
Submitted:
22 April 2024
Posted:
23 April 2024
You are already at the latest version
Abstract
Accurate clinical diagnosis of patients presenting to primary care settings with acute sore throat remains challenging, often resulting in the over-prescribing of antibiotics. Using point-of-care tests (POCTs) to differentiate between respiratory infections is well-accepted, yet evidence on the application within primary care is sparse. We assessed the application of testing patients (n=160) from three family practices with suspected Streptococcal infections using rapid molecular tests (ID NOW Strep A2, Abbott). In addition to comparing clinical evaluation and prescription rates with either usual care or with testing, patients and staff completed a questionnaire about their experience of molecular POCT in primary care. The immediate availability of the result was important to patients (100%) and staff (≈90%) stated that molecular testing improved quality of care. Interestingly, only 22.73% of patients with a Centor score >2 tested positive for Strep A and overall, less than 50% of Centor scores 3 and 4 tested positive for Strep A with the ID NOW testing platform. The addition of rapid molecular POCTs to clinical assessment resulted in a 55- 65% reduction in immediate and deferred antibiotic prescriptions. The intervention was popular with patients and medical staff but was associated with increased cost and a longer appointment length.
Keywords:
Point-of-Care-Testing
; GAS infections
; molecular
; quality improvement
; antimicrobial stewardship
1. Introduction
Sore throats remain one of the most common acute presentations in primary care across the UK, accounting for nearly 10% of all GP appointments each year [1]. Although the umbrella term of ‘sore throat’ refers to both pharyngitis and tonsillitis, this study focused primarily on that latter. Differentiating between viral and bacterial causes of tonsillitis based on clinical assessment is often difficult, especially in periods with overlapping prevalence. Streptococcus pyogenes (Group A Streptococcus; GAS) has become highly adapted to the human host and is the most common pathogenic bacterial cause of tonsillitis [2]. GAS infections can be asymptomatic, presenting as mild conditions such as strep throat or impetigo or develop into severe or life-threatening invasive infections, peri-tonsillar abscess and glomerulonephritis. In primary care, most children present with acute sore throats with or without tonsillar exudate, fever and general malaise, with prevalence highest during the winter months and in the 5–15-year-old age group [3].
Accurate diagnosis and treatment of GAS infections is crucial to prevent serious complications. The National Institute for Health and Care Excellence (NICE) in the UK recommends prompt treatment with antibiotics in suspected cases, with additional treatment of susceptible close contacts where indicated [4,5]. Currently the recommended choices are phenoxymethylpenicillin for 5-10 days or Clarithromycin for 5 days in a patient with penicillin allergy [6]. Asymptomatic carriage rates in this age group are around 8% [7] making clinical differentiation of illness rather than carriage important.
Despite viruses accounting for over 70% of cases presenting to primary care, antibiotics are still prescribed for 40% of patients [8], causing concerns over inappropriate antibiotic prescribing. The overuse of antibiotics has been attributed to the absence of reliable rapid diagnostic tests prior to prescription, with microbiological culture taking up to 72 hours before a result is available [9]. Poor antibiotic stewardship is associated with increased health costs, risk of side effects and allergic reactions for patients, and growing rates of antibiotic resistance. As a result many guidelines, including those from NICE [4) suggest the use of Centor criteria [10] or the FeverPAIN score as decision making tools to support the clinical assessment. These scores range from 0-4 with points accumulated for specified symptoms or signs: i) Tonsillar exudate, ii) tender anterior cervical lymphadenopathy or lymphadenitis, iii) Fever (≥38°C), and iv) absence of cough. Individuals with a low total score (less than 2) have a lower probability of streptococcal tonsillitis and therefore antibiotic prescribing may be avoided, while higher scores support either immediate or deferred antibiotic prescription.
Although a meta-analysis [11] showed that Centor criteria may be useful in ruling out GAS if there is a score of 0, scores greater than 1 are associated with variable predictive value of streptococcal infection, with a score of 4 being associated with positive culture in around 55% of cases. Prescribing antibiotics to this cohort of patients following clinical assessment with Centor scoring, will therefore result in around 45% of patients who do not have a bacterial infection being treated with antibiotics. Thus, having a combination of clinical scoring and confirmatory testing would strengthen clinical management and reduce unnecessary antibiotic prescriptions.
Although no gold standard exists for the diagnosis of Strep throat, historically, throat swabs for microscopy, culture and sensitivities (MC&S) have been used. However, these have several limitations in that they have low sensitivity and specificity and may take up to 3 days for results to be obtained [9]. In comparison, a POC test (either lateral flow or rapid molecular) can result in confirmation in as little as 5-10 minutes and may be performed on site during the first patient visit, saving both time and reducing diagnostic uncertainty in the meantime. Collectively, the evidence suggests the implementation of adjunct point of care (POC) testing in addition to scoring systems and clinical judgement [9] may improve the identification of symptomatic streptococcal tonsillitis while reducing unnecessary antibiotic prescriptions. Nardi and colleagues recently demonstrated that identification of viral aetiology in children using rapid molecular point-of-care testing resulted in a 9-fold reduction in antibiotic prescriptions [12] supporting the potential expansion of POC testing into routine care.
The uptake of POC testing has been slow in primary care in the past, however a study undertaken in Ireland [13] revealed that GPs perceive point of care tests as beneficial and expressed a desire for increased availability of such tests in their daily clinical practise. Among the total of 143 participants, 92 of them indicated their interest in accessing POCTs, citing guidance in decision making as the primary benefit (43%), followed by reduced referral rates (29%) and assistance in diagnosis (13%) [13]. Moreover, during the Covid-19 pandemic, studies in primary care practices in Germany and the United Kingdom using molecular testing showed patient satisfaction in terms of prompt testing and trusted results, reduced further testing and improved workflow and better patient care for high-risk groups [14,15,16].
This quality improvement study sought to investigate the effect of POC testing on antibiotic prescribing in patients presenting to primary care with an acute sore throat. It aimed to determine the financial and time costs associated with POC testing when compared to usual care and assess the feasibility of its implementation. Furthermore, it endeavoured to understand the opinions of patients and staff involved in the testing for a holistic view of POC testing in an NHS setting.
2. Materials and Methods
2.1. Study Design
Between December 2023 and February 2024, a prospective quality improvement project was designed to evaluate the impact of point-of-care-testing on the management of acute sore throat in ambulatory patients presenting to primary care settings in the towns of Seaton, Colyton and Axminster, in Devon in the United Kingdom. This quality improvement project complied with the General Data Protection Regulation (GDPR) in accordance with the principles of Good Clinical Practice.
2.2. Clinical Assessment of Patients
All patients presenting to the General Practice clinics at Townsend House Medical Centre, Seaton and Colyton Medical Practice and Axminster Medical Practice with acute sore throat were assessed according to usual practice. In addition, patients presenting to Townsend House Medical Centre were offered the option of a consultation at Seaton Pharmacy, a local community pharmacy. The pharmacist arm was included to assess the feasibility of pharmacist led assessment and management of throat infections, prior to the introduction of Pharmacy First, an NHS England initiative to improve access for minor illness, where pharmacists can treat 7 defined minor illnesses without recourse to a doctor.
All patients were assessed by a clinician. Where the decision was then made to consider either immediate or deferred prescription for antibiotics for a clinical diagnosis of streptococcal infection, clinicians were offered the option to follow a new POC pathway or continuing with usual care (see Figure 1). Where the patient and clinician agreed to follow the POC pathway assessment the ID NOW Strep A2 test used as a rapid diagnostic tool. NICE guidance recommends either FeverPain or Centor scoring systems [4,5,6]. In this study the Centor score was used for patient assessment due to clinician familiarity.
Following clinical assessment, patients with a score of 2, 3 or 4, received a molecular based POCT Group A streptococcus, during the consultation. Nice guidance [4] recommends immediate or deferred prescriptions for patients with a Centor score of 3 or 4; however, during the severe outbreak in the UK between October 2022 and March 2023 this recommendation was amended to a lower threshold for antibiotic prescribing. This amended guideline was removed on February 15th, 2023 [17] but high levels of parental anxiety around childhood streptococcal infections remain which can influence prescribing decisions in the context of shared decision-making discussions between patients (or their parents) and clinicians. Thus, in this study, this protocol was used which reflects current clinical practice, rather than strict adherence to NICE guidance. Patients who tested positive with the molecular POCT were treated according to local protocols [18], while those testing negative received advice on symptom management such as taking paracetamol for fever and pain, adequate intake of fluids or trying medicated lozenges, and safety netting advice to seek medical help if symptoms worsen rapidly or significantly, fail to improve after 1 week or the person becomes systematically unwell. An overview of the patient testing synopsis can be viewed in Figure 1.
2.3. Point-of-Care Testing Molecular Diagnostics
This project used the Strep A2 test on the molecular Abbott ID NOWTM platform which is a simple rapid molecular test that is user-friendly and does not require specific microbiology equipment making it ideal for direct POC diagnostics. This molecular isothermal test is based on NEAR (nicking enzyme-combined isothermal amplification) technology, which detects the cepA gene encoding the C5-peptidase with a manufacturer's specified limit of detection (LOD) between 25 and 147 CFU/ml [19,20]. Following a throat swab, the test results are available after 2 minutes, with no warm-up time required (Abbott Rapid Diagnostic Ltd, UK). Tests were consistently carried out according to the instructions for use for the ID NOW™ and Strep A2 test after all staff involved received training.
2.4. Study Population
Patients were recruited during the initial clinical assessment. The median age of patients in this study was 17 years. The range was from 2 months old to 86 years. 36% of patients were male (n=57), 37 % female (n=103). The inclusion criteria were patients presenting with acute sore throat (less than one week duration) to one of the three GP practices participating in the study. There were no age or comorbidity restrictions. Patients who fulfilled the inclusion criteria were offered a throat swab for molecular POC testing following initial clinical assessment as described in the section above. Verbal consent from the patient was obtained by the clinician. Patients who declined were managed according to usual clinical care, with prescribing decision made by the treating clinician.
2.5. Data Collection
The nature of the clinical process required minimal demographic information to be recorded, and these were kept on a paper log and stored in a locked filing cabinet in the primary care sites, with access restricted to clinical staff involved in direct patient care. Patient results were transcribed anonymously onto an electronic database using Excel, stored on a secure hard drive at Townsend House Medical Centre.
The following patient data were collected: Name, date of birth, Centor score and POC test result. In addition, the length of consultation time in usual care and POC arms, and the time required to process the POC test was documented in a sample of patients. This was performed by the staff at each site responsible for testing.
2.6. Questionnaire
In addition to the data on the Centor score and POC test result, patients and clinician satisfaction was also measured using an online survey at the end of the study period, using Online surveys [21]. The questionnaire was based on the expertise of the primary care physicians involved in the study. Patients were asked to answer 5 questions that were rated on a five-point Likert scale (which measure the degree of agreement. All data were collated in an anonymous fashion. All participating members of staff and all patients who received a POC test were invited to complete the questionnaire, which also included items exploring aspects of usability and feasibility of the POCT.
2.7. Statistical Analysis
Results in the POCT group were expressed as a binary outcome: positive or negative test result. Analysis of subgroups was then carried out to determine the relationship between Centor score and test result. Appointment duration was measured retrospectively by analysis of consultation start and finish times in the electronic healthcare records of 40 consecutive patients who had point of care testing, and 40 who received antibiotics, but did not have POC testing. Sample processing time was calculated through a prospective recording of test processing duration by the staff member (pharmacist or nominated staff member in GP practice, using a stopwatch in a sample of consecutive 20 patients.
3. Results
3.1. Molecular POCT Increases the Diagnostic Accuracy of Clinical Evaluation of Strep A Diagnosis
POCT is defined as a diagnostic test, performed during the first patient consultation with available test results within 15 minutes. Using an oral-based swab, the ID NOW Strep A2 test can provide a positive molecular assessment from 2 mins and has a documented sensitivity of 98.5% and specificity of 93.4% [19]. As well as Strep A, the platform can detect viral infections (influenza A&B, RSV and SARS-CoV-2), making it a potentially useful adjunct to standard clinical assessments and has been shown in hospitals settings to improve clinical managements of patients, reduce antibiotic prescription rates and reduce unnecessary secondary testing [22,23,24,25]. Previously, this group and others have assessed the practicality of implementing rapid molecular POCT for SARS-CoV-2 into primary care settings [16]. During the evaluation period here, it was determined if POCT improved the clinical diagnosis of Strep A when compared to usual care (Figure 2).
A total of 160 patients were included in the analysis and were recruited into the study if the clinical picture reflected a bacterial infection and a Centor score was over 1. Figure 2A shows the distribution of Centor score according to patient age with significantly more patients with a score of 2 than 4 and a significant correlation (P=0.002) between age and score (r=-0.2970). Following a pharyngeal swab, testing was performed using the ID NOW Strep A2 test and the mean time to process the test was 5.8 mins. Of 160 results, a total of 10 tests were invalid, 7 of which were due to operator error, in the initial week of the evaluation process. Once retraining had been given, there were a 3 further invalid results, giving an invalid sample rate of 1.9%. Furthermore, 6 patients with a Centor score of 1 were included in error and thus removed from the analysis, giving a total of 144 patients. Figure 2B shows the comparison of negative and positive ID NOW Strep A2 results according to the Centor Score and no significant differences were observed between the two groups. Figure 2C depicts the number of patients testing positive or negative for Strep A according to the Centor score and shows that less individuals actually tested positive. Table 1 summarises the testing result and clinical picture with the comparison between Centor score grades and the result of the patient’s swab following molecular POCT for Strep A. Interestingly, only 22.73% of patients presenting a Centor score of 2 tested positive for Strep A. There was a higher correlation of positive results with increasing Centor score assessments. However, overall, less than 50% of Centor scores 3 & 4 were positive for Strep A with the ID NOW device demonstrating that many cases of throat infection were not due to Strep A. In all of these cases and according to the NICE guidelines, antibiotics would have been prescribed for these patients even though 65.28% of these prescriptions would have been unneccessary.
3.2. Longer Consultation Times for POCT Result in Higher Accuracy of Diagnosis
Molecular POCT is not yet a standard practice in primary care offices and one of the hurdles that needs to be overcome is the concept of longer consultation periods. In this multi-centre evaluation, records were retrospectively reviewed to document the mean length of time required for patients in the normal care pathway that resulted in antibiotics or when a POCT was used prior to prescribing. It was shown that the mean duration of consultation was 17 minutes for patients presenting with sore throats in the usual care pathway and resulting in an antibiotic prescription (n=40). . When a molecular POCT was used, The mean duration of the consultation in the POCT group (including Centor Scoring and POCT process) was 24 minutes (n=40); so an average of 7 minutes longer. In the usual care group, no type of testing such as rapid antigen testing was performed, evaluations were purely clinical based. The cohort of individuals in this assessment was a true cross- of the population since patients ranged from 2 months to the elderly. Although it was not analysed in this study due to lack of an electronic healthcare record to objectively record consultation times, discussions with the pharmacist involved suggest that the addition of point of care testing did not lengthen consultations, where a single clinician undertook the clinical assessment, testing and analysis, rather than passing the sample to a colleague to analyse, through efficient structuring of consultation tasks. Discussions with clinicians involved, also suggested that there is a learning curve and that duration of consultation reduced with experience.
3.3. Patient Responses Following the Availability of Immediate Test Results
Among the POCT cohort 21 out of 144 (14.6) patients consented to engage in the survey. Scoring was formatted using a Likert scale (Figure 3) with dark blue and orange bars denoting high agreement with grey and yellow indicating disagreement. Light blue bars showed undecided opinions or no answer. Overall, patients considered having the test done on-site was excellent (100%) and 88% would like the test to be available in the future. Nearly 90% of patients considered it reassuring to learn the correct diagnosis during the consultation period and over 80% considered that patient care and management was improved. Some statements from the patients included “Great service, great to be able to have test done there and then speed, accuracy, reassurance and quick correct treatment as result”, “Excellent service. Quick results resulting in no need for antibiotics which is always the best outcome if possible” and “As my daughter has strep throat and glandular fever last May, it was important that she was tested for strep throat, otherwise she could of fallen ill again. It was do quick and easy to go the swab test at the GP surgery, we waited 5mins for the results. And it put our minds at rest”.
3.4. Staff Survey
At the end of the study, a total of 29 staff members from the four primary care sites responded to a survey to share their opinions about the implementation of molecular POCT per se. Respondents included 15 doctors (53.6%), 3 paramedics (10.8%), 4 nurses (14.3%), 3 administration staff (10.8%) and 3 practice managers (10.8%) and 1 pharmacist (3.6%). From these individuals, 82.8% had been directly involved in the POC testing process providing viewpoints across the entire practice staff. The Paramedics who responded are employed in primary care rather than emergency care roles, under the NHS England Primary Care Network Additional Roles Reimbursement Scheme. The collated results of the staff survey are shown below in Figure 4 and results as presented in the Likert form with dark blue and orange denoting agreement whereas yellow and light blue show disagreement. Grey and green showing undecided and not applicable respectively. 72% of staff members would like to continue using molecular POCT in the future and most found it easy to use. Over 90% stated that it improved treatment options which was also reflected in the positive outcome for reducing antibiotics, further microbiological testing and reducing consultations for sore throats. Strong disagreement was noted in administration aspects. Some overall individual comments from the different staff members included “This equipment has changed my practice . Much better than centor or fever pain”, “It increases administrative time but decreases clinical time overall”, “…this QI project has shown that by doing the tests antibiotics have not been prescribed when they otherwise would have been and the patient is reassured. It also means that contact tracing and antimicrobial use is targeted”.
4. Discussion
According to the recommendations outlined in the NICE guideline, antibiotic prescription is advised for patients with Centor Scores of 3 or 4. Within the purview of our investigation, a total of 78 patients (53 patients scored 3 and 25 patients scored 4) were identified with a Centor Score of 3 or 4, indicating the need for antibiotic treatment. However, our quality improvement project revealed that 43 out of these 78 patients tested negative for Strep A following molecular POC testing. This finding suggests that 55% of the study cohort assessed as having high Centor Scores did not require antibiotic prescription (immediate or delayed). This demonstrates that the utilization of molecular POC testing effectively reduces unnecessary antibiotic prescribing, while continuing to target patients with a confirmed streptococcal throat infection. Interestingly, a primary care study using lateral flow tests also noted a trend in reduced antibiotic prescriptions in children presenting a sore throat score over 3 and noted that prescriptions were provided due to lack of trust in the lateral test result [26]. In this study both patients and doctors trusted the outcome of the rapid molecular test which corresponds to opinions and attitudes observed in earlier studies carried out in primary care sectors [14,15,16].
Although NICE guidelines recommend the utilization of scoring systems to determine antibiotic prescriptions, clinicians also need to manage patient’s (or their parents) ideas, concerns and expectations around prescribing, particularly in the context of recent increases in the incidence of streptococcal infections [27]. A recent study conducted in England revealed a notable rise in patient demand for antibiotics, increased from 65% to 84% between 2010 and 2017. Through corresponding analyses, a positive correlation was established between increasing demands on GP’s and their propensity to prescribe broad spectrum antibiotics [28]. Point of care testing in combination with clinical decision making has the potential to significantly improve antimicrobial stewardship by reassuring patients that antibiotics are not required, as shown in the patient survey carried out as part of this study.
The need for a more systematic and accurate process for the diagnosis and management of suspected streptococcal throat infection was highlighted by the outbreak of invasive group A streptococcal infection in the UK in the autumn and winter of 2022/2023 [27]. During that season there were significant increases in children presenting with not only non-invasive group A strep infections (tonsillitis and scarlet fever) but invasive infections too with several reported deaths. According to the UK Health and Security Agency, a total of 58,972 cases of scarlet fever were reported from week 37 to week 24 of that season (2022 to 2023) in England, with a pre-Christmas peak of 10,069 cases in week 49. This compares with an average of 12,906 cases (range 1,296 to 28,303) for this same time-period (weeks 37 to 24) in the previous 5 years [29]. This increase in primary care notifications for scarlet fever was accompanied by a similar increase in GP consultations for sore throat and high levels of anxiety.
As a result of the significant increases seen in the incidence of tonsillitis, scarlet fever and invasive group A streptococcal infection combined with national guidance to reduce the threshold for prescribing antibiotics [30], antibiotic prescriptions in primary care increased significantly with parental anxiety playing a significant role. At the peak of the above-mentioned outbreak, prescribing of phenoxymethylpenicillin was 6.1 times higher than in the equivalent time-period during previous years [31] and serious shortage protocols were required for several antibiotics to allow pharmacists to make substitutions where prescribed antibiotics were unavailable [32]). Suspected group A streptococcal infections can result in much higher prescribing rates than other bacterial infections, due to the need to treat close contacts, further highlighting the risks to supply chains and the need for accurate point of care testing.
The results presented here suggest that the addition of point of care testing to usual clinical assessment significantly reduces antibiotic prescribing and is popular with patients and medical staff but is associated with additional cost and consultation time. In association, earlier studies with the ID NOW testing platform have shown reduced antibiotic prescriptions (upto 9-fold) and use (33%) [12,24]. It was also shown that 30% of physicians changed the care plan for the patient following correct diagnosis [33]. Although the additional cost of the point of care testing equipment is £20 per tested patient, this is offset by lower costs for microbiology throat swabs (NHS tariff cost £12, [34], a potential lower rate of reattendance for patients managed with reassurance and symptom control at first contact and reduced antibiotic prescribing costs. Indeed, Nardi and colleagues showed that 50% less costs were incurred for antibiotics following implementation of molecular POCT [12]. The list prices including dispensing costs in the England as of February 2024 are below:
Phenoxymethylpenicillin suspension £23.32 for 7 days, £30.67 for 10 days
Phenoxymethylpenicillin tablets £5.33 for 7 days, £7.17 for 10 days
Clarithromycin suspension £11.62 for 10 days
Clarithromycin tablets £3.28 for 7 days and £5.19 for 10 days
The 65% reduction in immediate or deferred prescriptions seen in the project reflects current clinical practice in the study setting, where there a Centor score of 2 will usually result in a deferred prescription after a discussion with patients, given high residual anxiety around group A streptococcal infections. Applying the reinstated NICE guidance [17] with a higher threshold of 3 or 4 for antibiotic prescribing would result in a 55% reduction in antibiotic prescribing.
These reductions in antimicrobial prescribing would be very beneficial during future streptococcal outbreaks as seen in 2022/3 when many pharmacies were unable to supply antibiotics due to unprecedented numbers of prescriptions for possible cases of streptococcal infection and their contacts [31]. Better targeting of antimicrobials to patients most in need is also a key component of attempts to reduce antimicrobial resistance, and this study suggests that point of care testing may have a significant role to play. In England in 2022, 2,896,095 prescriptions were issued for phenoxymethylpenicillin [35], the majority of which will have been for sore throat. Assuming that these were all prescribed according to NICE guidance, if the results in the project were replicated, the addition of point of care testing to usual care would be expected to reduce this by up to 54.7%.
In addition, where patients who choose to access local emergency departments for sore throat, each attendance costs £152.00 (D. Chant, personal communication, February 29, 2024). This suggests that the system costs of reduced return consultations in primary care, patient and vulnerable contact antibiotic prescribing, microbiological swab testing and potential reductions in attendances to urgent and unscheduled care will balance out the increase in consultation time and consumable costs at the first clinical contact. Additional benefits would also be expected from rapid assessment of cases in terms of limiting outbreaks through early identification and isolation of cases, and reduced time off work and school for patients and their caregivers, although this was not assessed in this study.
The successful inclusion of a community pharmacy in this project, also suggests that community pharmacists can effectively provide extra capacity in managing acute respiratory infections, either as a regular service or as surge capacity in epidemics as seen in the UK in winter 2022/3. The recent advent of the Pharmacy First scheme [36], provides a dedicated minor illness service that could be expanded to incorporate this service.
Limitations of the project described here include the lack of a control group. This was a quality improvement project rather than a clinical trial and used an intervention at the point where a decision had been made by the treating clinician to use either a deferred or immediate prescription, rather than patients being allocated to control or intervention at the point of entry into the primary care assessment pathway. Consultation durations for both POC and usual care pathways were longer than expected, which may reflect the fact that the majority of these consultations in this study were undertaken by nurse practitioners or primary care paramedics, rather than doctors, who tend to have shorter appointments. Further work to look at work flow aspects of this care pathway would be useful to further explore the economic impact of POC testing.
Comparisons with previous years data are difficult, as the incidence of streptococcal throat infections varies greatly year by year, making comparison of antibiotic prescribing rates between winter 2023/4 and 2022/3 unreliable. Although it would be possible to compare prescribing rates with a neighbouring Primary Care Network with similar demographics, the relatively small number of patients (160 in this study) will make statistically significant comparisons difficult to obtain. Similarly, it has not been possible to identify changes in terms of re-consultation or use of secondary care services for the same reasons.
This project will continue beyond the end of February 2024 to collect more data, allowing the collection of a larger data set, and facilitating comparison of patients managed with or without POC testing and also allowing subgroup analysis of patients with different Centor scores to determine the correlation between Centor score and POC result. The data presented here do suggest that the POC test result is in line with Centor predictions, but the sample size for subgroups is small. In addition, we intend to look in future at the relationship between Centor score, Fever Pain score [37] and POC test results.
Although this project took place in 3 GP practices and a community pharmacy, the population of Seaton and Axminster has a relatively low proportion of deprived and ethnic minority patients and is semi-rural with the nearest acute hospital 23 miles away, with relatively poor transport links. As a result, locality-based interventions may be more effective due to limited choice of accessible alternative providers. Whether these results would be seen in a more diverse metropolitan population is unclear, but the inclusion of community pharmacies does suggest that in urban areas the additional capacity they might offer may be a valuable adjunct to current services and reduce demand on emergency department and out of hours services. Further studies in other settings would shed more light on this, and the introduction of Pharmacy First will offer the opportunity to study this in more detail.
5. Conclusions
Streptococcal throat infections cause significant morbidity and mortality and are responsible for large numbers of antibiotic prescriptions in primary care, while existing clinical judgement and diagnostic support tools have poor sensitivity and specificity. The results of this project demonstrate that point of care testing has the potential to significantly improve the accuracy of diagnosis and thus reduce unnecessary antibiotic prescribing. In addition, the ease of use in non-medical settings offers potential to significantly expand the provision of community based acute respiratory infection services. The use of this technology in routine practice is popular with patients and staff but does increase consultation times by around 7 minutes.
Supplementary Materials
Figure 1: Patient flow and clinical management. Figure 2: Comparisons of Centor score, age and molecular test result. Figure 3: Rating of Available Molecular Point-of-Care Testing for Strep A in Primary Care Practices Figure 4: Perceptions of primary practice staff members regarding molecular POC testing for cases involving sore throat. Table 1: Comparison of Centor score grading and outcome of Strep A testing using the ID NOW TM platform.
Author Contributions
This study was designed and conducted by R.D. and colleagues at Townsend House Medical Centre, United Kingdom. Conceptualization, Methodology, Project Administration, Funding Acquisition, Investigation, R.D and K.B. software, validation, formal analysis, investigation, resources, Data curation and analysis, R.D and E.M. Original draft preparation, editing and review of manuscript R.D and E.M. All authors have read and agreed to the published version of the manuscript.
Funding
Dr Daniels: staff and patients at Townsend House Medical Centre received no other financial support for the research, authorship, and/or publication of this article. Consumables were provided by the Southwest Peninsula Pathology Network supplied at a discounted price by Abbott Rapid Diagnostics Limited.
Rights retention
For the purpose of open access, the author has applied a Creative Commons Attribution (CC BY) licence to any Author Accepted Manuscript version arising’.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the fact that this was a service evaluation project which used the ID NOW equipment in a clinical environment, which is fully licensed for this purpose. As there were no perceived risks to patients this protocol was not submitted to a Research Ethics Committee. No additional swab was taken from patients. Only the device used to perform the test is different. The technology of this device is already validated, and our study is not a performance study. There was, therefore, no impact on the quality of the diagnosis itself. The study complied with the General Data Protection Regulation (GDPR). The processing of the personal data of participants was minimized by making use of a unique participant study number only on all study documents and any electronic database(s). All documents were stored securely and only accessible by study staff and authorized personnel. The study staff safeguarded the privacy of participants’ personal data.
Informed Consent Statement
All participants involved in this study provided oral informed consent.
Data Availability Statement
The data used in this study are not publicly available due to data privacy restrictions on other health-related issues of the participating individuals.
Acknowledgments
We would like to thank the patients, clinical, pharmaceutical and administrative staff who participated in the study. We would also like to thank David Gibbs, Roanna George and Sarah-Jayne Heard and their colleagues at the Southwest Pathology Network for their advice and financial support.
Conflicts of Interest
Abbott Rapid Diagnostics had no role in the design of the study, collection, analysis or interpretation of data, or the decision to publish the results. None of the authors had any conflicts of interest.
References
- Mantzourani, E., Wasag, D., Cannings-John, R., Ahmed, H., & Evans, A. (2022). Characteristics of the sore throat test and treat service in community pharmacies (STREP) in Wales: cross-sectional analysis of 11 304 consultations using anonymized electronic pharmacy records. The Journal of antimicrobial chemotherapy, 78(1), 84–92. [CrossRef]
- Worrall G. J. (2007). Acute sore throat. Canadian family physician Medecin de famille canadien, 53(11), 1961–1962.
- Bower J. R. (2012), Pharyngitis. Netter’s Infectious Diseases. 177–182. [CrossRef]
- Overview: Sore Throat (acute): Antimicrobial prescribing: Guidance NICE. Available at: https://www.nice.org.uk/guidance/ng84 (Accessed: 01 March 2024).
- Management-of-contacts-of-invasive-group-A- ... Available at: https://assets.publishing.service.gov.uk/media/64071ec5d3bf7f25fa417a91/Management-of-contacts-of-invasive-group-a-streptococcus.pdf (Accessed: 09 March 2024).
- Group A streptococccus in children. NICE Guidelines 2022. https://www.england.nhs.uk/wp-content/uploads/2022/12/PRN00080-Interim-clinical-guidance-summary-for-case-management-for-prophylaxis-please-refer-to-community-conta.pdf.
- Oliver J, Malliya Wadu E, Pierse N, Moreland NJ, Williamson DA, Baker MG. Group A Streptococcus pharyngitis and pharyngeal carriage: a meta-analysis. PLoS neglected tropical diseases. 2018 Mar 19;12(3):e0006335.
- Gulliford, M. C. , Moore, M. V., Little, P., Hay, A. D., Fox, R., Prevost, A. T., Juszczyk, D., Charlton, J., & Ashworth, M. (2016). Safety of reduced antibiotic prescribing for self-limiting respiratory tract infections in primary care: cohort study using electronic health records. BMJ (Clinical research ed.), 354, i3410. [CrossRef]
- Thompson TZ, McMullen AR. Group A Streptococcus Testing in Pediatrics: the Move to Point-of-Care Molecular Testing. J Clin Microbiol. 2020 May 26;58(6):e01494-19. [CrossRef] [PubMed] [PubMed Central]
- Centor RM; Witherspoon JM; Dalton HP; Brody CE; Link K (1981). "The diagnosis of strep throat in adults in the emergency room". Medical Decision Making. 1 (3): 239–246. [CrossRef]
- Willis, B. H., Coomar, D., & Baragilly, M. (2020). Comparison of Centor and McIsaac scores in primary care: a meta-analysis over multiple thresholds. The British journal of general practice: the journal of the Royal College of General Practitioners, 70(693), e245–e254. [CrossRef]
- Nardi, S, Carolis L, Iannini R, De Sandro MV, Solito G, Calafatti M, Gizzi C. (2022). Usefulness of rapid molecular tests in pediatric respiratory tract infections Ital J Pediatr. 48(1):21. [CrossRef]
- Varzgalien, L, Heerey A, Cox C, McGuinness T, McGuire G, Cals JW, O'Shea E, Kelly M. (2017) Point-of-care testing in primary care: needs and attitudes of Irish GPs. BJGP Open. 15;1(4):bjgpopen17X101229. [CrossRef]
- Wolf F, Matthes A, Markwart R, Bleidorn J. 2022. Perspectives of physicians and medical assistants on the implementation of NAAT-based point-of-care testing for SARS-CoV-2 in primary care in Germany. Z Evid Fortbild Qual Gesundhwes. 2022 Dec;175:43-49. [CrossRef]
- Matthes A, Wolf F, Bleidorn J, Markwart R. 2022. "It Was Very Comforting to Find Out Right Away." - Patient Perspectives on Point-of-Care Molecular SARS-CoV-2 Testing in Primary Care. Patient Prefer Adherence. 10;16:2031-2039. [CrossRef]
- Daniels R., Cottin J., Khanafer N. (2023). Point-of-Care Testing for SARS-CoV-2: A Prospective Study in a Primary Health Centre. Diagnostics (Basel) 28;13(11):1888. [CrossRef]
- NHS England. (2023). Group A Streptococcus: reinstatement of NICE sore throat guidance for children and young people and withdrawal of NHS England interim guidance. Publication reference: PR00247. https://www.england.nhs.uk/wp-content/uploads/2022/12/PRN00247_Group-A-Streptococcus-reinstatement-of-NICE-sore-throat-guidance-for-children-and-young-people-and-wi.pdf.
- North & East Decon Formulary and Referral. Upper respiratory tract infections. NICE CG69: Respiratory tract infections (self-limiting): prescribing antibiotics. https://northeast.devonformularyguidance.nhs.uk/formulary/chapters/5-infections/upper-respiratory-tract-infections.
- ID NOWTM Strep A2. Available at: https://dam.abbott.com/en-gb/panbio/ID-NOW-Strep-A%202-Product-Sheet-EME-English.pdf.
- Thompson T.Z and A.R. McMullen. (2020). Group A Streptococcus Testing in Pediatrics: the Move to Point-of-Care Molecular Testing. J. Clin Microbiology. 58:6. [CrossRef]
- Online surveys. Available at: https://www.onlinesurveys.ac.uk/ (Accessed: 06 April 2024).
- Burdino E, Cerutti F, Milia MG, Allice T, Gregori G, Aprà F, De Iaco F, Aluffi E, Micca G, Ghisetti V. 2022. Fast and reliable real life data on COVID-19 triaging with ID NOW. J Clin Virol Plus. 2(1):100065. [CrossRef]
- Barnacle JR, Houston H, Baltas I, Takata J, Kavallieros K, Vaughan N, Amin AK, Aali SA, Moore K, Milner P, Gupta Wright A, John L. 2022. Diagnostic accuracy of the Abbott ID NOW SARS-CoV-2 rapid test for the triage of acute medical admissions. J Hosp Infect. 123:92-99. [CrossRef]
- Trabattoni E, Le V, Pilmis B, Pean de Ponfilly G, Caisso C, Couzigou C, Vidal B, Mizrahi A, Ganansia O, Le Monnier A, Lina B, Nguyen Van JC. Implementation of Alere i Influenza A & B point of care test for the diagnosis of influenza in an ED. Am J Emerg Med. 2018 Jun;36(6):916-921. Epub 2017 Oct 18. [CrossRef]
- O'Connell S, Conlan C, Reidy M, Stack C, Mulgrew A, Baruah J. The impact of point-of-care testing for influenza A and B on patient flow and management in a medical assessment unit of a general hospital. BMC Res Notes. 2020 Mar 10;13(1):143. [CrossRef]
- Wächtler H, Kaduszkiewicz H, Kuhnert O, Malottki KA, Maaß S, Hedderich J, Wiese B, Donner-Banzhoff N, Hansmann-Wiest J (2023). Influence of a guideline or an additional rapid strep test on antibiotic prescriptions for sore throat: the cluster randomized controlled trial of HALS (Hals und Antibiotika Leitlinien Strategien). BMC Prim Care. 24(1):75. [CrossRef]
- Guy, R. et al. (2023) ‘Increase in invasive group a streptococcal infection notifications, England, 2022’, Eurosurveillance, 28(1). [CrossRef]
- Allen T, Gyrd-Hansen D, Kristensen SR, Oxholm AS, Pedersen LB, Pezzino M. Physicians under Pressure: Evidence from Antibiotics Prescribing in England. Med Decis Making. 2022 Apr;42(3):303-312. Epub 2022 Jan 12. [CrossRef] [PubMed] [PubMed Central]
- Group A streptococcal infections: 15th update on seasonal activity in England (no date) GOV.UK. Available at: https://www.gov.uk/government/publications/group-a-streptococcal-infections-activity-during-the-2022-to-2023-season/group-a-streptococcal-infections-15th-update-on-seasonal-activity-in-england (Accessed: 09 March 2024).
- Group A streptococcus in children. Available at: https://www.england.nhs.uk/wp-content/uploads/2022/12/PRN00058-group-a-streptococcus-in-children-december-2022.pdf (Accessed: 09 March 2024).
- Espaur-Report-2022-TO-2023.PDF. Available at: https://assets.publishing.service.gov.uk/media/65cf498ee1bdec001132225c/ESPAUR-report-2022-to-2023.pdf (Accessed: 09 March 2024).
- Further 5 serious shortage protocols (ssps) phenoxymethylpenicillin products to enable the supply of alternative antibiotics, RPS brandmark. Available at: https://www.rpharms.com/publications/pharmacy-alerts/details/Further-5-Serious-Shortage-Protocols-SSPs-phenoxymethylpenicillin-products-to-enable-the-supply-of-alternative-antibiotics (Accessed: 09 March 2024).
- Gunnarsson RK, Orda U, Elliott B, Heal C, Gorges H, Glasziou P, Del Mar C. (2021). Improving antibiotics targeting using PCR point-of-care testing for group A streptococci in patients with uncomplicated acute sore throat. Aust J Gen Pract. 50(1-2):76-83. [CrossRef]
- NIHR. Available at: https://www.nihr.ac.uk/search-results.htm?search=tariff (Accessed: 04 March 2024).
- Mikulic, M. (2023) Top antibacterial drugs dispensed in England by items 2022, Statista. Available at: https://www.statista.com/statistics/377978/top-ten-antibacterial-drugs-dispensed-by-item-in-england/ (Accessed: 09 March 2024.
- NHS choices. Available at: https://www.england.nhs.uk/primary-care/pharmacy/pharmacy-first/ (Accessed: 01 March 2024).
- Seeley, A., Fanshawe, T., Voysey, M., Hay, A., Moore, M., & Hayward, G. (2021). Diagnostic accuracy of Fever-PAIN and Centor criteria for bacterial throat infection in adults with sore throat: a secondary analysis of a randomised controlled trial. BJGP open, 5(6), BJGPO.2021.0122. [CrossRef]
Figure 1.
Patient flow and clinical management. *Patients were offered a choice of initial consultation at either GP surgery or high street pharmacy, according to patient choice.
Figure 1.
Patient flow and clinical management. *Patients were offered a choice of initial consultation at either GP surgery or high street pharmacy, according to patient choice.
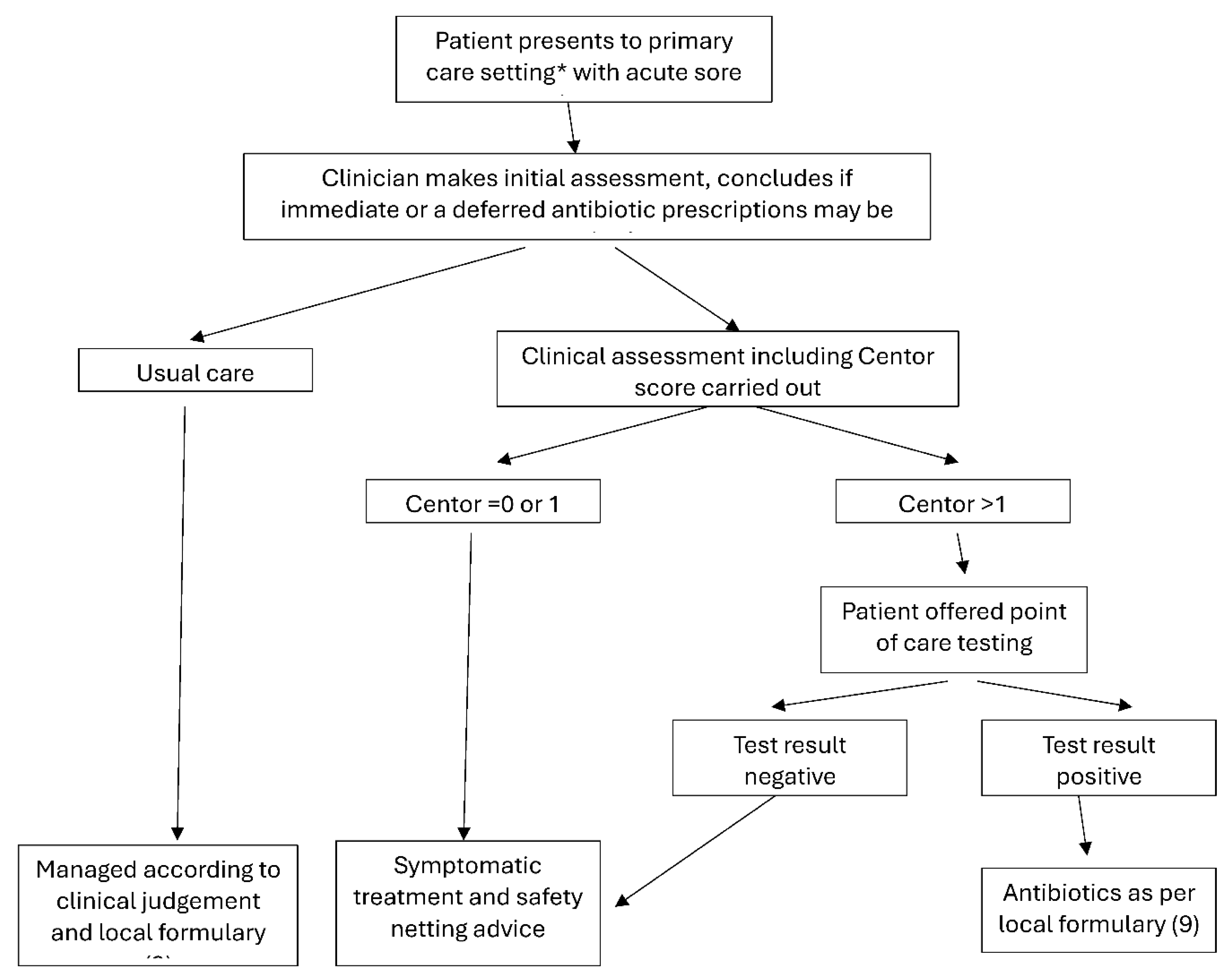
Figure 2.
Comparisons of Centor score, age and molecular test result. (A) Distribution of Centor score according to age (2 months to 86 years). Statistical significant following t-tests between the individual groups. (B) Comparison of positive and negative molecular Strep A results according to the Centor Score. (C) Number of patients with presenting with either Centor scores 2,3 or 4 and their corresponding positive and negative molecular test result for a Strep A infection.
Figure 2.
Comparisons of Centor score, age and molecular test result. (A) Distribution of Centor score according to age (2 months to 86 years). Statistical significant following t-tests between the individual groups. (B) Comparison of positive and negative molecular Strep A results according to the Centor Score. (C) Number of patients with presenting with either Centor scores 2,3 or 4 and their corresponding positive and negative molecular test result for a Strep A infection.
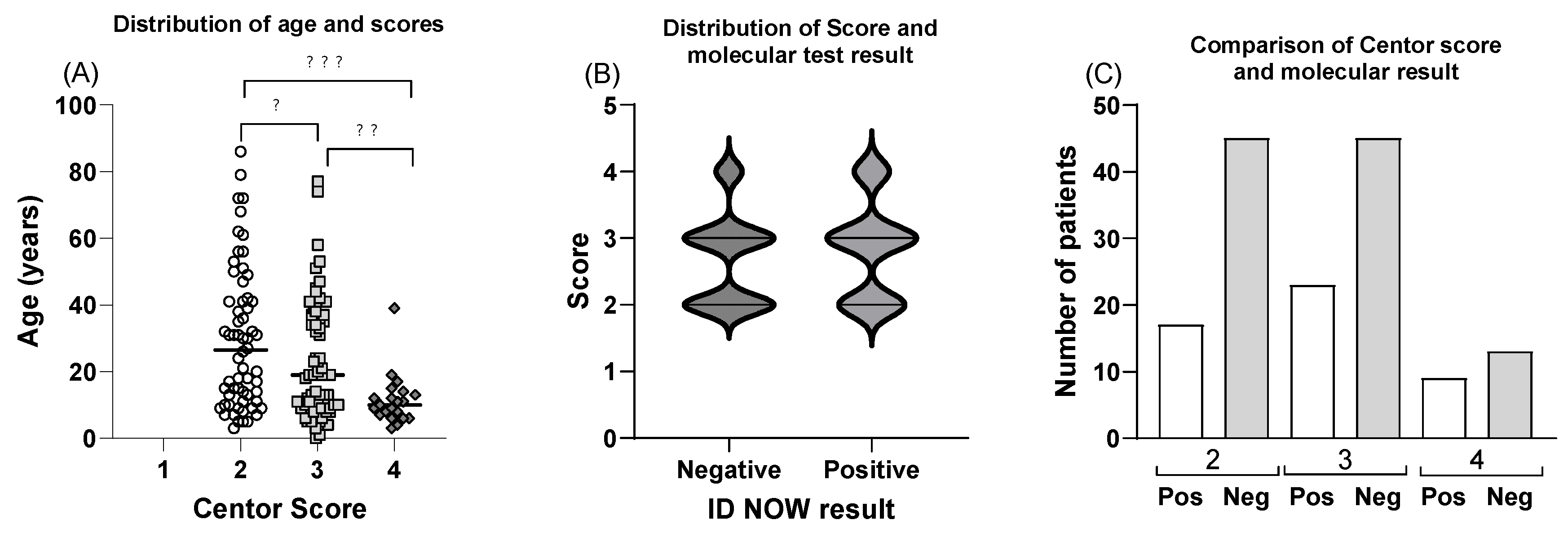
Figure 3.
Rating of Available Molecular Point-of-Care Testing for Strep A in Primary Care Practices. Patients that were offered and agreed to have a molecular test for Strep A at the practice office further participated in an on-line anonymous survey. Following a Likert format, patients rated their responses from full agreement to full disagreement or not applicable.
Figure 3.
Rating of Available Molecular Point-of-Care Testing for Strep A in Primary Care Practices. Patients that were offered and agreed to have a molecular test for Strep A at the practice office further participated in an on-line anonymous survey. Following a Likert format, patients rated their responses from full agreement to full disagreement or not applicable.
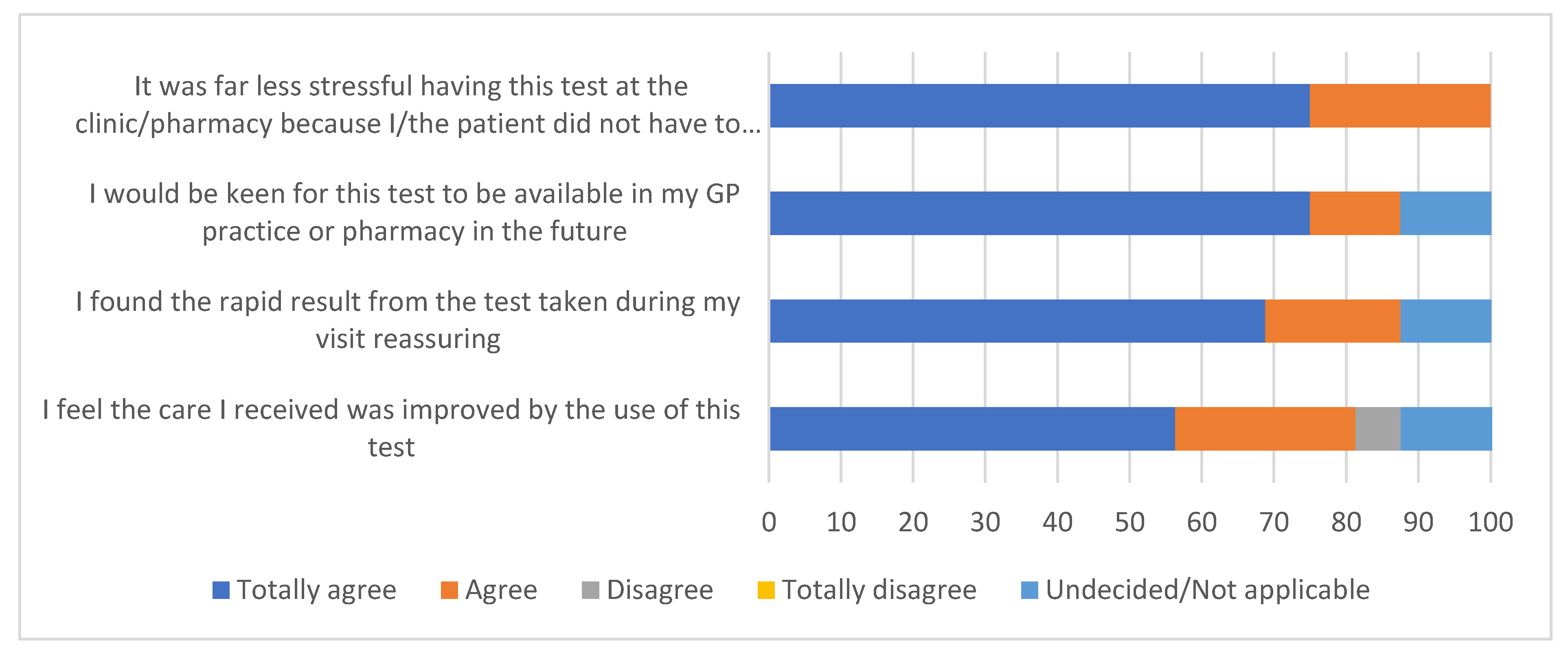
Figure 4.
Perceptions of primary practice staff members regarding molecular POC testing for cases involving sore throat. From the participating four practices in Devon, all staff members completed an on-line questionnaire which is presented using a Likert scale ranging from agreement to disagreement.
Figure 4.
Perceptions of primary practice staff members regarding molecular POC testing for cases involving sore throat. From the participating four practices in Devon, all staff members completed an on-line questionnaire which is presented using a Likert scale ranging from agreement to disagreement.
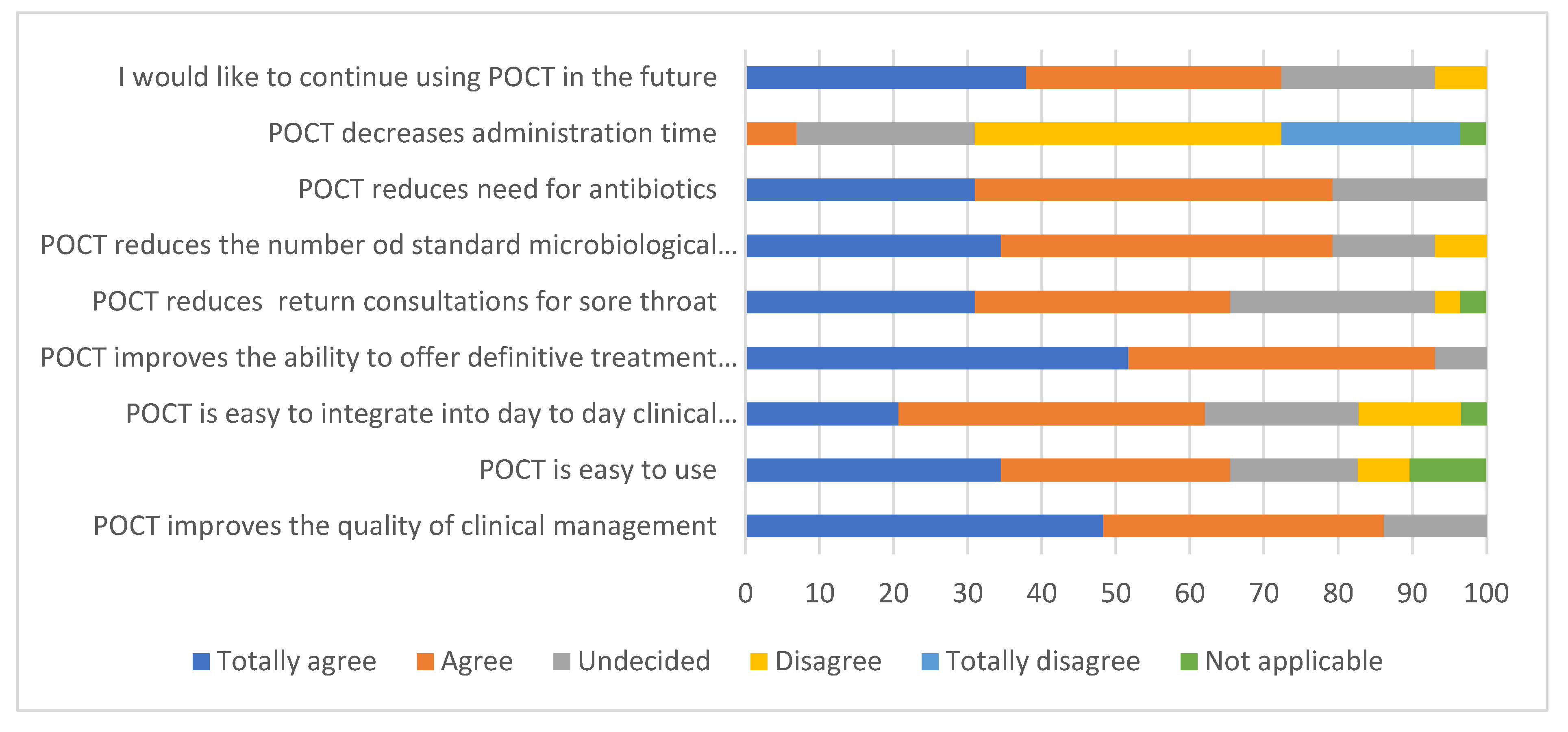

Table 1.
Comparison of Centor score grading and outcome of Strep A testing using the ID NOWTMplatform. Following a clinical assessment for sore throat symptoms, oral swabs from 144 patients underwent further molecular diagnosis. Data shows the number of positive POCT results compared to those testing negative and the overall percentage of positive individuals per score.
Table 1.
Comparison of Centor score grading and outcome of Strep A testing using the ID NOWTMplatform. Following a clinical assessment for sore throat symptoms, oral swabs from 144 patients underwent further molecular diagnosis. Data shows the number of positive POCT results compared to those testing negative and the overall percentage of positive individuals per score.
| Centor Score | POCT Results: Positive | Negative | % Positive (95% confidence interval) |
|---|---|---|---|
| 2 | 15 | 51 | 22.73 (14.18 to 34.28) |
| 3 | 20 | 33 | 37.74 (25.91 to 51.22) |
| 4 | 15 | 10 | 60.00 (40.70 to 76.64) |
| 3 or 4 | 35 | 43 | 44.87 (34.33 to 55.89) |
| Total | 50 | 94 | 34.72 (27.42 to 42.81) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



