Submitted:
26 March 2024
Posted:
28 March 2024
You are already at the latest version
Abstract
Risk stratification for malignant ventricular arrhythmias and sudden cardiac death is a daunting task for physicians in daily practice. Multiparametric mapping sequences obtained via cardio-vascular magnetic resonance imaging can improve the risk for malignant ventricular arrhythmias by unveiling the presence of pathophysiological pro-arrhythmogenic processes. However, their employment in clinical practice is still restricted. The present review explores the current evidence supporting the association between mapping abnormalities and the risk of ventricular arrhyth-mias in several cardiovascular diseases. The key message is that further clinical studies are needed to test the additional value of mapping techniques beyond conventional cardiovascular magnetic resonance imaging for selecting patients eligible for an implantable cardioverter defibrillator.
Keywords:
Ventricular arrhythmias
; Sudden cardiac death
; Cardiovascular magnetic resonance
; mapping
Introduction
Risk stratification for malignant ventricular arrhythmias and sudden cardiac death (SCD) is a daunting task for physicians in daily practice. Left ventricular (LV) ejection fraction is the main traditional imaging parameter used for SCD risk stratification in ischemic and non-ischemic heart diseases, however it is not accurate to detect myocardial tissue alterations, which could trigger ventricular arrhythmias [1,2]. For instance, myocardial fibrosis and edema modulate myocardial electrical properties and represent a potential substrate for malignant ventricular arrhythmias [3]. Conventional cardiovascular magnetic resonance (CMR) sequences can unveil focal myocardial edema and fibrosis through T2-weighted imaging and late gadolinium enhancement (LGE). LGE has been repeatedly associated with an increased risk of SCD in ischemic and non-ischemic cardiomyopathies [4–7] and has been implemented in daily practice for clinical decision-making [8]. The introduction of the novel sequences of parametric mapping has unveiled diffuse pathophysiological processes, including extensive myocardial inflammation and/or interstitial myocardial fibrosis, which could not be captured with conventional tissue characterization techniques [9]. These sequences provide absolute quantification of the myocardial T1- and T2- relaxation values, potentially improving the accuracy, reproducibility, sensitivity and specificity of underlying pathophysiological processes compared to conventional imaging [10].
T1-mapping reflects the longitudinal or spin-lattice myocardial relaxation time, which is determined by how rapidly protons re-equilibrate their spins after being excited by a radiofrequency pulse. The Modified Look-Locker Inversion recovery (MOLLI) pulse sequences are among the most used CMR techniques to measure T1 relaxation times over 17 successive heartbeats. A pixel-wise illustration of absolute T1 relaxation times is represented on a color map. Pre-contrast and post-contrast T1-mapping are used to derive the myocardial extracellular volume (ECV), given that gadolinium-based contrast agents are distributed throughout the extracellular space and shorten T1 relaxation times of myocardium proportional to the local concentration of gadolinium. Estimation of the ECV can be obtained according to the formula:
T2-mapping reflects the transverse relaxation time, corresponding to the decoherence of the transverse nuclear spin magnetization. It is assessed through pixel-wise fitting for a T2 decay curve of a series of T2-weighted sequences. Turbo-Spin-Echo sequences with varying echo times are typically used, but alternative sequences are commercially available [10].
T2-mapping values are increased because of edema associated with acute myocardial inflammation or necrosis. Pre-contrast T1-mapping values are reduced in the presence of sphingolipid storage. Pre-contrast T1-mapping and ECV values are increased in case of acute inflammation or necrosis, replacement fibrosis, and diffuse fibrosis [11]; (see Figure 1).
Cardiovascular diseases can predispose to ventricular arrhythmias through several underlying structural mechanisms. An expansion of the myocardial extracellular space leads to mechanical and vasomotor dysfunction, key elements of electrical vulnerability. Increased automaticity can result from alterations of the basic cellular ion exchange secondary to several myocardial pathologies. The latter can also represent electrical obstacles, paving the way for re-entry arrhythmias. Moreover, myocardial inflammation can alter cell action potentials, triggering abnormal impulse initiation [12,13].
By sensitively and accurately unveiling potentially arrhythmogenic tissue alterations, mapping sequences are promising features to improve SCD risk stratification. The present review explores the current evidence supporting the association between these mapping abnormalities and the risk of malignant ventricular arrhythmias/SCD in ischemic and nonischemic cardiomyopathies; (see Table 1).
Figure 1.
Cardiovascular diseases and associated multiparametric CMR mapping changes. From left to right pre-contrast T1-mapping, T2-mapping and ECV variations are shown. ↑ increased, ↑↑ markedly increased, ↑= slightly increased or normal, ↓ reduced. DCM: dilated cardiomyopathy; HCM: hypertrophic cardiomyopathy.
Figure 1.
Cardiovascular diseases and associated multiparametric CMR mapping changes. From left to right pre-contrast T1-mapping, T2-mapping and ECV variations are shown. ↑ increased, ↑↑ markedly increased, ↑= slightly increased or normal, ↓ reduced. DCM: dilated cardiomyopathy; HCM: hypertrophic cardiomyopathy.
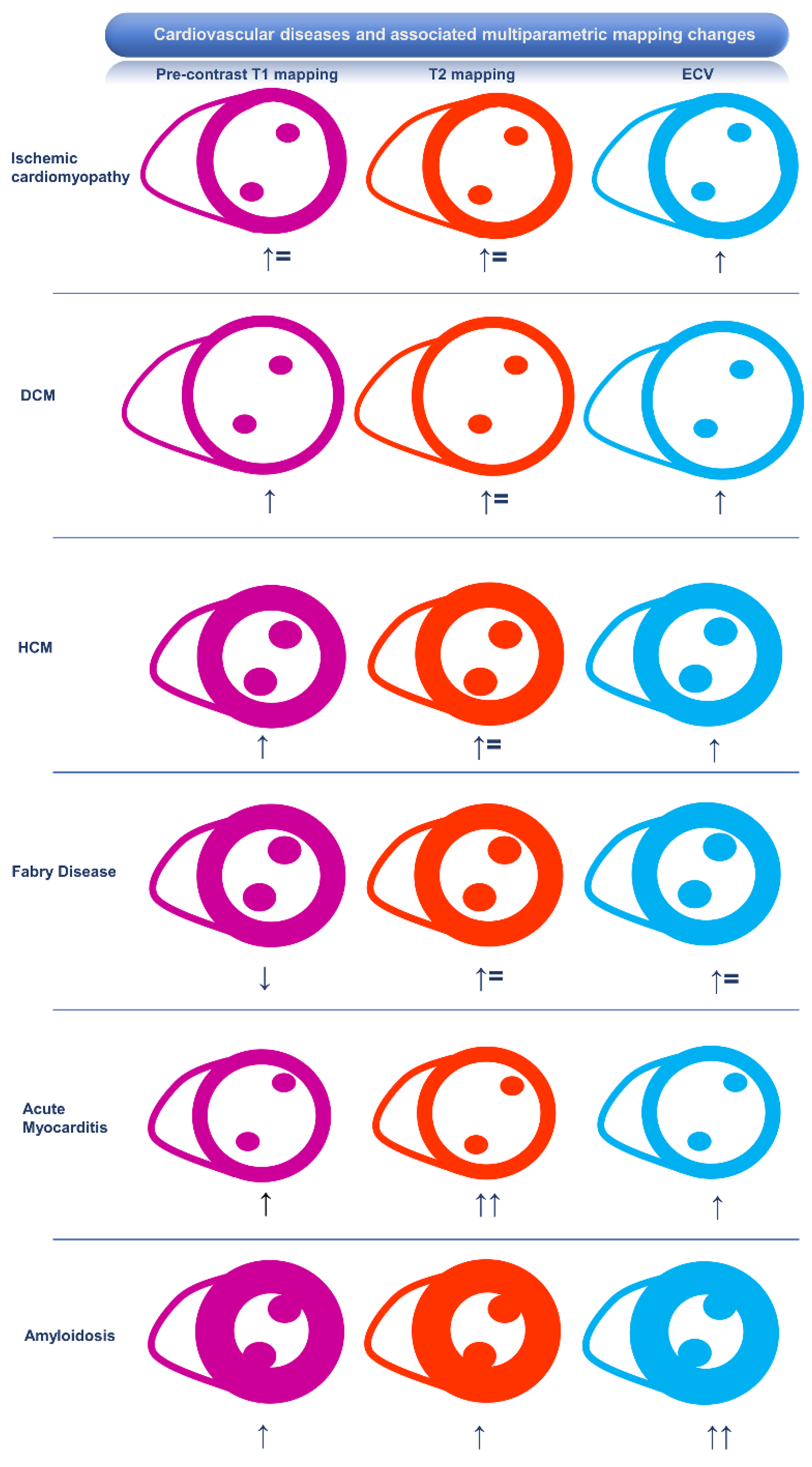
Figure 2.
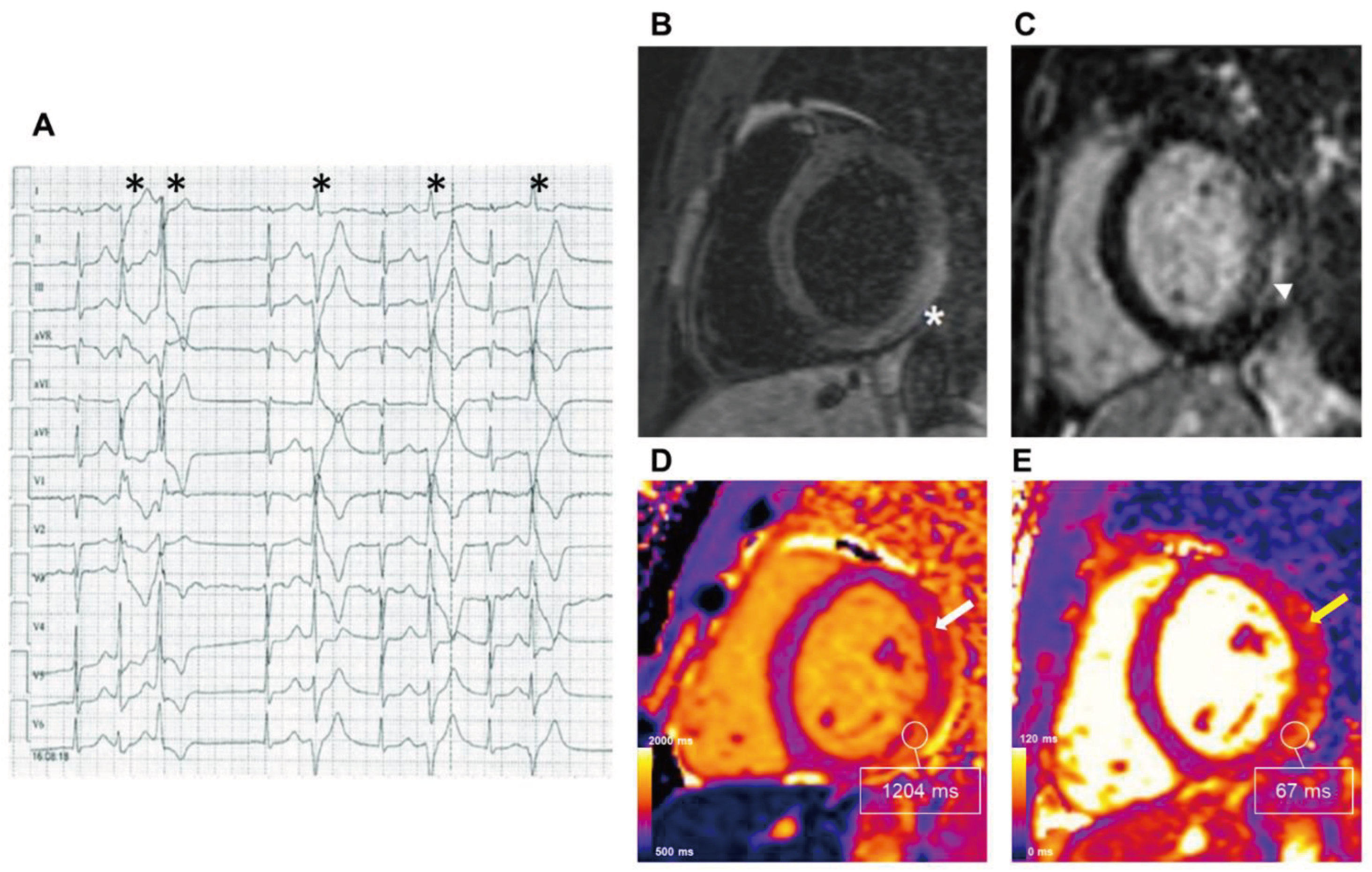
CMR findings in Acute Myocarditis presenting with ventricular arrhythmias. A 42-year-old female was admitted to the emergency department for palpitations, pre-syncope, and chest pain. Two days before she performed an ECG-Holter with evidence of frequent premature ventricular complexes and couplets, with RBBB morphology and superior axis (Panel A; asterisks). 1.5 T CMR was carried out three days later. (Panel B) T2W-TSE image in the short-axis plane revealed high signal intensity of the LV infero-lateral wall (asterisk). (Panel C) T1W post-contrast delayed inversion recovery sequences demonstrated areas of enhancement of the subepicardial region of the myocardium with normal subendocardial layer (short arrow), (Panel D) Short-axis native T1-mapping with an average of 1110 ms, mid-septum 1047 ms, infero-lateral wall 1204 ms, reference value <950 ms. (Panel E) Short axis T2-mapping revealed increased values with an average of 60 ms, mid-septum of 53 ms, and infero-lateral wall of 67 ms, reference value <55 ms. The tissue alterations were more evident and extensive in mapping sequences than those shown by conventional sequences, affecting also the antero-lateral LV wall (white and yellow arrows in Panels D and E, respectively). CMR: cardiovascular magnetic resonance; LV: left ventricular; RBBB: right bundle branch block.
Figure 2.
CMR findings in Acute Myocarditis presenting with ventricular arrhythmias. A 42-year-old female was admitted to the emergency department for palpitations, pre-syncope, and chest pain. Two days before she performed an ECG-Holter with evidence of frequent premature ventricular complexes and couplets, with RBBB morphology and superior axis (Panel A; asterisks). 1.5 T CMR was carried out three days later. (Panel B) T2W-TSE image in the short-axis plane revealed high signal intensity of the LV infero-lateral wall (asterisk). (Panel C) T1W post-contrast delayed inversion recovery sequences demonstrated areas of enhancement of the subepicardial region of the myocardium with normal subendocardial layer (short arrow), (Panel D) Short-axis native T1-mapping with an average of 1110 ms, mid-septum 1047 ms, infero-lateral wall 1204 ms, reference value <950 ms. (Panel E) Short axis T2-mapping revealed increased values with an average of 60 ms, mid-septum of 53 ms, and infero-lateral wall of 67 ms, reference value <55 ms. The tissue alterations were more evident and extensive in mapping sequences than those shown by conventional sequences, affecting also the antero-lateral LV wall (white and yellow arrows in Panels D and E, respectively). CMR: cardiovascular magnetic resonance; LV: left ventricular; RBBB: right bundle branch block.
Association of CMR Mapping Alterations and Ventricular Arrhythmias in Cardiovascular Diseases
Ischemic Heart Disease
Areas with previous myocardial infarction are characterized by increased ECV and native-T1 values and normal T2 values. These mapping changes indicate the replacement of myocyte loss by scar, a potential substrate for ventricular arrhythmias [13]. In a cohort of consecutive patients (130 patients: 71 ischemic and 59 non–ischemic) undergoing CMR, pre-contrast T1 values were significantly higher in patients experiencing a study endpoint including appropriate implantable cardioverter-defibrillator (ICD) therapy or sustained ventricular tachycardia [2]. Indeed, a recent study showed that diffuse myocardial fibrosis quantified by ECV is associated with ventricular arrhythmias requiring ICD therapy in a dose-response fashion, and provides superior discrimination compared to focal fibrosis identified by LGE [14].
In the context of an acute myocardial infarction, intramyocardial hemorrhage secondary to reperfusion damage leads to reduced T1- and T2-mapping values because of the paramagnetic effect of hemoglobin degradation products in the infarct core [10].
Native T1-mapping values are also reduced in lipomatous metaplasia within the area of myocardial infarction [15]. The presence of fat alters the electrical properties of the myocardium and might play a role in post-myocardial infarction arrhythmogenesis [16].
To the best of our knowledge, the role of T2-mapping as a marker of ventricular arrhythmias has not been explored. Overall, there is very limited evidence suggesting a potential role for multiparametric mapping in the identification of patients with ischemic heart disease and an increased risk of ventricular arrhythmias, but additional clinical studies may provide further clarification.
Inflammatory Cardiomyopathy
Ventricular arrhythmias are common in inflammatory cardiomyopathy, and 20-40% of cases of SCD have been associated with myocardial damage secondary to myocardial inflammation [17]. Increased pre-contrast T1-mapping values or ECV may be secondary to edema occurring in in areas of active inflammation or irreversible fibrotic tissue alterations after the acute phase of the disease has resolved [18]. Increased T2-mapping values only reflect active inflammation and are not impacted by underlying fibrosis, providing better differentiation between the active and chronic phases of inflammatory diseases [19].
Myocarditis
The proportion of SCD attributed to myocarditis at autopsy varies by age, causing approximately 2% of infant (0-2 years), 5% of childhood (3-18 years), and less than 10% to 20% of young (19-44 years) SCDs [20–22]. Recent evidence about parametric mapping in myocarditis stems from studies regarding immune check-point inhibitors (ICI)-related myocarditis, a condition associated with the use of ICI, drugs targeting the host immune regulatory pathways used in cancer therapy for an increasing number of malignancies, in some as first-line therapy. ICI-related myocarditis is an uncommon immune-related adverse event but associated with a high reported mortality [23]. Thavendiranathan et al. demonstrated an independent association between higher T1-mapping values and cardiovascular events in a cohort of patients with ICI-related myocarditis. This association, however, could not be replicated for T2 mapping values [24]. In patients with clinically suspected acute myocarditis, ECV ≥ 35% was found to be independently associated with a composite endpoint, including all-cause death, heart failure hospitalization, heart transplantation, documented sustained ventricular arrhythmia, and recurrent myocarditis [25]. Importantly, only the latter maintained a significant association with clinical outcomes in a multivariable model including age, LV ejection fraction, LGE, and increased ECV.
Sarcoidosis
The incidence of SCD in cardiac sarcoidosis is exceptionally high, up to 10.7% [26]. The presence of increased T2-mapping signal has been associated with more frequent adverse cardiac events, including significant arrhythmias (both atrial and ventricular) and related symptoms (palpitations or near syncope) [27]. Crouser et al. have shown an association between T2 elevation and electrophysiologic study abnormalities (atrial arrhythmia, ventricular arrhythmia, atrioventricular block, or QRS complex duration > 120 ms) [28]. In their population, the authors found that increased T2-mapping values in conjunction with LGE better predicted electrocardiographic abnormalities and arrhythmias compared with either parameter alone.
Connective Tissue Disorders
Autoimmune diseases affect the myocardium diffusely, and mapping sequences have shown an incremental diagnostic value compared to LGE sequences [29]. However, a recent study of thirty-four patients with systemic sclerosis found no association between ventricular arrhythmias and CMR multiparametric mapping alterations in asymptomatic patients [30].
Chagas Disease
The incidence of SCD is relevant in Chagas disease and risk stratification is poor with conventional assessment. A study including 90 patients with Chagas Disease demonstrated that remote native T1-values of more than 1100 ms were predictive of the composite endpoint, including ICD implantation, heart transplantation, or death [31].
Takotsubo Cardiomyopathy
Takotsubo cardiomyopathy is a reversible condition characterized by inflammation and edema, potentially associated with SCD [32,33]. Increased T2-mapping values typically normalize early after the acute phase whereas increased T1 mapping values might persist for months after the acute phase, despite normalization of LV ejection fraction and chamber dimensions and normal ECV [34–39]. To the best of our knowledge, no study explored the association between mapping alterations and ventricular arrhythmias in this condition.
Overall, further studies are necessary to corroborate a clinical role for multiparametric mapping in detecting patients with inflammatory heart diseases at increased risk of malignant ventricular arrhythmias.
Hypertrophic Cardiomyopathy and Phenocopies
Hypertrophic Cardiomyopathy
Predicting the risk of SCD in patients with hypertrophic cardiomyopathy (HCM) is crucial to selecting individuals who could benefit from prophylactic ICD implantation. The evaluation of LGE, especially if assessed quantitatively, has dramatically improved risk stratification as it is a high-risk feature of adverse outcomes [40–42] and has been consequently incorporated in currently recommended guideline algorithms. However, in addition to LGE, HCM is also typically characterized by diffuse myocardial fibrosis, which cannot be accurately distinguished by LGE, in contrast to T1-mapping and ECV. In a prospective study evaluating predictors of major adverse cardiovascular events in 203 HCM patients, it was found that, at multivariate analysis native T1 was associated with adverse outcomes (HR 1.45; p< 0.001), even in a subgroup of patients judged as low-risk per European and American guidelines [43]. In a study of 73 patients with HCM [44], global ECV was the best parameter to identify patients with a risk of SCD ≥4% and patients with syncope or non-sustained ventricular tachycardia (NSVT) at follow-up. Using a cut-off value of 34%, global ECV had an area-under-the-curve (AUC) of 0.83 to identify patients at higher risk of SCD, significantly higher than that of LGE. Similarly, ECV performed better than LGE in identifying patients with syncope or NSVT, and the addition of ECV to the recommended SCD risk score provided the best discriminatory ability to identify patients who could benefit most from ICD implantation. Another study of 108 HCM patients [45] suggested that ECV was an independent predictor of SCD (HR 1.27, p<0.001) and, compared to T1-mapping parameters, LGE and conventional risk score stratification, it was the most potent predictor of SCD with good discriminatory ability (AUC 0.85).
Post-contrast T1 values, an expression of interstitial myocardial fibrosis, were found to be associated with NSVT and aborted SCD, in a cohort of 100 patients with HCM [46]. While LGE presence did not differ between patients presenting with or without NSVT, patients with NSVT had significantly reduced values at post-contrast T1-mapping.
Higher values at T2-mapping, potentially signaling edema due to ischemia or microvascular dysfunction, are commonly found both in the hypertrophied and non-hypertrophied segments in HCM patients compared to normal controls [47]. In a prospective study of almost 700 patients with HCM [48], during a median follow-up of 3 years, patients with LGE and higher T2 values had a higher risk of the composite endpoint of cardiovascular death and appropriate ICD shocks. Including T2-mapping significantly increased the predictive performance of established risk factors, including extensive LGE.
Nevertheless, further prospective work is needed to establish the role of myocardial mapping parameters as prognostic factors in HCM and to integrate that information into current clinical algorithms. At present, the quantitative evaluation of LGE among other clinical and imaging predictors remains crucial for risk stratification. Patients presenting with significantly elevated T1, T2, or ECV values and lacking conventional risk factors should probably be followed more closely as they might carry a higher risk of ventricular arrythmias. A lower threshold for ICD implantation could be considered, while conclusive evidence is awaited.
Fabry Disease
Given that a reduction of native T1-mapping reflects globotriaosylceramide (Gb3) myocardial accumulation occurring before LV hypertrophy becomes manifest, CMR-based mapping allows an early diagnosis of Fabry Disease (FD) cardiac involvement [49]. FD cardiomyopathy progression leads to LV hypertrophy, “pseudo-normalization” of T1-mapping values, increased ECV, and eventually LGE in the infero-lateral LV wall [49–52]. Recently, Orsborne et al. developed a prognostic model for predicting adverse cardiac outcomes in this cohort of patients. In their study, T1 dispersion (standard deviation of per voxel [a single sample or data point] myocardial T1 relaxation times) was an independent predictor of a composite clinical outcome, which included ventricular tachycardia, aborted SCD, and appropriate ICD therapy. The authors hypothesized that a wider distribution of myocardial T1 relaxation time (i.e., T1 dispersion) would better reflect glycosphingolipid accumulation and consequent fibrosis/inflammation [53].
Amyloidosis
In patients with amyloidosis, the incidence of malignant ventricular arrhythmias is relatively low compared to other cardiac diseases [54]. Mapping alterations have been shown to be predictors of all-cause mortality or heart failure [55,595], but there is currently no evidence to suggest a role for these tissue alterations in ventricular arrhythmias.
Dilated Cardiomyopathy
T1-mapping techniques show potential in improving risk assessment for ventricular arrhythmias in patients with dilated cardiomyopathy (DCM) [57–59]. Interstitial fibrosis, characterized by intrinsic myocardial remodeling due to complex pathophysiological processes affecting the myocardium diffusely (not just focally), as shown by LGE, has been recently associated with life-threatening arrhythmias and all-cause mortality in DCM. A higher ECV has been independently associated with a composite endpoint of cardiovascular death, hospitalization for heart failure and appropriate ICD discharge [59].
In a recent investigation by Nakamori et al., DCM patients with a history of complex ventricular arrhythmias showed increased global native T1 values compared with age-matched DCM patients without any documented ventricular arrhythmia after adjusting for LV ejection fraction and LGE [60]. Pre-contrast T1 Z-score and ECV were independent predictors of arrhythmia-related events in a population of 225 patients with DCM [61]. In patients with DCM and without LGE, pre-contrast T1 and ECV values showed the best associations with a study endpoint, including heart failure, ventricular arrhythmias, and ICD or cardiac resynchronization therapy implantation, suggesting an added role for T1-mapping techniques on top of LGE conventional imaging [62]. Moreover, ECV might outperform LGE in the prediction of arrhythmias. In a population of patients with DCM, despite a similar distribution and extent of LGE between patients with and without ventricular arrhythmias, global and segmental ECV was higher in the group of patients with arrhythmias (global ECV: 30.3 ± 4.2 vs. 27.9 ± 4.9; p < 0.02), in line with an independent association of global ECV (HR 1.12, p < 0.02) and the arrhythmic burden [63]. T2 mapping values are altered in a subgroup of patients with DCM showing an underlying inflammatory background. However, there is no available evidence exploring the impact of these alterations on the arrhythmic risk [57]. As noted above, the evidence supporting a role for T1-mapping techniques appears almost ready for primetime in daily practice.
Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy
The annualized incidence rate of SCD in arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C) is 0.06% [64]. Biventricular and left-dominant disease variants have been identified [65]. In the multiparametric tissue characterization of patients with ARVD/C, elevated pre-contrast T1 values are consistent with advanced fibrosis, and reduced values with fibrofatty infiltration. The thin right ventricular wall limits the feasibility of T1-mapping analysis [65]. Chun et al. retrospectively analyzed 60 patients with ARVD/C. Kaplan-Meier survival analysis revealed that heart-failure-related events were more frequent in patients with increased values of pre-contrast T1-mapping and ECV. However, the authors found no association between mapping alterations and ventricular arrhythmias [66]. Further studies are awaited to explore the value of multiparametric mapping for prediction of ventricular arrhythmias in arrhythmogenic cardiomyopathy.
Mitral Valve Prolapse
A subgroup of patients with mitral valve prolapse (MVP) is exposed to an increased risk of SCD, the so-called “arrhythmic MVP.” Myocardial fibrosis, particularly in the sites most subject to the mechanical traction related to MVP mechanisms (i.e., papillary muscles and LV posterior wall), is emerging as a detrimental player in this setting [67]. Notably, myocardial fibrosis depicted in pathological studies was “interstitial,” which can be missed by conventional LGE, whereas T1-mapping techniques are potentially more accurate. Patients with MVP have shown increased pre-contrast T1 values in basal- and mid-posterior segments compared to other myocardial segments [68].
Accordingly, mapping techniques have been tested to unveil patients at higher risk of arrhythmias. In an investigation including 23 patients with MVP with ECG-Holter monitoring, LV septal post-contrast T1 times were shorter in patients with complex ventricular arrhythmias compared to those without [69]. Accordingly, in another study including 30 patients with MVP, basal posterior ECV > 33.5% and LGE performed equally in identifying those with a history of aborted SCD. Among patients with available ECG-Holter monitoring, ECV was more accurate than LGE in identifying those with complex ventricular arrhythmias, suggesting an additional value beyond conventional tissue characterization in the arrhythmic risk stratification [70]. These findings were not confirmed in a subsequent investigation, including 42 patients with MVP, in which the ECV in the basal segments did not differ between patients with and without complex ventricular arrhythmias [71]. Similarly, no associations between T1-mapping values and complex ventricular arrhythmias were found in a study including 34 patients with MVP [72]. Thus, despite the potential theoretical advantages, mapping techniques have provided conflicting results on the association with ventricular arrhythmias in patients with MVP. Small sample sizes and methodological discrepancies in evaluating the arrhythmic outcome via T1-mapping may explain such inconsistencies.
Future Perspectives for CMR Mapping in Clinical Practice
The potential advantage of CMR-mapping sequences in the clinical context of ventricular arrhythmias is the possibility of accurately identifying and quantifying arrhythmogenic pathological processes that escape conventional tissue characterization, ultimately, with the goal of improving the risk stratification for SCD. As a result, selection of patients undergoing primary prevention ICD implantation would be expected to improve. Further development of more robust non-invasive cardiac imaging selection criteria could solidify the pathway cardiologists and invasive cardiac electrophysiologists follow for primary prevention of sudden cardiac death [73]. ICD implantation impacts health system costs, quality of life, and may result in clinical complications [74]. Dedicated, large, multicenter studies comparing the potential benefits of mapping sequences to conventional tissue characterization (e.g., LV ejection fraction) are needed before the clinical implementation of these sequences are used in daily practice to select patients for ICD implantation and effectively prevent SCD. In this scenario, ECV might be preferred over absolute T1-mapping measurements given the better reproducibility and the less influence of local variables on its values [75].
Another potential application of CMR mapping sequences is the guidance of invasive ablation procedures. Conventional LGE imaging is used for this purpose. It allows targeting the arrhythmic substrate and evaluating the location, depth, and possible gaps between radiofrequency lesions without ionizing radiation [76–78]. However, the lack of sensitivity and accuracy for subtle, diffuse pathological processes renders this approach prone to failure in some myocardial pathologies, particularly in non-ischemic cardiomyopathies. In contrast, CMR-mapping sequences might better delineate arrhythmogenic myocardial areas, reducing failure rates following LGE imaging alone. The latter relies on an arbitrary scale of the relative signal intensity difference detected between regions of dense scar and regions of user-defined “normal” tissue. Even in patients with ischemic heart disease, non-infarct regions seen as “normal” on contrast enhanced CMR imaging may contain diffuse interstitial fibrosis as a result of adverse remodeling and are potentially arrhythmogenic [2]. To our knowledge, CMR mapping sequences have yet to be tested for this potential clinical role.
Conclusions
The present review highlights that current evidence supporting the clinical use of mapping techniques to improve the risk stratification for SCD, although promising, is unproven in most clinical contexts. Larger clinical studies are awaited to test the additional value of mapping techniques beyond conventional CMR imaging for selecting patients eligible for a primary prevention ICD in daily practice.

Table 1.
Evidence exploring the association between CMR multiparametric mapping and Ventricular Arrhythmias/Sudden Cardiac Death in cardiovascular diseases.
Table 1.
Evidence exploring the association between CMR multiparametric mapping and Ventricular Arrhythmias/Sudden Cardiac Death in cardiovascular diseases.
| Study First Author, Year | Type of Cardiomyopathy | Number of patients | Type of study | Mapping parameter | Study endpoint | Association of mapping parameter with the study endpoint |
|---|---|---|---|---|---|---|
| Chen, 2015 [2] | Ischemic cardiomyopathy | 130 | Prospective | 10 ms increase of native T1 mapping | Appropriate ICD therapy or documented sustained VA | HR 1.1 (95% CI 1.0-1.2) |
| Olausson, 2023 [13] | Ischemic cardiomyopathy | 215 | Retrospective | 5% increase in ECV | Time from ICD implantation to appropriate shock or anti-tachycardia pacing | HR 2.2 (95% CI 1.2-4.0) |
| Gräni, 2019 [24] | Myocarditis | 179 | Retrospective | ECV ≥ 35% | MACE (all-cause death, HF hospitalization, heart transplantation, documented sustained VA, and recurrent myocarditis) | HR 3.3 (95% CI 1.4-8.0) |
| Thavendiranathan, 2021 [23] | Myocarditis | 136 | Retrospective | Every 1-unit increase in T1-mapping z-score | MACE (cardiovascular death, cardiogenic shock, cardiac arrest and complete heart block) | HR 1.4 (95% CI 1.1-1.8) |
| Crouser, 2014 [27] | Sarcoidosis | 50 | Retrospective | T2 mapping | Conduction system disease and cardiac arrhythmias (atrial arrhythmia, ventricular arrhythmia, atrioventricular block, or QRS complex duration > 120 ms) | T2-mapping significantly higher in patients with the study endpoint |
| Crouser, 2016 [26] | Sarcoidosis | 8 | Retrospective | T2 mapping > 70 ms | Reversible cardiac arrhythmias (atrial arrhythmia, ventricular arrhythmia, atrioventricular block, or QRS complex duration > 120 ms) after immune suppression therapy | T2-mapping significantly higher in patients with the study endpoint |
| Pinheiro, 2020 [72] | Chagas | 62 | Cross-sectional | T1 mapping > 1200 ms, ECV > 25% | NSVT | AUC 0.81 (95% CI 0.65–0.97) and 0.85 (95% CI 0.71–0.99), respectively. |
| Qin, 2021 [42] | HCM | 203 | Prospective | Native T1 mapping > 1,299.6 ms | MACE (cardiac death, transplantation, HF admission, and ICD implantation) | HR 1.45 (95% CI 1.26-1.77) |
| Avanesov, 2017 [43] | HCM | 73 | Retrospective | Global ECV ≥ 35% | SCD, syncope, NSVT | AUC 0.83 (95% CI 0.73-0.91) |
| Yu, 2023 [44] | HCM | 108 | Retrospective | Global ECV ≥ 35% | SCD | HR 1.27 (95% CI 1.1-1.47) |
| McLellan, 2016 [45] | HCM | 100 | Prospective | Post-contrast T1 mapping (median value 422 ± 54 ms) | NSVT | Post-contrast T1 (p = 0.004) |
| Xu, 2023 [47] | HCM | 674 | Prospective | 2 ms increase in T2-mapping | Cardiovascular death and appropriate ICD discharge | HR 1.43 (95% CI 1.18-1.72) |
| Orsborne, 2022 [52] | Fabry disease | 200 | Prospective | T1 dispersion | Adverse cardiac outcome (first hospitalization for HF, MI, coronary revascularization, VT sustained or nonsustained, new AF, bradyarrhythmia necessitating PM implantation, aborted SCD, appropriate ICD therapy, or cardiovascular death | HR 1.012 (95% CI 1.002-1.021) |
| Nakamori, 2018 [59] | DCM | 107 | Retrospective | 10 ms increment in T1-mapping | Complex VA | OR 1.14 (95% CI 1.03-1.25) |
| Barison, 2015 [58] | DCM | 89 | Retrospective | ECV > 29% | Cardiovascular death, hospitalization for HF and appropriate ICD intervention | p < 0.05 |
| Cadour, 2023 [60] | DCM | 225 | Prospective | T1 mapping Z-score > 4.2, ECV > 30.5% | MACE (HF-related events and arrhythmia-related events) | HR 2.86 (95% CI 1.06-7.68) and HR 2.72 (95% CI 1.01-7.36), respectively |
| Li, 2022 [73] | DCM | 659 | Retrospective | T1 mapping > 1000 ms, ECV > 30.5% | Cardiac-related death, heart transplantation, hospitalization for HF, VA, and ICD or CRT implantation | HR 1.13 (95% CI 1.10-1.36) and HR 1.32; (95% CI 1.12-1.53), respectively |
| Rubiś, 2021 [62] | DCM | 102 | Prospective | ECV | Arrhythmic burden (ventricular tachycardia or a high burden of PVCs) | HR 1.12 (95% CI 1.0-1.25) |
| Chun, 2022 [65] | ARVD/C | 60 | Retrospective | T1 mapping, T2 mapping, ECV | HF-related events (hospitalization, heart transplantation, and cardiac death) and ventricular tachycardia events | More HF-related events: higher native T1 (log-rank p = 0.002), T2 (log-rank p = 0.002) and ECV (log-rank p = 0.002) |
| Pavon, 2021 [69] | MVP | 30 | Retrospective | Synthetic ECV > 27% | Ventricular arrhythmic events (recent history of unexplained resuscitated OHCA and complex PVC) | AUC 0.83 |
| Bui, 2017 [68] | MVP | 41 | Retrospective | Post-contrast T1 mapping | Complex VA | Shorter post-contrast T1 in patients with complex VA |
ARVD/C: Arrhythmogenic right ventricular dysplasia/cardiomyopathy; AUC: area under the curve; CMR: cardiovascular magnetic resonance; HR: hazard ratio; OR: odds ratio; CI: confidence interval; MACE: major adverse cardiovascular events; HCM: hypertrophic cardiomyopathy; SCD: sudden cardiac death; NSVT: non-sustained ventricular tachycardia; ICD: implantable cardioverter-defibrillator; CRT: cardiac resynchronization therapy; PM: pace-maker; ComVA: complex ventricular arrhythmias; PVC: premature ventricular complex; HF: heart failure; MI: myocardial infarction; VT: ventricular tachycardia, AF: atrial fibrillation; MVP: mitral valve prolapse; VA: ventricular arrhythmias; OHCA: out-of-hospital cardiac arrest.
Funding
This research received no external funding.
Institutional Review Board Statement
This literature review study did not require ethical approval.
Informed Consent Statement
Not applicable: literature review.
Data Availability Statement
Data sharing not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| DCM | dilated cardiomyopathy |
| ECV | extracellular volume |
| FD | Fabry Disease |
| HCM | hypertrophic cardiomyopathy |
| ICD | implantable cardioverter-defibrillator |
| ICI | immune check-point inhibitor |
| LGE | late gadolinium enhancement |
| LV | left ventricular |
| MVP | mitral valve prolapse |
| SCD | sudden cardiac death |
References
- Tamene, A.; Tholakanahalli, V.N.; Chandrashekhar, Y. Cardiac imaging in evaluating patients prone to sudden death. Indian Heart J. 2014, 66 (Suppl. 1), S61–S70. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Sohal, M.; Voigt, T.; Sammut, E.; Tobon-Gomez, C.; Child, N.; Jackson, T.; Shetty, A.; Bostock, J.; Cooklin, M.; et al. Myocardial tissue characterization by cardiac magnetic resonance imaging using T1 mapping predicts ventricular arrhythmia in ischemic and non-ischemic cardiomyopathy patients with implantable cardioverter-defibrillators. Heart Rhythm. 2015, 12, 792–801. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.C.; Messroghli, D.R.; Kellman, P.; Piechnik, S.K.; Robson, M.D.; Ugander, M.; Gatehouse, P.D.; Arai, A.E.; Friedrich, M.G.; Neubauer, S.; et al. Myocardial T1 mapping and extracellular volume quantification: a Society for Cardiovascular Magnetic Resonance (SCMR) and CMR Working Group of the European Society of Cardiology consensus statement. J. Cardiovasc. Magn. Reson. 2013, 15, 92. [Google Scholar] [CrossRef] [PubMed]
- Keil, L.; Chevalier, C.; Kirchhof, P.; Blankenberg, S.; Lund, G.; Müllerleile, K.; Magnussen, C. CMR-Based Risk Stratification of Sudden Cardiac Death and Use of Implantable Cardioverter–Defibrillator in Non-Ischemic Cardiomyopathy. Int. J. Mol. Sci. 2021, 22, 7115. [Google Scholar] [CrossRef] [PubMed]
- Figliozzi, S.; Georgiopoulos, G.; Lopes, P.M.; Bauer, K.B.; Moura-Ferreira, S.; Tondi, L.; Mushtaq, S.; Censi, S.; Pavon, A.G.; Bassi, I.; et al. Myocardial Fibrosis at Cardiac MRI Helps Predict Adverse Clinical Outcome in Patients with Mitral Valve Prolapse. Radiology 2023, 306, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Georgiopoulos, G.; Figliozzi, S.; Pateras, K.; et al. Comparison of Demographic, Clinical, Biochemical, and Imaging Findings in Hypertrophic Cardiomyopathy Prognosis: A Network Meta-Analysis. JACC Heart Fail 2023, 11, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Georgiopoulos, G.; Figliozzi, S.; Sanguineti, F.; et al. Prognostic Impact of Late Gadolinium Enhancement by Cardiovascular Magnetic Resonance in Myocarditis: A Systematic Review and Meta-Analysis. Circ Cardiovasc Imaging 2021, 14, e011492. [Google Scholar] [CrossRef]
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J 2022, 43, 3997–4126. [Google Scholar]
- Carrabba, N.; Amico, M.A.; Guaricci, A.I.; Carella, M.C.; Maestrini, V.; Monosilio, S.; Pedrotti, P.; Ricci, F.; Monti, L.; Figliozzi, S.; et al. CMR Mapping: The 4th-Era Revolution in Cardiac Imaging. J. Clin. Med. 2024, 13, 337. [Google Scholar] [CrossRef]
- Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J. Cardiovasc. Magn. Reson. 2017, 19, 75. [Google Scholar] [CrossRef]
- Jugdutt, B.I. Ventricular remodeling after infarction and the extracellular collagen matrix: when is enough enough? Circulation 2003, 108, 1395–403. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.C.; Messroghli, D.R.; Kellman, P.; Piechnik, S.K.; Robson, M.D.; Ugander, M.; Gatehouse, P.D.; E Arai, A.; Friedrich, M.G.; Neubauer, S.; et al. Myocardial T1 mapping and extracellular volume quantification: a Society for Cardiovascular Magnetic Resonance (SCMR) and CMR Working Group of the European Society of Cardiology consensus statement. J. Cardiovasc. Magn. Reson. 2013, 15, 92. [Google Scholar] [CrossRef] [PubMed]
- Antzelevitch, C.; Burashnikov, A. Overview of Basic Mechanisms of Cardiac Arrhythmia. Card. Electrophysiol. Clin. 2011, 3, 23–45. [Google Scholar] [CrossRef] [PubMed]
- Amoni, M.; Dries, E.; Ingelaere, S.; Vermoortele, D.; Roderick, H.L.; Claus, P.; Willems, R.; Sipido, K.R. Ventricular Arrhythmias in Ischemic Cardiomyopathy—New Avenues for Mechanism-Guided Treatment. Cells 2021, 10, 2629. [Google Scholar] [CrossRef] [PubMed]
- Olausson, E.; Wertz, J.; Fridman, Y.; et al. Diffuse myocardial fibrosis associates with incident ventricular arrhythmia in implantable cardioverter defibrillator recipients. medRxiv 2023. [Google Scholar] [CrossRef]
- Haaf, P.; Garg, P.; Messroghli, D.R.; Broadbent, D.A.; Greenwood, J.P.; Plein, S. Cardiac T1 Mapping and Extracellular Volume (ECV) in clinical practice: a comprehensive review. J. Cardiovasc. Magn. Reson. 2016, 18, 89. [Google Scholar] [CrossRef] [PubMed]
- de Bakker, J.M.; van Capelle, F.J.; Janse, M.J.; A Wilde, A.; Coronel, R.; E Becker, A.; Dingemans, K.P.; van Hemel, N.M.; Hauer, R.N. Reentry as a cause of ventricular tachycardia in patients with chronic ischemic heart disease: electrophysiologic and anatomic correlation. Circulation 1988, 77, 589–606. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, M.G.; Sechtem, U.; Schulz-Menger, J.; et al. Cardiovascular magnetic resonance in myocarditis: A JACC White Paper. J Am Coll Cardiol 2009, 53, 1475–1487. [Google Scholar] [CrossRef]
- Ferreira, V.M.; Piechnik, S.K.; Dall’Armellina, E.; Karamitsos, T.D.; Francis, J.M.; Choudhury, R.P.; Friedrich, M.G.; Robson, M.D.; Neubauer, S. Non-contrast T1-mapping detects acute myocardial edema with high diagnostic accuracy: a comparison to T2-weighted cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2012, 14, 42. [Google Scholar] [CrossRef]
- Fernández-Jiménez, R.; Sánchez-González, J.; Aguero, J.; del Trigo, M.; Galán-Arriola, C.; Fuster, V.; Ibáñez, B. Fast T2 gradient-spin-echo (T2-GraSE) mapping for myocardial edema quantification: first in vivo validation in a porcine model of ischemia/reperfusion. J. Cardiovasc. Magn. Reson. 2015, 17, 92. [Google Scholar] [CrossRef]
- Harmon, K.G.; Asif, I.M.; Maleszewski, J.J.; Owens, D.S.; Prutkin, J.M.; Salerno, J.C.; Zigman, M.L.; Ellenbogen, R.; Rao, A.L.; Ackerman, M.J.; et al. Incidence and etiology of sudden cardiac arrest and death in high school athletes in the united states. Mayo Clin. Proc. 2016, 91, 1493–1502. [Google Scholar] [CrossRef]
- Maron, B.J.; Udelson, J.E.; Bonow, R.O.; Nishimura, R.A.; Ackerman, M.J.; Estes, N.M.; Cooper, L.T.; Link, M.S.; Maron, M.S. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: task force 3: hypertrophic cardiomyopathy, arrhythmogenic right ventricular cardiomyopathy and other cardiomyopathies, and myocarditis: A scientific statement from the american heart association and american college of cardiology. J. Am. Coll. Cardiol. 2015, 66, 2362–2371. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.T. Ventricular arrhythmias and sudden cardiac death in lymphocytic myocarditis. J. Am. Coll. Cardiol. 2020, 75, 1058–1060. [Google Scholar] [CrossRef] [PubMed]
- Palaskas, N.; Lopez-Mattei, J.; Durand, J.B.; Iliescu, C.; Deswal, A. Immune Checkpoint Inhibitor Myocarditis: Pathophysiological Characteristics, Diagnosis, and Treatment. J. Am. Heart Assoc. 2020, 9, e013757. [Google Scholar] [CrossRef] [PubMed]
- Thavendiranathan, P.; Zhang, L.; Zafar, A.; Drobni, Z.D.; Mahmood, S.S.; Cabral, M.; Awadalla, M.; Nohria, A.; Zlotoff, D.A.; Thuny, F.; et al. Myocardial T1 and T2 Mapping by Magnetic Resonance in Patients With Immune Checkpoint Inhibitor–Associated Myocarditis. J. Am. Coll. Cardiol. 2021, 77, 1503–1516. [Google Scholar] [CrossRef] [PubMed]
- Gräni, C.; Bière, L.; Eichhorn, C.; Kaneko, K.; Agarwal, V.; Aghayev, A.; Steigner, M.; Blankstein, R.; Jerosch-Herold, M.; Kwong, R.Y. Incremental value of extracellular volume assessment by cardiovascular magnetic resonance imaging in risk stratifying patients with suspected myocarditis. Int. J. Cardiovasc. Imaging 2019, 35, 1067–1078. [Google Scholar] [CrossRef]
- Nordenswan, H.-K.; Pöyhönen, P.; Lehtonen, J.; Ekström, K.; Uusitalo, V.; Niemelä, M.; Vihinen, T.; Kaikkonen, K.; Haataja, P.; Kerola, T.; et al. Incidence of Sudden Cardiac Death and Life-Threatening Arrhythmias in Clinically Manifest Cardiac Sarcoidosis With and Without Current Indications for an Implantable Cardioverter Defibrillator. Circulation 2022, 146, 964–975. [Google Scholar] [CrossRef] [PubMed]
- Crouser, E.D.; Ruden, E.; Julian, M.W.; Raman, S.V. Resolution of abnormal cardiac MRI T2 signal following immune suppression for cardiac sarcoidosis. J. Investig. Med. 2016, 64, 1148–1150. [Google Scholar] [CrossRef]
- Crouser, E.D.; Ono, C.; Tran, T.; He, X.; Raman, S.V. Improved detection of cardiac sarcoidosis using magnetic resonance with myocardial T2 mapping. Am. J. Respir. Crit. Care Med. 2014, 189, 109–112. [Google Scholar] [CrossRef]
- Mayr, A.; Kitterer, D.; Latus, J.; Steubing, H.; Henes, J.; Vecchio, F.; Kaesemann, P.; Patrascu, A.; Greiser, A.; Groeninger, S.; et al. Evaluation of myocardial involvement in patients with connective tissue disorders: a multi-parametric cardiovascular magnetic resonance study. J. Cardiovasc. Magn. Reson. 2016, 18, 67. [Google Scholar] [CrossRef]
- Ross, L.; Costello, B.; Brown, Z.; Hansen, D.; Lindqvist, A.; Stevens, W.; Burns, A.; Prior, D.; Nikpour, M.; La Gerche, A. Myocardial fibrosis and arrhythmic burden in systemic sclerosis. Rheumatology 2022, 61, 4497–4502. [Google Scholar] [CrossRef]
- Melo, R.J.L.; Assunção, A.N., Jr.; Morais, T.C.; Nomura, C.H.; Scanavacca, M.I.; Martinelli-Filho, M.; Ramires, F.J.A.; Fernandes, F.; Ianni, B.M.; Mady, C.; et al. Detection of Early Diffuse Myocardial Fibrosis and Inflammation in Chagas Cardiomyopathy with T1 Mapping and Extracellular Volume. Radiol. Cardiothorac. Imaging 2023, 5, e220112. [Google Scholar] [CrossRef] [PubMed]
- Manolis, T.A.; Melita, H.; Manolis, A.S. Takotsubo syndrome and sudden cardiac death. Angiology 2023, 74, 105–128. [Google Scholar] [CrossRef] [PubMed]
- Koh, Y.; Voskoboinik, A.; Neil, C. Arrhythmias and their electrophysiological mechanisms in takotsubo syndrome: A narrative review. Heart Lung Circ. 2022, 31, 1075–1084. [Google Scholar] [CrossRef]
- Citro, R.; Okura, H.; Ghadri, J.R.; Izumi, C.; Meimoun, P.; Izumo, M.; Dawson, D.; Kaji, S.; Eitel, I.; Kagiyama, N.; et al. Multimodality imaging in takotsubo syndrome: a joint consensus document of the European Association of Cardiovascular Imaging (EACVI) and the Japanese Society of Echocardiography (JSE). Eur. Heart J. Cardiovasc. Imaging 2020, 21, 1184–1207. [Google Scholar] [CrossRef]
- Scally, C.; Rudd, A.; Mezincescu, A.; Wilson, H.M.; Srivanasan, J.; Horgan, G.; Broadhurst, P.; Newby, D.E.; Henning, A.; Dawson, D. Persistent Long-Term Structural, Functional, and Metabolic Changes After Stress-Induced (Takotsubo) Cardiomyopathy. Circulation 2018, 137, 1039–1048. [Google Scholar] [CrossRef]
- Schwarz, K.; Ahearn, T.; Srinivasan, J.; Neil, C.J.; Scally, C.; Rudd, A.; Jagpal, B.; Frenneaux, M.P.; Pislaru, C.; Horowitz, J.D.; et al. Alterations in Cardiac Deformation, Timing of Contraction and Relaxation, and Early Myocardial Fibrosis Accompany the Apparent Recovery of Acute Stress-Induced (Takotsubo) Cardiomyopathy: An End to the Concept of Transience. J. Am. Soc. Echocardiogr. 2017, 30, 745–755. [Google Scholar] [CrossRef]
- Mathai, S.; Sehmi, J.; Auger, D.; Heureux, C.L.; Keenan, N.G. Role of T1 mapping in identification of convalescent Takotsubo cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2021, 22 (Supplement_1). [Google Scholar] [CrossRef]
- Cau, R.; Pisu, F.; Porcu, M.; Cademartiri, F.; Montisci, R.; Bassareo, P.; Muscogiuri, G.; Amadu, A.; Sironi, S.; Esposito, A.; et al. Machine learning approach in diagnosing Takotsubo cardiomyopathy: The role of the combined evaluation of atrial and ventricular strain, and parametric mapping. Int. J. Cardiol. 2023, 373, 124–133. [Google Scholar] [CrossRef]
- Gil, K.E.; Truong, V.T.; Zareba, K.M.; Varghese, J.; Simonetti, O.P.; Rajpal, S. Parametric mapping by cardiovascular magnetic resonance imaging in sudden cardiac arrest survivors. Int. J. Cardiovasc. Imaging 2023, 39, 1547–1555. [Google Scholar] [CrossRef]
- Chan, R.H.; Maron, B.J.; Olivotto, I.; Pencina, M.J.; Assenza, G.E.; Haas, T.; Lesser, J.R.; Gruner, C.; Crean, A.M.; Rakowski, H.; et al. Prognostic value of quantitative contrast-enhanced cardiovascular magnetic resonance for the evaluation of sudden death risk in patients with hypertrophic cardiomyopathy. Circulation 2014, 130, 484–495. [Google Scholar] [CrossRef]
- Weng, Z.; Yao, J.; Chan, R.H.; He, J.; Yang, X.; Zhou, Y.; He, Y. Prognostic Value of LGE-CMR in HCM: A Meta-Analysis. JACC: Cardiovascular Imaging 2016, 9, 1392–140. [Google Scholar] [PubMed]
- Stankowski, K.; Figliozzi, S.; Lisi, C.; Catapano, F.; Panico, C.; Cannata, F.; Mantovani, R.; Frontera, A.; Bragato, R.M.; Stefanini, G.; et al. Solving the Riddle of Sudden Cardiac Death in Hypertrophic Cardiomyopathy: The Added Role of Cardiac Magnetic Resonance. J. Cardiovasc. Dev. Dis. 2023, 10, 226. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; Min, J.; Chen, C.; Zhu, L.; Gu, S.; Zhou, M.; Yang, W.; Yan, F. Incremental values of T1 mapping in the prediction of sudden cardiac death risk in hypertrophic cardiomyopathy: A comparison with two guidelines. Front. Cardiovasc. Med. 2021, 8, 661673. [Google Scholar] [CrossRef]
- Avanesov, M.; Münch, J.; Weinrich, J.; Well, L.; Säring, D.; Stehning, C.; Tahir, E.; Bohnen, S.; Radunski, U.K.; Muellerleile, K.; et al. Prediction of the estimated 5-year risk of sudden cardiac death and syncope or non-sustained ventricular tachycardia in patients with hypertrophic cardiomyopathy using late gadolinium enhancement and extracellular volume CMR. Eur. Radiol. 2017, 27, 5136–5145. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Cai, Z.; Yang, Z.; Lin, W.; Su, Y.; Li, J.; Xie, S.; Shen, J. The Value of Myocardial Fibrosis Parameters Derived from Cardiac Magnetic Resonance Imaging in Risk Stratification for Patients with Hypertrophic Cardiomyopathy. Acad. Radiol. 2023, 30, 1962–1978. [Google Scholar] [CrossRef]
- McLELLAN, A.J.A.; Ellims, A.H.; Prabhu, S.; Voskoboinik, A.; Iles, L.M.; Hare, J.L.; Kaye, D.M.; Macciocca, I.; Mariani, J.A.; Kalman, J.M.; et al. Diffuse ventricular fibrosis on cardiac magnetic resonance imaging associates with ventricular tachycardia in patients with hypertrophic cardiomyopathy. J. Cardiovasc. Electrophysiol. 2016, 27, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Ran, L.; Zhao, P.; Tang, D.; Han, R.; Ai, T.; Xia, L.; Tao, Q. MRI native T1 and T2 mapping of myocardial segments in hypertrophic cardiomyopathy: tissue remodeling manifested prior to structure changes. Br. J. Radiol. 2019, 92, 20190634. [Google Scholar] [CrossRef]
- Xu, Z.; Wang, J.; Cheng, W.; Wan, K.; Li, W.; Pu, L.; Xu, Y.; Sun, J.; Han, Y.; Chen, Y. Incremental significance of myocardial oedema for prognosis in hypertrophic cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2023, 24, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Camporeale, A.; Pieroni, M.; Pieruzzi, F.; Lusardi, P.; Pica, S.; Spada, M.; Mignani, R.; Burlina, A.; Bandera, F.; Guazzi, M.; et al. Predictors of clinical evolution in prehypertrophic fabry disease. Circ. Cardiovasc. Imaging 2019, 12, e008424. [Google Scholar] [CrossRef]
- Nordin, S.; Kozor, R.; Medina-Menacho, K.; Abdel-Gadir, A.; Baig, S.; Sado, D.M.; Lobascio, I.; Murphy, E.; Lachmann, R.H.; Mehta, A.; et al. Proposed stages of myocardial phenotype development in fabry disease. JACC: Cardiovasc. Imaging 2019, 12 (8 Pt 2), 1673–1683. [Google Scholar] [CrossRef]
- Figliozzi, S.; Camporeale, A.; Boveri, S.; Pieruzzi, F.; Pieroni, M.; Lusardi, P.; Spada, M.; Mignani, R.; Burlina, A.; Graziani, F.; et al. ECG-based score estimates the probability to detect Fabry Disease cardiac involvement. Int. J. Cardiol. 2021, 339, 110–117. [Google Scholar] [CrossRef]
- Augusto, J.B.; Nordin, S.; Vijapurapu, R.; et al. Myocardial edema, myocyte injury, and disease severity in fabry disease. Circ Cardiovasc Imaging 2020, 13, e00171. [Google Scholar] [CrossRef] [PubMed]
- Orsborne, C.; Bradley, J.; Bonnett, L.J.; Pleva, L.A.; Naish, J.H.; Clark, D.G.; Abidin, N.; Woolfson, P.; Nucifora, G.; Schmitt, M.; et al. Validated model for prediction of adverse cardiac outcome in patients with fabry disease. J. Am. Coll. Cardiol. 2022, 80, 982–994. [Google Scholar] [CrossRef] [PubMed]
- Khanna, S.; Lo, P.; Cho, K.; Subbiah, R. Ventricular arrhythmias in cardiac amyloidosis: A review of current literature. Clin. Med. Insights Cardiol. 2020, 14, 1179546820963055. [Google Scholar] [CrossRef]
- Banypersad, S.M.; Fontana, M.; Maestrini, V.; Sado, D.M.; Captur, G.; Petrie, A.; Piechnik, S.K.; Whelan, C.J.; Herrey, A.S.; Gillmore, J.D.; et al. T1 mapping and survival in systemic light-chain amyloidosis. Eur. Heart J. 2015, 36, 244–251. [Google Scholar] [CrossRef]
- Martinez-Naharro, A.; Kotecha, T.; Norrington, K.; Boldrini, M.; Rezk, T.; Quarta, C.; Treibel, T.A.; Whelan, C.J.; Knight, D.S.; Kellman, P.; et al. Native T1 and Extracellular Volume in Transthyretin Amyloidosis. JACC: Cardiovasc. Imaging 2019, 12, 810–819. [Google Scholar] [CrossRef] [PubMed]
- Nelson, T.; Garg, P.; Clayton, R.H.; Lee, J. The Role of Cardiac MRI in the Management of Ventricular Arrhythmias in Ischaemic and Non-ischaemic Dilated Cardiomyopathy. Arrhythmia Electrophysiol. Rev. 2019, 8, 191–201. [Google Scholar] [CrossRef]
- Porcari, A.; De Luca, A.; Grigoratos, C.; Biondi, F.; Faganello, G.; Vitrella, G.; Nucifora, G.; Aquaro, G.D.; Merlo, M.; Sinagra, G. Arrhythmic risk stratification by cardiac magnetic resonance tissue characterization: disclosing the arrhythmic substrate within the heart muscle. Heart Fail. Rev. 2022, 27, 49–69. [Google Scholar] [CrossRef]
- Barison, A.; Del Torto, A.; Chiappino, S.; Aquaro, G.D.; Todiere, G.; Vergaro, G.; Passino, C.; Lombardi, M.; Emdin, M.; Masci, P.G. Prognostic significance of myocardial extracellular volume fraction in nonischaemic dilated cardiomyopathy. J. Cardiovasc. Med. 2015, 16, 681. [Google Scholar] [CrossRef]
- Nakamori, S.; Bui, A.H.; Jang, J.; El-Rewaidy, H.A.; Kato, S.; Ngo, L.H.; Josephson, M.E.; Manning, W.J.; Nezafat, R. Increased myocardial native T1 relaxation time in patients with nonischemic dilated cardiomyopathy with complex ventricular arrhythmia. J. Magn. Reson. Imaging 2018, 47, 779–786. [Google Scholar] [CrossRef]
- Cadour, F.; Quemeneur, M.; Biere, L.; Donal, E.; Bentatou, Z.; Eicher, J.-C.; Roubille, F.; Lalande, A.; Giorgi, R.; Rapacchi, S.; et al. Prognostic value of cardiovascular magnetic resonance T1 mapping and extracellular volume fraction in nonischemic dilated cardiomyopathy. J. Cardiovasc. Magn. Reson. 2023, 25, 7. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhou, D.; Sirajuddin, A.; et al. T1 mapping and extracellular volume fraction in dilated cardiomyopathy: A prognosis study. JACC Cardiovasc Imaging 2022, 15, 578–590. [Google Scholar] [CrossRef] [PubMed]
- Rubiś, P.P.; Dziewięcka, E.M.; Banyś, P.; Urbańczyk-Zawadzka, M.; Krupiński, M.; Mielnik, M.; Łach, J.; Ząbek, A.; Wiśniowska-Śmiałek, S.; Podolec, P.; et al. Extracellular volume is an independent predictor of arrhythmic burden in dilated cardiomyopathy. Sci. Rep. 2021, 11, 24000. [Google Scholar] [CrossRef] [PubMed]
- McKenna, W.J.; Maron, B.J.; Thiene, G. Classification, epidemiology, and global burden of cardiomyopathies. Circ Res 2017, 22, 722–730, Agbaedeng, T.A.; Roberts, K.A.; Colley, L.; Noubiap, J.J.; Oxborough, D. Incidence and predictors of sudden cardiac death in arrhythmogenic right ventricular cardiomyopathy: a pooled analysis. Europace 2022, 24, 1665–1674.. [Google Scholar]
- Dowd, R.; Dhanjal, T.; Schmucki, M.; Kanagala, P.; Khan, J.N. Unique role of cardiovascular magnetic resonance imaging parametric mapping in the diagnosis of arrhythmogenic left ventricular cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2021, 22, e96. [Google Scholar] [CrossRef] [PubMed]
- Chun, K.-H.; Oh, J.; Hong, Y.J.; Yu, H.T.; Lee, C.J.; Kim, T.; Joung, B.; Pak, H.; Lee, M.; Kim, Y.J.; et al. Prognostic cardiac magnetic resonance markers of left ventricular involvement in arrhythmogenic cardiomyopathy for predicting heart failure outcomes. J. Am. Heart Assoc. 2022, 11, e023167. [Google Scholar] [CrossRef] [PubMed]
- Noseworthy, P.A.; Asirvatham, S.J. The knot that binds mitral valve prolapse and sudden cardiac death. Circulation 2015, 132, 551–552. [Google Scholar] [CrossRef] [PubMed]
- Guglielmo, M.; Fusini, L.; Muscogiuri, G.; Baessato, F.; Loffreno, A.; Cavaliere, A.; Rizzon, G.; Baggiano, A.; Rabbat, M.G.; Muratori, M.; et al. T1 mapping and cardiac magnetic resonance feature tracking in mitral valve prolapse. Eur. Radiol. 2021, 31, 1100–1109. [Google Scholar] [CrossRef] [PubMed]
- Bui, A.H.; Roujol, S.; Foppa, M.; Kissinger, K.V.; Goddu, B.; Hauser, T.H.; Zimetbaum, P.J.; Ngo, L.H.; Manning, W.J.; Nezafat, R.; et al. Diffuse myocardial fibrosis in patients with mitral valve prolapse and ventricular arrhythmia. Heart 2017, 103, 204–209. [Google Scholar] [CrossRef]
- Pavon, A.G.; Arangalage, D.; Pascale, P.; Hugelshofer, S.; Rutz, T.; Porretta, A.P.; Le Bloa, M.; Muller, O.; Pruvot, E.; Schwitter, J.; et al. Myocardial extracellular volume by T1 mapping: a new marker of arrhythmia in mitral valve prolapse. J. Cardiovasc. Magn. Reson. 2021, 23, 102. [Google Scholar] [CrossRef]
- Guglielmo, M.; Arangalage, D.; Bonino, M.A.; Angelini, G.; Bonanni, M.; Pontone, G.; Pascale, P.; Leo, L.A.; Faletra, F.; Schwitter, J.; et al. Additional value of cardiac magnetic resonance feature tracking parameters for the evaluation of the arrhythmic risk in patients with mitral valve prolapse. J. Cardiovasc. Magn. Reson. 2023, 25, 32. [Google Scholar] [CrossRef]
- Pradella, S.; Grazzini, G.; Brandani, M.; Calistri, L.; Nardi, C.; Mori, F.; Miele, V.; Colagrande, S. Cardiac magnetic resonance in patients with mitral valve prolapse: Focus on late gadolinium enhancement and T1 mapping. Eur. Radiol. 2019, 29, 1546–1554. [Google Scholar] [CrossRef] [PubMed]
- Argentiero, A.; Carella, M.C.; Mandunzio, D.; Greco, G.; Mushtaq, S.; Baggiano, A.; Fazzari, F.; Fusini, L.; Muscogiuri, G.; Basile, P.; et al. Cardiac Magnetic Resonance as Risk Stratification Tool in Non-Ischemic Dilated Cardiomyopathy Referred for Implantable Cardioverter Defibrillator Therapy—State of Art and Perspectives. J.Clin.Med. 2023, 12, 7752. [Google Scholar] [CrossRef] [PubMed]
- Køber, L.; Thune, J.J.; Nielsen, J.C.; Haarbo, J.; Videbæk, L.; Korup, E.; Jensen, G.; Hildebrandt, P.; Steffensen, F.H.; Bruun, N.E.; et al. Defibrillator Implantation in Patients with Nonischemic Systolic Heart Failure. N. Engl. J. Med. 2016, 375, 1221–1230. [Google Scholar] [CrossRef]
- Rabbat, M.G.; Kwong, R.Y.; Heitner, J.F.; Young, A.A.; Shanbhag, S.M.; Petersen, S.E.; Selvanayagam, J.B.; Berry, C.; Nagel, E.; Heydari, B.; et al. The Future of Cardiac Magnetic Resonance Clinical Trials. JACC: Cardiovasc. Imaging 2022, 15, 2127–2138. [Google Scholar] [CrossRef] [PubMed]
- Tampakis, K.; Pastromas, S.; Sykiotis, A.; Kampanarou, S.; Kourgiannidis, G.; Pyrpiri, C.; Bousoula, M.; Rozakis, D.; Andrikopoulos, G. Real-time cardiovascular magnetic resonance-guided radiofrequency ablation: A comprehensive review. World J. Cardiol. 2023, 15, 415–426. [Google Scholar] [CrossRef] [PubMed]
- De Zan, G.; Calò, L.; Borrelli, A.; Guglielmo, M.; De Ruvo, E.; Rier, S.; van Driel, V.; Ramanna, H.; Patti, G.; Rebecchi, M.; et al. Cardiac magnetic resonance-guided cardiac ablation: a case series of an early experience. Eur. Heart J. Suppl. 2023, 25 (Suppl. C), C265–C270. [Google Scholar] [CrossRef]
- Guglielmo, M.; Rier, S.; Zan, G.; Krafft, A.J.; Schmidt, M.; Kunze, K.P.; Botnar, R.M.; Prieto, C.; van der Heijden, J.; Van Driel, V.; et al. Cardiac magnetic resonance for early atrial lesion visualization post atrial fibrillation radiofrequency catheter ablation. J. Cardiovasc. Electrophysiol. 2024, 35, 258–266. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



