Submitted:
05 February 2024
Posted:
06 February 2024
You are already at the latest version
Abstract
New onset diabetes mellitus after transplantation (NODAT) is a common complication following solid organ transplantation, with varying incidence rates due to discrepancies in defining NODAT and follow-up duration, alongside modifiable and non-modifiable risk factors. NODAT adversely affects patient survival and graft longevity, warranting early detection, especially in countries experiencing a rise in kidney transplant cases, emphasizing the need for understanding diagnostic criteria, risk factors, pathogenic mechanisms, and post-transplant outcomes.
Keywords:
NODAT
; transplant
; Kidney
; HbA1c
; GLP1 AR
; Metformin
1. Introduction
Kidney Transplantation is associated with improved quality of life and overall survival than being on dialysis [1]. However, it's crucial to recognize that this life-improving procedure comes with its set of metabolic challenges, most notably the risk of NODAT [2]. NODAT is a common complication after transplant associated with adverse effects on the patient and graft survival.
The development of NODAT is intricately linked to the use of essential immunosuppressive medications posttransplantation, such as glucocorticoids and Calcineurin inhibitors (CNIs) [3]. Moreover, the risk factors for NODAT extend beyond the pharmacological implications of post-transplant care. They also include elements common to the general population predisposing individuals to type 2 diabetes, such as age, family history of diabetes, ethnicity, and pre-transplantation glucose intolerance. Additionally, transplant-specific factors that exacerbate these risks [4] include the type of organ transplanted, the intensity of the immunosuppressive regimen required, and the overall health and preexisting conditions of the transplant recipient. NODAT not only affects the quality of life but is also associated with increased patient and graft loss. Understanding the multifaceted nature of NODAT's etiology is crucial for the medical community. This requires careful selection and management of immunosuppressive therapies, regular monitoring of blood glucose levels, and lifestyle interventions that can help reduce the overall risk of diabetes. Through such comprehensive care strategies, healthcare providers can significantly contribute to improving both the quality and longevity of life for kidney transplant recipients.
Our review article aims to delve into the intricate realm of NODAT in kidney patients, unraveling its complex pathophysiology while shedding light on diverse treatment modalities.
2. Prevalence, Diagnosis, and Risk Factors
2.1. Prevalence and Diagnostic Criteria for NODAT in Kidney Transplant Recipients
Following a kidney transplant (KT), around 10% to 40% of patients experience NODAT, depending on the year after the transplant and the method for diagnosis [5, 6]. The incidence of NODAT was approximately 10% to 20% at 1 year and 25% to 35% at 3 years after KT [7]. The incidence of NODAT is higher in non-kidney organ transplant recipients. The incidence of NODAT in heart transplant recipients ranges between 20% and 30%; in liver transplant recipients, 20%-40%; and in lung transplant recipients, 20%-40% in the first 5 years [8].
The first clear diagnostic criteria for NODAT were introduced in 2003 by the American Diabetes Association and the World Health Organization [9]. This includes a fasting glucose ≥ 126 mg/dL (7 mmol/L) on more than one occasion, random glucose ≥ 200 mg/dL (11.1 mmol/L) with symptoms, or a 2-hour glucose level after a 75-g oral glucose tolerance test (OGTT) of ≥ 200 mg/dL (11.1 mmol/L) or HbA1C > 6.5% (48 mmol/mol) (Table 1). NODAT may be underdiagnosed amid significant anemia rates and reliance on Hba1c [10].
2.2. Risk Factors for NODAT
NODAT development involves multiple factors, primarily centered around β-cell dysfunction alongside insulin resistance. The use of immunosuppressive drugs with diabetogenic effects can contribute to NODAT, particularly in high-risk patients [11]. Table 2 outlines the risk factors for NODAT, which can be divided into two groups— modifiable and non-modifiable. Non-modifiable risk factors include age, ethnicity, male gender, and family history of diabetes, whereas modifiable risk factors include immuno-suppression, rejection episodes, obesity, and hepatitis C virus infection [12].
2.2.1. Age
Advanced age and an extended duration of dialysis have been identified as factors contributing to an elevated risk of developing NODAT. These factors are closely associated with a decline in the Psoas Muscle Index (PMI) and an increase in intermuscular adipose tissue, both indicators of deteriorating muscle health and quality. Research indicates that a lower PMI correlates with higher levels of high-molecular-weight adiponectin, which can exacerbate insulin resistance and elevate the risk of NODAT [13].
In addition to the loss of muscle mass, aging is linked to a reduction in the efficiency of glucose transport into muscle cells, primarily due to decreased functionality of the GLUT4 transporter. This impairment is compounded by increased adiposity and inflammation commonly associated with aging, further contributing to insulin resistance in elderly individuals [14]. Moreover, increasing age in transplant recipients is also tied to enhanced apoptosis in aging islet β cells. This cellular decline results in diminished insulin secretion, posing a higher risk of NODAT, particularly in recipients aged 45 years or older [15]. Understanding these interconnected factors is crucial for managing and mitigating the risk of NODAT in the transplant population, especially among older recipients.
2.2.2. Gender
Males are at a heightened risk for developing NODAT compared to their female counterparts. This increased susceptibility in males can be attributed to a combination of genetic, hormonal, and physiological factors [16] [17]. Males typically have a higher prevalence of visceral obesity – fat stored within the abdominal cavity, which is a known risk factor for insulin resistance and type 2 diabetes [18, 19]. Conversely, females are found to have a risk of NODAT due to lower muscle mass, resulting in reduced blood sugar uptake [13].
2.2.3. Genetic Predisposition to NODAT
Over the past two decades, studies have highlighted the increased risk of type 2 diabetes associated with genetic predisposition, although the risk tied to each gene is relatively small [20]. Several studies have identified an association between NODAT in kidney transplant recipients and specific common single nucleotide polymorphisms (SNPs). These SNPs are found in genes responsible for proteins involved in β-cell apoptosis, ATP-sensitive potassium channels, adiponectin, leptin, inflammatory pathways, and elements of the innate immune system. Individuals carrying multiple SNPs in diabetic genes faced an amplified risk. NODAT has also been correlated with SNPs in various IL genes, notably IL-2, IL-7R, IL-17R, IL-1B, IL-4, IL-17-RE, IL-17R, and IL-17RB [21]. Additionally, SNPs in transcription factor NFATc4 and adiponectin were associated with NODAT [22, 23]. Limited literature suggests that African Americans and Hispanics face a higher susceptibility to developing NODAT in comparison to whites. The risk ratio for NODAT is elevated by 32–68% in Black patients and 35% in Hispanic patients when compared to their white counterparts [16].
2.2.4. Obesity
NODAT exhibits a strong connection with visceral obesity, leading to the generation of inflammatory cytokines such as interleukin-6 and tumor necrosis factor-α, along with reduced levels of adiponectin associated with insulin resistance [19, 24, 25]. Visceral fat demonstrates resistance to the lipolytic effects of insulin and, upon mobilization, can impede liver metabolism. This interference may result in heightened hepatic gluconeogenesis, diminished apolipoprotein B degradation, and increased production of triacylglycerol-rich lipoproteins [26].
2.2.5. Immunosuppressive Agents
Various immunosuppressive agents have well-documented diabetogenic effects. Corticosteroids can diminish insulin sensitivity in the body's periphery, hinder pancreatic insulin production and secretion, and heighten hepatic gluconeogenesis. Calcineurin Inhibitors (CNIs) like Tacrolimus and Cyclosporine decrease insulin synthesis and secretion. Sirolimus exacerbates peripheral insulin resistance and disrupts the pancreatic beta-cell response. Antimetabolites such as azathioprine and mycophenolic acid derivatives (like Mycophenolate mofetil and Mycophenolate sodium) do not induce diabetes.
2.2.6. Viral Infection
Hepatitis C virus (HCV) infection poses a risk for NODAT [27] , as observed in a retrospective study involving 427 kidney transplantation recipients [28]. The heightened risk of NODAT associated with HCV infection may be attributed to multiple factors, such as direct replication of the HCV virus in pancreatic islet β cells leading to dysfunction and autoimmune destruction, causing inadequate insulin synthesis and secretion; direct damage to liver cells by HCV, resulting in impaired insulin utilization and insulin resistance; and the potential impact of HCV on the synthesis of insulin-related proteins through mediation of the insulin signaling pathway, ultimately affecting insulin secretion [29].
3. Pathophysiology of NODAT
NODAT exhibits similarities to pre-transplant diabetes mellitus but encompasses other distinct mechanisms leading to hyperglycemia, marking it as a separate entity due to post-transplant risk factors that accelerate the risk of developing diabetes. Impaired insulin sensitivity [30, 31], abnormal insulin production from pancreatic β-cell dysfunction [32, 33], uncontrolled glucagon release [34], hypertriglyceridemia, and obesity all contribute to the risk for NODAT. Although the dominant pathophysiological process behind NODAT is debated, some groups highlight β-cell dysfunction as a primary mechanism [32, 33]. (Figure 1)
3.1. Insulin Resistance
Factors contributing to reduced insulin sensitivity in transplant recipients include age, male gender, obesity, and renal function [35]. Medications commonly used in transplantation, such as CNIs and rapamycin, have been associated with heightened insulin resistance. Cyclosporine A and Tacrolimus, at therapeutic levels, hinder glucose uptake independently of insulin signaling by accelerating endocytosis, leading to GLUT4 removal from cell surfaces, thus fostering insulin resistance [36]. The calcineurin/NFAT pathway, among others, controls gene transcription in skeletal muscle, with its inhibition potentially promoting insulin-resistant myosin fast fibers and contributing to insulin resistance onset [37].
Insulin resistance and insulin deficiency work together to cause hyperglycemia after kidney transplantation. [30] Studies tracking insulin sensitivity posttransplantation reveal a decline early on, showing defects in insulin secretion that correlate with glucose tolerance and the development of NODAT. Patients with NODAT sustain reduced insulin secretion even years after transplantation, while differences in insulin sensitivity become less pronounced than those with normal glucose levels. This sustained decrease in insulin secretion might stem from the ongoing use of immunosuppressive medications that harm β-cells, while insulin sensitivity tends to fluctuate.
3.2. β-Cell Dysfunction
β-cell dysfunction plays a major role in the pathogenesis of NODAT [32]. The development of NODAT is closely linked to β-cell dysfunction, which is influenced by factors such as glucolipotoxicity, reduced insulin biosynthesis and secretion, and decreased β-cell mass. This dysfunction is often a result of β-cell dedifferentiation, a process wherein cells regress from a specialized to a less specialized state under stress, involving critical transcription factors [38, 39]. This dedifferentiation serves as a defensive mechanism against various stresses, including glucolipotoxicity, oxidative and endoplasmic reticulum stress, mitochondrial dysfunction, and inflammation. During this process, cells revert to a more primitive developmental stage without undergoing cell death, thereby altering their form and function [40].
Before transplantation, B cell damage may already be present and play a role in NODAT, as demonstrated by research. Immunosuppressive medications, notably Tacrolimus and cyclosporine A, contribute to NODAT, particularly in patients with pre-transplant risk factors such as obesity and dyslipidemia. These drugs hinder insulin secretion and content, especially in individuals with preexisting damage to β cells, underscoring the significance of prior dysfunction in the development of NODAT [40]. Proinsulin, a marker indicating pancreatic β-cell dysfunction, reflects β-cell stress when insulin demands surpass current capacity, preceding diabetes diagnosis and serving as a predictor for NODAT development, even with normal glucose levels. Elevated proinsulin levels (>10 pmpl/L) signify insulin resistance, as demonstrated by the IRIS-II study [41], with 80% of Renal Transplant Recipients in the Pancreatic β-Cell Dysfunction risk for NODAT study surpassing this threshold, suggesting compromised β-cell function due to metabolic demands and prolonged exposure to immunosuppressive medications, thereby heightening NODAT risk for transplant recipients [33].
Insulin resistance and β-cell dysfunction are early indicators in the progression of diabetes, characterized by a hyperbolic relationship influenced by a negative feedback loop. Normally, Pancreatic β-cells adjust to variations in insulin sensitivity, maintaining near-normal plasma glucose levels through compensatory increases in insulin secretion in healthy individuals. However, kidney transplant recipients (KTR) exhibit heightened insulin resistance, influenced by factors like obesity, waist-to-hip ratio, and prednisolone treatment, as demonstrated by Oterdoom et al. [33].
3.3. Role of Immunosuppressive Medications
Immunosuppressive medications such as glucocorticoids, CNIs, and mammalian target of rapamycin inhibitors significantly contribute to the onset of NODAT [7, 42,43,44], and hold greater significance than conventional risk factors.
3.3.1. Glucocorticoids
The process behind how glucocorticoids cause high blood sugar involves several factors: they make the body more resistant to insulin, decrease insulin production, and increase the creation of new glucose. They trigger the liver to generate more glucose by activating specific genes and boosting the impact of hormones like glucagon and epinephrine [45]. Glucocorticoids also disrupt normal appetite control, resulting in weight gain and further insulin resistance. The question of whether steroids induce weight gain or if it stems from improved appetite due to reduced uremia remains a topic of debate.
Although all forms of glucocorticoids can raise blood sugar levels, it's more likely to happen with higher doses and longer treatment periods [45]. Administration of high-dose glucocorticoids, specifically at a dosage of 10 mg or higher, has the potential to trigger insulin resistance. Information gathered from registries suggests that regimens devoid of steroids carry a reduced risk of developing DM [46]. In a study encompassing 57 KTRs, the gradual reduction of prednisolone dosage from 10 mg to 5 mg daily resulted in improved insulin sensitivity. Notably, completely discontinuing prednisolone did not yield any additional enhancement in insulin sensitivity [47].
3.3.2. CNIs
CNIs, a set of medications used to suppress the immune system in autoimmune diseases and post-organ transplants, play a vital role in preventing T cell-mediated immune reactions. However, while their primary function is inhibiting immune responses, these drugs can lead to elevated blood sugar levels due to their interference with calcineurin phosphatase activity, inhibiting insulin production by B-cells. This enzyme is not only present in immune cells but is also distributed in tissues like the pancreas, impacting insulin secretion and resulting in hyperglycemia. The process leading to high blood sugar involves multiple stages of insulin secretion, from mRNA transcription to post-translational modification [48].
The effect of CNIs on blood sugar varies significantly among individuals. The degree of hyperglycemia is influenced by the dosage and the specific medication used. Tacrolimus has been linked to higher rates of elevated blood sugar compared to cyclosporine. This difference might be due to the differing concentrations of their binding proteins in various tissues. Tacrolimus binding protein is highly concentrated in pancreatic cells, affecting insulin production, while cyclosporine binding protein is more prevalent in other organs like the heart, liver, and kidneys [49]. Hence, Tacrolimus, a commonly prescribed immunosuppressant post-transplant, requires diligent monitoring of indicators like blood drug concentration, plasma glucose levels, and kidney function. Furthermore, other immunosuppressant’s, like Sirolimus and Everolimus, present a lower risk of disrupting glucose metabolism than CNIs [50].
3.3.3. Sirolimus
mTOR inhibitors diminish insulin signaling by suppressing the phosphorylation of protein kinase B in liver, fat, and muscle cells and induce β-cell apoptosis [51]. Administration of Sirolimus, an inhibitor targeting the mammalian target of rapamycin (mTOR), has been recognized as a contributing factor to the emergence of NODAT. Johnston et al. conducted an analysis using USRDS data, revealing that Sirolimus, irrespective of its combination with a calcineurin inhibitor or an antimetabolite like mycophenolate mofetil or azathioprine, was independently linked to an elevated risk of NODAT [52]. Meanwhile, Teutonico et al. observed in a prospective study involving renal transplant recipients that substituting calcineurin inhibition with Sirolimus exacerbated insulin resistance and diminished insulin responsiveness. Notably, these disruptions in glycemic control were correlated with an escalation in serum triglyceride levels, a well-known side effect associated with the use of mTOR inhibitors [53].
3.3.4. Everolimus
A recent meta-analysis examining the combination of CNI plus mTOR inhibitors in new KTRs found no significant increase in the incidence of NODAT at the 1-year mark compared to CNI plus antiproliferative agents across 13 studies involving 4561 participants (relative risk 1.16, 95% confidence interval 0.97–1.38, P = .10) [54]. These findings were corroborated by the TRANSFORM study, a 24-month prospective trial involving 2037 new KTRs randomized to receive Everolimus with reduced-exposure CNI versus mycophenolate with standard-exposure CNI, where no difference in NODAT incidence was observed (risk ratio 1.09, 95% CI 0.87–1.37), along with comparable efficacy and graft function [55]. Despite the absence of variance in NODAT incidence, the potential cause could be attributed to the reduction in CNI dosage.
4. Management and Treatment
4.1. Pharmacological Management of NODAT
4.1.1. Immunosuppressive Drug Adjustments
The initiation of an immunosuppressive regimen before a kidney transplant aims to lower the recipient's immune function. The tailored selection of this regimen hinges on the recipient's circumstances and the perceived immunological risk. Presently, there's no consensus on the preferred immunosuppression regimen to prevent NODAT. However, in the modern era of immunosuppression, the regimen should balance immunologic risk against potential complications like NODAT in kidney transplant recipients [43, 56, 57]. In the HARMONY trial, which centered on recipients treated with Tacrolimus and mycophenolic acid, it was discovered that swift withdrawal of corticosteroids decreased the occurrence of NODAT without elevating the risk of rejection [58].
Younger and overweight patients experience advantages from steroid avoidance protocols, particularly when the risk of rejection is offset by T-cell-depleting therapy (such as TMG/ALEM), as highlighted in a study published in Kidney Med [46]. Moreover, the response to steroid withdrawal appears to differ based on age. In older Solid Organ Transplant recipients, a population-based study indicated more favorable outcomes, including reduced NODAT and mortality, following early steroid withdrawal. However, this benefit is tempered by an elevated risk of rejection. A registry analysis involving 6,070 KTRs emphasized that discontinuing steroids after anti-IL-2 induction therapy within the initial 18 months posttransplantation correlated with a heightened risk of graft loss compared to continuous steroid maintenance. Considering these findings, the decision to pursue a steroid avoidance regimen should be carefully assessed against potential graft-related risks. When contemplating steroid avoidance, induction therapy with lymphocyte depletion may represent a prudent approach [59].
Immunosuppressive drugs significantly contribute to NODAT development. Customizing these drugs could mitigate the NODAT risk, but such adjustments should not jeopardize graft survival. Decreasing corticosteroid dosage during the initial post-transplant year has notably enhanced glucose tolerance. Swift tapering of steroids in low immunological risk patients with a high NODAT risk and personalized steroid-sparing protocols show promise [60]. Retrospective trials favoring corticosteroid-sparing regimens at discharge exhibited significant benefits concerning NODAT at three years compared to corticosteroid-containing regimes [61]. For patients at high NODAT risk but low immunological risk, the other choices of immunosuppressive regimen include belatacept-based or cyclosporine therapies. In cases where it is difficult to control NODAT, a switch from Tacrolimus to Cyclosporine might be beneficial[9] . Moreover, Effective management of renal transplant patients involves baseline assessments pre-transplantation and personalized immunosuppressive therapy selection, especially for those at high NODAT risk posttransplantation. Close monitoring posttransplantation, particularly for patients with abnormal glucose metabolism [62] .
4.1.2. Antidiabetic Medications
The use of different medications to manage NODAT involves multiple approaches, each with distinct effects and considerations. Insulin therapy in the early months of posttransplantation aims to counter stress hyperglycemia and preserve β-cell function. Studies suggest that early insulin supplementation could potentially reduce NODAT cases by safeguarding β-cells[8]. However, larger trials regarding aggressive blood sugar control using insulin in the early transplant phase showed inconclusive outcomes. For mild hyperglycemia after transplantation, antihyperglycemic agents are preferred over insulin [63].
Metformin is recommended as a first-line oral therapy if certain conditions are met for kidney transplant recipients. Its potential benefits, including glucose reduction and improved insulin sensitivity, have been noted, although its safety posttransplantation remains uncertain[64]. Studies exploring metformin's safety in kidney transplant recipients indicate no significant negative impact on patient or graft survival, and it can be used in subjects with eGFR >30ml/min. Yet, the safety and efficacy of metformin posttransplantation require further substantiation through large randomized controlled trials [65].
Dipeptidyl peptidase 4 inhibitors (DPP4i) have shown promise in NODAT treatment by potentially improving insulin sensitivity and protecting β-cell mass. DPP-4 inhibitors work by blocking the action of DPP-4, an enzyme that destroys the hormone incretin. Incretins help the body produce more insulin only when it is needed and reduce the amount of glucose being produced by the liver when it is not needed. These inhibitors, like sitagliptin, have demonstrated increased insulin sensitivity in patients with NODAT. Their tolerability and minimal side effects make them a more frequent choice for NODAT treatment, particularly due to their limited interaction with common immunosuppressive drugs [66,67,68] . In a study with a total 61 patients, they found that Initiating sitagliptin promptly in the initial week post-transplant for hyperglycemia (blood glucose >200 mg/dL) and discontinuing it by the third month in non-diabetic patients led to a notable 18.06% absolute risk reduction in abnormal OGTT outcomes [69] .
Glucagon-like peptide-1 receptor agonists (GLP-1 RA) have proven beneficial in improving insulin secretion and reducing hypoglycemia episodes [34] . They offer weight loss benefits and potentially enhance cardiovascular health. However, their use may lead to gastrointestinal issues and requires consideration of their interaction with immunosuppressive drugs [70, 71]. GLP-1 RA primarily functions by inhibiting post-meal glucagon secretion and reducing hepatic glucose production while also slowing gastric emptying and suppressing appetite. Notably, in KTRs, these agents offer benefits, including a 1.5-2% decrease in HbA1c, reduced insulin needs, lower postprandial and fasting blood sugars, and a 2 kg weight loss within three weeks [72].
Sodium–glucose cotransporter 2 inhibitors (SGLT2) reduce blood sugar levels and have demonstrated cardiovascular benefits in non-transplant populations. However, their effects and safety in renal transplant recipients remain unclear. While they can effectively control glucose and body weight, especially in patients with good graft function, their potential complications, including urinary tract infections and risks of hypotension or acute kidney injury, warrant careful evaluation.[73] The risk-benefit ratio of using SGLT2 inhibitors in the immediate post-transplant period needs cautious assessment, considering their potential complications, especially in cases of insulin deficiency or acute illness [74]. SGLT2 inhibitors, particularly empagliflozin, have been shown to exhibit positive effects on blood glucose levels and have the potential to slow chronic kidney disease progression. It has also been shown to be useful in KTRs. In the in vitro model, Empagliflozin demonstrated renal protection against the adverse effects of Tacrolimus, mitigating kidney damage in laboratory settings. Tacrolimus increases SGLT-2 levels, but empagliflozin counteracts this effect by reducing these levels, promoting sugar excretion in urine, enhancing blood sugar regulation, increasing insulin production, and protecting against Tacrolimus-induced kidney damage[75, 76].
In summary, various medications show promise in managing NODAT posttransplantation, but larger randomized controlled trials are essential to confirm their efficacy and safety in this specific patient population. The choice of medication needs to consider its potential benefits and its interactions with immunosuppressive drugs and the individual patient's condition to optimize outcomes and minimize adverse effects.
4.2. Potential Novel Therapies or Approaches
Novel therapies, extensively studied in the context of T2DM, hold considerable promise for addressing the challenges of managing NODAT. By leveraging advanced insulin formulations, medications targeting compromised mitochondrial function like Imeglimin, and drugs that enhance GLP-1 production, along with oral GLP-1 receptor agonists available in small molecular form, individuals with NODAT can potentially benefit from improved blood sugar control and weight management. Moreover, exploring single-molecule peptides interacting with multiple gut hormone receptors, particularly GIP and GLP-1 co-agonists and potential agonists for GLP-1 and peptide YY, presents opportunities for addressing metabolic challenges in NODAT patients. Thus, the translational potential of these therapies from T2DM to NODAT offers hope for more effective management strategies in this patient population [77].
4.3. Lifestyle Interventions and Dietary Considerations
Adopting habits to encourage fat and energy expenditure, engaging in moderate physical activity, and aiming for moderate weight loss are recommended strategies for lowering the risk of type 2 diabetes mellitus [78, 79]. In the DIADEM-I study conducted by Taheri et al. in primary care and community settings, intensive lifestyle interventions resulted in significant weight loss within 12 months, diabetes remission in over 60% of participants, and normalization of blood sugar levels in more than 30% [80]. However, there is insufficient clear evidence regarding the impact of lifestyle changes on the risk of NODAT. Another trial involving 103 kidney transplant recipients, focusing on glycemic control strategies and led by renal dietitians, showed no improvement in surrogate markers of glucose metabolism despite active lifestyle intervention [81]. Nevertheless, recent smaller studies have indicated promising results from moderate-to-vigorous physical exercise and adherence to Mediterranean-style or plant-based diets in potentially reducing NODAT risk [82, 83].
Boosting physical activity and muscle mass can aid in preventing NODAT. Physical activity stimulates 5-alpha-AMPKs, which improves glucose absorption, fatty acid oxidation, and enhances muscle glucose uptake [84]. Lastly, bariatric surgery, such as gastric sleeve, provides considerable advantages for obese patient’s post-kidney transplantation, offering significant and enduring weight loss along with improvements in comorbidities and graft function. This procedure is favored over the Roux-en-Y method due to its association with lower risks of oxalate stones and decreased absorption of immunosuppressants [85].
5. Complications and Long-Term Consequences
5.1. Short-Term Complications of NODAT
After the onset of NODAT, nephropathy has been detected in transplanted kidneys [87,88]. Additionally, neuropathy is linked to this condition [89]. Studies have indicated that NODAT correlates with diminished inner neuro-sensory retinal layers while vascular density remains relatively unchanged. This implies that early neuroretinal degeneration might precede vascular alterations due to NODAT [86].
5.2. Long-Term Consequences on Graft and Patient Survival
NODAT significantly impacts patient survival, graft rejection, graft loss, and infectious complications post-kidney transplant. A study involving 173 renal transplant recipients showed that 1-year patient survival rates were notably lower in those with NODAT compared to those without (83% vs. 98%, respectively; P < 0.01) [87]. Data from over 11,000 Medicare beneficiaries revealed that NODAT increased the risk of graft failure by 63%, death-censored graft failure by 46%, and mortality by 87% compared to individuals without diabetes [7].
5.3. Impact on Cardiovascular Health
NODAT is associated with a 60% increase in posttransplantation myocardial infarction, increased risk of cerebrovascular accidents, as well as aortic or lower extremity arterial disease [88] [89]. There has been noted to have a strong correlation between fasting hyperglycemia and cardiovascular (CV) risk post-transplant, akin to associations observed in the general population. The findings imply a continuous relationship between elevated fasting plasma glucose levels and CV risk in transplant recipients, suggesting a notably brief interval between the onset of hyperglycemia, heightened CV risk, and mortality, possibly due to preexisting cardiovascular disease in patients with post-transplant diabetes mellitus [90].
NODAT, characterized by hyperglycemia, shares similarities with DM2's impact on the cardiovascular system. Oxidative stress emerges as a critical factor contributing to the complications associated with NODAT, affecting both microvascular and cardiovascular health. The experimental evidence reviewed here underscores how the metabolic irregularities characteristic of diabetes contributes to an excess production of mitochondrial superoxide. This heightened production serves as a central mediator in the tissue damage seen in diabetes, activating five pathways implicated in complication pathogenesis and directly impairing two antiatherosclerotic enzymes, endothelial nitric oxide synthase and prostacyclin synthase [91]. (Figure 2)
Furthermore, the interplay between hyperglycemia and hypertension, often attributed to factors like obesity, insulin resistance, and hyperinsulinemia, underscores a complex relationship. Hyperglycemia itself can instigate changes in vascular function and structure, leading to hypertension. This hypertensive state, in turn, can precipitate conditions such as hypertrophic cardiomyopathy and coronary artery disease (CAD). These insights emphasize the multifaceted nature of cardiovascular complications associated with NODAT and underscore the importance of addressing both hyperglycemia and hypertension in mitigating its impact on cardiovascular health [92].
6. Prevention Strategies
6.1. Strategies for Preventing NODAT Pre-Transplant
The initial step in averting NODAT involves recognizing the risk factors preceding transplantation. Individuals awaiting kidney transplants necessitate a comprehensive assessment of their diabetes susceptibility before being enlisted. High-risk patients should be advised on preventive measures such as weight management, lifestyle adjustments, monitoring caloric intake, and engaging in physical activity. For individuals at heightened risk of NODAT, like those aged over 45 years [16], individuals with a familial history of diabetes, individuals with metabolic syndrome coupled with elevated triglyceride levels [93], high blood pressure, impaired fasting glucose [94] , or those with HCV infection[95], it is recommended to assess HbA1c levels and conduct OGTTs [8,96].
6.2. Early Post-Transplant Interventions to Minimize NODAT Risk
HbA1c levels may not accurately reflect blood glucose in the initial phase following a transplant due to factors such as bleeding, bone marrow suppression, or erythropoietin administration in cases of delayed graft function [97]. Jenssen T et al. proposed maintaining fasting plasma glucose below 7 mmol/L (126 mg/dL) and post-meal glucose levels below 10 mmol/L (180 mg/dL) during the early post-transplant period [98]. It's typically advised to aim for HbA1c levels between 7.0% and 7.5% (53–58 mmol/mol) during this time [99].
7. Current Ongoing Research in the Field
In terms of ongoing research, one study [100] presents compelling evidence suggesting that human B cell dysfunction triggered by Tacrolimus and Sirolimus in NODAT patients is reversible and preventable. According to the study, the dysfunction induced by these drugs can be reversed upon discontinuation of the medication and can be prevented through coadministration of the GLP-1 agonist Exendin-4 (Ex-4). These findings hold significant clinical relevance. Notably, Ex-4 and tacrolimus target overlapping pathways, with tacrolimus inhibiting calcineurin, while GLP-1 receptor (GLP-1R) signaling in β cells has been demonstrated to activate calcineurin. Findings suggest that activating calcineurin through the GLP-1R in β cells can counteract the inhibition induced by Tacrolimus, thereby averting insulin secretory deficits. These insights provide valuable guidance for managing B cell dysfunction in post-transplant DM patients, offering potential avenues for therapeutic intervention and improved patient outcomes. However, further corroborative research and clinical trials are imperative to solidify the reliability of these conclusions and establish concrete preventive measures against the adverse effects of Tacrolimus and Sirolimus on β cell function.[100]
Recent advancements in genome sequencing have catalyzed extensive investigation into the role of the gut microbiota in various diseases, notably metabolic disorders such as diabetes. Despite strides in comprehending the intricate relationship between gut bacteria and the host, particularly concerning inflammation and disease progression, establishing a definitive causal link remains a formidable task. Dysbiosis, characterized by gut bacteria imbalance, has been associated with diabetes and its complications, including retinopathy, neuropathy, and cardiac diseases.[101] Studies have revealed associations between antidiabetic medications like metformin and the gut microbiome, shedding light on their antidiabetic mechanisms by modulating inflammation, gut permeability, glucose homeostasis, and Short-chain fatty acids (SCFA)-producing bacteria. [102] Conversely, the impact of SGLT2 inhibitors on the gut microbiome remains relatively unexplored, contrasting with the well-documented effects of metformin. While some trials have shown no significant differences in microbiome composition between dapagliflozin and gliclazide, others have observed empagliflozin promoting beneficial bacteria, such as Eubacterium and Faecalibacterium, while reducing potentially harmful ones. The early and consistent alterations in gut microbiome and plasma metabolites following empagliflozin initiation suggest adaptability to biochemical shifts, necessitating longer-term assessments and more frequent monitoring for conclusive insights. [103] While certain bacteria exhibit promises as therapeutic targets, further investigation, particularly through human trials, is imperative to explore the efficacy of interventions like prebiotics, probiotics, and fecal microbiota transfer in managing diabetes and its associated complications, which can be applied on NODAT patients.
8. Conclusions
In conclusion, NODAT can impact over 20% of patients following kidney transplantation, leading to increased risks of graft and patient loss, as well as decreased quality of life due to various complications, such as cardiovascular diseases. Therefore, it is crucial to consider NODAT in post-transplant care. This study examines factors predisposing patients to NODAT risk, including immunosuppression, age, viral infections, gender, and obesity. Moreover, it discusses treatment options, including oral antidiabetic medications, adjustment of immunosuppressants, and lifestyle modifications, which serve both as treatment and preventive measures against NODAT. Recognizing these factors and implementing appropriate interventions are essential for optimizing patient outcomes posttransplantation.
Author Contributions
Both authors contributed to the study design and writing.
Funding
None.
Institutional Review Board Statement
None.
Informed Consent Statement
Not needed.
Data Availability Statement
.
Acknowledgments
None.
Conflicts of Interest
None.
References
- R A Gatchalian and, D.J. Leehey, Mortality among patients on dialysis, patients on dialysis awaiting transplantation, and transplant recipients. 2000.
- Addendum. 2. Classification and Diagnosis of Diabetes: <i>Standards of Medical Care in Diabetes—2021</i>. Diabetes Care 2021;44(Suppl. 1):S15–S33. Diabetes Care 2021, 44, 2182–2182. [CrossRef]
- Hecking, M. , et al. , Management of post-transplant diabetes: immunosuppression, early prevention, and novel antidiabetics. Transplant International, 2021, 34, 27–48. [Google Scholar] [CrossRef] [PubMed]
- Hecking, M. , et al. , Novel views on new-onset diabetes after transplantation: development, prevention and treatment. Nephrology Dialysis Transplantation, 2013, 28, 550–566. [Google Scholar] [CrossRef] [PubMed]
- Hagen, M. , A 6-year prospective study on new onset diabetes mellitus, insulin release and insulin sensitivity in renal transplant recipients. Nephrology Dialysis Transplantation, 2003, 18, 2154–2159. [Google Scholar] [CrossRef]
- Porrini, E.L. , et al., Clinical evolution of post-transplant diabetes mellitus. Nephrology Dialysis Transplantation, 2016, 31, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Bertram L Kasiske 1, J.J.S. , David Gilbertson, Arthur J Matas, Diabetes mellitus after kidney transplantation in the United States. American Journal of Transplantation, 2003.
- Jenssen, T. and A. Hartmann, Post-transplant diabetes mellitus in patients with solid organ transplants. Nature Reviews Endocrinology, 2019, 15, 172–188. [Google Scholar] [CrossRef]
- Davidson, J. , AlanDantal, JacquesDotta, FrancescoHaller, HermannHernandez, DomingoKasiske, Bertram L. Kiberd, BryceKrentz, AndrewLegendre, ChristopheMarchetti, PieroMarkell, Marianavan der Woude, Fokko J.Wheeler, David C., NEW-ONSET DIABETES AFTER TRANSPLANTATION: 2003 INTERNATIONAL CONSENSUS GUIDELINES. 2003, 75, ss3–ss24. [Google Scholar] [CrossRef]
- Katwal, P.C. , et al., The Effect of Anemia and the Goal of Optimal HbA1c Control in Diabetes and Non-Diabetes. Cureus, 2020.
- Didier Ducloux and, C. Courivaud, Prevention of Post-Transplant Diabetes Mellitus: Towards a Personalized Approach. Journal of Personalized Medicine, 2022.
- Adnan Sharif Dr and, S.C. MD, Posttransplantation diabetes—state of the art. 2016; 4, 337-349. [Google Scholar] [CrossRef]
- Adachi, H. , et al., Long-term retrospective observation study to evaluate effects of adiponectin on skeletal muscle in renal transplant recipients. Scientific Reports, 2020, 10. [Google Scholar] [CrossRef]
- Houmard, J.A. , et al., , Skeletal Muscle GLUT4 Protein Concentration and Aging in Humans. Diabetes, 1995, 44, 555–560. [Google Scholar] [CrossRef]
- T. Abe, T.O., H. Tahara, H. Tashiro, K. Ishiyama, K. Ide, M. Ohira, and H. Ohdan, Risk Factors for Development of New-Onset Diabetes Mellitus and.
- Progressive Impairment of Glucose Metabolism After Living-Donor.
- Liver Transplantation. Transplantation Proceedings, 2014; 55(10).
- Cosio, F.G. , et al,, Post-transplant diabetes mellitus: Increasing incidence in renal allograft recipients transplanted in recent years. Kidney International, 2001, 59, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Da-Wei Li, et al. Risk factors for new onset diabetes mellitus after liver transplantation: A meta-analysis.
- Li DW, Lu TF, Hua XW, Dai HJ, Cui XL, Zhang JJ, Xia Q. Risk factors for new onset diabetes mellitus after liver transplantation: A meta-analysis. World J Gastroenterol 2015, 21, 6329–6340, World Journal of Gastroenterology, 2015. [CrossRef]
- Romanowski, M. , et al., adiponectin and leptin gene polymorphisms in patients with post-transplant diabetes mellitus. Pharmacogenomics, 2015, 16, 1243–1252. [Google Scholar] [CrossRef] [PubMed]
- Jøran Hjelmesaeth 1, A.F. , Trond Jenssen, Jan Frystyk, Thor Ueland, Monica Hagen, Anders Hartmann, Hypoadiponectinemia is associated with insulin resistance and glucose intolerance after renal transplantation: impact of immunosuppressive and antihypertensive drug therapy. CJASN, 2006.
- Monica Szabo, B.M. , Katalin Csép, Theodora Benedek, Genetic Approaches to the Study of Gene Variants and Their Impact on the Pathophysiology of Type 2 Diabetes. Biochemical Genetics, 2018.
- Yang Gyun Kim 1, C.-G.I. , Tae Won Lee, Sang Ho Lee, Kyung Hwan Jeong, Ju Young Moon, Joo-Ho Chung, Su Kang Kim, Yeong Hoon Kim, Association of genetic polymorphisms of interleukins with new-onset diabetes after transplantation in renal transplantation. TRANSPLANTATION, 2012.
- Yan Chen 1, M.S.S. , Jae Wook Yang, David Min, Ian V Hutchinson, Genetic polymorphisms of the transcription factor NFATc4 and development of new-onset diabetes after transplantation in Hispanic kidney transplant recipients. TRANSPLANTATION, 2012.
- Bruna B Nicoletto 1, G.C.S. , Natasha K O Fonseca, Analaura Centenaro, Roberto C Manfro, Luís Henrique S Canani, Luiz Felipe Santos Gonçalves, Association between 276G/T adiponectin gene polymorphism and new-onset diabetes after kidney transplantation. 2013.
- Cron, D.C. , et al., Using analytic morphomics to describe body composition associated with post-kidney transplantation diabetes mellitus. Clinical Transplantation, 2017, 31, e13040. [Google Scholar] [CrossRef] [PubMed]
- Marit Elizabeth von Düring 1 2, T.J. , Jens Bollerslev 2 4, Anders Åsberg 1 5 6, Kristin Godang 4, Ivar Anders Eide 1 2, Dag Olav Dahle 1 2, Anders Hartmann 1 2, Visceral fat is better related to impaired glucose metabolism than body mass index after kidney transplantation. 2015.
- Després, J.-. and I. Lemieux, Abdominal obesity and metabolic syndrome. Nature, 2006, 444, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Hung-Tien Kuo 1, M.S.S. , Xiaoyi Ye, Pavani Reddy, Paul Martin, Suphamai Bunnapradist, Risk factors for new-onset diabetes mellitus in adult liver transplant recipients, an analysis of the Organ Procurement and Transplant Network/United Network for Organ Sharing database. TRANSPLANTATION, 2010.
- Roy D Bloom 1, V.R. , Francis Weng, Robert A Grossman, Debbie Cohen, Kevin C Mange, Association of Hepatitis C with Posttransplant Diabetes in Renal Transplant Patients on Tacrolimus. JASN, 2002.
- Burra, P. Becchetti, and G. Germani, NAFLD and liver transplantation: Disease burden, current management and future challenges. JHEP Reports, 2020, 2, 100192. [Google Scholar] [CrossRef] [PubMed]
- A V Ekstrand 1, J.G.E. , C Grönhagen-Riska, P J Ahonen, L C Groop, Insulin resistance and insulin deficiency in the pathogenesis of posttransplantation diabetes in man. TRANSPLANTATION, 1992.
- Morten B Jørgensen 1, M.H. , Gerrit van Hall 2, Claus Bistrup 3, Jesper M Hansen 4, Elisabeth R Mathiesen 5, Bo Feldt-Rasmussen 1, The impact of kidney transplantation on insulin sensitivity. TRANSPLANT INTERNATIONAL, 2017.
- J H Nam 1, J.I.M. , S I Kim, S W Kang, K H Choi, K Park, C W Ahn, B S Cha, Y D Song, S K Lim, K R Kim, H C Lee, K B Huh, beta-Cell dysfunction rather than insulin resistance is the main contributing factor for the development of postrenal transplantation diabetes mellitus. TRANSPLANTATION, 2001.
- Zelle, D.M. , et al., Pancreatic β-Cell Dysfunction and Risk of New-Onset Diabetes After Kidney Transplantation. Diabetes Care, 2013, 36, 1926–1932. [Google Scholar] [CrossRef] [PubMed]
- Halden, T.A.S. , et al., GLP-1 Restores Altered Insulin and Glucagon Secretion in Posttransplantation Diabetes. Diabetes Care, 2016, 39, 617–624. [Google Scholar] [CrossRef] [PubMed]
- Leendert H Oterdoom 1, A.P.J.d.V. , Ron T Gansevoort, Willem J van Son, Jaap J Homan van der Heide, Rutger J Ploeg, Paul E de Jong, Reinold O B Gans, Stephan J L Bakker, Determinants of insulin resistance in renal transplant recipients. TRANSPLANTATION, 2007.
- Pereira, M.J. , et al., Cyclosporine A and Tacrolimus Reduce the Amount of GLUT4 at the Cell Surface in Human Adipocytes: Increased Endocytosis as a Potential Mechanism for the Diabetogenic Effects of Immunosuppressive Agents. The Journal of Clinical Endocrinology & Metabolism, 2014, 99, E1885–E1894. [Google Scholar] [CrossRef] [PubMed]
- Harini A Chakkera 1, L.J.M. , Calcineurin inhibition and new-onset diabetes mellitus after transplantation. TRANSPLANTATION, 2013.
- Talchai, C. , et al., Pancreatic β Cell Dedifferentiation as a Mechanism of Diabetic β Cell Failure. Cell, 2012, 150, 1223–1234. [Google Scholar] [CrossRef] [PubMed]
- Bensellam, M. -C. Jonas, and D.R. Laybutt, Mechanisms of β-cell dedifferentiation in diabetes: recent findings and future research directions. Journal of Endocrinology, 2018, 236, R109–R143. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rodríguez, A.E. , et al., Post-Transplant Diabetes Mellitus and Prediabetes in Renal Transplant Recipients: An Update. Nephron, 2021, 145, 317–329. [Google Scholar] [CrossRef] [PubMed]
- PfüTzner, A. , et al., Fasting Intact Proinsulin Is a Highly Specific Predictor of Insulin Resistance in Type 2 Diabetes. Diabetes Care, 2004, 27, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Ebru Sulanc 1, J.T.L. , Susan E Puumala, Gerald C Groggel, Lucille E Wrenshall, R Brian Stevens, New-onset diabetes after kidney transplantation: an application of 2003 International Guidelines. TRANSPLANTATION, 2005.
- Lane, J.T. and S. Dagogo-Jack, Approach to the Patient with New-Onset Diabetes after Transplant (NODAT). The Journal of Clinical Endocrinology & Metabolism, 2011, 96, 3289–3297. [Google Scholar] [CrossRef] [PubMed]
- Sharif, A. , Preventing and managing hyperglycemia in kidney transplant patients. Current Opinion in Nephrology and Hypertension, 2012.
- Antonio Perez 1, S.J.-C. Ignasi Saigi, M Rosa Bernal-Lopez, Inka Miñambres, Ricardo Gomez-Huelgas, Glucocorticoid-induced hyperglycemia. Journal of Diabetes 2014. [Google Scholar] [CrossRef]
- Axelrod, D.A. , et al., Posttransplant Diabetes Mellitus and Immunosuppression Selection in Older and Obese Kidney Recipients. Kidney Medicine, 2022, 4, 100377. [Google Scholar] [CrossRef] [PubMed]
- Midtvedt, K. , JøranHartmann, AndersLund, KirstenPaulsen, DagEgeland, ThoreJenssen, Trond, Insulin Resistance after Renal Transplantation : The Effect of Steroid Dose Reduction and Withdrawal. JASN, 2004, 15. [Google Scholar] [CrossRef] [PubMed]
- Chakkera, H. Kudva, and B. Kaplan, Calcineurin Inhibitors: Pharmacologic Mechanisms Impacting Both Insulin Resistance and Insulin Secretion Leading to Glucose Dysregulation and Diabetes Mellitus. Clinical Pharmacology & Therapeutics, 2017, 101, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Heisel, O. , et al., New Onset Diabetes Mellitus in Patients Receiving Calcineurin Inhibitors: A Systematic Review and Meta-Analysis. American Journal of Transplantation, 2004, 4, 583–595. [Google Scholar] [CrossRef] [PubMed]
- Charlton, M. , et al., Everolimus Is Associated With Less Weight Gain Than Tacrolimus 2 Years After Liver Transplantation. Transplantation, 2017, 101, 2873–2882. [Google Scholar] [CrossRef]
- Fraenkel, M. , et al., mTOR Inhibition by Rapamycin Prevents β-Cell Adaptation to Hyperglycemia and Exacerbates the Metabolic State in Type 2 Diabetes. Diabetes, 2008, 57, 945–957. [Google Scholar] [CrossRef] [PubMed]
- Johnston, O. , et al., Sirolimus Is Associated with New-Onset Diabetes in Kidney Transplant Recipients. Journal of the American Society of Nephrology, 2008, 19, 1411–1418. [Google Scholar] [CrossRef] [PubMed]
- Annalisa Teutonico 1, P.F.S. , Salvatore Di Paolo, Glucose metabolism in renal transplant recipients: effect of calcineurin inhibitor withdrawal and conversion to Sirolimus. JASN, 2005.
- Montero, N.M. , PhD1; Quero, Maria MD1; Melilli, Edoardo MD, PhD1; Pérez-Sáez, María José MD, PhD2; Redondo-Pachón, Dolores MD, PhD2; Bestard, Oriol MD, PhD1; Crespo, Marta MD, PhD2; Cruzado, Josep M. MD, PhD1; Pascual, Julio MD, PhD2, Mammalian Target of Rapamycin Inhibitors Combined With Calcineurin Inhibitors as Initial Immunosuppression in Renal Transplantation: A Meta-analysis. TRANSPLANTATION, 2019. [Google Scholar]
- Stefan Berger 1, C.S. , Oliver Witzke 3 4, Helio Tedesco 5, Steve Chadban 6, Shamkant Mulgaonkar 7, Yasir Qazi 8, Johan W. de Fijter 9, Federico Oppenheimer 10, Josep M. Cruzado 11, Yoshihiko Watarai 12, Pablo Massari 13, Christophe Legendre 14, Franco Citterio 15, Mitchell Henry 16, Titte R. Srinivas 17, Flavio Vincenti 18, Maria Pilar Hernandez Gutierrez 19, Ana Maria Marti 19, Peter Bernhardt 19…Julio Pascual 20, Two-year outcomes in de novo renal transplant recipients receiving everolimus-facilitated calcineurin inhibitor reduction regimen from the TRANSFORM study. 2019.
- Phuong-Thu T Pham 1, P.-C.T.P. , Gerald S Lipshutz, Alan H Wilkinson, New onset diabetes mellitus after solid organ transplantation. Endocrinology and Metabolism Clinics of North America, 2007.
- Cehic, M.G. , et al., Management Strategies for Posttransplant Diabetes Mellitus after Heart Transplantation: A Review. Journal of Transplantation, 2018, 2018, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Oliver Thomusch 1, M.W. , Mirian Opgenoorth 3, Andreas Pascher 4, Rainer Peter Woitas 5, Oliver Witzke 6, Bernd Jaenigen 1, Markus Rentsch 7, Heiner Wolters 8, Thomas Rath 9, Tülay Cingöz 10, Urs Benck 11, Bernhard Banas 12, Christian Hugo 13, Rabbit-ATG or basiliximab induction for rapid steroid withdrawal after renal transplantation (Harmony): an open-label, multicentre, randomised controlled trial. the lancet, 2016.
- Haller, M.C. , et al., Steroid withdrawal after renal transplantation: a retrospective cohort study. BMC Medicine, 2017, 15. [Google Scholar] [CrossRef] [PubMed]
- E Steve Woodle 1, M.R.F. , John Pirsch, Fuad Shihab, A Osama Gaber, Paul Van Veldhuisen; Astellas Corticosteroid Withdrawal Study Group, A prospective, randomized, double-blind, placebo-controlled multicenter trial comparing early (7 day) corticosteroid cessation versus long-term, low-dose corticosteroid therapy. 2008.
- Sneha Palepu 1, G.V.R.P. , New-onset diabetes mellitus after kidney transplantation: Current status and future directions. world journal of diabetes 2015. [Google Scholar] [CrossRef]
- Chadban, S. , New-onset diabetes after transplantation--should it be a factor in choosing an immunosuppressant regimen for kidney transplant recipients. Nephrology Dialysis Transplantation, 2008, 23, 1816–1818. [Google Scholar] [CrossRef] [PubMed]
- Manfred Hecking 1, M.H. , Dominik Döller, Johannes Werzowa, Andrea Tura, Jinyao Zhang, Hilal Tekoglu, Johannes Pleiner, Thomas Wrba, Susanne Rasoul-Rockenschaub, Ferdinand Mühlbacher, Sabine Schmaldienst, Wilfred Druml, Walter H Hörl, Michael Krebs, Michael Wolzt, Giovanni Pacini, Friedrich K Port, Marcus D Säemann, Early basal insulin therapy decreases new-onset diabetes after renal transplantation. JASN, 2012.
- Chowdhury, T.A. , et al., Association of British Clinical Diabetologists and Renal Association guidelines on the detection and management of diabetes post solid organ transplantation. Diabetic Medicine 2021, 38. [Google Scholar] [CrossRef] [PubMed]
- Vest, L.S. , et al., Metformin use in the first year after kidney transplant, correlates, and associated outcomes in diabetic transplant recipients: A retrospective analysis of integrated registry and pharmacy claims data. Clinical Transplantation, 2018, 32, e13302. [Google Scholar] [CrossRef] [PubMed]
- B Richter 1, E.B.-E. , K Bergerhoff, C L Lerch, Dipeptidyl peptidase-4 (DPP-4) inhibitors for type 2 diabetes mellitus. Cochrane Library, 2008.
- Wajchenberg, B.L. , β-Cell Failure in Diabetes and Preservation by Clinical Treatment. Endocrine Reviews, 2007, 28, 187–218. [Google Scholar] [CrossRef] [PubMed]
- Vijay Shivaswamy 1, R.G.B. , Cara C Clure 3, Brendan Ottemann 3, John S Davis 4, Jennifer L Larsen 5, Frederick G Hamel 5, Tacrolimus and Sirolimus have distinct effects on insulin signaling in male and female rats. Translational Research, 2014.
- Delos Santos, R.B. , et al., Sitagliptin Versus Placebo to Reduce the Incidence and Severity of Posttransplant Diabetes Mellitus After Kidney Transplantation-A Single-center, Randomized, Double-blind Controlled Trial. Transplantation, 2023, 107, 1180–1187. [Google Scholar] [CrossRef] [PubMed]
- Defronzo, R.A. , et al., Effects of Exenatide (Exendin-4) on Glycemic Control and Weight Over 30 Weeks in Metformin-Treated Patients With Type 2 Diabetes. Diabetes Care, 2005, 28, 1092–1100. [Google Scholar] [CrossRef] [PubMed]
- Garber, A.J. , Long-Acting Glucagon-Like Peptide 1 Receptor Agonists. Diabetes Care, 2011, 34 (Supplement_2), S279-S284. [Google Scholar] [CrossRef] [PubMed]
- Priyamvada Singh 1, M.T. , Todd E Pesavento 1, Kenneth Washburn 1, Debbie Walsh 1, Shumei Meng 1, Comparison of the glucagon-like-peptide-1 receptor agonists dulaglutide and liraglutide for the management of diabetes in solid organ transplant: A retrospective study. Diabetes, Obesity and Metabolism, 2020.
- Heerspink, H.J.L. , et al., Renoprotective effects of sodium-glucose cotransporter-2 inhibitors. Kidney International, 2018, 94, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Aditi Ujjawal 1, B.S. , Ashish Verma 3, Sodium-glucose cotransporter-2 inhibitors (SGLT2i) in kidney transplant recipients: what is the evidence? Therapeutic Advances in Endocrinology and Metabolism, 2022.
- Jin, J. , et al., Effect of Empagliflozin on Tacrolimus-Induced Pancreas Islet Dysfunction and Renal Injury. American Journal of Transplantation, 2017, 17, 2601–2616. [Google Scholar] [CrossRef]
- Ko, E.J. , et al., Effect of dual inhibition of DPP4 and SGLT2 on tacrolimus-induced diabetes mellitus and nephrotoxicity in a rat model. American Journal of Transplantation, 2022, 22, 1537–1549. [Google Scholar] [CrossRef] [PubMed]
- Michael A Nauck 1, J.W. , Juris J Meier 2, Treatment of type 2 diabetes: challenges, hopes, and anticipated successes. The Lancet Diabetes & Endocrinology 2021. [Google Scholar] [CrossRef]
- Chakkera, H.A. , et al., Can New-Onset Diabetes After Kidney Transplant Be Prevented? Diabetes Care, 2013, 36, 1406–1412. [Google Scholar] [CrossRef] [PubMed]
- William C Knowler 1, E.B.-C. , Sarah E Fowler, Richard F Hamman, John M Lachin, Elizabeth A Walker, David M Nathan; Diabetes Prevention Program Research Group, Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. 2002.
- Shahrad Taheri 1, H.Z. , Odette Chagoury 3, Sara Elhadad 3, Salma Hayder Ahmed 3, Neda El Khatib 4, Rasha Abou Amona 4, Katie El Nahas 4, Noor Suleiman 5, Abdulla Alnaama 6, Abdulla Al-Hamaq 4, Mary Charlson 7, Martin T Wells 8, Samya Al-Abdulla 6, Abdul Badi Abou-Samra 5, Effect of intensive lifestyle intervention on bodyweight and glycaemia in early type 2 diabetes (DIADEM-I): an open-label, parallel-group, randomised controlled trial. The Lancet Diabetes & Endocrinology 2020. [Google Scholar] [CrossRef]
- Kulli Kuningas 1, J.D. , Reena Mair 2, Helen Smith 3, Mary Dutton 1, Edward Day 4, And Adnan Sharif 1 5, Comparing Glycaemic Benefits of Active Versus Passive Lifestyle Intervention in Kidney Allograft Recipients: A Randomized Controlled Trial. transplantation, 2020.
- Byambasukh, O. , et al., Physical Activity and the Development of Post-Transplant Diabetes Mellitus, and Cardiovascular- and All-Cause Mortality in Renal Transplant Recipients. Journal of Clinical Medicine, 2020, 9, 415. [Google Scholar] [CrossRef] [PubMed]
- Osté, M.C.J. , et al., Mediterranean style diet is associated with low risk of new-onset diabetes after renal transplantation. BMJ Open Diabetes Research & Care, 2017, 5, e000283. [Google Scholar] [CrossRef]
- Merz, K.E. and D.C. Thurmond, Role of Skeletal Muscle in Insulin Resistance and Glucose Uptake. Comprehensive Physiology, 2020: p. 785-809.
- Cohen, J.B. , et al., Bariatric surgery before and after kidney transplantation: long-term weight loss and allograft outcomes. Surgery for Obesity and Related Diseases, 2019, 15, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Do Carmo Chaves, A.E.C. , et al., Early retinal neurovascular findings in post-transplant diabetes mellitus patients without clinical signs of diabetic retinopathy. International Journal of Retina and Vitreous, 2023, 9. [Google Scholar] [CrossRef] [PubMed]
- J P Boudreaux, L.M. , D M Canafax, N Ascher, D E Sutherland, W Payne, R L Simmons, J S Najarian, D S Fryd, The impact of cyclosporine and combination immunosuppression on the incidence of posttransplant diabetes in renal allograft recipients. TRANSPLANTATION, 1987.
- Krista L Lentine 1, D.C.B. , Mark A Schnitzler, Incidence and predictors of myocardial infarction after kidney transplantation. JASN, 2005.
- Rianne P Wauters 1, F.G.C. , Maria L Suarez Fernandez, Yogish Kudva, Pankaj Shah, Vicente E Torres, Cardiovascular consequences of new-onset hyperglycemia after kidney transplantation. Transplantation, 2012.
- Cosio, F.G. , et al., New onset hyperglycemia and diabetes are associated with increased cardiovascular risk after kidney transplantation. Kidney International, 2005, 67, 2415–2421. [Google Scholar] [CrossRef] [PubMed]
- Giacco, F. and M. Brownlee, Oxidative Stress and Diabetic Complications. Circulation Research, 2010, 107, 1058–1070. [Google Scholar] [CrossRef] [PubMed]
- Brownlee, M. , The Pathobiology of Diabetic Complications. Diabetes, 2005, 54, 1615–1625. [Google Scholar] [CrossRef] [PubMed]
- Esteban Porrini 1, P.D. , Alejandra Alvarez, Marian Cobo, Lourdes Pérez, José M González-Posada, Luis Hortal, Roberto Gallego, José J García, Maria Checa, Adelaida Morales, Eduardo Salido, Domingo Hernández, Armando Torres, The combined effect of pre-transplant triglyceride levels and the type of calcineurin inhibitor in predicting the risk of new onset diabetes after renal transplantation. 2008.
- Henrik Andreas Bergrem 1, T.G.V. , Anders Hartmann, Harald Bergrem, Jøran Hjelmesaeth, Trond Jenssen, Glucose tolerance before and after renal transplantation. 2010.
- Chen, T. , et al., New onset diabetes mellitus after liver transplantation and hepatitis C virus infection: meta-analysis of clinical studies. Transplant International, 2009, 22, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Ponticelli, C. Favi, and M. Ferraresso, New-Onset Diabetes after Kidney Transplantation. Medicina, 2021, 57, 250. [Google Scholar] [CrossRef] [PubMed]
- Hare, M.J.L. E. Shaw, and P.Z. Zimmet, Current controversies in the use of haemoglobin A<sub>1c</sub>. Journal of Internal Medicine, 2012, 271, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Jenssen, T. and A.Hartmann, Emerging treatments for posttransplantation diabetes mellitus. Nature Reviews Nephrology, 2015, 11, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Sharif, A. , et al., Proceedings From an International Consensus Meeting on Posttransplantation Diabetes Mellitus: Recommendations and Future Directions. American Journal of Transplantation, 2014, 14, 1992–2000. [Google Scholar] [CrossRef] [PubMed]
- Dai, C. , et al., Tacrolimus- and sirolimus-induced human β cell dysfunction is reversible and preventable. JCI Insight, 2020, 5. [Google Scholar] [CrossRef] [PubMed]
- Iatcu, C.O. Steen, and M.Covasa, Gut Microbiota and Complications of Type-2 Diabetes. Nutrients, 2021, 14, 166. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.B. , et al., The Relationship between the Gut Microbiome and Metformin as a Key for Treating Type 2 Diabetes Mellitus. International Journal of Molecular Sciences, 2021, 22, 3566. [Google Scholar] [CrossRef]
- Lecamwasam, A. and E.I. Ekinci, Novel Associations of Empagliflozin on the Gut Microbiome and Metabolome in Type 2 Diabetes. The Journal of Clinical Endocrinology & Metabolism, 2022, 107, e4246–e4247. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The figure illustrates the risk factors and the main pathophysiological mechanisms implicated in the pathogenesis of NODAT.
Figure 1.
The figure illustrates the risk factors and the main pathophysiological mechanisms implicated in the pathogenesis of NODAT.
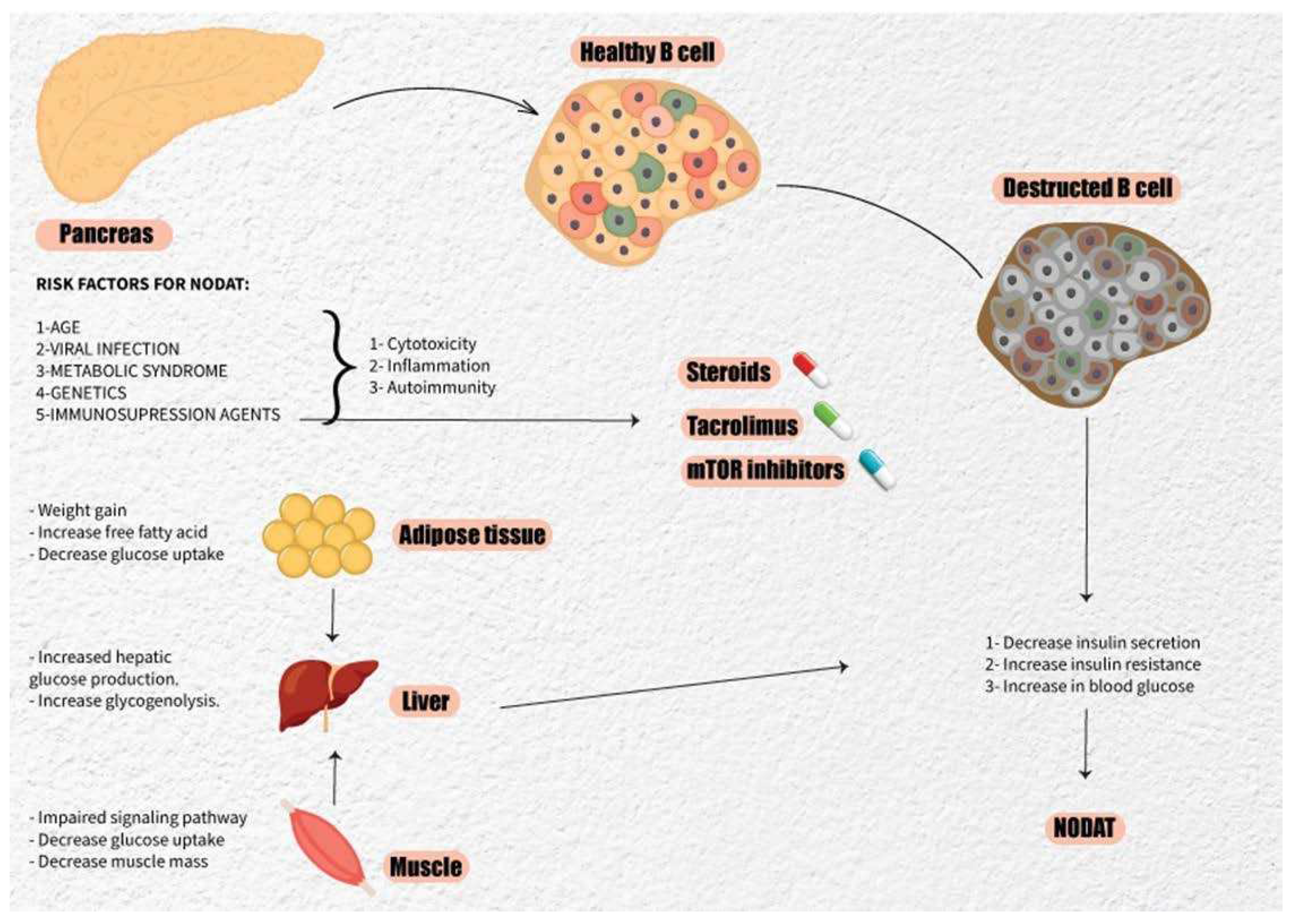
Figure 2.
This figure illustrates the cascading effects of NODAT on various physiological processes, particularly hypertension, inflammation, and oxidative stress, ultimately leading to cardiac complications. NODAT caused by hyperglycemia and increases insulin resistance, contributing to elevated blood pressure and systemic inflammation. These interconnected factors heighten oxidative stress levels, exerting detrimental effects on cardiac function and health.
Figure 2.
This figure illustrates the cascading effects of NODAT on various physiological processes, particularly hypertension, inflammation, and oxidative stress, ultimately leading to cardiac complications. NODAT caused by hyperglycemia and increases insulin resistance, contributing to elevated blood pressure and systemic inflammation. These interconnected factors heighten oxidative stress levels, exerting detrimental effects on cardiac function and health.
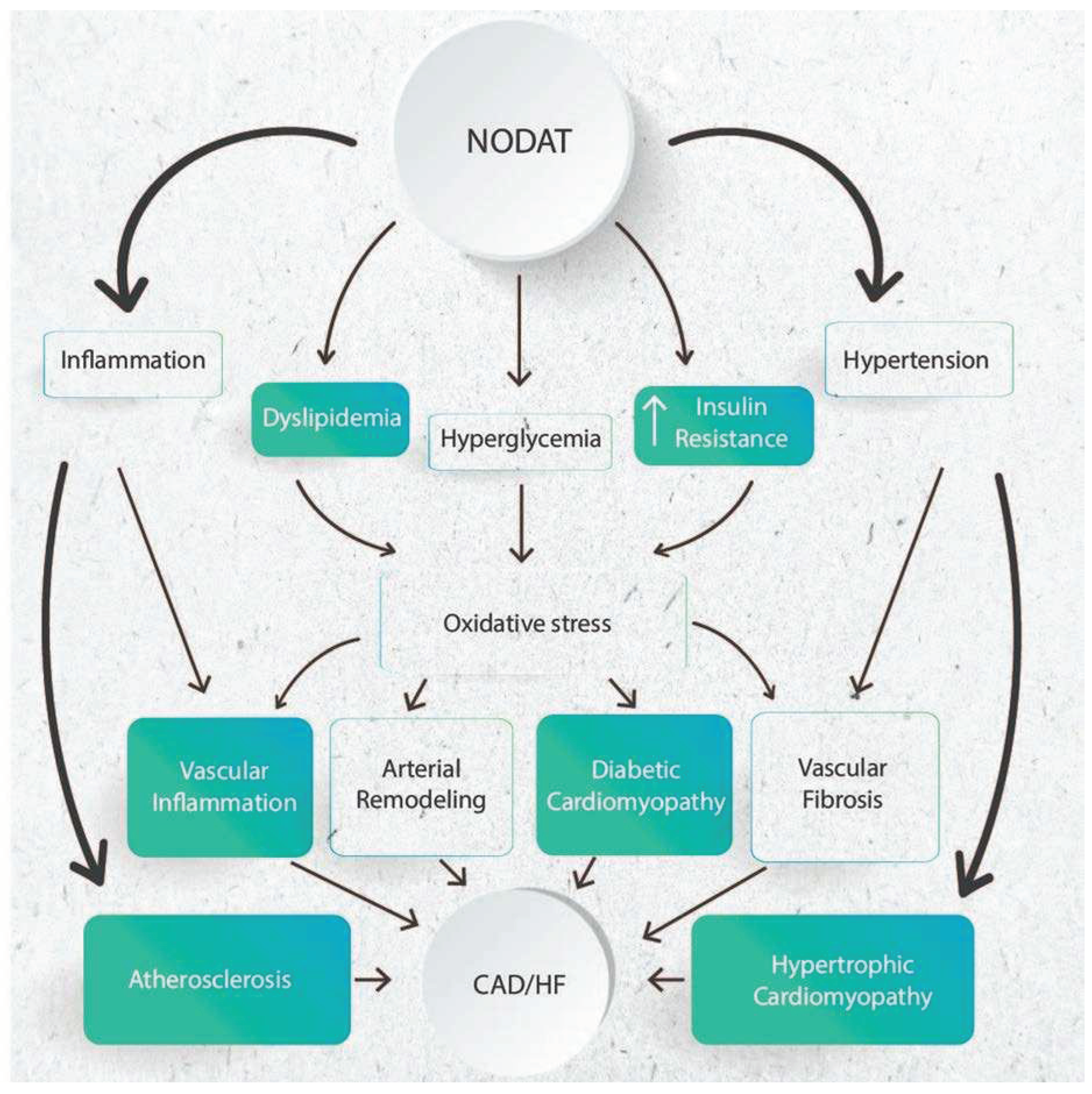

Table 1.
This table provides a comprehensive overview of the diagnostic criteria used to identify NODAT.
Table 1.
This table provides a comprehensive overview of the diagnostic criteria used to identify NODAT.
| Test | Result |
|---|---|
| Fasting Glucose | ≥ 126 mg/dL (7 mmol/L) on more than one occasion. |
| Random Glucose | ≥ 200 mg/dL (11.1 mmol/L) with symptoms. |
| Two-hour glucose after a 75-g OGTT | ≥ 200 mg/dL (11.1 mmol/L). |
| HbA1c | > 6.5% |
Table 2.
This table provides an overview of both modifiable and non-modifiable risk factors associated with NODAT, facilitating risk stratification and targeted interventions to mitigate the development of diabetes mellitus after solid organ transplantation.
Table 2.
This table provides an overview of both modifiable and non-modifiable risk factors associated with NODAT, facilitating risk stratification and targeted interventions to mitigate the development of diabetes mellitus after solid organ transplantation.
|
Modifiable risk factors |
Immuno suppression Rejection episodes Obesity Metabolic syndrome Hepatitis C virus infection |
|
Non-modifiable risk factors |
Age Ethnicity Male gender Family history of diabetes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



