Submitted:
12 February 2024
Posted:
14 February 2024
You are already at the latest version
Abstract
Study design: Technical note.
Objectives: To present a novel technique of treatment for patient with basilar invagination.
Background : Basilar invagination (BI) is considered a congenital condition and can compress the cervicomedullary junction, causing neurologic deficit. Severe neurological deficit due to BI should be treated surgically. However, there is controversy regarding whether an anterior or posterior approach should be used. Anterior approach is optimal for decompression of cervicomedullary junction, but this approach has high complication rates. Posterior reduction has a high risk of occipital screws backout and/or instrument failure.
Materials and Methods : A 15-year-old boy with severe myelopathy was referred to our hospital. He had neck pain, muscle weakness of bilateral upper limbs, gait disturbance appeared 3 months before he visited our hospital, he drops a cup several times recently. In the examination, he had hyperreflexia of upper and lower limbs and muscle weakness of bilateral arms (MMT 4), hypoesthesis was observed bilaterally below elbow and both legs. He also had clumsiness of bilateral hands, mild urinary and bowel incontinence, and spastic gait. His 10 second grip and release test was 16 in both hands. His grip power was 20 kg in right and 17 kg in left. Radiograms showed severe BI and spinal cord was severely compressed with odontoid process..
Results : The patinet underwent posterior surgery with C-arm free technique. All screws including occipital screws were inserted adequate position under navigation guidance. Reduction was achieved with skull rotation and distraction. A follow-up at one year we have these results : Manual muscle testing results and sensory function tests showed almost full recovery, bilateral arms (MMT 5) ,walking smoothly. Cervical Japanese orthopedic association score of the patient has improved from 9/17 to 16/17. Post-operative images showed an excellent spinal cord decompression, and no major or severe complications has occured .
Conclusions/Level of Evidence : Basilar invagination with Klippel-Feil syndrome is relatively rare condition. Posterior approach and occipito-cervical fixation for BI treatment with navigation technique is a safe method to treat severe myelopaty with reducible odontoid. This novel navigation technique provides an excellent results for a patient with BI. Level V.
Keywords:
Basilar invagination
; Klippel-Feil syndrome
; Navigation
; C-arm free
; Novel technique
1. Introduction
Klipple-Feil Syndrome (KFS) is an abnormal fusion of 2 or more vertebrae in the cervical spine caused by a failure in the division or normal segmentation in the early fetal development. It is believed that KFS occurs in 1 out of 42,000 births [1]. The clinical triad of Klippel-Feil Syndrome (KFS) consists of a shortened neck leading to facial asymmetry, a low hairline, and restricted neck mobility. These characteristics were first described by Andre Klippel and Maurice Feil in 1912 [2]. The patients of KFS may have spinal stenosis, neurologic deficit, cervical spinal deformity, and instability. The patients with KFS are sometimes asymptomatic, however this instability may potentially lead to death [3].
Basilar impression (BI) has been firstly reported by Ackermann in 1790 [4]. BI is considered a congenital malformation and characterized by odontoid displacement of the axis inwards towards the foramen magnum, which can compress the cervicomedullary junction, causing neurologic deficit [5]. The primary cause of basilar invagination (BI) is believed to be the presence of microtraumas resulting from repetitive lesions caused by instability [6]. In 1911, Schuller reported the radiological criteria for BI [7]. The recent diagnosis is made by odontoid is protruded over McGregor’s line [8] or McRae’s line [9]. McGregor’s line is defined as a line connecting the posterior edge of the hard palate to the most caudal point of the occipital curve. The diagnosis of basilar invagination (BI) is established when the tip of the dens lies more than 4.5 mm above this line [8]. McRae’s line, on the other hand, is a radiographic line drawn on a lateral skull radiograph. BI is diagnosed when the tip crosses this line [9] (Figure 1). The symptoms of BI are headache and/or neck pain, cranial nerve dysfunction, and quadriplegia [10]
The authors present the technical notes of a case involving a 15-year-old boy exhibiting symptoms attributed to basilar impression associated with Klippel-Feil syndrome. This study received approval from the ethics committee of our institute (No. 480), and necessary consents were obtained from the patient and his parents.
1.1. Patient history
A 15-year-old boy with severe myelopathy was referred to our hospital. He had been experiencing neck pain, muscle weakness in both upper limbs, and numbness in both hands for 4 years. Increased numbness and gait disturbance emerged 3 months before his visit to our hospital. He is unable to run and has recently experienced dropping a cup several times.
1.2. Physical examination
During the examination, he exhibited hyperreflexia in both upper and lower limbs and muscle weakness in both arms (MMT 4). Hypoesthesia was observed bilaterally below the elbows and in both legs. Additionally, he demonstrated clumsiness in both hands, mild urinary and bowel incontinence, and a spastic gait. His 10-second grip and release test yielded a score of 16 in both hands, with grip power measured at 20 kg in the right hand and 17 kg in the left. The cervical Japanese Orthopaedic Association (JOA) score of the patient was 9/17.
1.3. Preoperative imaging
Preoperative cervical radiographs revealed a short neck and a C2/3 fusion anomaly. Dens protrusion into the foramen magnum measured 9.4 mm above McGregor’s line and 4.2 mm above McRae’s line, with an anteroposterior (AP) diameter of the foramen magnum measuring 10.7 mm (Figure 2). Preoperative magnetic resonance imaging (MRI) depicted severe compression of the cervicomedullary cord by the dens, with a cervicomedullary angle (CMA) measuring 116 degrees (Figure 3).
1.4. Surgery
This patient underwent posterior reduction with cervical pedicle screw fixation under the guidance of O-arm navigation, without a C-arm. The patient was positioned prone, with the neck in a neutral position on a Jackson frame equipped with a full carbon skull clamp to facilitate the O-arm scan. The procedure was conducted under neuromonitoring. The occiput and C1-5 were exposed with a 10-cm posterior midline incision. Initially, a reference frame was attached to the C2 spinous process.
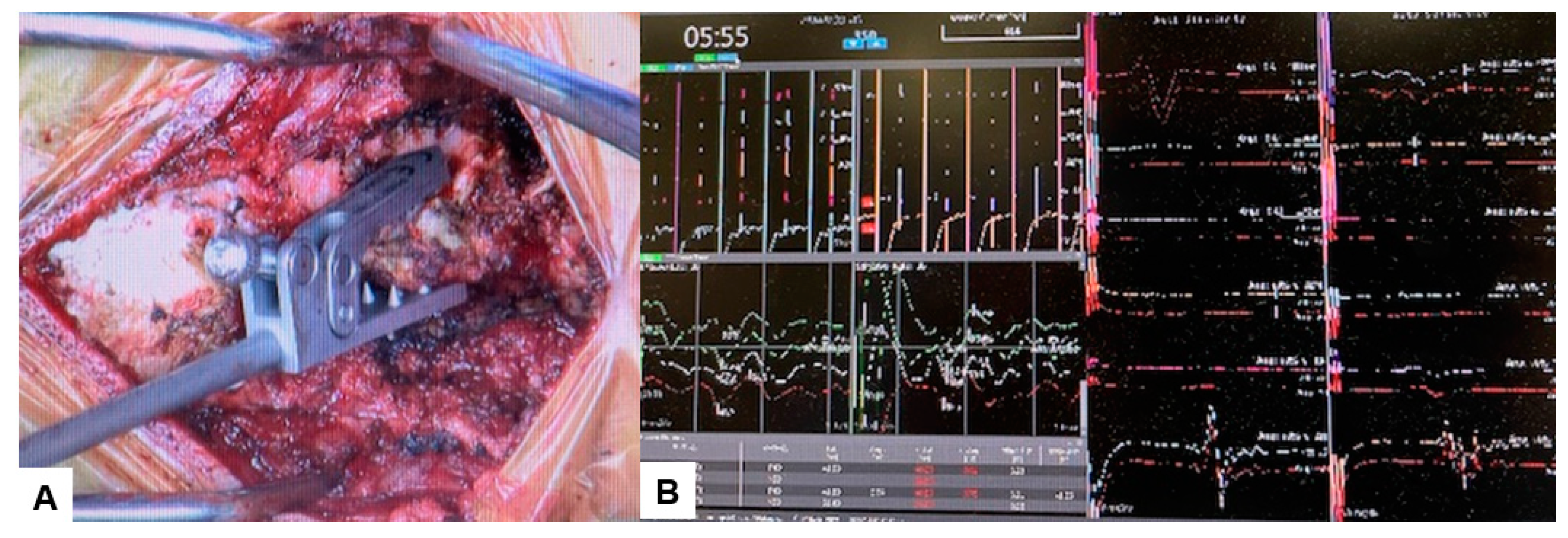
Figure 6.
Reference frame and neuromonitouring, A: Reference frame, B: Neuromonitouring.
Subsequently, the O-arm was positioned, and three-dimensional (3-D) reconstruction images were obtained. Following the verification of each navigated mapped spinal instrument, bilateral C2 laminar screws (Figure 5) and C4-5 pedicle screws (Figure 6) were inserted under navigation.
Figure 5.
Bilateral C2 laminar screw, A: sagittal view, B: Axial view, C: Oblique view.
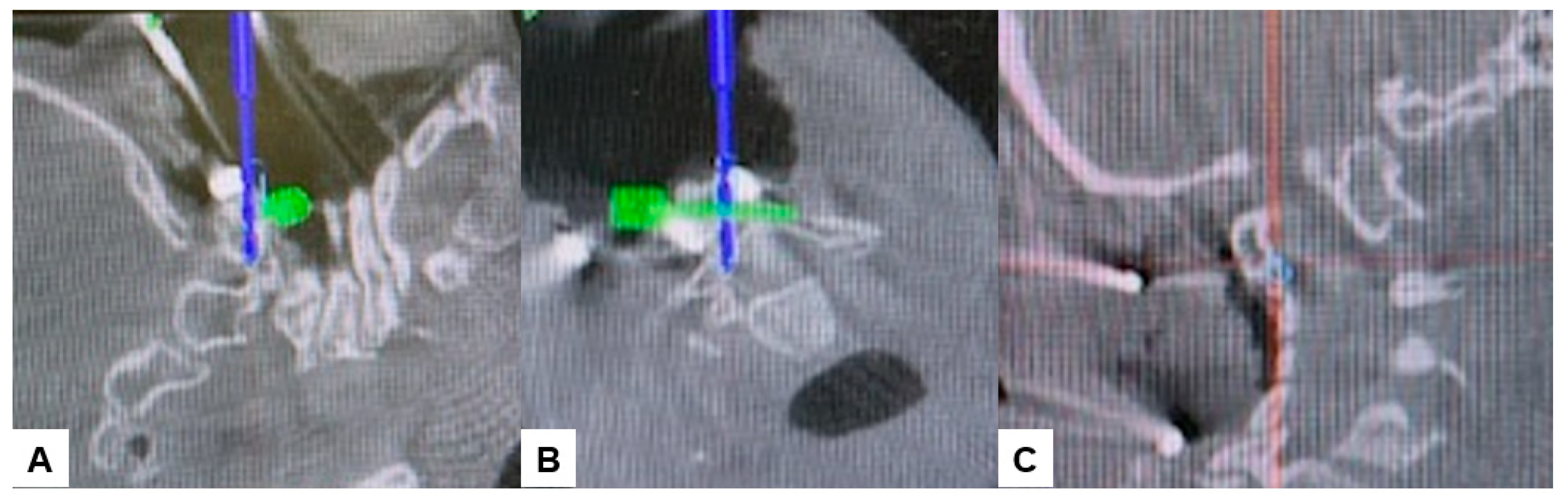
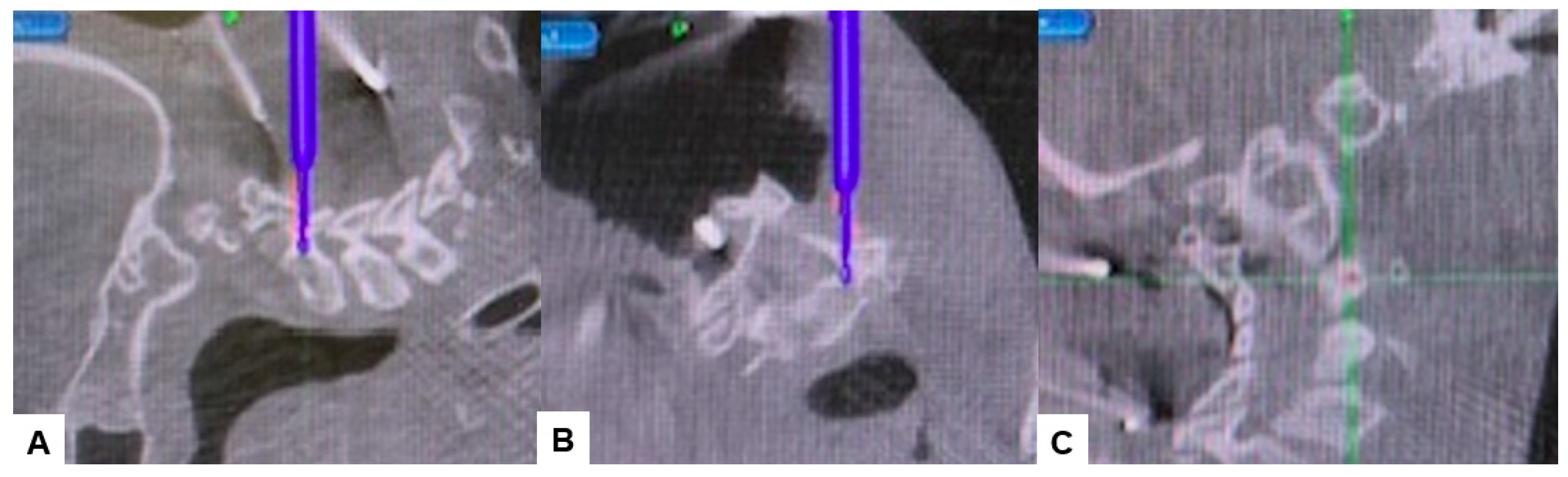
Figure 6.
Pedicle screw fixation, A: sagittal view, B: Axial view, C: Oblique view.
Then, under navigation guidance, the thickest portion for occiput screws was identified, and a total of 6 occipital screws were inserted using a navigated high-speed burr and pointer (Figure 7). The sagittal rotation connector of Mayfield skull clamp was loosened and the skull was ratated forward, refixed (Figure 8A,B). Finally, two cobalt-chrome rods were connected to the screw head (Figure 8C) and distraction was done for adequate reduction (Figure 8D and Figure 9).
Figure 7.
Occipital screwing, A: sagittal view, B: Axial view, C: 3D view, The adequate screw point was indicated by the navigated pointer.
Figure 7.
Occipital screwing, A: sagittal view, B: Axial view, C: 3D view, The adequate screw point was indicated by the navigated pointer.
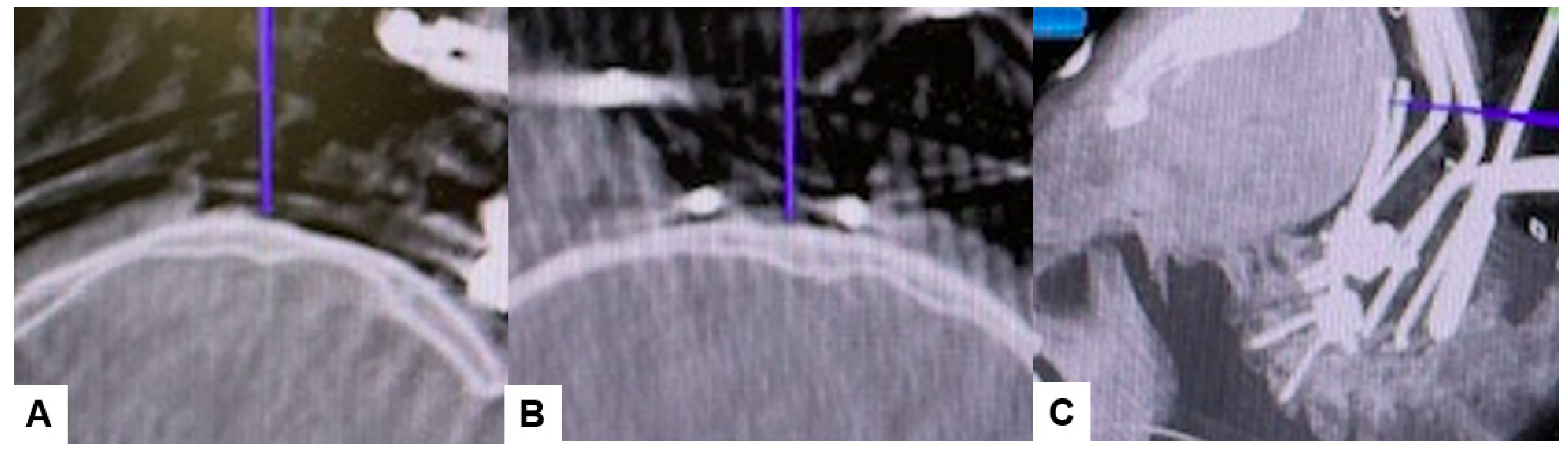
Figure 8.
Reduction manuvour, A: Before reduction, B: Ratational reduction with Mayfield skull cramp ratation, C: Distraction with screws and rods, D; After reduction.
Figure 8.
Reduction manuvour, A: Before reduction, B: Ratational reduction with Mayfield skull cramp ratation, C: Distraction with screws and rods, D; After reduction.
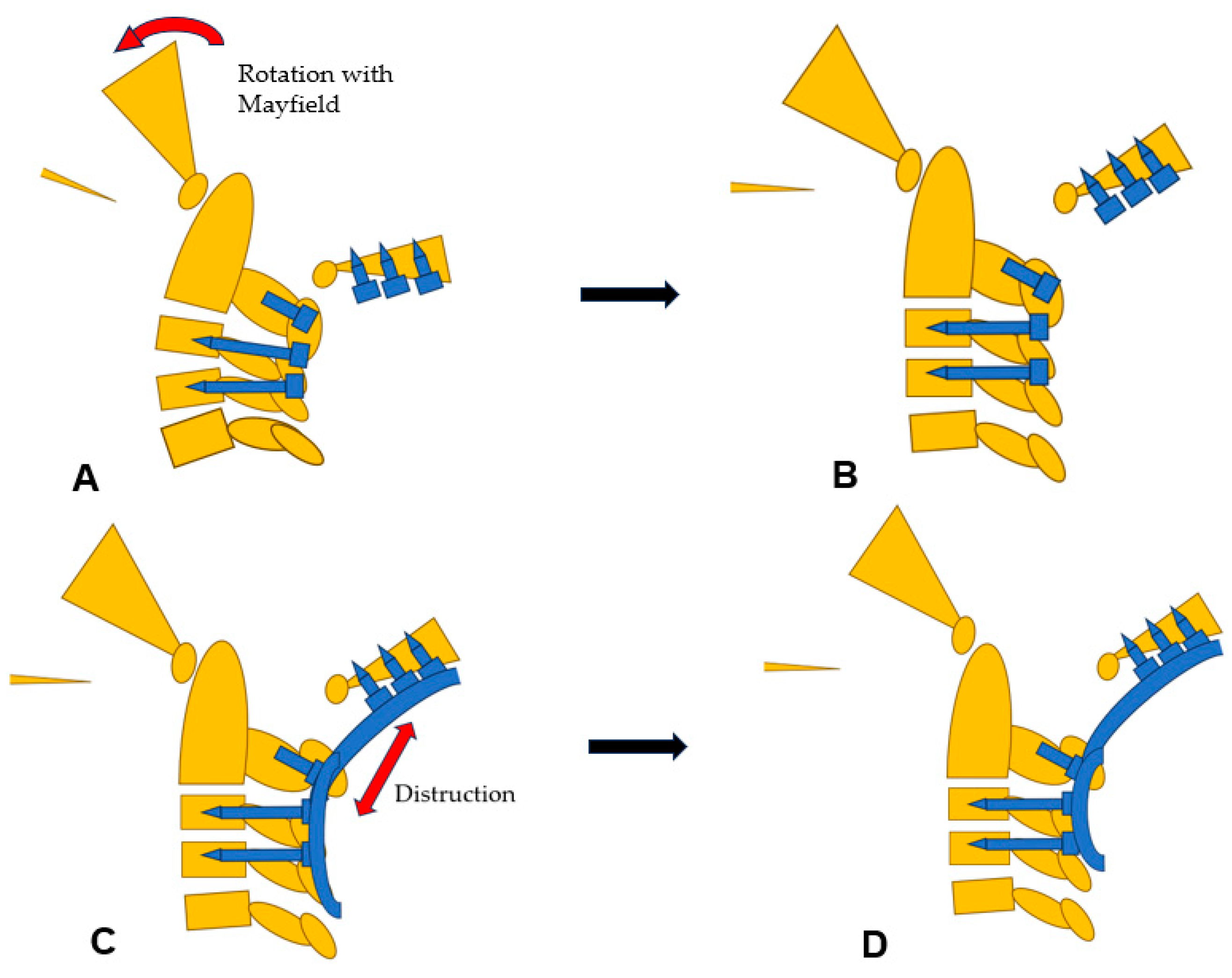
Figure 9.
Intraoperative images, A: Occip@ital screwing, B: Rod insertion.

1.5. Postoperative imagings
Postoperative radiographs and CT scans demonstrated successful reduction, realignment, and appropriate screw positioning. The tip of the dens now measures 6.3 mm above McGregor’s line and 2.5 mm below McRae’s line, with the cervicomedullary angle (CMA) measuring 130 degrees. Additionally, the anteroposterior (AP) diameter of the foramen magnum increased to 19.3 mm (Figure 10, Figure 11 and Figure 12).
Figure 10.
Postoperative radiograms, A: Laterl ragiogram, B: Mid-Sagittal reconstraction CT, C: 3D CT.
Figure 10.
Postoperative radiograms, A: Laterl ragiogram, B: Mid-Sagittal reconstraction CT, C: 3D CT.
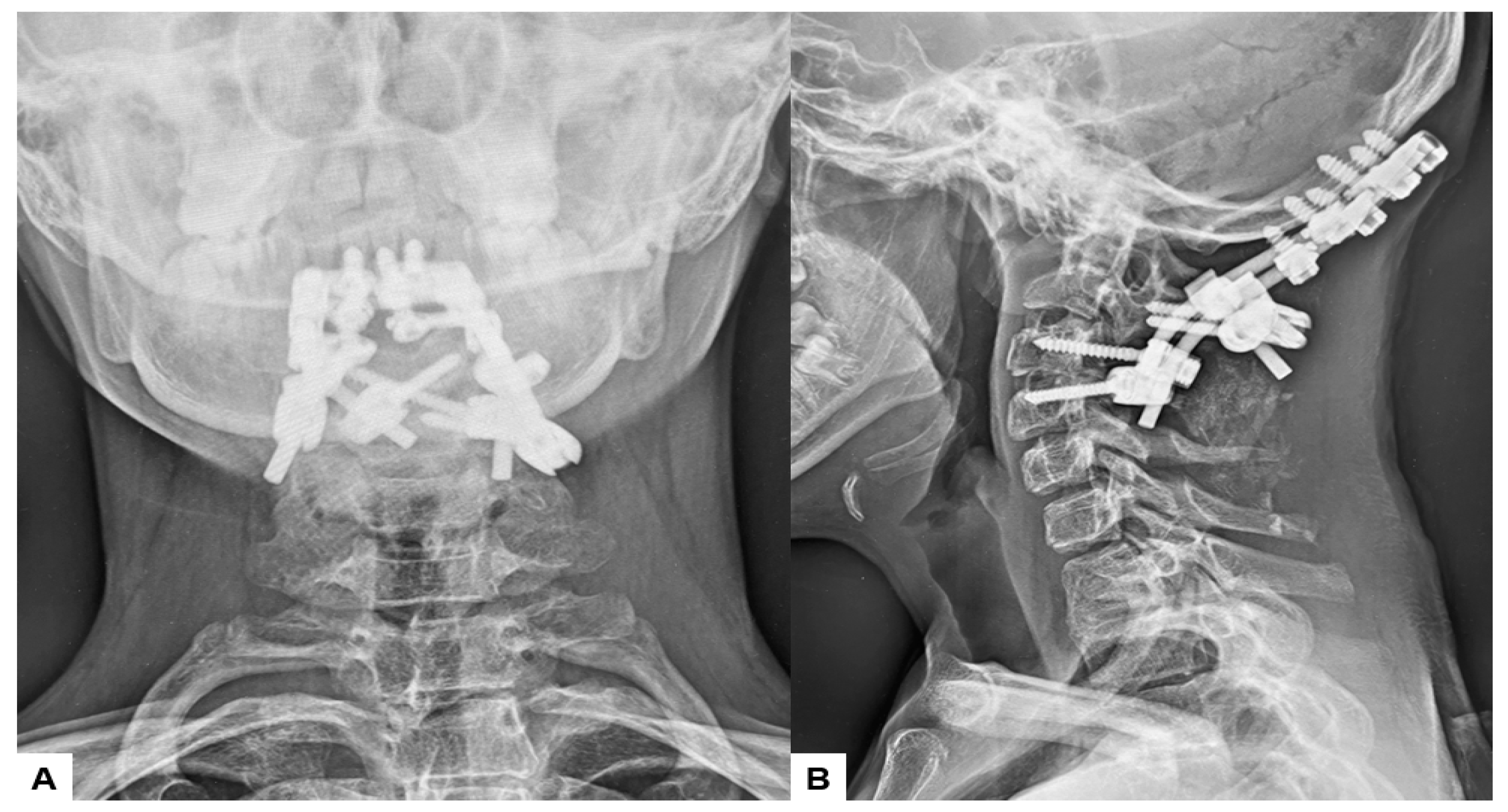
Figure 11.
Postoperative CT.
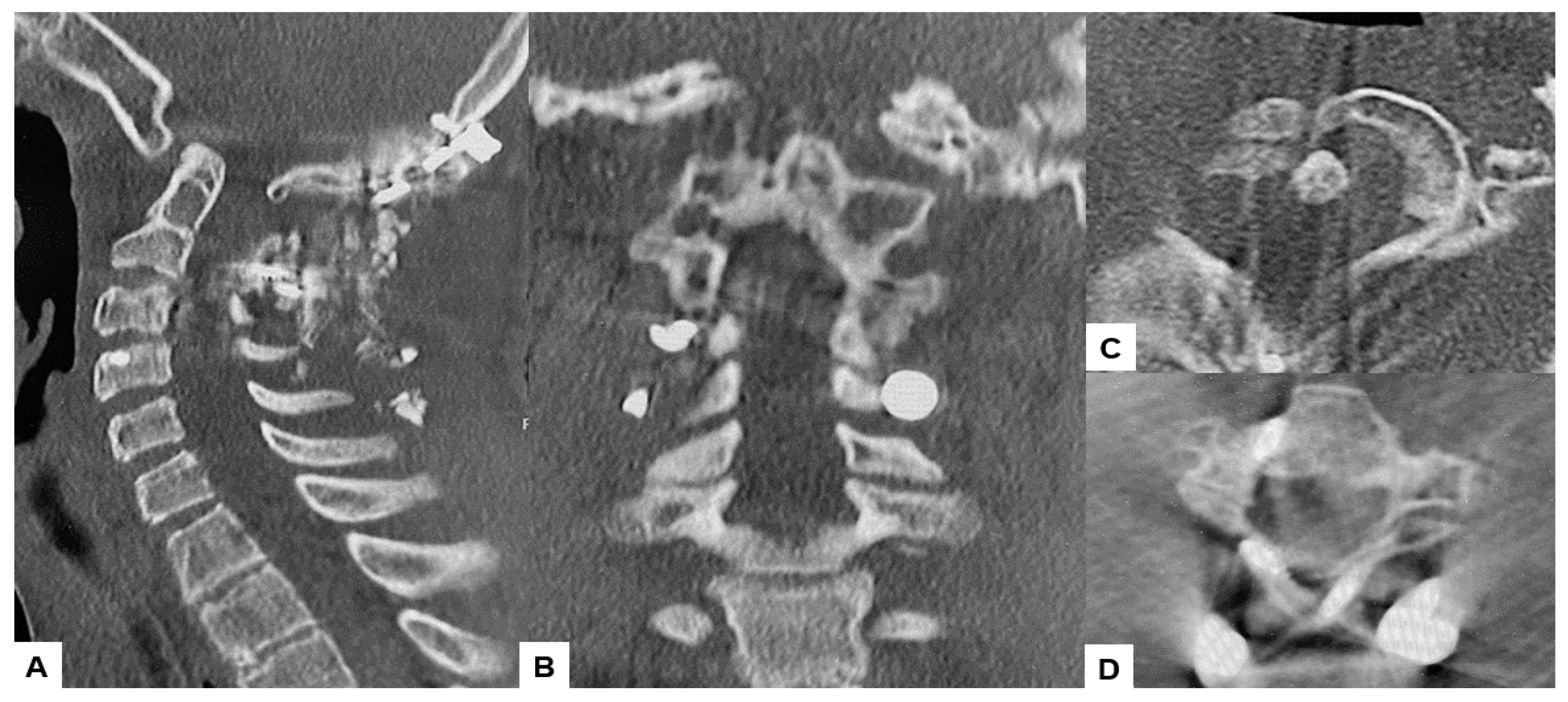
Figure 12.
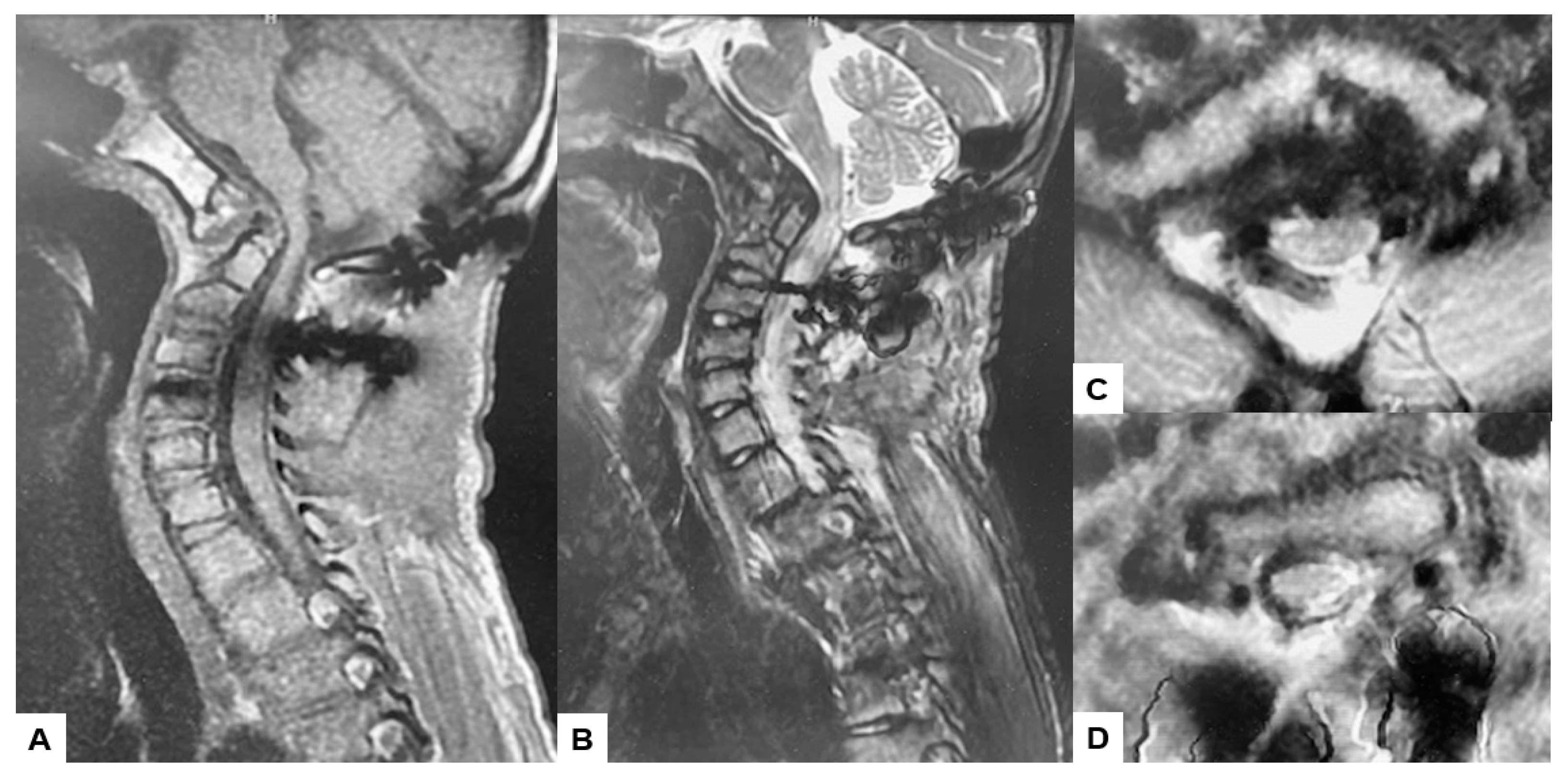
Follow-up images, A: Mid sagittal T1-weighted MR imaging, B: Mid sagittal T2-weighted MR imaging. C: Axial T2-weighted MR imaging at C1, D: Axial T2-weighted MR imaging at C2, Spinal cord was adequately decompressed.
Figure 12.
Follow-up images, A: Mid sagittal T1-weighted MR imaging, B: Mid sagittal T2-weighted MR imaging. C: Axial T2-weighted MR imaging at C1, D: Axial T2-weighted MR imaging at C2, Spinal cord was adequately decompressed.
1.6. One year follow-up
Postoperative MRI indicated excellent spinal cord decomression (Figure 11).
2. Results
Surgically, the patient was successfully treated, with a surgical time of 139 minutes and an estimated blood loss of 180 ml. During the one-year follow-up, manual muscle testing results and sensory function tests indicated almost full recovery in both bilateral arms (MMT 5). The patient is now walking smoothly without any gait disturbance, and the cervical Japanese orthopedic association score score has improved from 9/17 to 16/17. Post-operative radiographs demonstrated excellent spinal cord decompression, with no loss of reduction or malalignment. The cervicomedullary angle (CMA) postoperatively measured 130 degrees. Furthermore, there were no major or severe complications reported.
3. Discussion
Klippel–Feil syndrome is a complex condition mainly with congenital malformation of the cervical spine where two or more vertebrae are fused. Patients typically present with radiculopathy and myelopathy, although instances of quadriparesis are infrequent. [11,12]. These neurological symptoms are usually caused by spondylosis or instability of the adjacent segments to the fused vertebrae or by radicular compression within frequently undersized neuroforamina. Feil categorized Klippel-Feil Syndrome (KFS) into three types: Type 1 entails extensive fusion affecting multiple vertebrae, Type 2 entails fusion of two vertebrae, and Type 3 encompasses either of the other types combined with anomalies in the thoracic or lumbar spine [13]. The clinical presentation varies based on the extent and levels of fusion. Typically, fusions involving the cranio-cervical junction or extensive fusions are associated with earlier onset due to cosmetic deformity, pain, and delayed developmental milestones. Manifestation of lower cervical fusion often occurs later in life [14]. Type 2 patterns may typically be asymptomatic and reported as incidental findings on radiographic imaging, or when subaxial instability occurs, potentially leading to basilar impression, as observed in our patient’s case.
Basilar invagination (BI) refers to the migration or displacement of the odontoid in an upward direction, resulting in compression of the spinomedullary cord. The lower brain stem can be significantly affected by the dens, as it is positioned abnormally through the foramen magnum and into the posterior fossa [15]. Congenital basilar invagination may coincide with other abnormalities, such as atlanto-occipital fusion, atlas hypoplasia, hemirings of C1 with lateral mass spreading, odontoid abnormalities, Klippel-Feil Syndrome (KFS), and achondroplasia [16]. Suspecting basilar invagination is warranted when the C1-2 facet complex cannot be sufficiently visualized on a standard open-mouth anteroposterior view of the upper cervical spine [17]. Although the wide use of plain radiographs with dynamic views as screening methods, MRI still the best imaging modality for the diagnosis because it shows how much there is neural impingement and the degree of cord compression [18]. CT angiography (CTA) is strongly advised preoperatively to detect any anomalous variations of carotid and vertebral arteries, aiming to reduce the risk of intraoperative injury [19,20,21].
The use of traction with external fixation is considered in the treatment of basilar invagination, but this technique may benefit only a few patients without any neurological deficits [22]. Sekir recommended the utilization of traction. For the minority of patients without neurological disturbances, preoperative traction, both clinically and radiologically, for disease progression has been proposed as a viable alternative to operative stabilization. [23,24]. In a case series by Goel et al., 82 patients without any associated Chiari malformation underwent cervical traction, leading to quick clinical improvement in 82% of these individuals after traction application [25]. Given that the patients included in the aforementioned studies exhibited mild neurological symptoms, this method may not be dependable for patients with severe basilar invagination and accompanying neurological deficits. Nonetheless, external fixation methods such as the halo vest pose several challenges, including pin loosening and infection risks, incomplete cervical spine fixation, inability to prevent progressive deformity, and the potential for serious complications like pin over penetration [26]. Following the approach outlined by Abumi et al., we opted not to undertake traction and manual reduction pre-operatively to mitigate the risk of complications associated with external fixation. Surgical intervention was determined as the appropriate course of action for the patient [27].
Surgical treatment options for basilar invagination (BI) encompass various approaches and techniques, yet ongoing debate surrounds the optimal timing and choice of approach [28]. The anterior approach is typically favored in cases where the protrusion of the odontoid process is irreducible and brainstem compression is severe [28,29]. The anterior approach is notably demanding, involving a complex technique with significant complications such as a higher incidence of postoperative infection and respiratory tract disorders. Additionally, it entails increased invasiveness and poses challenges in achieving primary fixation, often necessitating posterior instrumentation in subsequent cases [30]. Decompression and instrumentation after acceptable reduction with posterior approach is feasible in many cases, where the lesion can be managed with less complications related to the anterior approach [31]. The posterior approach generally provides stable fixation without requiring supportive external fixation or secondary stabilization. Unlike the anterior approach, this allows for early mobilization [32]. However, in irreducible cases, additional anterior surgery is necessary alongside posterior fixation [28].
In our novel technique, we demonstrate the effectiveness of a C-arm free approach utilizing the O-arm with navigation via the posterior approach, allowing for reduction, decompression, and fixation of C0, C2, C4, and C5. Postoperatively, follow-up revealed successful reduction and achieved rigid fixation with smooth recovery, without any serious complications occurring. It has been reported that accuracy of screw placement in the cervical spine is enhanced by the O-arm [33]. Additionally, the safe performance of atlantoaxial fixation using the O-arm has been demonstrated by Wada et al. [34]. Changes in navigation accuracy may occur during surgery, particularly if the position of the reference frame is inadvertently altered, potentially impacting the procedure’s accuracy. Reviewing the literature [Table 1], the main technique used for screw insertion is free hand technique using C-arm fluroscopy and still there is a risk for mal-insertion or violating important vital structure using this technique [35,36,37]. Although, to our knowledge, no other study has addressed occipital screw fixation under navigation. Van de Kelft et al. (2012) reported a pedicle screw violation rate of 2.5% using navigation in the cervical spine [38]. In contrast, free-hand and fluoroscopy-assisted techniques have been linked to significantly higher rates of incorrect pedicle screw placement, ranging from 15% to 40% [39,40]. Another drawback of the C-arm technique is the increased radiation exposure for both the surgical team and the patient compared to our C-arm-free approach, which minimizes exposure for all parties involved [41].
Positioning occipital screws in occipitocervical instability poses a significant challenge and precision. It is crucial to accurately identify the thickest part of the lower occiput to safely insert the screws without risking injury to surrounding anatomical structures or the dura, which could lead to cerebrospinal fluid (CSF) leakage (Figure 7). Successful placement of occipital screws necessitates a thorough understanding of bone anatomy and its relationship with neurovascular structures, the spinal canal, hypoglossal canal, vertebral arteries, and the jugular foramen [42]. In our technique, utilizing navigation-mapped high-speed burr and probe, we achieve precise insertion of occipital screws with optimal length by directly visualizing and identifying the thickest part of the occiput. This approach, guided by navigation, ensures high accuracy and enhances screw purchase and strength.
This study has several limitations, including a small sample size, short follow-up duration, lack of a control group, and the need for statistical assessment of patient outcomes and complications with a larger population. A comparative study comparing navigational support to current methods of treating BI is warranted to further evaluate the efficacy of this technique.
4. Conclusion
Basilar invagination (BI) occurring alongside Klippel-Feil syndrome is a relatively uncommon occurrence. Utilizing a C-arm-free technique for posterior reduction and fusion proves to be a safe approach in addressing this condition. This innovative method yields favorable outcomes for individuals with BI and a reducible odontoid.
Author Contributions
M.T.: conceptualisation, writing—original draft preparation; A.K.A.: writing—review and editing; C.K.: writing—review and editing; S.A: data collection; T.K.: data collection; T.T.: data collection.; K.U.: data collection, Y.O.: data collection, All authors have read and agreed to the published version of the manuscript.
Funding
This study received funding from Japan Organization of Occupational Health and Safety.
Institutional Review Board Statement
This study was conducted in accordance with the guidelines of the Declaration of Helsinki and approved by the institutional review boards at Okayama Rosai Hospital (approval No. 480, Dec 5,, 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available in the article.
Acknowledgments
This study was supported by Okayama Spine Group.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Da Silva, E.O. Autosomal recessive Klippel-Feil syndrome. J Med Genet. 1982, 19, 130–4. [Google Scholar] [CrossRef]
- Klippel, M.; Feil, A. Un cas d’absence des vertebres cervicales. Avec cage thoracique remontant jusqu’a la base du crane (cage thoracique cervicale). Nouv Iconog Salpetriere. 1912, 25, 223–50. [Google Scholar]
- Nagib, M.G.; Maxwell, R.E.; Chou, S.N. Identification and management of high-risk patients with Klippel-Feil syndrome. J Neurosurg. 1984, 61, 523–30. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, J.F. Ueber die Kretinen, einebesondereMenschenabart in den Alpen. Gotha, in der EttingerschenBuchhandlung. 1790. [Google Scholar]
- Joaquim AF, Ghizoni E, Giacomini LA, Tedeschi H, Patel AA. Basilar invagination: surgical results. J Craniovertebr Junction Spine. 2014; 5, 78–84. [CrossRef]
- Goel, A. Instability and basilar invagination. J Craniovertebr Junction Spine. 2012, 3, 1–2. [Google Scholar] [CrossRef]
- Schüller, A. Zur Röntgendiagnose der basilären impression des schädels. Wien Med Wochenschr. 1911, 61, 2594–99. [Google Scholar]
- McGregor, M. The significance of certain measurements of the skull in the diagnosis of basilar impression. Br J Radiol 1948, 21, 171e81. [Google Scholar] [CrossRef]
- McRae, D.L.; Barnum, A.S. Occipitalization of the atlas. AJR Am J Roentgenol 1953, 70, 23. [Google Scholar]
- Brito, J.N.P.O.; Santos, B.A.D.; Nascimento, I.F.; Martins, L.A.; Tavares, C.B. Basilar invagination associated with chiari malformation type I: A literature review. Clinics (Sao Paulo). 2019, 74, e653. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, K.M.; Spivak, J.M.; Bendo, J.A. Embryology of the spine and associated congenital abnormalities. Spine J 2005, 5, 564–576. [Google Scholar] [CrossRef]
- Greenberg MS (2010) Klippel–Feil syndrome. In: Greenberg MS (ed) Handbook of neurosurgery, 7th edn. Thieme Medical Publishers,New York, pp 253–254.
- Thomsen, M.N.; Schneider, U.; Weber, M.; Johannisson, R.; Niethard, FU. Scoliosis congenital anomalies associated with Klippel–Feil syndrome types, I. –.I.I.I. Spine 1997, 22, 396–401. [Google Scholar] [CrossRef]
- Tracy, M.R.; Dormans, J.P.; Kusumi, K. Klippel-Feil syndrome: clinical features and current understanding of etiology. Clin Orthop Relat Res July 2004 (424):183–90. [CrossRef]
- Donnally, I.I.I.C.J.; Munakomi, S.; Varacallo, M. Basilar Invagination. [Updated 2023 Aug 13]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Ferreira, J.A.; Botelho, R.V. The odontoid process invagination in normal subjects, Chiari malformation and Basilar invagination patients: pathophysiologic correlations with angular craniometry. Surg Neurol Int. 2015, 6, 118–7806160322. [Google Scholar] [CrossRef]
- McRae, D.L.; Barnum, A.S. Occipitalization of the atlas. Am J Roentgenol Radium Ther Nucl Med 1953, 70, 23–46. [Google Scholar] [PubMed]
- Chamnan, R.; Chantarasirirat, K.; Paholpak, P.; Wiley, K.; Buser, Z.; Wang, J.C. Occipitocervical measurements: correlation and consistency between multi-positional magnetic resonance imaging and dynamic radiographs. Eur Spine J. 2020, 29, 2795–2803. [Google Scholar] [CrossRef]
- Zhou, L.P.; Zhang, R.J.; Zhang, H.Q.; Jiang, Z.F.; Shang, J.; Shen, C.L. Effect of High-Riding Vertebral Artery on the Accuracy and Safety of C2 Pedicle Screw Placement in Basilar Invagination and Related Risk Factors. Global Spine J. 2024, 14, 458–469. [Google Scholar] [CrossRef] [PubMed]
- Su, C.; Chen, Z.; Wu, H.; Jian, F. Computed tomographic angiography to analyze dangerous vertebral artery anomalies at the craniovertebral junction in patients with basilar invagination. Clin Neurol Neurosurg. 2021, 200, 106309. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.P.; Zhang, R.J.; Jiang, Z.F.; Tao, E.X.; Shang, J.; Shen, C.L. Ideal entry point and trajectory for C2 pedicle screw placement in basilar invagination patients with high-riding vertebral artery based on 3D computed tomography. Spine J. 2022, 22, 1281–1291. [Google Scholar] [CrossRef] [PubMed]
- Joaquim, A.F.; Tedeschi, H.; Chandra, P.S. Controversies in the surgical management of congenital craniocervical junction disorders - A critical review. Neurol India. 2018, 66, 1003–1015. [Google Scholar]
- Al Jishi, A. Commentary: Comprehensive Drilling of C1-2 Facets in Congenital Atlanto-Axial Dislocation and Basilar Invagination: Critical Review. Oper Neurosurg (Hagerstown). 2019, 16, 58–59. [Google Scholar] [CrossRef]
- Joaquim, A.F.; Tedeschi, H.; Chandra, P.S. Controversies in the surgical management of congenital craniocervical junction disorders - A critical review. Neurol India. 2018, 66, 1003–1015. [Google Scholar]
- Goel, A. Basilar invagination, Chiari malformation, syringomyelia: a review. Neurol India. 2009, 57, 235–46. [Google Scholar] [CrossRef] [PubMed]
- Garfin, S.R.; Botte, M.J.; Waters, R.L.; Nickel, V.L. Complications in the use of the halo fixation device. The Journal of Bone and Joint Surgery. 1986, 68, 320–5. [Google Scholar] [CrossRef]
- Abumi K, Takada T. Shono Y, Kaneda K, Fujiya M. Posterior occipitocervical reconstruction using cervical pedicle screws and plate-rod systems. Spine (Phila Pa 1976). 1999 Jul 15:24(14):1425–34. [CrossRef]
- Menezes, A.H.; VanGilder, J.C.; Graf, C.J.; McDonnell, D.E. Craniocervical abnormalities. A comprehensive surgical approach. J Neurosurg. 1980, 53, 444–55. [Google Scholar] [CrossRef]
- Goel, A. Craniovertebral junction instability: a review of facts about facets. Asian Spine J. 2015, 9, 636–44. [Google Scholar] [CrossRef]
- Zileli, M.; Akıntürk, N. Complications of occipitocervical fixation: retrospective review of 128 patients with 5-year mean follow-up. Eur Spine J. 2022, 31, 311–326. [Google Scholar] [CrossRef]
- Das, K.K.; Pattankar, S.; Srivastava, A.K. Arterial Fencing: A Challenge During Complex Craniovertebral Junction Surgery. World Neurosurg. 2022, 161, 147–148. [Google Scholar] [CrossRef] [PubMed]
- Jain VK, Mittal P, Banerji D et al. Posterior occipitoaxial fusion for atrantoaxial dislocation associated with occipitalizedatlas. J Neurosurg 1996, 84, 559–564.
- Ishikawa Y, Kanemura T, Yoshida G, et al. Intraoperative, full-rotation, three-dimensional image (O-arm)-based navigation system for cervical pedicle screw insertion. J Neurosurg Spine. 2011, 15, 472–478.
- Wada K, Tamaki R, Yui M, et al. C1 lateral mass screw insertion caudally from C2 nerve root —an alternate method for insertion of C1 screws: a technical note and preliminary clinical results. J Orthop Sci. 2017, 22, 213–217. [CrossRef]
- El-Gaidi, M.A.; Eissa, E.M.; El-Shaarawy, E.A. Free hand placement of occipital condyle screws: a cadaveric study. Eur Spine J 2014, 23, 2182–8. [Google Scholar] [CrossRef]
- Helgeson MD, Lehman RA, Jr, Sasso RC, et al. Biomechanical analysis of occipitocervical stability afforded by three fixation techniques. Spine J 2011, 11, 245–50. [CrossRef]
- Takigawa T, Simon P, Espinoza Orias AA, et al. Biomechanical comparison of occiput-C1-C2 fixation techniques: C0-C1 transarticular screw and direct occiput condyle screw. Spine (Phila Pa 1976) 2012, 37, E696–701. [CrossRef]
- Van de Kelft, E.; Costa, F.; Van der Planken, D.; Schils, F. A prospective multicenter registry on the accuracy of pedicle screw placement in the thoracic, lumbar, and sacral levels with the use of the O-arm imaging system and Stealth Station navigation. Spine. 2012, 37, E1580–E1587. [Google Scholar] [CrossRef]
- Weinstein, J.N.; Spratt, K.F.; Spengler, D.; Brick, C.; Reid, S. Spinal pedicle fixation: reliability and validity of roentgenogram-based assessment and surgical factors on successful screw placement. Spine. 1988, 13, 1012–1018. [Google Scholar] [CrossRef]
- Vaccaro, A.R.; Rizzolo, S.J.; Balderston, R.A. Placement of pedicle screws in the thoracic spine. Part II: an anatomical and radiographic assessment. J Bone Jt Surg. 1995, 77, 1200–1206. [Google Scholar]
- Giordano, B.D.; Baumhauer, J.F.; Morgan, T.L.; Rechtine, G.R. Cervical spine imaging using standard C-arm fluoroscopy: patient and surgeon exposure to ionizing radiation. Spine (Phila Pa 1976) 2008, 33, 1970–1976. [Google Scholar] [CrossRef]
- Bosco A, Venugopal P, Shetty AP, et al. Morphometric evaluation of occipital condyles: defining optimal trajectories and safe screw lengths for occipital condyle-based occipitocervical fixation in Indian population. Asian Spine J 2018, 12, 214–23. [CrossRef]
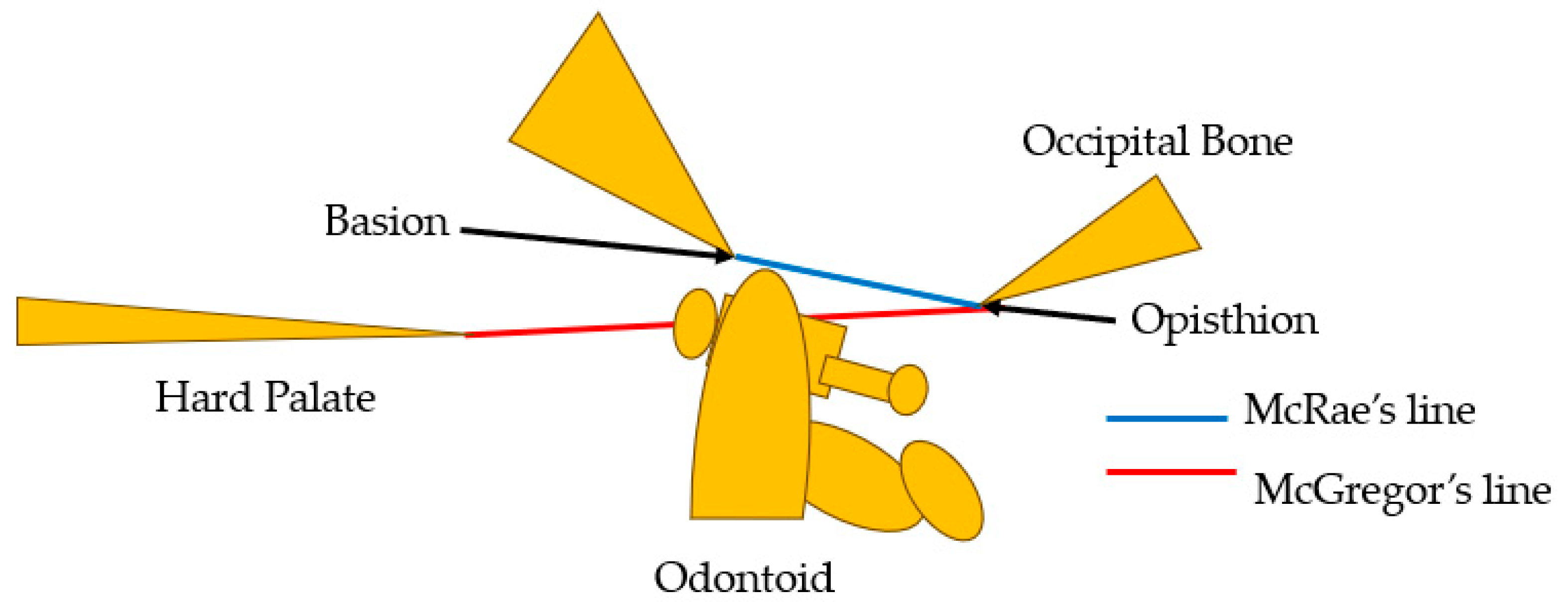
Figure 2.
Preoperative radiograms, A: Antero-posterior radiogram, B: Lateral flexion radiogram, C: Lateral extension radiogram.
Figure 2.
Preoperative radiograms, A: Antero-posterior radiogram, B: Lateral flexion radiogram, C: Lateral extension radiogram.
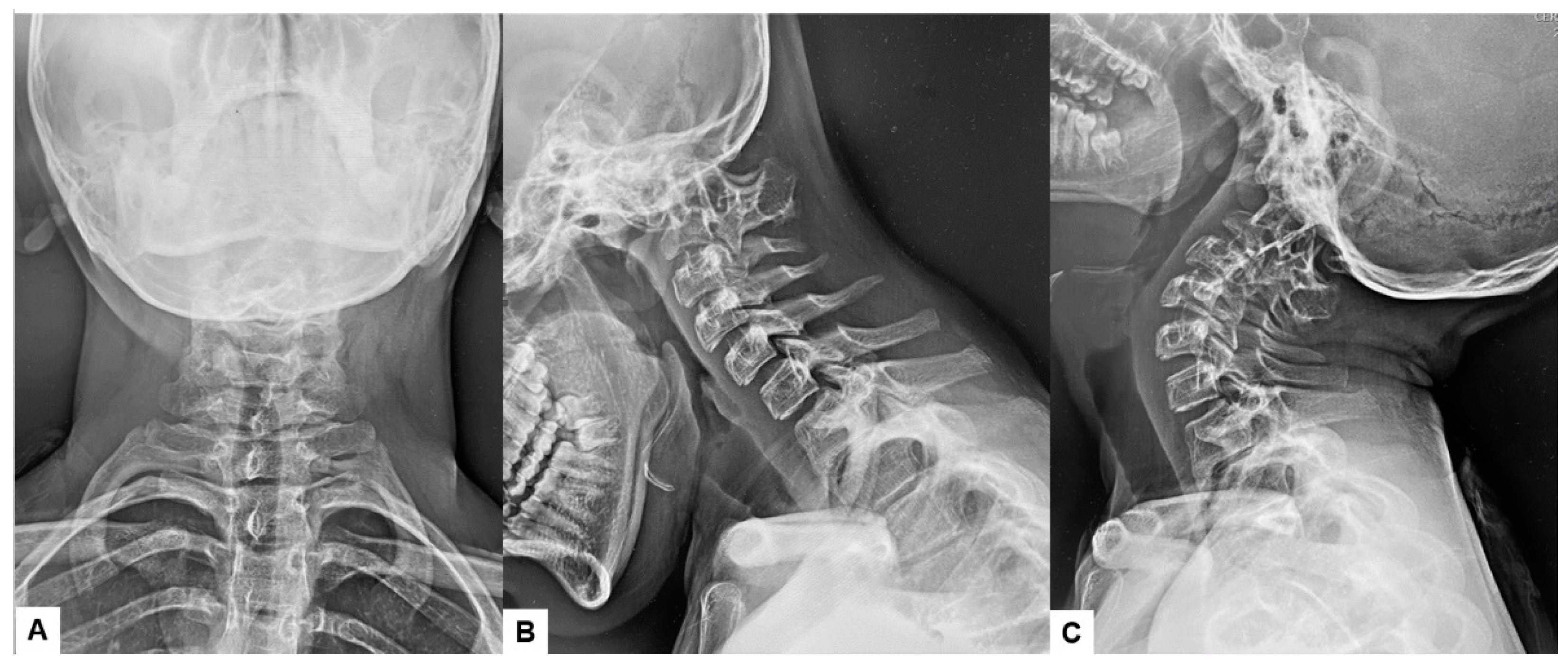
Figure 3.
Preoperative MR imaging, A: T1 weighted mid-sagittal MR imaging, B: T2 weighted mid-sagittal MR imaging, C: T2 weighted axial MR imaging at C1, D: T2 weighted axial MR imaging at C2. Spinal cord was compressed severely due to basilar invagination.
Figure 3.
Preoperative MR imaging, A: T1 weighted mid-sagittal MR imaging, B: T2 weighted mid-sagittal MR imaging, C: T2 weighted axial MR imaging at C1, D: T2 weighted axial MR imaging at C2. Spinal cord was compressed severely due to basilar invagination.
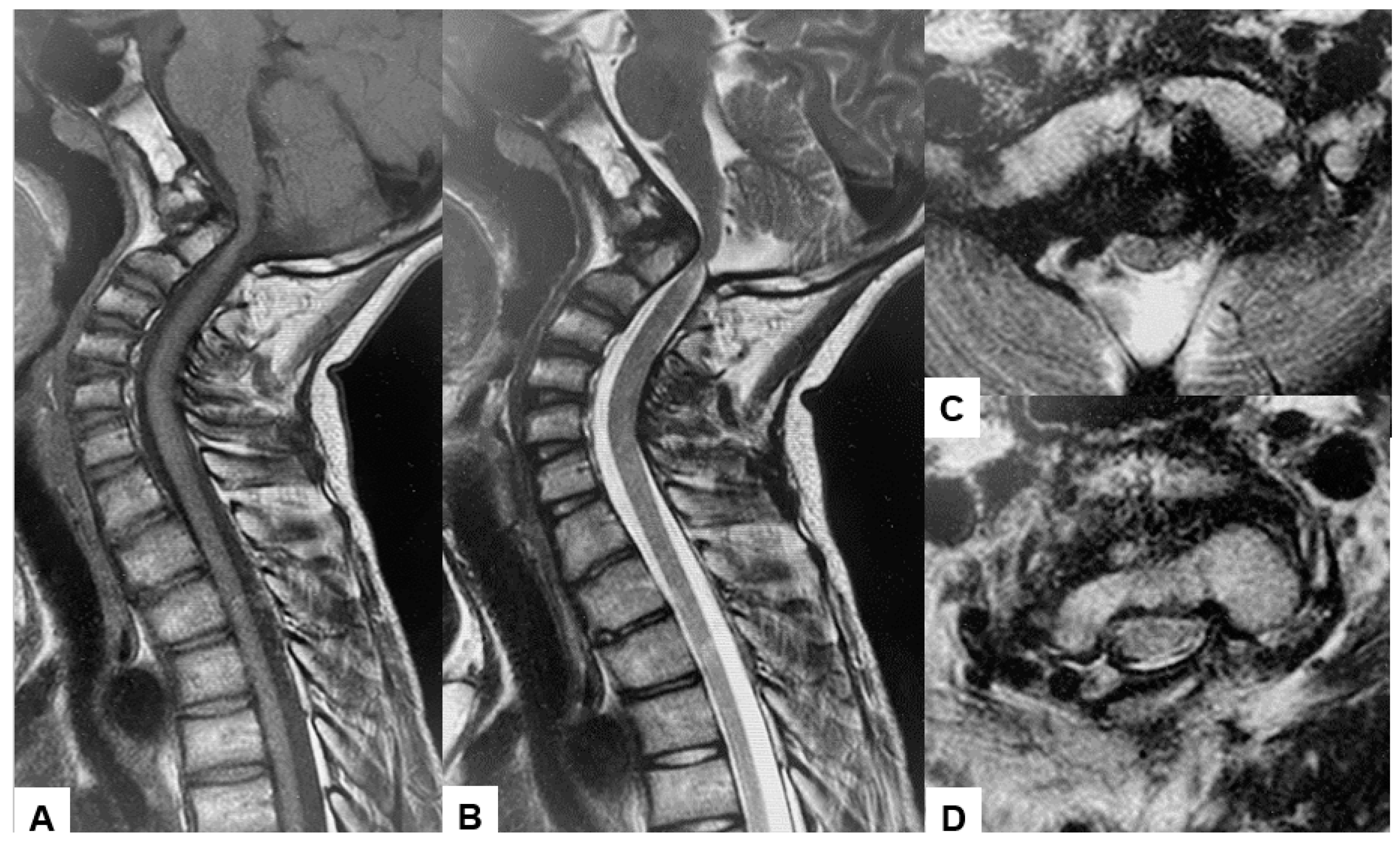
Figure 4.
Preoperative CT, A: Right sagittal reconstruction CT, B: Mid-sagittal reconstruction CT, C: Right sagittal reconstruction CT, D: Axial CT at C1/2. The odontoid process was protruded into foramen magnum.
Figure 4.
Preoperative CT, A: Right sagittal reconstruction CT, B: Mid-sagittal reconstruction CT, C: Right sagittal reconstruction CT, D: Axial CT at C1/2. The odontoid process was protruded into foramen magnum.
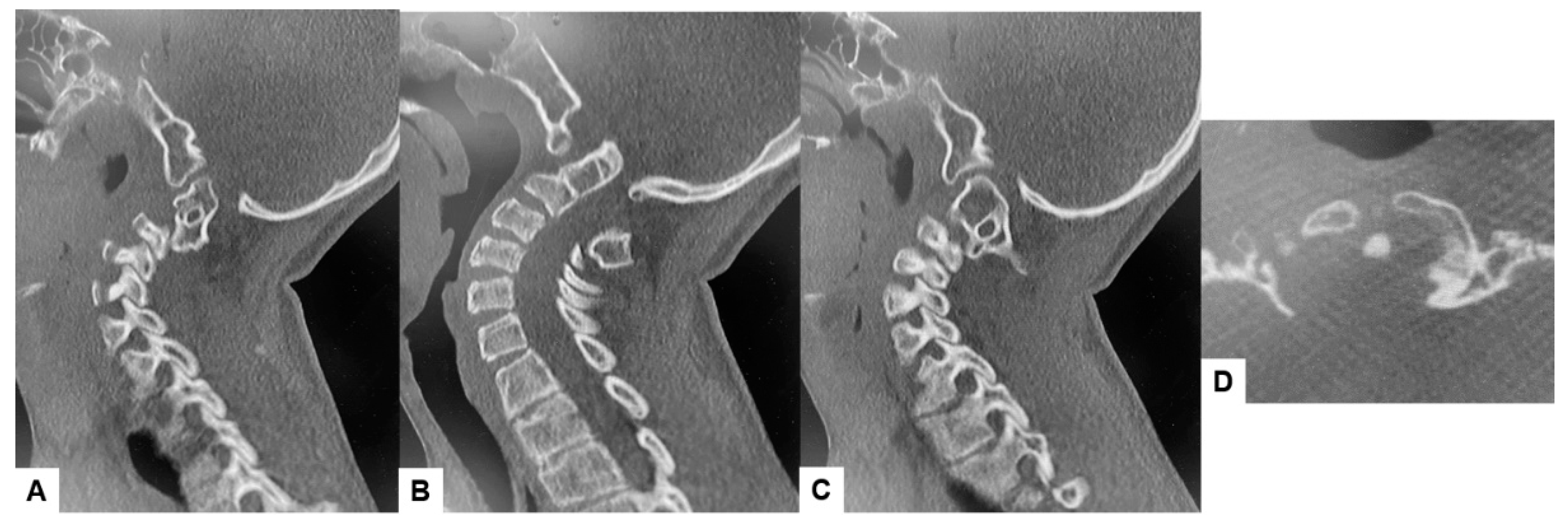
Figure 5.
Preoperative 3D-CT and 3D-CT angiogram, A: Lateral view 3D-CT, B: Posterior view 3D CT, C: Lateral view 3D-CT angiogram, D: Posterior view 3D CT angiogram.
Figure 5.
Preoperative 3D-CT and 3D-CT angiogram, A: Lateral view 3D-CT, B: Posterior view 3D CT, C: Lateral view 3D-CT angiogram, D: Posterior view 3D CT angiogram.
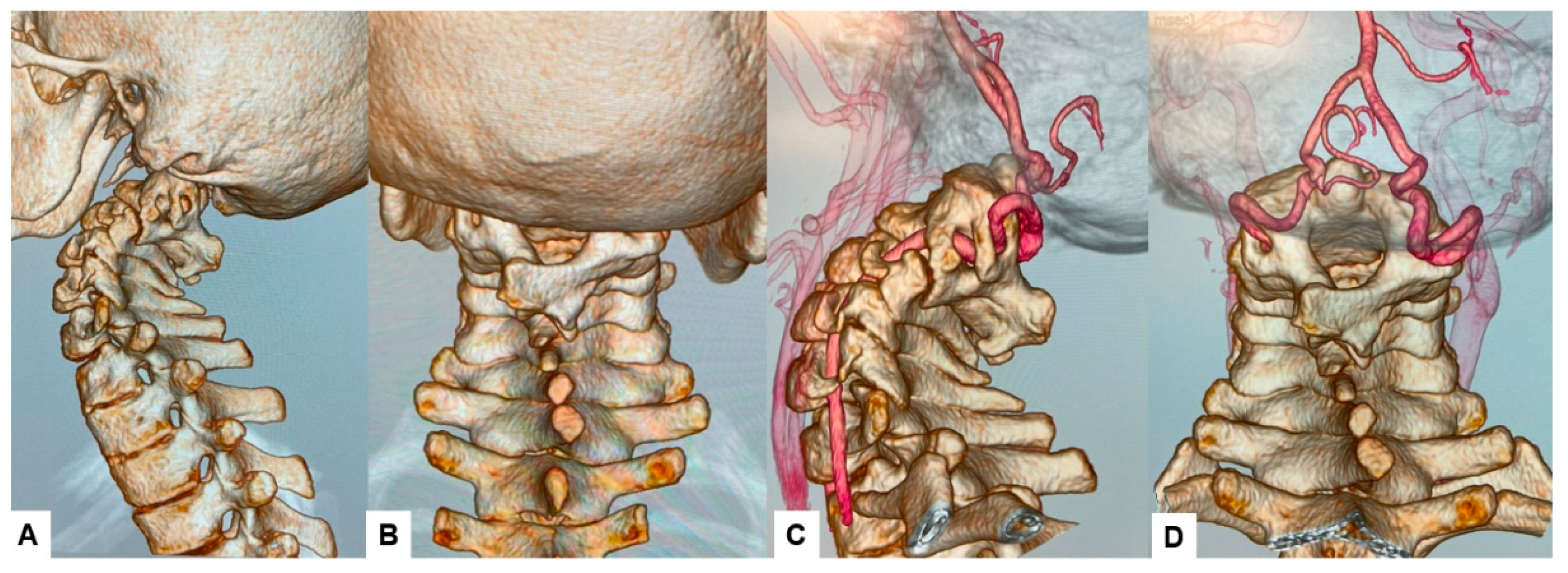

Table 1.
Cranial screw position, lengths, and diameters.
| Author | Safe permissible sagittal plane angulation (degrees) | Medial plane angulation (degrees) | Screw length† (mm) | Screw diameter (mm) |
| La Marca et al. | 30 caudal | 10 medial | 22 (intraosseous) | 3.5 |
| Uribe et al. | Zero to 5 cranial | 15 medial | 20 (intraosseous) | 3.5 |
| El-Gaidi et al. | 4±6.2 caudad angulation (range, from 5 cranially to 12 caudally) | 30±6.7 (range, 20–40) medial | 22±3.1 (intraosseous) | 3.5 |
| Bosco et al. | From 0 to 5 cranial | 23–38 medial | 19.9±2.3 (intraosseous) | 3.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



