
Submitted:
19 March 2024
Posted:
22 March 2024
You are already at the latest version
Abstract
Introduction: Accommodation is the ability of the eye to change its refractive power (by altering the curvature of the crystalline lens) with the aim of focusing on different distances. In modern times, close working distances require good accommodation to ensure quality work without vision problems. However, dysfunction in accommodation is not uncommon. Specifically, accommodation insufficiency is the most common dysfunction associated with accommodation that can be observed at any age. Accommodation insufficiency is characterized by the eye's inability to reach its maximum potential for accommodation (amplitude of accommodation) based on age, with many individuals experiencing deviations equal to or greater than 2 diopters (2D) from the theoretically normal range. Finally, measuring the amplitude of accommodation and near vision tests should be established in routine eye examinations, as life now involves a variety of different distances.
Objective: To record the rates of accommodative insufficiency in young Caucasian adults.
Methods: The method used was minus to blur, and the comparison charts were based on Donder's and Hofstetter's values. Depending on the result, they were categorized as "normal," which refers to deviations from zero to 1 diopter (1D) (due to the fact that minus lenses underestimate or are quite strict regarding the range of accommodation compared to other methods in free space (e.g., push-up); "borderline," which refers to deviations from 1.25D to 1.75D or 2D with at least one eye deviating by less than 1.75D; and "accommodation insufficiency," which refers to deviations greater than 2D from the expected values, as proposed in other studies.
Results: The results show a significant percentage of accommodation insufficiency in these age groups, with the percentage exceeding 50%. Additionally, men had significantly lower rates of normal accommodation amplitude compared to women. Further research is needed to study the role of refractive errors in accommodation problems.
Conclusions: In a broader context, accommodation insufficiency appears to be a significant issue in young age groups, and additional studies should be conducted to analyze the problem in depth and determine its prevalence. Furthermore, a universal system for measuring the range of accommodation should be established to obtain safer results. Additionally, it would be interesting to observe the role and contribution of the ciliary muscle in the accommodation process in young adults, as theoretically, the crystalline lens is almost transparent, the issue with adaptation primarily concerns the majority's inability of the ciliary muscle to function effectively.
Keywords:
Amplitude of accommodation
; accommodation insufficiency
1. Introduction
Accommodation is the ability of the eye to change its refractive power with the aim of focusing on objects at different distances. Numerous factors, both psychological and physical, influence the function of accommodation. Specifically, factors include refractive errors, light exposure, ethnicity, urbanization, ambient temperature, dyslexia, learning difficulties, intraocular pressure (IOP), diabetes, Down syndrome, thyroid dysfunction, alcohol, premature birth, time of day, etc. [12].
In modern times, close working distances have become a significant part of our vision. Research has shown that in Korea in 2018, 89.6% of individuals over the age of three were mobile phone users, with 19.1% categorized as “addicted” [1]. Long-term use of digital screens has been correlated with various visual and ocular issues, including adaptation problems, due to intense and prolonged use [1,12,14,24,25]. Furthermore, close working distances have been associated with the onset and progression of myopia. This is based on studies suggesting that the lag of accommodation plays a role in myopia development. However, there is also a contrary view that suggests the lag of accommodation was present before myopia appeared. Interestingly, children with early-onset myopia and adults with delayed-onset myopia exhibit greater accommodation instability compared to emmetropic individuals under similar visual stimuli. This instability may potentially contribute to myopia development [24,25]. Finally, close working distances (10–40 cm) in combination with poor posture can lead to different accommodation needs.For many, measuring the maximum range to which an individual can accommodate (amplitude of accommodation) is a routine assessment and should take place regardless of age. Furthermore, it is a key measurement for the onset and progression of presbyopia. The ability to accommodate exists from birth but improves dramatically in the first months of life [16]. Previous studies have shown that the most significant changes are observed between the ages of 20 and 50 [7]. Measuring the accommodation amplitude is a very important method for identifying various dysfunctions related to accommodation, with the most common being accommodation insufficiency (A.I.). Specifically, A.I. is a non-strabismic condition characterized by the inability of a non-presbyopic individual to activate accommodation to a degree considered normal based on their age group. As a condition, it can lead to a variety of problems in close-range tasks, such as blurred vision, diplopia, headaches, etc. The prevalence of accommodation insufficiency varies from 1% to 61.6%, depending on the research. Specifically, the prevalence has been recorded to reach up to 17% in children aged 8 to 16, while in the Caucasian population, this percentage is estimated at 6.2%. Conversely, lower values are reported in students in countries such as Iran and South Africa, with rates of 4% and 4.5%, respectively. Higher rates are recorded in children with learning difficulties, syndromes, and special needs. Specifically, in children with learning difficulties, the prevalence of accommodation insufficiency is 26%, and in children with Down syndrome, this percentage ranges between 55% and 76% [10]. Finally, it has been recorded that symptoms are more commonly observed in individuals with a difference of more than 2D from the expected age value [2,16]. Therefore, in this study, pure A.I. is recorded in individuals with a difference of 2D or more.
There are several methods for measuring amplitude of accommodation, such as push-up, push- down, minus to blur, dynamic retinoscopy, etc.
1.1. Push-Up Method
The push-up method is the most common and simplest clinical technique for measuring the A.I. In this method, the patient is fully corrected for distance vision, and as the target is brought closer, they are asked, “at what distance does the first minimum sustained blur occur?” This method has statistically significant errors due to subjectivity, primarily in reaction time. Finally, studies show that the above method yields higher values compared to other methods [7,12].
1.2. Push-Down Method
The push-down method is a modification of the push-up method. In this method, the object is gradually moved away from the eyes until the examinee reports that they see it clearly for the first time. This method is simpler and easier, as it requires less target resolution compared to the push- up method [12].
1.3. Minus Lens
In this method, negative lenses are added to the correction, with simultaneous observation of a near fixed target until permanent blur occurs. For some, this method should only be used in monocular vision, as it can disrupt binocular vision in an optically susceptible system, especially between convergence and accommodation. However, it is the most reliable and objective method with the highest repeatability, although its results yield lower values compared to other methods [7,12].
2. Methods
For this experiment, individuals with visual acuity for distance or near, binocular or monocular, which was less than 6/6–3, were excluded. The experiment was conducted in an examination room under ample lighting conditions (Figure 1). A chart of letters (Figure 2) with a size of 20/30 was used as the target, placed at a distance of 35 cm from the examinee (Figure 3). The size of the letters and the distance of the target were chosen to make the test more demanding for the examinee. In the final measurement, an addition of 2.5D corresponding to a distance of 35 cm was added. The chosen measurement method was the “minus lens” method, in which negative lenses are added until permanent minimum blur occurs despite the examinee’s efforts to clear the image. The “minus lens” method was selected due to its greater objectivity compared to other methods and its highest repeatability. It is important to note that the “minus lens” method yields smaller values for the adaptation range compared to the other methods. Instructions given to the examinees were to focus on letters on the 20/30 chart and report when they could no longer clear the letter despite their best effort. This was repeated three times per person, once binocularly and twice monocularly (once for each eye). For the categorization of the results, considerations were made based on suggestions that accommodation insufficiency should be considered a deviation greater than 2D from the normal value for the respective age. Furthermore, there are two other categories: “borderline,” which refers to deviations from 1.25D to 1.75D or 2D with at least one eye having a deviation less than 1.75D, and “normal,” which refers to zero to deviations on the order of 1D. This is because the “minus lens” method either underestimates or is quite strict in terms of the adaptation range compared to other methods in free space (e.g., push-up). Finally, for better and more accurate categorization, the values given by Donder for the age group measured and Hofstetter’s equation were used. Regarding the Hofstetter equation, the lowest value was considered, as it appears to be the most accurate.
Figure 1.
The examination room and lighting conditions used for the measurements.
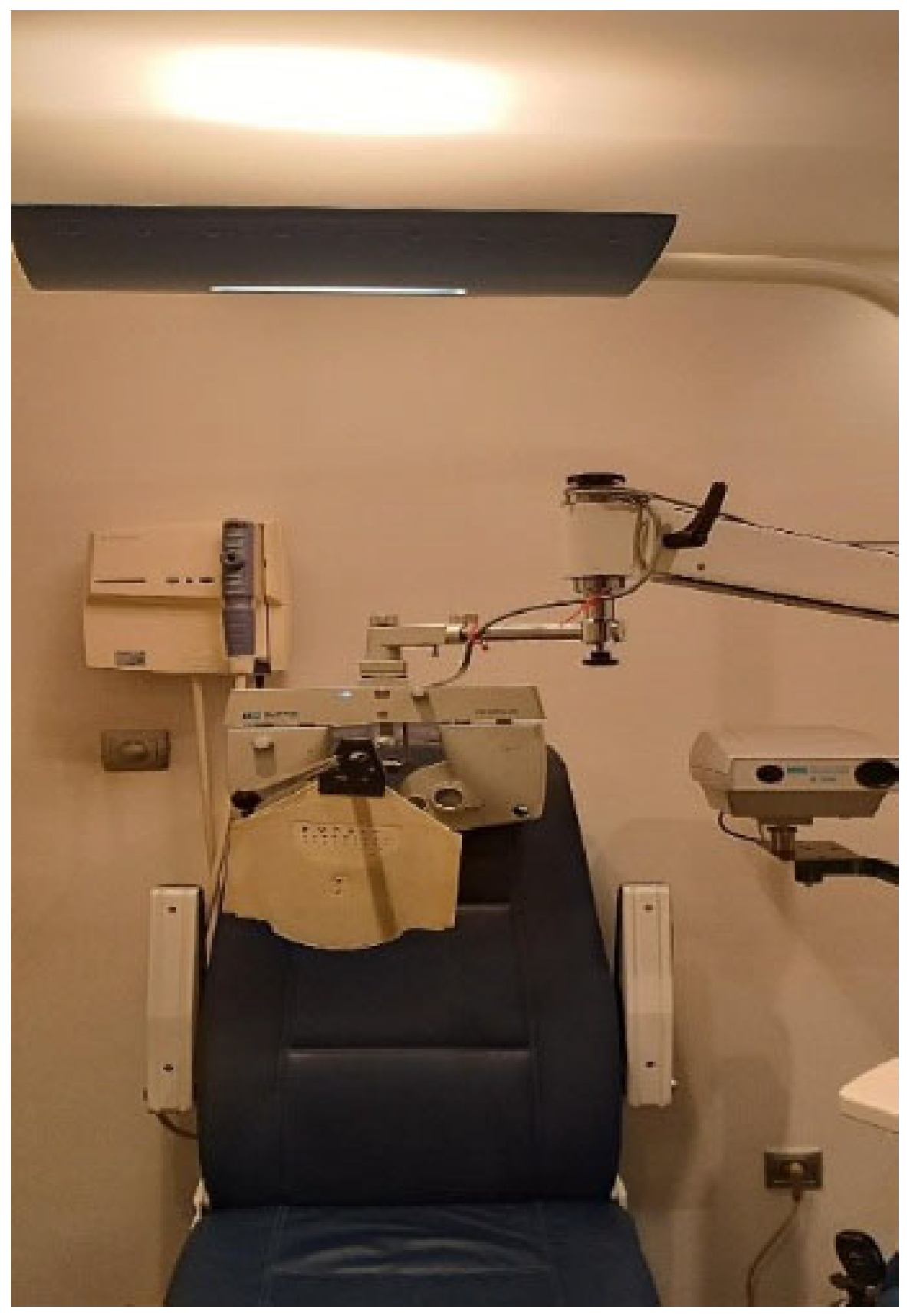
Figure 2.
The near visual acuity chart with a size of 20/30 used as the target.
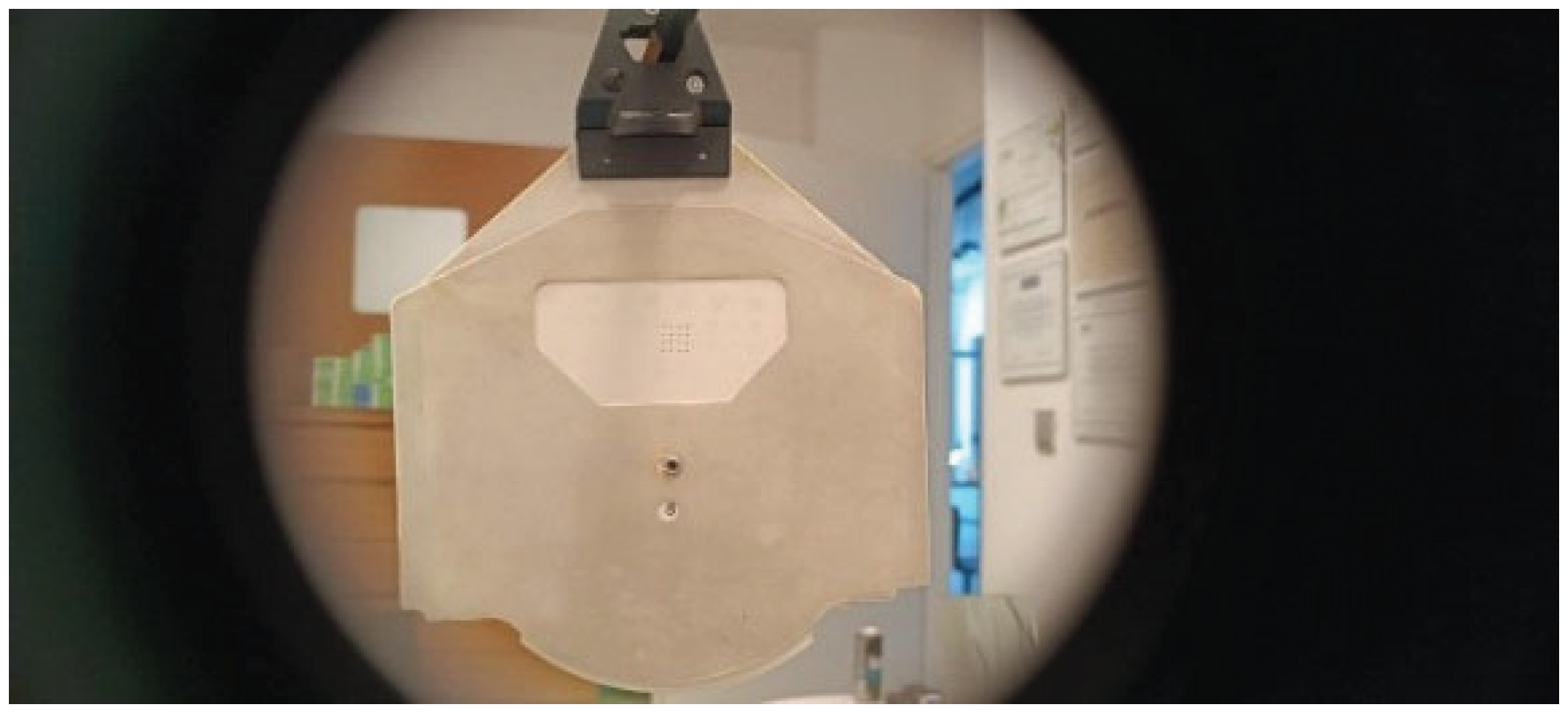
Figure 3.
The distance of 35 cm at which the near visual acuity chart was placed as the target.


Table 1.
Donder’s Amplitude of accommodation chart.
| Donder’s Amplitude of accommodation chart | |
| Age | Nomral Amplitude of Accommodation |
| 5 | 15D |
| 10 | 12.50D |
| 20 | 9.75D |
| 30 | 7.25D |
| 40 | 4D |
| 50 | 2.5D |
| 60 | 1.25D |
| 70 | 0.50D |
| 75 | 0.00D |
Table 2.
Hofstetter’s Amplitude of Accommodation equation.
| Hofstetter’s Amplitude of Accommodation equation | |
| Max | expected 25 - (0.4 x Age) |
| Normal | 18 - (0.3 x Age) |
| Minimum | expected 15 - (0.25 x Age) |
3. Statistic Analysis
Table 3.
Amplitude_of_accommodation_binocular.
| Sample size | 41 |
| Lowest value | 3,2500 |
| Highest value | 9,7500 |
| Arithmetic mean | 6,7439 |
| 95% CI for the mean | 6,2994 to 7,1884 |
| Median | 6,7500 |
| 95% CI for the median | 6,4404 to 7,2500 |
| Variance | 1,9828 |
| Standard deviation | 1,4081 |
| Relative standard deviation | 0,2088 (20,88%) |
| Standard error of the mean | 0,2199 |
| Coefficient of Skewness | -0,1409 (P=0,6881) |
| Coefficient of Kurtosis | 0,09811 (P=0,7134) |
| D’Agostino-Pearson test for Normal distribution |
accept Normality (P=0,8624) |
Figure 4.
Diagram showing normal distribution plot of amplitude of accommodation binocular.
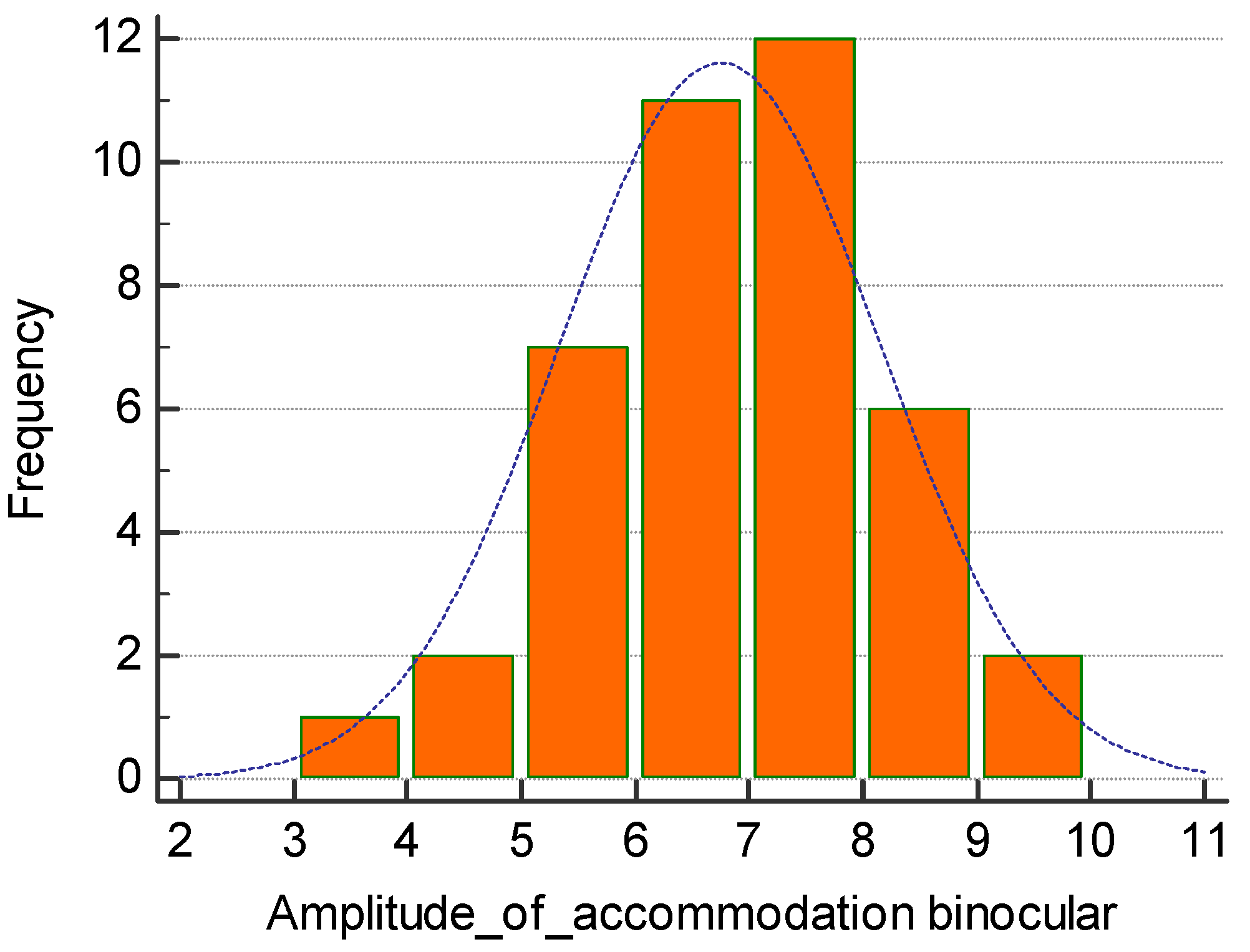
Table 3.
Amplitude_of_accommodation_binocular for male.
| Sample size | 19 |
| Lowest value | 3,2500 |
| Highest value | 8,7500 |
| Arithmetic mean | 6,2368 |
| 95% CI for the mean | 5,5812 to 6,8925 |
| Median | 6,7500 |
| 95% CI for the median | 5,2500 to 7,0545 |
| Variance | 1,8505 |
| Standard deviation | 1,3603 |
| Relative standard deviation | 0,2181 (21,81%) |
| Standard error of the mean | 0,3121 |
| Coefficient of Skewness | -0,4906 (P=0,3288) |
| Coefficient of Kurtosis | 0,001913 (P=0,8147) |
| D’Agostino-Pearson test for Normal distribution |
accept Normality (P=0,6039 |
Figure 5.
Diagram showing normal distribution plot of amplitude of accommodation binocular for male.
Figure 5.
Diagram showing normal distribution plot of amplitude of accommodation binocular for male.
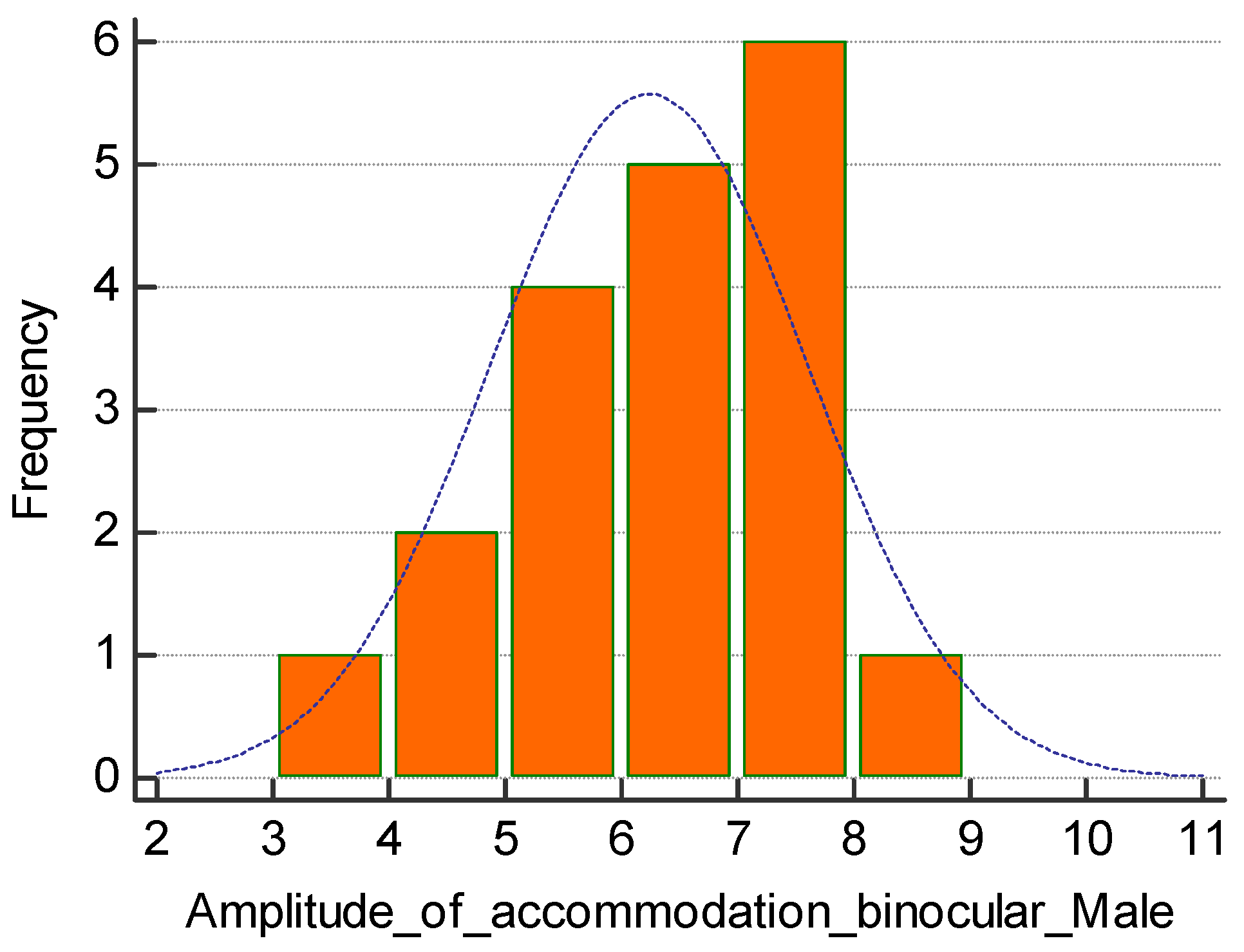
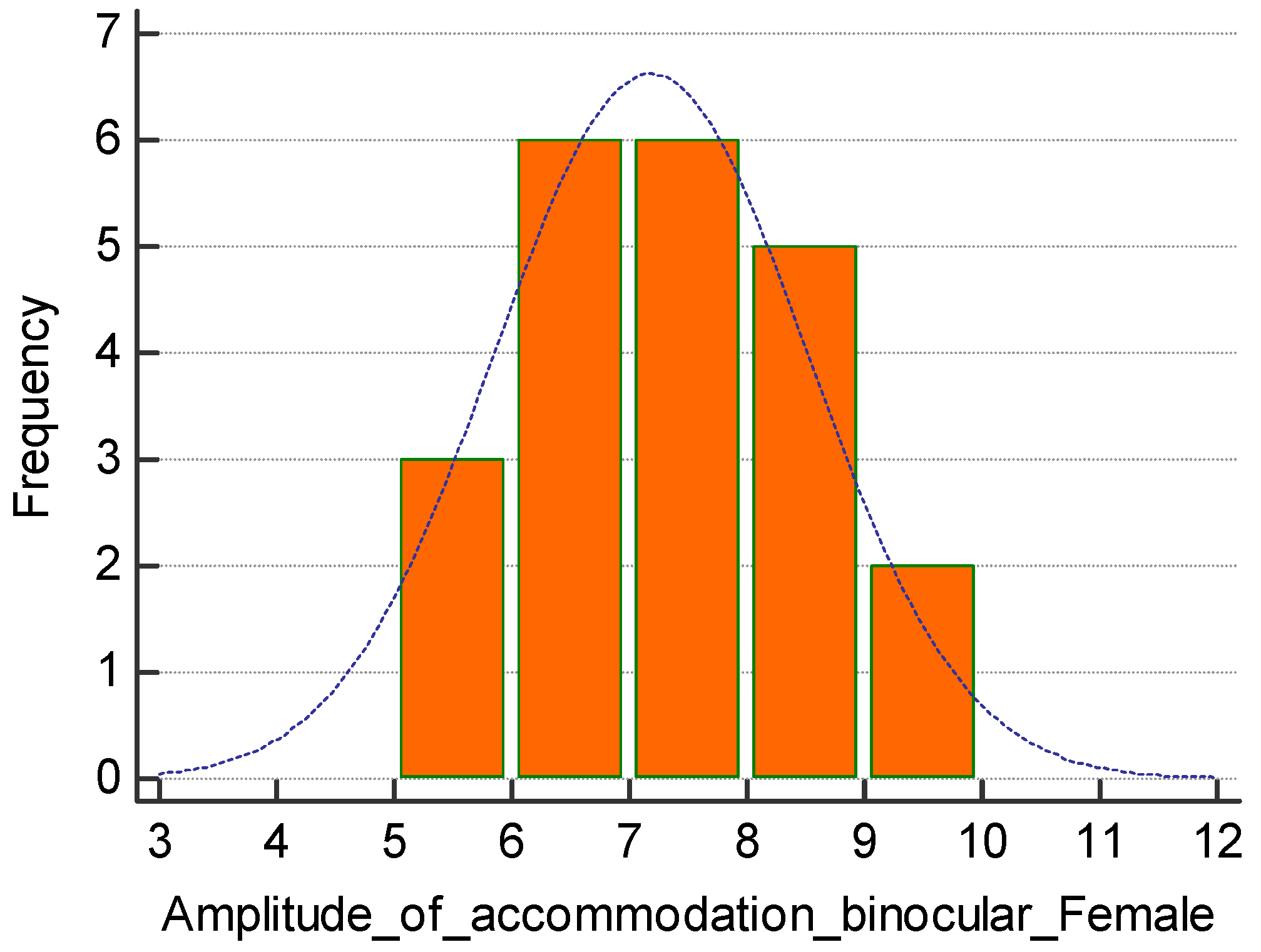
Figure 6.
Diagram showing normal distribution plot of amplitude of accommodation binocular for female.
Figure 6.
Diagram showing normal distribution plot of amplitude of accommodation binocular for female.
4. Results
The total sample collected for the study consisted of 41 individuals and a total of 82 eyes. Out of the total 41 individuals, 53.66% (22 individuals) were females, and 46.34% (19 individuals) were males, with an average age of approximately 23.71 years. Furthermore, out of the total 41 individuals, 78.04% (32 individuals) had myopia, 17.07% (7 individuals) had emmetropia, and 4.87% (2 individuals) had hypermetropia. Among the total 41 individuals, 24.39% (10 individuals) had a normal amplitude of accommodation (deviation up to 1D from the lowest expected based on age), 19.51% (8 individuals) had a borderline amplitude of accommodation (deviation from 1.25D to 1.75D or 2D with at least one eye deviating less than 1.75D from the lowest expected based on age), and 56.10% (23 individuals) had a low amplitude of accommodation (Table 4). Among the 32 individuals with myopia, 9 (28.125%) had a normal amplitude of accommodation, 4 (12.5%) had a borderline amplitude of accommodation, and the remaining 19 (59.375%) had a low amplitude of accommodation. Regarding the emmetropic individuals, out of the total of 7 individuals, 1 (14.29%) had a normal amplitude of accommodation, 4 (57.14%) had a borderline range, and 2 (28.57%) had a low amplitude of accommodation. As for the hypermetropic individuals, none had a normal or borderline amplitude of accommodation, so both of the 2 individuals (100%) had a low amplitude (Table 3, Table 4 and Table 5). Safe comparisons cannot be made due to the lack of samples in the emmetropic and hypermetropic categories. Regarding gender, as mentioned, 53.66% were females and 46.34% were males. Among females, 36.37% had a normal amplitude of accommodation, 13.63% had a borderline range, and 50% had a low amplitude, while the corresponding percentages for males were 10.53%, 26.32%, and
Table 4.
Amplitude_of_accommodation_binocular for female.
| Sample size | 22 |
| Lowest value | 5,0000 |
| Highest value | 9,7500 |
| Arithmetic mean | 7,1818 |
| 95% CI for the mean | 6,5941 to 7,7695 |
| Median | 7,1250 |
| 95% CI for the median | 6,4766 to 8,0117 |
| Variance | 1,7570 |
| Standard deviation | 1,3255 |
| Relative standard deviation | 0,1846 (18,46%) |
| Standard error of the mean | 0,2826 |
| Coefficient of Skewness | 0,1741 (P=0,7069) |
| Coefficient of Kurtosis | -0,5226 (P=0,6447) |
| D’Agostino-Pearson test for Normal distribution |
accept Normality (P=0,8378 |
Table 5.
Amplitude_of_accommodation_binocular for myopes.
| Myopes | Amplitude of accommodation |
| Normal amplitude of accommodation | 9 |
| Borderline amplitude of accommodation | 4 |
| Low amplitude of accommodation | 19 |
| 32 |
63.15%. Therefore, it is observed that females have higher percentages in both normal and borderline categories (Table 6). Now, regarding the binocular and monocular amplitude of accommodation, 46.34% (19 individuals) had a binocular amplitude of accommodation greater than the respective monocular range. None had a binocular amplitude of accommodation identical to the monocular amplitude of accommodation, 14.63% (6 individuals) had a binocular amplitude of accommodation identical to the greater monocular range, 2.34% (1 individual) had a binocular amplitude of accommodation identical to the smaller monocular range, 17.07% (7 individuals) had a binocular amplitude of accommodation between the monocular ranges, and 19.5% (8 individuals) had a binocular amplitude of accommodation smaller than the monocular range (Table 7). Additionally, the deviation of monocular amplitude of accommodation from binocular range greater than 0.5D was observed in at least one eye for 41.46% (17 individuals), while a deviation smaller than 0.5D was observed in 58.54% (24 individuals). Finally, identical monocular ranges of accommodation between the two eyes were recorded in 8 individuals, while different values were recorded in 34 individuals (Table 8). These results may arise from factors such as body posture that may affect one eye more than the other, dominance of one eye over the other, errors in the examiner’s or examinee’s estimation of accommodation, or other reasons.
Table 6.
Amplitude_of_accommodation_binocular for hyperopes.
| Hyperopes | Amplitude of accommodation |
| Normal amplitude of accommodation | 0 |
| Borderline amplitude of accommodation | 0 |
| Low amplitude of accommodation | 2 |
| 2 |
Table 7.
Amplitude_of_accommodation_binocular for emmetropes.
| Emmetropes | Amplitude of accommodation |
| Normal amplitude of accommodation | 1 |
| Borderline amplitude of accommodation | 4 |
| Low amplitude of accommodation | 2 |
| 7 |
Table 8.
Amplitude_of_accommodation_binocular according to gender.
| Amplitude of accommodation & Gender | ||
| Amplitude of accommodation | Women | Men |
| Normal | 8 | 2 |
| Borderline | 3 | 5 |
| Low | 11 | 12 |
| 22 | 19 | |
Table 9.
Deviation of amplitude of accommodation monocular vs binocular.
| Deviation of amplitude of accommodation monocular - binocular | |
| Deviation of monocular amplitude of accommodation from binocular range greater than 0.5D (at least one eye) |
17 |
| Deviation less than 0.5D | 24 |
| 41 | |
Table 10.
Identification between binocular range and monocular accommodation range.
| Identification between binocular range and monocular accommodation range | |
| Binocular amplitude of accommodation > monocular amplitude of accommodation | 19 |
| Binocular amplitude of accommodation = Monocular amplitude of accommodation | 0 |
| Binocular amplitude of accommodation = greater than monocular amplitude of accommodation | 6 |
| Binocular amplitude of accommodation = least monocular amplitude of accommodation | 1 |
| Binocular amplitude of accommodation between two monocular amplitude of accommodation | 7 |
| Binocular amplitude of accommodation < monocular amplitude of accommodation | 8 |
| 41 | |
5. Conclusions
In this specific study, using the methods and parameters that were employed and analyzed above, the following conclusions can be drawn. Firstly, the percentage of inadequate accommodation (which exceeds a deviation of 2D from the lower or normal value for age) is very high and affects 56.10% of the individuals who participated in this study. Furthermore, it is observed that females have higher percentages of normal range of adaptation compared to males, with these percentages reaching 36.37% and 10.53% respectively. Additionally, the binocular range of adaptation was higher than the monocular range of adaptation in 46.34%, while a lower binocular range of adaptation was observed in 19.5%. Differences were also observed in the maximum dioptric power between the two eyes. The cause cannot be confirmed; however, possible causes could be that one eye is dominant and functions at better levels, incorrect body posture resulting in one eye accommodating more than the other (as observed in other studies), incorrect estimation of the first curvature by the examinee or examiner, and other reasons.
Regarding the values used to compare our results, the Donder’s physiological values, though old, seem to still yield realistic results even today. In contrast, Hofstetter’s equation regarding the upper and normal limit for age does not appear realistic. However, if we maintain the lower expected value from Hofstetter’s equation as normal, then the results are indeed realistic and similar to Donder’s, with a deviation of about 0.25D between the two values.
In a broader context, inadequate accommodation seems to be a significant problem in young age groups, and further studies need to be conducted to thoroughly analyze the issue and its prevalence. Furthermore, a universal system for measuring the range of accommodation should be established to obtain safer results. Additionally, it would be interesting to observe the action and contribution of the ciliary muscle in the accommodation process in young adults, as theoretically, the crystalline lens is almost transparent, so the problem in accommodation primarily concerns the inability of the ciliary muscle to act effectively. Finally, inadequate accommodation implies problems with close-range work, but this is unlikely to improve overall, as orthoptic exercises and vision training cannot be universally used to manage or address this problem. Consequently, among other factors, presbyopia is likely to begin at even younger ages.
References
- Kang, J.W., Chun, Y.S. & Moon, N.J. A comparison of accommodation and ocular discomfort change according to display size of smart devices. BMC Ophthalmol 21, 44 (2021). [CrossRef]
- Hashemi H, Nabovati P, Khabazkhoob M, Yekta A, Emamian MH, Fotouhi A. Does Hofstetter’s equation predict the real amplitude of accommodation in children? Clin Exp Optom. 2018 Jan;101(1):123-128. Epub 2017 May 17. [CrossRef] [PubMed]
- Domínguez-Vicent A, Monsálvez-Romín D, Esteve-Taboada JJ, Montés-Micó R, Ferrer- Blasco T. Effect of age in the ciliary muscle during accommodation: Sectorial analysis. J Optom. 2019 Jan-Mar;12(1):14-21. Epub 2018 Apr 4. [CrossRef] [PubMed] [PubMed Central]
- E.S. Pateras. (2012). Measurement of the eye accommodation range in young people with different daily habits. e-Journal of Science & Technology, vol 7, issue 2, p. 9-14.
- Veselý P, Hanák L, Beneš P. Digital Eye Strain in a Population of Young Subjects. CeskSlov Oftalmol. 2019 Winter;74(4):154-157. English. [CrossRef] [PubMed]
- Gantz L, Stiebel-Kalish H. Convergence insufficiency: Review of clinical diagnostic signs. J Optom. 2022 Oct-Dec;15(4):256-270. Epub 2021 Dec 25. [CrossRef] [PubMed] [PubMed Central]
- Momeni-Moghaddam H, Kundart J, Askarizadeh F. Comparing measurement techniques of accommodative amplitudes. Indian J Ophthalmol. 2014 Jun;62(6):683-7. [CrossRef] [PubMed] [PubMed Central]
- Zapata-Díaz JF, Radhakrishnan H, Charman WN, López-Gil N. Accommodation and age- dependent eye model based on in vivo measurements. J Optom. 2019 Jan-Mar;12(1):3-13. Epub 2018 Mar 21. [CrossRef] [PubMed] [PubMed Central]
- Liang, X., Wei, S., Li, SM. et al. Effect of reading with a mobile phone and text on accommodation in young adults. Graefes Arch Clin Exp Ophthalmol 259, 1281–1288 (2021). [CrossRef]
- Hussaindeen JR, Murali A. Accommodative Insufficiency: Prevalence, Impact and Treatment Options. Clin Optom (Auckl). 2020 Sep 11;12:135-149. [CrossRef] [PubMed] [PubMed Central]
- Horwood AM, Toor SS, Riddell PM. Change in convergence and accommodation after two weeks of eye exercises in typical young adults. J AAPOS. 2014 Apr;18(2):162-8. Epub 2014 Feb 28. [CrossRef] [PubMed] [PubMed Central]
- Burns, David & Evans, Bruce & Allen, Peter. (2014). Clinical measurement of amplitude of accommodation: a review. Optometry in Practice. 15. 75-86.
- Ostadimoghaddam H, Hashemi H, Nabovati P, Yekta A, Khabazkhoob M. The distribution of near point of convergence and its association with age, gender and refractive error: a population-based study. Clin Exp Optom. 2017 May;100(3):255-259. Epub 2016 Sep 22. [CrossRef] [PubMed]
- Jaiswal S, Asper L, Long J, Lee A, Harrison K, Golebiowski B. Ocular and visual discomfort associated with smartphones, tablets and computers: what we do and do not know. Clin Exp Optom. 2019 Sep;102(5):463-477. Epub 2019 Jan 21. [CrossRef] [PubMed]
- Hashemi H, Nabovati P, Yekta AA, Ostadimoghaddam H, Forouzesh S, Yazdani N, Khabazkhoob M. Amplitude of accommodation in an 11- to 17-year-old Iranian population. Clin Exp Optom. 2017 Mar;100(2):162-166. Epub 2016 Aug 22. [CrossRef] [PubMed]
- Shukla Y. Accommodative anomalies in children. Indian J Ophthalmol. 2020 Aug;68(8):1520-1525. [CrossRef] [PubMed] [PubMed Central]
- Mihelčič M, Podlesek A. Cognitive workload affects ocular accommodation and pupillary response. J Optom. 2023 Apr-Jun;16(2):107-115. Epub 2022 Jun 25. [CrossRef] [PubMed] [PubMed Central]
- Ward LM, Gaertner C, Olivier L, Ajrezo L, Kapoula Z. Vergence and accommodation disorders in children with vertigo: A need for evidence-based diagnosis. eClinicalMedicine. 2020 Apr 18;21:100323. [CrossRef] [PubMed] [PubMed Central]
- Hashemi H, Pakbin M, Ali B, Yekta A, Ostadimoghaddam H, Asharlous A, Aghamirsalim M, Khabazkhoob M. Near Points of Convergence and Accommodation in a Population of University Students in Iran. J Ophthalmic Vis Res. 2019 Jul 18;14(3):306-314. [CrossRef] [PubMed] [PubMed Central]
- Coulter RA, Bade A, Jenewein EC, Tea YC, Mitchell GL. Near-point Findings in Children with Autism Spectrum Disorder and in Typical Peers. Optom Vis Sci. 2021 Apr 1;98(4):384-393. [CrossRef] [PubMed] [PubMed Central]
- Kaphle D, Varnas SR, Schmid KL, Suheimat M, Leube A, Atchison DA. Accommodation lags are higher in myopia than in emmetropia: Measurement methods and metrics matter. Ophthalmic Physiol Opt. 2022 Sep;42(5):1103-1114. Epub 2022 Jul 1. [CrossRef] [PubMed] [PubMed Central]
- Jang JU, Park IJ, Jang JY. The distribution of near point of convergence, near horizontal heterophoria, and near vergence among myopic children in South Korea. Taiwan J Ophthalmol. 2016 Oct-Dec;6(4):187-192. Epub 2016 Sep 28. [CrossRef] [PubMed] [PubMed Central]
- Wiecek EK, Roberts TL, Shah AS, Raghuram A. Vergence, accommodation, and visual tracking in children and adolescents evaluated in a multidisciplinary concussion clinic. Vision Res. 2021 Jul;184:30-36. Epub 2021 Apr 7. [CrossRef] [PubMed] [PubMed Central]
- Logan NS, Radhakrishnan H, Cruickshank FE, Allen PM, Bandela PK, Davies LN, Hasebe S, Khanal S, Schmid KL, Vera-Diaz FA, Wolffsohn JS. IMI Accommodation and Binocular Vision in Myopia Development and Progression. Invest Ophthalmol Vis Sci. 2021 Apr 28;62(5):4. [CrossRef] [PubMed] [PubMed Central]
- Yu H, Zeng J, Li Z, Hu Y, Cui D, Zhao W, Zhao F, Yang X. Variability of Accommodative Microfluctuations in Myopic and Emmetropic Juveniles during Sustained near Work. Int J Environ Res Public Health. 2022 Jun 9;19(12):7066. [CrossRef] [PubMed] [PubMed Central]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



