
Submitted:
27 March 2024
Posted:
28 March 2024
You are already at the latest version
Abstract
The prevalence of Noncommunicable Diseases (NCDs) in South Africa is increasing annually, with the burden projected to escalate by 2030. Devastatingly, factors such as lifestyle changes, urbani- sation, and an aging population significantly contribute to a rising burden of Cardiovascular disease (CVDs), diabetes, and cancer which directly impact the mortality and morbidity rates seen in South Africa. Recognising this, the South African government has seen the need for emphasis on developing policies and interventions tar- geting physical inactivity to prevent and manage NCD, particularly cost-free and easy to administer training protocols. However, phys- ical inactivity remains a significant issue, leading to various health concerns in rural communities, including injuries and Fetal Alcohol Spectrum Disorders (FASD). Despite effort to promote physical ac- tivity, the prevalence of NCDs continues to rise, necessitating target- ed interventions to ensure equitable healthcare among South African citizens. On the Contrast, preservation and promotion of traditional games is vital as they offer indigenous populations accessible and culturally relevant means to maintain health and wellness. In this regard, it is important to recognize the importance of preserving and promoting traditional games as they potentially serve as a method for indigenous people to maintain their health and wellness in a way that is accessible and culturally relevant to them. These games have gained popularity in South Africa, with initiatives underway to show- case them globally fostering cultural exchange. Further, revitalizing and conserving these games can cultivate a culture of health and wellbeing in South Africa.
Keywords:
Rural settings
; Non-communicable diseases
; Exercise intervention
; Cardiovascular conditions
; Physical health and wellbeing
Background
NCDs are commonly grouped into nonmodifiable and modifiable risk factors [1]. Nonmodifiable risk factors include exposure to environmental stressors such as pollutants, noise, artificial light, and climate change [1]. Additionally, social determinants of health, genetics, stress, sleep, substance use, malnutrition, and demographics contribute to these risk factors [1]. Modifiable behavioral risk factors for NCDs include unhealthy habits such as tobacco use, unhealthy diet, physical inactivity, and excessive alcohol [2]. Effective self-management, lifestyle modification awareness campaigns, health policy decisions, and global health strategies are important in preventing NCDs pandemics [1].
On that note, such risk factors and prevention strategies need to be addressed through multi sectoral partnerships, knowledge management, and innovative approaches [1,2]. Statistics reveal that approximately 30% of the population in South African rural communities is affected by NCDs, such as CVD, diabetes and cancer [3]. These diseases have as a significant health threat in South Africa, driven by lifestyle changes, urbanisation, and an aging demographic [4]. The high prevalence of NCDs in rural communities is concerning, as these areas often lack access to quality healthcare and resources for prevention and management [5]. Furthermore, the impact of NCDs in rural communities is exacerbated by factors such as poverty, limited education, and lack of awareness about healthy lifestyles [3]. Many individuals in these communities do not have the means to afford proper healthcare or access to nutritious food, leading to a higher risk of developing these diseases [3,4]. Additionally, the lack of healthcare facilities and professionals in rural areas makes it difficult for individuals to receive timely diagnosis and treatment, further worsening the situation [5].
Immediate interventions are needed to address the growing burden of NCDs in South African rural communities and ensure equitable healthcare for all [6]. For example, in a rural community in South Africa, many individuals are unable to afford regular check-ups or screenings for conditions such as diabetes or heart disease [7]. Without early detection and intervention, these diseases can progress and lead to serious complications [7]. Moreover, the limited number of healthcare professionals in the area means that individuals may have to travel long distances to receive necessary medical care, causing delays in diagnosis and treatment [8]. This lack of access exacerbates the health disparities faced by rural communities [9] and underscores the urgency for targeted interventions that aim to improve healthcare access and outcomes in these areas [10].
In this regard, efforts should be made to increase the number of healthcare professionals, such as biokineticists, with their expertise so they may serve rural communities, as well as implement telemedicine initiatives that can provide remote medical consultations and monitoring [11]. Additionally, community health education programs can play a crucial role in raising awareness about preventive measures and early warning signs of chronic diseases, empowering individuals to take control of their own health [12]. By addressing these challenges head-on, we can work towards bridging the healthcare gap between rural and urban areas, limiting further increases of NCD-related fatalities and ensuring that all individuals have equal opportunities for a healthy and fulfilling life [13].
Noncommunicable Disease (NCD) Risk Factors
The methods of research for the etiology(s), prevention and treatment strategies of NCDs has been thoroughly developed from various descriptive epidemiological studies to forthcoming cohort studies [14,15,16]. This prospective number of studies include identifying the population sample, clinically assessing the sample and monitoring the sample for several years for any signs of non-communicable disease [16]. Interestingly, as part of NCDs, a Framingham study conducted in the United States of America (USA) is currently one of the most referenced studies since it has generated information that now presently assist in the early detection and prevention of coronary artery disease (CAD) and commonly referred as “risk factor hypothesis study” [17].
As part of the risk factors, tobacco use and in particular, cigarette smoking is the single most preventable cause of morbidity and mortality worldwide [9,18,19,20]. Studies have reported that in 2030, smoking rate will approximately increase by 80% of the current total population of smokers with significant contribution predominantly by college-aged smokers in rural areas [9,19,20]. Smoking results in multiple alterations on the performance of the cardiovascular system [9]. For instance, a toxic chemical released during cigarette smoking called nicotine causes catecholamine release which triggers an increase in the heart rate, Blood Pressure (BP) and cardiac output (Q) [9,19,20,21]. Moreover, various studies using smokers has indicated negative changes in Stroke Volume (SV), myocardial contraction force, myocardial oxygen consumption, myocardial velocity of contraction and further plays a significant role in the development of arrhythmia and changes of ballistocardiographic and Electrocardiographic (ECG) patterns [4,22,23]. In this regard, studies have shown that smokers are more likely to possess reduced chronotropic incompetence index levels than non-smokers (26% versus 16%) and are more prone to failure in achieving an age-predicted maximum heart rate during exercise than non-smokers (32% versus 22%) [21].
Nonetheless, apart from smoking, alcohol consumption is another serious public health concern globally, and particularly among the youth population especially in universities in South Africa with significant contribution by those in rural areas [24,25]. Nevertheless, alcohol consumption does not appear to have a causal relationship with smoking behaviour in young adults [26,27]. Moderate and heavy drinking have been found to impact smoking cessation efforts, with recent moderate drinking associated with short-term continued smoking and heavy drinking associated with relapse in the short and long term [14,26]. Studies have revealed that there are several factors that contribute to alcohol use among different race, sex, culture and ethnicity. On that note, a study conducted in rural areas of Limpopo province using high school learners indicated that having parents and friends who consume alcohol were among the highest ranked [28].
Furthermore, in rural northeast South Africa, reports have shown that the community collective efficacy and alcohol outlet density are associated with young men’s drinking, with informal social control and cohesion showing protective associations and alcohol outlet density being associated with potential problem drinking [29]. There is evidence showing a cardioprotective effect of light to moderate alcohol consumption in many populations, but whether alcohol consumption reduces CVD risk in an African population remains unclear [14]. Among a community sample of rural South Africans, a significant proportion of men were classified as high-risk drinkers and with probable alcohol dependence [30]. In this vein, alcohol contributes to the global burden of disease, including NCDs, and is associated with various health issues in South Africa, including injuries and Fetal Alcohol Spectrum Disorders (FASD) [31,32]. FASD encompass a spectrum of disorders that arise as a result of maternal alcohol consumption during pregnancy, and these disorders have profound and enduring consequences on the individual who is affected [32,33]. Within certain high-risk communities, South Africa exhibits the highest documented prevalence rate of FASD worldwide [31,32]. Nonetheless, the country presently lacks a comprehensive national strategy or policy that is harmoniously designed to tackle this pressing concern [34].
It worth to note that literature indicates that youth living in rural and remote areas are more likely to drink alcohol and experience alcohol-related harm compared to those in urban locations [34,35]. Strategies to reduce risky alcohol consumption among youth in rural areas have been evaluated, but no interventions can be broadly recommended at this time [28,34]. Additionally, the expectations towards alcohol consumption have been found to be related to alcohol consumption among young people in both rural and urban areas [28]. In terms of CVD, heavy drinking has been identified as a risk factor for coronary heart disease and hypertension in rural populations, particularly among men [34]. Therefore, alcohol consumption in rural areas, especially among youth, is contributing to negative health outcomes and further research is needed to develop effective strategies to address this issue [36].
Although a sedentary lifestyle places an individual at greater risk for development of various disorders and diseases, regular exercise is often associated with a wider variety of psychological and physical health benefits [9,19,20]. According to the American Association of cardiovascular and pulmonary rehabilitation (AACVPR) in 1999, physical inactivity has been declared the most prevalent NCD risk factor [37].
Physical inactivity is a noteworthy concern in South Africa, particularly among the adult population [38]. Research findings have demonstrated that the prevalence of physical inactivity has remained considerably high over the course of time, with a reduction of merely 16% and 8% between the years 2012 and 2020 for females and males, respectively [39]. This elevated occurrence of physical inactivity has been associated with various NCDs. In actuality, physical inactivity accounts for a substantial portion of the disease burden in South Africa, with 30% of ischaemic heart disease, 27% of colon cancer, 22% of ischaemic stroke, 20% of type 2 diabetes, and 17% of breast cancer being attributable to physical inactivity [40,41]. The burden of disease resulting from physical inactivity is noteworthy, contributing to 3.3% of all deaths and 1.1% of all disability-adjusted life years (DALYs) in the year 2000 [42]. These statistics underscore the pressing necessity for policies and interventions aimed at promoting physical activity and mitigating physical inactivity in South Africa as a means to prevent and manage NCDs [38].
Numerous studies have shown that physical activity levels are lower in rural areas compared to urban areas [43,44,45]. Factors such as older age, being female, living in informal settlements, and having poorer self-rated health are associated with decreased likelihood of engaging in vigorous physical activity in rural communities [44]. Additionally, lower educational attainment and engagement in physical exercise are associated with increased odds of NCDs in both rural and urban areas [43]. These findings highlight the need for targeted interventions to promote physical activity in rural communities, particularly among disadvantaged individuals and those with unhealthy lifestyles. Creating safe walking/riding trails and introducing physical education lessons in public schools are recommended strategies to combat physical inactivity and reduce the burden of NCDs in South Africa.
Correspondingly, unhealthy eating contributes to the burden of NCDs in South Africa. The shift from traditional diets to a western diet high in sugar and processed foods, coupled with income and wealth inequalities, has led to an increased prevalence of NCDs in the country [45]. The rise in NCDs has been attributed to factors such as economic growth, shifts in societal norms, and unhealthy dietary habits [46]. The South African government has recognized the need to prove prevention and management of NCDs, particularly CVD, through interventions that address risk factors like unhealthy diets [47]. The concentration of real food expenditure among the rich and the increased burden of diet-related NCDs among lower socioeconomic groups further highlight the impact of unhealthy eating on health inequality [48]. To combat this trend, there is a need for more stringent measures to address common risk factors and invest in NCD prevention and control as part of sustainable socioeconomic development [47].
In the context of CVDs, obesity indicators such as waist circumference have a positive relationship with the environment domain of QOL [9]. Hypertension and sedentary lifestyle are prevalent risk factors for CVD in women during the climacteric period, leading to a significant impact on QOL, particularly in social, emotional, and mental health domains [49]. Social factors play a crucial role in the course and consequences of NCDs, affecting the QOL of individuals. Factors such as access to medicines, finances, and sociostructural resources influence the work lives and overall outcomes of individuals with NCDs [9]. Age-related macular degeneration (AMD) also affects QOL, with lower scores in visionand health-related domains [50]. In this vein, overall understanding and addressing of the risk factors associated with NCDs is essential for improving the QOL of affected individuals [49].
Concurrently, the challenges presented by NCDs in South Africa may undermine the development of effective and sustainable primary and secondary interventions [51]. Disappointingly, studies indicate that implementing such nonpharmacological interventions (exercises to increase physical activity) may be difficult in South Africa [52,53,54] due to the predominant biomedical model practice within an acute ineffective and segregated healthcare model [53]. The findings of a qualitative study further shows that treatment adherence among patients with diabetes, hypertension or both, in a South African community, suggest that factors that may influence adherence to exercise interventions may be multifactorial, including the attribution of the origin of the illness, previous experiences with the public healthcare system, concerns about the consequences of poor adherence, financial problems, transport problems and social support [52]. It worth to note that, the intervention utilised in the study was, however, predominantly pharmacological. Moreover, a recent in-depth qualitative-exploration study on nonspecific chronic low back pain in rural Nigeria report that patients may view non-pharmacological intervention as illegitimate treatment possibly influenced by the predominant acute infective model of healthcare [55]. This suggests that poor treatment adherence may be more pronounced, with interventions having little or no pharmacological component [55].
Incidence and Cost of Noncommunicable Diseases (NCDs)
Globally, NCDs have been reported to have a significant incidence and cost [56]. The economic ramifications of NCDs encompass direct expenses, such as medical care, and nonmedical costs, such as transportation and lost income [57]. These costs are considerable, with estimates projecting that they will surpass US$30 trillion in the next two decades, which equates to approximately 48% of global GDP in 2010 [57,58]. The financial burden of NCDs on patients and households residing in LMICs is substantial, with the average total costs per year ranging from R1017.05 to R7386.71 [59].
Furthermore, NCDs not only impose an economic burden but also significantly impact industry competitiveness and can render millions of individuals below the poverty line [56,59]. Cost-effective strategies for NCD prevention and control have been identified, including tobacco and alcohol control policies, mass media campaigns, and treatment options for CVD and cancer [60]. Nonetheless, the quadruple burden of HIV/AIDS, TB, high maternal and child mortality, high levels of violence and injuries, and a growing burden of NCDs have already crippled the South African public health care system, making it necessary to lower the cost of public health interventions [61,62,63].
Regarding this, the South African Department of Health has stated that the cost of using doctors to address physical inactivity has been estimated to be R11.80 (roughly £0.58) per head compared to R4.50 (roughly £0.22) per head for worksite interventions, effectively demonstrating the costeffectiveness and necessity of biokineticists in such PA interventions [64].
Indigenous Knowledge and Practices: Taxonomy of Indigenous Games
Indigenous knowledge refers to the unique knowledge, practices, and beliefs developed by indigenous communities over generations [65]. This knowledge encompasses traditional healing methods, herbal remedies, and holistic approaches to health and well-being [66]. Indigenous games are traditional sports and activities that have been passed down through generations within indigenous communities [65]. These games hold cultural significance and are deeply rooted in the history and identity of the indigenous people. They often involve physical strength, agility, and teamwork, and are played for various purposes such as building community bonds, honouring ancestors, and promoting physical and mental well-being [67]. Moreover, indigenous games serve as a means of preserving and transmitting cultural knowledge and traditions from one generation to another [66].
Interestingly, these games are not only a form of entertainment but also a way to connect with the natural world and maintain a harmonious relationship with the environment [65]. Studies indicate that through participating in these games, indigenous communities can reinforce their cultural identity and strengthen their sense of belonging [66]. Furthermore, these games provide an opportunity for intergenerational interaction, fostering a sense of unity and solidarity among community members [67]. Remarkably, the elders pass down their knowledge and skills to the younger generation, ensuring the preservation of their heritage [67]. Further, by engaging in these traditional games, the community members not only learn from each other but also create bonds that transcend age and bring everyone together [65]. It is through these interactions that the values and wisdom of their ancestors are imparted, instilling a deep sense of pride and responsibility within the community to carry forward their customs and traditions for future generations [68]. Ultimately, these games serve as a powerful tool for cultural resilience and the continuity of indigenous way of life.
Interestingly, a previous South African Indigenous Games project conducted in 2004 on children successfully identified a total of 536 indigenous games in all racial populations combined [69]. However, some of the games are variations of one another, as such, they found about 37 variations of rope jumping, 18 variations of hide-and-seek and 13 hop scotch [69]. Moreover, these games have further been classified using different frameworks, although the differences mainly existed along the lines of age, rather than any other denominator [66]. Senior citizens mainly reference a ‘place’ (indoors versus outdoors), ‘context’ (hunting or different social gatherings), ‘intension’ (lover’s games) or ‘apparatus’ (ball games) as category indicators [69]. Contradictory to Cheska’s classification of games, and three others who did not follow the same procedures for an ‘emic’ classification, the South African Indigenous Games project attempted to construct a representative taxonomy (Figure 1).
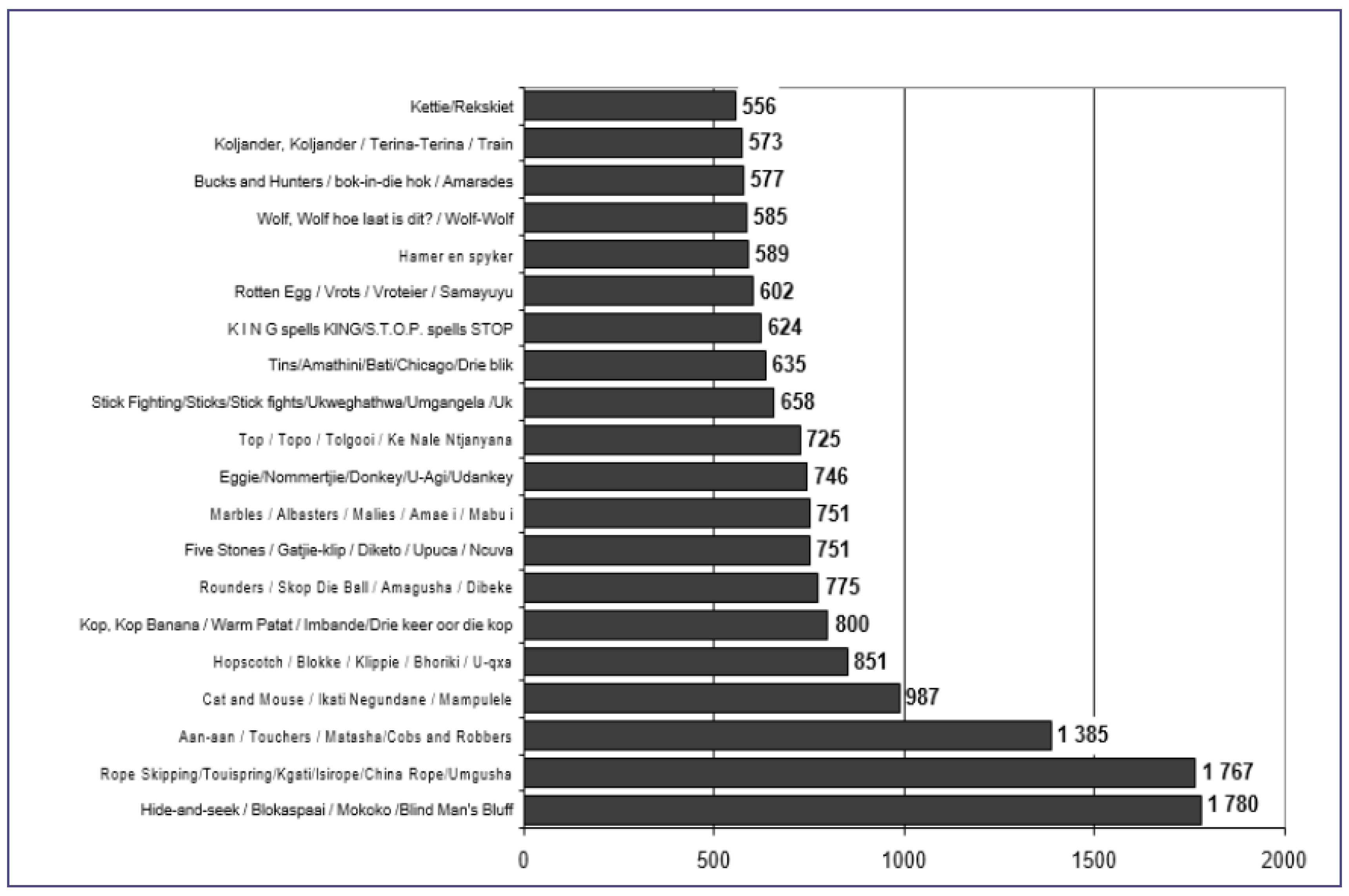
Studies have noted that by organizing the games based on the proportion of children who are familiar with or have played them, an overview is provided regarding the level of popularity of these games [67]. It is important to acknowledge that these games may be known by various names, and even if a game is recognized by a specific name within a particular language group of children, alternative names are included to signify the relevant group of games [69]. The graph (Figure 2) visually displays the ranking of the top 20 games that have been identified as the most popular by all participants from different population segments, mainly children [69].
Indigenous Games and Non-Communicable Diseases
In recent years, there has been growing recognition of the potential of indigenous knowledge in addressing the burden of NCDs [70]. Indigenous communities have often developed effective strategies for preventing and managing these diseases, based on their deep understanding of the interconnectedness between individuals, communities, and the environment [69]. By incorporating indigenous knowledge into mainstream healthcare systems, there is an opportunity to enhance the effectiveness and cultural appropriateness of interventions for NCDs [71]. This can be achieved through collaborative partnerships with indigenous communities, where their traditional healing practices and knowledge are valued and integrated into healthcare delivery [69]. By recognizing and incorporating indigenous knowledge, healthcare systems can promote holistic approaches to health and well-being, which may lead to improved outcomes and reduced health disparities for indigenous populations mainly in rural-based communities [72]. Moreover, this integration can also contribute to preserving and revitalizing indigenous cultures and traditions, fostering a sense of pride and identity within these communities [71]. Nonetheless, the integration of indigenous knowledge into healthcare systems is that it may lead to the promotion of unproven or pseudoscientific practices, potentially compromising patient safety and outcomes [71]. In this regard, prioritizing indigenous knowledge over evidence-based medicine could undermine the principles of standardization and consistency in healthcare delivery [71]. However, studies argue that proponents of integrating indigenous knowledge can complement evidence-based medicine, providing a more holistic approach to healthcare that considers cultural beliefs and practices [71]. By incorporating indigenous knowledge, healthcare systems can better understand and address the unique healthcare needs of indigenous communities, ultimately improving patient outcomes [69]. As such, striking a balance between evidence-based medicine and indigenous knowledge is crucial in achieving culturally competent healthcare that respects and values diverse perspectives.
It worth to note that, cultural practices and lifestyle factors that contribute to reduced NCD rates in indigenous communities include a diet rich in traditional foods, regular physical activity through activities like indigenous games, hunting and gathering, as well as a strong sense of community support and belonging [69]. Previous studies have indicated that these practices promote overall wellness and help prevent the development of NCDs such as heart disease, diabetes, and obesity [69,73]. Additionally, the deep connection to nature and the environment encourages a holistic approach to health, fostering a sense of harmony and balance within individuals and their communities [74]. In this regard, the reliance on traditional foods ensures that community members have access to nutrientdense and minimally processed options, which contribute to better overall health [69].
Regular physical activity not only helps maintain a healthy weight but also improves cardiovascular health and indirectly improves mental well-being [9]. Lastly, the strong sense of community support and belonging provides a safety net for individuals, fostering emotional well-being and reducing stress levels which result in an overall improvement of QOL [20]. Together, these factors create a foundation for optimal health and well-being within Indigenous communities. For example, in indigenous communities, there may be initiatives that promote traditional farming practices and educate community members on the importance of consuming fresh fruits and vegetables. This not only increases access to nutrientdense foods but also helps preserve cultural traditions and knowledge [74]. Additionally, community-led physical activity programs such as group hikes or traditional dance classes can bring people together, promoting social connections while improving physical fitness [17]. These initiatives can have a significant impact on the overall health and wellbeing of indigenous communities. Moreover, physical activity programs not only improve physical fitness but also contribute to mental and emotional well-being by reducing stress and promoting positive social interactions as well as reducing the risk of chronic diseases such as diabetes and obesity that are prevalent in many Indigenous communities [74]. These activities create opportunities for individuals to connect with others who share similar interests and goals, which creates a supportive and inclusive community environment [70]. Moreover, participating in physical activities together encourages individuals to stay motivated and accountable, leading to long-term lifestyle changes and improved overall health outcomes which has a potential to decrease high rates of premature mortality and morbidity seen in rural-based communities [17]. Ultimately, the combination of indigenous knowledge and practice systems such as promoting physical activity through games can significantly enhance the QOL in Indigenous communities, reduce NCDs and promote a holistic well-being for all individuals in rural communities [70].
Importance of Indigenous Games as an Exercise Intervention for Non-Communicable Diseases (NCDs)
Previous studies have noted that the importance of exercise interventions for NCDs cannot be overstated [70]. In indigenous communities, where traditional games play a significant role, exercise becomes a fundamental component of their daily lives [75]. These physical activities not only promote physical well-being but also serve as preventive measures against NCDs such as diabetes and CVD [75]. By engaging in these games, indigenous people can improve their overall health and reduce the risk of developing these chronic conditions, ensuring a healthier and more vibrant community for generations to come [74]. Further, the traditional games passed down through generations also help to strengthen the social bonds within the indigenous community [76]. Through these activities, they not only engage in friendly competition but also cultivate a sense of togetherness and unity [75]. The shared experiences and camaraderie fostered during these games contribute to a close-knit community that supports one another’s well-being both physically and emotionally [76].
Overall, traditional games not only play a vital role in promoting physical health but also contribute to the holistic wellness of indigenous people [77]. While traditional games may indeed foster social bonds and unity within the indigenous community, it is important to consider that physical health and holistic wellness can also be achieved through a variety of other activities and practices [78]. However, such practices have been deemed to be from a western hemogenic and are not easily accessible by every South African individual mostly from rural areas such as proper gyms, or sport facilities [79]. These individuals often rely on traditional games and activities that have been passed down through generations for their physical fitness and overall well-being [74]. Therefore, it is crucial to acknowledge the importance of preserving and promoting traditional games as they provide a means for indigenous people to maintain their health and wellness in a way that is accessible and culturally relevant to them. By supporting and encouraging the continuation of these activities, we can ensure that indigenous communities have the resources and opportunities to lead healthy and fulfilling lives.
Interestingly, studies are still warranted that indicate that indigenous games can serve as effective exercise interventions for preventing and managing NCDs [75,80,81]. These traditional games often involve physical activity and require participants to use their bodies in ways that promote strength, agility, and endurance [77]. In this vein, through engaging in these activities regularly, indigenous people can improve their cardiovascular health, strengthen their muscles, and maintain a healthy weight, all of which contribute to the prevention and management of NCDs (Natalucci et al., 2023) [81]. Therefore, by recognizing the value of indigenous games as exercise interventions, we can empower indigenous communities to take control of their health and reduce the burden of NCDs [77].
In rural-based communities in South Africa, preserving and promoting traditional games is crucial for the health and wellness of indigenous people [82,83]. Furthermore, indigenous games can also play a crucial role in preserving the rich cultural heritage of indigenous communities [83]. For example, in the Maori culture of New Zealand, a traditional game called ki-o-rahi is played. This game involves teams competing to score points by carrying a ball and touching it on designated markers. Ki-o-rahi not only provides physical exercise but also promotes teamwork, strategy, and cultural pride among Maori youth [84]. Through incorporating this traditional game into school curriculums and community events, the Maori people can pass down their cultural heritage while simultaneously promoting health and well-being [85]. In this regard, the inclusion of ki-o-rahi in school curriculums allows non-Maori students to gain a deeper understanding and appreciation of Maori culture which nurtures cultural diversity and inclusivity, promoting a sense of unity among all students [86]. Additionally, the popularity of ki-o-rahi has grown beyond New Zealand, with international tournaments being held, further spreading awareness and recognition of Maori traditions on a global scale [84].
Concurrently, in South Africa, indigenous games like murabaraba and diketo play a significant role in preserving and promoting the country’s diverse cultural heritage [87]. Murabaraba, a traditional board game, and diketo, a stone throwing game, have been integral to indigenous South African communities for centuries [69,88]. These games not only provide entertainment but also serve to pass down ancestral knowledge and values to younger generations [88]. The popularity of these indigenous games has grown within South Africa, and efforts are being made to showcase them internationally, promoting cultural exchange and understanding [88]. Moreover, games such as tag or donkey are also popular among South African children [69]. These games, although not necessarily indigenous, still play a significant role in fostering social interaction, physical activity, and problem-solving skills [89]. As South Africa continues to embrace its diverse cultural heritage, the revival and preservation of these traditional and modern games contribute to a sense of national pride and unity among its people [88]. This game has an overall potential to reduce NCDs by one third as they encourage regular physical activity and help combat sedentary lifestyles [69], however their effects on different age groups or populations is still limited [69,88,90]. Furthermore, these games provide an opportunity for children and adults to bond and interact, fostering social connections and a sense of community that is essential for overall well-being. Through the revival and preservation of these games, South Africa can create a culture of health and wellness, reducing the burden of NCDs and promoting a vibrant and united nation.
Author Contributions
Conceptualization, methodology, software, and validation were completed by N.M.S., M.L.M., B.S.S., and I.S., including data curation, visualization, and project administration. Formal analysis was completed by N.M.S., M.L.M., B.S.S., and I.S., and N.M.S. wrote the original draft. Review and editing were completed by N.M.S., M.L.M., B.S.S., and I.S. All authors have read and agreed to the published version of the manuscript. Funding: This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of University of Zululand Research Ethics Committee and approved by the Institutional Review Board at the University of Zululand Research Ethics Committee (IRB approval UZREC 171110-030) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the participants to publish this paper.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Budreviciute A, Damiati S, Sabir DK, Onder K, Schuller-Goetzburg P, et al. (2020) Management and Prevention Strategies for Non-communicable Diseases (NCDs) and Their Risk Factors 8. [CrossRef]
- Bolarinwa O, Olagunju OS, Budu E, Seidu AA, Odetokun IA, et al. (2020) Prevalence of Non-Communicable Diseases and Associated Factors in South Africa: Evidence from National Income Dynamics Survey, 20082017. Research Square.
- Wong EB, Olivier S, Gunda R, Koole O, SurujdeenA, et al. (2021) Convergence of Infectious and NonCommunicable Disease Epidemics in Rural South Africa: A Cross-sectional, Population-based Multimorbidity Study. The Lancet Global Health 9: 967-976.
- Godward S (2023) Adult Public Health and Non-Communicable Diseases. Essential Public Health: Theory and Practice 231.
- Hunter DJ, Reddy KS (2013) Noncommunicable Diseases. New England Journal of Medicine 369: 1336-1343.
- Countdown NCD (2022) NCD Countdown 2030: Efficient Pathways and Strategic Investments to Accelerate Progress towards the Sustainable Development Goal Target 3.4 in Low-Income and Middle-Income Countries. Lancet (London, England) 399: 1266.
- Gumede M (2022) Development of a Policy Framework for the Establishment of Physical Exercise Programmes in Reducing Non-Communicable Diseases in the Province of KwazuluNatal, South Africa (Doctoral Dissertation).
- Famogun BU (2023) Lived Experiences of African American Men with Type 2 Diabetes Living in Rural Areas (Doctoral dissertation, Walden University).
- Shandu NM, Mathunjwa ML, Shaw BS (2023) Effects of High-Intensity Interval Training and Continuous Aerobic Training on Health-Fitness, Health Related Quality of Life, and Psychological Measures in College-Aged Smokers. International Journal of Environmental Research and Public Health 20: 653.
- O’Brien N, Li E, Chaibva CN, Gomez Bravo R, Kovacevic L, et al. (2023) Strengths, Weaknesses, Opportunities, and Threats Analysis of the Use of Digital Health Technologies in Primary Health Care in the Sub-Saharan African Region: Qualitative Study. J of Med Int Res 25: 45224. [CrossRef]
- Rakers MM, van Os HJ, Recourt K, Mosis G, Chavannes NH, et al. (2023) Perceived Barriers and Facilitators of Structural Reimbursement for Remote Patient Monitoring, A Exploratory Qualitative Study. Health Policy and Technology 12: 100718.
- Diab P, Flack P (2013) Benefits of Community-Based Education to the Community in South African Health Science Facilities. The African Journal of Primary Health Care & Family Medicine 5: 474.
- Rocha RO, Takahashi ARW, Segatto AP (2023) How does Social Innovation Generate Social Impact?: Contributions from a Meta-synthesis. Revista de Empreendedorismo e Gestão de Pequenas Empresas 12: 3.
- Aparicio-Rodríguez YD, Alonso-Morillejo E, García-Torrecillas JM (2023) Epidemiological Situation of High-Prevalence Non-Communicable Diseases in Spain: A Systematic Review. Journal of Clinical Medicine 12: 7109.
- Reynales-Shigematsu LM, Barnoya J, Cavalcante T, Aburto TC, Romieu I, et al. (2023) Latin America and the Caribbean Code Against Cancer 1st edition: Tobacco and Nicotine-related Products, Second-hand Smoke, and Alcohol and Cancer. Cancer Epidemiology 86: 102413.
- Saina S, Senthil P, Prakash O (2023) Burden of Illness, Risk Factor and Physical Activity in Cardiovascular Disease-A Review. Biomedicine 43: 1080-1093.
- Shaw I, Shaw BS, Krasilshchikov O (2009) Comparison of Aerobic and Combined Aerobic and Resistance Training on Low-density Lipoprotein Cholesterol Concentrations in Men: Cardiovascular Topic. Cardiovascular Journal of Africa 20: 290-295.
- Peto R, Lopez AD (2004) The Future Worldwide Health Effects of Current Smoking Patterns. Tobacco and Public Health: Science and Policy 281-286.
- Shandu NM, Mathunjwa ML, Shaw BS, Shaw I. (2023) Effects of High-Intensity Interval Training on Health-Fitness, Health Related Quality of Life, and Psychological Measures in College-aged Smokers. Journal of. Physical. Education and Sport 23: 200-209.
- Shandu NM, Mathunjwa ML, Shaw I (2023) Exercise Effects on Health-Related Quality of Life (HRQOL), Muscular Function, Cardiorespiratory Function, and Body Composition in Smokers: A Narrative Review. International Journal of Environmental Research and Public Health 20: 6813.
- Kolci KÜBRA, Garipkuş SN, Rengin REİS (2023) Thirdhand Smoke Exposure and its Toxicological Impacts: A Review on Target Organ-based Studies. Fabad Journal of Pharmaceutical Sciences 48: 303-318.
- Hendriks T, van Dijk R, Alsabaan NA, Harst PV (2020) Active Tobacco Smoking Impairs Cardiac Systolic Function. Scientific Reports 10: 6608.
- Qian Y, Ye D, Wu DJ, Feng C, Zeng Z, et al. (2019) Role of Cigarette Smoking in the Development of Ischemic Stroke and its Subtypes: A Mendelian Randomization Study. Clinical Epidemiology 11: 725-731. [CrossRef]
- Choudhary S, Gupta A, Kumari S (1995) Impact of Smoking and Alcohol Consumption on Blood Pressure and Anthropometric Parameters. Hip 7.
- Kugbey N (2023) Prevalence and Correlates of Substance Use Among School-Going Adolescents (11-18years) in Eight Sub-Saharan Africa Countries. Substance abuse treatment, prevention, and policy 18: 44.
- Britton M, Derrick JL, Shepherd JM, Haddad S, Garey L, et al. (2021). Associations Between Alcohol Consumption and Smoking Variables among Latinx Daily Smokers. Addictive behaviours 113: 106672. [CrossRef]
- Jee Y, Park S, Yuk E, Cho SI (2021) Alcohol Consumption and Cigarette Smoking among Young Adults: An Instrumental Variable Analysis Using Alcohol Flushing. Int J of Environ Res Pub Health 18: 11392.
- Maserumule OM, Skaal L, Sithole SL (2019) Alcohol Use Among High School Learners in Rural Areas of Limpopo Province. S Afr J Psychiatr 25: 1183.
- Leslie HH, Ahern J, Pettifor AE, Twine R, Kahn K, et al. (2015) Collective Efficacy, Alcohol Outlet Density, and Young Men’s Alcohol Use in Rural South Africa. Health Place 34: 190-198.
- Peltzer K (2006) Prevalence of alcohol use by rural primary care outpatients in South Africa. Psychological Reports 99: 176-178.
- Boua PR, Soo CC, Debpuur C, Maposa I, Nkoana S, et al. (2021) Prevalence and Socio-Demographic Correlates of Tobacco and Alcohol Use in Four Sub-Saharan African Countries: A Cross-Sectional Study of Middle-Aged Adults. BMC Public Health 21: 1126. [CrossRef]
- Popova S, Charness ME, Burd L, Crawford A, Hoyme HE, et al. (2023) Fetal Alcohol Spectrum Disorders. Nature Reviews Disease Primers 9: 11.
- Pisa PT, Vorster HH, Kruger A, Margetts B, Loots du T (2015) Association of Alcohol Consumption with Specific Biomarkers: A Cross-Sectional Study in South Africa. Journal of Health, Population and Nutrition 33: 146-156.
- Yun M, Kim E (2022) Gender Difference in the Association Between Alcohol Consumption and Depressive Symptoms among the Elderly in Rural Areas. Journal of Ethnicity in Substance Abuse 21: 36-54.
- Cibich M, Hines S, Carey TA (2023) Effectiveness of Strategies to Reduce Risky Alcohol Consumption among Youth Living in Rural or Remote Areas: A Systematic Review. JBI evidence synthesis 10: 11124.
- Ebling SBD, Silva MRSD (2020) Alcohol Consumption among Women Living in Rural Contexts. Revista Brasileira de Enfermagem 73.
- Karthijekan K, Cheng HY (2022) Effectiveness of a Motivated, Action-Based Intervention on Improving Physical Activity Level, Exercise Self-Efficacy and Cardiovascular Risk Factors of Patients with Coronary Heart Disease in Sri Lanka: A Randomized Controlled Trial Protocol. Plos one 17: 0270800. [CrossRef]
- Kruger HS, Venter CS, Vorster HH (2003) Physical Inactivity as a Risk Factor for Cardiovascular Disease in Communities Undergoing Rural to Urban Transition: The THUSA Study: Cardiovascular Topics. Cardiovasc J of S Afri 14: 16-23.
- Neethling I, Lambert EV, Cois A, Roomaney RA, Awotiwon OF, et al. (2022) Estimating the Changing Burden of Disease Attributable to Low Levels of Physical Activity in South Africa for 2000, 2006 And 2012. S Afri Med J 112: 639-648.
- Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, et al. (2012) Effect of Physical Inactivity on Major NonCommunicable Diseases Worldwide: An Analysis of Burden of Disease and Life Expectancy. Lancet 380: 219229. [CrossRef]
- Malambo P, Kengne AP, Lambert EV, De Villiers A, De Villiers A (2016) Prevalence and Socio-demographic Correlates of Physical Activity Levels among South African Adults in Cape Town and MountFrere Communities in 2008-2009. Arch Public Health 74: 54.
- Oyeyemi AL, Moss SJ, Monyeki MA (2016) Measurement of Physical Activity in Urban and Rural South African Adults: A Comparison of Two Self-Report Methods. BMC Public Health 16: 1-13.
- Ajaero CK, De Wet N, Odimegwu CO (2020) Integrating Rural–Urban Differentials in the Appraisal of Prevalence and Risk Factors of Non-Communicable Diseases in South Africa. GeoJournal 1-15.
- Mlangeni L, Makola L, Naidoo I, Chibi B, Sokhela Z, et al. (2018) Factors Associated with Physical Activity in South Africa: Evidence from a National Population-Based Survey. Open Pub Health J 11: 1. [CrossRef]
- Monyeki KD (2021) Selected Papers from the 2nd Ellisras Longitudinal Study and Other NonCommunicable Diseases Studies International Conference” Special Issue Editorial Children 8: 146.
- Mphekgwana PM, Monyeki KD, Mothiba TM, Makgahlela M, Kgatla K, et al. (2022) Screening and Interventions for Cardiovascular Disease Prevention in the Limpopo Province, South Africa: Use of the Community Action Model. Metabolites 12: 1067.
- Omotoso KO (2022) Inequalities in Household Food Expenditures in South Africa: Implications for the Burden of Non-Communicable Diseases (NCDs) and Health Inequality. Afri J of Develop Studies 12: 225.
- Mungal-Singh V (2011) United Nations High Level Meeting and NCD in South Africa. Glob Heart 4: 215-217.
- Sharma JR, Mabhida SE, Myers B, Apalata T, Nicol E, et al. (2021) Prevalence of Hypertension and Its Associated Risk Factors in a Rural Black Population of Mthatha Town, South Africa. International Journal of Environmental Research and Public Health 18: 1215.
- Mitchell J, Bradley C (2006) Quality Of Life in Age-Related Macular Degeneration: A Review of the Literature. Health Qual Life Outcomes 4: 97.
- Marquez PV, Farrington, JL (2013) The Challenge of Non-Communicable Diseases and Road Traffic Injuries in Sub-Saharan Africa: An Overview. Washington DC: World Bank.
- Barnes RY, Jelsma J, Parker R (2019) Improvements in Health-Related Quality of Life and Function in Middle-Aged Women with Chronic Diseases of Lifestyle after Participating in A Non-Pharmacological Intervention Programme: A Pragmatic Randomised Controlled Trial. African Journal of Disability 8: 1-14.
- Igwesi-Chidobe CN, Godfrey EL, Kengne AP (2015) Effective Components of Exercise and Physical Activity-related Behaviour-Change Interventions for Chronic Non-Communicable Diseases in Africa: Protocol for a Systematic Mixed Studies Review with Meta-analysis. BMJ open 5: 008036.
- Sparling PB, Owen N, Lambert EV, et al. (2000) Promoting Physical Activity: The New Imperative for Public Health. Health Education Research 15: 367-376. [CrossRef]
- Igwesi-Chidobe CN, Godfrey EL, Kitchen S, Onwasigwe CN, Sorinola IO (2019) Community-based Selfmanagement of Chronic Low Back Pain in a Rural African Primary Care Setting: A Feasibility Study. Primary Health Care Research & Development 20: 45.
- Santos AC, Willumsen J, Meheus F, Ilbawi A, Bull FC, et al. (2023) The Cost of Inaction on Physical Inactivity to Public Health Care Systems: A Population-Attributable Fraction Analysis. The Lancet Global Health 11: 32-39. [CrossRef]
- Wang H, Zeng W, Kabubei KM, Rasanathan JJK, Kazungu J, et al. (2023) Modelling the Economic Burden of SARSCoV-2 Infection in Health Care Workers in Four Countries. Nature Communications 14: 2791. [CrossRef]
- Narayan KV, Ali MK, Koplan JP (2010) Global Noncommunicable Diseases-Where Worlds Meet. New England Journal of Medicine 363: 11961198.
- Riza Y, Budiarto W, Haksama S, Kuntoro K, Yudhastuti R, et al. (2023) Health Services for Catastrophic Patients Through the National Health Insurance Program: Literature Review. Journal of Public Health in Africa 14: 2559. [CrossRef]
- Jauhari S, Pandit P, Agarwal M, Bajpai M, Kumar P, et al. (2023) Effectiveness of Educational Interventions on Knowledge and Behavioural Practices of Adolescents for Prevention of Non-Communicable Diseases in Low-and Middle-income Countries: A Systematic Review protocol. Int J of Noncommunicable Dis 8: 110-114.
- Evans RW, Smith T, Kay P, McWade D, Angouras N, et al. (2016) The Need for Biokineticists in the South African Public Health Care System. South African Journal of Sports Medicine 28: 85-86.
- Morris LD, Grimmer KA, Twizeyemariya A, Coetzee M, Leibbrandt DC, et al. (2021) Health System Challenges Affecting Rehabilitation Services in South Africa. Disability and Rehabilitation, 43: 877-883. [CrossRef]
- Zungu NP, Mabaso ML, Kumalo F, Sigida S, Wabiri N, et al. (2019) Prevalence of Non-Communicable Diseases (NCDs) and Associated Factors among HIV Positive Educators: Findings from the 2015/6 Survey of Health of Educators in Public Schools in South Africa. PLoS One 14: 0209756.
- Department of Health (2013) Strategic Plan for the Prevention and Control of NonCommunicable Diseases 2013-17. Department of Health, South Africa.
- McGregor D, Latulippe N, Whitlow R, Leora Gansworth K, McGregor L, et al. (2023) Towards Meaningful Research and Engagement: Indigenous Knowledge Systems and Great Lakes Governance. Journal of Great Lakes Research 49: 22-31. [CrossRef]
- Sibandze GF, Dludlu MN (2023) Interfacing Indigenous Knowledge with Scientific Knowledge for Improved Health Outcomes: Lessons from Eswatini. In Socio-Ecological Systems and Decoloniality: Convergence of Indigenous and Western Knowledge 33-49.
- Bucea-Manea-Țoniș R, Păun DG, Mîndrescu V (2023) A Managerial Perspective on Physical Education and Sports. Cambridge Scholars Publishing.
- Maspul KA, Almalki FA (2023) Preserving Local Wisdom: Unaizah’s Coffee Culture and Dates Farming Sustaining Cultural Heritage. J-CEKI: J Cendekia Ilmiah 2: 639-664.
- Burnett C, Hollander WJ (2004) The South African Indigenous Games Research Project of 4802001/2002. South African Journal for Research in Sport, Physical Education and Recreation 26: 9-23.
- Spires M, Delobelle P, Sanders D (2016) Diet-related Non-Communicable Diseases in South Africa: Determinants and Policy Responses. South African Health Review 2016: 35-42.
- Rasmus SM, Whitesell NR, Mousseau A, Allen J, et al. (2020) An Intervention Science to Advance Underrepresented Perspectives and Indigenous Self-Determination in Health. Prevention Science 21: 83-92. [CrossRef]
- Calzada I (2023) Smart Rural Communities: Action Research in Colombia and Mozambique. Sustainability 15: 9521.
- Ndubuisi NE (2021) Noncommunicable Diseases Prevention in Lowand Middle-Income Countries: An Overview of Health in All Policies (HiAP). Inquiry 58.
- Cole A, Pethan J, Evans J (2023) The Role of Agricultural Systems in Teaching Kitchens: An Integrative Review and Thoughts for the Future. Nutrients 15: 4045.
- Walter M, Suina M (2023) Indigenous Data, Indigenous Methodologies and Indigenous Data Sovereignty. Educational Research Practice in Southern Contexts 22: 207-220.
- Tao D, Awan-Scully R, Cole A, Gao Y, Ash G, et al. (2023) Integration of Exercise Prescription into Medical provision as a treatment for non-communicable diseases: A scoping review. Frontiers in Public Health 11. [CrossRef]
- Mohd Salim J, Anuar SN, Omar K, Tengku Mohamad TR Sanusi NA (2023) The Impacts of Traditional Ecological Knowledge towards Indigenous Peoples: A Systematic Literature Review. Sustainability 15: 824.
- Griffiths K, Davies L, Savage C, Shelling M, Dalziel P, et al. (2023) The Value of Recreational Physical Activity in Aotearoa New Zealand: A Scoping Review of Evidence and Implications for Social Value Measurement. International Journal of Environmental Research and Public Health 20: 2906. [CrossRef]
- Hargreaves J (2013) Heroines of Sport: The Politics of Difference and Identity. Routledge.
- Azlan A, Ismail N, Fauzi NFM, Talib RA (2021) Playing Traditional Games vs. Free Play During. Physical Education Lesson to Improve Physical Activity: A Comparison Study. Pedagogy of Physical Culture and Sports 25: 178-187. [CrossRef]
- Natalucci V, Marmondi F, Biraghi M, Bonato M (2023) The Effectiveness of Wearable Devices in Non-Communicable Diseases to Manage Physical Activity and Nutrition: Where We Are?. Nutrients 15: 913.
- Mdiya L, Taruvinga A, Mushunje A, Mopipi K, Ngarava S (2021) Rural Community Use and Perception of Rangeland Products in Eastern Cape Province, South Africa. African J of Sci Tech Inn Dev 13: 757-768.
- Otto J, Zerner C, Robinson J (2013) Natural Connections: Perspectives in Communitybased Conservation. Island press.
- Glover M, Kira A, Kira G, McRobbie H, Breier BH, et al. (2017) An Innovative Team-Based Weightloss Competition to Reduce Cardiovascular and Diabetes Risk Among Māori and Pacific People: Rationale and Method for the Study and its Evaluation. BMC nutrition 3: 1-9. [CrossRef]
- Salter G (2003) Maori Culture and Tradition in the Mainstream: Teaching Te Reo Kori1 in Sport Education. New Zealand Physical Educator 36: 27.
- Bowkett MT (2015) Towards Collaborative Pathways of Leadership in Education for Māori: a Thesis Presented in Partial Fulfilment of the Requirements for the Degree of Doctor of Education, at Massey University, Manawatū, New Zealand (Doctoral dissertation, Massey University).
- Mogamisi MS (2022) Indigenous Games, Dance, and Music for Promoting Health and Wellbeing of the Aged, North-West Province (Doctoral dissertation, North-West University (South Africa)).
- Madima TJ (2021) Exploring the Cultural Heritage Preservation through Digitisation: A Case Study of Traditional Children’s Games in Limpopo Province, South Africa (Doctoral Dissertation).
- Pramanik R (2018) Play and Indigenous Games of Children: A Cultural Heritage of Western Odisha, India. Knowledge Cultures 6: 96-110.
- Mudzielwana TN (2020) Factors Influencing Non-Participation of Youth on Indigenous Games in Thulamela Municipality of Vhembe District in Limpopo Province (Doctoral dissertation).
Figure 1.
Adapted from the taxonomy of indigenous games constructed by South African children 2001/2002.
Figure 1.
Adapted from the taxonomy of indigenous games constructed by South African children 2001/2002.

Figure 2.
Ranking of indigenous games by all participants.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



