Submitted:
25 February 2024
Posted:
07 March 2024
You are already at the latest version
Abstract
Mediterranean Diet (MD), rich in minimally processed plant foods and in monounsaturated fats, but low in saturated fats, meat and dairy products, represents one of the most studied diets for cardiovascular health. It has been shown, from both observational and randomized controlled trials, that MD reduces body weight, improves cardiovascular disease surrogates such as waist-to-hip ratio, lipids, and inflammation markers, and even prevents the development of fatal and non-fatal cardiovascular disease, diabetes, obesity, and other diseases. However, it is unclear whether it offers cardiovascular benefits from its individual components or as a whole. Furthermore, limitations in the methodology of studies and meta-analyses have raised some concerns on its potential cardiovascular benefits.
MD is also associated with characteristic changes in the intestinal microbiota, mediated through its constituents. These include increased growth of species producing short-chain fatty acids, such as Clostridium leptum and Eubacterium rectale, increased growth of Bifidobacteria, Bacteroides and Faecalibacterium prausnitzii species, and reduced growth of Firmicutes and Blautia species. Such changes are known to be favorably associated with inflammation, oxidative status, and overall metabolic health.
This review will focus on the effects of MD on cardiovascular health through its action on gut microbioma.
Keywords:
Western-type diet
; Mediterranean-type diet
; gut microbiota
; short-chain fatty acid
; trimethylamine N-oxide
; bile acids
; cardiovascular disease
; atherosclerosis
; nutrients
1. Introduction
Numerous studies spanning several decades have demonstrated that adherence to the Mediterranean diet (MD) is associated with a reduced risk of cardiovascular disease, cancer, and enhanced cognitive health. Broadly speaking, the MD represents the customary dietary pattern of populations residing along the Mediterranean Sea coast. Nevertheless, variations exist among the diets of the Mediterranean coastal countries, with the consistent element being the consumption of virgin olive oil.
Ancel Keys initially characterized the MD during the 1960s as a diet low in saturated fat and rich in vegetable oils, predominantly observed in regions like Greece and Southern Italy.
The definitions encompass specific guidelines emphasizing a high consumption of extra virgin (cold-pressed) olive oil, vegetables, including leafy greens, fruits, cereals, nuts, and legumes, along with moderate intakes of fish, meats, dairy products, and red wine. Conversely, the MD encourages limited consumption of eggs and sweets. Each description provides recommendations regarding the frequency of consumption, such as “often,” “daily,” or “biweekly,” and offers subjective terms like “abundance,” “high,” “moderate,” “low,” “some,” and “vast” to indicate the quantities of these foods within the diet. Most descriptions do not provide specific numerical servings or serving sizes and do not specify the quantities of dietary additives, such as sauces, condiments, tea, coffee, salt, sugar, or honey. Some definitions do emphasize the consumption of predominantly wholegrain cereals [1].
In general, the traditional Mediterranean diet (MD) is characterized by: (a) Elevated consumption of vegetables, fruits, cereals, legumes, nuts, and olive oil. (b) Moderate to substantial fish intake. (c) Reduced consumption of red meats and meat derivatives. (d) Moderate consumption of poultry and dairy products. (e) Moderate alcohol intake, typically in the guise of red wine [2]. Surprisingly, the exact mechanisms of action are not yet fully understood and various hypotheses have been proposed to explain the potential beneficial effects of the MedDiet. Among these, a presumed link between the MedDiet and the intestinal microbiota was put forward no more than a few years ago; this idea is therefore considered relatively new.
two human studies have now made progress towards better understanding the role of the gut microbiota and the MedDiet in disease risk factors [3] studied healthy overweight or obese subjects with sedentary lifestyles who habitually consumed small amounts of fruits and vegetables during an 8-week follow-up.6 In Among the different food products offered to the MedDiet group there were less meat and refined grain products and more fish, fruit, vegetables, legumes and whole grains, as well as a daily portion of nuts. Therefore, this diet doubled the total amount of fiber, increased the ratio of plant to animal protein by 2.5 times, and included fewer saturated fatty acids and more polyunsaturated fatty acids.
Metabolomic analyzes of stool, urine, and blood revealed a clear change after MedDiet implementation, and this change was characterized by significant changes in several metabolomic biomarkers (e.g., higher urolithins, tryptophan betaine, and oxindole acid). lower 3-acetic and carnitine, p-cresol and indoxyl sulphate) considered presumed signs of adherence to the MedDiet. In addition to the metabolome, the authors found specific changes in the composition of the gut microbiota, such as a higher abundance of Faecalibacterium prausnitzii and Roseburia and a lower abundance of Ruminococcus gnavus and R. torques. Interestingly, the change in insulin resistance was linked to specific bacteria, and subjects who reduced their index of insulin resistance had higher baseline levels of Bacteroides uniformis and B. vulgatus and lower levels of Prevotella covers [4]. The authors reported how that the higher adherence to the MedDiet led to a greater abundance of diverse taxa that are positively associated changes in the composition of the gut microbiota. According to the authors, this is mainly due to the intake of fibre, some vitamins (C, B6, B9) and various minerals. In contrast, in the control group, the changes were mostly related to a greater increase in total fat intake. Although at baseline there were already some differences in the composition of the gut microbiota between countries (mainly related to local dietary habits), the diversity was similar and adherence to the MedDiet was associated with an attenuated loss of microbiome diversity. Seventy-five operational taxonomic units (OTUs) provided high predictive performance for identifying microbiome response to the MedDiet. Furthermore, 44 OTUs showed a positive association with diet adherence, i.e., they had a higher abundance when the MedDiet was strictly observed, while 45 OTUs were negatively associated with diet adherence. The authors called these OTUs “diet positive” or “diet negative”. Diet-positive OTUs included F. prausnitzii, Eubacterium rectale, Roseburia, Bacteroides thetaiotaomicron, P. Copri, and Anaerostipes hadrus. Diet-negative OTUs included R. torques, Collinsella aerofaciens, Coprococcus came, Dorea formicigenerans, Clostridium ramosum, Veillonella dispar, Flavonifractor plautii, and Actinomyces lingnae. It is important to note that these different taxa were shared between countries, reinforcing the fact that despite different baselines and specific dietary habits between countries, MedDiet drives the composition of the gut microbiota consistently.
On the light of the possible interplay between Mediterranean Diet, its components and intestinal microbioma the aim of this review will be to sintesize the possible relationship between the adherence to a Mediterranean Diet Style and the microbiota changes and its potential effects on positive modulation of cardiovascular health.
2. The Mediterranean Diet Components
The MD can be conceptually simplified through a pyramid representation. At the base of the pyramid, one finds the essential food items that should constitute the foundation of the diet, contributing the highest energy intake. As you ascend the pyramid, you encounter foods that should be consumed in moderate quantities, including those of animal origin and items rich in sugars and fats, which warrant moderation and reserved for rarely consumption for special [2].
The most important foods of the MD are [5]:
2.1. Extra-Virgin Olive Oil (EVOO)
EVOO serves as the primary source of unsaturated fatty acids and various constituents, including fat-soluble vitamins, polyphenols, chlorophylls, and phytosterols. The polyphenols found within olive oil exhibit a spectrum of beneficial properties, encompassing anti-inflammatory, antioxidant, neuroprotective, cardioprotective, anticancer, anti-obesity, anti-diabetic, antimicrobial, and antisteatotic effects. These effects are predominantly attributed to the presence of secoiridoid derivatives, notably oleuropein, oleacein, and oleocanthal, as well as simple phenolic compounds such as tyrosol and hydroxytyrosol [6]. Polyphenols may play a pivotal role in the acknowledged pharmacological attributes of the olive oil, which encompass anti-atherogenic, antihepatotoxic, hypoglycemic, anti-inflammatory, antitumoral, antiviral, analgesic, purgative, and immunomodulatory activities. Furthermore, these polyphenols contribute to safeguarding against age-related neurodegenerative conditions [7]. Hence, the quality of EVOO is contingent not only upon the levels of free fatty acids stemming from triacylglycerol degradation (acidity) but also on its polyphenol content, the compounds accountable for its flavor profile and a multitude of its health-promoting attributes [8]. Studies have indicated that hydroxytyrosol diminishes mitochondrial oxidative stress and neuroinflammation in Alzheimer’s disease (AD)-prone transgenic mice by triggering Nrf2-dependent gene expression [9] and EVOO polyphenols additionally boost Nrf-2 activation within the liver, resulting in the release of antioxidant enzymes [10]. Nrf2 is considered the principal regulator of redox homeostasis and its activation inhibits pro-inflammatory mediators like a cytokines, COX-2 and iNOS [11]. Polyphenols present in EVOO mitigate inflammation by decreasing the expression and activity of transcription factors NF-κB and AP-1. This effect is attributed to their capability to scavenge free radicals, break radical chains, and minimize the generation of reactive oxygen species (ROS) and reactive nitrogen species (RNS) [12]. Research findings have indicated that hydroxytyrosol demonstrates in vitro antimicrobial activity against several infectious agents in the gastrointestinal and respiratory tracts, including Vibrio cholerae, Vibrio parahaemolyticus, Haemophilus influenzae, Salmonella typhi, Moraxella catarrhalis, and Staphylococcus aureus. This antimicrobial effect is observed at relatively low inhibitory concentrations. Additionally, hydroxytyrosol exhibits antimicrobial properties against foodborne pathogens like Listeria monocytogenes, Yersinia enterocolitica, and Salmonella enterica [13].
2.2. Legumes, Cereals, and Nuts
The Mediterranean diet commonly incorporates legumes such as beans, lentils, and chickpeas. These legumes are frequently combined with various cereals, fish, meats, and vegetables. Similarly, seeds and nuts like hazelnuts, almonds, tree nuts, and pistachios have been integral to the diet for millennia and are consumed on a daily basis. Nuts and legumes have been traditional dietary staples in the Mediterranean region, as well as in Asia and the Americas. The primary constituents of pulses and beans are flavanols, a category of polyphenols characterized by a ketone group in their chemical structure. These flavanols are associated with the reduction of endothelial dysfunction, the lowering of cholesterol and blood pressure, and the regulation of energy metabolism [14]. On a molecular level, a substantial portion of these effects is facilitated through interactions with nitric oxide metabolism in the endothelial cells lining the blood vessels. This interaction results in the amelioration of endothelial dysfunction, leading to enhanced vasodilation and reduced blood pressure. These biomarkers collectively serve as indicators of cardiovascular disease risk, thereby substantiating the protective influence of flavanols in the prevention of chronic cardiovascular conditions [15]. The germ of whole grains harbors a polyamine known as spermidine, which has demonstrated the capacity to extend the chronological lifespan in various organisms, including flies, nematodes, rodents, and human cells. Spermidine is recognized for its inhibition of histone acetyltransferases, thereby conferring greater resistance to oxidative stress, augmenting autophagy, and significantly diminishing subclinical inflammation and the occurrence of cell necrosis during the aging process [16].
2.3. Fruits and Vegetables
The Mediterranean climate provides an ideal environment for the cultivation of numerous vegetables and fruits that constitute a significant portion of the MD. Indigenous Mediterranean vegetables encompass turnips, artichokes, lettuce, and radishes. Interactions with external regions have led to the introduction of novel varieties of fruits and vegetables. For instance, citrus fruits and eggplant were introduced from North Asia and India, while zucchini, tomatoes, potatoes, peppers, corn, and green beans were introduced to the Mediterranean region from the Americas. Epidemiological evidence demonstrates that dietary supplementation with fruits and vegetables rich in polyphenols offers benefits in both preventing and ameliorating the adverse effects of aging on neuronal communication and behavior [17].
Another prominent characteristic of the Mediterranean diet is its exceptionally elevated content of fiber, particularly insoluble fiber, with notable bioavailability. It has been demonstrated that the consumption of a high-fiber diet induces substantial alterations in the gut microbiota composition, both in rodents and humans, resulting in a reduction of Firmicutes and an increase in Bacteroidetes, notably Bacteroides acidifaciens. This shift in microbiota composition yields heightened production of short-chain fatty acids, including acetate, propionate, and butyrate. Accumulating evidence from experimental animal studies suggests that the microbial generation of these short-chain fatty acids from dietary fiber exerts suppressive effects on the development of numerous inflammatory, autoimmune, and allergic diseases [18]. In accordance with the World Cancer Research Fund (WCRF), the consumption of vegetables has been associated with a decreased risk of developing cancers affecting the oral cavity, pharynx, larynx, esophagus, and stomach. However, the available evidence regarding the impact of vegetable consumption on the risk of cancers affecting the colorectum, endometrium, ovary, lung, and nasopharynx is limited [19]. The vegetables featured in the Mediterranean diet (MD) are abundant in various chemical compounds that exhibit potential benefits in the context of diverse cancer types. These compounds include lycopene in tomatoes, organosulfur compounds in onions and garlic, capsaicin in hot peppers, indol-3-carbinol, isothiocyanates, and sulforaphane in cruciferous vegetables, monoterpenes in oranges and lemons, polyacetylenes in pumpkin and carrots, spermidine and ferulic acid in whole grains, and ginkgetin in capers. Furthermore, the presence of estrogenic molecules with low potency, such as biochanin A, formononetin, daidzein, coumestans, and genistein in beans, enables them to compete with endogenous estrogens for binding to estrogen receptors, thereby obstructing their mitogenic effects [20].
2.4. Dairy Products
Traditionally, Mediterranean countries have exhibited low consumption of milk and dairy products, yet the ample availability of land dedicated to raising goats and sheep for their meat, milk, and wool has facilitated the production of yogurt, cheese, and other fermented dairy products. Milk serves as a rich source of lacto-fermented foods, including yogurt and cheese. Lactose in milk undergoes fermentation to lactic acid through the action of lactic acid bacteria (LAB), specifically Lactobacillus delbrueckii subsp. bulgaricus and Streptococcus thermophilus. This fermentation process results in a reduction in milk pH, thus thwarting the proliferation of pathogenic microorganisms [21]. The presence of bacteria in yogurt contributes to the transient microbiota and thereby enhances the gut environment. Several studies have indicated potential benefits of yogurt in the management of type 2 diabetes. For example, a meta-analysis of randomized controlled trials evaluating the use of yogurt in type 2 diabetes management reported a reduction in complications associated with regular consumption [22]. Another well-known fermented dairy product in the Mediterranean region is cheese, including varieties such as pecorino, halloumi, brie, chevre, manchego, feta, Parmigiano Reggiano, and ricotta. Consumption of cheese in modest amounts is recommended within the MD. During the initial stages of fermentation, LAB utilize milk carbohydrates, resulting in the production of indigestible oligosaccharides. The consumption of these oligosaccharides exerts prebiotic effects and enhances the beneficial gut microbiota [23]. Furthermore, the short-chain fatty acids generated through the metabolism of oligosaccharides and resistant starch, both prevalent in the Mediterranean diet, by the gut microbiota have the capacity to induce satiety by delaying gastric emptying. This process leads to an increase in the production of gut hormones, such as glucagon-like peptide-1 and peptide-YY. Importantly, the MD, in addition to promoting weight loss, has been associated with a significant reduction in fasting glucose, C-peptide levels, and free and total testosterone levels [24].
2.5. Fish
The Mediterranean region boasts a robust fishing tradition, resulting in substantial fish consumption. Nevertheless, environmental contaminants have hindered the potential benefits of omega-3 fatty acids. Polyunsaturated fatty acids (PUFAs) encompass long-chain ω-3 PUFAs, notably eicosapentaenoic acid (EPA, 20:5n–3), and docosahexaenoic acid (DHA, 22:6n–3), primarily obtained from fish and seafood, as well as alpha-linolenic acid, derived from various plant sources. Among PUFAs, ω-3 free fatty acids elicit anti-inflammatory effects via the generation of specialized pro-resolving mediators, known as oxylipins, through oxygenated metabolites [25]. A recent report from the American Heart Association has suggested that ω-3 PUFA supplements may decrease the risk of death resulting from coronary heart disease in patients with a history of coronary heart disease. This potential benefit may be attributed to a reduction in ischemia-induced sudden cardiac death. However, the treatment did not demonstrate a reduction in the occurrence of recurrent nonfatal myocardial infarction. Furthermore, the American Heart Association recommends a daily ω-3 supplement of 1 gram for patients with cardiovascular disease. This supplementation is advocated for its potential advantages, including lowering triglyceride (TG) levels and the prevention of arrhythmias and atherosclerosis. [26].
3. ω-3 PUFA Possess Potential Antithrombotic and Anti-Platelet-Activating Factor (PAF) Effects, and There Is a Suggestion that They May Serve as Immunomodulatory Agents in the Context of COVID-19 [27]
3.1. Wine
In European Mediterranean countries, the MD is notably associated with the moderate consumption of wine during meals. Some studies have sought to identify biomarkers of polyphenol intake and specifically polyphenols derived from certain food groups, including those originating from red wine [28]. Researchers have observed that polyphenols present in the MD exert a direct influence on the process of autophagy, for instance, resveratrol, a polyphenol found in nuts, wine, and grapes, functions as an autophagy inducer [29]. The impact of resveratrol on autophagy may be elucidated by its capacity to enhance the activity of the deacetylase sirtuin 1, which subsequently regulates the activity of numerous autophagy-related proteins. Similarly, polyphenols found in virgin olive oil, such as oleocanthal and oleuropein, have been documented to promote autophagy [30]. Moreover, the connection between autophagy and atherosclerosis and cardiovascular diseases has been delineated [31], for example autophagy plays a pivotal role in the effective development and functioning of cardiomyocytes (Bravo-San Pedro). Furthermore, autophagy plays a fundamental role in regulating the inflammatory response of macrophages, potentially by constraining the activity of the inflammasome and the formation of foam cells, likely through the modulation of lipid turnover [32]
4. MD and Cardiovascular Outcomes: Clinical, Epidemiological and Intervention Studies
The concept that higher adherence to the MD was associated with a lower cardiovascular disease (CVD) incidence and mortality was first proposed in the 1950s. From then, epidemiological studies in Italy [33,34] Greece [35,36,37,38] and Spain [39,40], and even in non-Mediterranean populations [41,42,43,44,45,46,47,48,49] showed benefits from long-term adhesion to the MD. As well as, randomized controlled intervention trials, like the secondary prevention trial Lyon Diet Heart Study [50], the PREDIMED (PREvención con DIeta MEDiterránea) trial in a low-risk population [51], and others [52] reported associations with lower CVD. A recent Cochrane review update on 30 RCTs (12,461 participants), showed, in primary prevention, little or no effect of the PREDIMED intervention (advice to follow a MD plus supplemental extra-virgin olive oil or tree nuts) compared to a low-fat diet on CVD mortality (hazard ratio (HR) 0.81, 95% confidence interval (CI) 0.50-1.32) or total mortality (HR 1.0, 95%CI 0.81-1.24) over 4.8 years. There was, however, a reduction in the number of strokes (HR 0.60, 95%CI 0.45-0.80). For secondary prevention, in the Lyon Diet Heart Study there was low-quality evidence of a reduction in adjusted estimates for CVD mortality (HR 0.35, 95%CI 0.15-0.82) and total mortality (HR 0.44, 95%CI 0.21-0.92) [53].
Systematic reviews [54,55,56,57], metanalysis [58,59,60,61] and umbrella reviews [62] confirmed the beneficial effects of traditional MD on cardiovascular health, albeit a moderate-high degree of inconsistency. This inverse association includes coronary heart disease (CHD), peripheral artery disease, chronic heart failure, sudden cardiac death, and ischemic stroke, but apparently not hemorrhagic stroke [38,60].
Despite the relatively large number of studies, there is still some uncertainty regarding the effects of a Mediterranean-style diet on clinical endpoints and cardiovascular disease (CVD) risk factors for both primary and secondary prevention. These different effects might depend on the definition of MD, with wide variety of dietary (i.e., MedDietScore.) and adherence (i.e., PREDIMED test) indices. There are also challenges with isolating the MD from the typical Mediterranean lifestyle and culture (including prolonged ‘social’ meals and siestas).
5. Favorable Mechanisms of MD on Cardiovascular Health
The exact biologic mechanism by which an increased adherence to the traditional MD exerts its beneficial effects on cardiovascular health is not known. However, accumulating evidence indicates that the most important adaptations induced by the MD pattern, high in antioxidants, micronutrients, flavonoids, nitrate, calcium, proteins, polyphenols, carotenoids, vitamins, and fibre, but low in saturated/trans-fat and sodium, are:
favorable effects on multiple specific cardiovascular risk factors [63,64] through a specific plasma metabolomic profile (mainly triglycerides and medium/long-chain acylcarnitines, aminoacids, and steroids). MD improves insulin resistance, increases adiponectin concentrations [65] and decrease the hepatic fat content [66] with beneficial effects on diabetes mellitus and metabolic syndrome [67,68]. Lipid profile improves, too, with a decrease in plasma cholesterol [3], oxidized low-density lipoprotein [65,69], LDL-cholesterol, ApoB, and ApoB/ApoA-I ratio, and an increase in ApoA-I [70,71]. There are also putative favorable changes in the blood fatty acid profile, with increased levels of eicosapentaenoic and docosahexaenoic acid [72]. Then, both systolic and diastolic blood pressure decrease [71]. Finally, MD-style may influence the potential negative relationship between elevated plasma ceramide concentrations and CVD [73];
modulating actions on sympathetic nervous system, reducing average heart rate [74] and heart rate variability, a measure of cardiac autonomic dysfunction [75];
protection against oxidative stress and inflammation. MD is associated with lower concentrations of inflammatory mediators, like C-reactive protein, interleukin-6, sICAM, P-selectin and Tumor Necrosis Factor-α [71], hallmarks of inflammaging, the peculiar low-grade, chronic, and “sterile” inflammatory state characterizing old age, that represents a background pathogenetic mechanism linking metabolic risk factors to increased risk of chronic degenerative diseases [73,76,77]. MD modulates the immune system, induces induction of detoxification enzymes [78], has a low Dietary Inflammatory Index [79], and is associated with lower intracellular reactive oxygen species production [80], an increase in serum markers of atheroma plaque stability, and a reduction in CD40 expression on monocyte surface [71]. Flavonoids, in particular, provide a variety of nutraceutical functions including antioxidant, antimicrobial, anti-inflammatory, antiangiogenic, antitumor, and improved pharmacokinetic properties [81]. MD was also significantly associated with lower levels of subclinical gut inflammation, defined by fecal calprotectin [82] and higher concentrations of faecal short-chain acids (FSCAs) (propionate and butyrate) [83];
antiatherosclerotic effects. Increase in endothelial progenitor cells [80,84] and endothelial-mediated nitric oxide (NO) synthesis leads to higher NO bioavailability [77,85] and consequent significant improvements in endothelial function [64], flow-mediated microvascular vasodilation [86,87] and arterial stiffness [88,89], as well as carotid intima-media thickness [90];
decrease in platelet aggregation and blood coagulation [65];
inhibition of nutrient sensing pathways by specific aminoacid restriction [91];
and, last, but not least, gut microbiota-mediated production of beneficial metabolites [92].
6. Microbiota: Definitions and Functions
The surfaces of the human body are heavily populated by a highly diverse collection of bacteria, fungi, archaea, viruses, and protozoa, termed the microbiota. The largest and richest site is the gut (small and, mainly, large intestine), that harbors >100 trillion microbial cells [93]. The microbiota, and their genes, called the microbiome, has been studied intensely through the past years using novel metagenomics, metatranscriptomics, and metabolomics approaches [73]. Fecal microbiota composition and diversity may be evaluated by three methods: living organisms are determined using bacterial cultures, total DNA taxonomic composition is estimated by next generation sequencing of rRNA gene and quantitative assessment of several taxa is performed using specific quantitative polymerase chain reaction (qPCR) [94]. Landmark microbiome–host genome-wide association studies have identified many SNPs associated with gut microbiota [95]. We distinguish α-diversity (eg, number of microbes) and β-diversity (eg, type and abundance of microbes) [96]. Bacterial DNA sequence found in healthy blood belongs mainly to the Firmicutes, Bacteroidetes, Proteobacteria, and Actinobacteria phyla.
This microbial ecosystem, co-evolved with humans across the millennia, is for the most part interactively co-dependent, both on one another and on their host, and capable of contributing to and reacting to circulating signaling molecules [97]. Microbes in the gut produce a wealth of low molecular weight metabolites (metabolome), including trimethylamine N-oxide (TMAO), SCFAs, secondary bile acid and indoxyl sulfate, from the exogenous dietary substances or endogenous metabolic compounds. These microbial-derived metabolites are the major factors in the host-microbiota cross-talk by activation of numerous complex signalling pathways [98], such as nuclear factor kappa-light-chain-enhancer of activated B cells, Bcl-2 interacting protein 3, NLR Family Pyrin Domain Containing inflammasome, and Proteinkinase RNA-like endoplasmic reticulum kinase [99], linked also to numerous types of programmed cell death, including apoptosis, autophagy, pyroptosis, ferroptosis, and clockophagy [100].
The view of humans as holobionts consisting of eukaryotic host cells and associated prokaryotic organisms, has opened up a new perspective on cardiovascular pathophysiology leading to the Human Microbiome Project commencement [101]. The number of bacterial genes encoded within the human gut vastly outnumber the total complement of genes in Homo sapiens, endowing the gut microbiome with enormous potential for production of functionally active metabolites [102]. Microbiota-derived metabolites, such as SCFAs, primary and secondary bile acids (Bas), TMAO, lipopolysaccharides (LPS), uremic toxins, phenylacetylglutamine (PAGln), branched chain aminoacids (BCAA), intestinal fatty acid binding protein (I-FABP), zonulin, and sphingomyelins, which are adsorbed in the intestine and distributed via the circulation, can exert beneficial or detrimental effects on various extraintestinal organs, including the brain, liver, and heart [11,103,104,105,106].
This virtually endocrine ‘organ’ plays an important role in the function of the gastrointestinal tract and in the human physiology, protecting from pathogen colonization through maintenance of gut barrier function, and participating in digestion, energy harvest from food sources indigestible by humans, vitamin synthesis, functions of the immune system, facilitation of biotransformation of drugs as statins and antihypertensives, regulation of brain function and behavior, as well as endocrine and glucose homeostasis and lipid and bile acid metabolism [73,98,107,108,109,110]. The importance of the gut-brain axis in regulating stress related responses and anxiety disordes by influencing, in particular, tryptophan metabolism through the kynurenine pathway, and consequently serotoninergic system, has long been appreciated [111].
Table 1 summarizes main components of microbiome associated with cardiovascular diseases.
7. Western Diet, Microbiome, and Cardiovascular Diseases
The gut microbiota functions as an endocrine organ that participate in the maintenance of cardiovascular homeostasis, and their dysfunction can directly influence the progression of cardiovascular disease [112] via abnormally activating signaling pathways, more swiftly when the gut barrier integrity is broken down (theory of “gut-heart axis”) [113].
Some microbial components are more represented in in the blood, fecal and plaque samples of patients with cardiovascular risk factors or disease [3,94,95,114,115,116,117,118,119,120].
Host diet is one of the most significant modulators of the gut microbial community in humans as well as in experimental animal models [73]. Bacterial metabolites are produced from food components, which in turn emphasizes the importance of nutrition. Evidence demonstrates that dietary habits such as the ‘Western diet’ model are related to perturbations in gut microbiome composition and function (called dysbiosis), with a significant decrease in Bacteroidetes and an increase in Firmicutes, Escherichia, Shigella, and Enterococcus, strongly associated with a wide range of human diseases, including celiac disease, inflammatory bowel disease, colorectal cancer, depression, anxiety, neurological disorders, rheumatoid arthritis, systemic lupus erythematous, asthma, allergies, insulin resistance, non-alcoholic fatty liver disease, chronic kidney disease, obesity, metabolic syndrome, arterial hypertension, type-2 diabetes and CVD [98,111,121,122,123,124,125,126,127,128,129,130,131]. Western diet can lead to increased permeability of the gut mucosa, known as “leaky gut,” resulting in endotoxemia and bacterial translocation [132]. In turn, gut dysbiosis and impaired intestinal permeability can alter gut bacterial metabolite signaling profile from the gut to the brain and heart [103,111].
Apart from diet, other conditions are associated with dysbiosis, eg antibiotics abuse. In older age groups, there is an increase in microorganisms secreting endotoxins, LPS and TMAO. Also several pathological conditions in the gastrointestinal tract may impair the intestinal barrier allowing translocation of bacteria and their metabolites.
The mechanisms linking gut microbiota to CVD are multifaceted and not yet fully understood, and may include direct effects of microbial metabolites on atherosclerosis and thrombosis development, as well as immune dysregulation and disturbance of neuro-enteroendocrine hormones by bacteria and their products [102,122,125]. Borton et al. assigned an atherosclerotic profile to the 6,341 microbial genomes that encoded metabolisms associated with heart disease, creating the open-access resource Methylated Amine Gene Inventory of Catabolism database (MAGICdb) [133].
One of the most-cited examples of the gut microbiome modulating human disease is the microbial metabolism of quaternary amines from protein-rich foods. Some species of the microbiota influence the metabolism of specific food components abundant in high-fat diets (such as carnitine, choline, betaine, phosphatidyl-choline), synthesizing through lyase enzymes (catalytic protein cutC), trimethylamine (TMA) (humans lack this ability), that enters the liver through the portal vein circulation and is oxidised by the hepatic flavin-containing mono-oxygenase family to TMAO, a molecule with documented harmful activity on atherosclerosis and thrombosis in vitro and in vivo (it damages vascular endothelium and promotes activation of macrophages and platelets and thrombus formation) [73,101,103,109,134,135,136,137,138,139,140]. There was no direct association of plasma TMAO and the extent of atherosclerosis, both in mice and humans. However, TMAO plasma levels are associated with atherosclerotic plaque instability [141]. Associations with diabetes mellitus and obesity suggest that TMAO might have a functional role in metabolic syndrome [142]. In a community-based cohort of older US adults, after multivariable adjustment, higher levels of TMAO were associated with a higher risk of incident ASCVD (HR 1.21 (95%CI, 1.02–1.42; P-trend=0.029) [143]. In PEGASUS-TIMI 54, higher TMAO quartiles were associated with risk of MACE (OR 1.43, 95%CI, 1.06–1.93, P=0.015) [144]. In patients with chronic heart failure after myocardial infarction, TMAO was a significant, independent predictor of MACE (HR 2.31, 95%CI 1.42–3.59, P < 0.01) and all-cause mortality (HR 2.15, 95%CI 1.37–3.24, P < 0.01) [145]. In a metanalysis, higher plasma TMAO level was associated with greater risks of MACEs (TMAO tertile 3 v tertile 1: HR, 1.68; 95%CI, 1.44-1.96) and of all-cause mortality (TMAO tertile 3 v tertile 1: HR, 1.67; 95%CI, 1.17-2.38) [146]. In another meta-analysis, high TMAO was positively associated with all-cause mortality (HR 1.38 [95%CI 1.306–1.460]) as well as adverse cardiovascular events (HR: 1.032 [95%CI: 1.014–1.051]) [147].
There are obviously many other candidate mechanisms. Immune cells such as T cells, B cells, and macrophages are extensively infiltrated in the gut and heart tissues and play a crucial role in the crosstalk between the heart and gut microbiota [104,148]. Studies of germ-free mice have provided evidence that microbiota diversity and the presence of a specific microbe in the gut can affect immune cells in hosts [149]. Lower cholesterol-degrading bacteria were considerably reduced in myocardial infarct ion [114]. Dysbiosis with decreased abundance of microbes with capacity for producing butyrate, like chronic stress, decreases SCFAs and bile acids, raising intestinal permeability [96,136,150]. In diets high in saturated fat and low in fiber, enhanced absorption of bacterial fragments and bacterial fermentation end products, such as LPS, promotes the onset of “metabolic endotoxemia,” defined as a 2- to 3-fold increase in circulating levels of bacterial endotoxin which could activate toll-like receptors, mediating a chronic, low grade inflammatory response [114,131,151]. In atrial fibrillation, gut-derived LPS may contribute to MACE incidence by increasing platelet activation [152]. Additionally, gut microbiota may influence drugs and food-derived bioactive compounds metabolism. In periodontal disease the oral microbiota is translocated through the bloodstream to the liver and intestine, generating intestinal dysbiosis [153]. Transfer of microbiota from obese animals induces metabolic disease and obesity in germ-free animals. Conversely, transfer of pathogen-free microbiota from lean healthy human donors to patients with metabolic disease can increase insulin sensitivity [128].
In heart failure (HF), current evidence has found links with alterations in microbial composition and function, associated with impaired intestinal barrier function, generation of uremic toxins, and bacterial translocation leading to inflammatory and immune responses [154,155]. Intestinal leakage, caused by haemodynamic changes in heart failure (congestion in the portal vein, drop in cardiac output, reduction in intestinal perfusion) induce in turn alteration in gut microbiota composition and systemic inflammation through microbial or endotoxin translocation into systemic circulation (“gut hypothesis” of HF) [93,109,136,140,156]. Circulating TMAO levels are associated with adverse outcomes in HF [101,157]. Another effect of alteration in microbiota composition reflects in the up-regulation of cotransporters (NHE3) with consequent salt and fluid overload [158].
Figure 1 summarizes some hypothesized pathways connecting western diet, microbiome, and CVD.
8. Effects of Mediterreanen Diet on Microbiome
Although RCTs and observational studies provided no clear evidence of a consistent effect of a MD on composition or metabolism of the gut microbiota [159], the consumption of a Mediterranean type diet is associated with a specific microbiota, characterized by a greater biodiversity (i.e., by a greater number of bacterial species identified and increase in gene richness) and by fiber-degrading ad butyrate-producing bacteria [3,68,73,82,92,126,134,160,161,162,163,164,165,166,167].
Table 2 shows the effects of MD on gut microbiota.
In summary, MD adherence is associated to an increase in the abundance of several Bacteroidetes taxa and a depletion of many Firmicutes taxa, with lower Firmicutes/Bacteroidetes ratio and higher bifidobacterial/E. coli ratio and Prevotella/Bacteroides ratio [162,164,168]. Typical components also seem to be associated with the presence of specific strains. Cereals, for example, with the presence of Bifidobacterium and Faecalibacterium, Tenericutes and Dorea with olive oil, red wine again with Faecalibacterium, vegetables with Rikenellaceae, Dorea, Alistipes, and Ruminococcus, legumes with Coprococcus [92].
9. MD, Microbiome, and Cardiovascular Health
The relationship between the gut microbiome, diet and cardiovascular diseases is complex and still not fully understood. Microbiome could represent, however, a possible intermediate of the effects of the MD on modulation of cardiovascular risk factors [73]. An interesting hypothesis suggests a bidirectional relationship between the MD and the gut microbiome, where gut microbiota assembly and biosynthetic capacity are responsive to the diet; in return, the microbiome-reachable nutrients shape and modulate the microbiome toward a characteristic probiotic state. It can be speculated that that primary health benefits of the MD are mediated by the bioactive compounds transformed by the microbiome [169].
First, adherence to MD led to a higher abundance of different taxa that are negatively correlated with markers of inflammation. This diet pattern positively affects the diversity and activity of various gut bacteria with saccharolytic activity (eg Bacteroides acidifaciens, Firmicutes, Faecalibacterium prausnitzii, Prevotella, clostridium cluster XIVa, Akkermansia, Roseburia and Ruminococcus genera, and Parabacteroides distasonis), that increases SCFAs, produced during microbial fermentation of complex carbohydrates and dietary fibre, hence improving host metabolism [3,73,126,134,164,166,170,171]. SCFAs, especially butyric acid, but also acetate and propionate, possess immunomodulatory and antiinflammatory properties (reducing some cytokines such as VEGF, MCP-1, IL-17, IP-10 and IL-12) and improve host metabolism [73,102,106,161,163,172]. Receptors binding these metabolites, such as G-protein coupled receptors GPR41,GPR43, GPR109a, and OLF78, placed on enteroendocrine and immune cells, have been shown in animal studies to have inverse roles in blood pressure regulation, and favorably impact cardiac function [73,173].
Apart from SCFAs, MD has some other interesting cardioprotective properties. MD, and in particular fruit and legumes, is inversely related to LPS levels, linked with baseline urinary excretion of TxB2 [152]. MD increase urinary urolithins, faecal bile acid degradation and insulin sensitivity [3]. The MD is rich in polyphenols, that are extensively metabolized by the gut microbiota. Among five microbial phenolic metabolites identified, urolithin B glucuronide was inversely associated with LDL-cholesterol [174]. Some genera related to MD seem to affect the bile acid metabolism. Bile acids represent a class of cholesterol derivatives that is essential for intestinal absorption of lipids and fat-soluble vitamins, plays an important modulator role in cholesterol turnover, improvement in insulin levels and in control of immunity and heart function [68,175]. Some strains, on the other hand, produce secondary metabolites originating from molecules present in food (such as enterodiol, which derives from lignin), characterized by a vascular protection activity [134]. Finally, the Mediterranean diet pattern, rich in unsaturated fats and fiber, may be one dietary strategy to reduce metabolic endotoxemia-microbiome derived.
Preclinical studies have demonstrated the differential effects of MD on the microbiota and metabolic health [176]. A systematic review of animal studies shows that MD-like diets rich in polyphenols fiber modified the gut microbiota composition and increased microbial metabolites’ activities, leading to an improvement in HF outcomes, such as a reduction in systolic blood pressure, cardiac hypertrophy, and left ventricular thickness [139].
However, human studies are lacking. MD adherence results in a better glycemic control in subjects with T2D. Bacterial richness was negatively correlated with fasting glucose levels and Homeostatic Model Assessment for Insulin Resistance (HOMA-IR). Fecal alkaline phosphatase activity, positively correlated with bacterial diversity, was negatively correlated with HbA1c [168].
Figure 2 summarizes some hypothesized pathways connecting MD, microbiome, and CV health.
10. Conclusions
The integration of microbiome analysis within nutrition science research will be fundamental to ensuring our full understanding of the complex and synergistic effects that foods or dietary patterns can have on human health. Intestinal microbiota is arising as a new element in the physiopathology of cardiovascular diseases. A healthy microbiota includes a balanced representation of bacteria with health promotion functions (symbiotes). It is rational to speculate that a positive modulation of the gut microbiome diversity, composition and function is one of the main factors intermediating the health effects of MD on the host. Figure 3 summarizes the complex relationship among MD, microbiome, and cardiovascular diseases.
Further research is needed to explore the specific mechanisms underlying the protective effects of this dietary pattern and to better understand the long-term effects of the MD on atherosclerosis and its associated risk factors in diverse populations, as well as the therapeutic potential of the gut-metabolite-heart axis as a novel target for the treatment of CVD. As consequence, more high-quality prospective cohorts and randomized clinical trials are warranted.
Nevertheless, promoting the adoption of the MD could be an effective strategy for mitigating the burden of CVDs globally [55]. We hope this article will draw the attention of society and the medical community to emphasize promoting healthy eating and proper eating habits in children and adults.
Author Contributions
Conceptualization, A.T.; Methodology, A.T.; Writing—Original Draft Preparation, V.A.; A.S. Writing—Review & Editing, A.T.; Visualization, G.P.; Supervision, A.T.
Funding
This research received no external funding.
Institutional Review Board Statement
n.a.
Informed Consent Statement
N.A.
Data Availability Statement
N.A.
Acknowledgments
None.
Conflicts of Interest
None.
References
- Davis C, Bryan J, Hodgson J, Murphy K. Definition of the Mediterranean Diet; A Literature Review. Nutrients. 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [PubMed]
- Bach-Faig A, Berry EM, Lairon D, et al. Mediterranean diet pyramid today. Science and cultural updates. Public. Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [PubMed]
- Meslier V, Laiola M, Roager HM, et al. Mediterranean diet intervention in overweight and obese subjects lowers plasma cholesterol and causes changes in the gut microbiome and metabolome independently of energy intake. Gut. 2020, 69, 1258–1268. [Google Scholar] [CrossRef] [PubMed]
- Ghosh TS, Rampelli S, Jeffery IB, et al. Mediterranean diet intervention alters the gut microbiome in older people reducing frailty and improving health status: the NU-AGE 1-year dietary intervention across five European countries. Gut. 2020, 69, 1218–1228. [Google Scholar] [CrossRef] [PubMed]
- Kiani AK, Medori MC, Bonetti G, et al. Modern vision of the Mediterranean diet. J. Prev. Med. Hyg. 2022, 63, 2S3:E36. [Google Scholar] [CrossRef]
- Bucciantini M, Leri M, Nardiello P, Casamenti F, Stefani M. Olive Polyphenols: Antioxidant and Anti-Inflammatory Properties. Antioxidants. 2021, 10, 1044. [Google Scholar] [CrossRef] [PubMed]
- Casamenti F, Stefani M. Olive polyphenols: new promising agents to combat aging-associated neurodegeneration. Expert. Rev. Neurother. 2017, 17, 345–358. [Google Scholar] [CrossRef]
- Barnes S, Prasain J, D’Alessandro T, et al. The metabolism and analysis of isoflavones and other dietary polyphenols in foods and biological systems. Food Funct. 2011, 2, 235. [Google Scholar] [CrossRef]
- Peng Y, Hou C, Yang Z, et al. Hydroxytyrosol mildly improve cognitive function independent of APP processing in APP/PS1 mice. Mol. Nutr. Food Res. 2016, 60, 2331–2342. [Google Scholar] [CrossRef]
- Soto-Alarcon SA, Valenzuela R, Valenzuela A, Videla LA. Liver Protective Effects of Extra Virgin Olive Oil: Interaction between Its Chemical Composition and the Cell-signaling Pathways Involved in Protection. Endocr. Metab. Immune Disord—Drug Targets. 2017, 18, 75–84. [Google Scholar] [CrossRef]
- Ahmadmehrabi S, Tang WHW. Gut microbiome and its role in cardiovascular diseases. Curr. Opin. Cardiol. 2017, 32, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Hornedo-Ortega R, Cerezo AB, De Pablos RM, et al. Phenolic Compounds Characteristic of the Mediterranean Diet in Mitigating Microglia-Mediated Neuroinflammation. Front. Cell Neurosci, 2018; 12, 373. [CrossRef]
- Naureen Z, Capodicasa N, Paolacci S, et al. Prevention of the proliferation of oral pathogens due to prolonged mask use based on α-cyclodextrin and hydroxytyrosol mouthwash. Eur. Rev. Med. Pharmacol. Sci. 2021, 25 (Suppl. S1), 74–80. [Google Scholar] [CrossRef]
- Williamson, G. The role of polyphenols in modern nutrition. Nutr. Bull. 2017, 42, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Loke WM, Hodgson JM, Proudfoot JM, McKinley AJ, Puddey IB, Croft KD. Pure dietary flavonoids quercetin and (−)-epicatechin augment nitric oxide products and reduce endothelin-1 acutely in healthy men. Am. J. Clin. Nutr. 2008, 88, 1018–1025. [Google Scholar] [CrossRef]
- Eisenberg T, Abdellatif M, Schroeder S, et al. Cardioprotection and lifespan extension by the natural polyamine spermidine. Nat. Med. 2016, 22, 1428–1438. [Google Scholar] [CrossRef] [PubMed]
- Pereira A, Maraschin M. Banana (Musa spp) from peel to pulp: Ethnopharmacology, source of bioactive compounds and its relevance for human health. J. Ethnopharmacol, 2015; 160, 149–163. [CrossRef]
- Thorburn AN, Macia L, Mackay CR. Diet, Metabolites, and “Western-Lifestyle” Inflammatory Diseases. Immunity. 2014, 40, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Clinton SK, Giovannucci EL, Hursting SD. The World Cancer Research Fund/American Institute for Cancer Research Third Expert Report on Diet, Nutrition, Physical Activity, and Cancer: Impact and Future Directions. J. Nutr. 2020, 150, 663–671. [Google Scholar] [CrossRef]
- Surh, Y.J. Cancer chemoprevention with dietary phytochemicals. Nat. Rev. Cancer. 2003, 3, 768–780. [Google Scholar] [CrossRef]
- Şanlier N, Gökcen BB, Sezgin AC. Health benefits of fermented foods. Crit. Rev. Food Sci. Nutr. 2019, 59, 506–527. [Google Scholar] [CrossRef]
- Barengolts E, Smith E, Reutrakul S, Tonucci L, Anothaisintawee T. The Effect of Probiotic Yogurt on Glycemic Control in Type 2 Diabetes or Obesity: A Meta-Analysis of Nine Randomized Controlled Trials. Nutrients. 2019, 11, 671. [Google Scholar] [CrossRef]
- Oliveira DL, Costabile A, Wilbey RA, Grandison AS, Duarte LC, Roseiro LB. In vitro evaluation of the fermentation properties and potential prebiotic activity of caprine cheese whey oligosaccharides in batch culture systems. BioFactors. 2012, 38, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Cani P, Delzenne N. The Role of the Gut Microbiota in Energy Metabolism and Metabolic Disease. Curr. Pharm. Des. 2009, 15, 1546–1558. [Google Scholar] [CrossRef] [PubMed]
- Jiang L, Wang J, Xiong K, Xu L, Zhang B, Ma A. Intake of Fish and Marine n-3 Polyunsaturated Fatty Acids and Risk of Cardiovascular Disease Mortality: A Meta-Analysis of Prospective Cohort Studies. Nutrients. 2021, 13, 2342. [Google Scholar] [CrossRef] [PubMed]
- Siscovick DS, Barringer TA, Fretts AM, et al. Omega-3 Polyunsaturated Fatty Acid (Fish Oil) Supplementation and the Prevention of Clinical Cardiovascular Disease: A Science Advisory From the American Heart Association. Circulation, 2017; 135. [CrossRef]
- Detopoulou P, Demopoulos CA, Antonopoulou S. Micronutrients, Phytochemicals and Mediterranean Diet: A Potential Protective Role against COVID-19 through Modulation of PAF Actions and Metabolism. Nutrients. 2021, 13, 462. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Fresno R, Llorach R, Perera A, et al. Clinical phenotype clustering in cardiovascular risk patients for the identification of responsive metabotypes after red wine polyphenol intake. J. Nutr. Biochem, 2016; 28, 114–120. [CrossRef]
- Morselli E, Mariño G, Bennetzen MV, et al. Spermidine and resveratrol induce autophagy by distinct pathways converging on the acetylproteome. J. Cell Biol. 2011, 192, 615–629. [Google Scholar] [CrossRef] [PubMed]
- Corella D, Coltell O, Macian F, Ordovás JM. Advances in Understanding the Molecular Basis of the Mediterranean Diet Effect. Annu. Rev. Food Sci. Technol. 2018, 9, 227–249. [Google Scholar] [CrossRef] [PubMed]
- De Meyer GRY, Grootaert MOJ, Michiels CF, Kurdi A, Schrijvers DM, Martinet W. Autophagy in Vascular Disease. Circ. Res. 2015, 116, 468–479. [Google Scholar] [CrossRef]
- Razani B, Feng C, Coleman T, et al. Autophagy Links Inflammasomes to Atherosclerotic Progression. Cell Metab. 2012, 15, 534–544. [Google Scholar] [CrossRef]
- Cangemi R, Miglionico M, D’Amico T, et al. Adherence to the Mediterranean Diet in Preventing Major Cardiovascular Events in Patients with Ischemic Heart Disease: The EVA Study. Nutrients. 2023, 15, 3150. [Google Scholar] [CrossRef]
- Bonaccio M, Di Castelnuovo A, Pounis G, et al. High adherence to the Mediterranean diet is associated with cardiovascular protection in higher but not in lower socioeconomic groups: prospective findings from the Moli-sani study. Int. J. Epidemiol. 2017, 46, 1478–1487. [Google Scholar] [CrossRef]
- Panagiotakos DB, Chrysohoou C, Pitsavos C, et al. The association of Mediterranean diet with lower risk of acute coronary syndromes in hypertensive subjects. Int. J. Cardiol. 2002, 82, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos DB, Arapi S, Pitsavos C, et al. The relationship between adherence to the Mediterranean diet and the severity and short-term prognosis of acute coronary syndromes (ACS): The Greek Study of ACS (The GREECS). Nutrition, 2006; 22, 722–730. [CrossRef]
- Pitsavos C, Panagiotakos DB, Chrysohoou C, et al. The effect of Mediterranean diet on the risk of the development of acute coronary syndromes in hypercholesterolemic people: a case–control study (CARDIO2000). Coron. Artery Dis. 2002, 13, 295–300. [CrossRef]
- Tektonidis TG, Åkesson A, Gigante B, Wolk A, Larsson SC. A Mediterranean diet and risk of myocardial infarction, heart failure and stroke: A population-based cohort study. Atherosclerosis. 2015, 243, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González MA, García-López M, Bes-Rastrollo M, et al. Mediterranean diet and the incidence of cardiovascular disease: A Spanish cohort. Nutr Metab Cardiovasc Dis. Published online January 21, 2010:S0939475309002403. [CrossRef]
- Miró Ò, Estruch R, Martín-Sánchez FJ, et al. Adherence to Mediterranean Diet and All-Cause Mortality After an Episode of Acute Heart Failure. JACC Heart Fail. 2018, 6, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Waldeyer C, Brunner FJ, Braetz J, et al. Adherence to Mediterranean diet, high-sensitive C-reactive protein, and severity of coronary artery disease: Contemporary data from the INTERCATH cohort. Atherosclerosis, 2018; 275, 256–261. [CrossRef]
- Levitan EB, Lewis CE, Tinker LF, et al. Mediterranean and DASH Diet Scores and Mortality in Women With Heart Failure: The Women’s Health Initiative. Circ. Heart Fail. 2013, 6, 1116–1123. [Google Scholar] [CrossRef] [PubMed]
- Shikany JM, Safford MM, Bryan J, et al. Dietary Patterns and Mediterranean Diet Score and Hazard of Recurrent Coronary Heart Disease Events and All-Cause Mortality in the REGARDS Study. J. Am. Heart Assoc. 2018, 7, e008078. [Google Scholar] [CrossRef] [PubMed]
- Hodge AM, Bassett JK, Dugué PA, et al. Dietary inflammatory index or Mediterranean diet score as risk factors for total and cardiovascular mortality. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Chang CY, Lee CL, Liu WJ, Wang JS. Association of Adherence to the Mediterranean Diet with All-Cause Mortality in Subjects with Heart Failure. Nutrients. 2022, 14, 842. [Google Scholar] [CrossRef]
- Fung TT, Rexrode KM, Mantzoros CS, Manson JE, Willett WC, Hu FB. Mediterranean Diet and Incidence of and Mortality From Coronary Heart Disease and Stroke in Women. Circulation. 2009, 119, 1093–1100. [Google Scholar] [CrossRef]
- Liang KW, Lee CL, Liu WJ. Lower All-Cause Mortality for Coronary Heart or Stroke Patients Who Adhere Better to Mediterranean Diet-An NHANES Analysis. Nutrients. 2022, 14, 3203. [Google Scholar] [CrossRef]
- Tong TYN, Wareham NJ, Khaw KT, Imamura F, Forouhi NG. Prospective association of the Mediterranean diet with cardiovascular disease incidence and mortality and its population impact in a non-Mediterranean population: the EPIC-Norfolk study. BMC Med. 2016, 14, 135. [Google Scholar] [CrossRef]
- Stefler D, Malyutina S, Kubinova R, et al. Mediterranean diet score and total and cardiovascular mortality in Eastern Europe: the HAPIEE study. Eur. J. Nutr. 2017, 56, 421–429. [Google Scholar] [CrossRef]
- De Lorgeril M, Salen P, Martin JL, Monjaud I, Delaye J, Mamelle N. Mediterranean Diet, Traditional Risk Factors, and the Rate of Cardiovascular Complications After Myocardial Infarction: Final Report of the Lyon Diet Heart Study. Circulation. 1999, 99, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González MA, Fernández-Jarne E, Serrano-Martínez M, Marti A, Martinez JA, Martín-Moreno JM. Mediterranean diet and reduction in the risk of a first acute myocardial infarction: an operational healthy dietary score. Eur. J. Nutr. 2002, 41, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Lista J, Alcala-Diaz JF, Torres-Peña JD, et al. Long-term secondary prevention of cardiovascular disease with a Mediterranean diet and a low-fat diet (CORDIOPREV): a randomised controlled trial. The Lancet. 2022, 399, 1876–1885. [Google Scholar] [CrossRef] [PubMed]
- Rees K, Takeda A, Martin N, et al. Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease. Cochrane Heart Group, ed. Cochrane Database Syst. Rev, 2019; 2019. [CrossRef]
- Gupta UC, Gupta SC, Gupta SS. An Evidence Base for Heart Disease Prevention using a MediterraneanDiet Comprised Primarily of Vegetarian Food. Recent. Adv. Food Nutr. Agric. 2023, 14, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Laffond A, Rivera-Picón C, Rodríguez-Muñoz PM, et al. Mediterranean Diet for Primary and Secondary Prevention of Cardiovascular Disease and Mortality: An Updated Systematic Review. Nutrients. 2023, 15, 3356. [Google Scholar] [CrossRef]
- Saulle R, Lia L, De Giusti M. A systematic overview of the scientific literature on the association between Mediterranean Diet and the Stroke prevention. Clin. Ter, 2019; 396–408. [CrossRef]
- Liyanage T, Ninomiya T, Wang A, et al. Effects of the Mediterranean Diet on Cardiovascular Outcomes—A Systematic Review and Meta-Analysis. Wright JM, ed. PLOS ONE. 2016, 11, e0159252. [Google Scholar] [CrossRef]
- Martinez-Gonzalez MA, Bes-Rastrollo M. Dietary patterns, Mediterranean diet, and cardiovascular disease. Curr. Opin. Lipidol. 2014, 25, 20–26. [CrossRef]
- Grosso G, Marventano S, Yang J, et al. A comprehensive meta-analysis on evidence of Mediterranean diet and cardiovascular disease: Are individual components equal? Crit. Rev. Food Sci. Nutr. 2017, 57, 3218–3232. [Google Scholar] [CrossRef]
- Rosato V, Temple NJ, La Vecchia C, Castellan G, Tavani A, Guercio V. Mediterranean diet and cardiovascular disease: a systematic review and meta-analysis of observational studies. Eur. J. Nutr. 2019, 58, 173–191. [Google Scholar] [CrossRef]
- Pant A, Gribbin S, McIntyre D, et al. Primary prevention of cardiovascular disease in women with a Mediterranean diet: systematic review and meta-analysis. Heart. 2023, 109, 1208–1215. [Google Scholar] [CrossRef] [PubMed]
- Dinu M, Pagliai G, Casini A, Sofi F. Mediterranean diet and multiple health outcomes: an umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef] [PubMed]
- La Torre G, Saulle R, Di Murro F, et al. Mediterranean diet adherence and synergy with acute myocardial infarction and its determinants: A multicenter case-control study in Italy. Lazzeri C, ed. PLOS ONE. 2018, 13, e0193360. [Google Scholar] [CrossRef]
- Korakas E, Dimitriadis G, Raptis A, Lambadiari V. Dietary Composition and Cardiovascular Risk: A Mediator or a Bystander? Nutrients. 2018, 10, 1912. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González MÁ, Ruiz-Canela M, Hruby A, Liang L, Trichopoulou A, Hu FB. Intervention Trials with the Mediterranean Diet in Cardiovascular Prevention: Understanding Potential Mechanisms through Metabolomic Profiling. J. Nutr. 2016, 146, 913S–919S. [Google Scholar] [CrossRef] [PubMed]
- Gepner Y, Shelef I, Komy O, et al. The beneficial effects of Mediterranean diet over low-fat diet may be mediated by decreasing hepatic fat content. J. Hepatol. 2019, 71, 379–388. [Google Scholar] [CrossRef]
- Whayne, T.F. Ischemic Heart Disease and the Mediterranean Diet. Curr. Cardiol. Rep. 2014, 16, 491. [Google Scholar] [CrossRef]
- Galié S, García-Gavilán J, Papandreou C, et al. Effects of Mediterranean Diet on plasma metabolites and their relationship with insulin resistance and gut microbiota composition in a crossover randomized clinical trial. Clin. Nutr. 2021, 40, 3798–3806. [Google Scholar] [CrossRef]
- Fitó M, Estruch R, Salas-Salvadó J, et al. Effect of the Mediterranean diet on heart failure biomarkers: a randomized sample from the PREDIMED trial. Eur. J. Heart Fail. 2014, 16, 543–550. [Google Scholar] [CrossRef]
- Solá R, Fitó M, Estruch R, et al. Effect of a traditional Mediterranean diet on apolipoproteins B, A-I, and their ratio: A randomized, controlled trial. Atherosclerosis. 2011, 218, 174–180. [Google Scholar] [CrossRef]
- Casas R, Sacanella E, Urpí-Sardà M, et al. The Effects of the Mediterranean Diet on Biomarkers of Vascular Wall Inflammation and Plaque Vulnerability in Subjects with High Risk for Cardiovascular Disease. A Randomized Trial. Hribal ML, ed. PLoS ONE. 2014, 9, e100084. [Google Scholar] [CrossRef]
- Giroli MG, Werba JP, Risé P, et al. Effects of Mediterranean Diet or Low-Fat Diet on Blood Fatty Acids in Patients with Coronary Heart Disease. A Randomized Intervention Study. Nutrients. 2021, 13, 2389. [Google Scholar] [CrossRef] [PubMed]
- Tuttolomondo A, Simonetta I, Daidone M, Mogavero A, Ortello A, Pinto A. Metabolic and Vascular Effect of the Mediterranean Diet. Int. J. Mol. Sci. 2019, 20, 4716. [Google Scholar] [CrossRef] [PubMed]
- Carlos S, De La Fuente-Arrillaga C, Bes-Rastrollo M, et al. Mediterranean Diet and Health Outcomes in the SUN Cohort. Nutrients. 2018, 10, 439. [Google Scholar] [CrossRef] [PubMed]
- Dai J, Lampert R, Wilson PW, Goldberg J, Ziegler TR, Vaccarino V. Mediterranean Dietary Pattern Is Associated With Improved Cardiac Autonomic Function Among Middle-Aged Men: A Twin Study. Circ. Cardiovasc. Qual. Outcomes. 2010, 3, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Di Giosia P, Stamerra CA, Giorgini P, Jamialahamdi T, Butler AE, Sahebkar A. The role of nutrition in inflammaging. Ageing Res. Rev, 2022; 77, 101596. [CrossRef]
- Kerley, C.P. Dietary patterns and components to prevent and treat heart failure: a comprehensive review of human studies. Nutr. Res. Rev. 2019, 32, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Giugliano D, Esposito K. Mediterranean Diet and Cardiovascular Health. Ann. N. Y Acad. Sci. 2005, 1056, 253–260. [Google Scholar] [CrossRef]
- Itsiopoulos C, Mayr HL, Thomas CJ. The anti-inflammatory effects of a Mediterranean diet: a review. Curr. Opin. Clin. Nutr. Metab. Care. 2022, 25, 415–422. [Google Scholar] [CrossRef]
- Yubero-Serrano EM, Fernandez-Gandara C, Garcia-Rios A, et al. Mediterranean diet and endothelial function in patients with coronary heart disease: An analysis of the CORDIOPREV randomized controlled trial. Rahimi K, ed. PLOS Med. 2020, 17, e1003282. [Google Scholar] [CrossRef]
- McGrail L, Garelnabi M. Polyphenolic Compounds and Gut Microbiome in Cardiovascular Diseases. Curr. Pharm. Biotechnol. 2020, 21, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Turpin W, Dong M, Sasson G, et al. Mediterranean-Like Dietary Pattern Associations With Gut Microbiome Composition and Subclinical Gastrointestinal Inflammation. Gastroenterology. 2022, 163, 685–698. [Google Scholar] [CrossRef]
- Gutiérrez-Díaz I, Fernández-Navarro T, Sánchez B, Margolles A, González S. Mediterranean diet and faecal microbiota: a transversal study. Food Funct. 2016, 7, 2347–2356. [Google Scholar] [CrossRef] [PubMed]
- Richardson LA, Izuora K, Basu A. Mediterranean Diet and Its Association with Cardiovascular Disease Risk Factors: A Scoping Review. Int. J. Environ. Res. Public. Health. 2022, 19, 12762. [Google Scholar] [CrossRef] [PubMed]
- Vogel RA, Corretti MC, Plotnick GD. The postprandial effect of components of the mediterranean diet on endothelial function. J. Am. Coll. Cardiol. 2000, 36, 1455–1460. [Google Scholar] [CrossRef] [PubMed]
- Shannon OM, Mendes I, KÖchl C, et al. Mediterranean Diet Increases Endothelial Function in Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Nutr. 2020, 150, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- Yubero-Serrano EM, Fernandez-Gandara C, Garcia-Rios A, et al. Mediterranean diet and endothelial function in patients with coronary heart disease: An analysis of the CORDIOPREV randomized controlled trial. Rahimi K, ed. PLOS Med. 2020, 17, e1003282. [Google Scholar] [CrossRef]
- Mattioli AV, Palmiero P, Manfrini O, et al. Mediterranean diet impact on cardiovascular diseases: a narrative review. J. Cardiovasc. Med. 2017, 18, 925–935. [Google Scholar] [CrossRef]
- Liu Y, Milner M, Klonizakis M. Physiological effects of a short-term lifestyle intervention based on the Mediterranean diet: comparison between older and younger healthy, sedentary adults. Nutrition, 2018; 55–56, 185–191. [CrossRef]
- Jimenez-Torres J, Alcalá-Diaz JF, Torres-Peña JD, et al. Mediterranean Diet Reduces Atherosclerosis Progression in Coronary Heart Disease: An Analysis of the CORDIOPREV Randomized Controlled Trial. Stroke. 2021, 52, 3440–3449. [Google Scholar] [CrossRef]
- Tosti V, Bertozzi B, Fontana L. Health Benefits of the Mediterranean Diet: Metabolic and Molecular Mechanisms. J. Gerontol. Ser. A. 2018, 73, 318–326. [Google Scholar] [CrossRef]
- Jin Q, Black A, Kales SN, Vattem D, Ruiz-Canela M, Sotos-Prieto M. Metabolomics and Microbiomes as Potential Tools to Evaluate the Effects of the Mediterranean Diet. Nutrients. 2019, 11, 207. [Google Scholar] [CrossRef] [PubMed]
- Tang WHW, Li DY, Hazen SL. Dietary metabolism, the gut microbiome, and heart failure. Nat. Rev. Cardiol. 2019, 16, 137–154. [Google Scholar] [CrossRef] [PubMed]
- Drapkina OM, Ashniev GA, Zlobovskaya OA, et al. Diversities in the Gut Microbial Patterns in Patients with Atherosclerotic Cardiovascular Diseases and Certain Heart Failure Phenotypes. Biomedicines. 2022, 10, 2762. [Google Scholar] [CrossRef]
- Asensio EM, Ortega-Azorín C, Barragán R, et al. Association between Microbiome-Related Human Genetic Variants and Fasting Plasma Glucose in a High-Cardiovascular-Risk Mediterranean Population. Medicina (Mex). 2022, 58, 1238. [Google Scholar] [CrossRef] [PubMed]
- Beale AL, O’Donnell JA, Nakai ME, et al. The Gut Microbiome of Heart Failure With Preserved Ejection Fraction. J. Am. Heart Assoc. 2021, 10, e020654. [Google Scholar] [CrossRef] [PubMed]
- Katsimichas T, Antonopoulos AS, Katsimichas A, Ohtani T, Sakata Y, Tousoulis D. The intestinal microbiota and cardiovascular disease. Cardiovasc. Res. 2019, 115, 1471–1486. [Google Scholar] [CrossRef] [PubMed]
- Alam MJ, Puppala V, Uppulapu SK, Das B, Banerjee SK. Human microbiome and cardiovascular diseases. In: Progress in Molecular Biology and Translational Science. Vol 192. Elsevier; 2022:231-279. [CrossRef]
- Masenga SK, Povia JP, Lwiindi PC, Kirabo A. Recent Advances in Microbiota-Associated Metabolites in Heart Failure. Biomedicines. 2023, 11, 2313. [Google Scholar] [CrossRef]
- Zhou W, Cheng Y, Zhu P, Nasser MI, Zhang X, Zhao M. Implication of Gut Microbiota in Cardiovascular Diseases. Oxid. Med. Cell Longev. 2020; 2020, 1–14. [CrossRef]
- Lv S, Wang Y, Zhang W, Shang H. Trimethylamine oxide: a potential target for heart failure therapy. Heart. 2022, 108, 917–922. [Google Scholar] [CrossRef]
- McMillan A, Hazen SL. Gut Microbiota Involvement in Ventricular Remodeling Post–Myocardial Infarction: New Insights Into How to Heal a Broken Heart. Circulation. 2019, 139, 660–662. [Google Scholar] [CrossRef]
- Zhang W, Dong XY, Huang R. Gut Microbiota in Ischemic Stroke: Role of Gut Bacteria-Derived Metabolites. Transl. Stroke Res. 2023, 14, 811–828. [Google Scholar] [CrossRef]
- Suganya K, Son T, Kim KW, Koo BS. Impact of gut microbiota: How it could play roles beyond the digestive system on development of cardiovascular and renal diseases. Microb. Pathog, 2021; 152, 104583. [CrossRef]
- Kasahara K, Rey FE. The emerging role of gut microbial metabolism on cardiovascular disease. Curr. Opin. Microbiol, 2019; 50, 64–70. [CrossRef]
- Naik SS, Ramphall S, Rijal S, et al. Association of Gut Microbial Dysbiosis and Hypertension: A Systematic Review. Cureus, Published online. 4 October 2022. [CrossRef]
- Tousoulis D, Guzik T, Padro T, et al. Mechanisms, therapeutic implications, and methodological challenges of gut microbiota and cardiovascular diseases: a position paper by the ESC Working Group on Coronary Pathophysiology and Microcirculation. Cardiovasc. Res. 2022, 118, 3171–3182. [Google Scholar] [CrossRef] [PubMed]
- Jia Q, Xie Y, Lu C, et al. Endocrine organs of cardiovascular diseases: Gut microbiota. J. Cell Mol. Med. 2019, 23, 2314–2323. [Google Scholar] [CrossRef] [PubMed]
- Tang WHW, Hazen SL. The contributory role of gut microbiota in cardiovascular disease. J. Clin. Invest. 2014, 124, 4204–4211. [Google Scholar] [CrossRef] [PubMed]
- Tuteja S, Ferguson JF. Gut Microbiome and Response to Cardiovascular Drugs. Circ. Genomic Precis. Med. 2019, 12, e002314. [Google Scholar] [CrossRef]
- MacKay M, Yang BH, Dursun SM, Baker GB. The Gut-Brain Axis and the Microbiome in Anxiety Disorders, Post-Traumatic Stress Disorder and Obsessive-Compulsive Disorder. Curr. Neuropharmacol, 2023; 21.
- Chen X, Zhang H, Ren S, et al. Gut microbiota and microbiota-derived metabolites in cardiovascular diseases. Chin Med J (Engl). 2023, 136, 2269–2284. [Google Scholar] [CrossRef]
- Wen Y, Sun Z, Xie S, et al. Intestinal Flora Derived Metabolites Affect the Occurrence and Development of Cardiovascular Disease. J. Multidiscip. Healthc, 2022; 15, 2591–2603. [CrossRef]
- Khan I, Khan I, Jianye Z, et al. Exploring blood microbial communities and their influence on human cardiovascular disease. J. Clin. Lab. Anal. 2022, 36, e24354. [Google Scholar] [CrossRef]
- Kelly TN, Bazzano LA, Ajami NJ, et al. Gut Microbiome Associates With Lifetime Cardiovascular Disease Risk Profile Among Bogalusa Heart Study Participants. Circ. Res. 2016, 119, 956–964. [Google Scholar] [CrossRef]
- Chen L, Ishigami T, Doi H, Arakawa K, Tamura K. The Types and Proportions of Commensal Microbiota Have a Predictive Value in Coronary Heart Disease. J. Clin. Med. 2021, 10, 3120. [Google Scholar] [CrossRef]
- Lawrence G, Midtervoll I, Samuelsen SO, Kristoffersen AK, Enersen M, Håheim LL. The blood microbiome and its association to cardiovascular disease mortality: case-cohort study. BMC Cardiovasc. Disord. 2022, 22, 344. [Google Scholar] [CrossRef]
- Palmu J, Börschel CS, Ortega-Alonso A, et al. Gut microbiome and atrial fibrillation—results from a large population-based study. eBioMedicine, 2023; 91, 104583. [CrossRef]
- Wan C, Zhu C, Jin G, Zhu M, Hua J, He Y. Analysis of Gut Microbiota in Patients with Coronary Artery Disease and Hypertension. Wan JY, ed. Evid. Based Complement. Alternat Med, 2021; 2021, 1–9. [CrossRef]
- Liao L, Huang J, Zheng J, Ma X, Huang L, Xu W. Gut microbiota in Chinese and Japanese patients with cardiovascular diseases: a systematic review and meta-analysis. Ann. Saudi Med. 2023, 43, 105–114. [Google Scholar] [CrossRef]
- Pevsner-Fischer M, Blacher E, Tatirovsky E, Ben-Dov IZ, Elinav E. The gut microbiome and hypertension. Curr. Opin. Nephrol. Hypertens. 2017, 26, 1–8. [CrossRef]
- Sata Y, Marques FZ, Kaye DM. The Emerging Role of Gut Dysbiosis in Cardio-metabolic Risk Factors for Heart Failure. Curr. Hypertens. Rep. 2020, 22, 38. [Google Scholar] [CrossRef] [PubMed]
- Dao MC, Everard A, Aron-Wisnewsky J, et al. Akkermansia muciniphila and improved metabolic health during a dietary intervention in obesity: relationship with gut microbiome richness and ecology. Gut. 2016, 65, 426–436. [CrossRef]
- Marques FZ, Mackay CR, Kaye DM. Beyond gut feelings: how the gut microbiota regulates blood pressure. Nat. Rev. Cardiol. 2018, 15, 20–32. [Google Scholar] [CrossRef] [PubMed]
- Anselmi G, Gagliardi L, Egidi G, et al. Gut Microbiota and Cardiovascular Diseases: A Critical Review. Cardiol. Rev. 2021, 29, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Moszak M, Szulińska M, Bogdański P. You Are What You Eat—The Relationship between Diet, Microbiota, and Metabolic Disorders—A Review. Nutrients. 2020, 12, 1096. [Google Scholar] [CrossRef] [PubMed]
- Kumar T, Dutta RR, Velagala VR, Ghosh B, Mudey A. Analyzing the Complicated Connection Between Intestinal Microbiota and Cardiovascular Diseases. Cureus, Published online. 19 August 2022. [CrossRef]
- Tuohy KM, Fava F, Viola R. ‘The way to a man’s heart is through his gut microbiota’—dietary pro- and prebiotics for the management of cardiovascular risk. Proc. Nutr. Soc. 2014, 73, 172–185. [Google Scholar] [CrossRef]
- Nesci A, Carnuccio C, Ruggieri V, et al. Gut Microbiota and Cardiovascular Disease: Evidence on the Metabolic and Inflammatory Background of a Complex Relationship. Int. J. Mol. Sci. 2023, 24, 9087. [Google Scholar] [CrossRef]
- Tang WHW, Hazen SL. The Gut Microbiome and Its Role in Cardiovascular Diseases. Circulation. 2017, 135, 1008–1010. [Google Scholar] [CrossRef]
- Özsoy S, Sultanoglu N, Sanlidag T. The role of mediterranean diet and gut microbiota in type- diabetes mellitus associated with obesity (diabesity). J. Prev. Med. Hyg, 2022; 63, 2S3:E87. [CrossRef]
- Merra G, Noce A, Marrone G, et al. Influence of Mediterranean Diet on Human Gut Microbiota. Nutrients. 2020, 13, 7. [Google Scholar] [CrossRef]
- Borton MA, Shaffer M, Hoyt DW, et al. Targeted curation of the gut microbial gene content modulating human cardiovascular disease. Messaoudi L, ed. mBio. 2023, 14, e01511-23. [Google Scholar] [CrossRef]
- Poli, A. What connection is there between intestinal microbiota and heart disease? Eur. Heart J. Suppl. 2020, 22 (Suppl. L), L117–L120. [Google Scholar] [CrossRef] [PubMed]
- Al-Rubaye H, Perfetti G, Kaski JC. The Role of Microbiota in Cardiovascular Risk: Focus on Trimethylamine Oxide. Curr. Probl. Cardiol. 2019, 44, 182–196. [Google Scholar] [CrossRef] [PubMed]
- Hemmati M, Kashanipoor S, Mazaheri P, et al. Importance of gut microbiota metabolites in the development of cardiovascular diseases (CVD). Life Sci. 2023; 329, 121947. [CrossRef]
- Kanitsoraphan C, Rattanawong P, Charoensri S, Senthong V. Trimethylamine N-Oxide and Risk of Cardiovascular Disease and Mortality. Curr. Nutr. Rep. 2018, 7, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Roberts AB, Gu X, Buffa JA, et al. Development of a gut microbe–targeted nonlethal therapeutic to inhibit thrombosis potential. Nat. Med. 2018, 24, 1407–1417. [Google Scholar] [CrossRef] [PubMed]
- Palombaro M, Raoul P, Cintoni M, et al. Impact of Diet on Gut Microbiota Composition and Microbiota-Associated Functions in Heart Failure: A Systematic Review of In Vivo Animal Studies. Metabolites. 2022, 12, 1271. [Google Scholar] [CrossRef] [PubMed]
- Nagatomo Y, Tang WHW. Intersections Between Microbiome and Heart Failure: Revisiting the Gut Hypothesis. J. Card. Fail. 2015, 21, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Koay YC, Chen YC, Wali JA, et al. Plasma levels of trimethylamine-N-oxide can be increased with ‘healthy’ and ‘unhealthy’ diets and do not correlate with the extent of atherosclerosis but with plaque instability. Cardiovasc. Res. 2021, 117, 435–449. [Google Scholar] [CrossRef]
- Ringel C, Dittrich J, Gaudl A, et al. Association of plasma trimethylamine N-oxide levels with atherosclerotic cardiovascular disease and factors of the metabolic syndrome. Atherosclerosis, 2021; 335, 62–67. [CrossRef]
- Lee Y, Nemet I, Wang Z, et al. Longitudinal Plasma Measures of Trimethylamine N-Oxide and Risk of Atherosclerotic Cardiovascular Disease Events in Community-Based Older Adults. J. Am. Heart Assoc. 2021, 10, e020646. [Google Scholar] [CrossRef]
- Gencer B, Li XS, Gurmu Y, et al. Gut Microbiota-Dependent Trimethylamine N-oxide and Cardiovascular Outcomes in Patients With Prior Myocardial Infarction: A Nested Case Control Study From the PEGASUS-TIMI 54 Trial. J. Am. Heart Assoc. 2020, 9, e015331. [Google Scholar] [CrossRef]
- Zhou X, Jin M, Liu L, Yu Z, Lu X, Zhang H. Trimethylamine N-oxide and cardiovascular outcomes in patients with chronic heart failure after myocardial infarction. ESC Heart Fail. 2020, 7, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Li W, Huang A, Zhu H, et al. Gut microbiota-derived trimethylamine N. -oxide is associated with poor prognosis in patients with heart failure. Med. J. Aust. 2020, 213, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Chen G, He L, Dou X, Liu T. Association of Trimethylamine-N-Oxide Levels with Risk of Cardiovascular Disease and Mortality among Elderly Subjects: A Systematic Review and Meta-Analysis. Cardiorenal Med. 2022, 12, 39–54. [Google Scholar] [CrossRef] [PubMed]
- Ren H, Zhu B, An Y, Xie F, Wang Y, Tan Y. Immune communication between the intestinal microbiota and the cardiovascular system. Immunol. Lett, 2023; 254, 13–20. [CrossRef]
- Bu J, Wang Z. Cross-Talk between Gut Microbiota and Heart via the Routes of Metabolite and Immunity. Gastroenterol. Res. Pract, 2018; 2018, 1–8. [CrossRef]
- Trøseid M, Andersen GØ, Broch K, Hov JR. The gut microbiome in coronary artery disease and heart failure: Current knowledge and future directions. EBioMedicine, 2020; 52, 102649. [CrossRef]
- Dubinski P, Czarzasta K, Cudnoch-Jedrzejewska A. The Influence of Gut Microbiota on the Cardiovascular System Under Conditions of Obesity and Chronic Stress. Curr. Hypertens. Rep. 2021, 23, 31. [Google Scholar] [CrossRef]
- Pastori D, Carnevale R, Nocella C, et al. Gut-Derived Serum Lipopolysaccharide is Associated With Enhanced Risk of Major Adverse Cardiovascular Events in Atrial Fibrillation: Effect of Adherence to Mediterranean Diet. J. Am. Heart Assoc. 2017, 6, e005784. [Google Scholar] [CrossRef]
- Hernández-Ruiz P, Amezcua-Guerra LM, López-Vidal Y, et al. Comparative characterization of inflammatory profile and oral microbiome according to an inflammation-based risk score in ST-segment elevation myocardial infarction. Front. Cell Infect. Microbiol, 2023; 13, 1095380. [CrossRef]
- Zabell A, Tang WHW. Targeting the Microbiome in Heart Failure. Curr. Treat. Options Cardiovasc. Med. 2017, 19, 27. [Google Scholar] [CrossRef] [PubMed]
- Kitai T, Tang WHW. Gut microbiota in cardiovascular disease and heart failure. Clin. Sci. 2018, 132, 85–91. [Google Scholar] [CrossRef]
- Mamic P, Chaikijurajai T, Tang WHW. Gut microbiome—A potential mediator of pathogenesis in heart failure and its comorbidities: State-of-the-art review. J. Mol. Cell Cardiol, 2021; 152, 105–117. [CrossRef]
- Anderson KM, Ferranti EP, Alagha EC, Mykityshyn E, French CE, Reilly CM. The heart and gut relationship: a systematic review of the evaluation of the microbiome and trimethylamine-N-oxide (TMAO) in heart failure. Heart Fail. Rev. 2022, 27, 2223–2249. [Google Scholar] [CrossRef]
- Gallo A, Macerola N, Favuzzi AM, Nicolazzi MA, Gasbarrini A, Montalto M. The Gut in Heart Failure: Current Knowledge and Novel Frontiers. Med. Princ. Pract. 2022, 31, 203–214. [Google Scholar] [CrossRef]
- Kimble R, Gouinguenet P, Ashor A, et al. Effects of a mediterranean diet on the gut microbiota and microbial metabolites: A systematic review of randomized controlled trials and observational studies. Crit. Rev. Food Sci. Nutr. 2023, 63, 8698–8719. [Google Scholar] [CrossRef]
- Rejeski JJ, Wilson FM, Nagpal R, Yadav H, Weinberg RB. The Impact of a Mediterranean Diet on the Gut Microbiome in Healthy Human Subjects: A Pilot Study. Digestion. 2022, 103, 133–140. [Google Scholar] [CrossRef]
- Pagliai G, Russo E, Niccolai E, et al. Influence of a 3-month low-calorie Mediterranean diet compared to the vegetarian diet on human gut microbiota and SCFA: the CARDIVEG Study. Eur. J. Nutr. 2020, 59, 2011–2024. [Google Scholar] [CrossRef] [PubMed]
- Mitsou EK, Kakali A, Antonopoulou S, et al. Adherence to the Mediterranean diet is associated with the gut microbiota pattern and gastrointestinal characteristics in an adult population. Br. J. Nutr. 2017, 117, 1645–1655. [Google Scholar] [CrossRef] [PubMed]
- Barber TM, Kabisch S, Pfeiffer AFH, Weickert MO. The Effects of the Mediterranean Diet on Health and Gut Microbiota. Nutrients. 2023, 15, 2150. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Mantrana I, Selma-Royo M, Alcantara C, Collado MC. Shifts on Gut Microbiota Associated to Mediterranean Diet Adherence and Specific Dietary Intakes on General Adult Population. Front. Microbiol, 2018; 9, 890. [CrossRef]
- Tagliamonte S, Laiola M, Ferracane R, et al. Mediterranean diet consumption affects the endocannabinoid system in overweight and obese subjects: possible links with gut microbiome, insulin resistance and inflammation. Eur. J. Nutr. 2021, 60, 3703–3716. [Google Scholar] [CrossRef] [PubMed]
- Muralidharan J, Moreno-Indias I, Bulló M, et al. Effect on gut microbiota of a 1-y lifestyle intervention with Mediterranean diet compared with energy-reduced Mediterranean diet and physical activity promotion: PREDIMED-Plus Study. Am. J. Clin. Nutr. 2021, 114, 1148–1158. [Google Scholar] [CrossRef] [PubMed]
- Pisanu S, Palmas V, Madau V, et al. Impact of a Moderately Hypocaloric Mediterranean Diet on the Gut Microbiota Composition of Italian Obese Patients. Nutrients. 2020, 12, 2707. [Google Scholar] [CrossRef] [PubMed]
- Ismael S, Silvestre MP, Vasques M, et al. A Pilot Study on the Metabolic Impact of Mediterranean Diet in Type 2 Diabetes: Is Gut Microbiota the Key? Nutrients. 2021, 13, 1228. [Google Scholar] [CrossRef]
- Gundogdu A, Nalbantoglu OU. The role of the Mediterranean diet in modulating the gut microbiome: A review of current evidence. Nutrition, 2023; 114, 112118. [CrossRef]
- Rosés C, Cuevas-Sierra A, Quintana S, et al. Gut Microbiota Bacterial Species Associated with Mediterranean Diet-Related Food Groups in a Northern Spanish Population. Nutrients. 2021, 13, 636. [Google Scholar] [CrossRef]
- De Filippis F, Pellegrini N, Vannini L, et al. High-level adherence to a Mediterranean diet beneficially impacts the gut microbiota and associated metabolome. Gut. 2016, 65, 1812–1821. [Google Scholar] [CrossRef]
- Clark JS, Simpson BS, Murphy KJ. The role of a Mediterranean diet and physical activity in decreasing age-related inflammation through modulation of the gut microbiota composition. Br. J. Nutr. 2022, 128, 1299–1314. [Google Scholar] [CrossRef]
- Muralitharan RR, Jama HA, Xie L, Peh A, Snelson M, Marques FZ. Microbial Peer Pressure: The Role of the Gut Microbiota in Hypertension and Its Complications. Hypertension. 2020, 76, 1674–1687. [Google Scholar] [CrossRef]
- García-López M, Martínez-González M, Basterra-Gortari F, Barrio-López M, Gea A, Beunza J. Adherence to the Mediterranean dietary pattern and heart rate in the SUN project. Eur. J. Prev. Cardiol. 2014, 21, 521–527. [Google Scholar] [CrossRef]
- Yntema T, Koonen DPY, Kuipers F. Emerging Roles of Gut Microbial Modulation of Bile Acid Composition in the Etiology of Cardiovascular Diseases. Nutrients. 2023, 15, 1850. [Google Scholar] [CrossRef]
- Bailey MA, Holscher HD. Microbiome-Mediated Effects of the Mediterranean Diet on Inflammation. Adv. Nutr. 2018, 9, 193–206. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A tentative, synthetic description of the pathways related to mediterranean diet, microbiome eubiosis, and cardiovascular health. Abbreviations: CV: Cardiovascular; CX3CR1: C-X3-C Motif Chemokine Receptor 1; FOXP3 forkhead box P3: GPR: G Protein receptor; HF: Heart failure; OLFR: Olfactory G-protein-coupled receptor-78: SCFA: Short chain fatty acids; TMAO: Trimethylamine-N-Oxide; Treg: Regulatory T cells.
Figure 1.
A tentative, synthetic description of the pathways related to mediterranean diet, microbiome eubiosis, and cardiovascular health. Abbreviations: CV: Cardiovascular; CX3CR1: C-X3-C Motif Chemokine Receptor 1; FOXP3 forkhead box P3: GPR: G Protein receptor; HF: Heart failure; OLFR: Olfactory G-protein-coupled receptor-78: SCFA: Short chain fatty acids; TMAO: Trimethylamine-N-Oxide; Treg: Regulatory T cells.
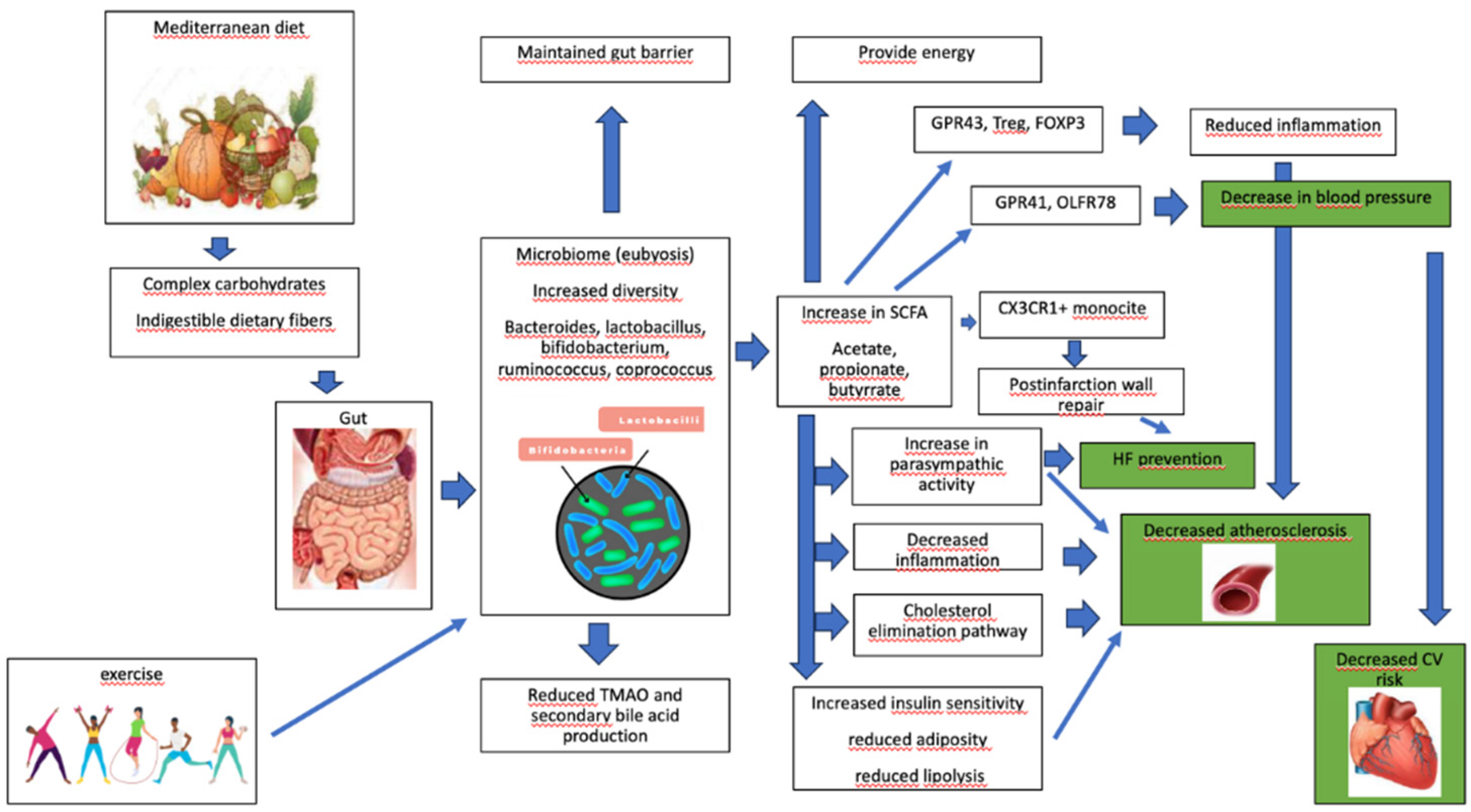
Figure 2.
A tentative, synthetic description of the pathways related to western diet, microbiome dysbiosis, and cardiovascular diseases. Abbreviations: CKD: Chronic kidney disease; FMO3: Flavin monooxygenase-3; LPS: Lipopolysaccharide; NFκβ: Nuclear factor κβ; NO: Nitric oxide; TLR4: Toll like receptor-4; TMA: Trimethylamine; TMAO: Trimethylamine-N-Oxide; TNFα: Tumor necrosis factor α.
Figure 2.
A tentative, synthetic description of the pathways related to western diet, microbiome dysbiosis, and cardiovascular diseases. Abbreviations: CKD: Chronic kidney disease; FMO3: Flavin monooxygenase-3; LPS: Lipopolysaccharide; NFκβ: Nuclear factor κβ; NO: Nitric oxide; TLR4: Toll like receptor-4; TMA: Trimethylamine; TMAO: Trimethylamine-N-Oxide; TNFα: Tumor necrosis factor α.
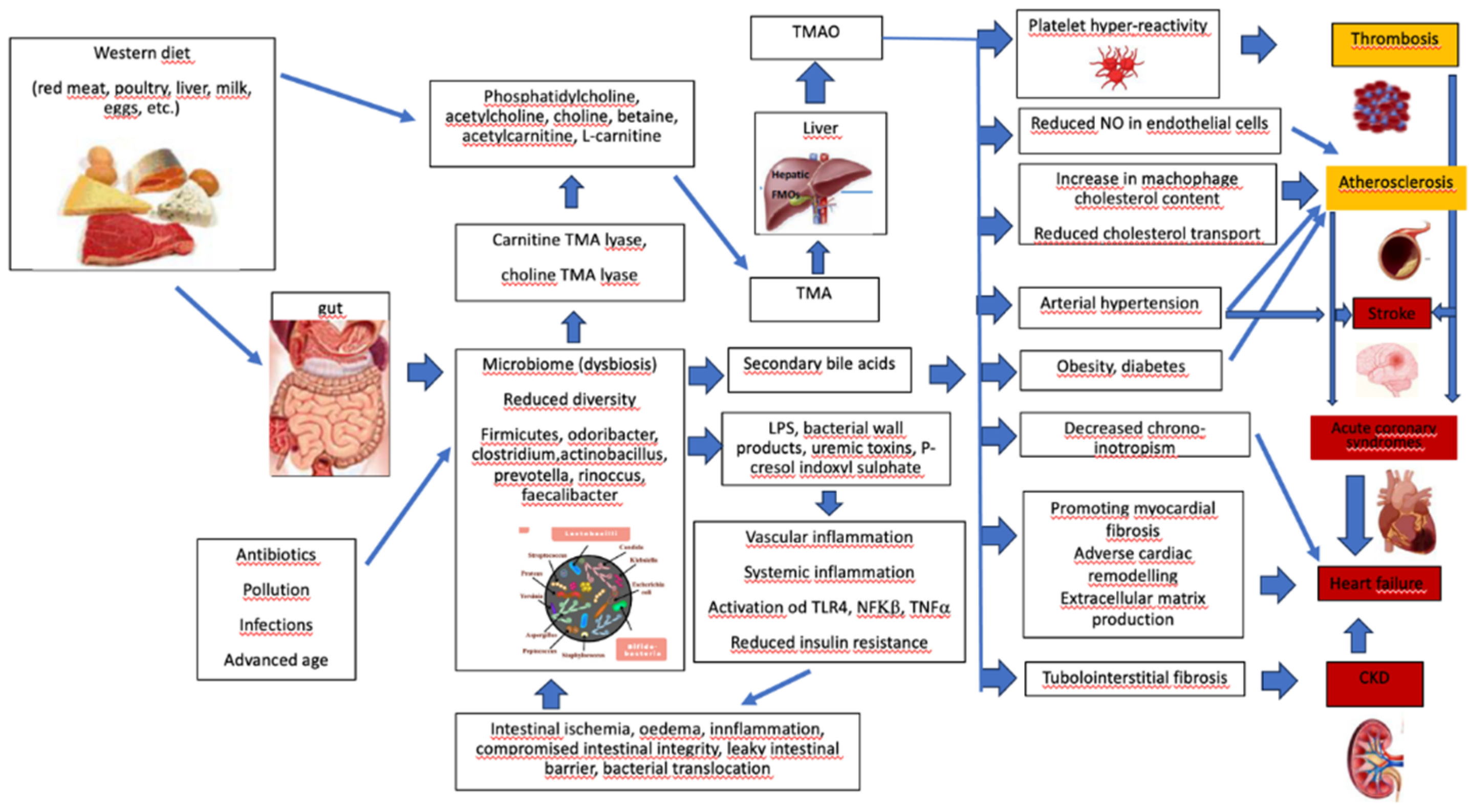
Figure 3.
The connection between Mediterranean diet, gut microbiome and cardiovascular diseases.
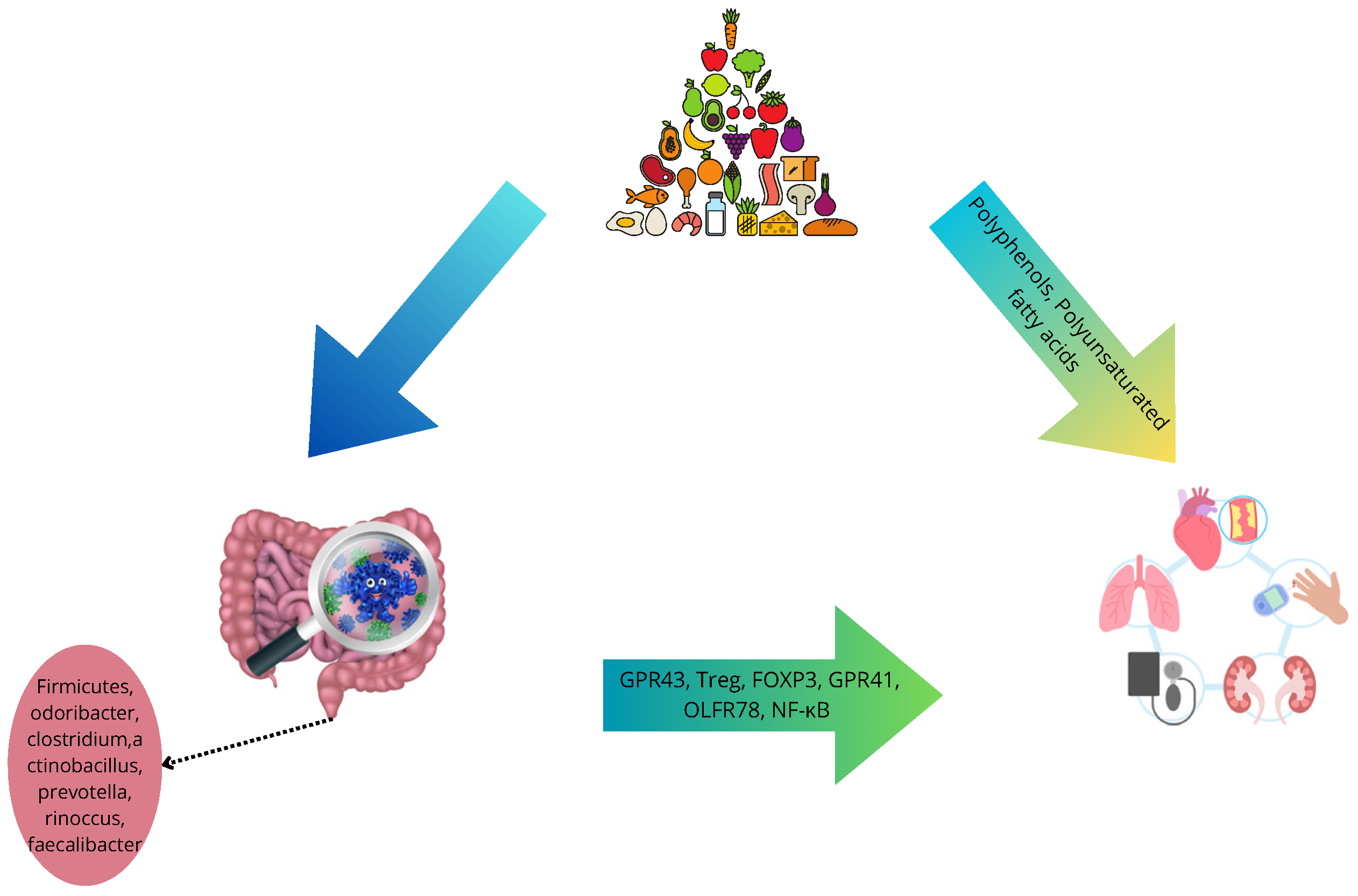

Table 1.
Main components of microbiome in cardiovascular diseases.
| Disease/Condition | Main Microbial Agents |
|---|---|
| Cardiovascular risk factors | Prevotella 2, Prevotella 7, Tyzzerella and Tyzzerella 4 genera, Bacteroides uniformis and B. vulgatus (low prevalence of Alloprevotella Prevotella copri. and Catenibacterium) |
| Arterial hypertension | Catabacter, Robinsoleilla, Serratia, Enterobacteriaceae, Ruminococcus torques, Parasutterella, Escherichia, Shigella, and Klebsiella (decreased abundance of Sporobacter, Roseburia hominis, Romboutsia spp., and Roseburia) |
| Atrial fibrillation | Enorma and Bifidobacterium genera |
| Diabetes mellitus | order Rhizobiales, family Desulfovibrionaceae, genus Romboutsia. |
| Coronary heart disease | Proteobacteria and Actinobacteria phyla, Bacteroides, Prevotella, Firmicutes, Veillonella, Clostridium, Lactobacillaceae (Lactobacillus plantarum) and Streptococcus (decreased prevalence of Caulobacterales order and Caulobacteraceae family, aminococcaceae and Odoribacteraceae) |
| Cerebrovascular disease | Firmicutes, Proteobacteria and Actinobacteria phyla |
| Heart failure | Ruminococcus gnavus, Escherichia Shigella, Streptococcus sp (sanguinus and parasanguinis), Veillonella sp, and Actinobacteria (relative depletion of Eubacterium, Prevotella, Faecalibacterium, SMB53, aminococcaceae, Odoribacteraceae and Megamonas) |
| Cardiovascular mortality | genera Kocuria and Enhydrobacter (genera Paracoccus was inversely related) |
Table 2.
Effects of MD on gut microbiota.
| Increase | Decrease |
|---|---|
|
Akkermansia muciniphila, Anaerostipes hadrus, Bacteroides thetaiotaomicron, Bifidobacteria animalis, Candida albicans, Catenibacterium, Christensenellaceae, Clostridium (cluster XIVa, leptum) Enterorhabdus, Eubacterium rectale, Faecalibacterium (Lactococcus, prausnitzii) Lachnoclostridium, Lachnospiraceae, Oscillospira (Flavonifractor), Parabacteroides, Phascolarctobacterium, Prevotellaceae, Prevotellae, Proteobacteria, Roseburia faecis, Ruminococcaceae bromii and plautii, Sphingobacteriaceae |
Actinomyces lignae, Butyricicoccus, Catenibacterium, Clostridium ramosum, Collinsella aerofaciens, Coprococcus Anaerostipes and comes, Dorea formicigenerans, Escherichia coli, Eubacterium hallii, Firmicutes, Flavonifractor plautii, Haemophilus, Lachnospiraceae Megamonas, Ruminiclostridium, Ruminococcus gnavus and torques Veillonella dispar |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



