42. [CrossRef]
- 11. Acroyd R, Kelty C, Brown N, Reed M. The history of photodetection and photodynamic therapy. Photochem Photobiol. 2001;74(5):656–669. [CrossRef]
- 12. MacCormack MA. Photodynamic Therapy. Adv Dermatol. 2006;22:219–258. [CrossRef]
- 13. Dolmans DEJGJ, Fukumura D, Jain RK. Photodynamic therapy for cancer. Nat Rev Cancer. 2003;3(5):380-387. [CrossRef]
- 14. Dougherty TJ, Kaufman JE, Goldfarb A, Weishaupt KR, Boyle D, Mittleman A. Photoradiation therapy for the treatment of malignant tumors. Cancer Res. 1978;38(8):2628-2635.
- 15. Ge R, Ahn JC, Shin JI, Bahk CW, He P, Chung PS. An in vitro and in vivo study of combination therapy with Photogem®-mediated photodynamic therapy and cisplatin on mouse cancer cells (CT-26). Photomed Laser Surg. 2010;29(3):155-160. [CrossRef]
- 16. Allison RR, Moghissi K. Photodynamic therapy (PDT): PDT mechanisms. Clin Endosc. 2013;46:24. [CrossRef]
- 17. Robertson CA, Evans DH, Abrahamse H. Photodynamic therapy (PDT): A short review on cellular mechanisms and cancer research applications for PDT. J Photochem Photobiol B Biol. 2009;96:1-8. [CrossRef]
- 18. Castano AP, Demidova TN, Hamblin MR. Mechanisms in photodynamic therapy: part two—cellular signaling, cell metabolism and modes of cell death. Photodiagn Photodyn Ther. 2005;2:1-23. [CrossRef]
- 19. A. Nowak-Stepniowska, P. Pergoł, A. Padzik-Graczyk [Photodynamic method of cancer diagnosis and therapy--mechanisms and applications] Postepy Biochem., 59 (2013), pp. 53-63.
- 20. Z. Luksiene Photodynamic therapy: mechanism of action and ways to improve the efficiency of treatment Med. (Kaunas), 39 (2003), pp. 1137-1150.
- 21. A. Juzeniene, J. Moan The history of PDT in Norway Photodiagn. Photodyn. Ther., 4 (2007), pp. 3-11. [CrossRef]
- 22. Fonseca SM, Pina J, Arnaut LG, Seixas de Melo J, Burrows HD, Chattopadhyay N, Alcácer L, Charas A, Morgado J, Monkman AP, Asawapirom U, Scherf U, Edge R, Navaratnam S. Triplet-state and singlet oxygen formation in fluorene-based alternating copolymers. J Phys Chem B. 2006;110:8278-8283. [CrossRef]
- 23. D. Kessel, N.L. Oleinick Photodynamic therapy and cell death pathways Methods Mol. Biol. (2010), pp. 35-46. [CrossRef]
- 24. E. Buytaert, M. Dewaele, P. Agostinis Molecular effectors of multiple cell death pathways initiated by photodynamic therapy Biochim. Biophys. Acta Rev. Cancer., 1776 (2007), pp. 86-107. [CrossRef]
- 25. N. Mehraban, H.S. Freeman Developments in PDT sensitizers for increased selectivity and singlet oxygen production Mater. (Basel Switz.), 8 (2015), pp. 4421-4456. [CrossRef]
- 26. Dugan M, Crawford E, Nseyo U. Photodynamic therapy (PDT) after transurethal resection (tur) for superficial papillary bladder carcinoma (SBC): a randomized trial. Proc ASCO. 1991;10:173.
- 27. Nseyo U, Dehaven J, Dougherty T. Photodynamic therapy (PDT) in the management of patients with resistant superficial bladder cancer: a long term experience. J Clin Laser Med Surg. 1998;16:61–68. [CrossRef]
- 28. Lightdale CJ, Heier SK, Marcon NE, McCoughan JS, Jr, Gerdes H, Overholt BF, et al. Photodynamic therapy with porfimer sodium versus thermal ablation therapy with Nd:YAG laser for palliation of esophageal cancer: a multicenter randomized trial. Gastrointest Endosc. 1995;42:507–512. [CrossRef]
- 29. Biel M. Photodynamic therapy and the treating of head and neck cancers. J Clin Laser Radiat Surg. 1996;14:239–244. [CrossRef]
- 30. Overholt BF, Panjehpour M. Photodynamic therapy for Barrett’s esophagus. Gastrointest Endosc Clin N Am. 1997;7:207–220. [CrossRef]
- 31. Van den Bergh, H. (2001). Photodynamic therapy of age-related macular degeneration: History and principles. Seminars in Ophthalmology, 16(4), 181–200. [CrossRef]
- 32. Sterry W, Stockfleth E. Malignant epithelial tumors. In: Braun-Falco’s Dermatology. 3rd ed. Berlin, Heidelberg: Springer-Verlag; 2009. pp. 1357–1376.
- 33. Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, Wolff K. Epidermal and appendageal tumors. In: Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York: McGrawHill; 2012. pp. 1007–1094.
- 34. Morton CA, Szeimies RM, Sidoroff A, Braathen LR. European guidelines for topical photodynamic therapy part 1: Treatment delivery and current indications - actinic keratoses, Bowen’s disease, basal cell carcinoma. J Eur Acad Dermatol Venereol. 2013;27:536–544. [CrossRef]
- 35. Hamblin MR. Photodynamic Therapy for Cancer: What's Past is Prologue. Photochem Photobiol. 2020 May;96(3):506-516. Epub 2020 Jan 7. [CrossRef] [PubMed] [PubMed Central]
- 36. Jurklies B, Anastassiou G, Ortmans S, Schüler A, Schilling H, Schmidt-Erfurth U, Bornfeld N. Photodynamic therapy using verteporfin in circumscribed choroidal haemangioma. Br J Ophthalmol. 2003 Jan;87(1):84-9. [CrossRef] [PubMed] [PubMed Central]
- 37. Berr F. Photodynamic therapy for cholangiocarcinoma. Semin Liver Dis. 2004 May;24(2):177-87. [CrossRef] [PubMed]
- 38. Moore CM, Pendse D, Emberton M. Photodynamic therapy for prostate cancer--a review of current status and future promise. Nat Clin Pract Urol. 2009 Jan;6(1):18-30. [CrossRef] [PubMed]
- 39. Usuda J, Kato H, Okunaka T, Furukawa K, Tsutsui H, Yamada K, Suga Y, Honda H, Nagatsuka Y, Ohira T, Tsuboi M, Hirano T. Photodynamic therapy (PDT) for lung cancers. J Thorac Oncol. 2006 Jun;1(5):489-93. [PubMed]
- 40. Smijs TGM, Bouwstra JA, Schuitmaker HJ, Talebi M, Pavel S. A novel ex vivo skin model to study the susceptibility of the dermatomycete Trichophyton rubrum to photodynamic treatment in different growth phases. J Antimicrob Chemother. 2007;59:433-440. [CrossRef]
- 41. Berking C, Herzinger T, Flaig MJ, Brenner M, Borelli C, Degitz K. The efficacy of photodynamic therapy in actinic cheilitis of the lower lip: a prospective study of 15 patients. Dermatol Surg. 2007 Jul;33(7):825-30. [CrossRef] [PubMed]
- 42. Morton C, Horn M, Leman J, Tack B, Bedane C, Tjioe M, Ibbotson S, Khemis A, Wolf P. Comparison of topical methyl aminolevulinate photodynamic therapy with cryotherapy or Fluorouracil for treatment of squamous cell carcinoma in situ: Results of a multicenter randomized trial. Arch Dermatol. 2006 Jun;142(6):729-35. [CrossRef] [PubMed]
- 43. Zane C, Capezzera R, Sala R, Venturini M, Calzavara-Pinton P. Clinical and echographic analysis of photodynamic therapy using methylaminolevulinate as sensitizer in the treatment of photodamaged facial skin. Lasers Surg Med. 2007 Mar;39(3):203-9. [CrossRef] [PubMed]
- 44. Wildeman MA, Nyst HJ, Karakullukcu B, Tan BI. Photodynamic therapy in the therapy for recurrent/persistent nasopharyngeal cancer. Head Neck Oncol. 2009 Dec 17;1:40. [CrossRef] [PubMed] [PubMed Central]
- 45. Allison RR, Sheng C, Cuenca R, Bagnato VS, Austerlitz C, Sibata CH. Photodynamic therapy for anal cancer. Photodiagnosis Photodyn Ther. 2010 Jun;7(2):115-9. Epub 2010 May 7. [CrossRef] [PubMed]
- 46. Jerjes W, Upile T, Hamdoon Z, Mosse CA, Akram S, Hopper C. Photodynamic therapy outcome for oral dysplasia. Lasers Surg Med. 2011 Mar;43(3):192-9. [CrossRef] [PubMed]
- 47. Yu YE, Kuohung V, Gilchrest BA, Penrose C, Shim H. Photodynamic therapy for treatment of hand warts. Dermatol Surg. 2012 May;38(5):818-20. [CrossRef] [PubMed]
- 48. Bombeccari GP, Guzzi G, Gualini F, Gualini S, Santoro F, Spadari F. Photodynamic therapy to treat periimplantitis. Implant Dent. 2013 Dec;22(6):631-8. [CrossRef] [PubMed]
- 49. Sotiriou E, Apalla Z, Vrani F, Lallas A, Chovarda E, Ioannides D. Photodynamic therapy vs. imiquimod 5% cream as skin cancer preventive strategies in patients with field changes: a randomized intraindividual comparison study. J Eur Acad Dermatol Venereol. 2015 Feb;29(2):325-329. Epub 2014 Apr 23. [CrossRef] [PubMed]
- 50. Shafirstein G, Rigual NR, Arshad H, Cooper MT, Bellnier DA, Wilding G, Tan W, Merzianu M, Henderson BW. Photodynamic therapy with 3-(1'-hexyloxyethyl) pyropheophorbide-a for early-stage cancer of the larynx: Phase Ib study. Head Neck. 2016 Apr;38 Suppl 1(Suppl 1):E377-83. Epub 2015 Jun 29. [CrossRef] [PubMed] [PubMed Central]
- 51. Zhao Y, Tu P, Zhou G, Zhou Z, Lin X, Yang H, Lu Z, Gao T, Tu Y, Xie H, Zheng Q, Gu Y, Tao J, Zhu X. Hemoporfin Photodynamic Therapy for Port-Wine Stain: A Randomized Controlled Trial. PLoS One. 2016 May 26;11(5):e0156219. [CrossRef] [PubMed] [PubMed Central]
- 52. Maździarz A, Osuch B, Kowalska M, Nalewczyńska A, Śpiewankiewicz B. Photodynamic therapy in the treatment of vulvar lichen sclerosus. Photodiagnosis Photodyn Ther. 2017 Sep;19:135-139. Epub 2017 May 17. [CrossRef] [PubMed]
- 53. Fan L, Yin R, Lan T, Hamblin MR. Photodynamic therapy for rosacea in Chinese patients. Photodiagnosis Photodyn Ther. 2018 Dec;24:82-87. Epub 2018 Aug 15. [CrossRef] [PubMed] [PubMed Central]
- 54. Fisher C, Ali Z, Detsky J, Sahgal A, David E, Kunz M, Akens M, Chow E, Whyne C, Burch S, Wilson BC, Yee A. Photodynamic Therapy for the Treatment of Vertebral Metastases: A Phase I Clinical Trial. Clin Cancer Res. 2019 Oct 1;25(19):5766-5776. Epub 2019 Jul 2. [CrossRef] [PubMed]
- 55. Niazi FH, Koppolu P, Tanvir SB, Samran A, Alqerban A. Clinical efficacy of photodynamic therapy in the treatment of necrotizing ulcerative periodontitis among HIV seropositive patients: A randomized controlled clinical trial. Photodiagnosis Photodyn Ther. 2020 Mar;29:101608. Epub 2019 Nov 23. [CrossRef] [PubMed]
- 56. Zhang H, Shi L, Zhang Y, Wang P, Zhang G, Cao Y, Zhou Z, Wang X. Modified photodynamic therapy to minimize pain in the treatment of condylomata acuminata: A prospective, randomized, self-controlled study. Photodiagnosis Photodyn Ther. 2020 Dec;32:101915. Epub 2020 Jul 4. [CrossRef] [PubMed]
- 57. Hassan SNE, Hussein TM, Eldeeb ME. Photodynamic therapy using methylene blue and intense pulsed light versus intense pulsed light alone in treatment of verruca: A randomized controlled study. Photodiagnosis Photodyn Ther. 2021 Dec;36:102541. Epub 2021 Sep 20. [CrossRef] [PubMed]
- 58. Buzzá HH, Stringasci MD, de Arruda SS, Crestana RHS, de Castro CA, Bagnato VS, Inada NM. HPV-induced condylomata acuminata treated by Photodynamic Therapy in comparison with trichloroacetic acid: A randomized clinical trial. Photodiagnosis Photodyn Ther. 2021 Sep;35:102465. Epub 2021 Jul 29. [CrossRef] [PubMed]
- 59. Vellappally S, Mahmoud MH, Alaqeel SM, Alotaibi RN, Almansour H, Alageel O, Hashem M, Fouad H, Saadaldin S, Sukumaran A. Efficacy of antimicrobial photodynamic therapy versus antiviral therapy in the treatment of herpetic gingivostomatitis among children: Aa randomized controlled clinical trial. Photodiagnosis Photodyn Ther. 2022 Sep;39:102895. Epub 2022 Apr 30. [CrossRef] [PubMed]
- 60. Swapna LA, Alawad AO, Abdullah AlAmri L, Sayed Abdul N, Qamar Z, Vempalli S, Niazi FH. Efficacy of 5-aminolevulinic acid-mediated photodynamic therapy in patients with nicotine stomatitis. Photodiagnosis Photodyn Ther. 2023 Mar;41:103152. Epub 2022 Dec 2. [CrossRef] [PubMed]
- 61. Bezerra DT, La Selva A, Cecatto RB, Deana AM, Prates RA, Bussadori SK, Mesquita-Ferrari RA, Motta LJ, Fernandes KPS, Martimbianco ALC, Frochot C, Pereira BJ, Rossi F, Mimica MJ, Horliana ACRT. Antimicrobial Photodynamic Therapy in the Nasal Decolonization of Maintenance Hemodialysis Patients: A Pilot Randomized Trial. Am J Kidney Dis. 2023 May;81(5):528-536.e1. Epub 2022 Nov 14. [CrossRef] [PubMed]
- 62. Shao J, Hu M, Wang W, Pan Z, Zhao D, Liu J, Lv M, Zhang Y, Li Z. Indocyanine green based photodynamic therapy for keloids: Fundamental investigation and clinical improvement. Photodiagnosis Photodyn Ther. 2024 Feb;45:103903. Epub 2023 Nov 19. [CrossRef] [PubMed]
- 63. Fernandez-Montero A, Zuaznabar J, Pina-Sanchez M, Maestro S, Martin-Navarro L, Muñoz-Rodríguez N, Olagüe C, Pastrana M, Martínez-Fernández M, Camps G, Rodriguez JA, Marchese FP, Zazpe J, Pozuelo M, Del Pozo JL, Quiroga J, Pineda-Lucena A, Reina G, Kolenda J, Moreno-Galarraga L, Gonzalez-Aseguinolaza G, Rua M, Smerdou C, Carmona-Torre F, Argemi J. Photodynamic nasal SARS-CoV-2 decolonization shortens infectivity and influences specific T-Cell responses. Front Cell Infect Microbiol. 2023 Jan 25;13:1110467. [CrossRef] [PubMed] [PubMed Central]
- 64. Li X, Lee S, Yoon J. Supramolecular photosensitizers rejuvenate photodynamic therapy. Chem Soc. 2018;47:1174−1188. [CrossRef]
- 65. Dyrała A, Kaleta-Richter M, Cylupa K, Porwoł P, Kawczyk-Krupka A. Zastosowanie hiperycyny w terapii fotodynamicznej – przegląd badań preklinicznych. Acta Bio-Optica et Informatica Medica. 2015;209-215.
- 66. Brown GC, Cooper CE. Nanomolar concentrations of nitric oxide reversibly inhibit synaptosomal respiration by competing with oxygen at cytochrome oxidase. FEBS Lett. 1994;356:295–298. [CrossRef]
- 67. Lu Y, Sun W, Du J, Fan J, Peng X. Immuno-photodynamic Therapy (IPDT): Organic Photosensitizers and Their Application in Cancer Ablation. ACS Au. 2023;3:682–699. [CrossRef]
- 68. Evensen JF, Moan J, Winkelman JW. Toxic and phototoxic effects of tetraphenylpophinesulphonate and haematoporphyrin derivative in vitro. Int J Radiat Biol Relat Stud Phys Chem Med. 1987;51:477-491. [CrossRef]
- 69. Berg K, Bommer JC, Moan J. Evaluation of sulfonated aluminum phthalocyanines for use in photochemotherapy. A study on the relative efficiencies of photoinactivation. Photochem Photobiol. 1989;49:587-594. [CrossRef]
- 70. Ma L, Moan J, Berg K. Evaluation of a new photosensitizer, meso-tetra-hydroksyphenyl-chlorin, for use in photodynamic therapy: comparison of its photobiological properties with those of two other photosensitizers. Int J Cancer. 1994;57:883-888. [CrossRef]
- 71. Cunderlikova B, Gangeskar L, Moan J. Acid-base properties of chlorin e6: relation to cellular uptake. J Photochem Photobiol B. 1999;53:81-90. [CrossRef]
- 72. Friberg EG, Cunderlikova B, Pettersen EO, Moan J. PH effects on the cellular uptake of four photosensitizing drugs evaluated for use in photodynamic therapy of cancer. Cancer Lett. 2003;195:73-80. [CrossRef]
- 73. Cunderlikova B, Sikurova L, Moan J. PH, serum proteins and ionic strength influence the uptake of merocyanine 540 by WiDr cells and its interaction with membrane structures. Bioelectrochemistry. 2003;59:1-10. [CrossRef]
- 74. Uzdensky AB, Bragin DE, Kolosov MS, Kubin A, Loew HG, Moan J. Photodynamic effect of hypericin and a water-soluble derivative on isolated crayfish neuron and surrounding glial cells. J Photochem Photobiol B. 2003;72:27-33. [CrossRef]
- 75. Peng Q, Brown SB, Moan J, Nesland JM, Wainwright M, Griffiths J, Dixon B, Cruse-Sawyer J, Vernon D. Biodistribution of a methylene blue derivative in tumor and normal tissue of rats. J Photochem Photobiol B. 1993;20:63-71. [CrossRef]
- 76. Graczykowa A. Fotodynamiczna metoda rozpoznawania i leczenia nowotworów. 1999.
- 77. Kübler AC. Medical Laser Application. 2005;20(1):37-45. [CrossRef]
- 78. Reddy GR, Bhojani MS, McConville P, Moody J, Moffat BA, Hall DE, Ross BD. Vascular targeted nanoparticles for imaging and treatment of brain tumors. Clin Cancer Res. 2006;12(22):6677–6686. [CrossRef]
- 79. Fakhar-E-Alam M, Ali SMU, Ibupoto ZH, Kimleang K, Atif M, Kashif M, Willander M. Sensitivity of A-549 human lung cancer cells to nanoporous zinc oxide conjugated with Photofrin. Lasers Med Sci. 2012;27(3):607–614. [CrossRef]
- 80. Jiang F, Lilge L, Grenier J, Li Y, Wilson MD, Chopp M. Photodynamic therapy of U87 human glioma in nude rat using liposome-delivered photofrin. Lasers Surg Med. 1998;22(2):74–80. [CrossRef]
- 81. Savarimuthu WP, Gananathan P, Rao AP, Manickam E, Singaravelu G. Protoporphyrin IX-gold nanoparticle conjugates for targeted photodynamic therapy–An in-vitro study. J Nanosci Nanotechnol. 2014;15(8):5577–5584. [CrossRef]
- 82. Juárez AAS, Alvarado EM, Gallegos ER. Cell death induced by photodynamic therapy with the conjugate of gold nanoparticles-PpIX in HeLa cell line. In AIP conference proceedings. 2019;2099:040008. [CrossRef]
- 83. Ashjari M, Dehfuly S, Fatehi D, Shabani R, Koruji M. Efficient functionalization of gold nanoparticles using cysteine conjugated protoporphyrin IX for singlet oxygen production in vitro. RSC Adv. 2015;5(127):104621–104628. [CrossRef]
- 84. Ning LG, Liu P, Wang B, Li CM, Kang ET, Lu ZS, Xu LQ. Hydrothermal derived protoporphyrin IX nanoparticles for inactivation and imaging of bacteria strains. J Colloid Interface Sci. 2019;549:72–79. [CrossRef]
- 85. Yang K, Wang C, Liu C, Ding S, Tian F, Li F. Bioluminescence-initiated photodynamic therapy bridged on high-luminescent carbon dots-conjugated protoporphyrin IX. J Mater Sci. 2019;54(4):3383–3391. [CrossRef]
- 86. Lismont M, Dreesen L, Heinrichs B, Páez CA. Protoporphyrin IX-functionalized AgSiO2 Core-Shell nanoparticles: Plasmonic enhancement of fluorescence and singlet oxygen production. Photochem Photobiol. 2016;92(2):247–256. [CrossRef]
- 87. Wang M, Geilich BM, Keidar M, Webster TJ. Killing malignant melanoma cells with protoporphyrin IX-loaded polymersome-mediated photodynamic therapy and cold atmospheric plasma. Int J Nanomedicine. 2017;12:4117–4127. [CrossRef]
- 88. Yan L, Miller J, Yuan M, Liu JF, Busch TM, Tsourkas A, Cheng Z. Improved photodynamic therapy efficacy of Protoporphyrin IX-loaded polymeric micelles using Erlotinib pretreatment. Biomacromolecules. 2017;18(6):1836–1844. [CrossRef]
- 89. Hinger D, Navarro F, Käch A, Thomann JS, Mittler F, Couffin AC, Maake C. Photoinduced effects of m-tetrahydroxyphenylchlorin loaded lipid nanoemulsions on multicellular tumor spheroids. J Nanobiotechnology. 2016;14(1):68. [CrossRef]
- 90. Amirshaghaghi A, Yan L, Miller J, Daniel Y, Stein JM, Busch TM, Tsourkas A. Chlorin e6-coated superparamagnetic Iron oxide nanoparticle (SPION) nanoclusters as a Theranostic agent for dual-mode imaging and photodynamic therapy. Sci Rep. 2019;9(1):2613. [CrossRef]
- 91. Kumari P, Rompicharla SVK, Bhatt H, Ghosh B, Biswas S. Development of chlorin e6-conjugated poly(ethylene glycol)-poly(d,l-lactide) nanoparticles for photodynamic therapy. Nanomedicine. 2019;14(7):819–834. [CrossRef]
- 92. Konan-Kouakou YN, Boch R, Gurny R, Allémann E. In vitro and in vivo activities of verteporfin-loaded nanoparticles. J Control Release. 2005;103(1):83–91. [CrossRef]
- 93. Wang S, Fan W, Kim G, Hah HJ, Lee YEK, Kopelman R, Pandey RK. Novel methods to incorporate photosensitizers into nanocarriers for cancer treatment by photodynamic therapy. Lasers Surg Med. 2011;43(7):686–695. [CrossRef]
- 94. Li L, Chen Y, Chen W, Tan Y, Chen H, Yin J. Photodynamic therapy based on organic small molecular fluorescent dyes. Chinese Chem Lett. 2019;30(10):1689-1703. [CrossRef]
- 95. Pogue BW, Gibbs-Strauss S, Valdés PA, Samkoe K, Roberts DW, Paulsen KD. Review of Neurosurgical Fluorescence Imaging Methodologies. IEEE J Sel Top Quantum Electron. 2010;25(1):1-16. [CrossRef]
- 96. Jing R, Wang Q, Chen L, Li G, Li R, Zhang L, Zhang H, Zuo B, Seow Y, Qiao X, Wang B, Xu J, Chen J, Song T. Functional imaging and targeted drug delivery in mice and patient tumors with a cell nucleolus-localizing and tumor-targeting peptide. Biomaterials. 2022;289:1-12. [CrossRef]
- 97. Fukushi J, Makagiansar IT, Stallcup WB. NG2 Proteoglycan Promotes Endothelial Cell Motility and Angiogenesis via Engagement of Galectin-3 and α3β1 Integrin. Mol Biol Cell. 2004;15(8):3580-3590. [CrossRef]
- 98. Bando Y, Grimm C, Cornejo VH, Yuste R. Genetic voltage indicators. BMC Biol. 2019;17:71. [CrossRef]
- 99. Morton CA, McKenna KE, Rhodes LE. British Association of Dermatologists' guidelines for the management of squamous cell carcinoma in situ (Bowen's disease) 2014. Br J Dermatol. 2014;170(2):245-260. [CrossRef]
- 100. Biel MA. Photodynamic therapy of head and neck cancers. Methods Mol Biol. 2010;635:281-293. [CrossRef]
- 101. Pervaiz S, Olivo M. Art and science of photodynamic therapy. Clin Exp Pharmacol Physiol. 2006;33(5-6):551-556. [CrossRef]
- 102. Allison RR, Bagnato VS, Cuenca R, Downie GH, Sibata CH. The future of photodynamic therapy in oncology. Future Oncol. 2006;2:53-71. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



