Submitted:
29 February 2024
Posted:
01 March 2024
You are already at the latest version
Abstract
Background: Healthcare workers are exposed to several hazardous chemicals in the workplace that can result in numerous adverse health effects. Several published studies from many different countries have documented the presence of metabolites from antineoplastic drugs in the urine of healthcare workers and demonstrated contaminated working surfaces with these agents. This study is a literature review that aims to compare the prevalence and degree of exposure to cyclophosphamide (CP), ifosfamide (IFO), and methotrexate (MTX) in physicians, nurses, and pharmacists in the hospital setting.
Methods: An extensive search was conducted on PubMed, Google Scholar, HINARI, OARE, and Science Direct where applicable research about healthcare workers and antineoplastic drugs exposure were identified. Medical Subject Headings (MeSH) keywords: occupational exposure, antineoplastic drugs (cytotoxic drugs, cyclophosphamide, ifosfamide, methotrexate), hazardous chemicals, healthcare workers (healthcare professionals, nurses, pharmacists, physicians), hospital setting, and adverse health outcomes were used. Thereafter, relevant articles from 2000 to 2020 were selected to perform this literature review.
Results: Review of literature demonstrated that cyclophosphamide was the most prevalent contaminant in the hospital setting. Additionally, pharmacists are among the group of healthcare workers with the highest prevalence of antineoplastic agents in urine samples while nursing stations had the highest rate of surface contamination.
Conclusion: There is an urgent need to develop a system to monitor and detect the pathway of environmental exposure to antineoplastic drugs in the healthcare setting, and to evaluate the effectiveness of the existing protective measures. Well designed studies focusing on improving the standard safety precautions is a priority to protect healthcare workers.
Keywords:
hedging
; transaction costs
; dynamic programming
; risk management
; post-decision state variable
1. Introduction
Cancer prevalence and mortality are rapidly rising worldwide and the yearly incidence is projected to increase to 29.4 million in 2040, from 18.1 million in 2010 (Bray et al., 2018; Wild, 2019). It is the second leading cause of death globally with a documented economic cost of US$ 1.16 trillion in 2010, which is expected to rise (Cancer, n.d.). For these reasons, a significant burden is placed on healthcare workers who care for patients with malignancies. Almost eight (8) million healthcare workers in the U.S. are exposed to harmful drugs in the workplace (Hazardous Drug Exposures in Health Care | NIOSH | CDC, n.d.). Similar occupational exposures have been reported in other parts of the world (Hall et al., 2017; Maeda et al., 2010; Occupational Exposure of Pharmacy Technicians and Cleaning Staff to Cytotox...: EBSCOhost, n.d.; Pałaszewska-Tkacz et al., 2019; Peters et al., 2015; Scarselli et al., 2007).
Over 100 antineoplastic agents are currently in use in the healthcare setting and a significant number have been identified as carcinogens (Graeve et al., 2017). Several studies have documented exposure to these agents, namely; cyclophosphamide, ifosfamide, and methotrexate among doctors, nurses, and pharmacists (Hedmer et al., 2008; Nyman et al., 2007; Pałaszewska-Tkacz et al., 2019; Pethran et al., 2003; Ramphal et al., 2015; Ratner et al., 2010; Shahrasbi et al., 2014; Sugiura et al., 2011; Yu, 2020) via dermal contact, ingestion, inhalation, and contact with contaminated surfaces (Connor, 2006; Loomis et al., 2018; Sugiura et al., 2011). Exposure tend to occur at higher rates in the hospital setting (Hon et al., 2015) with a number of documented acute and chronic adverse effects ranging from skin disorders to reproductive issues, and even malignancies (Hall et al., 2017; Rai et al., 2020; Ratner et al., 2010; Yu, 2020).
This review is valuable to compare the prevalence of antineoplastic drug exposure among different groups of healthcare professionals and sets out to answer the following research question: Which group of workers is most exposed to antineoplastic drugs in the hospital setting? The main purpose of this literature review is to evaluate exposure to cyclophosphamide, ifosfamide, and methotrexate among physicians, nurses, and pharmacists in the hospital setting. It is hypothesized that there is a difference in the degree of exposure among doctors, nurses, and pharmacists.
Results from this review will aid employees and government officials in the enhancement and provision of targeted preventative measures as this growing problem is preventable through effective exposure control strategies.
2. Materials and Methods
A search of PubMed and Google Scholar search engines was performed. Research articles were also reviewed from Science Direct, HINARI, and OARE databases. The search strategy included the following Medical Subject Headings (MeSH) keywords: occupational exposure, antineoplastic drugs (cytotoxic drugs, cyclophosphamide, ifosfamide, methotrexate), hazardous chemicals, healthcare workers (healthcare professionals, nurses, pharmacists, physicians), hospital setting, and adverse health outcomes, which were combined with the Boolean operator “AND” using two to three terms at a given time.
The initial search generated 87 studies that were saved on Mendeley desktop. Duplicates were checked on Mendeley and 12 studies were removed. Thereafter, the titles and abstracts were reviewed, and 21 articles met the inclusion criteria.
The inclusion criteria included cross-sectional peer reviewed articles, published in English, that quantified exposure (concentration of drug/ metabolites in urine or on contaminated surfaces), and explored the prevalence of exposure of the three above mentioned drugs among doctors, nurses, and pharmacists, respectively, which were published between January 2000 and November 2020. Studies published in languages other than English, publication with a qualitative exposure measure (i.e., exposed or not exposed), exposure assessed in settings apart from the hospital, and exposures in healthcare workers other than doctors, nurses, and pharmacists were excluded. Sixty-seven (67) studies were eliminated for the following reasons: 31 studies were out of topic, 29 had qualitative exposure measures, 5 were conducted outside of the hospital setting, and 2 were in Dutch. Finally, the reference lists of included articles were examined, and one (1) additional article was added. Nine (9) articles were selected to perform this review. These steps were represented by a PRISMA flow diagram as depicted in Figure 1.
A data extraction form was developed and applied to all included papers. Data extracted included: the study, method, study population, exposure drug, number of persons exposed/samples tested, limit of detection (LOD), and the results. Data obtained were recorded using Microsoft Excel and prevalence ratios were calculated for each antineoplastic agent among each group of healthcare workers. This was then compared to determine the group of workers with the highest degree of exposure.
3. Results
Review of literature led to arrangement of two tables, each with eight (8) categories. Table 1 looked at drug concentrations of cyclophosphamide, methotrexate, and ifosfamide detected in urine samples of physicians, nurses, and pharmacists. Table 2 focused on surface contamination with the abovementioned agents in the hospital setting, mainly at the pharmacy and on the wards.
Generally, the results demonstrated that healthcare workers are exposed to antineoplastic agents in their work environments. Exposure data was well documented for nurses and pharmacists, however information on physician exposure was limited. Additionally, cyclophosphamide was the most prevalent exposure drug with nursing stations demonstrating the highest level of surface contamination and pharmacists being the group with the highest degree of urinary contamination.
4. Discussion
Biological Monitoring of Healthcare Workers
Healthcare workers are at risk of exposure to antineoplastic agents at their workplace despite the use of personal protective equipment (PPE) and adherence to standard safety precautions. Results obtained showed that there is a difference in the degree of exposure among the groups studied. Ae et al., 2003 quantified exposure to CP and IFO in 670 urine samples over 14 German hospitals. The researchers performed 24-hour urine collections prior to work shifts in three (3) separate cycles. Positive samples obtained throughout the cycles were not statistically different. This study was conducted over a period of three (3) years, during that time an average of 1,200 IFO and 1,100 g CP were handled per hospital per year and each study participant performed 40-50 mixtures of antineoplastics agents per day. The findings suggested that CP was the most prevalent drug detected in the urine of subjects under study when compared to IFO. Furthermore, pharmacists had a higher prevalence of exposure at 38% when compared to nurses at two percent (2%). This is in keeping with data obtained from Crul et al., 2020 that evaluated hand rinsed samples of healthcare workers for antineoplastic agents. They found that CP was the most prevalent antineoplastic agent and hand samples of pharmacists showed highest level of contamination compared to other groups of healthcare workers. There are limitations to this study given the lack of information on other categories of healthcare workers, particularly physicians. Baniasadi et al., 2018 evaluated pre- and post-shift urine samples from controls, and subjects with known exposure to CP and IFO. For subjects, it was found that 46.66% of samples were positive for CP and 6.66% for IFO. Samples collected from controls had no detectable concentrations of antineoplastic agents. Some of the factors attributed to these findings were inadequate PPE for handling antineoplastic agents, inadequate safety controls, and large amounts of drugs handled.
Healthcare workers can be protected from exposure to antineoplastic agents through effective prevention control strategies and strict adherence to protective measures. This was demonstrated by Hedmer at al., 2008. These authors quantified concentration of CP and IFO among nurses and pharmacist, but focused on the variability of contamination in urine and surface samples. They collected pre- and post-shift urine samples from 22 healthcare workers in a university hospital. There were no drug concentrations detected in the urine of subjects, however the authors found a variation in surface contamination which will be discussed later. On average pharmacists handled 24g of IFO and 12g of CP per day compared to nurses who handled 2.4g IFO and 1.1g CP per day. This study demonstrated that the subjects under study had exemplary personal protective work practices as guided by the Swedish Work Environment Authority. Evaluation of only one workplace and a small sample of healthcare workers limited this paper. Similar results were found in Sottani et al., 2012 where the urine of healthcare workers was not contaminated with antineoplastic agents. These researchers examined four (4) hospitals in Italy for urine and surface contamination. Evidence obtained demonstrated that surface contamination is not statistically significantly when correlated to positive urine samples. Utilizing rigorous protection measures can potentially reduce exposure and protect healthcare workers.
Hon et al., 2015 evaluated 103 subjects, from which two (2) sets of 24-hour urine samples were collected and assessed for CP concentration in the urine of nurses and pharmacists within a Canadian healthcare facility. Fifty-six percent (56%) of nurses and 44% of pharmacists had urine samples positive for CP that were greater than the LOD. Questionnaires done by these researchers further assessed factors associated with the findings. The researchers attributed two (2) main factors that correlated to CP urine levels. Higher concentrations were seen in the urine of healthcare workers whose duty involved direct handling of the drug and those that did not receive control measures training. Further studies are needed to assess the effectiveness of control measures that exists in healthcare systems globally so that necessary enhancements can be made.
Surface Contamination of Work Surfaces
The reviewed literature demonstrated surface contamination in all healthcare facilities examined. From every one of the studies examined, surface contamination was an important and constant source of exposure to antineoplastic agents among healthcare workers. It occurred despite the use of current cleaning measures and adherence to existing safety guidelines. Graeve et al., 2017 collected 62 surface samples from 27 locations in a university hospital from nursing stations, physician workrooms and pharmacy areas. The sample collection was preceded by questionnaires taken by 163 nurses, physicians, and pharmacists. Areas known to have potential antineoplastic drug exposure with high levels of usage were selected. Six percent (6%) of samples from nursing stations tested above the LOD, while two percent (2%) from pharmacy areas tested above the LOD and no samples in physician work areas detected antineoplastic agents. The authors attributed the difference in the levels of surface contamination among the different groups of staff to variations in job tasks performed. Nurses for instance performed multiple tasks involving the drugs under study that ranged from drug administration to disposal, with several interruptions by family members and patients. Pharmacists on the other hand performed a specific task which is drug preparation with no interruptions. Further studies are needed to evaluate this.
Hedmer et al., 2008 collected wipe samples from the oncology ward and pharmacy, using a new glove for each sample to limit contamination. The highest level of contamination was seen in ward areas with the highest usage of antineoplastic drugs.
Rhamphal et al., 2015 focused their study on the oncology pharmacy and used the main pharmacy that did not handle antineoplastic drugs as a control. Wipe samples were collected before and after cleaning and demonstrated contamination of work surfaces with CP and MTX on both instances. IFO was only found on post cleaning wipe samples. The main pharmacy showed no contamination. The shows that current cleaning measures are inadequate. Dugheri et al., 2018 used a similar sample collection technique both pre- and post-shift. These researchers collected 4814 wipe samples over a nine (9) year period from nine (9) hospitals. They also incorporated staff training throughout the study and despite this, surface contamination with CP (17%), IFO (15.4%), and MTX (0.5%) were detected. Sottani et al., 2012 provided further support to this claim.
Future studies are needed to assess the cleaning measures that exist among different healthcare facilities and determine ways to improve existing protocols as surface contamination was reported in all reviewed studies.
Significance to Public Health
These findings suggest that healthcare workers have varying degree of exposure to antineoplastic agents in their workplace that is influenced by varying factors. More importantly, it also demonstrated that healthcare workers can be protected through effective control strategies. This information is vital to public health as:
It can be used to better understand the factors that contribute to exposure and incorporate control measures to address them.
Aid in the development of a pathway that outlines the different points of exposure so that targeted preventative measures can be developed.
Varying degree of protection is utilized in different healthcare facilities as they follow different safe handling guidelines. Guidelines should be evaluated and standardized.
The effectiveness of current safe handling guidelines needs to be assessed and tackled.
Malignancy is a growing problem globally, and the individuals that are providing care for patients with cancers are being negatively affected through exposure to antineoplastic agents. Public health interventions that reduce the risk of exposure to antineoplastic agents among healthcare workers are vital in protecting staff.
5. Conclusion
In this article, the prevalence of exposure to antineoplastic agents have been addressed. This study focused on physicians, nurses, and pharmacists, however other categories of workers like cleaners, and the administrative support staff have potential for exposure in the healthcare setting. Exposure among these groups of workers should be investigated in future studies and these groups of workers should be incorporated in control strategies.
It is evident that healthcare workers have varying degree of exposure to antineoplastic agents at their jobs and this needs to be addressed to protect staff from adverse health outcomes. There is an urgent need to develop a system to monitor and detect the pathway of environmental exposure to antineoplastic drugs in the healthcare setting, and to evaluate the effectiveness of the existing protective measures. Well-designed studies focusing on improving the standard safety precautions is a priority to protect healthcare workers and will aid in standardization of guidelines globally.
References
- Ae, A. P., Schierl, R., Karlheinz, A. E., Carl-Heinz, H., Ae, G., Boos, K.-S., Nowak, D., Pethran, A., Schierl, R., Hauff, K., Grimm, C.-H., Boos, K.-S., & Nowak, D. (2003). Uptake of antineoplastic agents in pharmacy and hospital personnel. Part I: monitoring of urinary concentrations. International Archives of Occupational and Environmental Health, 76(1), 5–10. [CrossRef]
- Baniasadi, S., Alehashem, M., Yunesian, M., & Rastkari, N. (2018). Biological monitoring of healthcare workers exposed to antineoplastic drugs: Urinary assessment of cyclophosphamide and ifosfamide. Iranian Journal of Pharmaceutical Research, 17(4), 1458–1464. [CrossRef]
- Bray, F., Ferlay, J., Soerjomataram, I., Siegel, R. L., Torre, L. A., & Jemal, A. (2018). Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians, 68(6), 394–424. [CrossRef]
- 4. Cancer. (n.d.). Retrieved November 5, 2020, from https://www.who.int/news-room/fact-sheets/detail/cancer.
- Connor, T. H. (2006). Hazardous anticancer drugs in health care: Environmental exposure assessment. Annals of the New York Academy of Sciences, 1076, 615–623. [CrossRef]
- Crul, M., Hilhorst, S., Breukels, O., Bouman-d’Onofrio, J. R. C., Stubbs, P., & van Rooij, J. G. (2020). Occupational exposure of pharmacy technicians and cleaning staff to cytotoxic drugs in Dutch hospitals. Journal of Occupational and Environmental Hygiene, 17(7–8), 1–10. [CrossRef]
- Dugheri, S., Bonari, A., Pompilio, I., Boccalon, P., Mucci, N., & Arcangeli, G. (2018). A new approach to assessing occupational exposure to antineoplastic drugs in hospital environments. Arhiv Za Higijenu Rada i Toksikologiju, 69(3), 226–237. [CrossRef]
- Graeve, C. U., McGovern, P. M., Alexander, B., Church, T., Ryan, A., & Polovich, M. (2017). Occupational Exposure to Antineoplastic Agents. Workplace Health and Safety, 65(1), 9–20. [CrossRef]
- Hall, A. L., Demers, P. A., Astrakianakis, G., Ge, C., & Peters, C. E. (2017). Estimating national-level exposure to antineoplastic agents in the workplace: CAREX Canada findings and future research needs. Annals of Work Exposures and Health, 61(6), 656–668. [CrossRef]
- Hazardous Drug Exposures in Health Care | NIOSH | CDC. (n.d.). Retrieved November 3, 2020, from https://www.cdc.gov/niosh/topics/hazdrug/default.html.
- Hedmer, M., Tinnerberg, H., Axmon, A., & Jönsson, B. A. G. (2008). Environmental and biological monitoring of antineoplastic drugs in four workplaces in a Swedish hospital. International Archives of Occupational and Environmental Health, 81(7), 899–911. [CrossRef]
- Hon, C. Y., Teschke, K., Shen, H., Demers, P. A., & Venners, S. (2015). Antineoplastic drug contamination in the urine of Canadian healthcare workers. International Archives of Occupational and Environmental Health, 88(7), 933–941. [CrossRef]
- Loomis, D., Guha, N., Hall, A. L., & Straif, K. (2018). Identifying occupational carcinogens: An update from the IARC Monographs. Occupational and Environmental Medicine, 75(8), 593–603. [CrossRef]
- Maeda, S., Miyawaki, K., Matsumoto, S., Oishi, M., Miwa, Y., & Kurokawa, N. (2010). Evaluation of environmental contaminations and occupational exposures involved in preparation of chemotherapeutic drugs. Yakugaku Zasshi, 130(6), 903–910. [CrossRef]
- Nyman, H., Jorgenson, J., & Slawson, M. (2007). Workplace Contamination with Antineoplastic Agents in a New Cancer Hospital Using a Closed-System Drug Transfer Device. Hospital Pharmacy, 42(3), 219–225. [CrossRef]
- Occupational exposure of pharmacy technicians and cleaning staff to cytotox...: EBSCOhost. (n.d.). Retrieved November 3, 2020, from http://web.a.ebscohost.com.periodicals.sgu.edu/ehost/detail/detail?vid=0&sid=96699d77-4514-4afd-99a7-8d31b5dfb0aa%40sdc-v-sessmgr03&bdata=JnNpdGU9ZWhvc3QtbGl2ZQ%3D%3D#AN=32633703&db=mnh.
- Pałaszewska-Tkacz, A., Czerczak, S., Konieczko, K., & Kupczewska-Dobecka, M. (2019). Cytostatics as hazardous chemicals in healthcare workers’ environment. International Journal of Occupational Medicine and Environmental Health, 32(2), 141–159. [CrossRef]
- Peters, C. E., Ge, C. B., Hall, A. L., Davies, H. W., & Demers, P. A. (2015). CAREX Canada: An enhanced model for assessing occupational carcinogen exposure. Occupational and Environmental Medicine, 72(1), 64–71. [CrossRef]
- Pethran, A., Schierl, R., Hauff, K., Grimm, C.-H., Boos, K.-S., & Nowak, D. (2003). Uptake of antineoplastic agents in pharmacy and hospital personnel. Part I: monitoring of urinary concentrations. International Archives of Occupational and Environmental Health, 76(1), 5–10. [CrossRef]
- Rai, R., Fritschi, L., Carey, R. N., Lewkowski, K., Glass, D. C., Dorji, N., & El-Zaemey, S. (2020). The estimated prevalence of exposure to carcinogens, asthmagens, and ototoxic agents among healthcare workers in Australia. American Journal of Industrial Medicine, 63(7), 624–633. [CrossRef]
- Ramphal, R., Bains, T., Goulet, G., & Vaillancourt, R. (2015). Occupational exposure to chemotherapy of pharmacy personnel at a single centre. Canadian Journal of Hospital Pharmacy, 68(2), 104–112. [CrossRef]
- Ratner, P. A., Spinelli, J. J., Beking, K., Lorenzi, M., Chow, Y., Teschke, K., Le, N. D., Gallagher, R. P., & Dimich-Ward, H. (2010). Cancer incidence and adverse pregnancy outcome in registered nurses potentially exposed to antineoplastic drugs. BMC Nursing, 9. [CrossRef]
- Scarselli, A., Montaruli, C., & Marinaccio, A. (2007). The Italian information system on occupational exposure to carcinogens (SIREP): Structure, contents and future perspectives. Annals of Occupational Hygiene, 51(5), 471–478. [CrossRef]
- Shahrasbi, A. A., Afshar, M., Shokraneh, F., Monji, F., Noroozi, M., Ebrahimi-Khojin, M., Madani, S. F., Ahadi-Barzoki, M., & Rajabi, M. (2014). Risks to health professionals from hazardous drugs in Iran: A pilot study of understanding of healthcare team to occupational exposure to cytotoxics. EXCLI Journal, 13, 491–501. [CrossRef]
- Sottani, C., Porro, B., Imbriani, M., & Minoia, C. (2012). Occupational exposure to antineoplastic drugs in four Italian health care settings. Toxicology Letters, 213(1), 107–115. [CrossRef]
- Sugiura, S. I., Asano, M., Kinoshita, K., Tanimura, M., & Nabeshima, T. (2011). Risks to health professionals from hazardous drugs in Japan: A pilot study of environmental and biological monitoring of occupational exposure to cyclophosphamide. Journal of Oncology Pharmacy Practice, 17(1), 14–19. [CrossRef]
- Wild, C. P. (2019). The global cancer burden: necessity is the mother of prevention. In Nature Reviews Cancer,19(3), 123–124. [CrossRef]
- Yu, E. (2020). Occupational Exposure in Health Care Personnel to Antineoplastic Drugs and Initiation of Safe Handling in Hong Kong. Journal of Infusion Nursing, 43(3), 121–133. [CrossRef]
Figure 1.
Flow diagram of literature search.
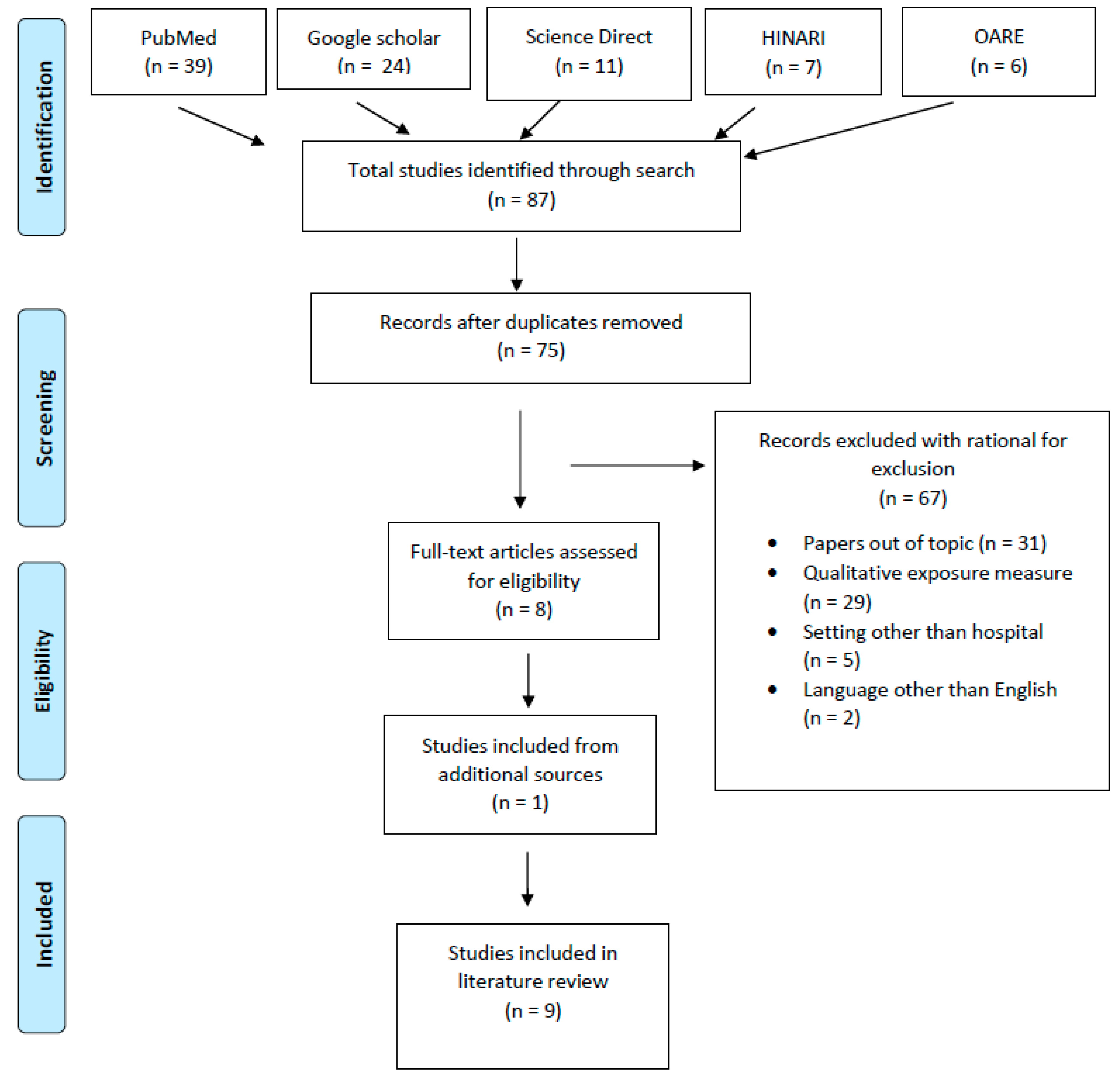

Table 1.
Drug concentrations detected in biological samples among healthcare workers.
| Study | Metdod | Study population (number) | Exposure drug assessed relevant to tdis review |
Number of persons exposed/ samples tested |
Limit of detection (LOD) | Results | Prevalence ratio |
| (Ae et al., 2003) |
Cross sectional | Nurses (87) Pharmacists (13) |
CP IFO |
100 persons exposed 670 samples tested: Nurses (589) Pharmacists (81) |
CP: 0.04 mcg/L IFO: 0.05 mcg/L |
Urine samples tested (670): Nurses: 11 positive samples for either CP or IFO Pharmacists: 31 positive samples for either CP or IFO CP: 72 samples >LOD IFO: 20 samples >LOD The concentrations of CP in urine ranged from 0.05 to 0.76 mcg/L, and IFO peaked at 1.90 mcg/L. |
Nurses: 0.02 (2%) Pharmacists: 0.38 (38%) Samples >LOD for CP: 0.11 (11%) Samples >LOD for IFO: 0.03 (3%) CP>IFO |
| (Hedmer et al., 2008) |
Cross sectional |
Nurses (15) Pharmacists (3) Other (4) |
CP IFO |
22 persons exposed |
CP: 10 ng/L IFO: 30 ng/L |
Drugs handled during biological monitoring: Nurses CP: average of 1.1g/day (range 0-5g) IFO: average of 2.4g/day (range 0-20g) Pharmacists CP: average of 12 g/day (range 2–36 g) IFO: average of 24 g (range 0–25 g) Drugs detected in urine during biological monitoring: Nurses: no CP/IFO detected in urine Pharmacists: no CP/IFO detected in urine |
Samples > LOD in urine: 0 Handling: IFO>CP Pharmacists>nurses |
| (Hon et al., 2015) |
Cross sectional | Nurses (29) Pharmacists (43) Others (31) |
CP | 103 persons, 98 provided a second sample, for a total of 201 urine samples |
CP: 0.05 ng/mL | Urinary concentrations of CP (in ng/mL): Slightly more than half of the samples (55 %) had CP levels greater than the LOD with a maximum reported concentration of 2.37 ng/mL The mean urinary CP concentration was 0.156 ng/mL |
Nurses: 0.56 (56%) of samples were >LOD Pharmacists: 0.44 (44%) of samples were >LOD |
| (Sottani et al., 2012) | Cross sectional | Nurses (78) Pharmacists (22) |
CP IFO |
100 persons | Not stated | CP or IFO not detected in urine | CP: 0 IFO: 0 |
| (Baniasadi et al., 2018) | Cross sectional | Nurses Nursing assistant |
CP IFO |
30 (1 sample per person) | Not stated | CP: 14 samples had detectable levels IFO: 5 samples had detectable levels CP and IFO concentrations were highest among nurses that administered these drugs |
CP: 0.466 (46.66%) IFO: 0.066 (6.66%) |
Table 2.
Surface contamination with Cyclophosphamide (CP), Methotrexate (MTX), and Ifosfamide (IFO) in the hospital setting.
Table 2.
Surface contamination with Cyclophosphamide (CP), Methotrexate (MTX), and Ifosfamide (IFO) in the hospital setting.
| Study | Metdod | Study population/ area |
Exposure drug assessed relevant to tdis review |
Surface samples collected | Limit of detection (LOD) | Results | Prevalence ratio |
| (Graeve et al., 2017) |
Cross sectional | Nursing station Physician work area Pharmacy |
CP MTX IFO |
62 | CP: 0.015 ng/cm2 MTX: 0.005 ng/cm2 IFO: 0.005 ng/cm2 |
Five (5) samples tested above the limit of detection for different antineoplastic agents Nursing station areas: 4 samples > LOD IFO >LOD in 3 samples at 0.06 ng/cm2 MTX was <LOD 1 sample tested above the LOD for a neoplastic agent not in this review Physician workroom areas: CP and IFO were <LOD Pharmacy areas: CP was <LOD 1 sample tested above the LOD for an antineoplastic agent not in this study |
Samples >LOD: 0.08 (8%) Nursing station samples >LOD: 0.06 (6%) Physician workroom samples >LOD: 0 Pharmacy area samples >LOD: 0.02 (2%) IFO>CP & MTX |
| (Hedmer et al., 2008) |
Cross sectional |
Oncology wards (231) Pharmacy (104) |
CP IFO |
335 | CP: 0.02 ng per wipe sample IFO: 0.05 ng per wipe sample |
Wipe sampling: Hospital oncology wards CP: ranged from not detectable (ND) – 3800pg cm2 IFO: ranged from ND – 2700pg cm2 Hospital pharmacy floor and work area CP: ranged from 2.2 – 45pg cm2 IFO: ranged from 11 – 78pg cm2 Measurable amounts of CP and IF were detected on most of the sampled surfaces |
Wards: 0.86-1.0 (86-100%) of samples were > LOD for CP 0.29-1 (29-100%) of samples were >LOD for IFO Pharmacy: 1.0 (100%) of samples were > LOD for both CP & IFO |
| (Ramphal et al., 2015) |
Cross sectional | Oncology pharmacy Main pharmacy (control) |
CP MTX IFO |
Not stated | Not stated | Wipe sampling before cleaning in oncology pharmacy CP: 0.08ng/cm2 MTX: 0.66ng/cm2 IFO: not measured Wipe sampling after cleaning in oncology pharmacy CP: ND-0.04ng/cm2 MTX: 0.25ng/cm2 IFO: 0.009ng/cm2 Wipe sampling in main pharmacy (control) CP: ND MTX: ND IFO: ND The before-cleaning surface wipes from the oncology pharmacy revealed CP contamination in 3 of 5 areas tested and MTX contamination in 1 of 6 areas tested |
CP: 0.6 (60%) MTX: 0.17 (17%) |
| (Dugheri et al., 2018) | Cross sectional | Nine (9) hospitals across Italy | CP MTX IFO |
4814 | Not stated | 1583 (32%) were above the LOD CP: 864 positive samples IFO: 762 positive samples MTX: 28 positive samples |
CP: 17.2% IFO: 15.4% MTX: 0.8% CP>IFO>MTX |
| (Sottani et al., 2012) | Cross sectional | Eight (8) pharmacies Nine (9) patient areas |
CP IFO |
Not stated | Not stated | Samples contaminated with antineoplastic agent: CP: 54% of samples IFO: 19% of samples |
CP: 0.54 (54%) IFO: 0.19 (19%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



