
Submitted:
29 January 2024
Posted:
30 January 2024
You are already at the latest version
Abstract
The practical problem-solving of incidental unreliability of intraoperative neuromonitoring may be the simultaneous neurophysiological recording and the inspection of the surgical field through the camera (the "Real-time neuromonitoring" concept). This would allow the immediate warning of the surgeon on the possibility of the spinal structures insult during but not after the application of the standard procedures in scoliosis surgery (the “Interactive verbal surgeon-neurophysiologist neuromonitoring" concept). This study aimed to compare the advantages, utility, reliability, and time-consuming of both intraoperative neuromonitoring scenarios using non-invasive and innovative recordings from peroneal nerves (PER) versus tibialis anterior muscles (TA) with surface electrodes of motor evoked potentials (MEP) bilaterally as a result of transcranial magnetic (TMS) or electrical (TES) stimulations. Studies were performed in two similar groups ("Real-time neuromonitoring", N=60 and "Interactive verbal sur-geon-neurophysiologist neuromonitoring", N=60) of patients treated surgically because of mainly Lenke 2 type idiopathic scoliosis (IS) pre- (T0), intra- (T1 – before surgical procedures, T2 – after surgical procedures) and postoperatively (T3) as well as in healthy volunteers (N=60, Control). The cumulative parameters of MEP amplitudes and latencies recorded from PER compared to those recorded from TA in healthy volunteers were approximately 67% (1100µV) lower at p=0.007 and 10.6% shorter (3.1 ms) at p=0.04, respectively. A similar trend was also observed in patients from both groups at each follow-up stage. MEP recordings from TA and PER in patients of both groups differed similarly in T0-T3 compared to controls at p=0.008-0.04. MEP parameters in all patients induced by TMS (T0) and TES (T1) did not differ. The parameters of MEP amplitudes recorded from TA and PER intraoperatively in T1 and T2 differed at p=0.04-0.03, indicating the bilateral improvement of neural spinal conduction due to the surgical intervention. Parameters of TMS-induced MEP amplitudes in T3 further increased bilaterally compared to the tests recorded in T0 at p=0.03-0.02. In both groups of patients, an average 51,8 BIS level of anaesthesia minimally affects the variability of the MEP amplitude, especially in PER recordings when ap-plied TES strength was at 98.2 mA. The number of MEP parameter fluctuations, mainly the amplitudes decreasing, was strictly associated with the neurophysiologist's warnings due to transpedicular screws implantation, corrective rods implantation, distraction, derotation, and compression procedures, respectively; at p=0.04-0.03 more in patients from the “Interactive S-N neuromonitoring” group. The average duration of the surgery was significantly shorter (p=0.04) by about 1 hour in the "Real-time neuromonitoring" group. The number of two-way communications between the surgeon and neurophysiologist and vice versa in the "Real-time neuromonitoring" group was reduced by approximately half at p=0.008. The study's results prove the advantages of using the "Real-time neuromonitoring" procedure in increasing safety and non-invasiveness, shortening the time, and lowering the costs of surgical treatment of patients with pathological lateral curvature of the spine. The modifications of the MEP nerve conduction recording technology with surface electrodes from nerves presented in this study enable precise and reliable information on the patient's neurological condition at every stage of applied surgical procedures, even in conditions of slight fluctuations in the anaesthesia.
Keywords:
idiopathic scoliosis
; intraoperative neurophysiological recordings
; real-time neuromonitoring
; transcranially evoked motor potentials
; muscle versus nerve recording
1. Introduction
Currently, the prevalence of pathological lateral spine curvature and its rotation may reach 5-6% in a worldwide population of adolescents, preferably girls [1,2]. The idiopathic scoliosis (IS) is the most common spinal deformity that needs to be treated surgically [3]. The conservative treatment with kinesiotherapy and bracing in the vast majority of girls with IS usually fails, and may only diminish or slow down the curvature progression; still, it is the treatment of the first choice [4,5,6,7]. Unfortunately, non-treated scoliosis may lead to neuropathies in lower extremities nerves and their consequences such as neurogenic muscle injuries and finally paralysis or advanced cardiopulmonary diseases (Daroszewski [8,9]). Spinal deformation surgery is an art of great complexity and constantly introduces new methods of possible different iatrogenic risks [10]. It is obvious, that a greater magnitude of preoperative deformity and surgical extent increases the risk of spinal cord injury identified by intraoperative neuromonitoring (IONM) alerts during correction of deformities in patients with IS [11]. It has been found that in about 13% of patients undergoing spinal deformity correction, it was required to alert the surgeon from the neuromonitoring team about the side effects of the surgery [12]. Moreover, the incidence of possible severe postoperative neurologic deficits has been assessed at about 3.2% for scoliosis surgery [13]. The successful surgical implantation of the pedicle screws and correction with the implanted corrective rods is fraught with the risk of many factors that may worsen the patient's neurological condition [14]. They mainly include the direct spinal cord trauma or the consequences of its stretch during deformity correction, ischemia, and cardiopulmonary abnormalities [12].
The neurophysiological monitoring supporting the proper proceeding of idiopathic scoliosis surgical correction becomes more and more trustful since the number of the iatrogenic side effects became incidental [15,16]. Although several algorithms for the response to neuromonitoring-related changes have been created, they evolve depending on the surgeries' modifications; none are widely accepted or used consistently in general practice for a variety of reasons [17]. Modifications of IONM brought the possibilities of improving, shortening, and making more reliable the cooperation of the neurophysiologist and surgeon to obtain the best results of cooperation [18]. The standards of neuromonitoring are constant and consist of checking every step of the surgical procedures and reacting to improper incidents [19]. Although a consensus-based checklist to guide surgeon reactions to IONM changes and the best practice guideline for their recording have been formulated [20] and their agreement has been confirmed and appreciated [21], they developed since new concepts appear [22,23,24]. It is obvious, that the surgical team of spine surgeons, anesthesiologists, and neurophysiologists cooperates more efficiently if their experience, technical skills, and equipment are advanced [25]. But not only, the best results are achieved if the threats are predictable and the effects of the surgeon's activities are assessed in real time not only neurophysiologically but also visually. It has been underlined by Levin et al. [26] that the communication between the anesthesiologists, neurophysiologists, surgeons, and nursing staff is fundamental to the effective use of IONM. If we consider that the elimination of discussed events and actions during the intraoperative warning may shorten the reaction time of both the neurophysiologist and the surgeon [22,27], the way practical problem-solving may be the simultaneous neurophysiological recording and the inspection of the surgical field through the camera. This would allow the immediate warning of the surgeon during but not after introducing the certain procedure to the spine, following pedicle screw implantation or the corrective rod mounting. Considering that scoliosis surgery often takes 4 to 6 hours [28], every attempt to make it shorter but simultaneously make it safer is of great interest, especially for the patient, whose health status may be greatly influenced by the anesthesia duration.
The motor evoked potentials (MEP) transcranially induced with the magnetic field stimulus (TMS) as a very precise tool are widely used for evaluation of the motor function of patients with degenerative myelopathy [29] or incomplete spinal cord injuries [30,31]. The diagnostic sensitivity of MEP in the detection of the spinal cord structure insult is evaluated at 98% [32]. MEP induced with trains of transcranially applied electrical stimuli (TES) are characterized by an almost 100% sensitivity and specificity of detection of the corticospinal tract injury in the anterior and lateral spinal cord funiculi, as well as its ischemia consequences during spinal deformity correction [33]. Due to the high amplitude potential recordings of more than 2000μV, they do not need averaging; if the stimulus strength to induce MEP is at 100 mA and the anesthesia level is kept stable, they are a reliable, affordable, and practical neuromonitoring tool during scoliosis correction [8]. Spinal cord motor function monitoring with MEP is generally considered based on recordings of the muscle responses to intermittent stimulation of the motor cortex in real time [19], which seems to be partially true. Contemporary, the real-time neuromonitoring concept is usually understood as the recording of evoked potentials after certain surgical procedures that are applied to IS patients to verify their non-invasiveness to the spinal cord neural transmission. The proposed in this paper "Real-time neuromonitoring" concept refers to the recording of evoked potentials during certain surgical procedures that are applied to IS patients to verify their non-invasiveness to the spinal cord neural transmission. They allow the immediate reaction of the surgeon after immediate warnings from the neurophysiologist.
During intraoperative neuromonitoring including the scoliosis surgery, bilateral recordings from the lower extremities muscles are used for the evaluation of the entire efferent neural transmission to the effector following TES of the motor cortex centers. This allows the evaluation of the supraspinal and intraspinal efferent pathways' transmission as well as neural transmission within the spinal ventral roots and motor fibers in the peripheral nerve [34,35]. The method is sensitive in the detection of motor deficits and spinal cord reaction to ischemia intraoperatively. However, the amplitude parameter of MEP is likely to be sensitive to the deep anesthesia influence, and the conditions of recordings preclude the use of the constant neuromuscular blockade. An interesting proposal that seems to resolve the above problems is the recording from the lower extremities nerves [36], when the amplitude parameters are approximately half as low as those recorded from the muscles [37], but stable recorded regardless of the level of anesthesia [Daroszewski et al Reumat].
The main aim of this paper is to present details of the “Real-time neuromonitoring” concept verifying the safety of procedures performed during the surgical correction of idiopathic scoliosis. To verify its effectiveness we compared the results of MEP recordings from lower extremities muscles versus nerves following TMS and TES, respectively. They were performed in two equal groups of neuromonitoring sessions in IS patients with similar advancement of the pathology; “Interactive S-N group” - based on bilateral surgeon-neurophysiologist verbal reports vs. “Real-time neuromonitoring group" - based on the simultaneous MEP recordings with the direct visual inspection of the operation field via the camera, without verbal reports. Our previous pilot studies on using “Real-time monitoring” in 35 cases of patients [22], allowed for preliminary evaluation of the utility of this method concerning the total surgical procedures duration which will be verified in this study on the larger population of IS patients.
2. Materials and Methods
2.1. Participants and Study Design
The basic research methods used in this work were pre-, double intra- (before and after correction of the scoliotic curvature) and post-operative recordings of motor potentials evoked as a result of their transcranial induction either with a single magnetic field pulse (TMS) or a series of electric pulses (TES) leading to the excitation of the efferent pathways from the brain motor centers. MEP parameters were analyzed bilaterally in recordings from the tibialis anterior (TA) muscles or from above the surface of the peroneal nerve (PER), lateral to the head of the fibula, in the place of its longitudinal, anatomical course. While the choice of recording from the TA muscle was dictated by the possibility of comparing MEP parameters with the descriptions of other researchers monitoring the overall efferent conduction from the level of the upper motor neuron to the effector, the recording from above the nerve surface is innovative, previously described in studies on a small population of patients with locomotor dysfunction as a consequence of disc-root conflicts [37] or scoliosis [8]. Its description in this paper aims to provide a detailed presentation of an alternative method of intraoperative neuromonitoring, possibly more resistant to the anesthesia agents' influence than recording from the muscle. To prove the superiority of one of the IONM methods ("Interactive S-N" versus "Real-time") we selected in three stages two almost similar populations of scoliotic patients treated surgically with the same method (Figure 1).
From our database of patients with idiopathic scoliosis treated surgically the first time between 2018-2023 (N=377), we have preliminary selected the results from motor evoked potential recordings (MEP) performed in girls with idiopathic scoliosis pre- (T0), intra- (T1 – before surgical procedures, T2 – after surgical procedures) and postoperatively (T3), as well as the detailed data included in the full IONM protocols collected in 298 subjects (Stage I). All patients were clinically evaluated (including the analysis of anterior-posterior and lateral X-rays) and treated at Wiktor Dega Orthopedic and Rehabilitation Hospital in Poznań, Poland by the same team of four surgeons; two experienced neurophysiologists and two neurologists evaluated their health status pre- and postoperatively as well as performed the neuromonitoring procedures.
Applying the criteria of similar demographic, anthropometric, and scoliosis characteristics (type and the curvature angle; Table 1), the extent of the surgical approach from T1 to L2 from the back, the same applied Nova Spine (Amiens, France) surgical corrective instrumentation (including a similar number of implanted transpedicular screws; from 8 to 16, 10 on average), we have selected the records of 231 IS patients (Figure 1, Stage II). Then (Stage III), based on the two ways the IONM scenarios but including the similar conditions of MEP recordings (bilaterally over tibialis anterior muscle - TA and from the surface of the peroneal nerve at the knee - PER ), the similar stimulus strength to evoke the motor potentials during TES (80 to 130 mA; mean of 98.2 ± 7.8 SD) and the level of applied anesthesia (Bispectral Index Monitor - BIS, between 40-60) [38,39,40], from the group of 146 patients we have randomly allocated the equal groups of 60 patients belonging to two groups; "Interactive S-N" (a group of scoliotic patients in whom mainly a verbal interaction between the surgeon and the neurophysiologist during intraoperative neuromonitoring was continuously kept) and "Real-time" (a group of scoliosis patients in whom the intraoperative neuromonitoring was mainly based on simultaneous evoked potential and camera recordings by neurophysiologist). Before surgeries, all the treated girls belonging to the two studied groups had applied with no exception the Cheneau-brace and the physiotherapy exercises but they only brought the slowing down scoliosis progression in about half of the patients.
Exclusion criteria for transcranial stimulation to induce MEP when applied pre- and postoperatively or intraoperatively during the neuromonitoring included: episodes of epilepsy, past brain lesions, skull defects, raised intracranial pressure, symptoms of cardiac and vascular diseases, intaking proconvulsant medications or anesthetics, implanted intracranial electrodes, vascular clips or shunts, cardiac pacemakers or other implanted biomedical devices [35]. We followed the rules of IONM according to the guidelines of MacDonald [34].
A control group of 60 healthy girls was examined once to establish reference values for neurophysiological recordings. To ensure comparability, the control group's demographics (gender, age, height, and weight) were adjusted to match those of the study group. Statistically significant differences in age, height, and weight between the study groups and healthy volunteers in the control group were not observed (Table 1). Parameters of amplitudes and latencies of MEP evoked following TMS or TES were compared at each of the observation periods in patients belonging to two studied groups and regarding the healthy volunteers.
The study was approved by the Bioethics Committee from the University of Medical Sciences (Poznań, Poland; decision No 942/2021). Ethical considerations were in agreement with the Helsinki Declaration (including the studies on healthy people). Each of the subjects or her parent/legal guardian provided the written consent for examinations and the medical data publication which were kept as confidential.
2.2. Anaesthesia, Spine Surgery, Neurophysiological Recordings and Neuromonitoring Principles
The surgeries of scoliotic patients were performed under Propofol/Remifentanil anesthesia (induction dose of Remifentanil 0.5 µg/kg and Propofol 2 mg/kg, and later Remifentanil 0.5–2.0 µg/kg/h and Propofol 2–4 mg/kg/h in continuous infusion) with a one-time dose of neuromuscular blockade (0.5 mg/kg of rocuronium bromide) at the beginning of the procedure. The level of anesthesia was monitored continuously in the Bispectral Index Monitor (BIS, GE Healthcare, Helsinki, Finland); it was kept constant from 40 to 60 during all applied surgery procedures and neuromonitoring MEP recordings [Medical]. Blood pressure (maintained between 80 and 100 mmHg), temperature, %SpO2, and CO2 partial pressure were continuously monitored and maintained within physiological limits. Inhalational anesthetics were not routinely used [43]. All anesthetic procedures were performed by the same two experienced anesthesiologists.
The implantation of a Nova Spine corrective instrumentation system (Amiens, France; Figure 2 Cd, Cl and Cr) was applied by a posterior approach in a prone position to the patients during the scoliotic spine surgery (Figure 1 Ca). The spine area from the upper thoracic to the lower lumbar vertebrae was prepped and draped. After the posterior midline skin incision was performed, the paraspinal muscles were dissected subperiosteally. The spine exposition was performed bilaterally from the midline along the spinous processes, laminas to the tip of transverse processes (Figure 1 Cc). To control bleeding, cauterization of the paravertebral muscles was necessary (Figure 1 Cb). For the final anatomical wound closure, the spinous processes with supraspinous ligament were preserved. The autografts for final fusion consisted of the removed pieces of the bones from processes and released spine joints. Eight to sixteen transpedicular screws were applied bilaterally (10 on average in each of the patients) with the free-hand technique for mounting the two corrective rods (Figure 1 Cd, Cl, and Cr). The transpedicular screws positions were verified with the control of X-ray C-arm (Figure 1 Ce) and neuromonitoring navigations (Figure 1 Cj and Co). The polyaxial and monoaxial transpedicular screws were used; two corrective rods (5.5 mm in diameter) were made of titanium alloy. The data mining in Stage II of the subjects selection for this study (Figure 1) was strictly subordinated to the regime so that in the future analysis, patients of both groups ("Interactive S-N" vs. "Real-time" neuromonitoring) met the same criteria of surgical treatment technique.
In general, the only difference in the analyzed treatment procedures in both groups of patients was the neuromonitoring scenario (Figure 3). The scoliosis correction was a result of the maneuvers as follows: the rod rotation on the convex side, apical translation, segmental derotation, distraction on the concave side, and compression on the convex side. A subfascial drain was applied and the wound was closed over in layers.
All the patients had performed the TES-induced MEP recordings pre- (T0 - a day before the surgery, Figure 2 Ci an Cn) and postoperatively (T3 - a week after surgery, Figure 2 Ck and p) in a supine position, in the same diagnostic room with a controlled temperature of 22 °C using the Key-Point Diagnostic System (Medtronic A/S, Skøvlunde, Denmark). A single, biphasic, 5 ms lasting magnetic stimulus generated by The MagPro X100 (Medtronic A/S, Skøvlunde, Denmark) was applied transcranially (Figure 2 Ab) with a circular coil (C-100, 12 cm in diameter) placed over the scalp in the M1 motor cortex area responsible mainly for innervation of the lower and less upper extremities muscles. The targeted excitation of the corticospinal tract cells of origin and their axons was achieved when the coil was placed exactly perpendicular to the skull surface. Likely, the cells of origin of the rubrospinal tract in the midbrain can be also excited, because the magnetic stream may reach 3 cm deep [31,44]. The MEP measures assessed the ability of the primary motor cortex to neuronal impulses output and evaluated the global efferent transmission of neural impulses to effectors via spinal cord descending tracts. The strength of the magnetic field stream at 70–80% of the resting motor threshold (RMT; 0.84–0.96 T) was applied. The consecutive movements of the magnetic coil distanced 5 mm from each allowed for assessing the location of the optimal stimulation, a "hot spot" in the area where TMS elicited the largest recorded MEP amplitude; Figure 2 Ac). The accurate photographic documentation of "hot spots marked" at a similar location of the transcranial stimulation allowed for the reproducibility of the similar MEP recordings at T0-T3. The TMS was not reported by the subjects as painful. The epileptic side effects were not observed.
Preoperatively (T0 period of observation), MEP was recorded with surface electrodes bilaterally from TA muscles or PER nerves (Figure 2 Aa) with a pair of disposable Ag/AgCl surface electrodes (5 mm2 of an active surface). During recordings from TA, the active electrode was placed on the muscle's belly, a reference electrode was placed on the muscle's distal tendon, and a ground electrode in its vicinity. During recordings from PER, the active electrode was placed proximally and a reference electrode distally, both at the knee level, lateral to the head of the fibula, in the place of PER longitudinal, anatomical course. The mountings of the electrodes for the neurophysiological recordings were performed in a supine position in T0, T1, and T3 observation periods. The resistance between the electrode surfaces and the skin was decreased with electro-conductive gel. The MEP outcome measures were amplitude in µV from peak to peak of the signal and the latency in ms from the stimulus application marked by the artifact in the recording to the onset of the positive inflection of potential. For the MEP acquisition, the low-pass filter of the recorder was set to 20 Hz, the high-pass filter to 10 kHz, the time base at 10 ms/D, and the amplification of signals between 200 and 5000 µV. During recordings bandwidth of 10 Hz to 1000 Hz and digitalization at 2000 samples per second and a channel were used.
The results of two types of intraoperative neuromonitoring (IONM) sessions in the theatre using the ISIS system (Inomed Medizintechnik, Emmendinger, Germany) were analyzed in this study. All IONM protocols included detailed data on demographic, anthropometric, and scoliosis characteristics including their type, range and angles of the pathological curvature (Table 2), time and type of performance of each activity by anesthesiologists and surgeons, screenshots of MEP recordings (Figure 1 Cg and Cf ) with (Figure 1 Co, in "Real-time" IONM sessions - based mainly on bilateral surgeon-neurophysiologist verbal reports) and without (Figure 1 Cj, in "Interactive S-N" IONM sessions - based on the simultaneous MEP recordings with the direct visual inspection of the operation field via the camera, without verbal reports) the surgical field camera photographs, BIS and stimulus strength for TES parameters, the frequency of neurophysiologist's warnings and anaesthesia related events, the incidence and source of false alarms, the averaged time of the surgery and number of bidirectional communications between the surgeon and neurophysiologists and vice versa. They were used for subsequent analyzes of variables and events associated with intraoperatively recorded MEP parameters fluctuations.
Intraoperatively (T1 and T2 periods of observation), MEP was recorded following the application of the transcranial trains of electrical stimuli (TES) in areas of the cortical motor fields in areas of innervation of the selected muscles in the upper and lower extremities. A sequence of four stimuli was applied, with a duration of a single pulse of 500 µs and an intensity of 98.2 mA on average via a pair of bipolar subcutaneous needle electrodes (Figure 2 Bc). The scalp electrodes impendence was about 0.6-0.8 kΩ. Positioning of stimulating electrodes was based on the compilation of descriptions by Deletis [35] and Legatt et al. [45] according to the 10-system; Cz–C3 3–6 cm to the left, and Cz to C4 3–6 cm to the right. The surface disposable Ag/AgCl electrodes (5 mm2 of an active surface) for MEP recordings from TA and PER as well as the other upper and lower extremities muscles (abductor pollicis brevis, extensor carpi group, rectus femoris, abductor hallucis longus) according to the previous descriptions were successfully used (Figure 2 Bb and Ba) [8,22]. MEP recordings from the TA muscle as a marker for the purposes of this study were subjected to detailed analysis due to the possibility of comparing their parameters with the descriptions of other researchers monitoring motor conduction intraoperatively in patients with IS. The only other used needle electrode was the ground one sterilely inserted at the iliac crest (Figure 2 Bb). The stimulating and recording electrodes were mounted and their connections were checked in the supine position as well the first MEP recordings were performed; considered as referenced. Later MEP was recorded in the prone position (T1 observation period), after the patient was transferred to the operating table (Figure 2 Ca), at every stage of surgical correction of scoliosis until it had been completed (T2 observation period). Intraoperatively recorded MEP (Figure 2 Cj and Co) were characterized by a variable amplitude from 100 to 2000 µV and latencies in the range of 27 to 40 ms, but they did not require averaging. The settings of the recorder for of measurements were as follows: filters hardware high-pass 30 Hz; software high-pass 0.5 Hz; software low-pass 2000 Hz; stimulation frequency (Hz) at 0.5–2.4 ms intervals.
2.3. Statistical Analysis
Data were analyzed and compared using Statistica, version 13.1 (StatSoft, Kraków, Poland). During the preliminary data mining, an attempt was undertaken to match patients from the two groups in this study and healthy volunteers concerning their age, sex, and basic anthropomorphic characteristics such as weight and height, as well as their number (Table 2). Minimal and maximal values (range), with mean and standard deviation (SD) were included in the descriptive statistics. The Shapiro–Wilk test and Levene’s test ascertained the normality distribution and homogeneity of variances. Bispectral Index data and the MEP stimulus strengths were of the ordinal scale type, while MEP amplitudes and latencies were of the interval scale type. None of the collected data represented a normal distribution; the Wilcoxon’s signed-rank test was used to compare the differences between results obtained before (T0) and after (T3) surgeries, as well as to compare results at the beginning (T1), and in the end (T2) of the surgical procedures. In the cases of independent variables, the non-parametric Mann–Whitney test was used. Any p-values of <0.05 were considered statistically significant. The results from all neurophysiological tests performed on patients were also calculated from the group of healthy subjects (control group) to achieve the normative parameters used to compare the health status between the patients and the controls. Results did not reveal any significant difference in values of parameters recorded in neurophysiological tests on the left and right sides in controls. Statistical software (StatSoft, Kraków, Poland) was used to determine the required sample size using the primary outcome variable of MEP amplitudes recorded from TA muscles before and after treatment with a power of 80% and a significance level of 0.05 (two-tailed). The mean and standard deviation (SD) were calculated using the data from the first 40 patients, and the sample size software estimated that more than 50 patients in each group with different neuromonitoring scenarios were needed for purposes of this study to observe the statistically significant differences.
3. Results
Subjects belonging to two groups of patients and the healthy volunteers did not differ in demographic and anthropometric characteristics, as well as the severity and extent of idiopathic scoliosis in cases of patients (Table 1). The number of subjects in each group was similar. It is not likely that these variables and factors influenced the differences found in comparing neurophysiological results in the studied groups of patients pre- and intra- and postoperatively and in comparison to the controls (Table 2).
In the group of healthy people (Control), the amplitude and latency parameters recorded from TA and PER did not differ significantly when comparing their values on the right and left sides. However, the cumulative parameters of MEP amplitudes recorded from PER compared to those recorded from TA were approximately 1100µV lower (67%) at p=0.007 (Figure 4A). The cumulative MEP latency parameter recorded bilaterally from PER compared to the recording from TA had values lower by 3.1 ms (10.6%) at p=0.04 Figure 4B).
This trend, an overall decrease in amplitude and shortening of latency in MEP recordings from PER, was also observed in patients from both groups at each follow-up stage at p=0.008-0.04 (Table 2, Figure 4).
In preoperative examinations (T0), the parameters of TMS-induced MEP amplitudes recorded from TA on the right and left sides differed significantly at p=0.04 in both groups of patients but not when recorded from PER. Bilateral MEP recordings from PER at T0 differed similarly in both groups, only significantly in the latency parameter, which was increased on the left side at p=0.04. In general, patients of both groups in MEP recordings from TA and PER differed similarly at the observation stages T0 and T3 compared to healthy volunteers regarding a decrease in amplitude parameters and an increase in latency at p=0.008-0.04. In both groups of patients, the MEP parameters induced by TMS (T0) and induced by TES (T1) did not differ significantly (Table 2, Figure 4). The parameters of MEP amplitudes recorded both from TA and PER intraoperatively in T1 and T2 differed significantly at p=0.04-0.03, indicating an improvement in overall efferent conduction as a result of the surgical intervention for scoliosis correction. One week after surgery (T3), the parameters of TMS-induced MEP amplitudes further increased bilaterally, compared to the tests recorded at T0 in the range of p=0.03-0.02.
The coincidence of the proper positioning of the electrodes stimulating the transcranially motor centers for the innervation of lower than the upper muscles using measurements according to the 10–20 system with the method of preoperative determining the “hot spots” for the recording MEP with the largest amplitudes was calculated at 85%.
The patients of both groups with different spinal efferent transmission neuromonitoring scenarios have been optimally anaesthetized at the same levels of BIS 51.8 on average (Table 3). Similarly to the results of our previous studies [8], the present observations indicate that this level of anaesthesia, when kept constant, minimally affects the variability of the MEP amplitude parameter when applying a TES stimulus strength at an average of 98.2 mA. We did not observe any significant differences in the variability of the MEP amplitude parameter when we applied both variables values mentioned above in the population of patients from the "Interactive S-N neuromonitoring" and "Real-time neuromonitoring" groups.
The number of MEP parameter fluctuations, mainly the amplitudes decreasing, was strictly related to the number of events during certain steps of the surgeries and the associated neurophysiologist's warnings (Table 3). They appeared most frequently, almost twice as much, during transpedicular screws implantation, corrective rods implantation, and during the distraction, derotation, and compression procedures, respectively, more significantly at p=0.04-0.03 in patients from an “Interactive S-N neuromonitoring” than “Real-time neuromonitoring” group. Other changes (5%) in the MEP parameters were detected during surgery field preparation, among others, as the effects of transient “warming” during cauterization (the latency increase) and shocks caused by releasing the vertebral joints (the amplitude drops). They were observed at almost the same frequency in both groups of treated patients. Overheating of the tissues accompanying the cauterization occasionally affected the temporary slowing down (increase the MEP latency parameter) of the conduction of nerve impulses in the spinal cord pathways within the white matter funiculi. The surgical area was rinsed with the 0.9% NaCl solution at 36.6 °C in these cases. This symptom retreated after the suction of the fluid was applied.
The changes in anaesthesia level occurred only occasionally, with no significant differences in frequencies between patients of the two studied groups (Table 3). If detected, they influenced amplitudes of the MEP recorded more from TA than from PER bilaterally. A comparison of recordings presented in Figure 5 may lead to the conclusion that MEP recorded from nerves undergo significant fluctuations of amplitudes at different stages of scoliosis corrections only following the surgeon interventions, and the anaesthesia level changes have greater meaning for MEP parameter fluctuations recorded from muscles but not from nerves.
The rarest reasons for warnings during neuromonitoring of two kinds with no significant differences were false alarms caused by technical malfunctions like electrode resistance changes or disconnections and movement-related artifacts following TES, which influenced the MEP amplitude changes (Table 2).
The average total duration of the operation, measured from the moment of initial anaesthesia and intubation of the patient to the moment of transfer from the operating table to the bed after the suturing of the surgical wound (sterile stimulating and grounding electrodes were removed in the meantime) was significantly (p=0.04) shorter by about 1 hour in the patients from "Real-time neuromonitoring" group. The number of two-way communication during surgery in patients from the "Real-time neuromonitoring" group between the surgeon and neurophysiologist and vice versa was significantly (at p=0.008) reduced by approximately half compared to procedures in patients from the "Interactive S-N neuromonitoring" group (Table 2).
4. Discussion
The main methodological finding in this study regarding TMS- and TES-induced MEP in healthy volunteers and patients with IS demonstrates the utility of recordings from nerves. It is reported that the quality of MEP recordings from muscles during intraoperative neuromonitoring can be significantly influenced by the depths of anaesthesia or muscle relaxant administration [43]. The consequences can be the decreased neuronal transmission along ascending and descending tracts at spinal and supraspinal levels as well as the blockade of transmission of the acetylcholine release at the level of neuromuscular junction. Moreover, MEP recording from muscle may fluctuate more than nerve recording, mainly due to motion artifacts resulting from the aftermath of stimulation. It should also be remembered that during prolonged neurosurgical procedures, the natural, gradual attenuation of the signals may occur more in children than adults, and the origin of these changes remains unexplained [22]. The results at different stages of observations in this study indicate that although the amplitudes of recordings from PER are significantly lower than those recorded from TA, they are resistant to variability in the level of anaesthesia and other factors occurring inevitably during the surgery. Our study provides evidence that in both groups of patients, anaesthesia level at an average 51,8 of BIS of minimally affects the variability of the MEP amplitude, especially in PER recordings when applied TES strength is at 98.2 mA. MEP recorded from nerves appears stable enough to provide reliable information regarding efferent neural conduction in patients with advanced neurogenic muscle changes.
The concept of the MEP recording from the nerve during neuromonitoring was mentioned by Gonzales et al. [46], but following the direct spinal cord stimulation; it is a pity that the methodological principles of this method haven’t been described in detail. Among the known descriptions of this method are motor evoked potentials recorded from nerves versus muscles following lumbar stimulation with the magnetic field in healthy subjects and patients with disc-root conflicts, provided by Garasz et al. [37]. In their studies, like in this report, mean values of MEP amplitudes recorded from nerves significantly differed from those recorded in anatomically related muscles in controls and patients; they were about 30% and 51% smaller, respectively. In both groups of subjects, latencies of MEP recorded from nerves were shorter at about 3.0 ms than those recorded from muscles. The non-invasive method of MEP recorded from nerves can help diagnose patients with visible atrophic changes in muscles and simultaneous symptoms of only slight pathology in the transmission of nerve impulses peripherally, similarly in cases of advanced IS patients.
In about 13% of cases of the patients in this study belonging to both studied groups who underwent spinal deformity correction, it was necessary to alert the surgeon from the neuromonitoring team about the fluctuations of MEP recording parameters. This corresponds well with the previous data provided by Vitale et al [20]. According to the data of Hicks et al. [47], the risk of incorrect implantation of pedicle screws during IS surgery is lower at 4.2%, the same may apply to the probable disruption of the spinal cord root structures. The estimates of Kwan et al. [48] are much more lower at approximately 0.95% rate of major complications and 1.32% rate of minor complications; however, it should be taken into account that they concern surgical treatment mainly of patients with Lenke 1 curvature type. Similarly to observations of the above mentioned authors, in our study the number of MEP parameter fluctuations, mainly the amplitudes decreasing, was strictly associated with the neurophysiologist's warnings due to transpedicular screws implantation, corrective rods implantation, distraction, derotation, and compression procedures, respectively; at p=0.04-0.03 more in patients from the “Interactive S-N neuromonitoring” group. A similar order of some sources of threats during IONM was reported by Lyon et al. [49], although in their opinion the distraction procedure during IS correction could be the most traumatic. We have found the movement-related artifacts following TES as the rarest reason which influenced the MEP amplitude changes during IONM like in the study of Yoshida et al. [50]. The fluctuation of the MEP amplitude parameter [51] less than the latency [52] is typical in describing the IONM most frequent reasons for alerts. The presented results from patients with IS mainly type 2 according to Lenke indicate that the permanent loss of neuromonitoring signals is likely to occur rarely during distraction and derotation procedures which supports the observation of Rizkallah et al. [53]. Our preliminary comparison of MEP recordings in T2 and T3 periods indicates that only patients with fluctuations of MEP amplitude but not latency parameters at the level of 45% compared to controls may show moderate unilateral motor deficits postoperatively, which is similar to opinion of Buckwalter et al. [54].
In all patients the motor evoked potentials parameters induced by TMS (T0) and TES (T1) did not differ in this study. This indicates the importance of a preoperative neurophysiological assessment, showing the current neurological status of a patient with IS, which should be expected in the perioperative period, also for the purposes of neuromonitoring, constituting a source of valuable knowledge for both the neurophysiologist and the surgeon. The same opinion is shared by Glasby et al. [55] and Virk et al. [56] together with Lo et al. [57], who also underline that early recognition of MEP properties is important to prevent false positives in the course of IONM for spinal surgery.
This and previous studies [8,22,23,24] indicate high sensitivity of recording surface electrodes when performing IONM, sufficient to ensure reliable verification of spinal efferent conduction during scoliosis surgery. According to our experience using surface electrodes for IONM purposes, the cost of a set of eight pairs compared to needle electrodes is nine times lower [22]. The postoperative disposal of surface electrodes is also safer, more accessible, ecological and cheaper than needle electrodes; their non-invasiveness is non-disputable.
The paediatric nature of the corrective spine procedures in patients with IS dictates the need for the least invasiveness, which in the current work is met by MEP recordings using surface electrodes from the muscles and nerves of the lower extremities. For IONM, we used a pair of needle electrodes (but not the standard corkscrew electrodes) applied bilaterally subcutaneously on the scalp for stimulation purposes and a single needle electrode at the level of the iliac crest as the ground electrode. Thanks to this choice, we avoided ecchymoses, bruises or rare infections which were reported during IONM [58], reddening of the skin, which was observed in 16% of patients with the accompanying symptom of increased pain, sometimes lasting up to 6 months after the surgery [59], and a significant risk of needle stick injuries by neurophysiologists and other workers in the theatre during electrode implantation and the removal after surgery.
In this report, as in the previous work [8], we demonstrated an immediate improvement in the parameters of nerve impulse conduction of efferent transmission in spinal pathways following surgical correction of scoliosis at T2. Similarly, in both groups with different neuromonitoring scenarios, we have also found further improvement at T3, based on the bilateral recordings of MEP amplitudes from the tibialis anterior TA muscles bilaterally, as well as recordings from the PER nerves. Moreover, we have found that the average duration of the surgery was significantly shorter by about 1 hour in the "Real-time neuromonitoring" group, and the number of two-way communications between the surgeon and neurophysiologist and vice versa was reduced by approximately half. This proves that the "Real-time neuromonitoring" scenario shortens two-way IONM communication between the neurophysiologist and the surgeon performing subsequent scoliosis correction procedures on the principle of "fewer words - faster response", increasing the effectiveness of neuromonitoring and the comfort of work of the surgeon who is solely engaged in performing IS correction procedures. This is yet another proof that the success of complex surgical correction of IS with the effective involvement of IONM depends on close cooperation and good coordination of the team of surgeons, anesthesiologists, neurophysiologists and instrument staff in the operating room [33].
One of the limitations of this study could be the allegation that the patients selected for the sample in both groups with different scenarios of IONM represented different types of IS curvatures according to Lenke from 1 to 3 (mainly 2), which would bias the study design, especially the recorded parameters of MEP in T0-T3 periods of observation. However, the preliminary selection intended to choose patients with similar primary and secondary spinal curvature angles in both groups (Figure 1).
Future neurophysiological studies should concentrate on the correlation of the morphology and parameters of MEP recorded pre- and postoperatively with the clinical evaluation of the curvature angles improvement which was not studied in detail in IS patients, which has not only cognitive but also practical meaning.
5. Conclusions
Even if the presented concept of "Real-time neuromonitoring" may be considered obvious, the results of its application may lead to the conclusion that the cooperation of the neurophysiologist with the surgeon with minimal two-way verbal communication during IONM increases his attention only to surgical procedures, and by increasing his comfort of work, it thus affects the safety of the entire surgery. The "real-time monitoring" shortens the overall duration of surgery which minimizes the side-effect impact of the anesthesia applied on the patient which is of the greatest importance, thinking about its long-term effects on the cardiac and the nervous system function. The modifications of the MEP nerve conduction recording technology presented in the study using surface electrodes from nerves allow for precise and reliable information about the patient's neurological condition at every stage of surgical procedures, even under conditions of slight fluctuations in anesthesia. It is non-invasive and more economical compared to standard needle recordings, justifiable for IONM in surgery on pediatric patients, including patients with IS.
Author Contributions
Conceptualisation, P.D., J.H. and T.K.; methodology, P.D., J.H., K.K. and T.K.; software, J.H.; validation, P.D., J.H., K.K. and T.K.; formal analysis, P.D., J.H., K.K. and T.K.; investigation, P.D., J.H., K.K., P.J., P.G., M.T. and T.K.; resources, P.D. and J.H.; data curation, P.D., J.H., K.K. and T.K.; writing—original draft preparation, P.D. and J.H.; writing—review and editing, P.D., J.H., P.J. and T.K.; visualisation, J.H.; supervision, P.D., J.H. and T.K.; project administration, P.D. and J.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Informed Consent Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Bioethics Committee of Poznań University of Medical Science, decision no 942/21 dated on 13th January 2022.
Data Availability Statement
All the data generated or analysed during this study are included in this published article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Dayer, R.; Haumont, T.; Belaieff, W.; Lascombes, P. Idiopathic scoliosis: etiological concepts and hypotheses. J. Childr. Orthop. 2013, 7, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Konieczny, M.R.; Senyurt, H.; Krauspe, R. Epidemiology of adolescent idiopathic scoliosis. J. Child. Orthop. 2013, 7, 3–9. [Google Scholar] [CrossRef]
- Hresko, M.T. Idiopathic Scoliosis in Adolescents. N. Engl. J. Med. 2013, 368, 834–841. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Antonini, G.; Carabalona, R.; Minozzi, S. Physical exercises as a treatment for adolescent idiopathic scoliosis. A systematic review. Pediatr. Rehabil. 2003, 6, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Minozzi, S.; Bettany-Saltikov, J.; Zaina, F.; Chockalingam, N.; Grivas, T.B.; Kotwicki, T.; Maruyama, T.; Romano, M.; Vasiliadis, E.S. Braces for idiopathic scoliosis in adolescents. Spine 2010, 35, 1285–1293. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, S.L.; Dolan, L.A.; Wright, J.G.; Dobbs, M.B. Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med. 2013, 369, 1512–1521. [Google Scholar] [CrossRef] [PubMed]
- Pepke, W.; Morani, W.; Schiltenwolf, M.; Bruckner, T.; Renkawitz, T.; Hemmer, S.; Akbar, M. Outcome of Conservative Therapy of Adolescent Idiopathic Scoliosis (AIS) with Chêneau-Brace. J. Clin. Med. 2023, 12, 2507. [Google Scholar] [CrossRef] [PubMed]
- Daroszewski, P.; Huber, J.; Kaczmarek, K.; Janusz, P.; Główka, P.; Tomaszewski, M.; Domagalska, M.; Kotwicki, T. Comparison of Motor Evoked Potentials Neuromonitoring Following Pre- and Postoperative Transcranial Magnetic Stimulation and Intraoperative Electrical Stimulation in Patients Undergoing Surgical Correction of Idiopathic Scoliosis. J. Clin. Med. 2023, 12, 6312. [Google Scholar] [CrossRef]
- Huh, S.; Eun, L.Y.; Kim, N.K.; Jung, J.W.; Choi, J.Y.; Kim, H.S. Cardiopulmonary function and scoliosis severity in idiopathic scoliosis children. Kor. J. Ped. 2015, 58, 218–223. [Google Scholar] [CrossRef]
- Kelly, J.; Shah, N.; Freetly, T.; Dekis, J.; Hariri, O.; Walker, S.; Borrelli, J.; Post, N.H.; Diebo, B.G.; Urban, W.P.; Paulino, C.B. Treatment of adolescent idiopathic scoliosis and evaluation of the adolescent patient. Curr. Orthop. Pract. 2018, 29, 424–429. [Google Scholar] [CrossRef]
- Lee, C.S.; Hwang, C.J.; Lee, D.H.; Cho, J.H.; Park, S. Risk Factors and Exit Strategy of Intraoperative Neurophysiological Monitoring Alert During Deformity Correction for Adolescent Idiopathic Scoliosis. Global Spine J. Published online March 14. 2023. [Google Scholar] [CrossRef] [PubMed]
- Vitale, M.G.; Moore, D.W.; Matsumoto, H.; Emerson, R.G.; Booker, W.A.; Gomez, J.A.; Gallo, E.J.; Hyman, J.E.; Roye, D.P. Jr Risk factors for spinal cord injury during surgery for spinal deformity. J. Bone Joint Surg. 2010, 92, 64–71. [Google Scholar] [CrossRef]
- Bridwell, K.H.; Lenke, L.G.; Baldus, C.; Blanke, K. Major intraoperative neurologic deficits in pediatric and adult spinal deformity patients. Incidence and etiology at one institution. Spine 1998, 23, 324–331. [Google Scholar] [CrossRef]
- Schwartz, D.M.; Auerbach, J.D.; Dormans, J.P.; Flynn, J.; Drummond, D.S.; Bowe, J.A.; Laufer, S.; Shah, S.A.; Bowen, J.R.; Pizzutillo, P.D.; Jones, K.J.; Drummond, D.S. Neurophysiological detection of impending spinal cord injury during scoliosis surgery. J. Bone J. Surg. 2007, 89, 2440–2449. [Google Scholar] [CrossRef]
- Pastorelli, F.; Di Silvestre, M.; Plasmati, R.; Michelucci, R.; Greggi, T.; Morigi, A.; Bacchin, M.R.; Bonarelli, S.; Cioni, A.; Vommaro, F.; et al. The prevention of neural complications in the surgical treatment of scoliosis: The role of the neurophysiological intraoperative monitoring. Eur. Spine J. 2011, 20, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.H.; Park, Y.G.; Kim, D.H.; Yoon, S.Y. Monitoring of Motor and Somatosensory Evoked Potentials During Spine Surgery: Intraoperative Changes and Postoperative Outcomes. Ann. Rehabil. Med. 2016, 40, 470–480. [Google Scholar] [CrossRef]
- Fehlings, M.G.; Brodke, D.S.; Norvell, D.C.; Dettori, J.R. The evidence for intraoperative neurophysiological monitoring in spine surgery: does it make a difference? Spine 2010, 35 (9 Suppl),, S37–S46. [Google Scholar] [CrossRef]
- Gonzalez, A.A.; Jeyanandarajan, D.; Hansen, C.; Zada, G.; Hsieh, P.C. Intraoperative neurophysiological monitoring during spine surgery: a review. Neurosurgical Focus 2009, 27, E6. [Google Scholar] [CrossRef]
- Lall, R.R.; Hauptman, J.S.; Munoz, C.; et al. Intraoperative neurophysiological monitoring in spine surgery: indications, efficacy, and role of the preoperative checklist. Neurosurgical Focus 2012, 33, E10. [Google Scholar] [CrossRef] [PubMed]
- Vitale, M.G.; Skaggs, D.L.; Pace, G.I.; Wright, M.L.; Matsumoto, H.; Anderson, R.C.; Brockmeyer, D.L.; Dormans, J.P.; Emans, J.B.; Erickson, M.A.; Flynn, J.M.; Glotzbecker, M.P.; Ibrahim, K.N.; Lewis, S.J.; Luhmann, S.J.; Mendiratta, A.; et al. Best Practices in Intraoperative Neuromonitoring in Spine Deformity Surgery: Development of an Intraoperative Checklist to Optimize Response. Spine Deformity 2014, 2, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Ziewacz, J.E.; Berven, S.H.; Mummaneni, V.P.; Tu, T.H.; Akinbo, O.C.; Lyon, R.; Mummaneni, P.V. The design, development, and implementation of a checklist for intraoperative neuromonitoring changes. Neurosurgical Focus 2012, a33, E11. [Google Scholar] [CrossRef]
- Daroszewski, P.; Garasz, A.; Huber, J.; Kaczmarek, K.; Janusz, P.; Główka, P.; Tomaszewski, M.; Kotwicki, T. Update on neuromonitoring procedures applied during surgery of the spine—Observational study. Reumatologia 2023, 61, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Gadella, M.C.; Dulfer, S.E.; Absalom, A.R.; Lange, F.; Scholtens-Henzen, C.H.; Groen, R.J.; Wapstra, F.H.; Faber, C.; Tamási, K.; Sahinovic, M.M.; et al. Comparing Motor-Evoked Potential Characteristics of Needle versus Surface Recording Electrodes during Spinal Cord Monitoring-The NERFACE Study Part I. J. Clin. Med. 2023, 12, 1404. [Google Scholar] [CrossRef] [PubMed]
- Dulfer, S.E.; Gadella, M.C.; Tamási, K.; Absalom, A.R.; Lange, F.; Scholtens-Henzen, C.H.; Faber, C.; Wapstra, F.H.; Groen, R.J.; Sahinovic, M.M.; et al. Use of Needle Versus Surface Recording Electrodes for Detection of Intraoperative Motor Warnings: A Non-Inferiority Trial. The NERFACE Study Part II. J. Clin. Med. 2023, 12, 1753. [Google Scholar] [CrossRef] [PubMed]
- Nuwer, M.R.; Dawson, E.G.; Carlson, L.G.; et al. Somatosensory evoked potential spinal cord monitoring reduces neurologic deficits after scoliosis surgery: results of a large multicenter survey. Electroencephalogr. Clin. Neurophysiol. 1995, 96, 6.e11. [Google Scholar] [CrossRef]
- Levin, D.N.; Strantzas, S.; Steinberg, B.E. Intraoperative neuromonitoring in paediatric spinal surgery. BJA Education 2019, 19, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Acharya, S.; Palukuri, N.; Gupta, P.; Kohli, M. Transcranial Motor Evoked Potentials during Spinal Deformity Corrections-Safety, Efficacy, Limitations, and the Role of a Checklist. Front Surg. 2017, 4, 8. [Google Scholar] [CrossRef] [PubMed]
- Winter, R. B. Neurologic safety in spinal deformity surgery. Spine 1997, 22, 1527–1533. [Google Scholar] [CrossRef]
- Yu, Z.; Pan, W.; Chen, J.; Peng, X.; Ling, Z.; Zou, X. Application of electrophysiological measures in degenerative cervical myelopathy. Front. Cell. Devel. Biol. 2022, 10, 834668. [Google Scholar] [CrossRef]
- Dietz, V.; Curt, A. Neurological aspects of spinal-cord repair: promises and challenges. Lancet Neurol. 2006, 5, 688–694. [Google Scholar] [CrossRef]
- Leszczyńska, K.; Huber, J. Comparing Parameters of Motor Potentials Recordings Evoked Transcranially with Neuroimaging Results in Patients with Incomplete Spinal Cord Injury: Assessment and Diagnostic Capabilities. Biomedicines 2023, 11, 2602. [Google Scholar] [CrossRef]
- Lo, Y.L.; Chan, L.L.; Lim, W.; Tan, S.B.; Tan, C.T.; Chen, J.L.; Fook-Chong, S.; Ratnagopal, P. Transcranial magnetic stimulation screening for cord compression in cervical spondylosis. J. Neurol. Sci. 2006, 244, 17–21. [Google Scholar] [CrossRef]
- Biscevic, M.; Sehic, A.; Krupic, F. Intraoperative neuromonitoring in spine deformity surgery: modalities, advantages, limitations, medicolegal issues - surgeons' views. EFORT Open Rev. 2020, 5, 9–16. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, D.B. Intraoperative motor evoked potential monitoring: Overview and update. J. Clin. Monit. Comput. 2006, 20, 347–377. [Google Scholar] [CrossRef] [PubMed]
- Deletis, V. Basic methodological principles of multimodal intraoperative monitoring during spine surgeries. Eur. Spine J. 2007, 16 (Suppl. S2), 147–152. [Google Scholar] [CrossRef]
- Charalampidis, A.; Jiang, F.; Wilson, J.R.F.; Badhiwala, J.H.; Brodke, D.S.; Fehlings, M.G. Use of Intraoperative Neurophysiological Monitoring in Spine Surgery. Global Spine J. 2020, 10, 104–114. [Google Scholar] [CrossRef]
- Garasz, A.; Huber, J.; Grajek, M.; Daroszewski, P. Motor evoked potentials recorded from muscles versus nerves after lumbar stimulation in healthy subjects and patients with disc-root conflicts. Int. J. Artif. Organs. 2023, 46, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Johansen, J.W.; Sebel, P.S. Development and clinical application of electroencephalographic bispectrum monitoring. Anesthesiology 2000, 93, 1336–1344. [Google Scholar] [CrossRef]
- Medical Advisory Secretariat. Bispectral index monitor: An evidence-based analysis. Ont. Health Technol. Assess. Ser. 2004, 4, 1–70. [Google Scholar]
- Viertiö-Oja, H.; Maja, V.; Särkelä, M.; Talja, P.; Tenkanen, N.; Tolvanen-Laakso, H.; Paloheimo, M.; Vakkuri, A.; Yli-Hankala, A.; Meriläinen, P. Description of the Entropy algorithm as applied in the Datex-Ohmeda S/5 Entropy Module. Acta Anaesthesiol. Scand. 2004, 48, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Lenke, L.G.; Betz, R.R.; Harms, J.; Bridwell, K.H.; Clements, D.H.; Lowe, T.G.; Blanke, K. Adolescent idiopathic scoliosis: A new classification to determine extent of spinal arthrodesis. J. Bone Jt. Surg. 2001, 83, 1169–1181. [Google Scholar] [CrossRef]
- Ovadia, D. Classification of adolescent idiopathic scoliosis (AIS). J. Child Orthop. 2013, 7, 25–28. [Google Scholar] [CrossRef]
- Soghomonyan, S.; Moran, K.R.; Sandhu, G.S.; Bergese, S.D. Anesthesia and evoked responses in neurosurgery. Front. Pharmacol. 2014, 14, 5–74. [Google Scholar] [CrossRef]
- Wincek, A.; Huber, J.; Leszczyńska, K.; Fortuna, W.; Okurowski, S.; Chmielak, K.; Tabakow, P. The Long-Term Effect of Treatment Using the Transcranial Magnetic Stimulation rTMS in Patients after Incomplete Cervical or Thoracic Spinal Cord Injury. J. Clin. Med. 2021, 10, 2975. [Google Scholar] [CrossRef]
- Legatt, A.D.; Emerson, R.G.; Epstein, C.M.; MacDonald, D.B.; Deletis, V.; Bravo, R.J.; López, J.R. ACNS Guideline: Transcranial Electrical Stimulation Motor Evoked Potential Monitoring. J. Clin. Neurophysiol. 2016, 33, 42–50. [Google Scholar] [CrossRef]
- Gonzalez, A.A.; Jeyanandarajan, D.; Hansen, C.; Zada, G.; Hsieh, P.C. Intraoperative neurophysiological monitoring during spine surgery: a review. Neurosurg. Focus 2009, 27, E6. [Google Scholar] [CrossRef]
- Hicks, J.M.; Singla, A.; Shen, F.H.; Arlet, V. Complications of pedicle screw fixation in scoliosis surgery: A systematic review. Spine 2010, 35, E465–E470. [Google Scholar] [CrossRef] [PubMed]
- Kwan, M.K.; Loh, K.W.; Chung, W.H.; Hasan, M.S.; Chan, C.Y.W. Perioperative outcome and complications following single-staged posterior spinal fusion using pedicle screw instrumentation in adolescent idiopathic scoliosis(AIS): A review of 1057 cases from a single centre. BMC Musculoskelet. Disord. 2021, 22, 413. [Google Scholar] [CrossRef] [PubMed]
- Lyon, R.; Lieberman, J.A.; Grabovac, M.T.; Hu, S. Strategies for managing decreased motor evoked potential signals while distracting the spine during correction of scoliosis. J. Neurosurg. Anesthesiol. 2004, 16, 167–170. [Google Scholar] [CrossRef]
- Yoshida, G.; Imagama, S.; Kawabata, S.; Yamada, K.; Kanchiku, T.; Fujiwara, Y.; Tadokoro, N.; Takahashi, M.; Wada, K.; Yamamoto, N.; et al. Adverse Events Related to Transcranial Electric Stimulation for Motor-evoked Potential Monitoring in High-risk Spinal Surgery. Spine 2019, 44, 1435–1440. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, K.; Imagama, S.; Ito, Z.; Ando, K.; Hida, T.; Ito, K.; Tsushima, M.; Ishikawa, Y.; Matsumoto, A.; Nishida, Y.; et al. Transcranial motor evoked potential waveform changes in corrective fusion for adolescent idiopathic scoliosis. J. Neurosurg. Pediatr. 2017, 19, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Luc, F.; Mainard, N.; Payen, M.; Bernardini, I.; El-Ayoubi, M.; Friberg, A.; Piccoli, N.D.; Simon, A.L. Study of the latency of transcranial motor evoked potentials in spinal cord monitoring during surgery for adolescent idiopathic scoliosis. Neurophysiol. Clin. 2022, 52, 299–311. [Google Scholar] [CrossRef] [PubMed]
- Rizkallah, M.; El Abiad, R.; Badr, E.; Ghanem, I. Positional disappearance of motor evoked potentials is much more likely to occur in non-idiopathic scoliosis. J. Child. Orthop. 2019, 13, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Buckwalter, J.A.; Yaszay, B.; Ilgenfritz, R.M.; Bastrom, T.P.; Newton, P.O. Harms Study Group Analysis of Intraoperative Neuromonitoring Events During Spinal Corrective Surgery for Idiopathic Scoliosis. Spine Deformity 2013, 1, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Glasby, M.A.; Tsirikos, A.I.; Henderson, L.; Horsburgh, G.; Jordan, B.; Michaelson, C.; Adams, C.I.; Garrido, E. Transcranial magnetic stimulation in the semi-quantitative, pre-operative assessment of patients undergoing spinal deformity surgery. Eur. Spine J. 2017, 26, 2103–2111. [Google Scholar] [CrossRef] [PubMed]
- Virk, S.; Klamar, J.; Beebe, A.; Ghosh, D.; Samora, W. The Utility of Preoperative Neuromonitoring for Adolescent Idiopathic Scoliosis. Int. J. Spine Surg. 2019, 13, 317–320. [Google Scholar] [CrossRef]
- Lo, Y.L.; Tan, Y.E.; Raman, S.; Teo, A.; Dan, Y.F.; Guo, C.M. Systematic re-evaluation of intraoperative motor-evoked potential suppression in scoliosis surgery. Scoliosis Spinal Disord. 2018, 13, 12. [Google Scholar] [CrossRef]
- Darcey, T.M.; Kobylarz, E.J.; Pearl, M.A.; Krauss, P.J.; Ferri, S.A.; Roberts, D.W.; Bauer, D.F. Safe use of subdermal needles for intraoperative monitoring with MRI. Neurosurg. Focus 2016, 40, E19. [Google Scholar] [CrossRef]
- Sanders, A.; Andras, L.; Lehman, A.; Bridges, N.; Skaggs, D.L. Dermal Discolorations and Burns at Neuromonitoring Electrodes in Pediatric Spine Surgery. Spine 2017, 42, 20–24. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of the study with the design and the scoliotic subjects selection criteria at the subsequent three stages. Abbreviations: MEPs – motor evoked potentials.
Figure 1.
Flow chart of the study with the design and the scoliotic subjects selection criteria at the subsequent three stages. Abbreviations: MEPs – motor evoked potentials.
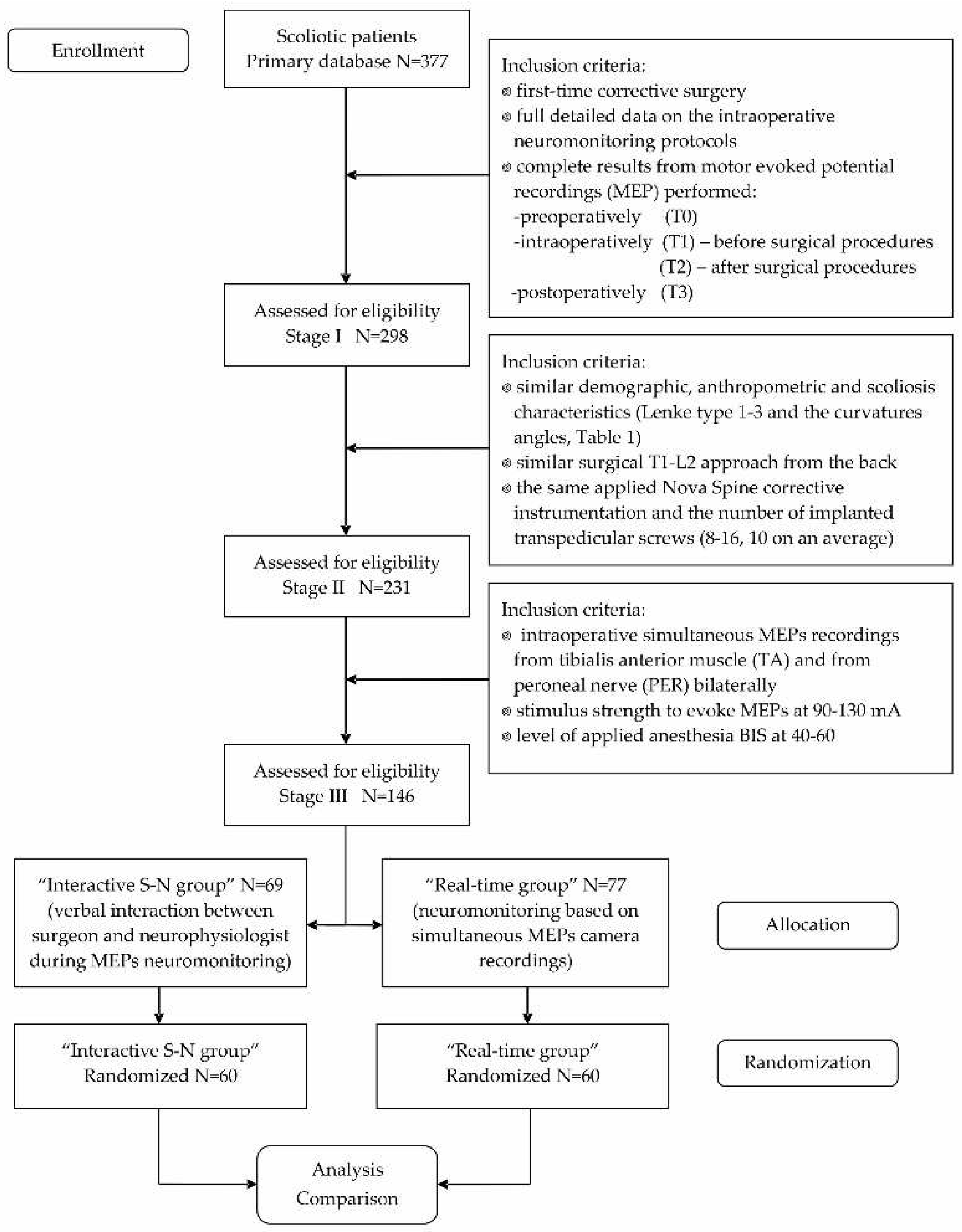
Figure 2.
Methodological principles, the study design, and examples of the most relevant recordings from the clinical and MEP neurophysiological studies in patients belonging to two studied groups. The same neurophysiological methodology was used in healthy volunteers once. Aa – location of the recording bipolar electrodes over the anatomical passage of the peroneal nerve (PER) and the surface of anterior tibial muscle (TA) applied in pre- and postoperative examinations. Ab – preoperative positioning of the stimulating coil over the scalp for the transcranial magnetic stimulation (TMS; experimentally changed following the tracking aimed to obtain the best, highest amplitude MEP recordings) which allowed markings black points of the “hot spots” (Ac) for the intraoperative stimulating electrodes application (Bc; for TES - transcranial electrical stimulation). The placement of the intraoperative recording bipolar electrodes over TA and PER as well as the rectus femoris muscle (RF, Ba) and over the forearm extensor carpi muscle group (EXT C, Bb) was stabilized with the adhesive patch tapes. Ca – prone position of the patient with the applied recording electrodes and prepared for the surgery from the back approach in the theatre. Photographs illustrating a view of the thoracolumbar spine preparation at the subsequent steps before (Cb,c) and after (Cd) implantation of two titanium rods for distraction and derotation procedures performed by the surgeon. The positioning of the transpedicular screws was also verified by X-rays with C-arm (Ce). The neuromonitoring recordings at the distant range from the surgical field aimed to verify the spinal neural motor transmission without (Cf, in “Interactive S-N” patients group) or with (Cg, in “Real-time” patients group) the camera picture support and the simultaneous MEP recordings. Photographs of the body silhouettes and anterior-posterior X-rays performed in T0 in patients belonging to both groups are shown in Ch and Cm, as well as in Cl and Cr in T3, for comparison of similarities, respectively. Note the diminishing of the primary and the secondary spine curvatures. Examples of the MEP recorded in T0 (Ci and Cn) and in T3 (Ck and Cp) following TMS and intraoperatively following TES (Cj versus Co) have been presented for comparison, to indicate the amplitudes increasing in patients (both Lenke 2 type) of two studied groups especially with PER recordings. Abbreviations: T0 – preoperative period of observation, T1 –intraoperative period of observation before surgical procedures, T2 – intraoperative period of observation after surgical procedures, T3 – postoperative period of observation after one week, r – recording, TA – tibialis anterior muscle recording, PER – peroneal nerve recording, MEP – motor evoked potential, TMS - transcranial magnetic stimulation; TES – transcranial electrical stimulation.
Figure 2.
Methodological principles, the study design, and examples of the most relevant recordings from the clinical and MEP neurophysiological studies in patients belonging to two studied groups. The same neurophysiological methodology was used in healthy volunteers once. Aa – location of the recording bipolar electrodes over the anatomical passage of the peroneal nerve (PER) and the surface of anterior tibial muscle (TA) applied in pre- and postoperative examinations. Ab – preoperative positioning of the stimulating coil over the scalp for the transcranial magnetic stimulation (TMS; experimentally changed following the tracking aimed to obtain the best, highest amplitude MEP recordings) which allowed markings black points of the “hot spots” (Ac) for the intraoperative stimulating electrodes application (Bc; for TES - transcranial electrical stimulation). The placement of the intraoperative recording bipolar electrodes over TA and PER as well as the rectus femoris muscle (RF, Ba) and over the forearm extensor carpi muscle group (EXT C, Bb) was stabilized with the adhesive patch tapes. Ca – prone position of the patient with the applied recording electrodes and prepared for the surgery from the back approach in the theatre. Photographs illustrating a view of the thoracolumbar spine preparation at the subsequent steps before (Cb,c) and after (Cd) implantation of two titanium rods for distraction and derotation procedures performed by the surgeon. The positioning of the transpedicular screws was also verified by X-rays with C-arm (Ce). The neuromonitoring recordings at the distant range from the surgical field aimed to verify the spinal neural motor transmission without (Cf, in “Interactive S-N” patients group) or with (Cg, in “Real-time” patients group) the camera picture support and the simultaneous MEP recordings. Photographs of the body silhouettes and anterior-posterior X-rays performed in T0 in patients belonging to both groups are shown in Ch and Cm, as well as in Cl and Cr in T3, for comparison of similarities, respectively. Note the diminishing of the primary and the secondary spine curvatures. Examples of the MEP recorded in T0 (Ci and Cn) and in T3 (Ck and Cp) following TMS and intraoperatively following TES (Cj versus Co) have been presented for comparison, to indicate the amplitudes increasing in patients (both Lenke 2 type) of two studied groups especially with PER recordings. Abbreviations: T0 – preoperative period of observation, T1 –intraoperative period of observation before surgical procedures, T2 – intraoperative period of observation after surgical procedures, T3 – postoperative period of observation after one week, r – recording, TA – tibialis anterior muscle recording, PER – peroneal nerve recording, MEP – motor evoked potential, TMS - transcranial magnetic stimulation; TES – transcranial electrical stimulation.

Figure 3.
Methodological concept of the “Real-time intraoperative neuromonitoring”, when changes in parameters of MEP bilateral recordings are analyzed during but not after performing subsequent steps of the surgical procedures which would insult the spinal cord structures. Observation of the surgical field with the camera picture allows an immediate warning reaction when MEP parameters change simultaneously. A – surgical field preparation with the muscles cauterization, B - transpedicular screw implantation, C - corrective rod implantation, correction, distraction, and derotation of the spine curvature, D - contralateral corrective rod fixation. Calibration bars for amplification (in µV) and time base (in ms) are the same for each of the MEP recordings. Note more stable nerve recordings in every step of the surgery even at slight changes in the anaesthesia level verified by BIS. Abbreviation: BIS - Bispectral Index Monitor; TA – tibialis anterior muscle recording, PER – peroneal nerve recording, T1 – period of observation before performing the surgical procedures, T2 - period of observation after completion of the surgical procedures.
Figure 3.
Methodological concept of the “Real-time intraoperative neuromonitoring”, when changes in parameters of MEP bilateral recordings are analyzed during but not after performing subsequent steps of the surgical procedures which would insult the spinal cord structures. Observation of the surgical field with the camera picture allows an immediate warning reaction when MEP parameters change simultaneously. A – surgical field preparation with the muscles cauterization, B - transpedicular screw implantation, C - corrective rod implantation, correction, distraction, and derotation of the spine curvature, D - contralateral corrective rod fixation. Calibration bars for amplification (in µV) and time base (in ms) are the same for each of the MEP recordings. Note more stable nerve recordings in every step of the surgery even at slight changes in the anaesthesia level verified by BIS. Abbreviation: BIS - Bispectral Index Monitor; TA – tibialis anterior muscle recording, PER – peroneal nerve recording, T1 – period of observation before performing the surgical procedures, T2 - period of observation after completion of the surgical procedures.
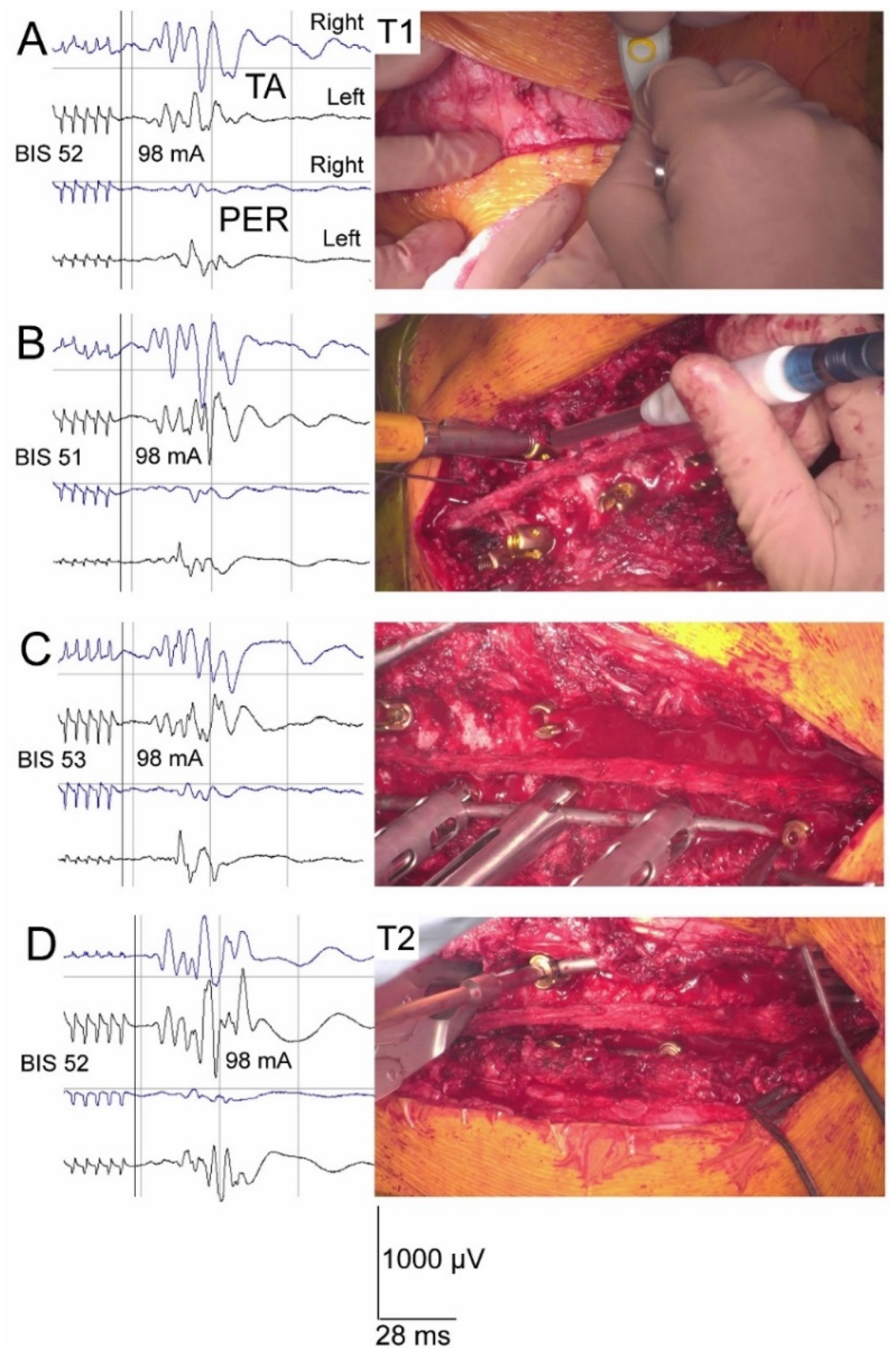
Figure 4.
Comparison of the amplitudes (A) and latencies (B) cumulative values of MEP recorded from tibialis anterior muscle (TA) and peroneal nerve (PER) in patients belonging to two groups with different neuromonitoring scenarios in four periods of observation (T0-preoperative, T1 – intraoperative before IS correction, T2 - intraoperative after IS correction, T3 – postoperative). Normative parameters are presented for comparison as well (Control).
Figure 4.
Comparison of the amplitudes (A) and latencies (B) cumulative values of MEP recorded from tibialis anterior muscle (TA) and peroneal nerve (PER) in patients belonging to two groups with different neuromonitoring scenarios in four periods of observation (T0-preoperative, T1 – intraoperative before IS correction, T2 - intraoperative after IS correction, T3 – postoperative). Normative parameters are presented for comparison as well (Control).
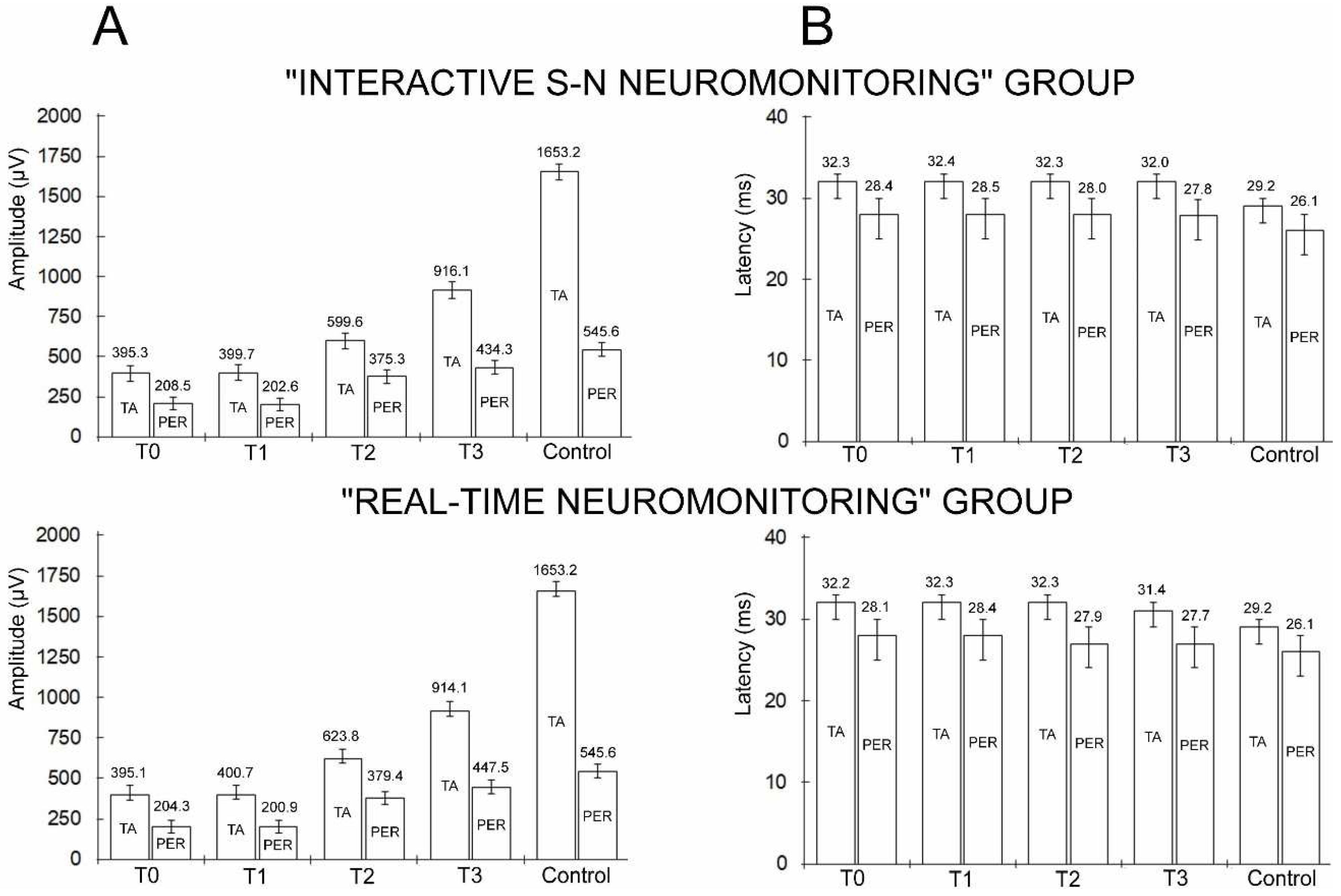
Figure 5.
Examples of the intraoperative MEP recordings in two patients from "Interactive S-N" (A) and "Real-time" group (B) undergoing the surgical correction of idiopathic scoliosis before surgical procedures (T1, a), after pedicle screws implantation (b) and after completion of all surgical procedures (T2, c). The arrangement of recording sites from muscles and nerves bilaterally presented in Aa is common for all examples. Note calibration bars for amplifications (in µV) are different for recordings in A and B. Recordings were performed in two patients at similar levels of anesthesia as indicated by BIS values and following the similar strengths of transcranial stimulation expressed in mA. Comparison of the amplitudes in MEP recordings especially from nerves convinces about the resistance to anesthetic condition changes, they only fluctuate following the surgeries procedures. Abbreviation: BIS - Bispectral Index Monitor; TA – tibialis anterior muscle recording, PER – peroneal nerve recording, T1 – period of observation before performing the surgical procedures, T2 - period of observation after completion of the surgical procedures.
Figure 5.
Examples of the intraoperative MEP recordings in two patients from "Interactive S-N" (A) and "Real-time" group (B) undergoing the surgical correction of idiopathic scoliosis before surgical procedures (T1, a), after pedicle screws implantation (b) and after completion of all surgical procedures (T2, c). The arrangement of recording sites from muscles and nerves bilaterally presented in Aa is common for all examples. Note calibration bars for amplifications (in µV) are different for recordings in A and B. Recordings were performed in two patients at similar levels of anesthesia as indicated by BIS values and following the similar strengths of transcranial stimulation expressed in mA. Comparison of the amplitudes in MEP recordings especially from nerves convinces about the resistance to anesthetic condition changes, they only fluctuate following the surgeries procedures. Abbreviation: BIS - Bispectral Index Monitor; TA – tibialis anterior muscle recording, PER – peroneal nerve recording, T1 – period of observation before performing the surgical procedures, T2 - period of observation after completion of the surgical procedures.
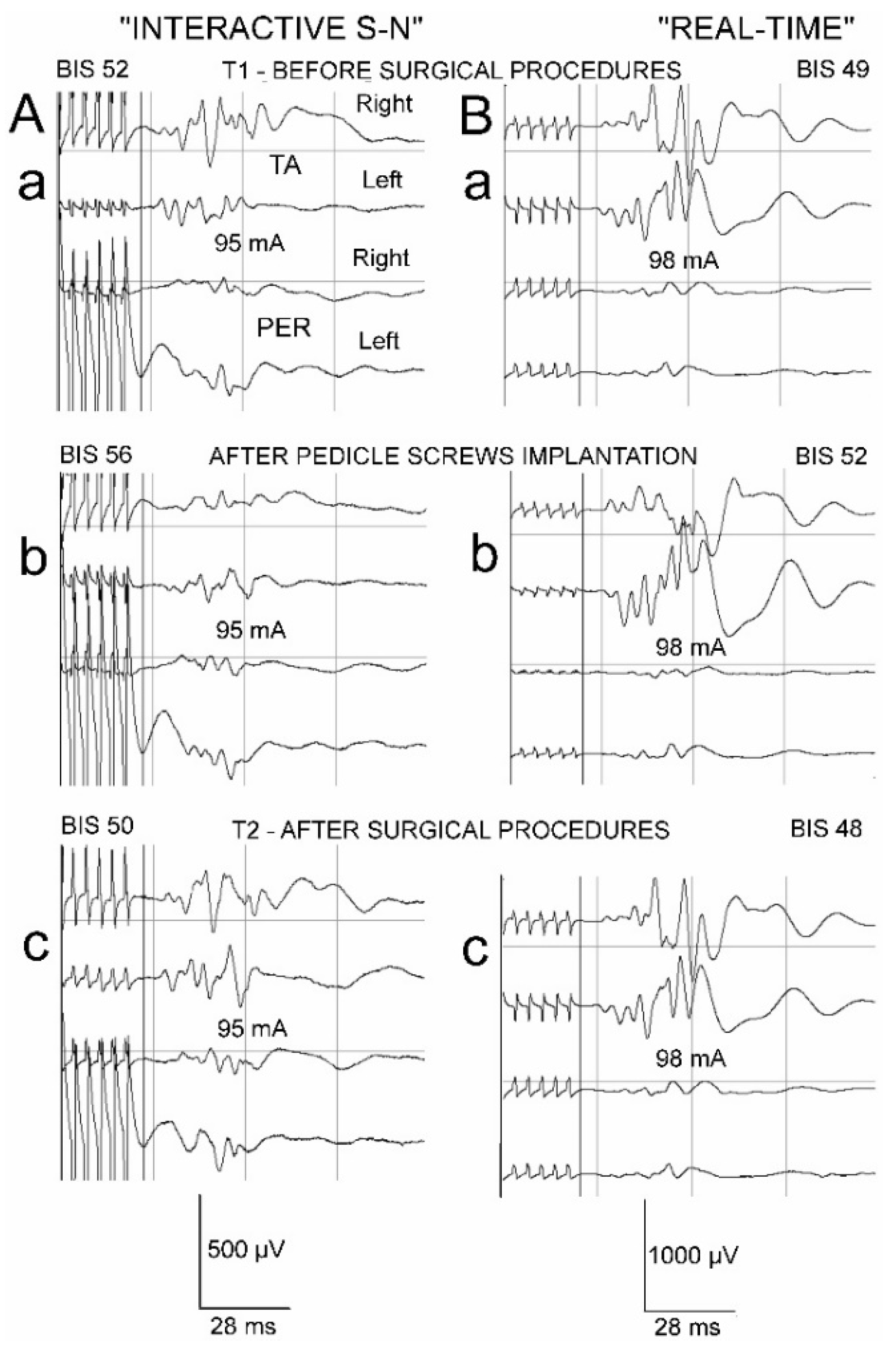

Table 1.
Demographic, anthropometric, and scoliosis characteristics of the patients from two studied groups and healthy volunteers from the control group. Minimum, maximum, mean values, and standard deviations are presented. p < 0.05 determines significant statistical differences.
Table 1.
Demographic, anthropometric, and scoliosis characteristics of the patients from two studied groups and healthy volunteers from the control group. Minimum, maximum, mean values, and standard deviations are presented. p < 0.05 determines significant statistical differences.
| Variable Group of subjects |
Age (years) | Height (cm) |
Weight (kg) | BMI | Scoliosis Type [41] |
Cobb’s angle [42] (Preoperatively) |
|---|---|---|---|---|---|---|
| “Interactive S-N” neuromonitoring group N = 60 ♀ |
8 – 17 14.2 ± 1.6 |
135 – 181 164.4 ± 2.0 |
30 – 84 54.5 ± 2.9 |
17.6 – 29.9 23.1 ± 4.0 |
Lenke 1 = 10 Lenke 2 = 48 Lenke 3 = 2 |
Primary 41 – 86 57.4 ± 6.6 Secondary 24 – 50 37.1 ± 3.3 |
| “Real-time” neuromonitoring group N = 60 ♀ |
9 – 18 14.7 ± 1.5 |
137 – 179 165.6 ± 2.5 |
29 – 83 53.1 ± 3.1 |
17.4 – 30.1 22.9 ± 3.9 |
Lenke 1 = 11 Lenke 2 = 46 Lenke 3 = 3 |
Primary 40 – 89 56.3 ± 7.1 Secondary 25 – 50 37.3 ± 3.9 |
| Healthy volunteers “Control” group N = 60 ♀ |
8 – 18 14.3 ± 1.5 |
134 – 183 166.1 ± 2.6 |
30 – 84 54.9 ± 5.3 |
17.4 – 29.8 22.8 ± 3.7 |
NA | NA |
|
p – value (difference) “Interactive S-N” vs. “Real-time” “Interactive S-N” vs. “Control” “Real-time” vs. “Control” |
0.223 NS 0.177 NS 0.082 NS |
0.182 NS 0.192 NS 0.091 NS |
0.171 NS 0.122 NS 0.079 NS |
0.183 NS 0.089 NS 0.119 NS |
0.062 NS | Primary angle 0.199 NS Secondary angle 0.328 NS |
Abbreviations: ♀ – female; “Interactive S-N group” – A group of scoliotic patients in whom mainly a verbal interaction between the surgeon and the neurophysiologist during intraoperative neuromonitoring was continuously kept; “Real-time group” – A group of scoliotic patients in whom the intraoperative neuromonitoring was mainly based on simultaneous evoked potential and camera recordings by neurophysiologist; NS – non-significant; NA – non-applicable.
Table 2.
Comparison of results from motor evoked potential recordings performed in two groups of 120 IS patients pre- (T0), intra- (T1 –before surgical procedures, T2 – after surgical procedures) and postoperatively (T3) and in 80 healthy volunteers (Control). Ranges, means and standard deviations are presented. p < 0.05 determines significant statistical differences marked in bold.
Table 2.
Comparison of results from motor evoked potential recordings performed in two groups of 120 IS patients pre- (T0), intra- (T1 –before surgical procedures, T2 – after surgical procedures) and postoperatively (T3) and in 80 healthy volunteers (Control). Ranges, means and standard deviations are presented. p < 0.05 determines significant statistical differences marked in bold.
| Test Parameter |
Side | TMS Control N=60 |
Scoliosis side |
TMS Patients Preoperative T0 |
Control vs. Patients T0 |
TES Patients Intraoperative T1 (Before IS correction) |
TMS Patients T0 vs. TES Patients T1 |
TES Patients Intraoperative T2 (After IS correction) |
TES Patients T1 vs. T2 |
TMS Patients Postoperative T3 |
TMS Patients T0 vs. T3 |
Control vs. Patients T3 |
|
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Min. – Max. Mean ± SD |
Min. – Max. Mean ± SD |
p - value | Min. – Max. Mean ± SD |
p - value | Min. – Max. Mean ± SD |
p - value | Min. – Max. Mean ± SD |
p - value | p - value | ||||
| MEP recorded from anterior tibial muscle - TA | |||||||||||||
| “INTERACTIVE S-N” NEUROMONITORING GROUP N=60 | Amplitude (µV) |
R | 1300 – 3600 1695.1 ± 92.8 |
Convex | 250 – 1400 412.1 ± 70.4 |
0.009 | 200 –1300 430.4 ±78.1 |
0.091 | 400 – 1850 688.2 ± 76.4 ↑ |
0.029 | 700 – 2400 977.1 ± 99.1 ↑ |
0.023 | 0.008 |
| L | 1000 – 3050 1611.9 ± 72.8 |
Concave | 200 – 1300 385.4 ± 49.8 |
0.009 | 150 –1050 369.9 ± 73.6 |
0.094 | 300 – 1650 511.1 ± 78.3 ↑ |
0.042 | 550 – 1900 855.3 ± 100.2 ↑ |
0.019 | 0.008 | ||
| p - value | R vs. L |
0.119 | Convex vs. Concave |
0.048 | NA | 0.047 | NA | 0.045 | NA | 0.048 | NA | NA | |
| Latency (ms) | R | 24.3 – 31.6 28.8 ± 1.4 |
Convex | 27.2 – 36.1 31.9 ± 3.1 |
0.036 | 28.9 – 38.1 31.7 ± 1.5 |
0.121 | 28.0 – 38.3 31.4 ± 1.4 |
0.299 | 28.5 – 39.1 30. 9 ± 2.0 |
0.058 | 0.031 | |
| L | 25.1 – 32.0 29.6 ± 1.5 |
Concave | 28.8 – 39.1 32.7 ± 2.6 |
0.037 | 29.4 – 39.6 32.9 ± 2.0 |
0.111 | 30.3 – 40.2 33.2 ± 2.6 |
0.298 | 30.5 – 40.0 33.2 ± 2.1 |
0.060 | 0.041 | ||
| p - value | R vs. L |
0.205 | Convex vs. Concave |
0.077 | NA | 0.052 | NA | 0.067 | NA | 0.058 | NA | NA | |
| MEP recorded from peroneal nerve - PER | |||||||||||||
| Amplitude (µV) |
R | 450 – 2050 565.7 ± 55.4 |
Convex | 100 – 800 213.2 ± 46.1 |
0.028 | 100 – 700 218.1 ±44.3 |
0.114 | 200 – 800 ↑ 388.3 ± 39.8 ↑ |
0.043 | 200 – 800 ↑ 443.6 ± 33.8 ↑ |
0.034 | 0.044 | |
| L | 400 – 2000 525.7 ± 58.2 |
Concave | 50 – 700 186.2 ± 36.3 |
0.029 | 50 – 600 187.2 ± 40.1 |
0.009 | 300 – 750 362.3 ± 38.1 |
0.041 | 350 – 800 425.1 ± 41.4 |
0.031 | 0.045 | ||
| p - value | R vs. L |
0.112 | Convex vs. Concave |
0.102 | NA | 0.052 | NA | 0.073 | NA | 0.072 | NA | NA | |
| Latency (ms) | R | 22.1 – 28.9 25.9 ± 1.6 |
Convex | 23.0 – 31.4 27.6 ± 3.4 |
0.042 | 22.9 – 31.1 27.8 ± 3.5 |
0.075 | 22.7 – 31.0 27.8 ± 3.3 |
0.321 | 22.5 – 31.3 27.6 ± 3.2 |
0.091 | 0.041 | |
| L | 22.9 – 30.0 26.3 ± 1.6 |
Concave | 23.6 – 33.5 29.2 ± 3.6 |
0.039 | 23.7 – 34.0 29.1 ± 3.3 |
0.111 | 23.4 – 32.1 28.4 ± 3.6 |
0.114 | 22.9 – 32.0 28.0 ± 3.1 |
0.061 | 0.046 | ||
| p - value | R vs. L |
0.095 | Convex vs. Concave |
0.048 | NA | 0.049 | NA | 0.051 | NA | 0.073 | NA | NA | |
| TA vs. PER cumulative (R+L) MEP amplitude difference (µV) |
1108.2 ↓ | 189.8 ↓ | 197.5 ↓ | 224.3 ↓ | 481.8 ↓ | ||||||||
| % of difference | 67.1 ↓ | 47.8 ↓ | 49.3 ↓ | 37.4 ↓ | 52.5 ↓ | ||||||||
| p - value | 0.007 | 0.009 | 0.009 | 0.022 | 0.008 | ||||||||
| TA vs. PER cumulative (R+L) MEP latency difference (µV) |
3.1 ↓ | 3.9 ↓ | 3.9 ↓ | 4.3 ↓ | 4.2 ↓ | ||||||||
| % of difference | 10.6 ↓ | 12.0 ↓ | 12.0 ↓ | 13.3 ↓ | 13.1 ↓ | ||||||||
| p - value | 0.043 | 0.032 | 0.032 | 0.031 | 0.030 | ||||||||
| MEP recorded from anterior tibial muscle - TA | |||||||||||||
| “REAL-TIME” NEUROMONITORING GROUP N=60 | Amplitude (µV) |
R | 1300 – 3600 1695.1 ± 92.8 |
Convex | 300 – 1350 410.9 ± 62.1 |
0.008 | 250 –1400 425.7 ±71.2 |
0.084 | 450 – 1900 696.9 ± 69.3 ↑ |
0.027 | 750 – 2300 975.4 ± 65.3 ↑ |
0.021 | 0.018 |
| L | 1000 – 3050 1611.9 ± 72.8 |
Concave | 150 – 1250 380.1 ± 45.4 |
0.009 | 200 –1200 375.8 ± 73.6 |
0.085 | 350 – 1950 550.7 ± 59.8 ↑ |
0.038 | 600 – 1850 852.9 ± 88.1 ↑ |
0.018 | 0.019 | ||
| p - value | R vs. L |
0.119 | Convex vs. Concave |
0.047 | NA | 0.046 | NA | 0.040 | NA | 0.047 | NA | NA | |
| Latency (ms) | R | 24.3 – 31.6 28.8 ± 1.4 |
Convex | 27.7 – 37.3 31.6 ± 3.5 |
0.032 | 28.8– 38.6 31.8 ± 2.8 |
0.185 | 28.1 – 38.6 31.3 ± 2.5 |
0.119 | 28.2 – 39.0 31. 1 ± 2.5 |
0.059 | 0.034 | |
| L | 25.1 – 32.0 29.6 ± 1.5 |
Concave | 28.7 – 38.9 32.8 ± 3.1 |
0.034 | 29.6 – 39.2 32.8 ± 3.2 |
0.206 | 30.4 – 41.9 33.4 ± 2.9 |
0.194 | 30.1 – 39.8 31.8 ± 2.8 |
0.061 | 0.038 | ||
| p - value | R vs. L |
0.205 | Convex vs. Concave |
0.081 | NA | 0.055 | NA | 0.061 | NA | 0.251 | NA | NA | |
| MEP recorded from peroneal nerve - PER | |||||||||||||
| Amplitude (µV) |
R | 450 – 2050 565.7 ± 55.4 |
Convex | 150 – 900 218.4 ± 45.8 |
0.031 | 150 – 750 215.9 ±48.2 |
0.123 | 300 – 900 390.8 ± 35.2 ↑ |
0.040 | 250 – 900 448.9 ± 36.1 ↑ |
0.029 | 0.046 | |
| L | 400 – 2000 525.7 ± 58.2 |
Concave | 100 – 800 189.8 ± 48.1 |
0.030 | 100 – 650 185.9 ± 38.3 |
0.008 | 300 – 800 368.1 ± 38.9 ↑ |
0.043 | 300 – 805 446.1 ± 38.1 ↑ |
0.027 | 0.048 | ||
| p - value | R vs. L |
0.212 | Convex vs. Concave |
0.108 | NA | 0.055 | NA | 0.065 | NA | 0.080 | NA | NA | |
| Latency (ms) | R | 22.1 – 28.9 25.9 ± 1.6 |
Convex | 23.4 – 31.8 27.2 ± 2.8 |
0.043 | 23.2 – 31.4 27.8 ± 3.5 |
0.074 | 22.6 – 31.4 27.8 ± 3.3 |
0.325 | 22.8 – 31.1 27.5 ± 2.8 |
0.082 | 0.040 | |
| L | 22.9 – 30.0 26.3 ± 1.6 |
Concave | 23.8 – 33.3 29.1 ± 3.1 |
0.041 | 23.5 – 33.9 29.0 ± 3.1 |
0.129 | 23.5 – 32.0 28.1 ± 3.1 |
0.121 | 22.7 – 32.1 28.0 ± 3.2 |
0.073 | 0.044 | ||
| p - value | R vs. L |
0.224 | Convex vs. Concave |
0.047 | NA | 0.047 | NA | 0.055 | NA | 0.081 | NA | NA | |
| TA vs. PER cumulative (R+L) MEP amplitude difference (µV) |
1108.2 ↓ | 191.2 ↓ | 199.8 ↓ | 244.4 ↓ | 466.6 ↓ | ||||||||
| % of difference | 67.1 ↓ | 48.3 ↓ | 49.8 ↓ | 39.1 ↓ | 51.0 ↓ | ||||||||
| p - value | 0.007 | 0.009 | 0.009 | 0.023 | 0.008 | ||||||||
| TA vs. PER cumulative (R+L) MEP latency difference (µV) |
3.1 ↓ | 4.1 ↓ | 3.9 ↓ | 4.4 ↓ | 3.7 ↓ | ||||||||
| % of difference | 10.6 ↓ | 12.7 ↓ | 12.0 ↓ | 13.6 ↓ | 11.7 ↓ | ||||||||
| p - value | 0.043 | 0.033 | 0.032 | 0.028 | 0.048 | ||||||||
Abbreviations: TMS - transcranial magnetic stimulation; TES – transcranial electrical stimulation; MEP – motor evoked potential; TA – tibialis anterior muscle; PER – peroneal nerve; NA – non-applicable; Arrows, ↓ indicate a decrease in the parameter when the cumulative values are compared, and ↑ increase when the MEP amplitude was recorded in T2 and T3.
Table 3.
Data on variables and the events associated with intraoperatively recorded MEP parameter fluctuations in 120 scoliotic patients belonging to the studied two groups for comparison. Ranges, means and standard deviations are presented as well as the number of incidences. p < 0.05 determines significant statistical differences marked in bold.
Table 3.
Data on variables and the events associated with intraoperatively recorded MEP parameter fluctuations in 120 scoliotic patients belonging to the studied two groups for comparison. Ranges, means and standard deviations are presented as well as the number of incidences. p < 0.05 determines significant statistical differences marked in bold.
| Variable Neurophysiological event Surgical event |
“Interactive S-N neuromonitoring” group N=60 |
“Real-time neuromonitoring” group N=60 |
Difference p |
|---|---|---|---|
| BIS level | 40-65 (52.4±4.1) | 40-60 (51.3±3.9) | 0.236 |
| TES strength (mA) during maximal amplitude MEP recordings |
80-124 (99.2±8.1) | 80-130 (97.3±7.3) | 0.194 |
| Number of neurophysiologist’s warnings associated with MEP parameters fluctuations: -During surgery field preparation (including effects of transient “warming” during cauterization and shocks caused by releasing the vertebral joints) -During pedicle screws implantation -During corrective rods implantation -During distraction, derotation, compression |
9/60 12/60 10/60 8/60 |
7/60 8/60 6/60 4/60 |
0.07 0.04 0.04 0.03 |
| Anaesthesia related events: -TA recorded bilaterally MEP -PER recorded bilaterally MEP |
5/60 1/60 |
4/60 2/60 |
0.135 0.163 |
| False alarms caused by technical malfunctions | 1/60 | 2/60 | 0.165 |
| False alarms caused by movement-related artifacts following TES |
1/60 | 0/60 | 0.239 |
| Averaged time of surgery | 5.5 | 4.5 | 0.04 |
| Number of bidirectional communications: -S vs. N -N vs. S |
587 396 |
292 191 |
0.008 0.008 |
Abbreviations: TES – transcranial electrical stimulation; “Interactive S-N group” – A group of scoliotic patients in whom mainly a verbal interaction between the surgeon and the neurophysiologist during intraoperative neuromonitoring was continuously kept; “Real-time group” – A group of scoliotic patients in whom the intraoperative neuromonitoring was mainly based on simultaneous evoked potential and camera recordings by neurophysiologist; TA – tibialis anterior muscle; PER – peroneal nerve; S – surgeon; N – neurophysiologist.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



