
Submitted:
14 March 2024
Posted:
15 March 2024
You are already at the latest version
Abstract
Hepatitis C virus (HCV) is a major public health threat associated with serious clinical consequences worldwide. The WHO reports an estimated 58 million people globally living with chronic hepatitis C virus (HCV) infection, with 1.5 million new cases and over 350,000 deaths annually due to HCV-related diseases. Despite the existence of multiple diagnostic methods, the accessibility of diagnosis and treatment is often hindered across the continent by limited resources, insufficient healthcare infrastructure, and low public awareness of Hepatitis C virus Hepatitis C virus infection is a major public health concern in African countries, which have the highest prevalence rates of HCV in the world (1–26%).
Egypt, African country which had the highest prevalence of Hepatitis C virus infection in the world. Its national hepatitis C elimination initiative emerges as an exemplary case of success an having screened over 60 million individuals, and treated more than 4 million, thereby markedly diminishing both the prevalence and incidence of the disease. The strategies employed by Egypt offer critical insights and adaptable frameworks for other African Countries facing analogous challenges.
The Aim of this Review is to highlight the triumphs and hurdles of Egypt's approach, while also providing strategic guidance for African Countries to accelerate the journey towards the eradication of hepatitis C.
Keywords:
Hepatitis C
; Elimination
; Africa
; Egypt
; Direct-acting antivirals
; Policy insights
; Hepatitis virus
Introduction
Hepatitis C virus (HCV) is a small enveloped positive sense stranded RNA virus belonging to the genus Hepacinivirus within the family Flaviviridae. World Health Organization (WHO) estimate that About 58 million individuals are chronically infected with hepatitis C virus (HCV) infection, and over 350,000 people die Annually from hepatitis C related Complications and Diseases [1]. Unlike other Hepatitis Viruses (such as HBV, et al), HCV have higher tendency to cause chronic infections which can persist for years without noticeable symptoms leading to long term liver damage; it exhibit remarkable genetic diversity with multiple genotypes and numerous subtypes which affect the treatment response and the course of disease; also unlike Hepatitis A and B, there’s no specific vaccine for HCV, Prevention relies on avoiding risk factors and practicing safe behaviors; and also HCV often progress silently with few early symptoms which can even sometimes appear, and simultaneously with significant liver damage have occurred [1,2,3,4]. HCV stands as a primary cause of chronic liver disease, with persistent infection linked to severe conditions such as cirrhosis, hepatocellular carcinoma, liver failure, and mortality [5,6,7]. while other hepatitis viruses (like HAV, and HEV) Primarily spread through contaminated water and food, HCV is mainly transmitted through blood-to-blood contact, and in that case intravenous drug use, unsafe medical procedures, and blood transfusion are the most common routes of transmission. [8,9].
The Available Estimates indicate that Hepatitis C virus (HCV) Remains a significant public health concern in Africa, where more than 91 million individuals are affected by Hepatitis B or C accounting for 26% of the global burden of these infections, resulting in Approximately 125, 0000 deaths annually, however several challenges hinder the effective management by which over 70% global hepatitis B cases occur in Africa necessitating robust prevention and treatment efforts [1,4,9,10]. Various risk factors for HCV infection in Africa include Traditional practices (such as Scarification), family history of viral hepatitis, geographical location, unsafe transfusion practices, unsafe injection drug use, and risky sexual behaviors leading to blood exposure [11,12,13]. While there have been significant advances in the treatment of hepatitis C, many people still do not have access to treatment. Lack of access is due to various barriers, such as high costs, limited healthcare resources, and lack of awareness Despite the existence of effective and cost-efficient Direct-Acting Antiviral (DAAs) medications capable of curing HCV in the majority of cases with minimal adverse effects [3,10,11]. Many countries adopted this goal of 90% reduction in chronic HCV incidence and a 65% reduction in HCV mortality by 2030, and established HCV elimination programs. However, the SARS-CoV-2 pandemic’s detrimental impact on the health system slowed or even suspended HCV elimination programs. [14],significant gaps persist in testing and treatment services for viral hepatitis. [14,15,16,17].
Nevertheless, amidst these challenges lie instances of success and innovation within the region that can serve as models for accelerating hepatitis C elimination efforts in other countries. [18]. Egypt had the highest HCV prevalence in the world; with over 6 million people infected due to unsafe injection practices in the past started in the 1960s when the government carried out mass treatment campaigns to eradicate Schistosomiasis among its population, Lack of sterilization and reuse of non-disposable needles led to the rapid spread of HCV.
Notably, Egypt's remarkable progress in combating hepatitis C serves as a beacon of hope. Egypt's proactive measures have yielded substantial results by significantly reducing new infection rates and achieving international recognition for their strides towards hepatitis C elimination [19]. Through years of coordinated government action, Egypt has launched a nationwide campaign (known as the “100 million seha” (100 million healthy lives)) to eliminate hepatitis C by 2023, offering free testing and treatment for everyone [19,20,21,22].
The Aims of this Review is to spotlight Egypt's achievements and obstacles in their hepatitis C elimination initiative, offering valuable insights and recommendations for other African Countries committed to eradicating this pressing public health concern.
Prevalence of Hepatitis C in Africa
Hepatitis C virus (HCV) remains a significant public health challenge in Africa. Sub-Saharan Africa has a substantial HCV disease burden, but a detailed epidemiology and understanding of the disease burden is absent. A severe limitation in this respect is the scarcity of reliable prevalence data, and population-based studies. According to WHO Over 70 million Africans are affected by chronic viral hepatitis, with approximately 60 million having hepatitis B and 10 million having hepatitis C. While hepatitis B infection is preventable and treatable, HCV infection is now curable [23]. The African region accounts for 26% of the global burden of hepatitis B and C, resulting in 125,000 associated deaths. Additionally, modelled data suggests that South Africa has a prevalence of HCV below 1%, with approximately 600,000 infected. Globally, HCV affects over 71 million people, with 14% residing in sub-Saharan Africa [1,2,4,24]. North Africa experiences some of the highest HCV prevalence rates, notably in Egypt, which historically had one of the world's highest rates of HCV infection with over 6 million people infected, largely due to unsafe injection practices, et al. [4,24,25]. Other countries with significant prevalence rates include Libya, Nigeria, Cameroon, Gabon, and the Democratic Republic of Congo. It is important to note that the prevalence data can differ between studies within the same region, reflecting the complexity of epidemiological surveillance. In 2019, the African region accounted for a considerable portion of the global HCV burden, with a significant number of deaths attributed to the disease (Figure 1). The WHO's efforts to track and address this public health challenge are ongoing, with the aim of reducing the incidence and impact of HCV across the continent.
The WHO's efforts to combat Hepatitis B and C include increasing the coverage of routine childhood vaccination against Hepatitis B, which is currently at 72% for the region, below the global target of 90%. Moreover, diagnosis and treatment rates for Hepatitis C are alarmingly low, with only an estimated 5% of infected persons diagnosed and close to 0% treated.
These statistics highlight the urgent need for improved healthcare interventions, including vaccination, safe injection practices, and access to diagnosis and treatment services to reduce the burden of Hepatitis C in Africa.
Strategies to Eradicate Hepatitis C in Africa
Although detailed and reliable HCV seroepidemiological data are scarce in many parts of sub-Saharan Africa, available estimates are indicative of a substantial burden.
The necessary tools for viral hepatitis elimination are already available, but worldwide implementation of a concerted viral hepatitis response is slow and faces many challenges. These include low levels of investments in health overall; inadequate data and weak surveillance systems; poor infrastructure; low awareness among policymakers, at-risk populations, and primary care practitioners; high prices of some diagnostics and treatments; and a lack of prioritization of viral hepatitis. To establish the true burden, systematic population-based seroprevalence studies should be included when constructing models of national programs for control of HCV in the region. Notably, the scarcity of seroprevalence data should not act as a barrier to the expansion of screening for HCV in people at risk and in the general population, or to the improvement of HCV detection, linkage to care, and effective treatment of HCV infection.
Efforts to address this silent epidemic require increased awareness, improved infrastructure, and targeted interventions to reduce the burden of HCV in the region. The WHO's 2016 Global Health Sector Strategy on viral hepatitis set a goal to eliminate the disease as a public health threat by 2030 (Table 1), aiming for a 90% reduction in incidence and a 65% reduction in mortality from 2015 levels [2,26,27]. This strategy provides a framework for countries to track their progress in reducing hepatitis B and C infections and related deaths, while also achieving high coverage of preventive interventions. These interventions include hepatitis B vaccinations for infants, blood and injection safety, harm reduction, and HBV/HCV testing and treatment, et al [14].
Despite this strategic direction, few African countries have developed a national hepatitis strategic plan, with most still in draft form. The region faces significant gaps in hepatitis testing and treatment, with fewer than eight countries offering subsidized services. Challenges include securing adequate funding, political commitment, health system capacity, community engagement, and human rights protection for those affected by hepatitis C [14,28,29].
Egypt's program, which began in 2014 and intensified in 2018, aimed to eradicate hepatitis C by 2023 is a remarkable example of how a country can overcome a major public health challenge. Key components included nationwide screening the entire adult population for hepatitis C and assess them for noncommunicable diseases (NCDs) such as diabetes and hypertension, to treat all people diagnosed with hepatitis C with direct-acting antivirals (DAAs), which can cure more than 95% of cases. The treatment was provided for free at public health facilities, and was supported by local production of generic DAAs, negotiated price reductions, and innovative financing mechanisms such as health insurance and social solidarity funds. [15,25], to prevent new infections by improving blood safety, infection control, and harm reduction practices. The program also promoted hepatitis B vaccination, which can prevent hepatitis D co-infection, and raised awareness among the public and health care providers about hepatitis C transmission and prevention, and a comprehensive surveillance system to monitor progress to monitor and evaluate the program's progress and impact using a comprehensive surveillance system, which included regular surveys, sentinel sites, and viral load testing. The program also collaborated with the World Health Organization (WHO) and other partners to validate its achievements and share its lessons learned [19,30,31,32,33].
The outcomes of the program were impressive and unprecedented. By 2022, the program had screened over 60 million people and treated more than 4 million people. The prevalence of hepatitis C in Egypt dropped from 10% in 2014 to 0.38% in 2022, and the incidence of new infections decreased from 300 per 100 000 in 2014 to 9 per 100 000 in 2022 [18,24].Egypt became the first country to achieve the "gold tier" status on the path to elimination of hepatitis C as per WHO criteria, which means that it fulfilled the programmatic coverage targets that will enable it to achieve the reduced incidence and mortality targets of full elimination by 2030 [26].
Lessons to Learn from Egypt’s Hepatitis C Elimination Program and Recommendations to Other African Countries
It is estimated that achieving hepatitis C elimination in Africa by 2030 could avert 1.4 million deaths, 3.5 million new infections, and 62 billion USD in economic losses [2,4,35,36,37]. Therefore, we call on all stakeholders to increase their investment, political commitment, and collaboration to achieve hepatitis C elimination in Africa, and to make it a reality for the millions of people who deserve a healthy and dignified life.
Egypt's model for eliminating hepatitis C could be a blueprint for other African countries that face a high burden of Hepatitis B or C Infections, but also have limited resources, infrastructure, and awareness [35,38]. However, each country needs to adapt the model and put in account the WHO Strategic plan to its own context, considering the epidemiology, transmission, and risk factors of hepatitis C, as well as the health system capacity, political situation, and cultural norms.
The key factors that enabled Egypt to achieve this remarkable feat were political commitment and leadership, innovative financing and partnerships, and community mobilization and awareness. These factors allowed Egypt to implement a comprehensive and ambitious program that covered screening, diagnosis, treatment, prevention, and surveillance of hepatitis C, and that reached millions of people across the country [16,19,37,39,40].
Based on Egypt's success story, we recommend the following actions for African governments, international organizations, and other stakeholders to accelerate hepatitis C elimination efforts in Africa:
- o
- Conduct a situation analysis and a gap assessment to understand the magnitude and characteristics of the hepatitis C epidemic, and the strengths and weaknesses of the existing response. This could include conducting seroprevalence surveys, reviewing policies and guidelines, and mapping stakeholders and resources [16,39].
- o
- o
- Establish a national coordination mechanism and a governance structure to oversee and monitor the program, and to ensure accountability and transparency. This could include setting up a national committee or a technical working group, involving representatives from the government, civil society, academia, and development partners
- o
- Mobilize domestic and external resources and partnerships to finance and implement hepatitis C elimination programs, and to leverage existing platforms and initiatives. This could include advocating for increased budget allocation, applying for grants from the Global Fund and other donors, negotiating with pharmaceutical companies for price reductions and voluntary licenses, and collaborating with other health programs such as HIV, tuberculosis, and noncommunicable diseases [18,29,34,38].
- o
- Implement hepatitis C elimination programs in a phased and prioritized manner, starting with the most affected and vulnerable populations and areas, and scaling up gradually and systematically [11,13,41,42]. The programs should cover the following components: screening, diagnosis, treatment, prevention, and surveillance, and should use a patient-centered and human rights-based approach.
- o
- Strengthen health systems and health workforce capacity to deliver quality and safe hepatitis C services, and to ensure the availability and accessibility of diagnostics and medicines [24,26,43]. This could include training and motivating health workers, improving infection control and blood safety practices, and enhancing supply chain and logistics management.
- o
- Monitor and evaluate the program's progress and impact, using a robust and standardized data collection and reporting system, and applying the WHO validation criteria and tools [18,26]. The program should also conduct regular reviews and evaluations and disseminate and use the findings and lessons learned to improve the program.
- o
- Enhance public awareness and community engagement to increase the demand and uptake of hepatitis C services, and to address stigma and discrimination against people living with or at risk of hepatitis C. This could include conducting social and behavior change communication campaigns, providing accurate and reliable information, and involving civil society organizations, religious groups, and celebrities in the program [44,45].
Other strategies and interventions that could support hepatitis C elimination efforts in Africa are: Improving access to diagnostics and treatment, by simplifying and decentralizing the service delivery model, integrating hepatitis C services with other health services, and using point-of-care and self-testing technologies [18,24]. Strengthening health systems, by building the capacity and motivation of health workers, ensuring the quality and safety of health services, and improving the supply chain and logistics of diagnostics and medicines [41,46]. Enhancing public awareness, by conducting social and behavior change communication campaigns, providing accurate and reliable information, and addressing stigma and discrimination against people living with or at risk of hepatitis B and C [3,44,46,47].
Conclusion
Elimination of HBV and HCV infections by 2030 will produce substantial benefits for public health and prevent millions of deaths. Much of what is needed to reach these goals is already in place. The elimination of chronic HCV is urgent and important. To reach this goal, clever interventions by African health systems to overcome barriers are needed. Adapting WHO’s goals and strategy, Resources, training, and awareness are important factors for success. Despite the challenges entailed, Egypt's national hepatitis C elimination program exemplifies a successful response to this challenge. learning from Egypt’s milestone is essential to reduce morbidity and mortality. Overall, countries that performed mass screening and treatment campaigns for HCV as a part of national programs had extraordinary success, while countries that did not carry out any national program remain with a heavy HCV burden. A collective effort from all stakeholders is essential to make hepatitis C elimination a reality for the millions who deserve a healthier, more dignified life.
References
- WHO, “Hepatitis C.” Accessed: Jan. 16, 2024. [Online]. Available: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c.
- M. W. Sonderup et al., “Hepatitis C in sub-Saharan Africa: the current status and recommendations for achieving elimination by 2030,” Lancet Gastroenterol. Hepatol., vol. 2, no. 12, pp. 910–919, Dec. 2017. [CrossRef]
- G. Taha, L. Ezra, and N. Abu-Freha, “Hepatitis C Elimination: Opportunities and Challenges in 2023,” Viruses, vol. 15, no. 7, Art. no. 7, Jul. 2023. [CrossRef]
- M. J. Karoney and A. M. Siika, “Hepatitis C virus (HCV) infection in Africa: a review,” Pan Afr. Med. J., vol. 14, no. 44, Art. no. 44, Jan. 2013. [CrossRef]
- L. J. de Oliveria Andrade, A. D’Oliveira, R. C. Melo, E. C. De Souza, C. A. Costa Silva, and R. Paraná, “Association Between Hepatitis C and Hepatocellular Carcinoma,” J. Glob. Infect. Dis., vol. 1, no. 1, pp. 33–37, 2009. [CrossRef]
- “Pathogenesis of hepatitis C virus-related hepatocellular carcinoma: evidence from recent studies - Maruyama - Journal of Public Health and Emergency.” Accessed: Jan. 16, 2024. [Online]. Available: https://jphe.amegroups.org/article/view/7483/html.
- “Hepatitis C Virus and Hepatocellular Carcinoma: A Narrative Review - PMC.” Accessed: Jan. 16, 2024. [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5863002/.
- “Systematic review of prevalence and risk factors of transfusion transmissible infections among blood donors, and blood safety improvements in Southern Africa | Request PDF,” ResearchGate, Oct. 2023. [CrossRef]
- Syed Hasan Mohamed El-Sagheer, Oswaldo Castro, and Samuel A Giday, “HCV in sickle cell disease.” Accessed: Jan. 16, 2024. [Online]. Available: https://www.researchgate.net/publication/9065255_HCV_in_sickle_cell_disease.
- “Trends of the Global Hepatitis C Disease Burden: Strategies to Achieve Elimination.” Accessed: Jan. 16, 2024. [Online]. Available: https://www.jpmph.org/journal/view.php?number=2154.
- R. Seu et al., “Challenges and Best Practices for Hepatitis C Care among People Who Inject Drugs in Resource Limited Settings: Focus Group Discussions with Healthcare Providers in Kenya,” Glob. Public Health, vol. 17, no. 12, p. 3627, Dec. 2022. [CrossRef]
- M. A. Mohd Suan, S. M. Said, P. Y. Lim, A. Z. F. Azman, and M. R. Abu Hassan, “Risk factors for hepatitis C infection among adult patients in Kedah state, Malaysia: A case–control study,” PLOS ONE, vol. 14, no. 10, p. e0224459, Oct. 2019. [CrossRef]
- Diana Nurutdinova, Arbi B. Abdallah, Susan Bradford, Catina C. O’Leary, and Linda B. Cottler, “Risk factors associated with Hepatitis C among female substance users enrolled in community-based HIV prevention studies - PMC.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3095996/.
- WHO africa region, “Hepatitis Scorecard for the WHO Africa Region Implementing the hepatitis elimination strategy,” WHO | Regional Office for Africa. Accessed: Jan. 17, 2024. [Online]. Available: https://www.afro.who.int/publications/hepatitis-scorecard-who-africa-region-implementing-hepatitis-elimination-strategy.
- WHO africa, “New WHO scorecard shows poor progress of the viral hepatitis response in the African region,” WHO | Regional Office for Africa. Accessed: Jan. 17, 2024. [Online]. Available: https://www.afro.who.int/news/new-who-scorecard-shows-poor-progress-viral-hepatitis-response-african-region.
- Johns Hopkins University, Baltimore, MD USA, “Progress towards elimination goals for viral hepatitis - PMC.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7376316/.
- S. Popping et al., “The global campaign to eliminate HBV and HCV infection: International Viral Hepatitis Elimination Meeting and core indicators for development towards the 2030 elimination goals,” J. Virus Erad., vol. 5, no. 1, p. 60, Jan. 2019. [CrossRef]
- WHO, “Access to treatment and care for all: the path to eliminate hepatitis C in Egypt.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.who.int/news-room/feature-stories/detail/access-to-treatment-and-care-for-all--the-path-to-eliminate-hepatitis-c-in-egypt.
- Ahmed Hassanin, “Egypt’s Ambitious Strategy to Eliminate Hepatitis C Virus: A Case Study - PMC.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8087425/.
- Ammal M. Metwally, ..., “Accelerating Hepatitis C virus elimination in Egypt by 2030: A national survey of communication for behavioral development as a modelling study - PMC.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7901784/.
- K. H. Ismail and D. E. L.-P. Iii, “The need to re-invigorate initiatives against Hepatitis C in Egypt,” Popul. Med., vol. 5, no. February, pp. 1–2, Feb. 2023. [CrossRef]
- Mohamed Hassany, Wael Abdel-Razek, and Mohamed AbdAllah, “WHO awards Egypt with gold tier status on the path to eliminate hepatitis C - The Lancet Gastroenterology & Hepatology.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.thelancet.com/journals/langas/article/PIIS2468-1253(23)00364-3/fulltext. [CrossRef]
- Mario J. Azevedo, “The State of Health System(s) in Africa: Challenges and Opportunities - PMC.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7123888/.
- S. E. Schröeder et al., “Innovative strategies for the elimination of viral hepatitis at a national level: A country case series,” Liver Int., vol. 39, no. 10, pp. 1818–1836, Oct. 2019. [CrossRef]
- Mohamed A. Daw, 1 , * Abdallah El-Bouzedi, 2 Mohamed O. Ahmed, 3 Aghnyia A. Dau, 4 and Mohamed M. Agnan 5, “Hepatitis C Virus in North Africa: An Emerging Threat - PMC.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5004010/.
- WHO, “WHO releases first-ever global guidance for country validation of viral hepatitis B and C elimination.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.who.int/news/item/25-06-2021-who-releases-first-ever-global-guidance-for-country-validation-of-viral-hepatitis-b-and-c-elimination.
- WHO, “Manual for the development and assessment of national viral hepatitis plans.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.who.int/publications/i/item/9789241509350.
- Raad et al., “Challenge of hepatitis C in Egypt and hepatitis B in Mauritania,” World J. Hepatol., vol. 10, pp. 549–557, Sep. 2018. [CrossRef]
- “The Opportunity to Eliminate Hepatitis C through Alternative Financing Mechanisms.” Accessed: Jan. 17, 2024. [Online]. Available: https://endhep2030.org/wp-content/uploads/2022/06/Policy-Brief_HCV.pdf.
- Felix Klein, “100 Million Seha: Egypt’s War against Hepatitis C,” PharmaBoardroom. Accessed: Jan. 17, 2024. [Online]. Available: https://pharmaboardroom.com/articles/100-million-seha-egypts-war-against-hepatitis-c/.
- WHO, “WHO commends Egypt for its progress on the path to eliminate hepatitis C.” Accessed: Jan. 17, 2024. [Online]. Available: https://assumption-prod.modolabs.net/parents__families/au_news/detail?feed=wr_crisis_response_who_news&id=7a0bad49-4b30-55eb-be91-6f9af408d33c&_kgoui_bookmark=f0f0ee60-484b-5273-9b0d-3c0e7b37a3fa.
- WHO, “Egypt becomes the first country to achieve WHO validation on the path to elimination of hepatitis C,” World Health Organization - Regional Office for the Eastern Mediterranean. Accessed: Jan. 17, 2024. [Online]. Available: http://www.emro.who.int/media/news/egypt-becomes-the-first-country-to-achieve-who-validation-on-the-path-to-elimination-of-hepatitis-c.html.
- James Jordano, Nina Curkovic, Sachin Aggarwal, and Kasey Hutcheson, “(PDF) Hepatitis C Treatment for Patients Without Insurance in a Student-Run Free Clinic: Analysis of Demographics, Cost, and Outcomes.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.researchgate.net/publication/374954336_Hepatitis_C_Treatment_for_Patients_Without_Insurance_in_a_Student-Run_Free_Clinic_Analysis_of_Demographics_Cost_and_Outcomes.
- Margaret Hellard,1,2,3,4 Sophia E. Schroeder,1,2 Alisa Pedrana, “The Elimination of Hepatitis C as a Public Health Threat - PMC.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7117951/.
- Elbahrawy, M. K. Ibrahim, A. Eliwa, M. Alboraie, A. Madian, and H. H. Aly, “Current situation of viral hepatitis in Egypt,” Microbiol. Immunol., vol. 65, no. 9, pp. 352–372, 2021. [CrossRef]
- T. Deress, Y. Million, T. Belachew, M. Jemal, and M. Girma, “Seroprevalence of Hepatitis C Viral Infection in Ethiopia: A Systematic Review and Meta-Analysis,” Sci. World J., vol. 2021, p. e8873389, Apr. 2021. [CrossRef]
- “Prevalence of Hepatitis B and Hepatitis C in Migrants from Sub-Saharan Africa Before Onward Dispersal Toward Europe | Journal of Immigrant and Minority Health.” Accessed: Jan. 17, 2024. [Online]. Available:. [CrossRef]
- WHO, “Prevention and Control of Viral Hepatitis Infection: Framework for Global Action.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.who.int/publications-detail-redirect/prevention-and-control-of-viral-hepatitis-infection-framework-for-global-action.
- “Viral hepatitis in resource-limited countries and access to antiviral therapies: current and future challenges | Future Virology.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.futuremedicine.com/doi/10.2217/fvl.13.11. [CrossRef]
- “The Art and Science of Eliminating Hepatitis: Egypt’s Experience.” Accessed: Jan. 17, 2024. [Online]. Available: https://www3.weforum.org/docs/WEF_The_Art_and_Science_of_Eliminating_Hepatitis_Egypt's_Experience_2022.pdf.
- Petruzziello, S. Marigliano, G. Loquercio, A. Cozzolino, and C. Cacciapuoti, “Global epidemiology of hepatitis C virus infection: An up-date of the distribution and circulation of hepatitis C virus genotypes,” World J. Gastroenterol., vol. 22, no. 34, pp. 7824–7840, Sep. 2016. [CrossRef]
- ministry of health malaysia, “National Institutes of Health - NIH Official Portal.” Accessed: Jan. 17, 2024. [Online]. Available: https://nih.gov.my/.
- Andrea L. Cox, Manal H. El-Sayed, Jia-Horng Kao, Jeffrey V. Lazarus, Maud Lemoine, Anna S. Lok & Fabien Zoulim, “Progress towards elimination goals for viral hepatitis | Nature Reviews Gastroenterology & Hepatology.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.nature.com/articles/s41575-020-0332-6.
- S. Ha and K. Timmerman, “Awareness and knowledge of hepatitis C among health care providers and the public: A scoping review,” Can. Commun. Dis. Rep., vol. 44, no. 7–8, pp. 157–165, Jul. 2018. [CrossRef]
- T. Li, R. Wang, Y. Zhao, S. Su, and H. Zeng, “Public awareness and influencing factors regarding hepatitis B and hepatitis C in Chongqing municipality and Chengdu City, China: a cross-sectional study with community residents,” BMJ Open, vol. 11, no. 8, p. e045630, Aug. 2021. [CrossRef]
- WHO, “Consolidated strategic information guidelines for viral hepatitis planning and tracking progress towards elimination: guidelines.” Accessed: Jan. 17, 2024. [Online]. Available: https://www.who.int/publications-detail-redirect/9789241515191.
- I. of M. (US) C. on the P. and C. of V. H. Infection, H. M. Colvin, and A. E. Mitchell, “Knowledge and Awareness About Chronic Hepatitis B and Hepatitis C,” in Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C, National Academies Press (US), 2010. Accessed: Jan. 17, 2024. [Online]. Available: https://www.ncbi.nlm.nih.gov/books/NBK220038/.
Figure 1.
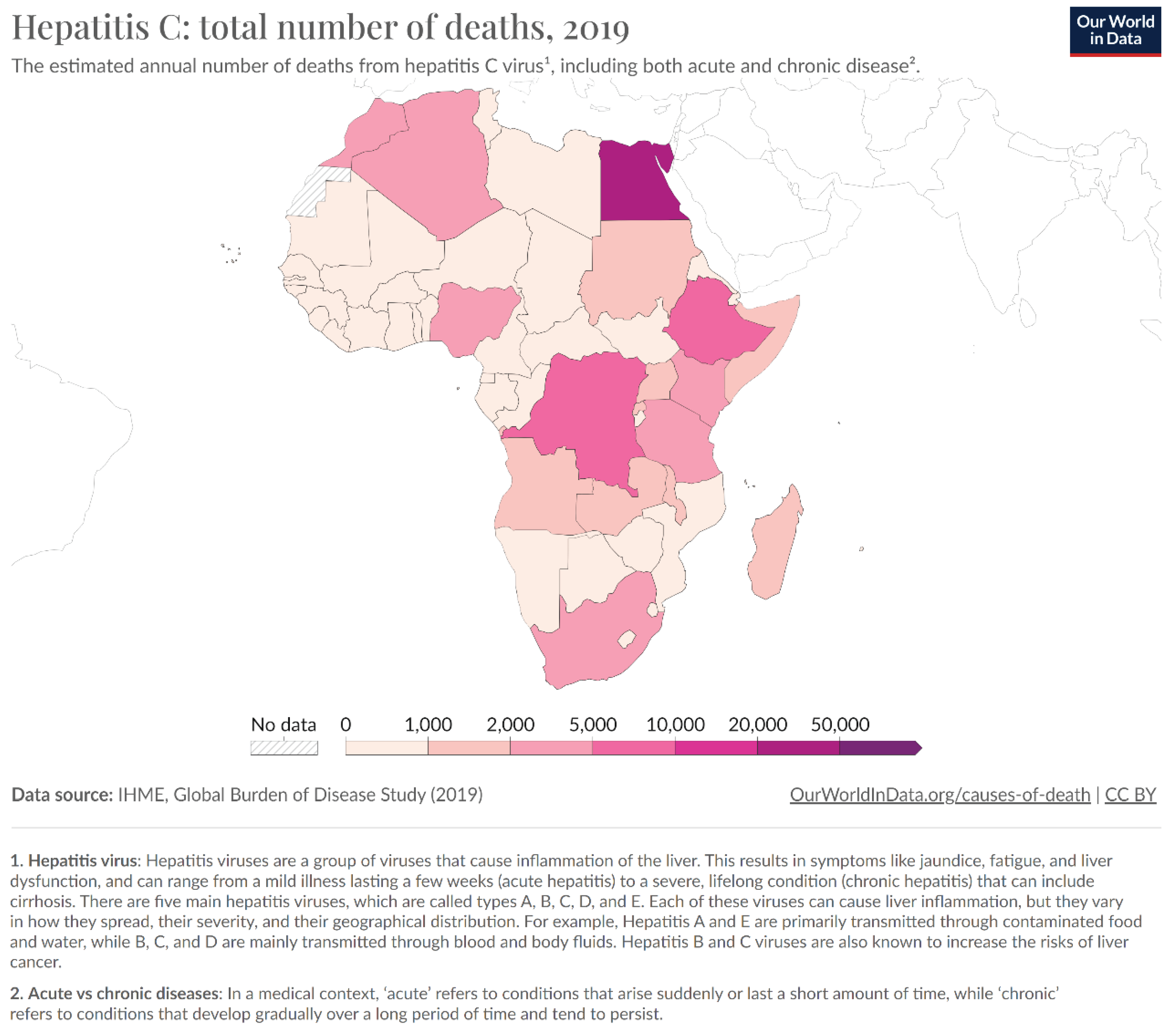

Table 1.
Impact and coverage indicators, targets, and milestones for viral hepatitis by 2030.
| Indicator | Baseline- 2020 | Targets-2025 | Targets-2030 | |
| Impact | Hepatitis B surface antigen (HBsAg) prevalence among children younger than 5 years old | 0.94% | 0.5% | 0.1% |
| Number of new hepatitis B infections per year | 1.5 million new cases 20 per 100 000 | 850 000 new cases 11 per 100 000 | 170 000 new cases 2 per 100 000 | |
| Number of new hepatitis C infections per year | 1.575 million new cases 20 per 100 000 | 1 million new cases 13 per 100 000 | 350 000 new cases 5 per 100 000 | |
| Number of new hepatitis C infections per year among people who inject drugs per year | 8 per 100 | 3 per 100 | 2 per 100 | |
| Number of people dying from hepatitis B per year | 820 000 deaths 10 per 100 000 | 530 000 deaths 7 per 100 000 | 310 000 deaths 4 per 100 000 | |
| Number of people dying from hepatitis C per year | 290 000 deaths 5 per 100 000 | 240 000 deaths 3 per 100 000 | 140 000 deaths 2 per 100 000 | |
| Coverage | Hepatitis B – percentage of people living with hepatitis B diagnosed / and treated | 30%/30% | 60%/50% | 90%/80% |
| Hepatitis C – percentage of people living with hepatitis C diagnosed / and cured | 30%/30% | 60%/50% | 90%/80% | |
| Percentage of newborns who have benefitted from a timely birth dose of hepatitis vaccine and from other interventions to prevent the vertical (mother-to-child) transmission of hepatitis B virus | 50% | 70% | 90% | |
| Hepatitis B vaccine coverage among children (third dose) | 90% | 90% | 90% | |
| Number of needles and syringes distributed per person who injects drugs | 200 | 200 | 300 | |
| Blood safety - proportion of blood units screened for bloodborne diseases | 95% | 100% | 100% | |
| Safe injections - proportion of safe health-care injections | 95% | 100% | 100% | |
| Milestones | Planning – number of countries with costed hepatitis elimination plans | TBD | 30 | 50 |
| Surveillance - number of countries reporting burden and cascade annually | 130 | 150 | 170 | |
| Hepatitis C virus drug access – percentage average reduction in prices (to equivalent generic prices by 2025) | 20% | 50% | 60% | |
| Hepatitis B virus drug access - percentage average reduction in average prices (alignment with HIV drug prices by 2025) | 20% | 50% | 60% | |
| Elimination of vertical (mother-to-child) transmission - number of countries validated for the elimination of vertical transmission of either HIV, hepatitis B, or syphilis | 15 | 50 | 100 | |
| Elimination - number of countries validated for elimination of hepatitis C and/or hepatitis B | 0 | 5 | 20 | |
| Integration - proportion of people living with HIV tested for/and cured from hepatitis C | TBD | 60%/50% | 90%/80% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



