Submitted:
22 April 2024
Posted:
23 April 2024
You are already at the latest version
Abstract
TAFRO syndrome (TS) is a rare variant of idiopathic multicentric Castleman's disease (iMCD) characterized by a confluence of symptoms: thrombocytopenia (T), anasarca (A), fever (F), reticulin myelofibrosis (R), and organomegaly (O). First described in Japan in 2010, the pathogenesis of the disease remains unclear. Due to its heterogeneous presentation and potential life-threatening delays in diagnosis, precise diagnosis is essential. According to the literature, no specific imaging modality has been recommended for the work-up of patients with suspected TS. Here, we report a case of TS and its management using 18F-FDG-PET/CT imaging as an attractive complementary diagnostic tool.
Keywords:
TAFRO syndrome
; multicentric Castleman disease
; iMCD
; 18F-FDG-PET/CT
Figure 1.
18F-FDG-PET/CT of the patient: (A) Maximum Intensity Projection image (MIP) of the chest, upper and lower abdomen respectively (left to the right), (B) PET images, (C) fused PET/CT images, (D) CT-images. A 44-year-old Mauritanian woman without significative pre-existing medical and recent traveling history presented with tiredness, and febrile non-bloody diarrhoea for 3 weeks. No other complaints. Physical examination revealed left cervical adenopathy, anasarca, and mild splenomegaly. Laboratory tests showed non-regenerative anaemia (5.5g/L), hypoplakettosis (23,000/µL), elevated serum concentration of C-reactive protein (121mg/dL), direct Coombs positive without acute haemolysis. Extensive work-up for infections (viral, bacterial, and fungi) and autoimmune diseases were also negatives. A thoracoabdominal scanner was realized and showed slightly enlarged cervicothoracic adenopathy (large white arrow), hepatosplenomegaly (head white arrow), and ascites (small white arrow). The bone marrow was initially explored via a sternal marrow puncture showing a dry tap, with inconclusive results (Figure 2A). An ensuing bone marrow biopsy was performed and exposed reticulin myelofibrosis, and numerous megakaryocytes bordering dilated sinusoids (Figure 2B). Metabolic imaging with 18F-FDG-PET/CT was achieved to assess underlying causes and identify the most active lymph node for biopsy. MIP (A) and fused images show increased and diffuse FDG uptake in the cervicothoracic lymph nodes (large yellow arrow), spleen (yellow head arrow) ascites (small yellow arrow), and vertebral medulla (orange arrow). Lymph node biopsy revealed rare follicles, atrophy of germinal centers, proliferation, hyperplasia of blood vessels, and plasma cells suggestive of Castleman’s disease (Figure 2C-D). Tests for herpes human virus-6 (HHV-6), HHV-8, and human immunodeficiency virus (HIV) were negative. These results, alongside the biological, CT-images and 18F-FDG PET/CT findings, suggest a diagnosis of TAFRO syndrome (TS). She was successfully treated with corticosteroid and immunotherapy (Interleukin-6 inhibitors) with a clinical and biological improvement. First described by Takai et al. in 2010, TAFRO syndrome (TS) is a rare inflammatory lymphoproliferative disease characterized by a highly heterogeneous clinical presentation and potential life-threatening implications [1]. As of now, the exact pathogenesis remains unclear, and it is regarded as a distinct clinicopathological variant of idiopathic multicentric Castleman’s disease (iMCD) [2,3,4]. While the majority of reported TS cases have originated in Japan, the syndrome has increasingly been recognized in non-Asian patients worldwide [5]. According to existing literature, no specific imaging modality has been universally recommended for the evaluation of suspected iMCD or TS cases. Typically, computerized tomography (CT-scan) reveals nonspecific multiple lymphadenopathies that may indicate other differential diagnoses such as lymphoproliferative disorders or granulomatosis [6]. Consequently, determining the highest metabolic activity using 2-[18F]-fluoro-2-deoxy-D-glucose positron emission tomography combined with computed tomography (18F-FDG-PET/CT) in enlarged lymph nodes potentially facilitates the identification of suitable biopsy targets, leading to earlier diagnosis. Moreover, certain disease features like myelofibrosis are challenging to detect on CT imaging alone, but 18F-FDG-PET/CT can demonstrate diffuse uptake in the marrow (orange arrow), capturing key findings of TS [7,8]. Additionally, uptake in hepatosplenomegaly provides supplementary information by reflecting sites of secondary hematopoiesis, aiding in diagnosis [7]. Identifying the cause of ascites poses a challenge due to its association with various pathologies, ranging from non-malignant conditions like chronic liver disease and heart failure to malignant neoplasms [9]. In our case, observing hypermetabolism in ascites is particularly intriguing. While ascites are generally present in all TS cases, different studies have described varying sensitivity and specificity values of 18F-FDG-PET/CT for its characterization [10,11]. Furthermore, combining metabolic imaging with tumor biomarkers such as interleukin-6 (IL-6) and vascular endothelial growth factor (VEGF) levels in effusions and serum can provide valuable insights for investigating TS [12,13,14]. To date, only a few TS cases have been reported, and the utilization of 18F-FDG-PET/CT as a complementary diagnostic tool remains limited. Given the heterogeneous presentation of the disease and potential life-threatening delays in diagnosis, accurate diagnosis is crucial to initiate appropriate treatment. In conclusion, 18F-FDG-PET/CT holds promise as a complementary tool for providing characteristic findings of TS. We suggest considering the diagnosis when a combination of PET/CT results, such as thrombocytopenia, fever of unknown origin, diffuse FDG uptake in the bone marrow, hepatosplenomegaly with elevated splenic FDG uptake, and lymphadenopathy with increased FDG uptake, is observed in a patient.
Figure 1.
18F-FDG-PET/CT of the patient: (A) Maximum Intensity Projection image (MIP) of the chest, upper and lower abdomen respectively (left to the right), (B) PET images, (C) fused PET/CT images, (D) CT-images. A 44-year-old Mauritanian woman without significative pre-existing medical and recent traveling history presented with tiredness, and febrile non-bloody diarrhoea for 3 weeks. No other complaints. Physical examination revealed left cervical adenopathy, anasarca, and mild splenomegaly. Laboratory tests showed non-regenerative anaemia (5.5g/L), hypoplakettosis (23,000/µL), elevated serum concentration of C-reactive protein (121mg/dL), direct Coombs positive without acute haemolysis. Extensive work-up for infections (viral, bacterial, and fungi) and autoimmune diseases were also negatives. A thoracoabdominal scanner was realized and showed slightly enlarged cervicothoracic adenopathy (large white arrow), hepatosplenomegaly (head white arrow), and ascites (small white arrow). The bone marrow was initially explored via a sternal marrow puncture showing a dry tap, with inconclusive results (Figure 2A). An ensuing bone marrow biopsy was performed and exposed reticulin myelofibrosis, and numerous megakaryocytes bordering dilated sinusoids (Figure 2B). Metabolic imaging with 18F-FDG-PET/CT was achieved to assess underlying causes and identify the most active lymph node for biopsy. MIP (A) and fused images show increased and diffuse FDG uptake in the cervicothoracic lymph nodes (large yellow arrow), spleen (yellow head arrow) ascites (small yellow arrow), and vertebral medulla (orange arrow). Lymph node biopsy revealed rare follicles, atrophy of germinal centers, proliferation, hyperplasia of blood vessels, and plasma cells suggestive of Castleman’s disease (Figure 2C-D). Tests for herpes human virus-6 (HHV-6), HHV-8, and human immunodeficiency virus (HIV) were negative. These results, alongside the biological, CT-images and 18F-FDG PET/CT findings, suggest a diagnosis of TAFRO syndrome (TS). She was successfully treated with corticosteroid and immunotherapy (Interleukin-6 inhibitors) with a clinical and biological improvement. First described by Takai et al. in 2010, TAFRO syndrome (TS) is a rare inflammatory lymphoproliferative disease characterized by a highly heterogeneous clinical presentation and potential life-threatening implications [1]. As of now, the exact pathogenesis remains unclear, and it is regarded as a distinct clinicopathological variant of idiopathic multicentric Castleman’s disease (iMCD) [2,3,4]. While the majority of reported TS cases have originated in Japan, the syndrome has increasingly been recognized in non-Asian patients worldwide [5]. According to existing literature, no specific imaging modality has been universally recommended for the evaluation of suspected iMCD or TS cases. Typically, computerized tomography (CT-scan) reveals nonspecific multiple lymphadenopathies that may indicate other differential diagnoses such as lymphoproliferative disorders or granulomatosis [6]. Consequently, determining the highest metabolic activity using 2-[18F]-fluoro-2-deoxy-D-glucose positron emission tomography combined with computed tomography (18F-FDG-PET/CT) in enlarged lymph nodes potentially facilitates the identification of suitable biopsy targets, leading to earlier diagnosis. Moreover, certain disease features like myelofibrosis are challenging to detect on CT imaging alone, but 18F-FDG-PET/CT can demonstrate diffuse uptake in the marrow (orange arrow), capturing key findings of TS [7,8]. Additionally, uptake in hepatosplenomegaly provides supplementary information by reflecting sites of secondary hematopoiesis, aiding in diagnosis [7]. Identifying the cause of ascites poses a challenge due to its association with various pathologies, ranging from non-malignant conditions like chronic liver disease and heart failure to malignant neoplasms [9]. In our case, observing hypermetabolism in ascites is particularly intriguing. While ascites are generally present in all TS cases, different studies have described varying sensitivity and specificity values of 18F-FDG-PET/CT for its characterization [10,11]. Furthermore, combining metabolic imaging with tumor biomarkers such as interleukin-6 (IL-6) and vascular endothelial growth factor (VEGF) levels in effusions and serum can provide valuable insights for investigating TS [12,13,14]. To date, only a few TS cases have been reported, and the utilization of 18F-FDG-PET/CT as a complementary diagnostic tool remains limited. Given the heterogeneous presentation of the disease and potential life-threatening delays in diagnosis, accurate diagnosis is crucial to initiate appropriate treatment. In conclusion, 18F-FDG-PET/CT holds promise as a complementary tool for providing characteristic findings of TS. We suggest considering the diagnosis when a combination of PET/CT results, such as thrombocytopenia, fever of unknown origin, diffuse FDG uptake in the bone marrow, hepatosplenomegaly with elevated splenic FDG uptake, and lymphadenopathy with increased FDG uptake, is observed in a patient.
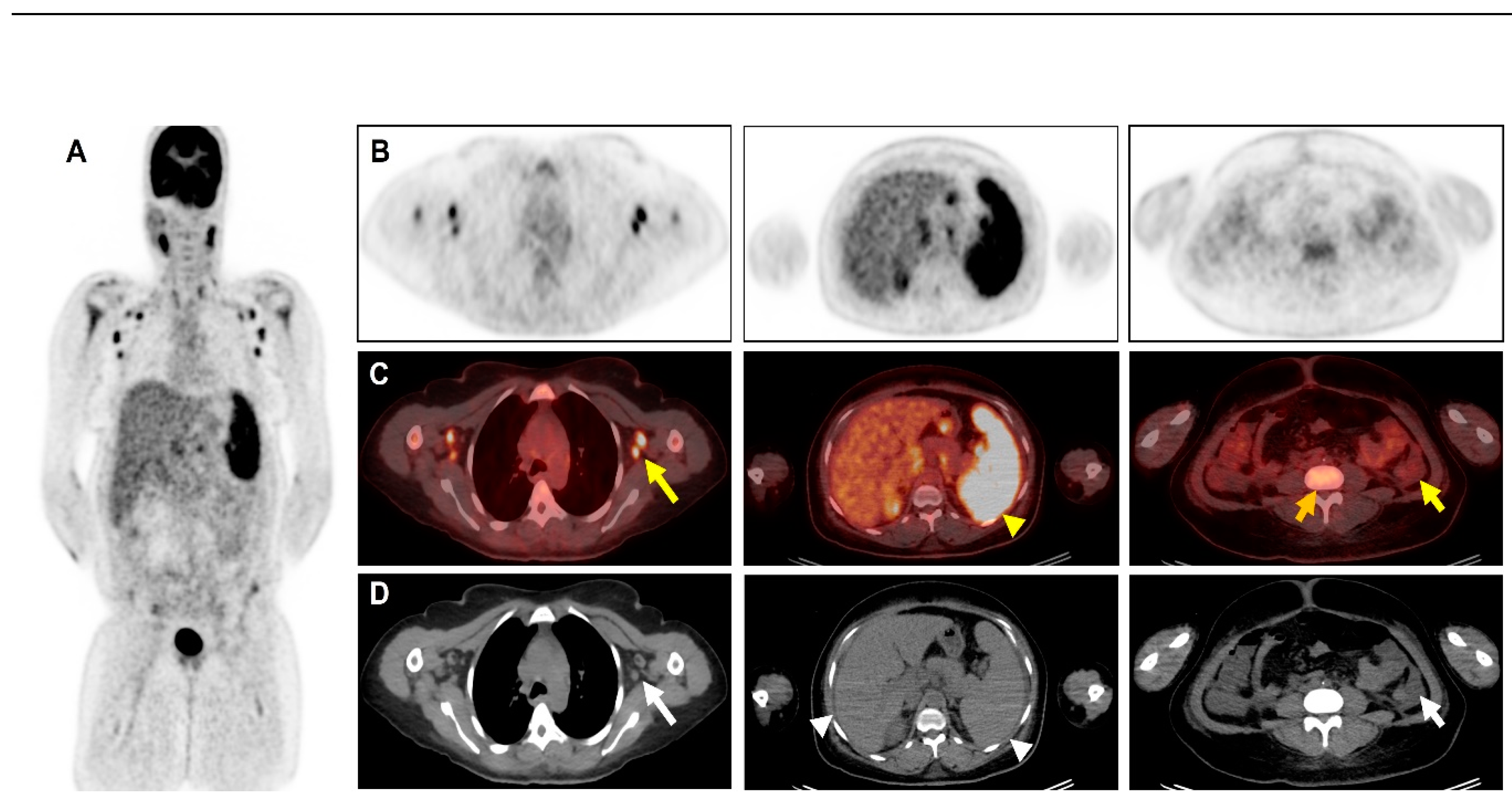
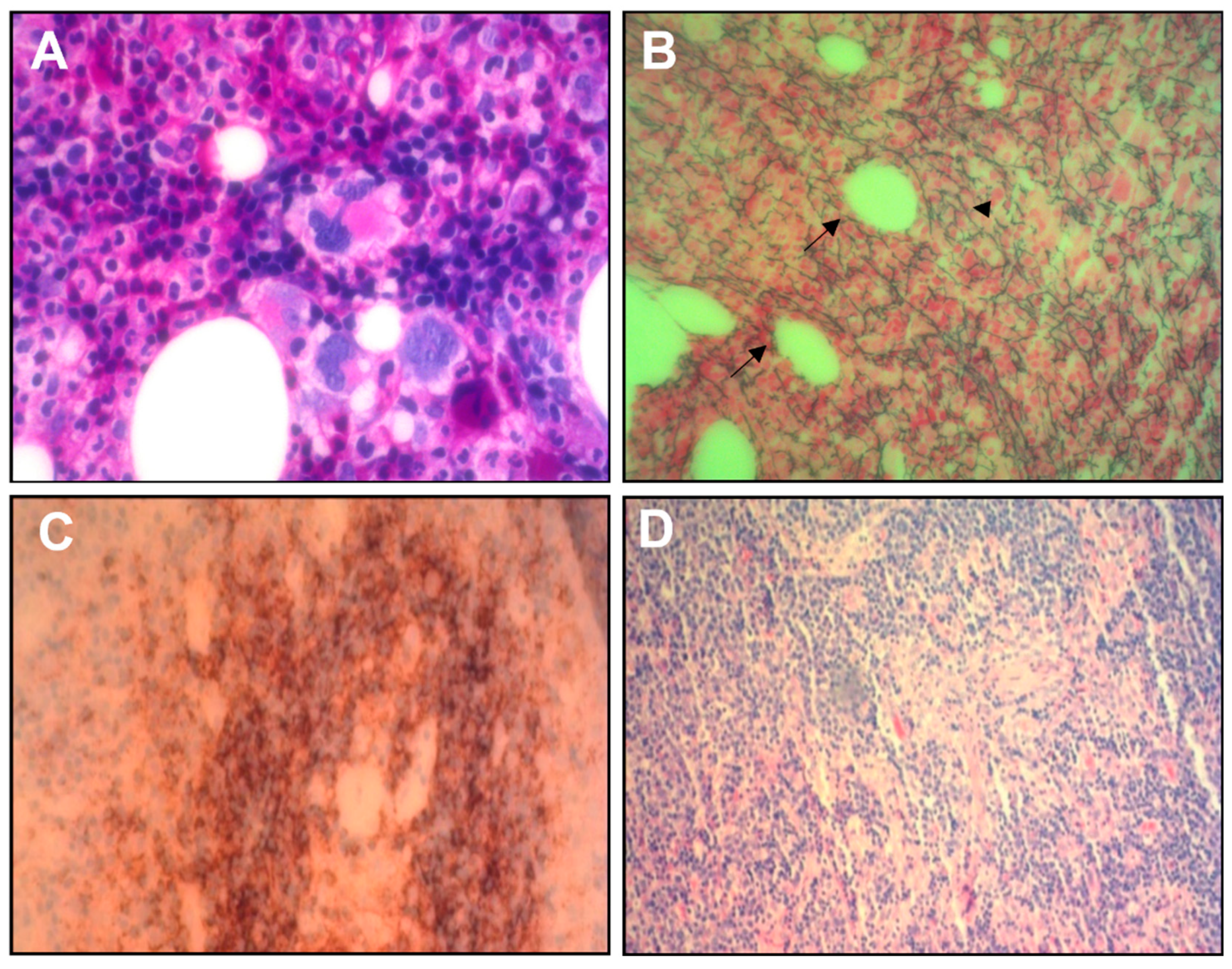
Figure 2.
(A) 100x hematoxylin- and eosin-stain of the marrow puncture showing a “dry tap” characterized by slightly hypercellular marrow with increased megakaryocytes. (B) Reticulin stain of bone marrow biopsy showed reticulin myelofibrosis (head arrow, green fibers), and numerous megakaryocytes bordering dilated sinusoids (arrow). Lymph node biopsy showed rare follicles, atrophy of germinal centers (C), proliferation, and hyperplasia of blood vessels (D).
Figure 2.
(A) 100x hematoxylin- and eosin-stain of the marrow puncture showing a “dry tap” characterized by slightly hypercellular marrow with increased megakaryocytes. (B) Reticulin stain of bone marrow biopsy showed reticulin myelofibrosis (head arrow, green fibers), and numerous megakaryocytes bordering dilated sinusoids (arrow). Lymph node biopsy showed rare follicles, atrophy of germinal centers (C), proliferation, and hyperplasia of blood vessels (D).
Funding
This research received no external funding.
Institutional Review Board Statement
This study did not receive ethical review and approval due to the nature of the research (case report).
Informed Consent Statement
Written informed consent was obtained from the patient. The consent form was obtained on 01.03.2024.
Data Availability Statement
The data used and analyzed in this study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Takai K, Nikkuni K, Shibuya H, Hashidate H. Thrombocytopenia with mild bone marrow fibrosis accompanied by fever, pleural effusion, ascites and hepatosplenomegaly. [Article in Japanese]. Rinsho Ketsueki 2010;51(5):320-5.
- Masaki Y, Kawabata H, Takai K, et al. Proposed diagnostic criteria, disease severity classification, and treatment strategy for TAFRO syndrome, 2015 version. Int J Hematol. 2016; 103:686–692. [CrossRef]
- Iwaki N, Fajgenbaum DC, Nabel CS, et al. Clinicopathologic analysis of TAFRO syndrome demonstrates a distinct subtype of HHV-8-negative multicentric Castleman disease. Am J Hematol. 2016;91(2):220–6. [CrossRef]
- Awano N, Inomata M, Sonoda Y, et al. A case of multicentric Castleman’s disease of mixed-type, which showed a constellation of symptoms, i.e., thrombocytopenia, anasarca, anemia, fever, myelofibrosis, and lymphadenopathy. J Clin Exp Hematol. 2013; 53:101–105.
- Coutier F, Meaux Ruault N, Crepin T, Bouiller K, Gil H, Humbert S, Bedgedjian I, Magy-Bertrand N. A comparison of TAFRO syndrome between Japanese and non-Japanese cases: a case report and literature review. Ann Hematol. 2018 Mar;97(3):401-407. [CrossRef]
- Kiguchi T, Sato C, Takai K, et al. CT findings in 11 patients with TAFRO syndrome: a variant of multicentric Castleman’s disease. Clin Radiol. 2017; 72:905. e1–905.e5. [CrossRef]
- Burrell SC, Fischman AJ. Myelofibrosis on F-18 FDG PET Imaging. Clin Nucl Med. 2005; 30:674. [CrossRef]
- Derlin T, Alchalby H, Bannas P, et al. Serial 18F-FDG PET for monitoring treatment response after allogeneic stem cell transplantation for myelofibrosis. J Nucl Med. 2016; 57:1556–1559. [CrossRef]
- Han N, Sun X, Qin C, Hassan Bakari K, Wu Z, Zhang Y, Lan X. Value of 18F-FDG PET/CT Combined With Tumor Markers in the Evaluation of Ascites. AJR Am J Roentgenol. 2018 May;210(5):1155-1163. [CrossRef]
- Zhang M, Jiang X, Zhang M, Xu H, Zhai G, Li B. The role of 18F-FDG PET/CT in the evaluation of ascites of undetermined origin. J Nucl Med 2009; 50:506–512. [CrossRef]
- Han N, Sun X, Qin C, Hassan Bakari K, Wu Z, Zhang Y, et al. Value of 18F-FDG PET/CT combined with tumor markers in the evaluation of Ascites. American Journal of Roentgenology. 2018;210(5):1155–63. doi:10.2214/ajr.17.18733. [CrossRef]
- Fajgenbaum, David C. Novel insights and therapeutic approaches in idiopathic multicentric Castleman disease. Blood, (), blood-2018-05-848671).
- Behnia F, Elojeimy S, Matesan M, Fajgenbaum DC. Potential value of FDG pet-CT in diagnosis and follow-up of TAFRO syndrome - annals of hematology [Internet]. Springer Berlin Heidelberg; 2016.
- Hotta M, Minamimoto R, Yashima A, Nakano M, Yamashita H. FDG PET/CT findings in TAFRO syndrome. Clinical Nuclear Medicine. 2018. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



