
Submitted:
26 April 2024
Posted:
28 April 2024
You are already at the latest version
Abstract
Multimedia resources, such as instructional videos, are currently enjoying a certain popularity in training programmes for medical and dental students. The major challenge is to create such resources that have quality content and are acceptable to students. We investigated the opinions of a sample of 551 students from 4 medical universities in Romania in order to identify the characteristics of the instructional videos that students prefer and we comparatively analysed these characteristics according to gender, age group, but also according to their general preferences for using Internet services. We used univariate (hypothesis testing) and multivariate (Two-Step Clustering) data analysis techniques and revealed three clusters of students, primarily determined by perceptions of the visual appearance of instructional videos. The structure of the clusters by gender and age group is relatively similar, but we recorded differences between them associated with students' expressed preferences for certain Internet services compared to others. Students who prefer instructional videos to contain images used only for aesthetic purposes, to fill in breaks, use Internet services mainly for communication, while students who prefer in videos the use of already drawn explanatory diagrams are slightly younger than the others and use Internet services mainly for information and communication.
Keywords:
instructional videos
; medicine students
; dental students
; e-learning
; data clustering
1. Introduction
Multimedia resources, such as instructional videos, have recently revolutionised the teaching style in undergraduate medical education, opening up a wide horizon of new and exciting opportunities. By enabling students to participate in immersive and dynamic learning sessions, this type of material allows them to understand complex concepts, develop real practical skills and thus acquire the knowledge needed to become good professionals. Their integration into academic medical curricula offers a multitude of advantages, bringing a clear added value to the teaching process, with certain benefits for students, who receive a new and useful tool to prepare for real medical practice [1]—with successful examples being reported in multiple fields [2,3,4,5,6]. Current technological progress allows teachers worldwide to create high-quality instructional videos at low cost and time investment [7]. Although relatively easy to produce from a technical point of view, teaching materials of this type are very complex in structure, including most forms of digital content—real footage, animations, simulations and interactive presentations; therefore, certain skills are required to produce them, which refer to the ability to organise and structure the material in a form that is as clear, coherent, correct and, at the same time, attractive to the target audience as possible. In the online environment today there is a real influx of medical instructional videos (a general Google search using the keywords “medical procedure” and video resources yielded no less than 303,000,000 results), but their quality and content are very varied, so it is often difficult for teachers to identify the most competent materials, to choose the best method of using them and the optimal teaching framework in which to implement them, and possibly to decide whether it is better to use pre-existing videos or to create original content [8].
In spite of these dilemmas, instructional videos are still today an indispensable practical tool for modern education, with an undisputed position among digital tools, promoting certain advantages and benefits, among which we can mention:
- Stimulating student interest and autonomous, flexible learning based on visual stimuli:
Well-crafted instructional videos enable the creation of visual representations for complex medical concepts, facilitating understanding of anatomical structures, physiological processes, surgical techniques and clinical manoeuvres. The visual learning provided by these materials promotes better understanding and retention of information. Dynamic images, animations and interactive elements capture students’ interest and hold their attention better; literature data show that students who view such materials are naturally stimulated to actively engage in discussions about them and retain information better over longer periods of time because they understand concepts and phenomena more deeply and completely [9,10].
Instructional videos are easy to distribute to students via educational websites, regardless of geographic location and time zone. They can be designed to be used in synchronous–interactive mode (live, broadcast live), but work equally well in asynchronous mode, which allows students to review material at their own pace and on their own schedule, according to their personal learning style [11].
A relevant example is again anatomy: there are studies showing that video tutorials aid in the recognition of structures during pre-dissection preparation, serve as a concise, sequential manual to assist during dissection manoeuvres, and subsequently serve as a useful resource for reviewing learned concepts [12,13].
- Realistic graphic simulations:
Instructional videos are one of the best suited tools to create realistic simulations of practical medical situations, allowing students to interact with virtual patients in interactive scenarios. They provide an immersive experience that facilitates the training of diagnostic skills, treatment planning and clinical decision-making in a safe and controlled environment. Embedded in augmented or virtual reality equipment, they have the potential to introduce innovative approaches to understanding complex medical concepts and offer numerous benefits, including the ease of repeating medical manoeuvres whenever needed, without harming patients in any way.
A wide range of simulators are currently available in medicine for training, ranging from static teaching videos and actors simulating human patients to full virtual reality (VR) systems. Static resources are widely used in surgical training programmes and are the primary platform for training basic practical skills. VR systems represent the next level of advanced skills training, using realistic computer-generated anatomical structures; in addition, they allow a shift from individual training to the cultivation of coordination and collaboration in a team of specialists who need to perform complex procedures [14,15]. Literature data have demonstrated the effectiveness of personalized practice on VR simulators, so it is becoming increasingly likely that simulation-based educational programs will be widely integrated into residency training [16]. Such an approach is justified by multiple considerations, primarily professional, but also social and legal [14], and can contribute significantly to mitigating the financial and ethical challenges associated with the use of conventional medical training methods (cadaver-based practice or advanced laboratory equipment [16].
- Access to advanced expert information:
Research studies show that video micro-lectures, delivered in real time or recorded in advance, are a successful pedagogical approach [8]. They are designed to complement traditional resources (textbooks, books, etc.) but diversify the range of study options, simplifying access to and dissemination of teaching materials and thus aligning with contemporary research [17]. This type of resource is of clear value as it promotes freedom of opinion and expression of health professionals, who can share their practical experience and knowledge in a fast and flexible way (through blog, videoblog or podcast tools), fully integrated into social media and easy to access by students and all interested people. As their quality improves, the use of such resources has the potential to revitalise medical education [18] as they provide students with in-depth, expert-level knowledge from professionals with extensive experience in the field. The main advantages of this type of teaching material, however, can also act as a hindrance because in the name of freedom of expression, material of questionable scientific value, biased, incomplete or even incorrect can just as easily be produced and promoted—and a censorship-type control of its real quality is almost impossible to implement [19,20].
- Procedural demonstrations:
As we have already pointed out, in the medical field the main role of instructional videos is to illustrate complex procedures in detail, such as surgical techniques, patient assessment or laboratory manoeuvres. This way of visual presentation is the clearest possible and ensures that students understand the steps correctly, preparing them for clinical practice in a safe and skilled way [20]. However, in order to ensure the appropriate quality of such resources, Chauvet et al. [21] recommend, as far as possible, their standardisation, regular updates and rapid accessibility through user-friendly platforms. There are also research groups that recommend the development of teaching videos based on CPA (cognitive process analysis) techniques, which provide students and residents with access to broader and deeper knowledge, allowing them to develop their analysis and clinical decision-making skills [22].
- Feedback and evaluation:
Feedback is an essential component in the educational process at any level, thus including undergraduate medical studies; its effectiveness, however, is determined by the nature, quantity and mode of its delivery. Teaching videos may contain sections of assisted feedback, which are of considerable effectiveness in training the clinical skills of novice students. Furthermore, instructional videos can be easily integrated into assessment systems, allowing students to perform directed tasks through them or to participate in virtual OSCE (Objective Structured Clinical Examination) sessions [23,24,25,26,27].
- Interdisciplinary learning:
It is anticipated that interdisciplinary assessment will be essential in the near future to deliver high quality care. However, universities currently face difficulties in implementing educational programmes that give students the opportunity to effectively participate in the interdisciplinary interactions inherent in some clinical practice situations. The reasons are objective and stem from the scientific complexity specific to such approaches, but also from logistical difficulties arising from the need to work with substantially larger numbers of students, with different specialisations and even from different faculties (e.g., in the case of interdisciplinary radiation oncology teams) [28]. A simple solution in this case is also represented by video resources [29], which can effectively illustrate interdisciplinary collaborations through real scenarios selected from practice, being the easiest way to convince students of the importance of teamwork and communication in medical practice.
It is therefore clear that instructional videos are one of the most effective learning tools, with multiple possibilities of use and indisputable benefits for both teachers and students. The major challenge, however, is to produce quality materials that are a real aid to the teaching process—not always a simple task, as it requires an investment of time and resources, but equally important, technical knowledge that university teachers do not have.
There is strong evidence in the literature that creating valuable teaching videos requires not only specialist knowledge of the subject area, but also a wide range of knowledge from other areas: IT, set design, directing, filming techniques or audio recording and processing [8]. The optimal solution is, in fact, for universities to employ professionals from these related fields to work with teachers and assist them in the production of video materials—but this obviously entails significant additional costs. In addition, studies have also shown that, apart from the technical aspects, quality teaching videos follow certain production rules that make them popular with students and enjoyable to watch, thus successfully achieving their intended purpose.
Our study aims to investigate for medical and dental students the validity of these rules that confer “popularity” to instructional videos, in correlation with basic demographic elements, but also with other characteristics, which refer to their general behaviour as users of digital technologies and in particular of Internet services—in order to substantiate the hypothesis that students who generally like digital resources position themselves differently from any teaching tool, compared to others. Therefore, for maximum effect, instructional videos should also be designed differently according to the type of students they are aimed at. This is an original approach, which we have not encountered in the literature, but which can prove very useful, as it allows the teacher to better understand the psychological profile of his/her students and their inner motivations, which determine whether or not they prefer the teaching tools proposed to them.
2. Materials and Methods
Participants: In order to obtain a representative sample, we invited in the study students at Medicine and Dental Medicine from all main Romanian Universities and all years of study. We recorded the opinions of 551 students at Dental Medicine or General Medicine, belonging to all years of study, from 4 main Universities in Romania (Iasi, Craiova, Timisoara, and Cluj-Napoca). The sample’s size was validated according to the calculation made for a finite population of 72167 Romanian students enrolled in 2022-2023, at Faculties of Health and Social Assistance, with a confidence level of 95%, and an accepted error of 5%—the study required a minimum of 383 participants.
Data collection: Students were asked to fill anonymously, online, a 15-items questionnaire in which they expressed their preferences for certain features that can be included in the instructional videos (Appendix A). The questionnaire also contained a supplementary question in which we proposed to the students four distinct categories of activities that can be carried out using Internet services (information, communication, entertainment and domestic facilities), and we asked them to rank these categories in order of preference (Appendix A). The questionnaire was presented and explained separately to each subject, along with the research goals.
Questionnaire: The questionnaire was adapted and developed starting from the models already existent in the scientific literature [30,31,32,33]. Its validity and reliability were assessed using several methods (expert opinion, item analysis, Kaiser–Meyer–Olkin coefficient, Bartlett test and factor analysis); on these bases, the questionnaire was considered suitable for being applied in our study.
Variables: The study’s variables were the students’ answers to the questionnaire, which were analysed comparatively by gender, age group and preferences for using particular Internet services.
Statistical analysis: The data from the questionnaire were recorded in a data file in SPSS 29.0 (SPSS Inc., Chicago, IL, USA) for Windows. The answers to each item were characterized through frequency distributions and contingency tables. The numerical variables were characterized through descriptive statistics (mean, standard deviation, range, and median). The comparisons between samples were performed using the Chi-squared test for categorical data. We considered the p ≤ 0.05 value as statistically significant (*) and the p ≤ 0.01 value statistically highly significant (**). In order to investigate the internal connections between the features of instructional videos, we used Two-Step Clustering; the number of clusters was calculated automatically, using the Schwarz’s Bayesian criterion (BIC) and a maximal limit of 15 clusters.
Ethical statement: Participation in our study was voluntary. The subjects were informed about the study and the content of the questionnaire, and they agreed with the informed consent. The questionnaires were filled anonymously in order to protect the subjects’ intimacy and to obtain objective answers as much as possible. The study was approved by the Ethical Committee of “Grigore T. Popa” University of Medicine and Pharmacy from Iasi, Romania.
3. Results
Three quarters of the students are female (76.2%); most of them are in years 1 and 2 of study (63.7%) and are aged between 18-20 years (53.9%), with a mean age of 21.78 ± 3.736 years; 90% of students have no previous higher education. The sample’s general features are presented in Table 1.
In general, there are not many significant differences between genders in terms of preferred features in instructional videos. However, it is observed that a higher proportion of boys prefer the narrator to be male (61.1%), while girls are almost equally divided between the two variants, although slightly more of them (51.4%) prefer the narrator to be female. Another statistically significant difference is noted in terms of the language in which the narrator speaks; the preferences are clearly towards Romanian. The majority of students want the text spoken by the narrator to be accompanied by headings at the bottom of the screen, but girls who expressed this preference (75.7%) are significantly more numerous than boys (64.9%). The majority of students want the spoken text to be accompanied by visuals highlighting important concepts (96.0%). In addition, 55.0% of boys prefer videos made as practical lessons, in which the teacher is recorded at the blackboard explaining and drawing, while 55.5% of girls prefer the instructional videos to be in the form of a PowerPoint presentation with pictures, diagrams and animated schemes. (Table 2).
There are not many significant differences of opinion between age groups either. Younger students, aged 18-20, prefer the narrator to be male in 57.6% of cases, while 57.6% of those aged 21-24 and 52.1% of those over 25 prefer the narrator to be female. In general, students prefer the narrator to speak slowly, in percentages that increase as they get older, from 62.0% of 18–20-year-olds to 77.8% of 21–24-year-olds and 72.9% of over 25-year-olds. The last element for which statistically significant differences between the 3 age groups were also reported is the place of the explanatory texts accompanying the schemes and drawings presented. The vast majority of students prefer to place them directly on the drawing, in the area to which they refer; young students in particular, aged 18-20, express this preference (81.1%), and their percentage decreases as they get older: 79.7% of students aged 21-24 and 64.6% of those over 25. Otherwise, no other statistically significant differences were noted (Table 3).
However, the objective of our study was to refine the results obtained by analysing the basic demographic characteristics of the group, through a more nuanced analysis of their preferences for the four general categories of Internet services—as this would provide useful information for the optimised design of instructional videos, better adapted to the target audience.
We will detail the results obtained in this respect below.
Students who use Internet services primarily for information differ statistically significantly from the others in that more of them (48.9%) prefer instructional videos in which the teacher is recorded at the blackboard explaining and drawing. Other preferences that slightly, if not statistically significantly, stand out are: the narrator to be female (50.0%), possibly speaking in English (23.9%) and even at high speed (33.3%); it is better if the video does not contain images used only for aesthetic purposes, to fill in the breaks (52.2%) and can be without titling at the bottom of the screen (30.6%). It is also found that, of the students who rank information as their 2nd preferred Internet service, a significantly higher percentage (16.4%) accept that the text spoken by the narrator is not accompanied by animated explanatory schemes (Table 4).
Students who use the Internet mainly for communication are also those who prefer the narrator to speak in Romanian (86.2%). No other statistically significant differences were observed. Other preferences that highlight this category of students are that the narrator should still be female (50.3%), that the narrator should speak in a conversational and friendly style (70.4%), and that the film should not contain background music (73.1%); explanatory texts will be placed directly on the drawing, in the area to which it refers (79.9%) and already drawn schemes are accepted, which will only be explained in the video (32.6%). It is also accepted that the video should present the subject matter heterogeneously, in the form of free exposition (12.0%), but PowerPoint presentations with pictures, diagrams and animated schemes are preferred (56.6%). In addition, a significant percentage of students in this category opt for videos with a maximum length of 6 minutes (25.1%) (Table 5).
Students who use Internet services primarily for entertainment stand out statistically significantly from the other categories in that they prefer spoken text to be accompanied by titling at the bottom of the screen (78.1%) and animated graphics to explain it more clearly (90.2%), and the video to present the subject in a structured way that gradually moves from simple to complex (87.4%). A higher percentage of students in this category accept that the narrator speaks in English (21. 3%), but still maintain a low speaking speed (68.9%), and the film may contain background music (32.2%). Explanatory texts should be placed directly on the drawing, in the area to which they refer (82.0%). Students who rank entertainment last in their preferences stand out significantly from others in that they prefer to use already drawn explanatory schemes and diagrams, which will only be explained in the film (52.9%)—Table 6.
Students who use Internet services for domestic facilities are not statistically significantly different from others in terms of their preferences for how to make instructional videos. It can be noted, however, that in this category the highest percentages of students were found to accept that the narrator speaks in English (25.7%) but at a slow speed (74.3%) and that the film contains background music (34.3%) and images used only for aesthetic purposes, to fill the breaks (51.4%), and that explanatory texts are placed at the bottom of the screen (28.6%) and diagrams and schemes are already drawn and only explained in the film (42.9%) A high percentage of students in this category also indicate that they prefer educational films with a length of 6 minutes or less (37.1%). In addition, students concerned with domestic facilities services, which are ranked second in the top preferences, prefer significantly more than the other categories that the narrator in instructional videos be female (61.8%)—Table 7.
The classification of the 15 items on the characteristics of the instructional videos preferred by the students led to the identification of 3 clusters of approximately equal size (Figure 1). The most important predictor among the 15 proposed was item FD7: Visually appealing—images used only for aesthetic purposes vs. their absence (predictor importance PI = 1.00), followed by item FD10: Explanatory schemes and diagrams already drawn vs. drawn simultaneously with explanations (PI = 0.85) and item FD5: Narrator’s conversational, friendly vs. formal, didactic style of expression (PI = 0.54)—Figure 2.
The classification of students according to the agreed characteristics of instructional videos is therefore determined by the perception of their visual appearance. The first cluster identified (35.4% of the cases) contains students who, in their vast majority, prefer instructional videos to contain images used only for aesthetic purposes, to fill the breaks (90.3%). These students also agree that the narrator’s voice is female (59.5%), the narrator speaks in Romanian (94.4%), with a low speed (79.5%). All students in this cluster want the narrator’s spoken text to be accompanied by animated diagrams to explain it more clearly and by graphics to highlight important concepts, and for the subject to be presented in a structured way, explaining simple concepts first and then complex ones (96.9%).
The second cluster also includes a third of students (34.8%), but the vast majority of them (88.0%) are not interested in instructional videos containing images used only for aesthetic purposes, to fill in the gaps, but want explanatory schemes and diagrams to be drawn at the same time as explanations (94.8%). Other specific preferences for students in this category are for the narrator’s voice to be male (65.6%), spoken text to be accompanied by titling at the bottom of the screen (86.5%) and explanatory text for diagrams and drawings to be displayed directly on them in the area to which they refer (89. 6%). The video should be designed as a practical lesson, with the teacher recorded at the blackboard explaining and drawing (65.1%), and should be as long as necessary, not requiring the 6-minute rule (93.8%).
The last cluster groups 29.8% of students, who are also not interested in instructional videos containing images used only for aesthetic purposes, to fill in the breaks (65.9%), but agree that the explanatory schemes and diagrams are already drawn and only explained in the film (76.2%). Slightly more than half of the students in this category (52.4%) agree that the narrator should speak at a high speed, compared to no more than 1/4 of the students in the other clusters, who usually prefer the narrator to speak at a low speed. In addition, the vast majority of students in this cluster do not consider it necessary for teaching films to contain background music (80.5%). Nearly 1/3 of them agree that films should also be made as free-form presentations (30.5%) and the vast majority (81.7%) want them to be designed as PowerPoint presentations with animated pictures, diagrams and schemes (Table 8).
We also characterized the identified clusters according to the criteria we proposed in the other sections of the study: gender, age group and general preferences of students among the 4 categories of Internet services we defined; the results are presented in Table 9.
Overall, no statistically significant differences were identified. The 3 clusters have similar structures by genders and age groups, although it can still be observed that the third cluster comprises slightly more young students, aged 18-20 (59.1%), and the first 2 clusters comprise more students aged 21-24. Students’ preferences for the 4 categories of Internet services tracked do not differ statistically significantly between the clusters separating them according to the preferred characteristics of the educational videos. The highest proportion of students using Internet services for information is found in the third cluster (77.5%), and the highest proportion of students using Internet services for communication is also found in the third cluster (91.4%), but also in the first cluster (90.8%). Students using the Internet mainly for entertainment are relatively evenly spread across the 3 clusters, and those using Internet services for domestic facilities are clustered slightly more frequently in the third cluster—Table 9.
4. Discussions
The literature provides a wealth of data demonstrating the effectiveness of instructional videos in education in general and in university medical education in particular.
Leela et al. [25] conducted a cross-sectional study of 324 third- and fourth-year medical and dental students in a private university; students were interviewed about their preferences for teaching methods. It was thus found that the teaching tool most preferred by the students was instructional videos (75.1%), followed by question-and-answer oriented learning (70.0%), problem-oriented learning (69.6%), interactive discussions (69.3%), case studies (67.2%) and traditional lectures (66.0%) and PowerPoint presentations (65.9%). Dental students rank video content first in order of preference, followed by PowerPoint presentations and traditional lectures, while medical students prefer interactive discussions, followed by quizzes and debates. The research group therefore shows that there is a need to move away from the traditional teaching style to a combination of alternative methods, including video resources, problem-based learning (PBL) and interactive discussions, which motivate students much better and are thus significantly more effective.
Ortega et al. [17] developed in 2017 the first textbook combined with interactive video content, dedicated to postgraduate medical training, and investigated its effectiveness through a questionnaire proposed to residents who used it. The results of the survey conducted again indicate the preference of medical residents for learning environments that integrate technology, combining traditional textbooks with interactive multimedia elements. Miranda et al. [34] produced narrative videos to illustrate neurosurgical manoeuvres, which they integrated into a telehealth system used for distance training of students during the COVID-19 pandemic; all students monitored used these resources to learn, and the vast majority found them extremely useful for understanding the concepts presented. Doherty et al. [9] assessed the correlation between students’ level of engagement in using lecture-style instructional videos and various characteristics of the videos. The videos tested presented topics in anatomy, physiology and clinical assessment, and student engagement was quantified by the amount of viewing time they allocated. It was thus found that the most viewed videos were those divided into relatively short segments, without subtitles and highlighting important information through different graphic elements. The students also perceived positively the appearance in the video, at regular intervals, of a human instructor to provide explanations. When a lesson consists of several videos, the research group recommends that the most important concepts are discussed first in the sequence.
Chauvet et al. [21] have also studied the characteristics of effective instructional videos, in the particular case of describing surgical manoeuvres. They too showed that the duration of the videos should be relatively short, 10 to 15 minutes, while also highlighting a number of specific elements: it is recommended that the videos provide details about the patient’s preparation for the procedure (e.g., his or her body mass index, degree of Trendelenburg position or pneumoperitoneum pressure), that they be organised in distinct stages and that they be uploaded to both educational and open platforms, where they remain fully accessible to those interested. It is further recommended that the videos show not only the correct manoeuvres, but also the mistakes that can be made (such as ‘so no’), as this approach is particularly appreciated by young surgeons.
Our data also confirms that students are very positive about the instructional videos. As regards the recommended features for the design of the videos, in some cases we recorded different opinions. Thus, three quarters of students (74.6%) do not particularly prefer shorter videos, with no significant differences between genders or age groups. Three quarters of students (73.1%) also prefer videos with subtitles—mostly girls, regardless of age. Almost all students (95.5%) want videos to contain graphics to highlight important concepts, and opinions are almost evenly divided on the presence of the human instructor: 47.0% of students like videos designed as lectures, where the teacher is filmed at the blackboard, while 53.0% like videos designed as PowerPoint presentations, with pictures and diagrams.
Other, more general, issues related to the effectiveness of teaching medical videos as part of more complex tools were also investigated.
Thus, Palter and Grantcharov [35] investigated whether one-on-one practice on virtual reality (VR) simulators that include video sequences leads to improved surgical skills. They demonstrated that resident physicians who trained on VR simulators developed superior skills compared to those who did not use such systems, even though their initial skill level was similar.
Melkers et al. [18] were concerned with the effectiveness of video microlectures in dentistry. They analysed 89 blogs and podcasts designed to provide professional content in various dental fields. 55% of their authors were practising dentists or hygienists, 30% were consultants, 9% were editors and moderators of discussion forums, and the rest were representatives of various professional organisations or corporations. The study authors thus highlighted the involvement of dentists and practicing hygienists in using social media platforms to disseminate valuable clinical information to dental colleagues and dental students. Lin et al. [19] and Paterson et al. [20], respectively, studied the quality benchmarks of video materials disseminated in medical educational blogs and podcasts to quantify the credibility and validity of this type of resource as a viable tool for medical education. A short list of quality indicators, significant for assessing credibility and relevance, has thus been highlighted: clear indication of authors and their expertise in the field, bibliographical references and possible conflicts of interest; explicit differentiation between personal opinions and factual statements, and respectively between the content itself and advertising material; delivery of accurate and professional information, consistent with the bibliographical references used and relevant to the intended audience; technical compatibility of the material with standard equipment, ensuring quick, easy and smooth access.
Matthan et al. [23] explored the side effects of video feedback, namely the potential anxiety induced in students when they perform simulated practical procedures. Two groups of students were comparatively analysed: one group that received supervised individualized video feedback (SIVF), and the other group that received general, unsupervised video feedback (GUVF). The majority of subjects reported that neither type of feedback induced significant stress for them, although they preferred individualized feedback (SIVF).
Rammell et al. [27] investigated the extent to which students retained practiced practical skills over a 7-week follow-up period after receiving either synchronous video feedback from experts or unsupervised asynchronous video feedback. Students who received synchronous video feedback from experts demonstrated significant improvement in practiced skills throughout the study period, whereas no significant change was observed in the others. Seifert et al. [24] also compared the effectiveness of individualized, but unsupervised, video feedback with conventional, direct, expert feedback in learning practical oral and maxillofacial surgery skills. The research group concluded that while direct feedback from experts is the most effective method, other feedback options are also viable alternatives. On the other hand, Phillips et al. [26] do not report significant additional benefits of direct expert feedback, similar results can be obtained using general videos made by experts, based on which students self-assess their performance. We did not include this issue in our study, but it is exciting and may be a direction for further research.
Nisbet et al. [29,36] and Jorm et al. [28] addressed the issue of interdisciplinary learning strategies using video tools. The research group initiated an experiment in which students with different medical specialties were grouped into interdisciplinary teams and asked to produce a treatment plan for a proposed clinical scenario; the treatment plan was to be presented in the form of a 5-minute video and a one-page written summary, after which the student teams were asked to peer review 3 other videos made by other teams participating in the experiment, based on predefined criteria: the correctness of the proposed treatment plan, the quality of the interdisciplinary collaboration, and the effectiveness of the video tools used to capture the audience’s attention. It was shown that the tasks proposed to the students, to present the treatment plan in the form of a video and to evaluate the work of their peers, stimulated their creativity and led to effective collaboration between them, thus being effective as interdisciplinary learning strategies. Feedback from participating students was also positive: 70.0% of them found the proposed tasks useful and 87.0% appreciated the relevance of their case study. The students also appreciated the contributions of their teammates and the importance of collaboration between them for the correct analysis of the clinical case and found the requirement to present their work in the form of a video innovative and stimulating.
5. Conclusions
Our study confirms the data in the literature, according to which students highly approve the instructional videos, although in some cases we recorded different opinions regarding the recommended characteristics for designing this type of material.
The new approach we have proposed, however, is to investigate more deeply the reasons that make students prefer or not certain features of instructional videos, which are related to their personal preferences and possibly to their developmental background. We started from the idea that technically savvy students, who are attracted to gadgets, computers and the internet, will also be more open to all modern learning technologies and, in particular, to instructional videos, and we indeed found significant results and definite associations between these elements, as already described.
Another novel approach was to classify students according to the features they preferred in the instructional videos by automatic clustering using the Two-Step Clustering procedure. We chose this method of data analysis because in this way we were not only able to identify relevant clusters among students, but also the most important predictors responsible for their creation; the predictors found are interesting to analyse because they are not similar to the items initially reported as most popular.
This approach is original, as the literature consulted indicates that it has not been used before in studies of students’ views on different features of the teaching process. Most studies of this type simply record student responses and compare them according to different criteria, without investigating the structure of the items. The analysis of the items using classification techniques, such as the one we have chosen, is instead a more accurate method of study, which allows their prioritisation and the grouping of students according to the identified hierarchies. In this way we can better understand the intimate reasons why students do or do not prefer a teaching tool and, consequently, we can make an informed selection of the optimal methods to make it effective. The results obtained are suggestive and paint a different, more complex picture in our opinion, of both the digital teaching tools that can work in higher medical education and the typology of students who will enjoy using such tools and be able to make the most of their benefits.
Author Contributions
Conceptualization, Cristina Gena Dascalu; Data curation, Claudiu Topoliceanu and Magda Ecaterina Antohe; Formal analysis, Cristina Gena Dascalu, Claudiu Topoliceanu and Magda Ecaterina Antohe; Investigation, Cristina Gena Dascalu; Methodology, Magda Ecaterina Antohe; Resources, Claudiu Topoliceanu; Writing—original draft, Cristina Gena Dascalu; Writing—review & editing, Cristina Gena Dascalu and Magda Ecaterina Antohe.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethical Committee of “Grigore T. Popa” University of Medicine and Pharmacy from Iasi, Romania (decision no. 21/16.11.2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical and privacy restrictions.
Acknowledgments
The authors want to address their special thanks to Georgeta Zegan, “Grigore T.Popa” UMPh Iasi, Diana Lungeanu, “Victor Babes” UMPh Timisoara and Sorana Bolboacă, “Iuliu Hatieganu” UMPh Cluj-Napoca, who disseminate this study among their students and invited them to participate at the survey.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
THE QUESTIONNAIRE’S STRUCTURE:
Please check the features you prefer to find at the instructional videos used for preparation at the specialty objects:
| Option 1: | Option 2: | ||
| FD1: The narrator’s voice is: | ☐ Human | ☐ Computer generated | |
| FD2: The narrator’s gender is: | ☐ Male | ☐ Female | |
| FD3: Narrator speaks in: | ☐ English | ☐ Romanian | |
| FD4: The speed at which the narrator speaks is: | ☐ High | ☐ Low | |
| FD5: Narrator’s speaking style is: | ☐ Conversational, friendly | ☐ Formal, didactic | |
| FD6: Soundtrack of the video: | ☐ It has background music | ☐ It doesn’t have background music | |
| FD7: Visually appealing: | ☐ The video contains images for aesthetic purposes only, to fill in the gaps | ☐ The video fails to contain images used only for aesthetic purposes, to fill in the gaps | |
| FD8: The narrator’s spoken text is: | ☐ Accompanied by written text (subtitle) at the bottom of the screen | ☐ Without written text (subtitle) at the bottom of the screen | |
| FD9: Explanatory text accompanying the diagrams and drawings are placed: | ☐ At the bottom of the screen | ☐ Directly on the drawing, in the area they refer to | |
| FD10: Explanatory diagrams and charts: | ☐ They are already drawn in the videos they are only explained | ☐ They are drawn simultaneously with the explanations | |
| FD11: Narrator’s spoken text is: | ☐ Accompanied by animated diagrams to explain it better | ☐ Without animated diagrams | |
| FD12: Narrator’s spoken text is: | ☐ Accompanied by graphic, visual elements to mark the important notions | ☐ Without graphic, visual elements to mark important notions | |
| FD13: The instructional video presents the suggested topic: | ☐ Structured, explaining first the simple and then complex notions | ☐ Heterogenous, as free speech | |
| FD14: The instructional film is designed as: | ☐ Regular class—the teacher is recorded at the blackboard, where he explains and draws | ☐ PowerPoint presentation with images, diagrams and animated drawings | |
| FD15: The instructional video has a total length of: | ☐ Maximum 6 minutes | ☐ Its length is not important | |
| The main activities for which I use Internet are (order them from 1 to 4, according to their importance—1 = the less important; 4 = the most important): | |||
| ☐ | Information | ||
| ☐ | Communication (e-mail, instant messaging, chatting with friends, dating) | ||
| ☐ | Entertainment (e-books, music, movies, games) | ||
| ☐ | Domestic facilities (shopping online, bills payment, job offers, services offers) | ||
References
- Berrocal, Y.; Regan, J.; Fisher, J.; Darr, A.; Hammersmith, L.; Aiyer, M. Implementing Rubric-Based Peer Review for Video Microlecture Design in Health Professions Education. Med Sci Educ 2021, 31(6), pp.1761-1765. [CrossRef]
- Kwan, K.; Wu, C.; Duffy, D.; Masterson, J.; Blair, G.K. (). Lights, camera, surgery: a novel pilot project to engage medical students in the development of pediatric surgical learning resources. J Pediatr Surg. 2011, 46(5), pp. 962–965. [CrossRef]
- Omar, H.; Khan, S.A.; Toh, C.G. Structured student-generated videos for first-year students at a dental school in Malaysia. J Dent Educ. 2013, 77(5), pp.640–647.
- Pereira, J.; Echeazarra, L.; Sanz-Santamaría, S.; Gutiérrez, J. Student-generated online videos to develop cross-curricular and curricular competencies in nursing studies. Comput Hum Behav. 2014, 31, pp.580–90. [CrossRef]
- Shuldman, M.; Tajik, M. The role of media/video production in non-media disciplines: the case of health promotion. Learning, Media and Technology 2010, 35(3), pp.357–62. [CrossRef]
- Haines, S.L.; Van Amburgh, J.A. A Vidcasting project to promote the pharmacist’s role in public health. Am J Pharm Educ. 2010, 74(6), 97. [CrossRef]
- Krumm, I.R.; Miles, M.C.; Clay, A.; Carlos, I.W.G.; Adamson, R. Making Effective Educational Videos for Clinical Teaching. Chest 2022, 161(3), pp.764-772. [CrossRef]
- Dong, C.; Goh, P.S. Twelve tips for the effective use of videos in medical education. Med Teach 2015, 37(2), pp.140-145. [CrossRef]
- Doherty, C. Using web log analysis to evaluate healthcare students’ engagement behaviours with multimedia lectures on YouTube. PLoS One 2023, 18(4), e0284133. [CrossRef]
- Rose, E.; Claudius, I.; Tabatabai, R.; Kearl, L.; Behar, S.; Jhun, P. The Flipped Classroom in Emergency Medicine Using Online Videos with Interpolated Questions. J Emerg Med. 2016, 51(3), pp.284-291. [CrossRef]
- Young, T.P.; Bailey, C.J.; Guptill, M.; Thorp, A.W.; Thomas, T.L. The flipped classroom: a modality for mixed asynchronous and synchronous learning in a residency program. West J Emerg Med. 2014, 15(7), pp.938-44. [CrossRef]
- Estai, M.; Bunt, S. Best teaching practices in anatomy education: A critical review. Ann Anat 2016, 208, pp.151-157. [CrossRef]
- Larkin, M.B.; Graves, E.; Rees, R.; Mears, D. A Multimedia Dissection Module for Scalp, Meninges, and Dural Partitions. MedEdPORTAL 2018, 22(14), 10695. [CrossRef]
- Rehrig, S.T.; Powers, K.; Jones, D.B. Integrating simulation in surgery as a teaching tool and credentialing standard. J Gastrointest Surg. 2008, 12(2), pp.222-33. [CrossRef]
- Beyer-Berjot, L.; Aggarwal, R. Toward technology-supported surgical training: the potential of virtual simulators in laparoscopic surgery. Scand J Surg 2013, 102(4), pp.221-226. [CrossRef]
- Barteit, S.; Lanfermann, L.; Bärnighausen, T.; Neuhann, F.; Beiersmann, C. Augmented, Mixed, and Virtual Reality-Based Head-Mounted Devices for Medical Education: Systematic Review. JMIR Serious Games 2021, 9(3), e29080. [CrossRef]
- Ortega, R.; Akhtar-Khavari, V.; Barash, P.; Sharar, S.; Stock, M.C. An innovative textbook: design and implementation. Clin Teach. 2017, 14(6), pp.407-411. [CrossRef]
- Melkers, J.; Hicks, D.; Rosenblum, S.; Isett, K.R.; Elliott, J. Dental Blogs, Podcasts, and Associated Social Media: Descriptive Mapping and Analysis. J Med Internet Res. 2017, 19(7), e269. [CrossRef]
- Lin, M.; Thoma, B.; Trueger, N.S.; Ankel, F.; Sherbino, J.; Chan, T. Quality indicators for blogs and podcasts used in medical education: modified Delphi consensus recommendations by an international cohort of health professions educators. Postgrad Med J. 2015, 91(1080), pp.546-50. [CrossRef]
- Paterson, Q.S.; Thoma, B.; Milne, W.K.; Lin, M.; Chan, T.M. A Systematic Review and Qualitative Analysis to Determine Quality Indicators forHealth Professions Education Blogs and Podcasts. J Grad Med Educ. 2015, 7(4), pp.549-54. [CrossRef]
- Chauvet, P.; Botchorishvili, R.; Curinier, S.; Gremeau, A.S.; Campagne-Loiseau, S.; Houlle, C.; Canis, M.; Rabischong, B.; Bourdel, N. What Is a Good Teaching Video? Results of an Online International Survey. J Minim Invasive Gynecol 2020, 27(3), pp.738-747. [CrossRef]
- Yeung, C.; McMillan, C.; Saun, T.J.; Sun, K.; D’hondt, V.; von Schroeder, H.P.; Martou, G.; Lee, M.; Liao, E.; Binhammer, P. Developing Cognitive Task Analysis-based Educational Videos for Basic Surgical Skills in Plastic Surgery. J Surg Educ. 2017, 74(5), pp.889-897. [CrossRef]
- Matthan, J.; Gray, M.; Nesbitt, C.I.; Bookless, L.; Stansby, G.; Phillips, A. Perceived Anxiety is Negligible in Medical Students Receiving Video Feedback During Simulated Core Practical Skills Teaching: A Randomized Trial Comparing Two Feedback Modalities. Cureus 2020, 12(3), e7486. [CrossRef]
- Seifert, L.B.; Herrera-Vizcaino, C.; Herguth, P.; Sterz, J.; Sader, R. Comparison of different feedback modalities for the training of procedural skills in Oral and maxillofacial surgery: a blinded, randomized and controlled study. BMC Med Educ. 2020, 20(1), p.330. [CrossRef]
- Leela, A.; Latt, S.S.; Afrose, T.; Kynn, I. Preferred Teaching Methods by Medical and Dental Students of a Private University: The Students’ Perception. IJIRMPS 2018, 6(5), pp.106-111. [CrossRef]
- Phillips, A.W.; Matthan, J.; Bookless, L.R.; Whitehead, I.J.; Madhavan, A.; Rodham, P.; Porter, A.L.R.; Nesbitt, C.I.; Stansby, G. Individualised Expert Feedback is Not Essential for Improving Basic Clinical Skills Performance in Novice Learners: A Randomized Trial. J Surg Educ. 2017, 74(4), pp.612-620. [CrossRef]
- Rammell, J.; Matthan, J.; Gray, M.; Bookless, L.R.; Nesbitt, C.I.; Rodham, P.; Moss, J.; Stansby, G.; Phillips, A.W. Asynchronous Unsupervised Video-Enhanced Feedback as Effective as Direct Expert Feedback in the Long-Term Retention of Practical Clinical Skills: Randomised Trial Comparing 2 Feedback Methods in a Cohort of Novice Medical Students. J Surg Educ. 2018, 75(6), pp.1463-1470. [CrossRef]
- Jorm, C.; Nisbet, G.; Roberts, C.; Gordon, C.; Gentilcore, S.; Chen, T.F. Using complexity theory to develop a student-directed interprofessional learning activity for 1220 healthcare students. BMC Med Educ 2016, 16, p.99. [CrossRef]
- Nisbet, G.; Jorm, C.; Roberts, C.; Gordon, C.J.; Chen, T.F. Content validation of an interprofessional learning video peer assessment tool. BMC Medical Education 2017, 17, 258. [CrossRef]
- Alshawish, E.; El-Banna, M.M.; Alrimawi, I. Comparison of blended versus traditional classrooms among undergraduate nursing students: A quasi-experimental study. Nurse Education Today 2021, 106, 105049. [CrossRef]
- Yu-Fong Chang, J.; Wang, L.H.; Lin, T.C.; Cheng, F.C.; Chiang, C.P. Comparison of learning effectiveness between physical classroom and online learning for dental education during the COVID-19 pandemic. Journal of Dental Sciences 2021, 16, 1281-1289. [CrossRef]
- Sezer, B. Faculty of medicine students’ attitudes towards electronic learning and their opinion for an example of distance learning application. Computers in Human Behavior 2016, 55, 932-939. [CrossRef]
- Ibrahim, N.K.; Al Raddadi, R.; Al Darmasi, M.; Al Ghamdi, A.; Gaddoury, M.; Al Bar, H.M.; Ramadan, I.K. Medical students’ acceptance and perceptions of e-learning during the Covid-19 closure time in King Abdulaziz University, Jeddah. Journal of Infection and Public Health 2021, 14, 17-23. [CrossRef]
- Miranda, S.P.; Glauser, G.; Wathen, C.; Blue, R.; Dimentberg, R.; Welch, W.C.; Grady, M.S.; Schuster, J.M.; Malhotra, N.R. Letter to the Editor “Incorporating Telehealth to Improve Neurosurgical Training During the COVID-19 Pandemic”. World Neurosurgery 2020, 139, pp.728-731. [CrossRef]
- Palter, V.N.; Grantcharov, T.P. Individualized deliberate practice on a virtual reality simulator improves technical performance of surgical novices in the operating room: a randomized controlled trial. Ann Surg. 2014, 259(3), pp.443-448. [CrossRef]
- Nisbet, G.; Gordon, C.; Jorm, C.; Chen, T. Influencing student attitudes through a student-directed interprofessional learning activity: a pilot study. Int. J.Pract.-Based Learn. Health Soc. Care 2016, 4(1), pp.1–15. [CrossRef]
Figure 1.
The sizes of the clusters identified among the preferred features of didactic videos.
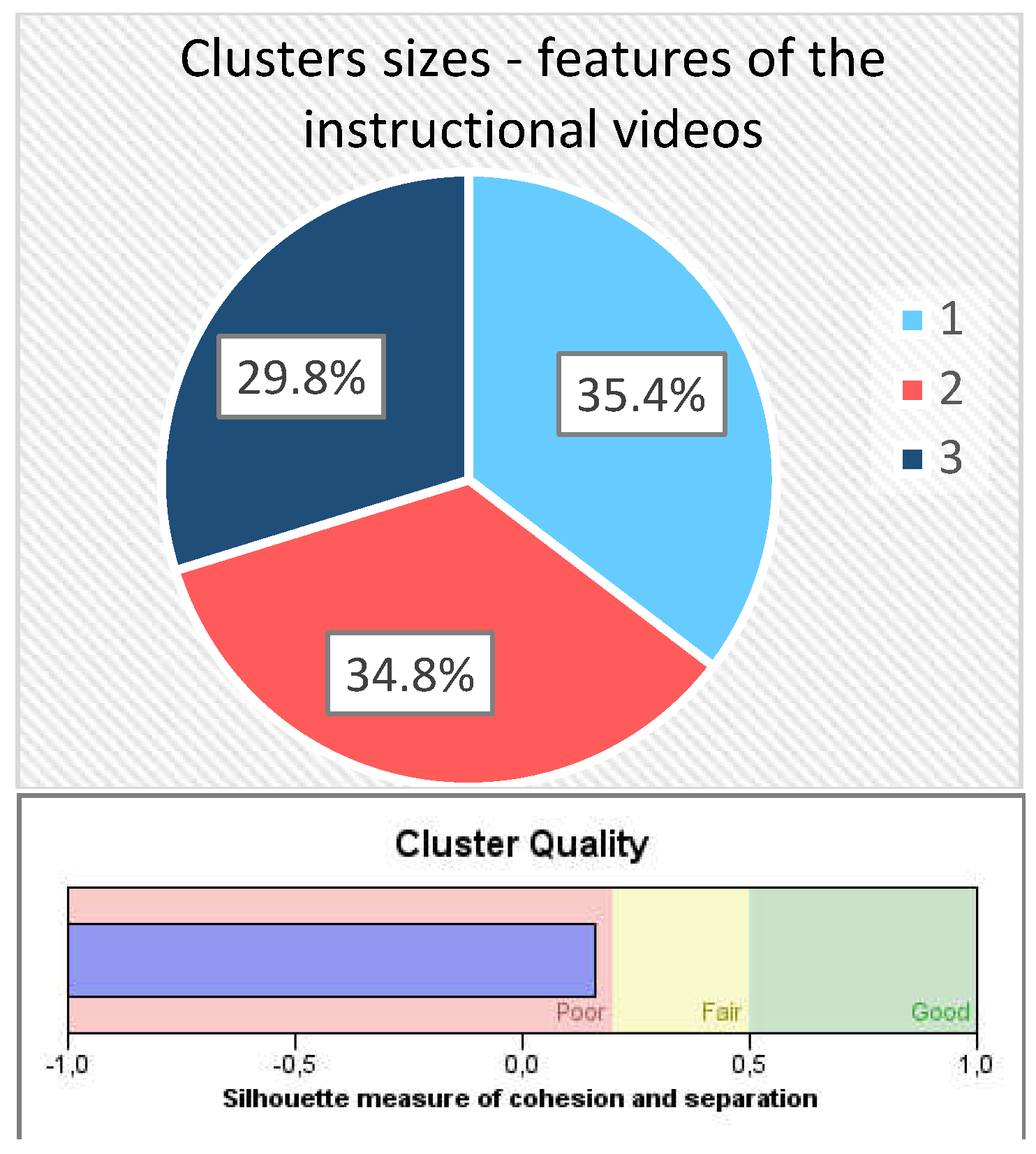
Figure 2.
The 15 features classification according to their PI coefficients (predictor importance).
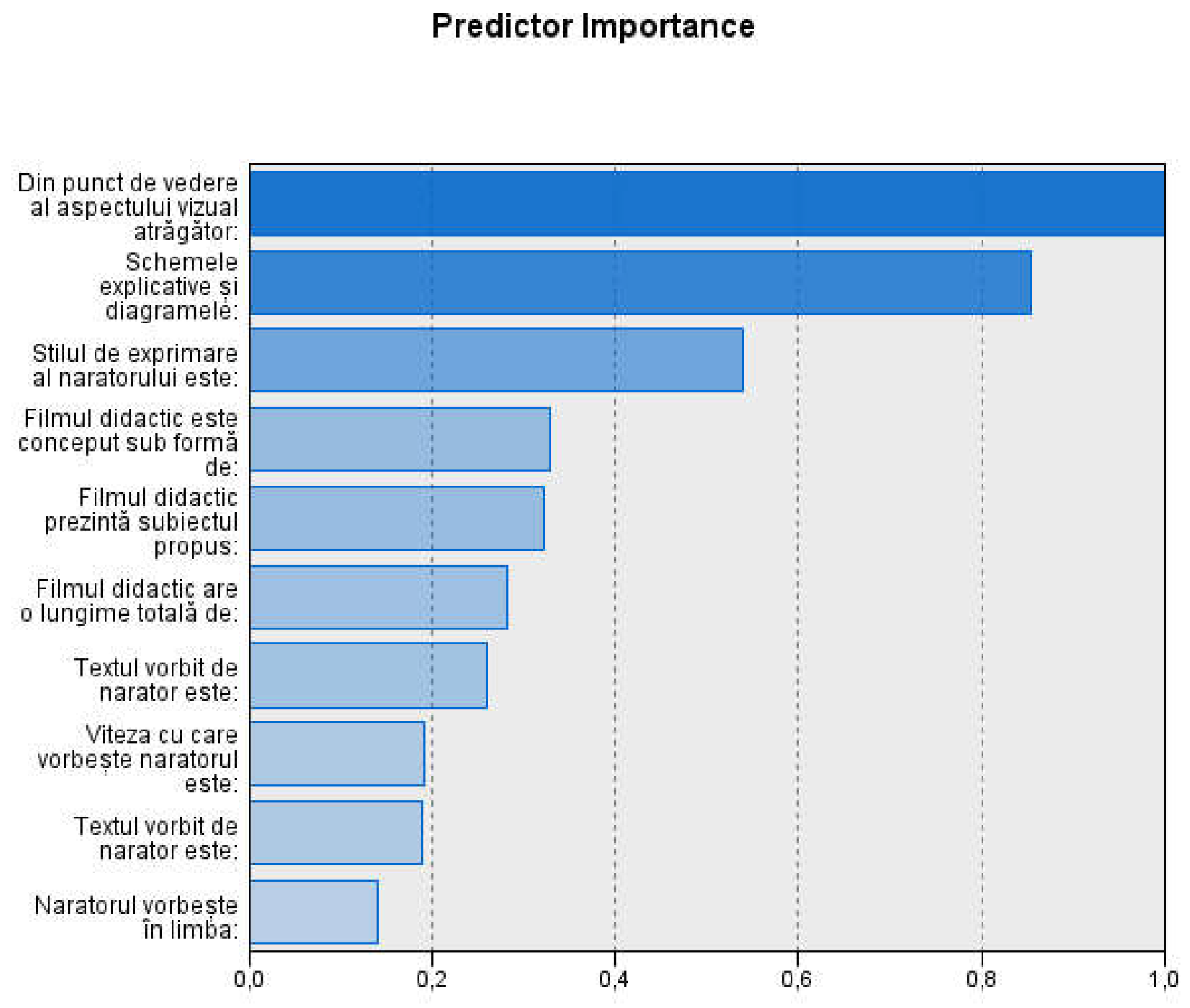

Table 1.
General features of the study group.
| n | % | ||
|---|---|---|---|
| Gender | male | 131 | 23.8 |
| female | 420 | 76.2 | |
| Age group | 18-20 years | 297 | 53.9 |
| 21-24 years | 158 | 28.7 | |
| over 25 years | 96 | 17.4 | |
| University | UMF “Grigore T. Popa” Iași | 356 | 64.6 |
| UMF Craiova | 108 | 19.6 | |
| UMF ”Victor Babeș” Timișoara | 80 | 14.5 | |
| UMF ”Iuliu Hațieganu” Cluj Napoca | 7 | 1.3 | |
| Previously graduated university studies | yes | 55 | 10.0 |
| no | 496 | 90.0 | |
| Total | 551 | 100.0 |
Table 2.
Features preferred by students at instructional videos—comparative study on genders.
| Gender | Total | p-value | |||||
|---|---|---|---|---|---|---|---|
| male | female | ||||||
| Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
||
| FD1 | 2 (1.5) | 129 (98.5) | 7 (1.7) | 413 (98.3) | 9 (1.6) | 542 (98.4) | .912 |
| FD2 | 51 (38.9) | 80 (61.1) | 216 (51.4) | 204 (48.6) | 267 (48.5) | 284 (51.5) | .012* |
| FD3 | 37 (28.2) | 94 (71.8) | 67 (16.0) | 353 (84.0) | 104 (18.9) | 447 (81.1) | .002** |
| FD4 | 39 (29.8) | 92 (70.2) | 135 (32.1) | 285 (67.9) | 174 (31.6) | 377 (68.4) | .610 |
| FD5 | 87 (66.4) | 44 (33.6) | 287 (68.3) | 133 (31.7) | 374 (67.9) | 177 (32.1) | .681 |
| FD6 | 38 (29.0) | 93 (71.0) | 119 (28.3) | 301 (71.7) | 157 (28.5) | 394 (71.5) | .881 |
| FD7 | 65 (49.6) | 66 (50.4) | 190 (45.2) | 230 (54.8) | 255 (46.3) | 296 (53.7) | .380 |
| FD8 | 46 (35.1) | 85 (64.9) | 102 (24.3) | 318 (75.7) | 148 (26.9) | 403 (73.1) | .015* |
| FD9 | 98 (74.8) | 33 (25.2) | 331 (78.8) | 89 (2.2) | 429 (77.9) | 122 (22.1) | .336 |
| FD10 | 40 (30.5) | 91 (69.5) | 140 (33.3) | 280 (66.7) | 180 (32.7) | 371 (67.3) | .551 |
| FD11 | 15 (11.5) | 116 (88.5) | 37 (8.8) | 383 (91.2) | 52 (9.4) | 499 (90.6) | .367 |
| FD12 | 11 (8.4) | 120 (91.6) | 14 (3.3) | 406 (96.7) | 25 (4.5) | 526 (95.5) | .015* |
| FD13 | 15 (11.5) | 116 (88.5) | 49 (11.7) | 371 (88.3) | 64 (11.6) | 487 (88.4) | .946 |
| FD14 | 72 (55.0) | 59 (45.0) | 187 (44.5) | 233 (55.5) | 259 (47.0) | 292 (53.0) | .037* |
| FD15 | 32 (24.4) | 99 (75.6) | 108 (25.7) | 312 (74.3) | 140 (25.4) | 411 (7.6) | .768 |
| Total | 131 (100.0) | 420 (100.0) | 551 (100.0) | ||||
| Pearson Chi-squared test; *p<0.05 statistically significant; **p<0.01 highly statistically significant | |||||||
Table 3.
Features preferred by students at instructional videos—comparative study on age groups.
| Age group | Total | p-value | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 18-20 years | 21-24 years | Over 25 years | |||||||
| Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
||
| FD1 | 6 (2.0) | 291 (98.0) | 2 (1.3) | 156 (98.7) | 1 (1.0) | 95 (99.0) | 9 (1.6) | 542 (98.4) | .734 |
| FD2 | 126 (42.4) | 171 (57.6) | 91 (57.6) | 67 (42.4) | 50 (52.1) | 46 (47.9) | 267 (48.5) | 284 (51.5) | .006** |
| FD3 | 57 (19.2) | 240 (80.8) | 33 (20.9) | 125 (79.1) | 14 (14.6) | 82 (85.4) | 104 (18.9) | 447 (81.1) | .451 |
| FD4 | 113 (38.0) | 184 (62.0) | 35 (22.2) | 123 (77.8) | 26 (27.1) | 70 (72.9) | 174 (31.6) | 377 (68.4) | .001** |
| FD5 | 203 (68.4) | 94 (31.6) | 102 (64.6) | 56 (35.4) | 69 (71.9) | 27 (28.1) | 374 (67.9) | 177 (32.1) | .465 |
| FD6 | 80 (26.9) | 217 (73.1) | 55 (34.8) | 103 (65.2) | 22 (22.9) | 74 (77.1) | 157 (28.5) | 394 (71.5) | .086 |
| FD7 | 136 (45.8) | 161 (54.2) | 78 (49.4) | 80 (50.6) | 41 (42.7) | 55 (57.3) | 255 (46.3) | 296 (53.7) | .569 |
| FD8 | 86 (29.0) | 211 (71.0) | 38 (24.1) | 120 (75.9) | 24 (25.0) | 72 (75.0) | 148 (26.9) | 403 (73.1) | .480 |
| FD9 | 241 (81.1) | 56 (18.9) | 126 (79.7) | 32 (20.3) | 62 (64.6) | 34 (35.4) | 429 (77.9) | 122 (22.1) | .002** |
| FD10 | 107 (36.0) | 190 (64.0) | 42 (26.6) | 116 (73.4) | 31 (32.3) | 65 (67.7) | 180 (32.7) | 371 (67.3) | .123 |
| FD11 | 28 (9.4) | 269 (90.6) | 13 (8.2) | 145 (91.8) | 11 (11.5) | 85 (88.5) | 52 (9.4) | 499 (90.6) | .694 |
| FD12 | 16 (5.4) | 281 (94.6) | 7 (4.4) | 151 (95.6) | 2 (2.1) | 94 (97.9) | 25 (4.5) | 526 (95.5) | .400 |
| FD13 | 42 (14.1) | 255 (85.9) | 12 (7.6) | 146 (92.4) | 10 (10.4) | 86 (89.6) | 64 (11.6) | 487 (88.4) | .107 |
| FD14 | 133 (44.8) | 164 (55.2) | 79 (50.0) | 79 (50.0) | 47 (49.0) | 49 (51.0) | 259 (47.0) | 292 (53.0) | .521 |
| FD15 | 66 (22.2) | 231 (77.8) | 51 (32.3) | 107 (67.7) | 23 (24.0) | 73 (76.0) | 140 (25.4) | 411 (7.6) | .060 |
| Total | 297 (100.0) | 158 (100.0) | 96 (100.0) | 551 (100.0) | |||||
| Pearson Chi-squared test; *p<0.05 statistically significant; **p<0.01 highly statistically significant | |||||||||
Table 4.
Features preferred by students at instructional videos—comparative study on preferred Internet services: Information.
Table 4.
Features preferred by students at instructional videos—comparative study on preferred Internet services: Information.
| Main activity on Internet: Information | p-value | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| The least important | Less important | Important | The most important | ||||||
| Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
||
| FD1 | - | 19 (100.0) | 5 (3.6) | 133 (96.4) | 2 (0.9) | 212 (99.1) | 2 (1.1) | 178 (98.9) | .197 |
| FD2 | 9 (47.4) | 10 (52.6) | 62 (44.9) | 76 (55.1) | 106 (49.5) | 108 (50.5) | 90 (50.0) | 90 (50.0) | .809 |
| FD3 | 5 (26.3) | 14 (73.7) | 24 (17.4) | 114 (82.6) | 32 (15.0) | 182 (85.0) | 43 (23.9) | 137 (76.1) | .112 |
| FD4 | 8 (42.1) | 11 (57.9) | 37 (26.8) | 101 (73.2) | 69 (32.2) | 145 (67.8) | 60 (33.3) | 120 (66.7) | .436 |
| FD5 | 11 (57.9) | 8 (42.1) | 94 (68.1) | 44 (31.9) | 151 (70.6) | 63 (29.4) | 118 (65.6) | 62 (34.4) | .568 |
| FD6 | 3 (15.8) | 16 (84.2) | 47 (34.1) | 91 (65.9) | 55 (25.7) | 159 (74.3) | 52 (28.9) | 128 (71.1) | .218 |
| FD7 | 10 (52.6) | 9 (47.4) | 63 (45.7) | 75 (54.3) | 96 (44.9) | 118 (55.1) | 86 (47.8) | 94 (52.2) | .881 |
| FD8 | 6 (31.6) | 13 (68.4) | 31 (22.5) | 107 (77.5) | 56 (26.2) | 158 (73.8) | 55 (30.6) | 125 (69.4) | .411 |
| FD9 | 17 (89.5) | 2 (10.5) | 102 (73.9) | 36 (26.1) | 170 (79.4) | 44 (20.6) | 140 (77.8) | 40 (22.2) | .385 |
| FD10 | 10 (52.6) | 9 (47.4) | 41 (29.7) | 97 (70.3) | 69 (32.2) | 145 (67.8) | 60 (33.3) | 120 (66.7) | .257 |
| FD11 | 1 (5.3) | 18 (94.7) | 3 (2.2) | 135 (97.8) | 35 (16.4) | 179 (83.6) | 13 (7.2) | 167 (92.8) | .000** |
| FD12 | 1 (5.3) | 18 (94.7) | 3 (2.2) | 135 (97.8) | 16 (7.5) | 198 (92.5) | 5 (2.8) | 175 (97.2) | .061 |
| FD13 | 1 (5.3) | 18 (94.7) | 15 (10.9) | 123 (89.1) | 29 (13.6) | 185 (86.4) | 19 (10.6) | 161 (89.4) | .615 |
| FD14 | 9 (47.4) | 10 (52.6) | 76 (55.1) | 62 (44.9) | 86 (40.2) | 128 (59.8) | 88 (48.9) | 92 (51.1) | .049* |
| FD15 | 5 (26.3) | 14 (73.7) | 39 (28.3) | 99 (71.7) | 50 (23.4) | 164 (76.6) | 46 (25.6) | 134 (74.4) | .783 |
| Total | 19 (100.0) | 138 (100.0) | 214 (100.0) | 180 (100.0) | |||||
| Pearson Chi-squared test; *p<0.05 statistically significant; **p<0.01 highly statistically significant | |||||||||
Table 5.
Features preferred by students at instructional videos—comparative study on preferred Internet services: Communication.
Table 5.
Features preferred by students at instructional videos—comparative study on preferred Internet services: Communication.
| Main activity on Internet: Communication | p-value | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| The least important | Less important | Important | The most important | ||||||
| Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
||
| FD1 | - | 5 (100.0) | - | 58 (100.0) | 3 (1.9) | 151 (98.1) | 6 (1.8) | 328 (98.2) | .754 |
| FD2 | 1 (20.0) | 4 (80.0) | 20 (34.5) | 38 (65.5) | 78 (50.6) | 76 (49.4) | 168 (50.3) | 166 (49.7) | .075 |
| FD3 | 3 (60.0) | 2 (40.0) | 22 (37.9) | 36 (62.1) | 33 (21.4) | 121 (78.6) | 46 (13.8) | 288 (86.2) | .000** |
| FD4 | 1 (20.0) | 4 (80.0) | 18 (31.0) | 40 (69.0) | 51 (33.1) | 103 (66.9) | 104 (31.1) | 230 (68.9) | .915 |
| FD5 | 2 (40.0) | 3 (60.0) | 36 (62.1) | 22 (37.9) | 101 (65.6) | 53 (34.4) | 235 (70.4) | 99 (29.6) | .262 |
| FD6 | 2 (40.0) | 3 (60.0) | 18 (31.0) | 40 (69.0) | 47 (30.5) | 107 (69.5) | 90 (26.9) | 244 (73.1) | .750 |
| FD7 | 1 (20.0) | 4 (80.0) | 26 (44.8) | 32 (55.2) | 71 (46.1) | 83 (53.9) | 157 (47.0) | 177 (53.0) | .680 |
| FD8 | - | 5 (100.0) | 15 (25.9) | 43 (74.1) | 46 (29.9) | 108 (70.1) | 87 (26.0) | 247 (74.0) | .442 |
| FD9 | 3 (60.0) | 2 (40.0) | 44 (75.9) | 14 (24.1) | 115 (74.7) | 39 (25.3) | 267 (79.9) | 67 (20.1) | .423 |
| FD10 | - | 5 (100.0) | 15 (25.9) | 43 (74.1) | 56 (36.4) | 98 (63.6) | 109 (32.6) | 225 (67.4) | .203 |
| FD11 | - | 5 (100.0) | 7 (12.1) | 51 (87.9) | 14 (9.1) | 140 (90.9) | 31 (9.3) | 303 (90.7) | .796 |
| FD12 | - | 5 (100.0) | 5 (8.6) | 53 (91.4) | 6 (3.9) | 148 (96.1) | 14 (4.2) | 320 (95.8) | .439 |
| FD13 | - | 5 (100.0) | 5 (8.6) | 53 (91.4) | 19 (12.3) | 135 (87.7) | 40 (12.0) | 294 (88.0) | .733 |
| FD14 | 3 (60.0) | 2 (40.0) | 31 (53.4) | 27 (46.6) | 80 (51.9) | 74 (48.1) | 145 (43.4) | 189 (56.6) | .208 |
| FD15 | 1 (20.0) | 4 (80.0) | 13 (22.4) | 45 (77.6) | 42 (27.3) | 112 (72.7) | 84 (25.1) | 250 (74.9) | .886 |
| Total | 5 (100.0) | 58 (100.0) | 154 (100.0) | 334 (100.0) | |||||
| Pearson Chi-squared test; *p<0.05 statistically significant; **p<0.01 highly statistically significant | |||||||||
Table 6.
Features preferred by students at instructional videos—comparative study on preferred Internet services: Entertainment.
Table 6.
Features preferred by students at instructional videos—comparative study on preferred Internet services: Entertainment.
| Main activity on Internet: Entertainment | p-value | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| The least important | Less important | Important | The most important | ||||||
| Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
||
| FD1 | - | 34 (100.0) | 1 (0.7) | 143 (99.3) | 6 (3.2) | 184 (96.8) | 2 (1.1) | 181 (98.9) | .218 |
| FD2 | 23 (67.6) | 11 (32.4) | 70 (48.6) | 74 (51.4) | 84 (44.2) | 106 (55.8) | 90 (49.2) | 93 (50.8) | .093 |
| FD3 | 5 (14.7) | 29 (85.3) | 21 (14.6) | 123 (85.4) | 39 (20.5) | 151 (79.5) | 39 (21.3) | 144 (78.7) | .367 |
| FD4 | 17 (50.0) | 17 (50.0) | 47 (32.6) | 97 (67.4) | 53 (27.9) | 137 (72.1) | 57 (31.1) | 126 (68.9) | .085 |
| FD5 | 18 (52.9) | 16 (47.1) | 103 (71.5) | 41 (28.5) | 134 (70.5) | 56 (29.5) | 119 (65.0) | 64 (35.0) | .130 |
| FD6 | 9 (26.5) | 25 (73.5) | 36 (25.0) | 108 (75.0) | 53 (27.9) | 137 (72.1) | 59 (32.2) | 124 (67.8) | .527 |
| FD7 | 13 (38.2) | 21 (61.8) | 71 (49.3) | 73 (50.7) | 89 (46.8) | 101 (53.2) | 82 (44.8) | 101 (55.2) | .660 |
| FD8 | 15 (44.1) | 19 (55.9) | 44 (30.6) | 100 (69.4) | 49 (25.8) | 141 (74.2) | 40 (21.9) | 143 (78.1) | .035* |
| FD9 | 26 (76.5) | 8 (23.5) | 110 (76.4) | 34 (23.6) | 143 (75.3) | 47 (24.7) | 150 (82.0) | 33 (18.0) | .431 |
| FD10 | 18 (52.9) | 16 (47.1) | 37 (25.7) | 107 (74.3) | 65 (34.2) | 125 (65.8) | 60 (32.8) | 123 (67.2) | .021* |
| FD11 | 8 (23.5) | 26 (76.5) | 10 (6.9) | 134 (93.1) | 16 (8.4) | 174 (91.6) | 18 (9.8) | 165 (90.2) | .027* |
| FD12 | 2 (5.9) | 32 (94.1) | 4 (2.8) | 140 (97.2) | 7 (3.7) | 183 (96.3) | 12 (6.6) | 171 (93.4) | .360 |
| FD13 | 10 (29.4) | 24 (70.6) | 12 (8.3) | 132 (91.7) | 19 (10.0) | 171 (90.0) | 23 (12.6) | 160 (87.4) | .005** |
| FD14 | 14 (41.2) | 20 (58.8) | 65 (45.1) | 79 (54.9) | 97 (51.1) | 93 (48.9) | 83 (45.4) | 100 (54.6) | .549 |
| FD15 | 9 (26.5) | 25 (73.5) | 37 (25.7) | 107 (74.3) | 47 (24.7) | 143 (75.3) | 47 (25.7) | 136 (74.3) | .994 |
| Total | 34 (100.0) | 144 (100.0) | 190 (100.0) | 183 (100.0) | |||||
| Pearson Chi-squared test; *p<0.05 statistically significant; **p<0.01 highly statistically significant | |||||||||
Table 7.
Features preferred by students at instructional videos—comparative study on preferred Internet services: Domestic facilities.
Table 7.
Features preferred by students at instructional videos—comparative study on preferred Internet services: Domestic facilities.
| Main activity on Internet: Domestic facilities | p-value | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| The least important | Less important | Important | The most important | ||||||
| Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
||
| FD1 | 6 (2.1) | 278 (97.9) | 1 (0.7) | 142 (99.3) | 1 (1.1) | 88 (98.9) | 1 (2.9) | 34 (97.1) | .647 |
| FD2 | 127 (44.7) | 157 (55.3) | 68 (47.6) | 75 (52.4) | 55 (61.8) | 34 (38.2) | 17 (48.6) | 18 (51.4) | .046* |
| FD3 | 60 (21.1) | 224 (78.9) | 26 (18.2) | 117 (81.8) | 9 (10.1) | 80 (89.9) | 9 (25.7) | 26 (74.3) | .089 |
| FD4 | 88 (31.0) | 196 (69.0) | 49 (34.3) | 94 (65.7) | 28 (31.5) | 61 (68.5) | 9 (25.7) | 26 (74.3) | .781 |
| FD5 | 202 (71.1) | 82 (28.9) | 91 (63.6) | 52 (36.4) | 58 (65.2) | 31 (34.8) | 23 (65.7) | 12 (34.3) | .403 |
| FD6 | 85 (29.9) | 199 (70.1) | 42 (29.4) | 101 (70.6) | 18 (20.2) | 71 (79.8) | 12 (34.3) | 23 (65.7) | .272 |
| FD7 | 129 (45.4) | 155 (54.6) | 64 (44.8) | 79 (55.2) | 44 (49.4) | 45 (50.6) | 18 (51.4) | 17 (48.6) | .814 |
| FD8 | 79 (27.8) | 205 (72.2) | 43 (30.1) | 100 (69.9) | 17 (19.1) | 72 (80.9) | 9 (25.7) | 26 (74.3) | .304 |
| FD9 | 225 (79.2) | 59 (20.8) | 114 (79.7) | 29 (20.3) | 65 (73.0) | 24 (27.0) | 25 (71.4) | 10 (28.6) | .451 |
| FD10 | 82 (28.9) | 202 (71.1) | 53 (37.1) | 90 (62.9) | 30 (33.7) | 59 (66.3) | 15 (42.9) | 20 (57.1) | .186 |
| FD11 | 21 (7.4) | 263 (92.6) | 17 (11.9) | 126 (88.1) | 11 (12.4) | 78 (87.6) | 3 (8.6) | 32 (91.4) | .346 |
| FD12 | 12 (4.2) | 272 (95.8) | 7 (4.9) | 136 (95.1) | 5 (5.6) | 84 (94.4) | 1 (2.9) | 34 (97.1) | .902 |
| FD13 | 27 (9.5) | 257 (90.5) | 22 (15.4) | 121 (84.6) | 12 (13.5) | 77 (86.5) | 3 (8.6) | 32 (91.4) | .281 |
| FD14 | 139 (48.9) | 145 (51.1) | 63 (44.1) | 80 (55.9) | 41 (46.1) | 48 (53.9) | 16 (45.7) | 19 (54.3) | .805 |
| FD15 | 71 (25.0) | 213 (75.0) | 39 (27.3) | 104 (72.7) | 17 (19.1) | 72 (80.9) | 13 (37.1) | 22 (62.9) | .195 |
| Total | 284 (100.0) | 143 (100.0) | 89 (100.0) | 35 (100.0) | |||||
| Pearson Chi-squared test; *p<0.05 statistically significant; **p<0.01 highly statistically significant | |||||||||
Table 8.
The description of the clusters identified among the preferred features of didactic videos.
Table 8.
The description of the clusters identified among the preferred features of didactic videos.
| Identified clusters | ||||||
|---|---|---|---|---|---|---|
| Cluster 1 (195 cases—35.4%) |
Cluster 2 (192 cases—34.8%) |
Cluster 3 (164 cases—29.8%) |
||||
| Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
Option 1: n (%) |
Option 2: n (%) |
|
| FD1 | 2 (1.0) | 193 (99.0) | 2 (1.0) | 190 (99.0) | 5 (3.0) | 159 (97.0) |
| FD2 | 116 (59.5) | 79 (40.5) | 66 (34.4) | 126 (65.6) | 85 (51.8) | 79(48.2) |
| FD3 | 11 (5.6) | 184 (94.4) | 53 (27.6) | 139 (72.4) | 40 (24.4) | 124 (75.6) |
| FD4 | 40 (20.5) | 155 (79.5) | 48 (25.0) | 144 (75.0) | 86 (52.4) | 78 (47.6) |
| FD5 | 186 (95.4) | 9 (4.6) | 126 (65.6) | 66 (34.4) | 62 (37.8) | 102 (62.2) |
| FD6 | 77 (39.5) | 118 (60.5) | 48 (25.0) | 144 (75.0) | 32 (19.5) | 132 (80.5) |
| FD7 | 176 (90.3) | 19 (9.7) | 23 (12.0) | 169 (88.0) | 56 (34.1) | 108 (65.9) |
| FD8 | 47 (24.1) | 148 (75.9) | 26 (13.5) | 166 (86.5) | 75 (45.7) | 89 (54.3) |
| FD9 | 147 (75.4) | 48 (24.6) | 172 (89.6) | 20 (10.4) | 110 (67.1) | 54 (32.9) |
| FD10 | 45 (23.1) | 150 (76.9) | 10 (5.2) | 182 (94.8) | 125 (76.2) | 39 (23.8) |
| FD11 | - | 195 (100.0) | 12 (6.3) | 180 (93.8) | 40 (24.4) | 124 (75.6) |
| FD12 | - | 195 (100.0) | 5 (2.6) | 187 (97.4) | 20 (12.2) | 144 (87.8) |
| FD13 | 6 (3.1) | 189 (96.9) | 8 (4.2) | 184 (95.8) | 50 (30.5) | 114 (69.5) |
| FD14 | 104 (53.3) | 91 (46.7) | 125 (65.1) | 67 (34.9) | 30 (18.3) | 134 (81.7) |
| FD15 | 85 (43.6) | 110 (56.4) | 12 (6.3) | 180 (93.8) | 43 (26.2) | 121 (73.8) |
Table 9.
The comparative study of the clusters identified among the preferred features of instructional videos.
Table 9.
The comparative study of the clusters identified among the preferred features of instructional videos.
| Cluster 1— FD7 = 1 and FD10 = 2 n (%) |
Cluster 2— FD7 = 2 and FD10 = 2 n (%) |
Cluster 3— FD7 = 2 and FD10 = 1 n (%) |
p-value | ||
|---|---|---|---|---|---|
| Gender | ,941 | ||||
| Male | 48 (24,6) | 45 (23,4) | 38 (23,2) | ||
| Female | 147 (75,4) | 147 (76,6) | 126 (76,8) | ||
| Age group | ,147 | ||||
| 18-20 years | 100 (51,3) | 100 (52,1) | 97 (59,1) | ||
| 21-24 years | 65 (33,3) | 58 (30,2) | 35 (21,3) | ||
| over 25 years | 30 (15,4) | 34 (17,7) | 32 (19,5) | ||
| Main activity on Internet: Information (on a scale from 1 to 4): | ,203 | ||||
| 1—the least important | 5 (2,6) | 6 (3,1) | 8 (4,9) | ||
| 2—less important | 54 (27,7) | 55 (28,6) | 29 (17,7) | ||
| 3—important | 78 (40,0) | 69 (35,9) | 67 (40,9) | ||
| 4—the most important | 58 (29,7) | 62 (32,3) | 60 (36,6) | ||
| Main activity on Internet: Communication (on a scale from 1 to 4): | ,201 | ||||
| 1—the least important | 1 (0,5) | 3 (1,6) | 1 (0,6) | ||
| 2—less important | 17 (8,7) | 28 (14,6) | 13 (7,9) | ||
| 3—important | 51 (26,2) | 57 (29,7) | 46 (28,0) | ||
| 4—the most important | 126 (64,6) | 104 (54,2) | 104 (63,4) | ||
| Main activity on Internet: Entertainment (on a scale from 1 to 4): | ,119 | ||||
| 1—the least important | 8 (4,1) | 8 (4,2) | 18 (11,0) | ||
| 2—less important | 54 (27,7) | 52 (27,1) | 38 (23,2) | ||
| 3—important | 69 (35,4) | 69 (35,9) | 52 (31,7) | ||
| 4—the most important | 64 (32,8) | 63 (32,8) | 56 (34,1) | ||
| Main activity on Internet: Domestic facilities (on a scale from 1 to 4): | ,296 | ||||
| 1—the least important | 99 (50,8) | 112 (58,3) | 73 (44,5) | ||
| 2—less important | 51 (26,2) | 43 (22,4) | 49 (29,9) | ||
| 3—important | 31 (15,9) | 28 (14,6) | 30 (18,3) | ||
| 4—the most important | 14 (7,2) | 9 (4,7) | 12 (7,3) | ||
| Total | 195 (100,0) | 192 (100,0) | 164 (100,0) | ||
| Pearson Chi-squared test; *p<0.05 statistically significant; **p<0.01 highly statistically significant | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



