Submitted:
22 January 2024
Posted:
23 January 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: Infections of Coronavirus Disease-2019 (COVID-19) can cause long-term effects known as long COVID. This pilot study aimed to evaluate the feasibility of a clinical study as well as the efficacy and safety of traditional East Asian herbal medicines in alleviating fatigue and cognitive dysfunction “brain fog” in patients with long COVID. Methods: This prospective pilot study investigated the use of three types of herbal medicines, Bojungikki-tang (BIT), Kyungok-go (KOG), and Cheonwangbosim-dan (CBD), for a 12-week period as potential treatments for fatigue and cognitive dysfunction in patients with long COVID. Forty-five patients with long COVID were recruited, and one of three drugs was given based on the patient’s symptoms and pattern identification. The effect of herbal medications on fatigue and cognitive function outcomes was assessed over a 36-week period, with patient adherence closely monitored. Results: After 12 weeks of herbal drug administration, fatigue symptoms improved significantly across all groups, with treatment success rates of 80%, 53.33%, and 46.67% in the BIT, KOG, and CBD groups, respectively. However, “brain fog” symptoms showed less improvement, with treatment success rates of 40%, 46.67%, and 13.33% in the BIT, KOG, and CBD groups, respectively. All adverse events reported were mild and unrelated to the medication. The study design was found to be feasible with high medication adherence. Conclusions: This study demonstrated the feasibility of conducting a clinical trial with three herbal medicines to treat long COVID symptoms like fatigue and “brain fog.”
Keywords:
Long COVID
; Post-acute sequelae of SARS-CoV-2 infection
; herbal medicine
; fatigue
; brain fog
; pilot clinical trial
1. Introduction
Although a significant number of patients have reported persistent symptoms following acute coronavirus disease 2019 (COVID-19), a global consensus on terminologies and definitions has yet to be established. The definition of long COVID, also known as chronic or postacute sequelae of SARS-CoV-2 infection (PASC), has, is not well defined, and different countries and institutions use different terms or definitions. According to the World Health Organization, post-COVID-19 conditions are defined as symptoms that usually occur within three months of the onset of COVID-19 symptoms, persist for at least two months, and are not explained by other alternative diagnoses [1]. In South Korea, chronic COVID-19 syndrome (long COVID) is defined as the persistence of one or more symptoms or signs that cannot be explained by another disease after 12 weeks of COVID-19 diagnosis [2]. These symptoms are diverse and can affect various systems, commonly including fatigue, shortness of breath, cough, chest pain, joint pain, muscle aches, “brain fog” (cognitive difficulties), headache, heart palpitations, sleep disturbances, depression, anxiety, and loss of taste or smell. A meta-analysis of 41 studies found that the global combined prevalence of PASC was 43%, with fatigue, memory problems, and dyspnea being the most common symptoms [3]. Similarly, other studies have found that fatigue and cognitive impairment are the most common and frequently reported PASC symptoms [4,5]. In addition, unlike other common symptoms of PASC, such as dyspnea and depression, there are currently no established and effective treatments for these conditions [6]. It is important to note that the prevalence of long COVID can vary based on factors such as the definition of long COVID used in the study, the population being studied, and the follow-up duration.
Several risk factors appear to be associated with PASC, including female gender, ethnic minority status, socioeconomic deprivation, smoking, obesity, and comorbidities [7]. Data from the United States, 153,543 adults, including 19,985 with long COVID, revealed that 14% of adults aged 18–84 (35.11 million) and 15.5% of adults at the working age of 18–64 (30.65 million) had long COVID by November 2022 [8]. In addition, approximately 27.7 million adults and 24.2 million adults at the working age may experience adverse socioeconomic and mental health outcomes due to long COVID. Furthermore, the estimated annual earnings loss among working-age adults was $175 billion. These findings highlight the significant public health and economic impact of long COVID, underscoring the need for further investigation and intervention [8].
Despite the significant impacts of long COVID, there is currently a lack of treatment methods supported by concrete evidence. There are several approaches available to manage symptoms and improve overall well-being in individuals with long COVID. For fatigue in patients with long COVID-19, treatment options include medications, alternative medicine, cognitive behavioral therapy, and exercise therapy. However, studies evaluating the effectiveness of these interventions are limited and lack high-quality evidence [9]. To date, the treatment strategies for various post-COVID-19 syndromes are inadequate. However, traditional medicine has been identified as a potential solution due to its ability to relieve symptoms, improve organic injuries, and affect immune function [10]. According to a previous study, a significant number of patients with post-COVID-19 syndrome who were identified with particular syndromes, such as Lung and Spleen Qi Deficiency and Qi and Yin Deficiency, in traditional East Asian medicine showed improvement in symptoms after treatment [11]. Furthermore, randomized controlled trials have suggested that traditional medicine can improve fatigue in post-COVID-19 patients [12]. However, these pieces of evidence appear to be insufficient for complementary and alternative medicine (CAM). There is a lack of published studies regarding the effectiveness and safety of CAM interventions for long COVID [13], highlighting the need for more clinical studies in this area.
According to reports, Korean medicine (KM) doctors consider Qi Deficiency as a major cause of chronic fatigue syndrome and prioritize prescribing Bojungikki-tang (BIT; Bu-Zhong-Yi-Qi-Tang in Chinese or Hochu-ekki-to in Japanese) as a treatment [14]. In Japan, Bojungikgi-tang is also frequently used to treat fatigue associated with long COVID [15]. During the pandemic period, the most commonly prescribed herbal medicine in South Korea for fatigue, weakness, and dry cough was Kyungok-go (KOG) [16]. Furthermore, Cheonwangbosim-dan (CBD) has the potential to improve or treat physical and mental illnesses, such as cognitive dysfunction, neurosis, insomnia, and cardiac malfunction-induced disease [17]. Therefore, these herbal medicines are considered potentially useful in alleviating long COVID symptoms. It is necessary to establish clinical evidence for these herbal medicines, not only to develop traditional medical treatment strategies for long COVID but also to provide them to the growing number of patients.
This was a phase 2 preliminary clinical trial that aimed to evaluate the safety and efficacy of frequently used herbal medicines in patients experiencing fatigue or “brain fog” associated with long COVID. The research objectives were to assess the feasibility of the intervention and gather evidence for future large-scale studies. Our data demonstrate a new possibility of herbal medicines against long COVID symptoms.
2. Materials and methods
2.1. Trial design
This was a prospective pilot study conducted at Kyung Hee University Korean Medicine Hospital in Seoul, Republic of Korea, with the aim of testing the feasibility and acceptability of using selected herbal medicines in patients experiencing fatigue or “brain fog” after COVID-19. This study was approved by the Institutional Review Board of Kyung Hee University KM Hospital (KOMCIRB 2020-12-002-001). The protocol of this study was published as a protocol paper [18] and registered at cris.nih.go.kr (KCT0006252) prior to the start of the clinical trial.
2.2. Participants
Patients with fatigue or cognitive symptoms were recruited for this study. Each patient was prescribed three KM herbal medications based on syndrome differentiation and symptom type. Since this clinical trial did not include a control group, randomization, allocation concealment, and blinding were not implemented. Patients had monthly visits for a 12-week medication period, and their symptoms and blood biochemistry were assessed up to 36 weeks after participation. The enrollment, intervention, and assessment schedules are summarized in Table 1.
This study included individuals over the age of 19 who had recovered from COVID-19, reported persistent fatigue or cognitive dysfunction for more than four weeks after their diagnosis but not before, achieved a total score of more than 76 points on the Checklist Individual Strength (CIS), had no overall cognitive function issues, and could provide written informed consent. However, individuals with conditions that could potentially cause fatigue or “brain fog” or interfere with drug intake or absorption as well as those with other allergic, hepatic, or nephrotic diseases, were excluded from the study. All participants provided written informed consent prior to participating in this study. All of the entry criteria are listed in Table S1.
2.3. Intervention
The KM syndrome differentiation was conducted by a Korean Medicine doctor specializing in internal medicine specialist, with over 10 years of clinical experience. Patients were classified into either the fatigue or cognitive dysfunction group based on the primary symptoms observed after COVID-19. Subsequently, they were assigned to the appropriate herbal medicine intervention group according to their specific sub-syndrome differentiation pattern. The criteria for syndrome differentiation can be found in Table 2. Based on syndrome differentiation, three different herbal medications were prescribed to each patient for 12 weeks. Among patients with fatigue, the pattern/syndrome of Lung-Spleen Qi Deficiency group received BIT (Kracie Bojungikgitang Extract Fine Granule, Kolmar Pharma, Korea) as one sachet (3.75 g) twice a day before or in between meals. In addition, the syndrome of Dual Deficiency of Qi and Yin group received KOG, KBPharm, Korea) as one sachet (20 g) twice a day in the morning and evening before or in between meals. Furthermore, the cognitive dysfunction group received CBD (Soonsimhwan, Hanpoong Pharm, Korea) as one sachet (one dose) once a day in between meals. All medications and their respective dosages were approved by the Ministry of Food and Drug Safety (MFDS). All medication ingredients are detailed in Table 3.
2.4. Outcome measures
The primary endpoint of this study was to determine the treatment success rate after 12 weeks of herbal medication for fatigue and cognitive dysfunction in patients who had recovered from COVID-19. The fatigue or cognitive dysfunction was assessed before and 13 weeks after the administration of herbal medicines using a Visual Analog Scale (VAS) score ranging from 0 to 100. A change in VAS score between before and after treatment greater than 15 points was defined as treatment success. The secondary endpoints included evaluating medication adherence and utilizing CIS [19], Chalder Fatigue Scale and Subscale [20], EQ-5D-5L for health-related quality of life [21], Pittsburgh Sleep Quality Index-K [22], Korean–Montreal Cognitive Assessment scale for cognitive function [23], Cognitive Failure Questionnaire for cognitive function [24], Beck’s Depression Inventory [25], Digit Span Test in the Korean–Wechsler Adult Intelligence Scale for assessing changes in cognitive dysfunction [26], and Korean–Boston Naming Test-15 for measuring language proficiency in cognitive impairments [27]. During the 12-week treatment period, patients had monthly visits. Following that, they had follow-up visits every 12 weeks over a total period of 24 weeks for outcome assessment.
To evaluate the study’s feasibility, the patient recruitment rate was calculated as the ratio of the number of recruited patients during the study period to the planned number of study patients (45 and 15 patients per intervention group, respectively). Dropout reasons were documented, and the dropout rate was calculated and compared for all study patients as well as for each intervention group.
The safety of the drugs was evaluated by monitoring the incidence of adverse events (AEs). AEs referred to all harmful and unintended symptoms of signs, including abnormal laboratory test results in patients received herbal medicine, without necessarily having a causal relationship. At Weeks 0 and 13, laboratory investigations, including blood chemistry, were performed, and an electrocardiogram was assessed. Laboratory tests determined the levels of red blood cells, hemoglobin, hematocrit, platelets, white blood cells, fasting blood sugar, BUN, creatinine, AST, ALT, and blood electrolytes (Na, K, Cl). AEs were assessed at all in-person visits occurring at 1, 5, 9, 13, 25, and 37 weeks. Detailed research methodology can be found in the previously published protocol paper [18].
2.5. Statistical analysis
To assess the feasibility of the study design, the subject recruitment rate, dropout rate, and dropout reasons were analyzed. Since this trial was conducted as a pilot study, the sample size was not calculated beforehand. The dropout rate was calculated for all participants and for each herbal medication group, and the dropout reasons were also assessed. For continuous variables used to assess the potential clinical effectiveness of the herbal medications, descriptive statistics such as standard deviation, median, minimum, and maximum values were presented for each time point. Statistical analysis was conducted on an intention-to-treat basis, and the last observation carried forward analysis was employed to handle missing data while evaluating effectiveness. An analysis of covariance (ANCOVA) was used to compare the different herbal medication groups (p < 0.05). In cases where the basic assumptions of ANCOVA, such as normality and equal variance of data, were violated, the Kruskal–Wallis test was used. The statistical analysis was conducted using the R software (R 4.1.2, The R Foundation, www.r-project.org, accessed on August 9, 2022). A full analysis set was used to analyze variables for effectiveness evaluation, while data for safety evaluation were analyzed using the safety set. All statistical tests, unless otherwise specified, were two-sided with a significance level of 5%.
3. Results
3.1. Participants
3.2. Baseline characteristics
In this study, fatigue and “brain fog” symptoms were assessed in patients with long COVID. Herbal drugs for fatigue symptoms (BIT and KOG) and “brain fog” (KOG) were prescribed to patients based on their symptoms and pattern identification diagnosis. Patients in the CBD group were older (average age: 51.33 years) than those in the fatigue herbal drug groups (BIT and KOG). The average duration of symptoms was 89.47 days in the BIT group, 114.8 days in the KOG group, and 119 days in the CBD group. The body mass index, educational level, and occupational status were comparable among the groups. When the National Early Warning Score (NEWS) was considered, the KOG and CBD groups showed a more severe status during the acute COVID-19, with fatigue symptoms being more severe in the BIT and KOG groups and “brain fog” symptoms being more severe in the CBD group (Table 4).
3.3. Feasibility assessment
Between August 2021 and July 2022, the targeted recruitment of 45 participants was successfully completed, achieving a 100% recruitment and enrollment rate. Among the included participants, 14 (31%) dropped out due to various reasons. A significant number of these dropouts were attributed to unexpected diseases, with six individuals experiencing a reinfection of COVID-19. However, no withdrawals were linked to AEs from the administered drug. In the BIT group, seven participants dropped out due to unexpected diseases (n = 3), pregnancy (n = 1), and withdrawal of consent (n = 3). In the KOG group, two dropped out due to unexpected diseases. In the CBD group, five dropped out due to unexpected diseases (n = 2) and withdrawal (n = 3) (Table 4 and Figure 1). Medication adherence among participants who completed 12 weeks of drug administration was high (92.27%, 96.26%, and 85.66% in the BIT, KOG, and CBD groups, respectively, Table 5). Considering these factors as well as participant recruitment, intervention administration, and long-term follow-up, the study design can be considered feasible.
3.4. Assessments of fatigue and “brain fog” symptoms
After 12 weeks of herbal drug administration, fatigue symptoms improved significantly in each group, with treatment success rates of 80%, 53.33%, and 46.67% in the BIT, KOG, and CBD groups, respectively. However, treatment success rates for “brain fog” symptoms were comparatively low (40%, 46.67%, and 13.33% in the BIT, KOG, and CBD groups, respectively). In addition, CIS showed significant improvement in each group at 13 weeks (mean difference: −29.53, 95% confidence interval [CI]: −40.96 to −18.2 in the BIT group, −31.47, 95% CI: −43.47 to −19.46 in the KOG group, and −23.4, 95% CI: −34.79 to −12.01 in the CBD group), 25 weeks, and 37 weeks, with no significant difference between groups after treatments. Similarly, the VAS score for fatigue showed significant improvement at 13 weeks (mean difference: −32.53, 95% CI: −46.07 to −19.00 in the BIT group, −30.13, 95% CI: −47.11 to −13.16 in the KOG group, and −16.73, 95% CI: −27.48 to −5.98 in the CBD group), 25 weeks, and 37 weeks in each group, with no significant difference between groups after treatments. In terms of the total, physical health, and mental health scores of ChFQ, significant improvement in each group was observed at 13 weeks (mean difference: −23.67, 95% CI: −35.09 to −12.24 in the BIT group, −21.27, 95% CI: −32.91 to −9.62 in the KOG group, and −10.93, 95% CI: −19.93 to −1.93 in the CBD group for the total score; −17.27, 95% CI: −25.58 to −9.15 in the BIT group, −14.2, 95% CI: −21.41 to −6.99 in the KOG group, and −6.27, 95% CI: −11.99 to −0.54 in the CBD group for the physical health score; −6.4, 95% CI: −10.98 to −1.82 in the BIT group, −7.07, 95% CI: −11.98 to −2.16 in the KOG group, and −4.67, 95% CI: −8.3 to −1.03 in the CBD group for the mental health score), 25 weeks, and 37 weeks, with no significant difference between groups (Table 5).
In terms of “brain fog” symptoms, no significant improvements were observed in each group. The VAS score for “brain fog” did not show significant improvement at 13 weeks (mean difference: −6.27, 95% CI: −26.71 to 14.17 in the BIT group, −5.4, 95% CI: −27.98, 17.18 in the KOG group, and 1.4, 95% CI: −10.8 to 13.6 in the CBD group), 25 weeks, or 37 weeks, with no significant difference between groups. However, the Korean–Montreal Cognitive Assessment score showed significant improvement in the KOG group at 13 weeks (mean difference: 1.80, 95% CI: 0.7 to 2.83), 25 weeks (mean difference: 1.87, 95% CI: 1.03 to 2.70), and 37 weeks (mean difference: 1.47, 95% CI: 0.53 to 2.40). In addition, the Cognitive Failure Questionnaire score showed significant improvement in the BIT and KOG groups at 37 weeks (mean difference: −4.40, 95% CI: −7.57 to −1.23 in the BIT group, −3.93, 95% CI: −11.57 to 3.70 in the KOG group, and −11.67, 95% CI: −21.07 to −2.26 in the CBD group), with no significant difference between groups. Furthermore, there was no significant improvement in the BIT and CBD groups at each follow-up period. Scores for the DF-forward test and DF-backward test did not show significant improvements at 13 weeks (mean difference: 0.27, 95% CI: −0.27 to 0.8 in the BIT group, 0, 95% CI: −0.47 to 0.47 in the KOG group, and −0.07, 95% CI: −0.46 to 0.42 in the CBD group for the DF-forward score and 1.4, 95% CI: 0.4 to 2.4 in the BIT group, 0.4, 95% CI: −0.26 to 1.06 in the KOG group, and 0.8, 95% CI: −0.21 to 1.81 in the CBD group for the DF-backward score), 25 weeks, or 37 weeks. Furthermore, the Korean–Boston Naming Test–15 score did not show significant improvement at 13 weeks (mean difference: 0.13, 95% CI: −0.06 to 0.33 in the BIT group, 0.13, 95% CI: −0.06 to 0.33 in the KOG group, and 0.33, 95% CI: −0.21 to 0.87 in the CBD group), 25 weeks, or 37 weeks (Table 5).
3.5. Other outcome and safety assessments
The EQ-5D did not show a significant difference between groups at 13 and 37 weeks, but there was a significant difference at 25 weeks (mean difference: 0.06, 95% CI: 0.02 to 0.11 in the BIT group, −0.01, 95% CI: −0.05 to 0.03 in the KOG group, and 0.03, 95% CI: −0.06 to 0.11 in the CBD group). In addition, the Pittsburgh Sleep Quality Index-K score showed significant improvement in the KOG group at 13 weeks (mean difference: −2.71, 95% CI: −3.76 to −1.67), 25 weeks (−2.08, 95% CI: −3.28 to −0.89), and 37 weeks (−2.82, 95% CI: −3.94 to −1.70), with no significant improvements in the BIT and KOG groups. Furthermore, the Beck’s Depression Inventory score showed significant improvement in the BIT and KOG groups at 13 weeks (mean difference: −3.80, 95% CI: −6.86 to −0.74 in the BIT group, −4.73, 95% CI: −6.87 to −2.59 in the KOG group, and −5.53, 95% CI: −11.21 to 0.14 in the CBD group), 25 weeks, and 37 weeks (Table 5).
Among the 45 participants, 10 (22.22%) reported AEs, with no significant differences in the incidence rates of AEs among groups (p = 0.2805). All AEs were mild, and none were found to be causally related to the medication. Furthermore, there were no significant differences among groups in terms of the proportion of normal laboratory test results after treatment termination (Table 6).
4. Discussion
Through this pilot study, we found that the research design and intervention for this study were feasible. Although a considerable number of participants dropped out during the follow-up period due to the COVID-19 pandemic, there were no AEs directly related to the intervention, and adherence to the medication was high. Fatigue symptoms improved significantly in all groups, regardless of the type of prescription administered. However, “brain fog” symptoms did not improve significantly, even in the CBD group where this symptom was predominant.
In this study, three interventions were selected as treatments for fatigue and “brain fog” symptoms that may occur after COVID-19. BIT had been widely used as a prescription to treat various symptoms of impaired gastric function caused by dietary irregularities or overexertion. It has been approved by the Korean regulatory agency (Ministry of Food and Drug Safety, MFDS) for weakness, fatigue, lethargy, post-disease debility, poor appetite, night sweating, and vulnerability to fatigue due to a lack of vitality and sluggish gastrointestinal movement. It is composed of Ginseng Radix, Atractylodis Rhizoma Alba, Astragali Radix, Angelicae Gigantis Radix, Zizyphi Fructus, Bupleuri Radix, Citri Unshius Pericarpium, Glycyrrhizae Radix et Rhizoma, Cimicifugae Rhizoma, and Zingiberis Rhizoma Recens. It has been to have many clinical effects, and the therapeutic mechanism may be related to immunological, neuropsychiatric, anti-inflammatory, and musculoskeletal regulation [28]. It has been suggested to be effective in alleviating chronic fatigue-related general symptoms [29]. In addition, it can improve the quality of life, fatigue, and immunological status of elderly patients with weakness [30]. A previous case report reported the use of BIT for fatigue symptoms after COVID-19 [31]. KOG has been widely used to treat chronic diseases and is approved for conditions such as illness-related weakness, post-disease debility, weak constitution, physical fatigue, lethargy, and menopausal disorders, serving as a tonic and strengthener in Korea. It is composed of Rehmanniae Radix, Ginseng Radix, Wolfiporia Cocos, and Honey. Its therapeutic mechanism may be related to immune system activation [32], fatigue reduction [33,34], and cognitive function enhancement [35] as well as its anti-inflammatory effects [36,37,38]. CBD has been used for the treatment of anxiety, palpitation, and cognitive dysfunction. It has been approved in Korea for a variety of conditions, including insomnia, anxiety, restlessness, thirst, palpitations, shortness of breath, nervous debility, “brain fog,” and feverishness. Its therapeutic effect may be attributed to its antioxidant, anticancer, anti-inflammatory, and growth-promoting properties without significant toxicity or AEs [39]. In animal models, it has been found to inhibit learning and memory impairment, suggesting a potential effect on cognitive function [40]. CBD has also been shown to reduce inflammatory responses [41] and improve sleep quality in patients with primary insomnia [42]. Furthermore, it exhibits neuroprotective [43], vasorelaxant, hypotensive [44], and anti-Alzheimer’s disease [45,46] effects. It is commonly prescribed for alleviating the psychological and behavioral symptoms of dementia related to Alzheimer’s disease [47].
This study has some limitations. First, it was a pilot study with no control group. Therefore, concrete evidence regarding the efficacy and safety of these three herbal medications for long COVID could not be established. However, the feasibility of the study design was confirmed, and future large-scale clinical trials are required. Second, the outcomes assessed may be inappropriate for assessing fatigue and “brain fog” in patients with long COVID. The definition of long COVID is currently ambiguous, and there is no clear description of the underlying pathologic mechanism of its symptoms. While the diagnosis and treatment of long COVID-related fatigue may be approached by considering post-viral syndrome, approaching “brain fog” is more challenging due to its distinct presentation from cognitive impairments observed in dementia. One possible reason for the lack of significant improvement in cognitive function before and after drug treatment in patients with “brain fog” in this study is that the condition they are experiencing differs from cognitive decline in Alzheimer’s dementia. As a result, existing assessment tools designed for patients with dementia may not be able to adequately evaluate their cognitive function, which is a significant consideration in this context. Third, approximately 30% of study participants dropped out, demonstrating a high dropout rate. This may be attributed to the study’s long-term participation requirements, which included a 12-week intervention period followed by a six-month follow-up. Furthermore, the ongoing COVID-19 pandemic has led to a significant number of patient re-infections. When conducting clinical trials for the management of patients with long COVID, it is important to consider the potential for a high dropout rate in the study design.
5. Conclusions
The feasibility of this study, which included patients with long COVID experiencing fatigue and “brain fog” symptoms and given three different herbal medicines (BIT, KOG, and CBD) for 12 weeks based on their symptom patterns, has been demonstrated. Given the impact of long COVID and the scarcity of studies evaluating the effects of interventions on fatigue and “brain fog,” this study is deemed valuable. Future clinical studies with an appropriate control group and a sufficient sample size are needed to establish the evidence for herbal medicine in the management of long COVID-19.
Supplementary Materials
Supplementary material associated with this article can be found, in the online version, at the website of this paper posted on Preprints.org.
Author Contributions
Tae-Hun Kim: conceptualization, methodology, investigation, data curation, project administration, supervision, writing-original draft preparation, writing-review and editing; Jiwon Yoon: conceptualization, formal analysis, visualization, validation, writing-original draft preparation, writing-review and editing; Sanghyun Kim: conceptualization, visualization, validation, writing-review and editing; Byoung-Kab Kang: formal analysis, visualization, validation; Jung Won Kang: validation, writing-review and editing; Sunoh Kwon: conceptualization, methodology, resources, project administration, supervision, funding acquisition, writing-original draft preparation, writing-review and editing; All authors agree to be accountable for all aspects of work ensuring integrity and accuracy.
Funding
This study was supported by the Korea Institute of Oriental Medicine (KSN1823223).
Data Availability Statement
Data are included in this article and/or supp. materials.
Acknowledgements
The authors would like to express their gratitude to all nurses and participants of Kyung Hee University Korean Medicine Hospital who helped in conducting the present study.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the result.
Abbreviations
AEs, Adverse events; BDI, Beck’s Depression Inventory; BIT, Bojungikki-tang; CAM, Complementary and alternative medicine; CFQ, Cognitive Failure Questionnaire; CBD, Cheonwangbosim; ChFS, Chalder Fatigue Scale; CIS, Checklist Individual Strength; COVID, Coronavirus disease; COVID-19, coronavirus infectious disease 2019; K-BNT-15, Korean-Boston Naming Test-15; KM, Korean Medicine;MFDS, The Ministry of Food and Drug Safety; KOG, Kyungok-go, PSQI-K, the Korean version of Pittsburgh Sleep Quality Index; SARS-CoV-2, severe acute respiratory syndrome coronavirus-2; VAS, Visual Analog Scale; WAIS, Digit Span Test in Korean-Wechsler Adult Intelligence Scale
References
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kim, S.E.; Kim, T.; Yun, K.W.; Lee, S.H.; Lee, E.; Seo, J.-W.; Jung, Y.H.; Chong, Y.P. Preliminary Guidelines for the Clinical Evaluation and Management of Long COVID. Infect. Chemother. 2022, 54, 566–597. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post-Coronavirus Disease 2019 (COVID-19) Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022, 226, 1593–1607. [Google Scholar] [CrossRef]
- Marshall, M. The lasting misery of coronavirus long-haulers. Nature 2020, 585, 339–341. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re'Em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Ceban, F.; Ling, S.; Lui, L.M.; Lee, Y.; Gill, H.; Teopiz, K.M.; Rodrigues, N.B.; Subramaniapillai, M.; Di Vincenzo, J.D.; Cao, B.; et al. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: A systematic review and meta-analysis. Brain, Behav. Immun. 2021, 101, 93–135. [Google Scholar] [CrossRef]
- Subramanian, A.; Nirantharakumar, K.; Hughes, S.; Myles, P.; Williams, T.; Gokhale, K.M.; Taverner, T.; Chandan, J.S.; Brown, K.; Simms-Williams, N.; et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat. Med. 2022, 28, 1706–1714. [Google Scholar] [CrossRef]
- D. Kim, Who Gets Long COVID and Suffers its Mental Health and Socioeconomic Consequences in the United States? Preliminary Findings from a Large Nationwide Study, medRxiv (2023) 2023.2001. 2006.23284199.
- Fowler-Davis, S.; Platts, K.; Thelwell, M.; Woodward, A.; Harrop, D. A mixed-methods systematic review of post-viral fatigue interventions: Are there lessons for long Covid? PLOS ONE 2021, 16, e0259533. [Google Scholar] [CrossRef]
- Jiang, L.; An, X.; Duan, Y.; Lian, F.; Jin, D.; Zhang, Y.; Yang, C.; Zhang, Y.; Kang, X.; Sun, Y. The pathological mechanism of the COVID-19 convalescence and its treatment with traditional Chinese medicine. Front. Pharmacol. 2023, 13, 1054312. [Google Scholar] [CrossRef]
- L.L.-D. Zhong, Y.-P. Wong, C.-Y. Leung, et al., Effects of Chinese medicine for COVID-19 rehabilitation: a multicenter observational study, Chin Med 17(1) (2022) 99. [CrossRef]
- W. Pang, F. Yang, Y. Zhao, et al., Qingjin Yiqi granules for post-COVID-19 condition: A randomized clinical trial, Journal of Evidence-Based Medicine 15(1) (2022) 30-38. [CrossRef]
- Kim, T.-H.; Jeon, S.-R.; Kang, J.W.; Kwon, S. Complementary and Alternative Medicine for Long COVID: Scoping Review and Bibliometric Analysis. Evidence-Based Complement. Altern. Med. 2022, 2022, 1–7. [Google Scholar] [CrossRef]
- Kim, J.W.; Kim, H.J.; Jang, E.S.; Jung, H.J.; Hwang, M.W.; Nam, D.H. Survey on Pattern Identification and Treatment of Chronic Fatigue in Korea Medicine. J. Physiol. Pathol. Korean Med. 2018, 32, 126–133. [Google Scholar] [CrossRef]
- Tokumasu, K.; Ueda, K.; Honda, H.; Sunada, N.; Sakurada, Y.; Matsuda, Y.; Nakano, Y.; Hasegawa, T.; Otsuka, Y.; Obika, M.; et al. Application of Kampo Medicines for Treatment of General Fatigue Due to Long COVID. Medicina 2022, 58, 730. [Google Scholar] [CrossRef]
- Jang, S.; Kim, D.; Yi, E.; Choi, G.; Song, M.; Lee, E.-K. Telemedicine and the Use of Korean Medicine for Patients With COVID-19 in South Korea: Observational Study. Psychopharmacol. 2021, 7, e20236–200. [Google Scholar] [CrossRef]
- Jeon, W.-Y.; Jin, S.E.; Sohn, E.; Jo, K.; Ha, H.; Shin, H.-K.; Lee, M.-Y. Anti-inflammatory and anti-allergic effects of Cheonwangbosim-dan water extract: An in vitro and in vivo study. Heliyon 2023, 9, e16172. [Google Scholar] [CrossRef]
- K.H. Jegal, J. Yoon, S. Kim, et al. (2022). Herbal Medicines for Post-Acute Sequelae (Fatigue or Cognitive Dysfunction) of SARS-CoV-2 Infection: A Phase 2 Pilot Clinical Study Protocol. In 10. (MDPI), pp. 1839. [CrossRef]
- Vercoulen, J.H.M.M.; Swanink, C.M.A.; Fennis, J.F.M.; Galama, J.M.D.; van der Meer, J.W.M.; Bleijenberg, G. Dimensional assessment of chronic fatigue syndrome. J. Psychosom. Res. 1994, 38, 383–392. [Google Scholar] [CrossRef]
- Ha, H.; Jeong, D.; Hahm, B.-J.; Shim, E.-J. Cross-Cultural Validation of the Korean Version of the Chalder Fatigue Scale. Int. J. Behav. Med. 2017, 25, 351–361. [Google Scholar] [CrossRef]
- Kim, S.-H.; Ahn, J.; Ock, M.; Shin, S.; Park, J.; Luo, N.; Jo, M.-W. The EQ-5D-5L valuation study in Korea. Qual. Life Res. 2016, 25, 1845–1852. [Google Scholar] [CrossRef]
- Sohn, S.I.; Kim, D.H.; Lee, M.Y.; Cho, Y.W. The reliability and validity of the Korean version of the Pittsburgh Sleep Quality Index. Sleep Breath. 2011, 16, 803–812. [Google Scholar] [CrossRef]
- Y.I. Jung, E.H. Jeong, H. Lee, et al., Validation of MoCA-MMSE conversion scales in Korean patients with cognitive impairments, Dementia and Neurocognitive Disorders 17(4) (2018) 148-155. [CrossRef]
- Broadbent, D.E.; Cooper, P.F.; FitzGerald, P.; Parkes, K.R. The Cognitive Failures Questionnaire (CFQ) and its correlates. Br. J. Clin. Psychol. 1982, 21, 1–16. [Google Scholar] [CrossRef]
- A.T. Beck, C.H. Ward, M. Mendelson, et al., An inventory for measuring depression, Arch Gen Psychiatry 4(6) (1961) 561-571.
- H. Kim, and T. Park, Korean norm for the difference between digits forward and digits backward, The Korean Journal of Clinical Psychology 22(3) (2003) 599-613.
- Kim, H.; Kim, S.R. Development of Short Form of the Korean Version- the Boston Naming Test (K-BNT-15) Based on Item Response Theory. J. Korea Contents Assoc. 2013, 13, 321–327. [Google Scholar] [CrossRef]
- J.-H. Kim, J.-K. Lee, and H.-K. Shin, Analysis of studies on Bojungikgi-tang (Buzhongyiqi-tang) to establish the fundament for Evidence Based Medicine (EBM), Korean Journal of Oriental Medicine 17(2) (2011) 135-167.
- Nam, D. The Effectiveness of Bojungikgi-tang and its modifications on Chronic Fatigue Syndrome: A Systematic Review And Meta-analysis. J. Korean Med. 2020, 41, 93–106. [Google Scholar] [CrossRef]
- Satoh, N.; Sakai, S.; Kogure, T.; Tahara, E.; Origasa, H.; Shimada, Y.; Kohoda, K.; Okubo, T.; Terasawa, K. A randomized double blind placebo-controlled clinical trial of Hochuekkito, a traditional herbal medicine, in the treatment of elderly patients with weakness N of one and responder restricted design. Phytomedicine 2005, 12, 549–554. [Google Scholar] [CrossRef]
- Oka, T. A patient who recovered from post-COVID myalgic encephalomyelitis/chronic fatigue syndrome: a case report. Biopsychosoc. Med. 2023, 17, 1–7. [Google Scholar] [CrossRef]
- E.-S. Lee, B.-I. Seo, J.-U. Lee, et al., The immunological activities of kyungohkgo and prescription of modified kyungohkgo, The Korea Journal of Herbology 17(2) (2002) 95-95.
- Y. Kim, S. Jin, S. Kim, et al., Anti-fatigue effect of Kyung-ok-Ko, Korean Journal of Pharmacognosy 47(3) (2016) 258-263.
- D.-G. Kim, W.-H. Park, and Y.-Y. Cha, Effect of Kyungohkgo on aerobic capacity and anti-fatigue in high school soccer players, Journal of Physiology & Pathology in Korean Medicine 25(5) (2011) 934-944.
- B.Y. Shin, Y.H. B.Y. Shin, Y.H. Lee, D.-h. Kim, et al., Ameliorating effect of a herbal medicinal prescription, Kyung-Ok-Ko, on scopolamine-induced memory impairment in mice, Journal of Traditional Medicines 26(1) (2009) 35-43. [CrossRef]
- M. Park, J.-S. Kim, A. Lee, et al., Inhibition of Inflammation by Kyeongok-go with Black Ginseng in LPS-induced RAW 264.7 Macrophages, The Korea Journal of Herbology 32(3) (2017) 19-27. [CrossRef]
- K.-S. Lee, G.-H. Kim, H.-H. Kim, et al., Qualities and anti-inflammatory activity of Kyungokgos sold in local markets, Journal of the Korean Society of Food Science and Nutrition 42(3) (2013) 335-341. [CrossRef]
- Jang, M.; Lee, M.J.; Lee, J.M.; Bae, C.-S.; Kim, S.-H.; Ryu, J.H.; Cho, I.-H. Oriental Medicine Kyung-Ok-Ko Prevents and Alleviates Dehydroepiandrosterone-Induced Polycystic Ovarian Syndrome in Rats. PLOS ONE 2014, 9, e87623. [Google Scholar] [CrossRef]
- Kim, J.-W.; Geum, J.-H.K.; Ha, W.-B.K.; Woo, H.-J.K.; Han, Y.-H.K.; Park, S.-H.K.; Lee, J.-H.K. The efficacy, effectiveness, and safety of Kyung-ok-ko: A narrative review. Medicine 2022, 101, e31311. [Google Scholar] [CrossRef]
- I.-C. Jung, S.-R. Lee, and J.-Y. Lee, Effects of ChenWhangBosimDan (CWBD) on Inhibition of Impairment of Learning and Memory, and Acetylcholinesterase in Amnesia mice, Journal of Oriental Neuropsychiatry 13(2) (2002) 149-171.
- O.-S. Kim, Y. Kim, S.-R. Yoo, et al., Cheonwangbosimdan, a traditional herbal formula, inhibits inflammatory responses through inactivation of NF-κB and induction of heme oxygenase-1 in raw264. 7 murine macrophages, Int J Clin Exp Med 9(2) (2016) 1692-1699.
- Kim, M.-J.; Bose, S.; Shin, N.-R.; Park, S.; Kwon, O.; Song, E.-J.; Nam, Y.-D.; Koo, B.-S.; Nam, D.-H.; Lee, J.-H.; et al. The Herbal Formula CWBSD Improves Sleep Quality Dependent on Oral Microbial Type and Tongue Diagnostic Features in Insomnia. J. Pers. Med. 2021, 11, 325. [Google Scholar] [CrossRef]
- S.-H. Kim, J.-W. Kim, C.-H. Kang, et al., The effects of Chenwangbosim-dan and herbs on mouse neuroblastoma 2a cells damaged by hypoxia-reoxygenation, Journal of Oriental Neuropsychiatry 17(2) (2006) 15-36.
- Kim, B.; Jo, C.; Choi, H.-Y.; Lee, K. Vasorelaxant and Hypotensive Effects of Cheonwangbosimdan in SD and SHR Rats. Evidence-Based Complement. Altern. Med. 2018, 2018, 1–8. [Google Scholar] [CrossRef]
- K.-W. Choi, and I.-C. Jung, The effects of Chenwhangbosindan (CBD) hot water extract & ultra-fine powder on the Alzheimer's disease model, Journal of Oriental Neuropsychiatry 19(2) (2008) 77-93.
- I.-C. Jung, Effects of Chenwhangbosim-dan and Sungsimjihwang-tang on protecting microglia and inhibiting acetylcholinesterase and oxidants, Journal of Physiology & Pathology in Korean Medicine 22(1) (2008) 120-125.
- Lin, S.-K.; Yan, S.-H.; Lai, J.-N.; Tsai, T.-H. Patterns of Chinese medicine use in prescriptions for treating Alzheimer’s disease in Taiwan. Chin. Med. 2016, 11, 12. [Google Scholar] [CrossRef]
Figure 1.
Flow chart for the study subjects.
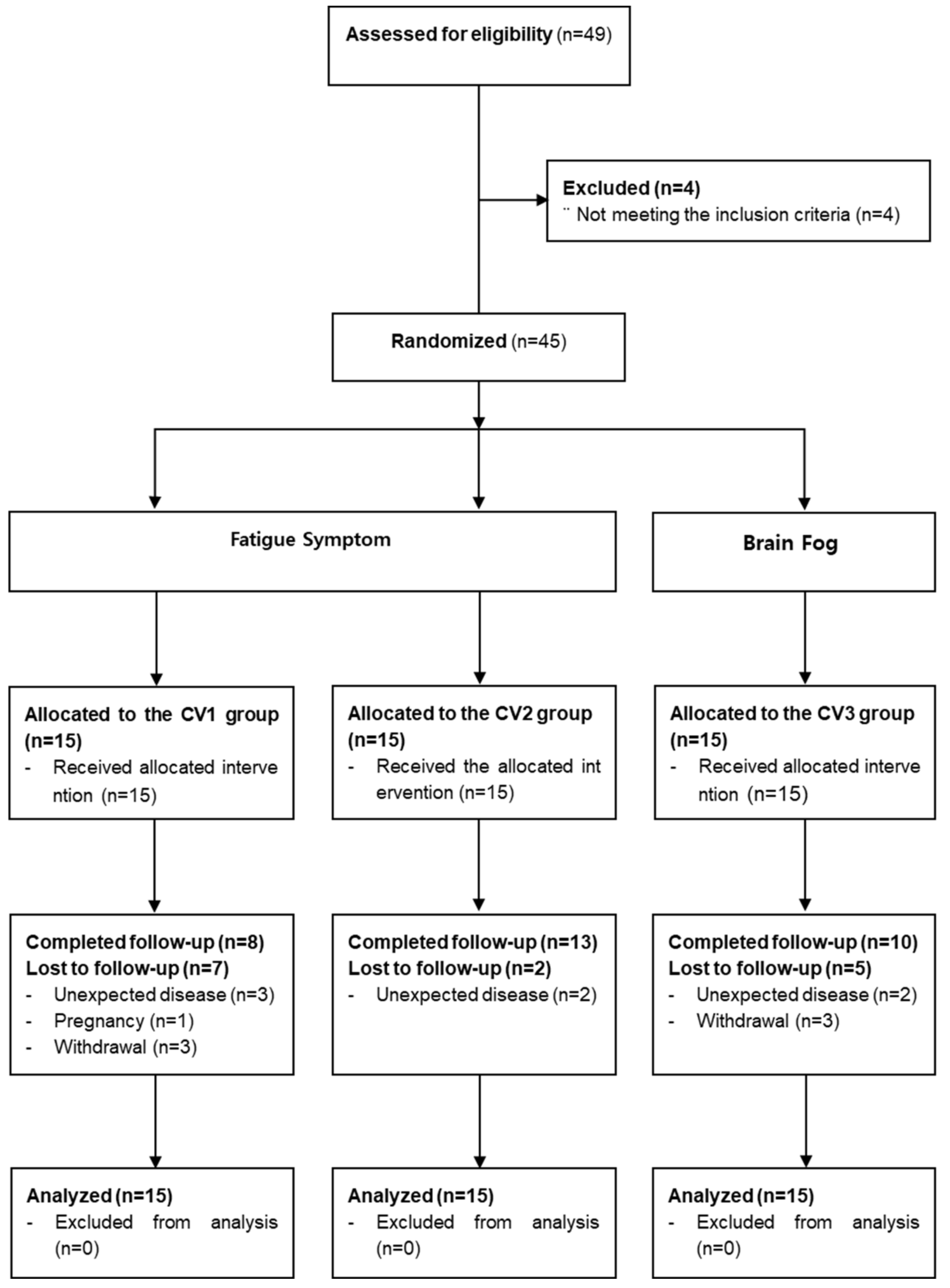
Figure 2.
Timeline for the study subjects.
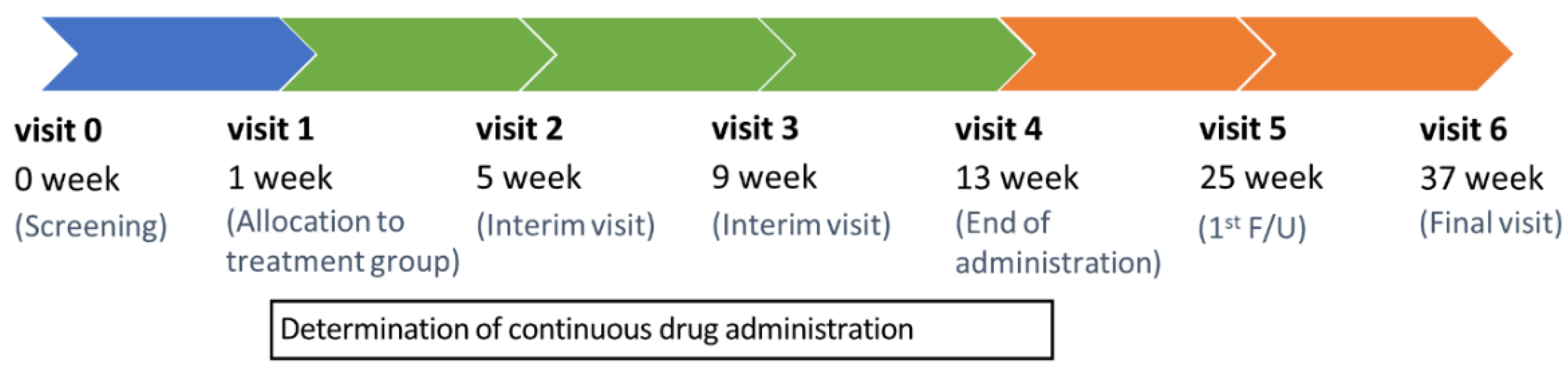

Table 1.
Schedule summary.
| Visit | 0 | V1 | V2 | V3 | V4 | V5 | V6 | UV * |
|---|---|---|---|---|---|---|---|---|
| Week | −7 | 1 | 5 | 9 | 13 | 25 | 37 | - |
| Visit Window (±Days) | - | 2 | ±7 | ±7 | ±7 | ±7 | ±7 | - |
| Informed consent for the study | ● | |||||||
| Demographic information | ● | |||||||
| Participation in other clinical trials | ● | |||||||
| Medical history | ● | |||||||
| Confirmation of diagnosis of COVID-19 infection | ● | |||||||
| Medication history | ● | |||||||
| Vital signs | ● | ● | ● | ● | ● | ● | ● | ● |
| Electrocardiogram | ● | ● | ● | |||||
| Laboratory test | ● | ● | ● | |||||
| Blood collection for immune response and metabolite analysis | ● | ● | ● | ● | ● | |||
| Pregnancy ** | ● | |||||||
| Evaluation of fatigue or “brain fog” | ● | |||||||
| CIS | ● | ● | ● | ● | ● | ● | ● | |
| VAS (0–100) score for fatigue or “brain fog” | ● | ● | ● | ● | ● | ● | ● | |
| Inclusion/exclusion criteria | ● | |||||||
| KM syndrome differentiation | ● | |||||||
| Prescription of herbal medicine *** | ● | ● | ● | |||||
| Drug adherence | ● | ● | ● | ● | ||||
| Check for combination therapy | ● | ● | ● | ● | ● | ● | ||
| ChFQ | ● | ● | ● | ● | ● | ● | ● | |
| EQ-5D-5L | ● | ● | ● | ● | ● | ● | ● | |
| PSQI-K | ● | ● | ● | ● | ● | ● | ● | |
| K-MoCA | ● | ● | ● | ● | ● | ● | ● | |
| CFQ | ● | ● | ● | |||||
| BDI | ● | ● | ● | ● | ● | ● | ● | |
| Digit span test in K-WAIS (DF, DB, and DF-DB) | ● | ● | ● | ● | ||||
| K-BNT-15 | ● | ● | ● | ● | ||||
| Adverse events check | ● | ● | ● | ● | ● | ● | ● |
●, check on visit * UV, unscheduled visit (), ** only fertile women, *** Evaluation for the continuation of herbal medicine administration at 5th and 9th weeks.
Table 2.
KM syndrome differentiation for allocation to treatment group.
| Fatigue | Cognitive Dysfunction | ||
|---|---|---|---|
| Code | BIT | KOG | CBD |
| Syndrome differentiation classification | Lung-Spleen Qi Deficiency | Dual Deficiency of Qi and Yin | Heart Yin Deficiency Heat |
| Symptom | Fatigue, appetite loss, cold sweat, shortness of breath, chest tightness, anxiety and others | Fatigue, dry cough and others | Forgetfulness, fever, insomnia, heart palpitation, stomatitis, tongue needles and others |
| Tongue diagnosis | Pale tongue, thin white fur | Dry mouth, dry tongue | Red tongue and low tongue coated |
| Pulse diagnosis | Vacuous, large, weak pulse/surging, large pulse | Fine pulse/vacuous, weak pulse | Fine, rapid pulse |
| Urine/feces | Difficult stool to pass/sloppy stool | Dry stool | Inhibited stool/sloppy stool |
Table 3.
Composition of Bojungikgi-tang, Kyungok-go and Cheonwangbosim-dan.
| Fomula / Product name |
Composition | Manufacturer / License Code |
Group / KM syndrome differentiation |
|
|---|---|---|---|---|
| Bojungikgi-tang (BIT, CV1) Kracie Bojungikgi-tang Extract Fine Granule |
Ginseng Radix | 4.0g | Kyungbang Pharmaceutical Co.,Ltd 201507212 |
Fatigue lung-spleen qi deficiency |
| Panax ginseng C. A. Meyer | ||||
| Atractylodis Rhizoma Alba | 4.0g | |||
| Atractylodes japonica Koidzumi | ||||
| Astragali Radix | 4.0g | |||
| Astragalus membranaceus Bunge | ||||
| Angelicae Gigantis Radix | 3.0g | |||
| Angelica gigas Nakai | ||||
| Zizyphi Fructus | 2.0g | |||
| Zizyphus jujuba Miller var. inermis Rehder | ||||
| Bupleuri Radix | 2.0g | |||
| Bupleurum falcatum Linné | ||||
| Citri Unshius Pericarpium | 2.0g | |||
| Citrus unshiu Markovich | ||||
| Glycyrrhizae Radix et Rhizoma | 1.5g | |||
| Glycyrrhiza uralensis Fischer | ||||
| Cimicifugae Rhizoma | 1.0g | |||
| Cimicifuga heracleifolia Komarov | ||||
| Zingiberis Rhizoma Recens | 0.5g | |||
| Zingiber officinale Roscoe | ||||
| Kyungok-go (KOG, CV2) Kyungbang Kyungokgo |
Rehmanniae Radix | 16.0g | Kyungbang Pharmaceutical Co.,Ltd 201708619 |
Fatigue dual deficiency of qi and yin |
| Rehmannia glutinosa Liboschitz ex Steudel | ||||
| Ginseng Radix | 2.5g | |||
| Panax ginseng C. A. Meyer | ||||
| Poria Sclerotium | 5.0g | |||
| Poria cocos Wolf | ||||
| Mel Honey | 16.6g | |||
| Cheonwang-bosim-dan (CBD, CV3) Soonsimhwan |
Rehmanniae Radix | 500.0mg | Hanpoong Pharmaceutical Co.,Ltd 200100075 |
“brain fog” heart yin deficiency |
| Rehmannia glutinosa Liboschitz ex Steudel | ||||
| Ginseng Radix | 62.5mg | |||
| Panax ginseng C. A. Meyer | ||||
| Scrophulariae radix | 62.5mg | |||
| Scrophularia buergeriana Miquel | ||||
| Salviae Miltiorrhizae Radix | 62.5mg | |||
| Salvia miltiorrhiza Bunge | ||||
| Polygalae Radix | 62.5mg | |||
| Polygala tenuifolia Willdenow | ||||
| Platycodonis Radix | 62.5mg | |||
| Platycodon grandiflorum A. De Candolle | ||||
| Poria Sclerotium | 62.5mg | |||
| Poria cocos Wolf | ||||
| Schisandrae Fructus | 125.0mg | |||
| Schisandra chinensis (Turcz.) Baillon | ||||
| Angelicae Gigantis Radix | 125.0mg | |||
| Angelica gigas Nakai | ||||
| Asparagi Radix | 125.0mg | |||
| Asparagus cochinchinensis Merrill | ||||
| Liriopis seu Ophiopogonis Tuber | 125.0mg | |||
| Liriope platyphylla Wang et Tang | ||||
| Thujae Orientalis Semen | 125.0mg | |||
| Thuja orientalis Linné | ||||
| Zizyphi Semen | 125.0mg | |||
| Zizyphus jujuba Miller var. spinosa Hu ex H. F. Chou | ||||
| Coptidis Rhizoma | 250.0mg | |||
| Coptis japonica Makino | ||||
*The dosage of each composition in the medicine is listed based on the raw material equivalent corresponding to a daily dose disclosed by the KFDA. Detailed information is provided at the address below.
Table 4.
Baseline characteristics.
| BIT (n = 15) | KOG (n = 15) | CBD (n = 15) | P-value | ||
| Age (mean, SD) | 43.80 (14.31) | 45.33 (12.57) | 51.33 (15.71) | 0.3656* | |
| Sex (M/F) | 9/6 | 8/7 | 6/9 | 0.6548** | |
| Body mass index (mean, SD) | 24.21 (3.56) | 23.17 (3.67) | 23.41 (3.07) | 0.8233* | |
| Final level of education | |||||
| Less than elementary school | 0 | 0 | 0 | 0.1742** | |
| Elementary school | 0 | 0 | 0 | ||
| Middle school | 0 | 0 | 0 | ||
| High school | 2 (13.33 %) | 5 (33.33 %) | 7 (46.67 %) | ||
| University or college | 13 (86.67 %) | 10 (66.67 %) | 8 (53.33 %) | ||
| Occupation | |||||
| Physical labor | 0 | 1(6.67 %) | 6(40.00 %) | 0.6692** | |
| Non-physical labor | 10 (66.67 %) | 11(73.33 %) | 8(53.33 %) | ||
| Others (unemployed, etc) | 5 (33.33 %) | 3(20.00 %) | 1(6.67 %) | ||
| Time duration since initial infection of COVID-19 (days, SD) | 8.87 (3.46) | 10.53 (4.61) | 10.20 (8.08) | 0.3310* | |
| NEWS* (SD) | 1.00 (2.54) | 2.47 (4.26) | 2.07 (4.03) | 0.3540* | |
| Symptom durations | |||||
| Fatigue (days, SD) | 89.47 (33.25) | 114.80 (92.11) | |||
| “Brain fog” (days, SD) | 119.13 (97.95) | ||||
| Baseline CIS score (mean, SD) | 100.60 (10.66) | 96.60 (15.36) | 105.4 (17.93) | 0.3331* | |
| Baseline VAS for fatigue symptom (mean, SD) | 76.87 (14.58) | 73.27 (9.05) | 70.33 (20.34) | 0.4900* | |
| Baseline VAS for “brain fog” (mean, SD) | 49.27 (24.86) | 40.60 (26.08) | 62.00 (24.65) | 0.1039* |
BIT: Bojungikgi- tang group; KOG: Kyungok-go group; CBD: Cheonwangbosim-dan group; NEWS: The national early warning score; CIS: Checklist individual strength; VAS: visual analogue scale; *Kruskal–Wallis test; ** Chi-squared test; SD: standard deviation.
Table 5.
Primary and secondary outcomes.
| BIT (n = 15) | KOG (n = 15) | CBD (n = 15) | P-value*** | |||
| Outcomes for feasibility assessment | ||||||
| Treatment success rate of VAS for fatigue (%)* | 12 (80) | 8 (53.33) | 7 (46.67) | 0.1431 | ||
| Treatment success rate of VAS for “brain fog” (%)* | 6(40) | 7 (46.67) | 2 (13.33) | 0.1225 | ||
| (n= 13) | (n= 14) | (n= 14) | ||||
| Medication adherence (%)** | 92.27(16.28) | 96.26 (15.75) | 85.66 (23.61) | |||
| Outcomes for fatigue symptoms | ||||||
| CIS (mean difference from baseline with 95% CI)** | ||||||
| At 5 weeks | -18.4, 95% CI[-26.89, -9.91] | -23, 95% CI[-33.03, -12.97] | -8.93, 95% CI[-16.27, -1.6] | 0.0181 | ||
| At 9 weeks | -27.2, 95% CI[-36.15, -18.25] | -25.93, 95% CI[-35.46, -16.41] | -15.53, 95% CI[-24.8, -6.27] | 0.0394 | ||
| At 13 weeks | -29.53, 95% CI[-40.96, -18.1] | -31.47, 95% CI[-43.47, -19.46] | -23.4, 95% CI[-34.79, -12.01] | 0.3391 | ||
| At 25 weeks | -30.2, 95% CI[-40.68, -19.72] | -25.33, 95% CI[-35.78, -14.89] | -26.87, 95% CI[-41, -12.73] | 0.7643 | ||
| At 37 weeks | -29.6, 95% CI[-39.11, -20.09] | -29.2, 95% CI[-39.72, -18.68] | -26.07, 95% CI[-40.95, -11.18] | 0.6119 | ||
| VAS for fatigue (mean difference from baseline with 95% CI)** | ||||||
| At 5 weeks | -28.87, 95% CI[-40.27, -17.47] | -22.27, 95% CI[-36.95, -7.59] | -6.47, 95% CI[-13.12, 0.18] | 0.0275 | ||
| At 9 weeks | -30.07, 95% CI[-42.12, -18.01] | -27.67, 95% CI[-43.02, -12.32] | -14, 95% CI[-25.25, -2.75] | 0.2353 | ||
| At 13 weeks | -32.53, 95% CI[-46.07, -19] | -30.13, 95% CI[-47.11, -13.16] | -16.73, 95% CI[-27.48, -5.98] | 0.2509 | ||
| At 25 weeks | -28.6, 95% CI[-40.93, -16.27] | -28.73, 95% CI[-43.44, -14.03] | -15.2, 95% CI[-24.56, -5.84] | 0.2537 | ||
| At 37 weeks | -32.27, 95% CI[-46.45, -18.08] | -20.07, 95% CI[-36.12, -4.01] | -15.67, 95% CI[-26.24, -5.1] | 0.2784 | ||
| ChFQ (mean difference from baseline with 95% CI)** | ||||||
| At 5 weeks | Total score | -12.73, 95% CI[-21.48, -3.99] | -11.33, 95% CI[-18.93, -3.73] | -5.27, 95% CI[-9.66, -0.87] | 0.1198 | |
| Physical health score | -9.13, 95% CI[-14.11, -4.15] | -7.2, 95% CI[-12.11, -2.29] | -1.53, 95% CI[-4.78, 1.71] | 0.0461 | ||
| Mental health score | -3.6, 95% CI[-8.53, 1.33] | -4.13, 95% CI[-7.42, -0.85] | -3.73, 95% CI[-5.44, -2.03] | 0.3220 | ||
| At 9 weeks | Total score | -20.07, 95% CI[-29, -11.13] | -15.2, 95% CI[-25.83, -4.57] | -5.6, 95% CI[-12.08, 0.88] | 0.0199 | |
| Physical health score | -13.8, 95% CI[-19.62, -7.98] | -9.87, 95% CI[-16.27, -3.46] | -2.27, 95% CI[-6.42, 1.89] | 0.0139 | ||
| Mental health score | -6.27, 95% CI[-10.36, -2.17] | -5.33, 95% CI[-9.86, -0.8] | -3.33, 95% CI[-6.34, -0.32] | 0.0174 | ||
| At 13 weeks | Total score | -23.67, 95% CI[-35.09, -12.24] | -21.27, 95% CI[-32.91, -9.62] | -10.93, 95% CI[-19.93, -1.93] | 0.0991 | |
| Physical health score | -17.27, 95% CI[-25.38, -9.15] | -14.2, 95% CI[-21.41, -6.99] | -6.27, 95% CI[-11.99, -0.54] | 0.0808 | ||
| Mental health score | -6.4, 95% CI[-10.98, -1.82] | -7.07, 95% CI[-11.98, -2.16] | -4.67, 95% CI[-8.3, -1.03] | 0.0469 | ||
| At 25 weeks | Total score | -22.4, 95% CI[-30.36, -14.44] | -17, 95% CI[-28.89, -5.11] | -14.6, 95% CI[-25, -4.2] | 0.4634 | |
| Physical health score | -16.53, 95% CI[-22.48, -10.59] | -11.93, 95% CI[-19.19, -4.67] | -8.73, 95% CI[-15.56, -1.91] | 0.2541 | ||
| Mental health score | -5.87, 95% CI[-9.23, -2.5] | -5.07, 95% CI[-9.97, -0.16] | -5.87, 95% CI[-10.13, -1.6] | 0.5669 | ||
| At 37 weeks | Total score | -25.53, 95% CI[-33.1, -17.97] | -18.27, 95% CI[-30.04, -6.49] | -14.93, 95% CI[-25.55, -4.32] | 0.2411 | |
| Physical health score | -19, 95% CI[-24.43, -13.57] | -12.6, 95% CI[-19.66, -5.54] | -8.27, 95% CI[-15.26, -1.28] | 0.0717 | ||
| Mental health score | -6.53, 95% CI[-10.45, -2.62] | -5.67, 95% CI[-10.59, -0.74] | -6.67, 95% CI[-10.75, -2.58] | 0.5402 | ||
| Outcomes for “brain fog” symptoms | ||||||
| VAS for “brain fog” (mean difference from baseline with 95% CI)** | ||||||
| At 5 weeks | -11.13, 95% CI[-32.3, 10.04] | -4.4, 95% CI[-22.91, 14.11] | -0.4, 95% CI[-9.84, 9.04] | 0.0477 | ||
| At 9 weeks | -7.73, 95% CI[-27.2, 11.73] | -9.33, 95% CI[-29.15, 10.48] | -3.87, 95% CI[-17.04, 9.3] | 0.0358 | ||
| At 13 weeks | -6.27, 95% CI[-26.71, 14.17] | -5.4, 95% CI[-27.98, 17.18] | 1.4, 95% CI[-10.8, 13.6] | 0.0472 | ||
| At 25 weeks | -6.73, 95% CI[-26.23, 12.77] | -7.27, 95% CI[-25.25, 10.71] | -5.87, 95% CI[-14.48, 2.75] | 0.2454 | ||
| At 37 weeks | -12.73, 95% CI[-32.8, 7.33] | -7.13, 95% CI[-24.32, 10.06] | -7.13(-15.81, 1.54] | 0.2193 | ||
| K-MoCA (mean difference from baseline with 95% CI)** | ||||||
| At 5 weeks | -0.53, 95% CI[-2.34, 1.28] | 0.20, 95% CI[-0.79, 1.19] | 0.87, 95% CI[-0.77, 2.50] | 0.5767 | ||
| At 9 weeks | 0.60, 95% CI[-1.10, 2.30] | 1.33, 95% CI[0.43, 2.24] | 1.27, 95% CI[-1.40, 3.93] | 0.5382 | ||
| At 13 weeks | 1.00, 95% CI[-0.51, 2.51] | 1.80, 95% CI[0.77, 2.83] | 1.13, 95% CI[-1.96, 4.22] | 0.3176 | ||
| At 25 weeks | 1.00, 95% CI[-0.29, 2.29] | 1.87, 95% CI[1.03, 2.70] | 0.80, 95% CI[-2.09, 3.69] | 0.1525 | ||
| At 37 weeks | 1.07, 95% CI[-0.30, 2.43] | 1.47, 95% CI[0.53, 2.40] | 1.00, 95% CI[-1.89, 3.89] | 0.4059 | ||
| CFQ (mean difference from baseline with 95% CI)** | ||||||
| At 37 weeks | -4.40, 95% CI[-7.57, -1.23] | -3.93, 95% CI[-11.57, 3.70] | -11.67, 95% CI[-21.07, -2.26] | 0.9368 | ||
| DF-forward (mean difference from baseline with 95% CI)** | ||||||
| At 13 weeks | 0.27, 95% CI[-0.27, 0.8] | 0, 95% CI[-0.47, 0.47] | -0.07, 95% CI[-0.46, 0.32] | 0.4532 | ||
| At 25 weeks | 0.07, 95% CI[-0.42, 0.56] | 0.47, 95% CI[0.11, 0.82] | -0.07, 95% CI[-0.86, 0.73] | 0.3573 | ||
| At 37 weeks | 0.33, 95% CI[-0.01, 0.68] | 0.47, 95% CI[0.11, 0.82] | -0.2, 95% CI[-0.96, 0.56] | 0.1230 | ||
| DF-backward (mean difference from baseline with 95% CI)** | ||||||
| At 13 weeks | 1.4, 95% CI[0.4, 2.4] | 0.4, 95% CI[-0.26, 1.06] | 0.8, 95% CI[-0.21, 1.81] | 0.2095 | ||
| At 25 weeks | 0.87, 95% CI[-0.04, 1.78] | 0.47, 95% CI[-0.31, 1.25] | 0.8, 95% CI[-0.23, 1.83] | 0.8091 | ||
| At 37 weeks | 1.13, 95% CI[0.13, 2.13] | 1.07, 95% CI[0.36, 1.78] | 0.8, 95% CI[-0.21, 1.81] | 0.4459 | ||
| K-BNT-15 (mean difference from baseline with 95% CI)** | ||||||
| At 13 weeks | 0.13, 95% CI[-0.06, 0.33] | 0.13, 95% CI[-0.06, 0.33] | 0.33, 95% CI[-0.21, 0.87] | 0.5933 | ||
| At 25 weeks | 0.13, 95% CI[-0.06, 0.33] | 0.2, 95% CI[-0.11, 0.51] | 0.07, 95% CI[-1.14, 1.28] | 0.6532 | ||
| At 37 weeks | 0.2, 95% CI[-0.11, 0.51] | 0.27, 95% CI[-0.06, 0.6] | 0.13, 95% CI[-1.07, 1.33] | 0.6417 | ||
| Other outcomes | ||||||
| EQ-5D-5L (mean difference from baseline with 95% CI)** | ||||||
| At 5 weeks | 0.01, 95% CI[-0.03, 0.04] | -0.03, 95% CI[-0.07, 0.02] | -0.04, 95% CI[-0.09, 0.01] | 0.1040 | ||
| At 9 weeks | 0.03, 95% CI[0, 0.06] | 0.01, 95% CI[-0.05, 0.07] | -0.01, 95% CI[-0.05, 0.04] | 0.2034 | ||
| At 13 weeks | 0.06, 95% CI[0.02, 0.11] | 0.02, 95% CI[-0.04, 0.07] | -0.01, 95% CI[-0.11, 0.08] | 0.1417 | ||
| At 25 weeks | 0.06, 95% CI[0.02, 0.11] | -0.01, 95% CI[-0.05, 0.03] | 0.03, 95% CI[-0.06, 0.11] | 0.3256 | ||
| At 37 weeks | 0.07, 95% CI[0.03, 0.11] | 0, 95% CI[-0.04, 0.05] | 0.03, 95% CI[-0.06, 0.12] | 0.4582 | ||
| PSQI-K (mean difference from baseline with 95% CI)** | ||||||
| At 5 weeks | 0.14, 95% CI[-1.16, 1.44] | -2.14, 95% CI[-3.10, -1.19] | 0.07, 95% CI[-1.14, 1.28] | 0.0364 | ||
| At 9 weeks | -0.85, 95% CI[-1.92, 0.22] | -3.07, 95% CI[-4.10, -2.05] | -0.64, 95% CI[-2.19, 0.90] | 0.0557 | ||
| At 13 weeks | -1.15, 95% CI[-2.96, 0.66] | -2.71, 95% CI[-3.76, -1.67] | -1.50, 95% CI[-3.35, 0.35] | 0.6978 | ||
| At 25 weeks | -1.25, 95% CI[-3.40, 0.90] | -2.08, 95% CI[-3.28, -0.89] | -1.55, 95% CI[-4.72, 1.63] | 0.9725 | ||
| At 37 weeks | -1.64, 95% CI[-3.72, 0.45] | -2.82, 95% CI[-3.94, -1.70] | -2.33, 95% CI[-4.51, -0.16] | 0.9540 | ||
| BDI (mean difference from baseline with 95% CI)** | ||||||
| At 5 weeks | -3.40, 95% CI[-5.50, -1.30] | -2.20, 95% CI[-3.77, -0.63] | -1.27, 95% CI[-4.87, 2.34] | 0.1882 | ||
| At 9 weeks | -3.27, 95% CI[-5.76, -0.77] | -3.40, 95% CI[-5.14, -1.66] | -4.13, 95% CI[-8.05, -0.21] | 0.8568 | ||
| At 13 weeks | -3.80, 95% CI[-6.86, -0.74] | -4.73, 95% CI[-6.87, -2.59] | -5.53, 95% CI[-11.21, 0.14] | 0.8669 | ||
| At 25 weeks | -4.60, 95% CI[-7.82, -1.38] | -3.80, 95% CI[-6.20, -1.40] | -6.53, 95% CI[-13.15, 0.08] | 0.9885 | ||
| At 37 weeks | -4.47, 95% CI[-7.38, -1.55] | -4.00, 95% CI[-6.62, -1.38] | -6.33, 95% CI[-11.20, -1.47] | 0.9212 | ||
BIT: Bojungikgi- tang group; KOG: Kyungok-go group; CBD: Cheonwangbosim-dan group; *Chi-squared test; **ANCOVA test (or Kruskal-Wallis test);*** p-value for group comparison; CI: confidence intervals.
Table 6.
Safety outcomes.
| BIT (n = 15) | KOG (n = 15) | CBD (n = 15) | P-value** | ||
| Number participants with adverse events (%)* | 5(33.33) | 1(6.67) | 4(26.67) | 0.2805 | |
| Type of AEs (n)* | |||||
| Back pain | 1 | 0 | 0 | ||
| Hypothyroidism | 1 | 0 | 0 | ||
| Common cold | 0 | 1 | 0 | ||
| High blood glucocorticoids level | 0 | 0 | 1 | ||
| Hypertension | 0 | 0 | 1 | ||
| Arthritis | 0 | 0 | 1 | ||
| Animal hair allergy | 1 | 0 | 0 | ||
| Insomnia | 1 | 0 | 0 | ||
| Rhinitis | 1 | 0 | 0 | ||
| Mucous cyst | 0 | 0 | 1 | ||
| Severity of AEs (n)* | |||||
| Mild | 5 | 1 | 4 | ||
| Moderate | 0 | 0 | 0 | ||
| Severe | 0 | 0 | 0 | ||
| Causality (n)* | |||||
| Drug-related AEs | 0 | 0 | 0 | ||
| Non-related AEs | 5 | 1 | 4 | ||
| Number of participants with normal laboratory test results at 13 weeks (n, %)* | BIT (n=13)*** | KOG (n=14)*** | CBD (n=14)*** | ||
| BUN | 10(76.92) | 9(64.29) | 12(85.71) | 0.4423 | |
| Creatinine | 11(84.62) | 14(100) | 14(100) | 0.0951 | |
| AST | 12(92.31) | 14(100) | 14(100) | 0.3171 | |
| ALT | 12(92.31) | 13(92.86) | 13(92.86) | 1.0000 | |
| ECG | 12(92.31) | 14(100) | 14(100) | 0.3171 |
BIT: Bojungikgi- tang group; KOG: Kyungok-go group; CBD: Cheonwangbosim-dan group; *Chi-squared test; **p-value for group comparison; ***Those who completed laboratory tests after treatment termination (13 weeks).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



