
Submitted:
12 April 2024
Posted:
15 April 2024
You are already at the latest version
Abstract
Background: Cardiovascular (CV) morbidity and mortality are many times higher in chronic kidney disease (CKD), as well as IgA nephropathy (IgAN), than in the general population. The occurrence of metabolic syndrome (MetS) and metabolic risk factors are independent risk factors for CV disease and renal progression. The study aimed to determine the prognostic role of metabolic profiles in a homogenous group of CKD patients.
Methods: One hundred and forty-five IgA nephropathy patients (92 male, 53 female, age 54.7 ± 13 years) with CKD stage 1-4 were investigated and followed for a median of 190 months. The composite (CV and renal) endpoints included all-cause mortality and any CV event such as stroke, myocardial infarction, revascularization (CV), end-stage renal disease, and renal replacement therapy (renal).
Results: Patients with MetS had significantly more endpoint events (16/27 patients vs. 15/98 patients, p = 0.001) compared to the nonMetS group. Of the secondary endpoints (CV or renal separately), the rate of the renal and CV endpoints was significantly higher in the MetS group (p = 0.001 and p = 0.029). The primary endpoint independent predictors of survival were dyslipidemia, eGFR, hemoglobin, urine albuminuria, and diabetes mellitus, as determined by Cox regression analysis. Independent predictors of secondary renal endpoint were dyslipidemia, hemoglobin, urine albumin, and eGFR. Predictors of secondary cardiovascular endpoints were gender, BMI, and diabetes. Kaplan-Meier curves showed significant differences in MetS and non-MetS when examined at the combined endpoints (CV and renal) or at each endpoint separately. The primary endpoint rate increased significantly with the increased number of MetS components (MetS comp. 0 vs. MetS comp. 2+, primary endpoints, p = 0.012).
Conclusion: Our results showed that the metabolic profile has a prognostic role not only for renal endpoints but also for CV endpoints in IgAN. BMI, hyperuricemia, hypertension, and diabetes have a predictive value for the prognosis of IgA nephropathy.
Keywords:
Chronic kidney disease
; IgA nephropathy
; Renal function
; Metabolic syndrome
; Arterial stiffness
Introduction
Cardiovascular (CV) morbidity and mortality in chronic kidney disease (CKD) is many times higher than in the general population [1,2], and in primary glomerular disease such as IgA nephropathy (IgAN), the absolute risk of cardiovascular disease (CVD) is roughly 2.5 times higher than in the population without any kidney disease [3]. The classification of CVD risk in these individuals may be improved by taking into account eGFR, proteinuria, the type of glomerular disease [3], and the patient's metabolic profile. Moderate and severe CKD are independent risk factors for cardiovascular disease [4]. IgA nephropathy is the most common primary glomerular disease worldwide and is a relatively common cause of end-stage kidney disease (ESKD) [5,6]. Long-term observational studies have shown that IgAN causes ESKD in 40% of patients within 20 years after diagnosis [7,8]. The clinical presentation is usually nephritic syndrome and hematuria with variable degrees of proteinuria. Pathologically, IgAN is defined by polymeric IgA1 being deposited in the glomerulus, primarily in the mesangium; mesangial hypercellularity and mesangial matrix expansion are also present, along with various degrees of interstitial fibrosis and glomerulosclerosis. The degree of glomerulosclerosis and tubulointerstitial fibrosis in renal pathology, the presence of hypertension and excessive proteinuria, and a marked decline in glomerular filtration rate (GFR) at the time of renal biopsy are all considered adverse prognostic indications [9,10].
Although research on MetS's independent relationship to the onset and progression of CKD has been increasingly studied, the results are inconsistent. According to a population-based study, patients with non-diabetic early-stage CKD (stages 1-3) are the only ones whose MetS has a substantial effect on the progression of CKD; patients with non-diabetic late-stage and diabetic CKD are not affected [11]. Independent of diabetes grades, a different investigation found a substantial correlation between CKD and components of the MetS [12]. Furthermore, despite a positive and considerable risk of estimated glomerular filtration rate (eGFR) decline, cohort research found no correlation between MetS and incident CKD [13]. Several meta-analyses were conducted to settle these disputes. According to a prior meta-analysis involving 11 cohort studies, MetS may promote the onset of CKD [14].
MetS and its components are putative risk factors for albuminuria and proteinuria, according to a different meta-analysis of 57 studies [15]. Previous meta-analyses, however, solely comprised research on individuals without CKD. There haven't been any meta-analyses done to look into the relationship between ESRD or renal events like eGFR decline and MetS and its components.
Apart from the aforementioned established risk factors, new research has also linked the advancement in the progression of IgAN to other cardiovascular risk factors, including hypertriglyceridemia, hyperuricemia, excessive body weight, and smoking [16,17]. However, there is limited data about the prevalence of metabolic syndrome and the metabolic profile association between metabolic syndrome (MetS) and renal and cardiovascular (CV) outcomes in IgAN patients. More focus is being placed on identifying and treating the modifiable risk factors that can stop or slow down the deterioration of renal function.
Earlier cross-sectional studies have also demonstrated a link between MetS and CKD [18,19]. Kurella et al. conducted only one longitudinal investigation [20], demonstrating a significantly increased risk of incident CKD in non-diabetic adults with MetS. However, in our study, we investigated the effects of MetS and metabolic profiles on the outcomes of IgAN.
Materials and Methods
We included 145 renal biopsy-proven IgAN patients in our follow-up study to our earlier 2013 investigation, and we analyzed their data prospectively (Figure 1A,B). The study procedure had been approved by the University of Pécs Regional Research Ethics Committee, and all participants provided written consent for its completion.
The inclusion criterion for the study was confirmed IgAN over the age of 18. Exclusion criteria were previous or current immunosuppressive treatment (due to the modifying effects of the metabolic components) and severe comorbidities (such as malignancies that required active treatment or acute infection).
Metabolic syndrome (MetS) was defined as the NCEP ATP III (National Cholesterol Education Program Adult Treatment Panel III) criterion: any three of the five criteria: waist circumference (>102 cm in males, >90 cm in females) or BMI >27 kg/m², fasting glucose ≥5,6 mmol/l, triglyceride ≥1,7 mmol/l, HDL cholesterol <1,0 mmol/l in males and <1,3 in females, systolic/diastolic blood pressure >130/85 mmHg.
An echocardiography examination was performed at the beginning of patient enrollment, and information about classic CV risk factors such as smoking, lipid abnormalities, obesity, diabetes, hypertension, and antihypertensive medications (ACEI/ARB, BB, and CCB) was also recorded. The obesity inclusion criterion was a BMI over 30 kg/m². The CKD-EPI formula was used to estimate renal function (eGFR, ml/min, 1.73 m2). A 24-hour blood pressure monitor was used by ABPM (Meditech, Hungary) devices to determine the patient’s 24-hour average systolic and diastolic blood pressure, pulse pressure, and diurnal index. At the start of the study, arterial stiffness and pulse wave velocity (PWV) were measured by a SphygmoCor System (AtCor Medical Australia). During these visits, medical events that had occurred since the previous visit were recorded, the patient's physical status was examined, and detailed laboratory tests were performed. Blood pressure values were determined from the average of three measurements taken after 10 minutes of rest. Serum parameters were determined by routine, standardized laboratory methods.
Statistical Analysis
Statistical analyses were performed using SPSS 21.0 software (SPSS, Inc., Chicago, IL, USA). A comparison of clinical and laboratory parameters was made using the Student’s t-test and ANOVA, as appropriate. The mean SD was used to express data from a normal distribution. Correlations between continuous variables were evaluated with linear regression using the Pearson test, and for categorical variables, the Spearman correlation test was used. The survival rates of the two groups were examined by the Mantel-Cox log-rank test. The effect of metabolic syndrome components on survival was evaluated by Cox regression analysis. Values of p < 0.05 were considered statistically significant.
Results
The study included 145 patients, but 20 patients were excluded: 10 patients due to immunosuppressive therapy, 9 patients lost follow-up, and 1 patient withdrew informed consent, so finally 125 patients’ data were investigated. The average age was 53.0 ± 12.7 years, of which 92 were male. The median follow-up time was 190 ± 170 months. Patients were divided into two groups based on MetS presence or absence. Baseline clinical data are shown in Table 1. There were significant differences between the two groups in systolic blood pressure, pulse pressure, systolic diurnal rhythm, diastolic dysfunction, BMI, prediabetes (impaired fasting glucose: IFG and impaired glucose tolerance: IGT), eGFR, PWV, HDL-cholesterol, TG, and uric acid, but not in age or gender. The distribution of metabolic parameters in the MetS presence and MetS absence groups is summarized in Table 2.
If we investigated the MetS components (HT, DM, BMI, dyslipidemia), the K-M curves showed significantly worse survival in cases of hypertension (primary endpoint: p=0.004, secondary renal endpoint: p=0.020, secondary CV endpoint: p=0.0038), diabetes mellitus (p=0.002, p=0.008, p=0.007), and higher BMI (cut off 25 kg/m²) (p=0.028, p=0.015, p=NS) in both primary and secondary endpoints. Surprisingly, there was a non-significant difference in the primary and secondary outcomes in the case of dyslipidemia, but we found significant differences in the case of hyperuricemia (cut of 360 umol/l) (p<0.001, p<0.001, p=0.029) (see Figure 2).
There were significant differences in survival on the K-M curves in the case of the primary combined endpoint (p<0.001) and the secondary renal (p = 0.001) and cardiovascular endpoints (p = 0.001) if we compared the IgAN patients with and without MetS (Figure 3).
There was a significant difference in survival only in the primary endpoint when we compared the patient with the MetS components (0 vs. 1. vs. 2+); the secondary endpoints were not significant (p = 0.028) (Figure 4).
If we combined the arterial stiffness, PWV (<10 m/s vs. ≥ 10 m/s), and MetS presence or absence in the survival examination, there was a significant difference between the low PWV group without MetS compared to the high PWV with MetS. All endpoints, the primary combined (p = 0.001) and both secondary endpoints (renal and cardiovascular) (p = 0.008; p = 0.005), were significant (Figure 5).
Multivariate analysis were performed on clinical data, metabolic parameters, echocardiographic parameters and laboratory results. The significant factors in competitive risk model were gender (OR= 4.333, p=0.001), age (OR=2.906, p=0.026), dyslipidemia (OR=3.474, p=0.034), hypertension (OR=5.806, p=0.018), diabetes (OR=1.912, p=0.011), BMI (OR=2.205, p=0.021), eGFR (OR=3.187, p=0.021), hemoglobin (OR=2.237, p=0.029), albuminuria (OR=2.568, p=0.013) and uric acid level (OR=1.837, p=0.021) (Table 3).
The primary endpoint independent predictors of survival were dyslipidemia, eGFR, hemoglobin, urine albuminuria, and diabetes mellitus, as determined by using Cox regression analysis. Secondary renal endpoint independent predictors were dyslipidemia, hemoglobin, urine albuminuria, and eGFR. Secondary cardiovascular endpoint predictors were gender, BMI, and diabetes (Table 4).
Cox regression analysis of the MetS components showed that the primary endpoint and secondary renal endpoint independent predictors were uric acid and diabetes (Table 5).
Discussion
In the present study, we demonstrated that metabolic syndrome and its components, especially hypertension, diabetes, obesity, and hyperuricemia, were significantly associated with the primary combined and secondary renal and cardiovascular outcomes, but not dyslipidemia. Due to the variability of serum lipids, one measurement has no impact on CV or renal endpoints. MetS development with increased PWV showed a worse renal and CV prognosis.
Survival curves stratified by MetS status (at least 3 factors from the above-mentioned) showed significant differences in the association with the various endpoints.
The key objective of the MetS diagnosis criteria was to identify the population most at risk of developing cardiovascular diseases [21,22]. In today's world, it is undeniable that individuals with MetS have a markedly increased risk of developing both CVD and CKD [23,24,25,26,27]. The majority of the observational studies covered in these articles discovered a strong correlation between MetS and CKD. Nevertheless, as most of the research was cross-sectional, it was unable to identify whether MetS is linked to long-term changes in renal function or to demonstrate a cause-and-effect relationship between the decline in kidney function and MetS.
In our earlier research, we found a strong correlation between MetS and the progressive loss of kidney function, except for ESKD, which may have an impact on the progression of the earliest stages of IgAN [23]. The present data support these observations, and not only the renal endpoints but also the CV endpoints are affected by the presence of MetS in IgAN.
Lee et al. have found that MetS had an impact on CKD progression only in early-stage CKD patients in their short follow-up (average 10.6 months) study [28]. The short follow-up may be the reason that the impact of MetS was not observed among late-stage and diabetic CKD patients. In our present study, there was more than ten times longer follow-up, clearly demonstrating the impact of MetS on primary (CV+renal) and secondary renal endpoints. The other important difference was that the proportion of diabetic patients was higher (in Lee et al.’s study, 53% vs. 24%), and our patients were homogenous for CKD.
The two main causes of CKD worldwide, diabetes and hypertension, are among the elements of MetS that have been extensively studied and reported. About the connection between diabetes and IgAN, Fliser et al. [29] reported that patients with IgAN or ADPKD who have incipient chronic renal disease already exhibit insulin resistance and hyperinsulinemia. These early changes may be worsened by the other MetS factors.
At the start of the patient follow-up in our current investigation, 30 patients, or 24% of the total, had diabetes mellitus (see Table 1). It is recognized that in patients with diabetes, IgAN may also be the only renal abnormality or that it may superimpose on diabetic nephropathy. Because IgA1 immune complexes or aggregates can be more easily deposited in diabetic patients' glomeruli due to metabolic changes, intraglomerular hypertension, and hyperfiltration, the relationship between IgAN and diabetes may not be a coincidence. Moreover, type 2 diabetes is frequently associated with malformations of the IgA immune system [30].
Common in CKD patients, hypertension is a predictor of cardiovascular morbidity and mortality, the same as it is in the general population. Patients with MetS and hypertensive CKD are extremely vulnerable to cardiovascular events. A U-shaped relationship has been shown between blood pressure and mortality; early mortality is predicted not only by high blood pressure but also by low mean systolic and diastolic blood pressure [31]. Strict blood pressure management enhances renal protection in IgAN, as was already indicated in the introduction. The progression of IgAN is more severe when hypertension is present [32]. It was therefore not surprising that, among the MetS parameters examined in our investigation, hypertension had the biggest impact on the prognosis of IgAN, consistent with our previous recommendation that IgAN patients require stringent blood pressure control [33].
Numerous epidemiological studies have linked obesity to an increased risk of developing CKD and ESKD [34,35,36].
Regardless of the existence of diabetes or hypertension, obesity, as measured by an elevated BMI, was linked to ESKD and reduced renal function in the populations under investigation. Losing weight slows the advancement of chronic kidney disease [37]. Increased BMI appears to be paradoxically associated with improved survival in advanced CKD and ESKD [38]. This link may be related to improved nutritional status in patients with an elevated BMI. Obesity was found to be a predictive factor for both the development of ESKD and hypertension in IgAN patients. Obese patients also exhibit glomerular enlargement and ultrastructural modification of the glomerular basement membrane, which are well-documented phenomena [29,39,40]. Based on our results, we were also able to confirm this in our 2013 study [23].
Observational studies and meta-analyses have shown dyslipidemia, namely atherogenic dyslipidemia (high triglyceride and low HDL cholesterol), as an independent risk factor for the onset and course of chronic kidney disease (CKD) [41,42]. Dyslipidemia was an important, significant factor by Cox regression analysis in the primary combined endpoints and secondary renal endpoints (see Table 3). The lower number of secondary CV endpoints may explain the non-significant connection between secondary CV endpoints and dyslipidemia.
Moreover, the progressive deterioration of renal function may increase oxidative stress and inflammation, which may trigger several metabolic changes, including hypertriglyceridemia, diabetes, and insulin resistance. These changes have the potential to create vicious cycles. In the study of Syrjänen et al. [16], elevated triglyceride levels were associated with progressive IgAN. Our long-term follow-up also supports these findings (see Table 3).
According to recent epidemiologic and experimental data, hyperuricemia may play a part in IgAN as well as serving as a risk factor for the onset and progression of renal illness in addition to serving as a marker of decreased kidney function [43,44].
In addition to being linked to renal tissue inflammation in patients with IgAN, serum uric acid may also have another role in the development of tubulointerstitial lesions [45]. In the Jerusalem Lipid Research Clinic cohort trial, serum uric acid was a long-term predictor of acute kidney injury and CKD that was not dependent on GFR [46], based on a follow-up of 2449 patients. Our results were very similar in a homogenous but lower number of patient group.
Previous meta-analyses have indicated individuals with MetS have a higher chance of developing chronic kidney disease (CKD), as evidenced by albuminuria or proteinuria [15] and a reduction in eGFR [14,47]. The results of previous research that examined the role of MetS and its components in the risk of developing renal disease in addition to incident CKD were inconsistent. The significant role that MetS plays in the evolution of CKD was highlighted by a large prospective cohort study conducted across the United States that demonstrated that people with MetS had a 2-fold increased risk of developing ESRD compared to people without the condition [48].
On the other hand, the African-American Study's secondary analysis showed that MetS is not directly linked to the advancement of CKD and that the relationship between it and CKD acceleration is complicated by other variables [49].
Li et al.'s meta-analysis provided evidence for a strong correlation between MetS and the acceleration of renal failure, indicating that MetS may be a separate predictor of disease progression from acute CKD [50]. To investigate the relative contributions of the various components of MetS to the risk of renal failure, a meta-analysis of individual components was conducted. In both industrialized and developing nations, diabetes and hypertension are the main causes of both CKD and ESRD [51]. However, this study indicated that the risk was highest for increased blood pressure and lowest for IFG. A few investigations have confirmed the link between increased blood pressure and renal insufficiency [52,53]. The study's risk estimate is consistent with earlier meta-analyses [47], which found a positive correlation between high blood pressure and poor kidney function, with an odds ratio (RR) of 1.37 (1.29–1.46).
Regarding the effect of prehypertension on new-onset CKD [54] and progression to ESRD [55], there was no indication of regional variations. One of the three studies in the non-Asian subgroup that reported a notable influence of hypertension could be the cause of this disparity [56]. In the meantime, the study participants' baseline characteristics revealed a greater prevalence of raised blood pressure with inadequate management and treatment [56].
Conversely, prior research examining the correlation between glycemic status and renal disease has yielded inconsistent findings. According to a recent meta-analysis, the risk of CKD was found to be slightly enhanced by prediabetes (RR = 1.11, 95% CI 1.02–1.21), which includes IFG, impaired glucose tolerance (IGT), and elevated glycated hemoglobin A1c [57]. In the non-diabetic group, IFG was not causally linked to the development of CKD, according to Mendelian randomization research [58].
The disparity could potentially be attributed to the distinct attributes of the research subjects. Individuals with diabetes at baseline or during follow-up may have been included in studies addressing IFG as part of MetS, whereas individuals with IGT may not have been included. Therefore, depending on different glycemic exposures, the link between IFG and renal impairment may change. Therefore, it is important to consider MetS when interpreting the risk estimations. IFG is not usually reported by itself; rather, it is thought to be the outcome of intricate interactions between several MetS components [59], particularly in individuals with chronic kidney disease (CKD), who are more likely to have prior cardiovascular disease, diabetes, hypertension, and abnormal lipid metabolism [60,61].
Furthermore, our study demonstrated that whereas dyslipidemia is not shown to be a significant predictor of new-onset CKD and subsequent disease progression in observational studies [62,63,64] and meta-analyses [65,66], other components of MetS, such as obesity, increased blood pressure, and diabetes, are. Even though some evidence suggests that diabetes and hypertension may be the primary causes of obesity-associated CKD [67], some studies have established obesity as an independent risk factor for promoting new-onset or accelerating pre-existing CKD [67,68].
In an individual-level meta-analysis of 5.5 million people in 39 general population cohorts, BMI values of 30, 35, and 40 kg/m2 were associated with an elevated risk of eGFR drop ≥40% by 18%, 69%, and 102%, respectively [69]. When comparing patients with and without baseline CKD, the relationship was quite similar.
Mechanistically, obesity-induced nephropathy develops and progresses due to inflammation, insulin resistance, abnormalities in renal hemodynamics, and diseases related to lipid metabolism [66]. A common condition among CKD patients is dyslipidemia. The dyslipidemic profile in CKD populations is influenced by elevated TG levels, reduced and dysfunctional HDL cholesterol, and variable levels of low-density lipoprotein cholesterol [70].
Studies on dyslipidemia and renal dysfunction have looked at different phases of chronic kidney disease. Cohort research found that among individuals without chronic kidney disease (CKD), increased TG was a risk factor contributing to the observed link between MetS and deterioration in renal function [71]. Data from a different investigation revealed that while high TG levels had no or inverse relationships with time to end-stage renal disease (ESRD) in CKD stages 4-5, they were linked to a higher incidence of CKD and a faster deterioration in renal function in non-CKD and CKD stage 3 [72]. In a different study, there was also no significant link found between TG and HDL-cholesterol levels and the development of renal replacement therapy and rapid renal progression in CKD stages 3-5 [73].
Prior studies have demonstrated that HDL-cholesterol is essential for the progression of chronic kidney disease [74]. A different cohort study that included participants with stages 3-5 of chronic kidney disease (CKD) found that the association between decreased HDL-cholesterol and kidney failure progression was eliminated when pertinent factors were taken into account in multivariate analysis [75]. The consequences of hyperlipidemia in patients with advanced chronic kidney disease (CKD), particularly those with end-stage renal disease (ESRD), may be obscured by the presence of more potent conventional CVD risk factors. The advancement of the disease may be more significantly impacted by altered energy metabolism, inflammation, malnutrition, and protein energy waste [72].
Our results allow nephrologists to concentrate on the initial phases of chronic kidney disease (CKD), perhaps resulting in the early implementation of therapies for metabolic disorders, like dietary changes or medication. Furthermore, prior research has shown that the distribution of fat, namely the amount in the abdomen rather than overall obesity, is a significant factor in poor renal outcomes [76]. Although the current study did not perform subgroup analysis based on fat distribution, there was a significantly higher abdominal circumference in males (p = 0.030) and females (p = 0.023) in the MetS group compared to the non-MetS group.
Lin et al. demonstrated that blood pressure is the most important component of MetS for renal outcomes in CKD 1-4 stage patients. The MetS group had a higher risk for renal outcomes and all-cause mortality (HR: 1.62 and 1.43) [77], and our results also confirm this.
We demonstrated in our previous study that arterial stiffness had predictive value for renal and CV prognosis in autosomal polycystic kidney disease [78], and the etiology of the kidney disease did not similarly alter the vascular function of different CKD groups. Blood pressure was an independent risk factor for PWV [79]. Arterial stiffness was associated with GFR and left ventricular hypertrophy (LVH) in IgAN [80]. In this study, we could demonstrate that if we combined MetS with an arterial stiffness parameter (PWV), the renal and cardiovascular risk prediction would be more pronounced. Vascular stiffness measurement could help nephrologists with further risk assessment.
In our other earlier study, we found an association between LVH and eGFR in IgAN. There was a strong correlation between left ventricular mass index (LVMI) and renal function in a homogenous immunocomplex-mediated CKD population of IgAN patients. An independent predictor of LVMI was the initial stage of renal function. Renal composite endpoints and CV were higher when LVMI was higher. An independent predictor of ESKD and CV events may be a higher LVMI. Increased LVMI should draw attention to CKD patients who require closer monitoring, referral for additional CV testing, and maximal renal and heart protection since they have a higher risk of cardiovascular and renal disease at an early stage of the disease (II–IV) [81]. In our current study, there was no significant difference in LVMI between the MetS and non-MetS groups.
Limitations of the Study
Firstly, this is a medium-term follow-up study conducted at a single center. Secondly, this cohort provides the basis for the cut-off value and the single baseline measurement. It might not be suitable for other racial and ethnic groups as a result. Thirdly, residual confounding effects from lifting style, drugs that alter CV risk, and comorbidity might introduce bias into prospective analysis. For this reason, larger sample sizes and more prospective research are required. Fourth, there were more men than women in this study, which could have influenced the findings.
Conclusions
In conclusion, our study proved that risk stratification of IgAN patients is very helpful in identifying high-risk individuals, especially when the metabolic profile is combined with an increased arterial stiffness evaluation for additional risk. Further, multicenter, randomized clinical trials with a large number of patients are warranted to confirm our results.
Author Contributions
All authors have read and approved the manuscript. Balázs Sági conceived and designed the study, the collection of clinical data, and the drafting and approval of the manuscript. Botond Csiky identified the study plot and contributed to the interpretation and drafting approval of the manuscript. Tibor Vas: identify the study plot, identify the classification of biopsies, perform statistical analysis, review, and approve the manuscript. Judit Nagy: drafting an application to the committee of ethics, organizing the database, reviewing, and approving the manuscript.
Funding
No funding.
Availability of Data and Materials
The data underlying this article cannot be shared publicly due to Hungarian regulations and the privacy of individuals who participated in the study. The data could be shared on reasonable request with the corresponding author if accepted by the Regional Committee for Medical and Health Research Ethics and local Data Protection Officials.
Declarations
Ethics, approval, and consent to participate. The study was approved by the University of Pécs Clinical Center Regional Research Ethical Committee (Reference No. 3170/2008). Informed consent was obtained from all subjects involved in the study. The research was done according to the Declaration of Helsinki.
Consent for publication
Not Applicable.
Acknowledgments
Special thanks to Ilona Varga Sámikné for the data collection.
Competing interests
Not Applicable.
References
- Jha V, Garcia-Garcia G, Iseki K, Li Z, Naicker S, Plattner B, Saran R, Wang AY, Yang CW: Chronic kidney disease: Global dimension and perspectives. Lancet 2013;382: 260–272. [CrossRef]
- Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, Jafar TH, Heerspink HJ, Mann JF, Matsushita K, Wen CP: Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013;382: 339–352. [CrossRef]
- Canney M, Gunning HM, Zheng Y, Rose C, Jauhal A et al. Risk of Cardiovascular Events in Individuals With Primary Glomerular Diseases. Am J Kidney Dis. 2022;80(6):740-750. [CrossRef]
- Ortiz A, Wanner C, Gansevoort R. Chronic kidney disease as cardiovascular risk factor in routine clinical practice: a position statement by the Council of the European Renal Association. Eur J of Prev Cardiol. 2022;29:2211–2215. [CrossRef]
- Kwon CS, Daniele P, Forsythe A, Ngai C. A Systematic Literature Review of the Epidemiology, Health-Related Quality of Life Impact, and Economic Burden of Immunoglobulin A Nephropathy. J Health Econ Outcomes Res 2021;8(2):36-45. [CrossRef]
- Schena FP, Pesce F. Epidemiology and ancestral difference. In: Lai KN (ed). Recent Advances in IgA Nephropathy. New Jersey: World Scientific Publishing Co., 2009, pp. 9–20.
- Berthoux CB, Mohey H. Clinical course of primary IgA nephropathy. In: Lai KN (ed). Recent Advances in IgA Nephropathy. New Jersey: World Scientific Publishing Co., 2009, pp. 107–120.
- Floege J, Feehally J. IgA nephropathy: recent developments. J Am Soc Nephrol 2000; 11: 2395–2403. [CrossRef]
- Barrat J, Feehally J. IgA nephropathy. J Am Soc Nephrol 2005; 16: 2088–2097.
- Bonett F, Deplere C, Sassolas A et al. Excessive body weight as a new independent risk factor for clinical and pathological progression in primary IgA nephritis. Am J Kid Dis 2001; 37: 720–727. [CrossRef]
- Lee CC, Sun C, Wu IW, Wang SY, Wu MS. Metabolic syndrome loses its predictive power in late-stage chronic kidney disease progression–a paradoxical phenomenon. Clin. Nephrol. 2011, 75, 141–149. [CrossRef]
- Wang Y, Sun B, Sheng LT, Pan XF, Zhou Y, Zhu J, Li X, Yang K, Guo K, Zhang X. et al. Association between weight status, metabolic syndrome, and chronic kidney disease among middle-aged and elderly Chinese. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 2017–2026. [CrossRef]
- Li Y, Xie D, Qin X, Tang G, Xing H, Li Z, Xu X, Xu X, Hou F. Metabolic syndrome, but not insulin resistance, is associated with an increased risk of renal function decline. Clin. Nutr. 2015, 34, 269–275. [CrossRef]
- Thomas G, Sehgal AR, Kashyap SR, Srinivas TR, Kirwan JP, Navaneethan SD. Metabolic Syndrome and Kidney Disease: A Systematic Review and Meta-analysis. Clin. J. Am. Soc. Nephrol. 2011, 6, 2364–2373. [CrossRef]
- Rashidbeygi E, Safabakhsh M, Aghdam SD, Mohammed SH, Alizadeh S. Metabolic syndrome and its components are related to a higher risk for albuminuria and proteinuria: Evidence from a meta-analysis on 10,603,067 subjects from 57 studies. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 830–843. [CrossRef]
- Syrjänen J, Mustonen J, Pasternack A. Hypertriglyceridaemia and hyperuricemia are risk factors for progression of IgA nephropathy. Nephrol Dial Transplant 2000; 15: 34–42. [CrossRef]
- Yamamoto R, Nagasawa Y, Shoji T et al. Cigarette smoking and progression of IgA nephropathy. Am J Kidney Dis 2010; 56: 313–324. [CrossRef]
- Lakka HM, Laaksonen DE, Lakka TA et al. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA 2002; 288: 2709–2716. [CrossRef]
- Chen J, Muntner P, Hamm LL et al. The metabolic syndrome and chronic kidney disease in US adults. Ann Intern Med 2004; 140: 167–174. [CrossRef]
- Kurella M, Lo JC, Chertow GM. Metabolic syndrome and the risk for chronic kidney disease among nondiabetic adults. J Am Soc Nephrol 2005; 16: 2134–2140. [CrossRef]
- Grundy SM, Cleeman JI, Daniels SR et al. Diagnosis and management of the metabolic syndrome: American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation 2005; 112: 2735–2752. [CrossRef]
- Reaven G. Metabolic syndrome: pathophysiology and implications for management of cardiovascular disease. Circulation 2002; 106: 286–292. [CrossRef]
- Kovács T, Vas T, Kovesdy CP, Késõi I, Sági B, Wittmann I, Nagy J. Metabolic syndrome and other cardiovascular risk factors associated with the progression of IgA nephropathy. Clin Kidney J. 2013 Aug;6(4):395-401. [CrossRef]
- Lastra G, Manrique C, McFarlane S, et al. Cardiometabolic syndrome and chronic kidney disease. Curr Diab Rep 2006; 6: 207–212. [CrossRef]
- Natali A, Pucci G, Boldrini B et al. Metabolic syndrome: at the crossroads of cardiorenal risk. J Nephrol 2009; 22: 29–38.
- Zoccali C. Overweight, obesity and metabolic alterations in chronic kidney disease. Contributions Soc Biol Med Sci MASA 2009; 30: 17–31.
- Thomas G, Sehgal AR, Kashyap SR et al. Metabolic syndrome and kidney disease: a systematic review and meta-analysis. Clin J Am Soc Nephrol 2011; 6: 2364–2373. [CrossRef]
- Lee CC, Sun CY, Wu IW et al. Metabolic syndrome loses its predictive power in late-stage chronic kidney disease progression — a paradoxical phenomenon. Clin Nephrol 2011; 75: 141–149. [CrossRef]
- Fliser D, Pacini G, Engelleiter R et al. Insulin resistance and hyperinsulinemia are already present in patients with incipient renal disease. Kidney Int 1998; 53: 1343–1347. [CrossRef]
- Ștefan G, Zugravu A, Stancu S. Mortality in IgA Nephropathy: A Long-Term Follow-Up of an Eastern European Cohort. Medicina (Kaunas). 2024 Jan 31;60(2):247. [CrossRef]
- Nagy J, Kovacs T. Special clinical syndromes. In: Lai KN (ed). Recent Advances in IgA Nephropathy. New Jersey: World Scientific Publishing Co., 2009, pp. 121–138.
- Kövesdy CP, Trivedi BK, Kalantar-Zadeh K et al. Association of low blood pressure with increased mortality in patients with moderate to severe chronic kidney disease. Nephrol Dial Transplant 2006; 21: 1257–1262. [CrossRef]
- Nagy J, Kovács T, Wittmann I. Renal protection in IgA nephropathy requires strict blood pressure control. Nephrol Dial Transplant 2005; 20: 1533–1539. [CrossRef] [PubMed]
- Kwan BCH, Murtaugh MA, Beddhu S. Associations of body size with metabolic syndrome and mortality in moderate chronic kidney disease. Clin J Am Nephrol 2007; 2: 992–998. [CrossRef]
- Kopple JD, Feroze U. The effect of obesity on chronic kidney disease. J Ren Nutr 2011; 21: 66–71. [CrossRef]
- Hsu C-Y, McCulloch CE, Iribarren C, et al. Body mass index and risk for end-stage renal disease. Ann Intern Med 2006; 144: 21–28. [CrossRef]
- Madero M, Sarnak MJ, Wang Y et al. Body mass index and mortality in CKD. Am J Kidney Dis 2007; 3: 404–411. [CrossRef]
- Kovesdy CP, Anderson JE, Kalantar-Zadeh K. Paradoxical association between body mass index and mortality in men with CKD not yet on dialysis. Am J Kid Dis 2007; 49: 581–591. [CrossRef]
- Tanaka M, Yamada S, Iwasaki Y et al. Impact of obesity on IgA nephropathy: comparative ultrastructural study between obese and non-obese patients. Nephron Clin Pract 2009; 112: 71–78. [CrossRef]
- Shimamoto M, Ohsawa I, Suzuki H, Hisada A, Nagamachi S, Honda D, Inoshita H, Shimizu Y, Horikoshi S, Tomino Y. Impact of Body Mass Index on Progression of IgA Nephropathy Among Japanese Patients. J Clin Lab Anal. 2015;29(5):353-60. [CrossRef]
- Muntner J, Coresh J, Smith J, et al. Plasma lipids and risk of developing renal dysfunction: the atherosclerosis risk in community study. Kidney Int 2000; 58: 293–301. [CrossRef]
- Fried F, Orchard TJ, Kasiske BL. Effect of lipid reduction on the progression of renal disease: a meta-analysis. Kidney Int 2001; 59: 260–269 400 T. Kovács et al. [CrossRef]
- Feig ID. Uric acid: a novel mediator and marker of risk in chronic kidney disease. Curr Opin Nephrol Hypertens 2009; 18: 526–530. [CrossRef]
- Obermayr RP, Temml C, Gutjahr G et al. Elevated uric acid increases the risk for kidney disease. J Am Soc Nephrol 2008; 19: 2407–2413. [CrossRef]
- Myllymäki J, Honkanen T, Syrjänen J, Helin H, Rantala I, Pasternack A, Mustonen J. Uric acid correlates with the severity of histopathological parameters in IgA nephropathy. Nephrol Dial Transplant. 2005;20(1):89-95. [CrossRef]
- Ben-Dov IZ, Kark JD. Serum uric acid is a GFR-independent long-term predictor of acute and chronic renal insufficiency: the Jerusalem Lipid Research Clinic cohort study. Nephrol Dial Transplant 2011; 26: 2558–2566. [CrossRef]
- Alizadeh, S.; Ahmadi, M.; Nejad, B.G.; Djazayeri, A.; Shab-Bidar, S. Metabolic syndrome and its components are associated with increased chronic kidney disease risk: Evidence from a meta-analysis on 11 109 003 participants from 66 studies. Int. J. Clin. Pract. 2018, 72, e13201. [CrossRef]
- Panwar, B.; Hanks, L.J.; Tanner, R.M.; Muntner, P.; Kramer, H.; McClellan, W.M.; Warnock, D.G.; Judd, S.E.; Gutiérrez, O.M. Obesity, metabolic health, and the risk of end-stage renal disease. Kidney Int. 2015, 87, 1216–1222. [CrossRef]
- Lea, J.; Cheek, D.; Thornley-Brown, D.; Appel, L.; Agodoa, L.; Contreras, G.; Gassman, J.; Lash, J.; Miller, E.R., 3rd; Randall, O.; et al. Metabolic Syndrome, Proteinuria, and the Risk of Progressive CKD in Hypertensive African Americans. Am. J. Kidney Dis. 2008, 51, 732–740. [CrossRef]
- Li X, Liang Q, Zhong J, Gan L , Zuo L. The Effect of Metabolic Syndrome and Its Individual Components on Renal Function: A Meta-Analysis. J Clin Med. 2023;12(4):1614. [CrossRef]
- Drawz, P.; Rahman, M. Chronic Kidney Disease. Ann. Intern. Med. 2015, 162, ITC1–ITC16. [CrossRef]
- Kim, H.W.; Park, J.T.; Joo, Y.S.; Kang, S.C.; Lee, J.Y.; Lee, S.; Chang, T.I.; Kang, E.W.; Ryu, D.-R.; Yoo, T.H. Systolic blood pressure and chronic kidney disease progression in patients with primary glomerular disease. J. Nephrol. 2021, 34, 1057–1067. [CrossRef]
- Wang, M.; Xia, M.; Yang, H.; Zhang, D.; Zhao, Y.; He, Y.; Liu, J.; Zhang, L.; Yin, C.; Bai, Y. Interaction effect of blood glucose and pressure on the risk of chronic kidney disease: A population-based prospective cohort study. Endocrine 2022, 77, 252–261. [CrossRef]
- Garofalo, C.; Borrelli, S.; Pacilio, M.; Minutolo, R.; Chiodini, P.; De Nicola, L.; Conte, G. Hypertension and Prehypertension and Prediction of Development of Decreased Estimated GFR in the General Population: A Meta-analysis of Cohort Studies. Am. J. Kidney Dis. 2016, 67, 89–97. [CrossRef]
- Huang, Y.; Cai, X.; Zhang, J.; Mai, W.; Wang, S.; Hu, Y.; Ren, H.; Xu, D. Prehypertension and Incidence of ESRD: A Systematic Review and Meta-analysis. Am. J. Kidney Dis. 2014, 63, 76–83. [CrossRef]
- Rashidi, A.; Ghanbarian, A.; Azizi, F. Are Patients Who Have Metabolic Syndrome without Diabetes at Risk for Developing Chronic Kidney Disease? Evidence Based on Data from a Large Cohort Screening Population. Clin. J. Am. Soc. Nephrol. 2007, 2, 976–983. [CrossRef]
- Echouffo-Tcheugui, J.B.; Narayan, K.M.V.; Weisman, D.; Golden, S.H.; Jaar, B.G. Association between prediabetes and risk of chronic kidney disease: A systematic review and meta-analysis. Diabet. Med. 2016, 33, 1615–1624. [CrossRef]
- Kim, H.; Park, S.; Kwon, S.H.; Jeon, J.S.; Han, D.C.; Noh, H. Impaired fasting glucose and development of chronic kidney disease in non-diabetic population: A Mendelian randomization study. BMJ Open Diabetes Res. Care 2020, 8, e001395. [CrossRef]
- Swi ˛ecicka-Klama, A.; Połtyn-Zaradna, K.; Szuba, A.; Zato ´nska, K. The Natural Course of Impaired Fasting Glucose. ´ Adv. Exp. Med. Biol. 2021, 1324, 41–50. [CrossRef]
- Barbour, S.; Er, L.; Djurdjev, O.; Karim, M.; Levin, A. The prevalence of hematologic and metabolic abnormalities during chronic kidney disease stages in different ethnic groups. Kidney Int. 2008, 74, 108–114. [CrossRef]
- Jankowski, J.; Floege, J.; Fliser, D.; Böhm, M.; Marx, N. Cardiovascular Disease in Chronic Kidney Disease: Pathophysiological Insights and Therapeutic Options. Circulation 2021, 143, 1157–1172. [CrossRef]
- Weldegiorgis, M.; Woodward, M. Elevated triglycerides and reduced high-density lipoprotein cholesterol are independently associated with the onset of advanced chronic kidney disease: A cohort study of 911,360 individuals from the United Kingdom. BMC Nephrol. 2022, 23, 312–319. [CrossRef]
- Ciardullo, S.; Ballabeni, C.; Trevisan, R.; Perseghin, G. Metabolic Syndrome, and Not Obesity, Is Associated with Chronic Kidney Disease. Am. J. Nephrol. 2021, 52, 666–672. [CrossRef]
- Chen, J.; Muntner, P.; Hamm, L.L.; Jones, D.W.; Batuman, V.; Fonseca, V.; Whelton, P.K.; He, J. The Metabolic Syndrome and Chronic Kidney Disease in U.S. Adults. Ann. Intern. Med. 2004, 140, 167–174. [CrossRef]
- Pinto, K.R.D.; Feckinghaus, C.M.; Hirakata, V.N. Obesity as a predictive factor for chronic kidney disease in adults: Systematic review and meta-analysis. Braz. J. Med. Biol. Res. 2021, 54, e10022. [CrossRef]
- Garofalo, C.; Borrelli, S.; Minutolo, R.; Chiodini, P.; De Nicola, L.; Conte, G. A systematic review and meta-analysis suggests obesity predicts onset of chronic kidney disease in the general population. Kidney Int. 2017, 91, 1224–1235. [CrossRef]
- Wang, M.; Wang, Z.; Chen, Y.; Dong, Y. Kidney Damage Caused by Obesity and Its Feasible Treatment Drugs. Int. J. Mol. Sci. 2022, 23, 747. [CrossRef]
- Berthoux, F.; Mariat, C.; Maillard, N. Overweight/obesity revisited as a predictive risk factor in primary IgA nephropathy. Nephrol. Dial. Transplant. 2013, 28, iv160–iv166. [CrossRef]
- Hsu, C.-Y.; McCulloch, C.E.; Iribarren, C.; Darbinian, J.; Go, A.S. Body Mass Index and Risk for End-Stage Renal Disease. Ann. Intern. Med. 2006, 144, 21–28. [CrossRef]
- Chang, A.R.; Grams, M.E.; Ballew, S.H.; Bilo, H.; Correa, A.; Evans, M.; Gutierrez, O.M.; Hosseinpanah, F.; Iseki, K.; Kenealy, T.; et al. Adiposity and risk of decline in glomerular filtration rate: Meta-analysis of individual participant data in a global consortium. BMJ 2019, 364, k5301. [CrossRef]
- Hager, M.R.; Narla, A.D.; Tannock, L.R. Dyslipidemia in patients with chronic kidney disease. Rev. Endocr. Metab. Disord. 2017, 18, 29–40. [CrossRef]
- Stefansson, V.T.; Schei, J.; Solbu, M.D.; Jenssen, T.G.; Melsom, T.; Eriksen, B.O. Metabolic syndrome but not obesity measures are risk factors for accelerated age-related glomerular filtration rate decline in the general population. Kidney Int. 2018, 93, 1183–1190. [CrossRef]
- Soohoo, M.; Hashemi, L.; Hsiung, J.-T.; Moradi, H.; Budoff, M.J.; Kovesdy, C.P.; Kalantar-Zadeh, K.; Streja, E. Association of Serum Triglycerides and Renal Outcomes among 1.6 Million US Veterans. Nephron 2022, 146, 457–468. [CrossRef]
- Chen, S.-C.; Hung, C.-C.; Kuo, M.-C.; Lee, J.-J.; Chiu, Y.-W.; Chang, J.-M.; Hwang, S.-J.; Chen, H.-C. Association of Dyslipidemia with Renal Outcomes in Chronic Kidney Disease. PLoS ONE 2013, 8, e55643. [CrossRef]
- Liao, S.; Lin, D.; Feng, Q.; Li, F.; Qi, Y.; Feng, W.; Yang, C.; Yan, L.; Ren, M.; Sun, K. Lipid Parameters and the Development of Chronic Kidney Disease: A Prospective Cohort Study in Middle-Aged and Elderly Chinese Individuals. Nutrients 2022, 15, 112. [CrossRef]
- Rahman, M.; Yang, W.; Akkina, S.; Alper, A.; Anderson, A.H.; Appel, L.J.; He, J.; Raj, D.S.; Schelling, J.; Strauss, L.; et al. Relation of Serum Lipids and Lipoproteins with Progression of CKD: The CRIC study. Clin. J. Am. Soc. Nephrol. 2014, 9, 1190–1198. [CrossRef]
- Lin HYH, Chang LY, Niu SW, Kuo IC, Yen CH et al. High risk of renal outcome of metabolic syndrome independent of diabetes in patients with CKD stage 1-4: The ICKD database. Diabetes Metab Res Rev. 2023 May;39(4):e3618. [CrossRef]
- Sági B, Késői I, Késői B, Vas T, Csiky B, Kovács T, Nagy J.Arterial stiffness may predict renal and cardiovascular prognosis in autosomal-dominant polycystic kidney disease. Physiol Int. 2018 Jun 1;105(2):145-156. [CrossRef]
- Késoi I, Sági B, Tóth OI, Vas T, Fazekas A, Kovács T, Pintér T, Wittmann I, Nagy J. Different effect of IgA nephropathy and polycystic kidney disease on arterial stiffness. Kidney Blood Press Res. 2011;34(3):158-66. [CrossRef]
- Sági B, Késői I, Vas T, Csiky B, Nagy J, Kovács TJ. Relationship between arterial stiffness, left ventricular diastolic function, and renal function in chronic kidney disease. BMC Nephrol. 2023 Sep 3;24(1):261. [CrossRef]
- Sági B, Késői I, Vas T, Csiky B, Nagy J, Kovács TJ. Left ventricular myocardial mass index associated with cardiovascular and renal prognosis in IgA nephropathy.BMC Nephrol. 2022:16;23(1):285. [CrossRef]
- Anders HJ, Peired AJ, Romagnani P. SGLT2 inhibition requires reconsideration of fundamental paradigms in chronic kidney disease, 'diabetic nephropathy', IgA nephropathy and podocytopathies with FSGS lesions. Nephrol Dial Transplant. 2022;37(9):1609-1615. [CrossRef]
- Caster DJ, Lafayette RA. The Treatment of Primary IgA Nephropathy: Change, Change, Change. Am J Kidney Dis. 2024;83(2):229-240. [CrossRef]
Figure 1.
The flow chart of recruited patients (A), and the flow chart of the study (B).
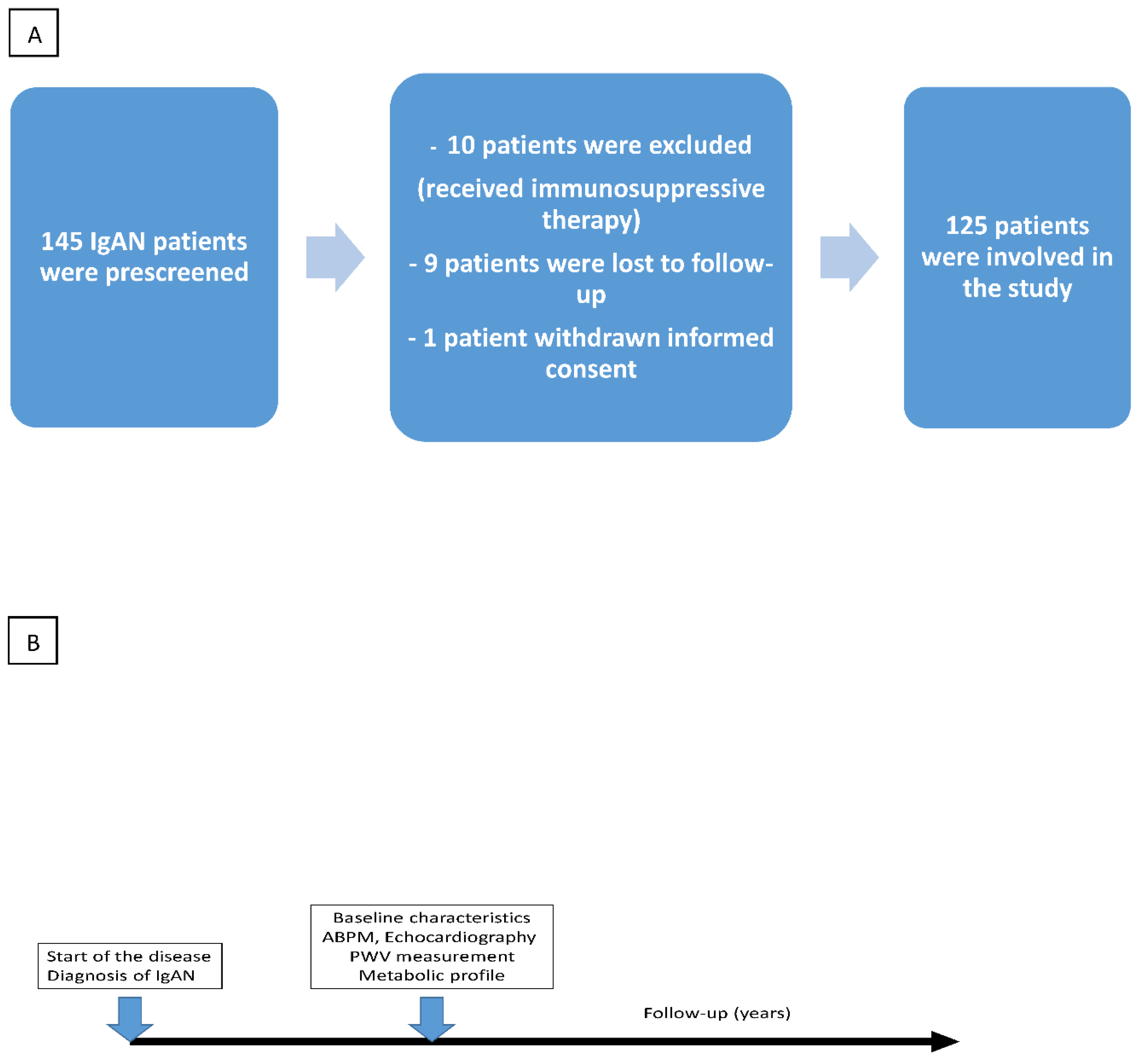
Figure 2.
Kaplan-Meier curves demonstrate the following primary combined endpoints: primary combined (A), renal (B), and cardiovascular (C) in patients with or without hypertension; primary combined (D), renal (E), and cardiovascular (F) in pa tients with diabetes; primary combined (G), renal (H), and cardiovascular (I) in patients with dyslipidemia; primary combined (J), renal (K), and cardiovascular (L) endpoints in patients with a BMI of 25 kg/m2; primary combined (M), renal (N), and cardiovascular (O) endpoints in patients with and without hyperuricemia.
Figure 2.
Kaplan-Meier curves demonstrate the following primary combined endpoints: primary combined (A), renal (B), and cardiovascular (C) in patients with or without hypertension; primary combined (D), renal (E), and cardiovascular (F) in pa tients with diabetes; primary combined (G), renal (H), and cardiovascular (I) in patients with dyslipidemia; primary combined (J), renal (K), and cardiovascular (L) endpoints in patients with a BMI of 25 kg/m2; primary combined (M), renal (N), and cardiovascular (O) endpoints in patients with and without hyperuricemia.
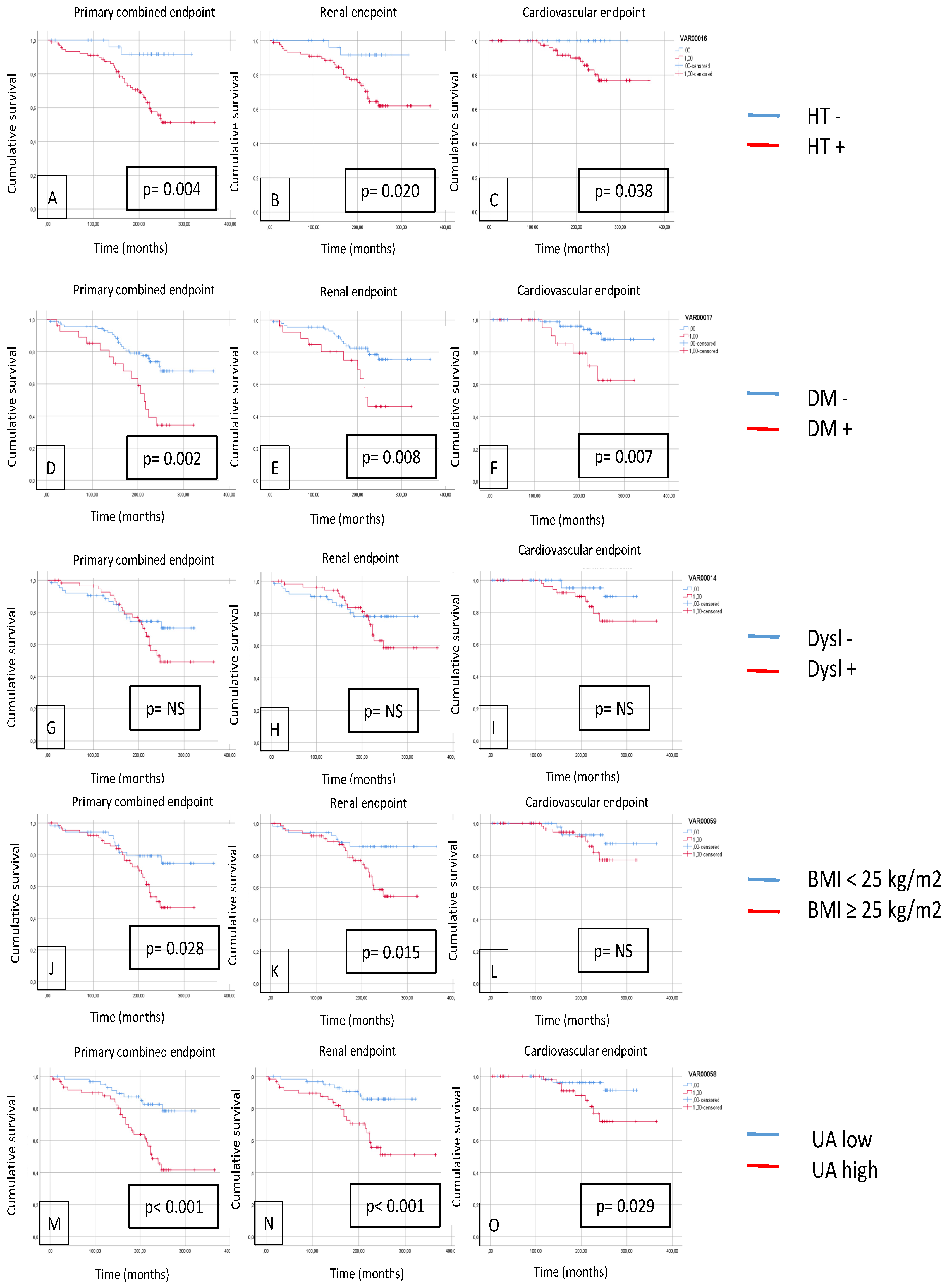
Figure 3.
Kaplan-Meier curves show primary combined (A), renal (B), and cardiovascular (C) endpoints in the case of patients with and without metabolic syndrome.
Figure 3.
Kaplan-Meier curves show primary combined (A), renal (B), and cardiovascular (C) endpoints in the case of patients with and without metabolic syndrome.
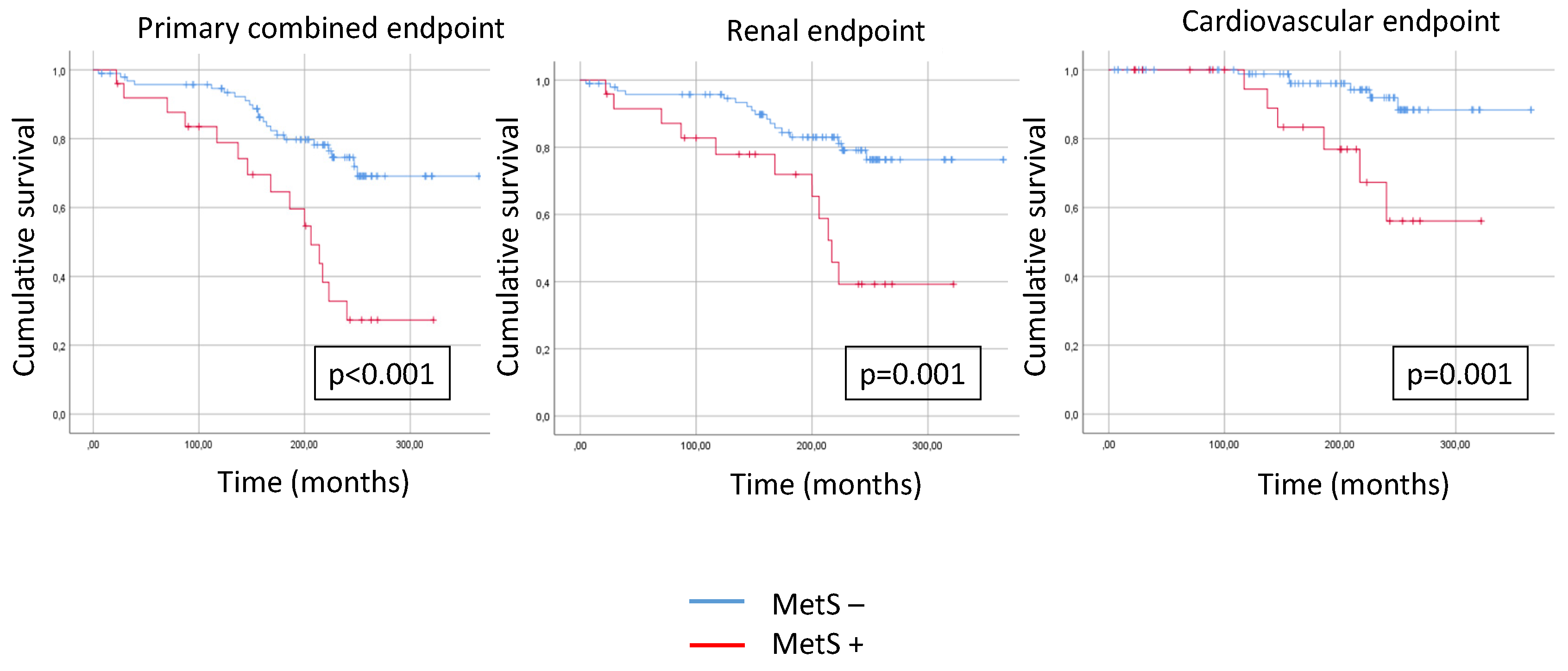
Figure 4.
Assuming metabolic syndrome components are detected, the Kaplan-Meier curves show the primary combined (A), renal (B), and cardiovascular (C) outcomes (0 vs. 1 vs. 2+).
Figure 4.
Assuming metabolic syndrome components are detected, the Kaplan-Meier curves show the primary combined (A), renal (B), and cardiovascular (C) outcomes (0 vs. 1 vs. 2+).
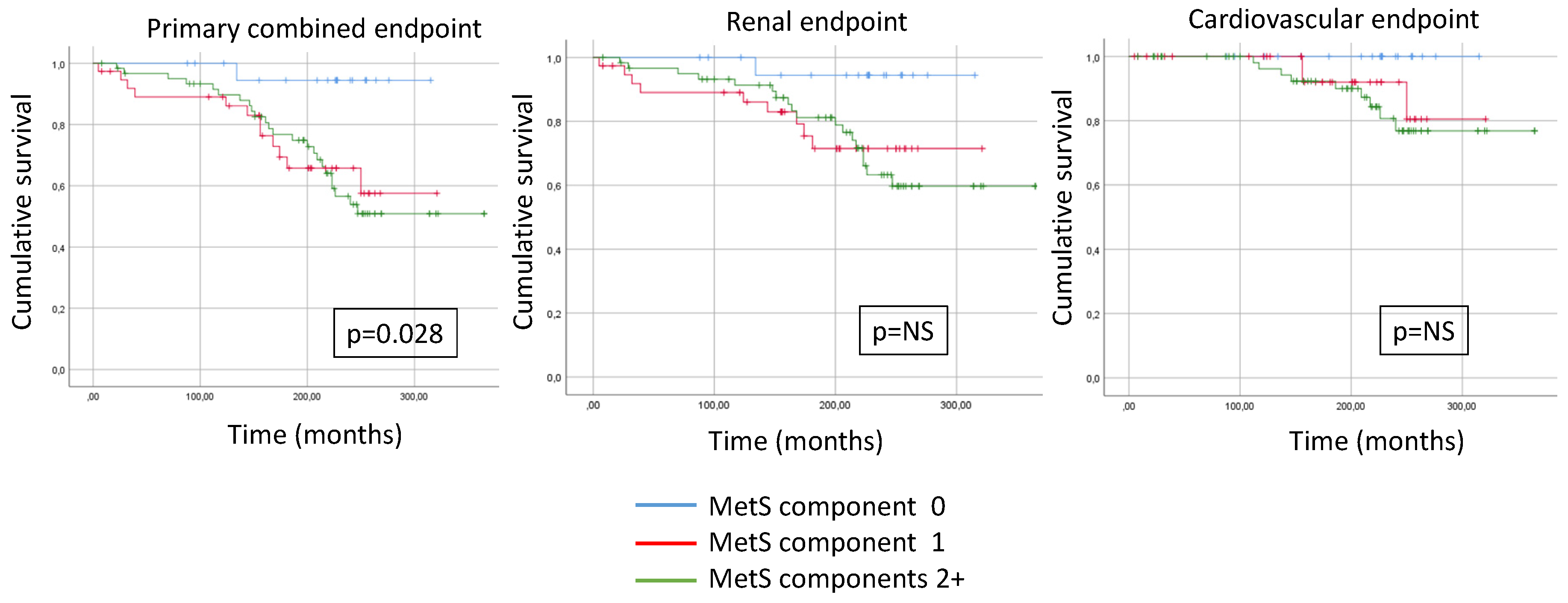
Figure 5.
Kaplan-Meier curves show primary combined (A), renal (B), and cardiovascular (C) endpoints in case of low or high PWV (< 10 m/s vs. ≥ 10 m/s ) and metabolic syndrome presence or absence (Met sy – vs. Met sy +).
Figure 5.
Kaplan-Meier curves show primary combined (A), renal (B), and cardiovascular (C) endpoints in case of low or high PWV (< 10 m/s vs. ≥ 10 m/s ) and metabolic syndrome presence or absence (Met sy – vs. Met sy +).
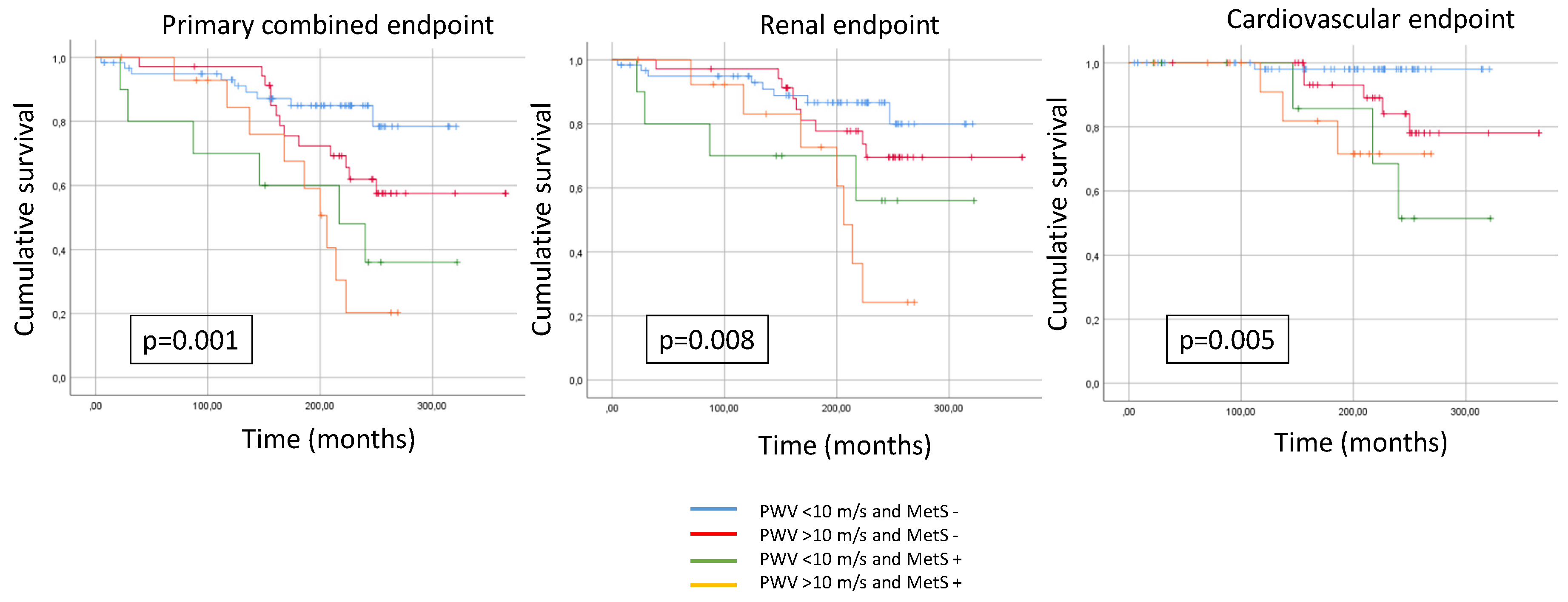

Table 1.
Baseline clinical data of IgAN patients.
| Clinical data (n=125) | Met sy – (n=60) |
Met sy + (n=65) |
p |
| Man/woman (n/%) | 36/24 (60/40) | 46/19 (71/29) | 0.079 |
| Age (year) (mean and 25-75 percentilis) | 53.2 (43.0-63.0) | 55.4 (44.0-64.0) | 0.109 |
| Average systolic BP (Hgmm) (mean and 25-75 percentile) | 123.5 (115.0-129.25) | 127.4 (117.3-131.2) | 0.002* |
| Average diastolic BP (Hgmm) | 73±9.6 | 75.7±9.5 | 0.231 |
| 24h pulse pressure (Hgmm) (mean and 25-75 percentile) | 49.35 (43.0-54.0) | 53.10 (44.5-56.5) | 0.012* |
| Diurnal index systolic (%) | 10.92±5.08 | 8.36±7.72 | 0.020* |
| Abdominal circumference in males (cm) | 100.2±4.2 | 112.1±6.5 | 0.030* |
| Abdominal circumference in females (cm) | 90.1±5.7 | 94.4±7.3 | 0.023* |
| Metabolic parameters | |||
| Hypertension (n,%) | 41 (68) | 53 (81) | 0.118 |
| BMI (kg/m²) (mean and 25-75 percentile) | 26.5 (22.9-29.7) | 28.6 (23.4-30.1) | 0.001* |
| Dyslipidemia (n,%) | 24 (40) | 34 (52) | 0.137 |
| Diabetes (n, %) | 9 (15) | 21 (32) | 0.087 |
| IFG and IGT (n/%) | 2 (3) | 10 (15) | 0.025* |
| Overweighted (n/%) | 3 (5) | 5 (8) | 0.098 |
| Obesity (n/%) | 2 (3) | 32 (49) | 0.001* |
| Visceral obesity (n/%) | 2 (3) | 28 (43) | 0.001* |
| eGFR (ml/min) | 94.6±29.3 | 78.9±37.9 | 0.005* |
| eGFR <60 ml/min (n/%) | 2 (3) | 4 (6) | 0.086 |
| Duration of kidney disease (year) | 10.2±9.7 | 8.8±9.1 | 0.101 |
| Smoking (n, %) | 7 (12) | 11(17) | 0.156 |
| Therapy | |||
| ACEI/ARB (n,%) | 46 (77) | 60 (92) | 0.079 |
| BB (n,%) | 12 (20) | 19 (29) | 0.178 |
| Statin (n,%) | 16 (27) | 22 (34) | 0.164 |
| CCB (n,%) | 9 (15) | 19 (29) | 0.082 |
| Echocardiographic parameters | |||
| LVEF (%)(mean and 25-75 percentile) | 62.8 (59.0-66.5) | 63.5 (60.1-66.7) | 0.211 |
| LVMI (g/m2) | 103.53±15.95 | 109.21±21.25 | 0.123 |
| LVEDD (cm) | 6.05±6.29 | 5.57±5.13 | 0.173 |
| DD (n/%) | 7 (11) | 17 (26) | <0.001* |
| E/A | 1.18±0.32 | 0.93±0.30 | <0.001* |
| Arterial stiffness | |||
| cfPWV (m/s) (mean and 25-75 percentile) | 9.97 (8.48-11.35) | 11.34 (10.1-12.2) | 0.003* |
| Laboratory results | |||
| Hb (g/dl) | 13.9±1.6 | 13.6±1.7 | 0.245 |
| AU (mg/day) (mean and 25-75 percentile) | 457.48 (65.0-700.0) | 558.34 (75.1-789.1) | 0.078 |
| UA (umol/l) | 303±97.4 | 342±84.9 | 0.009* |
| Total cholesterol (mmol/l) (mean and 25-75 percentile) | 4.97 (4.28-5.51) | 4.79 (4.35-5.41) | 0.124 |
| HDL cholesterol (mmol/l) (mean and 25-75 percentilis) | 1.27 (1.03-1.44) | 1.21 (1.0-1.38) | 0.029* |
| TG (mmol/l) (mean and 25-75 percentilis) | 1.72 (0.93-2.04) | 1.99 (0.99-2.34) | 0.012* |
| Hypercholesterinemia (n/%) | 9 (15) | 21 (32) | 0.04* |
| Hypertriglyceridemia (n/%) | 5 (8) | 52 (80) | 0.001* |
| Earlier CV disease | |||
| Heart failure | 0 (0) | 1(1) | 0.176 |
| Stroke | 0 (0) | 1 (1) | 0.187 |
| CAD | 1 (2) | 3 (5) | 0.087 |
| COPD | 0 (0) | 1 (1) | 0.139 |
*= p <0.05. BP: blood pressure; BMI: body mass index; IFG: impaired fasting glucose; IGT: impaired glucose tolerance; eGFR: estimated glomerular filtration rate; ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; BB: beta blocker; CCB: calcium channel blocker; CAD: coronary artery disease; LV EF: left ventricle ejection fraction; LVMI: left ventricle mass index; LVEDD: left ventricular end-diastolic diameter; DD: diastolic dysfunction; E/A: early and late mitral inflow; cfPWV: carotid-femoral pulse wave velocity; Hb: hemoglobin; AU: albuminuria; UA: uric acid; HDL cholesterol: high-density lipoprotein cholesterol; TG: triglyceride; CAD: coronary artery disease; COPD: chronic pulmonary obstructive disease.
Table 2.
Distribution of metabolic parameters in MetS - and MetS + groups.
| HT (n/%) |
IFG/ IGT (n/%) |
DM (n/%) |
Obesity (n/%) |
Triglyceride (n/%) | HDL cholesterol (n/%) |
Number of positive parameters/ patients (average/n) |
|
| MetS + (n=65) | 53 (82) | 10 (15) | 21 (32) | 32 (49) | 52 (80) | 33 (51) | 201 (3.09) |
| MetS - (n=60) |
41 (68) | 2 (3) | 9 (15) | 2 (3) | 5 (8) | 15(25) | 74 (1.23) |
HT: hypertension; IFG: impaired fasting glucose, IGT: impaired gucose tolerance; DM: diabetes mellitus; MetS: metabolic syndrome, HDL: high-density lipoprotein.
Table 3.
Multivariate analyses on clinical data, metabolic parameters, echocardiographic parameters, and laboratory results in a competitive risk model.
Table 3.
Multivariate analyses on clinical data, metabolic parameters, echocardiographic parameters, and laboratory results in a competitive risk model.
| Clinical data (n=125) | OR | CI (95%) | p |
| Gender | 4.333 | 3.973-4.761 | 0.001* |
| Age | 2.906 | 2.198-3.214 | 0.026* |
| Average systolic BP | 0.800 | 0.290-0.993 | 0.354 |
| Average diastolic BP | 0.576 | 0.119-0.626 | 0.615 |
| 24h pulse pressure | 0.737 | 0.174-0.947 | 0.535 |
| Diurnal index systolic | 0.559 | 0.283-0.874 | 0.693 |
| Metabolic parameters | |||
| HT | 5.806 | 5.301-6.455 | 0.018* |
| DM | 1.912 | 1.808-2.178 | 0.011* |
| BMI | 2.205 | 1.913-2.742 | 0.021* |
| Dyslipidemia | 3.474 | 2.237-4.546 | 0.034* |
| Diabetes | 0.456 | 0.174-0.826 | 0.982 |
| IFG and IGT | 0.564 | 0.118-0.922 | 0.787 |
| Overweighted | 0.479 | 0.340-0.941 | 0.109 |
| Obesity | 0.367 | 0.204-0.530 | 0.607 |
| eGFR | 3.187 | 2.455-4.366 | 0.021* |
| Duration of kidney disease | 0.718 | 0.387-0.972 | 0.284 |
| Smoking | 0.341 | 0.327-0.823 | 0.499 |
| Echocardiographic parameters | |||
| LVEF | 0.635 | 0.602-0.968 | 0.526 |
| LVMI | 0.460 | 0.068-0.691 | 0.772 |
| LVEDD | 0.508 | 0.285-0.952 | 0.293 |
| Laboratory results | |||
| Hb | 2.237 | 2.151-2.486 | 0.029* |
| AU | 2.568 | 1.933-3.653 | 0.013* |
| UA | 1.837 | 1.735-1.952 | 0.021* |
| Total cholesterol | 0.903 | 0.450-0.937 | 0604 |
| HDL cholesterol | 0.476 | 0.045-0.846 | 0.997 |
| TG | 0.806 | 0.463-0.944 | 0.143 |
*= p<0.05. BP: blood pressure; HT: hypertension; DM: diabetes mellitus; BMI: body mass index; IFG: impaired fasting glucose; IGT: impaired glucose tolerance; eGFR:estimated glomerular filtration rate; LVEF: left ventricle ejection fraction; LVMI: left ventricle mass index; LVEDD: left ventricular end-diastolic diameter; Hb: hemoglobin; AU:albuminuria; UA: uric acid; HDL cholesterol: high-density lipoprotein cholesterol; TG: triglyceride.
Table 4.
Cox regression for the primary and secondary renal and cardiovascular endpoints.
| B | p | Exp(B) | 95% CI for Exp(B) lower |
95% CI for Exp(B) upper |
|
| Primary combined endpoint | |||||
| Gender | -0.898 | 0.078 | 0.408 | 0.150 | 1.104 |
| Age | 0.027 | 0.093 | 1.028 | 0.995 | 1.061 |
| Dyslipidemia | 1.144 | 0.034* | 3.140 | 1.091 | 9.042 |
| HT | -0.774 | 0.363 | 0.461 | 0.087 | 2.447 |
| DM | -0.964 | 0.031* | 0.381 | 0.159 | 0.914 |
| BMI | 0.014 | 0.787 | 1.014 | 0.916 | 1.123 |
| eGFR | -0.021 | 0.010* | 0.980 | 0.964 | 0.995 |
| Hb | -0.344 | 0.006* | 0.709 | 0.555 | 0.905 |
| AU | 0.001 | 0.001* | 1.001 | 1.001 | 1.002 |
| UA | 0.004 | 0.083 | 1.004 | 0.999 | 1.009 |
| Secondary renal endpoint | |||||
| Gender | -0.492 | 0.416 | 0.611 | 0.186 | 2.003 |
| Age | 0.021 | 0.234 | 1.021 | 0.986 | 1.058 |
| Dyslipidemia | 1.964 | 0.003* | 7.130 | 1.931 | 26.328 |
| HT | -0.743 | 0.430 | 0.476 | 0.075 | 3.011 |
| DM | -0.568 | 0.285 | 0.567 | 0.200 | 1.605 |
| BMI | 0.087 | 0.151 | 1.091 | 0.969 | 1.228 |
| eGFR | -0.030 | 0.004* | 0.971 | 0.951 | 0.991 |
| Hb | -0.493 | 0.002* | 0.611 | 0.444 | 0.841 |
| AU | 0.002 | 0.001* | 1.002 | 1.001 | 1.002 |
| UA | 0.005 | 0.119 | 1.005 | 0.999 | 1.011 |
| Secondary CV endpoint | |||||
| Gender | -2.632 | 0.029* | 0.072 | 0.007 | 0.759 |
| Age | 0.072 | 0.095 | 1.075 | 0.987 | 1.170 |
| Dyslipidemia | 0.571 | 0.531 | 1.771 | 0.296 | 10.581 |
| HT | -11.318 | 0.961 | 0.001 | 0.001 | 126.263 |
| DM | -2.240 | 0.002* | 0.106 | 0.025 | 0.454 |
| BMI | -0.231 | 0.029* | 0.794 | 0.646 | 0.976 |
| eGFR | -0.002 | 0.874 | 0.998 | 0.969 | 1.027 |
| Hb | -0.260 | 0.192 | 0.771 | 0.521 | 1.140 |
| AU | 0.001 | 0.744 | 1.000 | 0.999 | 1.001 |
| UA | 0.002 | 0.542 | 1.002 | 0.995 | 1.010 |
*= p <0.05. HT: hypertension; DM: diabetes mellitus; BMI: body mass index; eGFR: estimated glomerular filtration rate; Hb: hemoglobin; AU: albuminuria; UA: uric acid.
Table 5.
Cox proportional hazard ratios of the metabolic syndrome parameters for the primary and secondary endpoints.
Table 5.
Cox proportional hazard ratios of the metabolic syndrome parameters for the primary and secondary endpoints.
| B | p | Exp (B) | 95% CI for Exp(B) lower | 95% CI for Exp(B) upper | |
| Primary endpoint | |||||
| Dyslipidemia | -0.008 | 0.981 | 0.992 | 0.493 | 1.995 |
| HT | -1.249 | 0.102 | 0.287 | 0.064 | 1.279 |
| DM | -0.800 | 0.051 | 0.449 | 0.201 | 1.002 |
| BMI | -0.013 | 0.743 | 0.987 | 0.913 | 1.067 |
| UA | 0.006 | 0.002* | 1.006 | 1.002 | 1.009 |
| Secondary renal endpoint | |||||
| Dyslipidemia | 0.114 | 0.777 | 1.121 | 0.508 | 2.475 |
| HT | -0.828 | 0.290 | 0.437 | 0.094 | 2.024 |
| DM | -0.549 | 0.258 | 0.578 | 0.223 | 1.496 |
| BMI | 0.040 | 0.357 | 1.041 | 0.955 | 1.135 |
| UA | 0.006 | 0.003* | 1.006 | 1.002 | 1.010 |
| Secondary CV endpoint | |||||
| Dyslipidemia | -0.728 | 0.254 | 0.483 | 0.138 | 1.687 |
| HT | -12.342 | 0.971 | 0.001 | 0.001 | 8.049 |
| DM | -1.840 | 0.005* | 0.159 | 0.044 | 0.567 |
| BMI | -0.128 | 0.077 | 0.880 | 0.763 | 1.014 |
| UA | 0.004 | 0.150 | 1.004 | 0.998 | 1.010 |
*= p < 0.05. HT: hypertension, DM: diabetes mellitus, BMI: body mass index, UA: uric acid.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



