
Submitted:
30 April 2024
Posted:
01 May 2024
You are already at the latest version
Abstract
Understanding and addressing dehumanization in healthcare is crucial due to its profound impact on patient care, ethical implications on patient dignity and autonomy, and its potential to affect the psychological well-being of healthcare professionals. The primary aim of this study was to develop reliable and valid instruments measuring two different types of dehumanization, namely animalistic dehumanization (i.e., stripping one of their uniquely human characteristics) and mechanistic dehumanization (i.e., striping one of their human nature characteristics) among healthcare professionals. In a cross-sectional validation study among healthcare professionals, we developed and tested measures of both animalistic and mechanistic dehumanization, focusing on dehumanization of patients (hetero-dehumanization) and oneself (self-dehumanization), respectively. All measures were developed and validated based on a concept analysis, a literature review, and an appraisal of pre-existing scales. The research was conducted among 400 nurses and medical doctors employed in Greek public hospitals. Coefficient Validity Ratio results showed that 100% of items were acceptable for both measures. The newly developed hetero-dehumanization scale encompassed two-factors (factor 1: animalistic dehumanization, factor 2: mechanistic dehumanization, Cronbach’s alpha was equal to 0.86 for each measure). The self-dehumanization scale was a mono-factorial measure mechanistic dehumanization (Cronbach’s alpha = 0.97). Two validated measures of (self and hetero-) animalistic and mechanistic dehumanization measures were developed for the assessment of dehumanization among health professionals, which will form the basis for future research in this important scientific field.
Keywords:
animalistic and mechanistic dehumanization
; hetero and self-dehumanization
; healthcare
; doctor
; nurse
; hospital
1. Introduction
Dehumanization is a concerning phenomenon that involves perceiving certain individuals as less than human, thereby stripping them of their inherent human qualities and rights, and it contributes to escalating discrimination and mistreatment. Specifically, dehumanization manifests as the tendency for some individuals to deny others their humanity (hetero-dehumanization), depriving them of fundamental rights such as respect and equity [1,2], as well as themselves (self-dehumanization), as a coping mechanism to shield themselves from emotional distress or to meet societal norms or expectations. This phenomenon concerns both interpersonal and intergroup relationships and is often accompanied by violence or aggression. As such, dehumanization involves socio-cognitive aspects and is associated with moral exclusion and moral disengagement [2,3,4].
1.1. Hetero-Dehumanization
The dehumanization literature identifies two types of hetero-dehumanization, namely animalistic and mechanistic dehumanization [2,3]. Animalistic dehumanization involves the reduced attribution of exclusively human qualities (human uniqueness) to others (e.g., logic, morality, sensitivity, kindness), thus considering people as driven by impulses, moods, and instincts similar to those of animals. As a result, animalistically dehumanized individuals are treated with disgust, contempt, and acts of humiliation. Mechanistic dehumanization involves stripping individuals of their inherent human qualities (human nature), such as emotional responsiveness, interpersonal warmth, and cognitive receptivity, which are fundamental aspects of their humanity.
Accordingly, mechanistically dehumanized human beings are treated as machines or objects and are considered to lack individual identity. As a result, mechanistically dehumanized targets are viewed as introverted and passive beings unworthy of moral concern or care [5,6,7].
Hetero-dehumanization, be it animalistic or mechanistic, is particularly relevant among healthcare professionals due to its potential impact on patient care, communication, trust, and health disparities [8]. When healthcare providers perceive patients as subhuman beings (i.e., animals) or objects rather than as autonomous entities with emotions, preferences, and rights, it can result in negligence, dismissiveness, or even mistreatment, thereby compromising the quality of care provided [9]. For instance, modern medicine often relies on standardized biomedical models, neglecting personalized care tailored to individual needs and emotional support. According to Lebowitz and Ahn (2014) [10], when physicians focus on the biological and genetic explanations for diseases, they can perceive patients as physiologically different from “healthy” people. Consequently, this perspective can diminish empathy and foster dehumanizing behaviors in healthcare settings [10], leading to the treatment of the body as a machine or object and illness as a malfunction of body mechanics. Institutions such as hospitals even favor such latent forms of dehumanization due to their structure and organization [11].
1.2. Self-Dehumanization
As previously stated, besides dehumanizing others, people often dehumanize themselves as well, which they do as a coping mechanism to protect themselves from emotional pain or to conform to social expectations [8]. Indeed, although self-dehumanization is associated with aversive self-awareness, lack of self-esteem or a meaningful life, and with the experience of intense negative feelings (such as shame, sadness, anger, and guilt), people may resort to self-dehumanization processes to mitigate the impact of witnessing others’ suffering [1,12]. More specifically, research shows that when employees are continuously exposed to stressful work environments, such as the healthcare environment, they tend to dehumanize themselves, an act that serves as a defensive mechanism that medical staff use to protect themselves from negative feelings. Unsurprisingly, self-dehumanization is related, in turn, to treating patients as objects rather than autonomous human beings [12]. In a similar vein, Trifiletti et al. (2014) [8] suggested that animalistic dehumanization of patients is a way for nurses to cope with work-related stress and stress-related symptoms [8,13].
Interestingly, previous research shows that when it comes to self-dehumanization individuals tend to exhibit more mechanistic rather than animalistic dehumanization. In essence, people are hesitant to strip themselves of their uniquely human qualities, yet they are inclined to disassociate from their human nature characteristics when confronted with emotionally challenging circumstances. This phenomenon can be attributed to two primary factors: First, animalistic dehumanization may not offer any adaptive advantages to individuals as it fails to serve as a defense mechanism. Secondly, animalistic dehumanization could be linked to a decrease in social standing, leading to feelings of inferiority that are detrimental to individuals’ well-being [14].
1.3. The Current Study
Despite its prevalence in healthcare settings, dehumanization remains inadequately explored, with a notable absence of validated questionnaires tailored to assess dehumanization within the healthcare domain. Given the emotionally taxing nature of healthcare, characterized by suffering and pain [13,15], we argue that validated measures specifically addressing dehumanization in this context are imperative. Furthermore, it is crucial to recognize that dehumanization is profoundly influenced by cultural and broader social factors [16]. Indeed, in contexts such as countries where healthcare institutions lack resources or infrastructure, both professionals and patients may encounter significant challenges. Greece exemplifies such a context, where healthcare professionals grapple with substantial difficulties in navigating the inherent suffering within the healthcare system. Therefore, investigating dehumanization among healthcare personnel in Greece presents an intriguing opportunity to explore the interplay of cultural dynamics, systemic challenges, and social contexts within the healthcare system. Greece’s economic crisis and influx of migrants and refugees may have contributed to the increased levels of dehumanization among healthcare providers [17]. Accordingly, understanding the prevalence and implications of dehumanization among healthcare providers in this context can inform efforts to enhance professional training, organizational support systems, and patient-provider relationships, ultimately contributing to the improvement of healthcare quality, equity, and compassion in Greece and beyond.
Thus, the main aim of the present study was the development and validation of appropriate tools measuring both forms of dehumanization, animalistic and mechanistic, targeted towards patients (hetero-dehumanization) and to oneself (self-dehumanization), among healthcare professionals, including doctors and nurses working in public hospitals in Greece.
2. Materials and Methods
2.1. Participants
The research was conducted in 6 public hospitals in Crete (Greece) and data were collected between November 2021 and January 2022. A convenience sample of 400 medical doctors and clinical nurses were recruited in total.
2.2. The questionnaires
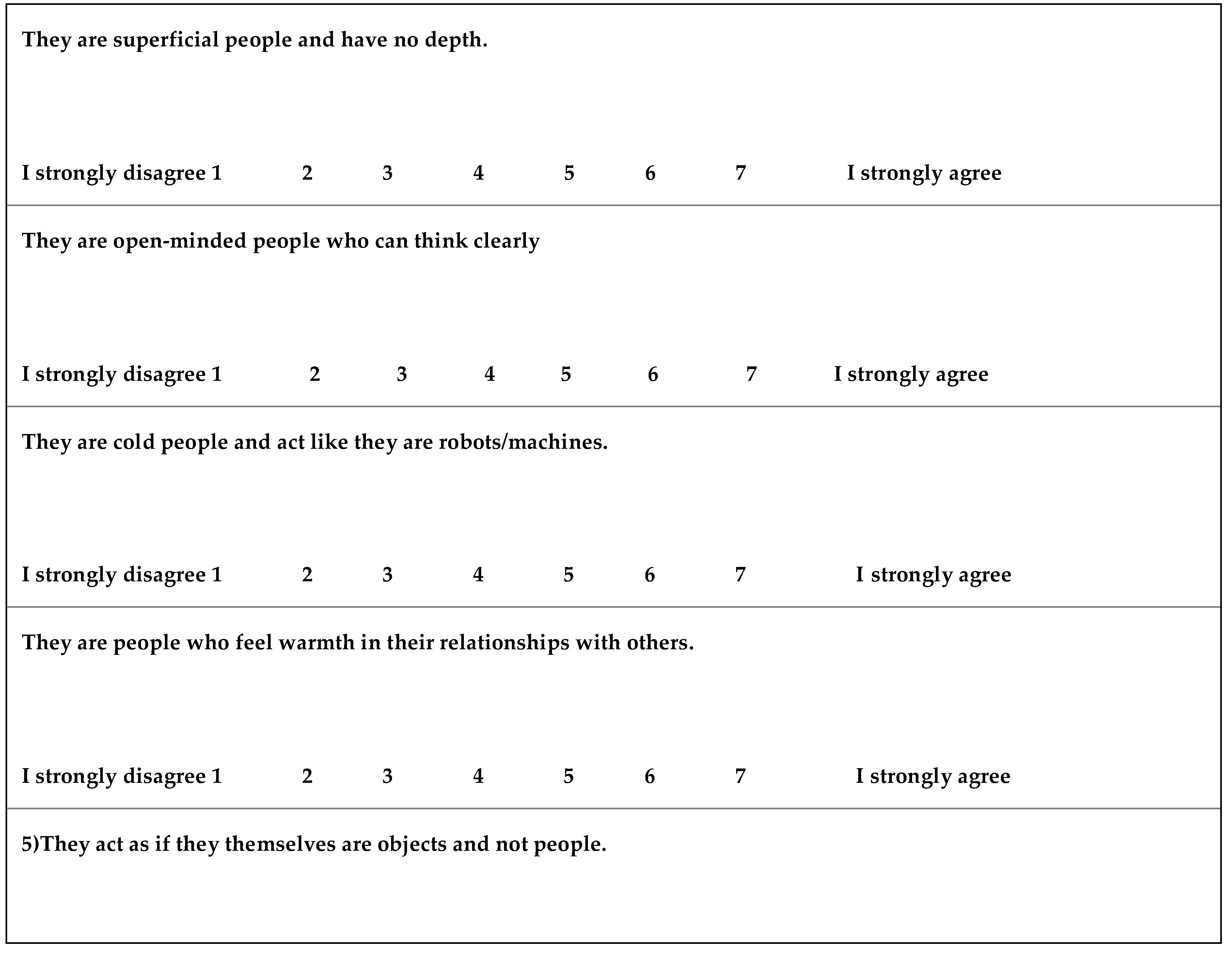
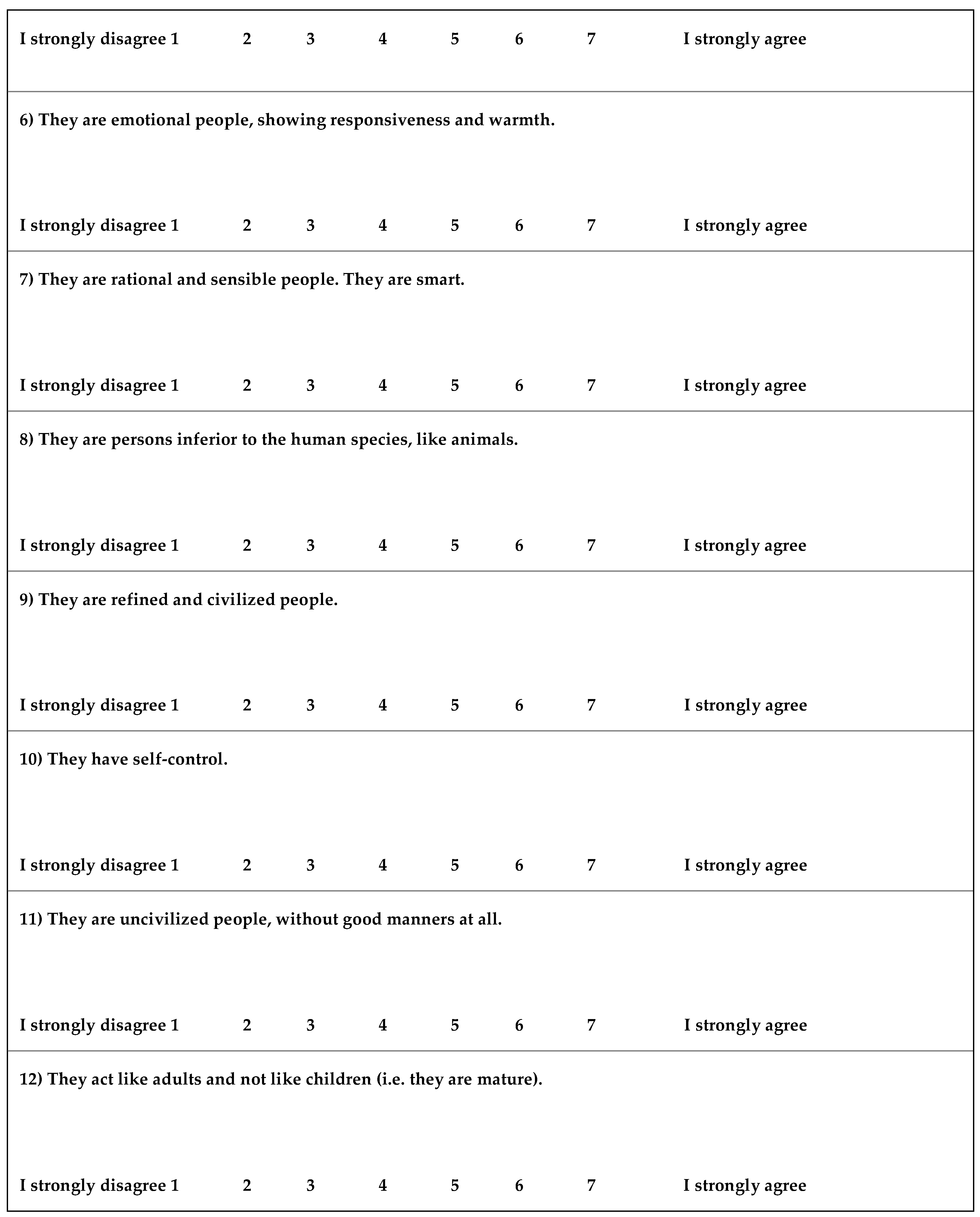
We developed a hetero-dehumanization scale consisting of 12 items measuring the dehumanization of patients. This scale consisted of two subscales: animalistic hetero-dehumanization and mechanistic hetero-dehumanization. Fousiani et al. (2019) [18] have previously developed a hetero-dehumanization scale based on Haslam’s (2006) [2] dehumanization model; however, that scale has not been used among healthcare professionals and has not been validated. The items were measured on a 7-point Likert scale (1=absolutely to disagree, 7=absolutely agree) [18]. A sample item for animalistic hetero-dehumanization was “7)They are rational and sensible people. They are smart. 8)They are persons inferior to the human species, like animals”. A sample item for mechanistic hetero-dehumanization was “1) They are superficial people and have no depth. 2) They are open-minded people who can think clearly. ”.
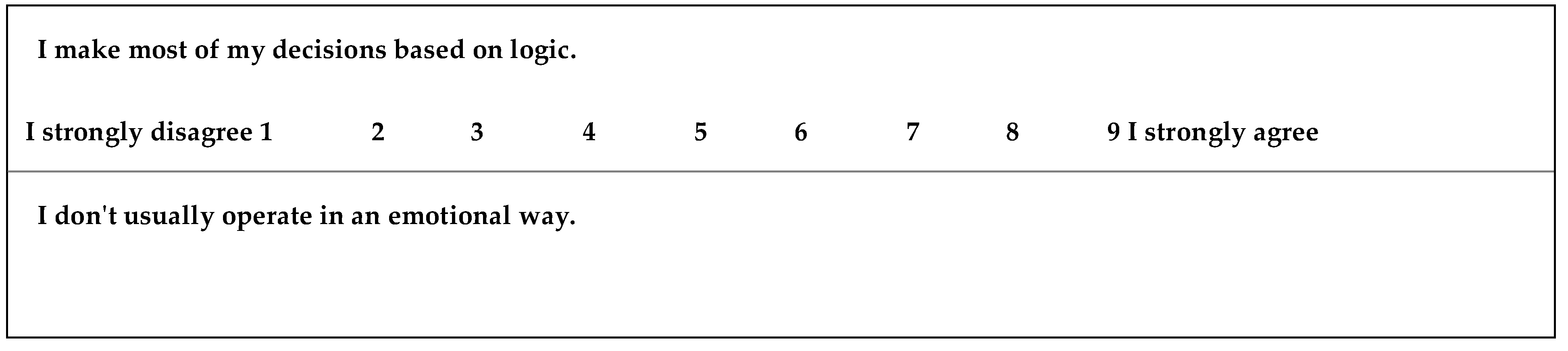
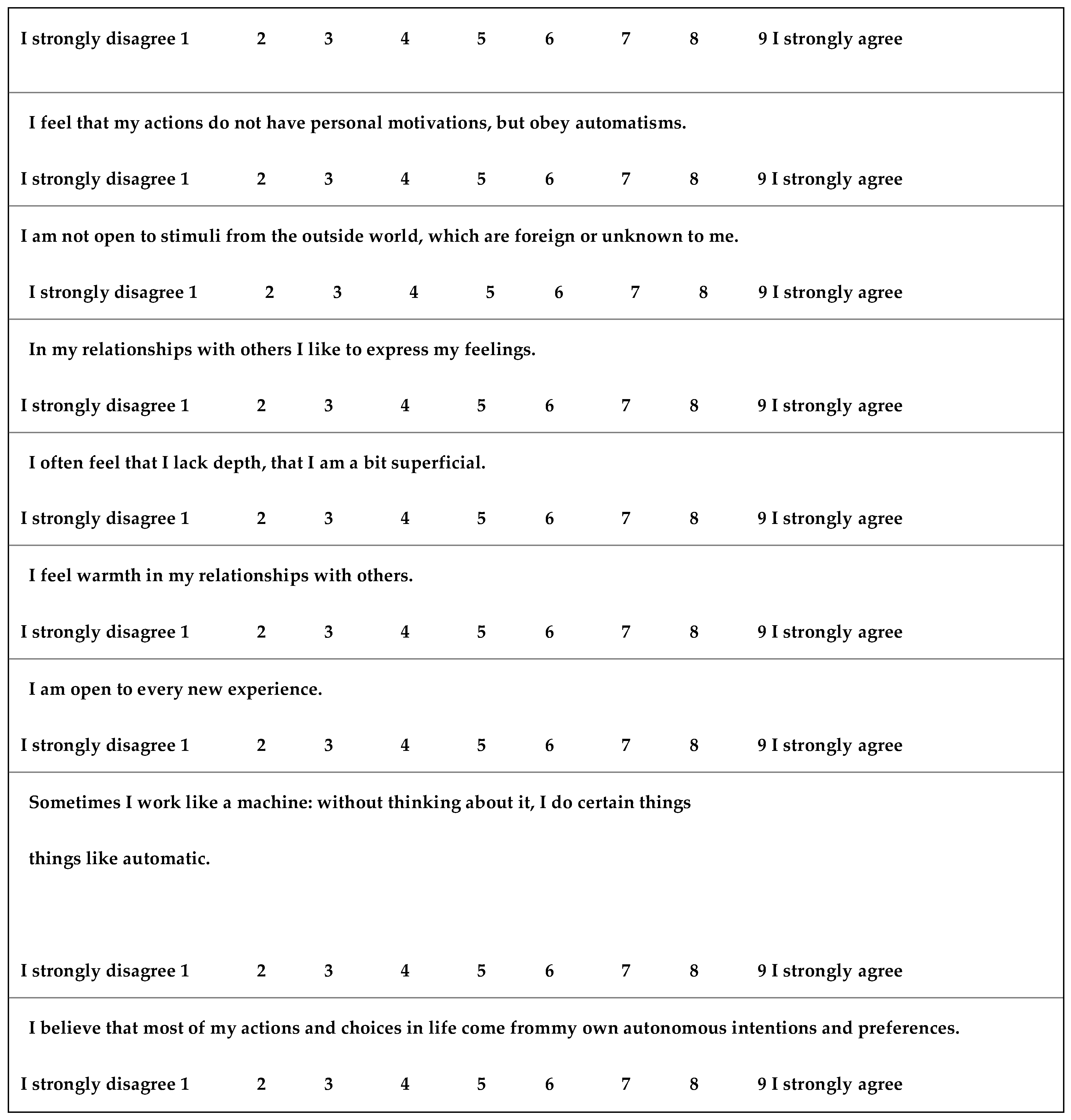
We also developed a self-dehumanization scale consisting of 10 items measuring dehumanization among healthcare personnel. The scale exclusively focused on mechanistic self-dehumanization, as prior research indicates that individuals’ are inclined to show a greater tendency towards mechanistic rather than animalistic dehumanization and was based on a pre-existing but not validated scale developed by Sakalakiet al. (2017) [1,2,5]. The items were measured on a 9-point Likert scale (1= absolutely disagree to 9= absolutely agree). A sample item was “1) I make most of my decisions based on logic. 2) I don't usually operate in an emotional way. ”.
Participants completed their socio-demographic characteristics, including some work-related questions. The questionnaire was evaluated by three experts in the field of dehumanization, who therefore had the experience and expertise to evaluate the tool, also to propose methods for improving it (content validity) [19]. Items with a Coefficient Validity Ratio (CVR) >0.70 were preserved in the final version of the instrument. We also calculated the content validity index (CVI) for the instrument as a whole, considering a value >0.80 to be adequate. Afterward, a group of five doctors and five nurses was invited to test the scale for its linguistic precision and clarity and confirm that the scale consists of questions that are consistent with the attribute to be measured and does not result in an incomplete response to the questions or misleading answers[20]. These individuals were excluded from the final study’s sample.
2.3. Ethical considerations
This survey was carried out in full compliance with the new General Data Protection Regulation (GDPR) [EU 2016/679] 25.5.2018 on sensitive personal data. Prior to its implementation, the relevant approval was secured by the respective services. The data collected were anonymous, their use was made solely for the purposes of the survey, and access to them by the lead researcher. The participants gave their informed consent prior to the data collection.
2.4. Analytical Plan
We performed the statistical analysis using SPSS version 26.0 (SPSS Inc., Chicago, IL, USA). To check the condition of normality, the Shapiro-Wilk test was used along with the study of the graphic representations "Normal Q-Q plot", "Detrended Normal Q-Q plot", and "Box Plot". For all tests, statistical differences were determined to be significant at p <0.05. Continuous variables were represented as mean ± standard deviation and categorical variables as frequency and percentage. To investigate the relationship between two continuous variables was used the Pearson coefficient, between a continuous and an ordinal variable the Spearman correlation coefficient, and between a continuous and a dichotomous variable the Point Biserial coefficient. Analysis of variance (ANOVA) was used to study the relationship between a continuous and a nominal variable. Internal consistency was assessed by Cronbach’s alpha. A Cronbach α coefficient >0.7 indicates sufficient reliability for research purposes and suggests that items are interdependent and homogeneous in terms of the construct they measure. For clinical applications α>0.8 is desirable. Exploratory Factor Analysis, using the principal component extraction method with Varimax rotation, was conducted to determine the factor structure of the items of the (Hetero) Dehumanization and Self-Dehumanization scales. Bartlett’s test of sphericity was conducted to examine the correlation among the items. The Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy was computed for quantifying the degree of intercorrelations among the variables and the appropriateness of factor analysis. To justify factor analysis, KMO values should exceed 0.60. For the final model, we used the combination of the following selection criteria: (a) sample size ≥250, (b) scree plot, (c) each factor contains items with loading ≥0.40 while at the same time loading <0.40 to all other factors, (d) each factor contains at least three items with loading ≥0.40, and (e) proportion of the total variance explained by the retained factors should be at least 60%.
3. Results
The sample comprised 400 participants, 297 (74.3 %) females and 103 (25.7 %) males, the mean age of 43.8 years (Table 1). Fifty-five percent (54.5%) of them lived in a city with >150,000 inhabitants, 31.8% in a city with >150,000 inhabitants and 13.8% in a village. Fifty-nine point three percent (59.3%) were married, 32.8% single, 7.3% divorced, and 0.8% widowed. Two hundred ninety-four percent (294) (73.5%) of the participants were nurses and 106 (26.5%) medical doctors. Eighty-two percent (81.5%) hold a master's degree and 18.5% a PhD. Fifty-two percent (51.3%) worked in closed sections and 48.7% in open sections. Seventy-five percent (74.5%) work in cyclical hours and 25.5% in shifts. The average working time in the department was 9.2 years. Psychotherapy session has been attended by 16.5%. Table 4 and Table 5 list in detail (absolute number and percentage) the responses given to each question in the questionnaires Hetero- and Self-Dehumanization.
3.1. Animalistic and Mechanistic Hetero-Dehumanization and Self-Dehumanization Scales
3.1.1. Animalistic and Mechanistic Hetero-Dehumanization Scale
CVR results showed that 100% (n = 12) of items were acceptable. The Bartlett Test of Sphericity was 1,798.24 (p <0.001). The Kaiser-Meyer-Olkin measure of sampling adequacy was 0.882, showing that the data is suitable for factor analysis. The 12 items were analyzed via Principal Component extraction method, using a Varimax rotation. The analysis resulted in a model of two factors (Figure 1) which explains, based on the initial solution, 58.35% of the total variance. This percentage of the total dispersion is 58.31%, if we take standardized values. We appear to have strong evidence for a two-factor model that included all 12 items (Table 2). Questions 1-6 load on factor 1 (mechanistic dehumanization) and questions 7-12 on factor 2 (animalistic dehumanization). Both mechanistic dehumanization and animalistic dehumanization had a Cronbach’s alpha equal to 0.86.
3.1.2. Mechanistic Self-Dehumanization Scale
CVR results showed that 100% (n = 10) of items were acceptable. The Bartlett Test of Sphericity was 4,043.93 (p <0.001). The Kaiser-Meyer-Olkin measure of sampling adequacy was 0.976, showing that the data was suitable for factor analysis. The 10 items were analyzed via Principal Component extraction method, using a Varimax rotation. The analysis resulted in a model of one factor (Figure 2) which explains, based on the initial solution, 77.0% of the total variance. This percentage of the total dispersion was 76.7%, if we take standardized values. We appear to have strong evidence for a single-scale factor model that included all 10items (Table 3) with Cronbach’s 0.966.

Table 2.
Rotated Component Matrix (Dehumanization scale).
| Raw | Rescaled | ||||
| Component | Component | ||||
| 1 | 2 | 1 | 2 | ||
| DS-1 | 0,894 | 0,757 | |||
| DS-2 | 0,872 | 0,749 | |||
| DS-3 | 0,923 | 0,775 | |||
| DS-4 | 0,902 | 0,774 | |||
| DS-5 | 0,876 | 0,744 | |||
| DS-6 | 0,896 | 0,766 | |||
| DS-7 | 0,942 | 0,782 | |||
| DS-8 | 0,837 | 0,717 | |||
| DS-9 | 0,842 | 0,745 | |||
| DS-10 | 0,944 | 0,789 | |||
| DS-11 | 0,906 | 0,781 | |||
| DS-12 | 0,918 | 0,768 | |||
| Extraction Method: Principal Component Analysis.Rotation Method: Varimax with Kaiser Normalization. | |||||
Table 3.
Rotated Component Matrix (Self-Dehumanization scale).
| Raw | Rescaled | |
| Component | Component | |
| 1 | 1 | |
| SDS-1 | 1,478 | 0,882 |
| SDS-2 | 1,429 | 0,873 |
| SDS-3 | 1,045 | 0,828 |
| SDS-4 | 1,417 | 0,888 |
| SDS-5 | 1,415 | 0,873 |
| SDS-6 | 1,417 | 0,872 |
| SDS-7 | 1,410 | 0,884 |
| SDS-8 | 1,486 | 0,896 |
| SDS-9 | 1,432 | 0,884 |
| SDS-10 | 1,366 | 0,871 |
| Extraction Method: Principal Component Analysis.SDS = Self-Dehumanization scale | ||
Table 4.
Dehumanization scale answers.
| TotallyDisagree | 2 | 3 | 4 | 5 | 6 | CompletelyAgree | ||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | |
| They are superficial people and have no depth. | 41 | 10.3 | 92 | 23.0 | 131 | 32.8 | 88 | 22.0 | 45 | 11.3 | 2 | 0.5 | 1 | 0.3 |
| They are open-minded people who can think clearly. | 49 | 12.3 | 93 | 23.3 | 130 | 32.5 | 92 | 23.0 | 34 | 8.5 | 1 | 0.3 | 1 | 0.3 |
| They are cold people and act like robots/machines. | 46 | 11.5 | 90 | 22.5 | 130 | 32.5 | 91 | 22.8 | 40 | 10.0 | 1 | 0.3 | 2 | 0.5 |
| They are people who feel warmth in their relationships with others. | 36 | 9.0 | 95 | 23.8 | 123 | 30.8 | 102 | 25.5 | 40 | 10.0 | 3 | 0.8 | 1 | 0.3 |
| They act as if they themselves are objects and not people. | 38 | 9.5 | 92 | 23.0 | 133 | 33.3 | 89 | 22.3 | 45 | 11.3 | 1 | 0.3 | 2 | 0.5 |
| They are emotional people, showing responsiveness and warmth. | 45 | 11.3 | 85 | 21.3 | 133 | 33.3 | 94 | 23.5 | 40 | 10.0 | 3 | 0.8 | 0 | 0.0 |
| They are rational and sensible people. They are smart. | 2 | 0.5 | 1 | 0.3 | 42 | 10.5 | 89 | 22.3 | 130 | 32.5 | 88 | 22.0 | 48 | 12.0 |
| They are people inferior to the human species, like animals. | 1 | 0.3 | 2 | 0.5 | 40 | 10.0 | 81 | 20.3 | 152 | 38.0 | 76 | 19.0 | 48 | 12.0 |
| They are refined and civilized people. | 1 | 0.3 | 1 | 0.3 | 44 | 11.0 | 80 | 20.0 | 150 | 37.5 | 89 | 22.3 | 35 | 8.8 |
| They have self-control. | 1 | 0.3 | 2 | 0.5 | 48 | 12.0 | 62 | 15.5 | 151 | 37.8 | 87 | 21.8 | 49 | 12.3 |
| They are uncivilized people, without good manners at all. | 1 | 0.3 | 2 | 0.5 | 46 | 11.5 | 88 | 22.0 | 144 | 36.0 | 81 | 20.3 | 38 | 9.5 |
| They act like adults and not like children (i.e. they are mature). | 2 | 0.5 | 1 | 0.3 | 47 | 11.8 | 86 | 21.5 | 128 | 32.0 | 96 | 24.0 | 40 | 10.0 |
Table 5.
Self-Dehumanization scale answers.
| Totally Disagree | 2 | 3 | 4 | 5 | 6 | 7 | 8 | TotallyDisagree | ||||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | N | % | N | % | |
| I make most of my decisions based on logic. | 24 | 6.0 | 18 | 4.5 | 11 | 2.8 | 111 | 27.8 | 98 | 24.5 | 104 | 26.0 | 12 | 3.0 | 10 | 2.5 | 12 | 3.0 |
| I don't usually operate in an emotional way. | 18 | 4.5 | 19 | 4.8 | 16 | 4.0 | 107 | 26.8 | 98 | 24.5 | 108 | 27.0 | 13 | 3.3 | 7 | 1.8 | 14 | 3.5 |
| I feel that my actions are not based personal motives, but are due to automatisms. | 7 | 1.8 | 12 | 3.0 | 34 | 8.5 | 118 | 29.5 | 134 | 33.5 | 61 | 15.3 | 34 | 8.5 | 0 | 0.0 | 0 | 0.0 |
| I am not open to stimuli from the outside world, which are alien or unknown to me. | 17 | 4.3 | 19 | 4.8 | 17 | 4.3 | 93 | 23.3 | 128 | 32.0 | 92 | 23.0 | 14 | 3.5 | 7 | 1.8 | 13 | 3.3 |
| In my relationships with others, I like to express my feelings. | 21 | 5.3 | 18 | 4.5 | 14 | 3.5 | 94 | 23.5 | 108 | 27.0 | 111 | 27.8 | 16 | 4.0 | 8 | 2.0 | 10 | 2.5 |
| I often feel that I lack depth, that I am a bit superficial. | 17 | 4.3 | 17 | 4.3 | 19 | 4.8 | 122 | 30.5 | 91 | 22.8 | 100 | 25.0 | 12 | 3.0 | 8 | 2.0 | 14 | 3.5 |
| I feel warmth in my relationships with others. | 16 | 4.0 | 19 | 4.8 | 18 | 4.5 | 104 | 26.0 | 111 | 27.8 | 98 | 24.5 | 12 | 3.0 | 11 | 2.8 | 11 | 2.8 |
| I am open to every new experience. | 21 | 5.3 | 22 | 5.5 | 10 | 2.5 | 107 | 26.8 | 103 | 25.8 | 103 | 25.8 | 10 | 2.5 | 14 | 3.5 | 10 | 2.5 |
| Sometimes I work like a machine: without thinking about it, I do certain things like an automaton. | 18 | 4.5 | 17 | 4.3 | 18 | 4.5 | 98 | 24.5 | 104 | 26.0 | 111 | 27.8 | 11 | 2.8 | 12 | 3.0 | 11 | 2.8 |
| I believe that most of my actions and choices in life come frommy own autonomous intentions and preferences. | 18 | 4.5 | 13 | 3.3 | 22 | 5.5 | 104 | 26.0 | 106 | 26.5 | 103 | 25.8 | 13 | 3.3 | 14 | 3.5 | 7 | 1.8 |
Table 6.
Correlations.
| Age | Biologicalsex | Place of residence* | Marital status | Profession | Annual income | Postgraduate degrees | Labour Department | Years of work in this department | Working hours | Have you attended any psychotherapy sessions? | ||
| Mechanisticdehumanization | Correlation | -0,060 | -0,013 | -0,001 | 0,019 | -0,055 | 0,017 | 0,102 | -0,072 | 0,031 | -0,001 | -0,007 |
| Sig. (2-tailed) | 0,230 | 0,802 | 0,981 | 0,699 | 0,275 | 0,729 | 0,363 | 0,149 | 0,538 | 0,986 | 0,888 | |
| N | 400 | 400 | 400 | 400 | 400 | 400 | 81 | 400 | 400 | 400 | 400 | |
| Animalistic dehumanization | Correlation | -0,075 | -0,016 | -0,019 | 0,015 | -0,050 | 0,024 | 0,097 | -0,067 | 0,008 | 0,013 | -0,017 |
| Sig. (2-tailed) | 0,132 | 0,755 | 0,699 | 0,765 | 0,316 | 0,637 | 0,390 | 0,184 | 0,880 | 0,795 | 0,739 | |
| N | 400 | 400 | 400 | 400 | 400 | 400 | 81 | 400 | 400 | 400 | 400 | |
| Self-Dehumanization | Correlation | 0,035 | 0,087 | 0,061 | -0,011 | -0,078 | -0,013 | -0,127 | 0,023 | 0,131 | -0,060 | 0,108 |
| Sig. (2-tailed) | 0,483 | 0,081 | 0,225 | 0,822 | 0,120 | 0,789 | 0,259 | 0,653 | 0,009 | 0,230 | 0,031 | |
| N | 400 | 400 | 400 | 400 | 400 | 400 | 81 | 400 | 400 | 400 | 400 | |
* Spearman Correlation.
Table 7.
Analysis of variance (ANOVA) between marital status and scales.
| Sum of Squares | df | Mean Square | F | Sig. | ||
| Mechanistic dehumanization | BetweenGroups | 0,944 | 3 | 0,315 | 0,387 | 0,762 |
| WithinGroups | 321,487 | 396 | 0,812 | |||
| Total | 322,431 | 399 | ||||
| Animalistic dehumanization | BetweenGroups | 6,041 | 3 | 2,014 | 2,556 | 0,055 |
| WithinGroups | 312,016 | 396 | 0,788 | |||
| Total | 318,057 | 399 | ||||
| Mechanistic self-dehumanization | BetweenGroups | 5,985 | 3 | 1,995 | 1,034 | 0,378 |
| WithinGroups | 764,335 | 396 | 1,930 | |||
| Total | 770,320 | 399 | ||||
3.1.3. Means Score of the Dehumanization and Self-Dehumanization
The mean score of the Mechanistic Dehumanization subscale was calculated as 4.98 ± 0.90. The mean score of the Animalistic Dehumanization subscale was calculated as 3.02 ± 0.89 (Figure 3). The mean score of the Mechanistic Self-Dehumanization scale was calculated as 4.83 ± 1.39 (Figure 4).
Table 6 depicts no association between socio-demographic and occupational factors and the mechanistic dehumanization and animalistic dehumanization subscales. A significant relationship was found between the self dehumanization scale and years of work in the department (more years correspond to a higher scale score, p = 0.009), attendance of a psychotherapy session (individuals who have attended psychotherapy sessions are associated with higher scores on the scale, p = 0.031).
4. Discussion
In recent years, the scientific community has shown an increased interest in the phenomenon of dehumanization, which has extensively been examined in the field of social psychology. This is highlighted in multiple recent studies such as those by Haslam et al. (2014, 2016) [1,21,22,23,24,25,26]. It is well known that healthcare professionals, and especially doctors and nurses, frequently have to face this particularly difficult task. Since health science is a human-centered profession, this dynamic scientific field requires that professionals show a lot of passion and love, to face challenges both psychologically and physically and maintain their integrity over time.
However, dehumanization does not always come from immoral behavior or social rejection. Everyday dehumanization is likely to be unintentional, arising from a variety of factors usually related to structural and organizational aspects of health care [9,26,27]. Unfortunately, multiple difficulties in public hospitals - workplaces, the nature of the profession, as well as the lack of staff and motivation, increase physical and psychological fatigue, which easily leads to real burnout [9]. We would add that elements of personality, empathy, technology, and the external pressures of everyday life are factors contributing to this behavior among professionals. In this context, dehumanization is a complex psychological defense that ironically helps healthcare providers cope with and survive multiple unpleasant and debilitating personal and professional conditions [10]. Therefore, it is an emotional regulation strategy used by health care professionals [9], as it mentally gives them a shield, to alleviate the anxiety and feelings of guilt that may arise from causing pain [8,28]. Furthermore, an empirical study of the effect of dehumanization in the era of computerized information was done through Amazon Mechanical Turkish. The results showed that there appears to be a negative effect of the computer on the doctor-patient relationship and the resulting patient care [29].
The result of all the above observations indicates that in medical environments, multiple behavioral events offend the dignity of patients. Some healthcare professionals use inappropriate communication styles, using baby talk when speaking to elders, while others display various forms of aggressive behavior when interacting with the mentally ill [30, 31, 32].
The main objective of this study was to develop and validate measures for the assessment of both types of dehumanization, namely animalistic and mechanistic dehumanization in the field of healthcare, where dehumanization is a rampant phenomenon [2,11]. To the best of our knowledge, there was a lack of validated instruments for measuring dehumanization among healthcare professionals in Greece but also globally, a gap that this research aims to fill. In fact, the lack of validated instruments can lead to under-investigation of the phenomena and research initiatives suspension [33]. Utilizing the developed questionnaires in our research, both for dehumanization and self-dehumanization will enable researchers to systematically investigate and establish correlations between this phenomenon and other variables, thereby bridging gaps in the existing literature. Also, the thoughtful evaluation of the dehumanization phenomenon can deepen health professionals' understanding of its complexities and guide focused interventions.
Results of the present study revealed that both newly developed and validated scales are psychometrically sound and theoretically valid measures of dehumanization and self-dehumanization. Factor analysis of the dehumanization scale resulted in a two-factor solution consisting of six items per factor and interpreting 58.35% of the total variance. The two factors were namely mechanistic and animalistic dehumanization. This result is in agreement with the theoretical framework of dehumanization proposed by Haslam (2006) [2] that distinguishes those two forms of dehumanization [2]. Furthermore, factor analysis resulted in a one-factor solution for the self-dehumanization scale interpreting 77.0% of the total variance in agreement with the Bastian (2014) theoretical model [34] and reinforcing previous studies that are considering and investigating self-dehumanization with unidimensional scales. All items in both scales exhibited excellent factor loadings all above the threshold value of 0.30, indicating an acceptable structural validity of the validated instruments [35]. Factor analysis was used to explore the questionnaire's validity, revealing clear dimensions that accurately represent the underlying concepts we aimed to measure. The high factor loadings indicate that each question effectively contributes to its respective dimension, confirming the questionnaire's validity.
In addition, according to our results, the Cronbach alpha indicator values were acceptable. More specifically the reported values were as follows 0.855 for the “Mechanistic dehumanization” subscale, and 0.858 for the “Animalistic dehumanization” subscale whereas for self-dehumanization the value was equal to 0.966. The mentioned values were above the threshold of 0.70 in indicating good reliability for the values above 0.80 and excellent for those above 0.90 [36]. This means that the questions consistently measure the intended concepts, making our questionnaire a dependable tool for research.
The statistical study’s results showed that doctors and nurses mechanistically dehumanized patients at a moderate to a high level, and also dehumanized themselves at a moderate level. These results are consistent with the existing literature. According to the correlations conducted in our research no socio-demographic and occupational factors were found to be associated with the Mechanistic-Dehumanization and Animalistic-Dehumanization subscales. A significant relationship was found between the Self-Dehumanization scale and: a) years of work in this department (more years correspond to a higher scale score, p = 0.009), b) attending a psychotherapy session (individuals who have attended psychotherapy sessions are associated with higher scores on the scale, p = 0.031). Furthermore, marital status was not found to be associated with any scale.
As aforementioned, more years of experience is a risk factor for increased levels of dehumanization for healthcare professionals. Prolonged exposure to high workloads, stressful environments, and emotionally challenging patient interactions can gradually diminish a healthcare professional's sense of self-esteem leading to feelings of burnout, emotional exhaustion, and a reduced ability to empathize with others. Additionally, although the finding that healthcare providers attending a psychotherapy session seems controversial, it may be reasonable considering that psychological distress and vulnerability, common reasons for seeking therapy, can contribute to the self-dehumanization or dehumanization of others. Also, the therapeutic process itself may lead to increased feelings of shame or inadequacy, feelings that can promote self-dehumanization or hetero-dehumanization as an outcome or a defensive reaction, respectively. The same effect can be triggered by the therapeutic environment which can disclose identity conflicts and internal struggles, exacerbating experiences of dehumanization. A recent study carried out at the Sotiria Hospital in Athens, Greece, showed that healthcare professionals mechanically dehumanize hospitalized patients [25]. Another study found that nurses stigmatized and dehumanized patients with a psychiatric disorder more often, compared to people without a mental illness [37]. This occurrence might be related to the cultural stigma associated with mental illness, resulting in unfavorable prejudices and stereotypes. Additionally, the complexities and challenges of managing psychiatric disorders in healthcare settings, combined with potential gaps in mental health education and training, may contribute to elevated stress and frustration among healthcare providers, influencing their attitudes and behaviors towards patients [37].
Moreover, nurses tended to dehumanize patients more, if they felt dehumanized by their supervisors, and less if they had quality contacts [37]. This emphasizes the pivotal role of workplace dynamics and organizational culture that influence nurses’ attitudes and behaviors toward patient care. Establishing a supportive and respectful workplace atmosphere is paramount for both fostering an empathetic and compassionate environment for patients and bolstering the overall effectiveness and well-being of nurses.
Self-dehumanization is a phenomenon that can result either from being treated negatively by others or from one’s behavior when it harms others [1,2,25]. We would dare to say that the "offender" is also a "victim". Their character and experiences led them to self-dehumanization and the dehumanization of others. Research studies have shown that self-dehumanization occurs most often when people feel isolated, powerless, or out of control. A literature review of several studies showed that self-dehumanization appears to be due to a sense of helplessness rather than a random change in mood or negative self-esteem [38]. In another research, it was shown that the suffering experienced by the person and unpleasant situations can cause the rejection of humanity both in ourselves and in others [1]. In a recent study in Greece, it was confirmed that mental health specialists and hospital workers consider themselves more human compared to the general population, attributing to themselves characteristics of human nature and uniqueness [25]. However, in some cases, self-dehumanization can encourage the individual to take social initiatives to restore humanity in the eyes of others and their self-concept [34], which can be a hope for reducing this phenomenon.
4.1. Limitations
The present research faced some limitations. First of all, women outnumbered men in the sample, which is due to the nature of the profession as the majority of nurses are women. Secondly, the collected sample of 400 individuals, although large enough for statistical analysis, was not randomly selected. Finally, the cross-sectional study design limits the ability to establish causal relationships or assess changes over time.
The development of valid questionnaires that are intended to evaluate different aspects of dehumanization among healthcare professionals is the main strength of the present study. Providing precise measures to evaluate dehumanizing actions and attitudes is one of how our research makes a direct contribution to the improvement of patient care and the development of a more compassionate and empathic atmosphere within the healthcare system. These scales not only improve research capacities in the area of studying dehumanization, but they also have practical use in the form of directing interventions and training programs that are targeted at encouraging patient-centered care and professional ethics among healthcare workers.
5. Conclusions
Our study concluded with two valid scales that can be used to investigate the phenomenon of the dehumanization of patients and the self-dehumanization of health professionals. The statistical analysis revealed that health professionals were found to mechanistically dehumanize patients at a moderate to high level, while they also dehumanize themselves at a moderate level. Dehumanization appears to be highly relevant to several important psychosocial aspects of medical care, including quality of care, health inequity, health behaviors, and person-centered care which poses the necessity for further investigation of this phenomenon. Future research through new questionnaires can explore the effectiveness of these interventions. Also, the thoughtful evaluation of this phenomenon can deepen our understanding of its complexities and provide guidance for focused interventions. The results can contribute to the creation of information and awareness programs and educational programs that will help doctors and nurses but also the students of these universities, to deal more humanely with their patients. Health professionals should be informed about the current situation and healthcare policymakers and stakeholders should take the necessary actions and measures to identify potential improvements, ensure accountability, and promote patient-centered care.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, A.R., A.P., E.C.F., K.F., A.L., K.G., and E.P.; methodology, A.R., A.P., E.C.F., K.F., A.L., K.G., and E.P.; software, A.R., A.P., E.C.F., and E.P.; validation, A.R., A.P., E.C.F., K.F., A.L., K.G., and E.P..; formal analysis, A.R., A.P., E.C.F., K.F., and E.P.; investigation, A.R., A.P., K.F., and E.P.; resources, A.R., A.P., and E.P.; data curation, A.R., A.P., K.F., A.L., K.G., and E.P..; writing—original draft preparation, A.R., A.P., E.C.F., K.F., A.L., K.G., and E.P.; writing—review and editing, A.R., A.P., E.C.F., K.F., A.L., K.G., and E.P.; visualization, A.R., A.P., E.C.F., K.F., A.L., K.G., and E.P.; supervision, A.R., A.P., and E.P. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediTtaxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Institutional Review Board Statement
This survey was carried out in full compliance with the new General Data Protection Regulation (GDPR) [EU 2016/679] 25.5.2018 on sensitive personal data. Prior to its implementation, the relevant approvals were secured by the respective services.
Informed Consent Statement
The data collected were anonymous, their use was made solely for the purposes of the survey, and access to them by the lead researcher. The participants gave their informed consent prior to the data collection
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request
Acknowledgments
The authors would like to thank all participants for their voluntary participation.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Dehumanization Scale
The answers to sentences 2, 4, 6, 7, 9 and 10 are reversed so that all 12 sentences have the same conceptual direction.
Appendix B
(Mechanistic) Self-dehumanization scale
The answers to sentences 5, 7, and 8 are reversed so that all 10 sentences have the same conceptual direction.
References
- M. Sakalaki, C. Richardson, and K. Fousiani, “Is suffering less human? Distressing situations’ effects on dehumanizing the self and others,” Hell. J. Psychol., vol. 14, no. 1, pp. 39–63, 2017.
- N. Haslam, “Dehumanization: an integrative review,” Personal. Soc. Psychol. Rev. Off. J. Soc. Personal. Soc. Psychol. Inc, vol. 10, no. 3, pp. 252–264, 2006. [CrossRef]
- N. Haslam, S. Loughnan, C. Reynolds, and S. Wilson, “Dehumanization: A new perspective,” Soc. Personal. Psychol. Compass, vol. 1, no. 1, pp. 409–422, 2007.
- N. Haslam and P. Bain, “Humanizing the self: Moderators of the attribution of lesser humanness to others,” Pers. Soc. Psychol. Bull., vol. 33, no. 1, pp. 57–68, 2007.
- H. M. Gray, K. Gray, and D. M. Wegner, “Dimensions of mind perception,” science, vol. 315, no. 5812, pp. 619–619, 2007.
- K. Gray, J. Knobe, M. Sheskin, P. Bloom, and L. F. Barrett, “More than a body: mind perception and the nature of objectification.,” J. Pers. Soc. Psychol., vol. 101, no. 6, p. 1207, 2011.
- K. Gray, L. Young, and A. Waytz, “Mind perception is the essence of morality,” Psychol. Inq., vol. 23, no. 2, pp. 101–124, 2012.
- E. Trifiletti, G. A. Di Bernardo, R. Falvo, and D. Capozza, “Patients are not fully human: A nurse’s coping response to stress,” J. Appl. Soc. Psychol., vol. 44, no. 12, pp. 768–777, 2014.
- C. J. Hoogendoorn and N. D. Rodríguez, “Rethinking dehumanization, empathy, and burnout in healthcare contexts,” Curr. Opin. Behav. Sci., vol. 52, p. 101285, 2023.
- M. S. Lebowitz and W. Ahn, “Effects of biological explanations for mental disorders on clinicians’ empathy,” Proc. Natl. Acad. Sci. U. S. A., vol. 111, no. 50, pp. 17786–17790, Dec. 2014. [CrossRef]
- O. S. Haque and A. Waytz, “Dehumanization in medicine: Causes, solutions, and functions,” Perspect. Psychol. Sci., vol. 7, no. 2, pp. 176–186, 2012.
- J. M. Twenge, R. F. Baumeister, C. N. DeWall, N. J. Ciarocco, and J. M. Bartels, “Social exclusion decreases prosocial behavior.,” J. Pers. Soc. Psychol., vol. 92, no. 1, p. 56, 2007.
- E. Elder, A. N. B. Johnston, M. Wallis, and J. Crilly, “The demoralisation of nurses and medical doctors working in the emergency department: A qualitative descriptive study,” Int. Emerg. Nurs., vol. 52, p. 100841, Sep. 2020. [CrossRef]
- A. C. Moller and E. L. Deci, “Interpersonal control, dehumanization, and violence: A self-determination theory perspective,” Group Process. Intergroup Relat., vol. 13, no. 1, pp. 41–53, Jan. 2010. [CrossRef]
- J. Molina-Praena, L. Ramirez-Baena, J. L. Gómez-Urquiza, G. R. Cañadas, E. I. De la Fuente, and G. A. Cañadas-De la Fuente, “Levels of Burnout and Risk Factors in Medical Area Nurses: A Meta-Analytic Study,” Int. J. Environ. Res. Public. Health, vol. 15, no. 12, Art. no. 12, Dec. 2018. [CrossRef]
- E. Diniz, P. Castro, A. Bousfield, and S. Figueira Bernardes, “Classism and dehumanization in chronic pain: A qualitative study of nurses’ inferences about women of different socio-economic status,” Br. J. Health Psychol., vol. 25, no. 1, pp. 152–170, 2020. [CrossRef]
- T. A. Eikemo et al., “Health in crises. Migration, austerity and inequalities in Greece and Europe: introduction to the supplement,” Eur. J. Public Health, vol. 28, no. Suppl 5, pp. 1–4, Dec. 2018. [CrossRef]
- K. Fousiani, M. Michaelides, and P. Dimitropoulou, “The effects of ethnic group membership on bullying at school: when do observers dehumanize bullies?,” J. Soc. Psychol., vol. 159, no. 4, pp. 431–442, Jul. 2019. [CrossRef]
- D. F. Polit and C. T. Beck, “The content validity index: are you sure you know what’s being reported? Critique and recommendations,” Res. Nurs. Health, vol. 29, no. 5, pp. 489–497, 2006.
- F. Gravetter and L. Forzano, “Research methods for the behavioral sciences (Gravetter),” Belmont Cengage Learn., 2010.
- N. Haslam and S. Loughnan, “Dehumanization and infrahumanization,” Annu. Rev. Psychol., vol. 65, pp. 399–423, 2014.
- N. Haslam and M. Stratemeyer, “Recent research on dehumanization,” Curr. Opin. Psychol., vol. 11, pp. 25–29, 2016.
- J. Leyens, S. Demoulin, J. A. F. Vaes, R. Gaunt, and M. P. Paladino, “Infra-humanization: the wall of group diffrences,” Soc. Issues Policy Rev., vol. 1, pp. 173–216, 2007.
- J. Vaes, J.-P. Leyens, M. Paola Paladino, and M. Pires Miranda, “We are human, they are not: Driving forces behind outgroup dehumanisation and the humanisation of the ingroup,” Eur. Rev. Soc. Psychol., vol. 23, no. 1, pp. 64–106, 2012.
- D. Lekka et al., “Dehumanization of Hospitalized Patients and Self-Dehumanization by Health Professionals and the General Population in Greece.,” Cureus, vol. 13, no. 12, p. e20182, Dec. 2021. [CrossRef]
- M. J. Basile et al., “Humanizing the ICU Patient: A Qualitative Exploration of Behaviors Experienced by Patients, Caregivers, and ICU Staff,” Crit. Care Explor., vol. 3, no. 6, p. e0463, Jun. 2021. [CrossRef]
- N. Katz, J. Jones, L. Mansfield, and M. Gold, “The Impact of Health Professionals’ Language on Patient Experience: A Case Study,” J. Patient Exp., vol. 9, p. 237437352210925, Apr. 2022. [CrossRef]
- A. Bandura, “Moral disengagement in the perpetration of inhumanities,” Personal. Soc. Psychol. Rev., vol. 3, no. 3, pp. 193–209, 1999.
- C. Maddock, “The dehumanization of the American healthcare professional: The Impact of technology on the ever-evolving world of medicine,” 2019.
- M. Grissinger, “Disrespectful Behavior in Health Care,” Pharm. Ther., vol. 42, no. 2, pp. 74–77, Feb. 2017.
- C. A. Shaw and J. K. Gordon, “Understanding Elderspeak: An Evolutionary Concept Analysis,” Innov. Aging, vol. 5, no. 3, p. igab023, Jul. 2021. [CrossRef]
- D. Capozza, “Dehumanization in medical contexts: An expanding research field,” TPM - Test. Psychom. Methodol. Appl. Psychol., no. 1, pp. 545–559. 2016. [CrossRef]
- J. L. Bastos, R. P. Duquia, D. A. González-Chica, J. M. Mesa, and R. R. Bonamigo, “Field work I: selecting the instrument for data collection,” An. Bras. Dermatol., vol. 89, no. 6, pp. 918–923. 2014. [CrossRef]
- B. Bastian and C. Crimston, “Self-dehumanization,” TPM - Test., vol. 21, pp. 241–250, Sep. 2014. [CrossRef]
- M. Tavakol and A. Wetzel, “Factor Analysis: a means for theory and instrument development in support of construct validity,” Int. J. Med. Educ., vol. 11, pp. 245–247, Nov. 2020. [CrossRef]
- M. Heo, N. Kim, and M. S. Faith, “Statistical power as a function of Cronbach alpha of instrument questionnaire items,” BMC Med. Res. Methodol., vol. 15, p. 86, Oct. 2015. [CrossRef]
- S. Fontesse, X. Rimez, and P. Maurage, “Stigmatization and dehumanization perceptions towards psychiatric patients among nurses: A path-analysis approach,” Arch. Psychiatr. Nurs., vol. 35, no. 2, pp. 153–161, 2021.
- W. Yang, S. Jin, S. He, Q. Fan, and Y. Zhu, “The impact of power on humanity: self-dehumanization in powerlessness,” PloS One, vol. 10, no. 5, p. e0125721, 2015. [CrossRef]
Figure 1.
Scree plot (Dehumanization scale).
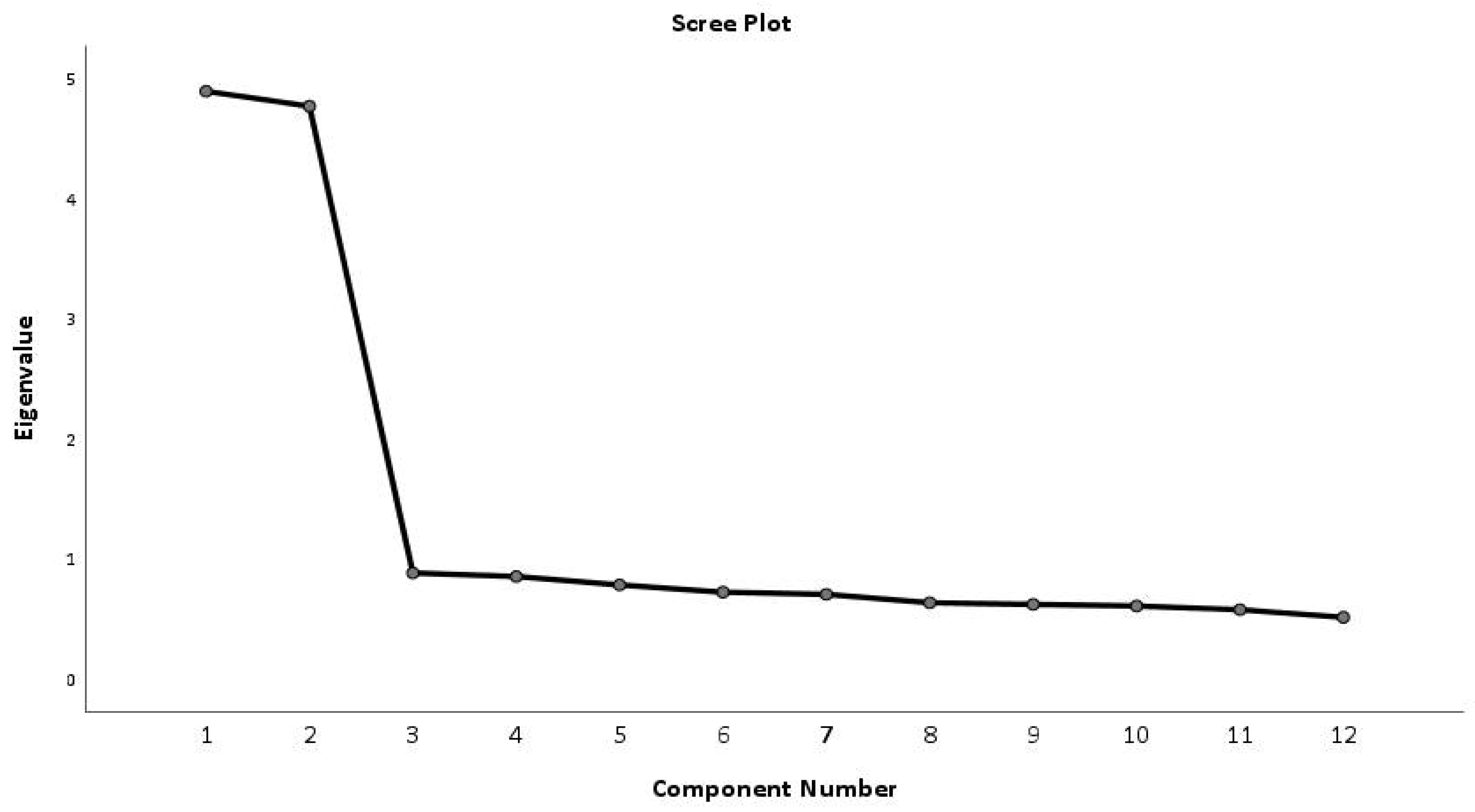
Figure 2.
Scree plot (Self-Dehumanization scale).
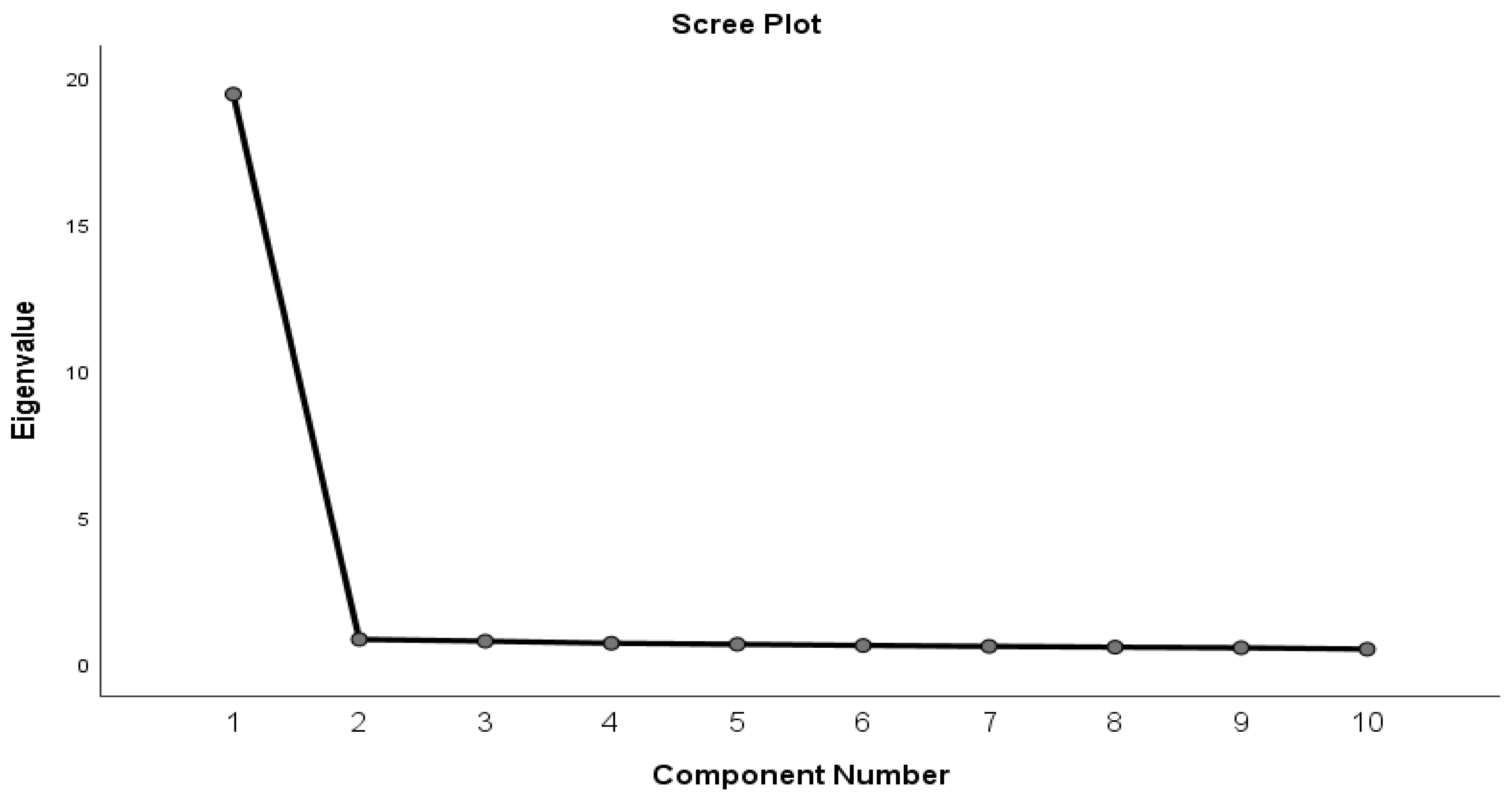
Figure 3.
Box plot showing the Hetero- Dehumanization Scale.
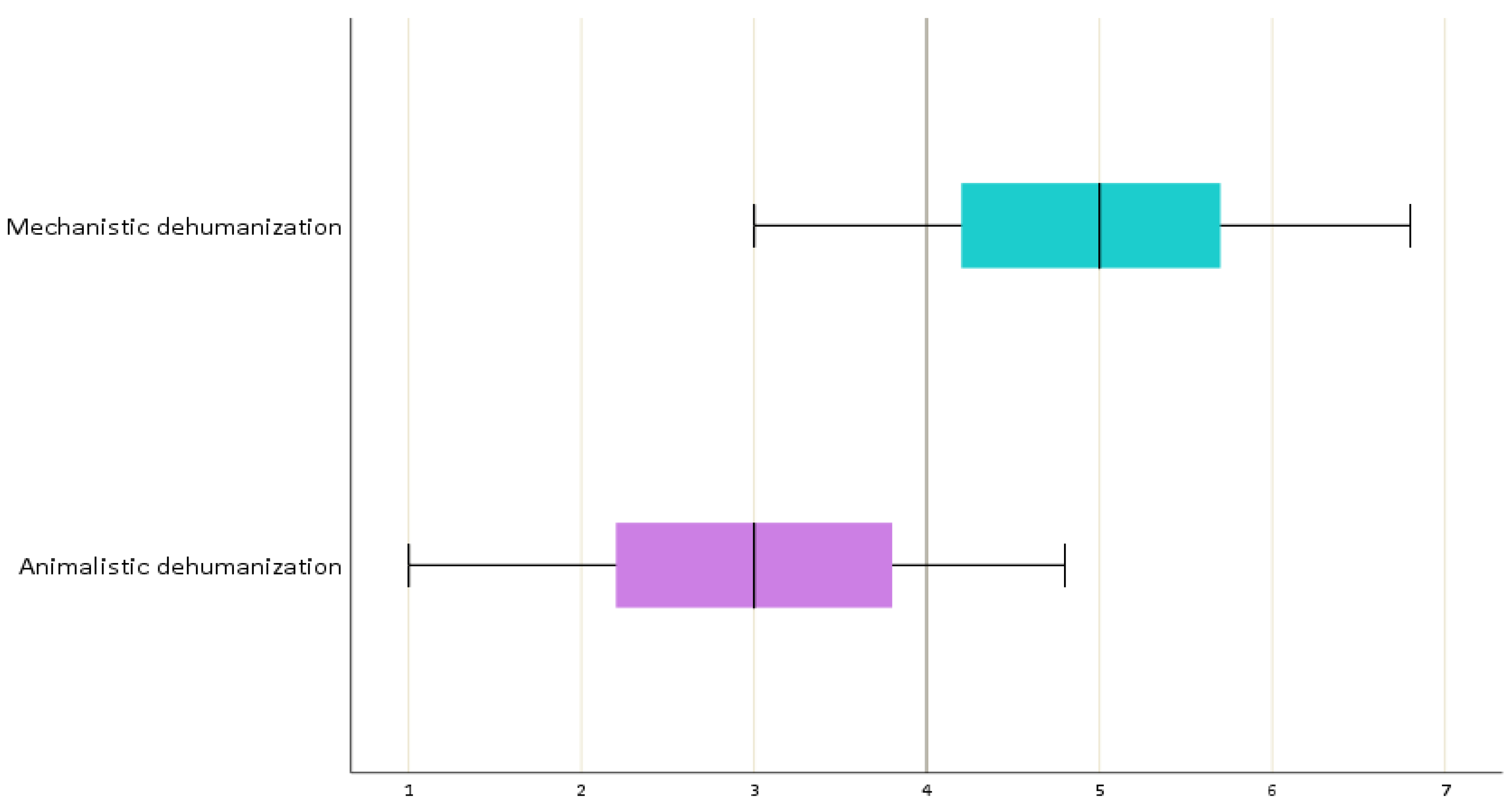
Figure 4.
Box plot showing the Mechanistic Self-dehumanization scale.
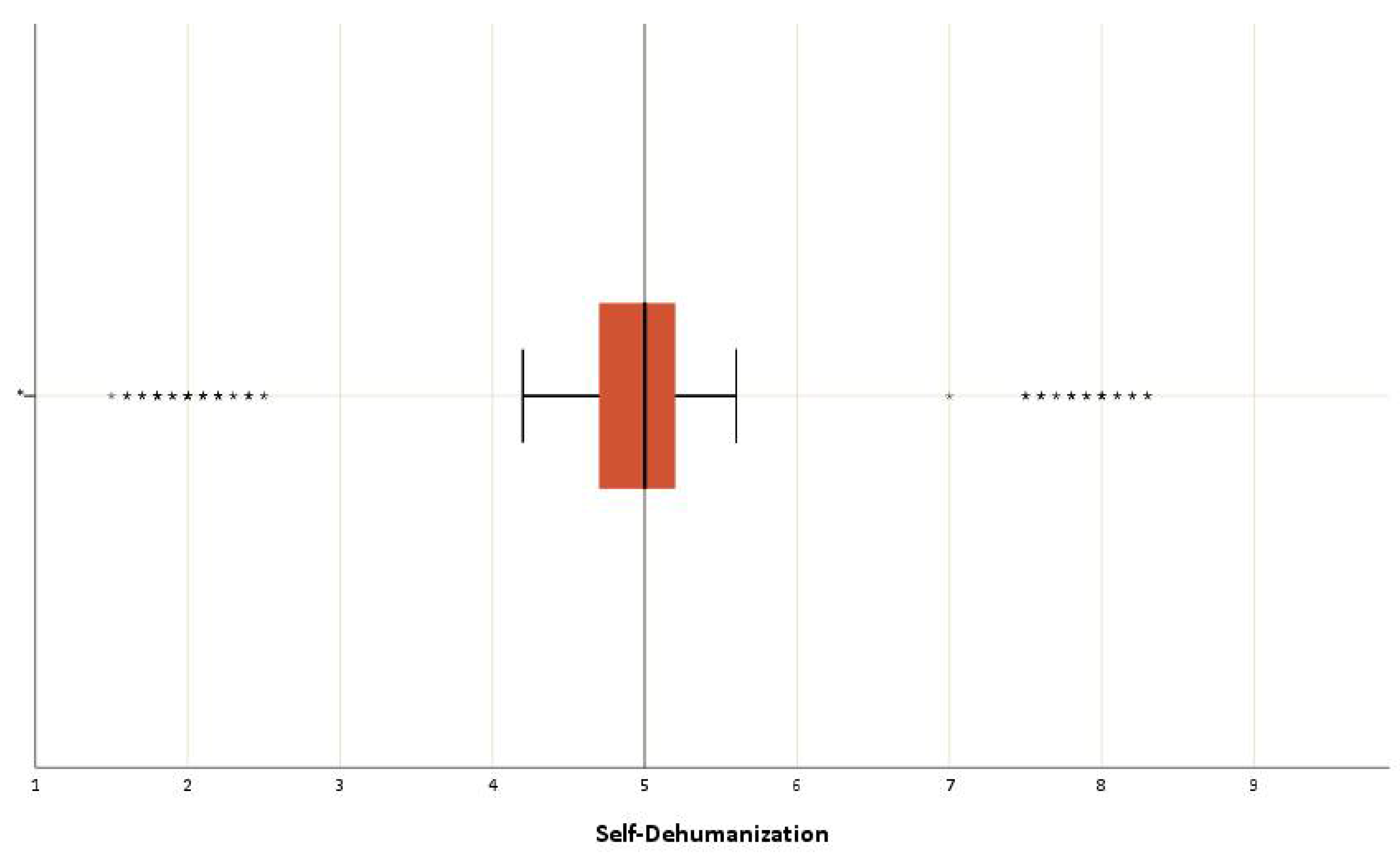
Table 1.
Characteristics of Sample.
| Mean (SD) | |||
| Age | 43.8 ± 10.5 | ||
| Working experience | 9.2 ± 8.8 | ||
| N | % | ||
| Biologicalsex | Male | 103 | 25.7% |
| Female | 297 | 74.3% | |
| Place of residence | Village | 55 | 13.8% |
| City<150,000 inhabitants | 127 | 31.8% | |
| City>150,000 inhabitants | 218 | 54.5% | |
| Marital status | Unmarried | 131 | 32.8% |
| Married | 237 | 59.3% | |
| Divorced | 29 | 7.3% | |
| Widower | 3 | 0.8% | |
| Profession | Nursing | 294 | 73.5% |
| Medicine | 106 | 26.5% | |
| Annualincome | ≤20.000 € | 343 | 85.8% |
| >20.000 € | 57 | 14.3% | |
| Post-graduatedegrees | MSc | 66 | 81.5% |
| PhD | 15 | 18.5% | |
| Labour Department | Open section | 195 | 48.7% |
| Closed section | 205 | 51.3% | |
| Workinghours | Circular timetable | 298 | 74.5% |
| Morning/afternoon schedule | 102 | 25.5% | |
| Have you attended any psychotherapy sessions? | Yes | 66 | 16.5% |
| No | 334 | 83.5% | |
a mean (standard deviation).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



