Submitted:
16 February 2024
Posted:
19 February 2024
You are already at the latest version
Abstract
Study design: Retrospective cohort study. Objectives: To investigate the outcomes of early ballon kyphoplasty (BKP) intervention compared with late intervention for osteoporotic vertebral fracture. Background: Osteoporotic vertebral fractures, can lead to kyphotic deformity, severe back pain, depression, and disturbances in activities of daily living (ADL). BKP has been widely utilized to treat symptomatic OVFs and has proven to be a very effective surgical option for this condition. BKP is relatively a safe and effective method due to less acrylic cement leakage and greater kyphosis correction. Materials and Methods: A retrospective comparative study was conducted at our hospital for patients who underwent BKP for osteoporotic vertebral fractures in the time frame between January 2020 and December 2022. Ninety-nine patients were included in this study, patients were classified into two groups: 36 patients underwent early BKP intervention (EI)
Keywords:
Ballon Kyphoplasty
; osteoporotic vertebral fractures
; kyphosis
1. Introduction.
Osteoporosis is increasing dramatically with the aging of the global population [1]. Osteoporosis-related fractures, such as femoral neck fractures, distal radius fractures, and vertebral fractures, are primary concerns for the elderly [2]. Furthermore, these fractures may increase the morbidity and mortality risk among osteoporotic patients [3]
Osteoporotic vertebral fractures (OVFs), the most common osteoporosis-related fractures, can lead to kyphotic deformity, severe back pain, depression, and disturbances in activities of daily living (ADL). Percutaneous balloon kyphoplasty (BKP) has been widely utilized to treat symptomatic OVFs and has proven to be a very effective surgical option for this condition [6]. Compared with simple percutaneous cement injection, BKP is a relatively safe and effective method due to less acrylic cement leakage and greater kyphosis correction [7,8].
According to current guidelines, patients are primarily recommended to undergo conservative treatment for osteoporotic vertebral fractures. Surgical intervention is recommended when conservative treatments are ineffective clinically or if there is radiographic progression of the fracture [9]. However, prolonged bed rest in the elderly may lead to complications such as dementia progression, bed sores, deep venous thrombosis, hypostatic pneumonia, progression to deformity and further progression of osteoporosis, [10]. Determining the appropriate duration of conservative therapy is crucial for symptomatic osteoporotic vertebral fractures to achieve clinical benefit [11].
Current guidelines lack consensus recommendations for the timing of percutaneous balloon kyphoplasty (BKP) [12,13]. Therefore, we did retrospective comparative cohort study to investigated clinical and radiographic outcomes, as well as complications, associated with early intervention of PKP to provide current evidence for spine surgeons.
2. Materials and Methods
This research was approved by the ethics committee of our institution (No. 472), and informed consent from patients undergoing surgery was duly obtained. A retrospective evaluation was conducted for patients who underwent percutaneous balloon kyphoplasty (PKP) for osteoporotic vertebral fractures (OVFs) at our hospital in the time frame between January 2020 and December 2022. The inclusion criteria for this research were as follows: 1) Presence of osteoporotic vertebral fractures, 2) Bone mineral density: T-score <1.5 SD, 3) Underwent balloon kyphoplasty. Exclusion criteria included : 1) Severe spinal deformity ( scoliosis , SVA >10cm) , 2) >1 level balloon kyphoplasty, 3) < Six months follow-up, 4) Inability to provide valid VAS scores, 5) History of spinal tumor (Figure 1), 6) Severe physical illness.
2.1. Clinical evaluation
The cohort of patients underwent clinical assessment using standard quantifiable measures including the visual analogue scale (VAS) for low back pain and the Oswestry Disability Index (ODI) for daily living activities. Clinical data were documented preoperatively, postoperatively, and at final follow-up time periods. Surgical duration and any complications, such as sensory motor deficits, surgical site infections, and the need for revision surgery, were noted during the intraoperative or postoperative periods. The visual analog scale (VAS) for back pain was used to assess clinical outcomes.
2.2. Radiological evaluation
For radiological evaluation, parameters such as the local kyphosis angle (LKA), vertebral kyphotic angle (VKA), cement leakage, and adjacent vertebral fractures (AVFs) were calculated preoperatively and postoperatively with plain radiographs. Additionally, preoperative bone mineral density (BMD) T-score and fracture level were evaluated.
2.3. Statistical evaluation
All collected data were expressed as means ± standard deviations (SDs). In comparing the groups, the Mann-Whitney U test analysis was used for continuous variables, while the chi-squared test and Fisher's exact test were used for dichotomous variables. McNemar's test was used to compare the p-values. A p-value < 0.05 was defined as statistically significant. ficant. All analyses were performed using SPSS version 19.0 (IBM, Beijin, China).
2.4. Surgery.
All procedures were conducted using a standardised kyphoplasty technique with patients under general anesthesia and positioned in the prone position. Balloon kyphoplasty (BKP) was consistently performed through the percutaneous transpedicular route bilaterally under C arm guidance ,using conventional kyphoplasty instrumentation with same cement in all patients (Kyphon Ballon Kyphoplasty System, Medtronic, Minneaplis, USA).
3. Results.
3.1. Clinical results
Ninety-nine patients were included in the study after meeting the criteria, and they were divided into two groups: an early intervention group (Group EI, <4 weeks) and a late intervention group (Group LI, ≥4 weeks). Group EI consisted of 11 male and 25 female patients with an average age of 81.8 ± 5.0 years, while Group LI consisted of 25 male and 38 female patients with an average age of 80.1 ± 8.2 years.The mean follow-up period for Group EI was 11.2 ± 7.4 months, while for Group LI it was 12.1 ± 9.4 months. The patients' demographics are summarized in Table 1.
3.2. Radiographic results
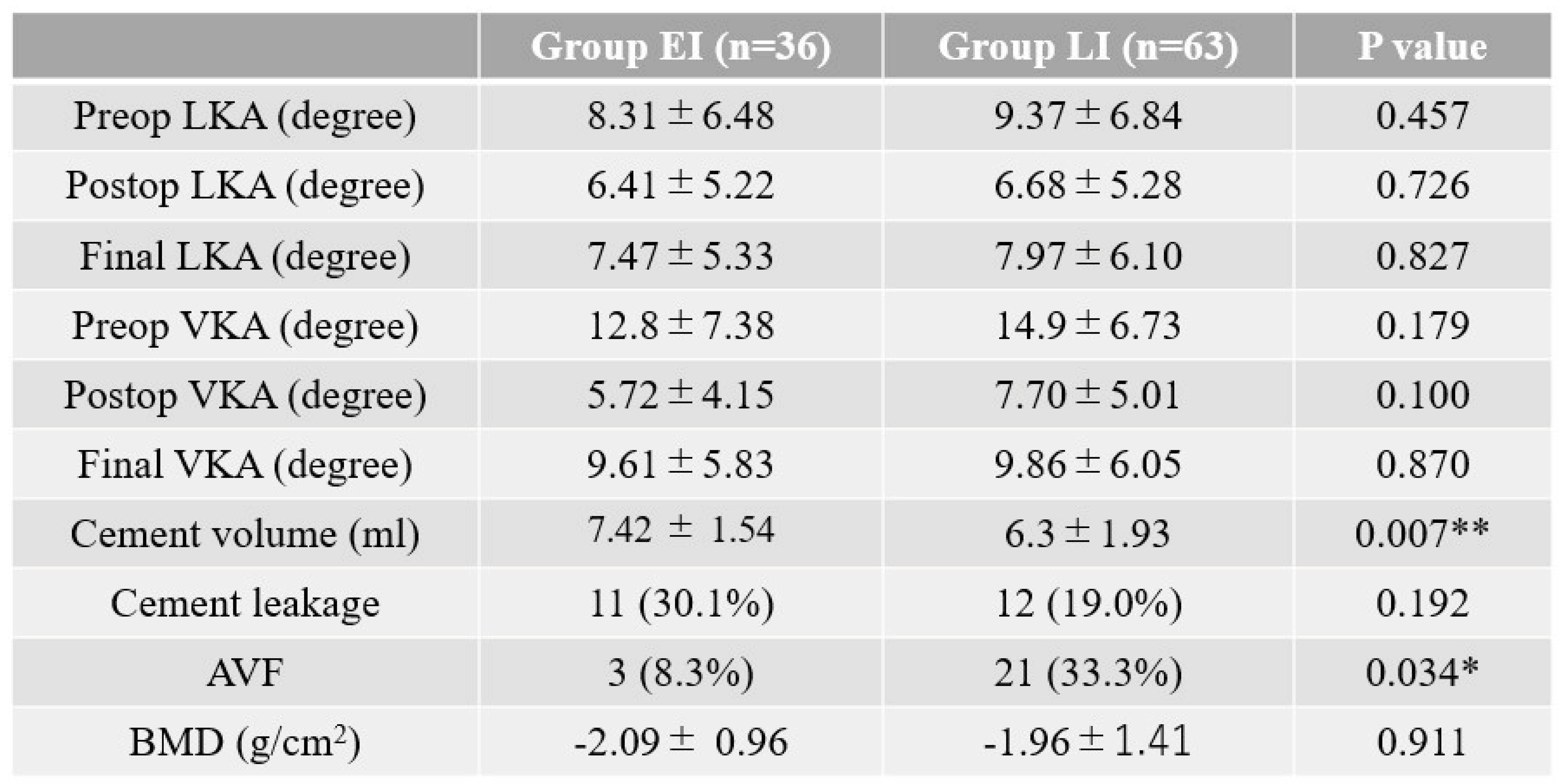
There was a significant improvement in postoperative vertebral angles (VKA) in both groups (Figure 2: p = 0.036, 0.00027). Adjacent segmental fractures (AVF) were more highly observed in the LI group compared to the EI group (Figure 3, 13.9% vs 33.3%, p = 0.034). Cement leakage was more highly observed in Group EI compared to Group LI, but the difference was not statistically significant (30.1% vs 19.0%, p = 0.192).
The level of fracture sites is summarized in Figure 4. The thoracolumbar area was the most common site of osteoporotic vertebral fractures in both groups.
Radiographic results are summarized in Table 3. In Group EI, the preoperative, postoperative, and final local kyphosis angles (LKAs) were 8.31 degrees, 6.41 degrees, and 7.47 degrees, respectively. In Group LI, the preoperative, postoperative, and final LKAs were 9.37 degrees, 6.68 degrees, and 7.97 degrees, respectively. There was no statistically significant difference between the two groups. Additionally, in Group EI, the preoperative, postoperative, and final vertebral kyphotic angles (VKAs) were 14.1 degrees, 6.5 degrees, and 11.1 degrees, respectively. In Group LI, the preoperative, postoperative, and final VKAs were 14.9 degrees, 7.7 degrees, and 10.4 degrees, respectively. Again, there was no statistically significant difference between the two groups (p = 0.35, 0.67, and 0.53). The bone mineral densities (BMDs) (T-score) of Group EI and Group LI were -2.1 and 1.6, respectively (p = 0.10), which was statistically insignificant.
4. Discussion
Osteoporotic vertebral fractures (OVFs) stand as the most prevailing fragility fractures. Studies indicate that about 25% of women aged over 70 years and over half of those aged above 80 years experience at least one OVF during their lifetime [14]. The elderly population most commonly experiences osteoporotic vertebral fractures (OVFs), resulting in significant pain and a notable decline in quality of life [15,16]. Conservative management, as well as percutaneous vertebroplasty (PVP), balloon kyphoplasty (BKP), and vertebral body stenting (VBS) are employed for their treatment [17]. Due to delayed diagnosis, inadequate awareness, and economic constraints, many patients opt for conservative treatment as their initial choice. Consequently, this delay in seeking vertebral body augmentation interventions, which can promptly alleviate pain and enhance functionality, ensues [10,18,19]. The mortality rate rises significantly in patients with osteoporotic vertebral fractures (OVFs), and this risk escalates with the number of affected vertebrae. Furthermore, for each diagnosed single OVF in a patient, the likelihood of subsequent fractures increases by a factor of five [20]. Despite adjusting for demographic characteristics and chronic comorbidities, the risk of mortality was 1.22 times higher in the OVFs. [21].
It is conceivable that fracture consolidation could restrict the possible height restoration if there is a lengthy period between the fracture and surgery. Percutaneous balloon kyphoplasty (BKP) is safe and helpful for patients with acute OVFs and ongoing discomfort. Following a percutaneous vertebroplasty, patients have rapid, long-lasting pain reduction that is affordable and far more than what would be possible with conservative care [2]. Important characteristics that set balloon kyphoplasty apart from percutaneous vertebroplasty are height restoration and decreased cement leakage [22]. Overall procedural complication incidents with vertebroplasty have been reported at 2.4% [23] as compared to 0.9% incidents with Kyphoplasty [7]. The best time to execute a balloon kyphoplasty has not been sufficiently investigated [8]. Some studies suggest a conservative treatment effort lasting two to three weeks, while others offer no advice at all about time [24,25].
In our study both early intervention (EI) and the late intervention (LI) groups demonstrated dramatic improvements in visual analogue scale (VAS) scores at final follow-up. However, no statistical differences were observed in final VAS scores between the EI and LI groups. This finding aligns with previous studies comparing outcomes based on different surgical timings of cement augmentation, where similar improvements in VAS scores were reported regardless of whether the operation was performed within 4 weeks or later. [13,26]. These consistent improvements in VAS scores suggest that the timing of BKP may not significantly impact pain outcomes in patients with OVFs. The similar pain outcomes in both early and late surgical intervention groups may be due to cement augmentation stabilizing micromovements and disrupting nerve endings, regardless of timing [27,28].
In terms of surgical times, we found a notable difference between groups EI (early intervention) and LI (late intervention). The mean surgical time for group EI was reported to be 30.2 ± 7.4 minutes, whereas it was 37.1 ± 8.9 minutes for group LI (Li et al., 2015). Our findings were supported by Li et al 2015 study [29]. Thoracolumbar area was the most common site of fracture for both the groups in the present study which was consistent with the results of a study by Oh et al. [8]. Our results demonstrated a significantly higher incidence of AVF in the LI group compared to the EI group (13.9% vs. 33.3%, p = 0.034). This finding suggests a potential association between delayed surgical intervention and an increased risk of adjacent segmental fractures, highlighting the importance of timely BKP in preventing such complications.
Our findings are consistent with previous retrospective studies that have investigated the impact of surgical timing on the risk of subsequent fractures following PKP or vertebroplasty [4,13,30,31]. The underlying mechanism of the vertebra recollapse remains unclear. The strain on neighboring vertebrae is increased by the significant kyphotic deformity of delayed BKP. AVFs have been linked to abnormal sagittal alignment of the vertebral bodies. In LI, endplate damage can result from repeated compressive pressure over the fracture site, which can cause bone loss close to the endplate. Repeated damage during everyday activities could cause a void to form above the LI fracture site. The incidence of AVFs may rise because of this void impact, which may also lessen the intergradient effect between the cement and bone. Extended bed rest in LI negatively impacts back muscles, leading to loss of muscle mass, which reduces vertebral body protection and increases the risk of further compression fractures [11]. This phenomenon is likely associated with changes in the local biomechanical environment that arise from kyphotic collapse of vertebral compression fractures [32].
The most frequent complication of kyphoplasty is the leakage of bone cement (PMMA), which can pose significant risks to patients, even when present in minimal amounts [7]. On the upper end of the spectrum, radiculopathy rates of 4% and cord compression rates of less than 0.5% have been reported [33]. Our results showed that cement leakage in the EI group compared to the LI group was not statistically significant. Interestingly, findings from another study. Huaquing guan et al [26] suggest that delayed operation may reduce the incidence of cement leaks. The rate of polymethylmethacrylate (PMMA) leakage is a subject of controversy and seems to be somewhat technique-dependent [34] or factors such as pressure, volume, and viscosity of the cement or technique used may play a more direct role in determining the risk of these types of leakage, rather than the timing of the surgical intervention [11]. One study suggests that reducing cement injection volume could potentially decrease cement leakage [35]. On the contrary, our study did not find a significant correlation between clinical outcomes and the volume of cement injected. We found that more cement could be injected in the early group. The volume of cement in early group was significantly more than that in late group. Both the EI and LI groups in our study exhibited improvements in VKAs from preoperative to final measurements. In our study, VKA in the final follow up in early group was slightly better than late group but there was no significant difference in it. While certain studies have demonstrated a notable improvement in VKA levels within the early treatment group compared to the late group [4,13,36]. While, similar to our study, the enhancement observed was not statistically significant in one study [6]. A larger retrospective study by Kaufmann et al. (2020) also did not find a significant association between injected cement volume and post-procedural pain [37] but the volume of injected cement was predicted factor of pain release [38].
It is important to acknowledge limitations of this study. As a retrospective study, its findings are subject to inherent biases. The short follow up and the relatively small sample size further constrain the generalizability of the results. Further research should investigate the biomechanics of adjacent fractures and the potential influence of gender on treatment outcomes.
Conclusions
In conclusion, early ballon kyphoplasty (BKP) may achieve better clinical and radiographic outcomes for treating osteoporotic vertebral fractures than delayed BKP. Early intervention BKP leads to more efficient surgical outcomes, including shorter operative times and reduced risk of subsequent vertebral fractures. Based on current evidence, early BKP intervention might be more beneficial to patients.
References
- Reginster JY, Burlet N. Osteoporosis: A still increasing prevalence. Bone 2006; 38:S4-S9. [CrossRef]
- Ploeg WT, Veldhuizen AG, The B, Sietsma MS. Percutaneous vertebroplasty as a treatment for osteoporotic vertebral compression fractures: A systematic review. Eur Spine J 2006; 15:1749-1758. [CrossRef]
- Johnell O. Advances in osteoporosis: Better identification of risk factors can reduce morbidity and mortality. J Intern Med 1996; 239:299-304. [CrossRef]
- Minamide A, Maeda T, Yamada H, et al. Early versus delayed kyphoplasty for thoracolumbar osteoporotic vertebral fractures: The effect of timing on clinical and radiographic outcomes and subsequent compression fractures. Clin Neurol Neurosurg 2018; 173:176-181. [CrossRef]
- to Y, Hasegawa Y, Toda K, Nakahara S. Pathogenesis, and diagnosis of delayed vertebral collapse resulting from osteoporotic spinal fracture. Spine J 2002; 2:101-106. [CrossRef]
- Takahashi S, Hoshino M, Terai H, et al. Differences in short-term clinical and radiological outcomes depending on timing of balloon kyphoplasty for painful osteoporotic vertebral fracture. J Orthop Sci 2018; 23:51-56. [CrossRef]
- Garfin SR, Yuan HA, Reiley MA. New technologies in spine: Kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine (Phila Pa 1976) 2001; 26:1511-1515.
- Oh GS, Kim HS, Ju CI, Kim SW, Lee SM, Shin H. Comparison of the results of balloon kyphoplasty performed at different times after injury. J Korean Neurosurg Soc 2010; 47:199-202. [CrossRef]
- Klazen CA, Lohle PN, de Vries J, et al. Vertebroplasty versus conservative treatment in acute osteoporotic vertebral compression fractures (Vertos II): An open-label randomised trial. Lancet 2010; 376:1085-1092. [CrossRef]
- Edidin AA, Ong KL, Lau E, Kurtz SM. Morbidity, and mortality after vertebral fractures: Comparison of vertebral augmentation and nonoperative management in the Medicare population. Spine (Phila Pa 1976) 2015; 40:1228-1241.
- Liu D, Xu J, Wang Q, Zhang L, Yin S, Qian B, Li X, Wen T, Jia Z. Timing of Percutaneous Balloon Kyphoplasty for Osteoporotic Vertebral Compression Fractures. Pain Physician. 2023 May;26(3):231-243.
- Kanis JA, Harvey NC, McCloskey E, et al. Algorithm for the management of patients at low, high, and very high risk of osteoporotic fractures. Osteoporos Int 2020; 31:1-12. [CrossRef]
- Zhou X, Meng X, Zhu H, Zhu Y, Yuan W. Early versus late percutaneous kyphoplasty for treating osteoporotic vertebral compression fracture: A retrospective study. Clin Neurol Neurosurg 2019; 180:101-105. [CrossRef]
- Goldstein S, Smorgick Y, Mirovsky Y, Anekstein Y, Blecher R, Tal S. Clinical and radiological factors affecting progressive collapse of acute osteoporotic compression spinal fractures. J Clin Neurosci. 2016 Sep;31:122-6. [CrossRef]
- B. Garg, V. Dixit, S. Batra, R. Malhotra, and A. Sharan, “Non-surgical management of acute osteoporotic vertebral compression fracture: a review,” Journal of Clinical Orthopaedics and Trauma, vol. 8, no. 2, pp. 131–138, 2017. [CrossRef]
- N. Evaniew, “Vertebral augmentation for osteoporotic compression fractures: review of the fracture reduction evaluation trial,” Journal of Long-Term Effects of Medical Implants, vol. 26, no. 3, pp. 205–208, 2016. [CrossRef]
- Zhang T, Peng Y, Li J. Comparison of clinical and radiological outcomes of vertebral body stenting versus percutaneous kyphoplasty for the treatment of osteoporotic vertebral compression fracture: A systematic review and meta-analysis. Jt Dis Relat Surg. 2024 Jan 1;35(1):218-230. [CrossRef]
- R. Rousing, K. L. Hansen, M. O. Andersen, S. M. Jespersen, K. Thomsen, and J. M. Lauritsen, “Twelve-months follow-up in forty-nine patients with acute/semiacute osteoporotic vertebral fractures treated conservatively or with percutaneous vertebroplasty: a clinical randomized study,” Spine (Phila Pa 1976), vol. 35, no. 5, pp. 478–482, 2010.
- J. Berenson, R. Pflugmacher, P. Jarzem et al., “Balloon kyphoplasty versus non-surgical fracture management for treatment of painful vertebral body compression fractures in patients with cancer: a multicentre, randomised controlled trial,” The Lancet Oncology, vol. 12, no. 3, pp. 225–235, 2011. [CrossRef]
- Cooper, C., Atkinson, E. J., O'Fallon, W. M., & Melton, L. J. (1992). Incidence of clinically diagnosed vertebral fractures: a population-based study in Rochester, Minnesota, 1985-1989. Journal of Bone and Mineral Research, 7(2), 221-227.
- Son HJ, Park SJ, Kim JK, Park JS. Mortality risk after the first occurrence of osteoporotic vertebral compression fractures in the general population: A nationwide cohort study. PLoS One. 2023 Sep 14;18(9):e0291561. [CrossRef]
- Patel, N., Jacobs, D., John, J. K., Fayed, M., Nerusu, L., Tandron, M., ... & Aiyer, R. (2022). Balloon Kyphoplasty vs Vertebroplasty: A Systematic Review of Height Restoration in Osteoporotic Vertebral Compression Fractures. Journal of Pain Research, 15, 1233-1245. [CrossRef]
- Kallmes DF, Schweickert PA, Marx WF, et al. Vertebroplasty in the mid- and upper thoracic spine. AJNR Am J Neu- orodadiol. 2002 23(7):1117–112026. Kim D, Yun Y, Wang J. Nerve root injections for the relief of pain in patients with osteoporotic vertebral fractures. J Bone Joint Surg Br. 2003 85B(2):250–253.
- Cosman F, de Beur SJ, LeBoff MS, Lewiecki EM, Tanner B, Randall S, Lindsay R, National Osteoporosis F (2014) Clinician's guide to prevention and treatment of osteoporosis. Osteoporos Int 25:2359–2381.
- Kanis JA, Cooper C, Rizzoli R, Reginster JY (2019) Scientific advisory board of the European society for C, Economic aspects of O, the committees of Scientific A, national societies of the international osteoporosis F European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 30:3–44.
- H. Guan, H. Yang, X. Mei, T. Liu, and J. Guo, “Early or delayed operation, which is more optimal for kyphoplasty? A retrospective study on cement leakage during kyphoplasty,” Injury, vol. 43, no. 10, pp. 1698–1703, 2012. [CrossRef]
- G. Baroud and M. Bohner, “Biomechanical impact of vertebroplasty,” Joint Bone Spine, vol. 73, no. 2, pp. 144–150, 2006. [CrossRef]
- G. Zhao, X. Liu, and F. Li, “Balloon kyphoplasty versus percutaneous vertebroplasty for treatment of osteoporotic vertebral compression fractures (OVCFs),” Osteoporosis International: a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA, vol. 27, no. 9, pp. 2823–2834, 2016.
- Li, Y., Tao, W., Wan, Q., Li, Q., Yang, Y., Lin, Y., Zhang, S., & Li, W. (2015). Erratum for Jiang et al., Zoonotic and Potentially Host-Adapted Enterocytozoon bieneusi Genotypes in Sheep and Cattle in Northeast China and an Increasing Concern about the Zoonotic Importance of Previously Considered Ruminant-Adapted Genotypes. Applied and Environmental Microbiology, 81, 5278-5278. [CrossRef]
- C. C. Yang, J. T. Chien, T. Y. Tsai, K. T. Yeh, R. P. Lee, and W. T. Wu, “Earlier vertebroplasty for osteoporotic thoracolumbar compression fracture may minimize the subsequent development of adjacent fractures: a retrospective study,” Pain Physician, vol. 21, no. 5, pp. E483–e491, 2018.
- He B, Zhao J, Zhang M, Jiang G, Tang K, Quan Z. Effect of Surgical Timing on the Refracture Rate after Percutaneous Vertebroplasty: A Retrospective Analysis of at Least 4-Year Follow-Up. Biomed Res Int. 2021 Nov 27;2021:5503022. [CrossRef]
- Taylor RS, Taylor RJ, Fritzell P. Balloon kyphoplasty and vertebroplasty for vertebral compression fractures. Spine (Phila Pa 1976) November 2006;31(23):2747e55. [CrossRef]
- Ma, X., Sun, H., Liu, S., Sang, L., Wang, K., Dong, Y., & Qi, X. (2022). Cement Leakage in Vertebral Compression Fractures Between Unilateral and Bilateral Percutaneous Vertebral Augmentation: A Meta-Analysis. Turkish Neurosurgery.
- Y.J. Chen, W.H. Chen, H.T. Chen, H.C. Hsu, Repeat needle insertion in vertebro- plasty to prevent re-collapse of the treated vertebrae, Eur. J. Radiol. 81 (2012) 558–561.
- Y. Kishikawa, Initial non-weight-bearing therapy is important for preventing ver- tebral body collapse in elderly patients with clinical vertebral fractures, Int. J. Gen. Med. 5 (2012) 373–380.
- Park HTL, Lee CB, Ha JH, Choi SJ, Kim MS, Ha JM (2010) Results of kyphoplasty according to the operative timing. Current Orthopaedic Practice 21:489–493.
- L D. Crandall, D. Slaughter, P.J. Hankins, C. Moore, J. Jerman, Acute versus chronic vertebral compression fractures treated with kyphoplasty: early results, Spine J. 4 (2004) 418–424.
- S. Erkan, T.R. Ozalp, H.S. Yercan, G. Okcu, Does timing matter in performing ky- phoplasty? Acute versus chronic compression fractures, Acta Orthop. Belg. 75 (2009) 396–404.
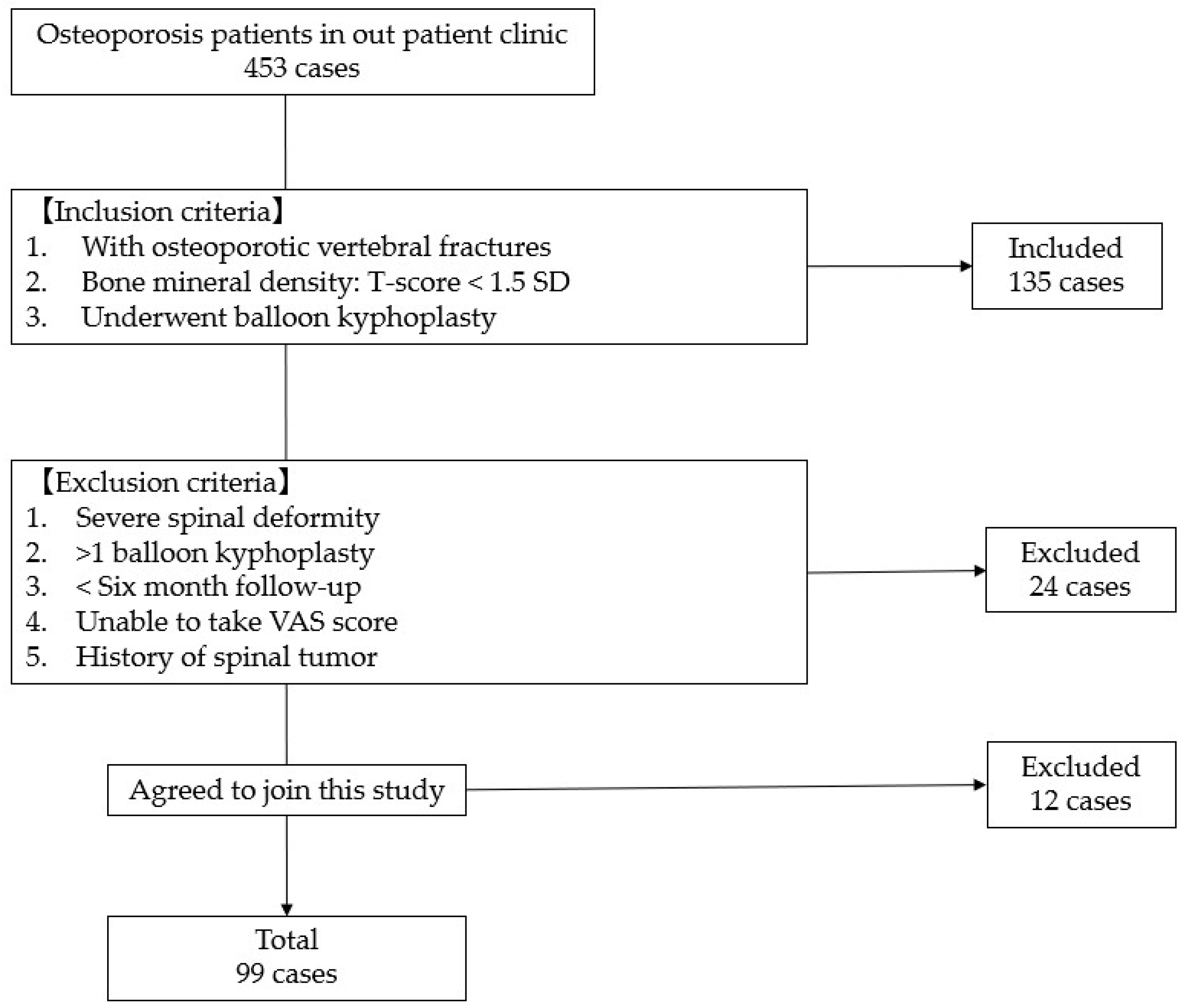
Figure 2.
Chronological results of vertebral kyphosis angle.
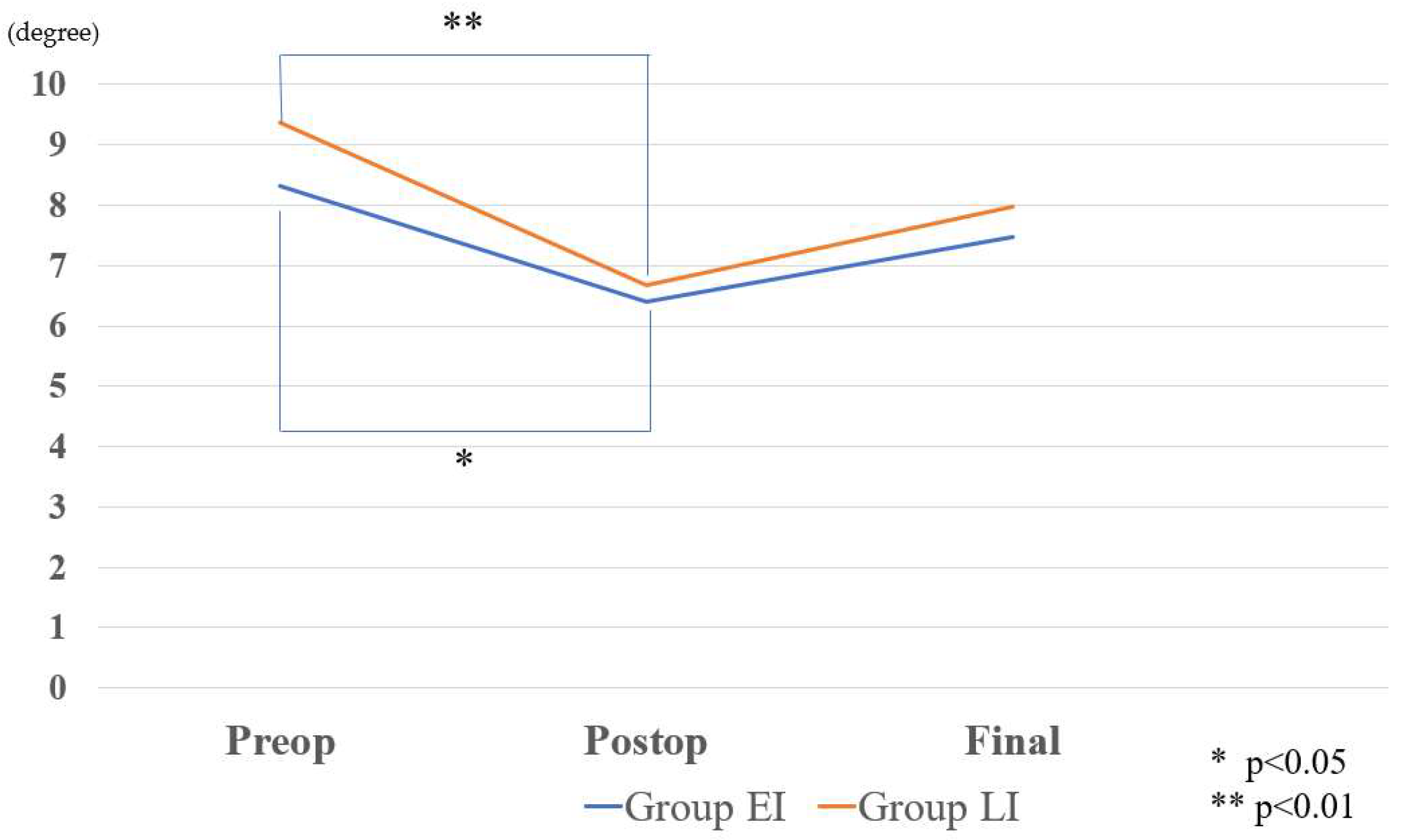
Figure 3.
Adjacent segmental fracture.
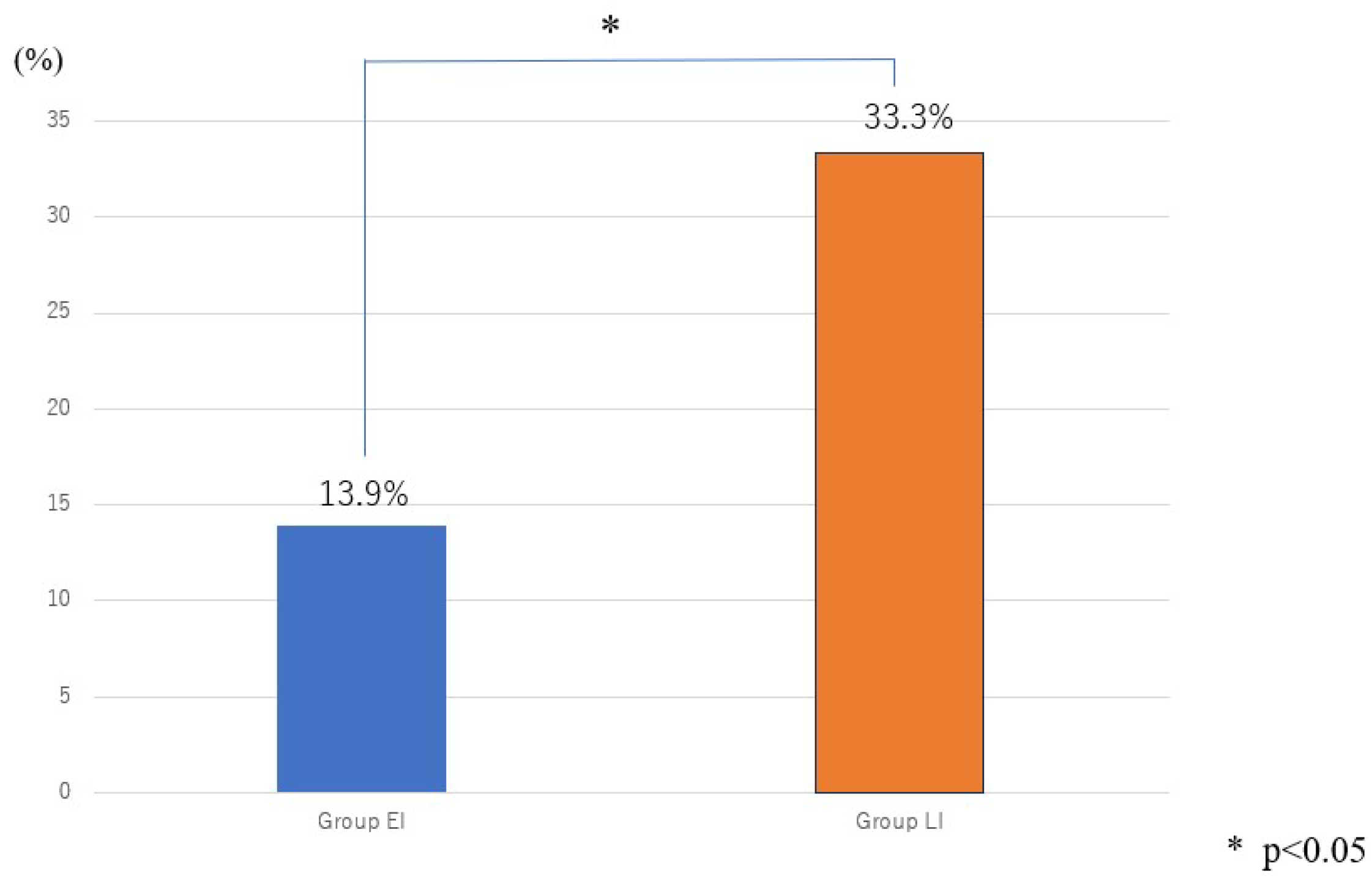
Figure 4.
Level of fracture site.
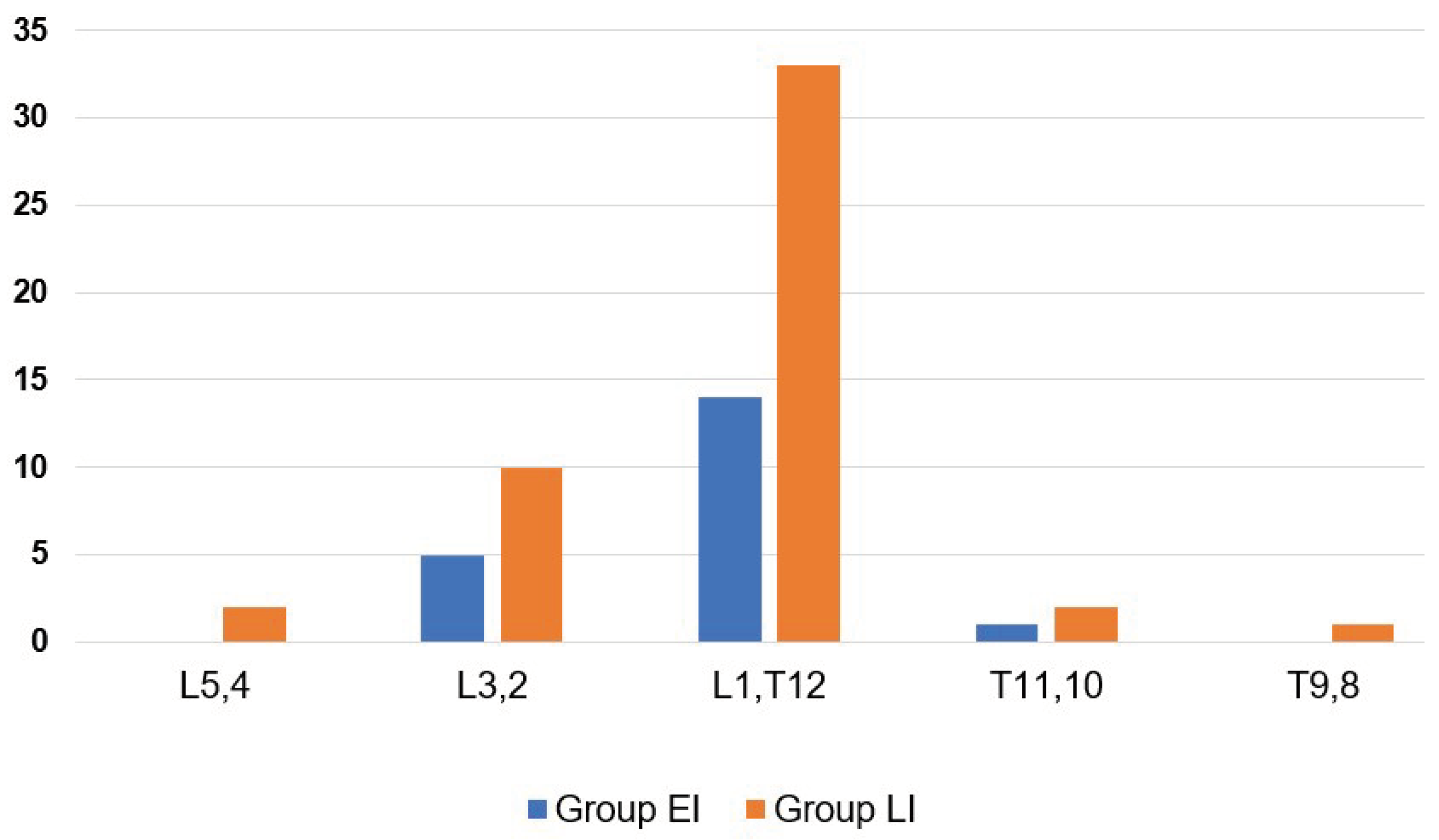

Table 1.
Patient demographic.
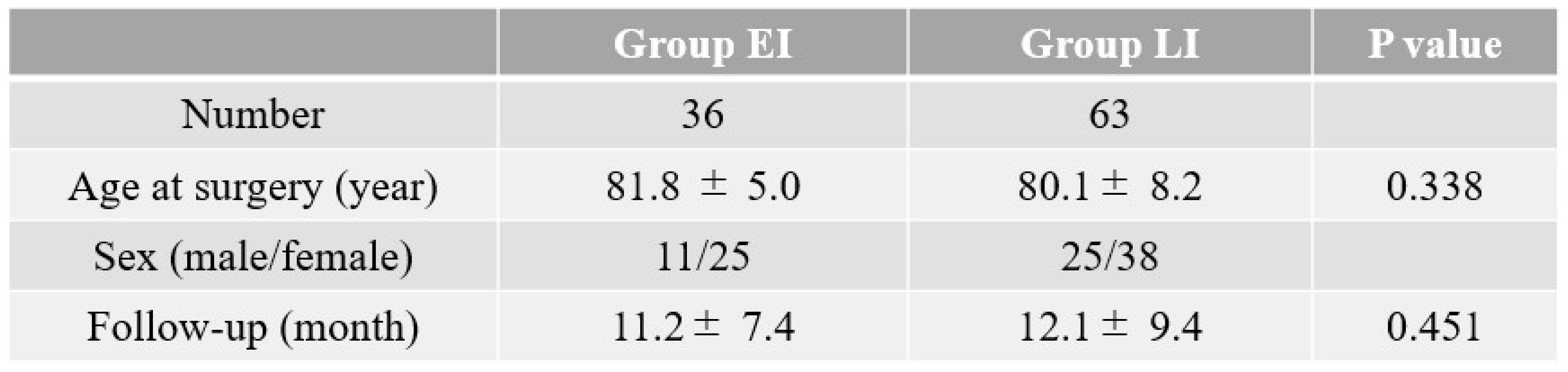 |
Table 2.
Clinical data.
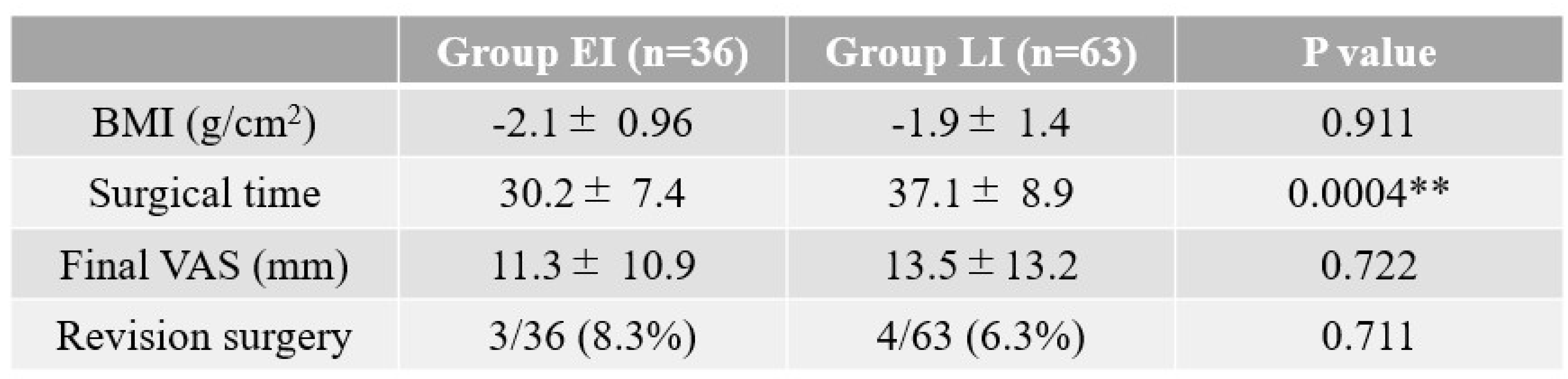 |
** p<0.01.
Table 3.
Radiological results.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



