Submitted:
19 February 2024
Posted:
19 February 2024
You are already at the latest version
Abstract
Synchronous electrical cardioversion is a relatively common procedure in the emergency department (ED), often performed for unstable supraventricular tachycardia (SVT) or unstable ventricular tachycardia (VT). However, it is also used for stable cases resistant to drug therapy, which carry a risk of deterioration. In addition to the inherent risks linked with procedural sedation, there is a possibility of malignant arrhythmias or bradycardia, which could potentially result in cardiac arrest following this procedure. Here, we present a case of complete heart block unresponsive to transcutaneous pacing and positive inotropic and chronotropic drugs for 90 minutes, resulting in multiple cardiac arrests. The repositioning of the transcutaneous cardio-stimulation electrodes, one of them placed in the left latero-sternal position and the other at the level of the apex, led to immediate stabilization of the patient. Extubation of the patient was performed the following day, while full recovery and discharge within 7 days, after insertion of a permanent pacemaker.
Keywords:
supraventricular tachycardia
; cardioversion
; unstable patient
; complete heart block
; ineffective pacing
; cardiac arrest
; advanced life support.
1. Introduction
Patients with symptomatic supraventricular arrhythmias commonly present in the emergency department (ED) necessitating urgent management. Sporadically, complications may arise, but there is a lack of comprehensive literature regarding post-cardioversion events for supraventricular tachycardia (SVT).
Traditionally, SVT encompasses all tachycardias except for ventricular tachycardias (VTs) and atrial fibrillation (AF), with atrial rates exceeding 100 beats per minute at rest [1]. Narrow QRS tachycardia is defined as QRS duration of 120 ms or less, while sometimes, they may display a widened QRS complex exceeding 120 ms, due to pre-existing conduction delays either related to heart rate, or to bundle branch blocks [1,2].
In the general population, the prevalence of SVT is 2.25 per 1000 individuals, with an incidence of 35 per 100,000 person-years [1]; evidence from the United States indicates that they contribute to approximately 50,000 ED visits each year [3]. However, epidemiological studies on SVT populations are limited. Women face twice the risk of developing SVT compared to men, while individuals aged 65 years or older have over five times the risk compared to younger counterparts [1].
The clinical presentations of SVT range extensively, spanning from asymptomatic cases to severe symptoms associated with hemodynamic instability and cardiogenic shock, which pose a risk to the patient's life. The assessment and management of all arrhythmias consider both the patient's condition and the characteristics of the arrhythmia. The goal is to prevent cardiac arrest.
Therefore, the initial approach in the ABCDE assessment involves identifying the patient's adverse features, such as shock, syncope, acute heart failure, and myocardial ischemia. Additionally, it is essential to consistently monitor the rhythm, blood pressure, and administer oxygen if SpO2 falls below 94%. Identifying and addressing reversible causes, such as electrolyte imbalances or hypovolemia, should be conducted in accordance with the 2021 European Resuscitation Council (ERC) Guidelines [4]. If these signs are absent in a patient with regular tachycardia, vagal maneuvers will be performed, with the inverted Valsalva maneuver demonstrated to be more efficient in adults [1]. In the ED, the standard protocol includes conducting a thorough history, physical examination, and a 12-lead ECG, supplemented by usual laboratory tests such as full blood counts, biochemistry profile, and thyroid function assessment. If feasible, transthoracic echocardiography should also be conducted.
If vagal maneuvers fail to resolve the issue, according to the 2019 ESC Guidelines on Supraventricular Tachycardia [1] and 2021 ERC Guidelines [4], the initial drug of choice is adenosine (6-12-18 mg). If adenosine proves ineffective, intravenous verapamil, diltiazem, or beta-blockers are the subsequent treatment options for narrow complex SVT, while intravenous procainamide or amiodarone are recommended for wide complex SVT. If these treatments are ineffective, synchronized cardioversion up to three attempts is advised to terminate the tachycardia. Having a stable patient provides the advantage of granting the emergency physician the opportunity to seek expert advice for both the differential diagnosis of SVT and its treatment if initial measures prove unsuccessful.
For unstable patients exhibiting life-threatening features, synchronized cardioversion with up to three attempts under sedation is the treatment of choice. If unsuccessful, administering intravenous amiodarone at a dose of 300 mg over 10-20 minutes or intravenous procainamide at a dose of 10-15 mg/kg over 20 minutes is recommended, followed by repeating synchronized shocks, if necessary [1,4].
When selecting the appropriate method for cardioversion, it is important to follow the current guidelines and carefully weigh the potential benefits and risks associated with each intervention. Sometimes, the patient is at the threshold of receiving either electrical or drug cardioversion and requires a prompt decision to distinguish between the two, given that both interventions carry inherent risks. Ventricular fibrillation (VF) as a complication of electrical cardioversion has been documented in numerous studies, particularly when cardioversion takes place during the vulnerable period of repolarization, typically around the peak of the T wave on the ECG [5,6]. In 2004, Lyndon and Abdul described such a case, highlighting the significance of adjusting the lead configuration on the defibrillator monitor to prevent mistaking the high T wave for the R wave, thereby averting the induction of VF during the administration of synchronous external electric shock [6]. Gronberg et al. also documented in FinCV study arrhythmic complications following electrical cardioversion among patients experiencing acute atrial fibrillation [7].
Sinus bradycardia or a slow junctional escape rhythm was reported in 22 cases after electrical cardioversion by Gallagher et al., with 20 resolving within minutes after procedure, and two patients requiring permanent pacing. They also studied the incidence of VF, non-sustained broad complex tachycardia and atrial fibrillation following shocks [8].
Here we describe a case of a patient requiring electrical cardioversion for SVT. Following the synchronized shock, the patient experienced severe bradycardia, subsequently progressing to complete heart block unresponsive to medication and pacing, culminating in cardiorespiratory arrest.
2. Case Presentation
A 53-year-old male patient, known smoker with no other comorbidities except for a right bundle branch block (RBBB), arrived at the ED via a physician-staffed ambulance. The patient presented with main complaints of palpitations and fatigue that started approximately 8 hours before arrival, along with diaphoresis and dyspnea exacerbated by minimal efforts, particularly in the last hour.
Before reaching the hospital, a 12-lead ECG (Figure 1) and vital signs monitoring were conducted, revealing SVT with RBBB, a heart rate of 174 BPM, SpO2 at 98%, and blood pressure of 130/80 mmHg. Deeming the patient's condition stable, the emergency physician attempted vagal maneuvers, which had no effect on the heart rate. Adenosine was administered in three doses (6mg, 12mg, 18mg), also with no impact on the patient's condition. After a 30-minute period during which 10mg of Metoprolol was slowly intravenously administered without success, the decision was made to transfer the patient to the ED.
Upon arrival at the ED, the patient appeared conscious and cooperative, but he was pale, diaphoretic, and exhibited dyspnea at rest. Vital signs indicated a peripheral oxygen saturation of 93%, blood pressure at 90/60 mmHg, heart rate of 174 BPM, capillary refill time of 3 seconds, and a barely detectable radial pulse. The ECG showed SVT with RBBB, as seen in Figure 2.
The patient was administered supplemental oxygen at a rate of 3L/min, blood work-up and arterial blood gas analysis was conducted (Table 1). After approximately 30 minutes, it was decided that synchronous cardioversion with 70 Joules was the optimal course of action. The patient provided consent for the procedure and was sedated beforehand.
Following the initial synchronous shock, the patient experienced severe bradycardia (Figure 3) for a few seconds, transitioning into asystole. Immediate resuscitation measures, including chest compressions and bag-mask ventilation, were initiated. After about 30 seconds, the patient exhibited spontaneous breathing and movement of limbs, opened his eyes, and responded to verbal stimuli.
A repeated ECG recording revealed 3rd degree AV block (Figure 4), with a heart rate of 23 BPM, and the patient was hemodynamically unstable. Intravenous Atropine 0.5 mg was administered, followed by additional doses every 2 minutes, up to a maximum of 3 mg. Simultaneously, Adrenaline was administered via a syringe infusion pump with 2 mcg/min, with no improvement in the patient's condition. Transcutaneous pacing was initiated with a frequency set to "Demand" at 70 BPM, 80 mA intensity. Although the monitor indicated efficient capture, the femoral pulse was not concordant. Pacing parameters were adjusted to 70 BPM with an increase in intensity up to 160 mA and even 200 mA for short periods of time, yet the myocardium remained unresponsive to external pacing.
Despite efforts to improve hemodynamic stability, the transcutaneous pacing remained ineffective (Figure 5). The patient's thorax was shaved to enhance transcutaneous conduction, and the initial electrode position (right subclavian/cardiac apex) was changed to an antero-posterior and later to latero-lateral position. The Adrenaline dose was increased from 2 mcg/min to 20 mcg/min. Additionally, alternative medications, including Aminophylline 24 mg over 10 minutes and Dopamine via a syringe infusion pump at 10 mcg/kg/min, were administered.
Throughout the patient's stay in the ED, he experienced cardiopulmonary arrest at least 10 times, manifesting as either asystole or pulseless electrical activity. Each time, the patient responded positively to external thoracic compressions, mechanical ventilation, and Adrenaline administration, achieving a return of spontaneous circulation in less than 2 minutes.
The on-call physician at the regional Institute for Cardiovascular Diseases was contacted and agreed to admit the patient once his condition would be stable for transport. Despite exhausting all available treatment options in the ED (which lacked equipment for transvenous pacing), the patient continued to experience severe hypotension between cardiopulmonary arrest episodes due to the unresponsiveness to transthoracic cardio-stimulation. Considering the inefficacy of pacing, attributable to the patient's thoracic anatomy with a large anterior-to-posterior diameter, a decision was made to reposition the transthoracic pacing leads to subclavicular left (latero-sternal) and cardiac apex (replacing ECG lead V6) positions (Figure 6). Upon reassessment, the change in lead position resulted in successful pacing capture, confirmed by femoral artery pulse and an increase in blood pressure values.
Approximately 90 minutes after the initial cardioversion attempt, the patient's stability allowed for transportation to the regional Institute for Cardiovascular Diseases for transvenous pacing. The final evaluation indicated a blood pressure of 115/50 mmHg, heart rate of 70 BPM, consistent femoral pulse, GCS of 3 with the patient mechanically ventilated under continuous sedative medication and receiving inotropic and vasopressor medication (Adrenaline and Dopamine). Emergency transthoracic echocardiography showed a left ventricle of normal size with preserved systolic function, an ejection fraction of 50%, medio-basal hypokinesia of the lateral wall, concentric left ventricular hypertrophy, grade II mitral and tricuspid regurgitation, medium secondary pulmonary hypertension, dilated right ventricle, and a posterior pericardial fluid blade measuring below 1 cm.
Upon arrival at the regional Institute for Cardiovascular Diseases, the patient's condition improved with the placement of the transvenous pacing probe, later replaced with a permanent pacemaker implant. The following day, the patient was extubated, demonstrating complete hemodynamic and neurologic recovery, and was discharged from the hospital a week later.
4. Discussion
Synchronized cardioversion, a potentially life-saving procedure, is commonly utilized in the emergency department for hemodynamically unstable tachyarrhythmias. Emergency physicians should possess a thorough understanding of the indications and potential complications before recommending or performing this intervention.
In our scenario, the patient was presented with recent-onset palpitations lasting several hours, and appropriate drug therapy had already been administered in prehospital settings. Given the unavailability of intravenous verapamil or diltiazem in our region, the only remaining option for terminating the tachycardia was electrical cardioversion. Considering the patient's known history of right bundle branch block, the tachycardia was managed as SVT. Chronologically, the decision to proceed with electrical cardioversion was made over an hour after the last bolus of metoprolol, during which time no significant reduction in heart rate was observed.
Severe bradycardia, immediately followed by complete heart block and subsequent cardiac arrest with pulseless electrical activity, was an unexpected and rarely reported complication of synchronized cardioversion. Similar outcomes were described by Gallagher et al., who conducted a retrospective cohort study examining the relationship between shock energy and arrhythmic complications of electrical cardioversion. Sinus bradycardia or a slow junctional escape rhythm was observed in 22 cases, with 20 resolving within minutes after cardioversion. While two patients required permanent pacing before hospital discharge, neither needed rate support while awaiting pacemaker implantation. None of these patients experienced cardiac arrest. They also found that the incidence of ventricular fibrillation (VF) following shocks of < 200 J was significantly higher compared to higher energy shocks (5 out of 2959 vs. 0 out of 3439 shocks, p = 0.021). Additionally, non-sustained broad complex tachycardia occurred in four cases, all lasting less than 10 seconds: two after shocks > 200 J, and two after shocks less than 200 J. The induction of atrial fibrillation (AF) was significantly more common with shocks of < 200 J (20 out of 930 shocks vs. 1 out of 313 shocks at ≥ 200 J, p = 0.015) [8].
The success of cardioversion relies on several factors, with time being the most crucial. In our case, the patient had been experiencing symptoms for several hours, and the initial EKG recording, which revealed SVT with a heart rate of 174, was conducted more than three hours prior to arriving at the ED. Nevertheless, the patient initially declined to come to the hospital. The prolonged duration of the tachyarrhythmia could potentially lead to both post-repolarization and conduction delays due to global ischemia, as described in other studies, which have reported VF as a complication following cardioversion for AF [9,10].
Furthermore, a proposed theory regarding the mechanism of complete heart block in our patient was the administration of intravenous metoprolol before cardioversion, given that beta blockers are known as drugs with sinoatrial and/or atrioventricular nodal–blocking properties [11]. In a retrospective and prospective study conducted by Osmonov et al. involving 108 patients treated with atrioventricular blockers and presenting symptomatic type II second- or third-degree AV block, 2:1 AV block, atrial fibrillation, and bradyarrhythmia, it was found that 36 patients treated with metoprolol experienced metoprolol-induced AV blocks that persisted or recurred in 24 patients [12].
However, the maximum therapeutic dose of 15 mg (recommended by ESC guidelines, American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society for stable SVT) [1,11] was not achieved in our patient; only 10 mg was administered intravenously in 2.5 mg boluses, with no discernible effect on heart rate following the last bolus. This hypothesis was considered due to the lack of effectiveness of the transcutaneous pacing assuming the patient had a stronger response to beta-blockers. Unfortunately, glucagon, the antidote for beta-blocker overdose, was unavailable at the time in any of the hospitals in the area preventing us to assess this hypothesis.
Also, myocardial ischemia or metabolic disturbances such as acidosis and hypoxia were described as factors that can elevate the pacing threshold and potentially prevent capture [13]. Our patient experienced both metabolic acidosis and severe hypoxemia in the period following cardioversion, conditions that were rectified only after successful cardiac pacing.
Successful capture is typically identified by a widened QRS complex, succeeded by a clear ST segment and broad T wave. A pulse rate manually confirmed in femoral artery or right carotid artery notably lower than the pacing rate displayed on the pacing unit monitor may suggest a lack of capture [13].
In our case, achieving efficient capture required placing the electrodes closer together. While we cannot definitively assert that this positional change was the sole factor stabilizing the patient, given the limited application to only one patient, it proved to be the sole measure in a unique and critical situation that yielded an immediate positive effect, leading to a sudden improvement in the patient's condition. Consequently, we cannot consistently advocate or recommend this procedure in routine practice. However, in similar situations where other well-known methods prove ineffective and the patient's condition continuously deteriorates, as exemplified in our case, it may be considered as a life-saving measure.
5. Conclusions
Cardiac arrest and complete heart block are uncommon complications following electrical cardioversion. Given the infrequency of capture failure cases with transcutaneous pacing, addressing each isolated case can provide significant benefits to both the ED and prehospital staff, particularly in the management of atypical situations.
Author Contributions
Conceptualization, A.M.M.; methodology, A.M.M. and C.B.; software, A.C.C.; validation, C.B., C.I.T. and A.P.; investigation, A.M.M., A.H. and C.I.T.; resources, A.M.M.; data curation, A.M.M.; writing—original draft preparation, A.M.M. and A.P.; writing—review and editing, A.M.M., D.S., C.B., A.C.C., A.H., A.P.; visualization, D.S. and A.C.C.; supervision, A.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Emergency Clinical Municipal Hospital from Timisoara, Romania (number 10050/12.04.2023).
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Brugada, J.; Katritsis, D.G.; Arbelo, E.; Arribas, F.; Bax, J.J.; Blomström-Lundqvist, C.; Calkins, H.; Corrado, D.; Deftereos, S.G.; Diller, G.-P.; et al. 2019 ESC Guidelines for the Management of Patients with Supraventricular TachycardiaThe Task Force for the Management of Patients with Supraventricular Tachycardia of the European Society of Cardiology (ESC). Eur Heart J 2020, 41, 655–720. [Google Scholar] [CrossRef] [PubMed]
- Bibas, L.; Levi, M.; Essebag, V. Diagnosis and Management of Supraventricular Tachycardias. Can Med Assoc J 2016, 188, E466–E473. [Google Scholar] [CrossRef] [PubMed]
- Murman, D.H.; McDonald, A.J.; Pelletier, A.J.; Camargo, C.A. U.S. Emergency Department Visits for Supraventricular Tachycardia, 1993–2003. Academic Emergency Medicine 2007, 14, 578–581. [Google Scholar] [CrossRef] [PubMed]
- Current ERC Guidelines. Available online: https://cprguidelines.eu/ (accessed on 31 January 2024).
- Ebrahimi, R.; Rubin, S.A. Electrical Cardioversion Resulting in Death from Synchronization Failure. Am J Cardiol 1994, 74, 100–102. [Google Scholar] [CrossRef] [PubMed]
- Xavier, L.C.; Memon, A. Synchronized Cardioversion of Unstable Supraventricular Tachycardia Resulting in Ventricular Fibrillation. Ann Emerg Med 2004, 44, 178–180. [Google Scholar] [CrossRef] [PubMed]
- Grönberg, T.; Nuotio, I.; Nikkinen, M.; Ylitalo, A.; Vasankari, T.; Hartikainen, J.E.K.; Airaksinen, K.E.J. Arrhythmic Complications after Electrical Cardioversion of Acute Atrial Fibrillation: The FinCV Study. EP Europace 2013, 15, 1432–1435. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, M.M.; Yap, Y.G.; Padula, M.; Ward, D.E.; Rowland, E.; Camm, A.J. Arrhythmic Complications of Electrical Cardioversion: Relationship to Shock Energy. Int J Cardiol 2008, 123, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Sucu, M.; Davutoglu, V.; Ozer, O. Electrical Cardioversion. Ann Saudi Med 2009, 29, 201–206. [Google Scholar] [CrossRef] [PubMed]
- SIMS, J.J.; MILLER, A.W.; UJHELYI, M.R. Regional Hyperkalemia Increases Ventricular Defibrillation Energy Requirements. J Cardiovasc Electrophysiol 2000, 11, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Page, R.L.; Joglar, J.A.; Caldwell, M.A.; Calkins, H.; Conti, J.B.; Deal, B.J.; Estes, N.A.M.; Field, M.E.; Goldberger, Z.D.; Hammill, S.C.; et al. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia: Executive Summary. Circulation 2016, 133. [Google Scholar] [CrossRef]
- OSMONOV, D.; ERDINLER, I.; OZCAN, K.S.; ALTAY, S.; TURKKAN, C.; YILDIRIM, E.; HASDEMIR, H.; ALPER, A.T.; CAKMAK, N.; SATILMIS, S.; et al. Management of Patients with Drug-Induced Atrioventricular Block. Pacing and Clinical Electrophysiology 2012, 35, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Doukky, R.; Bargout, R.; Kelly, R.F.; Calvin, J.E. Using Transcutaneous Cardiac Pacing to Best Advantage: How to Ensure Successful Capture and Avoid Complications. J Crit Illn 2003, 18, 219–225. [Google Scholar] [PubMed]
Figure 1.
ECG from the ambulance.
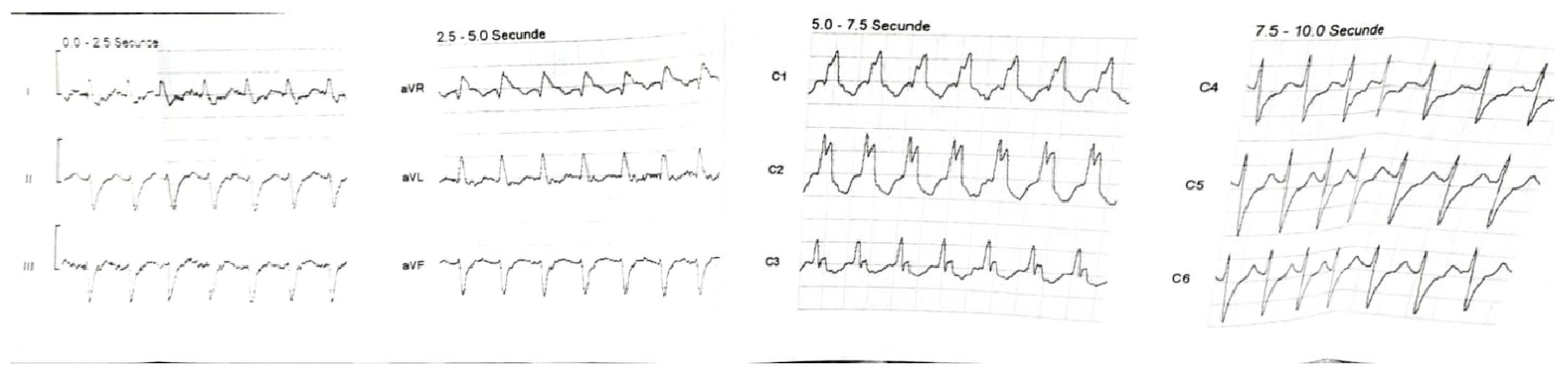
Figure 2.
First ECG from ED – SVT with RBBB.
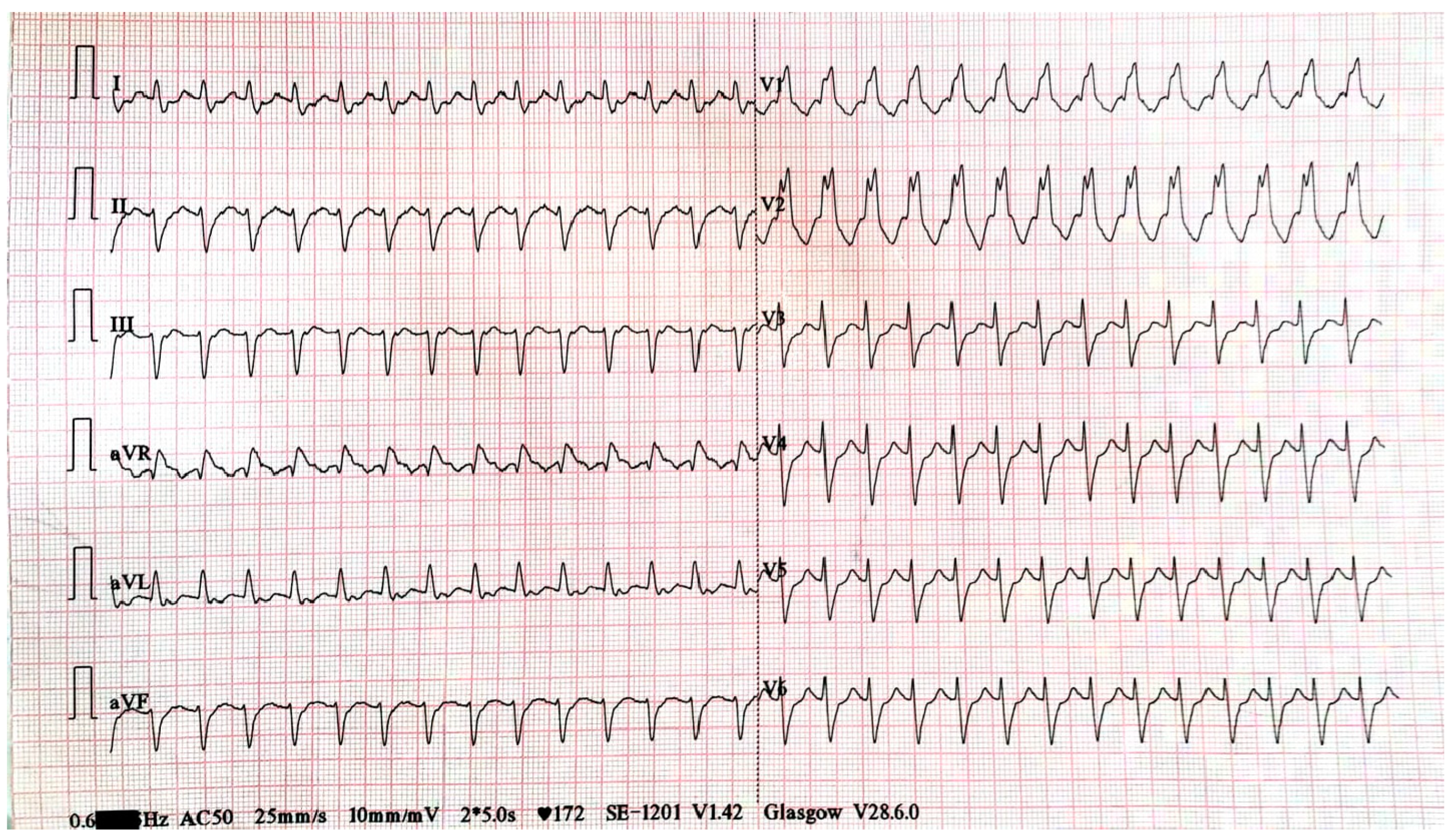
Figure 3.
The defibrillator's rhythm recording during the electrical cardioversion.
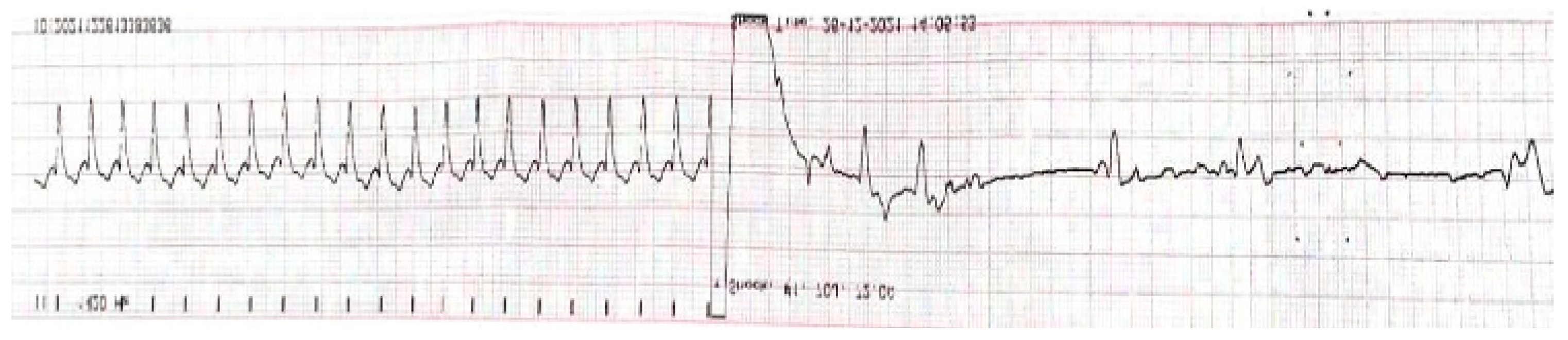
Figure 4.
Complete heart block after ROSC.
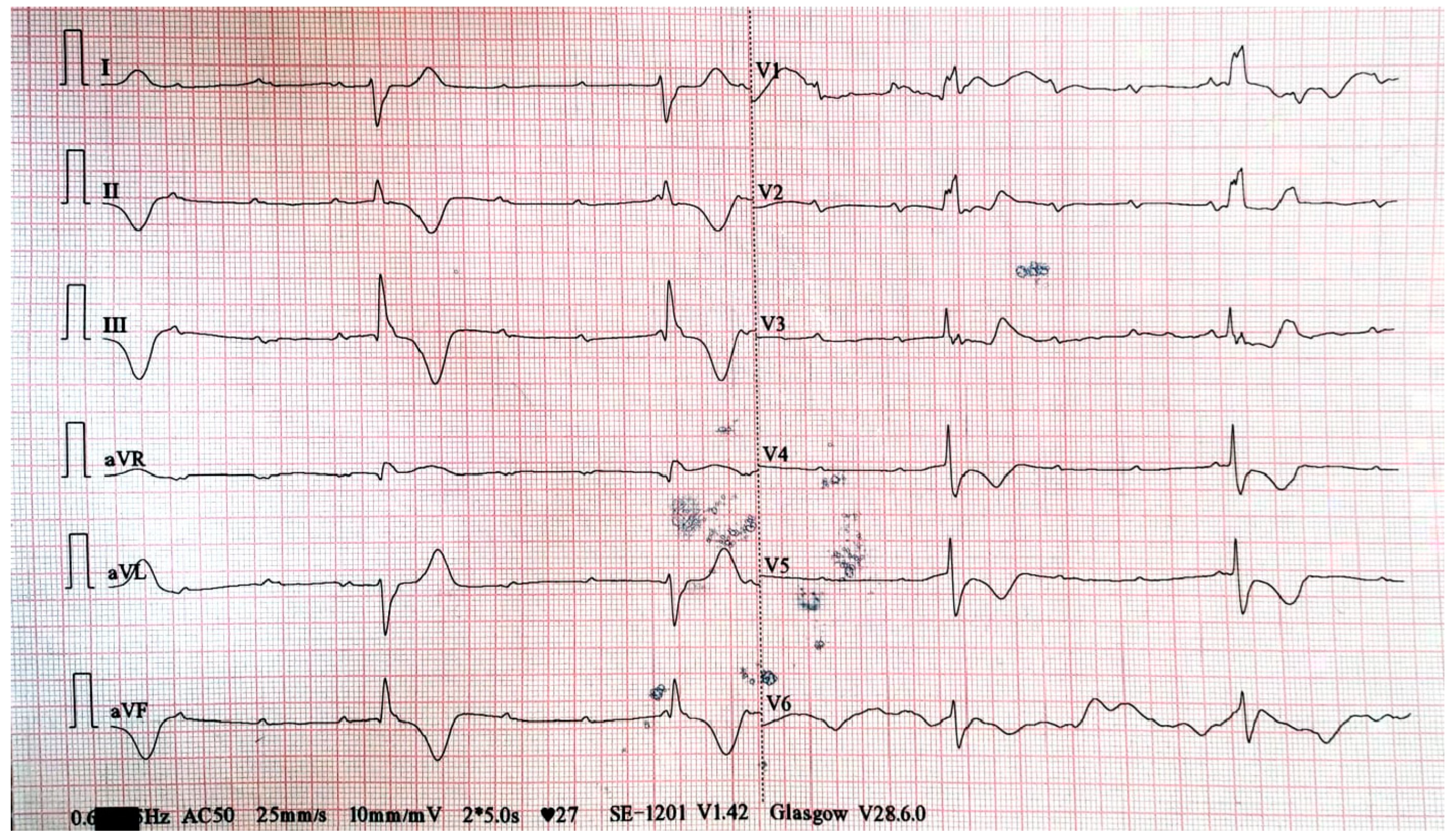
Figure 5.
Transcutaneous pacing with ineffective capture and inconsistent femoral pulse.

Figure 6.
Placement of both transcutaneous stimulation electrodes on the left hemithorax: subclavicular left (latero-sternal) and cardiac apex (replacing ECG lead V6) positions.
Figure 6.
Placement of both transcutaneous stimulation electrodes on the left hemithorax: subclavicular left (latero-sternal) and cardiac apex (replacing ECG lead V6) positions.
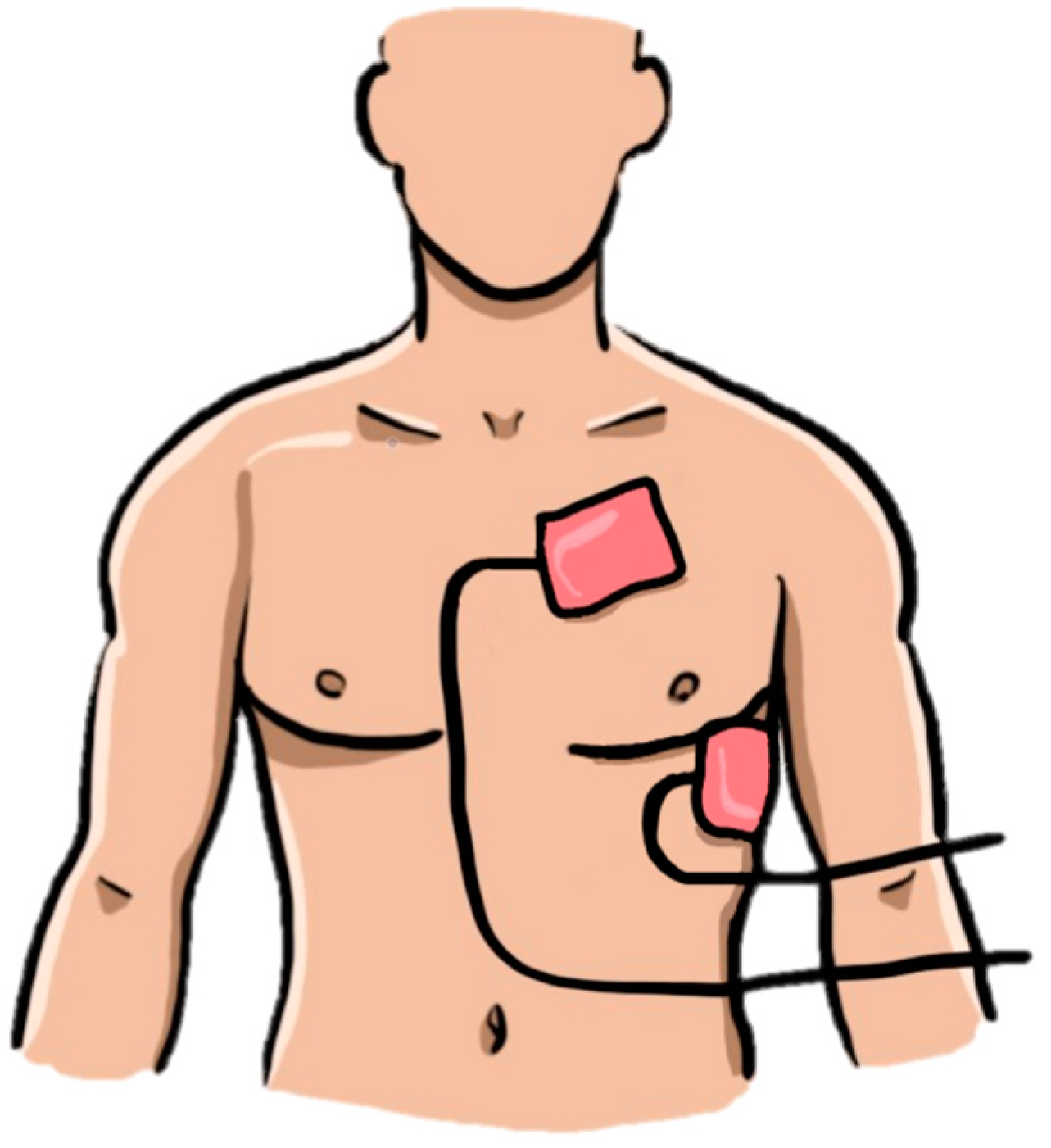

Table 1.
Pathological values of the laboratory tests performed upon arrival in the ED.
| Laboratory Test | Value | Reference Range Value | Conventional Units |
|---|---|---|---|
| White blood cells | 11.1 | 4.0-10.0 | ×109/µL |
| Creatinine | 1.52 | 0.70-1.30 | mg/dl |
| Blood glucose | 146 | 74-106 | mg/dl |
| D-dimer | 1.89 | 0-0.68 | mg/L |
| NT-pro-BNP | 10217 | 0-125 | pg/ml |
| Troponin I | 58.2 | 17-50 | ng/L |
| Lactate | 2.52 | 0.36-0.75 | mmol/L |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



